
System Quality Review SPECIAL ISSUE PROCEEDINGS OF THE SYMPOSIUM
System Quality Review
SPECIAL ISSUE
PROCEEDINGS OF THE SYMPOSIUM
Quality 2020: A Vision of the Future
November 21, 2014
Co-sponsored with the Healthcare Association of New York State &
Greater New York Hospital Association
Editorial Board
Steven J Corwin, MD
Chief Executive Officer
NewYork-Presbyterian Hospital and Healthcare System
Wayne M Osten
Karen S Westervelt
Henry H Ting, MD, MBA
Brian K Regan, PhD
Robert E Kelly, MD
President
NewYork-Presbyterian Hospital
Karen A Scott, MD
____________________________________
Aileen Alapan Maderich, MBA
Laura L Forese, MD MPH
Group Senior Vice President & Chief Operating Officer
NewYork-Presbyterian Hospital/Weill Cornell
President, NewYork-Presbyterian Healthcare System
Arthur J Hedge, Jr.
Trustee, NewYork-Presbyterian Hospital and Healthcare
System
Grimilda Mendez-Augsburg, MBA
Marcia Brinson, RD MPH
Kathleen Ciccone, RN MBA
Yael Coppleson, MPH
Natalee Hill, MPA
Marc L Boom, MD MBA FACHE
President & Chief Executive Officer
Houston Methodist (Houston, Texas)
Roberta L Schwartz, PhD
Executive Vice President
Houston Methodist Hospital (Houston, Texas)
Debra L Hollenberg, RN MSN
Patricia Keill, RN
Nancy Landor, RN MS CPHQ
I-Fong S Lehman, PhD
Christy Listenbee, MHA
Robert A Phillips, MD PHD FACC
Executive Vice President & Chief Medical Officer
Houston Methodist (Houston, Texas)
President & Chief Executive Officer
Houston Methodist Specialty Physician Group
Jamie R MacDonald, RN MSN MBA
Tochi N Okorie, MBA RN
Scott W Possley, PA-C MPAS
Stephen Rimar, MD MBA
Kenneth E Raske
President & Chief Executive Officer
Greater New York Hospital Association
Lorraine M Ryan, Esq RN
Dennis Whalen
Denise Stone, RN
President
Healthcare Association of New York State
Brian R Taylor, PhD
Steven Silber, DO, ScM
Alfred A Villacara, DMD
Acknowledgements
The editors of SQR gratefully acknowledge the assistance of Anna Malkin for her
dedication, organizational skills, and planning expertise. Gratitude is expressed most
especially to those practitioners and performance improvement leaders who show their
commitment to quality patient care through their contribution herein.
NewYork-Presbyterian Healthcare System Quality Symposium 2014
Quality 2020: A Vision of the Future
2014 System Quality Review Special Issue
The NewYork-Presbyterian Healthcare System Quality Symposium is an annual event
co-sponsored by NewYork-Presbyterian Healthcare System and the Houston
Methodist System in collaboration with HANYS and GNYHA. A key feature of our
Quality Symposium has been the opportunity for hospitals to submit abstracts for
inclusion in the NewYork-Presbyterian System Quality Review (SQR) Special Issue.
This SQR Special Issue is a compilation of all abstracts submitted. Abstracts go
through a peer-review process and authors of highly-rated abstracts are invited to
present at the poster session during the Quality Sympoisum. Highly-rated abstracts are
identified with a ribbon. Thank you to all hospitals who submitted abstracts. Your
abstract submissions contributed to the success of this year’s SQR Special Issue.
System Quality Review
1
NewYork-Presbyterian Healthcare System Quality Symposium 2014
Quality 2020: A Vision of the Future
Table of Contents
1. Columbia University, Department of Biomedical Informatics ............................................................14
Impact of Noise on Clinical Performance in the ED: Compromising Patient Safety
Mary L. Little, RN, MSN1; Osman R. Sayan, MD2; Edward H. Suh, MD2; Vimla L. Patel, PhD1,3
1Dept. of Biomedical Informatics, Columbia University; 2New York-Presbyterian Hospital; 3New York Academy of
Medicine, New York, NY
2. Burke Rehabilitation Hospital............................................................................................................. 20
Patient/Family Participation in Multidisciplinary Rounds Conferences: A Pilot Program in an Inpatient
Rehabilitation Hospital
Kristen Bonistall, MS, MSW; Donna Russo, LCSW, CCM; Richard Novitch, MD, Adina Safdeye
3. Cohen Children's Medical Center of New York .................................................................................. 23
Improving Discharge Velocity: Testing the Visual Communication About Throughput (V-CAT) Board
Kathy Albert, RN, DNP; Brian Belpanno, MBA; Nancy Palumbo, MD; Diane Diver, RN, MSN, Helen Scott,
MD
4. Cohen Children's Medical Center of NY ............................................................................................. 28
Implementation of a Standard Urinary Catheter Process Eradicates CAUTI's at a Single Pediatric Tertiary
Care Center
Aaron Kessel, MD; Kathy Albert, RN; Samantha Fensterman, RN; Colleen O'Hara, RN; Fiona Levy, MD
5. Cohen Children's Medical Center of NY ............................................................................................. 33
Making Joint Commission Continuous Readiness Fun and Easy
Karen Halom RN MS, Assistant Direct Quality Management, Cohen Children's Medical Center of NY
6. Cohen Children's Medical Center of NY, NS-LIJ Hofstra Medical School ........................................ 36
S.K.I.N.D.E.E.P Tool for Pressure Ulcer Prevention in Critical Neonatal and Pediatric Population
Undergoing Extracorporeal Membrane Oxygenation (ECMO)
Vita Boyar, MD,FFAP, CWCP, FAPWCA; Karen Clemens,RN; Marcia Zinger,RN
7. Elmhurst Hospital Center.................................................................................................................... 39
Evolving Towards High Reliability in the Operating Room: Design and Implementation of a New Surgical
Safety Process
Benjamin D. Malkin, MD; Roderick A. Calandria, RN, MSN, CCRN, BC; Carol White, MPH; William
McDonagh, RN, BSN, MPA
System Quality Review
2
NewYork-Presbyterian Healthcare System Quality Symposium 2014
Quality 2020: A Vision of the Future
8. Hospital for Special Surgery .................................................................................................................41
A Case Series of Understanding Ileus: A Potentially Fatal Complication of Orthopedic Surgery
Kelianne Cummings, BA; Sara Choi, BA; Ting Jung Pan, MPH; Allina Nocon, MPH; Mayu Sasaki, MPH; Lisa
A. Mandl, MD, MPH; Steven Magid, MD; Susan M. Goodman, MD
9. Hospital for Special Surgery, Quality Research Center ....................................................................... 44
Falls Among Hospitalized Orthopedic Patients: A Prospective Case-Control Study
Mayu Sasaki, MPH; Lisa A. Mandl, MD MPH; Wei-Ti Huang, MSc; Ting Jung Pan, MPH; Jaimie Lee; Tina
Bailey, MS; Eric Greenberg, PharmD; Danielle Edwards, DPT; Patricia Quinlan, PhD, MPA RN; and Steven K.
Magid, MD
10. Houston Methodist Hospital .............................................................................................................. 46
Pharmacist Active Involvement in Patient’s Continuity of Care After Hospital Discharge
Rafael Felippi, PharmD, BCPS; Michael Liebl, PharmD, BCPS; Janice Finder, RN, MSN
11. Jacobi Medical Center......................................................................................................................... 48
A Multidisciplinary Patient Navigation Program Improves Compliance with Adjuvant Breast Cancer
Therapy in a Public Hospital
Maria T. Castaldi, MD, FACS; Dina Podolsky, MD; Saman Safadjou, MD; John McNelis, MS, FACS
12. Kings County Hospital Center.............................................................................................................51
A Lean Approach to Refine Observation Monitoring at Kings County Behavioral Health Services
Linda Paradiso, RN, MSN, NEA-BC; Renuka Ananthamoorthy, MD; Jill Bowen, PhD; Roumen Nikolov, MD;
Chao Ma
13. Kings County Hospital Center............................................................................................................ 55
Kings County Hospital Behavioral Health Ongoing Journey to Safety
Louise Wright-Browne, RN-BC, MA; Rita Hall-Hutchinson, RN, MSN-ANP, MA; Anne Paulin, MS, CPHRM;
Liliane Rocha, BCBA, LBA; Renuka Ananthamoorthy, MD; Roumen Nikolov, MD; Linda Paradiso, RN, MSN,
NEA-BC; Jill Bowen, PhD; Karen Quick, PhD, Chao Ma
14. Kings County Hospital Center............................................................................................................ 58
From Restrictive to Non Restrictive Interventions: A Culture Shift in Managing Challenging Behaviors at
Kings County Hospital Behavioral Health Services
Liliane Rocha, BCBA, LBA; Jill Bowen, PhD; Renuka Ananthamoorthy, MD; Roumen Nikolov, MD; Linda
Paradiso, RN, MSN,NEA-BC; Chao Ma
15. Krasnoff Quality Management Institute - a Division of the North Shore-LIJ Health System ........... 62
Using Death to Understand Disease
Kevin D. Masick, PhD; Marcella De Geronimo, MS; Jacqueline Parrish MSN, RN; Mark Jarrett, MD
System Quality Review
3
NewYork-Presbyterian Healthcare System Quality Symposium 2014
Quality 2020: A Vision of the Future
16. Memorial Sloan Kettering Cancer Center ........................................................................................... 65
An Interdisciplinary Approach to Minimize the Use of Therapeutic Duplicate Pain Medications in a
Comprehensive Cancer Center
Priti Patel, BS, RPh; Raymond J. Muller, MS, RPh; Vivek Malhotra, MD, MPH; Damon Douglas, PharmD,
MBA, MS; Svetlana Granovsky, MS; Donna Robinson; Lauren Koranteng, PharmD; Mary Dowling, MSN, RN;
James Gillson, MPH.; Leonard Saltz, MD
17. Memorial Sloan Kettering Cancer Center, Department of Surgery .................................................... 69
Decreased Incidence of Post-Operative Venous Thromboembolism Following a Multi-Specialty Quality
Improvement Initiative at a Specialty Cancer Center
Mindy Sovel MA; Daniel D. Sjoberg MA; Margaret McSweeney NP; Damon Douglass PharmD MBA MS; Vivian
E. Strong MD; Nicola Fabbri MD; Gerald A. Soff MD; Inderpal (Netu) Sarkaria MD
18. New York Hospital Queens - Emergency Medical Associates .......................................................... 72
Improving Pre-Hospital and Trauma Team Activation for Injured Older Adults Age 65 Years or Older
Presenting to the Emergency Department
Radeos, Michael S MD MPH; Kaldis, Vasileios MD; Ali, Zuhair MD: Torres, Jose MD; Jazarevic, Slobodan MD;
Sample, Jason MD; Zimmermann, Mary Ellen BSN CEN, Ourian, Ariel MD; Dickason, Robert M MD
19. New York Hospital Queens - Emergency Medical Associates .......................................................... 75
Reducing the Use of Computed Tomography Scans for the Diagnosis of Acute Appendicitis by Using
Ultrasound as the Sole Diagnostic Study
Radeos, Michael S. MD MPH; Kaldis, Vasileios MD; Ali, Zuhair MD; Triantos, Georgios-Efthymios MD; Babovic,
Maja MD; Khin, Sandi MD
20. New York Hospital Queens................................................................................................................ 78
A Hospital's Journey to Stage 2 Meaningful Use
Kenneth R. Ong, MD, MPH; Camela Morrissey; Caroline Keane; Bebe Rahamatalli, PA
21. New York Hospital Queens.................................................................................................................91
Measures Taken To Improve The Rate of Documentation of Sonographic FAST Exams Performed in
Blunt Trauma Presentations
Nick Copeli MD, Mary Ellen Zimmerman RN, Manish Sharma DO, Zuhair Ali MD, Michael S. Radeos MD,
MPH, Mark Kindschuh MD, Jason Sample MD, N Khan MD, Nidhi Garg MD
22. New York Hospital Queens................................................................................................................ 95
A Multidisciplinary Team Approach to Morning Report Improves Core Measures in Critical Care
James Gasperino MD, PhD, MPH; Luciano Lemos-Filho, MD, MS; Keziah S. Narayana-jaya, PA; Mimi Lim
RN; Stephanie Barrett, MD; Michael Hansen, MD, Divya Sohal, MD; Qi-Ming Zhu, MD, Melvin Hochman, MD;
Seema Kurian, RN
System Quality Review
4
NewYork-Presbyterian Healthcare System Quality Symposium 2014
Quality 2020: A Vision of the Future
23. New York Hospital Queens................................................................................................................ 98
Impact of Antibiotic Stewardship Program Interventions on Multi-drug Resistant Organism Resistance
Rates and Hospital Costs
Nishant Prasad MD; Nathan Warren RPA-C; Anna Kula RPA-C; Noriel Mariano; Carl Urban PhD; Deborah
Figueroa BS PharmD; Sorana Segal-Maurer MD
24. New York Hospital Queens............................................................................................................... 102
Analysis of Low Intensity ICU Staffing Model at NYHQ
Ronni Levy MD, James A. Gasperino MD, PhD, MPH, Michael S. Radeos MD, MPH, Zuhair Ali MD, Sun Mon
Aye MD, Nidhi Garg MD
25. New York Hospital Queens............................................................................................................... 104
Intervention and Medical Documentation of Hospital Acquired Hypoglycemic Episodes – A Retrospective
Chart Review Study
Mark Vinelli, DO; Jing Guo, MD; Tagenarayan Niwaz, DO; Nejat Zeyneloglu, MD; Roxana Lazarescu, MD
26. New York Hospital Queens............................................................................................................... 109
Impact of Palliative Care Program on Utilization of Tracheostomies
Cynthia X Pan MD; Cristina Gutierrez MD; Min Min Maw MD; Amanda Kansler MPH, CCRP; Liam Gross
MD; Romana Kanta MD; Subroto Paul MD
27. New York Methodist Hosital............................................................................................................. 112
Standardization of Diabetic Foot Infection Admissions: A Review of Current Guidelines with Generalized
Recs.
Kirsti A. Diehl, DPM; Eric C. Storts, DPM; Kirsten L. Barisonek, DPM; Ronald L. Soave, DPM
28. New York Methodist Hospital........................................................................................................... 114
Improving Inpatient Satisfaction
Anthony Mungo; Michael Ficorelli; Alfred Usuriello; Steven Garner, M.D
29. New York Methodist Hospital........................................................................................................... 116
NICU Radiation Reduction "Sucess Story"
Steven Garner, MD; Claudia Lapidus, MD; Anthony Mungo; Michael Ficorelli; Alfred Usuriello
30. New York Methodist Hospital........................................................................................................... 120
Optimizing the Accuracy and Utility of Surgical Outcomes Data Through the Integrated Use of COQPIT
and the American College of Surgeons Surgeon Specific Registry
James C Rucinski MD, FACS; Diren Patel MD; Amani Jambhekar MD; Donald A Risucci PhD; Anthony J
Tortolani MD, FACS
System Quality Review
5
NewYork-Presbyterian Healthcare System Quality Symposium 2014
Quality 2020: A Vision of the Future
31. New York Methodist Hospital........................................................................................................... 127
Twice Daily Interdisciplinary Rounding Decreases Length of Stay Index on Medicine Units
Steven H. Silber, DO, ScM; Joanne Lagnese, RN; Joann Amitrano, RN; Dennis Laurence, MD; Zohirul Islam, MD;
Lily Fung
32. New York Methodist Hospital........................................................................................................... 132
Higher Success Rates in Difficult Venous Access Patients with Guidewire Associated Peripheral
Intravenous Catheter
Gerardo Chiricolo, MD, FACEP; Andrew Balk, MD; Wendy Wen, MD; Athena Mihailos, MD; Samuel Ayala,
MD; Ryan Giorgetti, MD
33. New York Methodist Hospital........................................................................................................... 136
Clinic "No Shows"- Boost Clinical Productivity
Eshan Patel, MD; Ashwad Afzal, MD; Janaki Patel, MD; Kamraan Madhani, MD; Parag Mehta, MD; Zohirul
Islam, MD; Mohammed Bashey, MD
34. New York Methodist Hospital........................................................................................................... 138
The "July Effect", Outdated or Still a Concern?
Ashwad Afzal MD; Iman Afzal MS; Eric Karu MD; Parag Mehta MD
35. New York Methodist Hospital........................................................................................................... 141
Better System, Better Team, Better Outcomes. Defeating Incomplete Medical Charts in a Community
Hospital Setting
Anna Avaliani, MD; Eric Karu, MD; Savath Chan; Parag Mehta, MD
36. New York Methodist Hospital........................................................................................................... 145
Pill Swallowing Physiology in Adults with Oropharyngeal Dysphagia
Riquelme, L.F., PhD, CCC-SLP, BCS-S; Tahhan, H.J., M.S., CCC-SLP; Teitcher, J.E. M.S., CF-SLP
37. New York Methodist Hospital........................................................................................................... 149
Physician Transition of Care: The Benefits of I-PASS and the Electronic Hand-Off System
Dr. Zainab Qayumi; Dr. Jasmine Walia; Dr. Bita Kharraz; Dr. Aamisha Gupta; Dr. Kandie Gearge; Dr. Usama
Samaan Dr. Nelson Eslao; Nayaab Khawarb, BS; Dr. Pramod Narula; Dr. Beata Dygulska
38. New York Methodist Hospital........................................................................................................... 155
Baby Boomers Beware: Implementation of a Hepatitis C Testing Protocol
Vahe Shahnazarian, MD MPH; Eric Karu, MD; Parag Mehta, MD, FACP
System Quality Review
6
NewYork-Presbyterian Healthcare System Quality Symposium 2014
Quality 2020: A Vision of the Future
39. New York Methodist Hospital........................................................................................................... 157
UTI & Dysphagia: Seeking Best Practice Patterns in Speech-Language Pathology
Rebecca D. Benjamin, M.S., CCC-SLP; Luis F. Riquelme, Ph.D., CCC-SLP, BCS-S; Laura M. Holtan, M.S.,
CCC-SLP
40. New York Methodist Hospital........................................................................................................... 161
Achieving the Goal of a Seemingly Impossible Task
Eric Karu MD; Parag Mehta MD
41. New York Methodist Hospital........................................................................................................... 166
New York Methodist Hospital Care Transition Management Interventions
Tiffany Bacchus FNP-BC, Amin Khalid MD MPH, Paraq Metha MD MPH
42. New York Methodist Hospital........................................................................................................... 168
High Value Cost Conscious Care
Eric Karu MD; Parag Mehta MD
43. New York Methodist Hospital........................................................................................................... 172
Implementing a Patient Check-In Scanner to Reduce Average Wait Times for Patients Receiving Radiation
Therapy
L. Tchelebi, MD; U. Gada, MBBS; K. Parikh, MD; S. McVorran, MHSA; H. Ashamalla, MD
44. New York Methodist Hospital........................................................................................................... 174
Using Social Media for Dynamic Curriculum on Demand
Eric Karu MD; Pauline Zaroovabeli MD; Parag Mehta MD; Sanjay Cherukuri MD
45. New York Methodist Hospital, Department of Speech-Language Pathology .................................. 177
NYM Dysphagia Screening: A Multidisciplinary Approach to Improving Compliance
Luis F. Riquelme, Ph.D., CCC-SLP, BCS-S, Speech-Language Pathology/Neurosciences; Barbara Gatton, M.D.,
Emergency Medicine; Rebecca D. Benjamin, M.S., CCC-SLP, Speech-Language Pathology; Jonathan S. Muller, MBA,
Neurosciences; Joshua E. Teitcher, M.S., CF, Speech-Language Pathology; Waleed Mina, Cerner Corporation
46. NewYork-Presbyterian Hospital ....................................................................................................... 181
Using Information Technology (IT) to Facilitate Infection Prevention and Control (IP&C) and
Communication during a Measles Outbreak
Maria Messina, RN, BSN, CIC1; Lesley Covington, MSPH; CIC1; Barbara Ross, RN, BSN, CIC2; Melissa
Stockwell, MD, MPH3,4; Mariellen Lane, MD5; Diane Mangino, RN, MSN, CIC1; Nancy Schneider, RN, MS,
CIC1; Krystal Balzer, RN, MSN1; Lilibeth Andrada, RN, MA, CIC, PNP1; Lisa Covington, RN, MPH, CIC1;
John D'agostino, RN, MSN, CIC1; Patrice Russell, RN, MSN, CIC1; Jean-Marie Cannon, RN, BSN, CIC1; Rohit
Chaudhry, MS6; Steven Kaplan, MD7,8; Helen Lee, MD, MPH9; David P. Calfee, MD, MS, FIDSA, FSHEA10;
Philip Graham III, MD, Msc11; Lisa Saiman, MD MPH3,12; E. Yoko Furuya, MD, MS13,14
System Quality Review
7
NewYork-Presbyterian Healthcare System Quality Symposium 2014
Quality 2020: A Vision of the Future
47. NewYork-Presbyterian/Lower Manhattan Hospital ........................................................................ 184
Adjustment for Admission Source and Other Clinical/Demographic Factors Does Not Abrogate the
Disparate Effects of Dementia on Hospitalization Discharge Disposition in Common Geriatric
Admissions
William Liao, BA; Robert Y Lin, MD; Brian C Scanlan, MD
48. NewYork-Presbyterian/Weill Cornell Medical Center...................................................................... 189
Pre-screening of Diabetic Patient Visits to Improve Point of Care A1C Utilization in an Outpatient
Resident Practice
William Zhang, MD; Marcus Goncalves, MD, PhD; Amanda Carmel, MD
49. NewYork-Presbyterian Hospital ....................................................................................................... 191
Improving Fistula Rates in Chronic ESRD Patients at NYP
Anthony Valeri, MD; Robin Ferrer, MSN, MBA; Ronald Vilotta, BSN; Taknida D. Tubo, MS
50. NewYork-Presbyterian Hospital ....................................................................................................... 195
Improving Efficiency by Automating Data
Elsie Binns-Irizarry, MS; Scott W. Possley, PA-C, MPAS; Peggy Liu, MS, RN; Brian Regan, PhD; Vanessa
Cheng; Hillary Shaw, MPA; Sarah Walker, MBA; Karthik Natarajan, PhD; Nicole Hitti, MSN; Linda Georges,
BSN
51. NewYork-Presbyterian/Columbia University Medical Center ......................................................... 198
Improving E-Prescribing Rates at Broadway Practice: a Resident-led QI Project
Jessica George, MD; Laura Robbins-Milne, MD; Mariellen Lane, MD
52. NewYork-Presbyterian/Weill Cornell Medical Center..................................................................... 203
Quality Improvement in Prostate Biopsy Fixation: Facilitation of Systems Review by Interdisciplinary
Housestaff Council
Ashley G Winter, MD; Paul J DiMaggio, MD; Ian R Drexler, MD; Zachary A Turnbull, MD; Susan L Faggiani,
RN BA CPHQ; Gregory E Kerr, MD MBA FCCM, Brian D Robinson, MD
53. NewYork-Presbyterian/Weill Cornell Medical Center..................................................................... 205
Keeping it Safe: A Multidisciplinary Approach to Creating a Culture of Safety
Barbara Alba, PhD(c), RN-IBCLC; Sara Pasciolla, RNC, MSN-Ed; Sharon Abramovitz, MD, Co-Director,
Obstetric Anesthesiology; Jeffery Jacinto, Manager, Quality and Patient Safety
54. NewYork-Presbyterian/Morgan Stanley Children's Hospital .......................................................... 213
"Clean It Like You Mean It." A three ICU Collaborative on Central Line Associated Bloodstream
Infection Prevention
Svetlana Streltsova, RN, MSN, CCRN; Kathy Lee, RN, BSN, CCRN; Regan Amanda Morimoto, RN, CCRN;
Myrlene Madelon, RN, MSN, CCRN
System Quality Review
8
NewYork-Presbyterian Healthcare System Quality Symposium 2014
Quality 2020: A Vision of the Future
55. NewYork-Presbyterian/Morgan Stanley Children’s Hospital .......................................................... 217
Triaging Pediatric Respiratory Patients
Chana Schwartz; Bettina Sheridan; Lydia Carson; Michael DeGuzman
56. NewYork-Presbyterian/Weill Cornell Medical Center...................................................................... 219
Reducing OR Holds: How Employee Engagement Successfully Improved Patient Flow
Stephanie Nolan RN, MSN, MBA, CPAN; Gregory Camacho, RN, MSN; Katherine O'Hara RN,BSN; Melanie
Quinn RN, BSN; Katrina Valdez, RN, BSN; Kristen Pellicano RN, BSN; Traci Steinberg RN, MSN CPAN;
Gary Allard Business Associate; Christine Teijo, RN, SSN, BSN; Courtney Donnell, RN, SSN, BSN; Joan
Leonard, RN, AAS; Ferron Zayas, RN, BC; Mitzie Wildman Parker Business Associate; Natalia Ivascu MD,
PACU Medical Director, Associate Professor of Clinical Anesthesiology
57. NewYork-Presbyterian/Weill Cornell Medical Center..................................................................... 222
Improving the Patient Pain Experience in Obstetrics
Cathy Crandall RN; Dayna Dixon RN; Neneh Kamara RN; Kjaer Klaus MD
58. New York-Presbyterian Hospital ..................................................................................................... 226
Multidisciplinary Approach to Collaborate and Implement Strategies for Reducing Surgical Site Infections
of Spinal Fusion Patients
Louis Bigliani, MD; Charla Fischer, MD; Yoko Furuya, MD; Jason Cohen, MSPT, MBA; Scott Possley, PA-C,
MPAS; Brian Regan, PhD; Lisa Covington, RN, MPH; Sandra Hyman, RN, MPA; Audrey Compton, MD,
MPH; Maiken Jacobs, MA, OTR/L; Richard Canjura, MBA
59. New York-Presbyterian Hospital/Weill Cornell Medical Center..................................................... 229
Compliance with Clostridium Difficile Prevention Guidelines
Mary B. Moran, MSN, FNP-BC, MPH, RN, CCRN; Natalie Hellmers, MSN, ACNP, CCRN; Annette
Davidek, MFA, BSN, CCRN; Nancy E. Trejo, PA-C; Jennifer Solan, RN, CCRN; Alisa Coleman, RN.
Advisors: Ernesto Perez-Mir, MSN, RN, CCRN, Director of Nursing; Baldeep Kaur, RN, Patient Care Coordinator
and James Horowitz, MD, Associate Director CCU
60. New York-Presbyterian/Columbia University Medical Center ....................................................... 232
Taking a Proactive Approach to Patient Safety
Robin Lynch MSN, RN; David Kessler MD, MSc
61. NewYork-Presbyterian Hospital ...................................................................................................... 234
Creating a Shared Mental Model
Tracey Lewis, MPH; Catherine Waters, RN, MSN, OCN, NEA-BC; Amy Silverstein, MPH; Joan Kaiser RN,
MA, AOCN; Sari Sloane, RN, MSN, NP-BC; Reza Kazerooni, Pharm.D., BCPS, BCOP; Justin Ramirez; David
Collado; Maria Lyons Zani, RN; J. Gregory Mears, MD; Joelle Coq, MS, RN, NEA-BC, OCN; Yon Sugiharto,
MA, CTDP; Rosemary Trinkle Baran
System Quality Review
9
NewYork-Presbyterian Healthcare System Quality Symposium 2014
Quality 2020: A Vision of the Future
62. NewYork-Presbyterian Hospital ...................................................................................................... 237
Making Care Better: Standardizing Care Redesign in Accordance with Evidence-based Practices
Lauren Hedinger, MPA; Brian R. Taylor, PhD; Simone B Zappa, RN, MBA; Katherine H. Pavlovich, MPH;
I-Fong Sun Lehman, DrPH, MS
63. NewYork-Presbyterian/Lawrence Hospital..................................................................................... 244
A Three Year Journey: Prevention of Central Line Associated Blood Stream Infections
Mary Ann Hauff, BS, MS, RN, ANP, CIC; Maria Otto, RN-C, CIC; Christina Hing, RN, MS, FNP-BC;
Dionne Bernadel, RN, MSN, Gail Wilson, RN, BSN, MHAN; Missy Paolicelli, RN, OCN, MSN; Tina Sokolik
RN, BSN, MSN; Barbara Choy, CCRN, BSN, MSA
64. NewYork-Presbyterian Hospital ...................................................................................................... 247
NSQIP-Focused Departmental Semiannual Grand Rounds Reports: Utilizing an Educational Conference
to Improve Outcomes
Carol Gellman, RN, MSN, Senior Performance Improvement Specialist; Theresa Frey, MS, PA, SCR-ACS NSQIP
65. NewYork-Presbyterian Hospital ....................................................................................................... 251
Targeted Continuous Real-Time Assessment of a Workflow Process Improves Quality of Care and
Decreases Expenditures
Irina Lutinger, FACHE, MPH, MASCP, MT(ASCP)DLM; Eldad A. Hod, MD; Alexander Kratz, MD, PhD
66. NewYork-Presbyterian/Columbia University Medical Center ........................................................ 254
Pediatric Surgical Care Improvement Project: Improving Perioperative Prophylaxis and Reducing Surgical
Site Infection Rates
Lisa Saiman, MD, MPH; Litty Varghese, BS; Michael Vitale, MD, MPH; David Roye, MD; Benjamin Roye, MD,
MPH; Jennifer Crotty RN, MSN, CPNP; Hiroko Matsumoto, MA; Rozelle Corda, FNP; Emile Bacha, MD;
Ganga Krishnamurthy, MD; Neil Fieldstein, MD, FACS; Rich Anderson, MD, FACS, FAAP; Bill Middlesworth,
MD; Gudrun Aspelund, MD, MS; Steve Stylianos, MD; Robert Kazim, MD; Anthony Clapcich, MD; Amy MesaJonassen, MD; Brian Thumm; Diane Mangino, Rn, MSN, CIC1; Maria Messina RN, BSN, CIC1; Natalie Neu,
MD, MPH; Ava Brozovich, MPH; Megan Murray, MPH; Elizabeth Salsgiver, MPH, and Philip L Graham, MD
MS
67. NewYork-Presbyterian/Columbia University Medical Center ......................................................... 261
MD Cart: Standardizing Supplies to Improve Provider Workflow
Hunt Tristan BS; Yang, Jesse MD
68. NewYork-Presbyterian/Weill Cornell Medical Center..................................................................... 269
Dissecting Transitions of Care Between Nursing Homes and the Emergency Department: How well are we
doing?
Dana C. Walker; Mary R. Mulcare, MD1; Tony Rosen, MD, MPH; Regina Mysliwiec, MD; Sunday Clark, ScD;
Michael E. Stern, MD; Mark S. Lachs, MD; Neal E. Flomenbaum, MD
System Quality Review
10
NewYork-Presbyterian Healthcare System Quality Symposium 2014
Quality 2020: A Vision of the Future
69. NewYork-Presbyterian Hospital/Weill Cornell Medical Center...................................................... 272
A Novel Clinical Protocol for Placement and Management of Indwelling Urinary Catheters in Older Adults
in the Emergency Department: Implementation and Impact Assessment
Mary R. Mulcare, MD; Tony Rosen, MD, MPH; Sunday Clark, ScD; Kartik Viswanathan, PhD; David P. Calfee,
MD, MPH; Michael E. Stern, MD; Neal E. Flomenbaum, MD
70. NewYork-Presbyterian Hospital/Weill Cornell Medical Center...................................................... 275
Using Targeted Interventions and Multidisciplinary Collaboration to Decrease Length of Stay for Leukemia
Patients at NewYork-Presbyterian/Weill Cornell
Kristen Fanti, MPA, BSN, RN, OCN
71. NewYork-Presbyterian Hospital/Weill Cornell Medical Center...................................................... 282
Improving Prehospital Geriatric Assessment and Care: A Qualitative Study of Emergency Medical Services
(EMS) and Emergency Department (ED) Provider Perspectives
Regina Mysliwiec MD; Tony Rosen MD MPH; Mary Mulcare MD; Sunday Clark MPH ScD; Michael Stern MD;
and Neal Flomenbaum MD
72. NewYork-Presbyterian/Columbia University Medical Center ........................................................ 285
Choosing Monitoring Wisely: Enhancing Patient Flow by Improving Inpatient Telemetry Use
Dan Henderson, MD, MPH; Christopher R. Kelly, MD; Deepa Kumaraiah, MD, MBA; Catherine Halliday, RN,
MSN, Hollis George, RN, MS; Robert Green, MD, MPH; and LeRoy Rabbani, MD
73. NYU Hospital for Joint Diseases...................................................................................................... 288
A Customized Prophylactic Antibiotic Program Reduces Surgical Site infections in Spine and Arthroplasty
Patients
Rainier Tejada, BA; Anthony A. Catanzano, BA; Michael Phillips, MD; Donald Chen, MD; Joseph A. Bosco III,
MD
74. NYU Langone Medical Center ......................................................................................................... 290
"Who's My Doctor, Anyway?" Implementation of Hospitalist Picture Pamphlet on the General Medicine
Service
Katherine Hochman, MD; Nicole Adler, MD; Nicole Kandinova
75. NYU Langone Medical Center ......................................................................................................... 293
Team-based Readmission Assessment Initiative Notes (T.R.A.I.N.): An Interdisciplinary Quality Education
Strategy
Adler, Nicole M MD FACP; Hochman, Katherine A MD FHM; Kandinova, Nicole; Francois, Fritz MD MSc
FACG
System Quality Review
11
NewYork-Presbyterian Healthcare System Quality Symposium 2014
Quality 2020: A Vision of the Future
76. Stamford Hospital ............................................................................................................................. 299
Reducing Blood Transfusions while Minimizing Risks in the Total Joint Replacement Population
Valentine, Deb MSN, RN, ONC, CCM; Frenk, Vlad, MD; Orthopedic Service Line Total Joint Replacement
Subcommittee
77. Stamford Hospital ............................................................................................................................. 302
Improvement in Preterm Infant Hypothermia by the Implementation of a Best Practice Bundle
Donna Bowman, DNP, FNP-BC, RNC-OB, Kathy LiVolsi, MHA, RNC; Jennifer Cabral, MD; John Ciannella,
MD; Beth Kelley, BSN, RNC-OB; Paul Bobby, MD; Gerry Rakos, MD
78. Stamford Hospital ............................................................................................................................. 307
Decreasing Incidents of Contraband on the Acute Inpatient Psychiatric Unit
Madeline Finegan, MS, RN
79. Stamford Hospital .............................................................................................................................. 311
"Racing to Responsiveness" An Organization’s Unique Journey to Engaging Staff in Hourly Rounding to
Increase Patient Satisfaction and Improve Quality Outcomes
Ruth Erway, RN; Megan Fortner, MA
80. Stamford Hospital .............................................................................................................................. 316
Unplanned Extubation of Patients Undergoing Mechanical Ventilation
Alberto Monegro MD; Marta Kokoszynska MD; Sharon Kiely MD; James Krinsley MD, FCCM, FCCP
81. Stamford Hospital ............................................................................................................................. 325
Reducing Unassisted Falls in the ED and Inpatient Setting
Ellen Komar BSN, RN, MCA, NEA-BC (VP of Patient Care Services and CNO); Kelly Maggiotto, BSN, RN;
Sarah Sanders, BSN, RN; Carolyn Hoffman-Kaminski, RN, MS, CPHQ, CPHRM; Kelly Maggiotto, BSN, RNBC; Jackie Kingston, MSN, RN; Michelle Watson, MSN, APRN, FNP-BC, C; Eileen Spenard, DNP, RN; Joan
Sorich, MSN, RN, AOCNS; Christina Curtin, BSN, RN; Maureen McCauley, BSN, RN; Roseann Cardi, MSN,
RN, CRRN; Madeline Cruz, DNP (c), BSN, RN, MS; Stephanie Porricelli, BSN, RN; Brigette Niesen, MSN,
RN; Ryan Strouse, BSN, RN; Gigi Kearney, D.P.T; Sokhak So, PharmD; Christopher Renz, MBA
82. Stamford Hospital ............................................................................................................................. 329
Improving Quality of Care and Patient Outcomes Through Management and Transparency of Hospital
Acquired Conditions and Patient Safety Indicators
Carolyn A. Hoffman-Kaminski, RN, MS, CPHQ, CPHRM; Karen Lawler, MPS, RHIA, CHPS, FABC; Rohit
Bhalla, MD, MPH
System Quality Review
12
NewYork-Presbyterian Healthcare System Quality Symposium 2014
Quality 2020: A Vision of the Future
83. Stamford Hospital ............................................................................................................................. 335
A Novel Protocol for Identification and Risk Reduction in Patients with Prolonged QTc on
Electrocardiogram
Geoffrey Gittleson, PharmD, M.S.; Sokhak So, PharmD; Ryan Brown, PharmD Candidate; Amanda Hubeny,
PharmD Candidate; Valerie Huynh, PharmD Candidate; Darell Grigerick, RDCS, M.A.; Steven Horowitz, M.D.,
F.A.C.C.
84. Stamford Hospital ............................................................................................................................. 340
No More Misses: Implementing a Newborn Screening Reconciliation Process
Kathy LiVolsi, RNC, MHA, NE-BC; Donna Bowman, DNP, FNP-BC, RNC-OB; Theresa Rovegno, BSN, RNC, Karen Bell
85. The SilverCrest Center for Nursing & Rehabilitation ...................................................................... 344
Reducing Avoidable Hospitalizations in Long-Term “Chronic-Critically Ill” Patients
Daniel Russo, CMD; Denise Lawson, RN; Loretta Mcmanus, RN; Karen Dikeman, MACCC-SLP
86. The Valley Hospital .......................................................................................................................... 349
An Innovative Approach to Decreasing Door to t-PA Times
Margaret Thornton RN, MSN, CEN
87. Winthrop-University Hospital ........................................................................................................... 351
Improving Patient Safety by Educating Physicians on a New MRI Conditional Pacemaker Device
Yuri Peterkin MD; Maria Khalid MD; Rakesh Shah MD; Orlando Ortiz MD
88. Winthrop-University Hospital .......................................................................................................... 353
A Quality Improvement Initiative to Improve Rates of Normothermia in the Delivery Room Using a
Checklist
Alexandra Vinci, MD; Bianca Fornier Karber, MD; Shahidul Islam, MPH; Nazeeh Hanna, MD; Amrita Nayak,
MD
89. Winthrop-University Hospital .......................................................................................................... 356
Our Journey to Improving our Patient Safety Culture
Joseph Greco, MD Chairman of Anesthesia and Patient Safety Officer; Stacey Pfeffer, Senior Vice President Human
Resources and Organizational Development; Monica Santoro, MS, BSN, RN, CPHQ, Vice President and Chief
Quality Officer
90. Winthrop-University Hospital - Pulmonary & Critical Care Medicine ............................................ 362
A Quality Improvement Study to Decrease COPD Related Readmission and Average Length of Stay
through the implementation of a COPD Transitions of Care Program
Grace Trimmer RN MSN; Cyril Cheriyan MD; Zubair Ali MD; Joyce Pang MD; Girish B. Nair MD; Sam Kirell
RHIA; Marie Bernstein RT; Jon Ilowite MD; Steve Salzman MD; Michael Niederman MD
System Quality Review
13
NewYork-Presbyterian Healthcare System Quality Symposium 2014
Quality 2020: A Vision of the Future
Columbia University, Department of Biomedical Informatics
Impact of Noise on Clinical Performance in the ED: Compromising Patient
Safety
Mary L. Little, RN, MSN1; Osman R. Sayan, MD2; Edward H. Suh, MD2; Vimla L. Patel, PhD1,3
1Dept. of Biomedical Informatics, Columbia University; 2New York-Presbyterian Hospital; 3New York Academy of
Medicine, New York, NY
Introduction
There is sufficient evidence to show that multitasking and interruptions compromise efficiency,
productivity, information transfer, and patient safety(1-4). In a hospital, excessive noise is a form
of interruption and has been shown to exhibit a detrimental effect on patients, staff, their
cognition performance, and communication(5-7). Additionally, there is a documented
cardiovascular response to stress with long-term health effects for those in noisy
environments(8). Numerous studies have also linked the nature of the physical environment to
patient and staff outcomes in areas of: stress, fatigue, patient safety, improved patient outcomes,
and improved overall healthcare quality(9,10). Specifically, sustained attention and performance
are affected by hospital noise levels which routinely exceed the World Health Organization
(WHO) guidelines. Caregivers must exert greater effort to maintain accuracy which in turn
increases physiological responses and fatigue(11). Thus, it is important to the delivery of quality
patient care to strive for decision-making environments that reduce or change the characteristics
of noise, workflow interruptions, and mitigate patient management errors.
Problem
Excessive noise levels interfere with cognition performance, transfer of crucial information, and
exert negative psychological and physiological effects on staff. This represents a threat to quality
patient care and safety, especially during the critical time of information exchange in care team
transition. Studies have also cited delayed healing and decreased satisfaction in patients due to
excessive noise(4,12,13). Delayed healing has the potential to increase patient length of stay
(LOS) and decreased patient satisfaction has the potential to negatively impact patient satisfaction
scores, one of the core measures in hospital evaluation.
Goals
In an effort to assess the noise level characteristics in a high-volume, tertiary-care hospital
emergency department (ED), and investigate staff perception and responses, both qualitative and
quantitative data were collected and analyzed using natural language data analyses. These included
ethnographic observations, semi-structured interviews and sound pressure level (SPL) recordings
at strategic times. This was a pilot study (Phase I) to look at the feasibility such that needed
modifications could be implemented in the future for phase 2.
System Quality Review
14
NewYork-Presbyterian Healthcare System Quality Symposium 2014
Quality 2020: A Vision of the Future
Specifically our aims included:
1. Evaluate staff perceptions of noise prior to any observable noise level recording to mitigate the
Hawthorne effect in collecting data.
2. Characterize staff workflow, communications, interruptions as well as any verbal responses to
perceived excessive noise.
3. Record the sound level using iPad sound meter applications (apps) and relate the noise to the
observed workflow.
Quantitative/Qualitative Measures
This investigation of SPLs in the ED is a part of a larger workflow information study of eight
interviews, and over 25 ethnographic physician shift-change observations with ED attending
physicians, residents, and medical students. The interviews were obtained to capture perceptions
of interruptions, workflow, and noise/sound interference using a semi-structured questionnaire
and data had both qualitative and quantitative information. Ethnographic observations with
prospective data capture of clinical workflow were captured using a standardized format
(quantitative data) as well as qualitative assessment in free style format during patient rounds.
Observation results were then reordered and transcribed after de-identification and used in
modeling the tasks and interactions within the complex workflow of the ED environment(14).
Task performance at varying sound levels was also captured to study the potential effect of high
SPLs on cognition and integrity in information transfer.
Methodologies
In the Phase I pilot study assessment, an iPad mini was transformed into a sound meter via
SPLnFF’s SPL meter application and AudioTools’ SPL meter application; observed readings in
an A-weighted frequency were causation coded. The iPad mini was held away from the observer’s
body by 12-18 inches to minimize any interference in SPL readings. Task performance at varying
sound levels was also captured to study the potential effect of high SPLs on cognition and
integrity in information transfer. Interviews were also recorded, de-identified and transcribed for
analyses, using using n-vivo program for analysis of natural language (14,15). Based on the
preliminary results, the authors felt the need for further evaluation with an automatic SPL digital
recording device. The Larson Davis Model 831 digital sound level meter was utilized to achieve
greater measurement precision. A pre-usage calibration check of the Model 831 revealed audio
capture levels to be within 0.06 dBs of factory settings. The digital SPL meter was programmed
to record minimum (LAFmin), maximum (LAFmax), and Z-Weighting peak (Lpeak) sound
pressure history values every 1 second.
Improvement Results
In the interviews with ED physicians and residents about the clinical workflow, EHR tasks with
workflow usability problems and inefficiencies were cited as major concerns. ED noise levels
were not highlighted by the staff, indicating the possibility of user belief in adjustment or
acceptance of the ED noise levels (alarm fatigue) despite literature citing the activation of the
sympathetic-adrenal-cortical axis and production of stress hormones(7). In ethnographic
observations of the patient handoff process, SPLs >95-100 elicited verbal noise complaints and
System Quality Review
15
NewYork-Presbyterian Healthcare System Quality Symposium 2014
Quality 2020: A Vision of the Future
requests to have the information repeated. The observations also revealed noisy linen and trash
carts being pushed through the middle or adjacent to the rounding team and various types of
interruptions such as personal greetings to members of the rounding team during information
transfer. In this Phase I pilot, sound booth testing showed the iMM-6 microphone falsely raised
the SPL recordings by 7-8.3 dBs. Without the iMM6 microphone, the dB readings of the SPLnFF
and AudioTools applications were within approximately 2.1 dBs with the AudioTools application
offering slightly more accurate readings. Average ED noise levels were 73.4 dBs. SPL recordings
varied among the 3 distinct ED patient care areas based on area characteristics such as total
patient capacity and proximity to the main corridor walking path among the ED areas. The
loudest SPL readings occurred with overhead announcements, averaging 87-91 dBs, with a
SPLmax readings of 108.1 dBs. Thus far, the Larson Davis digital sound meter recordings show
the continuous time average sound level (LAeq) to be 63.85 + 0.35 dBs and the mean maximum
sound exposure level (LAE), to be 96.65 + 2.25 dBs. Besides the advantage of digital recording
precision, the ability to record peak sound levels in sudden noise scenarios offers a glimpse of the
true peak sound pressure wave. To date, the mean LPeak value is 106.8 + 2.7 dBs. As well noted
in literature, these noise interruptions during physician and nursing handoffs have the potential to
lower cognitive performance resulting in medical performance errors .
Sustainability Strategies
Both the observational Pilot using the iPad mini sound meter application and the Model 831
digital sound level meter show the occurrence of noise events over 90 dBs. These SPLs
correspond to subway noise and a construction jackhammer at 3 feet away (Table 1) (16). Noise
of this magnitude at a critical time in team transition affects information integrity, cognition(17)
and decision-making. Moreover, there are many strategies that can assist in reducing noise levels
especially during critical team transition time. An immediate and much needed strategy is to
implement a prohibited “non-essential interruption” zone for nursing and physician team
handoffs as well as implementation of a volume-level control for overhead pages. Additionally,
simple environmental revisions are possible, as seen in many strategies employed by
Massachusetts General Hospital’s Lunder Building. Gathering from the innovations utilized in
the Lunder Building, potential strategies for implementation include noise –reducing acoustical
ceiling tiles, supply cart wheels coated in rubber, cell phone or beeper paging systems rather than
overhead announcements, and sound reducing fabric for patient cubicle curtains(18).
Lessons Learned
The top three lessons thus far from this pilot study are:
1. Do not underestimate the impact of sound levels/noise on clinicians’ adverse performance
outcomes or on patients’ health. The alarm/noise fatigue is dangerous and compromises patient
safety.
2. Improvements in performance and patient satisfaction can be made by some simple
modifications to the noise levels or characteristics
3. Our investment in recording evidence-based research on impact on noise/sound on patients’
health and clinicians’ cognitive functioning in the ED can have impact beyond the ED to other
parts of the hospital.
System Quality Review
16
NewYork-Presbyterian Healthcare System Quality Symposium 2014
Quality 2020: A Vision of the Future
Conclusion
There are three major conclusions from our pilot study: 1) Clinicians in the ED become
accustomed to sound levels and reduce situational attention to sound. This alarm/noise fatigue is
dangerous and compromises patient safety; 2)There were many unnecessary interruptions during
physician and nursing handoffs in the form of greetings, patient interruptions, cart movements
adjacent to rounding teams, and overhead pages; 3.) The majority of staff requests to repeat
handoff information were in response to loud overhead pages which obstructed delivery of vital
patient information. Aviation’s sterile cockpit rule prohibits non-essential distractions during
critical flight times (19). Medicine has not emphasized solutions for the distracting and potentially
harmful effect of excessive SPLs on cognitive functions of patients, staff, and workflow
communications. The lack of recent medical research regarding the effect of noise levels on
patients, staff, cognition, and information exchange, highlights the need for more thorough
studies in this area using the gold standard of binaural audio recordings(20). We need future
studies to include interactions with electronic health records (EHRs) for provider information
retrieval, effective alerts, and safe care team transitions. Use of noise reduction solutions such as
sound absorbing panels and volume-limit controls on audio announcements and other
communication devices could be implemented since sound reduction has been shown to improve
patient satisfaction(21). The need to reduce the noise level environment is key to improving
patient satisfaction, a core measures in hospital evaluation for payment via the value-based
purchasing program and a factor in reduce LOS(22-24). For all concerned, we need to keep the
jackhammers out of our cockpit environment especially during the takeoff and landing periods of
patient care.
Impact of Noise on Clinical Performance in the ED: Compromising Patient Safety
Mary L. Little, RN, MSN1; Osman R. Sayan, MD2; Edward H. Suh, MD2; Vimla L. Patel, PhD1,3
1Dept.
of Biomedical Informatics, Columbia University; 2New York-Presbyterian Hospital; 3New York Academy of
Medicine, New York, NY
Table 1 Comparison of Sounds, dB levels, & Hospital Noise:
Environmental Protection Agency hospital maximum is 45 dbs.
Sound Associations
dB
Level
Hospital Noise Found at this
Level
Washing Machine
40
None
Vacuum Cleaner at 1 meter
70
Staff conversations (avg), patient alarms
Garbage Disposal
80
Raised voices
Police Whistles, Subway
90
Paging announcements (avg)
Jackhammer at 1 meter
100+
Paging announcements (max)
System Quality Review
17
NewYork-Presbyterian Healthcare System Quality Symposium 2014
Quality 2020: A Vision of the Future
References
1.
2.
3.
4.
5.
6.
7.
8.
9.
10.
11.
12.
13.
14.
15.
16.
17.
18.
19.
Laxmisan A, Hakimzada F, Sayan OR, Green RA, Zhang J, Patel VL. The multitasking clinician:
decision-making and cognitive demand during and after team handoffs in emergency care.
International journal of medical informatics. 2007;76(11):801-11.
Patel VL, Zhang J, Yoskowitz NA, Green R, Sayan OR. Translational cognition for decision
support in critical care environments: a review. Journal of biomedical informatics.
2008;41(3):413-31.
Brixey JJ, Robinson DJ, Johnson CW, Johnson TR, Turley JP, Zhang J. A Concept Analysis of
the Phenomenon Interruption. Advances in Nursing Science. 2007;30(1):E26-E42.
Busch-Vishniac IJ, West JE, Barnhill C, Hunter T, Orellana D, Chivukula R. Noise levels in
Johns Hopkins hospital. The Journal of the Acoustical Society of America. 2005;118(6):3629-45.
Ratnapalan S. Physicians' Perceptions of Background Noise in a Pediatric Emergency
Department. Pediatric emergency care. 2011;27(9):826-33.
Konkani A. Noise in hospital intensive care units--a critical review of a critical topic. Journal of
critical care. 2012;27(5):522.e1-9.
Banbury SP, Macken WJ, Tremblay S, Jones DM. Auditory distraction and short-term memory:
Phenomena and practical implications. Human Factors: The Journal of the Human Factors and
Ergonomics Society. 2001;43(1):12-29.
Babisch W. The noise/stress concept, risk assessment and research needs. Noise and health.
2002;4(16):1.
Ulrich, R., Quan, X., Zimring, C., Joseph, A., & Choudhary, R. (2004). The role of the physical
environment in the hospital of the 21st century: a once-in-a-lifetime opportunity. Concord CA:
Center for Health Design.
Dickerman, K.N., Barach, P., & Pentecost, R.A. (2008). We shape our buildings, then they kill
us: Why healthcare buildings contribute to the error pandemic. www. ihf-fih.org, 44(2), 15.
Barach, P., Forbes, M.P., & Forbes, I. (2009). Designing safe intensive care units of the future. In
Intensive and Critical Care Medicine (pp. 525-541. Springer Milan.
Konkani A. Noise in hospital intensive care units--a critical review of a critical topic. Journal of
critical care. 2012;27(5):522.e1-9.
Fife, D., & Rappaport, E. (1976). Noise and hospital stay. American Journal of Public Health,
66(7), 680-681.
Malhotra S, Jordan D, Shortliffe E, Patel VL. Workflow modeling in critical care: Piecing
together your own puzzle. Journal of Biomedical Informatics. 2007;40(2):81-92.
Patel, V. L., Zhang, J., Yoskowitz, N. A., Green, R., & Sayan, O. R. (2008). Translational
cognition for decision support in critical care environments: a review. Journal of biomedical
informatics, 41(3), 413-431.
Environmental Protection Agency, U. S. (1974). Information on levels of environmental noise
requisite to protect public health and welfare with an adequate margin of safety. EPA/ONAC
550/9-74-004. United States Environmental Protection Agency.
Campbell T. The cognitive neuroscience of auditory distraction. Trends in cognitive sciences.
2005;9(1):3-5.
All’s Quiet on the Lunder Floors. (2012, July 16). Department of Radiation Oncology.
Massachusetts General Hospital. Retrieved from
http://www.massgeneral.org/radiationoncology/news/newsarticle.aspx?id=3663
Broom, M. A., Capek, A. L., Carachi, P., Akeroyd, M. A., & Hilditch, G. (2011). Critical phase
distractions in anaesthesia and the sterile cockpit concept. Anaesthesia, 66(3), 175-179.
System Quality Review
18
NewYork-Presbyterian Healthcare System Quality Symposium 2014
Quality 2020: A Vision of the Future
20.
21.
22.
23.
24.
Zwicker E, Fastl H, Frater H. Psychoacoustics, Facts and Models, volume 22 of Springer Series
of Information Sciences. Springer, Berlin, 2nd updated edition; 1999.
Topf M. Hospital noise pollution: an environmental stress model to guide research and clinical
interventions. Journal of Advanced Nursing. 2000;31(3):520-8.
Tsai TC, Orav EJ, Jha AK. Patient Satisfaction and Quality of Surgical Care in US Hospitals.
Annals of Surgery. 2014.
Berenson RA, Pronovost PJ, Krumholz HM. Achieving the potential of health care performance
measures. Princeton (NJ): Robert Wood Johnson Foundation. 2013.
Vaughn T. Governing board, C-suite, and clinical management perceptions of quality and safety
structures, processes, and priorities in U.S. hospitals. Journal of healthcare management.
2014;59(2):111-28.
System Quality Review
19
NewYork-Presbyterian Healthcare System Quality Symposium 2014
Quality 2020: A Vision of the Future
Burke Rehabilitation Hospital
Patient/Family Participation in Multidisciplinary Rounds Conferences: A Pilot
Program in an Inpatient Rehabilitation Hospital
Kristen Bonistall, MS, MSW; Donna Russo, LCSW, CCM; Richard Novitch, MD, Adina Safdeye
Introduction
Problem statement: When patients experience a poorly executed transition in care, there is an
increased likelihood of hospital readmission, ineffective patient and caregiver education,
discharge summaries that are incomplete, and poor patient social support (Li, Young, & Williams,
2014). When patients and families are engaged in the decision making process related to
transitions in care, there are direct correlations with healthy behavior, better health outcomes, and
better care experiences (Hubbard & Greene, 2013).
Project aim: To engage patients and families in the discharge planning process from an inpatient
rehabilitation hospital, a pilot program (February 2014-August 2014) was initiated in which
patients and/or families were invited to actively participate in a round table discussion at a
multidisciplinary rounds conference on a Cardio-Pulmonary unit where discharge dates and
discharge planning was discussed. The aim was to increase team cooperation, improve patient
satisfaction, and to engage patients in their own discharge planning. All patients were given a
notice by their Social Worker on admission that invited patients and families to attend rounds for
brief updates from all of the multidisciplinary team members currently treating the patient
(Physician, Head Nurse, Physical Therapist, Occupational Therapist, Respiratory Therapist and
Social Worker). Interested patients and/or family members then spoke to the Social Worker to
schedule a 5-10 minute time slot to attend.
Quantitative/Qualitative Measures
After discharge, participating patients and/or families were contacted on the phone for an
anonymous survey about their experience. A five point Likert scale was used on a nine question
telephone survey. Additional comments provided by survey respondents were analyzed
qualitatively. Staff were queried at regular intervals so that any adjustments to improve the
process could be incorporated in real time. Medical chart review on all patients on the unit during
the study period was utilized to determine the percentage of patients who opted to participate in
rounds meeting, demographic information, patient diagnoses, length of stay, discharge dates, and
discharge destinations. Patient satisfaction data from Press Ganey was compared between 3rd
quarter 2013 and 3rd quarter 2014 for the entire Cardiopulmonary unit on discharge –related
questions.
System Quality Review
20
NewYork-Presbyterian Healthcare System Quality Symposium 2014
Quality 2020: A Vision of the Future
Methodologies
The main goal of the pilot program was to engage patients and families in their care, which is
keeping in line with the QI principles of person-centeredness, family engagement, and valuing
patient preferences. Because patients who want to work with their health care providers in
making decisions about their care often lack the necessary understandable information, this
program sought to bring together the multidisciplinary team in a way that was helpful, not
overwhelming for the patients, and could maximize the patient-specific information presented in
a short time. Additionally, we sought to foster transparency so that patients, families, and
discharge planners all have the information necessary to ease the patients’ transition in care.
Feedback on the program was obtained anonymously from multiple stakeholders, including
patients, families, and providers who participated, and ongoing process improvement suggestions
from the team were incorporated in real time.
Improvement Results
During this time period, there were approximately 191 admissions on the unit. In this cohort, 31
(16%) patients and/or patient families opted to participate in the rounds discussion. Of these 31
patients, one patient and/or patient family attended 5 times, and 4 patients and/or patient
families attended twice. Nine patients and eleven family members completed phone interviews.
Everyone except for one patient family member rated their overall experience as “extremely
positive”, and all 100% of patients would recommend these meetings to other patients and
families. Surprisingly, 18 out of 20 patients and families felt that the 5-10 minute time slot was
adequate to hear updates from the team and answer their specific questions about discharge
plans. Patient satisfaction data for the unit was compared between 3rd quarter 2013 and 3rd
quarter 2014, but no mean significant differences in satisfaction were found on discharge-related
survey questions. Staff feedback noted an increase in caregiver involvement in therapy, more
consistency in the discharge planning process, and increased likelihood of aftercare compliance.
Sustainability Strategies
The likelihood of continuing this program is high, as it requires only 10-20 minutes of nontreatment staff time, following a meeting where the team is already assembled. Participating
patients have rated it as an “extremely positive” experience. To increase the number of patients
and families who actually attend, future plans may involve additional reminders to patients during
education groups run by social workers, as well as focused efforts to include patients who need a
discharge date set in the upcoming meeting.
Lessons Learned
1) Patients were highly satisfied with even 5-10 minutes of the team’s time spent updating them
on progress and discussing discharge plans.
2) These meetings promoted more interaction with staff, and as a result, more caregiver training
and involvement in therapy.
3) Hospital wide satisfaction surveys (i.e. Press Ganey data) may lack the sensitivity or clarity in
wording to accurately assess the patients’ satisfaction with all of the components of the discharge
planning process.
System Quality Review
21
NewYork-Presbyterian Healthcare System Quality Symposium 2014
Quality 2020: A Vision of the Future
Conclusion
Extending a weekly team meeting to include a round table discussion with patients and/or
families of patients with complex illness undergoing inpatient rehabilitation was implemented and
studied. The process may lead to better outcomes in transitions to the community and increased
patient/family satisfaction, all while minimizing the time commitment of staff to the discharge
planning process. Further study will be required to better understand the relationship to overall
hospital satisfaction, and whether the patients who opted out of this program were statistically
different from those who opted in (i.e. diagnoses, social supports, and/or communication
barriers).
Patient/Family Participation in Multidisciplinary Rounds Conferences:
A Pilot Program in an Inpatient Rehabilitation Hospital
Count of Survey Respondents
Rounds Participation Follow-Up Survey Data
20.0
19.0
18.0
17.0
16.0
15.0
14.0
13.0
12.0
11.0
10.0
9.0
8.0
7.0
6.0
5.0
4.0
3.0
2.0
1.0
0.0
1=Do Not Agree
2=Somewhat Disagree
3=Neither Agree Nor
Disagree
4=Somewhat Agree
5=Agree Completely
The purpose
My
I felt
I felt
The team
There was The meeting
was clear. expectations welcomed comfortable presented
adequate helped me
were met.
into the
speaking to information
time to
take an
group
the group. in clear, easy address my active role in
discussion.
to
questions
my
understand
and
treatment
concerns.
and
language.
discharge
planning.
Survey Questions
System Quality Review
22
NewYork-Presbyterian Healthcare System Quality Symposium 2014
Quality 2020: A Vision of the Future
Cohen Children's Medical Center of New York
Improving Discharge Velocity: Testing the Visual Communication About
Throughput (V-CAT) Board
Kathy Albert, RN, DNP; Brian Belpanno, MBA; Nancy Palumbo, MD; Diane Diver, RN, MSN, Helen Scott, MD
Introduction
At Cohen Children's Medical Center, patients admitted through the Emergency Department
(ED) waited as long as 7 -12 hours from time of disposition to arrival on the unit. This caused
increased ED patient boarding, long delays, and extreme customer and provider dissatisfaction.
Due to these long delays, there was an increase in patients leaving without being seen in the ED,
posing a potential safety risk.
While addressing this quality issue, it was discovered that long ED delays from disposition to
arrival were due in part to lack of bed availability on the units caused by a misalignment of
discharge time and ED volume.
Supply and demand curves were created to display patient ebb and flow of admissions from the
ED and Surgery as well as discharges from the patient units. It was discovered that 70% of all
discharges and admissions occurred within the 6 hour period of 12:00 and 18:00. This caused a
deficit of beds when demand was highest. Analysis, observations and interviews confirmed that
discharge orders were being placed later than necessary to meet the demand. In addition, patients
typically remained in the bed 2.3 hours after being discharged.
It was determined that patients were actually medically ready for discharge much earlier in the
day, typically as early as 7am on a short-stay unit, but interdepartmental tasks and discharge
requirements were not aligned and done within a timely manner. Lacking was a shared mental
model of discharge predictability and no forum for accountability of discharge tasks. As a result,
communication was fragmented causing unnecessary delays in discharge. Anecdotal data showed
that delays were caused by lack of timely transportation, incomplete discharge paperwork, and
patients/families waiting to eat a final meal before departing.
Problem Statement: Due to a lack of structured interdisciplinary communication and mechanism
for tracking patient progress, delays in discharges caused a deficit of bed supply as the demand
increased.
Project Aim: Align (by increasing or decreasing) the percentage of discharge orders placed to the
calculated optimal percentage of orders placed.
Project Aim: Align (by increasing or decreasing) the percentage of patient exits to the calculated
optimal percentage of patient exits.
System Quality Review
23
NewYork-Presbyterian Healthcare System Quality Symposium 2014
Quality 2020: A Vision of the Future
Quantitative/Qualitative Measures
1. The percentage difference between the actual percent of discharge orders placed by hour and
the optimal percent placed by hour.
2. The percentage difference between the actual percent of patient exits by hour and the optimal
percent of patient exits by hour.
Since patients cannot exit until they are discharged, the timing of exits needs to be shifted to fit
within the constraints of level-loading supply and demand.
The optimal orders and exits are calculated by level loading the sum of admissions and discharges
by hour between 8am and 8pm. Since admissions cannot be adjusted, the timing of discharge
orders needs to be shifted
3. The number of hours between discharge order placed and patient exit.
4. Staff satisfaction with the process.
Methodologies
The framework put forth by the Institute of Medicine (IOM) states that quality domains in
healthcare should be efficient, effective, safe, equitable, timely, and patient-centered. The concept
of Demand-Supply Alignment was combined with the Lean principle of Heijunka (level loading)
to determine the optimal number of patients exiting each hour so as not to overwhelm the
workforce and create bottlenecks. To address timeliness and efficiency, Cohen Children's Medical
Center used IHI Improvement Science Methodology to ask the questions: What are we trying to
accomplish? How will we know that change is an improvement? and What change can we make
that will result in an improvement? Multiple PDSA cycles were conducted doing small tests of
change to develop and refine a unit care throughput board that illustrated each patient's journey
from arrival to exit. Small tests of change were done to improve the timing of board rounds, the
categories on the board and the assignment and accountability of board updating. Discharge
Process Improvement: A Case Study by Barnes-Jewish Hospital of St. Louis; Laurie D. Wolf, MS,
CPE was the template to create the throughput process.
Improvement Results
Process improvement was the creation of a V-CAT (visual communication about throughput)
Board. To achieve this, a cross-functional team consisting of nursing, physicians and Quality
participated in a brainstorming session to determine the tasks which commonly need to be
completed before a patient can exit. These tasks were put into a grid containing patient names
and was posted on a large piece of paper on a wall in the nursing station for the staff to comment
on and see if it met the needs of the project. The tasks included: labs/radiology/consults
completion, need for transportation, discharge paperwork completion, patient education,
equipment ordered/obtained, medically ready for discharge, and discharge order placed, etc. The
first iteration of the board was tested on 1 patient during 1 shift (small test of change). After the
shift, the team briefed and revised the board. The team went through multiple PDSA cycles
before the board was fully implemented. The final board was a 3'x5' white board using grid tape
and colored magnet discs. The magnets were used to indicate the status of each task. Red = "not
started", Yellow="in progress" Green="completed", and Blue="not applicable". The board
System Quality Review
24
NewYork-Presbyterian Healthcare System Quality Symposium 2014
Quality 2020: A Vision of the Future
enabled tasks to be updated for real-time visualization by all care providers. The rounding
process was changed from informal individual reviews to formal interdisciplinary team reviews
meeting 2x daily for the purpose of updating patient throughput status and addressing
delays/challenges/etc. At each rounding, magnets were changed to appropriate colors to reflect
the most recent updates. In addition, the board was used to predict discharge dates and times to
better manage bed utilization.
Utilization of the V-CAT Board resulted in the following: 1) A shift in the time discharge orders
are written that is closer to optimal by an average of 1.5 hours. This results in earlier exits. 2) A
shift in the time of patient exits that is closer to optimal by an an average of 2.0 hours. This
created a larger bed supply to meet ED demand.
Sustainability Strategies
In order to sustain the process, several actions were taken. Quality and physician leadership took
an active role in ensuring that the direct care providers huddled at the board at established times
daily. Assignment and accountability of board updates were designated to the appropriate
personnel. To ensure consistent and timely updates, the responsible party was listed on the board
and called upon during huddles. Bi-monthly hospital-wide throughput meetings mandated that
staff report on the status, usage, and improvement ideas to ensure that the current process is
sustainable and user-friendly to all. Percentage of usage is reported and tracked. Multiple PDSA
ramps were conducted during the initial phase to develop a process that would generate
consistent usage and sustainability. Testing over several months has yielded a process that is
resilient on the current unit and will be spread hospital-wide in the near future. Random audits
showed that the staff is engaged, board huddles are being conducted as per schedule, and updates
are consistent, accurate, and timely.
Lessons Learned
1. Think carefully about where the board will be placed on the unit. Location, it turns out, is
critical to engagement and group gathering. There needs to be a balance between visibility and
HIPAA compliance.
2. Leadership presence is key to sustainability. Influencing the end-users to its merits so that the
newness, inconvenience, and change are outweighed by its benefits in the long-term.
3. A manual board is a great start to develop proof of concept. However, to achieve true, realtime data, a computerized, virtual board would allow caregivers that are not on the unit (ie: Case
Management) to update live from desk top computers at any location.
Conclusion
The use of the V-CAT board resulted in earlier daily bed availability by gathering the team at
standardized times and visually bringing awareness of each patient's status and encouraging
reliable discharge predictions. This, in turn, provided earlier available beds for admitted
Emergency Department patients.
The board has brought a level of awareness to the value-stream that did not previously exist. Any
staff member can easily visualize the patient's progression toward discharge and bottlenecks
impeding the process. Staff members are encouraged to turn their patients' magnets to green in
System Quality Review
25
NewYork-Presbyterian Healthcare System Quality Symposium 2014
Quality 2020: A Vision of the Future
real-time to provide up-to-the-minute representation. The board places accountability on all
departments and their role in patient discharge. In the future, a computerized virtual board will
enable data collection to drive improvements. In the meantime, the V-CAT board has served as a
reliable and realistic prototype to achieve our goals.
System Quality Review
26
NewYork-Presbyterian Healthcare System Quality Symposium 2014
Quality 2020: A Vision of the Future
System Quality Review
27
NewYork-Presbyterian Healthcare System Quality Symposium 2014
Quality 2020: A Vision of the Future
Poster Presentation
Cohen Children's Medical Center of NY
Implementation of a Standard Urinary Catheter Process Eradicates CAUTI's
at a Single Pediatric Tertiary Care Center
Aaron Kessel, MD; Kathy Albert, RN; Samantha Fensterman, RN; Colleen O'Hara, RN; Fiona Levy, MD
Introduction
Catheter associated urinary tract infections (CAUTI) are one of the more prevalent types of
hospital acquired infections. The incidence of both bactiuria and urinary tract infection increases
with each day that a urinary catheter is left in place. This can lead to a CAUTI occurrence rate as
high as 1.6 per 1000 catheter days in pediatric studies. Infection rates among critically ill patients
in pediatric intensive care units is even higher, with an incidence as high as 3.1 per 1000 catheter
days. (Lo, et al. 2014) These infections are associated with multiple morbidities including
bacteremia, sepsis, and urethral inflammation, which can lead to longer hospital stays and higher
costs.
In the absence of standardized protocols and practices to prevent such occurrences, the baseline
CAUTI rate at Cohen Children's Medical Center was 5 per 1000 catheter days with high monthly
variability, suggesting an unacceptably high rate of infection.
As such, we sought to develop a plan to decrease our hospital's rate of CAUTI's by creating a
standardized work flow, as well as a culture of safety governing the placement and treatment of
urinary catheters. As part of a broader nationwide safety collaborative it was our aim to decrease
the rate of CAUTI's in our hospital by 40% over an eighteen month period.
Quantitative/Qualitative Measures
Multiple measures were taken to help decrease our high CAUTI rate, including increased urinary
catheter monitoring, improving staff knowledge and awareness, and fostering behavioral change
regarding the care of urinary catheters.
Initially, we examined the pattern of CAUTI's in the hospital and identified means to lower this
infection rate. We created a standardized process for insertion and maintenance as well as a
monitoring tool to gauge compliance with the new processes. With continued monitoring, we
identified process elements that were not being followed, and areas of the hospital that were less
compliant. We investigated the causes of these deficits and aimed to correct them via a number
of interventions including education, supply improvement and involvement of hospital and floor
leaders.
System Quality Review
28
NewYork-Presbyterian Healthcare System Quality Symposium 2014
Quality 2020: A Vision of the Future
Methodologies
We followed the standard model for improvement starting with a SMART aim document and a
key driver diagram to identify modifiable elements that would help us achieve our goal. We
performed multiple PDSA cycles to improve specific elements and reassess our goals and
achievements throughout the course of the initiative.Specific examples include the creation of
urinary catheter insertion and maintenance bundles which highlighted a few, easily memorable
points that have been shown to decrease the rate of CAUTI's. We encouraged, monitored and
educated staff to increase bundle reliability. Additionally, physician and nursing leadership were
included and given a sense of ownership for their respective floors on the hospital's daily safety
call, in which the number and need for urinary catheters was discussed, to encourage their
removal.
Improvement Results
Since the beginning of our quality improvement process, approximately two years ago, we have
improved our reliability with urinary catheter insertion and maintenance bundles. We have also
markedly reduced the number of CAUTI's within the hospital.
As shown in figure 1, we continuously monitor reliability for the insertion bundle in the Pediatric
Intensive Care Unit and the operating rooms. Over the last two years compliance with the
insertion bundle has increased. The total compliance has increased from 75% in our first month
to 100% for the last 6 months. When looking at the OR and PICU separately, compliance in the
OR has increased from 90% to 100%. Compliance in the PICU has increased from 50% in some
months, to 100% overall.
Similarly, our compliance with the maintenance bundle has increased over time, as shown in
figure 2. We continuously monitor the pediatric wards and PICU by performing twice weekly
audits. Our compliance over the two year period is 83%. It has increased markedly over this
period from 65% in our first month to 98% in June 2014. Overall compliance in the PICU over
the 2 year period is 91%, with an improvement from 85% to 100% in the last month measured;
the corresponding data from the pediatric wards is 70% compliance over 2 years with an
improvement from 40% to 94%.
Lastly, and most importantly, is our hospital CAUTI rate which has fallen over the last 2 year
period. It has been over one year since our last CAUTI with a change in our centerline from 5 to
0 CAUTI's per 1000 catheter days. Our monthly and yearly rate, with associated interventions, is
displayed in figure 3.
Sustainability Strategies
We are continually implementing new practices and products to help us sustain the
improvements that we have made and improve even further.
We are now stocking the PICU, pediatric floors and operating rooms with a standard urinary
catheter insertion kit. This kit contains a closed urinary drainage system pre-connected to a
urinary catheter, as well as all required supplies for catheter insertion. We have also created a
urinary catheter insertion form which is completed upon catheter insertion and becomes part of
the medical record. The twice weekly floor audits will continue to remind staff of the
System Quality Review
29
NewYork-Presbyterian Healthcare System Quality Symposium 2014
Quality 2020: A Vision of the Future
maintenance bundle, and encourage staff, together with our daily safety call, to remove the
urinary catheter when it is no longer necessary. Lastly, we are beginning an initiative to educate
parents and families about urinary catheters with a handout or hanging sign, to facilitate increased
familial involvement with any decisions relating to the urinary catheter.
Lessons Learned
Lessons learned over the last two years:
1. Key factors leading to a reduction in CAUTI rates include limiting the number of urinary
catheters that are inserted, and the prompt removal of catheters that are no longer necessary.
Compliance with insertion and maintenance bundles is also very important in reducing the
CAUTI rate.
2. Increasing situation awareness though daily phone conversations, repeated visits to patient care
areas, and intermittent posters, helps to increase everyone's sense of responsibility and empowers
them to act both as a team and as individuals.
3. A team of people from many disciplines is better able to develop an action plan, and carry out
that plan in a number of hospital locations.
Conclusion
Catheter associated urinary tract infections are hospital acquired infections that have a high
morbidity and cost, however are preventable with changes in culture and practice. By raising
CAUTI awareness in our institution, creating bundles to foster best practice, and educating staff
about these practices, we have substantially lowered our CAUTI rate over the last 2 years and
hope to continue this positive trend.
System Quality Review
30
NewYork-Presbyterian Healthcare System Quality Symposium 2014
Quality 2020: A Vision of the Future
Figure 1: Insertion Bundle Compliance
100%
80%
60%
Total
PICU
OR
40%
Total
Ju…
M…
Ap…
M…
Fe…
Ja…
De…
No…
Oc…
Se…
Au…
Ju…
Jul…
M…
0%
Ja…
Fe…
M…
Ap…
20%
Figure 2: Maintenance Bundle Compliance
100%
90%
80%
70%
60%
50%
40%
30%
20%
10%
0%
Total
PICU
Floors
Total
System Quality Review
31
NewYork-Presbyterian Healthcare System Quality Symposium 2014
Quality 2020: A Vision of the Future
System Quality Review
32
NewYork-Presbyterian Healthcare System Quality Symposium 2014
Quality 2020: A Vision of the Future
Cohen Children's Medical Center of NY
Making Joint Commission Continuous Readiness Fun and Easy
Karen Halom RN MS, Assistant Direct Quality Management, Cohen Children's Medical Center of NY
Introduction
Problem Statement:
Continuous Joint Commission Readiness is often seen by hospital staff as tedious and boring.
The JC Standards information is often difficult for staff to integrate and prioritize in their daily
job performance role. Classroom style review of information is time consuming and inefficient in
the unpredictable 24/7 hospital environment. Employee retention of information and ability to
potentially address issues with the JC Surveyor is an ongoing challenge for hospital
administration.
Project Aim/Goal:
Joint Commission University© (JCU©) was created to ensure continuous survey readiness in a
user friendly and fun environment for all healthcare staff. The program was developed to meet
adult learner needs whenever individual staff members had available time. Team reinforcement of
important information was built into the project plan using a variety of creative, fun and user
friendly strategies for retention of knowledge. Ultimately, all JC University graduates goal was to
earn a Joint Commission Readiness (JCR) degree and feel ready and confident to speak with the
JC Surveyor at the actual unannounced JC Survey.
Project Description:
A virtual and actual Joint Commission University© was created in the Children’s Hospital.
Hospital staff were sent a JCU© Admission Acceptance Letter and officially registered in the
University. JCU© references and information were available as a "free service" on the
Unit(s)/Departments and at the JCU© Bookstore. Creative educational methodologies included
Joint Commission University© Newsletters sent by e-mail to all JC Preppies, innovative study
aids such as "Free Study Help from Cliffs Notes". JCU© Professors with previous JC Survey
experience mentored staff during periods of low acuity and decreased volume. JC competency
was evaluated through Mock JC Tracers and spot checks. Multiple unannounced JC Learning Lab
opportunities were planned. Pop quizzes involved fun activities such as word finds and/or
scavenger hunts. The overall JCU© project involved incorporating a virtual University into every
aspect of the daily activities of the hospital units/departments in order to prepare staff for the
actual unannounced Joint Commission Survey.
System Quality Review
33
NewYork-Presbyterian Healthcare System Quality Symposium 2014
Quality 2020: A Vision of the Future
Quantitative/Qualitative Measures
Quantitative indicators of JCU© survey readiness were evaluated through ongoing audits. Data
on multiple performance improvement projects is monitored ongoing and presented to the staff.
For example how many patients who required translation services had the services provided and
was this documented in the medical record was tracked and trended monthly and presented to
staff in weekly rounds, newsletters and communications. Healthcare providers, who successfully
documented translation services, and their managers, received a kudos e-mail for doing a good
job. Mock tracer activity reports were reviewed to determine areas of strength and weakness for
curriculum planning and evaluating readiness.
Qualitative indicators of JCU© success included staff enthusiasm for the project, direct feedback
to JCU© via e-mail and program evaluations.
Methodologies
Methodologies included creating an academic, fun culture for learning and meeting the JC
standards.
Teamwork and unit/departmental commitment contributed to success. Staff on all levels were
involved in processes for improving quality and had opportunities to practice discussion in JCU©
Rounds and " Mock Tracers".
The Medical staff participation sent a powerful message of the importance of the program and
provided validation of the need for structured processes around regulatory compliance. The
JCU© Professors provided continuous, on the spot feedback to participants.
Improvement Results
Staff learned the JC standards and rationales for why processes and policies are in place. This
knowledge reinforced and further standardized best practices. There where many policies and
guidelines which needed updates or revisions. The staff identified barriers and deficiencies prior
to the JC survey and partnered in the development of process changes to achieve compliance.
The frontline staff were empowered to become actively involved in patient safety initiatives and
creation of a culture of transparency. Healthcare providers were able to practice discussion in a
safe and fun learning environment before the actual unannounced JC Survey. Participants
expressed high levels of satisfaction for the methods the information was presented. The
program fostered an environment which improved teamwork and respect among the staff; which
made it all happen. Ultimately, the accreditation survey was very successful with no direct impact
JC citations.
Sustainability Strategies
Continuous survey readiness can be maintained and sustained through the JCU© methodologies
used. Following our unannounced JC Survey staff have requested that the program be continued
on a modified basis.
System Quality Review
34
NewYork-Presbyterian Healthcare System Quality Symposium 2014
Quality 2020: A Vision of the Future
Lessons Learned
1. Healthcare quality can improve through education of staff on the JC Standards.
2. Utilizing creative strategies, efficient and effective culture changes can occur impacting quality
outcomes.
3. Incorporating a new program into an existing structure is a key to success.
4. Joint Commission Survey preparation can be fun and rewarding!
Conclusion
Using creative educational strategies for continuous Joint Commission readiness can provide
opportunity to create a culture of teamwork, improve and maintain best practice outcomes, in a
fun and user friendly environment.
System Quality Review
35
NewYork-Presbyterian Healthcare System Quality Symposium 2014
Quality 2020: A Vision of the Future
Poster Presentation
Cohen Children's Medical Center of NY, NS-LIJ Hofstra Medical
School
S.K.I.N.D.E.E.P Tool for Pressure Ulcer Prevention in Critical Neonatal and
Pediatric Population Undergoing Extracorporeal Membrane Oxygenation
(ECMO)
Vita Boyar, MD,FFAP, CWCP, FAPWCA; Karen Clemens,RN; Marcia Zinger,RN
Introduction
In recent years a growing awareness has emerged over high risk of Pressure Ulcers (PU) in
pediatric population. Studies indicate that intensive care units patients have a 6-27% risk of
acquiring a PU during their stay. One of the strongest predictors of skin breakdown in ICU is
presence of medical devices. Others include immobility, friction, sensory deficit, poor perfusion,
edema and intolerance to handling. Patients undergoing Extracorporeal Membrane Oxygenation
(ECMO) for provision of cardiopulmonary support posses all risk factors. ECMO supports
infants and children with life-threatening pulmonary, oncologic, cardiac and sepsis-related
diseases. Critical status impedes frequent skin-to-toe skin assessments. PU rate was found to be
significant.
Goal-- Prevent PU in high-risk population by changing institution culture as part of Children's
Hospital's Solution for Patient Safety Network. Cohen Children's Medical Center PU HAC Team
developed hospital-wide comprehensive education initiative to decrease incidence of PU,
challenging hospital-acquired condition.
PU Prevention Bundle was followed by PDSA cycles to determine the need for improvement.
A need for a simple visual tool, engaging front-line team members in daily PU prevention was
realized.
SKINDEEP is a tool developed for prevention of PU.
Quantitative/Qualitative Measures
Occurrence of Pressure Ulcers
Execution of preventative strategies
Documentation of preventative strategies
System Quality Review
36
NewYork-Presbyterian Healthcare System Quality Symposium 2014
Quality 2020: A Vision of the Future
Methodologies
After the review of current statistics/ policies/ guidelines a PU Prevention Bundle was put
together, incorporating 6 elements that National Pressure Ulcer Advisory Panel (NPUAP)
endorses. This bundle was disseminated throughout the hospital. Compliance with bundle
elements was observed with unsatisfactory results. PDSA cycles revealed gaps in education,
documentation and in need of simple, daily tool to use by caregivers. Incidence of PUs was
significant. Hospital-wide education on significance of PU eradication was launched. Prevention,
recognition, staging, treatment and family involvement were stressed. Reduction by 40% in a year
with eventual goal of 0 was emphasized.
Pressure Ulcer Prevention Bundle was modified to one-page tool “S.K.I.N.D.E.E.P”, capturing 6
main prevention elements and including a pictorial of at risk areas and preventative products. The
tool was implemented in neonatal and pediatric ICU's ECMO recipients.
Improvement Results
Retrospective review of PU occurrence during 03/12-06/13(pre-implementation) era revealed 14
pressure ulcers. Total of 14 patients undergone 144 ECMO days. (6 patients were PU-free, 8 had
1 or more PU).
SKINDEEP was implemented in 06/2013. ECMO staff was educated on the importance of PU
prevention, shifting the thinking that PU in ICU is unavoidable. Emphasis was placed on
mandatory prevention, patient/parent involvement in skin care, decreasing morbidity &cost of
care and avoiding reportable “never events” in the hospital. Post-Implementation era (07/13—
08/14) included 13 ECMO recipients, 121 ECMO days and only 1 PU.
Compliance with tool use was 100%, documentation of measures in electronic medical record
improved.
Family members participated in PU Prevention discussion daily during rounds.
Sustainability Strategies
Continue audits on tool use in all patients undergoing ECMO.
Pressure Ulcer HAC Leads visit every ECMO patient and reviewSKINDEEP tool with staff.
Ensure that all elements of the tool are executed and documented.
Continue hospital-wide PU education.
Lessons Learned
1. Significant change involves education of all involved parties and leadership support.
2. Most pressure ulcers are avoidable
3.Proactive approach with prevention measures and rigorous audits of ongoing compliance are
necessary
System Quality Review
37
NewYork-Presbyterian Healthcare System Quality Symposium 2014
Quality 2020: A Vision of the Future
Conclusion
Pressure ulcers prevention should be an integral element of Quality Improvement initiatives in
children’s hospitals, especially in ICU. Incidence of PU can be drastically reduced with
implementation of evidence-based practices, staff education and continuous leadership support.
System Quality Review
38
NewYork-Presbyterian Healthcare System Quality Symposium 2014
Quality 2020: A Vision of the Future
Elmhurst Hospital Center
Evolving Towards High Reliability in the Operating Room: Design and
Implementation of a New Surgical Safety Process
Benjamin D. Malkin, MD; Roderick A. Calandria, RN, MSN, CCRN, BC; Carol White, MPH; William McDonagh,
RN, BSN, MPA
Introduction
Wrong-site surgery continues to be a problem nationally, in New York state and locally.
Nationwide, a subset of 13 states reported 220 wrong-site events in 2010. At our facility, a
surgical safety process based on the World Health Organization “Surgical Safety Checklist” was
in use; however, a number of near misses compelled us to examine our existing process and
identify opportunities for improvement. Our goal was to design and put into practice a highly
reliable surgical safety process to prevent wrong-person, -site and -procedure events, embed the
use of evidence-based teamwork strategies and improve patient outcomes.
Quantitative/Qualitative Measures
We measured number of staff trained in the new surgical safety process and post-training staff
survey responses, and will be collecting ongoing compliance data.
Methodologies
A multipronged approach—with broad support from administrative and clinical leaders—was
used to redesign our surgical safety process. This included the use of failure modes and effects
analysis, Lean problem solving tools, TeamSTEPPS and working with a consultant to incorporate
best practices adapted from the aviation industry.
Improvement Results
We developed 4 checklists to be used in the operating room (OR) during designated team events
(i.e., Brief, Time Out, Confirmatory Time Out and Debrief). Based on the aviation model, each
checklist had a version for use during the actual event and an “amplified” version that detailed
the correct way to perform each step of the checklist. Using a prescriptive, role-based format, we
defined standard work and supported the creation of a shared mental model for all team
members. To assist staff in learning the new process, we also filmed a demonstration video
showing a “gold standard” example of the checklists being used.
The new process was rolled out over a 2-week period. Ten 1-hour, multidisciplinary classes were
held for all staff; attendance was ensured by delaying the OR case starts for the teams scheduled
for training. We used a “flipped classroom” approach, distributing the material for review
beforehand. During the training sessions, teams participated in multiple simulated run-throughs
of the checklists—giving them the opportunity to practice using the amplified checklists and
System Quality Review
39
NewYork-Presbyterian Healthcare System Quality Symposium 2014
Quality 2020: A Vision of the Future
source documents (e.g., surgical consent)—with live coaching in the classroom and then in the
OR. We trained 48/48 (100%) nurses and 69/93 (74%) surgeons and anesthesiologists. A
debriefing session and subsequent post-training evaluation gave staff the opportunity to provide
feedback and express concerns. Respondents rated an average 79% improvement in their
knowledge/skill and 96% agreed or strongly agreed that they were confident in their ability to
apply the knowledge and skills learned from the training.
Sustainability Strategies
We have additional live training sessions for new staff and are developing an online training
module. Ongoing random compliance audits will allow us to identify problems and address them
in real time. We will also be instituting a coaching program that includes random and targeted
coaching sessions during actual cases in the OR.
Lessons Learned
1. Employing a variety of quality improvement tools helps in developing a robust product.
2. Training is most successful when it is done in a multidisciplinary, simulation-based, safe
learning environment.
3. Explanations as to “why” as well as to “how” promote user buy-in and compliance with
checklists and other methods to promote teamwork.
Conclusion
Patient safety in the OR is paramount and represents a constant challenge. Creating a highly
reliable safety process necessitates the use of proven principles, such as defining standard work
for all team members and incorporating TeamSTEPPS tools. Successful implementation can be
accomplished by giving staff dedicated time for training in a multidisciplinary team, with coaching
support during each step of the process.
System Quality Review
40
NewYork-Presbyterian Healthcare System Quality Symposium 2014
Quality 2020: A Vision of the Future
Hospital for Special Surgery
A Case Series of Understanding Ileus: A Potentially Fatal Complication of
Orthopedic Surgery
Kelianne Cummings, BA; Sara Choi, BA; Ting Jung Pan, MPH; Allina Nocon, MPH; Mayu Sasaki, MPH; Lisa A.
Mandl, MD, MPH; Steven Magid, MD; Susan M. Goodman, MD
Introduction
Post-operative ileus (POI) has been reported to complicate orthopedic surgery in 0.7- 4.0% of
cases. Although some interruption of bowel function is an expected and normal consequence of
anesthesia and surgery, when prolonged, ileus can be a significant determinant of morbidity and
mortality, leading to prolonged lengths of stay, patient discomfort, and/or physical injury. The
incidence of clinically significant ileus appears to be increasing, and POI in orthopedic patients is
poorly understood. Complications of ileus have resulted in patient death, indicating a need to
better understand this potentially lethal complication. The specific aims of this study are to define
POI, establish the incidence of POI, identify adverse events associated with POI, determine the
clinical factors associated with POI, and complications associated with POI.
Quantitative/Qualitative Measures
Descriptive statistics of 77 cases were performed with SAS version 9.3 (Cary, NC, USA).
Continuous variables are presented as means and standard deviations. Medians are presented for
categorical variables.
Methodologies
This is a retrospective case series that examines post-op ileus (POI) in patients after orthopedic
surgery at the Hospital for Special Surgery. 273 POI cases were identified using ICD-9 codes
from March 1, 2009 through April 30, 2011.Patient and surgical variables were systematically
abstracted from medical charts. Severe ileus was defined by the following criteria: (1)
Recommendation or administration of methylnaltrexone or nasogastric tube (unless put in
prophylactically or used for reason other than ileus); (2) Patient with distention and having no
bowl movement until on or after post-op day 4; (3) Ileus diagnosed by a GI consult on or after
post-op day 4; (4) Patient made or kept NPO due to distention and patient having no bowl
movement on or after post-op day 4.
Improvement Results
The study cohort was comprised of 77 cases identified by physician review / 273 cases identified
by ICD-9 codes. It consisted of 59.7% men, mean age was 61.5+/-16.3 years and body mass
index (BMI) 28.7+/-7.7 kg/m2. Incidence rates by procedure were: 1.14% spine surgeries, 0.17%
knee surgeries, 0.15% hip surgeries. Mean highest systolic blood pressure during the operation
was 138.6+/-18.4, lowest diastolic blood pressure was 46.2+/-7.73. Mean surgery time: 4.4+/2.9 hours; anesthesia time: 5.6+/-3.2 hours. Average length of stay 14.9+/-23.0 days; 88.3% of
System Quality Review
41
NewYork-Presbyterian Healthcare System Quality Symposium 2014
Quality 2020: A Vision of the Future
the cases had one surgery. Ileus first mentioned on post-op day 2(6.5%), 3(18.2%), 4(27.3%),
5(46.8%), and 6(1.3%). Average highest pain score on the day ileus was first mentioned was 6.
Nasogastric tube: 38/77 (post-op day 1(3.9%), 2(7.8%), 3(19.5%), 4+(32.5%), not recorded in
39(50.7%) of the cases. Methylnaltrexone: 44/77 (post-op day 2(3.9%), 3(11.7%), 4+(45.5%), not
recorded in 33(42.9%) of the cases. 12(15.6%) had diabetes and 6(7.8%) had a history of ileus.
Drug use prior to admission: iron supplements 11(14.3%), Proton Pump Inhibitor 24(31.2%),
non-anti-cholinergic anti-depressant 18(23.4%), calcium channel blockers 17(22.1%), calcium
supplements 15 (19.5%), beta-blockers 17 (22.1%), anti-cholinergics 15 (19.5%), and opioids 25
(32.5%). Previous abdominal surgery 37(48.1%). Pre-op NPO (92.2%) or clears (10.4%). GI
histories included: none (42.9%), GI bleed (1.3%), constipation (22.1%), difficulty
swallowing/chewing (3.9%), hepatitis(1.3%), diarrhea(7.8%), specific food preferences(9.1%),
prescribed diet (5.2%), ulcers (1.3%), diverticulitis(7.8%), ulcerative colitis/Crohns (5.2%), and
IBS(2.6%). Anesthesia: general (61.0%), CSE(32.5%), and PNB(18.2%). PCA(97%). PCA
discontinued =24 hours before ileus 47(61%). 2 cases tested positive for C. difficile. IV
medications before ileus: PCA hydromorphone(74.0%), Ondansetron (55.8%), Nalbuphine
(49.4%), Metoclopramine(46.8%). Elixhauser comorbidities: hypertension (49.4%), depression
(19.5%), obesity (18.2%), chronic pulmonary disease (18.2%), and uncomplicated diabetes
(14.3%). 54.6% were given an ASA score of 2 (mild systemic disease) and 40.3% of the cases
were given a score of 3 (severe systemic disease). See Figure 1 for the following variables: passing
flatus, bowl sounds, bowl movement, and nausea/vomiting.
Sustainability Strategies
Currently, ileus is poorly defined. This study has defined clinically significant post-op ileus, in the
orthopedic setting, which will facilitate communication among departments. This study will
provide data for protocols for the prevention, recognition, and treatment of POI at HSS. This
evidence base will be used to formulate guidelines for identification, monitoring, and prevention
of POI in high-risk patients.
Lessons Learned
1. The incidence of POI as identified by ICD-9 codes (273 cases) was 3.5 times greater than the
incidence of clinically significant POI determined by chart review (77), thus the hospital is over
diagnosing POI.
2. Spine surgeries have the highest incidence rate of the major orthopedic procedures done at
HSS.
3. Pre-admission use of proton pump inhibitors and opioids, IV administration of
HYDROmorphone, Ondansetron, and Naluphine, hypertension, depression, obesity, and
chronic pulmonary disease frequently precede POI
Conclusion
In this study we have so far demonstrated that the incidence of POI, as identified by IDC-9
codes, is much greater than the incidence of clinically significant POI. Decreased bowel function
is a normal consequence of anesthesia and surgery. Applying our definition of POI has resulted
in a reduction of what we define “true” ileus cases over a two year period from 273 to 77. Future
studies will be performed to further explore POI in the orthopedic setting.
System Quality Review
42
NewYork-Presbyterian Healthcare System Quality Symposium 2014
Quality 2020: A Vision of the Future
Figure 1. Ileus Indicators
80
Number of ileus cases (% total cases)
70
65 (84.4%)
65 (84.4%)
67 (87%)
60 (77.9%)
60
51 (66.2%)
48 (62.3%)
50
39 (50.7%)
40
39 (50.7%)
23 (29.9%)
22 (28.6%)
20
0
10 (13%)
5 (6.5%)
2 (2.6%)
1 (1.3%)
8 (10.4%)
6 (7.8%)
11 (14.3%)
11(14.3%)
15(19.5%)
Bowel
movement
Nausea/vomi
ting
13 (16.9%)
6 (7.8%)
4 (5.2%)
Post-Op Day 0 Post-Op Day 1 Post-Op Day 2 Post-Op Day 3 Post-Op Day 4+
System Quality Review
Bowel
sounds
Passing flatus
29 (37.7%)
30
10
41 (53.3%)
N/A
43
NewYork-Presbyterian Healthcare System Quality Symposium 2014
Quality 2020: A Vision of the Future
Hospital for Special Surgery, Quality Research Center
Falls Among Hospitalized Orthopedic Patients: A Prospective Case-Control
Study
Mayu Sasaki, MPH; Lisa A. Mandl, MD MPH; Wei-Ti Huang, MSc; Ting Jung Pan, MPH; Jaimie Lee; Tina Bailey,
MS; Eric Greenberg, PharmD; Danielle Edwards, DPT; Patricia Quinlan, PhD, MPA RN; and Steven K. Magid, MD
Introduction
Minimizing falls is an important safety initiative. Falls are the most frequently reported in-hospital
accidents. Falls result in morbidity, mortality, and they can initiate a pernicious “fear of falling”
cycle, which can result in the ongoing restriction of movement impaired mobility, and significant
mental distress. Falls are also associated with a longer hospital stay and increased costs. The
specific aim of this case-control study was to examine risk factors associated with inpatient falls
in an orthopedic center of excellence. The secondary aim of this study was to determine the
incidence and severity of injury that results from falls. Investigating risk factors associated with
patient falls will result in increased awareness of clinicians and hospital staff with regards to a
patient’s propensity to fall and will allow staff to initiate effective, evidence based measures to
prevent future falls. This study will also improve falls risk assessment specific to orthopedic
patients. In addition, in comparing our results to the previous work, we will be able to determine
which risk factors for falling are universal and which risk factors pertain specifically to orthopedic
surgical patients.
Quantitative/Qualitative Measures
Differences between cases and controls were compared using t-test or chi-square test, as
appropriate. A multivariate logistic regression was performed to identify predictors of falls.
Methodologies
Researchers prospectively studied falls from 5/2/10-5/1/12. Two controls were matched to
every fall on age, post-operative day (POD), type of orthopedic procedure, and time of day that
the fall occurred. Data were collected via chart review and patient questionnaire. Medical record
data for controls was abstracted from last note prior to the fall time or first note after.
Improvement Results
There were 169 falls during the study timeframe. One patient fell twice. The fall rate was 0.87 of
in-patient orthopedic admissions; 2.1 falls/1000 in-patient days. The average age of cases was
68.1 yrs, (SD 12.9), 53.5% were women, mean BMI was 29.6, (SD 6.6), and average POD was 2.9
(SD 2.6). 63.1% of cases had a Charlson index of 0, 24.8% had an index of 1, 7.0% had an index
of 2 and 5.1% had an index of 3 or higher. 40.8% of falls occurred in total knee replacements
(TKR), 23.6% in total hip replacements (THR), 26.1% in spine procedures, 7.0% in lower
extremity procedures and 0.0% in other procedures. Neither a known history of falls nor wearing
System Quality Review
44
NewYork-Presbyterian Healthcare System Quality Symposium 2014
Quality 2020: A Vision of the Future
a “falls risk” bracelet was associated with falling. Fallers were less likely to use a crutch or cane,
more likely to use a walker, and more likely to be in a single occupancy room. Cases walked
significantly fewer feet than controls. Of 168 first falls, there were 45 adverse events, most of
which were minor. 4 falls (2.6%) resulted in dehiscence/return OR, 3 (1.9%) were transferred to
a higher level of care, 2 (1.3%) resulted in dislocations and 1 (0.6%) had a fracture. There we no
deaths or intracranial/epidural bleeds. Cases had a significantly higher number of administrations
of sedatives and pain medications than controls. Controls were more likely to have PCA
administered than cases.
In a multivariate logistic regression controlling for single room occupancy, confusion, being
assigned canes/crutches, using a walker, number of feet ambulated with an assistive device,
Charlson index and being administered sedatives the 24 hours prior to a fall, variables
significantly associated with falling include confusion (OR 1.87; 95% CI 1.00-3.49), using a
walker (OR 26.28; 95% CI 5.89-117.22), and having had a sedative administered (OR 1.51 for
each time a sedative was given in the 24 hours previous to a fall 95% CI 1.20-1.91). Being in a
double occupancy room (OR 0.49; 95% CI 0.27-0.91) and having a cane or crutches assigned
(OR 0.32; 95% CI 0.12-0.88) were significantly associated with not falling. The Charlson index
and number of feet ambulated were not significantly associated with falling.
Sustainability Strategies
These data identify specific risk factors for falling which could be incorporated into permanent
anti-falling initiatives.
Lessons Learned
After controlling for other possible confounding variables:
1. For every additional administration of sedative in the 24 hours prior to a fall, an orthopedic
inpatient has 1.51 times the odds of falling.
2. An inpatient has 0.49 times the odds of falling when staying in a double occupancy room than
an inpatient who is in a single occupancy room.
3. An inpatient has 1.87 times the odds of falling when confused than an inpatient who is not
confused
Conclusion
The rate of falls and adverse events in this patient population was low. This large series identified
confusion, using a walker and being administered sedatives as being associated with falling among
orthopedic in-patients. Larger studies are needed to confirm these results, and fall prevention
initiatives incorporating these data should be tested in similar populations.
System Quality Review
45
NewYork-Presbyterian Healthcare System Quality Symposium 2014
Quality 2020: A Vision of the Future
Houston Methodist Hospital
Pharmacist Active Involvement in Patient’s Continuity of Care After Hospital
Discharge
Rafael Felippi, PharmD, BCPS; Michael Liebl, PharmD, BCPS; Janice Finder, RN, MSN
Introduction
The period after hospital discharge is a vulnerable time for patients. Medication errors are
common as a result of changes in the regimen during hospitalization, suboptimal discharge
instructions, and prolonged time to follow-up. This frequently causes increased drug-related
problems that can lead to re-hospitalization and increased morbidity and mortality. A recent
study suggests that approximately 20% of patients discharged to home from a hospital will
experience an adverse event during this transition and that 66-72% of these events are
“avoidable” or “ameliorable” with simple instructions provided at discharge. The purpose of this
study was to evaluate the role of the pharmacist as one of the key members of the patient’s
continuity of care after hospital discharge.
Quantitative/Qualitative Measures
Number and type of pharmacist interventions during the post-discharge follow-up calls.
Methodologies
The setting of this study was in an outpatient clinic that follows up telephonically with patients
discharged from Houston Methodist System Hospital. Care Navigator Nurses arranged phone
call appointments with pharmacist for patients 2-3 days after discharge who were identified with
drug-related problems or at high risk for medication issues. Pharmacy interventions included:
reviewing and educating patients on their current drug regimen; highlighting differences in the
patient’s current regimen and the discharge medication list; identifying duplicative therapies;
discussing symptoms that are possible adverse reactions from medications; recommending cost
effective alternatives; and communicating to physicians any significant or concerning findings.
Improvement Results
In a period of 5 weeks, 100 patients were referred to a pharmacist. Of those, 86 patients accepted
referral and were contacted by pharmacist. The average number of discharge medications per
patient was 14 and 94% of contacted patients had at least one pharmacist intervention. There
were a total of 160 pharmacist interventions; the most common being non-compliance (25%),
followed by incomplete/inaccurate medication list (19%) and unnecessary drug therapy (11%).
System Quality Review
46
NewYork-Presbyterian Healthcare System Quality Symposium 2014
Quality 2020: A Vision of the Future
Sustainability Strategies
The results of this project was presented to hospital leadership and it helped create a full-time
pharmacist position to join a team of nurses and case managers in following up with patients
after discharge. The ongoing results will be presented to various hospital subcommittees to
promote these services and expand patient outreach.
Lessons Learned
1) Medication management conducted by pharmacists improve
clinical outcomes for patients with chronic diseases
medication adherence and
2) Pharmacist-provided medication management can be cost saving
3)Pharmacist-provided medication reconciliation can detect and reduce medication discrepancies
Conclusion
Pharmacists making post-discharge follow-up calls can identify and intervene in many types of
drug-related problems and potentially improve patient care while reducing hospital utilization
after discharge.
System Quality Review
47
NewYork-Presbyterian Healthcare System Quality Symposium 2014
Quality 2020: A Vision of the Future
Jacobi Medical Center
A Multidisciplinary Patient Navigation Program Improves Compliance with
Adjuvant Breast Cancer Therapy in a Public Hospital
Maria T. Castaldi, MD, FACS; Dina Podolsky, MD; Saman Safadjou, MD; John McNelis, MS, FACS
Introduction
Problem Statement: Breast Cancer is the second most common cause of cancer death in women.
Black women are less likely than white woman to develop breast cancer, but they are more likely
to die of the disease. This discrepancy can be due to under use of adjuvant therapies that have
been proven to increase and prolong survival. In New York City, black and Hispanic women
who underwent surgical treatment for their breast cancer were twice as likely as white women to
experience underuse of adjuvant chemotherapy and radiation therapy. In one third of these cases,
the surgeon recommended and referred for adjuvant treatment but the patient did not follow
through with care. These system failures occurred more often in minority women treated at
hospitals serving predominately minority patients.
This project was conducted at a 430 bed public tertiary care hospital in New York City over four
years. The Breast Health Program is certified by the National Accreditation Program for Breast
Centers (NAPBC). Retrospective chart review of breast cancer patients was performed over two
years (2009-2010) to determine baseline compliance rates with the following National Quality
Forum (NQF) measures: 1) Administration of combination chemotherapy for women with Stage
(defined by the American Joint Committee on Cancer, AJCC) T1c, II, or III hormone receptor
negative (HRN) breast cancer within 120 days, 2) Administration of endocrine therapy (HT) for
women with AJCC Stage T1c, II, or III hormone receptor positive breast cancer (HRP) within
365 days, and 3) Radiation therapy (xRT) for women receiving breast conserving surgery (BCS)
within 365 days. The findings suggested low compliance rates with the above measures. We
define the baseline compliance as those patients receiving usual care (UC), or patients without
having been assigned a patient navigator. These trends triggered the use of patient navigation to
improve compliance with quality measures and meet benchmark, defined as navigated care (NC).
The goal of this project was to implement a multidisciplinary patient navigation program at an
inner city public hospital to track the use of recommended adjuvant chemo and radiation therapy
with the aim to improve compliance in meeting breast cancer care quality measures with the
ultimate goal of improved survival in breast cancer patients.
System Quality Review
48
NewYork-Presbyterian Healthcare System Quality Symposium 2014
Quality 2020: A Vision of the Future
Quantitative/Qualitative Measures
Retrospective chart review of breast cancer patients was performed over two years (2009-2010)
to determine baseline compliance rates with the following National Quality Forum (NQF)
measures: 1) Administration of combination chemotherapy for women with Stage (defined by the
American Joint Committee on Cancer, AJCC) T1c, II, or III hormone receptor negative (HRN)
breast cancer within 120 days of diagnosis of breast cancer, 2) Administration of endocrine
therapy (HT) for women with AJCC Stage T1c, II, or III hormone receptor positive breast
cancer (HRP) within 365 days of diagnosis of breast cancer, and 3) Radiation therapy (xRT) for
women receiving breast conserving surgery (BCS) within 365 days of diagnosis of breast cancer.
Methodologies
This project was conducted at a 430 bed public tertiary care hospital in New York City over four
years. We paired a patient navigator to newly diagnosed breast cancer patient for duration of
treatment for breast cancer. Patient navigator assignment was determined at time of positive
biopsy for breast cancer. Introduction of patient navigator to newly diagnosed breast cancer
patient was done at the first outpatient breast surgery visit that discussed positive biopsy results.
The same patient navigator was paired with the patient through surgery until the patient began
chemotherapy, radiation therapy or hormonal treatment. Once adjuvant breast cancer therapy
was initiated a second patient navigator, a breast oncology navigator, was paired with the patient.
The patient navigators made a reminder phone call prior to outpatient surgery, medical oncology,
and/or radiation oncology appointment. The breast surgery and breast oncology patient
navigators met the patient at all outpatient surgical and oncology outpatient appointments
respectively, and both navigators (breast surgery and breast oncology) were present to meet the
patient at the support group sessions.
Improvement Results
For UC, 82% of women received adjuvant chemotherapy for HRN breast cancer, 96% received
hormone treatment for HRP breast cancer and 83% of women had xRT after BCS. Compared
to NC (n=114) the following two years, there was 100% compliance for NQF measure 1 (n=18,
p<0.001) and 2 (n=96, p= 0.06), with the mean time to receiving adjuvant chemotherapy for
HRN breast cancer of 72±26 days (p<0.001 versus measure 1); and mean time to receiving HT
of 195±102 days (p <0.001, versus measure 2). Mean time to xRT within one year of diagnosis of
breast cancer for those with BCS is 169±87 days with 100% compliance (p <0.001).
Sustainability Strategies
Risk of underuse of adjuvant chemo and radiation therapy for the treatment of breast cancer
exists in underserved, minority communities. A robust multidisciplinary patient navigation
program has been implemented and proven successful to combat this problem in an inner city
public hospital.
Lessons Learned
1. Implementation of a multidisciplinary patient navigation program can improve compliance
with adjuvant chemo and radiation therapy for breast cancer
System Quality Review
49
NewYork-Presbyterian Healthcare System Quality Symposium 2014
Quality 2020: A Vision of the Future
2. Implementation of a multidisciplinary patient navigation program will improve cancer therapy
disparities in public hospitals.
3. This improved adherence to treatment via a multidisciplinary patient navigation program
presumes to improve survival in breast cancer and helps eliminate disparities in underserved
communities.
Conclusion
Implementation of a patient navigation program facilitated compliance with National Quality
Forum Standards and ultimately assured improved adherence to consensus generated treatment
regimens ultimately presumed to improve patient outcomes and survival in breast cancer. A
multidisciplinary patient navigation program can result in improved outcomes and better quality
of life in underserved, minority communitites.
System Quality Review
50
NewYork-Presbyterian Healthcare System Quality Symposium 2014
Quality 2020: A Vision of the Future
Kings County Hospital Center
A Lean Approach to Refine Observation Monitoring at Kings County
Behavioral Health Services
Linda Paradiso, RN, MSN, NEA-BC; Renuka Ananthamoorthy, MD; Jill Bowen, PhD; Roumen Nikolov, MD; Chao
Ma
Introduction
This project reflects the use of the Toyota Production Systems Lean approach in the
development and refinement of observation monitoring on our inpatient psychiatric units. We
identified that despite one to one nursing observation we still had failure in protecting patients
and staff from harm. While engaged in transformational activities to improve our safety and
quality of care, we identified that one to one observation was a restrictive intervention that was
not patient centered and was not providing the safety we expected. Using a Lean Rapid
Improvement Event we identified the most common risks for ordering one to one level of
observation, which included aggression, suicidality, self-harm, elopement, fall prevention,
disorganization, and sexual preoccupation. Monitoring standards and nursing interventions were
developed based upon the patient's risk. It was identified, particularly for aggressive behavior,
that one to one monitoring was not the most appropriate intervention to address such behavior.
One to one monitoring for aggression dropped significantly with fiscal improvement as a
welcome by-product.
Following a patient death, utilizing the Lean A3 thinking and problem solving approach, a gap
between safety observation and sleeping rounds was identified. Overnight staff were required to
monitor each patient’s respirations during sleep regardless of the type of safety observation
rounds ordered. Our staff reported that patients often awoke while being monitored and became
angry or paranoid from the intrusions, and staff experienced "fatigue" with the frequent and
often unnecessary monitoring. Our team determined that observations could actually be
decreased in frequency while improving care to the patient. We determined that a respiratory
assessment conducted upon admission by both the RN and MD would identify which patients
are at risk and require monitoring while asleep. Now we monitor respiration appropriate to the
level of risk.
Quantitative/Qualitative Measures
Outcome measures include One to One Observation Rates across inpatient services, rates of
aggression, and fiscal expenditures.
System Quality Review
51
NewYork-Presbyterian Healthcare System Quality Symposium 2014
Quality 2020: A Vision of the Future
Methodologies
Measures of Observation Monitoring are obtained based on number of physician orders and are
measured monthly. Rates of aggression are aggregated, monitored and reported monthly in
Incident Review meetings.
Improvement Results
Restrictive interventions, including outcome measure of One to One Observation order rates,
have shown a notable decline over the past two years. Rates reflect normal variation within the
upper and lower control limits and show a clear downward trend line (see Figure 1).
Fiscal savings are reflected monthly for same monitoring period. (see Figure 2).
Aggression rates have shown a clear decline over the past two years (see Figure 3).
Sustainability Strategies
By developing standard interventions based upon the type of behavior exhibited our unlicensed
staff were better prepared to intervene thus moving from a restrictive “monitoring” to an
intervening “treatment” approach.
A standard respiratory assessment conducted upon admission by both the RN and MD assists in
the identification of which patients are at risk and the designation of Respiratory Risk
observation and interventions.
Lessons Learned
1. Realization that one to one observation monitoring is not necessarily a higher level of
treatment.
2. We monitor our most acute patients with our least prepared staff (at least by licensure) and
many felt unprepared in identifying the best intervention when faced with behaviors that were
difficult to manage
3. Monitoring is most effective when it is based on appropriate assessment and linked to
appropriate treatment
Conclusion
Training and Clinical Strategies have been successful in impacting and sustaining a decrease in
one to one observation rates on the acute care services at Kings County Hospital Behavioral
Health Services. Utilizing Lean methodology, a robust quality management system, and an
increasing understanding of trauma informed care, initiatives were developed to provide
interventions and treatment when assigning staff to one to one monitoring. We now pay close
attention to each of our patient’s risks when determining the type of observation monitoring we
provide. Each safety or respiratory observation monitoring has its own set of standard work
interventions to ensure we are actually providing a higher level of care to our patients instead of
just watching them.
System Quality Review
52
NewYork-Presbyterian Healthcare System Quality Symposium 2014
Quality 2020: A Vision of the Future
System Quality Review
53
NewYork-Presbyterian Healthcare System Quality Symposium 2014
Quality 2020: A Vision of the Future
1.5
1.4
1.6
1.2 1.1
0.8
1.5
1.3
1.4
1.0
Aggression Rate - Inpatient
January 1, 2012 - July 31, 2014
(per 100 Pt Days)
1.0
0.9
1.0
0.9
0.6
0.4
0.2
1.1
0.8
0.7
0.8
0.6
UCL, 1.2
1.1
1.1
1.0
0.8
0.6
0.5 0.6
0.4
0.3
0.7
0.9
0.7
0.6
0.5
0.6
Average, 0.7
0.5
0.3
LCL, 0.2
0.0
Figure 3
System Quality Review
54
NewYork-Presbyterian Healthcare System Quality Symposium 2014
Quality 2020: A Vision of the Future
Kings County Hospital Center
Kings County Hospital Behavioral Health Ongoing Journey to Safety
Louise Wright-Browne, RN-BC, MA; Rita Hall-Hutchinson, RN, MSN-ANP, MA; Anne Paulin, MS, CPHRM;
Liliane Rocha, BCBA, LBA; Renuka Ananthamoorthy, MD; Roumen Nikolov, MD; Linda Paradiso, RN, MSN,
NEA-BC; Jill Bowen, PhD; Karen Quick, PhD, Chao Ma
Introduction
“The journey of a thousand miles begins with a single step” (Tuz, Lao, circa 600 BC). Kings
County Hospital's Behavioral Health Department has made numerous steps towards improving
patient and staff safety. These changes occurred in the context of the tragic death of a patient in
our care. The Department has undergone dramatic changes over the last six years as our model
of patient care delivery was to undergo a transformation. The new motto was “safety, safety,
safety.” Through the use of principles and techniques from the Lean Toyota Production System,
including A3 thinking and problem solving and Rapid Improvement Events (RIE), processes
were developed yielding significant results. During the course of this transformation we have
identified major safety initiatives and strategies. Outcomes of these efforts have included
substantial decrease in instances of aggression. More recently, we have extended our scope with
an eye toward staff wellness and trauma informed care, and have identified further challenges and
improvement strategies in impacting perception of staff safety, which will be a focus of
discussion in this presentation.
The Goals and of this Poster/Storyboard include summarizing the initiatives and outcome data,
as well as the follow-up survey that revealed that staff perception of safety remains a major
concern despite improvements attained.
Quantitative/Qualitative Measures
Outcome measures include Aggression Rates across inpatient services and results of an internal
staff survey on the "Mental Anguish of Physical Trauma on Behavioral Health Staff."
Methodologies
Measures of aggression are obtained based on incidents of patient to patient assaults and patient
to staff assaults, measured monthly in the Behavioral Health Adult and Child & Adolescent
Inpatient Services. The survey on "Mental Anguish of Physical Trauma on Behavioral Health
Staff" was part of a performance improvement project as part of a department-wide Quality Fair
with focus on trauma-informed care.
System Quality Review
55
NewYork-Presbyterian Healthcare System Quality Symposium 2014
Quality 2020: A Vision of the Future
Improvement Results
Outcome measure on Aggression rates have shown a notable decline over the past two years.
Rates reflect normal variation within the upper and lower control limits and show a clear
downward trend line (see Figure 1).
Survey results of staff on the questionnaire, "Mental Anguish of Physical Trauma on Behavioral
Health Staff," reflect that 59% of the respondents reported that they do not feel safe (see Figure
2).
Sustainability Strategies
Decreased aggression rates are sustained via standard work on unit-based processes including:
organized unit roles during crises - Crisis Management Unit (CMU), primary nursing care model,
ongoing training and booster sessions of Prevention and Management of Crisis Situations PMCS
at the unit level as well as for all new employees, table top exercises focused on trauma-informed
care, robust incident review processes, including video ethnography reviews and learning
opportunities extrapolated from these reviews, development and integration into clinical teams of
Behavioral Health Associates (BHAs), community constant observations, and increased us of
behavioral strategies supported by our Behavioral Support Team (BST).
A Staff Wellness department was created within behavioral Health Services, as well as several
Staff Wellness initiatives, including: 24 hour Staff Safety Coordinators (SSC) to respond and
support staff in the event of an incident, a staff healing room, EAP referrals, regular leadership
walks to engage and support staff, monthly BH forums with BH leadership, and other leadership
outreach efforts to staff in the event of injury.
Lessons Learned
1. Impacting aggression rates requires multiple initiatives, including training and clinical strategies
2. Data collection and sharing at the unit level is essential
3. Leadership involvement early helps build resilience and early recognition and response of
leadership can help to support recovery
Conclusion
Training and Clinical Strategies have been successful in impacting and sustaining a decrease in
aggression rates on the acute care services at Kings County Hospital Behavioral Health Services.
These approaches were driven by the need to transform services following a tragic and highly
publicized event. Utilizing Lean methodology, a robust quality management system, and an
increasing understanding of trauma informed care, initiatives were developed to address and
monitor incidents on the units. Continuing our efforts to improve processes for patients and
staff, a focus on staff wellness has been instrumental in furthering our understanding of the
impact of trauma on staff. This further informs our safety strategies.
System Quality Review
56
NewYork-Presbyterian Healthcare System Quality Symposium 2014
Quality 2020: A Vision of the Future
Figure 1
Figure 2
System Quality Review
57
NewYork-Presbyterian Healthcare System Quality Symposium 2014
Quality 2020: A Vision of the Future
Poster Presentation
Kings County Hospital Center
From Restrictive to Non Restrictive Interventions: A Culture Shift in
Managing Challenging Behaviors at Kings County Hospital Behavioral Health
Services
Liliane Rocha, BCBA, LBA; Jill Bowen, PhD; Renuka Ananthamoorthy, MD; Roumen Nikolov, MD; Linda Paradiso,
RN, MSN,NEA-BC; Chao Ma
Introduction
The use of restrictive interventions is traumatizing for patients and staff. These types of
interventions include the use of IM stat medications. Injuries and subsequent trauma for both
patients and staff were prevalent. Kings County Hospital, as part of an overall transformation,
developed several approaches in line with increasing focus on patient centered care, staff and
patient wellness, and trauma-informed care. This presentation reflects a culture shift in our
approach to the management of challenging behaviors from one in which STAT IM medications
were a predominant response to one in which behavioral interventions are a predominant
response. Data will be examined which describes the impact of behavioral interventions on the
reduction of restrictive interventions in Behavioral Health Inpatient Services. In addition, case
study data will be shown describing the effects of such interventions on particular patients.
Quantitative/Qualitative Measures
Data on the use of STAT IM was tracked over a 30-month period. Use of behavioral
interventions for the same time period was tracked and the results correlated with the use of
STAT IMs (Figure 1).
Methodologies
The use of restrictive interventions is monitored monthly in the Behavioral Health Adult
Inpatient Service, in an effort to understand the effectiveness of the various strategies
implemented to reduce the overall use of restrictive interventions, particularly the use of STAT
IM. A performance improvement review was established and analysis of the impact of behavioral
interventions on the use of restrictive interventions was investigated more thoroughly. These
strategies are taught to staff in approaches that are patient centered and trauma-informed.
Improvement Results
Traditionally, the first choice for the management of challenging behaviors related to psychiatric
illness has been the use of restrictive interventions, particularly STAT IM medications. As the use
of behavioral interventions have become more prevalent on the units at Kings County Hospital,
the team has learned to use psychosocial tools that are effective in managing such behaviors, and
that many times avoid the use of restrictive interventions completely. This utilization of
System Quality Review
58
NewYork-Presbyterian Healthcare System Quality Symposium 2014
Quality 2020: A Vision of the Future
alternative strategies to engage the patient and address the challenging behaviors in a nonrestrictive manner represents a significant culture shift in approach to patient care. This
empowers the staff and patient to employ learning strategies. These strategies translate to the
next level of care and can be re-employed immediately in the event the patient is in need of
readmission to acute care (Figure 3).
Overall, there is a negative correlation between the use of Stat IM and BST interventions (r=0.46) indicating that more behavioral interventions are being employed with less use of IM STAT
medications, indicative of the desired culture change (see Figure 1).
Sustainability Strategies
Kings County Hospital Behavioral Health Services continues to monitor the use of STAT IM
and behavioral interventions monthly, both through Quality Council data and performance
reviews. Standard work on unit-based processes include visual feedback posted on each of the
units which reflects staff behavior and its effects on patient behavior. As can be seen in Figure 2,
as staff appropriately employ behavioral strategies, challenging behaviors are decreased. In
addition, person centered treatment planning and training initiatives including: new employee
orientation, Journal Club, and trauma-informed care table top exercises emphasize the use of
alternative measures to restrictive interventions and play a key role in ensuring sustainment of
these improvements.
Lessons Learned
1. Behavioral interventions are effective tools in managing challenging behavior, including for
high risk repeat admissions patients.
2. Training, support and development of staff with regards to alternative evidence-based
techniques for management of challenging behavior has a positive impact on safety.
3. Monitoring current practices allows opportunity for improvement and evaluation of various
initiatives.
Conclusion
Training and Clinical Strategies have been successful in impacting and sustaining a decrease in the
use of restrictive interventions on the acute care services in Kings County Hospital Behavioral
Health Services. The use of behavioral interventions developed by the Behavioral Support Team
has been a successful strategy in increasing safety and decreasing the use of restrictive
interventions including STAT IM . Frequent monitoring, analysis, and reflection of our practices
allows us to continue to develop a transformation and constant improvement on the care we
offer to those we serve.
System Quality Review
59
NewYork-Presbyterian Healthcare System Quality Symposium 2014
Quality 2020: A Vision of the Future
Figure 1.
The Impact of Behavioral Interventions on
the Use of STAT IM
BST Int.
STAT IM
Linear (BST Int.)
Linear (STAT IM)
SD above or below mean
4
3
2
1
0
-1
-2
-3
Figure 2.
System Quality Review
60
NewYork-Presbyterian Healthcare System Quality Symposium 2014
Quality 2020: A Vision of the Future
Figure 3.
Patient A. Challenging Behaviors Requiring Intervention
Re-Admission –
behavior plan
immediately
employed
8
7
Frequency
6
5
Physical Agg
4
Seuxal Comments/Gestures
3
Disrobing
2
Threatening
1
Property Destruction
4/8/2014
4/16/2014
4/18/2014
12/13/2013
12/14/2013
12/15/2013
12/17/2013
12/18/2013
12/19/2013
12/22/2013
12/23/2013
12/25/2013
1/1/2014
1/7/2014
1/8/2014
1/10/2014
1/14/2014
1/17/2014
1/19/2014
1/21/2014
1/23/2014
1/26/2014
1/29/2014
2/2/2014
0
Patient A. Alternative Behaviors Learned
16
14
Frequency
12
10
Takes Medications
8
Engaged in group activities
6
Asks for activities
4
Speaks without sex comment
2
Earned reinforcer
0
System Quality Review
61
NewYork-Presbyterian Healthcare System Quality Symposium 2014
Quality 2020: A Vision of the Future
Krasnoff Quality Management Institute - a Division of the North
Shore-LIJ Health System
Using Death to Understand Disease
Kevin D. Masick, PhD; Marcella De Geronimo, MS; Jacqueline Parrish MSN, RN; Mark Jarrett, MD
Introduction
Hospitals face a challenge with developing a standardized mortality review process to understand
cause of death and identify any patterns or trends for improvements. Currently, the North ShoreLIJ Health System has 11 hospitals that have individualized independent processes for reviewing
mortalities. This lack of standardization in data collection and analysis creates a problem not only
for sharing findings among hospitals, but also permits variability within each hospital.
Standardizing the approach, using health care analytics, enables insight into end of life care,
exposes opportunities for examining appropriate care practices (ICU and comfort care practices),
ensures proper patient management and provides further direction for a more sophisticated and
specific second level site review.
The North Shore-LIJ Health System partnered with IHI to improve the understanding of end of
life care. Clinicians and quality leads expanded their 2x2 mortality tool, which was designed to
analyze an inpatient expired patient population, adding additional clinical indicators that enabled
us to provide insight into care management processes and identify gaps in care for an average of
400 monthly mortalities.
Our health system created a patient safety department with a team of nurses who have a wide
range of clinical expertise, along with a physician advisor to standardize the first level mortality
review process for all of our hospitals. Utilizing this standardized process has led to an increase in
the validity and reliability of the data captured; the data can be aggregated and analyzed at a
hospital and system level and shared to promote best practices by generating general themes (for
example, breakdown in communication, planning, or recognition, causes of mortality, and
appropriateness of care). Next steps include creating a standardized second level site review tool
(hospital and/or physician mortality review) and developing a mortality dashboard to track
performance and promote transparency about the expired population.
Quantitative/Qualitative Measures
The mortality database was developed to primarily capture quantitative measures focused on
metrics related to the hospitalization, adverse events, causes of expiration, care planning, post
mortem documentation, triggers for a second level hospital review, and end of life care.
Qualitative measures (free text) were captured to ensure that any variables which were not
System Quality Review
62
NewYork-Presbyterian Healthcare System Quality Symposium 2014
Quality 2020: A Vision of the Future
defined could be analyzed, such as a summary of the hospital stay, admission diagnosis, physician,
and cause of death from death certificate.
Methodologies
To create a standardized platform for data analysis and reporting, the Krasnoff Quality
Management Institute Analytic Team developed a streamlined process to capture clinical data.
The Krasnoff Quality Management Institute created two interactive web-based tools to capture
the necessary clinical information. This first web tool is used concurrently for capturing clinical
information for a first level review of all mortalities. This concurrent data collection affords a
clinician the opportunity to have data near real time. The second web tool was developed for a
second level hospital review. To alert hospitals that a review is necessary, an email is sent to the
medical director and quality lead at the hospital. This review is triggered by specific indicators
that lead to a hospital having to conduct a second level review. The methodology for data
collection, a web-based tool, was vetted by a team of physicians and nurses utilizing existing
clinical literature. Once the thorough testing was complete, senior leadership approved the
implementation of the mortality web based tool at all hospitals.
Improvement Results
Standardized reports have been developed and shared with hospital leadership to better
understand common themes and issues involved in mortality which stimulate process
improvement initiatives to improve the care of our patients. Currently, our data are shared with
mortality review committees at the hospital to discuss gaps in care that are related to the
mortality. This standardization allows for themes to emerge that permits aggregation of all
mortalities, regardless of the complexity of the patients’ disease. Although it is too early to make
conclusions, findings suggest improvements can be made around planning and coordination of
care
Sustainability Strategies
The web-based tool which is user friendly, has been successfully adopted by clinicians, who are
becoming more comfortable with data entry and analysis. The standardized reports have been
greeted with enthusiasm as physicians and administrators receive reliable information about
mortalities.
Lessons Learned
1. Getting buy-in for the standardization of mortality review takes time and requires education of
clinicians.
2. Developing generalized themes for data collection has helped to significantly standardize the
mortality review process, which allows for comparison of mortalities across hospitals.
3. IT solutions in the form of interactive web based data entry and analytics can become the
foundation for standardized reports across multiple organizations with different cultures.
System Quality Review
63
NewYork-Presbyterian Healthcare System Quality Symposium 2014
Quality 2020: A Vision of the Future
Conclusion
The successful development and application of this web-based first level mortality database and
its adoption and acceptance by users who were somewhat uncomfortable using data to represent
care management has transformed our understanding of mortality and help to identify gaps in
care and best practices. Clinicians are able to analyze trends and identify gaps in care for
improvement. The data collected are being used to implement new areas of improvement and
open up lines of communication between clinicians and administrators to begin to develop
processes for enhancing patient care and early recognition of potential clinical problems.
Furthermore, the success of this initial program has led to the development of a standardized
second level hospital review web-based tool as well as the development of a dashboard devoted
to mortality. A better understanding of issues surrounding end of life care is valuable for
improving the patient experience and increasing the appropriateness of hospital resources.
System Quality Review
64
NewYork-Presbyterian Healthcare System Quality Symposium 2014
Quality 2020: A Vision of the Future
Poster Presentation
Memorial Sloan Kettering Cancer Center
An Interdisciplinary Approach to Minimize the Use of Therapeutic Duplicate
Pain Medications in a Comprehensive Cancer Center
Priti Patel, BS, RPh; Raymond J. Muller, MS, RPh; Vivek Malhotra, MD, MPH; Damon Douglas, PharmD, MBA,
MS; Svetlana Granovsky, MS; Donna Robinson; Lauren Koranteng, PharmD; Mary Dowling, MSN, RN; James Gillson,
MPH.; Leonard Saltz, MD
Introduction
Memorial Sloan Kettering Cancer Center (MSK) was established in 1884 as a tertiary facility
devoted solely to the prevention, treatment and care of patients with cancer. It is one of the
largest comprehensive cancer centers in the world. Its 473 inpatient beds have a 83% occupancy
rate with an average length of stay of 6.4 days. It has accredited training programs in virtually
every area of medicine, nursing, and pharmacy.
Studies have shown that 24-60% of patients with cancer undergoing active treatment have pain;
rates are as high as 62-86% for those with more progressive disease (Annals of Oncology
2007;18: 1437-49). Experience at our center shows that over 75% of our inpatients are prescribed
medications for pain relief. Many of these patients may be prescribed sustained release
medication coupled with an immediate release breakthrough medication. Too often, in an effort
to reduce pain, multiple overlapping medications may be prescribed (e.g. multiple breakthrough
medications for similar clinical indications). This leads to unnecessary side effects, dosing
confusion and the potential for diversion. Effective pain management needs a focused approach:
a single sustained release medication with clear indications for all breakthrough indications.
Clarity is the key to success, particularly with opiates where the potential for misuse and harm is
high.
In October 2013 the Joint Commission (JC) cited the institution to prevent therapeutic
duplication, particularly in our PRN orders related to pain. They requested a more specific PRN
indication to give the RN and Pharmacist precise guidance. Standard MM.05.01.01 EP8 requires
pharmacist evaluation of therapeutic duplication as part of the comprehensive review for the
appropriateness of all medication orders. Adherence to this standard remains among the most
challenging of all medication management issues in the country. Among surveyed organizations
in 2013, approximately 15% received Requirements for Improvement (RFI) related to
MM.05.01.01 EP8. Our institution’s RFI focused on inpatient non-compliance, specifically PRN
pain medications.
Toward a goal >90% of sustained compliance for 4 consecutive months, the hospital engaged an
interdisciplinary working group, comprised of physicians, pharmacists, nurses, information
system professionals and administrators. The Physician-in-Chief appointed the Pharmacy &
Therapeutics (P&T) Committee as the clinical and administrative body to oversee development
System Quality Review
65
NewYork-Presbyterian Healthcare System Quality Symposium 2014
Quality 2020: A Vision of the Future
and outcome measures. To achieve the stated goal, we planned to: 1) review and correct
electronic PRN pain medication orders and containing order sets; 2) convert free-text electronic
PRN pain indications into a categorized therapeutic standard: Mild Pain, Moderate Pain, Severe
Pain, Mild to Moderate Pain, Moderate to Severe Pain, and All Levels of Pain; 3) install a clinical
decision support alert to block prescriber PRN pain indication duplication during electronic
order entry; 4) educate staff and provide continuous feedback on compliance.
Quantitative/Qualitative Measures
Three pharmacists evaluated compliance by measuring the number of inpatients without a
therapeutic duplication for pain over 8 consecutive months. Baseline compliance rose from 56%
to a sustained 97% for 5 consecutive months:
12/13
1/14
2/14
3/14
4/14
5/14
6/14
7/14
No. with PRN pain
indications
217
299
298
305
278
313
254
297
No. with therapeutic
duplicates
95
86
34
10
5
10
9
% noncompliance
% compliance
44
29
11
56
71
89
3
97
2
98
3
97
4
97
8
3
97
Methodologies
To reach the stated compliance goal, the institution employed several quality improvement
principles. An Anesthesiologist and member of the P&T committee reviewed all 1,200 electronic
order sets containing PRN pain indications. Each drug was assigned an appropriate therapeutic
standard indication. For example, Mild Pain and Moderate to Severe Pain was assigned to
ibuprofen and fentanyl, respectively. The service chief and nurse leader who owned each order
set, approved this indication assignment. We converted the PRN indication free-text entry into a
categorized therapeutic standard dropdown: Mild Pain, Moderate Pain, Severe Pain, Mild to
Moderate Pain, Moderate to Severe Pain, and All Levels of Pain. The hospital employed a
multidisciplinary working group and achieved immediate and comprehensive education and
awareness, including periodic e-mail notification from the center's physician and chief and
chairman of Pharmacy and Therapeutics committee. Task force members were readily available
to answer questions leading to improved compliance. Thereafter, regularly scheduled updates
were conveyed to leaders in medicine, pharmacy, nursing and administrators throughout the
center.
System Quality Review
66
NewYork-Presbyterian Healthcare System Quality Symposium 2014
Quality 2020: A Vision of the Future
Improvement Results
Outcome Events and Measures:
Nov 06, 2013 - Educational e-mail from Physician-in-Chief to all clinical staff
Nov 11, 2013 - Corrective action plan filed and accepted by The Joint Commission(TJC)
Nov 13, 2013 - P&T committee directive
Dec 10, 2013 - Audit: 122 patients with only one PRN pain indication (56% compliance; N=217
patients)
Jan 27, 2014 - Audit: 213 with only one PRN pain indication (71% compliance; N=299)*
Feb 19, 2014 - 1200 order sets updated to reassign standardized therapeutic indication; email
announcement.
Feb 26, 2014 - Audit: 264 with only one PRN pain indication (89% compliance; N=298)*
Mar 05, 2014 - P&T review of audit results
Mar 12, 2014 - Clinical decision support alert to block noncompliant prescriber electronic order
entry
Mar 17, 2014 - Audit: 295 with only one PRN pain indication - (97% compliance; N=305)*
Apr 22, 2014 - Audit: 273 with only one PRN pain indication - (98% compliance; N=278)
May 08, 2014 - Audit: 293 with only one PRN pain indication - (97% compliance; N=313)
Jun 08, 2014 - Audit: 245 with only one PRN pain indication - (97 % compliance; N=254)
Jun 10, 2014 - P&T review of audit results
Jul 08, 2014 - Audit: 289 with only one PRN pain indication - (97% compliance; N=297)
Aug 08, 2014 - Audit results accepted and issue deemed closed by TJC
* - p < 0.005 vs previous audit.
Sustainability Strategies
To sustain goal compliance, the hospital implemented a comprehensive review and correction of
electronic PRN pain medication orders and containing order sets. We converted free-text
electronic PRN pain indications into six categorized therapeutic standards: Mild Pain, Moderate
Pain, Severe Pain, Mild to Moderate Pain, Moderate to Severe Pain, and All Levels of Pain.
These pain levels were also mapped to standard assessment tools used by the nursing staff . This
permitted flexibility in ordering while maintaining consistency with existing practices.
When a PRN pain medication was ordered that would result in an overlapping indication, a
therapeutic duplication was triggered. This duplication resulted in a "hard stop" that required the
prescriber to correct the duplication before proceeding. Explanations were provided within the
System Quality Review
67
NewYork-Presbyterian Healthcare System Quality Symposium 2014
Quality 2020: A Vision of the Future
alert on how to proceed. The cause of the alert was immediately obvious as was the means to
rectify it. Regular compliance monitoring provided program feedback to all care givers. In
addition, prescribers provided feedback on how to streamline the alert.
Lessons Learned
1) Intuitive solutions that fit within existing practices lead to easier adoption and comprehension.
In this case the free text already in use was standardized using drop down explanations. Minimal
education of the new workflow was required.
2) Identifying therapeutic duplication with a popup alert at point of prescribing and immediate
instructions on how to proceed minimized confusion and complaints by prescribers.
3) Standardization of processes permits metrics to be obtained faster with more reliability.
Conclusion
In response to the Joint Commissions RFI, the hospital rapidly mobilized interdisciplinary
collaboration and dramatically increased compliance from 56% to 97% for this challenging
medication management standard. Finding a simple, intuitive solution allowed for the change to
be implemented quickly. Immediate feedback from prescribers was used to fine tune the system
quickly to facilitate end user perceptions of benefit. As a result minimal changes to the system
have been required since the early days of adoption. Compliance has been consistent suggesting
the change is sustained and durable. This method has provided a template for future issues of a
similar nature.
System Quality Review
68
NewYork-Presbyterian Healthcare System Quality Symposium 2014
Quality 2020: A Vision of the Future
Memorial Sloan Kettering Cancer Center, Department of Surgery
Decreased Incidence of Post-Operative Venous Thromboembolism Following
a Multi-Specialty Quality Improvement Initiative at a Specialty Cancer Center
Mindy Sovel MA; Daniel D. Sjoberg MA; Margaret McSweeney NP; Damon Douglass PharmD MBA MS; Vivian E.
Strong MD; Nicola Fabbri MD; Gerald A. Soff MD; Inderpal (Netu) Sarkaria MD
Introduction
The National Surgical Quality Improvement Project (ACS-NSQIP) is a nationally validated,
prospective, risk-adjusted outcomes-based program that allows member institutions to measure
their surgical outcomes and compare themselves to other institutions. Memorial Sloan Kettering
Cancer Center (MSKCC) was identified as having a higher than expected rate of post-operative
venous thromboembolism (VTE) and as a result convened a multispecialty task force to examine
the hospital’s VTE prophylaxis policies. Following an extensive literature review the panel
recommended a pilot project investigating the administration of a single dose of pre-operative
chemoprophylaxis according to service specific guidelines.
Quantitative/Qualitative Measures
The pilot project tracked the rates of post-operative deep venous thrombosis (DVT), pulmonary
embolism (PE), post-operative bleeding, and blood transfusion.
Methodologies
Attending surgeons on the Colorectal, Gastric and Mixed Tumor, Gynecologic Oncology,
Thoracic, and Urologic Oncology services developed service – specific guidelines of patient
inclusion and patients were screened of eligibility by nurse practitioners on the pre-surgical
testing service. Eligible patients were ordered for 40mg Enoxaparin or, if the patient was
planned to receive epidural analgesia, 5,000 units unfractionated heparin. Select patients were
tested for heparin inducted thrombocytopenia and thrombocytosis (HITT) prior to ordering preoperative anticoagulation. Post-operative VTE prophylaxis was according to current hospital
policy, which was not altered as part of the pilot. Patients in the pilot (August 2013 – January
2014) were compared to identically selected historical controls (January 2012 – June 2013) who
did not receive pre-operative VTE prophylaxis but otherwise had identical care.
Improvement Results
From August 1, 2013 through January 31, 2014, 2,058 eligible patients underwent operation at
Memorial Sloan Kettering Cancer Center. Identical eligibility criteria identified 4,960 patients in
the comparison time period (January 2012 – June 2013). A total of 1,463 patients (71%) were
screened by the pre-surgical testing nurse practitioners, and 59% of all patients (1,206 / 2,058) in
the pilot received pre-operative anticoagulation. Almost 60% of anticoagulated patients (706 /
1,206) received low molecular weight heparin, even though the pilot’s preferred drug was
System Quality Review
69
NewYork-Presbyterian Healthcare System Quality Symposium 2014
Quality 2020: A Vision of the Future
Enoxaparin. As compared to the comparison time period, institution of pre-operative VTE
prophylaxis lowered our DVT rate from 1.3% to 0.2% (Absolute difference: 1.1%, 95% CI:
0.7%, 1.4%, p = <0.0001) and our PE rate from 1% to 0.4% (Absolute difference: 0.6%, 95%
CI: 0.2 – 1%, p = 0.017). Interestingly, the blood transfusion rate decreased from 17% to 14%
(Absolute difference: 3.5%, 95% CI: 1.7 – 5%, p = 0.0003) although the rate of major bleeding
complications requiring invasive treatment did not significantly change (0.8% - 0.5%, Absolute
difference: 0.3%, -0.1 – 0.7%, p = 0.2) (Table 1). Less than 3% of patients (10/373) had positive
or borderline – positive HITT tests, no patients had clinical evidence of HITT. Administration
of pre-operative Enoxaparin presented barriers care in patients scheduled to receive epidural
analgesia and was frequently changed to unfractionated heparin.
Sustainability Strategies
A specific order set within the electronic medical record was created for the pilot project, and a
subsequent order set was created following completion of the pilot. Barriers to efficient clinical
care (screening HITT testing and pre-operative Enoxaparin) were abandoned following pilot
completion.
Lessons Learned
1) Electronic documentation is vitally important to a medication focused quality improvement
project.
2) Clinical intervention quality improvement projects must be clinician driven.
3) Interventions that provide barriers to current clinical care may be unnecessarily disruptive to
optimal patient care and should be avoided.
Conclusion
Instituting pre-operative chemoprophylaxis caused a decrease in post-operative symptomatic
DVT and PE. Pre-operative Enoxaparin and HITT testing caused unnecessary barriers to
efficient clinical care and were abandoned. Service specific guidelines for the pre-operative
administration of unfractionated heparin are currently being finalized and implemented, with
follow-up analysis of data planned in the future.
System Quality Review
70
NewYork-Presbyterian Healthcare System Quality Symposium 2014
Quality 2020: A Vision of the Future
Table 1: Pilot cohort compared to comparison cohort. All eligible patients are included within the
pilot cohort, regardless of whether or not they received pre-operative anticoagulation.
Any Bleeding *
Bleed Grade 3+
Any Transfusion
RBC Transfusion
DVT
PE
Pilot
(n=2058)
52 (2.5%)
11 (0.5%)
285 (14%)
280 (14%)
4 (0.2%)
9 (0.4%)
Comparison
(n=4960)
210 (4.2%)
42 (0.8%)
860 (17%)
829 (17%)
63 (1.3%)
50 (1.0%)
Absolute
Difference
1.7%
0.3%
3.5%
3.1%
1.1%
0.6%
95% CI
p-value
0.8%, 2.6%
-0.1%, 0.7%
1.7%, 5%
1.3%, 4.9%
0.7%, 1.4%
0.2%, 1.0%
0.001
0.2
0.0003
0.001
<0.0001
0.017
* Bleeding includes SSE entries of Anemia, GI bleeding, Hemorrhage, Hematoma, Hematuria,
Bladder, Vaginal Bleeding, and Hemothorax
System Quality Review
71
NewYork-Presbyterian Healthcare System Quality Symposium 2014
Quality 2020: A Vision of the Future
New York Hospital Queens - Emergency Medical Associates
Improving Pre-Hospital and Trauma Team Activation for Injured Older Adults
Age 65 Years or Older Presenting to the Emergency Department
Radeos, Michael S MD MPH; Kaldis, Vasileios MD; Ali, Zuhair MD: Torres, Jose MD; Jazarevic, Slobodan MD;
Sample, Jason MD; Zimmermann, Mary Ellen BSN CEN, Ourian, Ariel MD; Dickason, Robert M MD
Introduction
In November 2012, the Eastern Association for the Surgery of Trauma (EAST) published
guidelines for the management of trauma in the elderly patient, aged 65 years or older. Among
their recommendations were the following Level 2 and Level 3 recommendations: "Injured
patients with advanced age (>= 65 years) and pre-existing medical conditions should lower the
threshold for field triage directly to a designated/verified trauma center" (Level 2); "An initial
aggressive approach should be pursued for management of the elderly patient unless in the
judgment of an experienced trauma surgeon it seems that the injury burden is severe and the
patient appears moribund" (Level 2); "A lower level for trauma activation should be used for
injured patients aged 65 years or older who are evaluated at trauma centers" (Level 3); and
"Elderly patients with severe anatomic injuries (e.g., one or more body systems with an
Abbreviated Injury Severity Scale (AIS) of >= 3 should be treated in designated trauma centers,
preferably in intensive care units (ICUs) staffed by surgeon-intensivists." (Level 3).
At our 535-bed tertiary-care academic New York State designated trauma center, we sought to
determine if our injured elder patients were receiving pre-hospital notifications as well as
emergency department (ED) full trauma team activations (FTTAs) when appropriate. We
reviewed our rates of pre-hospital notifications and ED FTTAs and found that we could
improve our performance. By categorizing elder patients as serious traumatic injuries, we wanted
to determine if these elder patients with significant traumatic injuries were getting the timely
intervention that is the intent of these notifications and activations. Through educational
intervention aimed at constant debriefing of pre-hospital and ED staff, we sought to increase
awareness of the need for these actions and to thereby increase their appropriate utilization.
Quantitative/Qualitative Measures
We measured rates of pre-hospital trauma notifications for all elderly injured patients presenting
to our ED. We also measured all of the full trauma team activations (FTTAs) for these patients.
We also measured trauma consults, where a trauma resident responds to the ED rather than the
FTTA.We also analyzed demographic and clinical data for these patients. We report results as
means (with standard deviation) or medians (with inter-quartile range (IQR) as appropriate. We
measure associations between dependent variables and the outcomes using chi-square or Fisher
System Quality Review
72
NewYork-Presbyterian Healthcare System Quality Symposium 2014
Quality 2020: A Vision of the Future
exact test for categorical data, and student t-test or Mann-Whitney U for continuous data, as
appropriate.
Methodologies
We designed a performance improvement (PI) study comparing a pre-intervention period
(September 3, 2012 through March 19, 2013) with a post-intervention period (March 20, 2013
through August 30, 2013). Our intervention was an educational outreach to our pre-hospital
personnel as well as our ED staff, stressing the increased level of awareness that our elderly
trauma patients required based on the new guidelines.
Improvement Results
There were 395 trauma patients who presented to NYHQ between September 3, 2012 and
August 30, 2013. Median age for all patients was 83 years (IQR 75-89). There were 229 (58.0%)
females; 276 (69.9%) White, 89 (22.5%) Asian; 22 (5.6%) Black, and 8 (2.0%) other; 42 (10.7%)
were Hispanic. There were no significant differences in patient demographics between the pretest and post-test periods. The majority of injuries in this population were same-level falls (SLFs):
204 (51.7%), followed by stairs or ladders: 71 (18.2%), and multi-level falls (MLFs): 54 (13.7%).
The demographics and types of falls did not vary significantly between the pre-test and post-test
periods.
Pre-hospital trauma notifications were made for 29 (24.1%) of elderly patients with significant
trauma in the pre-test group and increased to 35 (35.4%) in the post-test group. Incidentally, 61
(15.5%) of patients arrived by private vehicle, and the rates of significant trauma in these patients
was identical to those brought by EMS (65.6% and 65.6%, respectively). FTTAs among elderly
patients brought in by ambulance were 35 (29.2%) in the pre-test group and increased to 40
(40.4%) in the post-test group. Trauma consults also increased in the post-test group from 19
(15.8%) to 22 (22.2%), P=0.034.
Sustainability Strategies
We plan to continue our educational initiatives to our pre-hospital personnel, our ED nurses and
ED physicians. We will reinforce this teaching in our monthly staff QI meeting and include this
data in our resident conferences as well as our inter-departmental conferences. We will maintain
high vigilance for elder trauma patients who come in with seemingly minor mechanism of injury
as these patients may harbor significant injuries. By involving the entire team, we are more likely
to continue improving our rates of appropriate notification and activation for the elderly injured
patient. A process of plan-do-check-act (PDCA) remains the cornerstone of our QI strategy.
Lessons Learned
1) Providing the team with the latest litearture (especially the latest guidelines) that become
available regarding the care of the elder injured patient. This will be done through continuing
medical education and reinforcing key elements of the guidelines with staff on an ongoing basis.
2) Continuous measurement of our pre-hospital trauma notifications and FTTAs so that we may
ensure the appropriateness of these activities.
System Quality Review
73
NewYork-Presbyterian Healthcare System Quality Symposium 2014
Quality 2020: A Vision of the Future
3) We are all realizing through this PI process that there may be complex reasons why the elderly
are more at risk than their younger counterparts. Some of these may relate to decreased pain
sensation, alteration of vital signs by cardio-active drugs and increased bleeding from older and
novel anticoagulants.
Conclusion
Through our PI efforts, we have shown a small but encouraging improvement in pre-hospital
trauma notifications as well as ED FTTAs. There still exists much room for continuing
improvement in the pre-hospital and ED settings.
System Quality Review
74
NewYork-Presbyterian Healthcare System Quality Symposium 2014
Quality 2020: A Vision of the Future
New York Hospital Queens - Emergency Medical Associates
Reducing the Use of Computed Tomography Scans for the Diagnosis of Acute
Appendicitis by Using Ultrasound as the Sole Diagnostic Study
Radeos, Michael S. MD MPH; Kaldis, Vasileios MD; Ali, Zuhair MD; Triantos, Georgios-Efthymios MD; Babovic, Maja
MD; Khin, Sandi MD
Introduction
In an effort to reduce the negative laparotomy rate in emergency department (ED) patients
suspected of having acute appendicitis, surgeons have been requesting increasing numbers of
computed tomography (CT) scans of the abdomen and pelvis in order to increase their diagnostic
certainty prior to operating. However, the increased use of CT scan has led to increased radiation
exposure and intravenous (IV) contrast nephropathy among ED patients with suspected
appendicitis, as well as increasing their length-of-stay (LOS) in the ED and potential for
perforation of a diseased appendix secondary to to that increased ED LOS.
At our academic medical center, a 535-bed New York State designated trauma center with
125,000 patient annual ED visits, we sought to determine whether an ultrasound-first protocol
might allow the surgeon sufficient diagnostic certainty to operate on a suspected appendicitis
without CT. Our Emergency Medicine Residency Training Program has been fully accredited by
the ACGME and we have had a Division of Ultrasound within our Department of Emergency
Medicine. The Ultrasound Division trains fellows in ultrasound as well as our residents, and they
constantly keep the residents and fellows updated as to the sensitivity and specificity of
ultrasound in the diagnosis of appendicitis. The key issue is that the sensitivity is not optimal, so
that a negative ultrasound study cannot exclude acute appendicitis. However, a positive
ultrasound study is quite specific and thus provides high diagnostic certainty that the patient
actually has the disease.
This project aimed to increase the awareness of emergency physicians in the utility of an
ultrasound first clinical strategy, to determine if we could reduce CT scans for our patients
suspected of having acute appendicitis.
Quantitative/Qualitative Measures
We examined all patients who had a diagnosis of acute appendicitis and retrospectively reviewed
what diagnostic tests the patients underwent prior to surgery. We noted whether patients had
surgery or conservative management with intravenous (IV) antimicrobials. We report results as
means (with standard deviation) or medians (with inter-quartile range [IQR} as appropriate. We
measure associations between dependent variables and the outcomes using chi-square or Fisher
exact test for categorical data, and student t-test or Mann-Whitney U for continuous data, as
appropriate.
System Quality Review
75
NewYork-Presbyterian Healthcare System Quality Symposium 2014
Quality 2020: A Vision of the Future
Methodologies
We designed a performance improvement (PI) study comparing a pre-intervention period
(December 23, 2011 through March 21 2013) with a post-intervention period (March 22, 2013
through March 27, 2014). Our intervention was an educational outreach to our ED staff,
stressing that they should consider ordering an ultrasound as the initial diagnostic imaging study
when they suspect appendicitis. We also explained the rationale behind this approach to the
radiologists who would read these studies as well as the surgeons who would determine whether
to operate based upon the ultrasound findings.
Improvement Results
There were 516 patients admitted to our institution between December 23, 2011 through March
27 2014 with acute appendicitis. Median age for all patients was 36 years (IQR 20-53). Our
pediatrics ED treats patients up to age 21. There 145 (28.1%) pediatric patients. There were 281
(54.5%) females. CT scans were ordered for 460 (89.2%) of patients. Race/ethnicity was available
for 489 (94.8%) of patients, and was: Asian 169 (34.6%); White 144 (29.5%); Black 29 (5.9%);
and Other 141 (28.8%). Ultrasounds were ordered for 152 (29.5%) of patients. In 123 (23.8%)
both an ultrasound and CT scan were ordered. Results of ultrasound were positive in 47 (35.9%)
patients. In the pre-group, CT scan was ordered despite a positive ultrasound in 11 (42.3%) of
cases. In the post-group, that number had increased to (76.2%). When we restricted our analysis
to pediatric patients, a similar pattern emerged. In the pre-group, CT scan was ordered despite a
positive ultrasound in 8 (36.4%) of cases. In the post-group, that number had increased to 10
(71.4%).
Sustainability Strategies
We plan to continue our educational initiatives to our emergency physicians (EPs), radiologists
and surgeons. We will reinforce this teaching in our monthly staff QI meeting and include this
data in our resident conferences as well as our inter-departmental conferences. By involving the
entire team, we are more likely to continue improving our rates of appropriate notification and
activation for the elder injured patient. A process of plan-do-check-act (PDCA) remains the
cornerstone of our QI strategy.
Lessons Learned
1) It is difficult to change practice in some cases. Appendicitis provides many reasons why this
may be so. First, EPs are concerned that ordering an ultrasound may be a waste of time as the
surgeon may not operate solely on a positive ultrasound study. Radiologists may fear that
ultrasound is operator dependent and that poor sensitivity may lead to missed diagnoses.
2) Educating the patients is also a challenge. If a patient (or patient's parent or care-giver in the
pediatric ED) understood that a positive ultrasound may allow them to avoid the radiation and
IV contrast of a CT scan they may persuade the surgeon to act on that limited information.
3) And all of us are concerned about malpractice in the face of a missed diagnosis. However, by
working together and balancing the reasonable risks and benefits, we can change the standard of
care for our patients.
System Quality Review
76
NewYork-Presbyterian Healthcare System Quality Symposium 2014
Quality 2020: A Vision of the Future
Conclusion
We could not show a reduction in the ordering of CT scans for acute appendicitis despite the
presence of an ultrasound that actually confirmed that diagnosis. This PI project shows how
difficult some changes can be. However, this initiative will continue as more patients and healthcare providers question the wisdom of exposing more people to CT radiation and IV contrast
nephropathy, especially when a safer diagnostic pathway exists.
System Quality Review
77
NewYork-Presbyterian Healthcare System Quality Symposium 2014
Quality 2020: A Vision of the Future
New York Hospital Queens
A Hospital's Journey to Stage 2 Meaningful Use
Kenneth R. Ong, MD, MPH; Camela Morrissey; Caroline Keane; Bebe Rahamatalli, PA
Introduction
Achieving Stage 2 of Meaningful Use (MU2) has been a national challenge. As of August 25,
2014, only 143 out of 4800 eligible hospitals have attested compliance.
The presentation shares the story of how New York Hospital Medical Center of Queens, a 535
bed acute care hospital, achieved MU2.
The two most challenging objectives for hospitals nationally has been the 10% threshold for the
electronic transmission of the Summary of Care and the 5% threshold for patient access to the
patient portal.
This poster presentation shares how we made workflow innovations to improve transitions of
care and promote patient engagement.
Quantitative/Qualitative Measures
16 Core Objectives and 3 Menu Objectives (http://www.cms.gov/Regulations-andGuidance/Legislation/EHRIncentivePrograms/Downloads/Stage2_MeaningfulUseSpecSheet_T
ableContents_EligibleHospitals_CAHs.pdf)
16 Clinical Quality Measures (http://www.cms.gov/Regulations-andGuidance/Legislation/EHRIncentivePrograms/Downloads/CQM2014_GuideEH.pdf)
Methodologies
Electronic Transmission of Summary of Care
Analysis of discharges revealed that 30 percent of discharges were referred to home health
agencies and long-term care providers. Eight of twenty of those provider organizations
purchased direct messaging inboxes from local health information service providers, i.e.,
MedAllies, Bronx RHIO. Case managers sent C-CDA Visit Summaries for all patients referred to
these eight provider organizations.
Patient Portal Adoption
Marketing lead a Patient Portal Campaign team comprised of representatives from Case
Management, Volunteer Services, Admitting/Registration, Corporate Compliance, Office of
Patient Experience, Nursing, H.I.M., Informatics, and Information Technology.
System Quality Review
78
NewYork-Presbyterian Healthcare System Quality Symposium 2014
Quality 2020: A Vision of the Future
Improvement Results
All 16 Core Objectives, 3 Menu Objectives, and 16 Clinical Quality Measures were met (see
Tables 1, 2, 3, 4, 5)
Sustainability Strategies
Electronic Transmission of Summary of Care
As more ambulatory physicians adopt MU2 compliant EHRs and/or join health information
exchanges with direct messaging, we will be able to send more Summary of Care C-CDAs to
improve transitions of care from inpatient and the ED. Plans are under way to add a data field in
our credentialing system to capture a physician's Direct Address. Future EHR software upgrades
promise to automate transmission via direct messaging.
Patient Portal Adoption
We hire Administrative Interns to serve as Patient Portal Concierges. As patient engagement
grows in our communities over the coming years, using patient portals will become more
common.
Lessons Learned
1. Transitions of Care: Referring and receiving providers want to improve care transitions.
Greater collaboration with post-acute care providers is a successful factor for this MU2 objective.
Direct messaging is an opportunity to improve care coordination by sharing HIPAA-secure Visit
Summaries.
2. Patient Portal Adoption: Like success elsewhere in healthcare, achieving Stage 2 of Meaningful
Use requires team-based work. Promoting patient engagement involves everyone from
registration, administrative interns, clinicians, and case managers.
Conclusion
Achieving Stage 2 Meaningful Use is a waypoint in health care transformation.
Sharing Visit Summaries in a HIPAA-compliant fashion improve transitions of care.
Promoting Patient Portal adoption is a significant step in engaging patients in their own health.
System Quality Review
79
NewYork-Presbyterian Healthcare System Quality Symposium 2014
Quality 2020: A Vision of the Future
Table 1.
Table 2.
System Quality Review
80
NewYork-Presbyterian Healthcare System Quality Symposium 2014
Quality 2020: A Vision of the Future
Table 3.
Table 4.
System Quality Review
81
NewYork-Presbyterian Healthcare System Quality Symposium 2014
Quality 2020: A Vision of the Future
Table 5.
Attestation of core, menu, clinical quality measures
Type
Core
Number Objective
1A Computerized provider order entry (CPOE): Medications
Denominator
Threshold
Numerator
60%
194176
194552
7/1 to 9/30 Attested
99.81%
Yes
Core
1B Computerized provider order entry (CPOE): Laboratory
30%
280820
280936
99.96%
Core
1C Computerized provider order entry (CPOE): Radiology
30%
21109
21169
99.72%
Compliant
Yes
Yes
Yes
Yes
Yes
Yes
Yes
Yes
Yes
Yes
Core
2 Demographics
80%
6528
6844
95.38%
Core
3 Vital Signs
80%
5583
6175
90.41%
Core
4 Smoking Status
80%
6144
6634
Core
5A Five Clinical Decision Support Interventions
Core
5B Drug-drug and drug-allergy interaction checks
Core
Core
Core
Core
Core
Core
6 Incorporate Clinical Lab Results
7 Patient list generation (VTE Overlap Therapy & VTE Prophylaxis
Noncompliant)
8A View, Download, & Transmit (Patient Portal): Health Information Available
to Patient Portal within 36 hours
8B View, Download, & Transmit (Patient Portal): View, Download, or Transmit
9 Patient Education
10 Medication Reconciliation
92.61%
Compliant
Compliant
55%
1433025
1479619
96.85%
50%
4867
6025
80.78%
5%
970
6025
16.10%
Yes
10%
4416
6175
71.51%
88.63%
Yes
Yes
Yes
Yes
Yes
Yes
Yes
Yes
Yes
Yes
50%
6066
6844
Core
11A Summary of Care: Summary of Care Given to Patient
50%
4806
6075
79.11%
Core
11B Summary of Care: Exchange Document Transmitted Electronically
10%
1287
6075
21.19%
Core
11C Summary of Care: Exchange Document Sent to Another E.H.R.
Compliant
Core
12 Public Health Reporting: Immunizations
Compliant
Core
13 Public Health Reporting: reportable laboratory results
Compliant
Core
14 Public Health Reporting: syndromic surveillance
Compliant
Core
15 Security Assessment & Action Plan
Core
16 Bar Code Medication Administration (electronic medication
administration record; eMAR).
1 Record whether a patient 65 years old or older has an advance directive.
Menu
Compliant
10%
43325
140542
30.83%
50%
2541
2634
96.47%
Menu
2 Record patient family health history as structured data.
20%
1761
6166
28.56%
Menu
3 Record electronic notes in patient records.
30%
5368
6175
86.93%
System Quality Review
Yes
Yes
Yes
82
NewYork-Presbyterian Healthcare System Quality Symposium 2014
Quality 2020: A Vision of the Future
Clinical Quality Measures
Patient access measure 2
Proportion Of Patients Logged In By Department
50%
45%
40%
35%
30%
25%
20%
15%
10%
5%
0%
System Quality Review
Percent
83
NewYork-Presbyterian Healthcare System Quality Symposium 2014
Quality 2020: A Vision of the Future
Labor & Delivery Patient Handout
System Quality Review
84
NewYork-Presbyterian Healthcare System Quality Symposium 2014
Quality 2020: A Vision of the Future
e-Mail Sent to Discharged Patients
System Quality Review
85
NewYork-Presbyterian Healthcare System Quality Symposium 2014
Quality 2020: A Vision of the Future
Patient portal guide
System Quality Review
86
NewYork-Presbyterian Healthcare System Quality Symposium 2014
Quality 2020: A Vision of the Future
System Quality Review
87
NewYork-Presbyterian Healthcare System Quality Symposium 2014
Quality 2020: A Vision of the Future
System Quality Review
88
NewYork-Presbyterian Healthcare System Quality Symposium 2014
Quality 2020: A Vision of the Future
Hospital Staff Patient Portal Button
Summary of care measure 2
C-CDA Recipients
70%
60%
50%
40%
30%
20%
10%
0%
System Quality Review
Percent
89
NewYork-Presbyterian Healthcare System Quality Symposium 2014
Quality 2020: A Vision of the Future
Health Information Service Providers
Bronx RHIO
MedAllies
29%
71%
System Quality Review
90
NewYork-Presbyterian Healthcare System Quality Symposium 2014
Quality 2020: A Vision of the Future
New York Hospital Queens
Measures Taken To Improve The Rate of Documentation of Sonographic
FAST Exams Performed in Blunt Trauma Presentations
Nick Copeli MD, Mary Ellen Zimmerman RN, Manish Sharma DO, Zuhair Ali MD, Michael S. Radeos MD, MPH,
Mark Kindschuh MD, Jason Sample MD, N Khan MD, Nidhi Garg MD
Introduction
US FAST is a frequently performed assessment tool for surveying abdominal blunt trauma in the
ED: making sure to document both performance and results in the ED is crucial for cohesive
patient care, reimbursement, as well as medicolegal accountability.
Quantitative/Qualitative Measures
US FAST documentation before the implementation of an EMR template for FAST results
Methodologies
This is a retrospective chart review study performed at an urban Level 1 trauma center with an
annual visit of 125,000 patients per year.All patients which were seen by trauma team either as
consult or full activation were reviewed from the period of June 1st - Sept. 2013.Demographic
data and vitals signs were collected in addition to the data like hospital disposition. Descriptive
analysis was performed followed by univariate analysis. In the end , logistic regression was
performed with documentation of FAST as positive outcome
Improvement Results
Total 495 adult patients >14 years of age who were evaluated by trauma team presented to ED
between January 1st, 2013 and September 30, 2013. Out of which 386 were full activation and
108 were trauma consults with total median age of 48 (IQR 30-69) yrs and 326 (65.9%) males,
432 (87.3%) arrived by EMS, median systolic blood pressure of 137 (IQR 122-156), median
diastolic blood pressure of 80 (IQR 70-91), median Heart Rate of 84 (IQR 73-98). FAST exam
was performed in 333 (67.3%) patients and documented in only 284 (57.3%). FAST was positive
in only 6 (1.2%) patients and CT scan of abdomen was performed in 103 (20.8%) patients. FAST
exam was always documented in case it was positive for free fluids. CT was done in case of 63
(12.7%) patients where FAST was documented and CT was done in case of 40 (8.1%) patients
where FAST was not documented. 64 (12.9%) went to OR after 1 patient had a positive FAST
and rest 63 - initial FAST was neg. FAST study was documented in 43 cases who went to OR
System Quality Review
91
NewYork-Presbyterian Healthcare System Quality Symposium 2014
Quality 2020: A Vision of the Future
and in rest 21 cases, there was no documentation of FAST.Total 345 (69.7%) were discharged
home, 79 (16.0%) were sent to nursing home or rehab, 26(5.2%) patients left AMA, 21 (4.2%)
died in the hospital, 11 (2.2%) were transferred, 12 (2.4%)were sent to police/jail and 1 (0.2%)
patient was homeless.There was a perfect correlation of FAST documentation to positive FAST
findings, there was no significant factor which was particularly attributable to non documentation
of FAST when FAST was negative.
Sustainability Strategies
Simple template implementation for US FAST result documentation to the EMR stands to be a
reliable and user-friendly means to incorporate trauma imaging results in the record.
Lessons Learned
1. Critical decision making studies could be potentially missed in documentation during busy
situations like Trauma.
2. Providers need a mandatory field in EMR to ensure it is documented.
Conclusion
We identify this as a system error and documentation bias for positive FAST. We intend the
improve the rate of documentation by making FAST note as mandatory part of trauma note.
Also, there is emerging evidence and data if repeat FAST should be performed in cases where
initial FAST was negative. In order, to perform second FAST , it is very important that results of
initial FAST be documented and then repeat FAST. Our template includes documentation of
both FAST results with time as FAST is time sensitive study.
System Quality Review
92
NewYork-Presbyterian Healthcare System Quality Symposium 2014
Quality 2020: A Vision of the Future
EMR Template
Date: MM/DD/YYYY
Time: HR: mIN (24 hrs format)
RUQ view
1. Neg for free fluid
2. Positive for free fluid
3. Indeterminate
LUQ view
1. Neg for free fluid
2. Positive for free fluid
3. Indeterminate
Suprapubic view
1. Neg for free fluid
2. Positive for free fluid
3. Indeterminate
Subxiphoid view
1. Neg for free fluid
2. Positive for free fluid
3. Indeterminate
FAST result:
1. Negative( if all 4 views neg)
2. Positive (if any view is positive)
3. Indeterminate (if no view is positive and/or all views negative but any view indeterminate)
REPEAT FAST (suggested at 1 Hr):
Date: MM/DD/YYYY
Time: HR: mIN (24 hrs format)
RUQ view
1. Neg for free fluid
2. Positive for free fluid
3. Indeterminate
LUQ view
1. Neg for free fluid
2. Positive for free fluid
3. Indeterminate
System Quality Review
93
NewYork-Presbyterian Healthcare System Quality Symposium 2014
Quality 2020: A Vision of the Future
Suprapubic view
1. Neg for free fluid
2. Positive for free fluid
3. Indeterminate
Subxiphoid view
1. Neg for free fluid
2. Positive for free fluid
3. Indeterminate
FAST result:
1. Negative( if all 4 views neg)
2. Positive (if any view is positive)
3. Indeterminate (if no view is positive and/or all views negative but any view indeterminate)
System Quality Review
94
NewYork-Presbyterian Healthcare System Quality Symposium 2014
Quality 2020: A Vision of the Future
Poster Presentation
New York Hospital Queens
A Multidisciplinary Team Approach to Morning Report Improves Core
Measures in Critical Care
James Gasperino MD, PhD, MPH; Luciano Lemos-Filho, MD, MS; Keziah S. Narayana-jaya, PA; Mimi Lim RN;
Stephanie Barrett, MD; Michael Hansen, MD, Divya Sohal, MD; Qi-Ming Zhu, MD, Melvin Hochman, MD; Seema
Kurian, RN
Introduction
Care of patients with critical illness is costly accounting for approximately 20% of a typical
hospital budget, and nearly 0.7 % of the gross domestic product. New health care delivery
models are emerging that reduce cost and improve quality of care for patients with critical illness.
These models emphasize shared decision making by a multidisciplinary team, and involve
horizontal integration across critical care settings. As part of a new high intensity intensive care
unit –physician staffing program, we implemented a structured morning report format comprised
of a multidisciplinary team of physician and non-physician providers caring for patients in our
medical intensive care unit (MICU) and coronary care unit (CICU). While the morning report
format has typically been viewed as an educational opportunity for housestaff (e.g., case-based or
evidenced-based learning), its utility as a process-targeted quality improvement tool is not known.
We tested the hypothesis that a structured morning report comprised of a multidisciplinary team
led by an intensivist could increase compliance with hospital guidelines for prophylaxis against
venous thromboembolic disease (VTE), and reduce the use of unnecessary indwelling urinary
catheters.
Quantitative/Qualitative Measures
We measured compliance with hospital guidelines for prophylaxis against venous
thromboembolic disease (VTE), prevalence of indwelling urinary catheters, and the incidence of
catheter-associated urinary tract infection in patients admitted to the medical intensive care unit
and coronary care unit.
Methodologies
We implemented a multidisciplinary team of physician and non-physician providers to function
as a process- targeted quality improvement tool. Using a paradigm that emphasized shared
decision making we focused on compliance with hospital guidelines for prophylaxis against VTE,
and use of indwelling urinary catheters. We employed a quality improvement method reminiscent
of FADE (focus, analyze, develop, execute,evaluate). To establish baseline values and identify
changes associated with our intervention, we collected data daily and compared it to values
obtained prior to our intervention. Using data to drive cultural change, we further refined our
System Quality Review
95
NewYork-Presbyterian Healthcare System Quality Symposium 2014
Quality 2020: A Vision of the Future
morning report structure to include additional key personnel, and developed action plans for
improvement.
Through constant monitoring and using opportunity teams to target specific quality metrics, we
have developed a structure to sustain our quality improvement efforts.
Improvement Results
During the study period, compliance with hospital guidelines for prophylaxis against VTE
increased from 37% to 100% (Pearson Chi-Square; p < 0.013) and from 46% to 100% (Pearson
Chi-Square; p<0.037) in the MICU and CICU, respectively. After controlling for patient days, the
morning report format was associated with a nearly 40% reduction in the prevalence of
indwelling urinary catheters in the MICU (Pearson Chi-Square; p <0.001), and a low rate of
catheter- associated urinary tract infections during the study period (MICU: 1.32/1,000 catheter
days; CICU: 0 /1,000 catheter days).
Sustainability Strategies
We developed an effective monitoring system by working closely with our hospital’s Department
of Quality and Patient Safety. In addition, we used the principles endorsed by the Agency for
Healthcare Research and Quality
(Quality improvement tool kit, Section E: Monitoring Progress for Sustainable Improvement.)
We chose a limited set of clinical measures (e.g., compliance with VTE prophylaxis, prevalence of
indwelling urinary catheters) based on potential opportunities for improvement at our institution.
Through a collegial and interdisciplinary environment, we created transparency at each level of
the process improvement program, as well as a format for communication. Measures of interest
were evaluated daily on each patient admitted to our MICU and CICU, and action plans were
implemented by the team at the point-of-care. Monthly scheduled reporting of our clinical
measures ensure our ability to sustain the program. The morning report format creates a clear
procedure for identifying and correcting deviations from best practices.
Lessons Learned
1. Shared decision making by members of a multidisciplinary team caring for critically ill patients
can improve clinical outcomes.
2. A successful quality improvement program can be implemented without a significant financial
investment.
3. Horizontal integration across critical care settings is an effective way to standardize care and
ensure best practices.
Conclusion
The financial constraints imposed on hospitals by health care reform have created a need for a
more efficient system to deliver critical care. New reimbursement polices, including the Valuebased Purchasing mandate, tie Medicare reimbursement to clinical outcome measures. Health
care providers (and health care systems) are encouraged to strive both for quality and costeffective treatment. A structured morning report that includes an intensivist and a
multidisciplinary team can be used as a process-targeted quality improvement tool to achieve this
System Quality Review
96
NewYork-Presbyterian Healthcare System Quality Symposium 2014
Quality 2020: A Vision of the Future
goal. Hospitals may realize significant improvements in core measures by applying this cost
effective format across all intensive care units.
System Quality Review
97
NewYork-Presbyterian Healthcare System Quality Symposium 2014
Quality 2020: A Vision of the Future
New York Hospital Queens
Impact of Antibiotic Stewardship Program Interventions on Multi-drug
Resistant Organism Resistance Rates and Hospital Costs
Nishant Prasad MD; Nathan Warren RPA-C; Anna Kula RPA-C; Noriel Mariano; Carl Urban PhD; Deborah Figueroa
BS PharmD; Sorana Segal-Maurer MD
Introduction
Data support that antimicrobial stewardship programs (ASP) reduce unnecessary antimicrobial
use, decrease hospital expenditure and length of stay, and improve patient outcomes. Reduction
in the incidence of drug resistant bacteria has been proposed. New York Hospital Queens
implemented a limited scope ASP in 2009 that matured to hospital wide in 2011. We evaluated
the ongoing impact of ASP interventions at our 535-bed community hospital over a three-year
period on the incidence of multi-drug resistant organisms, Clostridium difficile associated
diarrhea (CDAD) incidence, antibiotic expenditure, and overall estimated cost savings.
Quantitative/Qualitative Measures
We measured the hospital wide expenditure on select antibiotics for 2012 and compared that to
expenditures from 2013. We enumerated the number and types of interventions performed by
the ASP, and the estimated cost savings of those interventions. We also counted the number of
adverse drug reactions recorded by the ASP. The incidence of select multi-drug resistant bacteria
(specifically Acinetobacter baumannii, Klebsiella pneumoniae, and methicillin-resistant
Staphylococcus aureus) for 2011 was compared to the incidence in 2013. The 2011 hospital wide
incidence of Clostridium difficile associated diarrhea was also compared to the 2013 incidence.
Methodologies
The ASP comprises a clinical pharmacist, physician assistant, Infectious Diseases fellow and
attending. The team evaluated the use of all restricted and select non-restricted antibiotics at the
hospital on all applicable admitted patients several times a week to daily. The team initiated
phone calls to care providers to recommend specific interventions designed to decrease
unnecessary antibiotic use, correct inappropriate antibiotic dosing, change antibiotic therapy
based on clinical scenario and reduce hospital expenditure all while maintaining maximal patient
care and safety. The care providers were at liberty to accept or reject the recommendation made
by the ASP. After the ASP had been in place for 3 years the effect on the above measures was
studied.
System Quality Review
98
NewYork-Presbyterian Healthcare System Quality Symposium 2014
Quality 2020: A Vision of the Future
Improvement Results
In 2013 the ASP saved an estimated $606,109 over 5147 interventions and reported 104 adverse
drug reactions (Table 1). The most significant cost savings occurred in daptomycin, cefepime
2gm, and meropenem expenditures (Graph 1). Increase in rifaximin expenditure was in
significant part due to non-infectious causes (i.e. hepatic encephalopathy). Increase in IV
rifampin expenditure was secondary to significant increase in the price of drug; overall use of IV
rifampin decreased by 22% (estimated cost avoidance of $30,272). Meropenem administration
was changed from 30 minutes to 3 hour extended infusion in 2013, decreasing total amount of
drug used. Over 60% of ASP interventions were renal adjustments, de-escalation, or
discontinuation of antibiotics (Chart 1). The incidence of MDRO and CDAD decreased (Table
2)
Sustainability Strategies
The ASP has shown financial sustainability with the above data, and we hope will continue to
show improvement in the rates of multi-drug resistant organisms and hospital acquired
infections.
Lessons Learned
1. The presence of an ASP was associated with decrease on antibiotic expenditure, notable
estimated cost savings, and decreases in the incidence of multi-drug resistant organisms and
hospital acquired infections.
2. ASP should continue to monitor the use of antibiotics at our hospital to improve patient safety
and quality of care.
Conclusion
The presence of a hospital wide ASP was associated with a decrease in incidence of multi-drug
resistant organisms and C. difficile associated diarrhea. A mature ASP operating hospital wide
was associated with significant decrease in expenditures on antibiotics. ASP interventions led to
significant estimated cost savings over a one year period. ASP may lead to increased adverse drug
reaction reporting, a joint commission mandate. In spite of numerous available best practice
guidelines ASPs most common interventions were renal dose adjustments and antibiotic deescalation or discontinuation, supporting the need for ongoing ASP.
System Quality Review
99
NewYork-Presbyterian Healthcare System Quality Symposium 2014
Quality 2020: A Vision of the Future
System Quality Review
100
NewYork-Presbyterian Healthcare System Quality Symposium 2014
Quality 2020: A Vision of the Future
Table 1: Interventions, Estimated Cost Savings and Adverse Drug Reactions for 2013
Physician Assistant
Interventions
Pharmacist
3311
1836
Estimated Cost Savings
$355,370
$250,739
Adverse Drug Reactions
Reported
41
63
Table 2: Select Multi-drug Resistant Organism and C difficile Associated Diarrhea Incidence in Percent (%)
Organism
2011
K. pneumoniae
17.7
11
40.7
A. baumannii
43.3
39.5
9
MRSA
56.8
41.6
26.8
CDAD
16.5
11.4
30.9
System Quality Review
2013 Reduction (%)
101
NewYork-Presbyterian Healthcare System Quality Symposium 2014
Quality 2020: A Vision of the Future
New York Hospital Queens
Analysis of Low Intensity ICU Staffing Model at NYHQ
Ronni Levy MD, James A. Gasperino MD, PhD, MPH, Michael S. Radeos MD, MPH, Zuhair Ali MD, Sun Mon Aye
MD, Nidhi Garg MD
Introduction
Approximately, 500,000 patients die in the Intensive Care Unit (ICU) each year. Evidence
suggests that staffing the ICU with Intensivist’s reduces mortality and decreases length of stay.
The demand though for Intensivists exceeds the supply. Consequently, adopting such staffing
practices has been difficult. Critically ill patients are predominately cared for by physicians who
lack specific training in critical care medicine. This model, the low intensity ICU staffing model,
has been associated with inferior outcomes for the critically ill patient.
The NY Hospital Queens Medical ICU sees approximately 1400 patients a year. It follows the
low intensity ICU staffing model. All patients are managed by house-staff and the admitting
physician, regardless of their specialty, assumes all decision-making responsibilities. It is their
option to utilize or not utilize critical care providers.
We aim to analyze the practices of low intensity ICU staffing model at NYHQ.
Methodologies
In November 2014, the medical ICU at NYQH will be transitioning to a high intensity ICU
physician staffing structure model compliant with the standard proposed by the Leapfrog Group
for Patient Safety. During the day shift, all ICU consults will require an Intensivist consult and all
ICU patients will be managed by the Intensivist with mandatory consult and mandatory
management. After 6pm and up until 7am, pulmonary-critical care fellows and house-staff will
assume direct care of critically ill patients. A critical care Attending, however, will always be
available by phone or in person if needed.
Improvement Results
For the month of January and February 2014, all ICU consults were analyzed. Total 209 MICU
consults were called by ED during this period with median age of 70 yrs (IQR 55-83), 108
(51.7%) males, 93 (44.5%) whites, 58 (27.7% ) asians, 27 (12.9%) African Americans and 31
(14%) others. Patients had median temp of 98.1 F (IQR 97.6-98.9), systolic blood pressure of 128
(IQR 101-153), diastolic blood pressure of 87 (IQR 71-99), heart rate of 97 (IQR 80-116),
respiratory rate of 20 (IQR 16-24), SPO2 of 98 (IQR 95-100), shock index 0.75 (IQR 0.61-1.01).
Total 32 (15.31%) were DNR and 20 (9.57%) DNI and 41 (19.6%) were from Nursing Home.
100% of the patients were seen initially seen by house-staff. Of these patients, 93 (44.5%) were
admitted to the ICU , 197 (94.26%) had critical care consult note written,195 notes were written
System Quality Review
102
NewYork-Presbyterian Healthcare System Quality Symposium 2014
Quality 2020: A Vision of the Future
by house staff of which 111 (76.5%) were cosigned by an attending and 2 were written by
attending itself. Critical care consult note was written for all patients who went to MICU but was
not written for 12 patients who were downgraded. Median hospital LOS was 6.57 days (IQR
3.78-12.9) for patients who went to MICU and 5.87 days (IQR 3.1-10.23) for patients who went
non ICU hospital bed. Inpatient mortality was 23 (24.7%) for MICU patients and 19 (16.4%) for
non MICU patients.
Sustainability Strategies
In November 2014 the MICU at NYHQ will change to a high-intensity staffing model. This
study will analyze the influence of the high-intensity staffing model on ICU and hospital
morbidity and mortality.
In our secondary analysis, we will examine ICU triaging in the high-intensity model. During off
hours (6pm to 7am) house-staff (a second year medical resident and a pulmonary-critical care
fellow) are responsible for critical care consults. They may or may not consult the Attending
Physician regarding these consults. House-staff though determine whether patients gain or do not
gain admission into the ICU. NYHQ MICU functions at 150% capacity. With a limited number
of beds not all patients receive ICU care. After implementation of the high intensity staffing
model, we predict more appropriate admissions and the severity of illness in the ICU will
increase.
Lessons Learned
1.Previous implementation of Low Intensity Staffing Model may have lead to increased morbidity
and mortality in ICU and hospital.
2. House-staff may miss ICU admissions during off-hours when an Intensivist is not on site.
3. Conversely, patients may be admitted into ICU who do not require admission and deny those
in need of an ICU bed.
Conclusion
After implementation of the high–intensity-staffing model, we predict morbidity and mortality
will decrease in the ICU and the hospital. Length of stay should be decreased in the ICU and
hospital. Furthermore, in the ICU the severity of illness based on APACHE 4 scores will
increase.
System Quality Review
103
NewYork-Presbyterian Healthcare System Quality Symposium 2014
Quality 2020: A Vision of the Future
New York Hospital Queens
Intervention and Medical Documentation of Hospital Acquired Hypoglycemic
Episodes – A Retrospective Chart Review Study
Mark Vinelli, DO; Jing Guo, MD; Tagenarayan Niwaz, DO; Nejat Zeyneloglu, MD; Roxana Lazarescu, MD
Introduction
Hypoglycemia in the hospital can be detrimental to a patient’s health and can often be avoided. It
frequently prolongs hospital stay and is associated with an increased mortality. Healthcare
providers need to be more rigorous in preventing hospital acquired hypoglycemic episodes. We
would like to find out if healthcare providers are identifying hypoglycemic episodes with their
documentation; if the episodes are being treated appropriately; what factors may contribute to
hypoglycemic episodes; and what adjustments healthcare providers are implementing to prevent
future episodes. Our goal is to raise awareness, and identify ways healthcare providers can
decrease the frequency of hypoglycemic episodes to improve the safety and quality of patient
care.
Quantitative/Qualitative Measures
This is a retrospective, single-center study, looking at 76 episodes of hypoglycemia during a 30
day period, involving 44 patients hospital wide, at New York Hospital Queens. An electronic
medical record chart review was conducted and these episodes were examined.
Methodologies
Hypoglycemia was defined as a blood glucose less than 50 mg/dL. The intervention after a
hypoglycemic episode was noted. The interventions included administration of Dextrose 50
intravenous push (IVP), glucagon IVP, and/or juice. In addition, we reviewed whether or not
there was documentation by nurses and/or physicians. The physician notes included daily
progress notes and free text notes, and the nursing notes included daily notes and critical value
acknowledgments. The means of feeding such as oral intake, tube feeding and withholding feeds
(NPO) was also examined. The ordered insulin regimen, such as basal bolus before meals (TID),
basal bolus every six hours (q6hrs), bolus insulin only, basal insulin only or other was analyzed.
Adjustments to insulin and/or oral hypoglycemic agents to reduce future episodes were also
reviewed.
System Quality Review
104
NewYork-Presbyterian Healthcare System Quality Symposium 2014
Quality 2020: A Vision of the Future
Improvement Results
Data analysis revealed that after the hypoglycemic episodes, 59% of the episodes had an
intervention, and 41% had no intervention (Figure 1). The interventions performed are as
follows: 45% given Dextrose 50 IVP, 13% given juice, and 4% given glucagon IVP (Figure 2).
58% had some form of documentation and 42% had no documentation (Figure 3). 45% of the
hypoglycemic episodes had nursing documentation, 28% had physician documentation, and14%
had both (Figure 4). 29 % were NPO, 9% had tube feeding, 62% had oral intake (Figure 5).
Insulin regimens were as follows: 76% had basal bolus TID, 8% basal bolus q6hrs, 8% bolus
only, 1% basal only, and 7% other (Figure 6). After 42% of the hypoglycemic episodes there was
an adjustment to the insulin regimen and/or oral hypoglycemic agents and in the remaining 58%
of the episodes there were no adjustments (Figure 7).
Sustainability Strategies
This data was presented at the New York Hospital Queens’ Annual Research Day for Residents
and Fellows on May 16, 2014 to raise awareness of hospital acquired hypoglycemic episodes,
decrease the incidence, and improve treatment and documentation. Since then our team has been
working with the New York Hospital Queens (NYHQ) Diabetes Working Group, which is an
interdisciplinary team that meets monthly to improve the safety and quality of patient care.
Lessons Learned
1. Providers are failing to treat and document hypoglycemic episodes.
2. Providers are failing to adjust insulin and/or oral hypoglycemic agent regimens after
hypoglycemic episodes.
3. NPO is a significant contributing factor that can lead to hypoglycemic episodes.
Conclusion
Overall, we identified many opportunities for improvement. Over one third of hypoglycemic
episodes did not have interventions taken, and nearly half of the episodes had no documentation.
This compromises awareness of these episodes, and can cause future episodes and patient harm.
A significant proportion of episodes occurred in patient's that were NPO, which should have
been anticipated and prevented. There was a lack of adjustments to insulin and/or oral
hypoglycemic agent regimens, which can lead to recurrence of hypoglycemia. A follow up study
is currently being conducted to improve documentation and see if it correlates with the incidence
of hypoglycemia. In addition, we are currently addressing these opportunities for improvement
at our monthly NYHQ Diabetes Working Group and are developing multiple quality
improvement projects.
System Quality Review
105
NewYork-Presbyterian Healthcare System Quality Symposium 2014
Quality 2020: A Vision of the Future
Figure 1- Interventions (Yes or No)
Intervention
No Intervention
Figure 2- Intervention Type
45%
50%
40%
D50
30%
Glucagon
13%
20%
Juice
4%
10%
0%
D50
Glucagon
Juice
Figure 3- Documentation
42%
58%
Documentation
No Documentation
System Quality Review
106
NewYork-Presbyterian Healthcare System Quality Symposium 2014
Quality 2020: A Vision of the Future
Figure 4- Documentation Type
28%
Physicans
45%
Nurses
Both
14%
0%
10%
20%
30%
40%
50%
Figure 5- Diet
62%
29%
NPO
Tube Feeding
Oral
9%
System Quality Review
107
NewYork-Presbyterian Healthcare System Quality Symposium 2014
Quality 2020: A Vision of the Future
Figure 6- Insulin Regimen
8%
1%
8%
7%
Basal Bolus TID
Basal Bolus Q6hr
Bolus Only
Basal Only
76%
Mixed Insulin
Other
Figure 7- Adjustment
58%
42%
Yes
No
System Quality Review
108
NewYork-Presbyterian Healthcare System Quality Symposium 2014
Quality 2020: A Vision of the Future
New York Hospital Queens
Impact of Palliative Care Program on Utilization of Tracheostomies
Cynthia X Pan MD; Cristina Gutierrez MD; Min Min Maw MD; Amanda Kansler MPH, CCRP; Liam Gross MD;
Romana Kanta MD; Subroto Paul MD
Introduction
Problem Statement:
Tracheostomies are typically provided to wean patients off the ventilator. However in many
circumstances tracheostomies are placed in patients who are at the end of their life with little
hope of meaningful recovery. Palliative care programs have been shown to decrease utilization of
such aggressive medical interventions in patients who are at the end of life.
Project Aim:
To determine the impact of establishing a palliative care program on tracheostomy utilization in a
community hospital.
Quantitative/Qualitative Measures
To compare demographics, comorbidities, in-hospital mortality, length of stay, and discharge
status of patients undergoing tracheostomy before and after a palliative care consult service was
formed.
Methodologies
Retrospective, natural experiment analysis of adult patients undergoing elective tracheostomy
from September 2008 to 2012, 2 years before and 2 years after September 10, 2010, when a
palliative care program was created. Patients undergoing tracheostomy for trauma were excluded.
Improvement Results
During the four year period, 790 patients undergoing tracheostomy were identified (n=406,
n=384 before and after 9/10/2010, respectively). The number of hospital admissions slightly
increased during these two time periods (58,926; 60,662, respectively). There were no statistical
differences in age (73 v. 72, p=0.83), gender (n=218 (54%) v. n=217 (57%) male, p=0.43), or
race (n=187 (52%) v. n=150 (50%) Caucasian, p=0.07) in the two time periods. However those
patients who underwent tracheostomy after 9/10/2010 had less comorbid disease (Charleson
Comorbidity Index: 2 v. 3, p=0.03), lower inpatient mortality (n=107 (28%) v. n=148 (37%,
p=0.01), greater discharge to home or rehab (n=262 (68%) v. n=249 (62%), p=0.01), and lower
rates of palliative extubation (n=61 (16%) v. n=113 (28%), p<0.001).
System Quality Review
109
NewYork-Presbyterian Healthcare System Quality Symposium 2014
Quality 2020: A Vision of the Future
Sustainability Strategies
The hospital continues to support the Palliative Care program, including its measured growth to
meet the high demand. The hospital is hiring a nurse practitioner for the Palliative Care program,
and dedicating an existing social worker to help meet the psychosocial needs of palliative care
patients and families. The Palliative Care program has worked closely with grants management to
obtain grant funding, and will continue to do so.
Lessons Learned
1. Palliative Care programs can help improve patient selection for tracheostomy.
2. Palliative Care programs effectively address end of life issues and prevent inappropriate use of
resources, and improved patient outcomes.
3. It is critical for health care disciplines and specialties to work collaboratively instead of in silos.
In this case, this project was an effective collaboration among critical care, cardiothoracic surgery,
the Lang Research Center, and palliative care programs.
Conclusion
The institution of a palliative care program appears to have led to improved patient selection for
tracheostomy with lower rates of inpatient mortality, improved rates of home discharge, and
lower rates of palliative extubation.
System Quality Review
110
NewYork-Presbyterian Healthcare System Quality Symposium 2014
Quality 2020: A Vision of the Future
Age, Median
Gender, Male (%)
Race
Cauc
Hispanic
African American
Asian/others
Prior to 9/10/2010
(n=406)
73, IQR (59 – 82)
218 (54%)
n=360
187 (52%)
31 (9%)
37 (10%)
105 (29%)
Home
Nursing Home
267 (66%)
138 (34%)
Race unknown
Came From (Home Vs. Nursing Home )
Other source
Comorbidities
Most Frequent Dx1: DM
Most Frequent Dx2:CHF
Most Frequent Dx3: CKD
Most Frequent Dx4: COPD
Most Frequent Dx5: ESRD
Charleston Comorbidity Index
Primary Dx at Admission
Most Frequent Dx
Dx1: Septicemia
Dx2: Acute respiratory failure
Dx3: Intracerebral Hemorrhage
Dx4: Pneumonia
Dx5: CHF
On Chemotherapy (Y/N)
On Pressors (Y/N)
On Renal Replacement Therapy
46
1
After 9/10/2010,
(n=384)
72, IQR (60 – 82)
217 (57%)
n=303
150 (50%)
22 (7%)
52 (17%)
79 (26%)
240 (63%)
143 (37%)
‘P’ value
Total (n=790)
p=0.827
p=0.426
73, IQR(60 – 82)
435 (55%)
n=663
337 (51%)
53 (8%)
89 (13%)
184 (28%)
p=0.073
81
p=0.339
1
507 (64%)
281 (36%)
127
2
110 (27%)
100 (25%)
48 (12%)
44 (11%)
20 (5%)
3, IQR (1 – 5)
47 (12%)
42 (11%)
21 (5%)
16 (4%)
12 (3%)
2, IQR (1 – 4)
p<0.001
p<0.001
p=0.002
p<0.001
p=0.199
p=0.025
157 (20%)
142 (18%)
69 (9%)
60 (8%)
32 (4%)
3, IQR(1 – 5)
64 (16%)
33 (8%)
18 (4%)
13 (3%)
15 (4%)
23(6%)
197 (49%)
% Y (n=38) i.e. either
CVVH or Hemodialysis
25/38 (66%)
13/38 (34%)
0 (0%)
11, IQR(6 – 18)
73 (19%)
16 (4%)
11 (3%)
20 (5%)
5 (1%)
30 (8%)
187 (49%)
% Y (n=48) i.e. either
CVVH or Hemodialysis
32/48, (67%)
16/48, (33%)
76 (20%)
10, IQR(7 --- 16)
p=0.228
p=0.021
p=0.241
p=0.159
p=0.032
p=0.228
p=0.961
p<0.001
p=0.877
137 (17%)
49 (6%)
29 (4%)
33 (4%)
20 (3%)
53 (7%)
384 (49%)
% Y (n=86) i.e. either
CVVH or Hemodialysis
57/86, (66%)
29/86, (34%)
76 (10%)
11, IQR(7 – 17)
Vent Support Removal/Palliative Extubation
113 (28%)
61 (16%)
p<0.001
174 (22%)
Inpatient Mortality
Place of Discharge
Rehab
Home/Private Residence
Hospice
148 (37%)
107 (28%)
p=0.009
255 (32%)
203 (50%)
46 (12%)
9 (2%)
236 (60%)
26 (8%)
15 (4%)
p=0.001
439 (56%)
72 (9%)
24 (3%)
Expired
Days With Tracheostomy (median)
LOS (median)
148 (36%)
17, IQR(7 – 29)
31, IQR(21 --- 45)
107 (28%)
15, IQR (9 – 22)
28, IQR (19 – 42)
CVVH
Hemodialysis
Palliative Care Consult (Y/N)
Days after Admission Trach was Placed
(median)
System Quality Review
p=0.931
p=0.574
p=0.127
255 (32%)
16, IQR (8 – 26)
29, IQR (20 – 44)
111
NewYork-Presbyterian Healthcare System Quality Symposium 2014
Quality 2020: A Vision of the Future
New York Methodist Hosital
Standardization of Diabetic Foot Infection Admissions: A Review of Current
Guidelines with Generalized Recs.
Kirsti A. Diehl, DPM; Eric C. Storts, DPM; Kirsten L. Barisonek, DPM; Ronald L. Soave, DPM
Introduction
Foot infections are a common reason for hospitalization and a cause of complications in patients
with diabetes. Currently in the United States, approximately 26 million people have diabetes and
15% of them will go on to develop a diabetic foot infection1. Diabetics admitted to the hospital
with lower extremity infections were hospitalized for longer than those without foot ulcers2. The
aim of this effort was to establish a standardization protocol for admissions involving lower
extremity diabetic foot ulcers in efforts to improve patient care and decrease total length of stay.
The assessment and treatment criteria of diabetic foot infections described in methods were
established after a literature review of diabetic foot infection treatment recommendations as well
as observed positive outcomes at NYMH.
Improvement Results
Upon admission, the patient will be evaluated as a whole, considering comorbid conditions and
current systemic state. If there is a concern for sepsis, the SICU team will evaluate the patient.
Admission labs (CBC, CMP plus, ESR, CRP, HgA1C), foot x-ray(s), EKG and chest x-ray (as
indicated), severity of infection using Infectious Diseases Society of America (IDSA) guidelines,
and grade/depth assessment using the Wagner Classification will be reviewed. If the patient is
taken to the OR for debridement or I&D, a tissue culture will be obtained.
Based on assessment of the infection and patient, the treatment plan as commanded by the
attending, involvement of advanced imaging, long term IV antibiotics, and/or surgical
intervention will be determined. Selected IDSA moderate infections with peripheral arterial
disease (PAD) or lack of home care support will be admitted for IV antibiotics or those who
have failed out-patient therapy Recorded data will be required. If the infection is moderate to
severe will give STAT doses of IV Vancomycin 1 gram and Zosyn 3.375g and then continue
them based on Creatinine Clearance. MRSA coverage will be continued until proven that MRSA
is not the cause of infection. Deep tissue cultures have proven more accurate in identifying
infectious organisms compared to wound swabs3.
System Quality Review
112
NewYork-Presbyterian Healthcare System Quality Symposium 2014
Quality 2020: A Vision of the Future
Conclusion
After each diabetic foot infections admission to podiatric surgical service, the aforementioned
data will be assessed. An annual review of the diabetic foot infection admissions will be
performed to assess the average length of stay. Length of stays longer than 7 days will be
reviewed in detail to determine why the patient’s discharge was delayed and what could have been
done to reduce the length of stay.
System Quality Review
113
NewYork-Presbyterian Healthcare System Quality Symposium 2014
Quality 2020: A Vision of the Future
New York Methodist Hospital
Improving Inpatient Satisfaction
Anthony Mungo; Michael Ficorelli; Alfred Usuriello; Steven Garner, M.D
Introduction
Rationale for Choice of Performance:
Due to the high demand of medical imaging required for inpatients and lack of knowledge of the
procedure our patients are apprehensive when arriving in the department. Additionally, inpatients
are not scheduled for procedures which leads to uncertainty. A means to develop a tentative time
frame is very important for both the inpatient and department of radiology.
Goal or Anticipated Outcome:
To create a more informed, less apprehensive patient.
1. Create patient information literature which will be distributed prior to their exam. This
literature is modality specific to give a patient the overall understanding of an MRI, CT, XR, US.
2. Create a daily managerial rounds team to visit hospitalized patients that are scheduled for a
radiological examination. This team would distribute literature and answer questions the patient
may have that pertains to their radiologic examination. This would allow the patient to
understand his procedure and put him at ease.
Quantitative/Qualitative Measures
107 Inpatients completed the survey during August, 2014. Below with the following averaged
results, based on a scale of 1-5, with 5 being excellent.
Did you find the Radiology visit informative= 5.0
Did the representative answer ALL of your questions= 5.0
Did the representative give you a time frame for your test to be performed= 5.0
How well did the representative explain your examination= 5.0
How would you rate your overall radiology experience= 5.0
Overall experience= 5.0
Methodologies
Inpatient surveys had been created to follow up with patients that were initially visited during
managerial rounds. (See above questions)
Feedback from staff was also utilized to assess efficiency.
System Quality Review
114
NewYork-Presbyterian Healthcare System Quality Symposium 2014
Quality 2020: A Vision of the Future
Improvement Results
Based on staff feedback and rounds surveys, there has been a dramatic improvement in the
attitude of inpatient undergoing radiological exams. There is decreased apprehension by both the
patient and their families. Studies have shown that a nervous patient has more adverse reactions
associated with their exam (eg. Difficulty positioning, anaphylaxis, etc.)
Sustainability Strategies
1. Continue to perform daily radiology managerial rounds.
2. Continue to perform follow up rounds to maintain quality survey results.
3. In-service new radiology staff members on the importance of patient feedback and
communication.
Lessons Learned
1. Communication: Our patients are happy to see and hear from us and openly ask questions
that pertain to their procedure. Patients demeanor can be modified with a relatively simple
methodology.
2. Procedural Knowledge: Patients are often unaware of the examination they are about to
undergo.
3. Inpatient Scheduling: Developing a system to schedule inpatients for radiologic examinations
would be benefical in the future. At the current time, this system does not exist, that is why direct
communication during patient rounds is imperative.
Conclusion
Through very simple measures, we've noticed that patients are much more comfortable when
arriving in the department for an imaging procedure. A LITTLE BIT OF COMMUNCATION,
GOES A VERY LONG WAY!
System Quality Review
115
NewYork-Presbyterian Healthcare System Quality Symposium 2014
Quality 2020: A Vision of the Future
New York Methodist Hospital
NICU Radiation Reduction "Sucess Story"
Steven Garner, MD; Claudia Lapidus, MD; Anthony Mungo; Michael Ficorelli; Alfred Usuriello
Introduction
Problem Statement:
Neonatal patients are among the most susceptible groups to the harmful effects of radiation. As
many of the NICU patients are on life support, chest and abdominal x-rays are part of the daily
regimen. Shielding and collimation are techniques that can significantly reduce radiation.
Implementation of these techniques require the efforts of the technologists as well collaboration
of NICU Staff. At the time the project was initiated there was great concern in New York City
for compliance with shielding and collimation requirements. At New York Methodist Hospital
we have achieved virtually 100% compliance.
AIM:
The aim is to institute processes at New York Methodist to achieve high compliance with
shielding and collimation guidelines.
Goal:
To have 100% compliance with shielding and collimation. This model can serve as a blueprint for
other hospitals to guide dose reduction in NICU patients.
Quantitative/Qualitative Measures
We have attached an analysis of shielding and collimation in the NICU for the past 3 years. (See
Attached Data)
Methodologies
1. Chief Technologist monitors all NICU x-rays performed for shielding and collimation
2. Communication with constant feedback
3. Interdisciplinary meetings to educate residents, fellows, and medical staff about the harmful
effects of radiation to infants. This affords us the opportunity to create a culture of radiation
safety for the institution
4. Reward desired behavior. Established CEO (Compassion, Empathy, Ownership) award
5. Compliance with shielding and collimation is a quality assurance indicator to be presented at
the radiation safety committee meeting
6. Placed mobile and stationary shields in the NICU to insure proper techniques are used
System Quality Review
116
NewYork-Presbyterian Healthcare System Quality Symposium 2014
Quality 2020: A Vision of the Future
7. The Technologist insures that the infant is properly shielded, and the image is collimated
Improvement Results
There was immediate improvement in compliance from all staff members involved with the
patient care. Utilizing a team approach, we have achieved 100% compliance. (See Attached Data).
Sustainability Strategies
To achieve sustainability, the following methods are employed;
1. Daily monitoring of NICU radiographs.
2. Continuous emphasis on the importance of shielding, collimation and radiation safety
3. We have built a multi-disciplinary framework within our hospital of radiation safety
Lessons Learned
1. Continuous radiation safety education which is easily understandable by all involved is
necessary
2. A multi-disciplinary framework is required to sustain success
3. An on-gong QA project is critical in order to maintain compliance
Conclusion
It is possible to attain virtually 100% compliance in shielding and collimation of patients in the
NICU. The methodology utilized at NYMH, may be used by other hospitals to gain the same
results. It is critical to achieve multi-departmental buy-in. Continuing Education is required to
maintain sustainability. As a result of implementing our radiation safety model , NICU patients
receive decreased radiation during routine radiographic exams and are less likely to have harmful
effects of radiation in their lifetime.
System Quality Review
117
NewYork-Presbyterian Healthcare System Quality Symposium 2014
Quality 2020: A Vision of the Future
NICU Shielding & Collimation Compliance
2011
100
50
2011
0
Jan
Feb Mar Apr May Jun
NICU Shielding & Collimation
100
80
2011
60
2012
40
2013
20
2014
System Quality Review
Dec
Nov
Oct
Sep
Aug
Jul
Jun
May
Apr
Mar
Feb
Jan
0
118
NewYork-Presbyterian Healthcare System Quality Symposium 2014
Quality 2020: A Vision of the Future
MONTH /YEAR
NUMBER OF IMAGES
PROPERLY
COLLIMATED / SHIELDED
March 2011
64
TOTAL NUMBER OF IMAGES IN COMPLIANCE RESULTS
87
73%
April 2011
72
77
93%
May 2011
87
93
93%
June 2011
82
83
98%
July 2011
110
111
99%
100%
August 2011
132
132
September 2011
109
112
97%
October 2011
113
113
100%
November 2011
87
87
100%
December 2011
100
101
99%
January 2012
113
113
100%
February 2012
140
140
100%
March 2012
143
143
100%
April 2012
116
117
100%
100%
May 2012
119
119
June 2012
127
128
99%
July 2012
107
107
100%
August 2012
145
146
99%
September 2012
156
158
98%
October 2012
126
126
100%
November 2012
117
117
100%
December 2012
107
108
99%
January 2013
101
101
100%
February 2013
113
113
100%
March 2013
124
124
100%
April 2013
168
169
99%
May 2013
116
116
100%
June 2013
96
96
100%
July 2013
162
162
100%
August 2013
171
171
100%
September 2013
157
157
100%
October 2013
797
79
100%
MONTH /YEAR
NUMBER OF IMAGES
PROPERLY
COLLIMATED / SHIELDED
TOTAL NUMBER OF IMAGES IN COMPLIANCE RESULTS
November 2013
December 2013
152
160
152
160
100%
100%
January 2014
February 2014
126
109
126
109
100%
100%
March 2014
April 2014
May 2014
June2014
July 2014
August 2014
75
116
123
134
161
124
75
116
123
134
161
124
100%
100%
100%
100%
100%
100%
System Quality Review
119
NewYork-Presbyterian Healthcare System Quality Symposium 2014
Quality 2020: A Vision of the Future
New York Methodist Hospital
Optimizing the Accuracy and Utility of Surgical Outcomes Data Through the
Integrated Use of COQPIT and the American College of Surgeons Surgeon
Specific Registry
James C Rucinski MD, FACS; Diren Patel MD; Amani Jambhekar MD; Donald A Risucci PhD; Anthony J Tortolani
MD, FACS
Introduction
The New York Presbyterian Health System employs the Comprehensive Quality and
Performance Improvement Tool (COQPIT) to assess risk-adjusted patient outcomes. Risk
adjustment is performed retrospectively based on statistical regression equations that estimate the
expected hospital length of stay (LOS), and probabilities of complications and death for each
patient. The equations are derived from analysis of historic demographic data and diagnosis and
procedure codes recorded on the hospital discharge "face sheet". While this approach provides
estimates of sufficient accuracy for retrospective performance review, there are other validated
methods for risk adjustment recommended by professional organizations such as the American
College of Surgeons (ACS) National Surgical Quality Improvement Program (NSQIP), which
provides a risk calculator that individual surgeons can use prospectively to assess individual
patient risk based upon preoperative clinical data. Surgeons, like many other physicians are
increasingly being encouraged to log their own cases into systems such as the ACS Surgeon
Specific Registry (SSR) and other Physician Quality Reporting System (PQRS)-qualified registries,
where they can easily track cases and outcomes and electronically submit data required for
recertification purposes.
Issue/Problem
Regression models for risk adjustment often yield different risk estimates if there are differences
in the variables used in the model. Since COQPIT and NSQIP models use different variables it is
conceivable that there may be differences in risk estimates. NSQIP's exclusive reliance on
preoperative data excludes from consideration the role of postoperative factors that could have
an important influence particularly on risk estimates for death and excessive LOS. In contrast,
COQPIT's reliance on coded data from discharge records may result in models and risk estimates
that can be difficult to translate into specific clinical risk factors and outcomes that individual
clinicians can attempt to improve and manage more effectively. Other factors that may affect the
congruity and usefulness of risk estimates include possible differences in the accuracy of the raw
data as coded and entered by professional coders (i.e. COQPIT) and by individual surgeons or
other clinicians/staff (i.e. NSQIP).
The Department of Surgery at NY Methodist Hospital has utilized available COQPIT surgeonspecific reports to assess risk adjusted patient outcomes associated with individual surgeons and
System Quality Review
120
NewYork-Presbyterian Healthcare System Quality Symposium 2014
Quality 2020: A Vision of the Future
surgical specialties/divisions. We have also begun to utilize the NSQIP calculator to estimate
clinical risks among patients presented at the Morbidity & Mortality (M&M) conference and
several surgeons in the department have been logging patient-level data into either the American
College of Surgeons Surgeon Specific Registry (SSR) or other specialty specific registries that can
provide risk estimates for individual patients (e.g. Society of Thoracic Surgeons registry for
cardiovascular and thoracic surgery patients). When we have examined patient-level COQPIT
data, we have discovered discrepancies in the attribution of surgeons to patients (e.g. patients
whose primary surgery was not performed by a surgeon listed on the face sheet) and the
identification of complications (e.g. pre-existing conditions coded as surgical complications or
surgical complications not captured by COQPIT) when compared with records maintained by
individual surgeons and/or surgical divisions.
Project Aim/Goal: to integrate and cross validate COQPIT patient level data and SSR data
maintained by a single surgeon for all patients on whom he operated during the 4-year period
between July 2009 and June 2013.
Quantitative/Qualitative Measures
Statistical methods (i.e.. Kappa and Chi-square statistics) were used to identify and evaluate
discrepancies in data attribution and coding between COQPIT and SSR patient level data and to
review SSR data in conjunction with COQPIT data to identify clinical factors that may contribute
to excess LOS and/or unexpected complications or deaths (according to the COQPIT model).
Methodologies
All SSR data for patients discharged during the study period were downloaded from the ACS
website in the form of an Excel spreadsheet. Likewise, all COQPIT patient-level data associated
with the study surgeon were downloaded and exported into an Excel spreadsheet. Table 1 lists
the patient level data collected by the SSR and COQPIT. All data were imported into the
Statistical Package for the Social Sciences (Version 21) and merged on the basis of medical record
number and discharge date.
Data analyses focused on identification of discrepancies between the two databases and
examination of variations in SSR data that may be associated with excess LOS and unexpected
complications and death as defined by the COQPIT risk adjustment models. Kappa statistics
were used to evaluate agreement between databases in identification of complications. Chi square
statistics were used to compare patients with LOS less than or equal to expectations to patients
with LOS greater than expected based on COQPIT regression models.
Improvement Results
Figure 1 provides a breakdown of the data acquired from both sources and how patients were
matched across databases. Querying the COQPIT database for cases listing the study surgeon
identified 528 discharges of 476 patients. Of these, the surgeon had logged 240 matching
discharges in 222 patients.
COQPIT identified a total of 8 patients that died prior to discharge; 4 of these died within 30
days and had been logged in the SSR as deaths within 30 days.
System Quality Review
121
NewYork-Presbyterian Healthcare System Quality Symposium 2014
Quality 2020: A Vision of the Future
Complications identified in COQPIT were analyzed in relation to post-operative occurrences
recorded in the SSR. There was a statistically significant level of agreement (kappa = 0.40; p
<0.001) between the two data sources with respect to whether or not patients experienced
complications or post-operative occurrences. However, according to COQPIT data,
complications occurred in 23 patients/discharges; of these 11 were also indicated as experiencing
a post-operative occurrence in the SSR while the remaining 12 were listed as having no postoperative occurrences. The SSR identified an additional 14 cases with post-operative occurrences
that were not listed as complications in COQPIT. Table 2 provides a list of complications and/or
occurrences that were identified in each database and those that were identified in both.
The difference between actual and expected LOS was calculate for each patient. LOS was equal
to, or below, the COQPIT expected LOS in 136 (57%) cases. Chi-square statistics were used to
compare these patients/discharges to those with excess LOS with respect to the following
variables from the SSR: patient gender, resident participation in operation (PGY 1-3 vs PGY 46), presence/absence of co-morbid conditions, ASA Class, emergent/non-emergent operation,
wound classification and presence/absence of post-operative occurrence(s). As shown in Table 3,
patients/discharges with excess LOS were significantly more likely than those with LOS at or
below the COQPIT expected number of days to be emergent operations and women patients.
Sustainability Strategies
Procedural and analytic differences employed by various systems for quality data management
and performance improvement point to the need to continually examine and cross validate data
from multiple sources in efforts to gather the most meaningful and actionable data.
Lessons Learned
1. When comparing patient level data as logged by an individual surgeon to patient level data
available in COQPIT (and other data management/risk adjustment systems that rely on diagnosis
and procedure codes from administrative discharge records), important discrepancies are likely to
be observed.
2. Integrating and reviewing data from multiple sources is essential to gather the most meaningful
and actionable data for quality improvement.
3. Addition of clinical data and information concerning health care delivery processes can
improve the accuracy and utility of risk-adjusted outcome assessments.
System Quality Review
122
NewYork-Presbyterian Healthcare System Quality Symposium 2014
Quality 2020: A Vision of the Future
Conclusion
This study demonstrated that it was feasible and informative to integrate patient-level data from
COQPIT and the ACS Surgeon Specific Registry maintained by an individual surgeon.
Approximately half of the discharges attributed to the surgeon by COQPIT were patients in
whom either a primary procedure was performed by another surgeon a/or in whom this surgeon
served in a consulting role or performed a minor procedure or portion of a procedure. By
integrating data from both sources we were able to identify those cases in which the surgeon
performed the patient's primary procedure and to drill down into more detailed data maintained
in the SSR to examine variables that may account for discrepancies between COQPIT estimates
of expected LOS and actual LOS.
Physicians are increasingly being encouraged to maintain their own logs of cases for purposes of
quality monitoring, outcome assessment and recertification. Simultaneously, hospitals, health
systems and professional organizations are developing, promoting and utilizing a variety of tools
to capture patient level data and quantify risk adjusted outcomes. Since these tools inevitably
differ with respect to data collection, coding and the specific statistical models employed for risk
adjustment, reliance on any single tool is likely to result in incomplete or inaccurate outcome
assessments. The current study demonstrates that efforts to integrate and analyze data from
multiple sources can help to clarify discrepancies, define meaningful outcomes and provide data
that is useful for clinicians in the process of improving care.
System Quality Review
123
NewYork-Presbyterian Healthcare System Quality Symposium 2014
Quality 2020: A Vision of the Future
Table 1. Patient - Level Data Elements: COQPIT and American College of Surgeons
Surgeon Specific Registry
COQPIT
• Medical Record #
• Discharge Date
• Actual LOS (days)
• Expected LOS (days)
• Mortality prior to discharge (yes, no)
• Expected Probability of Mortality
• One or more Complications (yes, no)
• Expected Probability of complication
ACS SSR
• Medical Record #
• Discharge Date
• Age
• Gender
• Admit Date
• Resident/assistant/PGY level
• Co-morbid Conditions
• Pre-operative diagnoses
• Post-operative diagnoses
• Pathology
• American Society of Anesthesiologist
(ASA) Class
• Emergent status
• Procedures performed
• Wound Classification
• Post-op occurrences and outcomes
• Unplanned readmissions
• Return to OR within 30 days
• Death within 30 days
Table 2. Congruence between Post-operative Occurrences Identified in SSR and
Complications identified in COQPIT among Patients/Discharges appearing in both
databases
Complications identified in
COQPIT
•
•
•
•
•
•
•
•
•
•
Cardio-respiratory
Arrest
Complication of
Hemodialysis Device
Disruption of
Operative Wound
Hemorrhage or
Hematoma
Post-op Metabolic
Derangement
Post-op Respiratory
System Complication
Post-operative
Septicemia
Procedure related
Laceration
Tracheostomy
Complication
Venous
Thrombembolism
Post-operative Occurrences
identified in SSR
•
•
•
•
•
•
•
•
•
•
•
•
System Quality Review
Abdominal abscess
Conversion to open
procedure
Enteric fistula
Organ/Space SSI
Respiratory infection
Postoperative blood
loss anemia requiring
transfusion of one unit
PRBC
Postoperative inpatient
recovery prolonged by
features of adynamic
ileus
Retained common duct
stone
Enterocutaneous
fistula
Enterotomy at previous
diverting ileostomy
site repaired with
functional end to end
stapled technique
Abscess
Systemic Sepsis Septic Shock
SSR Post-operative
occurrences identified as
complications in COQPIT
• Bleeding > 4 units
RBCs
• Coma > 24 hours
• Myocardial Infarction
• On Ventilator > 48
hours
• Percutaneous drainage
of pleural effusion
necessary
• Respiratory
insufficiency
associated with pleural
effusion.
• Early postoperative
intestinal obstruction
requiring re-operative
management
• Unplanned Intubation
• Wound dehiscence
• Small bowel
obstruction
124
NewYork-Presbyterian Healthcare System Quality Symposium 2014
Quality 2020: A Vision of the Future
Table 3. Statistics comparing Patients with LOS at or below the COQPIT Expected
number of days and those with Excess LOS relative to COQPIT Expected number of days
LOS at or
below
Expected
N (%)
Excess LOS
N (%)
p-value
Gender
Male
Female
60 (46)
71 (54)
34 (34)
65 (66)
0.05
Resident assistant
PGY 1-3
PGY 4-6
62 (50)
61 (50)
43 (44)
55 (56)
0.20
Comorbidities
No
Yes
81 (60)
55 (40)
56 (54)
48 (46)
0.37
ASA Class
1
81 (61)
61 (59)
0.15
2
3
4
5
28 (21)
19 (14)
4 (3)
1 (1)
33 (32)
8 (8)
1 (1)
0 (0)
Emergent Procedure No
Yes
44 (32)
92 (68)
22 (21)
82 (79)
0.04
Wound
Classification
Clean
Clean-Contaminated
Contaminated
Dirty/Infected
26 (20)
81 (61)
1 (1)
25 (19)
15 (15)
76 (75)
4 (7)
7 (7)
0.16
Post-op
Occurrences
No
Yes
126 (93)
10 (7)
89 (86)
15 (14)
0.06
System Quality Review
125
NewYork-Presbyterian Healthcare System Quality Symposium 2014
Quality 2020: A Vision of the Future
Figure 1: Matching of cases between COQPIT and SSR
Period of Review: July 2009 - June 2013
ACS Surgeon Specific Registry (SSR) data:
N = 602 entries/operations in 579 patients
N=287 in-patient
entries/operations in
268 patients
COQPIT: N = 528 discharges of 476
in-patients attributed to same surgeon
N = 315 outpatient
entries/operations
in 311 patients
N = 240 matching
inpatient discharges in
222 patients
System Quality Review
126
NewYork-Presbyterian Healthcare System Quality Symposium 2014
Quality 2020: A Vision of the Future
Poster Presentation
New York Methodist Hospital
Twice Daily Interdisciplinary Rounding Decreases Length of Stay Index on
Medicine Units
Steven H. Silber, DO, ScM; Joanne Lagnese, RN; Joann Amitrano, RN; Dennis Laurence, MD; Zohirul Islam, MD; Lily
Fung
Introduction
Hospital overcrowding is caused by a combination of high patient volume and clinical
inefficiencies. Improving the inefficiencies increases the value of the patient encounter to the
institution by increasing capacity, decreasing costs, improving emergency department gridlock
and by improving patient satisfaction and safety.
The majority of patients admitted to Medicine are admitted through the Emergency Department
with either undifferentiated illnesses or for illnesses where the trajectory of the disease and
recovery aren't always predictable. Inefficiencies are common when dealing with unscheduled
admissions and there is a great opportunity to effect positive process changes in this population.
A full team approach is required to effect a safe, efficient, and patient centric discharge.
Consensus communication among all disciplines and with the patient and family regarding the
daily care plan, the anticipated date of discharge, and the post discharge arrangements must
occur. As the discharge day approaches, all stakeholders must be on the same page.
The Length of Stay Index (LOSI) is the product of the Actual Length of Stay (ALOS) divided by
the Expected Length of Stay (ELOS). It is more informative than raw length of stay values, as the
ELOS values are severity adjusted according to case mix. The LOSI can be used as a proxy for
efficiency of care coordination.
The goal of our project was to institute a robust multidisciplinary team approach to improve
efficiency of care and to troubleshoot issues in real time in order to effect efficient care, an
effective discharge, and ultimately a decreased LOSI on a Medicine unit. We compared robust
twice daily rounding with robust daily rounding and with usual care.
Quantitative/Qualitative Measures
One Medicine unit was designated as Medicine Pilot Unit 1 (MPU-1). Comprehensive
interdisciplinary rounds were held twice daily. Morning rounds began between 8 and 9 a.m. to
review the patient care coordination tasks to be addressed that day. A second, shorter, set of
rounds occurred between 3 and 4 p.m. to review what had been completed, to troubleshoot
issues in real time and to set the agenda for the next day's care.
System Quality Review
127
NewYork-Presbyterian Healthcare System Quality Symposium 2014
Quality 2020: A Vision of the Future
A second similar Medicine unit served as Medicine Pilot Unit 2 (MPU-2). Robust
interdisciplinary rounds were conducted once daily in the morning. A third similar Medicine unit
was designated as the Medicine Control Unit (MCU).
Data for the 4 month period prior to implementation were compared to data for 3 months post
implementation.
Methodologies
Multiple planning meetings were two months prior to the anticipated project implementation
date to discuss the requirements of expedited discharge and strategies to overcome obstacles.
Each discipline (Medicine, Nursing, Care Coordination, Admitting, Ancillary Services, Transport)
also discussed what they required of each other in order to effect an expeditious discharge.
Consensus was developed around these requirements and a plan of action was developed.
Post implementation, stakeholder meetings were held twice weekly to discuss progress and to
troubleshoot obstacles.
Improvement Results
The unit based data are presented in Chart 1 and the outcome comparisons are illustrated in
Figure 1.
For the MPU-1, the Average Monthly LOSI was 1.59 for the four months prior to program
implementation compared to 1.38 for the three months post implementation, for a Delta LOSI
of 0.21. This corresponds to a13.19 percent decrease in the Average ALOS.
For the MPU-2, the Average Monthly LOSI was 1.63 for the four months prior to program
implementation compared to 1.51 for the three months post implementation, for a Delta LOSI
of 0.13. This corresponds to a 7.80 percent decrease in the Average ALOS.
For the MCU, the Average Monthly LOSI was 1.55 for the four months prior to program
implementation compared to 1.71 for the three months post implementation, for a Delta LOSI
of -0.17. This corresponds to a 10.75 percent increase in the Average ALOS.
Analysis of data from MPU-1 revealed that there were 760 discharges and 4,332 patient days in
the four months prior to the program, with an ALOS of 5.70.
Applying the 13.19 percent decrease in the ALOS to that time period results in an Adjusted
ALOS of 4.95, with a capacity increase of 571 bed days, or the opportunity to place 116 new
patients in those beds. Annualized, that equates to a potential for 1,714 new open bed days and
345 new patients on one unit alone.
Sustainability Strategies
The robust interdisciplinary daily rounding initiative did not incur any additional costs.
The program will continue on MPU-1 and attempts will be made to replicate its success on the
five other Medicine units in the hospital.
System Quality Review
128
NewYork-Presbyterian Healthcare System Quality Symposium 2014
Quality 2020: A Vision of the Future
Lessons Learned
1. Daily interdisciplinary rounds among all stakeholders proved effective in decreasing LOSI on
Medicine units.
2. Twice daily rounds proved more effective than once daily rounds.
3. Communication regarding the needs of each discipline relative to other disciplines is an
essential determinant of success.
Conclusion
Robust interdisciplinary daily rounding is effective for improving efficiencies and decreasing
LOSI on Medicine Units. In this study, twice daily robust rounding has an incremental benefit
over robust once daily morning rounding. Both types of robust rounding have been shown to
have a significant beneficial effect over usual care rounding.
As a large percentage of patients with medical DRGs are admitted to the hospital through the
Emergency Department with illnesses for which the trajectory of improvement isn't alway
predictable, there is a great opportunity to positively effect care coordination in this population.
Each discipline must determine what is required from the other disciplines in order for them to
be efficient and in order for the team to achieve success.
If this intervention can be as successfully implemented on the other Medicine units in the
hospital, there would be a potential increased capacity for up to 1000 new admissions.
This decompression would have a major impact on hospital expenses, flow, emergency
department gridlock, and patient satisfaction.
System Quality Review
129
NewYork-Presbyterian Healthcare System Quality Symposium 2014
Quality 2020: A Vision of the Future
Effects of Interdisciplinary Rounding on Medicine Units
Table 1: Medicine Unit Data
MPU - 1
# of Dischgs
Pt Days
Avg LOS
Jan
Avg ELOS
Avg LOS ELOS
LOSI
CMI
MPU - 2
# of Dischgs
Pt Days
Avg LOS
Jan
Avg ELOS
Avg LOS ELOS
LOSI
CMI
MCU
# of Dischgs
Pt Days
Avg LOS
Avg ELOS
Avg LOS ELOS
LOSI
CMI
Jan
177
1,081
6.11
Feb
190
995
5.24
Mar
197
1,070
5.43
Apr
196
1,186
6.05
May
231
1,191
5.16
Jun
233
1,057
4.54
Jul
226
1,115
4.93
3.68
3.40
3.54
3.68
3.63
3.48
3.46
2.42
1.66
1.20
1.83
1.54
1.04
1.90
1.54
1.15
2.37
1.64
1.22
1.53
1.42
1.20
1.05
1.30
1.09
1.48
1.43
1.12
213
1,257
5.90
Feb
212
1,044
4.92
Mar
196
1,191
6.08
Apr
181
1,114
6.15
May
218
1,175
5.39
Jun
199
1,032
5.19
Jul
197
986
5.01
3.46
3.33
3.71
3.60
3.53
3.45
3.37
2.44
1.70
1.09
1.59
1.48
1.03
2.37
1.64
1.14
2.56
1.71
1.08
1.86
1.53
1.04
1.74
1.50
1.05
1.64
1.49
0.98
163
1,121
6.88
Feb
167
833
4.99
Mar
168
999
5.95
Apr
161
893
5.55
May
160
1,140
7.13
Jun
164
929
5.66
Jul
161
1,044
6.48
3.87
3.65
3.91
3.65
3.66
3.74
3.87
3.00
1.78
1.27
1.34
1.37
1.13
2.04
1.52
1.30
1.89
1.52
1.17
3.47
1.95
1.21
1.92
1.51
1.19
2.61
1.67
1.28
System Quality Review
Pre LOSI
Post LOSI
Delta
LOSI
LOSI
Variance
1.59
1.38
0.21
13.19%
Pre LOSI
Post LOSI
Delta
LOSI
LOSI
Variance
1.63
1.51
0.13
7.80%
Pre LOSI
Post LOSI
Delta
LOSI
LOSI
Variance
1.55
1.71
-0.17
-10.75%
130
NewYork-Presbyterian Healthcare System Quality Symposium 2014
Quality 2020: A Vision of the Future
Figure 1: Length of Stay Index Comparison
2.00
1.80
MPU-1
1.60
MPU -2
MCU
1.40
1.20
Jan
System Quality Review
Feb
Mar
Apr
May
Jun
Jul
131
NewYork-Presbyterian Healthcare System Quality Symposium 2014
Quality 2020: A Vision of the Future
New York Methodist Hospital
Higher Success Rates in Difficult Venous Access Patients with Guidewire
Associated Peripheral Intravenous Catheter
Gerardo Chiricolo, MD, FACEP; Andrew Balk, MD; Wendy Wen, MD; Athena Mihailos, MD; Samuel Ayala, MD;
Ryan Giorgetti, MD
Introduction
Venous access is an early and essential step in the management of most Emergency Department
patients, particularly those who are critically ill. There is a significant subset of patients with
limited venous access options and are deemed to have difficult venous access (DVA) due to a
variety of factors well established in the literature, including obesity, vasculopathies, previous
frequent phlebotomy or IV attempts, and intravenous drug abuse. Frequently, there are multiple
failed attempts on these patients before success is achieved. These procedures are time
consuming, consume vital resources, cause pain, discomfort, and cause anxiety to the patients
and increase the infection rates. Decreasing failed attempts equates to cost savings and improved
satisfaction.
Recently dynamic ultrasound guidance for vascular access in DVA patients has been shown to be
advantageous. Ultrasound-guided vascular access has been shown to be rapid, safe, and in many
cases can help avoid central line placement and its associated cost and complications. Access to
ultrasound equipment and clinicians trained in ultrasound-guided technique are often obstacles to
implementing this technology. Furthermore, using ultrasound for a vascular access guidance
procedure usually involves a physician. This may not, however, be the best utilization of
physician’s time in a busy ED while caring for multiple sick patients.
As the patient volume in our Emergency Department has significantly increased, so has the
demand on physicians to expeditiously see more patients. As physicians spend time performing
non-critical procedures, they are unavailable to attend to new patients. Efficiency is of critical
importance. Recently, clinicians have been relying heavily on the ultrasound division faculty to
place ultrasound-guided intravenous catheters. Similar to their clinical colleagues, every time an
Emergency Ultrasound physician takes the time to place an ultrasound-guided peripheral IV, he
or she is less available to care for other patients or perform emergent diagnostic ultrasound
examinations.
Recently a guidewire attached peripheral intravenous catheter (GAPIV, AccuCath™) has been
introduced to the marketplace. This product theoretically would make intravenous catheter
placement easier, decrease posterior vessel wall rupture and thus reduce the number of failed
attempts.
Our goal is to decrease the number of vascular access attempts thus cutting waste and improving
patient satisfaction scores on difficult access patients presenting to the Emergency Department.
System Quality Review
132
NewYork-Presbyterian Healthcare System Quality Symposium 2014
Quality 2020: A Vision of the Future
Quantitative/Qualitative Measures
We identified that physicians were being utilized to obtain intravenous access on difficult access
Emergency Department patients on average 5 times per day. The physician members of the
emergency ultrasound division were asked for assistance in the majority of those encounters. We
explored the options available to improve intravenous catheter success rates and determined that
a guidewire associated intravenous catheter (GAIV) would improve first attempt success rates.
While alternating the GAIV catheter with our conventional catheter, we gathered data on first
pass success rates as well as patient and physician satisfaction. The number of wasted catheters
were also recorded. We analyzed the data after implementation.
Methodologies
The division of Emergency Ultrasound was gifted 120 Accucath™ products for evaluation by
Vascular Pathways, Inc. There are no other financial disclosures apart from the 120 units of
product and in-service educational time. We alternated placement of the GAPIV with placement
of our currently used catheter the BD autoguard (conventional catheter) when any of the
participating physicians were called for assistance with difficult access patients as a convenience
sample. We proceeded to assess and record the factors for and level of difficulty in obtaining
vascular access. We then recorded the number of attempts, the patient satisfaction score using a
traditional 1 to 5 Likert scale with 5 being most satisfied. Finally, we recorded the performing
physician’s satisfaction with the product using the same Likert scale with 5 representing most
satisfied.
Improvement Results
We evaluated a total of 200 difficult access placements presenting to the Emergency Department
for care. We alternated use between the GAPIV product and the conventionally used catheter.
The average number of catheters per patient used for the GAPIV product was 1.18 versus 1.91
catheters used per patient with the conventional catheter. The first pass success of the GAPIV
was 82% versus 22% with the conventional catheter. Total number of intravenous catheter
placement attempts was 118 with the GAPIV catheter and 191 conventional catheter placement
attempts. The GAPIV had an average patient satisfaction score of 4.59 compared with the
conventional catheter score of 2.44. Physician satisfaction score for ease of use and likelihood to
use the GAPIV product for difficult access patients was 4.76. The physicians scored the
conventional catheter on average a 3.3 for ease of use and satisfaction with the product.
Sustainability Strategies
The guidewire associated intravenous catheter appears to decrease the unnecessary utilization of
emergency ultrasound physicians and may be taught to other ER personnel allowing those
physicians to spend that time evaluating other patients. The guidewire associated intravenous
catheter increased first pass success rates significantly and decreased product waste almost at a
ratio of 2 to 1. It also improved patient satisfaction to the procedure significantly as they
experienced less pain due to fewer attempts at intravenous access. Physicians were also satisfied
as they spent less time at the bedside securing intravenous access and had higher first pass
success. Utilizing a guidewire associated intravenous catheter appears to be better for patient
System Quality Review
133
NewYork-Presbyterian Healthcare System Quality Symposium 2014
Quality 2020: A Vision of the Future
care in difficult access patients and improves patient satisfaction to the procedure making a
GAPIV catheter a valuable option for those patients.
Lessons Learned
1. Obtaining vascular access in those patients with difficult access demands excessive resources
and time.
2. Guidewire associated intravenous catheters improve first attempt success rates.
3. Guidewire associated intravenous catheters improve patient satisfaction of the procedure
Conclusion
A guidewire associated peripheral venous catheter product significantly decreased failed first
attempts rate, had less product waste and had higher patient satisfaction and physician
satisfaction scores than the conventional venous catheter. Furthermore, this type of catheter may
be used by other Emergency Department personnel limiting the unnecessary utilization of
valuable system resources.
System Quality Review
134
NewYork-Presbyterian Healthcare System Quality Symposium 2014
Quality 2020: A Vision of the Future
TABLE 1: GAPIV vs CONVENTIONAL CATHETER
GAPIV
Conventional
Catheter
Patients Enrolled
100
100
Patient Attempt Count = 1
82
22
Patient Attempt Count = 2
18
65
Patient Attempt Count = 3
0
13
Total Number of Attempts
118
191
First Attempt Success
82%
22%
Catheters Per IV Start
1.18
1.91
IV First Pass Failure Rate
18%
78%
Patient Satisfaction Insertion
4.59
2.44
Patient Comfort Comparison
4.56
2.51
Physician Satisfaction
4.76
3.30
GAPIV = Guidewire Associated Peripheral Intravenous Catheter
IV = Intravenous
System Quality Review
135
NewYork-Presbyterian Healthcare System Quality Symposium 2014
Quality 2020: A Vision of the Future
New York Methodist Hospital
Clinic "No Shows"- Boost Clinical Productivity
Eshan Patel, MD; Ashwad Afzal, MD; Janaki Patel, MD; Kamraan Madhani, MD; Parag Mehta, MD; Zohirul Islam,
MD; Mohammed Bashey, MD
Introduction
Patient nonattendance (also known as “no-shows”) at scheduled medicine outpatient clinic
appointments is worrisome for many outpatient medical clinics. On a national level, no show
rates in outpatient medical clinics have been reported between 23% and 34%. New York
Methodist Hospital reports a no show rate of 22.3% (604/2709) during a time span of October
1st - December 31st, 2013. Our no show rate for clinic appointments is concerning because they
can create obstacles to continuity of patient care and financial burdens for the hospital and for
patients. We hypothesize that patients with multiple co morbidities were more likely to miss with
their appointments in medicine clinic.
Quantitative/Qualitative Measures
We selected 250 clinic patients who missed 1 or more scheduled clinic appointments over a 3month time period from one section of our medicine clinic. We also selected another 250
patients who kept their appointment during same 3-month time period. We studied patients
who missed their clinic appointments and their correlation with age, sex, ethnicity, language and 6
common co morbidities which includes Diabetes Mellitus, Hypertension, End Stage Renal
Disease, Congestive Heart Failure, Chronic Obstructive Pulmonary Disease, and Asthma. We
also screened "show" patients using same variables.
Methodologies
Data showed that when looking specifically at age, ethnicity or gender, there was no significant
difference between the numbers of patients who missed their appointments from the patients
that kept their appointments. However, when taking into account native language, there was a
significant difference in the no show rate. We also found a significant difference amongst patients
who missed their appointments from those who kept their appointments when comparing the
seven individual co-morbidities. Patients noted to miss their appointments more frequently had
either Diabetes Mellitus, Congestive Heart Failure, or End Stage Renal Disease on Hemodialysis.
Hypertension, Coronary Artery Disease, Asthma, and Chronic Obstructive Pulmonary Disease
were not major variables contributing to missed appointments. Special attention was paid to
group of patient who had Diabetes Mellitus, Congestive Heart Failure and End Stage Renal
Disease on Hemodialysis. We conducted survey on "No Show" patient by contacting them ( via
mail, phone) regarding reasons to miss an appointment, using variables such as forgetfullness,
lack of transportation, elect not to attend and unsatisfactory care.
System Quality Review
136
NewYork-Presbyterian Healthcare System Quality Symposium 2014
Quality 2020: A Vision of the Future
Improvement Results
Data showed that majority of patient who did not keep their appointments were due to
forgetfulness. We implemented system in which multiple attempts to remind patients of
upcoming clinic appointments are made. Attempts were made through mail and telephone
reminder day before the appointment. Patient who had either Diabetes Mellitus, Congestive
Heart Failure and/or End Stage Renal Disease predisposes patients to missing clinic
appointments because this sub set of patients have multiple appointments in various sub specialty
clinics that they must coordinate on top of their medicine follow up appointment. We
implemented system in which Diabetes patient can have multiple appointment with sub-specialty
clinic and medicine clinic on same day. Similarly, patients with End Stage Renal Disease may have
improved compliance with their clinic appointments if appointments are made of non-Dialysis
days. After implementing such rules and constant remainder to patient regarding their
appointments, our no show rate decreased to 18.6%.
Sustainability Strategies
Telemedicine as part of modern medicine. Telemedicine can facilitate medical education and
compliance; potentially significantely reducing the overall cost of medical care. The importance of
multi-disciplinary care to provide most comprehensive treatment plan to our patients. Multidisciplinary clinic improves quality and safety for patient with major chronic comorbidities.
Lessons Learned
1. Telemedicine is important to improve "No Shows"
2. Multiple major co morbidities were more likely to miss with their appointments: combating
the chronic care
3. Multidisciplinary healthcare approach to reduce multiple appointments
Conclusion
Our quality improvement project showed the importance of telemedicine in modern healthcare.
Telemedicine improves appointment compliance, reduce financial burdens and achieve higher
quality of patient care. Our results showed three most prevalent co morbidities present in patients
who miss clinic appointments are Diabetes, Congestive Heart Failure, and End Stage Renal
Disease on Hemodialysis. We believe that the presence of diabetes predisposes patients to
missing clinic appointments because this sub set of patients have multiple appointments in
various sub specialty clinics that they must coordinate on top of their medicine follow up
appointment. By identifying major factors associated with no shows in medical clinic, we can
now better target these specific individuals and reinforce education regarding the importance of
regular follow up. This project supports the implementation of multi-disciplinary clinics so that
patients are able to be seen by multiple sub specialties on the same day rather than have different
appointments on different days. Similarly, patients with End Stage Renal Disease may have
improved compliance with their clinic appointments if appointments are made of non-Dialysis
days. Further studies are currently being planned to investigate the success of multi disciplinary
clinics.
System Quality Review
137
NewYork-Presbyterian Healthcare System Quality Symposium 2014
Quality 2020: A Vision of the Future
New York Methodist Hospital
The "July Effect", Outdated or Still a Concern?
Ashwad Afzal MD; Iman Afzal MS; Eric Karu MD; Parag Mehta MD
Introduction
Patient care in a teaching hospital is provided by residents under the direct supervision of
Physicians. There are numerous residents that start in the month of July who lacks clinical
experience, knowledge, and are unfamiliar with the hospital system such as the use of electronic
medical records (EMRs), use of medications appropriately, performing procedures and many
other experiences. As a result of this turnover with new residents, there have been multiple
reports on higher mortality rates in teaching hospitals during the month of July. Our goal was to
identify if there was a significant difference in mortality in July when residents first started their
training versus June 2014 when residents completed their yearly training and implement a system
to reduce the mortality rate.
Quantitative/Qualitative Measures
Our retrospective analysis involved determining the mortality rates in July 2013 when residents
first started their training versus June 2014 when residents completed their yearly training. We
evaluated the number of admissions, rapid response teams (RRTs) and mortality rates.
Methodologies
We performed a retrospective analysis in a community hospital with a residency program that
serves over 36,000 inpatients yearly with a total of 650 beds. The residency program consist over
150 residents involving Medicine, Surgery, Podiatry, Obstetrics and Gynecology. All patients on
adult medical floors were included in the data except for critical care units, hospice care and
neonatal pediatrics. We excluded all critically ill patients that were admitted directly from the
emergency department to the critical care units as majority of first year residents did not rotate
through units. However, we included all patients that were admitted to the medical floors that
were subsequently transferred to the critical care units.
Improvement Results
There were 2,789 admissions with an overall mortality rate of 0.82%, 192 RRTs amongst 138
patients in July 2013. In comparison, there were 2,940 admissions with an overall mortality rate
0.68%, 158 RRTs amongst 114 in June 2014. There were fewer admissions but more RRTs called
in the month of July in comparison to June. Mortality rate remained <1% in both months.
System Quality Review
138
NewYork-Presbyterian Healthcare System Quality Symposium 2014
Quality 2020: A Vision of the Future
Sustainability Strategies
Contrary to the belief of increased mortality rates in the month of July, we found no difference in
mortality rates in July when residents first started their training versus June 2014 when residents
completed their yearly training. Therefore, we do not need a sustainability strategy and rather
need to focus on other areas and not on the level of resident training.
Lessons Learned
Why were there no significant changes in the mortality rate despite having a large difference in
clinical experience and knowledge when comparing July and June? One significant identifiable
factor was the increased number of RRTs called in July. These RRTs were mainly called by
nursing staff with established experience within the hospital. Perhaps nursing staff awareness of
more critical patients play a significant role in July. There are also other factors to be considered
such as:
- Heightened awareness of multidisciplinary teams (nursing staff, pharmacist, respiratory
therapist, etc) with closer supervisions by senior residents and physicians
- Reducing the workload for residents by not allowing admissions to new residents for the first
month until they have familiarized themselves with the hospitals system such as EMR training.
Conclusion
The mortality rate in this teaching hospital remains relatively the same when comparing July
versus June. We believe that increased number of RRTs with heightened awareness by
multidisciplinary teams play a significant role in reducing mortality rates.
System Quality Review
139
NewYork-Presbyterian Healthcare System Quality Symposium 2014
Quality 2020: A Vision of the Future
The "July Effect", outdated or still a concern?
Months
Total number of admissions
Total number of RRTs
Total number of patients with RRTs
Percent of patients with RRTs per admission
Ratio of RRTs per patient*
Total number of expirations
Mortality rate with admissions
Mortality rate with RRTs
System Quality Review
Jul-13
2789
192
138
4.95%
1.39
23
0.82%
16.67%
Jun-14
2940
158
114
3.88%
1.39
20
0.68%
17.54%
140
NewYork-Presbyterian Healthcare System Quality Symposium 2014
Quality 2020: A Vision of the Future
New York Methodist Hospital
Better System, Better Team, Better Outcomes. Defeating Incomplete Medical
Charts in a Community Hospital Setting
Anna Avaliani, MD; Eric Karu, MD; Savath Chan; Parag Mehta, MD
Introduction
Project: Find innovative solutions and implement them to reduce delinquent charts in 12 months
Problem: Delinquent medical records pose a significant issue for many organizations.
Incomplete, inadequate, or unsigned medical records can have serious impact on timely
reimbursement as well as patient care. It is unfortunately a common problem that affects almost
all organizations nationwide.
New York Methodist is a community hospital with 591 adult beds and 60 bassinets. We had a
total of 33,971 adult admissions and 5,689 newborn admissions combined for a total of 39,660
admissions and 24,503 inpatient surgical procedures in the year of 2012. Signature requirement
on History and Physical and Discharge summary would add up to 79,320 in addition to 24, 503
post operative reports, which together add up to a total of 103,823 documentation requirements
in a 12 month period, which can further be divided into 8652 documentations in one month. Our
Hospital’s anticipated numbers for the year of 2013 were even greater considering recent closure
of Long Island College Hospital and the new influx of those patients to our facility.
In a 12 month period from 6/11/2013 to 5/22/14 number of delinquent charts has decreased
from 3126 to 399.
Our study identified incomplete medical charts as files missing documentation or a signature
from the following notes: History and Physical, Discharge Summary and Operative report.
We offered a multi disciplinary approach in order to reduce their numbers. We involved the
teams from Information Technology Department, Health Informatics Management Department,
Appropriate Departmental Chair persons, as well as the Hospital administration. The following
steps were implemented over the 12 months time period:
1. Weekly list generation of incomplete medical records
2. Notification of Health Informatics Management Department
3. Notification of appropriate Department Chairman
4. Notification of suspension
5. Suspension of admission privileges
6. Suspension action in effect
System Quality Review
141
NewYork-Presbyterian Healthcare System Quality Symposium 2014
Quality 2020: A Vision of the Future
Review of delinquent charts identified discharge summary to be the most incomplete note type.
Further review revealed that attending physicians were selecting inappropriate note type. It was
also found to be very cumbersome to type discharge summaries for many attending with high
volume. Our solution was to create a new and better discharge summary to reduce this error
and make it user friendly. The use of electronic medical records made this transition possible in a
speedy time frame.
Goal: 1.Generate a weekly report of the number of delinquent charts by using smart technology
2. Identify physicians individually or based on their appropriate department. 3. Implement
solutions by informing and educate.
Quantitative/Qualitative Measures
In a 12 month period from 6/11/2013 to 5/22/14 number of delinquent charts has decreased
from 3126 to 399. (see Graph 1)
Methodologies
We created team work and utilized smart technology of Electronic medical records. Our team
consisted of IT, Medical Records, Departmental Chairman’s, and the Hospital administration.
Information Technology department generated a list of incomplete medical records. The list was
separated by department name and further divided by individual attending physician name. We
initially asked the medical records department to personally contact each physician via phone and
discuss the need to complete the medical record and the penalties associated for noncompliance.
Later, we asked that the Chairman of their designated department's to further reiterate the
importance of completion of all the incomplete medical charts in a timely manner, which was
done by sending out a notice of possible suspension. If the medical charts were not completed in
an allocated time frame, the initial action of temporary suspension was applied. (Graph 2)
Electronic Medical records allowed for easy identification and generation of the lists. The
progress of each attending physician was tracked weekly and was recorded with creation of
suspension lists for incomplete records.
Improvement Results
In a 12 month period from 6/11/2013 to 5/22/14 number of delinquent charts has decreased
from 3126 to 399. The report of incomplete medical charts was generated on weekly basis.
After only 4 months, the number of charts declined from 3129 to 1500. Additionally, 4 more
months later, the total number declined to 658.
At the end of 12- month period, the weekly number of incomplete medical charts reached 399.
The continued decline and improvement was attributed to involvement of more authoritative
hospital administration as well as the involvement of each appropriate departmental Chairman.
This improvement was also possible due to the ease of computer generated lists with the help of
IT department as well as the personalized assistance provided to each physician who needed help.
Appropriate physician education and training in addition to and ease of their availability and
accessibility were some of the key factors contributing to out overall success.
System Quality Review
142
NewYork-Presbyterian Healthcare System Quality Symposium 2014
Quality 2020: A Vision of the Future
Sustainability Strategies
Generation of weekly medical delinquency lists
Assistance of hospital administration and the Departmental Chairman's
Generation of suspension lists
Suspension of admitting privileges
Advocating for Accountability for actions
Lessons Learned
1. Better System: Redesign of Discharge summary to reduce redundancy and smart use of
technology of EMR
2. Better Team: Reeducation of the hospital housestaff and successful team work approach
involving Information Technology department , Health Informatics Management Department,
Hospital administration and appropriate Chairman of the Departments
3. Better Outcomes: request to demand to restrict access to referendum and reprimand
Conclusion
Delinquent medical records represent a serious impact on timely insurance reimbursement and
also pose a risk for improper patient care.
We introduced a well organized and multidisciplinary approach and achieved a tremendous
success in decreasing the number of incomplete charts. We utilized Smart Use of Technology
with Electronic medical records. We achieved an impressive decline of delinquent charts in a 12month period, starting with 3129 charts and ending with only 399. The continued decline and
improvement was attributed to involvement of more authoritative hospital administration as well
as the involvement of each appropriate departmental Chairman.
Our IT department has offered personalized training and easy accessibility and availability for all
physicians that requested.
Weekly list generations have proven to be essential in monitoring and evaluation of our
approach.
Redesign of discharge summary and ability of the physicians to sign the notes from hospital, their
office or their home in the era of modern technology contributed to great success and decrease
of incomplete records. EMR eliminated the need to go to medical records department, locate
actual charts, hand write notes and file the system. All progress is tracked by weekly generation
of reports and feedback is provided to any physician upon request.
System Quality Review
143
NewYork-Presbyterian Healthcare System Quality Symposium 2014
Quality 2020: A Vision of the Future
Graph 1
Graph 2
• Lessons
learned:
• Better
outcome
System Quality Review
Restrict access
Reprimand
Request, then
Demand
accountability
Redesign to
reduce
redundancy
• Better
system
Reeducate
• Better
Team
144
NewYork-Presbyterian Healthcare System Quality Symposium 2014
Quality 2020: A Vision of the Future
New York Methodist Hospital
Pill Swallowing Physiology in Adults with Oropharyngeal Dysphagia
Riquelme, L.F., PhD, CCC-SLP, BCS-S; Tahhan, H.J., M.S., CCC-SLP; Teitcher, J.E. M.S., CF-SLP
Introduction
Swallowing is a complex process that involves the control and coordination of numerous
structures of the aerodigestive tract. A disruption at any point in this process may result in
dysphagia. Individuals with neurological etiologies often present with deficits in the oral and/or
pharyngeal phases of swallowing. The literature on the geriatric population suggests changes
occur in the physiology of the oropharyngeal swallow as a person ages. These changes, due to
neurological etiologies and/or aging, may lead to a compromised swallow mechanism that has the
potential to significantly alter a person’s quality of life and daily living (Robbins et al., 2005).
Many older persons are prescribed oral medications for the maintenance of good health and/or
to alleviate symptoms of a broad variety of illnesses. The introduction of oral medications, in the
form of pills, creates new challenges for the swallowing mechanism of the healthy elder or
neurologically impaired patient due to the addition of a new challenge to the already
compromised oropharyngeal swallow mechanism.
Presbyphagia, or characteristic changes in the swallowing mechanism of otherwise healthy older
adults, is increasingly common as the general population ages. Difficulty swallowing is the second
most commonly reported symptom in geriatric medicine. Older adults are more vulnerable to
difficulty swallowing. The increased threat of acute illness, medications and any number of agerelated conditions, they can cross the line from a healthy older swallow to being dysphagic.
The purpose of this study was to determine if pill swallowing yields changes to the oropharyngeal
swallow physiology of patients who present with an oropharyngeal dysphagia for foods and/or
liquids. Namely, will the characteristics of the swallow physiology, and resulting oropharyngeal
dysphagia, differ with the presence of a pill? It was hypothesized that pill swallowing challenges
the overall oropharyngeal swallow dynamics in patients with dysphagia. A second purpose of the
proposed study was to correlate changes in penetration/aspiration for foods/liquids to swallow
dynamics for oral pill intake.
Quantitative/Qualitative Measures
For this pilot prospective study, oropharyngeal swallow efficiency measurements included oral
transit time (OTT), pharyngeal transit time (PTT) and oropharyngeal swallow effeciency (OPSE)
for each participant for 4 bolus conditions: TL (thin liquid), SS (semi-solid pudding or
applesauce), TL-pill (pill with thin liquids), and SS-pill (pill with semi-solids).
System Quality Review
145
NewYork-Presbyterian Healthcare System Quality Symposium 2014
Quality 2020: A Vision of the Future
Methodologies
Fifteen participants over age 65 underwent a videofluoroscopic swallow study at New York
Methodist Hospital. Each patient signed a consent form approved by the New York Methodist
Hospital IRB prior to participating in the study. Each patient was assigned to one of four
randomization groups. Groups differed by administration order of standard VFSS protocol and
trials of thin liquid with pill and semi-solid with pill during the videofluoroscopic swallow
evaluation (Table 1). Patients were seated upright in a Hausted videoflouroscopy chair and
viewed in the lateral plane.
The Kay/Pentax Digital Swallow Workstation Model 7120 and fluoroscopy was utilized for data
acquisition and analysis. Imaging was acquired at 60 fields (30 frames) per second. The X-ray
beam captured the oral cavity, pharynx, upper airway and cervical esophagus of each participant
in the lateral projection. Barium used included VARIBAR Thin Liquid, EZ-HD powder mixed
with applesauce for semi-solids; all barium products are produced by EZ-EM, Inc. Capsules were
filled with barium powder.
Improvement Results
The pharyngeal transit times (PTT) for thin liquid comparison between pill and no pill conditions
showed statistical significance (p = 0.003). This denotes a shorter PTT in the presence of a pill
swallowed with a thin liquid bolus.
As noted in Table 2, other temporal measures for absence/presence of the pill were not
significant. Of note was the lack of statistical significance for the Penetration/Aspiration scale
scores under both conditions. This is possibly due to the overall low Pen/Asp scores in the
samples analyzed.
Also noted was a trend for OTT measures across consistencies. OTT for thin liquids (p = 0.066)
and semi-solids (p = 0.082) were found to be marginally longer in the presence of a pill.
Further investigation of the influence of a pill on swallow physiology and on overall temporal
measures is warranted.
Sustainability Strategies
Both the neurogenic and elderly population experience increasingly complex medical issues,
which requires intervention with various medications. The administration of these medications
orally in the form of a pill may create a new challenge for an already compromised oropharyngeal
swallow mechanism. This study contributes preliminary data to understanding how the
oropharyngeal swallow physiology may be impacted with the introduction of a pill.
Further research should be done to better understand how the oropharyngeal swallow physiology
is altered during pill swallows in both the neurogenic/elderly population, as well as a medically
healthy control group. Results as more data is gathered will allow for the future development of
safe swallow strategies for adults taking medications orally. This data may also serve to improve
patient compliance with medication administration, as well as assist nurses during medicine
administration for patients with dysphagia.
System Quality Review
146
NewYork-Presbyterian Healthcare System Quality Symposium 2014
Quality 2020: A Vision of the Future
Lessons Learned
1. The introduction of a pill during the swallow changes the oropharyngeal swallow physiology,
most notably by shortening pharyngeal transit time in the presence of a pill swallowed with thin
liquid compared to non-pill swallows with thin liquid.
2. Oral transit time was also noted to marginally increase with both thin liquid and semi-solid
consistencies in the presence of a pill.
3. Further research is warranted regarding how oropharyngeal swallow physiology is altered
during pill swallows in both the neurogenic/elderly population, as well as a medically healthy
control group.
Conclusion
The introduction of a pill with both thin liquid and semisolid consistencies was shown to change
the oropharyngeal swallow physiology in neurogenic and elderly patients. As these patients take
many oral medications, it is important to understand that the pill can alter an already
compromised swallow mechanism. Presbyphagia, or swallowing problems in healthy aging, is
prevalent in the United States and as older adults live longer, strategies to maximize function,
including swallowing and managing pills orally, increases in importance.
Further data, via ongoing data collection for this study, should serve to better understand how
the oropharyngeal swallow physiology is altered during pill swallows in both the
neurogenic/elderly population, as well as a medically healthy control group. This will serve to
improve swallow safety for oral medications in patients with oropharyngeal dysphagia.
System Quality Review
147
NewYork-Presbyterian Healthcare System Quality Symposium 2014
Quality 2020: A Vision of the Future
Table 1
Randomization Groups:
GROUP
1A
1B
2A
2B
Standard VFSS
Standard VFSS
Pill with Thin Liquid X2
Pill with Semisolid X2
Pill with Thin Liquid X2
Pill With Semisolid X2
Pill with Semisolid X2
Pill with Thin Liquid X2
Pill With Semisolid X2
Pill with Thin Liquid X2
Standard VFSS
Standard VFSS
Table 2
Thin Liquids
Without Pill
OTT
Mean = .5667
PTT
Mean = 1.1695
OPSE
Mean = 69.29
Pen/Asp
Mean = 1.2917
With Pill
OTT
Mean = .61
PTT
Mean = .91
OPSE
Mean = 60.08
Pen/Asp
Mean = 1.42
t-Test
With Pill
OTT
Mean = .1.95
PTT
Mean = 1.22
OPSE
Mean = 50.62
Pen/Asp
Mean = 1.000
t-Test
p = .066
p = .003
p = .787
p = .969
Semi-Solids
Without Pill
OTT
Mean = 1.1983
PTT
Mean = 2.4726
OPSE
Mean = 40.7339
Pen/Asp
Mean = 1.000
System Quality Review
p = .082
p = .897
p = .935
N/A
148
NewYork-Presbyterian Healthcare System Quality Symposium 2014
Quality 2020: A Vision of the Future
New York Methodist Hospital
Physician Transition of Care: The Benefits of I-PASS and the Electronic
Hand-Off System
Dr. Zainab Qayumi; Dr. Jasmine Walia; Dr. Bita Kharraz; Dr. Aamisha Gupta; Dr. Kandie Gearge; Dr. Usama Samaan
Dr. Nelson Eslao; Nayaab Khawarb, BS; Dr. Pramod Narula; Dr. Beata Dygulska
Introduction
According to Patient Safety America, the total number of Americans dying from medical errors is
around 400,000 each year and has become the third leading cause of death in the United States,
behind cancer and heart disease. Communication errors are a contributing cause of approximately
two-thirds of these sentinel events, over half of which involve handoff failures.
With the ACGME’s new regulations in duty hours, an increase in time is needed for transition of
patient care. In addition to the increasing complexities of medical treatment and care seen in
hospitals today, the importance of effective communication between providers is necessary. It
has also been studied that introduction of new information technology tools into the health care
setting can provide benefits for positive impact on work flow. These benefits include reduction in
transcription errors, decreased omission of information, reduced time needed to transcribe
information manually and accessibility from any location.
The overall goal for this project is to develop a uniform transition of care in order to provide the
highest quality of care to patients. Along with uniformity, the project aims to convert the
standardized system into an electronic format to ensure efficiency and efficacy in utilizing patient
information, also, while seeking to enhance resident satisfaction and comfort level in regards to
usage of electronic handoff system. With these changes, the project targets to improve resident
compliance, accessibility and consistency with the new system in different areas of resident
practice.
Quantitative/Qualitative Measures
In this prospective study, three phases were completed (Figure 1). The initial phase involved
observation of written resident-to-resident transition of care on the Pediatric Floor and Newborn
nursery. 100 observations were completed in each department by attending physicians and/or
Pediatric chief residents. The second phase involved implementation of the I-PASS system with
observation of100 post-intervention sign-outs. Finally, the third phase involved integration of the
standardized sign-out into an electronic system with observation of 100 sign-outs. Each
observation involved the completion of a 12-point survey, answered by yes or no. In the end, a
resident survey was administered, to determine the resident's satisfaction with the new sign-out
process.
System Quality Review
149
NewYork-Presbyterian Healthcare System Quality Symposium 2014
Quality 2020: A Vision of the Future
Methodologies
The 12-item survey completed by attending physicians or chief residents while observing sign-out
included: Patient identification data; Illness severity; Patient summary; Action list; Situation
awareness, Contingency planning; Synthesis by receiver; Actively engages receiver to ensure
shared understanding; Appropriately prioritizes key information, concerns, actions;
Miscommunication or transfer of erroneous information; Omissions of important information;
Tangential or unrelated conversation and Optimally paced handoff. A satisfaction survey was
completed by all pediatric residents to assess the new electronic hand-off system.
Improvement Results
Data from the three phases were compiled. In the pediatric floor: patient Identification and
patient summary saw a significant change in each phase (p=0.002); Illness severity, actively
engaging receivers, omissions of important information and tangential or unrelated conversations
were all significant throughout the phases (p=0.000); Miscommunication of erroneous
information saw improvement between groups (p=0.003); Optimally paced handoff also was
significant (p=0.001); Situation awareness, contingency planning and Action list saw no change
(p= 0.520 p=0.158; respectively)(Table 1) .
In the Nursery: Illness severity, situation awareness, contingency planning, synthesis of receiver,
actively engage receiver miscommunication of erroneous information, omissions of important
information, tangential or unrelated conversation and optimally paced handoff were all significant
(p=0.000); Patient summary also was significant in between phases (0.048); Action list and
appropriately prioritize key information was not significant in this group throughout the phases
(p=1.000, p=0.363; respectively)(Table 2).
From the resident survey completed after implementation of the I-PASS system and Electronic
Physician Hand-Off system, it was noted that all 28 residents found the new system beneficial
but thought the server was too slow and not enough computers were available.
Sustainability Strategies
Considering this electronic sign-out system is incorporated into the EMR along with the
acceptance by the current pediatric residents, the new system should continue to be a main part
of the current transition of care. With frequent checks by the attending physician or Pediatric
chief residents, maintaining the system can be achieved for recurrent use.
Lessons Learned
1. Communication errors are an important concern during resident sign-out.
2. In transition of care, our department was deficient in contingency planning, read back and
identifying the severity of patients.
3. Residents prefer electronic sign out due to the efficiency and accessibility
Conclusion
Since various miscommunication are a leading cause of adverse events in hospitals. an optimal
hand-off process is essential for patient safety. Changing from an informally structured, written
System Quality Review
150
NewYork-Presbyterian Healthcare System Quality Symposium 2014
Quality 2020: A Vision of the Future
sign-out to a standardized electronic hand-off with provide a consistent, efficient and organized
means for transition of care between resident physicians. Our future goals are to use this
Electronic Physician Hand-off to improve the interdisciplinary communication between resident
physicians and the nursing staff.
System Quality Review
151
NewYork-Presbyterian Healthcare System Quality Symposium 2014
Quality 2020: A Vision of the Future
Table 1. Compliance in Pediatric Floor between Three Phases
PEDIATRIC FLOOR
Phase 1
PRE IPASS
YES
Patient Identification data
Illness Severity
Patient Summary
Action List
Situation Awareness, Contingency
Planning
Synthesis of Receiver
Actively engage receiver
Appropriately prioritize key information
Miscommunication of erroneous
information
Phase 2
POST IPASS
NO
YES
NO
Phase 3
POST EMR
YES
PVALUE
NO
85%
30%
15%
70%
91%
41%
9%
59%
99%
64%
1%
36%
0.002
0.000
100%
0
98%
2%
91%
9%
0.002
92%
8%
84%
16%
84%
16%
0.158
21%
79%
84%
19%
55%
45%
0.000
47%
53%
52%
48%
55%
45%
0.520
8%
92%
59%
41%
54%
46%
0.000
95%
5%
92%
8%
78%
22%
0.000
0 100%
10%
90%
11%
89%
0.003
Omissions of important information
19%
81%
67%
33%
17%
83%
0.000
Tangential or unrelated conversation
84%
16%
11%
89%
18%
80%
0.000
Optimally paced Handoff
95%
5%
94%
6%
80%
20%
0.001
System Quality Review
152
NewYork-Presbyterian Healthcare System Quality Symposium 2014
Quality 2020: A Vision of the Future
Table 2. Compliance in Newborn Nursery between Three Phases
NEWBORN NURSERY
Phase 1
PRE IPASS
YES
Patient Identification data
NO
Phase 2
POST IPASS
YES
Phase 3
POST EMR
NO
YES
P-VALUE
NO
100
0
100
0
100
0
1.000
0
100
62
38
99
1
0.000
Patient Summary
100
0
100
0
97
3
0.048
Action List
100
0
100
0
100
0
1.000
Situation Awareness, Contingency
Planning
12
88
83
27
95
5
0.000
Synthesis of Receiver
24
76
83
17
83
17
0.000
9
91
15
85
98
2
0.000
Appropriately prioritize key information
98
2
98
2
100
0
0.363
Miscommunication of erroneous
information
18
82
0
100
0
100
0.000
Omissions of important information
23
77
14
86
0
100
0.000
Tangential or unrelated conversation
100
0
23
77
2
98
0.000
Optimally paced Handoff
100
0
100
0
100
0
0.000
Illness Severity
Actively engage receiver
System Quality Review
153
NewYork-Presbyterian Healthcare System Quality Symposium 2014
Quality 2020: A Vision of the Future
Figure 1. TIMELINE OF EVENTS FOR I-PASS AND ELECTRONIC
HAND-OFF SYSTEM
PHASE I:
PHASE Ia:
PHASE II:
Data collection from
written resident sign out
without IPASS
intervention
Implementation of
IPASS standardized
system to Residents
Data collection from
written resident sign out
with IPASS intervention
System Quality Review
PHASE IIIa:
PHASE III:
Resident Survey of and
evaluation of sign out
with new system
Initiation of Electronic
Physician hand off
system (EPHS)
154
NewYork-Presbyterian Healthcare System Quality Symposium 2014
Quality 2020: A Vision of the Future
New York Methodist Hospital
Baby Boomers Beware: Implementation of a Hepatitis C Testing Protocol
Vahe Shahnazarian, MD MPH; Eric Karu, MD; Parag Mehta, MD, FACP
Introduction
The CDC and USPSTF have recommended that adults born between the years of 1945-1965
should receive one-time testing for the Hepatitis C Virus (HCV). In fact, Governor Andrew
Cuomo of the State of NY signed a bill on October 23, 2013 that mandated hospitals and
healthcare providers to offer HCV testing to all “Baby Boomers.” The law excludes the
emergency department. This law took effect on January 1, 2014. The objective is to increase the
rate and efficiency of our compliance with this recent NY State law. The importance of this law
lies in the fact that people who have HCV and are identified early on can benefit from early
treatment and avoid liver complications. The later the HCV infection is found, the lower the
chance that the treatment will have a sustained response. Also, HCV-associated disease is the
number one cause of liver transplantation and hepatocellular carcinoma (HCC) in the United
States. The incidence of HCC and transplant are increasing in people who have HCV, and these
numbers are projected to substantially increase in the coming decade. Given the advancement of
current HCV therapies, the interferon-free regimens will likely dominate, making treatment easier
to follow, so having early, successful treatment of HCV infection will have undeniable long-term
benefits.
Quantitative/Qualitative Measures
The measures being studied for this project as a whole include a number of demographics such
as age, birth year, sex, ethnicity, and type of insurance. The main measures being studied include
HCV infection status, HCV testing status, and acceptance or rejection of HCV testing. The
percentage of total HCV testing being offered is also being studied; that is the main outcome
measure. The study's success will be gauged by the monthly percentage of eligible patients being
offered HCV testing, and whether or not there is a statistically significant increase in this
percentage until our goal of 100% is reached.
Methodologies
Approval of the Institutional Review Board was obtained to begin this study. In conjunction with
the Information Technology Services Department (IT), two separate workflows were designed:
one for all patients admitted to any service in the hospital, and the other for patients visiting our
primary care ambulatory clinics. The two are essentially the same in that they automatically check
the patient’s birth year, and if the patient is a “Baby Boomer” (born between 1945-1965), their
Hepatitis C testing status is checked. After that, there are constant reminders to order the testing
for qualified patients, or to never offer testing again if the patient refused or has been tested in
the past. The main difference between the inpatient and ambulatory testing is in how often a
System Quality Review
155
NewYork-Presbyterian Healthcare System Quality Symposium 2014
Quality 2020: A Vision of the Future
reminder will pop up for the clinician. In the ambulatory setting, the reminder will occur much
more frequently given the shorter nature of the visit. This was implemented on Tuesday, April
15, 2014.
Improvement Results
A total of 3987 patients were included in the study in a three-month period. In December 2013,
one month prior to the enactment of the Hepatitis C testing law in NY State, 41.1% of our
patients were tested. In the month after the law was implemented (January 2014), we still had a
41.4% rate for patient testing. However, in the month after our testing protocol was
implemented, that percentage went up to 46.6% of patients either being tested or being offered
testing. When comparing the December group to the Intervention group, the result was
statistically significant with a p-value of 0.008; when comparing the January group to the
Intervention group, that result was also statistically significant with a p-value of 0.0048.
Sustainability Strategies
This intervention is completely sustainable with no further work required. It has been fully
integrated into our electronic medical record (EMR) system thanks to our close work with the IT
Department. In fact, it must be actively removed from the system should we choose to end the
intervention. The current integrated system can also be fully modified without even halting the
program at all, which has been done multiple times already and will be done in the future until we
achieve our goal of 100% testing-offered.
Lessons Learned
1. EMR pop-up alert fatigue is a real issue and must be addressed early on.
2. House staff education is very important in order to implement a successful intervention.
3. House staff input on that intervention is equally important in ensuring the intervention's
success as well.
Conclusion
Since the implementation of our testing protocol, we have seen an increase in the number of
patients being offered Hepatitis C testing (very strong statistical significance with a p- value <
0.01). The protocol has already undergone a number of Plan-Do-Study-Act (PDSA) cycles,
whose outcomes we will be studying in the coming weeks. Our ultimate goal with the protocol is
to attain 100% offering of testing to our patient population, thereby providing them with the best
care possible in this regard. We believe this is possible, but will require further PDSA cycles to
accomplish.
System Quality Review
156
NewYork-Presbyterian Healthcare System Quality Symposium 2014
Quality 2020: A Vision of the Future
New York Methodist Hospital
UTI & Dysphagia: Seeking Best Practice Patterns in Speech-Language
Pathology
Rebecca D. Benjamin, M.S., CCC-SLP; Luis F. Riquelme, Ph.D., CCC-SLP, BCS-S; Laura M. Holtan, M.S., CCCSLP
Introduction
Patients with urinary tract infection (UTI) often present with signs and symptoms of
oropharyngeal dysphagia, including dehydration, failure to thrive, and altered mental status.
Comorbidities may contribute to overall patterns of breakdown in the swallow mechanism. The
effects of UTI on swallow patterns are poorly understood. This study sought to address how a
UTI diagnosis affects swallowing, and how to best approach this patient population. In order to
provide best care, the speech-language pathologist (SLP) should approach the patient as a whole.
This can be facilitated by developing a collaborative approach with other medical professionals
and better understanding the impact of UTI on overall swallow function. Collaboration consists
of understanding the plan of care and goals of other professionals, and integrating those goals
with the specific expertise of the SLP.
This retrospective study, conducted via chart review, investigated the hospital course of patients
admitted over a 6-month period with a primary diagnosis of UTI and who also presented with
dysphagia. Conclusions of this study were drawn from medical chart reviews; specifically the
exploration of past medical history (e.g., dementia, recurrent UTI) and problem history (including
precursors of dysphagia such as failure to thrive and dehydration). Best practices for patients
referred to, and seen by the SLP, were to be identified.
This study also identified those patients who were and were not referred to the SLP; and also
explored if SLP involvement resulted in differences in care regarding the most appropriate means
of nutrition and diet level, as well as overall outcomes.
Quantitative/Qualitative Measures
A total of 40 charts of adult patients admitted to New York Methodist Hospital over a six-month
period (January 2012- June 2012) with a primary diagnosis of UTI were retrospectively reviewed
for this study. Patients admitted to pediatric or maternity units were excluded from this study.
Patients were divided into two groups: Group 1 were charts of patients who were consulted by
SLP (N=20) and Group 2 were charts of patients who were not consulted by SLP (N=20).
Group 1 consisted of adults with a mean age of 90.2, range 75-102 years. Group 2 consisted of
adults with a mean age of 83.1, range 66-100 years.
System Quality Review
157
NewYork-Presbyterian Healthcare System Quality Symposium 2014
Quality 2020: A Vision of the Future
Methodologies
In order to compare diets, a numerical scale was developed (see Table 1). Additionally, outcomes
data were reviewed for Group 1 comparing dysphagia level at time of the consult with that at
time of discharge. The ASHA NOMS (National Outcomes Measurement System) was employed.
Specifically, the functional communication measure (FCM) for swallowing (Table 2) was applied
to this sample. The ASHA NOMS is a data collection system developed to illustrate the value of
SLP services. The FCM's are a series of seven point scales used to describe the change in an
individual's functional communication or swallowing ability over time.
Improvement Results
Intergroup analysis: Group 1 (consulted) to Group 2 (not consulted)
-Age: The Kruskal-Wallis test for age comparison of both groups was statistically significant
(p=0.0227) at the 95% confidence interval.
-LOS (length of stay): Comparison of both groups for length of stay was not statistically
significant (p=0.1611) at the 95% confidence interval.
-Diet on admission: Comparison of both groups showed statistical significance (p-0.0354) at the
95% confidence interval. Patients not consulted (Group 2) showed a significantly less restrictive
diet when compared to Group 1(consulted by SLP).
-Diet at D/C: Comparison of both groups did not reach statistical significance at time of
discharge (p=0.0659).
Intragroup analysis: Group 1(consulted)
-Diet: Signed rank test for the mean difference between diet recommended on admission with
diet recommended by the SLP upon consultation was not statistically significant (p=0.1102).
Comparison of diet recommended by the SLP upon consultation and diet at discharge was also
not significant (p=0.1485).
NOMS: Improvement in the NOMS FCM for swallowing was attained when comparing data at
the time of the SLP consultation with data at discharge (p=0.0248).
Sustainability Strategies
As the SLP role for these patients has been deemed significant, a continuation of referrals to SLP
is necessary for patients with UTI who present with s/s oropharyngeal dysphagia. In order to
improve upon these preliminary findings, further investigation is warranted. A closer
consideration to patients' past medical history (i.e. +/- Dementia) will improve upon these
findings.
Lessons Learned
1) It is significant to correlate signs/symptoms of dysphagia with acute UTI.
2) The SLP plays an important role for this patient population re: returning to a PO diet.
3) Further investigation is needed to determine specific practice patterns with this complex
population.
System Quality Review
158
NewYork-Presbyterian Healthcare System Quality Symposium 2014
Quality 2020: A Vision of the Future
Conclusion
There was a statistical significance demonstrated between groups 1 and 2 for age and for diet on
admission. Group 2, or the patients that were not consulted by SLP, were younger in comparison
to Group 1. The diet on admission for Group 2 was also less restrictive when compared to
Group 1. This may indicate that the group of patients not consulted by SLP were possibly
patients without overt signs of dysphagia, possibly patients with less comorbidities on admission
and possibly with less severe UTI's.
For the group of patients that were consulted by SLP (group 1), improvement in NOMS was
evident. This denotes an improvement in swallowing status for this period. It is, therefore,
suspected that Group 1 presented with more overt s/s dysphagia. It may also be hypothesized
then that the SLP involvement was of relevance to this outcome.
The non-significance of the comparison of diet on admission with that recommended by the SLP
upon consultation is important to note. It is hypothesized that the ongoing collaboration between
SLPs and physicians at New York Methodist Hospital has allowed for better choice of oral diets
upon admission.
Overall, this study shows that the involvement of SLP is significant for improvement in
swallowing status for patients admitted with UTI and with signs and symptoms of dysphagia.
Comparison between those consulted and not consulted showed no significance for length of
stay, which is relevant in today's healthcare environment.
System Quality Review
159
NewYork-Presbyterian Healthcare System Quality Symposium 2014
Quality 2020: A Vision of the Future
TABLE 1
Diet Scale
1
2
3
4
Tube feeding
Puree
Mechanical soft
Regular
TABLE 2
System Quality Review
160
NewYork-Presbyterian Healthcare System Quality Symposium 2014
Quality 2020: A Vision of the Future
New York Methodist Hospital
Achieving the Goal of a Seemingly Impossible Task
Eric Karu MD; Parag Mehta MD
Introduction
After having achieved the requirements for meaningful use stage 1, our next goal was to meet all
of the requirements for meaningful use stage 2. The reporting period began on July 1st 2014 and
ends on September 30th 2014. We were meeting the goals for every measure except for one,
which is "Summary of Care at Transition."
These are items, which must be taken care of in patients' charts via the electronic medical record
prior to their discharge. When documenting a medical problem via our Cerner EMR, they are
documented as either active, inactive, or resolved. The majority of inpatient medical problem
documentation are done by the residents and PAs. Some of the residents were free texting their
problems, frequently misspelling a problems or typing nonsensical words, which were not
medical problems at all. For reasons, which are still unknown, some of the appropriately
documented medical problems, were also not mapping to any problem. Initially, there were
522,614 problems which were unmapped in all. CMS is only concerned with Medicare patients
with active medical problems, which had originally amounted to 158,808. These problems
consisted of both codified and free text problems. On August 11th 2013, our percentage in terms
of meeting the "Summary of Care at Transition" measure was only 32.7%, which was well short
of the 50% goal. Being nearly half way towards the deadline, achieving that 50% goal was
seemingly impossible. Initially, the residents were educated that they were no longer permitted to
free text medical problems and the hospital IT department had disabled that feature. The
information technology fellow had used something called the problem migration tool within the
Cerner EMR to map medical problems to the appropriate diagnoses. He had spent countless
hours manually mapping unmapped medical problems. Initially his progress was very swift
because many problems were grouped together, then progress has slowed down a great deal
because each problem had to be mapped individually, which was painstaking process. Despite the
dramatic drop in unmapped problems, the percentage increase of the measure was rising at a
much slower rate. The reason for this is that the majority of unmapped problems, which were
fixed were on patients, who were already discharged. The measure only counts for problem lists
being fixed prior to the discharge of that particular patient. During the noon conference, the
residents were educated on how to appropriately problem lists. A report was created by the IT
department to show which residents were not document their problem lists correctly. Residents
names would appear on the report if their problem lists were empty or contained problems which
were all resolved. If the patient did in fact have a chronic problem, then they are to simply
document that as being an active medical problem in the problem list. If the patient had no
chronic problems, then they have to select click a field which is labeled "no chronic problems."
System Quality Review
161
NewYork-Presbyterian Healthcare System Quality Symposium 2014
Quality 2020: A Vision of the Future
Every morning a report was printed and the IT fellow would round with the residents in the
morning and educated them individually on appropriate documentation. The list of residents with
improperly documented problems had gone down from 100+ to 5-10. That in itself is a great
achievement. Giving our progress, I have no doubts that we will achieve our goal for Meaningful
Use Stage 2.
Quantitative/Qualitative Measures
Patients with improperly documented problem lists prior to departure, which was monitored on a
daily basis.
Methodologies
The Cerner Electronic Medical Record system is a highly sophisticated tool to get results,
document notes, medical problems, allergies, place orders and many other things. Learning how
to use all the features is crucial to ensure patient safety and meet standards set forth by the
Centers for Medicare and Medicaid Services. In this case, many of the residents were not properly
documenting their problem lists. During a noon conference, the information technology fellow
had given a brief presentation on how to properly document their problem lists. Through a
report it was possible to find out which residents were responsible for either having empty
problem lists or improperly documented problem lists. The majority of those residents were at
the PGY-1 level, which makes sense being that they were still new to the system. The IT fellow
had both rounded with the residents to give them hands on help on how to properly document
their problem lists. In addition, the IT fellow contacted residents individually to help them with
proper documentation.
Improvement Results
As a result of the interventions made by the IT fellow, resident documentation had improved
dramatically and the reports showed fewer and fewer patients with improperly documented
problem lists.
Please see Attachment.
Sustainability Strategies
To ensure that residents document their charts properly and effectively it's important to identify
those users who are in need of remediation early. If the institution is not meeting their goals in
documentation and it's due to repeat offenders, then warnings and/or a disciplinary action must
be taken.
Lessons Learned
1. When trying to achieve goals in meaningful use, it's essential to start early on because if you
start late into the measuring period, achieving that goal could become a seemingly impossible
task.
2. It's essential to have innovative tools which can identify the users who are having the most
trouble with using the EMR early on, so they can be corrected early on.
System Quality Review
162
NewYork-Presbyterian Healthcare System Quality Symposium 2014
Quality 2020: A Vision of the Future
3. It is vital for an institution to have a physician liaison, who has a medical background allowing
them to identify problems, reach out to the users, and provide guidance, when needed.
Conclusion
As can be seen in the results, on September 8th 2014 we are at 49.40% and we will easily exceed
our goal of 50% well before the September 30th deadline. In mid-August (half way through our
90 measuring period, achieving that 50% goal seemed nearly impossible. However, by gaining the
right understanding of the problem, the path to achieving our goal became clearer and clearer.
We had learned important lessons from this project. We learned that we must never put off until
tomorrow, what we can do today. It's never a good thing to start a big project too late. We
learned that through reports we were able to find out which residents were having issues with
documentation and we were able to reach out to them. Starting on October 1st, we must
maintain these goals for one fiscal year. We are confident that we will be able to achieve that goal
through right understanding, getting an early start, and plenty of hard work.
System Quality Review
163
NewYork-Presbyterian Healthcare System Quality Symposium 2014
Quality 2020: A Vision of the Future
System Quality Review
164
NewYork-Presbyterian Healthcare System Quality Symposium 2014
Quality 2020: A Vision of the Future
System Quality Review
165
NewYork-Presbyterian Healthcare System Quality Symposium 2014
Quality 2020: A Vision of the Future
New York Methodist Hospital
New York Methodist Hospital Care Transition Management Interventions
Tiffany Bacchus FNP-BC, Amin Khalid MD MPH, Paraq Metha MD MPH
Introduction
The goal of the hospital medical home program is to coordinate our patient’s follow up care
between specialty and medical providers after the patient’s hospitalization. It is our expectation
that a seamless transition of care will enhance better patient outcomes, reduce readmission rates
and educate patient on self-management of chronic illness thus decreasing the outpatient no
show rates for scheduled appointments. We have implemented the Care Transition Management
process in October 2013 after the addition of the Nurse Practitioner who serves as a care
coordinator. The care coordinator serves as a liaison in-between the inpatient and outpatient
setting. During the course of a patient’s hospitalization the care coordinator will visit the
admitted patient. During this face to face interaction a brief physical and social assessment is
completed. If issues are identified the care team is notified and the issues are addressed. The care
team consists of the medical doctor, social worker, case manager, and nurse manager. When the
patient has been discharged the care coordinator will call the patient at home within 72 hours and
evaluate their condition. During this call any questions or concerns are addressed and patient
education on illness, medications, self-management and follow up care is discussed.
Appointments for all post hospital follow up care are scheduled during this phone interview.
Prior to the appointment day Patients receive a call 48 hours before their appointment from an
automated system as a reminder of their scheduled appointment. This project was designed to
evaluate the effectiveness of the care transition process.
Quantitative/Qualitative Measures
We evaluated the effectiveness of the Care Transition Management (CTM) interventions over
three reporting quarters that spanned from October 2013 until June 2014. Each quarter the
numbers of patients that had a face to face interaction with in the quarter, the amount of patients
that received a TCM call, Scheduled appointments and reported for follow up appointment were
evaluated. Readmission rate was also evaluated each quarter and common readmission diagnosis.
Methodologies
New York Methodist Hospital is located in an urban setting in New York City. Care transition
practices take place in the inpatient and the outpatient setting. This is controlled trial conducted
in between October 2013 and June 2014. Established outpatient clinic patients are identified
during daily chart reviews done in the Electronic Medical Record. Patients that are selected have
Medicaid /Medicaid HMO insurances and are between the ages of 21-65. All interaction between
the care coordinator and the patient is documented in the Electronic Medical record (Cerner) in a
Transitional Care Management form. The care coordinator’s role is to improve the patient’s
System Quality Review
166
NewYork-Presbyterian Healthcare System Quality Symposium 2014
Quality 2020: A Vision of the Future
continuity of care by arranging follow up care post hospitalization and educating the patient to
become an active participant in their self-care management. Data was evaluated each quarter and
documented.
Improvement Results
The baseline data from October-December 2013 is as follows 56% of the admitted patients had a
face to face interaction with the care coordinator, 74% of those patients had received a TCM call
within 72 hours, and 71% scheduled follow up appointments, 66% of scheduled patients
reported to their scheduled follow appointment. During this time we had a 9% readmission rate.
During Quarter #1 January –March 2014 there was an increase in patient volume. 66% of our
admitted patients received a face to face interaction, 73% received a TCM call with in the 72 hour
window. 74% scheduled their follow up appointments and 52% reported for their appointments.
The readmission rate was 27%. In Quarter #2 is from April-June 2014. 64% of our admitted
patients had a face to face interaction. 89% of the patients received a TCM call, 81 % 74%
scheduled their follow up appointments 65% reported for their appointment. The readmission
rate was 33%. Due to an increase in patient volume in Quarter #1 and Quarter #2 variance is
noted in the report rate and the patient’s readmission rate.
Sustainability Strategies
The face to face interaction formulating a connection with the patient while hospitalized has
proven to be helpful in alleviating patient’s anxiety about post hospital care. The follow up
(TCM) phone calls and coordination of follow up care in between the medical and the specialty
services has increased the number of patients that return to follow up care. Due to the
implementation of an improved patient tracking system we have a more accurate way of tracking
our progress.
Lessons Learned
1. Better patient education is necessary for better patient out comes.
2. Increase communication between patient and providers increases follow.
3. Increase and continued post hospital follow up care is necessary to prevent patient
readmissions.
Conclusion
Prior to the implementation of these additional steps we had no consistent process to track
patients through their transition after hospitalization. The evolution of our team and transition
process in a short period of time is extraordinary. Continued intervention to insure that all the
needs and concerns of our patients are met is necessary to evaluate the long term effectiveness of
New York Methodist care transition management. We continue to work on improving our post
hospital follow up processes.
System Quality Review
167
NewYork-Presbyterian Healthcare System Quality Symposium 2014
Quality 2020: A Vision of the Future
New York Methodist Hospital
High Value Cost Conscious Care
Eric Karu MD; Parag Mehta MD
Introduction
To reduce unwarranted finger sticks for the purpose of blood glucose testing.
1. Inappropriate frequency
2. Inappropriate timing
3. Eliminate chem strip orders completely on patients, who do no have a definitive diagnosis
of Diabetes Mellitus
There were roughly ½ a million finger sticks, which were done in 2013 alone at NYM so the
pattern of glucose testing was studied via several multidisciplinary committee meetings. Their
findings were that. #1 Chem strips were ordered on patients without a diagnosis of diabetes. #2
the frequency and timing of chem strip orders were variable and often ordered Q4 or Q6 hours.
A guideline was then developed to cut down on unnecessary glucose testing in an effort to
provide high value, cost conscious care to our patients. There was no restriction on the frequency
of finger sticks for patients in the ICU, uncontrolled diabetic patients or patients who may
require more than a BID frequency of finger sticks. Physicians, nursing hospital administration,
pharmacy, and IT departments were all involved.
A rule and order set were created via cerner. It was decided that providers may place an order for
chem strips if and only if a patient has a definitive diagnosis of diabetes mellitus. The frequency
of finger sticks was also adjusted to BID (before breakfast & dinner) in controlled diabetic
patients.
The staff and residents were educated on daily round in order to achieve the goal of reducing
unwarranted finger sticks and consequently increase patient satisfaction and a reduction in
wasted, time, resources, and costs. The study concerned the number of chem strip orders on
well controlled diabetic patients on the medical floors every month vs the number of admissions
and number of inpatients with a diagnosis of diabetes mellitus (2013 vs 2014).
Quantitative/Qualitative Measures
1. Chem strip frequency reduced from Q4-Q6 hours to BID AC (before breakfast & before
dinner) for controlled diabetic patients (HBA1C < 7.0)
Please see graphs.
System Quality Review
168
NewYork-Presbyterian Healthcare System Quality Symposium 2014
Quality 2020: A Vision of the Future
Methodologies
The Plan, Do, Study Act cycle was repeatedly performed and the staffing were repeated educated
on appropriate finger stick testing.
Identification of problems
Identification of the work flow
Arriving at Solutions
Educating Resident Physicians and House Staff
Evaluating
Providing Collaborate feedback
Improvement Results
As can be seen in the attached data & graphs, the number of patients with a diabetes diagnosis
was on average significantly here for 2014 vs 2013. However, the number of chem strip orders
had significantly decreased following the intervention to reduce unnecessary chem strips.
Sustainability Strategies
1. Ease of running a report by any users and at any time .
2. Those reports are assigned to certain people to run them regularly.
3. Communication with any people who are responsible for these matters
Lessons Learned
1. Patient Safety, Patient Satisfaction, High Quality Health Care is possible at any level & similar
strategies can be applied to other high care testing.
2. Reducing wastage of valuable resources is in everyone's best interests
3. This model can be applied to many other high cost testing.
Conclusion
There’s absolutely no question that patients with a diagnosis of diabetes mellitus should have
their blood sugar checked regularly to prevent complications. The New York Methodist Hospital
medical staff was educated on the new guidelines on BID finger stick testing as recommended by
the American Diabetic Association. By the simple creation of an order set, placing a simple rule
via the EMR, and educating the medical staff, we had managed to curtail the unnecessary testing
by a significant amount without compromising patient safety. This represents a reduction in costs
of approximately $30,000 a year in medical supplies (Chem Strips, Lancets, Alcohol Pads) and a
reduction of 5,000 man hours (or two full time employees). In addition to reduced costs to the
patient and hospital, there’s a reduction of pain, reduction of inconvenience, while preserving
patient satisfaction.
System Quality Review
169
NewYork-Presbyterian Healthcare System Quality Symposium 2014
Quality 2020: A Vision of the Future
Inpatients with Diabetes Diagnosis
1200
1000
800
600
2013
400
2014
200
0
January February March
April
May
June
July
Fingersticks per month 2013 vs 2014
25000
20000
15000
10000
5000
Fingersticks per Month
(2013)
Fingersticks per Month
(2014)
0
System Quality Review
170
NewYork-Presbyterian Healthcare System Quality Symposium 2014
Quality 2020: A Vision of the Future
Admission and # of Finger Sticks in 2013 &
2014
25000
20000
15000
10000
admission
finger sticks
5000
2013
System Quality Review
July
June
May
April
March
February
January
July
June
May
April
March
February
January
0
2014
171
NewYork-Presbyterian Healthcare System Quality Symposium 2014
Quality 2020: A Vision of the Future
New York Methodist Hospital
Implementing a Patient Check-In Scanner to Reduce Average Wait Times for
Patients Receiving Radiation Therapy
L. Tchelebi, MD; U. Gada, MBBS; K. Parikh, MD; S. McVorran, MHSA; H. Ashamalla, MD
Introduction
Patient quality of life is significantly impacted by the length of time spent waiting in doctors’
offices. This is particularly relevant to the field of Radiation Oncology which cares for cancer
patients receiving daily therapy for several weeks duration. Delays in treatment are both
inconvenient and emotionally disruptive for those already stressed by their cancer diagnosis.
Unfortunately, certain treatment delays are unavoidable. As a quality assurance measure, we
sought to assess the average wait time for outpatients in our department. We then analyzed our
data to identify potential causes for prolonged wait times. We found that our department lacked a
reliable and systematic means of checking into the department, thereby causing patients to wait
longer for treatment. We therefore implemented a patient check-in scanner to improve
documentation of patient arrival and re-assessed the data.
Quantitative/Qualitative Measures
Our initial investigation consisted of distributing punch cards to 20 randomly selected patients
undergoing treatment during the month of February 2014. 10 patients received treatment on a
Varian Clinac 2100C and the remaining 10 patients were treated on a Clinac iX Linear
Accelerator. Each patient was asked to punch in upon arrival to our department. We then
calculated the difference between patients check-in times and their actual treatment times. We
found that patients were waiting on average 58 minutes. On subset analysis, patients on the
2100C were waiting on average 70 minutes while patients on the iX were waiting on average 45
minutes.
Methodologies
Our data indicated that our department lacked a reliable and systematic means of measuring
check-in times. This resulted in an inaccuracy in measuring wait times in addition to contributing
to treatment delays due to a lack of communication between the waiting room and the treatment
area to alert the therapists to the patients’ arrival. We therefore purchased a Varian Voyager
Patient Check-In Scanner and assigned a volunteer to monitor patient check-in. Each time a
patient arrived, s/he was reminded to scan their personal barcode into the treatment system. The
therapists were thus alerted to the patient’s arrival, facilitating more timely treatment.
System Quality Review
172
NewYork-Presbyterian Healthcare System Quality Symposium 2014
Quality 2020: A Vision of the Future
Improvement Results
After implementing the scanner, we randomly selected 20 patients who presented for treatment
during the month of August 2014. As before, 10 patients were treated on each machine. There
was a statistically significant difference in wait times before and after the implementation of the
check-in scanner. We found that the average wait time decreased from 58 to 37 minutes
(P<0.0001). On subset analysis, we found that the wait time on the iX was decreased from 45 to
26 minutes (P<0.0001), while the average wait time on the 2100C was shortened from 70 to 48
minutes (P=0.004). This dramatic decrease in wait times is unlikely to be solely due to a lack of
awareness of patient arrival, but may also be due to inaccuracies in measuring wait times using the
punch-card method which is both tedious and unreliable.
Sustainability Strategies
With continued and routine use of the patient check-in scanner, we should be able to eliminate
delays in treatment due to lack of awareness of patient arrival to our department. While we may
not always have a volunteer present to remind patients to check-in, once the use of the scanner
becomes routine, patients should themselves remember to check-in without having to be
reminded. This will also allow us to more accurately collect and analyze data in the future so that
we can better identify and eliminate further causes of treatment delay.
Lessons Learned
1. It is important to have an accurate and systematic means of checking patients in to our
department
2. Improvement in communication between the waiting room and the treatment area has resulted
in decreased wait times for our patients
3. There is a relatively prolonged wait time for the 2100C . We need to identify and eliminate
factors resulting in this delay
Conclusion
Patients receiving radiation therapy treatments are obligated to come to the department every day
for several weeks. Any sources of prolonged wait times in the department should be eliminated.
Having a precise and efficient means of checking-patients into the Radiation Oncology
Department is an important aspect of quality assurance. We found that implementing a patient
check-in scanner to accurately document patient arrival improved the quality of patient care in
our department as there was a statistically significant decrease in wait times. This does so both by
alerting therapists to patients’ arrival so that they may be called in for treatment more expediently
and by making future analysis of wait times more accurate.
System Quality Review
173
NewYork-Presbyterian Healthcare System Quality Symposium 2014
Quality 2020: A Vision of the Future
New York Methodist Hospital
Using Social Media for Dynamic Curriculum on Demand
Eric Karu MD; Pauline Zaroovabeli MD; Parag Mehta MD; Sanjay Cherukuri MD
Introduction
For centuries, traditional medical teaching has occurred in classrooms, lecture halls, and on ward
rounds. Frequently, students have a limited attention span during the course of a lecture and they
may feel overwhelmed by the sheer volume of material that's being covered during that period.
Students may also feel less eager to participate in the classroom setting due to shyness or
embarrassment. Medical residents have limited time to allocate to learning in the classroom
setting, given their grueling work schedules.
Today, we learn, teach, and practice medicine in the digital era. Social networking websites and
applications, such as Whatsapp, Facebook, Twitter, and many others are used by many of us for
personal networking, but very few are using it for education. The use of social media in the
academic setting has many advantages. It is interactive, on demand, and users are more inclined
to participate vs the classroom setting. It was decided that Whatsapp would be used for the
purpose of allowing medicine residents to become more confident in reading EKGs. Users or the
administrator would take a photograph of various EKGs and the users would respond with
analysis and discussion of those EKGs. Initially, there were concerns with regard to maintaining
HIPAA compliance. Even though Whatsapp messages are in fact encrypted between the phones
of the users and Whatsapp servers, it was decided for added security that no patient information
would be displayed on the images.
The group was started by the administrator on 3/5/2014 and it contained only PGY-1 residents.
Initially, the features of normal EKGs were discussed. The Admin would post up to 5 EKGs
during the course of the day and the residents would reflect on them when they were free to
respond. The atmosphere was relaxed and many the participants were eager to respond with
questions, observations and diagnoses. As the months went by, the residents became more and
more confident in reading the EKGs.
Quantitative/Qualitative Measures
A survey monkey survey containing 5 questions was distributed to the Whatsapp EKG group
chat to assess their option on this type of learning versus the classroom setting. Whether they are
more confident in reading EKGs and whether they are comfortable in teaching others how to
read EKGs. There are also free text sections where the residents can express specific likes and
dislikes, suggestions for improvement, and whether teaching in this method is worthwhile.
System Quality Review
174
NewYork-Presbyterian Healthcare System Quality Symposium 2014
Quality 2020: A Vision of the Future
Methodologies
A group administrator had started a whatsapp group chat and has control on the inclusion and
exclusion of members. A curriculum on teaching EKGs was designed by the administrator, who
is an attending Cardiologist that is very enthusiastic about teaching. Each member was educated
on the importance of privacy and instructed on the learning objectives. Group members not
following the rules would be eliminated from the group. The group chat allows for users to ask
questions, request topics of interest, and post images of EKGs. During the past 6 months we
have accumulated 50 PGY-2 & PGY-3 residents, who have been actively participating in these
group discussions throughout the day. Initially, normal EKGs were studied and then afterwards,
we began evaluating abnormal EKGs, which included arrhythmias, ischemic cardiac disease, and
many others.
Improvement Results
Over a 5 month period (March-July 2014) there were 470 messages, 67 of which contained
images (22 non EKG images).
Sustainability Strategies
In order for teaching and learning to be effective, it must be enjoyable, it must be interactive, and
it must be in a setting which makes it comfortable for active participation. There are some
professors and teachers who use the Socratic method of teaching, where people in a classroom
setting are called up randomly to answer questions. That could be an uncomfortable experience,
especially if you don't know the answer to the question. Using social media to teach and learn is a
relaxing yet engaging method of teaching in which members of the groups are more inclined to
participate.
Lessons Learned
1. Users are more inclined to participate in this type of learning environment
2. In the classroom setting, one's attention span is highest in the beginning and towards the end
of the class, therefore losing focus in the middle. That is not an issue with learning via social
media which is more interactive and can be studied at one's convenience.
3. The success and enthusiasm displayed by the participants suggest that this type of teaching
should be employed more often.
Conclusion
During the past 6 months, we realize that the residents were thrilled with this way of teaching.
They especially liked that it’s in real time, on demand, and users were immediately available to
answer their questions at their convenience. The most common questions concerned Atrial
Fibrillation and Arrhythmias. We will modify the curriculum and focus accordingly, based on
feedback from the residents. This is a great way to provide direct and indirect supervision in the
best interests of maintaining patient safety and quality.
System Quality Review
175
NewYork-Presbyterian Healthcare System Quality Symposium 2014
Quality 2020: A Vision of the Future
System Quality Review
176
NewYork-Presbyterian Healthcare System Quality Symposium 2014
Quality 2020: A Vision of the Future
New York Methodist Hospital, Department of Speech-Language
Pathology
NYM Dysphagia Screening: A Multidisciplinary Approach to Improving
Compliance
Luis F. Riquelme, Ph.D., CCC-SLP, BCS-S, Speech-Language Pathology/Neurosciences; Barbara Gatton, M.D.,
Emergency Medicine; Rebecca D. Benjamin, M.S., CCC-SLP, Speech-Language Pathology; Jonathan S. Muller, MBA,
Neurosciences; Joshua E. Teitcher, M.S., CF, Speech-Language Pathology; Waleed Mina, Cerner Corporation
Introduction
The purpose of this project was to ensure compliance with all procedures set forth for dysphagia
screening of patients with signs/symptoms of stroke presenting to New York Methodist Hospital
Emergency Department. This allows for reduced aspiration risk and increased patient safety,
upon compliance with appropriate PO status following the NYM dysphagia screening. Prior
performance improvement studies showed inconsistent compliance and action plans included
improved education to resident in the ED and the Acute Stroke Unit, as well as development of
electronic medical record data tracking and automatization.
Dysphagia has been reported to occur in 42-60% of patients with acute stroke within a median of
3 days from stroke diagnosis. Aspiration has been reported to occur in 38%-70% of this
population. Silent aspiration occurs in 40-67% of patients with dysphagia who aspirate. These
high numbers are of great concern because of the potential for airway obstruction, malnutrition,
aspiration pneumonia and subsequent complications.
At New York Methodist Hospital (NYM), the dysphagia screen is a protocol that includes
swallowing three sips of water from a cup. This approach was chosen based on emerging
literature support (Suiter & Leder, 2008). This screening is administered by the ER physician.
Several signs and symptoms following water sips are documented electronically, including clear
voice, absence of dysarthria, good voluntary cough and normal eating/drinking prior to arrival.
Upon passing the NYM Dysphagia Screen, the patient is placed on an oral diet and medications
are administered PO. If the patient fails, patient is placed NPO (including medications) and
referred to Speech-Language Pathology (SLP) for a clinical swallowing evaluation. Compliance
with such procedures is the focus of this study.
Quantitative/Qualitative Measures
All measures were obtained via retrospective chart review. A total of 350 charts qualified for the
study. Measures obtained included: candidacy for NYM Dysphagia Screen, compliance with
completion of the Screen, diet orders following the Screen and referral to Speech-Language
Pathology (SLP) when Screen was failed.
System Quality Review
177
NewYork-Presbyterian Healthcare System Quality Symposium 2014
Quality 2020: A Vision of the Future
Methodologies
Via retrospective chart review, all charts for patients admitted with neurological signs/symptoms
between April 2013 and April 2014 were analyzed. All patients who met the stroke criteria as set
forth by the NYSDOH/AHA Get with the Guidelines program were included (this does not
include patients under age 18, patients with complete recovery of all neurological deficits prior to
arrival, and strokes occurring after arrival to ED). A total of 350 patient charts were reviewed;
compliance with the NYM Dysphagia Screen, appropriate referral to SLP and appropriate diet
orders following screening were assessed.
Improvement Results
Data analysis for the 350 patients admitted with signs/symptoms of stroke to NYM from April
2013 to April 2014 revealed that 95% underwent the NYM Dysphagia Screen. Prior compliance
reports were in the 89-95% range. In addition, referrals to Speech-Language Pathology upon
failure of the Screen improved from 57% to 100% (see Table 1). Improvements noted are
directly related to operational changes that were instituted. These included increased physician
education, electronic tracking for compliance with screening and PO status and automatic
referrals to SLP upon screen failure.
Of an N=350, 66% passed and 34% failed the screen. 89% of patients who failed the dysphagia
screen were kept NPO, as per policy. Of patients who failed the screen, 76% were also referred
by physician for a Speech Pathology consult; in addition to the automatic referral (Table 1).
Interestingly, only 76% of patients were placed on PO diets upon passing screen; indicating 24%
of patients were kept NPO until Speech-Language Pathology consultation. This warrants further
analysis.
Sustainability Strategies
In order to sustain current compliance, ongoing physician training and electronic record tracking
needs to continue. New SLP policy includes generating a weekly report with information for
tracking screen failures and referrals received. If low compliance, contacting EMR and the
medical resident following the patient will be implemented.
(1) In addition, per low compliance for diet orders following screens, further analysis is needed to
determine appropriate plans of action.
(2) Referrals to Speech-Language Pathology upon failed screens will continue via electronic
medical records system.
(3) Compliance with conducting the Screen will be further supported via automatic
announcements in the electronic medical record system. Namely, the physician will be unable to
exit the patients' chart without completing electronic documentation for the Screen.
Lessons Learned
(1) Compliance with clinical protocols requires a multidisciplinary approach.
(2) Ongoing education and training of new personnel increases compliance.
System Quality Review
178
NewYork-Presbyterian Healthcare System Quality Symposium 2014
Quality 2020: A Vision of the Future
(3) Utilizing the support of the electronic medical record system allows for continued compliance
with protocols and procedures.
Conclusion
This data denotes excellent compliance with completion of the NYM Dysphagia Screen, as well
as excellent compliance with PO status orders upon completing the Screen. Great improvement
also noted in the appropriateness of referrals to Speech-Language Pathology for swallowing
assessment upon failure of the screen. Following systematic policy changes, 100% of screen
failures are now referred to SLP. Appropriateness of diet orders, following results of the Screen,
warrant further analysis. This may speak to the NYM dysphagia screening protocol itself, and/or
physician compliance with results. Improvement in compliance rates was judged to be significant,
and directly related to increased use of supports provided by the electronic medical record
system, and the institution of an ongoing physician education program. Action plans for prior
performance improvement projects in this area allowed for the greater focus on compliance and
charting support.
System Quality Review
179
NewYork-Presbyterian Healthcare System Quality Symposium 2014
Quality 2020: A Vision of the Future
Table 1
Dysphagia Screening Grid
Total screen eligible
Total screened
Passed
Failed
Referred to SLP upon
Failure
Not referred to SLP upon
Failure
Upon Failure, kept NPO
Placed on PO diets upon
Passing screen
Kept NPO upon Passing
screen
System Quality Review
Qtr 1: 2012
Qtr 3: 2013
Year:
74
67 (89%)
42 (75%)
14 (25%)
8 (57%)
51
48 (95%)
30 (63%)
18 (37%)
17 (94%)
350
350
221 (66%)
114 (34%)
114 (100%)
6 (43%)
1 (6%)
0 (0%)
N/A
N/A
N/A
N/A
113 (89%)
167 (76%)
N/A
N/A
54 (24%)
April 2013- April 2014
180
NewYork-Presbyterian Healthcare System Quality Symposium 2014
Quality 2020: A Vision of the Future
NewYork-Presbyterian Hospital
Using Information Technology (IT) to Facilitate Infection Prevention and
Control (IP&C) and Communication during a Measles Outbreak
Maria Messina, RN, BSN, CIC1; Lesley Covington, MSPH; CIC1; Barbara Ross, RN, BSN, CIC2; Melissa Stockwell,
MD, MPH3,4; Mariellen Lane, MD5; Diane Mangino, RN, MSN, CIC1; Nancy Schneider, RN, MS, CIC1; Krystal
Balzer, RN, MSN1; Lilibeth Andrada, RN, MA, CIC, PNP1; Lisa Covington, RN, MPH, CIC1; John D'agostino,
RN, MSN, CIC1; Patrice Russell, RN, MSN, CIC1; Jean-Marie Cannon, RN, BSN, CIC1; Rohit Chaudhry, MS6;
Steven Kaplan, MD7,8; Helen Lee, MD, MPH9; David P. Calfee, MD, MS, FIDSA, FSHEA10; Philip Graham III,
MD, Msc11; Lisa Saiman, MD MPH3,12; E. Yoko Furuya, MD, MS13,14
Introduction
Our multi-campus medical center responded to a rapidly evolving measles outbreak in New York
(NYC). We have >25,000 healthcare providers (HCPs) at 5 acute care facilities, 5 Emergency
Departments (EDs) with >275,000 annual visits and >1.8 million ambulatory visits. We describe
innovative uses of IT to facilitate communication for: 1) measles exposures 2) managing
suspected measles and 3) increasing vaccination.
Quantitative/Qualitative Measures
Outcome measures assessed included the number of unvaccinated children identified, contacted,
and vaccinated as well as the number of healthcare-associated Measles cases at our facility.
Methodologies
Having a surveillance system developed by a team which included an IP&C practitioner allowed
us to customize our processes to meet the specific needs of our organization during a Measles
outbreak. We focused on coordinating care throughout our healthcare system to enhance patient
safety. From 2/5/14 – 4/29/14, there were 26 cases of measles in NYC; we saw 13 (10 children,
3 adults; 4 months – 35 years). IT resources mobilized for our medical center response were:
intranet website for HCPs, IP&C's electronic surveillance system (EpiPortal), patient and HCP
electronic health records (EHR), linked immunization registries, and text messaging.
Improvement Results
We disseminated educational materials to HCPs via a measles intranet site. In response to
measles exposures, our immunization registry was synchronized with the NYC registry to assess
the vaccination status of 537 potentially exposed patients. Knowing that some of the 287
exposed patients with no/unknown immunity might return during their communicable periods
(CP), we configured an EpiPortal alert within the EHR for Airborne Isolation if exposed patients
returned (Figure). In all, 57 (20%) exposed patients returned during their CP (16 ED, 35
ambulatory, 6 inpatient). The HCP EHR identified 8 non-immune HCPs; all had medical
contraindications to vaccination. We created a measles order set in the patient EHR to prompt
System Quality Review
181
NewYork-Presbyterian Healthcare System Quality Symposium 2014
Quality 2020: A Vision of the Future
HCPs to order the correct tests and included hyperlinks to Department of Health specimen
forms. This order set was linked to EpiPortal, which can generate a list of tested patients to alert
IP&C of suspect cases. The hospital immunization registry identified 266 patients 12-72 months
old who had not received measles vaccination. We sent text messages asking these families to
return to have their child vaccinated urgently and providing walk-in hours; to date, 127 (48%)
have been vaccinated.
Sustainability Strategies
We have the flexibility to continually modify and update our electronic surveillance systems when
any new epidemiologically significant event arises. We maintain the ability to mine data, evaluate
effectiveness, and plan for future outbreaks. We continue to cultivate inter-departmental
relationships which facilitate our response to rapidly-evolving situations across the healthcare
system. We plan to continue our use of electronic communication to more efficiently reach our
patient population.
Lessons Learned
1) IT resources can be refined to increase patient and HCP safety by rapidly identifying
potentially infectious patients who require isolation.
2) Text messaging is an important IT resource that can be utilized to increase vaccination rates in
the community especially in an outbreak setting.
3) Harnessing IT resources early on in a rapidly-evolving outbreak situation maximizes the efforts
of the IP&C team.
Conclusion
Given the complexity of our medical center, IT resources were invaluable in communication and
implementing our comprehensive response. No healthcare-associated measles was identified.
Processes established during this outbreak can be modified for future outbreaks.
System Quality Review
182
NewYork-Presbyterian Healthcare System Quality Symposium 2014
Quality 2020: A Vision of the Future
System Quality Review
183
NewYork-Presbyterian Healthcare System Quality Symposium 2014
Quality 2020: A Vision of the Future
NewYork-Presbyterian/Lower Manhattan Hospital
Adjustment for Admission Source and Other Clinical/Demographic Factors
Does Not Abrogate the Disparate Effects of Dementia on Hospitalization
Discharge Disposition in Common Geriatric Admissions
William Liao, BA; Robert Y Lin, MD; Brian C Scanlan, MD
Introduction
Brief introduction & background:
Prevention quality indicators(PQIs) are a hospitalization based measures that identify quality of
care for "ambulatory care sensitive conditions"(ACSC). These are conditions for which highquality, community-based primary care, hospitalization for these conditions often can be avoided.
They thus can be used to provide a window into the community — to identify unmet community
health care needs, to monitor how well complications from a number of common conditions are
being avoided in the outpatient setting, and to compare performance of local health care systems
across communities.
Another concept in prevention quality relates to hospitalizations that could have been avoided
and by treatment in a nursing home, nursing home sensitive avoidable conditions(NHSAC).
However prevention quality indicators related specifically to NHSAC have not be formulated, as
of yet.
As dementia is a common diagnosis that results in nursing home care, we decided to examine the
several hospitalization diagnostic groups(including several PQI's) for the influence of dementia
on hospital discharge to nursing home. We hypothesized that certain hospitalizations prevalent
with dementia would be more likely to be admitted due to perceived nursing facility needs and
that this would be reflected in a greater predictive effect on discharge disposition. Such a finding
would point towards a prevention quality issue in specific diagnostic categories associated with
dementia.
Statement of the issue or problem:
Caring for dementia patients is most frequently performed in the outpatient setting. Institutional
care is often required with more advanced disease. Last year at this symposium, we presented our
findings that hospitalized patients with dementia, upon discharge, required further
institutionalized care (instead of being discharged home) in a differential pattern for certain
disease entities. We did not include adjustment for the admission source. We thus sought to
determine whether differential influence of dementia on discharge disposition remained after this
important adjustment. This effect was also examined in an enlarged number of hospitalization
categories, 12 disease related groups (DRGs), prevalent with dementia, using an updated dataset.
System Quality Review
184
NewYork-Presbyterian Healthcare System Quality Symposium 2014
Quality 2020: A Vision of the Future
Project goal(s):
The primary goal was to assess the adjusted predictor effects of a dementia diagnosis on hospital
discharge disposition in DRGs which have a high prevalence of dementia. The secondary goals
were to further categorize diagnosis related group hospitalizations which have a high prevalence
of dementia in the United States in the second millennium.
Quantitative/Qualitative Measures
The National Inpatient Sample (NIS) of the Healthcare Cost and Utilization Project (HCUP) is
funded by the United States (US) government's Agency for Healthcare Research and Quality
(AHRQ) and contains annual hospital discharge data from a stratified, random sample of
hospitals across the US. The twelve DRGs chosen were 79(respiratory infections and
inflammations)[non-CAP], 320(kidney & urinary tract infections age >17 with complications or
comorbidities [CC][UTI]), 141(syncope & collapse with complications, comorbidities)[syncope],
14 (intra-cranial hemorrhage and stroke with infarction)[stroke], 89(simple pneumonia & pleurisy
age >17 with CC)[CAP], 127(heart failure & shock)[CHF], 88(chronic obstructive pulmonary
disease)[COPD], 138(cardiac arrhythmias & conduction disorders)[arrhythmia], 316(kidney
failure)[AKI], 182(esophagitis/gastroenteritis age>17 with CC)[enteritis], 174(gastrointestinal
hemorrhage with CC)[GI bleed], and 296(nutritional and miscellaneous metabolic
disorders)[dehydration]. All hospitalizations of patients aged 65 or older for each DRG were
examined.
Methodologies
Most summary data generation and all logistic regression analysis were performed using SPSS for
Windows Version 13. Multinomial logistic regression was also performed to examine for the role
of dementia on discharge disposition with non-home no-expiration discharges as the reference
group(transfer to another institution). The predictor variables included the updated Charlson
comorbidities and gender. As all patients chosen were age 65 or older, the age Charlson predictor
variable was not part of the primary model. An alternative coding for dementia, included
Alzheimer disease(ICD9 331.0) in addition to the enhanced ICD9 coding algorithm(Quan et al).
Additional models added predictor variables: nursing home source of admission, decade of age,
calendar year, Medicaid or self-pay status(socioeconomic status), Medicare alone status, a coding
for a fall(E880-E888), using the published enhanced ICD9 dementia coding as well as the
expanded dementia algorithm which included Alzheimer’s disease hospitalizations added to the
Charlson comorbidity defined dementia hospitalizations. Regression analyses were performed
without race, as this was missing in a significant number of discharges.
Improvement Results
A significant positive time effect (negative binomial regression) was observed for dementia
proportions in all DRG’s except 79(non-CAP), 89(CAP), and 296(dehydration). When
Alzheimer’s disease hospitalizations were added to the dementia hospitalizations, trend
characteristics differed from the dementia alone hospitalizations in 5 DRG’s: 79, 89,
141(syncope), and 320(UTI). Nominal regression showed an adjusted odds ratio of less than 0.5
for dementia as a predictor of home discharge for all DRGs. For DRG’s 174(GI bleed),
88(COPD), 182(gastroenteritis), 138(arrhythmia), 127(CHF) and 89, the adjusted odds ratio was
System Quality Review
185
NewYork-Presbyterian Healthcare System Quality Symposium 2014
Quality 2020: A Vision of the Future
<= 0.25. This contrasted with DRG’s 14(stroke), 79 and 320 where the adjusted odds ratio was
>=0.40. Including additional covariates (including admission source) in addition to the Charlson
criteria resulted in odds ratios that were generally higher and had a better model fit, but had the
same relative order in terms of larger to smaller odds ratios for dementia effect. When
Alzheimer’s disease was added to the dementia category, the overall findings were similar. See
Table 1.
Sustainability Strategies
Dementia in particular was a significant negative predictor of home discharge, with stronger
negative effects(odds ratios) in certain DRGs. For example in DRG 174(gastro-intestinal
bleeding) the odds ratio for dementia in predicting home discharge was 0.19 (95%CI 0.19, 0.19),
whereas in DRG 320(urinary tract infection) the odds ratio was 0.40 (95%CI 0.41, 0.40). Thus the
adjusted likelihood of dementia patients being discharged home with gastro-intestinal bleeding
was less than half of that in dementia patients with urinary tract infections. The logical influence
of admission source did not abrogate this disparate effect on discharge disposition. We suggest
that looking at a given comorbidity’s predictive effect on home discharge may be a gauge of
ACSC and NHSAC. Furthermore, these findings suggest that greater financial support for SNF
admissions relating to dementia could reduce hospitalizations in certain diagnostic categories. The
concept of NHSAC as a prevention quality indicator needs to account for the level of financial
support that is provided for the particular condition. Without adequate financial support ,
governmental promotion of care provision in a non-hospitalized setting, particularly SNF's,
would only constitute an unfunded mandate.
Lessons Learned
1. The diagnoses CHF and COPD, as well as dementia, have been shown to have statistical
predictor effects for acute ambulatory care sensitive hospitalizations. ACSC and NHSAC relate
to hospitalizations that could have been avoided by care in their respective non-hospital settings.
2. The increasing dementia proportion in both CHF and COPD DRGs suggests that dementia
may be influencing the potential for avoidable hospitalizations in recent years.
3. CHF and COPD were 2 of the DRGs that had a stronger dementia predictor effect in not
being discharged to home in multivariate modeling especially when compared to the predictor
effects observed in DRG’s 79[respiratory inflammations], 320[UTI] and 14[stroke].
Conclusion
There is a possibility that patients with CHF and COPD were more likely (than DRG
79[respiratory inflammations] and 14[stroke] patients) to be admitted because they could not be
managed in a non-institutionalized setting and/or because they needed skilled nursing
facility(SNF) or long term custodial care. Medicare has targeted syncope in their recovery audit
program. DRG 141[syncope] was one of the DRGs in our study that had an intermediate
dementia predictor effect in not being discharged to home. These data also raise the possibility
that a certain proportion of syncope hospitalizations may have been driven by awareness to these
non-acute needs. In this present study dementia had the strongest effect on home discharge for
DRG 174[gastrointestinal hemorrhage], which has also been targeted by Medicare(CMS). There is
a dilemma for hospitals seeking to provide SNF/long term care to poorly functioning elderly
System Quality Review
186
NewYork-Presbyterian Healthcare System Quality Symposium 2014
Quality 2020: A Vision of the Future
patients who present to the hospital with no clear acute hospitalization indication. Current
Medicare policy disallows reimbursement for SNF transfer admissions unless preceded by a 3-day
acute care hospitalization. These hospitals face a dilemma of whether to admit patients and keep
them hospitalized for the requisite period of time in order to allow for SNF care to be provided
or to deny this option to patients by discharging them sooner (or not admitting them at all).
When medical necessity is inadequately documented or not present, this places hospitals at risk
for payment denial.
System Quality Review
187
NewYork-Presbyterian Healthcare System Quality Symposium 2014
Quality 2020: A Vision of the Future
DRG
DRG
descriptor
14
79
320
141
296
316
89
127
138
182
88
174
stroke
non-CAP
UTI
syncope
dehydration
AKI
CAP
CHF
arrhythmia
GI disorders
COPD
GI bleed
dementia with covariates
dementia
dementia hospitalizations only non-dementia hospitalizations
home discharge
likelihood
% Predicted
correctly
home discharge
likelihood
% Predicted
correctly
Home
Discharge(%)
Expired(%)
Home
Discharge(%)
Expired(%)
0.48 (0.47, 0.46)
0.47 (0.47, 0.46)
0.40 (0.41, 0.40)
0.35 (0.35, 0.34)
0.31 (0.31, 0.31)
0.29 (0.30, 0.29)
0.25 (0.25, 0.25)
0.24 (0.24, 0.24)
0.22 (0.22, 0.22)
0.22 (0.22, 0.22)
0.21 (0.22, 0.21)
0.19 (0.19, 0.19)
54.6
53.8
57.5
77.4
62.7
58.5
65.1
70.0
76.6
80.0
79.5
73.3
0.55 (0.56, 0.55)
0.51 (0.52, 0.51)
0.45 (0.45, 0.44)
0.38 (0.39, 0.38)
0.36 (0.36, 0.35)
0.35 (0.36, 0.35)
0.30 (0.30, 0.30)
0.30 (0.30, 0.30)
0.28 (0.28, 0.27)
0.27 (0.28, 0.27)
0.30 (0.28, 0.27)
0.24(0.24, 0.23)
58.2
56.1
59.7
77.5
64.0
59.2
66.1
70.0
76.8
80.1
76.8
73.2
25.5%
20.6%
34.1%
56.9%
33.8%
30.1%
31.7%
41.7%
45.2%
49.6%
47.7%
37.1%
8.6%
13.6%
2.0%
0.4%
4.0%
7.6%
7.6%
6.0%
3.2%
1.8%
2.3%
4.2%
38.8%
36.7%
55.8%
78.5%
62.4%
57.7%
65.1%
69.9%
77.2%
80.8%
79.7%
73.6%
10.7%
12.8%
2.0%
0.4%
3.7%
7.3%
4.8%
4.1%
2.4%
1.2%
1.8%
3.0%
System Quality Review
188
NewYork-Presbyterian Healthcare System Quality Symposium 2014
Quality 2020: A Vision of the Future
NewYork-Presbyterian/Weill Cornell Medical Center
Pre-screening of Diabetic Patient Visits to Improve Point of Care A1C
Utilization in an Outpatient Resident Practice
William Zhang, MD; Marcus Goncalves, MD, PhD; Amanda Carmel, MD
Introduction
We conducted a pilot quality improvement intervention using pre-visit planning by a nurse care
manager (NCM) to improve the efficiency of point-of-care hemoglobin A1C (POC A1C) testing
for diabetic patients at Weill Cornell Internal Medicine Associates (WCIMA).
In our resident practice, up to 50% of the POC A1Cs ordered are not resulted prior to case
presentation to the attending physician, thus discouraging many residents from utilizing this tool.
We aimed to increase the percentage of POC A1C tests resulted prior to the attending
presentation through multiple PDSA cycles over a 6 month period.
Quantitative/Qualitative Measures
The number of eligible patients receiving a POC A1C test and the test result times were evaluated
in the intervention and control groups. Qualitative data on residents’ views on the efficiency and
utility of the new POC A1C methodology were also collected.
Methodologies
A NCM reviewed residents’ next day schedules to identify patients meeting the following criteria:
1) a diagnosis of diabetes, 2) either the last Hgb A1C = 8 and not rechecked in the past 3
months, or no A1C checked in the past 6 months. Patients were added to a central list in the
electronic medical record. Either a dedicated A1C nurse or the NCM identified the listed patients
upon arrival to the clinic and performed the Hgb A1C testing prior to the beginning of the
medical visit. Result times were obtained from chart review of the electronic medical record
(EMR), and resident responses were obtained by survey. These were compared with a control
group of residents during the same time period.
Improvement Results
Summing over 4 PDSA cycles, 97% of the patients meeting the above criteria in the intervention
group vs. 55% in the control group had POC A1C testing (p = 0.008). 41% of the control group
who met criteria had serum A1C testing instead. 83% of the POC A1C tests resulted prior to case
presentation with the attending physician in the intervention group vs. 61% in the control group
(p < 0.001). Surprisingly, 71% of the providers in the intervention group felt that the POC A1C
result changed their management vs. 100% in the control group.
System Quality Review
189
NewYork-Presbyterian Healthcare System Quality Symposium 2014
Quality 2020: A Vision of the Future
Sustainability Strategies
Additional nurses will provide point-of-care testing, with the goal to ultimately include the entire
resident practice. Practice-changing sessions are being started to educate residents about POC
A1C testing and pre-visit planning in order to identify patients needing a POC A1C in advance of
the visit start time.
Lessons Learned
1. While our intervention increased the percentage of POC A1C tests resulted prior to the
attending presentation, such an “automated” approach may conflict with provider autonomy.
Pre-defined criteria for testing may not always be consistent with individual providers’ practice
habits.
2. Providers may need more education about the utility of POC A1C testing and pre-visit
planning for diabetic visits.
Conclusion
Pre-visit planning by a NCM for diabetic patient visits significantly increased the percentage of
diabetic patients who received POC A1C testing as well as the percentage of patients who had a
POC A1C result prior to case presentation with the attending physician. Additional changes are
ongoing to improve the efficiency of point-of-care A1C testing while still preserving provider
autonomy and patient ownership.
System Quality Review
190
NewYork-Presbyterian Healthcare System Quality Symposium 2014
Quality 2020: A Vision of the Future
NewYork-Presbyterian Hospital
Improving Fistula Rates in Chronic ESRD Patients at NYP
Anthony Valeri, MD; Robin Ferrer, MSN, MBA; Ronald Vilotta, BSN; Taknida D. Tubo, MS
Introduction
Project Description: Creation of a functioning Arterio-venous fistula (AVF) for hemodialysis
patients is crucial to minimizing complications in hemodialysis, specifically, to minimize the risk
of infections. Temporary dialysis access in the form of tunneled dialysis catheters carry a
significant increase risk of CLABSI (central line associated bloodstream infection). We sought to
reduce the number of patients using tunneled dialysis catheters for a prolonged period (> 90
days) and increase the number of patients with AVF as their permanent dialysis access. Patients
identified as requiring chronic hemodialysis treatment were referred as soon as possible for vein
mapping by USG to identify the best sites for AVF creation in consultation with a peripheral
vascular surgeon to schedule AVF surgery as soon as possible. Patients were educated on the
need for prompt creation of AVF to minimize the risk of infection. We face a unique challenge
because of a high turnover rate of our patients being transferred to chronic outpatient dialysis
facilities once stabilized. We monitored the prevalence rates of tunneled dialysis catheters and
AVF in our chronic outpatient hemodialysis population.
Quantitative/Qualitative Measures
As reported in the Dialysis Facility Reports produced by the University of Michigan Kidney
Epidemiology and Cost Center (July 2011, July 2012, July 2013 and July 2014), the arterial venous
fistula (AVF) rates at our outpatient dialysis facility improved from 36.9% in 2011, to 44.7% in
2012 and further to 52.7% in 2013, compared to the national averages of 58.9%, 60.5% and
61.8% respectively.
Tunneled dialysis catheter (TDC) rates favorably decreased within the same time period at our
facility from 45.9% in 2011 to 42.2% in 2012 and to 33.2% in 2013. The national averages for
TDC within the same time periods were 21.1%, 19.7% and 19.1% respectively.
Under the Fistula First Initiative, CMS has set a national goal of 68% of prevalent hemodialysis
patients receive treatment by fistulas. Our ESRD network mandated an interim 52.31% achieved
by September of 2014 based on our baseline prevalence rates, acknowledging that time was
needed to achieve the targeted rates. We have exceeded that target and our YTD average fistula
rate for 2014 at the time of this abstract submission is 66.6%.
System Quality Review
191
NewYork-Presbyterian Healthcare System Quality Symposium 2014
Quality 2020: A Vision of the Future
Methodologies
To promote improved patient outcomes, our team encouraged and pro-actively facilitated
patients having consultations with a vascular surgeon, vein mapping by Ultrasound, getting the
earliest appropriate operating room schedule time, educated patients on the risks and benefits of
each vascular access type, and provided educational materials and literature in both English and
Spanish.
Improvement Results
As illustrated, since 2011, we have observed a favorable increase in the percentage of patients
that receive hemodialysis using arterial venous fistulas in each year from 2011 to 2014 as well as a
complementary favorable reduction in the use of tunneled dialysis catheters.
Sustainability Strategies
To sustain and improve on the achievements outlined in this abstract, we have continued and
intend to improve the staff communication and patient education about the benefits of fistula use
on patient outcomes; continue monitoring for evidence of improving trends in fistula use,
continue staff education on fistula care to reduce the occurrence of access dysfunction, identify
and refer chronic patients for vascular surgery consult, vein mapping and operating room times
as soon as possible.
Our observation of a continuing favorable trend is supported by internal data on chronic ESRD
patients in the months that follow the December 2013 data points of the 2014 Dialysis Facility
Report. In 2014, the percentage of patients using AVF from January through August are 59.3%,
61.9%, 55.0%, 72.7%, 60.9% 65.4% and 83.0%.
Lessons Learned
We have learned that 1) communication and patient education is a critical component in
understanding why patients choose an access type and is necessary before overcoming barriers to
patient consent for fistula placement, 2) vein mapping by ultrasound, is beneficial in achieving
high rates of successful fistulae creation, and 3) early appointment with vascular surgeons reduces
delays in fistula placement.
Conclusion
Conclusion: Early referral for vein mapping, vascular surgery consultation and patient education
can have a significant impact on reducing chronic dialysis catheter rates and increasing AVF rates
which, in turn, can reduce the risk of serious infections.
System Quality Review
192
NewYork-Presbyterian Healthcare System Quality Symposium 2014
Quality 2020: A Vision of the Future
NYPH/CU Dialysis Arterial Venous Fistula
Rates
70
% of Patients with AVF
60
50
40
30
NYP/CU Arterial Venous
Fistula Rates
20
National Average Arterial
Venous Fistula Rates
10
0
2011
2012
2013
Data Source:Dialysis Facility Reports
University of Michigan Kidney Epidemiology
and Cost Center
System Quality Review
193
NewYork-Presbyterian Healthcare System Quality Symposium 2014
Quality 2020: A Vision of the Future
NYP/CU Dialysis Tunneled Dialysis Catether
Rates
50
45
% Patients with TDC
40
35
30
25
NYP/CU Tunneled Dialysis
Catheter Rates
20
15
National Average Tunnel
Dialysis Catheter Rates
10
5
0
2011
2012
2013
Data Source:Dialysis Facility Reports
University of Michigan Kidney Epidemiology
and Cost Center
NYPH/CU Dialysis Arterial Venous Fistula Rates
January - July 2014
90.0
% of Patients with AVF
80.0
70.0
60.0
50.0
40.0
Arterial Venous Fistula Rates
January - July 2014
30.0
20.0
Linear (Arterial Venous Fistula
Rates January - July 2014)
10.0
0.0
Jan
Feb March April May June July
Aug
Data Source: NYP/CU Dialysis Department
System Quality Review
194
NewYork-Presbyterian Healthcare System Quality Symposium 2014
Quality 2020: A Vision of the Future
NewYork-Presbyterian Hospital
Improving Efficiency by Automating Data
Elsie Binns-Irizarry, MS; Scott W. Possley, PA-C, MPAS; Peggy Liu, MS, RN; Brian Regan, PhD; Vanessa Cheng;
Hillary Shaw, MPA; Sarah Walker, MBA; Karthik Natarajan, PhD; Nicole Hitti, MSN; Linda Georges, BSN
Introduction
The tracking and reporting of Core Measures requires dedicated staff to manually abstract the
information from patient charts. As the number of Core Measures continues to increase,
hospitals are under immense pressure to automate the process of obtaining quality clinical data in
an efficient and timely manner. The challenge is that much of the information needed to review
cases for compliance resides in an unstructured (free text) format. Through the use of analytic
technology and the development of structured fields, hospitals can streamline the abstraction
process in order to shorten the time spent on researching and analyzing data when investigating
cases. Even partial automation of measures can reduce abstraction time by half.
In addition to Core Measures, NewYork-Presbyterian Hospital has nineteen distinct registries,
databases, and regulatory reports that have the potential for either full or partial electronic
abstraction. Allocation of expert staff to ensure understanding and compliance with the measures
is a constant challenge. If data abstraction is automated, the organization may see significant
savings in time, money and effort.
Quantitative/Qualitative Measures
A multidisciplinary committee (including Quality & Patient Safety, clinicians, IT, and
administrative leaders) met weekly to discuss what information was needed to analyze compliance
for each measure and where that information was located within the electronic medical record
(EMR). Upon review, the committee was able to move four measures to automated abstraction
through the use of structured fields.
Changes to structured notes used by clinicians went live on January 1, 2014. Random audits were
conducted to determine if the new structured fields were being used. These audits exposed
inconsistencies, which led the committee to make additional changes to the structured fields.
The data for each measure is uploaded into our abstraction software, reducing the need for data
entry. The committee reviews cases that have not passed per CMS rules to validate the outcome
and determine if documentation improvement is needed. The committee will continue to
monitor and make changes to documentation and educate providers as needed.
Improvement Results
A total of 411 charts were uploaded between March and July. (figure 1)
75% of the data was automatically obtained. (figure 1)
System Quality Review
195
NewYork-Presbyterian Healthcare System Quality Symposium 2014
Quality 2020: A Vision of the Future
25% of cases needed to be manually abstracted from multiple notes. (figure 1)
The most common problem was obtaining the parity element from the NYP/Cornell medical
record. The number of cases needing manual abstraction dropped in June upon identifying
another location to extract the parity element.
Some additional issues revolve around physician documentation not being consistent across
campuses. Standardizing documentation across sites will be a key initiative in the next few
months.
The committee expects to be successful in automating the data to facilitate compliance with
documenting the information needed and ensure the capability of creating reports to
automatically compile the information and ease the data quest. If so, this will lead the way to
improving documentation in other areas in which manual abstraction of data is currently the only
option.
The committee expects to save a minimum of four full-time employees (FTE’s) with automation.
These staff members will be re-directed to performance improvement initiatives on patient care
units and concurrent case reviews.
Conclusion
The number of mandatory publicly reported quality indicators and initiatives are growing rapidly.
Using information technology to automate the collection and abstraction of quality clinical data
can potentially benefit hospitals financially. Automating data abstraction and using structured
fields can provide hospitals with the ability to monitor all quality measures and troubleshoot
issues in real time. Expanding this process to other quality measures can free skilled staff
(including nurses) from administrative tasks and provide more time to ensure patient care
remains the focal point.
Although little has been reported on using automation to improve quality clinical data, it can give
hospitals better access to information in a less burdensome and timely manner while at the same
time ensuring that data is a tool used for decision and support and not a hindrance.
We have also identified opportunities to work with electronic health record vendors to include
common metrics in their products and to anticipate the expanding burden of chart abstraction
for quality and regulatory purposes.
System Quality Review
196
NewYork-Presbyterian Healthcare System Quality Symposium 2014
Quality 2020: A Vision of the Future
System Quality Review
197
NewYork-Presbyterian Healthcare System Quality Symposium 2014
Quality 2020: A Vision of the Future
Poster Presentation
NewYork-Presbyterian/Columbia University Medical Center
Improving E-Prescribing Rates at Broadway Practice: a Resident-led QI
Project
Jessica George, MD; Laura Robbins-Milne, MD; Mariellen Lane, MD
Introduction
With the growing capabilities of electronic health record technology, health care providers can
harness new advances to deliver better care to patients. E-prescribing has been shown to improve
patient care through many avenues. Particularly important in pediatrics, where dosing errors are
the most common medication error, e-prescribing is associated with decreased error rate.
Electronically submitting prescriptions directly to the pharmacy eliminates the need for the
pharmacist to manually enter prescription details, and avoiding this step has been shown to nearly
halve the risk of dispensing errors. When a prescription is electronically submitted, a direct line of
communication with the pharmacist is opened, allowing for immediate clarification of details
such as dose, route, and indication. It also allows easy communication regarding generic
substitutions, and avoiding higher co-payments can improve medication adherence. Patient
satisfaction and adherence is also improved by eliminating the step of dropping off a paper
prescription to be filled. E-prescribed medications are acknowledged by the pharmacy often
while the patient is still in the office, and the prescription can be picked up directly after the
appointment. E-prescribing has also been shown to improve practice efficiency. Time waiting to
print and sign prescriptions is saved, chronic medications can be readily renewed, and alternate
providers within the practice can more easily send refills or new prescriptions on patients for
whom they are not the primary provider.
In addition, e-prescribing is a Core Measure of the Centers for Medicare and Medicaid's
Meaningful Use for Eligible Professionals Incentive Program. The objective of Meaningful Use is
to use electronic health record technology to improve quality and safety of patient care and
reduce health disparities, ultimately leading to better clinical outcomes. At the time of our study,
Core Measure four called for 40% of all permissible prescriptions to be electronically prescribed.
E-prescribe rates for Broadway Clinic providers were calculated from the period of July 1, 2013
to the end of August 2013. The resident e-prescribe rate was 45%, with a range from 0 to 80%,
and the attending rate 51%, with a range of 39 to 83%, for an overall e-prescribing rate for
Broadway Clinic of 48%. Though initial rates were above the goal set for Meaningful Use, the
benefits to the patient when medications are electronically transmitted suggest that the large set
of patients who are provided paper prescriptions are getting substandard care. We sought to close
this gap by improving our e-prescribing rates via a resident-led quality improvement project
spanning the academic year. Residents at Broadway Clinic developed monthly Plan-Do-Study-Act
(PDSA) cycles using the Model for Improvement.
System Quality Review
198
NewYork-Presbyterian Healthcare System Quality Symposium 2014
Quality 2020: A Vision of the Future
Our AIM statement was to increase the rate of e-Prescribing to 75% among all providers at the
Broadway Clinic by the end of the academic year, June 2014. Our secondary AIM was to increase
the percentage of patients with preferred pharmacies entered to more than 70% from a baseline
of 41.9%.
Quantitative/Qualitative Measures
Quantitative measures: E-prescribe rates were measured during monthly PDSA cycles
throughout the year. By the end of the academic year, June 2014, the e-prescribe rate was 71.5%
for the clinic, up from 48%. Percentage of patients with a preferred pharmacy entered was used
as a process measure. By the end of the project, 80.7% of patients had a preferred pharmacy
entered, up from 41.9%. See graph 1 for an overview of specific interventions and subsequent
changes in percentage of patients with a preferred pharmacy. Provider report cards with
individual e-prescribe rates were given to all residents and attendings.
Qualitative measures: Pre and post surveys were given to parents in the waiting room. Presurveys revealed few parents knew about e-prescribe but felt it would be a good option. Postsurveys showed that parents both knew about e-prescribe and preferred it to paper prescriptions,
with common remarks being “It’s easier”, “It’s faster”, and “I used to lose the paper ones”. Pre
and post surveys were also given to providers. 50% of providers felt e-prescribing was faster than
paper scripts in our provider post-survey, compared to only 35% in the pre-survey.
Methodologies
To improve e-prescribe rates, a resident led year-long project was initiated using the Model for
Improvement. Monthly PDSA cycles were done to implement and track progress towards our
goal. QI principals applied include:
1. Addressing systems and processes: Barriers to e-prescribing were identified through provider
surveys. Subsequent changes were geared towards making e-prescribing more efficient, including
changing the Televox message to remind patients to bring pharmacy info to appointments and
creating a streamlined reporting process for errors and technical problems with the EHR. 2.
Focus on patients: The literature shows that e-prescribing has been shown to reduce medication
errors. Patients were surveyed in the waiting room to gauge satisfaction with e-prescribe. 3.
Engaging the team: Patient financial advisors, medical assistants, and nurses were taught to enter
preferred pharmacies, a step which was then incorporated into the patient registration and refill
request processes. Residents led the project with attending supervision. 4. Using data as a
measure of change: Monthly PDSA cycles measured preferred pharmacy rates. Providers were
given report cards of their e-prescribe rates.
Improvement Results
The clinic e-prescribe rate by the end of the academic year was 71.5%, close to the AIM
statement goal of 75%.
The range of resident e-prescribe rates was 23-100% and the range for attendings was 50-84%.
The percentage of patients with a preferred pharmacy entered was a process measure. This
number was measured using monthly one-week chart reviews, which is reflected in the annotated
run chart (graph 1). Report cards with individual provider rates, given to both attendings and
System Quality Review
199
NewYork-Presbyterian Healthcare System Quality Symposium 2014
Quality 2020: A Vision of the Future
residents, resulted in an increase in preferred pharmacies entered. Attending report cards were
sent in September, with preferred pharmacy rates then increasing from 49.5% to 54%. Resident
report cards were sent in November, rates improved from 49% to 61.2%. After the complete
team was involved in the project and taught how to enter preferred pharmacies in January, rates
increased from 65.2% to 74%. However, a gradual decline is noted starting in February. At this
point, the run chart (graph 1), completed through March, was posted throughout the clinic
showing our progress with a line marking our AIM statement goal. Maps of commonly used
pharmacies were also posted in providers’ rooms. Rates of preferred pharmacies entered then
sharply increased to our final year-end rate of 80.7%. Resident e-prescribe rates were compared
across all ambulatory care network pediatric clinics in March 2014, with Broadway Clinic having
the highest rate at 65%, compared the other clinics, whose rates were 39 to 44%. Higher eprescribe rates were also associated with higher levels of training. At the end of the project,
attendings had the highest e-prescribe rate, meeting the AIM statement goal at 76%. First year
residents had the lowest rates at just over 50% and third year residents had numbers approaching
those of the attendings, nearing 75%.
Sustainability Strategies
Roughly 81% of patients have preferred pharmacies entered, making e-prescribing easier and
more efficient. Nurses, medical assistants, and patient financial advisors now enter a pharmacy
when registering a patient or taking a patient call for a prescription refill request. A preferred
pharmacy column was created on the patient list in the EHR so ancillary staff can easily see if a
patient has a pharmacy entered without extra clicks. The Televox messaging system was changed
to remind patients to bring their pharmacy information to appointments. Posted pharmacy maps
make it easier to quickly look up and enter a pharmacy. Resident and attending report cards keep
physicians informed of their individual e-prescribe rates and the clinic’s overall rates, providing
an impetus to continue to e-prescribe. There was also a meeting with the medical directors of the
other ambulatory care network clinics, and didactics on the benefits of e-prescribing and how to
enter a preferred pharmacy, as well as the maps of common pharmacies in the area, were shared.
Residents at all clinics will now be receiving e-prescribe report cards. A streamlined process for
reporting technical issues, i.e. transmission failures and inactivated e-prescribe accounts, as
created.
Lessons Learned
Many of our preconceived barriers to e-prescribing were challenged throughout the project.
1. Though we thought patients would not know their pharmacy, the vast majority had their
information on hand, and for the few who did not, our pharmacy maps were very helpful.
2. We assumed patients would prefer paper prescriptions, but waiting room surveys indicated that
many find e-prescribe faster and easier. It omits the added time of dropping off the prescription.
Electronically sending the prescription also avoids the step of the pharmacist copying
prescription information into the computer, eliminating an opportunity for human error.
3. E-prescribing can be faster and more efficient than printing prescriptions when a system is in
place that makes e-prescribing an integrated part of work flow and allows for smooth error
reporting and resolution.
System Quality Review
200
NewYork-Presbyterian Healthcare System Quality Symposium 2014
Quality 2020: A Vision of the Future
Conclusion
Electronic health record technology should be used to improve patient care and satisfaction and
help to create a more efficient work flow in the ambulatory setting. A resident-led and teambased quality improvement project can drive change and help meet meaningful use goals for
hospital based eligible providers. By making gradual changes over time using the Model for
Improvement, systems changes can be put into place to close gaps in care. Before implementing
interventions, barriers to reaching patient care goals need to be assessed and can then guide
interventions. The interventions of this project revolved around education, access, and feedback.
Providers were educated on the rationale and literature supporting e-prescribing, promoting
provider buy-in for our AIM statement goal. Using a team base approach, patient financial
advisors, medical assistants, and nurses were educated on how to enter a patient's preferred
pharmacy. Access to information was provided by increasing the percentage of patients with
preferred pharmacies entered, posting maps of commonly used pharmacies, and reminding
patients via the Televox messaging system to bring pharmacy information to their appointments.
Feedback was given through both provider report cards and by posting the run chart outlining
the year's progress throughout the clinic. This provided an impetus to residents and attendings to
continue to e-prescribe. At 71.5%, e-prescribe rates at Broadway Clinic are now higher than the
Meaningful Use goal of 40% and are close to our AIM statement goal of 75%. Higher e-prescribe
rates have resulted in improved patient and provider satisfaction and increased efficiency in our
clinic's work flow.
System Quality Review
201
NewYork-Presbyterian Healthcare System Quality Symposium 2014
Quality 2020: A Vision of the Future
Percent of patients with preferred pharmacy
Preferred Pharmacy Rates by Date
90
80.7
80
74
70
61.2
60
50
40
49.5
10
49
41.9
30
20
54
Attendings
given report
cards on
ePrescribe
rates
0
1. Providers, nurses
and PFAs trained on
ePrescribe
2. Instructions on
how to enter
preferred pharmacy
hung at nurse and
PFA cubicles
65.2
1. Didactic to
providers on
how to write
prescriptions
2. Resident
report cards
through
August sent
MAs
trained
how to
enter
pharmacy
info
Resident
report
cards
from
Nov-Dec
sent
70.7
Goal
65
All
resident
eRx
working
1. Run chart
posted in provider
work rooms
2. Pharmacy lists
created and
posted throughout
clinic
Date range
System Quality Review
202
NewYork-Presbyterian Healthcare System Quality Symposium 2014
Quality 2020: A Vision of the Future
Poster Presentation
NewYork-Presbyterian/Weill Cornell Medical Center
Quality Improvement in Prostate Biopsy Fixation: Facilitation of Systems
Review by Interdisciplinary Housestaff Council
Ashley G Winter, MD; Paul J DiMaggio, MD; Ian R Drexler, MD; Zachary A Turnbull, MD; Susan L Faggiani, RN
BA CPHQ; Gregory E Kerr, MD MBA FCCM, Brian D Robinson, MD
Introduction
Adequate specimen fixation is critical to the appropriate histologic interpretation of prostate
biopsies. Sub-optimal fixation processes may lead to artifactual nuclear "halos," smudged nuclei,
indistinct cellular boundaries, and stromal retraction, among other findings. While the fixation
process begins in the urologic procedure suite, the effects of fixation artifact are only first
observed by the interpreting pathologist.
Pathologists recognized under-fixation artifact from the prostate biopsies at one urology practice
site, indicating a potential site-specific aberration in specimen processing. Interdepartmental
collaboration initiated through a quality-focused interdisciplinary group (Housestaff Quality
Council-HQC) sought to "bridge the gap," in specimen collection, processing, and interpretation.
The goal was to improve specimen fixation, accuracy of diagnosis, and ultimately patient care.
Quantitative/Qualitative Measures
Qualitative measures included independent, blinded, pathologic review of biopsy fixation quality.
Quantitate measures included percentage of adequately-fixed biopsy specimens over defined time
periods.
Methodologies
Hypothesis generation through independent review of clinical results.
On-site vetting of clinical processes.
Revision of clinical processes based on hypothesis-testing and institutionally generated data.
Interdisciplinary-patient safety minded collaboration.
Improvement Results
To identify a potential practice-site specific aberration in prostate biopsy fixation, all prostate
biopsies performed over the one-month period of April 2014 were reviewed by a pathologist
blinded to practice site. It was noted that 100% of under-fixed specimens originated at a single
practice site ("Site 1").
Procedures for biopsy fixation were then analyzed at various sites via walk through with
technicians, nurses, and practice managers. Procedural review highlighted use of sterile water
System Quality Review
203
NewYork-Presbyterian Healthcare System Quality Symposium 2014
Quality 2020: A Vision of the Future
during initial specimen processing (site 1 only). Hypotonic solutions, such as sterile water, may
interfere with formalin fixation, and immediate revision of processes at Site 1 was recommended.
Biopsy fixation procedures at Site 1 were immediately revised to utilize normal saline instead of
water. Data on quality of biopsy fixation was then prospectively collected over a one month
period. Percentage of specimens with adequate fixation improved significantly following
implementation of normal saline use (18.2% pre- vs 100% post- intervention, respectively p<
0.0001).
Sustainability Strategies
The revision of departmental policies following this intervention is highly sustainable. All
practicing technicians have been educated to use normal saline, and the change has been
formalized in departmental procedures. Furthermore, the cost differential is negligible.
It is expected that these changes will become the new-standard of care, with permanent benefits
to quality of prostate biopsy histologic specimens and patient care.
Lessons Learned
1. Interdepartmental communication can lead to rapid hypothesis testing of institutional
procedures and facilitate formalized improvement processes.
2. Use of normal saline (instead of sterile water), during initial prostate biopsy processing lead to
improvement in quality of tissue fixation.
3. Cross-disciplinary, quality-focused organizations may provide further groundwork for similar
projects.
Conclusion
Normal saline may be used during initial processing of prostate biopsy cores without
compromise to quality of histologic review. Changes in biopsy fixation protocol were easily
instituted and highly sustainable. Interdisciplinary, quality-focused organizations should be
utilized for devising and instituting meaningful improvements in patient care.
System Quality Review
204
NewYork-Presbyterian Healthcare System Quality Symposium 2014
Quality 2020: A Vision of the Future
NewYork-Presbyterian/Weill Cornell Medical Center
Keeping it Safe: A Multidisciplinary Approach to Creating a Culture of Safety
Barbara Alba, PhD(c), RN-IBCLC; Sara Pasciolla, RNC, MSN-Ed; Sharon Abramovitz, MD, Co-Director, Obstetric
Anesthesiology; Jeffery Jacinto, Manager, Quality and Patient Safety
Introduction
Problem Statement:
At New York Presbyterian-Weill Cornell Medical Center, potentially unsafe behaviors and
conditions had been observed, but had not always been openly identified or corrected in a timely
fashion. A root cause analysis conducted with nursing and obstetrical staff identified various areas
for improvement, including a perceived punitive culture with fear of retaliation, lack of a formal
process for review and feedback of reported events, and an inconsistent use of events reporting
system. Staff also identified a need for greater support in an environment where unsafe behaviors
had become integrated within the culture due to a constellation of factors.
Project Aim:
Once the problem had been identified, the team recognized the need to consider options for
correcting the deficits described above and change the culture. Recognizing that multiple points
of intervention may be required due the complexity of multidisciplinary teamwork, buy-in from
senior leadership would be imperative to its success.
Initially utilizing in-house resources, the adoption of TeamSTEPPS was nurtured by the Director
of Obstetrics, Co-Directors of OB Anesthesiology, and OB Safety Nurse who became the first
master trainers for the department. The team identified cases where communication deficits
effected teamwork and jeopardized patient care. Using master trainers and the support of the
Chairman of Obstetrics, Vice President of Specialty Services and others, one of the first
obstetrical debriefs was held. It was here that the entire team was able to recognize the need for
this framework of communication and teamwork to gain traction.
Goal:
The goal was the successful implementation of an innovative program to improve the culture of
safety within the obstetrical unit. Using TeamSTEPPS as a basis, the obstetrical team
transformed a less safe working environment into a safer, more efficient practice.
Quantitative/Qualitative Measures
Team performance is measured on three levels; attitudes, processes, and outcomes. The initial
AHRQ survey, conductedto evaluate the obstetric departments identification (attitudes) of their
culture of safety ideals, was conducted in March of 2012 to set a baseline for the unit. This
AHRQ survey is conducted every two years with six month pulse checks. The original medical
System Quality Review
205
NewYork-Presbyterian Healthcare System Quality Symposium 2014
Quality 2020: A Vision of the Future
events reporting system, MERS, was replaced in July of 2013 with KEEPSAFE, a best-in-class
incident management reporting system. TeamSTEPPS training was required for all staff within
the obstetrical area. This addressed the process level along with quantification of debriefs taking
place amongst the department. Outcomes were best measured by a monthly updated
TeamSTEPPS dashboard where near misses, wet taps, hemorrhages, unplanned term NICU
admissions, cesarean sections, and on time starts would be discussed.
Methodologies
Three principal strategies were used to guide the culture of safety program. The first strategy was
the development of Senior Administrative Safety Sessions (SASS). These monthly meetings with
frontline staff, providers, management and senior nursing administration were conducted to
assess the safety concerns, challenges, and to brainstorm possible solutions. Led by the obstetrical
safety nurse, these meetings provide a safe, non-judgemental, non-punitive environment for the
entire obstetrical team to report events, near-misses, and ways to improve practice and patient
care. Next, New York Presbyterian adopted KEEPSAFE as part of the hospitals ongoing
initiative to achieve a high reliability culture and to provide the safest environment for the
patients. Finally, based on a Joint Commission Sentinel Events Report, NY Presbyterian
embraced TeamSTEPPS, which was implemented in the obstetrical area in 2013. TeamSTEPPS
is an evidence-based system for health care professionals that works to improve communication,
patient safety, and high-performance teamwork.
Improvement Results
Once staff had the background understanding, leadership from the nursing, obstetrics, and
anesthesia teams were able to better promote the use of these tools, including multidisciplinary
morning and evening briefs, huddles, debriefs, creating a general non-punitive, transparent
department. Here anyone can speak up, anyone can "stop the line" and a listening environment is
fostered. At the same time, a new electronic event reporting system was rolled out.
Increases in the evaluation of safety metrics over a two year interval were noted in four domains
of a Culture of Safety survey. When patient safety issues or events are identified and reported to
leadership, staff response realized (a) 6% increase in feeling their issues were heard, (b) a 14%
increase in feeling that action was taken to address the event, (c) a 13% increase in feeling the
action taken/planned in response prevented future harm or similar events from occurring, and
(d) a 17% increase in feeling feedback and communication about the event is given.The
evaluation of patient safety culture and of staff knowledge, skills, and attitudes to teamwork and
communication indicated a significant improvement in two dimensions: frequency of events
reporting and organizational learning (TeamSTEPPS), requiring engagement at all levels.
There has been a 45% increase in incident reporting. More than 450 obstetrical staff have been
trained in the TeamSTEPPS modalities over the last two years. This is approximately 85% of the
entire labor and delivery and post-partum departments including more than 10 disciplines
(nursing, OB, anesthesia, pediatrics, nutrition, security, clerks & registrars, patient care assistants,
scrub technicians, etc.)
System Quality Review
206
NewYork-Presbyterian Healthcare System Quality Symposium 2014
Quality 2020: A Vision of the Future
Sustainability Strategies
Sustainability will be maintained through ongoing education in TeamSTEPPS along with direct
mentoring by OB leadership who will stimulate teamwork and communication. Second,
continued systems for reporting and analyzing adverse events through use of KEEPSAFE will
prompt a means to reduce safety issues. Third, continued monthly SASS rounds will provide a
forum for ongoing identification and evaluation of safety concerns and issues. These will also
provide a means of "closing the loop" on events with a goal of improving outcomes and
providing systems for quality and safety improvements. Finally, positive team behaviors will
continue to be recognized and reinforced in group forums including, brief, debriefs, and huddles.
Lessons Learned
1. To maintain a safe working environment for all, staff members need to constantly strive to
improve the culture of safety by improving communication and mutual support across all
disciplines.
2. Setting clear behavioral guidelines for all members of the OB team is necessary.
3. Team members should not fear that speaking up will undermine their working relationships
and create conflicts. Staff now know how to bring up their concerns in ways that are respectful,
constructive, and promote problem solving with minimal defensiveness.
Conclusion
Implementation of the above methodologies has provided a substantial impact on the culture of
safety, teamwork, and communication within the obstetrical area. It has encouraged a culture of
learning from patient safety incidents and provided continuous opportunities for improvement in
clinical practice. Recognizing that this is a day-to-day process with daily mentoring by leadership,
the obstetrics department has made huge strides as witnessed by the multidisciplinary briefings,
the successful SASS rounds, and the success in entering KEEPSAFES. We are continuously
monitoring outcome measures to look for improvements.
System Quality Review
207
NewYork-Presbyterian Healthcare System Quality Symposium 2014
Quality 2020: A Vision of the Future
System Quality Review
208
NewYork-Presbyterian Healthcare System Quality Symposium 2014
Quality 2020: A Vision of the Future
System Quality Review
209
NewYork-Presbyterian Healthcare System Quality Symposium 2014
Quality 2020: A Vision of the Future
System Quality Review
210
NewYork-Presbyterian Healthcare System Quality Symposium 2014
Quality 2020: A Vision of the Future
System Quality Review
211
NewYork-Presbyterian Healthcare System Quality Symposium 2014
Quality 2020: A Vision of the Future
System Quality Review
212
NewYork-Presbyterian Healthcare System Quality Symposium 2014
Quality 2020: A Vision of the Future
Poster Presentation
NewYork-Presbyterian/Morgan Stanley Children's Hospital
"Clean It Like You Mean It" A three ICU Collaborative on Central Line
Associated Bloodstream Infection Prevention
Svetlana Streltsova, RN, MSN, CCRN; Kathy Lee, RN, BSN, CCRN; Regan Amanda Morimoto, RN, CCRN;
Myrlene Madelon, RN, MSN, CCRN
Introduction
For the neonatal and pediatric intensive care settings, does continuous education sessions, central
line maintenance protocol and weekly surveillance by nurse champions, reduce the incidence of
central line associated blood stream infections?
The “Clean It Like You Mean It” campaign is a collaborative initiative shared amongst the
Neonatal, Pediatric, and Pediatric Cardiac Intensive Care Units. The team utilizes evidence based
best practice to prepare hospital nurses with the knowledge, skills, and practice guidelines to
reduce and maintain low incidence of central line associated bloodstream infections (CLABSIs).
The goal for this initiative is to decrease the morbidity associated with CLABSIs in our patient
population, reinforce and improve best practices, decrease hospital overall cost, and hospital
length of stay associated with central line infections.
Continued education strategies included education and practice validation through return
demonstration on central line maintenance and care, dressing changes, line changes, scrubbing
the hub, chlorhexidine baths, and use of alcohol impregnated caps on needleless ports. CLABSI
prevention education occurred in groups and in one-on-one sessions. The team conducted
weekly central lines surveillance within each of the units assessing sites, lines, dressings, the length
of time the central line has been in place, and real time maintenance care.
Our goal is to reduce CLABSI incident by 50% within the three units and each unit will remain
below the hospital's 2014 standardized infection ratio (SIR) goal. The NICU, PICU, and PCICU
will work to remain at or below the 2013 SIR for their each respective unit.
Quantitative/Qualitative Measures
NYP-MSCHONY 2013 Data by ICU unit: The NYP overall goal SIR for 2013 was 0.58
compared to national SIR goal of 0.65
7 NICU CLABSIs
SIR 0.43
CL-Days 7,430
4 PICU
CLABSIs
SIR 0.43
CL-Days 3,072
6 PCICU CLABSIs
SIR 0.51
CL-Days 3,572
System Quality Review
213
NewYork-Presbyterian Healthcare System Quality Symposium 2014
Quality 2020: A Vision of the Future
MSCHONY 2014 Data to date: 6 NICU CLABSIs with CL-Days of 4,443; 3 PICU CLABSIs
with CL-Days of 1,779; 0 PCICU CLABSIs with CL-Days of 1,930.
Morgan Stanley Children's Hospital of New York Presbyterian spent anywhere between
$62,900- $493,000 for ICU CLABSIs in 2013 alone depending on severity of infection and an
average increase length of stay of 7 days due to CLABSIs. Based on this data, if there is a 50%
reduction in CLABSIs between the three ICUs, the hospital may save as much as $250,000 or
more on infection cost and have a decrease length of stay.
Methodologies
The Plan-Do-Study-Act (PDSA) tool was utilized for testing practice change in preventing
central line infections.
Our objective was identified as decreasing CLABSIs and the team identified missed opportunities
in infection prevention. A logic model was created as a time line for intervention implementation,
surveillance, data collection and data dissemination. Education and practice validation was
implemented on all aspects of central line care, maintenance, CHG baths, scrubbing the hub and
timely removal of central lines when no longer necessary. CLABSI prevention posters were
placed in all the units as well as scrub the hub hang tags on all IV poles. Through weekly
surveillance, the nurse champion team analyzed how well nurses are sustaining evidence based
practice in central line care in all three units, best practice in accessing lines, dressing changes, use
of alcohol impregnated caps on needleless ports, and CHG baths. A central line resource board
was established in all three ICUs, CLABSI prevention champions have been identified in the
ICUs, continued weekly surveillance, frequent unit huddles, and reeducation on central line care
and CLABSI prevention was established in the unit.
Improvement Results
The CLABSI prevention team performed 297 central line assessments. The findings included 10
(0.03%) lines that were saturated saturated with blood, improper connections, or not dated, 5
(0.01%) needleless caps were saturated with blood and not changed, 3 (0.01%) instances of the
use of improper needleless caps, 2 (0.006%) central line sites were reddened, 17 (0.06%) sites
were either leaking or bleeding, and 25 (0.08%) central line dressings were found to be loose,
soiled, overdue to be changed, or not dated.
The current 2014 CLABSI data to date demonstrate a 15% decrease in CLABSI rate for the
NICU, a 25% decrease for the PICU and a 50% decrease for the PCICU in CLABSI rate.
Collectively, we were successful in reducing CLABSI rate in all three units combined by 30%.
There is an increase in nurse and physician awareness and involvement in central line daily care
and maintenance. ICU staff is diligent in advocating for early removal of central lines to decrease
risk of infection. We have seen an increase in the use of alcohol impregnated caps to needless
ports and better compliance with scrubbing the hug. We have identified areas of missed
opportunity in infection prevention such as in inaccurate chlorhexidine baths technique and
accessing central lines. These opportunities were supplemented with reeducation and policy
review.
System Quality Review
214
NewYork-Presbyterian Healthcare System Quality Symposium 2014
Quality 2020: A Vision of the Future
Sustainability Strategies
Nurse CLABSI prevention champions are continuing weekly surveillance of central lines in the
unit. The three ICUs hold huddles on central line infection prevention, best practice in central
line care, and identify any barriers to evidence based best practice. Nurse champions are
identifying MVPs in CLABSI prevention, providing them with a small token of reward on their
efforts in reducing infection in the unit. We are identifying unit central line champions to assist
and troubleshoot with daily line maintenance and care such as dressings and line changes.
Continued education and practice validation are held within the units for nursing and medical
staff throughout the year, as well as identifying new medical products that will support our
initiative to prevent CLABSIs in our hospital.
Lessons Learned
1. It was often difficult for the nurses to step away from the bedside to listen and participate in
education sessions to prevent practice deviation from policy.
2. It is challenging to collaborate with multiple disciplines such as the ICU Medical team,
operating room staff, specialty physicians, interventional suites, and other units to maintain
proper practice as upheld within our units.
3. The CLABSI prevention team is very passionate in reducing CLABSIs in their units, we need
to assure protected time to continue to facilitate education, central line surveillance, and reinforce
best practice.
Conclusion
Central line associated bloodstream infections are preventable. Nurses are empowered and have a
strong responsibility in CLABSI prevention on a daily basis. It is essential to communicate any
updated practice or protocol changes pertaining to central line care via e-mail, huddles, posters,
and one-on-one awareness on all units in a timely fashion. Continued education, practice
validation, and surveillance improves adherence to proper central line insertions technique,
maintenance, and care. It is imperative to continue surveillance on central venous catheter care
within each unit as well as recruiting “champions” on units to assist and encourage staff
involvement in CLABSI prevention.
System Quality Review
215
NewYork-Presbyterian Healthcare System Quality Symposium 2014
Quality 2020: A Vision of the Future
System Quality Review
216
NewYork-Presbyterian Healthcare System Quality Symposium 2014
Quality 2020: A Vision of the Future
NewYork-Presbyterian/Morgan Stanley Children’s Hospital
Triaging Pediatric Respiratory Patients
Chana Schwartz; Bettina Sheridan; Lydia Carson; Michael DeGuzman
Introduction
Inaccurate Emergency Severity Index (ESI) assignment causes inappropriate wait time for
patients in need of immediate intervention, leading to concern for patient safety. Prior to
beginning our project, we estimated that only 40% of pediatric respiratory patients were being
accurately triaged based on the ESI algorithm. The objective for our project was to improve ESI
assignment during the triage process by 15% for pediatric patients with respiratory complaints.
Quantitative/Qualitative Measures
The defining primary measure for this project is ESI Triage Level as assigned by the triage nurse.
This is a dichotomous quantitative measure collected both via chart review and assessment test.
Data agreement was compared to pre-determined answers based on the ESI algorithm and the
investigative team’s expertise.
Methodologies
DMAIC (Define, Measure, Analyze, Improve, Control) was used to outline the approach to this
quality improvement project. Measurements were collected via randomized chart reviews and
assessment tests. Analysis was performed on baseline data and possible drivers resulting in
inaccuracy considered. During Improve, based on previous findings a tailored in-service was
developed and implemented. For Control, a full analysis of pre/post data was performed,
sustainability outlined but not yet fully maintained.
Improvement Results
Baseline chart reviews (n=100) of respiratory patients revealed a 44% level of ESI accuracy
resulting in 56% of patients being either over-triaged (11%) or under-triaged (45%). Postintervention, chart reviews (n=100) revealed a 61% level of accuracy resulting in 39% of patients
being either over-triaged (23%) or under-triaged (16%).
Baseline pre-tests (n=29) revealed a 60% level of agreement among staff with the remaining 40%
being either over-triaged (5%) or under-triaged (35%). Post-tests (n=29) revealed a 67% level of
agreement with the remaining 33% being either over-triaged (20%) or under-triaged (13%).
Sustainability Strategies
To make sure that the correct process stays in place we addressed secondary root causes and have
implemented the following:
System Quality Review
217
NewYork-Presbyterian Healthcare System Quality Symposium 2014
Quality 2020: A Vision of the Future
1. The creation and initiation of a standardized triage training process that includes triage RN
eligibility and orientation processes. We created an audit tool to evaluate the accuracy of nurses’
implementation of ESI for respiratory patients during the triage process
2. Education to staff on triage documentation for patients with respiratory complaints
3. A recommendation to hospital management to increase qualified RN staff in triage.
4.We are also in the process of collaborating with the Unit Practice Council to provide nurses
with a specific color chart for patients with ESI level 1.
Lessons Learned
1.Targeted approach to ESI improvement is manageable and can improve ESI overall
2.ESI improvement projects also uncover opportunities to improve triage operations
3.Continuous training and education is imperative for maintaining a standardized practice
Conclusion
Results indicate that we reached our goal of 15% improvement of ESI assignment for respiratory
patients during the triage process. Triage has a direct impact on patient outcome and when
patients are assigned an inaccurate ESI level during triage, the outcome of the patient suffers.
Improving the accuracy of ESI assignment for respiratory patients to 61% during the triage
process has allowed us to prevent further patient deterioration as well as improved the ED flow.
System Quality Review
218
NewYork-Presbyterian Healthcare System Quality Symposium 2014
Quality 2020: A Vision of the Future
NewYork-Presbyterian/Weill Cornell Medical Center
Reducing OR Holds: How Employee Engagement Successfully Improved
Patient Flow
Stephanie Nolan RN, MSN, MBA, CPAN; Gregory Camacho, RN, MSN; Katherine O'Hara RN,BSN; Melanie
Quinn RN, BSN; Katrina Valdez, RN, BSN; Kristen Pellicano RN, BSN; Traci Steinberg RN, MSN CPAN; Gary
Allard Business Associate; Christine Teijo, RN, SSN, BSN; Courtney Donnell, RN, SSN, BSN; Joan Leonard, RN,
AAS; Ferron Zayas, RN, BC; Mitzie Wildman Parker Business Associate; Natalia Ivascu MD, PACU Medical Director,
Associate Professor of Clinical Anesthesiology
Introduction
Background/Problem Statement
In response to increasing operating room hold times, also known as Post Anesthesia Care
Unit(PACU) holds, the New York Presbyterian cross campus flow committee established a goal
for a 5 % reduction in holds for 2014.
For this project the term PACU hold was used. A "PACU hold" is defined and recorded by the
Operating Room (OR) when the patient is ready to leave the OR but cannot be received by the
PACU.
In alignment with New York Presbyterian's culture and strategic initiatives, a multidisciplinary
PACU hold reduction committee was formed. The committee consisted of the PACU anesthesia
medical director, Registered Nurses, Business Associates, Patient Care Directors and the Director
of Nursing for PeriAnesthesia Services. The committee met bi-weekly to clearly define holds,
identify root causes, then design and implement strategies to reduce hold times.
Quantitative/Qualitative Measures
Quantitative measures included hours of OR holds per per month as reported out institutionally
cross campus'.
In order to assist with establishing root causes, holds were further looked at by the committee by
amount of holds per day per PACU, individually by service, time of day, and length of each hold.
Methodologies
Deming's Plan Do Check Act cycle was used as a dynamic cycle for continuous improvement.
Additional principles applied were principles of lean methodology in an effort to optimize
resources, streamline processes, and reduce waste.
System Quality Review
219
NewYork-Presbyterian Healthcare System Quality Symposium 2014
Quality 2020: A Vision of the Future
Improvement Results
The PACU hold reduction committee was formed in March 2014. We began with clearly defining
a hold in collaboration with the Operating Room and understanding the root causes to holds.
The team developed strategies to address each of the issues.
Five months after implementation (April through August), there has been an average 75%
reduction in PACU hold times from January 2014, with a maximum of 89% reduction in holds
for the month of August alone.
In terms of hours of time, this was a reduction from 106.4 total hold hours in January to a total
of 12.1 hours in August. We sustained an average of 27.4 hold hours for all 5 months(Please see
attached pdf for hold reduction graph).
After the significant reduction in holds by month two, the committee revised the 5% institutional
target goal for reduction in holds and committed to sustain a 50% reduction in holds for 2014.
We continue to successfully maintain this.
Sustainability Strategies
Results show that we have sustained a greater than 50% reduction in holds for 5 consecutive
months. This is reflective of a sustained change of culture and operations in both PACU's.
However, continued sustainable census of the PACU is dependent on both internal and external
variables. Internal PACU variables include available beds, proper nurse staffing , length of stay
and patient acuity. External factors include inpatient census and bed availability, ease in giving
floor reports, and OR volume.
Data driven reports such as a daily hold report has allowed us to closely monitor and analyze
trends in holds by day of week and time of day. Additionally this report has allowed for
accountability amongst staff and proper management of internal PACU variables. External
factors have been sustained with increased communication and collaboration amongst other
departments and disciplines. Our team is committed to sustaining this reduction and continuing
to look for innovative ways to further reduce hold times.
Lessons Learned
1- Employee engagement was critical to the success of this initiative and the overwhelmingly
positive results
2- Increased patient flow and reduction of holds can be achieved without additional costs,
through optimization of current resources and streamlining processes. Small changes led to big
results.
3-Communication, collaboration, and transparency were key factors in identifying the root causes
to holds and building trust within the system.
System Quality Review
220
NewYork-Presbyterian Healthcare System Quality Symposium 2014
Quality 2020: A Vision of the Future
Conclusion
PACU flow is a dynamic, complex problem with inherent unpredictability. Improvements in
PACU flow requires increasing operational efficiency, while maintaining high quality care. The
successful reduction in hold times was directly related to engaged employees that committed to
the team objectives, openly communicated the root causes, and were the key drivers for the
change.
System Quality Review
221
NewYork-Presbyterian Healthcare System Quality Symposium 2014
Quality 2020: A Vision of the Future
NewYork-Presbyterian/Weill Cornell Medical Center
Improving the Patient Pain Experience in Obstetrics
Cathy Crandall RN; Dayna Dixon RN; Neneh Kamara RN; Kjaer Klaus MD
Introduction
Review of pain management practices for the obstetrical units revealed qualitative and
quantitative evidence that patient’s did not always rate their experience with pain management
highly. The goal of this project was to improve the patients’ pain experience.
Barriers to effective pain management were explored by a multidisciplinary team of OB
physicians, nurses and anesthesiologist in partnership with the pharmacy, and information
technology team members. Information was obtained from standardized surveys and patient
surveys created by the Obstetric Pain Task Force that interviewed patients in “real time”. Seven
themes where identified as core areas for improvements:
1) Clarity of pain plan as interpreted by RNs and patients
2) Accessibility to providers for pain medication orders
3) Practice variation in pharmacological pain management choices by providers
4) Delays in administration of pain medication
5) Variety of pain sources (eg. GI, breast pain, cramping)
6) Inefficiency or incompatibility of pharmacological agent chosen
7) Transitions of care from waiting area and triage to labor floor and OR, as well as to recovery
room and postpartum floor
This project addresses these areas systematically and in a multidisciplinary way using the Define
Measure Analyze Improve and Control (DMAIC) framework for quality improvement.
Define- The problem; “Patient’s do not always rate their pain experience highly”
Measure- HCAHPS, Press Ganey, Patient Interviews
Analyze- Analysis yielded the seven core areas mentioned above
Improve- Many interventions were launched to create improvement as will be expanded on
throughout this abstract. The improvements were multi-faceted and multidisciplinary.
Continuous Quality Improvement concepts will create sustainability for the improvements made
as a result of the interventions applied in this project.
System Quality Review
222
NewYork-Presbyterian Healthcare System Quality Symposium 2014
Quality 2020: A Vision of the Future
Quantitative/Qualitative Measures
Quantitative – Baseline data was reviewed via HCAHPS and Press Ganey. These standardized
surveys measured the patient experience. Two specific areas were used for the purpose of this
project; (i) How labor discomfort was controlled (Press Ganey) (ii) Staff doing everything to help
with pain (HCAHPS). The Obstetrical units used the best hospitals national benchmark for
comparison.
Qualitative – The Obstetric Pain Task Force conducted real time patient interviews near the day
of discharge to assess patient’s pain experience throughout to characterize and discuss sources of
pain. This data was synthesized to identify immediate and longer-term opportunities for
improvement.
Methodologies
This project used the DMAIC framework for quality improvement to address the the seven core
areas mentioned before to systematically, and in a multidisciplinary way create positive change in
the patient experience of pain. A variety of interventions were used to create improvement. This
included implementation of Pain Rounds and Focused Event Reviews for pain related issues,
computerized pain management order sets, standardized pain management medications specific
to delivery mode (c/s or vaginal delivery) as well as transitions in care (OR to recovery room and
labor floor to postpartum); charge nurses spoke to patients in the waiting area and triage to set
expectations when delays occurred. The concept that the patient is part of the care team (from
TeamSTEPPS) was a core driver for the communication between the patient and the care team.
Improvement Results
The multidisciplinary creation of the computerized pain management order sets utilized an
informatics based solution for the standardization of the pain management of order sets. These
pain management order sets were created as a BI-CAMPUS collaborative with obstetricians,
anesthesiology, pediatrics and pharmacy to address the various types of pain and the relationships
of various pharmaceutical agents to the types of pain. Elements such as medication efficiency as
well as pharmokinetics regarding medication timing and absorption were considered when
designing these orders. The goal was to give the patient the most effective management of pain
throughout labor and during the transitions in care period from one area of patient care to
another. This multidisciplinary and systematic approach was effective in addressing the identified
areas of difficulty in managing the patient experience. These changes were implemented
throughout the first quarter of 2014.
Measured Improvement: The data reveals an increase from the scores of the 4th quarter of 2013
to an increase during and after the implementation of the strategies discussed. This increase was
evident by the first quarter of the 2014. For the Press Ganey question "How labor discomfort
was controlled", October 2013 reported 84.5% and March 2014 reported 90.8% for satisfaction
(See attached slides Fig. 1). The HCAHPS question "Staff did everything to help with pain" in
October 2013 scored 75% and increased to 85.5% in April 2014 showing a 10.5% increase. (See
attached slides Fig. 2)
Supplemental to this initiative was the utilization of the TeamSTEPPS structure for
communication to address pain outliers via briefings, huddles, and Handoff using SBAR.
System Quality Review
223
NewYork-Presbyterian Healthcare System Quality Symposium 2014
Quality 2020: A Vision of the Future
Sustainability Strategies
The strategies expected to have the most impact on sustainability are:
Visibility- discussion regarding pain management practices needs to visible and consistent as it
pertains to each patient in an individualized manner.
Accountability- Consistency and follow-up as well as feedback to the care team is vital to
developing a culture that will seek to continually improve
Leadership- The preceding two strategies require strong leadership to help create and foster this
environment and build on the growing culture of communication and collaboration
Lessons Learned
1) Patient education will need to be a greater part of this project moving forward. The EMR will
be a tool for disseminating specific pain management information to this clinical demographic.
2) Information technology can help play a role in this project in greater way through the
utilization of instant alerts; for example from the patient to the nurse and provider, so medication
can be adjusted more quickly and seamlessly.
3) Communication – Communication is always a vanguard for any project. This project facilitated
collaboration and ignited discussions for best practice and innovation. Communication is
constant and opportunities will always exist for continuous improvement.
Conclusion
Ongoing assessment of response to interventions and adjustment for continuous quality
improvement are expected to aid sustainability. There will be ongoing measurement of the
quantitative parameters and analysis of the the results to guide improvement efforts. There has
been positive progress, this has been a multidisciplinary and inclusive project. The focus has been
to create a patient centered care and team collaborative approach and it has yielded promising
results and a stronger structure for quality control and future improvement.
System Quality Review
224
NewYork-Presbyterian Healthcare System Quality Symposium 2014
Quality 2020: A Vision of the Future
FIGURE 1
Press Ganey- How labor discomfort was controlled ?
95
90
y = 0.1596x + 84.578
85
Press GaneyHow labor
discomfort
was
controlled ?
80
75
70
FIGURE 2
90
HCAHPS - Staff do everything help with pain - % Always
85
y = 0.5099x + 75.206
80
75
70
HCAHPS Staff do
everything
help with
pain - %
Always
65
60
System Quality Review
225
NewYork-Presbyterian Healthcare System Quality Symposium 2014
Quality 2020: A Vision of the Future
Poster Presentation
New York-Presbyterian Hospital
Multidisciplinary Approach to Collaborate and Implement Strategies for
Reducing Surgical Site Infections of Spinal Fusion Patients
Louis Bigliani, MD; Charla Fischer, MD; Yoko Furuya, MD; Jason Cohen, MSPT, MBA; Scott Possley, PA-C, MPAS;
Brian Regan, PhD; Lisa Covington, RN, MPH; Sandra Hyman, RN, MPA; Audrey Compton, MD, MPH; Maiken
Jacobs, MA, OTR/L; Richard Canjura, MBA
Introduction
Problem Statement:
Many studies show the costly impact of Surgical Site Infections (SSI) on the overall health care
system. Further, SSIs increase length of stay and lead to higher 30-day readmission rates. This
retrospective study examines spinal fusion SSI rates from January 1, 2011 to March 31, 2014 for
the Department of Orthopaedics at NewYork-Presbyterian/Columbia University Medical Center
(NYP/CU) campus.
Project Aim/Goal:
To use a multidisciplinary approach utilizing the Orthopaedic Quality Committee to improve a
sudden rise in the standardized infection ratio with regard to the surgical site infections of the
spinal fusion population. Spinal Fusion procedures at NYP/CU are performed by both the
Neurosurgical and Orthopaedic Surgery Departments.
In 2011 and 2012, the spinal fusion SIR rates were 1.17 and 1.21 respectively, which are above
the national benchmark of 1.0. In 2011, there were 8 spinal fusion cases with SSIs attributed
evenly between the two services. However, as the Q1 and Q2 data for 2012 was made available
through the Infection Prevention and Control department, it was evident that the majority of
SSIs were attributable to the Orthopaedic service line. Ultimately, there were 10 spinal fusion
cases with SSIs, 9 of which were orthopaedic cases. This prompted a task force from the
Orthopaedic Quality Committee to perform a root cause analysis and formulate a corrective
action plan to decrease the SIR below the 1.0 benchmark.
Quantitative/Qualitative Measures
The department of Infection Prevention and Control at NYP/CU performs SSI surveillance
utilizing the Centers for Disease Control and Prevention (CDC) National Healthcare Safety
Network (NHSN) definitions. Cases are tracked for up to 90 days when implantable devices are
placed, during which time any SSI will be attributed towards the initial procedure. SSI data are
then reported into NHSN and benchmarked against national data using the Standardized
Infection Ratio (SIR).
System Quality Review
226
NewYork-Presbyterian Healthcare System Quality Symposium 2014
Quality 2020: A Vision of the Future
Methodologies
Using process mapping and the Results Approaches Deploy Assess and Refine (RADAR)
methodology, an action plan was created in order to decrease the incidence of infection in the
targeted population.
Improvement Results
The following action items were established and implemented:
• The initiation of pre-operative Chlorhexidine wipes.
• Replacement of the C-Arm Drape used in the OR.
• An enhanced cleaning process for the C-Arm.
• Bundle Strategy for Infection Prevention in the OR including: surgical hand prep, patient skin
prep, traffic control, draping, maintaining the sterile field, and antibiotic prophylaxis with
Cefazolin and gram-negative coverage is either Gentamicin or Tobramycin.
• Postoperative dressing change on day 3 to prevent post-op wound contamination.
• Replacing tape and gauze with sterile dressings.
• 3% Betadine wound irrigation protocol used prior to bone graft and placement.
The effect of implementing the performance improvement action plan in September of 2012,
resulted in a decrease in the number of orthopaedic spinal fusion SSI’s for 2013. In 2013, there
were 4 SSIs in total with an associated SIR of 0.60. Since the interventions were clearly effective
in 2013 they were maintained in 2014, resulting in 0 orthopaedic spinal fusion infections through
Q1 2014. (See Figure 1 below)
Sustainability Strategies
To sustain our results we will continue to utilize the Orthopaedic Quality Committee monthly
meetings as a forum to discuss SSIs and monitor the SIR for the spinal fusion population at
NYP/CU. Since every case involving Spinal Fusion SSIs is presented at the monthly Quality
Committee meeting, a Root Cause analysis is performed by a Spinal Surgeon. Additionally, the
Infection Prevention and Control department reviews each spinal fusion infection case and
provides the Quality Committee with infection category classification and organism information.
Knowing the classification and organism is important in understanding how the infection was
acquired and to prevent the spread of the infection.
Lessons Learned
1) A Multidisciplinary approach allows for greater cross-departmental communication and
collaboration. This approach also fosters an environment where employees feel engaged and
empowered to make a positive impact within the organization.
2) Impartiality and transparency within our group was paramount for meaningful discussions and
lead to unison on our multifaceted plan of action.
3) Using regularly scheduled meetings with assigned action items allows for ongoing data analysis,
as well as, a highly adaptive project management process.
System Quality Review
227
NewYork-Presbyterian Healthcare System Quality Symposium 2014
Quality 2020: A Vision of the Future
Conclusion
The Department of Orthopaedics at NYP/CU was able to implement best practices that would
reduce SSI for spinal fusion procedures. The result was a significant reduction in SIR for spinal
fusions for 2013 (0.60) from 2011 and 2012 (1.17 and 1.21). Further, there have been no
incidences of SSIs through the 1st quarter of 2014. Utilizing the monthly Orthopaedic Quality
Committee meetings have proven effective. These monthly meetings reach a variety of disciplines
who are motivated to improve the quality of care and reduce SSIs especially as they relate to their
service line.
Figure 1. Surgical Site Infection (SSI): Spinal Fusion NYP/CU for Year End (YE) 2011; SIR =
1.17 (CI 0.48, 1), YE 2012; SIR = 1.21 (CI 0.63, 1.01), YE 2013; SIR = 0.6 (CI 0.41, 0.86), and
Q1 of 2014; SIR = 0.
System Quality Review
228
NewYork-Presbyterian Healthcare System Quality Symposium 2014
Quality 2020: A Vision of the Future
New York-Presbyterian Hospital/Weill Cornell Medical Center
Compliance with Clostridium Difficile Prevention Guidelines
Mary B. Moran, MSN, FNP-BC, MPH, RN, CCRN; Natalie Hellmers, MSN, ACNP, CCRN; Annette Davidek,
MFA, BSN, CCRN; Nancy E. Trejo, PA-C; Jennifer Solan, RN, CCRN; Alisa Coleman, RN. Advisors: Ernesto
Perez-Mir, MSN, RN, CCRN, Director of Nursing; Baldeep Kaur, RN, Patient Care Coordinator and James Horowitz,
MD, Associate Director CCU
Introduction
Clostridium Difficile: Compliance and Prevention Guidelines
Problem Statement: Clostridium Difficile is an anaerobic, spore forming bacterial organism. It is
virulent and resistent to traditionally used antibiotics. It produces both an enterotoxins and
cytotoxins that cause diarrhea and bowel inflammation. Major complication include Toxic
Megacolon which can lead to an increase in patient mortality [14,000/year]. The average total
cost for a single inpatient C. difficile infection (CDI) is more than $35,000 and the estimated
annual cost burden for the healthcare system exceeds $3.2 billion annually in the USA. CDI has
replaced methicillin-resistant Staphylococcus Aureus (MRSA) as the most common cause of
Hospital Associated Infections (HAI). There are also increasing reports of CDI in children and
healthy people who have had minimal or no recent exposure to healthcare settings as well as in
peripartum healthy women. This last statement raises the question of CDI being transmitted by
(healthy) visitors and/or Medical Staff to the general community population.
Project Aim: Prevent C. difficile infection, decrease patient mortality, shorten hospital length of
stay (averages 2.6 to 4.5 days); decrease cost. Identify patients at high risk such as patients on
antibiotics, proton pump inhibitors, recent GI surgery, immunosuppressed, advanced age and
long hospital stays. Evaluate the Mode of Transmission such as via the hands of healthcare
workers, contaminated surfaces (spores live on dry surfaces a long time) and person to person
contact.
Overall Goals: In the year 2013, NYPH-Cornell, the cardiac care unit in particular saw facilityonset CDI incidents that were at a rate of 15% higher than expected. Our aim was to reduce the
rate of CDI by 10%. In the year 2013, there were 16 cases of CDI YTD by end of December
2013. Hospitals are compared to national data using the standardized infection ratio (SIR), a ratio
of the observed # of cases to the expected # of cases. SIRS > 1 indicates a higher rate of CDI
than expected. In the year 2013, NYP-Weill Cornell SIR = 1.23 (1.085 - 1.379) out 275 cases
(overall whole facility). To reiterate that meant we were at a rate of 15% higher than expected.
After a team coordinated effort (listed presenter and advisors) our Cardiac Care Unit (4 South)
was able to reduce the rate of CDI from 16 (YTD 2013) to ZERO (YTD August 2014). Data can
be found at the NYP Infection Prevention and Control Infonet website.
System Quality Review
229
NewYork-Presbyterian Healthcare System Quality Symposium 2014
Quality 2020: A Vision of the Future
Quantitative/Qualitative Measures
We kept close monitoring with the the NYP-Weill Cornell Infectious Disease and Epidemiology
Department as well as researched various publications that included but are not limited to the
CDC, the Cleveland Clinic, SHEA (Society for Healthcare and Epidemiology of America), IDSA
(The Infectious Diseases Society of Americas), AJN The American Journal of Nursing 2014, and
Gut Microbes 2011.
Methodologies
Intense focus on researching prevention measures such as hand hygiene, environmental cleaning,
isolation precautions, covering equipment, ensuring visitor compliance with isolation practices.
The most exciting and technologically newest idea was the implementation (at the end of 2013
and now being consistently used): The Xenex Machine: UV disinfection system that kills C-Diff
spores; (2) Exclusive new bleaching product and sterile covers for our EKG machines and the
SonoSite Ultrasound Machine; (3) CCU purchased high quality stethoscopes that are dedicated to
be used as one per room/patient; (4) Last but not least the judicious use of antibiotics and PPIs.
Improvement Results
The rate of CDI in the Cardiac Care Unit was 16 in the year 2013. As of January 2014 ,we have
had ZERO number cases CDI in the CCU since the implementation of staff education,
reinforcement of proven old methods and the use of newer technology, equipment protection
and adherence to prevention of horizontal transmission of CDI.
Sustainability Strategies
The cost of purchasing the different type of Clorox Bleach we use now on all our equipment,
equipment covers, one time expense for purchasing high end stethoscopes, and using the
XENEX Machine is almost neglible in comparison to the $3.2 billion annually lost to treating this
disease.
Lessons Learned
1. CDI causes 14,000 human deaths per year. Utilizing the aforementioned prevention and
treatment modalities can cut the CDI rate to zero. Patients do not have to die from hospital
acquired disease/infections.
2. Prevention methods are not difficult to implement. Good Old fashion Hand Hygiene,
cleaning & isolation precautions, and utilizing the latest newest technology such as the XENEX
machine.
3. Practices in improving quality and safety of inpatient care avails itself to prevention of this
deadly disease (CDI). In fact even possible prevention of spreading it to the general community.
I was quite impressed and made fearful to learn that there are cases of CDI in non-patient people
in the community.
System Quality Review
230
NewYork-Presbyterian Healthcare System Quality Symposium 2014
Quality 2020: A Vision of the Future
Conclusion
Wash your hands, use the proper cleaning agents, make patient and family education your dogma,
stay current on CME topics, and most importantly human lives can be saved. Deaths can be
prevented. It's really not difficult at all. The major driving component is staff adherence and
compliancy.
System Quality Review
231
NewYork-Presbyterian Healthcare System Quality Symposium 2014
Quality 2020: A Vision of the Future
New York-Presbyterian/Columbia University Medical Center
Taking a Proactive Approach to Patient Safety
Robin Lynch MSN, RN; David Kessler MD, MSc
Introduction
With early roots in flight training, healthcare simulation technology has evolved from the
mannequins of the 1950’s -to high-tech, interactive, realistic patient simulators with the ability to
mimic human response to illness (Hodson-Carlton, 2009). Research has found simulation
promotes knowledge acquisition, self-efficacy, self-confidence, and their development of
prioritization, delegation and critical thinking skills (Kaddora, 2010; Kaplan & Ura, 2010; Lewis &
Ciak, 2011; Schlairet & Pollock, 2010; Sinclair & Ferguson, 2009). At New York-Presbyterian we
use simulation to promote communication and teamwork; specifically for crisis resource
management (CRM) training. We conduct a wide array of simulations in multiple departments
(in-situ) focusing on low frequency/high risk scenarios to better prepare our clinicians to work as
a team to effectively manage a patient in crisis. During the course of these simulations we
sometimes discover latent safety threats (LST). Latent safety threats are frequently described as
"accidents waiting to happen" or systems-based threats to patient safety that have previously
been undiscovered. Examples of LSTs include delays in treatment, malfunctioning equipment,
missing medications and supplies, and knowledge deficits related to hospital policies and
procedures. Historically, these LSTs are reported antecdotally to department heads with the
intention of promoting a change. With our adoption of KEEPSAFE software, the hospital has
an opportunity to implement a mechanism of action for reporting and addressing LSTs
discovered during the course of simulation and a process for identifying trends. I have proposed
a revision to the KEEPSAFE submission form to allow for specifying a LST discovered during
simulation as a drop-down option after selecting "the incident did not affect a patient." All other
processes would remain the same regarding dissemination of the reports to responsible parties.
With this change, we have the ability to improve patient safety by taking a proactive approach to
risk management.
Quantitative/Qualitative Measures
I am proposing a formal collaboration with Quality and Patient Safety and the Simulation Center
to work together to identify and prioritize future simulation efforts based on data collected
through KEEPSAFE (both LST and actual event trends). When systems problems and
knowledge deficits are identified, we can use simulation to educate clinical and ancillary staff as
well as test system/policy modifications. Specific initiatives can be tracked through longitudinal
data collection related to incidents such as falls, medication errors, and infection rates.
System Quality Review
232
NewYork-Presbyterian Healthcare System Quality Symposium 2014
Quality 2020: A Vision of the Future
Methodologies
All four core principles of Quality Improvement are addressed:
QI work as systems and processes
Focus on patients
Focus on being part of the team
Focus on use of the data
Improvement Results
This is a work in progress, however with this change we can hypothesize there will be a
significant impact on our current approach to risk management.The current process of incident
reporting through KEEPSAFE ensures that department managers address incidents in a timely
manner. The transparency of the system serves as a second mechanism to ensure accountability.
With the proposed revision, the simulation centers will have access to view reports generated by
the discovery of LSTs, ensure LSTs are addressed and work with hospital departments and teams
to offer additional simulation learning experiences when appropriate.
Sustainability Strategies
As with any change, we will need administrative buy-in and some system-wide education of this
change to KEEPSAFE. Simulation is being done to some extent at all campuses, but we lack a
centralized process to address LSTs. A simulation collaborative should be formed with directors
and managers of simulation as well as members of the Quality and Patient Safety department to
ensure proper training of faculty/clinicians/educators of the change and the process of reporting
LSTs identified during simulation and training activities. Additionally, simulation departments can
serve as an additional safeguard by ensuring LSTs identified on their respective campus are
addressed.
Lessons Learned
1. There currently is not a system for reporting and addressing LSTs discovered during
simulation activities
2. Revising the current KEEPSAFE entry form will standardize the process of reporting LSTs
3. With this revision, NYP will be taking a proactive approach to patient safety
Conclusion
Latent Safety Threats, left unaddressed, have the potential to cause preventable harm to patients
and staff. NYP has the opportunity by revising KEEPSAFE to take a proactive approach to
patient safety. This change also promotes a collaboration between NYP's Quality and Patient
Safety and Simulation departments which may lead to future alignment of patient safety and
simulation initiatives.
System Quality Review
233
NewYork-Presbyterian Healthcare System Quality Symposium 2014
Quality 2020: A Vision of the Future
NewYork-Presbyterian Hospital
Creating a Shared Mental Model
Tracey Lewis, MPH; Catherine Waters, RN, MSN, OCN, NEA-BC; Amy Silverstein, MPH; Joan Kaiser RN, MA,
AOCN; Sari Sloane, RN, MSN, NP-BC; Reza Kazerooni, Pharm.D., BCPS, BCOP; Justin Ramirez; David Collado;
Maria Lyons Zani, RN; J. Gregory Mears, MD; Joelle Coq, MS, RN, NEA-BC, OCN; Yon Sugiharto, MA, CTDP;
Rosemary Trinkle Baran
Introduction
On an average day, the Herbert Irving Adult Infusion Center at NewYork Presbyterian Hospital
/ Columbia treats over 100 patients receiving chemotherapy, infusion and injection services and
coordinates patient care along side over 75 referring providers. Interdisciplinary teams of Nurses,
Patient Access Representatives, Pharmacists, Phlebotomists, Registered Dieticians, Social
Workers and Housekeeping personnel work inside the Infusion Center. Complexities in care
delivery require consistent communication and teamwork to ensure a strong patient experience
and mitigate potential quality and patient safety risks. With AHRQ Culture of Safety Scores at
72% in overall communication and Press Ganey Patient Satisfaction Scores ranking in the 1st
percentile when compared to peer hospitals, the team faced a “call to action” with the anticipated
continued growth of services and locations in 2014.
The journey towards improvement began in July 2013 when the leadership team worked to
identify key improvement domains from the Culture of Safety Survey. Staff feedback highlighted
lack of role clarity, little delegation of responsibilities or tasks, strained interpersonal relationships
impacting the opportunity for feedback and little cooperation among team members. The
combination of these perceptions and attitudes indicated a readiness for TeamSTEPPS training.
We created training modules and scenarios to target key dimensions including Leadership,
Situation Monitoring, Mutual Support and Communication.
Our poster will highlight key steps taken along our Journey and will demonstrate markers of
success in areas of Patient Satisfaction, improved communication of quality and safety events,
increased trust among caregivers and ultimately an increase in the Culture of Safety survey scores.
Quantitative/Qualitative Measures
Culture of Safety Scores
Patient Satisfaction Scores / Total Grievances and Patient Complaints
Reported Patient Safety Errors / Events
System Quality Review
234
NewYork-Presbyterian Healthcare System Quality Symposium 2014
Quality 2020: A Vision of the Future
Methodologies
Use of TeamSTEPPS tools and methodology. Includes use of Leadership Tools (safety briefings,
delegation), Situation Monitoring (situational awareness) and Mutual Support (task assistance).
Improvement Results
Patient Satisfaction Scores - Q2 2014 overall score 88.1 - highest score since Q4 2011
Shared mental model - Staff and leadership believe the unit gained traction in implementing other
departmental changes because the team shares the same mental model.
Interdisciplinary huddles (safety briefings)- Use of morning daily huddles increased from 25% in
January 2014 to 95% by March 2014. Morning huddles are used to review and close the loop on
patient safety events; 91% of reported events or near misses were reviewed during huddle within
3 days.
During TeamSTEPPS training, other opportunities were identified to improve communication
and collaboration:
Reinforce education around existing tools and resources (i.e. use of electronic Patient Tracker)
Lunch & Learns / Meet & Greets with referring physicians
Operational improvements were introduced alongside TeamSTEPPS training sessions:
Improvements to workflow to improve patient experience and decrease wait time
Improvements within chemo pharmacy
Information handoff between registration and phlebotomy
Event reports (KeepSafe):
Staff feel more comfortable reporting events and do not see reporting as punitive
Sustainability Strategies
Develop sustainability and accountability plan to ensure consistent interdisciplinary huddles when
unit leader is offsite.
Engage staff to observe application of TeamSTEPPS behaviors using performance observations.
Reinforce use of task assistance in real time to reduce patient safety risks.
Improve use of electronic patient tracker to monitor patient flow. Use data to identify and inform
future improvement opportunities.
Lessons Learned
1. Physician buy-in is key
2. TeamSTEPPS requires continuous reinforcement and opportunities to provide real time
feedback
3. A "leadership as trainers" model was valuable to ensure leadership provided positive feedback
and identified missed opportunities. Engaged leadership helped to empower staff to apply
advocacy and assertion, feedback and CUS, on their own, rather than having to mediate.
System Quality Review
235
NewYork-Presbyterian Healthcare System Quality Symposium 2014
Quality 2020: A Vision of the Future
Conclusion
In conclusion, the implementation of the TeamSTEPPS methodology in the Adult Infusion
Center has helped the interdisciplinary team create a shared vision to mitigate the risks of patient
safety events and have improved patient satisfaction scores and fostered a culture of safety.
While communication will continue to be an ongoing improvement strategy, the tools
implemented will help enable the team to focus their communication efforts towards the most
vulnerable areas. These area include minimizing the "halo effect" associated with positions of
leadership and degree, managing interruptions and proper adherence to protocol. The team is
more equipped to assess the situation around them, ask for assistance and escalate any patient
safety concerns.
System Quality Review
236
NewYork-Presbyterian Healthcare System Quality Symposium 2014
Quality 2020: A Vision of the Future
NewYork-Presbyterian Hospital
Making Care Better: Standardizing Care Redesign in Accordance with
Evidence-based Practices
Lauren Hedinger, MPA; Brian R. Taylor, PhD; Simone B Zappa, RN, MBA; Katherine H. Pavlovich, MPH;
I-Fong Sun Lehman, DrPH, MS
Introduction
In recent years, healthcare organizations across the US have focused on strategic initiatives that
improve the quality, safety, and efficiency of healthcare services while, at the same time,
decreasing the cost of care. In order to accomplish this, the Joint Commission has promoted the
concept of a “high reliability organization” - an institution committed to providing the same high
level of care for every patient at every opportunity. A necessary component of achieving high
reliability is the use of evidence-based care. Much like other healthcare organizations, NYP has
implemented numerous care redesign initiatives based on best practice to try and achieve this
benchmark. However, a defined infrastructure by which to implement standardized quality
improvement has been needed.
Making Care Better (MCB) launched in January of this year as an umbrella program for
standardizing care across inpatient units. The program is spearheaded by senior leadership from
Clinical Operations, Strategy and Quality and Patient Safety and oversight of the implementation
has been provided by the Director of Clinical Innovation. The aim of the program, which
incorporates the fundamental principles underlying high reliability organizations, is to standardize
care processes that will improve quality of care, reduce variability, and improve satisfaction for all
NYP inpatients. These goals are achieved by focusing on improved communication and
collaboration, fostering a culture of leadership and accountability and infusing care management
into the inpatient experience through a rapid cycle improvement process. MCB was initiated
across a select group of 12 medical, surgical, and pediatric units and, over time, will be rolled out
to additional units until the initiative is embedded in all patient care units throughout the
Hospital.
MCB units work to operationalize 13 care redesign process elements that were selected after a
review of best practices at other healthcare organizations and existing clinical transformation
initiatives that required a refocus on implementation. These elements are grouped into three
improvement categories: 1) communication; 2) care management; and 3) patient engagement (see
Figure 1). Efforts on each unit are led by a core unit team. Each core unit team consists of a
patient care director (nurse manager), a unit medical director, and chief resident (optional) and is
supported directly by a Quality & Patient Safety Improvement (QPSI) Manager. This structure is
designed to foster a culture of shared accountability between physician and nursing leadership as
they work together to operationalize and implement the elements on their unit.
System Quality Review
237
NewYork-Presbyterian Healthcare System Quality Symposium 2014
Quality 2020: A Vision of the Future
Quantitative/Qualitative Measures
Data are available to the core unit leadership in a variety of forms. Unit-level performance of
each element can be tracked and trended real-time at the patient-level through online reporting
tools. These tools allow units to track short- and long-term progress as well as identify
bottlenecks and address needed process changes. For example, the “Document Care Team”
process measure tracks how often care team members document themselves in an EHRembedded tool called the Care Team widget. Every day, unit leaders can identify which patients
did not have care team documentation and immediately address the oversight while also
monitoring long-term trends. Defining these process measures is an iterative process: metrics that
are not helpful to unit leadership are modified by the MCB analytics team based on feedback
from the frontline. In addition, quarterly unit-level dashboards provide performance
measurement on four outcome domains: Patient Satisfaction, Patient Safety, Infection Control,
and Efficiency. Unit-level performance on each outcome measure is compared to and scored
against national benchmarks or hospital benchmarks if national ones are unavailable (see Figure 2
for sample).
Methodologies
As each process element is rolled out on an MCB unit, the core unit team provides immediate
feedback to process owners and MCB leadership, providing opportunities for improvement or
rectifying specific challenges to implementation. This iterative process allows for rapid cycle
improvement of the elements as they are implemented. Unit-level improvement is data driven.
Together the team reviews performance data and identifies improvement opportunities which
subsequently drive change. Since each unit is unique in its patient population and workflow, unit
leadership is encouraged to work together to develop and implement the 13 elements in a manner
tailored to their unit’s unique needs and challenges to support optimal achievement of the desired
outcomes. The QPSI manager safeguards standardization by ensuring elements are implemented
according to their core tenets and connects the core unit team with the process owners
responsible for each of the elements. This working partnership and culture of collaboration is
supported by unit leadership meetings, daily interdisciplinary rounds, safety huddles and monthly
safety rounds.
Improvement Results
Anecdotally, staff report improved teamwork between the nurses and other medical staff as well
as a general sense of increased job satisfaction. Interdisciplinary rounds are key to facilitating
overall culture change and implementation of the other 12 elements. Additionally, as care teams
work together to implement the 13 MCB elements, they expose other challenges and barriers to
quality patient care. Barriers at the unit level are addressed by the core team. Where the barriers
exist beyond the unit level, unit leaders are empowered and encouraged to develop solutions and
communicate challenges back to MCB leadership- creating an ongoing quality improvement
cycle. Results from an organization-wide culture of safety “check-up”, expected in October 2014,
will hopefully highlight greater improvements for MCB units relative to non-MCB units, thereby
reinforcing the value of the initiative.
While it is too early to attribute improvements to MCB, immediate gains in patient satisfaction
and length of stay (LOS) scores were observed for initial MCB units in the 3-month period
System Quality Review
238
NewYork-Presbyterian Healthcare System Quality Symposium 2014
Quality 2020: A Vision of the Future
following implementation. Specifically, compared to non-MCB units, MCB units showed gains in
communication-related HCAHPS domains such as RN and MD communication, pain
management, and discharge information (see Figure 3). Improvement in LOS scores was also
observed in MCB units; units showed a 12% decrease in the variance between their actual LOS
and their expected LOS (See Figure 4).
Current outcome data are inherently subject to time lags, accentuating the need for more
immediate understanding of performance. While process metrics have not been identified for all
elements due to inherent documentation barriers, those that do have defined capabilities have
shown clear changes in behavior. For instance, screening patients for discharge planning within
24 hours of admission significantly increased post-implementation and proper use of the NYP
Care Team widget has steadily improved since January 2014. Additional measures are being
developed based on feedback from the frontline teams.
Sustainability Strategies
MCB is not a program limited to implementing the 13 elements; rather it represents a culture
shift in how NYP approaches evidence-based quality improvement. Once a working partnership
is established between the unit Medical Director and Patient Care Director, QPSI Mangers are
able to transition to serve as outside support. At this point, change and accountability are wholly
owned at the unit level and the tracking of outcomes and process measures contribute to the
accountability of the core teams. As such, trends in data serve as signals that can drive innovation
across the areas of communication, patient engagement and care management. Many of the
elements, such as the Care Team Widget and interdisciplinary rounds, serve to support this
culture change.
As MCB is rolled out to the remaining units, the initial units will share lessons learned; ultimately
each unit will undertake its own rapid cycle improvement process though as its core team learns
what’s optimal for their group. Once the elements are implemented across the institution they
will become part of the culture and accepted standard practices at NYP as well as integrated into
the onboarding of new residents and nurses. This infrastructure and culture change will allow
NYP to continue to improve standardized care across the institution.
Lessons Learned
1. Resource Support: Units need dedicated project management resources, even if only
temporarily, to implement and sustain changes and to empower unit leadership.
2. Defined Goals: Reasonable targets that allow units to quickly achieve short-term successes
need to be identified and clearly defined
3. Metrics and Accountability: Data need to be continuously reviewed at all levels of leadership to
ensure continuous improvement and accountability.
Conclusion
Making Care Better has created a defined infrastructure by which evidence-based care redesign
initiatives can be implemented in a standardized way across NYP. The 13 elements facilitated the
creation of this infrastructure by improving unit-level leadership, enhancing communication and
collaboration both within and between units, fostering a culture of accountability, and infusing
System Quality Review
239
NewYork-Presbyterian Healthcare System Quality Symposium 2014
Quality 2020: A Vision of the Future
care management into the inpatient experience through a rapid cycle improvement process.
Elements that reinforced communication and collaboration had the greatest short-term effect.
Although identifying process measures that isolate and measure short-term change continues to
be a challenge, additional measures are being developed based on feedback from the core unit
teams. Some immediate, short-term improvements in outcome measures have been realized and
anecdotal evidence from core unit teams indicate continuing support for the initiative.
The structures put in place through MCB will continue to support a culture of communication.
Once the elements are implemented, the availability of trended and real-time data allows units to
track their progress in real time, thereby fostering a culture of leadership and accountability which
drives change. The emphasis on data as an essential component of monitoring unit performance
will help ensure that unit leadership remains accountable for sustaining the core tenets of the
initiative.
Figure 1.
System Quality Review
240
NewYork-Presbyterian Healthcare System Quality Symposium 2014
Quality 2020: A Vision of the Future
Figure 2.
System Quality Review
241
NewYork-Presbyterian Healthcare System Quality Symposium 2014
Quality 2020: A Vision of the Future
Figure 3 - Cohort A Performance
Changes in HCAHPS Scores
Variance in HCAHPS Scores
Pre- vs. Post-MCB Implementation
Overall Rating (9-10)
Comm. w/ Nurses
3.6%
0.2%
Comm. w/ Doctors
Comm. about Meds
0.1%
Pain Management
-2.6%
-1.9%
-0.1%
Discharge Info
3.4%
2.8%
2.3%
2.1%
Cleanliness
0.2%
MCB Cohort A Units
Pre-MCB Implementation HCAHPS Scores
4.0%
0.0%
0.7%
0.5%
Staff Responsiveness
Quietness
3.7%
1.2%
MCB units showed greater gains-especially in
communication-in the 3 months post-MCB
implementation but…generally they had lower scores at
baseline compared to non-MCB units.
4.2%
Overall Rating
Comm. w/ Nurses
Comm. w/ Doctors
Staff Responsiveness
Comm. about Meds
Pain Management
Quietness
Cleanliness
Discharge Info
50%
60%
Non-MCB Units
70%
80%
90%
MCB Cohort A Units
Notes
Based on “Discharge Date” not “Survey-Received Date”
Positive values indicate improvement
3-month period prior to MCB: Dec 1, 2013 – Feb 28, 2014; 3-month period post-MCB: Mar 1,
2014 – May 31, 2014
System Quality Review
242
100%
NewYork-Presbyterian Healthcare System Quality Symposium 2014
Quality 2020: A Vision of the Future
Although 8 out of 12 MCB units showed gains in
reducing their LOS variance in the 3 months
following MCB implementation compared to the
3-month period prior to implementation…MCB
units showed only a 12% reduction in LOS
variance pre- vs. post-MCB while non-MCB units
showed a 32% reduction in LOS variance over
the same time period.
Change in LOS Variance (Actual – Expected)
Pre- vs. Post-MCB Implementation
3.00
0.07
0.00
-0.83 -0.72
-0.66
-2.11
-3.00
-0.49
-0.24 -0.17
-0.07
0.47
0.32 0.42
2.00
1.57
1.50
1.00
0.50
0.00
0.45
0.30
Non-MCB Units
MCB Cohort A Units
Notes
Negative values indicate improvement (i.e., reduction in actual LOS compared to expected LOS).
3-month period prior to MCB: Dec 1, 2013 – Feb 28, 2014; 3-month period post-MCB: Mar 1,
2014 – May 31, 2014
System Quality Review
1.38
243
NewYork-Presbyterian Healthcare System Quality Symposium 2014
Quality 2020: A Vision of the Future
Poster Presentation
NewYork-Presbyterian/Lawrence Hospital
A Three Year Journey: Prevention of Central Line Associated Blood Stream
Infections
Mary Ann Hauff, BS, MS, RN, ANP, CIC; Maria Otto, RN-C, CIC; Christina Hing, RN, MS, FNP-BC; Dionne
Bernadel, RN, MSN, Gail Wilson, RN, BSN, MHAN; Missy Paolicelli, RN, OCN, MSN; Tina Sokolik RN, BSN,
MSN; Barbara Choy, CCRN, BSN, MSA
Introduction
Catheter Associated Blood Stream infections are associated with increased patient morbidity and
mortality, prolonged lengths of stay and decreased patient satisfaction. Leadership and the Board
of Governors identified this as a priority for the institution.
At the outset of this project, the 2011 Infection Control surveillance identified 23 catheter
associated infections between house-wide, and CCU. Housewide rates were 10.74 catheter
infections per 1,000 device days. The Critical Care Unit infection rate for the same period was
5.72 infections per 1,000 device days.
The organization set a goal of 0 central catheter associated infections by December, 2013.
Utilizing a multi-pronged approach the organization has significantly decreased the central line
associated infection rate. The house-wide CLABSI rate declined to 1.87 in 2012, and to 0.73 in
2013. Through July, 2014 this rate has further declined to 0.38.
The Critical Care Unit infection rate for the same period was 5.72 infections per 1,000 device
days in 2011 and 1.59 and 1.17 in 2012 and 2013, respectively. Through July, 2014 this rate has
increased slightly to 1.24.
Quantitative/Qualitative Measures
The Central Line Associated Blood Stream Infection Surveillance is conducted by the Infection
Control Department.
At the onset of this initiative in 2011, the house-wide CLABSI rate was 10.74 per 1,000 device
days. This rate declined to 1.87 in 2012, and to 0.73 in 2013. Through July, 2014 this rate has
further declined to 0.38.
The Critical Care Unit infection rate for the same period was 5.72 infections per 1,000 device
days in 2011 and 1.59 and 1.17 in 2012 and 2013, respectively. Through July, 2014 this rate has
increased slightly to 1.24.
System Quality Review
244
NewYork-Presbyterian Healthcare System Quality Symposium 2014
Quality 2020: A Vision of the Future
Methodologies
The organization utilizes the PDCA model for all of its Performance Improvement Projects.
The most critical aspects of this implementation were the engagement of multiple levels of
personnel, the use of multiple strategies, ongoing measurement of outcomes and the
implementation of additional interventions to achieve the desired results.
Improvement Results
The organization utilized multiple strategies designed to achieve this goal.
This included implementation of evidence based practices that have demonstrated efficacy in the
reduction of central line associated infections such as the central line insertion checklist. The
checklist was accompanied by practice changes including the adoption of of antibiotic
impregnated PICC lines by the Department of Radiology, color coding IV tubing labels to
indicated tubing changes, adding SwabCap to all IV lines and the addition of Biopatch dressing to
all central lines. These initial interventions were followed by the introduction of Chlorhexidene
baths for all patients with central lines.
It was recognized that the proper nursing maintenance and documentation of central line care
was essential to achievement of this goal. A major educational initiative was undertaken in 2012
that included presentation of Grand Rounds on Prevention of Central Line infections by the IV
nurse, inclusion of central line care in the annual nursing competency day, observation of central
line dressing changes by the IV nurse.
Femoral lines are used only in an emergency and must be removed within 24 hours.
Leadership was involved in daily rounding of patients with central lines and observed practice at
the bedside to stress to staff the importance of improving practice.
The effectiveness of these interventions was evaluated by the ongoing measurement of the
central line associated infection rate and the reporting of these results to all levels of the
organization including all nursing units, the Infection Control Committee and to the Board.
Sustainability Strategies
Nursing managers have taken a significant role in leading this initiative and ensuring its ongoing
success at the unit level.
Data measuring the incidence of central line associated infections is shared with all nursing
personnel on an ongoing basis and is prominently posted on all nursing units.
Lessons Learned
1. All levels of leadership must demonstrate their engagement in the process.
2. Practice change must include classroom education as well as observation at the bedside.
3. Frequently share the data with the staff responsible for the process.
System Quality Review
245
NewYork-Presbyterian Healthcare System Quality Symposium 2014
Quality 2020: A Vision of the Future
Conclusion
NewYork Presbyterian/ Lawrence Hospital established a goal of 0 Central Line Associated Blood
Stream Infections. At the onset of this initiative in 2011the House-wide Catheter related infection
rate was 10.74 per 1,000 catheter days, far above the NHSN benchmark of 1.2.
With the introduction of various initiatives, the house-wide CLABSI rate declined to 1.87 in
2012, and to 0.73 in 2013. Although the 0 goal was not achieved by the end of 2013, through
July, 2014 this rate has further declined to 0.38.
The Critical Care Unit infection rate for the same period was 5.72 infections per 1,000 device
days in 2011 and 1.59 and 1.17 in 2012 and 2013, respectively. The actual number of infections
dropped from 23 in 2011 to 2 through July 2014.
System Quality Review
246
NewYork-Presbyterian Healthcare System Quality Symposium 2014
Quality 2020: A Vision of the Future
Poster Presentation
NewYork-Presbyterian Hospital
NSQIP-Focused Departmental Semiannual Grand Rounds Reports: Utilizing
an Educational Conference to Improve Outcomes
Carol Gellman, RN, MSN, Senior Performance Improvement Specialist; Theresa Frey, MS, PA, SCR-ACS NSQIP
Introduction
Urinary tract infections and surgical site infections are common hospital acquired infections.
These infections increase length of stay, costs, readmission rates and patient morbidity and
mortality. The American College of Surgeons-National Surgical Quality Improvement Program
(NSQIP) is an outcomes-based program to measure such infections, and provides data to initiate
interventions to improve the quality of surgical care. Efforts at improving surgical outcomes have
previously focused on procedural length, structural and process measures. The use of NSQIP
data provides a key tool in the process required to facilitate surgical quality improvement.
Starting in 2010, the Department of Surgery, along with the Division of Quality and Patient
Safety, presented semi-annual reports summarizing NSQIP data at Departmental Grand Rounds.
Many outcomes were rated "exemplary" or "as expected". However, two outcomes, urinary tract
infections and surgical site infections were noted as "needs improvement". An educational forum
was initiated to promote awareness of NSQIP data, educate surgical providers about needed
improvements, identify quality improvement targets and deliver updates about improvements
after interventions. The goal was to reduce UTI and SSI rates to below the national benchmark.
The long range goal is to continue tracking performance, further reduce hospital acquired
infections, and improve the quality of care. We are striving for all results to be "exemplary".
This enhancement of care identifies future quality improvement targets, improves patient care
and outcomes, and decreases institutional healthcare costs.
Quantitative/Qualitative Measures
A multidisciplinary team was formed to perform an intensive case-by-case analyses of each
urinary tract infection and surgical site infection. The root cause of the each infection was
investigated & several causative factors were identified. Factors for UTIs included appropriate
use of Foley catheter, technique of insertion, length of time for indwelling catheter left, and
management of urinary retention. Factors for SSIs included pre-operative antibiotic prophylaxis,
temperature control, skin preparation and wound closure.
System Quality Review
247
NewYork-Presbyterian Healthcare System Quality Symposium 2014
Quality 2020: A Vision of the Future
Methodologies
NSQIP methodology was utilized. NSQIP is a validated, data-driven, outcomes based program
to measure and improve the quality of surgical care. All measures are 30-day outcomes and are
compared to other NSQIP participating hospitals. There are approximately 450 participating sites
in the US and around the world.
The program prospectively collects clinical data to quantify 30-day risk adjusted surgical
outcomes and allows for external benchmarking of outcomes among participating hospitals.
Case-by-case analyses, literature reviews and reviews of best practices led to the development of
specific quality improvement initiatives. Blind physician summary was provided for individual
audit and feedback.
Improvement Results
Although the forums were initiated in 2010, significant results started to occur in 2012.
UTI rates in Q2 2012 were as high as 3.3%, with a benchmark of 1.5%. There was a significant
decrease in Q3 down to 1.8%, nearing the benchmark of 1.5%. In Q1 2013, the rates fell below
the benchmark, which was the first time in several years. By Q4 2013, the UTI rate was 1.4%. As
can be seen in the linear rate, there is a steady, continual downward trending. (Slide 1)
The SSI rate was 3.1% in Q2 2012, which was above the benchmark of 2.9%. By Q1 2013, the
rate steadily decreased down to 1.6%, well below the benchmark of 2.6%. By Q3 2013, the SSI
rate was down to 1.2%, well below the benchmark of 2.5%. As can also be seen in the linear rate,
there is a steady, downward trending. (Slide 2)
Sustainability Strategies
Incorporating surgical outcomes and NSQIP data into faculty and resident education is an
effective method of increasing awareness of quality improvement initiatives and improving
surgical outcomes. Quarterly Grand Round have been planned to continue utilizing NSQIP data.
The Skills Acquisition Laboratory, a simulated training lab, is utilized for education in correct
aseptic technique insertion and care for Foley catheters. This is now a mandatory requirement for
all incoming residents and medical students.
Lessons Learned
1. Communication is a powerful tool to raise awareness and encourage participants to take
ownership and responsibility.
2. Don't re-invent the wheel.
3. Strong leadership is essential, but quality improvement is a multi-disciplinary effort.
Conclusion
Targeted Departmental educational meetings such as Grand Rounds is a suitable forum to review
surgical data and outcomes. The establishment of NSQIP-focused Grand Rounds led to
significant, sustained improvement in urinary tract infection and surgical site infection rates. This
will lead to improvement in surgical care, decreased length of stay and significant cost savings.
System Quality Review
248
NewYork-Presbyterian Healthcare System Quality Symposium 2014
Quality 2020: A Vision of the Future
The departmental lead approach is a proven, durable method to improve surgical outcomes.
These initiatives would be at a greater benefit if expanded hospital-wide.
NYP/WC NSQIP UTI Rates
30 Day Outcomes
4
3
Percent
2
1
0
3.3
1.5
Q2
2012
1.4
1
Q3
2012
UTI Rate
Q4
2012
Q1
2013
Benchmark
Q2
2013
Q3
2013
Q4
2013
Linear (UTI Rate)
ACS NSQIP Post-Operative Summary
System Quality Review
249
NewYork-Presbyterian Healthcare System Quality Symposium 2014
Quality 2020: A Vision of the Future
NYP/WC NSQIP SSI Rates
30 Day Outcomes
4
3
3.1
2.9
2.5
2
1.2
1
0
Q2 2012 Q3 2012 Q4 2012 Q1 2013 Q2 2013 Q3 2013
SSI Rates
ACS
System Quality Review
NSQIP
Benchmark
Linear (SSI Rates)
Post-Operative
Summary
250
NewYork-Presbyterian Healthcare System Quality Symposium 2014
Quality 2020: A Vision of the Future
Poster Presentation
NewYork-Presbyterian Hospital
Targeted Continuous Real-Time Assessment of a Workflow Process Improves
Quality of Care and Decreases Expenditures
Irina Lutinger, FACHE, MPH, MASCP, MT(ASCP)DLM; Eldad A. Hod, MD; Alexander Kratz, MD, PhD
Introduction
Problem Statement:
In order to start potentiallly life-saving procedures in a timely manner and to be able to discharge
patients quickly, all Emergency Departments (EDs) need rapid turnaround times for certain
laboratory tests. An example of such an assay is the cardiac marker troponin. Rapid availability of
this result allows faster diagnosis of heart attacks and enables ED staff to start potentially lifesaving therapy sooner. It also allows faster decisions as to whether a patient needs to be admitted
or can be safely discharged from the ED.
Until December 2013, the NYPH/CUMC Core Laboratory offered a special STAT Troponin
assay to the patients of the adult ED: This assay was performed 24/7/365 on dedicated
instruments in the STAT area of the Core Laboratory by technologists assigned to performing
this test, in a workflow entirely separate from troponin testing for all other samples submitted to
the laboratory for troponin testing. This setup was associated with additional expenditures for
labor, instrumentation, and reagents, yet it did not consistently meet the turnaround time needs
of the patients and clinical staff of the ED.
Project Aim: The aim of this project was to demonstrate that with appropriate supervision and
intensive, continous monitoring, separate workflows that have been created to serve
subpopulations of patients can be safely integrated in the general workflow, with improvements
in the quality of patient care and significant reductions in hospital expenditures.
Quantitative/Qualitative Measures
The measures used to monitor the success of the initiative were:
1) The percentage of troponin samples from the Milstein ED that were completed within one
hour.
2) The amount of Laboratory Technologist FTE time that was assigned to performing troponin
testing for the Milstein ED.
System Quality Review
251
NewYork-Presbyterian Healthcare System Quality Symposium 2014
Quality 2020: A Vision of the Future
Methodologies
The Quality Improvement Principles applied were: Customer focus, team approach, data-driven
decisions, improve entire processes, continual improvement.
We reached out and met with the Emergency Department's clinical leadership to assess their
needs and service expectations regarding troponin testing (customer focus) and determined with
them the best approach to meet these expectations (team approach). We then collected data on
the present level of service, performed an intervention, and collected data on the situation after
the intervention (data-driven decisions). We strove to improve the process, not individual
performance, and we continue to monitor and look for ways to further improve our service
(continual improvement).
Improvement Results
We collected data on the lenght of time it took the Core Laboratory to result samples received
for troponin testing before the intervention. Turnaround Times (TAT) were defined from receipt
in the laboratory to reporting of the results in the hospital's electronic medical record. These data
were obtained through reports run in the Laboratory Information System. The reports indicated
that it took the Core Laboratory
90 minutes to report over 90% of all samples received for STAT troponin testing. Service
expectations were completion of over 90% of samples within one hour.
We concluded that in spite of the use of instrumentation and staff dedicated to troponin testing
for the ED, our turnaround times did not meet service expectations.
After discussions with ED leadership, we discontinued the use of dedicated instruments and staff
for ED troponins. Instead, all ED samples are now analyzed on the same instruments and by the
same staff as samples from all other areas of the hospital. All clerical staff, laboratory
technologists, and supervisors were in-serviced on the need to analyze STAT troponin samples as
quickly as possible. The Assistant Director of the Laboratory monitored the troponin turnaround
times daily and followed up on each sample that missed service expectations. The root causes of
each service delay was determined and addressed. For example, when we discovered that
samples with very low results were not automatically released, we implemented an IT solution to
this problem.
Turnaround times for troponin assays for the ED improved dramatically. Over 90% of samples
are now resulted within 45 minutes. This is a significant improvement for patient care and
throughput of the ED. Furthermore, by eliminating the use of dedicated staff for these assays,
approximately 2.2 Laboratory Technologist FTEs were saved and redistributed to other critical
testing areas. Finally, the Whole Blood Troponin instruments with all associated costs were
eliminated. See Table 1.
Sustainability Strategies
Monitoring of turnaround times for troponin for the ED continues. At the end of every 8-hour
shift, the shift supervisors review all troponin results and include in their shift reports the number
of samples received and the number of outliers. All outliers are investigated by the supervisors
and explained in the shift report. The shift report is sent to all supervisors, managers, and
System Quality Review
252
NewYork-Presbyterian Healthcare System Quality Symposium 2014
Quality 2020: A Vision of the Future
directors. Monthly statistics are compiled and sent to all stakeholders and discussed at QA
meetings.
Lessons Learned
1) A dedicated separate workflow for "special" samples is not necessarily faster or better than an
optimized workflow for all samples.
2) Close assessment of a workflow process can significantly improve the outcome and lead to
better service and substantial labor savings.
3) Continuous real-time monitoring of a process can sustain its smooth functioning and avoid
relapse.
Conclusion
We discontinued the use of separate instrumentation and personnel for certain samples and
replaced it with continous, real-time monitoring of the general workflow. This allowed us to
improve turnaround times for clinically crucial laboratory results and to realize significant savings
in labor costs. This approach may be applicable in other areas of the hospital's laboratories as
well as in other areas of the NYPH Health Care System.
Table 1
Service Improvement:
Time to complete 90% of samples received
Financial Improvements:
Laboratory technologist FTEs
to ED troponin testing
Savings in cost of labor
dedicated
Savings in cost of reagents/consumables
System Quality Review
Before Intervention
After Intervention
90 minutes
45 minutes
2.2
0
Approximately $
154,000/year
Approximately
$252,000/year
253
NewYork-Presbyterian Healthcare System Quality Symposium 2014
Quality 2020: A Vision of the Future
Poster Presentation
NewYork-Presbyterian/Columbia University Medical Center
Pediatric Surgical Care Improvement Project: Improving Perioperative
Prophylaxis and Reducing Surgical Site Infection Rates
Lisa Saiman, MD, MPH; Litty Varghese, BS; Michael Vitale, MD, MPH; David Roye, MD; Benjamin Roye, MD,
MPH; Jennifer Crotty RN, MSN, CPNP; Hiroko Matsumoto, MA; Rozelle Corda, FNP; Emile Bacha, MD; Ganga
Krishnamurthy, MD; Neil Fieldstein, MD, FACS; Rich Anderson, MD, FACS, FAAP; Bill Middlesworth, MD;
Gudrun Aspelund, MD, MS; Steve Stylianos, MD; Robert Kazim, MD; Anthony Clapcich, MD; Amy Mesa-Jonassen,
MD; Brian Thumm; Diane Mangino, Rn, MSN, CIC1; Maria Messina RN, BSN, CIC1; Natalie Neu, MD, MPH;
Ava Brozovich, MPH; Megan Murray, MPH; Elizabeth Salsgiver, MPH, and Philip L Graham, MD MS
Introduction
Surgical Site Infections (SSIs) are responsible for significant mortality, morbidity and healthcare
costs. The impact of standardizing peri-operative antibiotic prophylaxis on SSIs has been studied
in adults as part of the Surgical Care Improvement Project (SCIP). The effect of standardizing
peri-operative antibiotic prophylaxis on SSI rates in the pediatric population is not well described.
We developed standardized guidelines for peri-operative prophylaxis in children cared for at
NewYork-Presbyterian Morgan Stanley Children's Hospital and monitored adherence to these
guidelines. Our program is called pediatric SCIP (pSCIP). We began our work with the pediatric
spine service in 2008, with the cardiothoracic surgery service and neurosurgeons in 2011, and
with general surgery in 2013.
For the pediatric spine service, in addition to peri-operative antibiotic strategies that were tailored
to the polymicrobial pathogens frequently associated with SSIs in this population, we also
developed an expanded pre-operative, intra-operative, and post-operative bundle to reduce SSIs.
Examples of pre-operative strategies included chlorhexidine bathing the night and morning prior
to surgery, intra-operative strategies included appropriate skin disinfection and instillation of
vancomycin into the operative site, and post-operative strategies included optimizing dressing
management. For the pediatric cardiac service, we discontinued the practice on continuing
prophylaxis until the chest tubes were removed. For the general surgery service, we characterized
the different types of surgery into discrete categories and developed specific recommendations
for each. We also developed recommendations for low risk general surgical procedures that did
not require peri-operative prophylaxis.
We hypothesize that measuring adherence to evidence-based peri-operative antibiotic prophylaxis
and providing feedback to the pediatric surgical and anesthesiology teams would improve
adherence to peri-operative prophylaxis. We further hypothesized that adherence would reduce
SSI rates.
Thus, the aims of this project were [1] to develop guidelines for appropriate antibiotic selection,
dose, pre-operative timing, intra-operative redosing for relevant cases, and discontinuation of
System Quality Review
254
NewYork-Presbyterian Healthcare System Quality Symposium 2014
Quality 2020: A Vision of the Future
antibiotics for scoliosis repair, cardiac surgery, ventriculoperitoneal (VP) shunt placement and
general surgical procedures, [2] to monitor adherence to these parameters for these types of
surgical procedures, and [3] to calculate SSI rates and associated pathogens for selected surgical
procedures.
Quantitative/Qualitative Measures
The following quality process measures were analyzed: [1] correct selection of antibiotics for
different types of procedures, [2] correct dose of each agent, [3] correct administration time prior
to surgical incision, [4] correct intra-operative dosing for surgical procedures > 4 hours in
duration, and [5] correct discontinuation of antibiotics.
The following quality outcome measures were analyzed: [1] SSI rates following scoliosis repair for
both idiopathic and non-idiopathic scoliosis and [2] neonatal and pediatric cardiac surgery.
Methodologies
During the past 5 years, we have been establishing interdisciplinary teams consisting of surgeons,
anesthesiologists, infectious disease specialists, pharmacologists, and infection prevention and
control experts to develop standardized peri-operative prophylaxis regimens based on review of
the literature, local practices, and the local epidemiology of SSI pathogens and their antimicrobial
susceptibility patterns. We established the quality process measures described above with these
teams and provided them with pre-pSCIP baseline rates of adherence to these parameters and
baseline SSI rates for selected surgical procedures. We then provided post-pSCIP feedback
quarterly to the relevant surgical and anesthesiology teams as well as the NYP SSI Prevention
Committee. We reviewed SSIs and adherence to the process measures for each SSI in small
group huddles with the relevant surgical teams.
Improvement Results
Adherence to peri-operative antibiotics improved substantially (Table). For scoliosis repair, the
rate increased from 83% to 95% for all 5 process measures by Q2 2014. For neonatal cardiac
surgery, the rate increased from 95% to 98% by Q2 2014. For pediatric cardiac surgery, the rate
remained stable at 96%. For VP shunt placement, the rate increased from 92% to 98%. Analyses
Q2 2014 for general surgical procedures is ongoing.
Furthermore, the SSI rate for scoliosis repair declined significantly (p=<0.0001). The decline in
rate associated with other preventive strategies is shown in the Figure. The SSI rate among
pediatric cardiothoracic surgery patients has been stable. In neonatal cardiac patients, the SSI rate
per 100 procedures was 4.72 in 2011 and 3.70 in 2013 and in pediatric cardiac patients was 0.96
in 2011 and 0.76 in 2013.
Sustainability Strategies
The strategies implemented in this project have been sustained for varying time periods for
different surgical services ranging from 2008 for the pediatric spine service to 2013 for the
general surgery service. By engaging the various surgical teams in both the audit and feedback
process at the Pediatric OR Committee meeting quarterly, we have sustained our efforts. As
further evidence of the success of our strategies, we will expand our efforts to the pediatric
System Quality Review
255
NewYork-Presbyterian Healthcare System Quality Symposium 2014
Quality 2020: A Vision of the Future
genitourinary surgical service in 2014 which will serve as their baseline adherence. It is critical to
provide both process and outcome measures to engage the key stakeholders.
Lessons Learned
[1] Interdisciplinary teams are key to developing successful strategies for quality improvement.
[2] Application of strategies developed in adult populations can be effective in the pediatric
population.
[3] Regular audit of data and feedback are critical to sustain key stakeholder buy-in and sustained
involvement.
Conclusion
In conclusion, we have successfully implemented standardized practices for perioperative
prophylaxis for children. Adherence to these recommendations continues to improve with an
associated decline in SSIs. Ongoing work will expand these efforts to other pediatric surgical
services including those at Weill Cornell.
System Quality Review
256
NewYork-Presbyterian Healthcare System Quality Symposium 2014
Quality 2020: A Vision of the Future
Table: Compliance with process measures by surgical service
≥95% adherence
90-94% adherence
<90% adherence
System Quality Review
257
NewYork-Presbyterian Healthcare System Quality Symposium 2014
Quality 2020: A Vision of the Future
Figure: Surgical Site Infection Rate following Scoliosis Repair and Association with Pre-, Intra-, and Postoperative Interventions to Reduce SSIs, 2008-2014
System Quality Review
258
NewYork-Presbyterian Healthcare System Quality Symposium 2014
Quality 2020: A Vision of the Future
Figure 2: Rate of SSIs in the Cardiac NICU
Number of Infections
MSCHONY NICU Surgical Site Infections 2010 - Q2 2014
Number of Procedures
SSI rate/100 Procedures
3.5
45
35
Number of Infections
2.5
30
2
25
1.5
20
15
1
Rate Per 100 Procedures
40
3
10
0.5
5
0
0
Quarterly Quarterly Q1 2012
Average Average
2010
2011
System Quality Review
Q2 2012
Q3 2012
Q4 2012
Q1 2013
Q2 2013
Q3 2013
Q4 2013
Q1 2014
Q2 2014
Quarter
259
NewYork-Presbyterian Healthcare System Quality Symposium 2014
Quality 2020: A Vision of the Future
Figure 3: Rate of SSIs in the Cardiac PICU
Number of Infections
Number of Procedures
SSI Rate/100 Procedures
MSCHONY PCICU Surgical Site Infections 2010 - Q2 2014
3.5
120
3
Number of Infections
2.5
80
2
60
1.5
40
1
Rate Per 100 Procedures
100
20
0.5
0
0
Q1 2012
Q2 2012
Q3 2012
Q4 2012
Q1 2013
Q2 2013
Q3 2013
Q4 2013
Q1 2014
Q2 2014
Quarter
System Quality Review
260
NewYork-Presbyterian Healthcare System Quality Symposium 2014
Quality 2020: A Vision of the Future
NewYork-Presbyterian/Columbia University Medical Center
MD Cart: Standardizing Supplies to Improve Provider Workflow
Hunt Tristan BS; Yang, Jesse MD
Introduction
Throughout the Milstein Hospital Building at New Presbyterian Hospital, every unit has a clean
supply room with an inventory tailored to the needs and utilization of that specific unit. As
required items and relative inventories have changed over the last several years, the organization
of each unit's supply room has adapted to accomodate those changes. While many units have
overlapping inventories, currently no two supply rooms are organized the same way.
For providers, especially residents, who have patients on multiple units, these varied
organizations can become a cause for significant frustration. Searching from floor to ceiling with
a sense that few items are ever in the same place wastes precious minutes for every visit to a
supply room while leaving providers disheartened. Often, providers abandon their search and
either take the needed items from other supply rooms or from the ICUs where they know the
items can be found. In addition, when providers do find high value items that are difficult to find,
they occasionally create stashes of these items in their white coats or resident lounges to avoid
future futile searches.
Thus, the lack of standardized organization across all the supply rooms wastes not only provider
time and energy, but also wastes hospital resources and complicates accounting as items are taken
from unit and ICU supply rooms that are not actually used for patient care in those locations.
To address this problem, we first aimed to quantitatively and qualitatively measure the time and
energy currently expended by residents to search for items in the supply rooms. Next, we
identified a list of items most commonly searched for by residents which were common to all
supply rooms. Finally, we designed a lay-out for an 'MD Cart' which would place each item from
that list in a specific location and which could be standardized across all supply rooms.
As a pilot, we implemented the MD Cart in 3 units which medicine residents use most often.
Our goal was to decrease both the time and energy expended by residents searching for supplies
while also decreasing waste due to personal stashes of items and taking items from other units.
System Quality Review
261
NewYork-Presbyterian Healthcare System Quality Symposium 2014
Quality 2020: A Vision of the Future
Quantitative/Qualitative Measures
We measured both nurses and residents on 30 random encounters in 3 different supply rooms
(10 nurses and 10 residents per supply room). For each encounter we measured the time spent in
the supply actively looking for items, which specific items were retrieved, and the physical path
taken by the individual through the supply room as they searched for items. Prior the individual
leaving the supply room, we asked whether any items could not be found.
In addition, 5 residents performed time trials in the 3 supply rooms. We established 6 different
kits of items to be retrieved - Phlebotomy, Paracentesis, Central Line, Duo/NG Tube, and 2
Miscellaneous. In each room, each resident selected 2 kits at random and we measured the time
it took to find the complete set of items as well measured the physical path they took to look for
items. If the resident could not find an item we asked them to continue searching until they felt
would abandon the search under normal circumstances.
Both the randomized encounters and time trials were measured pre- and post-MD Cart
implementation.
Methodologies
-5S Principles (Sort, Set, Shine, Standardize, Sustain)
-Systems based practice - understanding what processes were involved in the current supply
room situation, who were the players involved in redesign, who would stand to benefit
-Data driven improvement - collected data on time and resources wasted with the current supply
room design
Improvement Results
Preliminary data collected of 20 nurses and 20 residents:
Average time for nurses to find an item: 19.4 seconds
Average time for residents to find an item: 88.9 seconds
P value - 3.6x10^(-5),
=Average time to find an item is significantly different between nurses and residents.
Please see Figure 1 and Figure 2
Final results are pending as the supply room redesign is currently underway. We will be collecting
data once the pilot redesign has been completed.
System Quality Review
262
NewYork-Presbyterian Healthcare System Quality Symposium 2014
Quality 2020: A Vision of the Future
Sustainability Strategies
At 6 months post implementation we will seek formal feedback about the supply rooms,
specifically asking if there any items providers cannot easily and consisently locate. At that time
we will check each supply room the MD Cart has been implement against the standard MD Cart
Layout to ensure items have not been moved or rearranged. If items have been re-arranged we
will work with materials management and Patient Care Directors of those specific to review
PARS data and determine why the organization occurred and whether a revision to the standard
MD Cart may be necessary.
Lessons Learned
1. Finding a way to quantitavely measure and capture subjective complaints can be very difficult.
2. Establishing and maintaining a standard layout and workflow within a large organization
requires dilligence, excellent forethought and a wide team of contributors.
3. Even small decisions and seemingly inconsequential choices can impact the quality and value
of patient care.
Conclusion
Through implementing a standard MD Cart through multiple supply rooms, we were able to ease
residents subjective complaints and frustrations while also reducing the amount of time spent
looking for supplies and potentially reducing the amount of clean supply waste. Sustaining these
improvements will require periodic review of the MD Cart items and layout as the needs of each
unit change. Furthermore, our project suggests a larger study would be warranted, exploring ways
to standardize the organization, lay out and even stocking system of the entire supply room.
System Quality Review
263
NewYork-Presbyterian Healthcare System Quality Symposium 2014
Quality 2020: A Vision of the Future
Figure 1
System Quality Review
264
NewYork-Presbyterian Healthcare System Quality Symposium 2014
Quality 2020: A Vision of the Future
System Quality Review
265
NewYork-Presbyterian Healthcare System Quality Symposium 2014
Quality 2020: A Vision of the Future
System Quality Review
266
NewYork-Presbyterian Healthcare System Quality Symposium 2014
Quality 2020: A Vision of the Future
System Quality Review
267
NewYork-Presbyterian Healthcare System Quality Symposium 2014
Quality 2020: A Vision of the Future
Figure 2:
System Quality Review
268
NewYork-Presbyterian Healthcare System Quality Symposium 2014
Quality 2020: A Vision of the Future
NewYork-Presbyterian/Weill Cornell Medical Center
Dissecting Transitions of Care Between Nursing Homes and the Emergency
Department: How well are we doing?
Dana C. Walker; Mary R. Mulcare, MD1; Tony Rosen, MD, MPH; Regina Mysliwiec, MD; Sunday Clark, ScD; Michael
E. Stern, MD; Mark S. Lachs, MD; Neal E. Flomenbaum, MD
Introduction
More than 25% of nursing home (NH) residents visit the emergency department (ED) at least
once annually. Significant barriers to providing high quality care to NH patients in the ED
include lack of access to important and relevant medical information, and ineffective
communication between NH, EMS and ED providers. To address these barriers, SAEM and
ACEP’s 2009 Geriatric Task Force created 11 quality indicators (QIs) for transitions between
NHs and EDs (see Table 1). The objective of this study was to determine how well providers
caring for NH residents transitioning to and from the ED fulfilled the 9 QIs applicable to the
immediate process.
One known study has assessed alignment with the first 5 QIs, but no known study has done this
for the remaining QIs. This study is unique as it assessed how well NH and ED providers
fulfilled the 9 QIs applicable to a NH resident’s arrival at and discharge from the ED.
Methodologies
We conducted a retrospective chart review of all patients presenting to NewYork-Presbyterian
Cornell's ED from NHs from April 2011- March 2012. Data pertinent to the quality indicators,
patient stay in the hospital, and demographics was captured for each patient from the electronic
medical record (EMR). Patients’ NH paperwork was assessed for alignment with QIs 1-5 and ED
provider notes were assessed for alignment with QIs 6-9. Data were analyzed using Stata, and
results were presented as proportions with 95% CIs.
Improvement Results
171 patients (11.5%) were transferred to the ED from a NH. As seen in Table 2, 85% percent of
NH paperwork contained a reason for transfer; 85% listed medication allergies; 52% noted
advanced directives; and 46% contained contact information for the NH provider should urgent
communication be required. 70% of NH paperwork included a medication list. NHs requested a
specific test to be done upon transfer in 4% of cases (all CT scans), and ED providers
documented acknowledgement this request 100% of the time. 12% of ED providers documented
communication with the NH prior to patient discharge. Our EMR requires an ED diagnosis to
be assigned prior to discharge and included in ED discharge paperwork. ED providers
documented including ED tests performed with results 2% of the time in discharge paperwork.
System Quality Review
269
NewYork-Presbyterian Healthcare System Quality Symposium 2014
Quality 2020: A Vision of the Future
Sustainability Strategies
NH paperwork must consistently contain each of the first 5 QIs 100% of the time. NH providers
must be educated on the QIs and transfer procedures must be standardized so that QIs 1-5 are
always being met. An important aspect of standardization will be updating the NH transfer
paperwork so that QIs 1-5 are represented on transfer forms and thus are more likely to be
included. In addition, transfer procedures must ensure that NH paperwork is consistently
transferred with the patient and scanned into his or her EMR upon ED arrival, as only 23% of
NH patients arrived to the ED with available paperwork. EPs need to significantly improve their
compliance with QIs 7-9. As is the case for NH providers, ED providers must be educated on
the QIs and ED-to-NH procedures must be standardized so that QIs 6-9 are always being met.
Lessons Learned
1. NH paperwork needs to consistently contain the first 5 QIs: reason for transfer, code status,
medication allergies, physician and family contact information, medication list.
2. Providers in our ED need to consistently align their care of NH patients with QIs 6-9:
documenting performance of tests requested by NHs, documenting communication with the NH
prior to patient discharge from the ED, and including ED diagnosis and tests performed with
results in patient transfer paperwork.
3. Standardization of transfer procedures and provider education on the QIs is essential for
alignment with SAEM's first 9 QIs.
Conclusion
The goal of this study was to assess how well NH and ED providers fulfilled the 9 SAEM
Quality Indicators applicable to a NH resident’s arrival at and discharge from the ED.
Compliance with each quality indicator was varied and ranged from 2% to 100%. Overall, NH
and ED providers are not universally complying with the first 9 SAEM Quality Indicators for
Transitional Care.
System Quality Review
270
NewYork-Presbyterian Healthcare System Quality Symposium 2014
Quality 2020: A Vision of the Future
TABLE 1. SAEM Quality Indicators.
Quality indicator
Reason for transfer
Code/resuscitation status
Medication allergies
Contact information for the NH, the primary care
or on-call physician, and the resident’s legal health
care representative or closest family member
5) Medication list
1)
2)
3)
4)
6) Tests requested by NH Providers
7) Communication between NH and ED Providers
8) ED diagnosis
9) Tests performed with results (and tests with
pending results)
10) If a NH resident is discharged from the ED back
to the NH and physician follow-up is
recommended, then the patient should receive
follow-up (or the medical record should indicate
why the follow-up did not occur)
11) If a NH resident is discharged from the ED back
to the NH and the ED provider prescribes or
recommends a medication, then the NH should
administer the medication (or document in the
medical record why the medication was not
administered)
Type
Critical Data for NH-to-ED transfer
Critical Data for NH-to-ED transfer
Critical Data for NH-to-ED transfer
Critical Data for NH-to-ED transfer
If a NH resident is transferred to an ED, then the NH
should provide a medication list in the transfer
paperwork
If a NH provider requests that specific tests be
performed in the ED, then the EP should document
performance of the requested tests (or document in the
medical record why the tests were not performed)
If a NH resident will be released from an ED back to the
NH, then the EP should document communication with
a nursing home provider or the primary care or on-call
physician prior to discharge from the ED (or document
attempts to do so)
Critical Data for the ED-to-NH Transfer
Critical Data for the ED-to-NH Transfer
Care Provided after ED Visits
Care Provided after ED Visits
TABLE 2. Percent of NH Paperwork Compliant with Quality Indicators 1-5.
Quality Indicator
Reason for transfer
Code/resuscitation status
Medication allergies
Contact information
Primary or on-call physician
HCP, POA or closest family member
5) Medication list
1)
2)
3)
4)
System Quality Review
Percent compliant
85%
52%
85%
46%
69%
70%
271
NewYork-Presbyterian Healthcare System Quality Symposium 2014
Quality 2020: A Vision of the Future
NewYork-Presbyterian Hospital/Weill Cornell Medical Center
A Novel Clinical Protocol for Placement and Management of Indwelling
Urinary Catheters in Older Adults in the Emergency Department:
Implementation and Impact Assessment
Mary R. Mulcare, MD; Tony Rosen, MD, MPH; Sunday Clark, ScD; Kartik Viswanathan, PhD; David P. Calfee, MD,
MPH; Michael E. Stern, MD; Neal E. Flomenbaum, MD
Introduction
Catheter-associated urinary tract infections (CAUTIs) are the most prevalent hospital-acquired
infections and have significant associated morbidity, mortality, and cost. Older adult patients
(aged 65 and older) are disproportionately affected, as they most commonly receive indwelling
urinary catheters (IUCs) and are more susceptible to urinary tract infections and associated
complications than younger patients. Older adults are also more susceptible to non-infectious
complications of IUCs, including falls from tethering, delirium, urethral trauma, and pain, which
likewise effect patient safety and outcome.
While potentially appropriate for critically ill patients or those with acute urinary obstruction,
urinary catheters are often placed unnecessarily and for staff convenience in certain patient
scenarios. Research suggests that as many as half of catheters placed in hospitalized patients do
not have documented physician orders.
Though much literature has focused on inpatient hospital efforts to reduce CAUTIs by
preventing inappropriate IUC placement and to remove IUCs as soon as no longer necessary,
only recently have researchers targeted the Emergency Department (ED) as a potential site for
intervention.
Thus the goal of this project was to implement and assess the impact of a novel clinical protocol
to assist ED providers with appropriate indications for placement, reassessment, and removal of
IUCs in older adults in the ED.
Quantitative/Qualitative Measures
Written surveys were administered before the intervention (outlined below), immediately after,
and at 6-months to assess providers’ baseline knowledge, attitudes, and practices, as well as the
protocol’s long-term impact. Surveys included asking providers for IUC management decisions
for 25 unique clinical scenarios. To objectively assess the clinical impact of the protocol, we
retrospectively compared rates of IUC placement in this ED in patients aged 65 and older in the
6-months before (1/1/13-6/30/13) and 6-months after (9/1/2013-2/28/2014) implementation
of the protocol.
System Quality Review
272
NewYork-Presbyterian Healthcare System Quality Symposium 2014
Quality 2020: A Vision of the Future
Methodologies
We developed a comprehensive, evidence-based clinical protocol and implemented it at Weill
Cornell Medical Center, a large, urban, academic medical center with over 67,000 adult patient
visits annually. We introduced the protocol to multiple ED providers, including attendings,
residents, mid-levels, and nurses with a 20-minute scripted slide presentation. Pocket cards were
distributed and the protocol was displayed in the ED.
Improvement Results
Of the 125 ED providers participating in the implementation phase of this study, 112 (90%)
completed 6-month follow-up. Immediately after protocol introduction, 98% of the participants
reported that the intervention made them more comfortable with the appropriate indications for
IUC placement. 87% reported anticipating that this intervention would reduce rates of IUC use
and increase patient safety. At 6-month follow-up, 80% felt that the protocol had changed their
practice and 38% reported frequently referencing the protocol. In the clinical vignettes, ED
providers correctly identified the appropriate approach for IUC placement in 33% of cases preintervention compared to 54% immediately post-intervention and 44% at 6-months (P<0.001).
4,967 (61%) of the 8,147 older adult evaluated in the ED during the 6-months prior to
implementation were admitted. Of those admitted, 935 (18.8%) received an IUC in the ED. In
the 6-months after implementation, 4,781 (59%) of the 8,119 older adults evaluated in the ED
were admitted, with 731 (15.3%) having received an IUC in the ED. This represents a relative
risk reduction of 18.6% (P<0.001) for ED use of IUCs in this population.
Sustainability Strategies
In order to continue and build upon the efficacy of this initial intervention, there will need to be
repeat educational interventions. Repeating the slide presentation and re-distribution of the
pocket cards will be most helpful during the summer, with the arrival of new residents and
faculty, and at intervals deemed most useful by the nurses with nursing turnover. Likewise our
physician assistant residents begin their year on November 1, and thus repeated education with
the mid-levels yearly around this time will be helpful.
Another method to ensure this project is sustainable is to report back to the ED staff about the
numbers of indwelling urinary catheters being placed and the resultant CAUTIs at regular
intervals. This will require support from the hospital DISCOVERY system. This feedback will
allow for self-evaluation of practice strategies.
Lessons Learned
1. This is the type of initiative that is very appropriate for a champion from the ED nurses. A
protocol such as this has empowered ED nurses to take an even more active and assertive role in
patient care with regards to patient safety and infection prevention.
2. Following the documentation trail of indwelling urinary catheter placement and the decision
making process is very difficult, and requires better use of and reporting from our electronic
medical record.
System Quality Review
273
NewYork-Presbyterian Healthcare System Quality Symposium 2014
Quality 2020: A Vision of the Future
3. In a very short period of time, a dramatic reduction in the number of indwelling urinary
catheters was realized after this intervention, supporting the cause for protocols in general going
forward to streamline patient care and safety.
Conclusion
Introduction of this comprehensive, evidence-based clinical protocol has been well received by
ED providers. It has led to sustained self-reported practice change and significant reduction in
overall IUC placement in older adults in our ED who were admitted to the hospital. Our next
steps include evaluating whether this reduction has concomitantly increased the proportion of
IUCs placed in the ED for appropriate indications, and to assess whether it has led to fewer
catheter-associated urinary tract infections during hospital admission and improved patientcentered outcomes.
System Quality Review
274
NewYork-Presbyterian Healthcare System Quality Symposium 2014
Quality 2020: A Vision of the Future
NewYork-Presbyterian Hospital/Weill Cornell Medical Center
Using Targeted Interventions and Multidisciplinary Collaboration to Decrease
Length of Stay for Leukemia Patients at NewYork-Presbyterian/Weill Cornell
Kristen Fanti, MPA, BSN, RN, OCN
Introduction
Ensuring safe and efficient patient discharge has been an ongoing focus in the healthcare
industry, and specifically at NewYork-Presbyterian Hospital. Increased length of stay (LOS) not
only has the potential for a negative financial impact to the organization, it also is a quality and
patient safety metric, with increased LOS linked to adverse patient outcomes and an
unsatisfactory patient experience. Each service has unique challenges, and thus service-specific
Barrier Reduction Teams (BRTs) were formed to identify and work through barriers to efficient
patient discharge. LOS variance refers to the variation between expected and actual LOS, with a
negative value meaning that discharge is occurring earlier than expected based on national
averages for a specific patient population. During the first quarter 2013, the inpatient oncology
units of 10 Central (10C) and 10 South (10S) at NewYork-Presbyterian/Weill Cornell Medical
Center (NYP/WC) showed a significant increase in LOS, compared to performance in 2012. In
2012, LOS variance for 10C and 10S was 0.93. In January 2013, there was an increase in LOS
variance to 3.28, with February’s LOS variance projected at 2.22. The original BRT meeting
structure was not proving to be effective, and attendance at the meetings and interest in the
initiative had declined. Participants did not feel that the data they were receiving was beneficial to
them and there was a mentality that “it was not my patient.” By working with IT and Quality, the
team was able to dissect the data and see exactly which specific patients were staying longer than
expected. During the first two months of 2013, the group was reformatted to focus on leukemia
LOS barriers, since early analysis of the data showed that it was this patient population that was
contributing to the positive variance in actual over expected LOS.
The objectives of this project were to:
• Determine specific factors that increase a leukemia patient’s LOS
• Determine which factors are actionable
• Engage key players in the LOS reduction initiative
• Decrease LOS in the leukemia patient population to align with hospital targets
System Quality Review
275
NewYork-Presbyterian Healthcare System Quality Symposium 2014
Quality 2020: A Vision of the Future
Quantitative/Qualitative Measures
The primary quantitative outcome measures included length of stay (LOS) data by: service,
disease related group (DRG), attending physician, and discharge disposition. The primary
qualitative outcome measure was BRT analysis of individual patients who stayed longer than
expected; this produced themes for further exploration, such as distance traveled to the hospital
and level of involvement on the part of the patient’s support person/caregiver.
Methodologies
In order to examine the identified problem, a two pronged approach was utilized: data review
and patient profile analysis. For the data review, the UHC Clinical Data Base/Resource Manager
(CDBRM) was used to target the relevant leukemia DRGs that had the highest LOS variance.
Based on that review, the LOS data was examined by common secondary diagnoses related to
those DRGs. For the patient profile analysis, focus groups and the BRT was utilized to analyze
patient specific reasons for increased LOS. Common themes were identified and used to further
drive performance improvement initiatives. Monthly BRT meetings, attended by social work,
nursing, leukemia physicians, care coordination, and physician assistants (PAs), were held to
analyze the data and review patient profiles. Other disciplines were brought into the group, such
as coding and physical therapy, as questions or issues arose. Ongoing data collection and analysis
allowed the group to see trends and track improvement and progress towards reaching the target.
Improvement Results
Early analysis of the data showed that leukemia patient discharges were the primary cause of the
positive LOS variance. Based on physician feedback, further data was collected using the UHC
database, to look at infection rates, percentage of ICU days, secondary diagnoses, and percentage
of patients with a “do not resuscitate” status for leukemia discharges. Most notable from those
results, the data showed that NYP/WC leukemia patients had a higher rate of many hospitalacquired or multi-drug resistant infections than other comparable institutions, as shown through
the coding of secondary diagnoses, and depicted in Table 1. This was thought to be a potential
determinate of increased LOS. Based on this finding, the multidisciplinary BRT decided to
pursue interventions to reduce these hospital-acquired infections as a potential means to improve
patient outcomes, and subsequently reduce LOS. A separate work group was formed which came
up with a series of interventions to reduce central line associated blood stream infection
(CLABSI) rates, which happened to be above the national average at the time. A decrease in
CLABSI rates was achieved, which correlated to a decrease in LOS variance over a similar time
period, from 3.65 in January 2013 to 0.41 in August 2013 for leukemia discharges.
Additional findings were made through analysis of patient profiles during monthly BRT
meetings. Missed opportunities in coding were discovered, meaning the patients’ severity of
illness (SOI) was not accurately being captured, leading to a lower estimated LOS. The Coding
Specialist was able to give in-services to the physicians and PA group so that they were using the
correct terminology in their notes, leading to more accurate coding.
Through the work of the BRT, LOS variance for leukemia patients was reduced from an average
of 2.59 (January to May 2013) to -0.41 (June to October 2013), as seen in Table 2, with monthly
System Quality Review
276
NewYork-Presbyterian Healthcare System Quality Symposium 2014
Quality 2020: A Vision of the Future
data seen in Table 3. Table 4 depicts the trend for 2014, with the two most recent months (June
and July 2014) projecting a leukemia LOS variance of -0.93 and -1.84 respectively.
Sustainability Strategies
In order for the successes shown to be sustainable, the BRT group continues to meet regularly to
discuss barriers and analyze the data. Data will continue to be examined for specific DRGs, with
further analysis and interventions based on general findings. A multidisciplinary approach proves
to be key, since each person brings unique insights to the table. Additionally, since ultimate
control over discharge lies in the hands of the medical team, ongoing collaboration with the
physicians is necessary for continued success.
Lessons Learned
1. Leukemia patients have complex diagnoses, making efficient discharge challenging.
Collaboration with the multidisciplinary team, and notably physician colleagues, is therefore
crucial for success of this performance improvement initiative.
2. Data analysis allows for more meaningful and targeted interventions, based on true
contributing factors to increased LOS, versus perceived factors.
3. Sustainability requires ongoing analysis of the data and follow-up if and when there are
unfavorable results.
Conclusion
Reducing length of stay is an ongoing initiative on the oncology units and NYP/WC as a whole.
Through multidisciplinary collaboration, the leukemia BRT has made progress in ensuring safe
and efficient patient discharge. Early data analysis and patient profile review helped the group
focus on actionable factors, which in turn allowed for more targeted interventions. This method
proved to be successful and sustainable, ultimately decreasing leukemia LOS variance and
improving patient outcomes from the beginning to end of 2013, with favorable results in 2014 to
date.
System Quality Review
277
NewYork-Presbyterian Healthcare System Quality Symposium 2014
Quality 2020: A Vision of the Future
Table 1: UHC Comparison Data for Leukemia* Discharges
% 2012 leukemia discharges* with each secondary diagnosis (potentially hospital-acquired or MDR)
NORTHWESTERN NYPCOLUMBIA CEDARS-SINAI
UCLA
CHICAGO
NYPCORNELL
2012 Discharges
78061 - fever w cce
486 - pneumonia organism nos
7907 - bacteremia
5990 - urinary tract inf nos
99592 - severe sepsis
00845 - c. difficile enteritis
0389 - septicemia nos
0549 - herpes simplex nos
99591 - sepsis
78552 - septic shock
04104 - group d strep infection
04149 - e. coli infect nec & nos
0413 - k. pneumoniae infect
04109 - strep infection nec
0793 - rhinovirus infect nos
03849 - gram-neg septicemia nec
04185 - gram-neg bact infect nec
0380 - streptococcal septicemia
03842 - e. coli septicemia
0388 - septicemia nec
4846 - pneum in aspergillosis
0785 - cytomegalovirial disease
0417 - pseudomonas infect nos
04111 - mssa
04112 - mrsa
4821 - pseudomonal pneumonia
03811 - mssa septicemia
03840 - gram-neg septicemia nos
48242 - mrsa pneumonia
48241 - mssa pneumonia
03843 - pseudomonas septicemia
511
24.30%
9.60%
10.60%
6.80%
6.30%
8.20%
2.90%
5.70%
3.90%
3.50%
3.50%
5.10%
2.30%
1.20%
1.80%
2.00%
1.60%
1.60%
1.20%
1.20%
0.40%
0.60%
1.00%
1.20%
0.80%
0.60%
0.80%
0.60%
0.60%
0.20%
0.40%
162
42%
17.90%
7.40%
13.60%
8.60%
3.70%
8.00%
6.80%
3.10%
5.60%
5.60%
3.70%
2.50%
2.50%
0.00%
0.60%
1.20%
0.60%
0.60%
2.50%
0.00%
1.20%
1.20%
0.60%
1.90%
0.60%
0.00%
0.00%
0.00%
0.00%
0.00%
159
38.40%
8.20%
8.20%
1.30%
4.40%
5.00%
5.00%
3.10%
2.50%
3.80%
3.80%
0.60%
0.60%
1.30%
0.00%
0.00%
0.60%
0.00%
0.60%
0.60%
1.30%
1.90%
0.60%
0.00%
0.60%
0.00%
0.00%
0.00%
0.00%
0.60%
0.00%
174
35.60%
13.80%
9.20%
10.30%
6.30%
5.20%
12.10%
0.60%
8.00%
3.40%
4.00%
4.00%
1.10%
2.90%
2.90%
0.00%
2.30%
1.10%
1.10%
0.00%
3.40%
0.00%
0.60%
1.10%
0.00%
0.00%
0.00%
0.00%
0.00%
0.60%
0.00%
63
20.60%
7.90%
22.20%
9.50%
6.30%
9.50%
7.90%
7.90%
7.90%
4.80%
7.90%
4.80%
6.30%
1.60%
4.80%
1.60%
1.60%
1.60%
3.20%
1.60%
0.00%
6.30%
3.20%
1.60%
0.00%
0.00%
0.00%
1.60%
1.60%
0.00%
0.00%
136
45.60%
13.20%
5.90%
5.10%
11.00%
8.10%
6.60%
2.20%
3.70%
4.40%
1.50%
2.20%
2.20%
0.70%
0.70%
2.90%
0.00%
1.50%
0.70%
0.70%
1.50%
0.00%
0.70%
0.70%
0.00%
1.50%
0.70%
0.00%
0.00%
0.00%
0.70%
note: some discharges
may possess multiple
secondary diagnoses
*Includes: MS‐DRG: 834 Acute leukemia w/o major O.R. procedure w MCC,835 Acute leukemia w/o major O.R. procedure w CC,836 Acute leukemia w/o
major O.R. procedure w/o CC/MCC,837 Chemo w acute leukemia as sdx or w high dose chemo agent w MCC,838 Chemo w acute leukemia as sdx w CC or
high dose chemo agent,839 Chemo w acute leukemia as sdx w/o CC/MCC
Excludes: discharges with LOS greater than 60 days, pediatric discharges (ages 0‐18)
^ all in‐hospital deaths except for Medicare or CHAMPUS hospice patients
System Quality Review
278
NewYork-Presbyterian Healthcare System Quality Symposium 2014
Quality 2020: A Vision of the Future
Table 2: Leukemia LOS 2013 Summary
Leukemia Pts
YTD Oct 2013*
LOS
EXCESS
VARIANCE
DAYS
CASES
ALOS
ELOS
250
278
15.34
11.43
12.75
11.84
2.59
-0.41
648
-113
3.91
25%
0.91
7%
3.00
116%
761
117%
Jan-May 2013
Jun - Oct 2013
Change (days)
% Change
CMI
ALOS>
ELOS
3.61
3.23
54%
39%
0.15
28%
*Discharges for Ball, Feldman, Lee, Ritchie, Roboz from 10C & 10S
Table 3: LOS variance for Leukemia and All 10C/10S Discharges, January to October 2013
Leukemia
only
# DCs
ALOS
ELOS
LOS
Variance
Excess
Days
CMI
Jan-13
46
16.30
12.66
3.65
168
3.28
Feb-13
45
15.51
12.51
3.00
135
3.52
Mar-13
56
16.86
14.16
2.70
151
3.84
Apr-13
50
12.98
12.04
0.94
47
4.19
May-13
53
14.98
12.21
2.77
147
3.20
Jun-13
56
10.38
10.80
-0.43
-24
2.93
Jul-13
56
11.29
12.01
-0.72
-40
3.59
Aug-13
51
11.43
11.02
0.41
21
3.10
Sep-13
57
11.74
12.71
-0.98
-56
3.49
Oct-13
55
12.42
12.14
0.28
16
2.92
System Quality Review
279
NewYork-Presbyterian Healthcare System Quality Symposium 2014
Quality 2020: A Vision of the Future
All
10C/10S
Discharges
CASES
ALOS
ELOS
LOS
VARIANCE
EXCESS
DAYS
CMI
January
105
13.27
9.99
3.28
344
2.52
February
93
11.72
9.50
2.22
207
2.64
March
109
13.39
11.35
2.04
222
2.93
April
126
9.77
9.40
0.37
46
2.83
May
151
12.07
10.00
2.07
312
2.58
June
151
9.25
8.80
0.45
68
2.38
July
176
8.69
9.01
-0.31
-55
2.59
August
114
9.31
9.52
-0.21
-24
2.58
September
117
10.55
10.81
-0.26
-31
2.81
October
133
10.96
8.95
2.01
267
2.19
2013 YTD
1275
10.73
9.66
1.06
1357
2.59
LOS Variance
LOS Variance for 10C & 10S, 2013 YTD Oct
Leukemia only
5
4
3
2
1
0
-1
-2
-3
-4
Jan-13
Feb-13
System Quality Review
Mar-13
Apr-13
All 10C/10S Discharges
May-13
Jun-13
Jul-13
Aug-13
Sep-13
Oct-13
280
NewYork-Presbyterian Healthcare System Quality Symposium 2014
Quality 2020: A Vision of the Future
Table 4: Leukemia LOS, January to July 2014
Leukemia
only
January
February
March
April
May
June
July
#
DCs
50
39
45
40
47
29
37
ALOS ELOS
15.14 13.12
13.36 13.38
15.89 14.53
13.10 12.38
11.74 13.70
14.03 14.97
11.68 13.51
LOS
Variance
2.02
-0.03
1.36
0.73
1.96
-0.93
-1.84
Excess
Days
101
-1
61
29
92
-27
-68
CMI
3.32
3.51
4.44
3.03
3.30
4.07
3.43
LOS Variance for 10C & 10S Leukemia Discharges, 2014 YTD
Leukemia only
3
LOS Variance
2
1
0
-1
-2
-3
System Quality Review
281
NewYork-Presbyterian Healthcare System Quality Symposium 2014
Quality 2020: A Vision of the Future
NewYork-Presbyterian Hospital/Weill Cornell Medical Center
Improving Prehospital Geriatric Assessment and Care: A Qualitative Study of
Emergency Medical Services (EMS) and Emergency Department (ED)
Provider Perspectives
Regina Mysliwiec MD; Tony Rosen MD MPH; Mary Mulcare MD; Sunday Clark MPH ScD; Michael Stern MD; and
Neal Flomenbaum MD
Introduction
As national awareness of the growing elderly population increases, acute care of older adults –
defined here as adults aged 65 or greater – has become a focus for improvement of patient care
and safety. In this population, failures of communication are a source of both medical errors and
patient dissatisfaction with care.Many of the first steps to improving elder care involved
developing comprehensive hospital discharge policies and checklists to ensure that essential
information is communicated prior to discharge. At NewYork-Presbyterian Hospital (NYPH),
we are taking advantage of our unique role as a large, urban, academic medical center situated in a
community with a large population of older adults to improve geriatric patient safety earlier in the
course of care – during transitions of care from the prehospital setting to the ED. This project is
particularly suited to NYPH given its close association with NewYork-Presbyterian EMS, which
is the largest private ambulance company in New York City as well as the largest voluntary
contributor to its 911-emergency system. EMS providers, who perform on-scene assessments of
ill and injured patients, have unique access to important information that may impact subsequent
care. This is particularly important for care of older adults with complicated medical histories,
who are often unable to give an accurate history and for whom the state of living environment
influences care decisions. This patient population makes up an increasingly large proportion of
EMS calls nationwide. Despite this, communication break-downs occur frequently with EMS
providers unable to convey the important information they have gathered and ED/hospital
providers unable to access it when needed. High quality communication of prehospital
assessment during handoff to the hospital can help providers deliver the best possible care well
beyond the ED. The aim of this qualitative study was to explore attitudes and self-reported
practices of EMS and ED/hospital providers surrounding care transitions for older adults and to
identify short-comings and potential solutions, including a standardized prehospital checklist for
use by NYP EMS providers.
Quantitative/Qualitative Measures
In this qualitative study, we sought to identify provider attitudes and practices surrounding
current methods of communicating prehospital assessment. The resulting themes will allow for
more targeted interventions, such as a checklist for standardized prehospital geriatric patient
assessment.
System Quality Review
282
NewYork-Presbyterian Healthcare System Quality Symposium 2014
Quality 2020: A Vision of the Future
Methodologies
In order to develop a communication tool for use by NYPH employees that would be both easily
adopted and easily sustainable, we conducted 7 semi-structured focus groups of NYPH
employees involved in the acute care of older adults. A total of 56 participants were recruited by
purposeful sampling and stratified by provider type: EMS providers (n=6), ED attending
physicians (n=9), ED resident physicians (n=11), ED physician's assistants (n=11), ED social
workers (n=5), and geriatric medicine specialists (n=14). A discussion guide of open-ended
questions was designed for all focus groups sessions. The sessions were audio-recorded, deidentified, and transcribed. Transcripts were reviewed for accuracy and data were coded using
Nvivo 10 software. Themes were identified by iterative coding and inductive analyses.
Improvement Results
All groups confirmed that EMS providers obtain critical information that is not otherwise rapidly
available and that this information is often difficult for ED/hospital providers to access.
Participants identified 23 barriers to high quality information transfer specific to older adults.
Categories included challenges for EMS in obtaining information, EMS documentation/verbal
report missing critical information, variations in protocols and training, poor adherence to
existing protocols for EMS-to-ED information transfer, issues with informal verbal reporting,
and challenges for hospital providers accessing prehospital information. During the discussion of
these barriers, all provider groups agreed that they want to improve interprovider communication
during transitions of care of older adults and that doing so would improve their care of older
adults. Additionally, all groups agreed that a standardized prehospital geriatric assessment
checklist would improve their ability to deliver high quality patient care.
Sustainability Strategies
In order to maximize sustainability of our intervention, we conducted focus groups in order to
involve providers in its development. Participants described 6 strategies to improve effective
communication of critical information, including an EMS-to-social work direct hotline, a
mechanism for EMS to flag high-risk ambulance care reports, an EMS/ED provider huddle for
sharing feedback, and a prehospital assessment checklist specific to older adults. Detailed
discussions of the characteristics and content of a checklist yielded a total of 6 preferred
characteristics and 31 potential content items, including smart phone photographs of patient
environments. EMS providers felt that use of a checklist would fit well into their current practice,
especially if the checklist was similar in design and attached to their current document template.
All provider groups expressed interest in continued involvement in the development of a
checklist.
Lessons Learned
1. EMS providers feel that they do not often have access to ED providers or receive adequate
feedback from ED providers to improve their handoff practice.
2. ED providers feel that they cannot access EMS written reports in a timely manner.
3. Both EMS and ED providers feel empowered by their participation in the development of a
new quality improvement protocol.
System Quality Review
283
NewYork-Presbyterian Healthcare System Quality Symposium 2014
Quality 2020: A Vision of the Future
Conclusion
EMS providers play a critical role in obtaining information essential to acute care of older adults.
Despite existing barriers, innovative strategies were identified to improve comprehensive
information transfer to ED and hospital personnel, including a checklist for prehospital
assessment of elderly patients. Limitations of this study include the lack of input from nurses,
who play a critical role in the transition of patient care from EMS-to-ED. Going forward, we
plan to hold 1-2 focus group sessions with ED nurses as well as additional groups of EMS
providers. Data collected from all of the groups will be used to create a prehospital geriatric
assessment checklist for use by NYP EMS. Future projects will include both quantitative and
qualitative analyses of post-implementation outcomes, to guide checklist modifications and
improve its sustainability and clinical usefulness.
System Quality Review
284
NewYork-Presbyterian Healthcare System Quality Symposium 2014
Quality 2020: A Vision of the Future
NewYork-Presbyterian/Columbia University Medical Center
Choosing Monitoring Wisely: Enhancing Patient Flow by Improving Inpatient
Telemetry Use
Dan Henderson, MD, MPH; Christopher R. Kelly, MD; Deepa Kumaraiah, MD, MBA; Catherine Halliday, RN, MSN,
Hollis George, RN, MS; Robert Green, MD, MPH; and LeRoy Rabbani, MD
Introduction
In 2013, our hospital, a 710-bed academic medical center, faced unprecedented demands in the
wake of a recent natural disaster and temporary closure of several major hospitals. In this context,
our institution identified continuous cardiac telemetry as a source of delayed care and waste of
resources. We redesigned the process of telemetry ordering to promote appropriate use and
minimize resource constraints.
Problem statement: Patients who have been planned for hospital admission face delays in the
emergency department (ED) due to limited availability of cardiac monitoring units. Widespread
overuse of telemetry where it may not be necessary exacerbates these resource constraints, and
leads to long ED waits. We sought to determine whether a quality improvement effort targeting
overuse would improve telemetry ordering practices and reduce or eliminate completely the
associated ED waits.
Aim: To eliminate waits in the emergency department for admitted patients due to a lack of
cardiac telemetry monitoring units.
Goals:
I. To define clinical guidelines for the use of cardiac telemetry for general medical ward patients,
a population for whom no such guidelines exist, in a large, urban, academic medical center.
II. To redesign the process of ordering cardiac telemetry around such guidelines, with oversight
of extended use of telemetry, in order to curtail overuse.
III. To evaluate the redesigned ordering process for effects on use and overuse of cardiac
telemetry.
Quantitative/Qualitative Measures
To assess the impact of the intervention on telemetry ordering practices, we assessed the rate of
ordering (proportion of admitted patients with any telemetry order) and analyzed a subsample of
cases for appropriateness of ordering according to the best available clinical guidelines (percent
appropriate, inappropriate, or indeterminate orders).
To assess the impact of the intervention on patient waits, we analyzed patient flow data from all
patients admitted from 9/3/2013 to 3/4/2014, including ED arrival time, time of decision to
admit, time of bed and team assignment and availability, and inpatient unit arrival time, to
System Quality Review
285
NewYork-Presbyterian Healthcare System Quality Symposium 2014
Quality 2020: A Vision of the Future
calculate ED length of stay, ED length of stay after bed and team were available, and total
inpatient length of stay. We excluded patients requiring ICU-level care or isolation beds.
Methodologies
We began by evaluating common practice through careful case review and discussion with
frontline clinicians, to determine the underlying causes of the current state.
We used the lessons learned to develop a bundled intervention. We aimed to level demand by
delaying the ordering of telemetry until the moment it was needed, and have telemetry orders
expire automatically at a time early enough to meet demand for patients soon to be admitted. We
used electronic health record (EHR) modifications to inform ordering clinicians about
appropriate use at the moment they began to place telemetry orders. Using a modified ordering
process with automatic expiration of orders and approval required for continuation, we
prevented inadvertent continuation of telemetry due to reflex renewal. We supplemented this
approach with an informational campaign to residents, PAs, and NPs.
Improvement Results
Our initial evaluation of usual practice revealed a lack of clear guidelines regarding the use of
telemetry, and widespread variation between clinicians, services, and units. The leading reason for
ordering telemetry outside of cardiology units was low-risk chest pain (23%). This was coupled to
a lack of feedback regarding the need to discontinue monitoring, alert fatigue, and sub-optimal
timing of interruptive reminders. Across all non-cardiology services, the median duration of
telemetry was 60 hours, with marked differences between major ordering services: Medicine 44
hours, 125,455 total tele-hours; neurology 55 hours, 35,803 total tele-hours; surgery 112 hours,
102,991 total tele-hours.
We developed organizational guidelines for appropriate and inappropriate telemetry, based on the
best available literature. We replaced the existing order with one including a prompt of instances
not to use telemetry, and disseminated guidelines to housestaff at noon conference-style
meetings. All orders were set to expire at the next noon 24 hours after ordering, to make the
process of expiration and removal or renewal predictable and suited to team work flow. For
extensions of telemetry, clinicians would need to page the telemetry fellow (the on-call
cardiology/electrophysiology fellow). After 48 hours, this restriction reset. This bundle was
implemented as a pilot program on core internal medicine units.
In the month after implementation, telemetry ordering on pilot floors decreased by 48%,
compared by 3% on non-pilot floors. On pilot floors, the proportion of appropriate telemetry
orders increased from 45% to 72% between the pre- and post-intervention periods (respectively).
We are currently waiting on data for the ED patient flow analysis, which is expected by the end
of September 2014.
System Quality Review
286
NewYork-Presbyterian Healthcare System Quality Symposium 2014
Quality 2020: A Vision of the Future
Sustainability Strategies
Sustaining the improved ordering practices and (we believe) the resultant improvements in
clinical quality and patient flow rests largely on automatic measures now part of the electronic
health record/computerized provider order entry system. The alerts and expirations do not need
champions to keep working. Beyond these automatic measures, however, it remains important to
continually evaluate the state of the practice. Further, the continued willingness of nurses to
remove expired telemetry units is critical to sustaining the gains of available telemetry. As patient
flow remains a key driver of quality, safety, and the experience of care, we believe the hospital has
significant incentives to sustain the program.
Lessons Learned
1. We were able to curtail telemetry overuse and improve practice with a bundled approach of
education, reminders, and a gatekeeper system.
2. Much of the excess telemetry use was driven by a lack of system supports, namely, unclear
guidelines, and poorly-timed alerts.
3. Full results are pending, but we believe telemetry represents an important constraint to patient
flow, and improved use of monitoring can relieve the bottleneck and reduce wait times.
Conclusion
The majority of telemetry ordered outside of cardiology units is of questionable value, but cardiac
monitoring remains an important adjunct to care. We implemented a bundled intervention,
including education via conference and quick alerts at the point of ordering, as well as a
redesigned system employing just-in-time principles to smooth flow, and a gatekeeper restriction
to prevent extended use of telemetry where not appropriate. These efforts yielded a prompt
reduction in the ordering of cardiac telemetry and a modest improvement in the proportion of
orders that were likely of higher value. Our institution saw a reduction in the number of patients
waiting in the ED for telemetry boxes, and we intend to fully evaluate this question once the data
are obtained, using multiple regression for the interaction between the presence of telemetry and
the demand for telemetry at the time of ordering (i.e. percentage of monitoring units already in
use).
It is our hope that this effort will inform other efforts to improve health care value and reduce
bottlenecks to patient flow, offering improvers a justification and means to get patients out of the
ED and up to their beds sooner.
System Quality Review
287
NewYork-Presbyterian Healthcare System Quality Symposium 2014
Quality 2020: A Vision of the Future
Poster Presentation
NYU Hospital for Joint Diseases
A Customized Prophylactic Antibiotic Program Reduces Surgical Site
infections in Spine and Arthroplasty Patients
Rainier Tejada, BA; Anthony A. Catanzano, BA; Michael Phillips, MD; Donald Chen, MD; Joseph A. Bosco III, MD
Introduction
Orthopedic surgeons have traditionally utilized an antibiotic prophylactic protocol based on 1g
of cefazolin. However, with rising isolates of Gram-negative bacteria (GNB), it may no longer be
adequate to use the same protocol for each patient. At our institution, investigators reported 30%
of arthroplasty-related and 25% of spine fusion-related SSIs were caused by GNB. We
customized the antibiotic protocol to address the GNB found in our population, by adding high
dose weight based gentamicin an aminoglycoside antibiotic with significant gram-negative
coverage. Our study evaluates the efficacy of gentamicin as prophylaxis for GNB SSIs in
arthroplasty and spine fusion operations.
Quantitative/Qualitative Measures
Prior to July 2012, all patients were given 2g of cefazolin, which represented the study's control.
After July 2012, patients were given 2g of cefazolin and gentamicin with a weight-based dosing
protocol. Those >75 years of age, >120kg, or with myasthenia gravis were given 2g of
aztreonam. Patients with a penicillin allergy were given a weight-based dose of vancomycin as
well as a GNB agent as mentioned above.
Methodologies
We prospectively reviewed all total hip arthroplasty and spine fusion patients at a single
institution from January 2009 through December 2013. The Center for Disease Control and
Prevention's National Healthcare Safety Network criteria was used to define SSIs. A list of
patients with surgery and antimicrobial prophylaxis type was merged with an SSI database to
identify patients with SSI. All p-values were calculated with a 2-sided Fisher Exact Test.
Improvement Results
A total of 6,804 cases were reviewed with 104 SSIs identified for an overall infection rate of
1.53%. Prior to the introduction of a GNB prophylactic agent (gentamicin or aztreonam), hip
arthroplasty and spine fusion had an SSI rate of 1.82%. However, after gentamicin or aztreonam
was included as part of the prophylactic protocol, the overall SSI rate decreased to 0.90%
(p=0.004) and SSIs of the hip and spine caused by GNB decreased from 0.53% to 0.19%
(p=0.04), although there was no significant decrease in deep SSIs caused by GNB in the hip and
spine. A review of the first 2000 patients receiving gentamicin revealed no associated increase in
nephrotoxicity compared to historic controls and no cases of ototoxicity.
System Quality Review
288
NewYork-Presbyterian Healthcare System Quality Symposium 2014
Quality 2020: A Vision of the Future
Sustainability Strategies
We have the organizational infrastructure to implement customized antibiotic regimens as well as
to obtain data and track our progress. The uniqueness of our single specialty orthopaedic center,
and our commitment to improve patient safety and outcomes ensured our project was completed
to the highest standard.
Lessons Learned
1. The effects of the customized antibiotic prophylaxis on our SSI rate and the unintended
consequences caused by resistant organisms.
2. Determined the biogram of the organisms causing SSIs at our institution.
3. How to customize a prophylactic antibiotic regimen based on our unique biogram.
Conclusion
With a constantly evolving pathogen profile, antibiotic prophylaxis protocols must be adjusted
accordingly in order to reduce SSIs. Our study indicates that, when added to a prophylactic
antibiotic protocol, gentamicin is a safe and effective means of reducing SSIs in hip arthroplasty
and spine fusion patients.
System Quality Review
289
NewYork-Presbyterian Healthcare System Quality Symposium 2014
Quality 2020: A Vision of the Future
NYU Langone Medical Center
"Who's My Doctor, Anyway?" Implementation of Hospitalist Picture
Pamphlet on the General Medicine Service
Katherine Hochman, MD; Nicole Adler, MD; Nicole Kandinova
Introduction
Problem Statement: Hospitalized patients are visited by numerous health care professionals daily.
The number of members of the health care team is even greater in academic medical centers,
where teams are augmented by fellows, residents and medical students. Furthermore, shortened
work hours lead to an increased number of hand-offs to still more providers. With such
complexity, hospitalized patients are often unable to identify the physician who is in charge of
their care. Not knowing who's in charge is a threat to patient safety and patient satisfaction.
Project Aim: We designed a Hospitalist Picture Pamphlet, a simple bi-fold card which detailed
specific information about the role of the hospitalist. We included an insert containing pictures
and names of every member of our hospitalist group (Figure 1). By distributing the Hospitalist
Picture Pamphlet to every patient, our aim was to increase our patients' ability to identify the
physician who is in charge of their care.
Quantitative/Qualitative Measures
We studied the percent of hospitalized patients on the general medicine service who are able to
correctly identify their attending physician.
Methodologies
Data Collection: All non-demented patients on two general medicine units in an academic
medical center were asked in person to identify “the doctor who is in charge of your care” on
hospital day #2. Responses were recorded as: 1.) Patient can identify the doctor in charge without
a prompt, 2.) Patient can identify the doctor in charge with a prompt (which included the
Hospitalist Picture Pamphlet). 3.) Patient identifies an incorrect doctor in charge, 4.) Patient
states “I don’t know”. 184 patients were surveyed before the intervention and 107 patients were
surveyed after the intervention.
Intervention: Every member of the hospitalist group was expected to distribute the Hospitalist
Picture Pamphlet to each new patient as part of the introduction. The Hospitalist Picture
Pamphlet would serve as a reminder to explain the role of the hospitalist, how hospitalists work
in teams and that there is always a hospitalist in charge as the attending physician. The hospitalist
would highlight his/her photograph in the insert as a means of reinforcing the introduction.
System Quality Review
290
NewYork-Presbyterian Healthcare System Quality Symposium 2014
Quality 2020: A Vision of the Future
Improvement Results
Results:
• Post intervention, the percentage of patients who were able to correctly identify their attending
physician without a prompt improved from 19% to 45% (Figure 2).
• Post intervention, the percentage of patients who were able to correctly identify their attending
physician both with and without a prompt increased from 40% to 54%.
• Post intervention, the percentage of patients who did not know their attending physician
decreased from 36% to 26%.
Sustainability Strategies
Distributing the Hospitalist Picture Pamphlet as a part of the introduction to every new patient
has been adopted as best practices in our hospitalist program. In addition, every incoming
hospitalist is on-boarded with the importance of incorporating the Hospitalist Picture Pamphlet
as part of daily practice. Furthermore, every Friday, the weekday hospitalist signs out to the
weekend hospitalist at the bedside with the Hospitalist Picture Pamphlet. This model ensures that
the patient knows exactly who is caring for them over the weekend.
Lessons Learned
1. This low-tech, highly portable intervention yielded modest but important gains in the
percentage of patients who were able to correctly identify the physician in charge, both with and
without a prompt.
2. Despite this intervention, a sizable percentage of patients were unable to correctly identify the
physician in charge, suggesting that a second or even third means of reinforcement is necessary.
3. Despite the intervention, about the same percentage of patients identified the incorrect (nonhospitalist) physician in charge, suggesting a lapse in hand-off communication from another
service in the hospital (ICU, SDU).
Conclusion
The complexity of care in the hospitalized patient is staggering. Despite a very strategic approach
to improving our patients’ ability to identify the physician in charge, our results were only
modestly improved.
Our next steps are twofold. First, in addition to distributing the Hospitalist Picture Pamphlet, we
will start adding specific information to our new patient care boards at the foot of every patient’s
bed. Second, we plan to adopt a geographic model of care in the Fall. Importantly, geography will
confine a single team to a single unit, allowing for longer and more frequent interactions between
the patient and the physician in charge.
System Quality Review
291
NewYork-Presbyterian Healthcare System Quality Symposium 2014
Quality 2020: A Vision of the Future
Figure 1: Hospitalist Picture Pamphlet
Figure 2:
Patient Interview Responses
50
45%
Percentage of Patients
45
40
36%
35
30
25
20
19%
24%
21%
26%
21%
Before Pamphlet
Distribution N=184
15
After Pamphlet
Distribution N=107
8%
10
5
0
Correctly
Correctly
Identified MD Identified MD
without Prompt with Prompt
System Quality Review
Identified
Incorrect MD
Did Not Know
292
NewYork-Presbyterian Healthcare System Quality Symposium 2014
Quality 2020: A Vision of the Future
NYU Langone Medical Center
Team-based Readmission Assessment Initiative Notes (T.R.A.I.N.): An
Interdisciplinary Quality Education Strategy
Adler, Nicole M MD FACP; Hochman, Katherine A MD FHM; Kandinova, Nicole; Francois, Fritz MD MSc FACG
Introduction
Problem Statement:
Approximately 20% of Medicare patients are readmitted to a hospital within one month of
discharge. In 2010, it’s estimated that readmissions cost the inpatient Medicare program alone
$17.5 billion. Readmission rates in other population subgroups are estimated to be similar, and it
is believed that approximately 80% of patients who are readmitted return to the original
discharging hospital.
Recent reviews also suggest that 27% of readmissions may be preventable. CMS is currently
looking at readmissions for acute myocardial infarction, congestive heart failure, and pneumonia,
and decreasing payments to hospitals with excessive readmission rates in these areas. The ability
to identify patients at high risk for readmission may be an important first step for preventing
them down the line, and if patients at high risk for readmission can be identified prior to
discharge, hospitals may be able to make interventions targeted to this patient population.
A review of the literature also shows that there are few studies that engaged residents in the
process of determining risk of readmission, either alone, or as an interdisciplinary team. As part
of the ACGME’s next accreditation system, one of the milestones used in the evaluation for
competency for graduation from an internal medicine residency training program is: “learns and
improves via performance audit.” This milestone speaks to the resident’s ability to actively engage
in quality improvement initiatives, and to apply common principles and techniques of quality
improvement to improve care for a panel of patients.
Project Aim:
Taking the above into account, we designed the Team-based Readmission Assessment Initiative
Notes (T.R.A.I.N.) project, to engage the entire interdisciplinary team in real-time,
interdisciplinary review of patients readmitted within thirty days to the medicine service, with the
goal of reducing the number of patients readmitted to the medicine service within 30 days.
Quantitative/Qualitative Measures
1. Thirty day readmission rates on the medicine service at Tisch hospital.
2. To what extent medicine house staff incorporate readmission risk assessments into their
discharge summaries after the intervention (i.e. present/absent).
System Quality Review
293
NewYork-Presbyterian Healthcare System Quality Symposium 2014
Quality 2020: A Vision of the Future
3. To evaluate the quality of readmission risk assessment in discharge summaries using a
developed grading rubric.
4. Determine what percentage of medicine house staff complete at least one T.R.A.I.N.
evaluation.
5. Determine what percentage of total thirty day readmissions to the Medicine service are
reviewed using the T.R.A.I.N. evaluation tool.
Methodologies
A list of all patients who are readmitted within thirty days of discharge from the Medicine service
is generated once weekly. The interdisciplinary members of each Medicine team receive an email
every Wednesday, if any existing patients on their service are “thirty day readmissions.” By the
following Friday, teams are asked to complete their chart review and input their findings with the
interdisciplinary team, using an online, secure survey tool (figure 1).
During the two month roll out period, teams were expected to evaluate their thirty day
readmissions without further intervention. After this period, an intervention directed at the
hospitalists around best practices for reviewing readmissions was employed.
Every team on the medicine service is included in the readmission review process, with each
medicine team having the opportunity to review one to two readmission cases weekly, ranging
from four to eight readmission cases over the span of their four week rotation.
Improvement Results
While this project is still in its data collection phase, to date we have evaluated 95 readmissions in
real time. The Inpatient-Outpatient (I.P.O.P) conference, a monthly, interdisciplinary conference,
was created to supplement the T.R.A.I.N. curriculum. Each month, a panel of health care
providers discuss a patient who has been readmitted within thirty days. Each conference focuses
on a specific high risk population, and explores themes related to those covered in T.R.A.I.N.
reviews. Multiple themes have emerged from the initial data collection, including the need for a
more robust post-discharge phone call process, a more cohesive strategy to partner with primary
care physicians to ensure timely post-discharge follow up appointments, and the need for a warm
handoff process when discharging patients our most vulnerable patients to subacute nursing
facilities.
Sustainability Strategies
Given that T.R.A.I.N. is an interdisciplinary project, it has become incorporated into part of
weekly interdisciplinary rounds. In addition, each team member is assigned a role in the
readmission review, adding to the engagement around the project. Because the reviews are done
in real time and by members of the health care team currently caring for the readmitted patient,
there is additional buy in from the members of the interdisciplinary team to participate in the
review to determine possible preventable causes of the patient’s readmission.
Lessons Learned
1. Continuous real time readmission reviews serve as a low hanging fruit to engage residents in
the quality improvement process.
System Quality Review
294
NewYork-Presbyterian Healthcare System Quality Symposium 2014
Quality 2020: A Vision of the Future
2. Convening the interdisciplinary team in real time facilitates a natural means of building team
work and improving communication around our most challenging patients.
3. The information learned from the T.R.A.I.N. reviews serves as a bridge to inform a systems
based approach to projects related to care transitions.
Conclusion
Although still in its early phases, the T.R.A.I.N. project is poised to change the culture of how the
medicine service engages around quality – specifically smoothing transitions of care and assessing
readmission risk. It is expected that every member of the interdisciplinary team know who their
patients are that have been readmitted within thirty days. Working collaboratively the goal is to
have each member of the health care team bring their expertise in identifying patients at highest
risk for readmission, and strategizing the safest post-acute care dispositions.
By creating a supplemental curriculum, we have developed a multi-faceted approach to educate
the house staff, and members of the interdisciplinary team, about readmission risk assessment
and tools to reduce readmissions.
System Quality Review
295
NewYork-Presbyterian Healthcare System Quality Symposium 2014
Quality 2020: A Vision of the Future
Figure 1. T.R.A.I.N. online secure survey
System Quality Review
296
NewYork-Presbyterian Healthcare System Quality Symposium 2014
Quality 2020: A Vision of the Future
System Quality Review
297
NewYork-Presbyterian Healthcare System Quality Symposium 2014
Quality 2020: A Vision of the Future
System Quality Review
298
NewYork-Presbyterian Healthcare System Quality Symposium 2014
Quality 2020: A Vision of the Future
Poster Presentation
Stamford Hospital
Reducing Blood Transfusions while Minimizing Risks in the Total Joint
Replacement Population
Valentine, Deb MSN, RN, ONC, CCM; Frenk, Vlad, MD; Orthopedic Service Line Total Joint Replacement
Subcommittee
Introduction
Proactive blood management has become an area of increasing importance in the total joint
replacement population, due to the increased volume of these procedures, and increased
utilization of allogeneic blood transfusions following these procedures. Historically, blood
transfusions were administered to achieve a numerical value. However, perioperative blood
transfusions have contributed to increased morbidity, mortality, hospital cost, and length of stay.
Accordingly, the orthopedic team looked at ways of decreasing the utilization of blood
transfusions.
Project Description: Following a Joint Commission disease specific certification evaluation, we
identified opportunities to improve on several performance measures. The Stamford Hospital
Blood Bank Department had also identified that 30% for our total joint replacement population
received blood transfusions. As a result, an interdisciplinary team of physicians, physician
assistants, nurses, physical therapists and administrative staff convened to improve blood
utilization.
The project aims/goals were to:
-Reduce the rates of blood transfusions among total hip and knee replacement patients by using
IV antifibrinolytics perioperatively
-Change the transfusion triggers from a pre-determined numerical value to individual clinical
situation based on patients' symptoms and cardiac history
-Minimize complications and improve patient outcomes
Quantitative/Qualitative Measures
Measures were established for a pre-intervention group of 61 total hip replacement and 104 total
knee replacements procedures performed from fiscal year 2012 Q2- Q4, and a post-intervention
group of 65 total hip replacements and 99 total knee replacements performed from fiscal year
2013 Q2-Q4.
Measures included percentages of patients requiring blood transfusion and numbers of venous
thromboembolism (VTE) events.
System Quality Review
299
NewYork-Presbyterian Healthcare System Quality Symposium 2014
Quality 2020: A Vision of the Future
Methodologies
The team used a systems approach and A3 methodology. After a literature review was completed,
we initially chose to use Amicar (aminocaproic acid) as the antifibrinolytic for this population.
An article by Camarassa, Olle, Serra, et al, in the British Journal of Anaesthesia (2006),
demonstrated that using antifibrinolytic agents, which included Amicar, significantly reduced
blood loss in total knee replacements. However, after noting 5 VTE events during fiscal year
2012 Q2-4, we reevaluated the use of Amicar, and chose to change to tranexamic acid, which is a
different antifibrinolytic
The decision was supported by an update of the current literature with demonstration of efficacy
of tranexamic acid in the Orthopedic population. Another intervention started during FY12 Q2
was being more pragmatic on blood transfusions triggers.
Improvement Results
Before the project was started, the transfusion rate for total joint replacement patients was 30%.
During the use of Amicar for FY12 Q2-Q4, we reduced the transfusion rate from 30% to 21%.
However, it coincided with an increase in VTE events. Therefore, the team revisited the
risk/benefit ratio of this approach, and identified evidence that supported the preferrential use of
tranexamic acid as an antifibrinolytic agent for the joint replacement population. Amicar was
stopped in FY12 Q4, and tranexamic acid was started in FY13 Q1. By FY13 Q2-Q4, there was
an additional reduction in transfusion rates from 21% to 14%, and a reduction from 5 to 1 VTE
events.
The other practice change established was reevaluation of when to transfuse patients.
Historically, we used a numeric value of hemoglobin 9-10, with some variability between certain
practitioners. Practitioners now look at the patient's symptomatology along with the numeric
hemoglobin value. The transfusion trigger has been reset to be > 7.5, with consideration of
hypovolemia and/or cardiac history. This practice remained consistent during FY12Q2 to the
present.
Sustainability Strategies
Continue with the utilization of tranexamic acid and continue to assess the symptomatology of
the total joint replacement population prior to transfusion.
Periodically evaluate transfusions rates of this patient population.
Lessons Learned
1. Use evidence based medicine to help support changes in practice
2. Monitor clinical outcomes when using antifibrinolytics
3. Recognize team effort and collaboration when changing practice
4. Assess patients in a clinical context, instead of strictly relying on numeric lab values
System Quality Review
300
NewYork-Presbyterian Healthcare System Quality Symposium 2014
Quality 2020: A Vision of the Future
Conclusion
Using a team approach and evidence based practice among physicians, physician assistants,
nursing, and physical therapists, our team adopted a contemporary practice standard and
improved patient safety.
Usage of tranexamic acid along with changes in triggers for blood transfusions for total joint
replacement patients have reduced the utilization of blood products, minimized risks to patients
and decreased overall healthcare cost.
System Quality Review
301
NewYork-Presbyterian Healthcare System Quality Symposium 2014
Quality 2020: A Vision of the Future
Poster Presentation
Stamford Hospital
Improvement in Preterm Infant Hypothermia by the Implementation of a Best
Practice Bundle
Donna Bowman, DNP, FNP-BC, RNC-OB, Kathy LiVolsi, MHA, RNC; Jennifer Cabral, MD; John Ciannella, MD;
Beth Kelley, BSN, RNC-OB; Paul Bobby, MD; Gerry Rakos, MD
Introduction
Background:
All newborn infants are susceptible to hypothermia due to a large body surface area to body mass
ratio as well as an immature thermoregulatory system. The greatest risk for temperature instability
is immediately after birth for the first 12 hours. Preterm infants are especially at risk for
hypothermia. Less body fat, less glycogen stores, immature skin structure and function as well as
poor vascular control leads to an inability to adequately respond to cold stress.
Infants with hypothermia are at higher risk for developing hypoglycemia, respiratory distress,
hypoxia, metabolic acidosis, coagulation defects, delayed transition to neonatal circulation, acute
renal failure, weight loss/failure to gain weight, necrotizing enterocolitis and death. Preterm (less
than 37 weeks gestational age) and Very Low Birth Weight (VLBW) infants (with birth weights
less than 1500 grams) are even more vulnerable to the risks of hypothermia.
Problem:
Through data analysis, a community hospital discovered suboptimal performance in maintaining
a neutral thermal environment for premature infants as compared to its peer groups. Data
submitted to the Vermont Oxford Network (VON) indicated that in comparison to similar
hospitals our Neonatal Intensive Care Unit was performing at the 25th percentile for admission
rectal temperature in VLBW infants. In addition, we began collecting data on all preterm infant
admission temperatures in response to observations by the nursing staff that many infants were
hypothermic on admission to the Neonatal Intensive Care Unit (NICU). The retrospective
baseline data included 45 infants at 36 weeks gestation and under 35 (78%) of those infants had
hypothermia.
Goal:
Our goal was to decrease the number of preterm infants with hypothermia on admission to the
NICU by implementing a bundle of best practices aimed at decreasing heat loss in the delivery
room.
System Quality Review
302
NewYork-Presbyterian Healthcare System Quality Symposium 2014
Quality 2020: A Vision of the Future
Quantitative/Qualitative Measures
Neonatal hypothermia is defined by the World Health Organization as a rectal temperature of
less than 36.5 degrees Celsius. The target temperature was 36.5 C as determined by the Vermont
Oxford Network (VON).
Data was collected monthly for all neonates admitted to the NICU at 36 weeks and under. The
post-implementation data collection took place from February 2013 to June 2014. Full term
infants admitted to the NICU were excluded and 36-week preterm infants who were admitted to
well baby nursery were excluded as well. The NICU admission log provided the list of neonates
who met the inclusion criteria. Their electronic medical records were audited for the data,
including: medical record number, gestational age, admission rectal temperature, mode of
delivery, and whether cord clamping was delayed. Normal (non-hypothermic) admission
temperature was defined as 36.5 Celsius or greater. A NICU RN measured temperatures with a
BD digital thermometer.
Methodologies
Using the PDCA methodology, an inter-professional team reviewed the literature, developed a
protocol based on best practices and educated all nursing and physician staff who attended
deliveries. Following implementation of the bundle, outcomes were tracked and disseminated on
a monthly basis.
The bundle included routine interventions that were already in place to prevent heat loss such as
pre-warming blankets, providing radiant heat or maternal skin-to-skin contact, thoroughly drying
the infant, removing wet linen immediately and placing a hat and diaper. Special measures for
preterm infants derived from the literature included the use of heated mattress pads for all
preterm infants and the use of polyethylene bags in infants 28 weeks and under. A Cochrane
review in 2010 found that both interventions were effective in preventing heat loss in preterm
infants. In addition, preterm infants were no longer weighed in the delivery room in order to
prevent convective and conductive heat loss, and the ambient operating room temperature was
set per the World Health Organization’s recommendation of 25 degrees Celsius for all preterm
births.
Improvement Results
Faced with poor performance in comparison to peer groups, we developed a hypothermia
prevention best practice bundle for preterm neonates to optimize outcomes in this population.
As a result of the new protocol there was an improvement in admission temperatures in preterm
infants admitted to the NICU. The retrospective baseline data included 45 infants. 10 (22%) of
those infants had an admission temperature of 36.5 or greater. Post bundle implementation, there
was a steady improvement in admission temperatures. 68% of infants in FY 14 Q3 had an
admission temperature of 36.5 or greater (see Figure 1).
In the VLBW infants tracked in VON, for the three years prior to the bundle implementation we
performed at 3.8%, 3.10% and 14.3%. The year post implementation, of 12 VLBW neonates,
75% met the standard for temperature on admission to NICU (see Figure 2).
System Quality Review
303
NewYork-Presbyterian Healthcare System Quality Symposium 2014
Quality 2020: A Vision of the Future
Sustainability Strategies
There are many physiological and environmental variables that have an effect infant
thermoregulation. While it is clearly our responsibility to take admission temperatures and
monitor various physiologic parameters in individual neonates, it is equally incumbent on the
health care team to collect and analyze aggregate data on various indicators to monitor overall
performance. More than 300 infant charts have been audited since this project began. Data
collection and dissemination has been a crucial factor in maintaining awareness of this problem
and providing the impetus for continued use of the bundle elements.
Conducting a case by case analysis of outliers is essential for ensuring that any gaps in
performance are recognized and rectified by providing education or counseling to individual
providers.
Lessons Learned
1. Sustained improvement requires a multipronged, interdisciplinary approach. Successful
implementation of the bundle would not have been possible without the commitment and
diligence of all staff involved.
2. The collection and dissemination of data on a monthly basis allowed the team to evaluate our
approach and make adjustments as necessary. We found that it was also necessary to audit
providers for compliance in bundle implementation to be sure that all neonates received the best
care possible.
3. Small practice changes, based on literature review, made a difference with our smallest babies.
Conclusion
Successful implementation of this project required a commitment from the obstetrics and
neonatal team by all physicians and nurses who attend deliveries. The science that forms the basis
of heat loss and generation in the neonate is well established. It is essential to stay abreast of
innovations in care that have been proven to optimize outcomes in this vulnerable population.
Our literature search led to the development of a practice bundle that was successfully
implemented and had a positive impact on the neonates entrusted to our care.
An initial limitation in this quality improvement project and the database is that there was no
documentation of compliance with the bundle elements. It was possible that there were some
staff members who were outliers in compliance and thereby responsible for a greater share of
infants who were hypothermic. The electronic medical record was modified to add a checklist for
the hypothermia prevention measures. Compliance has recently been added to the quality audit
tool and staff will receive feedback accordingly.
The interventions led to an improvement in the admission rectal temperatures of the preterm
neonates admitted to the NICU. However, we need to strive for even better results with this
population. It is clear that there needs to be a continuing effort to improve our practice by
auditing compliance with current best practices and conducting periodic reviews of the literature
to maintain excellent practice standards.
System Quality Review
304
NewYork-Presbyterian Healthcare System Quality Symposium 2014
Quality 2020: A Vision of the Future
Figure 1 All preterm infants admitted to the NICU (N=275)
System Quality Review
305
NewYork-Presbyterian Healthcare System Quality Symposium 2014
Quality 2020: A Vision of the Future
Figure 2 VLBW from the VON database (N = 91)
VLBW Infants Admission Temperature
80
% Normothermic Infants
70
60
50
40
30
20
10
0
2010
2011
2012
2013
SH % Normothermic
3.8
3.1
14.3
75
Database % Normothermic
48.8
51.1
53.9
55.8
System Quality Review
306
NewYork-Presbyterian Healthcare System Quality Symposium 2014
Quality 2020: A Vision of the Future
Stamford Hospital
Decreasing Incidents of Contraband on the Acute Inpatient Psychiatric Unit
Madeline Finegan, MS, RN
Introduction
Background and Problem:
In February 2014, a conundrum emerged on the acute inpatient psychiatric unit at Stamford
Hospital (South 1). Despite the locked doors and security measures that were in place, South 1
experienced a surge of illicit contraband that was being trafficked onto the unit. Upon reviewing
all of the documented incidents, it was determined that a total 8 incidents occurred between
March 2013 and February 2014. These incidents were not just a violation of policy, but they
endangered the health and well-being of our patients and staff. Because of the high risk nature of
these incidents, thorough investigations were conducted and unit policies were reviewed. It was
determined that contraband was making its way onto the unit through visitors coming to see the
patients. A vast initiative was commenced to make changes to the South 1 visitation policy in
order to eliminate the potential for contraband to be brought onto the unit.
Goal Statement:
Incidents of contraband on South 1 will be reduced to 1 per quarter by September 1, 2014.
Quantitative/Qualitative Measures
Stamford Hospital utilizes the QASYS system for reporting all incidents/near-miss incidents that
occur, including contraband. An analysis of all QASYS reports was conducted for South 1
starting from March 1, 2013 through February 28, 2014. A total of 8 incidents of contraband
were reported during this time period. Further analysis of these 8 incidents indicated that
contraband was being brought into the unit by visitors that came to see the patients. We aimed to
implement a strategy to decrease the number of contraband related incidents on South 1 to 1 per
quarter by September 1, 2014.
Methodologies
D-M-A-I-C methodology was used for problem solving and getting to the solution.
D- Define- South 1 staff identified a problem with contraband making its ways onto the acute
psychiatric unit.
M- Measure- Upon reviewing all incidents on South 1, it was determined that a total of 8
incidents of contraband were recorded between March 1, 2013 and February 28, 2014.
A- Analysis- After reviewing and analyzing all 8 incidents that occurred during the identified time
frame, it was determined that patient visitors were bringing the contraband onto the unit.
System Quality Review
307
NewYork-Presbyterian Healthcare System Quality Symposium 2014
Quality 2020: A Vision of the Future
I- Improve- The South 1 unit-based council collaborated and reviewed the unit's Visitation
Policy, and made changes to the visitation procedures for South 1 to eliminate the potential for
contraband to get onto the unit.
C- Control- South 1 unit staff, including nurses and psychiatric technicians have taken ownership
of the revised Visitation Policy. Staff have been trained to strictly adhere to the policy and
enforce the use of the lockers for ALL visitor belongings. All staff are accountable for ensuring
that these procedures are complied with.
Improvement Results
Due to the continuous incidents of contraband being discovered on the unit, a new initiative was
put into place to revise the policy and procedures for visitation on South 1. In February 2014, the
UBC on South 1 collaborated with leadership to make necessary policy changes to ensure that all
guests requesting to visit with patients on South 1 follow specific procedures. The UBC met with
all its members and conducted research on existing evidence-based practice models for visitation
on acute psychiatric units. Additionally, they looked into what practice models were being utilized
on other similar units within the surrounding community. The team then collaboratively decided
upon new visitation procedures. These new procedures included the use of free lockers,
revocation of visitation privileges for non-compliance with policy, and visitation restriction.
Free lockers would be provided for securing personal items and are to be used by all visitors
entering South 1. All visitors must utilize these lockers to prevent contraband from being
brought onto South 1. Visitors may be asked to leave the unit and/or the hospital at the request
of the patient or under certain circumstances, such as inability to follow rules and instructions.
Smoking, unknown drugs/ illicit substances, and contraband (lighter, matches, combustibles,
items that can cause harm to patients) are prohibited on the unit. Failure to comply with this rule
jeopardizes the safety of others and may result in discharge from the hospital, if indicated, and
will result in revoked visitation privileges. Patients admitted to the unit with a positive toxicology
screen (substance and alcohol) will have a visitation restriction for 72 hours, as ordered by the
physician. Decisions to restrict patient’s visitors will be fully explained to the patient and
documented in the patient’s medical record.
After the appropriate changes were made, the new policy was discussed with all staff at the
monthly unit meeting. Input was obtained from all staff and the appropriate changes were made.
The new policy was then rolled out to all of the staff on South 1. Training began in February
2014 and was completed by March 1, 2014. In-services were held for all staff on South 1 and the
new policy was fully implemented on March 1, 2014.
Sustainability Strategies
Since the implementation of the revised South 1 visitation policy in March 2014, there have been
no incidents of illicit contraband reported on South 1. The new policy is strictly adhered to by all
staff. It has also been received well by our patients and their families. No patient or family
complaints have resulted because of the changes.
Sustainability:
System Quality Review
308
NewYork-Presbyterian Healthcare System Quality Symposium 2014
Quality 2020: A Vision of the Future
South 1 unit staff, including nurses and psychiatric technicians have taken ownership of the
revised Visitation
Policy. Staff have been trained to strictly adhere to the policy and enforce the use of the lockers
for ALL visitor belongings. Policy guidelines are posted outside of the unit for reference. All
visitors are thoroughly searched before entering the unit. All unit staff are accountable for
ensuring that these procedures are complied with.
We used a shared governance approach to create opportunities for frontline staff to be directly
involved in this quality improvement initiative. Using this approach enhanced staff buy-in and
sustainability.
Staff will continue to monitor the data and investigate any future incidents.
Lessons Learned
1. Many assumptions were made on how contraband was making its way onto the unit. Many
staff thought that patients were concealing it under their clothing. Staff was surprised to learn
that visitors were the ones bringing the contraband onto the unit.
2. Upon changing the policy, unit staff expressed that they believed the new policy would not be
received well by patient and their families. They were surprised to learn that the education they
provided to patients and their families on the new policy was effective and no complaints were
made.
3. By directly involving frontline staff in the implementation of this initiative, they became
engaged in the process which aided in the sustainability efforts.
Conclusion
Although there are strict policies and procedures that exist for the safety and security of acute
inpatient psychiatric units, staff are often faced with unexpected challenges that require a reassessment of current safety practices. Upon investigating the increased incidents of contraband
being found on South 1, the staff initiated a plan to review current evidence-based practice
models and to make changes to existing practices in order to improve the overall safety of the
staff and patients on South 1. The changes to the visitation policy were seamlessly implemented
and resulted in very positive outcomes. Since March 1, 2014, when the new policy was fully
implemented, there have been no incidents of contraband on South 1. Appropriate policies and
procedures for visitation on acute inpatient psychiatric units has proven to positively impact the
safety of all staff and patients on the unit.
System Quality Review
309
NewYork-Presbyterian Healthcare System Quality Symposium 2014
Quality 2020: A Vision of the Future
System Quality Review
310
NewYork-Presbyterian Healthcare System Quality Symposium 2014
Quality 2020: A Vision of the Future
Stamford Hospital
"Racing to Responsiveness" An Organization’s Unique Journey to Engaging
Staff in Hourly Rounding to Increase Patient Satisfaction and Improve Quality
Outcomes
Ruth Erway, RN; Megan Fortner, MA
Introduction
According to the Studer Group, “Hourly Rounding is one of the most important actions
caregivers can take to improve patient safety (Studer Group Toolkit, p. 25, 2007).” Since first
implemented at Stamford Hospital in June 2011, the clinical staff responsible for hourly rounding
(HR) faced challenges. There had been a lack of shared governance in the original
implementation so staff was not vested in the process, there was no formal policy in place,
recording logs were repetitive and cumbersome, and the staff was not always compliant with
documentation. HR was viewed by nursing staff as a time-consuming, frustrating initiative that
increased their work load and therefore was not being performed on a consistent basis. Staff was
also unaware of the outcomes HR could provide. The only form of accountability for ensuring
the rounding process was taking place was through a validation process carried out by the nurse
managers.
To reinvigorate and engage the staff, a friendly competition called "Racing to Responsiveness"
was implemented in February 2014. The goals of the project were to:
• Create an environment where HR was streamlined and hard-wired into Stamford Hospital’s
nursing care delivery model through a shared governance approach.
• Increase the HCHAPS domain “response of hospital staff” to a goal of greater than or equal
to 70% always.
• Increase the Press Ganey custom question "the extent to which someone checked on you on a
regular basis" to a goal of greater than or equal to 91.
• Decrease unassisted patient falls to less than or equal to 2.0 falls per 1000 patient days.
• Decrease major skin issues to less than or equal to 6 per quarter.
Two committees worked collaboratively to implement this project; the Responsiveness of Staff
Sub-Committee (reporting to the Patient Satisfaction Steering Committee) and the Clinical
Coordinator Rounding Team.
A well-attended Hourly Rounding Fair was held on February 14, 2014, to kick-off the "Racing to
Responsiveness" competition. At the fair staff was educated on the benefits of the "best practice"
of HR. Each unit created a poster board for display which communicated the impact hourly
System Quality Review
311
NewYork-Presbyterian Healthcare System Quality Symposium 2014
Quality 2020: A Vision of the Future
rounding has on improving quality outcomes and patient and nursing satisfaction. At this event a
new benchmark measure was announced; a score of 91.0 on the custom Press Ganey question,
"The extent to which someone checked on you on a regular basis." This measure was used to
validate participation in the rounding process. On a monthly basis the unit that achieved the
highest score while reaching the benchmark was recognized with a trophy celebration and
acknowledgement by nursing leadership.
Quantitative/Qualitative Measures
Quantitative measurements included the results of the custom Press Ganey question for the
quarter prior to implementation in February 2014, and for three additional quarters assessing
performance in patient satisfaction scores for participating units (see Table 1). Additionally, the
Hospital Consumer Assessment of Healthcare Providers and Systems (HCAHPS) Response of
Hospital Staff Domain was used as an indicator of consistency in rounding in relation to staff
response performance (see Table 1).
Nursing and hospital quality indicators including the measurement of unassisted falls (measured
by inpatient falls per 1000 patient days) and major skin issues (breakdowns, ulcerations and
pressure ulcers) were used to identify a correlation between HR and improved patient outcomes
(see Table 2).
Qualitative measures included review of all patient satisfaction survey comments to give survey
respondents an opportunity to convey meaningful information not captured in the survey scores.
Methodologies
The custom Press Ganey question "The extent to which someone checked on you on a regular
basis" was used to measure staff performance of HR. This metric was also used to determine
which units met or exceeded the target goal and which units won the monthly competition.
Along with creating a friendly competition between the units, applying a shared governance
approach for quality improvement was imperative. The direct engagement of the frontline staff
and their input on how to best hard-wire this practice into their daily nursing tasks was integral to
the project’s success. The Clinical Coordinator Rounding Team members solicited feedback from
their unit’s front line staff. Using this information they identified barriers that impeded their
ability to round on patients efficiently. As barriers were identified, the committee worked on ways
to make rounding an easier, more efficient process. Tangible changes such as a new hospital
policy and hourly rounding log were created by staff members to provide a streamlined process
of rounding. Scorecards were distributed on a weekly basis to keep the staff informed of their
progress and to encourage units to strive to meet their goal.
Improvement Results
After the implementation of the "Racing to Responsiveness" competition, the following
improvements were noted for the period of February 2014 (Q2) through present.
• Mean score of the custom Press Ganey question increased by 1 point (see Table 1).
• HCAHPS Response of Hospital Staff Domain increased by 4 percentage points, from 66% to
70% for This measure exceeds the national average by 2 percentage points (see Table 1).
System Quality Review
312
NewYork-Presbyterian Healthcare System Quality Symposium 2014
Quality 2020: A Vision of the Future
• Unassisted Inpatient Falls Rate decreased by 1.1 falls per 1000 patient days (see Table 2).
• A decrease in major skin breakdown, ulcerations and ulcers from 12 in Q1 & Q2 to 5 from the
beginning of Q4 to present, a decrease of 7 (see Table 2).
Sustainability Strategies
Stamford Hospital continues to support the "Racing to Responsiveness" competition celebrating
success throughout the organization.
• The Clinical Coordinator Rounding Team meets monthly to share success strategies, continue
to address barriers and identify ways to keep staff engaged and accountable to the rounding
process. The clinical coordinators disseminate this information to the frontline staff at Unit
Based Council meetings and at unit huddles.
• Staff is recognized publicly on their unit with a surprise visit from nursing leadership to award
them the coveted race horse theme trophy to be displayed on the unit throughout the month.
Cupcakes are included.
• Staff is recognized at high level, multidisciplinary meetings that include executive leadership.
• Weekly scorecards are sent to all units and nursing leadership and are posted on bulletin boards
on all units.
• A Racing to Responsiveness bulletin board in the Main Cafeteria showcases each unit’s
performance.
• News stories on winning units have appeared in the organization’s newsletter, Newsline. The
plan is to continue the competition into the next fiscal year with a new theme of Car Racing, to
foster continued enthusiasm.
Lessons Learned
1. Reward and recognition of staff from leadership for their accomplishments in the work of
hourly hounding served to increase morale as staff was appreciated for their dedication and hard
work.
2. Identifying and addressing key barriers to success was a critical component of the program.
One example was a shift to a shared governance approach which created opportunities for
frontline staff to be directly involved in the process. This was an improvement over the
previously attempted top-down approach. Also, a shift to nurse manager validation contributed
to staff success.
3.Peer-to-peer accountability proved to be successful in streamlining HR into the care delivery
model and reinforcing compliance by staff with this "Best Practice." Clinical coordinators were
empowered in the role of champion to ensure this process was integrated into nursing daily
routine.
Conclusion
In conclusion, implementation of the Racing to Responsiveness competition has had a positive
impact on Stamford Hospital’s HR program as evidenced by improved patient satisfaction scores
and reduced unassisted inpatient falls and major skin issues. The importance of a shared
System Quality Review
313
NewYork-Presbyterian Healthcare System Quality Symposium 2014
Quality 2020: A Vision of the Future
governance model in engaging frontline staff was imperative in addressing barriers to success.
Along with striving for excellent patient care outcomes, the culture of our organization supports
a fun atmosphere that promotes innovation to improve quality, safety and the patient experience.
The success of the Racing to Responsiveness initiative supports engaging staff in a nontraditional way to improve outcomes for our patients.
Table 1.
100%
95%
98
PG Mean Score
96
90%
Intervention:
Racing to
Responsiveness
Competition
94
85%
92
80%
90
75%
88
70%
86
65%
84
60%
82
55%
80
Q1
Q2
Q3
Q4
PG "Extent to which someone
checked on you on a regular
basis"
88.5
88.8
90.1
89.5
HCAHPS Response of Hospital
Staff
69%
66%
70%
70%
System Quality Review
50%
314
HCAHPS Percentage
100
Patient Experience: Press Ganey & HCAHPS
FY 2014
NewYork-Presbyterian Healthcare System Quality Symposium 2014
Quality 2020: A Vision of the Future
Table 2.
3
12
Intervention:
Racing to
Responsivenes
2.5
10
2
8
1.5
6
1
4
0.5
2
0
Q1
Q2
Q3
Q4
Unassisted Falls Rate
2.6
1.95
1.6
1.5
Major Skin Issues
12
12
7
5
System Quality Review
0
315
Reportable skin issues
Inpatient falls per 1000 pt days
3.5
Unassisted Inpatient Falls & Major Skin Issues
FY 2014
14
NewYork-Presbyterian Healthcare System Quality Symposium 2014
Quality 2020: A Vision of the Future
Stamford Hospital
Unplanned Extubation of Patients Undergoing Mechanical Ventilation
Alberto Monegro MD; Marta Kokoszynska MD; Sharon Kiely MD; James Krinsley MD, FCCM, FCCP
Introduction
I. PROJECT DESCRIPTION
Among critically ill patients undergoing mechanical ventilation (MV), unplanned extubation (UE)
is a major concern as it is associated with increased mortality and morbidity (1-5). Reported rates
of UE range from 1% to 14% of episodes of MV. Reintubation after UE has been reported to
occur in 22% to 78% of patients, and is associated with increased intensive care unit (ICU) length
of stay (LOS), the development of nosocomial pneumonia, and death.
We sought to identify the characteristics of patients sustaining UE with the purpose of
developing a risk assessment tool that would enable clinicians to target high risk patients who
would need greater surveillance. We also conducted a subset analysis comparing outcomes of
patients who had UE and required reintubation (RE-I) to those who did not require reintubation
(NO RE).
Our goal is to reduce the occurrence of UE in our ICU and thereby improve patient outcomes by
decreasing ICU LOS, duration of MV, nosocomial pneumonia and death.
Quantitative/Qualitative Measures
This is a retrospective analysis of prospectively collected data and information abstracted from
the patient's electronic medical record and includes every patient who experienced UE between
1/1/06-9/30/13. Data elements abstracted from the Stamford Hospital's ICU database include
age; ICU LOS; MV days; Acute Physiology and Chronic Health Evaluation (APACHE IV)
predicted hospital mortality; mortality; ICU-acquired infections. Data elements abstracted from
the electronic medical record include history of excessive alcohol use preceding hospitalization;
English not primary language; and aspects of patient care at the time of UE including: MV mode
and FiO2; Richmond Agitation Sedation Scale (RASS) score; use of restraints; sedation
administration; description of airway secretions. Continuous data are compared using the MannWhitney rank sum test or Student's t test, as appropriate. Categorical data are compared using the
Chi square test. We created a multivariable model to assess (1) whether UE was independently
associated with death, and (2) among the UE cohort, whether RE-I was independently associated
with death.
System Quality Review
316
NewYork-Presbyterian Healthcare System Quality Symposium 2014
Quality 2020: A Vision of the Future
Methodologies
We sought to improve risk stratification for patients undergoing MV who are at increased risk for
UE. We approached the quality improvement using the FADE model.
Focus: We reviewed the medical literature to better understand risk factors for UE. We then
generated a comprehensive list of factors to study in our patient population at Stamford Hospital
that would be feasible and practical to track prospectively.
Analyze: We performed a retrospective analysis of information abstracted from the ICU's
comprehensive database as well as additional information obtained from review of the patients'
electronic medical record.
Develop: We identified potential risk factors that needed further analysis. We developed a worksheet to be filled at the time of event that would include input from nursing staff, respiratory
therapist, and physicians.
Execute: We are in the process of obtaining commitment to use this worksheet in our ICU.
Improvement Results
Of the 7,896 patients who were admitted to the Stamford Hospital ICU between 1/1/069/30/13 2,874 (36.4%) required MV and 91 experienced UE (3.2% of those undergoing MV).
*Table 1 compares clinical characteristics of patients with and without MV, as well as patients
sustaining UE. Patient undergoing MV had a higher severity of illness, reflected by the APACHE
IV predicted mortality (APIV PM) (p<0.0001), longer ICU LOS (p<0.0001), higher mortality
(p<0.0001) and higher observed:expected mortality ratio than did those not undergoing MV.
Patients with UE had lower APIV PM (p=0.0181) and longer ICU LOS (p=0.0006) compared to
those who undergoing MV without UE, but similar age, distribution of admitting diagnoses and
mortality.
*Table 2 details selected clinical characteristics of the UE cohort, comparing RE-I and NO RE.
There was no difference in the number of days of MV prior to the UE event comparing RE-I
and NO RE. RE-I tended to be older (p=0.0598) and had a higher APIV PM (p=0.0051)
compared to NO RE. However, there were no significant differences in percentages of patients
with English not as a primary language; history of excessive alcohol use prior to admission;
restraint use; presence of heavy airway secretions; RASS score; or MV mode comparing these
two groups.
*Table 3 illustrates important differences in outcomes comparing RE-I and NO RE. RE-I had
markedly longer ICU LOS (p=0.0002) and duration of MV (p<0.0001) as well as a much higher
rate of ICU-acquired pneumonia (p=0.0411) and other ICU-acquired infections (p=0.0020). The
higher mortality among RE-I did not reach statistical significance.
*Among patients undergoing MV, multivariable analysis demonstrated that UE was not
independently associated with increased risk of death: OR 1.11 (0.60-2.04) p=0.7496. Among
patients sustaining UE, RE-I was not independently associated with increased risk of death: OR
1.20 (0.37-3.94) p=0.7581.
System Quality Review
317
NewYork-Presbyterian Healthcare System Quality Symposium 2014
Quality 2020: A Vision of the Future
Sustainability Strategies
Through the utilization of our Unplanned Extubation Worksheet we hope to identify parameters
contributing to UE that include difficult to measure factors such as nursing workload, bedside
treatments and maneuvers occurring at the time of the UE event and sedation immediately
preceding UE. This quality improvement project will be cyclical in nature and eventually should
help to create a risk assessment tool as well as the design of process measures to improve care
with the goal of reducing the occurrence of UE. Prospective evaluation of these data will be
shared with the clinical staff, including physicians, nurses and respiratory therapists, in order to
further refine practice patterns and increase awareness of risk factors for UE.
Lessons Learned
1. Factors contributing to UE need to be studied using a multidisciplinary approach involving
input from physicians, nursing staff, and respiratory therapists.
2. Additional data obtained at the time of the UE event may provide further insight into risk
factors for UE and allow more detailed comparison of those patients undergoing MV with and
without UE.
3. At this point we cannot identify a single factor that can easily predict which patients are at
increased risk of UE, providing an opportunity for the development of a risk stratification tool
that uses multiple parameters to better predict risk.
Conclusion
*Unplanned extubation (UE) was a relatively uncommon event, occurring among 3.2% of
patients undergoing mechanical ventilation (MV) in this large cohort of patients admitted to an
adult ICU over a 7 year period.
*Among patients undergoing MV, UE was associated with increased ICU length of stay and days
of MV as well as increased rates of ICU-acquired pneumonia and other ICU-acquired infections,
but not death.
*Strengths of this analysis include the comprehensive metrics captured in the ICU database as
well as the numerous elements abstracted from the patients' electronic medical record. However,
the relatively small number of patients with UE limited statistical comparison of those patients
requiring reintubation to those not requiring reintubation. An additional limitation of this analysis
is the absence of important data relating to nursing workload, bedside treatments or maneuvers
occurring at the time of the UE event.
*These findings have important clinical implications. UE is associated with significant morbidity
and is worthy of efforts to reduce its occurrence. Future work will entail the development and
promulgation of a UE risk assessment tool to guide bedside therapy with the goal of improving
patient outcomes.
System Quality Review
318
NewYork-Presbyterian Healthcare System Quality Symposium 2014
Quality 2020: A Vision of the Future
Table 1
Clinical characteristics and outcomes of patients admitted to the Stamford Hospital ICU 1/1/06 – 9/30/13
All
All non-vent
All vent
Vent no UE
UE
7,896
5,022
2,874
2,783
91
64.7 (18.5)
64.3 (18.8)
65.4 (18.1)
65.5 (18.1)
62.9 (17.4)
Medical
55.0
50.6
62.7
64.2
71.4
Surgical
34.1
37.3
29.1
26.9
19.8
Trauma
10.9
12.1
8.2
8.9
8.8
1.5 (0.9-3.2)
1.1 (0.8-1.9)
3.2 (1.5-8.0)
3.1 (1.5-7.9)
5.2 (2.3-12.8)
N/A
3 (2-7)
3 (2-7)
4 (2-11)
18.7 (24.6)
9.8 (14.0)
35.8 (30.8)
36.1 (30.9)
27.4 (24.3)
Mortality (%)
13.6
6.0
26.7
26.9
22.0
O:E
0.72
0.61
0.75
0.75
0.80
Number
Age
Service (%)
ICU LOS
Vent days
APIV PM
Vent – requiring mechanical ventilation
UE – unplanned extubation
LOS – length of stay
Vent days – days of mechanical ventilation
APIV PM – APACHE IV prediction of mortality
Mortality – defined as hospital discharge status
O:E – observed: expected mortality ratio
Data are displayed as percentages, mean (standard deviation), or median (interquartile range)
N/A – not applicable
System Quality Review
319
NewYork-Presbyterian Healthcare System Quality Symposium 2014
Quality 2020: A Vision of the Future
Table 2
Clinical characteristics of patients with unplanned extubation: comparison of those with and without need for
reintubation
Not
Reintubated
58
Reintubated
60.3 (18.9)
67.4 (13.5)
0.0598
2 (1-4)
2 (1-7)
0.9562
Medical
72.4
66.7
NS
Surgical
20.7
27.2
Trauma
6.9
6.1
22.1 (21.9)
36.9 (25.8)
0.0051
Alcohol (%)
15.5
15.2
0.7968
English not primary (%)
29.3
15.3
0.2148
Secretions heavy (%)
12.1
24.2
0.2261
Restraints (mitts) (%)
36.2
39.4
0.9386
RASS A +2 - +4
22.2
25.9
NS
RASS B -2 - +1
72.2
66.7
RASS C -5 - -3
5.6
7.5
Volume Control
40.4
36.4
Pressure Support
49.1
36.4
Tube Compensation
10.5
21.2
Pressure control
0.0
6.1
67.2
46.9
Number
Age
Days on vent before UE
P value
33
Service
APIV PM (%)
RASS (%)
Vent mode (%)
Weaning (%)
NS
0.0936
FiO2
System Quality Review
320
NewYork-Presbyterian Healthcare System Quality Symposium 2014
Quality 2020: A Vision of the Future
< 0.35
49.1
33.3
NS
0.35 – 0.50
43.9
51.5
> 0.50
7.02
15.2
Propofol
36.2
33.3
0.9615
Fentanyl
27.6
18.2
0.4513
Intermittent benzo
12.4
24.2
0.2451
Antipsychotic
6.9
6.1
0.7758
Sedation (%)
UE – unplanned extubation
Vent – mechanical ventilation
APIV PM – APACHE IV prediction of mortality
Alcohol – history of alcohol abuse
RASS – Richmond Agitation Sedation Scale
FiO2 – fractional concentration of oxygen delivered by mechanical ventilator at time of UE
Benzo - benzodiazepine
Data are displayed as percentages, mean (standard deviation), or median (interquartile range)
NS – not statistically significant
System Quality Review
321
NewYork-Presbyterian Healthcare System Quality Symposium 2014
Quality 2020: A Vision of the Future
Table 3
Outcomes of patients with unplanned extubation: comparison of those with and without need for
reintubation
Not Reintubated
Reintubated
Number
58
33
Vent days
3 (2-6)
13 (6-20)
<0.0001
4.6 (1.7-8.8)
12.9 (4.0-18.9)
0.0002
Nosocomial pneumonia (%)
(1.7)
(15.2)
0.0411
Other nosocomial infection (%)
(1.7)
(34.2)
0.0020
Mortality (%)
17.2
30.3
0.2367
O:E
0.78
0.82
ICU LOS (median, IQR)
P value
UE – unplanned extubation
LOS – length of stay
Vent days – days of mechanical ventilation
Mortality – defined as hospital discharge status
O:E – observed: expected mortality ratio
Data are displayed as percentages, mean (standard deviation), or median (interquartile range)
NS – not statistically significant
System Quality Review
322
NewYork-Presbyterian Healthcare System Quality Symposium 2014
Quality 2020: A Vision of the Future
UNPLANNED EXTUBATION WORKSHEET
Date of UE: ________
Time of UE: ________
SEDATION:
2hr prior
1h
At time of UE
Propofol
Versed
Fentanyl
Ativan
RASS
RESPIRATORY FACTORS
Was patient being weaned? ( ) Yes, () No; if yes; time weaning was started: _____________
ET tube securing method:
PATIENT CHARACTERISTICS:
Language barrier: Yes ( ) No ( )
Native Language of patient:
Patient follows commands: Yes ( ) No ( )
Is there smoking history ( ) Yes (); is the patient an active smoker ( ) Yes, ( ) No
System Quality Review
323
NewYork-Presbyterian Healthcare System Quality Symposium 2014
Quality 2020: A Vision of the Future
NURSING
Number of patients per nurse
Was nurse able to redirect in patient’s own language (if other than English)
Did a new admission arrive to unit within two hours of event: Yes () No ()
Was the event witnessed: ( ) Yes, ( ) No; if yes, was it ( ) deliberate or ( ) unintentional
Restraint: Yes ( ) No ( ); if yes, type of restraint: _________
COMMENTS:
System Quality Review
324
NewYork-Presbyterian Healthcare System Quality Symposium 2014
Quality 2020: A Vision of the Future
Stamford Hospital
Reducing Unassisted Falls in the ED and Inpatient Setting
Ellen Komar BSN, RN, MCA, NEA-BC (VP of Patient Care Services and CNO); Kelly Maggiotto, BSN, RN; Sarah
Sanders, BSN, RN; Carolyn Hoffman-Kaminski, RN, MS, CPHQ, CPHRM; Kelly Maggiotto, BSN, RN-BC; Jackie
Kingston, MSN, RN; Michelle Watson, MSN, APRN, FNP-BC, C; Eileen Spenard, DNP, RN; Joan Sorich, MSN,
RN, AOCNS; Christina Curtin, BSN, RN; Maureen McCauley, BSN, RN; Roseann Cardi, MSN, RN, CRRN;
Madeline Cruz, DNP (c), BSN, RN, MS; Stephanie Porricelli, BSN, RN; Brigette Niesen, MSN, RN; Ryan Strouse,
BSN, RN; Gigi Kearney, D.P.T; Sokhak So, PharmD; Christopher Renz, MBA
Introduction
Inpatient falls are a significant patient safety and quality concern. In a document on fall and injury
prevention published by the Agency for Healthcare Research and Quality (AHRQ) it was
reported that patient falls occur in approximately 1.9 to 3% of all acute care hospitalizations. The
Joint Commission reported that an estimated 30% of inpatient falls resulted in serious injury or
harm. Additionally, according to the Institute for Healthcare Improvement (IHI), falls are a
leading cause of death in people 65 years of age or older and 10% of fatal falls for the elderly
occurs in hospitals.
The National Database of Nursing Quality Indicators (NDNQI) defines a major injury as a fall
resulting in an insult requiring surgery, casting, traction, consultation for neurological or internal
injury, patients with any type of fracture regardless of treatment, or patients with a coagulopathy
who receive blood products as a consequence of the fall. In addition to patient harm, patient falls
affect hospitals fiscally secondary to increased lengths of stay, added diagnostic procedures,
surgery, and follow up care. The Centers for Disease Control and Prevention (CDC) estimated
the cost to an acute care facility to treat the 30% of falls resulting in serious injury is expected to
reach $54.9 billion in 2020.
While Stamford Hospital has consistently focused on reducing the number of patient falls, we
recognized that there was an opportunity to further evaluate our fall prevention program on an
organizational level. Our goal was to reduce the number of harm events associated with patient
falls. Stamford Hospital elected to focus on an unassisted fall rate, falls in which a staff member
was not present and therefore was unable to minimize the impact of the fall. At the culmination
of quarter 1, fiscal year, 2014 (October, November, December 2013), the committee identified
that the hospital's, unassisted fall rate had increased over the past two quarters (Table 1).
Quantitative/Qualitative Measures
Quantitative: Stamford Hospital utilizes the QASYS system for reporting all incidents/near-miss
incidents that occur, including patient falls. An analysis of all inpatient units and Emergency
Department falls were evaluated. It was determined that there was a sustained increase over the
past two quarters in the unassisted fall rate. When evaluating causation of the falls, it was
System Quality Review
325
NewYork-Presbyterian Healthcare System Quality Symposium 2014
Quality 2020: A Vision of the Future
determined that a majority of them may have been preventable. We aimed to decrease our
unassisted fall rate on the inpatient units and Emergency Department.
Methodologies
D- Define- Stamford Hospital’s Fall Committee identified a problem with an increased unassisted
fall rate.
M- Measure- Upon reviewing the unassisted fall rate, it was determined that the fall rate for
FY’14 Q1 was 2.6/1000 patient days.
A- Analysis- After reviewing and analyzing the unassisted falls, it was determined that a majority
of these falls may have been preventable.
I- Improve- Stamford Hospital’s Fall Committee created an overall Fall Prevention Action Plan
to decrease the number of unassisted falls.
C- Control- All staff have been trained in the Fall Prevention Action Plan and the changes it
enforces. All staff are held accountable for ensuring the safety of their patient’s and that fall
prevention strategies are followed.
Improvement Results
The Hospital utilizes the John Hopkins Fall Scale to assess fall risk in the hospitalized patient.
The team examined the efficacy of the tool. After much research, it was determined that the John
Hopkins Fall Scale was an appropriate tool to accurately assess risk for falls in our patient
population.
The team then identified challenges surrounding the staff’s response time to bed and chair
alarms. Staff members participated in a pilot in which bed and chair alarms were purposely
engaged and response times recorded. With this, the observers were also asked to take note of
practice and environmental factors that may pose barriers, inhibiting staff responses to alarms.
During this assessment, the average response time to these alarms was 46 seconds. Staff
participating in the pilot also observed that, non-nursing and ancillary staff members often
walked past the alarming patient’s room and were unaware of what the bed and chair alarm
meant. In response an immediate “No Pass Zone” (NPZ) was created. The team communicated
to ancillary departments via huddles. The team provided education on fall prevention strategies
and how to respond to alarms consistent with their scope of practice. There has been a sustained
decrease in bed and chair alarm response times for the past three quarters. Another effective
strategy identified by the team was to reduce the congestion of the patient rooms. The team
determined that equipment and furniture could be strategically located in a manner that would
provide a clear trajectory to the bathroom and enhance patient safety. Previously the practice had
been to place the patient’s chair next to the window, the farthest distance from the bathroom
with many interfering obstacles for patients and staff. The team collaborated with environmental
services to clone the set-up of the rooms with this safety strategy. The ED developed an action
specific to their population and environment specifically aimed at identifying fall risk patients at
the point of triage so fall prevention strategies can be initiated. As a result of the improvement
strategies developed for the inpatient areas and the ED the unassisted fall rate went from as high
System Quality Review
326
NewYork-Presbyterian Healthcare System Quality Symposium 2014
Quality 2020: A Vision of the Future
as 2.99/1000 patient days in September 2013, to being consistently less than 1.90 for the past 5
months (Table 1)
Sustainability Strategies
Sustainability Strategies- Since the implementation of the Falls Prevention Action Plan, there has
been a decreased number of unassisted falls. All staff have taken ownership of fall prevention
strategies as outlined in the action plan. Reward and recognition have proven useful in staff buyin and sustainability. Positive reinforcement and rewards are provided to staff on an ongoing
basis to encourage these best practices. Staff responding promptly to the patient’s bed alarms or
promptly intervening to prevent a patient from falling are provided with positive reinforcement
and are recognized during huddles on their units with other staff members present. Unit based
unassisted fall numbers are watched closely by the Fall Committee. Units reaching fall free
milestones have been recognized with cakes, certificates, and candy to recognize staff for all their
hard work and dedication to fall prevention.
The Fall Committee continues to monitor the unassisted fall rate on a weekly basis, adds
strategies to their Fall Action Plan.
Lessons Learned
1) Expectations regarding alarm response accountability cannot be assumed. Staff at all levels
need clearly defined expectations related to bed and chair alarm response consistent with their
scope.
2) A "No Pass Zone" is essential if you are going to reach a patient in time and reduce unassisted
falls.
3) An interdisciplinary approach allowed us to leverage the intellect and expertise of multiple
stakeholders contributing to the reduction in unassisted falls.
Conclusion
Although Stamford Hospital has a Fall Prevention Protocol in place, the Fall Committee noted
the high number of unassisted falls in FY’14 Q1. This prompted an immediate Fall Action Plan.
Using evidence- based practice models; strategies were implemented to further enhance our fall
prevention practices. The changes set forth in the action plan decreased the number of unassisted
falls, enhancing patient safety. The Fall Committee evaluates the Fall Action Plan on an on-going
basis and we are making strides in further enhancing fall prevention within the organization.
System Quality Review
327
NewYork-Presbyterian Healthcare System Quality Symposium 2014
Quality 2020: A Vision of the Future
Table 1
System Quality Review
328
NewYork-Presbyterian Healthcare System Quality Symposium 2014
Quality 2020: A Vision of the Future
Stamford Hospital
Improving Quality of Care and Patient Outcomes Through Management and
Transparency of Hospital Acquired Conditions and Patient Safety Indicators
Carolyn A. Hoffman-Kaminski, RN, MS, CPHQ, CPHRM; Karen Lawler, MPS, RHIA, CHPS, FABC; Rohit
Bhalla, MD, MPH
Introduction
Since the Institute of Medicine’s report, "To Err is Human," there has been a growing focus from
the Centers for Medicare & Medicaid Services (CMS) and other oversight agencies, on hospital
patient safety. Over the past decade, Medicare has developed pay-for-performance programs for
hospitals including one focused on hospital-acquired conditions. The Hospital Acquired
Condition (HAC) Reduction program is one of three pay-for performance programs developed
by CMS. The others are the Hospital Readmissions Reduction and Value Based Purchasing
programs.
In 2008, CMS implemented a policy of not paying hospitals for the care of patients who
sustained preventable hospital acquired conditions. Currently the CMS HAC list has been
expanded to include fourteen conditions. These include: foreign object retained after surgery, air
embolism, blood incompatibility, pressure ulcers stages III and IV, falls and trauma, catheter
associated urinary tract infections (CAUTI), vascular catheter associated infections,
manifestations of poor glycemic control, surgical site infections (SSI)-mediastinitis following
coronary artery bypass graft, SSI following cardiac implantable electronic devices, deep vein
thrombosis and pulmonary embolism following certain orthopedic procedures and, iatrogenic
pneumothorax with venous catheterization.
For federal fiscal year 2015, the HAC Reduction Program will include 2 domains. Domain 1
focuses on the Agency for Healthcare Care Research and Quality Patient Safety Indicator (PSI)
Composite 90, and Domain 2 includes CAUTI and Central Line Associated Blood Stream
Infections (CLABSI). Hospitals that perform in the lowest 25th percentile of the program will be
penalized 1% of their Medicare payment.
The organization’s review processes did not typically include a re-confirmation of pertinent
diagnoses following coding of medical records. The burden rested primarily on Health
Information Management coders who based their decision solely on documentation in the
medical record or lack thereof, and on the quality professionals whose role includes monitoring
trends in performance.
The organization sought to improve overall patient safety through the reduction of HACs and
PSIs, through intensive review of these events. Key initial interventions included expert case
review by related specialty services, improved clinical provider documentation, further training
System Quality Review
329
NewYork-Presbyterian Healthcare System Quality Symposium 2014
Quality 2020: A Vision of the Future
for coders on HAC criteria and exclusions, HAC and PSI specific action plans, and expanded
transparency of data.
Quantitative/Qualitative Measures
The hospital focused on the reduction of Hospital Acquired Conditions, listed above, as well as
those Patient Safety Indicators outlined in the AHRQ Patient Safety Indicator (PSI) 90
Composite. The AHRQ PSI 90 Composite includes: pressure ulcer stage III and IV, iatrogenic
pneumothorax, CLABSI, post-operative hip fracture, post-operative pulmonary embolism or
deep vein thrombosis, post-operative sepsis, post-operative wound dehiscence and accidental
puncture or laceration.
Methodologies
Oversight of the hospital’s HAC and PSI reduction program consisted of a multidisciplinary team
known as the Public Reported Safety Measures (PRSM) team coordinated by the Directors of
Quality and Health Information Management. Members of the team included the Chief Quality
Officer, physician Director of Hospitalist services, physician Director of Case Management and
Utilization Review, an HIM Analyst, a representative from the Organizational Clinical
Effectiveness Group, a Systems Analyst, an RN Manager of Infection Prevention, an Intensivist,
and the Nursing Director of Clinical Operations and Quality. Team roles and responsibilities
were assigned, and a project charter was developed and approved by the team and executive
management. Lean Six Sigma methodology was utilized to design process steps, analyze
problems, identify interventions and potential solutions and monitor effectiveness and ongoing
sustainability. A process map was developed outlining the current review process (see Diagram
1). Inefficiencies in our workflow process were identified as well as causes affecting performance.
2011 baseline data was also obtained to identify safety events with the highest incidence.
Improvement Results
Improvement strategies directly targeted improving patient outcomes. Improvement strategies to
address pressure ulcers included increases in wound care RN availability to 5 days/week, wound
care product enhancements and Emergency Department present on admission wound care
review. Catheter hub maintenance re-education and certification on central lines, daily device
rounds and implementation of a device board was effective in reducing hospital-wide central line
associated blood stream infections. Meditech templates, order sets, daily prophylaxis worklists
and staff education played a major role in the reduction of deep vein thrombosis and pulmonary
embolism prevention. Other solutions included implementation of a sepsis bundle, continuous
insulin infusion therapy protocol and early ambulation program in the ICU, remote telemetry
boxes and Inspiron usage improvement to address post-operative respiratory failure.
Finally, the team developed a concurrent HAC and PSI identification review process (see
Diagram 2). Meditech IT program reports were created by our systems analysts to generate
weekly HAC and monthly PSI reports. These reports were reviewed by our Senior Coding
Analyst to validate code inclusion and criteria. Those cases that met HAC and PSI coding criteria
were assigned to the appropriate specialist for a physician medical review to confirm diagnosis.
Those cases not meeting both coding and medical diagnostic criteria were reviewed by the PRSM
System Quality Review
330
NewYork-Presbyterian Healthcare System Quality Symposium 2014
Quality 2020: A Vision of the Future
team to determine next steps. This could include further clarification and/or documentation
needed by the attending physician or an additional case review by coding and a second physician.
Figures 1 and 2 depicts baseline data for HAC and PSI from FY 2011. The project
implementation phase encompasses the following two and a half fiscal years for our HAC efforts
and 27 months for our PSI efforts respectively. During these time periods the hospital
experienced a 62% reduction in our HAC and an 25% reduction in our PSI. Annualized rates for
HAC over the past six months and nine months for PSI suggest rates have leveled off. (See
Figure 1 and 2).
Sustainability Strategies
The Publicly Reported Safety Measures (PRSM) team will continue to meet monthly to review
ongoing trends. The effectiveness of the concurrent review process will be monitored for any
identified inefficiencies or inconsistencies with the process. Target improvement strategies
previously implemented will remain in place. Additional action plans will be identified by the
PRSM team based on trend analysis. Lastly, transparency of data to front line staff, leadership
and the Board, is imperative to ensure tactical focus and improving patient outcomes.
Lessons Learned
1. Transparency of hospital performance indicators to all hospital constituents positively
influences patient outcomes and staff motivation.
2. Focusing and raising the level of awareness of quality indicators and financial implications
assists in reducing adverse patient safety events and patient care costs.
3. Multiple innovative strategies are needed to address healthcare challenges and changes.
Conclusion
Patient safety and adverse outcomes will continue to increase public attention as well as create an
additional financial burden for hospitals. Implementation of proactive protocols, prevention
strategies and transparency of data by a multidisciplinary team resulted in a significant reduction
in hospital acquired conditions and inpatient complications. Ongoing hospital-wide attention to
process improvement and patient safety will ensure sustainability in current practices, and allow
identification of additional opportunities for improvement.
System Quality Review
331
NewYork-Presbyterian Healthcare System Quality Symposium 2014
Quality 2020: A Vision of the Future
Diagram 1: Hospital Acquired Conditions and Patient Safety Indicators Review Process- Post
Discharge
System Quality Review
332
NewYork-Presbyterian Healthcare System Quality Symposium 2014
Quality 2020: A Vision of the Future
Diagram 2: Hospital Acquired Conditions and Patient Safety Indicators Concurrent Review Process
System Quality Review
333
NewYork-Presbyterian Healthcare System Quality Symposium 2014
Quality 2020: A Vision of the Future
Figure 1: Stamford Hospital - Hospital Acquired Condition Reduction
Hospital Acquired Conditions
FY'11 - FY'14
60
53
50
40
30
30
20
20
23
10
0
FY 2011
FY 2012
FY 2013
FY 2014
Annualized
Figure 2: Stamford Hospital - Patient Safety Indicator Reduction Program
Patient Safety Indicators
FY'11 - FY'14
100
80
84
90
60
63
64
FY 2013
FY 2014
Annualized
40
20
0
FY 2011
System Quality Review
FY 2012
334
NewYork-Presbyterian Healthcare System Quality Symposium 2014
Quality 2020: A Vision of the Future
Stamford Hospital
A Novel Protocol for Identification and Risk Reduction in Patients with
Prolonged QTc on Electrocardiogram
Geoffrey Gittleson, PharmD, M.S.; Sokhak So, PharmD; Ryan Brown, PharmD Candidate; Amanda Hubeny, PharmD
Candidate; Valerie Huynh, PharmD Candidate; Darell Grigerick, RDCS, M.A.; Steven Horowitz, M.D., F.A.C.C.
Introduction
PROBLEM STATEMENT:
QTc prolongation on electrocardiogram (ECG) is a cause of torsade de pointes, a potentially
lethal arrhythmia, responsible for approximately 13% of sudden cardiac deaths.
At present there is no standardized approach for identification of QTc prolongation and
concomitant pharmacologic evaluation and management in hospitalized patients.
PROJECT AIM:
To create an inpatient QTc monitoring and intervention program through a collaborative effort
between Pharmacy and Cardiology.
Stamford Hospital initiated a Pharmacy & Therapeutics Committee approved policy for critical
drug regimen review and monitoring by pharmacists in patients with prolonged QTc interval.
The protocol categorizes the risk potential of medications that can cause torsade de pointes.
Assessment of risk was based on the ArizonaCert, which consists of three classifications:
medications with known risk (‘risk’), possible risk (‘possible’) or conditional risk (‘conditional’).
Using these three categories, pharmacists reviewed each patient chart and placed a call to the
physician in one of the following scenarios:
Patient has a QTc of 500 msec or has a QTc interval increase of 60 msec from prior ECG and is
on one or more medications with ‘risk’ for torsade de pointes.
Patient has a QTc of 500 msec or has an a QTc interval increase of 60 msec from prior ECG and
is on one or more medications with ‘risk’ for torsade de pointes plus one or more medications
with ‘possible’ or ‘conditional’ risk for torsade de pointes.
Patient has a QTc of 580 msec or greater and is on one or more medications with 'risk', 'possible'
or 'conditional' risk for torsade de pointes.
System Quality Review
335
NewYork-Presbyterian Healthcare System Quality Symposium 2014
Quality 2020: A Vision of the Future
Quantitative/Qualitative Measures
A retrospective analysis was conducted from January 1, 2014 through July 29, 2014 which
identified patients with prolonged QTc intervals of greater than or equal to 500 msec and their
associated interventions. Data obtained included:
QTc interval duration
Patient age and gender
QTc prolonging medications prescribed
Comments and interventions from the pharmacy
Prescriber response
The collected data was categorized based on the pharmacist’s documentation of the patient's drug
regimen and/or a call placed to the physician.
Methodologies
Pharmacist Calls - Outcome Options:
1. Physician accepted pharmacist's recommendation to discontinue medication.
2. Physician acknowledged recommendation but continued medication.
Pharmacist Calls Not Placed– Reasons were:
1. Patient with no identifiable medication associated with QTc prolongation.
2. Patient already discharged from the hospital.
3. Patient on chronic maintenance medication (e.g., amiodarone).
4. Medication with QTc prolonging potential already discontinued.
Improvement Results
Over the 7 month review 181 patients with prolonged QTc intervals were identified.
Calls placed to physicians (n = 97 patients) (Fig 1)
----------------------------------------------------------- The physician acknowledged the pharmacist’s and
discontinued the medication (n=27).
No calls placed to physician (n= 84 patients)
(Fig 2)
------------------------------------------------------- No identifiable medication associated with QTc
prolongation (n=70).
- The physician acknowledged the pharmacist’s
recommendations but chose to continue the
medication (n=70).
- Already discharged from the hospital (n=6).
On chronic maintenance medication such as
amiodarone (n=5).
- QTc medication discontinued prior to review
(n=3).
System Quality Review
336
NewYork-Presbyterian Healthcare System Quality Symposium 2014
Quality 2020: A Vision of the Future
Additional Results:
--------------------------Average QTc interval was 528 msec.
Gender: (111 males, 70 females).
The top five medications found to be most frequently associated with QTc prolongation were
ondansetron, amiodarone, azithromycin, quetiapine and levofloxacin. (Fig 3)
Sustainability Strategies
A novel protocol was developed to identify and intervene on inpatients with prolonged QTc at
risk of developing torsade de pointes. The ongoing protocol, representing a collaboration
between Cardiology and Pharmacy, alerts physicians via pharmacist intervention to the possible
dangers of specific QTc prolonging medications that have been ordered for their patients.
Lessons Learned
1) A protocol can be used to provide an additional layer of safety for patients with prolonged
QTc who may be receiving a QTc prolonging medication that puts them at risk for torsade de
pointes.
2) Initiation of an electronic pop-up alert in addition to a pharmacist's call serves to inform the
physician about the patient’s QTc interval and the potential for drug-related QTc prolongation.
(Fig 4)
3) The creation of this new protocol emphasizes the importance of collaboration between
departments to enhance patient safety.
Conclusion
To diminish the risk of torsade de pointes, a potentially fatal arrhythmia, a protocol was
developed through a collaboration between Pharmacy and Cardiology which provides a thorough
medication review in patients with prolonged QTc.
Over a 7 month period, the protocol identified 181 patients, representing 0.02% of all patients
having ECG's. Of these, 53% with prolonged QTc interval warranted a pharmacy call.
Evaluation of the impact of the protocol revealed that physician responses were variable,
including acceptance of the pharmacist’s recommendation by modifying therapy (28% ) or
rejection of the recommendation as a clinical decision (72%).
During the course of the protocol, an electronic pop-up alert called ‘QTc prolongation’ was
created to alert the physician of the combination of a prolonged QTc interval and a prescribed
drug that may induce QTc prolongation.
This novel protocol provides an additional layer of patient safety and serves as a model of
collaboration between cardiologists, pharmacists and primary care physicians.
System Quality Review
337
NewYork-Presbyterian Healthcare System Quality Symposium 2014
Quality 2020: A Vision of the Future
A Novel Protocol for Identification and Risk Reduction in Patients with Prolonged QTc Interval on
Electrocardiogram
Figure 1
Figure 2
System Quality Review
338
NewYork-Presbyterian Healthcare System Quality Symposium 2014
Quality 2020: A Vision of the Future
Figure 3
Figure 4: Pop-Up Alert
System Quality Review
339
NewYork-Presbyterian Healthcare System Quality Symposium 2014
Quality 2020: A Vision of the Future
Stamford Hospital
No More Misses: Implementing a Newborn Screening Reconciliation Process
Kathy LiVolsi, RNC, MHA, NE-BC; Donna Bowman, DNP, FNP-BC, RNC-OB; Theresa Rovegno, BSN, RN-C,
Karen Bell
Introduction
Background:
Newborn screening debuted as public health screening in the United States in the early 1960's.
The first disorder detected by newborn screening programs was phenylketonuria, a metabolic
condition in which the the inability to break down the essential amino acid phenylalanine can
cause irreversible brain damage unless detected early.
Newborn screening has expanded over the years to include many other disorders, though the
total number of disorders screened for varies from state to state. It is a public health program
designed to screen infants shortly after birth and prior to discharge from the hospital for an
extensive list of conditions that are not clinically apparent in the newborn period, but are
predominantly treatable. Every year, over four million newborns in the United States are screened
for genetic and metabolic conditions including cystic fibrosis, hearing loss, and in some states,
critical congenital cardiac defects. For babies who test positive for any of these conditions, rapid
identification and treatment can mean the difference between health and disability, and
sometimes death.
Problem:
After a poor patient outcome, our hospital determined that a newborn screening sample had
been performed on an infant, but had never reached the state lab. After consulting with both the
Department of Public Health and various hospitals in our state, it was apparent that the
expectations for reconciliation of metabolic newborn screening samples per DPH protocol was
not widely known and was not being followed.
Goal:
Our goal was simply to implement a newborn screening reconciliation program so that no infant
born in our institution was at risk for an adverse patient outcome as a result of our lack of
performance.
Quantitative/Qualitative Measures
Prior to our adverse patient outcome, we audited all newborn records prior to patient discharge
to verify that completion of newborn screening had been documented. We lacked a process that
thoroughly identified the steps from performing the screening prior to discharge, ensuring timely
System Quality Review
340
NewYork-Presbyterian Healthcare System Quality Symposium 2014
Quality 2020: A Vision of the Future
mailing to state lab, verifying a received result on every test performed, and timely physician
notification for any abnormal result.
Upon implementation of our newborn reconciliation process, we reviewed all our electronic
medical record for documentation improvement strategies. Our newborn data base was reviewed
and revamped to create necessary fields that captured pertinent information related to newborn
screening. These additional field included: the date the screening was performed, date test mailed
out, Fed-Ex tracking number, date specimen received at state lab, date result received, result of
test, and date of physician notification.
Methodologies
Using the PDCA methodology, a multidisciplinary team reviewed the state statues related to
newborn screening. A policy was developed and shared with all nursing and clerical staff,
physician and nursing leadership and risk management. Following implementation of the new
process, all newborn metabolic screenings were audited. However, our institution was committed
to ensuring that we did not miss any patient's mandated testing and we expanded our
reconciliation process to include cystic fibrosis screenings, newborn hearing screening,
transcutaneous bilirubin screening prior to discharge, and in 2013, we added critical congenital
cardiac screenings on all eligible newborns. Additionally, we created a document to send out with
each mailing that included a "packing list," where each completed test had a patient identification
sticker initialed by the RN performing the test. Once all tests had been adequately collected and
entered into the newborn data base, the charge RN and unit coordinator signed off on the
"packet", verifying that all samples included in the mailing matched the "packing list".
Improvement Results
While we initially lacked a process that verified reconciliation of each newborn screening, we
implemented a new process where we audited every newborn record for every newborn
screening performed. Our institution averages 2500 births annually with every baby receiving at
least five newborn screenings prior to discharge.
Upon implementation of our reconciliation process, each screening measure was added to our
Perinatal Quality and Safety Scorecard with the commitment to disseminate and be completely
transparent with data while being innovative in implementing a best practice to improve neonatal
outcomes.
In 2013, we achieved the following results:
-100 % of eligible infants had a reconciled metabolic and cystic fibrosis screening
-100 % of eligible infants had critical congenital cardiac screening performed
-97 % of eligible infants had hearing screening performed with adequate follow-up documented
-98 % of eligible infants had transcutaneous bilirubin screening performed prior to discharge
System Quality Review
341
NewYork-Presbyterian Healthcare System Quality Symposium 2014
Quality 2020: A Vision of the Future
Sustainability Strategies
Data collection and dissemination of information has been essential in maintaining awareness and
accountability of newborn screening reconciliation. Initially, we set the expectation that every
staff member would participate in every step of the process. We quickly realized that created
confusion, duplication, and lack of follow through. Every staff member was held accountable for
performing screenings, documenting screenings and educating parents. Clerical staff were
essential in accurately completing the newborn data base and every charge nurse was held
accountable for verifying the "packing list" with the unit coordinator.
Two staff members stepped up and volunteered to be responsible for auditing records and
analyzing our performance monthly. Scheduled time is built into their shift work to
accommodate this extensive task. Any recognized "miss" is corrected immediately if possible.
The newborn screening process is "owned" by us until we have a final result, even if the infant is
transferred or needs follow up testing with their physician in the community. Not having an
adverse outcome since the implementation of our new process is a sustainability strategy in and
of itself.
Lessons Learned
1. A robust, fail-safe reconciliation process requires adequate staff training and resources to
ensure follow through, and requires documentation for each step.
2. It was essential to partner with our state lab, forming relationships that promoted open
communication and dialogue so that obstacles could be eliminated and a smooth process could
ensue.
3. As devastating as our adverse event was, we could not change the outcome for that particular
baby and family. What we could do was commit to ensuring that every baby born from that point
on would benefit from our diligence and attention to detail as a result of our reconciliation
process.
Conclusion
In December of 2013, Connecticut and national media addressed the challenges with newborn
screenings, including a lack of a reconciliation process in many hospitals, delays in reaching state
labs, and adverse patient outcomes as a result of failed or missed screenings.
The Connecticut Department of Public Health provided data which detailed the average time it
took for them to receive screening specimens from Connecticut hospitals. Of 30 hospitals in the
state, we came in 3rd overall, with an average time of 2.3 days, slightly above the 48 hour
expected "receive" time according to state statute. Of hospitals that delivered over 1000
newborns annually, we were first. Upon dissemination of this information, hospitals questioned
the validity of the information, given that DPH is closed on weekends and holidays. Additionally,
mailings sent on Fridays that arrive on Saturdays are not credited until Mondays, prolonging the
"receive time" unnecessarily. Changes at the state level were made to collect Saturday deliveries.
At our institution, we added a Saturday Fed-Ex pick up to expedite those test results. We await
this year's results for timeliness of received specimens. However, we are confident in our
System Quality Review
342
NewYork-Presbyterian Healthcare System Quality Symposium 2014
Quality 2020: A Vision of the Future
program and our commitment to patient safety and expect an improvement in our performance
when that information becomes public.
Connecticut Hospitals with Late Samples
2012
% of late samples (=6 days)
40
35
30
25
Hospital
20
% of Late Samples
15
10
5
0
1 2 3 4 5 6 7 8 9 1011121314151617181920212223242526272829
CT Hospitals : SH in RED
System Quality Review
343
NewYork-Presbyterian Healthcare System Quality Symposium 2014
Quality 2020: A Vision of the Future
Poster Presentation
The SilverCrest Center for Nursing & Rehabilitation
Reducing Avoidable Hospitalizations in Long-Term “Chronic-Critically Ill”
Patients
Daniel Russo, CMD; Denise Lawson, RN; Loretta Mcmanus, RN; Karen Dikeman, MACCC-SLP
Introduction
The goal of the project was an overall 20% reduction in facility hospital transfer, hospitalization
and 30-day readmission rates, through the early identification, evaluation, management,
documentation and communication of changes in resident’s condition. The facility hospitalization
and 30-day re-admission rate is above benchmark in part because of the acuity of the population,
in particular 80 ventilator dependent and 40 tracheostomized patients. Hospitalization is taxing
on residents, costly to the facility, and involves extraordinary time, expenditure and work effort.
Specifically, the goals were:
1.
To decrease the facility hospitalization rate by 20%
2.
To reduce re-hospitalization within 30 days of admission/readmission.
3.
Reduce the hospitalization of ventilator-dependent and trachoesotomized residents.
Quantitative/Qualitative Measures
Metrics to be reported: total transfers, hospital admissions, 30-day re-admissions (facility)
ventilator admissions.
Methodologies
PDCA
Plan: Reducing avoidable hospitalization was identified as a quality of care and business priority
in the 2013 and 2014 QAPI Plan due to a high volume of transfers and admissions.
Do: The facility entered into collaborative efforts with CMS INTERACT and the NYPHS
Continuing Care Council aimed at reducing avoidable hospitalization. An interdisciplinary Project
Work Group chaired by the Medical Director was commissioned to identify opportunities for
improvement, implement tools and guidelines from collaborative, and make recommendations
based on findings.
Check/study: The PWG reviewed all transfers at the weekly meeting to determine if the transfer
was avoidable or not, and to identify trends, such as diagnosis, unit, day, time and transferring
physician.
Act: Continued implementation of revised processes, tools and clinical pathways for high-volume
areas. Increase collaboration with area partner hospitals.
System Quality Review
344
NewYork-Presbyterian Healthcare System Quality Symposium 2014
Quality 2020: A Vision of the Future
Improvement Results
Period 1/1/13 to 8/31/14
1.
34% reduction in total hospital admissions from 1/1/14 to 8/31/14 as compared to the
same period of 2013
2.
42.7% reduction in 30 day readmission
3.
41.9% reduction in ventilator patient hospital admissions
Period 1/1/14 to 6/30/14
1.
22.8% reduction in transfers in the second quarter
2.
24.1% decrease in hospitalization
3.
22.6% reduction in 30 day readmission
4.
27.5% reduction in ventilator patient hospital admissions
Sustainability Strategies
1. Monitor consistent identification, communication and treatment of symptoms utilizing project
tools via the facility daily 24-hour report. Staff not using project tools receive additional inservice.
2. Weekly case review of all hospital transfers by Project Work Group. The PWG determines if
the transfer was avoidable or not, identifies trends, and makes recommendations for
improvement when process vulnerabilities or failures are identified.
3. Communication of findings and recommendations of the PWG are presented at departmental
meetings and monthly to the PI Committee. Education is provided to staff upon changes
resulting from recommendations and on orientation.
Lessons Learned
1. Physician buy-in had the most significant impact. Increased physician to physician
communication helps prevent hospitalizations.
2. Empowering ancillary staff (including CNAs) is a key to success.
3. Improved, critical thinking by licensed personnel has facilitated the management of residents
in-house
4. The availability of palliative care services and residents/families acceptance of palliative care
has been the greatest challenge.
System Quality Review
345
NewYork-Presbyterian Healthcare System Quality Symposium 2014
Quality 2020: A Vision of the Future
Conclusion
Significant reduction in hospital transfers is achievable through interdisciplinary collaboration and
teamwork.Families and residents have gained confidence in the facility’s ability to treat more
clinically complex conditions on-site.
The facility has identified the need to improve palliative care services in order to prevent further
hospital transfers and support resident/family/staff in the care of these often chronically,
critically ill residents.
2013 vs 2014 Total Hospital Transfers
300
250
200
150
100
50
0
Q1
2013 Total Hospital Transfers
System Quality Review
Q2
2014 Total Hospital Transfers
346
NewYork-Presbyterian Healthcare System Quality Symposium 2014
Quality 2020: A Vision of the Future
2013 vs 2014 Hospital Admissions
180
160
140
120
100
80
60
40
20
0
2013 Hospital Admissions
2014 Hospital Admissions
Q1
Q2
2013 vs 2014 Hospital Admissions by
Thousand Patient Days
20
15
10
5
0
Q1
Q2
2013 Hospital Admissions /1000 Resident Days
2014 Hospital Admissions /1000 Resident Days
System Quality Review
347
NewYork-Presbyterian Healthcare System Quality Symposium 2014
Quality 2020: A Vision of the Future
2013 vs 2014 30-Day
Hospital Re-Admissions
100
80
60
40
20
0
Q1
2013 30 Day Hospital Re-Admissions
Q2
2014 30 Day Hospital Re-Admissions
2013 vs 2014 Vent Unit
90
80
70
60
50
40
30
20
10
0
Q1
Q2
2013 Vent Unit
System Quality Review
2014 Vent Unit
348
NewYork-Presbyterian Healthcare System Quality Symposium 2014
Quality 2020: A Vision of the Future
The Valley Hospital
An Innovative Approach to Decreasing Door to t-PA Times
Margaret Thornton RN, MSN, CEN
Introduction
The concept of the “Neuro ED RN” was created to decrease door to tPA times. On each shift,
one RN is responsible for caring for patients that present with acute onset of stroke symptoms.
These RNs were given specific training in our algorithm for stroke treatment, stroke recognition,
and utilizing a POC INR. The "Neuro ED RN" has drastically improved our treatment times for
Acute Ischemic Stroke. When evaluating the current stroke process, several areas for
improvement were identified. Our average door to treatment time in 2013 was 73 minutes, which
is above the recommended time frame for effective stroke centers. In 2014 we were dedicated to
implementing a process to improve our door to t-PA times.
Quantitative/Qualitative Measures
A review of the data indicated that door to CT scan times were delayed, result of INR times were
variable, and ED MD practices were not consistent. Our average door to CT times were 20.6
minutes and our average door to INR times were 34.9 minutes. Furthermore, some ED MDs
were comfortable assessing patients in the CT area and others requested that patients be brought
to rooms for assessment prior to initiating a stroke protocol. Our ED wanted to develop a
process that could be effectively and consistently applied to all patients presenting with Acute
Stroke Symptoms. The “Neuro ED RN” was created to achieve this goal.
Methodologies
This role was developed using the principles applied to trauma care at trauma centers. On each
shift, one RN is responsible for caring for patients that present with acute onset of stroke
symptoms. Thirty RNs were chosen and were given specific training focusing on the concept of
ensuring patients were moved quickly through the triage process. They were also given
specialized training in stroke recognition and the NIHSS. These RNs were also trained in utilizing
a Point of Care machine for INR testing. Finally, the initial assessment of stroke patients by the
ED MD was moved from the bedside to the CT scanner. This process addressed all three areas
we identified as needing improvement.
Improvement Results
The implementation has been successful for many reasons. The combination of selecting a core
group of outstanding RNs and providing them with specific training was pivotal. These RNs are
dedicated to the process and improving the care of stroke patients in our department. The ED
MDs were involved in the beginning phases to ensure that the MDs and RNs were unified in the
System Quality Review
349
NewYork-Presbyterian Healthcare System Quality Symposium 2014
Quality 2020: A Vision of the Future
approach. For every patient that is identified as having acute stroke symptoms, all ED MDs have
agreed to meet the patient near the CT scanner for initial evaluation. Simulation was utilized to
ensure competence prior to implementation. Our door to t-PA times have decreased to 46
minutes in 2014 and we are expecting that trend to continue. Specifically we have decreased our
door to CT times to 13.5 minutes for t-PA eligible patients. The INR results have decreased to 2
minute turnaround by implementing the point of care machine. We have also achieved our
“personal best” door to tPA time of 23 minutes.
Sustainability Strategies
The “Neuro ED RN” has given our stroke process consistency and reliability. It has improved
communication with ED MDs, the Neurologists, and the ancillary staff in our department. The
process for tPA patients has become seamless and efficient. The Neuro ED RN initial course will
be offered on a yearly basis to RNs who have been chosen by ED Leadership to become Neuro
ED RNs. This will ensure appropriate staffing with nursing turnover. All Neuro ED RNs are also
required to attend a quarterly educational session to ensure continuing education. If multiple
patients arrive with stroke symptoms at the same time, the Neuro ED RN will assume a
leadership role mentoring colleague RNs in the care of the patient to ensure multiple patients
receive the appropriate level of care. Also, if another Neuro ED trained RN is present in the
department, he or she can be pulled to assist the assigned Neuro ED RN to ensure appropriate
level of care. As an additional safety net, all the Charge RNs have been trained as Neuro ED
RNs. In a case where there is no other option, a Charge RN can assume the Neuro ED RN
position and call the Nurse Manager or House Supervisor to be in charge of the department.
Lessons Learned
1. The importance of involving stakeholders at onset. This was primarily a ED initiative. I think
we might have had an easier time with implementation if the Neurology group had been involved
from the beginning. We had to circle back to include them and it definitely could have been more
seamless with them involved.
2. We did a lot of education for the Neuro ED RNs but the education for the other RNs should
have been more formalized. We had role confusion and although the Neuro ED RN was the
team leader, the entire team needed to be educated to ensure a cohesive team for safe patient
care.
3. Creating early wins is the key to a great process. Our ED is invigorated by the process and the
RNs love to see the results and times. They are dedicated to providing excellent patient care for
our stroke patients.
Conclusion
The “Neuro ED RN” has given our stroke process consistency and reliability. It has improved
communication with ED MDs, the Neurologists, and the ancillary staff in our department. We
have been very successful in improving our IV t-PA rate, door to CT, and door to t-PA times.
System Quality Review
350
NewYork-Presbyterian Healthcare System Quality Symposium 2014
Quality 2020: A Vision of the Future
Winthrop-University Hospital
Improving Patient Safety by Educating Physicians on a New MRI Conditional
Pacemaker Device
Yuri Peterkin MD; Maria Khalid MD; Rakesh Shah MD; Orlando Ortiz MD
Introduction
MRI is increasingly becoming a routine part of patient care. The presence of a pacemaker was
once an absolute contraindication for an MRI. However, with advances in technology, MRI
conditional cardiac pacemakers are becoming increasingly more common, yet many physicians
are unaware. The Medtronic MRI conditional pacemaker is the first FDA approved pacemaker
that was designed, tested and approved for MRI use. Over 2,700 patients have been tested in
three prospective clinical trials resulting in no MRI related complications. This project was
designed to educate clinicians and radiologist about MRI conditional cardiac pacemakers and
their safe use in the MR environment.
Quantitative/Qualitative Measures
Educational material and surveys will be provided annually, via email, to all attendings, fellows,
and resident physicians at our institution to assess knowledge of MRI coniditional cardiac
pacemakers. Results can then be reviewed to demonstrate the efficacy of internet based
educational material. The radiology department will also recieve mandatory education on the
MRI conditional pacemaker device annually.
Methodologies
Utilizing internet based survey tool software, a 15-question survey assessing knowledge of MRI
conditional pacemakers and the safe performance of MRI studies on patients with MRI
conditional pacemakers was sent via the hospital email server to all attendings, fellows, residents,
and medical students at our institution. The survey included additional demographic questions
assessing the current position and specialty of the responder and the approximate number of
MRI studies ordered by the responder annually. Respondents were then provided with
educational materials consisting of a 10-slide Powerpoint presentation. They were also emailed
the answers to the survey, and asked to complete a follow up survey to assess the efficacy of the
survey as an educational tool. Additionally, all members of the radiology department also received
a mandatory survey which was completed after viewing the educational material in a Powerpoint
presentation via a departmental website, documenting that all attending and resident radiologists
in the department had been properly educated on this device.
System Quality Review
351
NewYork-Presbyterian Healthcare System Quality Symposium 2014
Quality 2020: A Vision of the Future
Improvement Results
A total of 35 respondents answered the survey with an average score of 10.4 out of 15. Based on
the level of training, differences in the knowledge base of respondents on MRI safety issues and
the MRI conditional pacemaker were assessed. A higher level of training was associated with only
a slightly better performance. Initial answers demonstrated significant misperceptions regarding
MRI safety issues at all levels of training regarding the safe use of MRI compatible pacemakers.
No correlation was found between the number of MRIs ordered and survey score. Follow up
survey results demonstrated this was an effective and well received method to improve MRI
safety and to provide MRI safety education to physicians. 87.5% of those who responded to the
follow-up survey found the survey to be a valuable learning tool that cleared previously held
misconceptions and agreed that the survey would impact their future decisions in regards to MRI
referrals. All radiology attendings and residents successfully accessed and utilized the educational
materials on the radiology department website and there was a 100% pass rate on the post test,
documenting that all physicians (24 atendings, 16 residents) in the department had been
successful educated on this new device utilizing web based educational and survey materials.
Sustainability Strategies
Sustainability strategies for educating clinicians and radiologist on the safe use of MRI conditional
cardiac pacemakers include instituting and educating clinicans on the departmental protocol for
ordering MRIs on patients with MRI conditional pacemakers. Annual mandatory surveys will be
completed by all attending and resident radiologist after viewing educational material provided on
the department website. An annual survey and powerpoint presentation will be emailed to all
attendings, fellows, residents, and medical students at our institution via the hospital email server.
Lessons Learned
1. Many clinicians are unaware of MRI conditional pacemakers, potentially denying patients of
diagnostic studies which may alter management.
2. Many radiologist are unaware of how to correctly identify an MRI conditional pacemaker on
chest radiographs.
3. Utilizing internet based educational materials and surveys effectively educated radiologist and
clinicians on the new MRI conditional pacemaker device at our institution.
Conclusion
MRI safety is critical not only for radiologists but also referring physicians who refer patients for
MRI studies. The newly approved MRI conditional pacemaker is an important advance which
will allow many patients to utilize previously contraindicated MRI examinations, however the
training and education of all physicians involved in the care of these patients is critical to the safe
use of this new technology. Our experience demonstrated the utilization and efficacy of internet
based educational materials to educate both radiologists and non radiologist physicians about
MRI safety issues, whose understanding is critical to the safe use of this new pacemaker device.
System Quality Review
352
NewYork-Presbyterian Healthcare System Quality Symposium 2014
Quality 2020: A Vision of the Future
Poster Presentation
Winthrop-University Hospital
A Quality Improvement Initiative to Improve Rates of Normothermia in the
Delivery Room Using a Checklist
Alexandra Vinci, MD; Bianca Fornier Karber, MD; Shahidul Islam, MPH; Nazeeh Hanna, MD; Amrita Nayak, MD
Introduction
Background: Newborns are born to a world that can be as cold as a 20 degree F difference from
their previous environment. Preterm babies considered very low birth weight (VLBW) are at
increased risk of hypothermia from deficiencies of brown fat and immature nervous systems. The
delivery room environment plays an important role in the development of hypothermia in VLBW
babies. Hypothermia (core body temperature of <36 C) can result in unwanted outcomes such as
hypoglycemia and neurological impairment. Each 1degree C decrease in body temperature is
associated with a 75% increase in mortality.
Aim: Our aim was to reduce hypothermia in VLBW infants born at Winthrop Hospital by 25%
in 2012 and 2013 using a simplified checklist. We intended to further prove its effect by
temporarily discontinuing its use in 2014 to determine if it had any lasting influences on practice.
Quantitative/Qualitative Measures
Using the checklist significantly reduced the hypothermia from 2011 to 2013. When the checklist
was discontinued the rate of hypothermia increased.
Methodologies
Methods: A delivery room checklist was created to reduce the incidence of hypothermia among
VLBW infants (<32 weeks gestation) admitted to the NICU. Retrospective chart reviews
assessed the project's success at one and two years later. Further analysis was done to examine
the separate effects of birth weight and gestational age on the incidence of hypothermia. Use of
the checklist was temporarily stopped in 2014. The incidence of hypothermia was again measured
retrospectively and compared to previous years. Cochrane-Armitage test was used to evaluate
trend over the years and the Chi-Square test was used to compare proportion of hypothermia.
SAS 9.3 was used for all calculations.
Improvement Results
Results: Among all VLBW infants <32 weeks, 53% had admission temperatures <36 C in 2011
prior to the intervention compared to 29% in 2012 after the checklist was instituted. Data from
2013 shows a plateau in the rate of hypothermia to 31%. There was a significant decrease in the
overall incidence of hypothermia from 2011 to 2013 (p=0.007). However, when the checklist was
stopped in 2014, the incidence of hypothermia increased to 39%. This is not significantly
System Quality Review
353
NewYork-Presbyterian Healthcare System Quality Symposium 2014
Quality 2020: A Vision of the Future
different compared to the pre-intervention period in 2011 (p-value=0.198). In regards to the
effects of birth weight and gestational age, a higher incidence of hypothermia in 2011, 2013, and
2014 occurred for babies born earlier (<28 weeks) and smaller (<1 kg). Surprisingly in 2012 (the
first year of intervention), there was no correlation between incidence of hypothermia and birth
weight or gestational age.
Sustainability Strategies
This project was sustainable until 2013. When the rates of hypothermia started to increase in
2014, the checklist was reinstated and re-education was provided to staff.
Lessons Learned
1) Checklists are effective and useful tools for initiating and sustaining quality improvement
measures.
2) Hypothermia can be prevented by outlining all necessary actions in a simple checklist format.
3) Re-education is important to make sure the checklist is being followed.
Conclusion
Simple measures put in place to prevent hypothermia, such as a checklist, are effective if well
executed and complied with. Non-enforcement of the checklist resulted in a decrease of
normothermia for VLBW babies, further supporting its utility. Periodic re-education of
practitioners should be employed to maintain success.
System Quality Review
354
NewYork-Presbyterian Healthcare System Quality Symposium 2014
Quality 2020: A Vision of the Future
hypothermia by year
60%
53%
50%
39%
40%
29%
30%
31%
pct_hypothermia
20%
10%
0%
1
2
3
Year
Variable
2011
2012
Temperature <36˚C, %
53%
29%
Temperature <36˚C, %
53%
29%
*p-values are from Cochran-Armitage trend test
System Quality Review
4
2013
31%
31%
2014 p-value
0.007
39% 0.198
355
NewYork-Presbyterian Healthcare System Quality Symposium 2014
Quality 2020: A Vision of the Future
Winthrop-University Hospital
Our Journey to Improving our Patient Safety Culture
Joseph Greco, MD Chairman of Anesthesia and Patient Safety Officer; Stacey Pfeffer, Senior Vice President Human Resources
and Organizational Development; Monica Santoro, MS, BSN, RN, CPHQ, Vice President and Chief Quality Officer
Introduction
A culture of safety is characterized by values, attitudes and behaviors that demonstrate a
commitment to safety; encourages and supports reporting of any situation that may threaten the
safety of patients, caregivers, or visitors; and views errors, near misses and identified risks as
opportunities for learning and improvement (2010. National Quality Forum, p.70). Medical errors
and adverse outcomes increase when the perceived risk of being blamed for mistakes is high
(2010. National Quality Forum, pp.87-88).
Perceptions of our staff related to patient safety using the Agency for Healthcare Research and
Quality (AHRQ) Hospital Survey on Patient Safety Culture administered in the fall of 2012
indicated opportunities for improvement in all domains; particularly perceptions related the nonpunitive response to error. We recognized the importance of creating a learning environment
where staff are comfortable reporting near misses/adverse events; and that we were missing
opportunities to identify risks in our care processes, learn, and improve due to our staff attitudes
and perceptions.
Our aim was to promote patient safety by improving our processes for learning from mistakes as
evidenced by an improvement in our composite scores on the AHRQ Culture of Safety Survey to
the New York State Partnership for Patients (NYSPFP) 50th percentile for the “non-punitive
response to error” and the “feedback and communication about error” domains by September
2013 when the survey would be repeated.
Under the leadership of an executive level Steering Committee we developed a comprehensive
plan to improve staff perceptions related to our response to error. The plan involved hospital
wide immersion which included adopting measurable components of a safety culture in the
corporate goals, increasing the frequency of Executive Leadership Patient Safety Rounds,
engaging medical staff, and formulation of a performance improvement (PI) team that included
front line staff. Tactics included training, from the Board of Trustees to the front line staff;
consistent use of the Just Culture Algorithm™ (Outcome Engenuity); adoption of our “Just
Culture Statement of Principles”; and improved feedback on incidents/near misses to share
lessons learned and demonstrate our emphasis on the process not the people.
Our Just Culture Statement of Principles includes four pillars: creating a learning culture; creating
a fair and open culture; designing safe systems; and managing behavioral choices. Staff and
System Quality Review
356
NewYork-Presbyterian Healthcare System Quality Symposium 2014
Quality 2020: A Vision of the Future
management training is centered on these pillars and case-based learning is used to reinforce the
concepts.
1- National Quality Forum (NQF). Safe Practices for Better Healthcare—2010 update: A
Consensus Report. Washington DC: NQF; 2010.
2- Outcome Engenuity, LLC.
Quantitative/Qualitative Measures
The Agency for Healthcare Research and Quality (AHRQ) Hospital Survey on Patient Safety
Culture was administered to the hospital staff in 2012 and 2013 to evaluate performance related
to staff perceptions. The survey has been tested for validity and reliability and has been
completed in over 1100 hospitals across the nation by over 567,000 respondents (AHRQ). The
survey was administered through the New York State Partnership for Patients. The survey was
administered online with champions assigned to each discipline to support participation. Staff
surveyed included: Nurses, PA/NP’s, Attending Physicians who spend the majority of their work
hours at the Hospital, Residents, Fellows, Clerical Support Associates, Nursing Assistants,
Respiratory therapists, Physical Therapists, Pharmacists, Technologists, Transporters, Dieticians,
Managers and Administrators.
AHRQ Hospital Survey on Patient Safety Culture: 2012 User Comparative Database Report.
Retrieved from:
http://www.ahrq.gov/professionals/quality-patientsafety/patientsafetyculture/hospital/2012/index.html
Methodologies
The Model for Improvement was used with repeated plan, do, study, and act cycles. Through
ongoing tests of change we recognized the need to modify our original plan which included
management, leadership, medical staff and trustee training. For example, following the manager
training we identified challenges in use of the Just Culture Algorithm™. Based on this several
leaders participated in advanced training to become certified. We also convened a Culture and
Leadership PI team that included front line staff. That team identified that though we had trained
the managers and leaders, most front line staff were not familiar with the principles of a just
culture. This lead to a house-wide education program for the entire staff on the pillars of our just
culture and its relationship to safety. The team also identified the need to improve our feedback
on incident reporting so the staff would recognize the use of incident/near miss reporting for
learning and improvement. Finally, a key component of use of the Just Culture Algorithm™ is
coaching staff who engage in at risk behaviors. Based on feedback that there was variation among
the managers in their ability to coach staff we provided training for managers in coaching.
Improvement Results
The AHRQ Survey was administered hospital wide in 2012 and 2013 with a 63% and 47%
response rate respectively. We exceeded our aim to meet the NYSPFP 50th percentile in the
AHRQ survey domain related to feedback and communication about error, improving 9
percentage points from 2012 to 2013 (61% to 70%; p-value < .0001), and exceeding the NYSPFP
mean of 66%. Staff perceptions also improved significantly on the non-punitive response to error
System Quality Review
357
NewYork-Presbyterian Healthcare System Quality Symposium 2014
Quality 2020: A Vision of the Future
domain improving 8 percentage points from 32% to 40% (p-value <.0001). This fell just short of
our aim to reach to the NYSPFP 50th percentile, which was 41%. The AHRQ National average
for domains that improve is 4-5 percentage points (AHRQ).
In addition, improved staff perceptions was demonstrated in all survey domains, with statistically
significant improvement in eleven out of twelve domains. Staff perceptions met or exceeded the
NYSPFP and 2013 National means in ten out of the twelve survey domains.
Details on the pre and post composite performance results on overall hospital safety
measurements and work area/unit measurements, as well as specific survey questions on the
target domains, are displayed in Exhibits 1 and 2 attached.
AHRQ Hospital Survey on Patient Safety Culture: 2012 User Comparative Database Report,
Table 7-3, Retrieved from:
http://www.ahrq.gov/professionals/quality-patientsafety/patientsafetyculture/hospital/2012/hosp12tab7-3.html
Sustainability Strategies
In order to sustain and continuously improve our performance the following strategies were
implemented and are ongoing: training is included in new employee orientation and new manager
orientation; trained Champions and Certified Trainers meet monthly to review a case to reinforce
principles and support continued improvement in use of the Algorithm™; managers are required
to participate annually in an update on use of the Algorithm™ that includes a case study;
promotion of our just culture is included in performance appraisals for all employees as part of
our core value standards, and for managers under leadership competencies; human resources was
engaged from the start and requires use of the Algorithm™ by managers when reviewing all cases
referred to employee relations; all serious events are reported to organizational leadership and the
governing body using the Just Culture Algorithm™ lexicon; we continue to conduct Executive
Patient Safety Rounds weekly and continue to publish our Patient Safety Talking Points to
Improve Patient Safety (TIPS) and our "Did you know..." Newsletter on a regular basis to share
lessons learned and demonstrate our use of medical errors, incident reports and good catches for
learning and improvement with an emphasis on systems and processes.
Lessons Learned
1. The value of complete immersion of the entire organization to achieve success in a PI priority.
2. Engaging leadership and front line staff in planning and execution including development of a
communication plan.
3. Ongoing development of leaders and managers in use of the Just Culture Algorithm™ and in
skills for coaching staff.
Conclusion
While Winthrop had previously implemented the principles of a just culture, our staff perceived a
punitive environment. Through organizational immersion in the principles of a just culture and
use of PDSA we had significant improvement in our staff perceptions. Working with a team of
front line staff we learned that training of managers was not sufficient but that the front line staff
System Quality Review
358
NewYork-Presbyterian Healthcare System Quality Symposium 2014
Quality 2020: A Vision of the Future
needed to understand the principles, the imperative from a patient safety standpoint, as well as
our commitment. As with other leadership initiatives, we also needed to demonstrate execution
of these principles in our day-to-day activities.
We are encouraged by the improvement. Going forward we plan to measure the impact on
incident and near miss reporting as well as on overall errors and patient harm. Our aim was to
promote patient safety by improving our processes for learning from mistakes by improving staff
perceptions related to our response to error. Next steps will seek to evaluate if the improved
perceptions is correlated with organizational learning and collective mindfulness, both features of
a high reliability organization, as evidenced by a decrease in patient harm.
System Quality Review
359
NewYork-Presbyterian Healthcare System Quality Symposium 2014
Quality 2020: A Vision of the Future
Winthrop University Hospital
AHRQ Culture of Safety Survey Results
2012 Response Rate = 63%
2013 Response Rate = 47%
Exhibit 1
System Quality Review
360
NewYork-Presbyterian Healthcare System Quality Symposium 2014
Quality 2020: A Vision of the Future
Exhibit 2
System Quality Review
361
NewYork-Presbyterian Healthcare System Quality Symposium 2014
Quality 2020: A Vision of the Future
Winthrop-University Hospital - Pulmonary & Critical Care Medicine
A Quality Improvement Study to Decrease COPD Related Readmission and
Average Length of Stay through the implementation of a COPD Transitions of
Care Program
Grace Trimmer RN MSN; Cyril Cheriyan MD; Zubair Ali MD; Joyce Pang MD; Girish B. Nair MD; Sam Kirell
RHIA; Marie Bernstein RT; Jon Ilowite MD; Steve Salzman MD; Michael Niederman MD
Introduction
Chronic Obstructive Pulmonary Disease (COPD) is the third leading cause of death in the
United States and patients with COPD utilize significant healthcare resources with an estimated
cost of 50 billion dollars annually. Centers of Medicare and Medicaid Services (CMS) has
proposed penalties on hospitals for readmissions with certain diagnoses, and in 2015 plans to
expand it to patients admitted with COPD exacerbation. Winthrop University Hospital (WUH)
implemented a multidisciplinary approach in an effort to decrease the rate of hospital length of
stay for patients with COPD exacerbations and prevent re-admissions.
Quantitative/Qualitative Measures
We analyzed pre and post intervention average length of stay (ALOS) and number of readmissions.
Methodologies
In a prospective quality improvement study, all patients admitted to WUH with COPD
exacerbation from January 2010 to May 2014 were included. A COPD Transitions of Care
Program (CTC) was initiated on January 2013 to develop an orderly transition from the hospital
to a safe discharge. CTC included educational initiatives for medical personnel, formation of a
specially-designed sub-acute rehabilitation transition program and development of a standardized
order set. A dedicated Pulmonary Nurse Specialist/ Transition Care Coordinator supervised the
program and education sessions. We analyzed pre and post intervention average length of stay
(ALOS) and number of re-admissions.
Improvement Results
A total of 1627 COPD admission cases were reviewed for a period of 52 months from January
2010 to May 2014. From 2010 to 2012, ALOS for COPD patients with exacerbations for WUH
was 6.60 days whereas ALOS was 5.83 days for other hospitals in the Long Island Health
Network (LIHN). Post-intervention ALOS was 5.53 days for WUH compared to 5.67 days for
LIHN in 2013 [Figure 1,2]. The readmission rate was 16.2% (n=180/1111) for WUH preintervention and 14.3% (n=74/516) post-intervention [Figure 3]. The post-intervention readmission rate was compared to the New York Presbyterian Healthcare system readmission rate
System Quality Review
362
NewYork-Presbyterian Healthcare System Quality Symposium 2014
Quality 2020: A Vision of the Future
of 18.5% in a 2013 Member Performance Report. Of the hospitals in the NYP system, Winthrop
had the second lowest readmission rate for COPD in 2013 (13.7%).
Sustainability Strategies
To sustain this quality improvement project, attendings, nurses and case managers collaborated
together in quarterly meetings. A hospital wide, multidisciplinary “Readmission Reduction Initiative
Committee” was formed. The group meets monthly to review all preventable readmissions and the
Pulmonary Nurse Speciailist coordinates care through hospitalization to subacute rehabilitation.
Lessons Learned
1. Through the implementation of a COPD Transitions of Care Program it is possible to reduce
the average length of stay (ALOS) and hospital re-admission rates in patients with COPD
exacerbation
2. By providing educational initiatives for medical personnel, developing a standardized order set
and sustaining communication between all parties involved in the care of patients with COPD,
WUH had decreased readmission rate and ALOS for COPD patients.
3. A Pulmonary Nurse Specialist/ Transition Care Coordinator was responsible for patient
follow-up and education, as well communicating with hospital staff and thus played an important
role to help to reduce COPD related readmission and ALOS.
Conclusion
In a single center quality improvement study, implementation of a COPD transition program
helped reduce readmission rates and ALOS. This study highlights the importance of collaborative
intervention aimed at education, early mobilization and physical rehabilitation.
References
1. Institute for Clinical Systems Improvement. Diagnosis and Management of Chronic
Obstructive Pulmonary Disease (COPD). 8th Edition. March 2011.
2. Centers for Medicare and Medicaid Services: Readmissions Reduction Program.
http://www.cms.gov/Medicare/Medicare-Fee-for-ServicePayment/AcuteInpatientPPS/Readmissions-Reduction-Program.html
3. Centers for Disease Control and Prevention (CDC). Chronic obstructive pulmonary disease
among adults--United States, 2011. MMWR Morb Mortal Wkly Rep 2012; 61:938.
4. American Thoracic Society / European Respiratory Society Task Force. Standards for the
Diagnosis and Management of Patients with COPD [Internet]. Version 1.2. New York:
American Thoracic Society; 2004 [updated 2005 September 8].
System Quality Review
363
NewYork-Presbyterian Healthcare System Quality Symposium 2014
Quality 2020: A Vision of the Future
Figure 1.
Days
Average Length of Stay For Patients
with COPD Exacerbations
8
7
6
5
4
3
2
1
0
Winthrop Univesity
Hospital
LIHN
2010
2011
2012
2013
Year
Figure 2.
Average Length of Stay For Patients
with COPD Exacerbations
7
6.5
6
Days
5.5
Winthrop University
Hospital
5
LIHN
4.5
4
3.5
3
Pre-Intervention
System Quality Review
Post-Intervention
364
NewYork-Presbyterian Healthcare System Quality Symposium 2014
Quality 2020: A Vision of the Future
Figure 3.
Re-Admission Rates for Patients with COPD at
Winthrop University Hospital
20.00%
Re-admission Percentage
19.00%
18.00%
17.00%
16.20%
16.00%
15.00%
14.34%
14.00%
Winthrop University Hospital
13.00%
12.00%
11.00%
10.00%
Pre-Intervention (2010- Post-Intervention (20132012)
2014)
System Quality Review
365




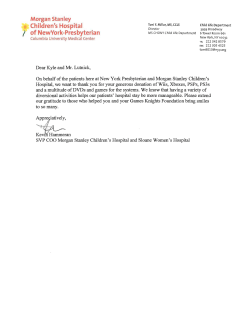





© Copyright 2026