
Evidence Based Practice Regarding Venous Catheterisation: Comparison
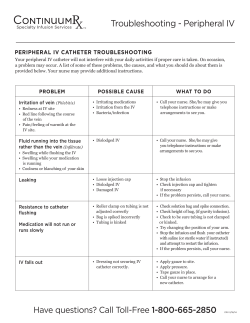
Evidence Based Practice Regarding Venous Catheterisation: Comparison between the UK, Greece & Lithuania Sophie Porter, Josephine Guzman, Ben Lambton, Magda and Lauryna Aims of the presentation • • • • • What is venous cannulation? Why do we use it? The risks on insertion and management Complication statistics The guidelines on insertion and management in the UK, Greece and Lithuania • Conclusion of international differences • Discussion and scenarios with the audience INTRODUCTION What is Venous Cannulation • Peripheral intravenous cannulation is a procedure in which the patient’s skin is punctured with a needle to allow insertion of a temporary plastic tube into a vein (Jackson, 2003) • The peripheral IV cannula is usually inserted into the metacarpal vein on the back of the hand or a vein in the lower arm, either the cephalic or basilic vein. (Dougherty, 2008) Image from:dermatologic.com.ar Why do we use venous cannulation? • Peripheral vascular access devices (VADs) can be inserted for intravenous (IV) access for medication, fluid, blood or nutrient delivery, haemodynamic monitoring or blood sampling (Lavery and Ingram, 2006) Cannula placement • When selecting a vein to perform peripheral venous cannulation consider: – Patient’s age – Patient’s preference – Patient’s activity – Previous medical history – Presence of a shunt or graft – Time of therapy – Type of solution – Condition of vein – Cannula size (Ahmed, n.d) Risks of cannulation and what to look out for Infection Haemmorhage Haematoma Vaso-vagal episode Needle phobias Catheter embolism Pain Nerve damage Arterial puncture Allergies Needle stick injuries The RCN IV Therapy Forum (2010) Risks after insertion • • • • • • • • Phlebitis- septic, mechanical, chemical Infection Drug reaction (allergy) Infiltration Extravasation Thrombosis/ Embolism Speed shock Fluid overload The RCN IV Therapy Forum (2010) Infection statistics related to cannulation • UK; A survey conducted that 5% of a total of 554 patients on 20 general wards with a cannula inserted developed site infection. The survey concluded that the low rate is due to the 72hrs policy of changing the cannula, thus validates the 72hr policy (Creamer et al 2003). UK Governing registration bodies in different countries • UK- Nursing and Midwifery Council (NMC) – provide a RN pin on completion of degree/diploma. Code of Conduct (2008) must be respected and adhered to by all registered nurses. There is also the “Guidance on Professional Conduct for Student Nurses and Midwifes” (2011) • Registered nurses must ensure their knowledge and skills related to the management of PVCs are up to date and evidence based (Nursing and Midwifery Council, 2008) Who performs cannulation in UK? Doctors Phlebotomists Nurses after training Health care assistant after training for an instance in A&E Training for nurses in the UK Registered nurses undertaking the insertion of vascular access devices will have undergone theoretical and practical training in the following: Anatomy and physiology of the circulatory system, in particular, the anatomy of the location in which the device is placed including veins, arteries and nerves and the underlying tissue structures • Assessment of patients’ vascular access needs, nature and duration of therapy and quality of life • improving venous access, for example the use of pharmacological and non-pharmacological methods • Selection of veins and problems associated with venous access due to thrombosed, inflamed or fragile veins, the effects of ageing on veins, disease process, previous treatment, Lymphoedema or presence of infection • Selection of device and other equipment • Infection control issues (hand-washing, skin preparation) • Pharmacological issues (use of local anaesthetics, Management of anxious patients, management of Haematoma, phlebitis, etc.) Hence, the nurse inserting devices and/or providing infusion therapy must be competent in all clinical aspects of infusion therapy and have validated competency in clinical judgement and practice, and practice in accordance with the NMC’s Code: that is, they will maintain their knowledge and skills (Collins et al., 2006; Hyde, 2008; NMC, 2008). Training contd. Nurses undertaking the administration • local and systemic complications of infusion therapy and care and • infection control issues management of vascular access • use of equipment, including infusion devices will have undergone equipment theoretical and practical • drug administration training in the following aspects • risk management/health and safety • legal, professional and ethical issues • care and management of vascular • anatomy and physiology access devices • fluid balance and blood administration • mathematical calculations related to medications • pharmacology and pharmaceutics (Lonsway, 2001; NICE, 2003; Hyde; related to NMC, 2008a; Hyde, 2008) reconstitution and administration UK Peripheral Venous Cannulation (PVC) Guidelines • High Impact Intervention: Peripheral intravenous cannula care bundle (Department of Health (DH) , 2011) • Health Protection Scotland (2012)- Targeted literature review: What are the key infection prevention and control recommendations to inform a PVC maintenance care quality improvement tool? What do the guidelines say? Insertion: • Ensure clinical indication for PVC • Hand hygiene is performed immediately prior to PVC insertion • Skin antiseptic containing 70% ispropyl antiseptic is used to clean skin and left to dry prior to insertion studies have advocated that proper skin preparation before IV medication (2% chlorhexidine and 70% alcohol) for 30 seconds has shown to reduce infection(Aziz 2009:244; Hadaway & Millam 2005:4) • Aseptic technique is maintained throughout • Sterile transparent, semi-permeable dressing is used to cover catheter site. Date should be written on dressing What do the guidelines say? Management: • Clinical need for PVC reviewed and documented each day • The need for IV drugs is reviewed daily by medical staff and switched to oral as soon as possible • Hand hygiene is performed prior to line access • PVC site is assessed using VIP score and removed where phlebitis and infection are clinically indicated • PVC dressing is in tact • 70% isopropyl alcohol is used to clean access ports for at least 15 seconds prior to access. • Remove after 72-96 hours unless clinically indicated sooner or if there is limited venous access it may be left in longer. • (Health Protection Scotland, 2012) and Department of Health (2011) Daily Assessment of Peripheral Venous Catheters (PVC) in the UK • CDC guidelines recommend replacement of peripheral intravenous (IV) catheters every 72 to 96 hours which is based on evidence which showed that the longer a PVC is in situ the greater the risk of complication. (Health Protection Scotland, 2012) • However a cochrane review has been published since which concluded that there was insufficient evidence of benefit from routinely removing catheters every 72 to 96 hours and suggested that catheters including PVCs, should be changed on clinical indication (Webster, et al, 2010) • Visual Infusion Phlebitis Scale (Jackson, 1998) -Assists nurses in asessing and managing PVC sites (Royal College of Nursing (RCN), 2012) • RCN (2010) and Health Protection Society (HPS) (2012) recommend that PVC sites are checked at least on a daily basis as well as during infusion of drugs and fluids. • If two or more signs indicative of phlebitis are present (Jackson, 1998), or if the PVC is not functioning, it should be removed immediately; it should only be resited if the clinical need for a PVC remains (HPS, 2012). Visual Infusion Phlebitis Scale (Jackson, 1998) Is the VIP score still reliable and valid? • Study by Gallant and Schaultz (2006) • Descriptive correlational design • Aim : to look at the effectiveness of the VIP score in determining when to remove a catheter to reduce rates of phlebitis • 851 PIV sites in 513 patients were monitored • Results: overall found to be clinically useful because it not only provided descriptions but also suggested actions by the nurse based on the scale score. Was considered to be a valid and reliable measure for determining when a PIV catheter should be removed. • Considerations: Inter user reliability – persons using the VIP score must have expert knowledge in using it for assessment and management purposes. Documentation of PVCs in the UK • Documentation plays an important role in the audit process, facilitates the generation of measurable realtime data (HPS, 2012; DH, 2011), and has been found to improve staff compliance with care bundles. • Document date, reason for insertion, catheter size, operator undertaking insertion and if insertion was high risk with signature (DH, 2011) • Document in notes details of date and time of removal of cannula, operator undertaking removal with signature and phlebitis score (RCN, 2012) Anecdotal practices in PVC insertion in the UK • Torniquet or manual compression by assistant (Mbmalu and Banerjee, 1999) Restricting blood flow for a short time (2-3 minutes) causes venous dilation and increased blood volume. • Gravity – dangling arm below level of heart helps to dilate veins (Alberta Health Services, 2004) • Gentle slapping of the skin overlying the vein (Mbmalu and Banerjee, 1999) contradicted by evidence that suggests slapping causes reflex vasoconstriction via pain receptors. • Using warming mittens for 10-15 minutes- Study by Lenhardt et al (2002) concluded that the use of carbon fibre heat mittens on lower arm and hand PVC insertions decrease the time staff spend inserting cannulas, reduce supply costs, and improve patient satisfaction • Spray GTN spray to vasodilate the veins- personal experience – no evidence base of using in cannulation but there is evidence to support that Glyceral Trinitrates cause vessel dilation- we know as we use commonly in angina and heart conditions! – CLINICAL EXPERTISE (LEVEL 5 EVIDENCE) LITHUANIA Nursing education in Lithuania • The general nurse qualification is acquired at higher education after completion of a nursing degree program. An overseas nurse qualification is gained which is recognised by Lithuanian legal acts. • This qualification gives you the right to engage in the general practice of nursing to a person of the Republic of Lithuania. This is according to the law, that you must be trained as a nurse and to hold a professional qualification • General nurses are guided by the Republic of Lithuania laws and regulations, the standard of medicine, the place of employment, statutes (regulations) and the internal rules of their job descriptions (MN 2011). Registration body for nurses: LITHUANIA medical standards MN 28 • This rule establishes the medical nurses professional activities, rights, duties, powers and responsibilities. • This medical standard is mandatory for all Republic of Lithuania nurses, their employers, as well as institutions in developing and improving the specialists and controlling their activities (Sukys 2011). Rights, duties, competencies and responsibilities in Lithuania • The general practice nurses who make mistakes, are guilty of negligence, improper assigned functions or violation of the requirements of bioethics, as well as the obligations of the Republic of Lithuania, are responsible to the MN where they are exceeding the statutory procedure (MN 2011). Rights, duties, competencies and responsibilities in Lithuania • Cannulation must only be carried out by a member of medical staff (doctors) or appropriately experienced NURSES. • Peripheral venous cannulation should only be performed by a member of staff who is competent and confident to perform or during a period of supervised practice by an assessor who is competent (NMC 2002). Guidelines for pheripheral venous cannulation in Lithuania Basic steps: • To check the name of the patient against the patient’s wristband. • To confirm the name of the patient verbally. • If verbal identification of identity is not possible, check patient’s identity with a second practitioner. • To assess individual needs of the patient. • To select where appropriate a suitable person for assisting with the procedure. Guidelines for pheripheral venous cannulation in Lithuania • To follow infection control precautions • To prepare and demonstrate correct and appropriate use of equipment. • To identify a suitable vein and position the patient appropriately. • To insert a peripheral cannula correctly (Addison 2003 ). Guidelines for pheripheral venous cannulation in Lithuania • To flush the cannula with 0.9% saline using a 10ml syringe. • To fixate the cannula using the appropriate dressing. • Safely dispose of all equipment according to Trust policies. • To document the procedure correctly (Addison 2003) Documentation You will see lots of different charts, forms and documentation. Every hospital, care home and community nursing service will have the same basic ones, but with small variations that work best locally. Documentation Catheter insertion documentation include: • Is the individual patient in any form of localised discomfort or pain? • The results of a risk assessment prior to Catheterisation. • Consent obtained for the procedure; • If the insertion was easy or difficult • Indications used to ensure catheter was inserted correctly . (Rando, 2005) GREECE Ε.Ν.Ε (Nurses Association ,Greece) • E.N.E is the public law entity,totally selfgoverning,which is under the supervision of the Ministry of Health. • It is also the government's and public establishments and undertakings adviser,which supervise on the items of primary,secondary and tertiary health care and health policy. • All nurses of higher education are registered members . Venous cannulation in Greece • According to the 4th Health Region of Macedonia & Thraki, inserting a venous catheter is defined as a nursing process. A nursing student is trained in venous cannulation during the second year of their study, either in the laboratory or during clinical practice at hospital. Greek Guidelines for venous cannulation-preparation • perform hand hygiene and organize the equipment • confirm patient's identity and explain the procedure to obtain consent • select size and type of venous catheter • Select with top priority left hand for right handed and respectively vica versa • Wear gloves and choose vein(mainly forearm,then wrist or dorsal surface of palm) *avoid volute or manifold veins Procedure guidelines for venous cannulation in Greece • • • • • • • • • fit elastic strapping 5-10cm from the cannulation point(carefully to the elderly and if it needed over the clothes) *do tied more than 90 seconds Check for presence of arterial pulse locate the exact site for venipuncture and clean with a solutione.g chlorrexidinis Use your thumb and apply slight tendency to the distal end of vein for stability Start from an angle 30 and continue with reduction of the angle during the insertion ease the catheter in to the vein gradually pulling the needle out at the same time Inserting all the catheter,apply slight tendancy to its the distal end stabilize and connect any lines as appropriate After two failed attempts you must ask the assistance of someone experienced Update and sign the patients hospital card monitoring of the venous catheter following insertion - Greece • overview gateway of venous cathetr observing for redness,edema,outflow etc and dressings on a daily basis • If there are no points of phlebitis change venous catheter every 96 hours • Change dressing in the case of ablation,fluid, blood escaping or moisture • Instruct the patient to observe for possible signs or symptoms of phlebitis and inform the nurse if they are concerned Nursing documentation • Recorded in patient's hospitalization card: the date of catheter placement the point of catheter placement the type and the size of the used catheter the name and the signature of the nurse which perform the vein cannulation also... • Recording in a prominent spot on the suffix: the date of catheter placement • The following is also documented in patients notes : • the level of cooperation with the patient • dressings that are used • the level of understanding instructions on the mobility restrictions as a result of catheterization • The instructions given about subsequent changes on venous catheter or suffix Conclusion • • • • As you can see the procedure for insertion of a peripheral venous catheter is much the same in all three countries. However , in the UK the guidelines are national, provided by two very reputable bodies and are published, adhered to and used by all medical staff, allied health professionals and nurses which are trained. Both Greece and Lithuania have local trust policies and university guidelines, and so they may vary from trust to trust. The main differences appear in the management and documentation. Although all three countries follow the 72- 96 hour rule the main difference is the use of the VIP score in the UK. Perhaps in Greece and Lithuania nurses are trusted to observe for phlebitis through clinical judgement and expertise. However in the UK there is what has been proven to be a very useful tool in reducing phlebitis and aiding a nurse in determining when to remove a cannula and what steps to make next. Despite the fact that it is dated. Other differences are in who performs cannulation, and the training undertaken. As previously discussed, in the UK you have to obtain a licence or training to perform such a skill. It is not something taught to you as a student nurse. This is much the same in countries like the US and Finland. However in both Lithuania and Greece, student nurses are taught in skills laboratories and on clinical placement. They are also allowed to perform this procedure on patients under the supervision of a registered nurse. scenarios Scenario 1 • A foreign male patient who does not speak your language is admitted to the ward where you work. He requires a cannula to be inserted to administer IV antibiotics promptly. However he is very scared of needles and does not understand why he needs a cannula. • How do you solve this situation and explain the reason for and the risks of having a cannula inserted? • And how do you make sure he understood? Scenario 2 • A female patient is admitted and requires IV fluids. She does not mind to have a cannula inserted, however she does not understand what to look out for and she is moving her arm and touches both the cannula and the bag of fluids all the time which interrupts the flow and increases risk of irritation to her skin. • How do you explain to her that she must not do this? • And how do you make sure she understood? References • • • • • • Collins M, Phillips S and Dougherty S (2006) A structured learning programme for venepuncture and cannulation, Nursing Standard, 20 (26), pp.34-40. (III) Nursing and Midwifery Council (2008b) The code:standards of conduct, performance and ethics for nurses and midwives, London: NMC. Hyde L (2008) ‘Legal aspects of IV Therapy’, in Dougherty L and Lamb J (editors) Intravenous therapy in nursing practice (2nd edition), Blackwell Publishing: Oxford. (III) Lonsway RA (2001) ‘IV therapy in the home’, in Hankins J, Lonsway RA, Hedrick C and Perdue MB (editors) Infusion therapy in clinical practice (2nd edition), Pennsylvania: WB Saunders, pp.501-534. (III) Nursing and Midwifery Council (2008a) Standards for medicines management, London: NMC. (III) NICE (2003) Infection control: prevention of healthcare-associated infection in primary and community care (clinical guidelines 2), London: NICE. Royal College of Nursing (RCN) (2010) The RCN IV Therapy Forum [online] available at: http://www.rcn.org.uk/__data/assets/pdf_file/0005/78593/002179.pdf accessed 140413 References • • • • • • • • • Jackson, A (2003) Reflecting on nursing contribution to vascular access. British Journal of Nursing 12(11): pp.657-65 Dougherty, L (2008) Obtaining peripheral venous access In: Dougherty, L and Lamb, J (eds) Intravenous therapy in nursing practice. 2nd ed Blackwell Publishing, London pp. 225-70 Image from dermatologic.com.ar Lavery, I and Ingram, P (2006) Prevention of infection in peripheral intravenous devices. Nursing Standard. 20(49) PP. 49-55 Ahmed, N (n.d) Revisiting Peripheral Intravenous Cannula Insertion. pp. 1-6 Jackson A (1998) Infection control: a battle in vein infusion phlebitis. Nursing Times; 94: 4, 68-71. Royal College of Nursing (RCN) (2012). Care of peripheral cannula venous sites. Nursing Times. 108(34). PP 13-15. Alberta Health Services (2004). INTRAVENOUS THERAPY: A PRACTICAL APPROACH. PP 1- 41. Lendhart, R., Seybold, T., Kimberger, O., Stoiser, B. and Sessler, D. (2002). Local warming and insertion of peripheral venous cannulas: single blinded prospective randomised controlled trial and single blinded randomised crossover trial. British Medical journal. 325. PP 409. [Online]. Available at http://www.bmj.com/content/325/7361/409.1. Last accessed 14th May 2013. References • Nursing and Midwifery Council (NMC)(2008). The Code: Standards of conduct, performance and ethics for nurses and midwives. [Online]. Available at http://www.nmc- uk.org/Documents/Standards/nmcTheCodeStandardsofConductPerformanceAndEthicsForNursesAndMidwives_LargePrintVersion.PDF. Last accessed 14th May 2013 • • • • • • • • • • Nursing and Midwifery Council (NMC)(2011). Guidance on professional conduct for nursing and midwifery students. [Online]. Available at http://www.nmc-uk.org/Documents/Guidance/Guidance-on-professional-conductfor-nursing-and-midwifery-students.pdf. Last accessed 14th May 2013. Department of Health (DH) (2011). High Impact Intervention: Peripheral intravenous cannula care bundle. [Online]. Available at http://webarchive.nationalarchives.gov.uk/20120118164404/hcai.dh.gov.uk/files/2011/03/2011-03-14HII-Peripheral-intravenous-cannula-bundle-FIN%E2%80%A6.pdf. Last accessed 14th May 2013. Health Protection Scotland (HPS)(2012). Targeted literature review: What are the key infection prevention and control recommendations to inform a peripheral vascular catheter (PVC) maintenance care quality improvement tool? . [Online]. Available at http://www.documents.hps.scot.nhs.uk/hai/infection-control/evidence-for-carebundles/literature-reviews/pvc-maintenance-review.pdf. Last accessed 14th May 2013. Mbamalu, D. and Banerjee, A. (1999). Methods of obtaining peripheral venous access in difficult situations. British Medical Journal. 75 (1), 459-462. Webster, J., Osborne, S., Rickard,C. and Hall, J. (2010). Clinically-indicated replacement versus routine replacement of peripheral venous catheters. [online]. Available at http://onlinelibrary.wiley.com/doi/10.1002/14651858.CD007798.pub2/abstract;jsessionid=413365C35E9C80A14D 687D75F744079F.d01t03. Last accessed 14th May 2013. http://tar.tic.lt/Default.aspx?id=2&item=results&aktoid=165610E0-375B-464B-B059-7DB50471C9A5 http://sam.lt/go.php/licenzijavimas Creamer E, Mc Carthy G, Smyth E (2003) A survey of 554 peripheral intravenous catheters: infection, duration of cannulation and documentation issues British Journal of Infection [online] available at: http://bji.sagepub.com/content/4/4/21 accessed 140513 Aziz,A.M. (2009). Improving peripheral IV cannula care:Implementing High impact interventions. British Journal of Nursing. 18(20). Pp 242-246. Gallant P and Schultz AA (2006) Evaluation of a visual infusion phlebitis scale for determining appropriate discontinuation of peripheral intravenous catheters. Journal of Infusion Nursing. vol. 29, no. 6, p. 338-45










© Copyright 2026