ABC
docz
Explore
Log in
Create new account
Download
Report
No category
Open the publication - UEF Electronic Publications - Itä
CrEATe brochure - Catering Services
Morning Announcements for Middle/High School
Exposure to air pollution in the first year of life increases
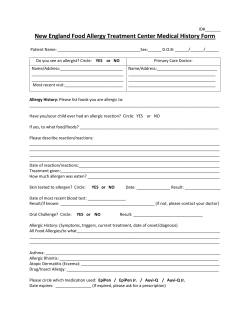
Patient Medical History - New England Food Allergy Treatment Center
Thomas Ridley Allergen Compliance Guide (EU FIC)
What Parents Need to Know One in 13 kids
Allergy Diagnostic Market To 2022 – Industry Analysis, Trends: Grand View Research, Inc.
Document 368858
How to help owners understand atopic dermatitis and its management
March 2015
© Copyright 2026
About abcdocz
DMCA / GDPR
Report