
I R C
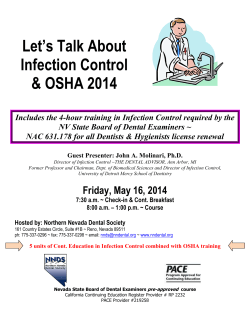
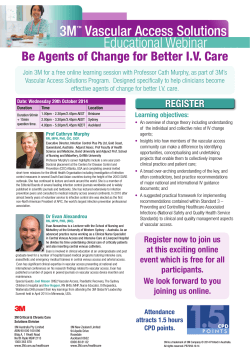
Patient Safety Issues I RATES IN INTENSIVE CARE UNITS BY ELECTROCARDIOGRAPHIC LEAD WIRE TYPE: DISPOSABLE VS REUSABLE NFECTION By Nancy M. Albert, PhD, CCNS, CHFN, CCRN, NE-BC, Ellen Slifcak, RN, BA, Joel D. Roach, BA, James F. Bena, MS, Gregory Horvath, RN, BA, MBA, Sue Wilson, RN, BSN, Rosslyn Van Den Bossche, RN, BSN, MBA, Nemy Vargas, RN, MSN, CCRN, CEN, Victoria Rhoades, RN, BSN, CCRN, Katrina M. Hartig, RN, BSN, MS, NE-BC, Heather Lachiewicz, RN, MSN, CCRN, CNML, and Terri Murray, RN, MSN CNE 1.0 Hour Notice to CNE enrollees: A closed-book, multiple-choice examination following this article tests your understanding of the following objectives: 1. Compare infection rates of patients in intensive care units who received disposable electrocardiographic (ECG) leads vs reusable ECG leads. 2. Identify sources of microorganisms that may promote hospital-acquired infections. 3. State the role of disposable ECG leads in a bundled infection control program. To read this article and take the CNE test online, visit www.ajcconline.org and click “CNE Articles in This Issue.” No CNE test fee for AACN members. ©2014 American Association of Critical-Care Nurses doi: http://dx.doi.org/10.4037/ajcc2014362 460 Background It is unknown if disposable electrocardiographic lead wires (ECG-LWs) reduce infection rates compared with cleaned, reusable lead wires. Purpose To compare infection rates in intensive care unit (ICU) patients receiving disposable versus reusable ECG-LWs. Methods Matched adult ICUs were randomly assigned to disposable or reusable ECG-LWs. Outcomes were bloodstream infection, ventilator-associated pneumonia, and chest surgical site infections. Patients’ characteristics and infections were collected from hospital databases. Event rates were described by using total counts and rates per 100 patient days and were compared between groups by using generalized linear mixedeffect models weighted by patients’ ICU length of stay. Results Overall, 4056 patients from 6 ICUs received disposable and 3184 patients from 5 ICUs received reusable ECG-LWs. The characteristics of the 2 groups were similar, except patients receiving disposable ECG-LWs were less likely to be discharged home (P = .03) and had more comorbid conditions (P = .002). Overall infection rates did not differ between ECG-LW groups, between groups in matched ICUs, between groups by infection type, or when only patients with ICU stays longer than 48 hours were considered (2578 cases). In multivariate analyses, infection rates did not differ between all patients in ECG-LW groups or for patients with ICU stays beyond 48 hours (both P = .10). Conclusions No difference was observed in infection rates of ICU patients receiving disposable versus reusable ECG-LWs. (American Journal of Critical Care. 2014;23:460-468) AJCC AMERICAN JOURNAL OF CRITICAL CARE, November 2014, Volume 23, No. 6 www.ajcconline.org H ospital-acquired infections (HAIs) have been a long-standing source of complications for patients. Compared with patients without HAIs, patients with HAIs had longer hospital length of stay, increased cost of care, more morbidity, and higher mortality.1-4 Decreasing the occurrence of HAIs, which are considered preventable, is a primary goal of many hospital-based quality improvement and patient safety programs. Infection control practices, such as hand hygiene, isolation precautions, environmental cleaning, and antimicrobial bathing, are the major focus of efforts to decrease HAI occurrence. Despite infection control practices surrounding cleaning techniques by hospital personnel, bacteria can remain latent on inanimate surfaces such as door knobs, identification badges, stethoscopes, bath basins, sharps containers, tourniquets,5-11 and electrocardiographic lead wires (ECG-LWs),13,14 and may be a source of crosscontamination and nosocomial infection, especially in patients who are immunocompromised.12,13 Although it is known that ECG-LWs are a reservoir source for microorganisms, it is unknown if disposable ECG-LWs would lead to a decrease in infection rates compared with cleaned, reusable ECG-LWs. Disposable ECG-LWs do not require adherence to optimal cleaning procedures because they are discarded after one use. Because disposable ECGLWs are not expected to harbor latent bacteria when packaged, they may offer advantages beyond reusable ECG-LWs that are cleaned after each use. In this comparative effectiveness research trial, the primary objective was to determine whether disposable ECG-LWs caused a reduction of cross-contamination risk and led to the following outcomes compared with cleaned, reusable ECG-LWs: lower rates of bloodstream infection (BSI) and ventilator-associated pneumonia (VAP) in adults treated in medical, cardiovascular surgery, general surgery, and neurological intensive care units (ICUs) and lower rates of sternal wound-surgical site infections (SSIs) in adults cared for in cardiovascular surgery ICUs. Specific aims were to examine between-group differences in overall infection rates, infection rates by ICU environment, infection rates by infection type (BSI, VAP, and SSI), infection rates for each infection type by ICU environment, and time to first infection in all ICU patients and in patients treated in the ICU for at least 48 hours, after adjusting for patients’ length of stay in the ICU. Disposable ECG lead wires are not expected to harbor latent bacteria when packaged. Methods About the Authors Nancy M. Albert is the associate chief nursing officer, Office of Research and Innovation–Nursing Institute and a clinical nurse specialist, Kaufman Center for Heart Failure–Heart and Vascular Institute at Cleveland Clinic in Cleveland, Ohio. She is also an adjunct professor at Aalborg University in Aalborg, Denmark, and an adjunct associate professor at Case Western Reserve University, Francis Payne Bolton School of Nursing in Cleveland, Ohio. Ellen Slifcak is a research nurse, Joel D. Roach is a research coordinator, James F. Bena is a statistician, Gregory Horvath was a nurse manager in the medical intensive care unit, Sue Wilson is a nurse manager in the surgical intensive care unit, Rosslyn Van Den Bossche is assistant nursing director of the Heart and Vascular Institute, Nemy Vargas is a nurse manager in the medical intensive care unit, Victoria Rhoades is a nurse manager in the neuroscience intensive care unit, Katrina M. Hartig was a nurse manager in the cardiovascular intensive care unit, Heather Lachiewicz is a nurse manager in the cardiovascular intensive care unit, and Terri Murray is a nurse manager in the cardiovascular stepdown/telemetry unit at Cleveland Clinic. Corresponding author: Nancy M. Albert, RN, PhD, CCNS, CHFN, CCRN, NE-BC, Cleveland Clinic, 9500 Euclid Avenue, J3-630 (J3-4), Cleveland, OH 44195 (e-mail: [email protected]). www.ajcconline.org The trial used a cluster, randomized controlled design. Matched ICUs were randomized to nonsterile, disposable ECG-LWs (intervention) versus cleaned, reusable ECG-LWs (usual care). This study received approval from the Cleveland Clinic’s institutional review board before initiation. Setting and Sample The unblinded trial was completed at the Cleveland Clinic, a quaternary-care medical center with more than 1200 beds in Northeast Ohio. Adult patients being treated in a medical, cardiovascular surgery, general surgery, or neurological ICU were included if their assigned ICU was 1 of a minimum of 2 matching units that had the same population of patients, leadership team, health care providers (physicians, acute care nurse practitioners, respiratory therapists, and in some ICUs, clinical nurses), and policies and procedures. Four cardiovascular ICUs, 3 general surgery ICUs, 2 medical ICUs, and AJCC AMERICAN JOURNAL OF CRITICAL CARE, November 2014, Volume 23, No. 6 461 Enrollment Assessed for eligibility (n = 7939 cases) Randomized by intensive care unit (ICU) assignment (n = 7939) Allocation Cases allocated to reusable ECG-LW (n = 3463) Cases allocated to disposable ECG-LW (n = 4476) • Excluded from analysis: • In hospital or ICU > 2 days before study start date (n = 104) • On study unit < 24 hours (n = 120) • Extended stay on study unit after enrollment stop date (n = 52) • Other (n = 3) • Excluded from analysis: • In hospital or ICU > 2 days before study start date (n = 31) • On study unit < 24 hours (n = 189) • Extended stay on study unit after enrollment stop date (n = 74) • Patient off assigned ECG-LW (n = 21) • Other (n = 5) Analysis Analyzed (n = 3184 cases) Analyzed (n = 4056 cases) Figure 1 Usual-care and intervention cases for electrocardiographic lead wires (ECG-LW) trial. 2 neurological ICUs participated. Each of the matched units was randomly assigned to usual care or intervention ECG-LWs by having nurse managers associate a specific ICU to a sealed envelope with an ECG-LW assignment written inside. The surgical ICU had 3 matched units, so 4 envelopes were available, 2 of each labeled with disposable and reusable ECG-LWs. Of 11 participating ICUs, 6 were assigned to disposable ECG-LWs and 5 were assigned to reusable ECG-LWs. Some patients had multiple ICU stays during 1 episode of care; thus, each ICU stay was considered a case if inclusion criteria were met. On the first day of study enrollment, patients who were currently in a study ICU were included if they had been previously admitted to the unit within 48 hours. On the day the study stopped enrollment, patients were included if they were discharged within 48 hours of the enrollment stop date. The enrollment stop date was dictated by inability to provide disposable ECG-LWs to newly admitted ICU patients, because the supply was depleted. Patients were excluded from analysis if they were admitted after midnight but were not in the ICU the following midnight, Data collection for 1 year would provide 80% power to detect differences of at least 25% between groups. 462 reflecting less than a 1-day stay according to billing criteria, received the wrong ECG-LW per random assignment, or had ECG-LWs removed (Figure 1). Sample size was determined on the basis of the following assumptions: randomization of matched units, not individual patients, required a much larger difference between groups in the primary outcome (overall infection rate), matched units would have a ρ of 0.5 (50% level of correlation among the like units), and usual care ICU BSI rate would be approximately 0.9 per 100 ICU days. Thus, to detect a 50% reduction in BSI, using 80% power in BSI infections, and assuming 10 beds per unit per day per group enrollment, cases would need to be enrolled to the matched units for a 1-year period. Sample size for SSI among cardiothoracic surgical ICU cases was based on an SSI rate of 2.4% among patients in the cleaned, reusable ECG-LW group. With an expected enrollment per group of 60 patients/month (total 420), there would be 80% power to detect a reduction of 90% or greater in the SSI rate in the disposable ECGLW group relative to the reusable ECG-LW group. After 4 months of data collection, a data review revealed 2 findings: the number of cases enrolled was nearly 2 times (double) what was anticipated, and ICU BSI rates were much lower than previous annual reports (BSI rate was approximately 0.15 per 100 ICU days). To evaluate the impact of the observed results on sample size requirements, an update of the previous sample size analysis was performed by using the methods described by Hayes and Bennett.14 Assuming the rate of enrollment of cases and all other effects remained the same, data collection for a 1-year period would provide 80% power to detect differences of at least 25% between groups. With low rates of BSI and other HAIs, a 25% difference between groups would provide clinical significance of group differences. Usual-Care and Intervention ECG-LW Groups Units assigned to usual care maintained standard-of-care procedures related to ECG-LW attachment, removal, cleaning, and storage when not in use. For all except the cardiovascular surgery ICUs, environmental service workers cleaned ECG-LWs after patients were discharged from the ICU, using standard wipes (Clorox Healthcare Germicidal Wipes, which effectively kill Clostridium difficile spores in 3 minutes and 50 other bacteria in 30 seconds or less) and procedures (wiped the entire length of each wire to clean visible and invisible debris and contaminants). For the cardiovascular ICUs, after patients were discharged, ECG-LWs were sent to the cardiovascular operating room for ultrasound cleaning AJCC AMERICAN JOURNAL OF CRITICAL CARE, November 2014, Volume 23, No. 6 www.ajcconline.org and reuse, per long-standing usual-care procedures. Nurses and other health care workers completed usual-care activities related to ECG monitoring for both groups. After random assignment was determined, units allocated to the intervention group were oriented to disposable ECG-LW cable-to-monitor connection, patient connection, and supply storage site. Nonsterile, disposable ECG-LW sets were wrapped in a clear plastic bag. The supply of ECG-LWs that were not in use was maintained in the sealed shipping box and stored in an office of the principal investigator. When patients were discharged from the ICU, disposable ECG-LWs were discarded. During the study enrollment period, all reusable ECG-LW sets were removed from the intervention group ICUs. One research nurse and 1 research coordinator made daily rounds to each study ICU to assess use of ECG-LWs per random assignment and ensure an adequate supply of disposable ECG-LWs. On the day that the study started, staff nurses switched all patients in intervention group ICUs from reusable to disposable ECG-LWs. Outcomes Rates of hospital-acquired BSI and VAP were retrieved from a database in the infection control department and included the date of the infection, type of bacteria, central-catheter BSI determination, and primary and secondary sources. All data retrieved were reviewed by researchers to ensure that the date of infection coincided with the ICU stay of record. Rates of SSIs were retrieved from data collected routinely for the Society of Thoracic Surgeons registry. An SSI was defined as 1 of 3 sternal infections, a sternal superficial wound infection, a deep sternal wound infection, or mediastinitis. Medical records of all cases were reviewed by researchers to ensure that the sternal infection had occurred during the current ICU admission and was not associated with a previous event or surgery. Patients’ data on age, sex, race, marital status, insurance type, discharge disposition, ICU length of stay, and hospital length of stay were retrieved from a billing database. Electronic medical records were reviewed for presence of 17 chronic medical conditions before hospital admission by using the Charlson Comorbidity Index (CCI). The CCI was developed to classify comorbid conditions that might change the risk of mortality.15-20 The score was categorized into 3 groups (score of 1-2 = 1; 3-4 = 3; 5 or more = 5), with a higher score reflecting greater morbidity and risk of mortality. In a study18 of 33 940 patients with ischemic heart disease, the index grouping demonstrated a strong relationship to mortality rate. In our study, the CCI was used to reflect patients’ acuity. www.ajcconline.org Data Collection Researchers identified cases daily by completing ICU rounds and by assessing patient admissions via the electronic medical record. Infection data and patients’ demographics were requested in batches, and valid cases were entered into an SPSS database (v19, IBM/SPSS) with CCI data that were retrieved retrospectively. Data retrieved from the billing database were merged with SPSS data by a statistician. Data Analysis Categorical factors were described by using frequencies and percentages, rates were described by using total counts and rate per 100 patient days, and continuous measures were described by using means and standard deviations. To compare infection rates across all unit types, generalized linear mixed-effect models were used, treating the counts as coming from a Poisson distribution. We used the generalized linear mixed-effect model because it was reported to perform better in situations that involved a small number of clusters (ICUs). Analysis was performed under assumptions of nonmatching within ICU type and also matching within each of the 4 ICU types (medical, cardiothoracic surgical, surgery, and neurological). For analysis within ICU type, traditional Poisson regression models were used. Models were fit by using the GLIMMIX and GENMOD procedures within SAS software (version 9.2). ECG-LW groups were compared by using mixed models for continuous measures and logistic regression with generalized estimating equations for binary measures. All models except the model comparing unit length of stay were weighted by the patient’s length of stay in the unit. Time-toevent analyses were performed by using KaplanMeier estimates of survival and Cox proportional hazards models. Analyses corrected for the correlation within patients by using adjustments within the Cox proportional hazards model. Models were fit by using the LIFETEST and PHREG procedures within SAS software. A significance level of .05 was considered statistically significant. One research nurse and one research coordinator made daily rounds to assess use of ECG lead wires. Results In a 12-month period, 7240 cases were enrolled with 1484 cases from 2 matched medical ICUs, 3260 cases from 4 matched cardiovascular surgery ICUs, 1540 cases from 3 matched general surgery ICUs (2 randomized to disposable and 1 randomized to AJCC AMERICAN JOURNAL OF CRITICAL CARE, November 2014, Volume 23, No. 6 463 Table 1 Demographics of 7240 patients in the study A. Continuous factors Mean (95% CI) Factor Reusable Days in intensive care unit Age, y Charlson Comorbidity Index Days in hospital Disposable Difference P 3.61 (3.44-3.77) 3.62 (3.47-3.76) 0.01 (-0.21-0.23) .94 62.83 (62.30-63.36) 62.29 (61.82-62.76) -0.54 (-1.25-0.17) .13 2.48 (2.40-2.55) 2.63 (2.56-2.70) 0.15 (0.05-0.25) .002 21.79 (21.02-22.57) 22.06 (21.41-22.72) 0.27 (-0.75-1.28) .60 B. Categorical factors Probability (95% CI) Reusable Disposable Discharge disposition Home Not home .38 (.36-.41) .62 (.59-.64) .35 (.32-.37) .65 (.63-.68) Sex Male Female .55 (.52-.58) .45 (.42-.48) .56 (.53-.59) .44 (.41-.47) Insurance type Government/self-pay Commercial .47 (.44-.50) .53 (.50-.56) .46 (.43-.49) .54 (.51-.57) Marital status Other Married .48 (.45-.51) .52 (.49-.55) .46 (.43-.49) .54 (.51-.57) Race White Nonwhite .79 (.76-.81) .21 (.19-.24) .77 (.74-.79) .23 (.21-.26) No. of infections per 100 patient days Factor .03 .69 .62 .21 .33 2.0 1.5 1.0 0.5 P = .48 P = .47 P = .47 Cardiovascular Medical Surgical P = .72 0.0 Neurological Type of intensive care unit Disposable Reusable Figure 2 Comparison of rate of infection between disposable and reusable electrocardiography lead wire by type of intensive care unit (N = 7240). Infections included bloodstream infections and ventilator-associated pneumonia for all types of intensive care units, with sternal surgical site wound infections also included for cardiovascular intensive care units. 464 P cleaned, reusable ECG-LWs), and 956 cases from the 2 matched neurological ICUs. Patients’ demographics were similar for most factors studied, except for discharge disposition and mean CCI score. Patients randomized to the disposable ECG-LW group were less likely to be discharged home and had a moderately higher CCI, both of which reflected higher acuity in patients randomized to disposable ECG-LWs (Table 1). Overall, the infection rate remained very low throughout the trial period, with only 86 BSIs, cases of VAP, or SSIs among 74 patients. Thus slightly more than 1% of the study population had an infection develop as defined by the research protocol. Of 61 BSIs, 16 (26%) were determined to be BSIs associated with a central catheter. A total of 19 cases of VAP and 6 cases of SSI occurred. No difference in total infection rate (BSI + VAP + SSI) was apparent between disposable and reusable ECG-LW groups based on 100 patient days; paired unadjusted relative risk (95% CI) was 1.35 (0.99-1.83; P = .06). Per matched ICUs, total infection rates per group did not differ by type of ICU (Figure 2). In addition, AJCC AMERICAN JOURNAL OF CRITICAL CARE, November 2014, Volume 23, No. 6 www.ajcconline.org Table 2 Multivariate analyses of infection rates between electrocardiographic lead wire groups after adjusting for discharge disposition and comorbidity index Infection type Disposable, No. (rate/100) Reusable, No. (rate/100) Paired, relative risk (95% CI) Paired P Full sample of cases (N = 7240) Alla BSI BSI + SSI 56 (0.379) 41 (0.277) 45 (0.304) 30 (0.260) 20 (0.173) 22 (0.191) 1.35 (0.94-1.95) 1.40 (0.91-2.16) 1.49 (0.97-2.29) .10 .12 .07 28 (0.313) 19 (0.213) 20 (0.224) 1.43 (0.93-2.19) 1.43 (0.89-2.30) 1.59 (0.97-2.61) .10 .14 .07 Sample with length of stay > 48 hours; n = 2578 Alla BSI BSI + SSI a 55 (0.479) 40 (0.349) 44 (0.383) Bloodstream infection (BSI) + ventilator associated pneumonia + sternal surgical site infection (SSI). each type of infection per group did not differ by type of ICU: BSI (P values, .61-.72), VAP (P values, 0.38-0.91), and SSI (P = .36; cardiovascular surgery ICU only). In the 2578 cases that involved an ICU stay longer than 48 hours, no difference in total infection rate based on 100 patient days was found between disposable and reusable ECG-LW groups (paired unadjusted relative risk [95% CI], 1.43 [0.97-2.12], P = .07), and no differences per group were apparent for each paired ICU environment, (P values, .39-.51). In multivariate analyses, after discharge disposition and CCI were adjusted for, no differences in total infection rates were apparent between ECG-LW groups for the full sample or for cases where the ICU stay was greater than 48 hours (Table 2). When just BSI rates and BSIs and SSIs combined were assessed, the relative risk of infection between groups remained relatively unchanged. Time to first infection was compared between groups to determine if disposable ECG-LWs would lengthen time to infection occurrences. Total infection rates, BSI, or BSI plus SSI did not differ between groups (P values, .26-.97). After discharge disposition and CCI were controlled for between groups, no differences were found in time to first infection. The disposable ECG-LW versus reusable ECG-LW hazard ratio (95% CI) for all infections was 1.21 (0.87-1.69; P = .25); for BSI, it was 1.45 (0.68-3.09; P = .34); and for BSI plus SSI, it was 1.40 (0.81-2.43; P = .23). Similar to the full sample, no differences in time to first infection were apparent between groups for the 2578 cases with ICU stays longer than 48 hours; P values were from .26 to .97. After discharge disposition and comorbid conditions were controlled for, hazard ratios for total infection, BSI, and BSI plus SSI were similar to hazard ratios for the full sample with P values of .23 to .33. www.ajcconline.org Discussion In this randomized controlled trial, the overall infection rate throughout the 1-year period was very low and stable over time, and infection rates did not differ between patients receiving nonsterile disposable ECG-LWs and patients receiving cleaned, reusable ECG-LWs. Before the start of the study, a much higher infection rate (0.9 per 100 ICU days) was seen among the hospital’s adult ICUs. Implementation of infection control practices drastically reduced the infection rate during the study. In the literature, clinicians suggested that reusable ECG-LWs might lead to cross-contamination of microorganisms, including resistant bacteria, and be a culprit in HAIs.15,21,22 Our findings represent new knowledge and provide evidence that reusable ECG-LWs are not more likely to be a source of pathogens that lead to HAIs. Further, our cardiovascular surgery ICUs cleaned reusable ECG-LWs by ultrasound. Previously, ultrasound cleaning of ECG-LWs was hypothesized to be the reason why fewer bacteria grew on ECG-LWs in ICUs.12 In this study, both the disposable and reusable cardiovascular surgery ICU ECG-LW groups had fewer HAIs than patients in other ICU environments; however, no between-group differences in the rate of HAIs were found. Thus, ultrasound cleaning of reusable ECG-LWs did not offer benefit over the cleaning practices used in the other adult ICUs and did not provide an explanation for the lower incidence of HAIs among the cardiovascular ICUs. Some hypotheses may explain our results. First, once clean, disposable ECG-LWs are removed from their original packaging, the risk of contamination with resistant microorganisms via handling and exposure to environmental factors (including health The groups did not differ in total infection rates for cases with an intensive care unit stay longer than 48 hours. AJCC AMERICAN JOURNAL OF CRITICAL CARE, November 2014, Volume 23, No. 6 465 care providers’ hands, airborne particulates associated with coughing or sneezing, and open wounds) is the same as the risk for cleaned, reusable ECGLWs. Risk of cross-contamination may be reduced initially, but the period of risk reduction might be very short, depending on environmental cleanliness and hand-washing practices of staff. In this research, we found no differences between groups in time to infection development based on the type of ECGLWs used. The first assessment was at 3 days after ICU admission. Therefore, any possible advantage of disposable ECG-LWs based on the assumption that reusable ECG-LWs would have a heavier burden of microorganisms from inefficient disinfection during cleaning was negated fairly quickly if it was a factor at all. Because disposable ECG-LWs are not sterile before use, it is unknown if microorganisms were present before patient contact, due to handling during packaging. Second, clinicians should not assume that exposure to resistant bacteria and other microorganisms found on ECG-LWs, no matter if the burden is heavy or light, automatically increases the occurrence of HAIs. Bacteria grow on many inanimate objects found in hospital ICU environments,23 and common nosocomial pathogens may survive or persist on surfaces for months,24 yet HAIs do not develop in most patients who are not immunocompromised. In this study, 3 of the 4 ICU environments included patients with surgical wounds, exposed incisions, and drains or catheters across the chest and abdomen that could have come in contact with the ECG-LWs. Because the infection rates did not differ between groups among matched ICUs, the rate of exposure of ECG-LW to open incisions and wounds was probably equal among disposable and reusable ECG-LWs and was not a factor in the risk of HAI. Finally, many hospitals have a bundled infection control program, especially in ICUs. Bactericidal solutions are used to bathe patients and clean equipment; adherence to optimal hand-washing techniques is monitored; intravenous, urinary, and other catheters are removed as soon as possible to stop infection; VAP prevention protocols are commonly used; and early mobility and extubation are encouraged. The combination of efforts that may have also included use of nonsterile disposable ECG-LWs, could have resulted in a reduction in the rate of HAI. For most bundled programs, it is difficult to determine the components that are truly effective in achieving Infection rates were very low and stable with no differences between disposable and reusable wires. 466 outcomes. In a review of the literature on transmission of methicillin-resistant Staphylococcus aureus, risk factors varied, but the most commonly reported factor was carriage from poor infection control/hand hygiene practices among health care workers. Other less common factors were patients’ comorbid conditions and recent use of antibiotics. One of 4 risk factors for persistence of transmission despite eradication included environmental contamination; the others were patient-centric factors such as comorbid conditions, mupirocin resistance, and sites of colonization.25 Thus, transmission of microorganisms to patients was most likely from personnel and patient factors, not environmental contamination. Based on results of this study, ECG-LW type alone may not provide HAI risk reduction. A bundled approach may be a more effective strategy for reducing HAIs related to BSI, VAP, or sternal SSI; however, hand hygiene is the most important intervention to prevent pathogen spread and reduce the occurrence of HAIs. This research has limitations. The research setting was a single center; however, it was uniquely suited to the study design because it is one of very few hospitals in the United States with multiple matched ICU environments near one another. The rate of HAIs from BSIs, VAP, and sternal wound SSIs was much lower than originally assumed when the study was powered; thus, the confidence intervals surrounding the relative risk and hazard ratios are wide. Methods of cleaning reusable ECG-LWs varied by unit, and health care providers were not blinded to interventions because the disposable ECG-LWs were a different color than the reusable ECG-LW system. However, the study was conducted for a long period, and the risk of bias due to various cleaning techniques and nonblinding was minimal, especially because use of ECG-LWs was the standard of care. Reusable ECG-LWs were occasionally discarded, so patients in the reusable ECG-LW group who were recipients of a newly opened reusable ECG-LW set mimicked patients in the disposable ECG-LW group. Our large sample size of more than 7000 cases minimized this limitation. Conclusion Disposable ECG-LWs may offer advantages to patient care in an ICU, including a reduction in initial exposure to microorganisms that are found on cleaned, reusable ECG-LWs; however, HAI rates did not differ between patients who received clean, reusable ECG-LWs and patients who received nonsterile, disposable ECG-LWs. Nurses must assess other cross-contamination pathways that might minimize or eliminate HAIs. AJCC AMERICAN JOURNAL OF CRITICAL CARE, November 2014, Volume 23, No. 6 www.ajcconline.org FINANCIAL DISCLOSURES The study was partially supported by a research grant from Covidien in Mansfield, Massachusetts. eLetters Now that you’ve read the article, create or contribute to an online discussion on this topic. Visit www.ajcconline.org and click “Responses” in the second column of either the full-text or PDF view of the article. SEE ALSO For more about disposable vs reusable electrocardiography leads, visit the Critical Care Nurse Web site, www.ccnonline.org, and read the article by Brown, “Disposable vs Reusable Electrocardiography Leads in Development of and Cross-contamination by Resistant Bacteria” (June 2011). REFERENCES 1. Fukuta Y, Cunningham CA, Harris PL, Wagener MM, Muder RR. Identifying the risk factors for hospital-acquired methicillin-resistant Staphylococcus aureus (MRSA) infection among patients colonized with MRSA on admission. Infect Control Hosp Epidemiol. 2012;33(12):1219-1225. doi:10.1086 /668420. 2. Song X, Chen Y, Li X. Differences in incidence and outcome of ventilator associated pneumonia in surgical and medical ICUs in a tertiary hospital in China [published online April 4, 2014]. Clin Respir J. 2014;8(3):262-268. doi: 0.1111/crj.12036. 3. Glance LG, Stone PW, Mukamel DB, Dick AW. Increases in mortality, length of stay, and cost associated with hospitalacquired infections in trauma patients. Arch Surg. 2011;146(7): 794-801. doi:10.1001/archsurg.2011.41. 4. The Joint Commission. Preventing Central Line–Associated Bloodstream Infections: A Global Challenge, a Global Perspective. Oak Brook, IL: Joint Commission Resources; 2012. http://www.jointcommission.org/assets/1/18/clabsi _monograph.pdf. Accessed July 29, 2014. 5. Johnson D, Lineweaver L, Maze LM. Patients’ bath basins as potential sources of infection: a multicenter sampling study. Am J Crit Care. 2009;18(1):31-38. 6. Ota K, Profiti R, Smaill F, Matlow AG, Smieja M. Identification badges: a potential fomite? Can J Infect Control. 2007; 2(162):165-166. 7. Kotsanas D, Scott C, Gillespe EE, Korman TM, Stuart RL. What’s hanging around your neck? Pathogenic bacteria on identity badges and lanyards. Med J Aust. 2008;188(1):5-8. 8. Runner JC. Bacterial and viral contamination of reusable sharps containers in a community hospital. Am J Infect Control. 2007;35:527-530. 9. Marinella MA, Pierson C, Chenoweth C. The stethoscope: a potential source of nosocomial infection? Arch Intern Med. 1997;157:786-790. www.ajcconline.org 10. Devine J, Cooke RP, Wright EP. Is methicillin-resistant Staphylococcus aureus (MRSA) contamination of wardbased computer terminals a surrogate marker for nosocomial MRSA transmission and handwashing compliance? J Hosp Infect. 2001;48:72-75. 11. Brennan SA, Walls RJ, Smyth E, Al Mulla T, O’Byrne JM. Tourniquets and exsanguinators: a potential source of infection in the orthopedic operating theater? Acta Orthop. 2009;80:251-255. 12. Albert NM, Hancock K, Murray T, et al. Cleaned, ready-touse, reusable electrocardiographic lead wires as a source of pathogenic microorganisms. Am J Crit Care. 2010;19(6): e73-80. doi:10.4037/ajcc2010304. 13. Falk PS, Winnike J, Woodmansee C, Desai M, Mayhall CG. Outbreak of vancomycin-resistant enterococci in a burn unit. Infect Control Hosp Epidemiol. 2000;21:575-582. 14. Hayes RJ, Bennett S. Simple sample size calculation for cluster randomized trials. Int J Epidemiol. 1999;28:319-326. 15. Charlson ME, Pompei P, Ales KL, MacKenzie CR. A new method of classifying prognostic comorbidity in longitudinal studies: development and validation. J Chronic Dis. 1987;40:373-383. 16. Singh B, Bhaya M, Stern J, et al. Validation of the Charlson comorbidity index in patients with head and neck cancer: a multi-institutional study. Laryngoscope. 1997;107(11 Pt 1): 1469-1475. 17. Chaudhry S, Jin L, Meltzer D. Use of a self-report-generated Charlson Comorbidity Index for predicting mortality. Med Care. 2005;43:607-615. 18. D’Hoore W, Bouckaert A, Tilquin C. Practical considerations on the use of the Charlson comorbidity index with administrative data bases. J Clin Epidemiol. 1996;49:1429-1433. 19. Sundararajan V, Henderson T, Perry C, Muggivan A, Quan H, Ghali WA. New ICD-10 version of the Charlson comorbidity index predicted in-hospital mortality. J Clin Epidemiol. 2004;57:1288-1294. 20. Fried L, Bernardini J, Piraino B. Charlson comorbidity index as a predictor of outcomes in incident peritoneal dialysis patients. Am J Kidney Dis. 2001;37:337-342. 21. Barnett TE. The not-so-hidden costs of surgical site infections. AORN J. 2007;86:249-258. 22. Brown DQ. Disposable vs reusable electrocardiography leads in development of and cross-contamination by resistant bacteria. Crit Care Nurs. 2011;31(3):62-68. 23. Boyce JM. Environmental contamination makes an important contribution to hospital infection. J Hosp Infect. 2007; 65:50-54. 24. Kramer A, Schwebke I, Kampf G. How long do nosocomial pathogens persist on inanimate surfaces? A systematic review. BMC Infect Dis. 2006;6:130. 25. Albrich WC, Harbarth S. Health-care workers: source, vector, or victim of MRSA? Lancet Infect Dis. 2008;8:289-301. To purchase electronic or print reprints, contact the American Association of Critical-Care Nurses, 101 Columbia, Aliso Viejo, CA 92656. Phone, (800) 899-1712 or (949) 362-2050 (ext 532); fax, (949) 362-2049; e-mail, [email protected]. AJCC AMERICAN JOURNAL OF CRITICAL CARE, November 2014, Volume 23, No. 6 467 CNE Test Test ID A1423063: Infection Rates in Intensive Care Units by Electrocardiographic Lead Wire Type: Disposable vs Reusable Learning objectives: 1. Compare infection rates of patients in intensive care units who received disposable electrocardiographic (ECG) leads vs reusable ECG leads. 2. Identify sources of microorganisms that may promote hospital-acquired infections. 3. State the role of disposable ECG leads in a bundled infection control program. 1. Which of the following trial designs is used in the study? a. Nonrandomized, comparative b. Qualitative, ethnography c. Cluster randomized, controlled d. Cross-sectional, descriptive 2. The unblinded trial was completed in Ohio in which type of site? a. A secondary-care community center b. A quaternary-care urban medical center c. A Veterans Affairs medical center d. A primary and home care health system 3. How many neurological intensive care units (ICUs) were included in the study? a. 2 c. 3 b. 4 d. 5 4. Out of all units in the study, which of the following units did not have environmental service workers clean the reusable electrocardiographic (ECG) leads? a. General surgery c. Neurological ICU b. Medical ICU d. Cardiovascular ICU 5. Rates of surgical site infections were retrieved from data routinely collected for which of the following organizations? a. Society of Thoracic Surgeons b. Society of Critical Care Medicine c. Society for Neuroscience d. Society of General Internal Medicine 6. In the study, the Charlson Comorbidity Index was used as a surrogate for which of the following? a. Infection burden c. Mortality rate b. ICU readmission d. Patient acuity 7. How long was the data collection period? a. 3 months c. 9 months b. 6 months d. 12 months 8. How many total cases were enrolled in the study? a. 1484 c. 1540 b. 7240 d. 3260 9. In this study, patient characteristics differed between groups for which of the following? a. Insurance type and marital status b. Marital status and discharge disposition c. Discharge disposition and Charlson Comorbidity Index d. Charlson Comorbidity Index and insurance type 10. In the review of literature on transmission of methicillin-resistant Staphylococcus aureus, the most commonly reported risk factor was which of the following? a. Environmental contamination b. Poor hand hygiene practices c. Comorbid conditions d. Recent use of antibiotics 11. Of the study sample, what was the mean hospital length of stay (days) for patients? a. 2.6 c. 63 b. 3.6 d. 22 12. According to Figure 1, which of the following was the most common reason for being excluded from analysis? a. Did not receive assigned ECG lead wires b. On unit more than 48 hours before the study start date c. On study unit for less than 24 hours d. On unit for multiple days after enrollment stopped Test ID: A1423063 Contact hours: 1.0; pharma 0.0 Form expires: November 1, 2017. Test Answers: Mark only one box for your answer to each question. 1. ❑ a ❑b ❑c ❑d 2. ❑ a ❑b ❑c ❑d 3. ❑ a ❑b ❑c ❑d 4. ❑ a ❑b ❑c ❑d 5. ❑ a ❑b ❑c ❑d 6. ❑ a ❑b ❑c ❑d 7. ❑ a ❑b ❑c ❑d 8. ❑ a ❑b ❑c ❑d 9. ❑ a ❑b ❑c ❑d 10. ❑ a ❑b ❑c ❑d 11. ❑ a ❑b ❑c ❑d 12. ❑ a ❑b ❑c ❑d Fee: AACN members, $0; nonmembers, $10 Passing score: 9 correct (75%) Category: CERP A Test writer: Darlene Pileski, ACNP Program evaluation For faster processing, take this CNE test online at www.ajcconline.org (“CNE Articles in This Issue”) or mail this entire page to: AACN, 101 Columbia, Aliso Viejo, CA 92656. Name Yes ❑ ❑ ❑ Objective 1 was met Objective 2 was met Objective 3 was met Content was relevant to my nursing practice ❑ My expectations were met ❑ This method of CE is effective for this content ❑ The level of difficulty of this test was: ❑ easy ❑ medium ❑ difficult To complete this program, it took me hours/minutes. No ❑ ❑ ❑ ❑ ❑ ❑ Address City Country State AACN Customer ID# Phone Payment by: Card # ZIP E-mail address* ❑ Visa ❑ M/C ❑ AMEX ❑ Check Expiration Date Signature *E-mail address required to receive notification of completion, access to your test results, and certificate for passing scores. The American Association of Critical-Care Nurses is accredited as a provider of continuing nursing education by the American Nurses Credentialing Center’s Commission on Accreditation. AACN has been approved as a provider of continuing education in nursing by the State Boards of Nursing of Alabama (#ABNP0062), California (#CEP1036) and Louisiana (#LSBN12). AACN programming meets the standards for most other states requiring mandatory continuing education credit for relicensure.








© Copyright 2026