
Hospital Acquired Delirium and Weakness: Rose Buckingham MSN Kelly Goetschkes MSN
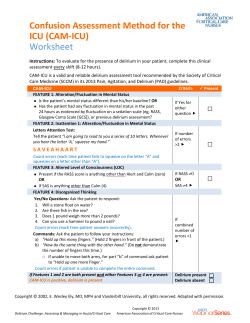
Hospital Acquired Delirium and Weakness: Our Journey at The Nebraska Medical Center Rose Buckingham MSN Kelly Goetschkes MSN Objectives • Describe what delirium is and common risk factors • Identify common symptoms, and implications of delirium for the hospitalized adult • Summarize TNMC ICU Outcomes Study results and what we learned going forward • Describe the Interdisciplinary Delirium Plan for the Prevention, Early Identification, & Treatment of delirium at TNMC THE PATIENT STORY OF NANCY ANDREWS Google: Nancy Andrews delirium Delirium Causes Cognitive Impairment in both older and younger patients • Pandharipande PP, N Engl J Med. 2013. Long-term cognitive impairment after critical illness. 369(14):1306-16. Delirium: A Never Event? Maybe not yet……BUT Blankenship, C. (2008). Non-payment of never events: Implications for practice. American Health Lawyers Association, 11(2) WHAT IS DELIRIUM? (Acute Confusional State) Definition: • acute decline in attention and cognition Characteristics: • • • • common problem serious complications often unrecognized may be preventable Delirium Hypotheses Reasoning proposed to explain physical effects manifested in the patient. Maldonado, J.R., (2008). Neurotransmitter Hypothesis Cell Signaling Hypothesis Neuronal Aging Inflammatory Hypothesis Physiological Stress Decreased cholinergic function with excess release of dopamine, norepinephrine, and glutamate. Decreased or increased levels of serotonergic (fluctuating levels correspond to the different symptoms seen in the clinical presentation hypo- hyper- or mixed active presentation ) Fundamental process of disruption to intra-neuronal signal transduction which greatly disturb neurotransmitter synthesis and release. Proposes that elderly patients are at increased risk of developing delirium due to age related cerebral changes in stress-regulating neurotransmitter and intracellular signal transduction systems. Increased cerebral secretions of cytokines as a result of widespread physical stresses lead to development of delirium by their effect on multiple neurotransmitter systems. Trauma, severe illness, and surgery lead to modifications to blood brain barrier permeability. “Delirium” is rarely called by name! – Altered mental status – Dementia – Confusion – ICU Psychosis – Sundowners – Acute Confusional State Symptoms you see with Delirium • Thinking is slow and muddled • Hallucinations/delusion 30% • Sleep/wake reversal • Mood swings • Psychomotor disturbances: 2 forms – Hyperactive – agitation or picking behaviors – Hypoactive - lethargy or sleepy Inouye,SK NEJM 2006 Hyperactive 1.4% Mixed 31.1% Hypoactive 67.6% of all delirium Bellelli, G., Speciale, S., Barisione, E., & Trabucchi, M., (2007) Patients with Delirium have… Longer Length of Stay 21 vs. 9 days Discharge to a SNF 47% vs. 18% at 6 months 43% vs. 8% at 15 months 33% vs. 11% Develop Dementia at 48 months 63% vs. 8% American Delirium Website, 2013 A Growing Problem 2015 = 40.2 M 2050 = 88.5 M U.S. Department of Health and Human Services (2013) Seniors currently make up 49% of all hospital inpatient days in the U.S. Fearing, M.A. & Inouye, S.K., (2009). Delirium. Focus, 7(1), 229-241. U.S. Delirium Costs: $143-$152B/Yr • $16,303 to $64,421 additional per delirious patient. • U.S. cost-of-care directly attributed to delirium ranges from $143 to $152 billion • Leslie, D.L. & Inouye, S.K. (2011). The importance of delirium: economic and societal costs. J am Geriatr Soc, 59(Suppl 2), S241-S243. Delirium Cost is about 2.5X’s Higher than Non-delirious Counterparts Estimated to occur in > 2.3M inpatients/year = 17.5M inpatient days Cardiac Surgery Study: • Additional cost post-op delirium was $6,150/pt (Ebert, 2001) Step-down Critical Care Unit: • 14% developed delirium & stayed 9.2 days longer • Costing $28,000/case = $5,880,000/year (Maldonado, Dhami, 2003) Cardiac Surgery Prevention Study: • Non-delirious $6,763 and Delirious $12,965 (Maldonadom Wysong, 2003) ICU Patients: • Costs were 31% higher: $41,836 vs. $27,106 (Milbrandt, 2004) Hospitalized Elderly Patients: • Cost from $16,303 to $64,421 per patient (Leslie, 2008) ( Rizzo,2001) ) IMPACT OF DELIRIUM Extends Beyond the Hospital Post-hospital costs (>$100 B/yr) • Institutionalization • Rehabilitation • Home care • Caregiver burden Ref: Leslie DL et al. Gerontologist 2005: 45 (Spec Iss II): 299. 5 patients become delirious in US Hospitals every minute Delirium Rates Hospital: • Prevalence (on admission) • Incidence (hospital-acquired) • Postoperative: • Intensive care unit: 10-40% 15-60% 15-53% 70-87% U.S. Dept HHS, AoA Report, Profile of Older Americans, 2011 Medical Populations Prevalence of Delirium (%) Medical Populations Prevalence of Delirium (%) General Medical 9-24 Hospitalization Admission 15 -23 HIV/AIDS 30-40 In nursing homes 15-60 Medical ICU 60-80 Frail elderly patient 60 Post-stroke 13-48 Elective hip or knee replacement 25 Post-operative Delirium 10-74 Bilateral knee replacement 41 General Surgical Units 7-52 Femoral neck fracture repair 65 Spine surgery 12.5 General Oncology 25-40 Post-CABG 25-32 Palliative Care Units 26-44 Post-Cardiotomy 50-67 Bone Marrow Transplant 73 Abdominal Aneurysm repair 33 Advanced Cancer Up to 85 Out-patient minor (cataract) surgery 4.4 Psychiatric patients 14.6 Maldonado, Critical Care Clinic, 2008; 24:657-722 Patient Vulnerability + Severity of Precipitating Risk Factor is WHY One Patient Develops Delirium, while a Similar Patient Does Not. Up to 40% of Hospital-Acquired DELIRIUM is PREVENTABLE • Common problem • Often unrecognized • Typically of multifactorial etiology • Serious complications • Often preventable (40-50% cases) DELIRIUM IS OFTEN CONFUSED WITH DEMENTIA Delirium is NOT Dementia Feature Delirium Dementia Onset Acute Gradual, usually insidious, but depends on cause Course Short, diurnal symptom fluctuations; worse at night and on awakening Long; No diurnal effects, progressive, but relatively stable over time Progression Abrupt Slow, but even Duration Hours to days; Up to 6 months Months to years Awareness Reduced Clear Alertness Fluctuates ; lethargic or hyper vigilant Generally normal Attention Impaired; fluctuates Generally normal Orientation Fluctuates in severity; generally impaired May be impaired Memory Recent and immediate impaired Recent and remote impaired Thinking Disorganized, distorted, fragmented, slow or accelerated, incoherent Difficulty with abstraction, makes poor judgments, word finding difficulty Perception Distorted; Illusions, delusions, & Misperceptions often absent hallucinations; difficulty distinguishing between reality and misperceptions fluctuations RELATIONSHIP OF DELIRIUM TO DEMENTIA Two Sides of the Coin Delirious patients 8X’s risk to get dementia. (Davis,2012) >50% dementia patients develop delirium & have a 25% increased risk of dying within 30 days. (Fick, 2013). Probability of transitioning to delirium increases dramatically (by 2%) for each year of life after 65 years. (Pandharipande, 2006) The Duration of delirium is an independent predictor of long-term cognitive impairment. (Girard et al., CCM 2010) Patient Factors Predisposing Disease Older age Alcohol/drug use Functional dependence Male gender Living alone Depression Dehydration Vision/Hearing impaired Cardiac disease Cognitive impairment Hx Delirium or dementia Pulmonary disease Pain poorly controlled Liver/Renal disease HIV Environment Admission via ED or through transfer Isolation/No visitors No clock No daylight Noise Use of physical restraints Tethers Sleep deprivation Inouye SK, et al. JAMA .1996;275:852. Skrobik Y. Crit Care Clin. 2009;25(3):585-591. Less Modifiable Acute Illness DELIRIUM More Modifiable Length of stay Fever/Infection/Sepsis Cardiac/Hip surgery Medicine service Malnutrition Hypotension Metabolic disorders Tubes/catheters/tethers Medications: - Anticholinergics - Corticosteroids - Benzodiazepines Van Rompaey B, et al. Crit Care 2009;13:R77. Devlin J, et al. ICM, 2007; 33:929-940. I’ve seen a dying eye Run round and round a room In search of something, as it seemed, Then cloudier become; And then, obscure with fog, And then be soldered down, Without disclosing what it be, ‘Twere blessed to have seen. Emily Dickinson DELIRIUM IS OFTEN UNRECOGNIZED NURSES’ RECOGNIZE DELIRIUM ONLY 31% of the time Inouye SK, Arch Intern Med. 2001;161:24672473 Brief-Confusion Assessment Method (B-CAM) & Confusion Assessment Method (CAM-ICU) SIMPLIFIED DIAGNOSTIC CRITERIA 4 features assessed by B-CAM: (1) inattention (2) acute onset or fluctuating course (3) altered level of consciousness (4) disorganized thinking -- The diagnosis of delirium requires the presence of criteria: (1), (2) and (3) or (4) RASS Description +4 Overtly combative, violent, immediate danger to staff +3 Very agitated, pulls or removes tube(s) or catheter(s); aggressive +2 Agitated, frequent nonpurposeful movement +1 Restless, anxious but movements not aggressive vigorous 0 Alert and calm -1 Drowsy, not fully alert, but has sustained awakening (>10 seconds) -2 Light sedation, briefly awakens with eye contact to voice (<10 seconds) -3 Moderate sedation, movement or eye opening to voice (but no eye contact) (Han et al., 2013) What to THINK if + for delirium Toxic Situations CHF, shock, dehydration Deliriogenic meds (tight titration, sedative choice) New organ failure, e.g., liver, kidney Hypoxemia; also, consider giving Haloperidol or other antipsychotics Infection/sepsis (nosocomial), Immobilization Nonpharmacological interventions Hearing aids, glasses, reorient, sleep protocols, music, noise control, ambulation K+ or Electrolyte problems DELIRIUM IN THE ICU ABCDE Bundle Outcomes Study at TNMC Outcomes/benefits identified in patients with bundle use in TNMC ICU’s: • Patients spent 3 more days ventilator free • 15% fewer ICU patients experienced delirium (incident delirium) • 17% reduction in ICU days spent delirious (prevalent delirium) • Odds ratio showed risk of developing delirium reduced by almost half • 18% more patients mobilized • 2.1 times increased odds of being mobilized • 8.6% reduction in the hospital mortality rate From this study we learned that • • • • Need to further lighten sedation Choice of sedation Provider use of order set Nursing education closer to implementation & targeted • Need for tighter pain assessment • Importance of Early Mobility Awakening ICU Spontaneous Awakening Trial Non-ICU A- Awakening Medications: – Pharmacy consult medication review – Poly-pharmacy taking 5 or more medications or 3 new started in 1 day – Review high-risk medications. Sleep Hygiene: – Promote and try non-pharmacological options first. – Progressive mobility. Avoid bed rest orders unless medically necessary. – We want our patients oriented to day/night sleep patterns and tired at night. – Promote private room with a view to the outside, lighting appropriate to time of day – Enforce quiet hours and nursing unit noise reduction. American Association of Critical Care Nurses, Delirium Assessment and Management. 2014. Retrieved from: http://www.aacn.org/wd/practice/content practicealerts/deliri um practice-alert.pcms?menu=practice Breathing ICU Spontaneous Breathing Trial Non-ICU B-Breathing • Hypoxia or risk of pulmonary complications: – Monitor and optimize oxygen saturation levels – Cough and deep breathe; promote use of incentive spirometer – Provide more frequent oral care pre-op/immobile patients to decrease the risk of hospital acquired pneumonia. – Speech Consult for patient aspiration concerns American Association of Critical Care Nurses, Delirium Assessment and Management. 2014. Retrieved from: http://www.aacn.org/wd/ practice /content practicealerts/deliri um practice-alert.pcms?menu =practice Coordination/Communication AND/OR Choice of Sedation ICU • Coordination, Communication and Choice of Sedation Non-ICU C-Coordination and Communication: – Communicate/intervene with ABCDE care plan interventions for patients at high risk for hospital acquired complications including delirium, falls, skin breakdown, dehydration, weakness, pneumonia, and DVT’s. – Communicate to involve/inform significant others. – Offer patient educational and safety hand-outs and videos. – Encourage family/caregiver involvement and visitation. American Association of Critical Care Nurses, Delirium Assessment and Management. 2014. Retrieved from: http://www.aacn.org/wd/ practice /content practicealerts/deliri um practice-alert.pcms?menu =practice Delirium Prevention, Screening, and Management ICU Non-ICU • CAM-ICU • Educate family to report cognitive changes & provide educational handouts D-Delirium Prevention and Management – – – – Determine your patient’s baseline cognitive status. Prevention is basic good nursing care tailored to meet each individual patient’s needs. Delirium is multi-factorial, balanced and governed by exposure to noxious stimuli and each individual’s unique ability and reserve to cope with it. Assess both non-modifiable and modifiable risk factors and consider these along with precipitating factors that may cause delirium that are part of the hospital experience when you tailor the ABCDE interdisciplinary care plan. American Association of Critical Care Nurses, Delirium Assessment and Management. 2014. Retrieved from: http://www.aacn.org/wd/ practice /content practicealerts/deliri um practice-alert.pcms?menu =practice Early Mobility ICU • Progressive mobilization of critically ill patients as early as possible Non-ICU E-Early Mobility: – – – – – – – Progressive mobilization plan on day one to preserve, maintain, and enhance the patient’s functional ability. Up in the chair X3 meals. Ambulation tid is a nursing unit expectation. Confused patient use video monitoring and bed/chair alarm Mobilize your patient as soon as possible after surgery. Schedule toileting with hourly rounds. Use bathroom or BSC rather than bedpan. Keep the commode beside the bed. Stay with delirious patients they will not always follow commands to use the call light. Assess pain level and administer analgesics to allow for progressive activity. Provide mobility aids as needed. American Association of Critical Care Nurses, Delirium Assessment and Management. 2014. Retrieved from: http://www.aacn.org/wd/ practice /content practicealerts/deliri um practice-alert.pcms?menu =practice ICU delirium and early mobility • “Kim”- 25 yo SAH from OSH arrived intubated with some complications. • Intubated several days • Q 1 hour neuro checks and strict bed rest for 35 days. It can be done! Morris PE, Goad A, Thompson C, et al: Early intensive care unit mobility therapy in the treatment of acute respiratory failure. Crit Care Med 2008; 36:2238–2243 Schweickert WD, Pohlman MC, Pohlman AS, et al: Early physical and occupational therapy in mechanically ventilated, critically ill patient A randomised controlled trial. Lancet 2009; 373:1874–1882 Early Mobility and the Hemorrhagic Stroke Patient Discharge Disposition for Hemorrhagic Stroke Patients Pre-Implementation of the PUMP-PLUS N = 46 Post-Implementation of the PUMP-PLUS N = 28 % of patients Skilled Nursing Facility [SNF] 6 % of patients 13.04% SNF 2 7.14% Long-Term Acute Care [LTAC] 3 6.52% LTAC 1 3.57% Inpatient Rehabilitation [REHAB] 20 43.48% REHAB 13 46.43% HOME 17 36.96% HOME 12 42.85% Comparison of Discharge Disposition chi square Discharge Disposition Pre Post X df p Home 17 (18.03) 12 (10.97) 0.2543 1 0.6141 Other 29 (27.97) 16 (17.03) Comparison of Mean LOS two tailed t Pump-Plus Protocol n M SD t df p 46 20.3 15.51 0.582 72 0.562 28 18.4 10.33 Pre-Implementation Post-Implementation Early Mobility and the SAH Patient The Comprehensive Delirium Initiative is: An Always Event Our goal at TNMC is the prevention, early identification, and reversal of hospital acquired delirium. • Laying a foundation for partnering with patients and their families • Leading to actions for an optimal patient experience and improved outcomes • A unifying force demonstrating an ongoing commitment to person- and family-centered care Hayward M, Endo J, Rutherford P. A Focus on "Always Events." Healthcare Executive. 2014 Jan/Feb;29(1):78-81. The Plan for TNMC • Risk Prediction tool on admission – coming • Delirium Brief-CAM Screen by nursing once a shift for early identification • New Delirium MD Order Set • Extended ABCDE Bundle to the Non-ICU nursing units for both prevention and treatment interventions • Only treatment for delirium is to identify the causative agent and reverse it Balas,M (2013). J Gerontol Nurs 39(8): 39-51. Create an Action Plan List 1 thing on your evaluation sheet that increases the risk of delirium where you work THAT COULD REALISTICALLY BE CHANGED RIGHT NOW Create a Wish List List at least 1 thing on your evaluation sheet that you would like to make available to your patients to reduce delirium where you work. Conclusions • Delirium is a significant problem for hospitalized patients and a predictor of many negative clinical outcomes. • Reliable and easy tools are available for identification of delirium in patients in the ICU and Non-ICU nursing units. • Processes of care are available to minimize incidence of modifiable risk factors. • Extended ABCDE Bundle can be incorporated into current practices with minimal additional resources. • Some operational culture change is involved The End... Questions? It is not enough for a great nation to merely have added new years to life Our objective must also be to add new life to those years - John F. Kennedy References American Association of Critical Care Nurses (2014). Delirium Assesment and Monitoring. Retrieved from: http://www.aacn.org/wd/practice/content/practicealerts/delirium-practicealert.pcms?menu=practice American Delirium Society Webite. Retrieved June 1, 2013 http://www.americandeliriumsociety.org/ Balas M, Buckingham R, Braley T, Saldi S, Vasilevskis EE. (2013). Extending the ABCDE Bundle to the post-intensive care unit setting. J Gerontol Nurs. 39(8):39-51. doi: 10.3928/00989134-2013053006. Balas, M.C., Vasilevskis, E.E., Olsen, K.M., Schmidt, K.K., Shostrom, M.S., Cohen, M.Z., Peitz, G., Gannon, D.E., Sisson, J., Sullivan, J., Stothert, J.C., Lazure, J., Nuss, S.L., Jawa, R.S., Freihaut, F., Ely, E.W., & Burke, W.J. (2014). Effectiveness and safety of the awakening and breathing coordination, delirium monitoring/management, and early exercise/mobility bundle. Crit CareMed Jan 3. [Epub ahead of print] Bellelli G, Speciale S, Barisione E, Trabucchi M. (2007). Delirium subtypes and 1-year mortality amongelderly patients discharged from a post-acute rehabilitation center J Gerontol A Biol Sci Med Sci 62 (10): 1182-1183 Blankenship, C. (2008). Non-payment of never events: Implications for practice. American Health Lawyers Association, 11(2): 1-5. Davis, D.H.J, Terrera, G.M., Keage, H., Rahkonen, T., Oinas, M., Matthews, F.E., Cunningham, C., Polvikoski, T., Sulkava, R., MacLullich, A.M., & Brayne C. (2012). Delirium is a strong risk factor for dementia in the oldest-old: a population based cohort study. Brain.135(Pt9):2809-16. doi: 10.1093/brain/aws190. Devlin, J.W., Fong, J.J., Fraser, G.L., (2007). Tools for diagnosing delirium in the critically ill. Intensive Care Med 33:929–940. Ebert, A.D., Walzer, T.A., Huth, C., & Herrmann, M. (2001). Early neurobehavioral disorders after cardiac surgery: A comparativeanalysis of coronary artery bypass graft surgery and valve replacement. Journal of Cardiothoracic and VascularAnesthesia (15)1: 15-19. Fearing, M.A. & Inouye, S.K., (2009). Delirium. Focus, 7(1), 229-241. Fick, D.M., DiMeglio, B., McDowell, J.A., & Mathis-Halpin, J. (2013). Do you know your patient? Knowing individuals with dementia combined with evidence-based care promotes function and satisfaction in hospitalized older adults. Journal of Gerontological Nursing 39(9):2–4. doi:10.3928/00989134-20130809-89. References Girard, T.D., Jackson, J.C., Pandharipande, P.P., Pun, B.T., Thompson, J.L., Shintani, A.K., Gordon, S.M., Canonico, A.E., Dittus, R.S., Bernard, G.R., Ely, E.W. (2010). Delirium as a predictor of long-term cognitive impairment in survivors of criticalillness. Crit Care Med. 38(7):1513-20. doi: 10.1097/CCM.0b013e3181e47be1. Inouye, S.K., (2006). Delirium in older persons. N Engl J Med 354: 1157-65. Inouye S.K., Foreman, M.D., Mion, L.C., Katz, K.H., & Cooney, L.M. (2001). Nurses' recognition of delirium and its symptoms: comparison of nurse and researcher ratings. Arch Intern Med.;161:2467-2473 Inouye, S.K., Charpentier, P.A., (1996). Precipitating factors for delirium in hospitalized elderly patients. JAMA 275(11):852-857. doi:10.1001/jama.1996.03530350034031. Leslie, D.L. & Inouye, S.K. (2011). The importance of delirium: economic and societal costs. J am Geriatr Soc, 59(Suppl 2), S241S243. Han, J.H., Wilson, A., Vasilevskis, E.E., Shintani, A., Schnelle, J.F., Dittus, R.S., Graves, A.J., Storrow, A.B., Shuster, J., & Ely, E.W., (2013). Diagnosing delirium in older emergency department patients: validity and reliability of the delirium triage screen and the brief confusion assessment method. Ann Emerg Med. Jul 31. Pii: S0196-0644(13)00436-8. Hayward M, Endo J, Rutherford P. A Focus on "Always Events." Healthcare Executive. 2014 Jan/Feb;29(1):78-81. Leslie, D.L., Marcantonio, E.R., Zhang, Y., Leo-Summers, L., & Inouye, S.K., (2008). One-year health care costs associated with delirium in the elderly population. Arch Intern Med, 168(1):27-32 Maldonado, J.R., (2008). Pathoetiological Model of Delirium: a Comprehensive Understanding of the Neurobiology of Delirium and an Evidence-Based Approach to Prevention and Treatment. Crit Care Clin 24 789–856 Maldonado, J.R. (2008). Delirium in the acute care setting: characteristics, diagnosis and treatment. 24(4):657-722, vii. doi: 10.1016/j.ccc.2008.05.008. Maldonado JR, Dhami N, Wise L. (2003). Clinical implications of the recognition and management of delirium in general medical wards. Psychosomatics, 44(2), 157-158. References Maldonado JR, Wysong A, van der Starre PJ. The role of the novel anesthetic agent dexmedetomidine on reduction of the incidence of ICU delirium in postcardiotomy patients. J Psychosom Research, 55, 150, 2003. Marcantonio, E.R. (2012). Postoperative delirium: a 76-year-old woman with delirium after surgery. JAMA. 308(1), 73-81. Milbrandt, E.B., Deppen, S., Harrison, P.L., Shintani, A.K., Speroff, T., Stiles, R.A.,Truman, B., Bernard, G.R., Dittus, R.S., & Ely, E.W. (2004). Costs associated with delirium in mechanically ventilated patients. Crit card Med (32)4: 955-962. Morris P. E., Goad, A., Thompson, C., Taylor, K., Harry, B., Passmore, L., Ross, A., et al. (2008). Early intensive care unit mobility therapy in the treatment of acute respiratory failure. Crit Care Med, 36, 2238–2243. Pandharipande PP, N Engl J Med. 2013. Long-term cognitive impairment after critical illness. 369(14):1306-16. Pandharipande, P., Shintani, A., Peterson, J., Pun, B.T., Wilkinson, G.R., Dittus,R.S., Bernard, G.R., Ely, E.W. (2006). Lorazepam is an independent risk factor for transitioning to delirium in intensivecare unit patients. Anesthesiology 104:21–6 Schweickert, W. D., Pohlman, M. C., Pohlman, A. S., Nigos, C., Pawlik, A. J., Esbrook, C. L., Spears, L., et al. (2009). Early physical and occupational therapy in mechanically ventilated,critically ill patients: A randomized controlled trial. Lancet, 373, 874–1882. Skrobik, Y. (2009). Delirium prevention and treatment. Crit Care Clinic 25(3): 585-591. U.S. Department of Health and Human Services (2013). Retrieved December 1, 2013 http://www.cdc.gov/features/agingandhealth/state_of_aging_and_health_in_america_2013.pdf U.S. Department of Health and Human Services Agency on Aging Report, Profile of older Americans(2011). Retrieved July 3, 2013 http://www.aoa.gov/Aging_Statistics/Profile/2011/docs/2011profile.pdf Van Rompaey, B., Elseviers, M.M., Schuurmans, M.J., Shortridge-Baggett, L.M., Truijen, S., & Bossaert, L. (2009). Risk factors for delirium in intensive care patients: a prospective cohort study. Crit Care 13:R77 PRECIPITATING FACTORS OR INSULTS Drugs Sedative hypnotics Narcotics Anticholinergic drugs Polypharmacy Alcohol or drug withdrawal Primary neurological diseases Stroke, particularly nondominant hemispheric Intracranial bleed Meningitis/encephalitis Environmental Intensive care unit admission Physical restraint use Bladder catheter use High number of procedures Pain Emotional stress Prolonged sleep deprivation Inouye SK. NEJM 2006;354:1157-65 Inter-current illnesses Infections Iatrogenic complications Severe acute illness Hypoxia Shock Fever/hypothermia Anemia Dehydration Poor nutritional status Low serum albumin Metabolic derangements (e.g., electrolytes, glucose, acid-base) Surgery Orthopedic surgery Cardiac surgery Duration of cardiopulmonary bypass Non-cardiac surgery 54 PREDISPOSING OR VULNERABILITY FACTORS Demographics Older age Male gender Cognitive status Dementia Cognitive impairment History of delirium Depression Functional status Functional dependence Immobility Poor activity level History of falls Sensory impairment Vision impairment Hearing impairment Inouye SK. NEJM 2006;354:1157-65 Decreased Intake Dehydration Malnutrition Drugs Multiple psychoactive drugs High number of drugs Alcohol abuse Medical Comorbidity High severity of illness High level of comorbidity Chronic renal or hepatic disease Previous stroke Neurologic disease Metabolic derangements Fracture or trauma Terminal illness HIV infection










© Copyright 2026