
1 2 5 key
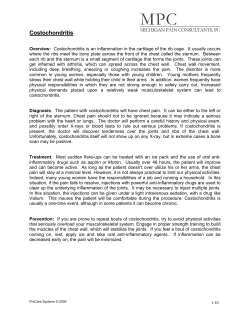
Nursing Practice Review Cardiology Keywords: Chest pain/Assessment/ Coronary heart disease ●This article has been double-blind peer reviewed Chest pain is a complex symptom with a variety of causes. It is essential that health professionals have good communication skills to ensure an accurate diagnosis Is chest pain always an emergency? In this article... auses of chest pain C Tools used to assess chest pain Case studies to illustrate chest pain assessment Author Helen Gaunt is cardiac nurse specialist, Rapid Access Chest Pain Clinic, University Hospitals of Leicester Trust. Abstract Gaunt H (2014) Is chest pain always an emergency? Nursing Times; 110: 44, 12-14. Chest pain is a complex symptom, which has a number of underlying causes. Accurate assessment is vital to ensure patients receive appropriate and timely care. This article provides an overview of the causes of chest pain and key features of the assessment process. Alamy I n the UK around 80,000 people die of coronary heart disease (CHD) each year (Townsend, 2012). One of the signs of CHD is chest pain, which 20-40% of people experience at some time in their life (Ruigomez et al, 2006). However, chest pain is a complex symptom with a number of causes, some of which are non-cardiac. Careful assessment is required to ensure patients receive appropriate management. The National Institute for Health and Care Excellence (2010) stresses the importance of “accurate” and “fast” diagnoses of chest pain, ensuring patients are treated appropriately and promptly. In our Rapid Access Chest Pain Clinic we see over 2,500 people each year with chest discomfort; roughly half have symptoms that are unlikely to be cardiac in origin. These patients are discharged to their GP to investigate alternative causes. Differential diagnosis of chest pain is given in Table 1. Causes of chest pain range from angina and acute myocardial infarction (MI) to more benign and self-limiting problems, such as musculoskeletal pain, and gastrooesophageal symptoms such as heartburn (Ebell, 2011). Assessment NICE (2010) recommends a structured assessment using algorithms to ensure high-risk patients are identified and treated appropriately and promptly. It also highlights the “red flags” that those carrying out the assessment should be aware of and suggests management plans, including: » Raised biochemical markers; » Electrocardiogram changes; » Signs the patient is haemodynamically unstable; » Associated symptoms such as nausea and vomiting, breathlessness or marked sweating. Albarran (2002) suggests nurses’ assessment of chest pain can be divided into: » Diagnosis; » Therapeutic care; » Conveying humanistic concern; » Improving and maintaining the nurse–patient relationship; » Accountability and legal implications. Comprehensive assessment and history taking is essential to ensure accurate diagnosis. Each episode of chest pain should be taken on its individual merit, irrespective of whether the patient has been assessed for chest pain in the past (Zitkus et al, 2010). Patients with chest pain do not always fit into a typical pattern of symptoms, particularly when they are anxious. Pain must be considered along with investigations including ECG and observation of the blood pressure, pulse, respiratory rate and oxygen saturations. Fass and Achem (2011) highlight that patients with a diagnosis of non-cardiac chest pain often have higher levels of anxiety and feel their symptoms are “less controllable” than those with a cardiac condition. It is important to listen carefully to 12 Nursing Times 29.10.14 / Vol 110 No 44 / www.nursingtimes.net 5 key points 1 80,000 people die of coronary heart disease each year Chest pain is a common presenting symptom in primary care There are non-cardiac causes of chest pain Accurate assessment is vital to ensure correct management A variety of assessment tools are available to assess chest pain 2 3 4 5 fig 1. Levine’s sign Nursing Times.net For articles on cardiology, go to nursingtimes.net/cardiology Table 1. differential diagnoses of chest pain Diagnosis Symptoms/characteristics Myocardial infarction ● Severe, band-like, crushing, gripping, squeezing pain ● Sudden onset ● May be associated with shortness of breath, nausea, sweating or dizziness ● Patients may also report a fear of impending doom Angina ● Tightness, squeezing, ache or crushing pain that may radiate to the neck, jaw, arms and through to the back ● Commonly occurring with exertion and usually relieved within minutes of rest ● Often worse when exercising in colder weather or after eating Musculoskeletal chest pain ● Can be severe at times ● Often a localised tenderness, which is made worse with moving or twisting and tends not to be related to exertion ● Commonly reproduced or made worse by palpation over areas of the chest wall ● Relieved by analgesics, such as non-steroidal antiinflammatory drugs Gastro-oesophogeal reflux disease ● Burning pain usually in the centre of the chest may radiate through to the back and up to the throat ● May be associated with acid reflux ● Linked to food and posture ● Relieved by dietary changes, antacids or proton pump inhibitors Non-organic pain ● The patients may pinpoint localised areas of discomfort, which may be left or right sided ● The symptoms are not usually linked to exertion ● Often related to anxiety and stress and occurs in younger people, particularly when there is a family history of heart disease each patient’s description of their problem during the initial assessment. This assessment should consider risk factors for CHD, gastro-oesophageal reflux disease, musculoskeletal chest pain and past medical history. NICE (2010) recommends an initial clinical assessment followed by diagnostic tests if these are indicated. Rick factors for CHD are outlined in Box 1. It is essential to assess the impact of the pain on patents’ lives. Ask them if they are still able to work and continue with their usual routine or whether they have modified it consciously or subconsciously. A variety of tools can be used as part of a chest pain assessment; selection is often based on individual preference (Oriolo and Albarran, 2010). As an example, mnemonics (Box 2) can be used to help guide assessment. The numerical visual analogue scale is often used to assess pain. The patient is asked to pick a number between 0 and 10, where 0 = no pain and 10 = the worst pain imaginable.This is typically used as an adjunct to the assessment as it identifies the pain as being whatever the patient says it is (McCafferey, 1979) and, as such, is highly subjective. Albarran (2002) suggests that although pain scores are quick and easy to use, they only measure intensity; in addition, older people may struggle to use them as they may find it difficult to quantify pain. The use of open-ended questions, good listening skills and acknowledging patients’ concerns regarding their health all help to obtain accurate information from patients and enhance the nurse– patient relationship (Albarran, 2002). Reading patients’ description of their condition back to them is a good way to ensure the facts are accurate and allows the opportunity for both parties to clarify any misunderstandings. Leicester is a large multicultural city and many of our patients do not speak English as a first language. Misunderstandings may occur with the words we use to describe symptoms. For example, we may say “in slight discomfort” but some patients may describe their pain as “slowly”, meaning a small amount. Access to translators, along with good verbal and Box 1. Risk factors for Coronary Heart disease ● Hypertension ● High cholesterol ● Diabetes ● Smoking ● Lack of exercise ● Overweight or obese ● Family history of coronary heart disease ● Ethnic background, for example rates of CHD in the UK are highest in South Asian communities non-verbal communication, is essential in these circumstances. Non-verbal cues Assessment should not rely on verbal communication but should also take into account non-verbal cues. When asked to describe their chest pain people often use hand movements to help illustrate their symptoms. Patients with ischaemic chest pain often place a clenched fist in the middle of their chest to represent their description of “gripping”. This is known as Levine’s sign (Fig 1). Edmondstone (1995) studied individuals admitted to coronary care and found that if patients used the Levine sign to describe their pain, there was a 77% chance the pain was ischaemic. Patients with pain associated with oesophageal problems tended to point up and down through the centre of their chest (Edmondstone, 1995), while fingertip pinpointing to localised areas over the chest wall is linked to musculoskeletal causes of chest pain. Case studies Case study 1 Harry Brown* is 49 years old and usually fit and well. He is anxious as his father had his first MI at the same age and mentions this repeatedly during the assessment. He has no other risk factors for CHD. Mr Brown presents with a history of new-onset, upper-left-sided chest pain after heavy gardening. The pain does not radiate and there are no other symptoms. The pain is almost constant, is worse when he moves his left arm and is eased a little with the help of regular paracetamol and non-steroidal anti-inflammatory drugs. Mr Brown rates the constant pain at 4/10 on the pain scale but says it can go up to 7 or 8 if it is particularly troublesome. The pain is not associated with exertion. He both feels and looks very anxious and worried. His blood pressure, pulse and www.nursingtimes.net / Vol 110 No 44 / Nursing Times 29.10.14 13 Nursing Practice Review respirations are recorded, as is an ECG and oxygen saturation levels. Using the CHEST mnemonic (Box 3): » C – Commenced in the past few weeks; » H – Symptoms occurred after heavy gardening, low risk for CHD; » E – No other associated symptoms; » S – Localised upper-left-sided chest pain and no radiation of pain; » T – Pain is almost constant. After the assessment the most likely cause of the pain is musculoskeletal. Mr Brown requires no further cardiac assessment and is advised to continue with simple pain relief, rest as able and to see his GP if there is no sign of improvement. Case study 2 Barbara Chaney* is 60 years old and woman and reported a recent onset of chest discomfort over the past few months. She attended her GP recently for an annual health check and decided to mention it. A full history of the complaint was obtained along with her blood pressure, pulse, ECG results, oxygen saturations and respiratory rate. Ms Chaney says what she feels is not a pain but more of an ache or tightness. The discomfort is across the centre of her chest and radiates up to her neck and jaw and, on occasion, into her left arm and she feels slightly short of breath. Symptoms occur most days. She has noticed them when she walks her dog and they usually start as she walks up an incline. If she stops for a few minutes the symptoms quickly subside and she is able to continue walking, albeit at a slower pace. She has noticed these same symptoms when climbing the stairs at home but she has neither had pain at rest nor pain for prolonged periods. Ms Chaney gave up smoking 25 years ago and has type two diabetes, which is controlled with diet. Her mother developed CHD at a similar age and died of an MI aged 65 years. Her latest cholesterol level was measured at 6mmol/L (5mmol/L is considered normal but a level of 4mmol/L is recommended for cardiac patients) (NHS Choices, 2013). Using the PQRST mnemonic (Box 3): » P – Pain always on exertion and relieved within minutes of rest; » Q – Quality of pain described as more of an ache or tightness; » R – Radiates to neck, jaw and arm; » S – Symptoms occur across the centre of her chest; » T – Symptoms started a few months previously and were initially not particularly troublesome. However, Ms Chaney has noticed that they Box 2. Mnemonics used to guide assessment CHEST ● C Commenced – When? ● H History – Is there evidence of risk factors for CHD or triggers? ● E Extra – Are there additional symptoms, that is nausea, shortness of breath? ● S Stays – Is it short lived? Does the pain radiate to the jaw, arms or throat? ● T Timing - How long does it last? Source: Jones et al (2002) PQRST ● P Provocation/palliative – What triggers the pain and what relieves the pain? ● Q Quality – Description: is it stabbing or sharp? How bad is it? ● R Radiation – Does the pain radiate to the shoulder arms or jaw? ● S Site – What is the exact site of the pain? ● T Timing – When did the pain start? Was onset sudden or gradual? Was it short term or long lasting? Source: Steadman (2010) have increased in frequency. On assessment the most likely cause of her symptoms is angina. Ms Chaney is prescribed 75mg aspirin as an antiplatelet, a beta-blocker to reduce her heart rate and cardiac workload, and a statin to help achieve a total cholesterol level of 4mmol/L or below. A glyceryl trinitrate (GTN) spray is also prescribed to relieve symptoms of pain. She is given advice regarding pain and symptoms management and use of the GTN. Ms Chaney is also referred to the cardiac rehabilitation programme for ongoing support, exercise and lifestyle advice. Documentation Clear, precise documentation of a chest pain assessment is vital for the initial and future management of patients presenting with symptoms. Ensuring that care is consistently documented enables patients’ symptoms to be compared over time and helps to identify any improvement or deterioration in symptoms. Conclusion Experiencing chest pain can be a frightening experiencing. The role of the cardiac nurse specialist in assessing individuals promptly and confidently, providing reassurance and education as support is vital. It can take years to develop the skills and ability to assess people well – chest pain assessment is, at times, challenging and complex. Assessing people who may find it difficult to articulate their experiences, in part due to anxiety and fears or because of language barriers, means that nurses need to quickly develop and build a trusting relationship, eliciting clear, precise facts, 14 Nursing Times 29.10.14 / Vol 110 No 44 / www.nursingtimes.net that will enable speedy, accurate and appropriate treatment. NT *Patients’ names have been changed. References Albarran J (2002) The language of chest pain. Nursing Times; 98: 4, 38-41. Townsend N (2012) Coronary Heart Disease Statistics. London: British Heart Foundation. tinyurl. com/BHF-stats-CHD Ebell MH (2011) Evaluation of chest pain in primary care patients. American Family Physician; 83: 5, 603-605. Edmondstone WM (1995) Cardiac chest pain: does body language help the diagnosis? The BMJ; 311: 1660-1661. Fass R, Achem SR (2011) Noncardiac chest pain: epidemiology, natural course and pathogenesis. Journal of Neurogastroenterology and Motility; 17: 2, 110-123. Jones G et al (2002) Emergency Nursing Care: Principles and Practice. London: Greenwich Medical Media. McCafferey M (1979) Nursing Management of the Patient with Pain. Philadelphia, PA: JB Lippincott. NHS Choices (2013) Diagnosing High Cholesterol - Getting a Cholesterol Test. tinyurl.com/ CHDcholesterol National Institute for Health and Care Excellence (2010) Chest Pain of Recent Onset: Assessment and Diagnosis of Recent Onset Chest Pain or Discomfort of Suspected Cardiac Origin. tinyurl. com/NICECG95 Oriolo V, Albarran JW (2010) Assessment of acute chest pain. British Journal Cardiac Nursing; 5: 12, 587-593. Ruigomez A et al (2006) Chest pain in general practice: incidence, comorbidity and mortality. Family Practice; 23: 2, 167-174. Steadman P (2010) Knowing when chest pain is an emergency. Independent Nurse; 4: 19. Tough J (2004) Assessment and treatment of chest pain. Nursing Standard; 18: 37, 45-53. Zitkus B (2010) Assessing chest pain accurately. Nursing; 40: 1-6. For more on this topic go online... Factors in attendance at cardiac rehabilitation B it.ly/NTCardiacRehabAttend









© Copyright 2026