ABC
docz
Explore
Log in
Create new account
Download
Report
No category
PRIOR AUTHORIZATION REQUEST FORM Well Sense Non-Preferred Medications Policy NH 9.302
Prior Authorization Cover Sheet - Santa Clara Family Health Plan
Topical Immunomodulators PA Form
PSMS New Hire Document Checklist and Fax Cover Sheet TO:
Hepatitis C Virus (HCV) Medication Prior Authorization Victrelis
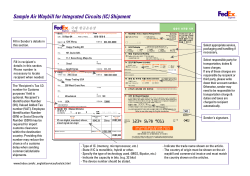
Sample Air Waybill for Integrated Circuits (IC) Shipment
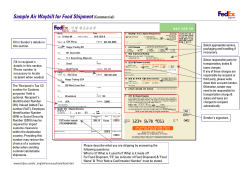
Sample Air Waybill for Food Shipment (Commercial)
School District: __________________________ School: ____________________________ Grade: _________
STUDENT EMERGENCY CONTACT CARD
Contra Costa Health Plan Prior Authorization Form 61-211
TOWN OF AMHERST YOUTH
Basic Business Letter Format
Dr. Emad Guirguis
© Copyright 2026
About abcdocz
DMCA / GDPR
Report