ABC
docz
Explore
Log in
Create new account
Download
Report
law, govt and politics
NEW ISSUE Ratings: Fitch: “AA-” BOOK ENTRY ONLY Moody’s: “Aa3”
Document 175072
2nd Annual Western PA Joint Professional Development Conference (PDC) SAVE THE DATE! Thursday,
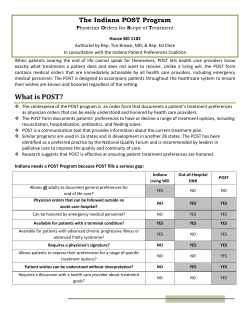
The Indiana POST Program
Document 3699
Document 39986
DISCOVER HOW TO CUT YOUR OPERATING COSTS
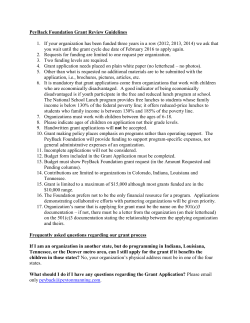
PeyBack Foundation Grant Review Guidelines
Building Learning Teams: How to Explicitly Create Teamwork Skills
How to contribute
No Shave Contest
© Copyright 2026
About abcdocz
DMCA / GDPR
Report