
The child’s social worker is directly responsible for delivery of... many of the services outlined in this section are provided... SECTION 6 SERVICES TO CHILDREN IN CARE
SECTION 6 SERVICES TO CHILDREN IN CARE 6.1 Social Worker Contact with the Child The child’s social worker is directly responsible for delivery of services to the child. While many of the services outlined in this section are provided by others under the direction of the social worker, the social worker must provide direct social work service to both the child and the child’s caregivers. The social worker must maintain regular direct contact with each child in care for whom they are responsible. Such contact should be purposeful and consistent with the comprehensive plan of care. Where the child is of an age and developmental ability to understand, such contact will be in private with the child and present the opportunity for the child’s input. The amount of contact the social worker has with the child will vary depending upon the child’s age, length of time the child has been in care, the circumstances under which the child was placed, the child’s adjustment to care, special needs, and placement stability. However, minimum standards are set to make sure that contact is maintained as part of ongoing casework services. Standard 6.1(a) The child’s social worker must have face to face contact with the child in their placement within the first 7 days of placement. The social worker must make have contact, either phone or face to face, every 30 days with the child. The social worker must have face to face contact with the child at a minimum of every 90 days for children and youth in care of the agency. This contact must occur in the child’s placement and may continue in the community. All contact with the child, attempted or completed must be recorded and documented on the case management system. • Section 6 Frequent contact should be maintained during the child’s initial placement period and regular contact thereafter. Services to Children in Care • Contact should take place both in the placement setting and outside of it. This will let the social worker observe the child in the placement setting and let the child have private meetings with the social worker to discuss any concerns they may have concerning the placement. • Those children living in less stable placements, during periods of crisis, or after a re placement will require more frequent contact. • Older adolescents living in independent living situations will also require more frequent contact to make sure their goals for independence are being met. Standard 6.1 (b) Children and adolescents in care must have access to a telephone and a contact number for their social worker or how to reach another worker or the supervisor in an emergency Purpose of Meeting with the Child Frequent contact during the first part of placement is necessary to assess the child’s initial adjustment to care, to help the child understand the reasons for coming into care, and to begin the process of developing the child’s comprehensive plan of care. Ongoing contact is essential in the development of a trusting relationship with the child, making sure the child’s comprehensive plan of care is being followed, and making sure that the child is making progress in the following areas: • • • • • • • 6.2 health education identity family and social relationships social presentation emotional and behavioural development self care skills Social Worker Contact with Caregivers Section 6 Services to Children in Care Standard 6.2 Social workers responsible for a child in care must have regular and meaningful contact with the child’s care providers, this includes foster parents and/or residential providers. The child’s social worker must have face to face contact with the care provider in the placement within the first seven days of placement. The social worker must make have contact with the care provider, either by phone or face to face, every 30 days. The social worker must have face to face contact with the care provider at a minimum of every 90 days while children are placed in their care. This contact must occur in the child’s placement. All contact with the care giver, attempted or completed documented on the case management system. 6.2.1 must be recorded and Frequency of Contact The initial period of placement requires frequent contact. It is also essential that regular contact with caregivers be maintained throughout the child’s time in care and is part of the social worker’s responsibility in supervising the placement. This includes personal contact with foster parents, group home staff, and residential staff that is separate from contact with the child. 6.2.2 The Purpose of Maintaining Contact with Caregivers The success of a placement depends in large part on the casework support that is provided to the foster family. Continuous and ongoing contact between the social worker and the foster family is essential in maintaining and supporting the foster family in addition to providing continuity to the child. For youth living in a group home or residential facility, contact, as outlined in Standard 6.2, is maintained to make sure lines of communication are clear and that comprehensive plans of care are developed with input from the significant people in the child’s life. The purpose of maintaining contact with caregivers is to: • Section 6 assess the initial adjustment period Services to Children in Care • develop plans to address the developmental dimensions for the child and identify who will be responsible to make sure action plans are carries out to meet these needs • provide information and seek input into the development of the child’s comprehensive plan of care • determine what supportive services are required • provide information to caregivers on the status of the family situation, comprehensive plan of care, and court update • provide additional background information on the child as it becomes available • review access arrangements, noting the caretakers’ observations of the child’s reactions prior to and following visits • make sure that the child’s religious, linguistic, racial, and cultural heritage is being recognized • make sure that caregivers are following through with medical and dental appointments, maintaining life books, and any and all of their responsibilities as outlined in the child’s comprehensive plan of care 6.2.3 Contact with Significant Others The child’s social worker should also establish contacts with people who are significant in the child’s life and whose input would be beneficial in the development of the comprehensive plan of care. Such people include birth parents, grandparents, siblings, or other extended family members as well as friends, teachers, and any other people important in the child’s life. Standard 6.2.3 (a) Children over 12 must be consulted on whom they consider significant and who they would like contacted (see Section 2.19: Access Services). 6.3 Transportation of Children in Care 6.3.1 Section 6 Transportation by Social Worker Services to Children in Care Standard 6.3(a) When a social worker or other agency staff is transporting a child in care, the social worker or agency staff must make sure that the children are properly restrained, either by seatbelt or by child restraint system, as appropriate. 6.3.2 Transportation by Taxicab According to the Nova Scotia Safety Council and the Nova Scotia Registry of Motor Vehicles, seatbelt use by passengers (or child restraint systems, as appropriate) in taxicabs is required by the Motor Vehicle Act. Taxicab drivers, however, are exempt from both wearing seatbelts and for making sure that their passengers use them. Standard 6.3(b) A child in care must not be transported by taxicab unless they are properly secured by either a child restraint system or a seatbelt, as appropriate, and as prescribed by the Motor Vehicle Act. Procedures When the social worker deems that a child is of sufficient maturity to travel alone by taxicab, the social worker should make sure that the child is aware of the necessity to wear a seatbelt. The operator of the cab should also be advised of this expectation. It is recommended that agencies develop their own agreements with taxicab companies that their drivers will make sure that children in care are properly secured when travelling by taxicab. It is also suggested that, when possible, children sit in the middle position in the back seat of the taxicab, as they are less vulnerable to side impact in this position. 6.4 Maintenance of Children in Care Agencies must provide for children in their care as would any wise and conscientious parent. This includes meeting the child’s needs for food, clothing and shelter but also the opportunity to participate in activities that nurture their talents and skills to help them to grow up to be healthy, well rounded adults. This may include the opportunity to participate in recreational activities such as sports, creative outlets such as painting or music or group activities such as Brownies or Scouts. Planning for children in care includes an assessment of the financial capacity of the parent to contribute toward the cost of their child’s maintenance, as set out in the Children and Family Services Act and Regulations. In almost all cases, the assessment will be completed by the family’s protection social worker, following the procedures outlined in Section 4 of the Child Protective Services - Policy Manual. However, there may be circumstances where this assessment falls to the child in care social worker if, for example, the original Section Section 6 Services to Children in Care 17 or Section 18 Agreement signed by the parents may need to be revised. In any situation where the child in care social worker is required to review the financial capacity of the parents’ ability to contribute toward maintenance, the Child Maintenance Guidelines in the Regulations of the Maintenance and Custody Act will be applied. The Guidelines are a well recognized, standardized tool, specifically developed to determine appropriate levels of parental support for their children. The Child Maintenance Guidelines can be found on the internet at the following website: http://www.gov.ns.ca/just/regulations/regs/fmcmg.htm. The Federal Child Support Guidelines which are referred to can be found at the following website: http://canada.justice.gc.ca/en/ps/sup/grl/glp.html Standard 6.4(a) Parents have an obligation to contribute financially to the care of their children. Agencies are required to review the financial capacity of all parents who enter into a Section 17 or Section 18 Agreement regarding their ability to contribute toward maintenance of their children in care, using the Child Maintenance Guidelines. Agencies or district offices provide board and clothing allowance to foster parents and restricted homes for the children in their care, or for the youth who are living in approved independent living situations along with covering other expenditures necessary to meet the needs of children and youth in care. Funding for parent counsellor homes, small option homes, group homes, and residential facilities is provided to meet the needs of the children in their care. The agency or district office that is responsible for the child is required to approve expenditures based on the rates and funding standards set by the Department of Community Services (see Policy Statement 94 and Policy Statement 75 in reference material for Section 6). 6.4.1 Section 6 Food Services to Children in Care Standard 6.4.1(a) A child in care must be provided with sufficient nourishing food to meet their individual needs for growth, development, and activity. A child’s individual needs for growth, development, and activity must take the following into account: • • general nutritional requirements of children the special nutritional requirements of the particular child, including any requirements or limitations diagnosed or prescribed by a health care provider the child’s views, including the child’s specific likes and dislikes the child’s culture and diet customs, if applicable any special requirements of the child relating to the manner in which food is served or prepared, if the child is young or has special needs • • • 6.4.2 Clothing Standard 6.4.2(a) A child in care must be provided with clothes that are of comparable style, quality, and condition as those of other children in their community. The agency should assess the child’s clothing needs when: • • • • the child enters care the child’s comprehensive plan of care is reviewed a request to do so is made by the child or caregivers the child leaves care. The agency should discuss the child’s clothing needs with the following, as appropriate: • • • 6.5 the child caregivers parents of the child Medical Care A child in care has the right to receive medical care when required to ensure their health, safety, and well-being. Section 6 Services to Children in Care Standard 6.5(a) A medical must be completed within 30 days of a child entering care and annually thereafter while in care. (See Appendix Section 3 for forms) Standard 6.5(b) A medical booklet must be provided and maintained for every child in care which must include the child’s health card number. Procedures The child’s social worker: • ascertains the medical status of the child when they come into care • arranges for accurate records to be kept of the child’s medical care, and for these records to be kept current; a child in care may consult a number of health care providers during the time they are in care and accurate records are necessary to determine appropriate health treatments and to provide an accurate medical history to the child when they reach adulthood (Policy Statement #64) • provides a medical booklet for each child in care including the child’s health card number • arranges for a child in care to receive medical care as required • makes sure the child’s medical records are treated as confidential and that the contents are not disclosed except to the extent necessary to ensure the child’s safety and well being and to protect others • assists the child and the child’s family in assuming responsibility for the child’s health when the child leaves care It may be necessary for a child to visit a doctor more than once a year to meet their medical needs. Any costs associated with a medical exam or routine prescriptions should be covered by the agency under the maintenance budget. Extraordinary medical expenses must be approved in advance by the executive director or district manager. In some cases, older youth in care may refuse to go for a medical. The social worker should discuss with the youth the importance of a medical; however, if they continue to refuse and there is no apparent risk to the health, safety, or well-being of the youth, the reasons for the refusal and a summary of the situation should be recorded. Section 6 Services to Children in Care The medical booklet should be updated by caregivers and maintained in safekeeping for the child. Where the child is living independently, the booklet should be kept by the youth or if they wish, held in safekeeping in their file. Refer to the Guidelines for Medical Treatment and Services, Section 10 of the Foster Care Manual for further clarification (see appendix for this section). 6.5.1 Dental Care Standard 6.5.1(a) A child in care must receive dental care as required to maintain their oral health, safety, and well-being. A dental checkup must be completed within 90 days of a child entering care and annually thereafter while in care. Procedures The child’s social worker: • ascertains the dental health status of children when they come into care • arranges for accurate, current records to be kept of the child’s dental care • arranges for the child to receive the dental care required If there is a dental problem, the child should be able to visit a dentist immediately. Any costs associated with a routine dental checkup should be covered by the agency under the maintenance budget. Extraordinary dental expenses such as orthodontic work must be approved in advance by the executive director or district manager. The Nova Scotia Children’s Oral Health Program provides coverage for routine dental care for children up to 10. 6.5.2 Consents to Treatment Parents may retain certain rights of guardianship including the right to consent to and arrange health care for the child under a temporary care Section 17 agreement or by court order. Where the child is in care by Section 17 agreement, Section 6 of the agreement addresses whether the parent retains the responsibility to consent to treatment or the parent consents to the agency assuming responsibility. Under Subsection 44(2) of the Act: Where an order for temporary care and custody is made, the court may impose as a term or condition of the order that the parent or guardian shall retain any right that the parent or guardian may have to give or refuse consent to medical treatment for the child. Section 6 Services to Children in Care In all other cases where the child is in temporary care or in care and custody by court order, the agency or district office has the right to consent to health care for the child including: • • • • routine medical and dental care recommended routine health care or treatment low-risk elective or emergency surgery unusual or extraordinary medical procedures or treatment (see sample Medical Consent form in the appendix for Section 7) The agency or district office may authorize caregivers to consent to medical or dental care. Consent is provided by completing the Letter of Medical Designation, Authority to Consent for Medical Treatment, Authorization for the Sharing of Medical Information about Children in Care (see Appendix for this section). Refer to the Guidelines for Medical Treatment and Services, Section 10 of the Foster Care Manual (also included in Appendix for this section) for further clarification. Standard 6.5.2(a) Where the child has the capacity to consent, the child’s consent to treatment must be obtained. 6.5.3 Health Care Planning In developing the health care component of a child’s comprehensive plan of care, the child’s social worker consults with the child, the child’s parent, and caregivers, as appropriate, and determines: • • • • the child’s current health status the child’s current and future health care needs how those needs will be met the specific responsibilities of the child’s parents, caregivers, the social worker, and, if appropriate, the child in meeting these needs The following factors should be considered: • • • • • • • Section 6 the age of the child the child’s views the child’s capacity the continuity and stability of the child’s relationships with health care providers attitudes of the child and the child’s family to health care the resources available to the agency to meet the child’s health care needs involvement by caregivers or the child’s parents, taking into account whether or not Services to Children in Care the parents continue to assume the rights and responsibilities for consent to health care 6.5.4 Medical and Dental Coverage Standard 6.5.4(a) A valid Nova Scotia health care number must be documented for each child in care on the case management system and made available to those persons responsible for overseeing the medical care of the child. Under the Nova Scotia Children’s Oral Health Program, children under 10 are provided routine dental care coverage.(Policy Statement #64) 6.5.5 Aboriginal Children Health Care Benefits Where the child is registered as having Indian Status, the costs for medical care should be covered by Indian and Northern Affairs Canada. Standard 6.5.5(a) Where the status of the child is not determined, the social worker must apply to Indian and Northern Affairs Canada to determine if the child is eligible for Indian status. For a child with Indian status, the social worker must clarify with Indian and Northern Affairs Canada which health care benefits the child may be entitled to receive. 6.5.6 Hospitalization of Children in Care When admitting a child in care to hospital, a family and health history, religion of the child, and guardian's name must be given to the admitting officer. Caregivers should request that their names be placed on the visible part of the chart rather than the agency's so as not to stigmatize the child. The responsibility for signing medical consents for medical treatment, X-rays or emergency surgery for the child rests with the executive director or district manager or social worker, or caregivers if delegated this authority by the district manager or executive director or social worker. Where the child is in temporary care, the consent of the parent is required (see Appendix 7). The executive director or district manager or social worker may authorize caregivers to Section 6 Services to Children in Care consent to medical care. Consent is provided by completing the Letter of Medical Designation, Authority to Consent for Medical Treatment, Authorization for the Sharing of Medical Information about Children in Care (see Appendix for this section). The responsibility for signing medical consents for planned surgery rests with the executive director or district manager or social worker delegated this authority by the agency or district office. When a child is admitted and discharged from hospital, it is necessary to complete an entry on the child movement screen. Foster parents or child caring facilities are eligible to receive board payments while the child is in hospital. While in hospital, the caregivers are expected to visit the child and provide the necessary ongoing care and support of the child. Spending money may continue to be sent to the caregiver while the child is in hospital. 6.6 Maintenance Expenditures for Children in Care In addition to the routine daily living requirements while in care, the child may have additional special needs related to their physical or emotional well-being. The comprehensive plan of care for the child should address the special needs of the child, how and by whom these needs will be met, and time lines. Department-approved rates for “Maintenance Expenditures for Children in Care” under Policy Statement 94 should be followed (see the appendix for this section). In addition to board*, clothing, and routine medical and dental care, the maintenance expenditures for a child in care include: • • • • • • • • • • • • • • • Section 6 prescriptions transportation camps, club memberships child care and/or babysitting* diapers and/or formula* driver’s education, driver’s license/insurance equipment, furniture and replacement of bedding* glasses and/or contact lenses hair care independent living medical equipment non-prescription items orthodontics school activities and items telephone calls Services to Children in Care • • • • • post-secondary education vacation costs school supplies spending allowances for children special occasion costs *foster care only 6.6.1 Service Agreements Service agreements are required where services are being provided by an independent service provider. These services may include but are not limited to: • • • • transportation tutoring counselling child care These agreements, including the service plan, should be completed in all cases where Policy Statement 75 applies (see the appendix for this section). 6.7 Sexual Health Sexuality is an integral part of the personality of everyone: man, woman and child. It is a basic need and aspect of being human that cannot be separated from other aspects of life. (World Health Organization 1994) Sexuality includes an individual's gender, sexual orientation, body image and self-esteem, feelings, values and beliefs, attitudes about touch and affection, decision-making, relationships, and sexual behaviour. All people are sexual beings and learning about sexuality is a life-long process. Sexual health involves the life-enhancing aspects of sexuality (e.g. the capacity to love) and the absence of negative outcomes (e.g. diseases, shame, or unplanned pregnancy). The foundation for sexual health begins in early childhood and learning opportunities and support for sexual health can occur throughout the life span. Learning about sexuality issues is an important part of a child's overall well-being and healthy development. Comprehensive sexuality education can help protect children and youth from peer pressure, sexual abuse and exploitation, unhealthy relationships, unplanned pregnancy, sexually transmitted infections, and shame and guilt (which act as obstacles to sexually healthy behaviours). Youth who have been exposed to comprehensive sexuality education are more likely to postpone sexual involvement and practise sexually healthy behaviours when they become sexually active. Section 6 Services to Children in Care Sexual health is an integral aspect of children's well-being and healthy development and all children and youth have a right to comprehensive sexuality education. In addition, youth have a right to access sexual health services and to choose among options that will help them make responsible informed decisions about their sexual health. The agency will strive to foster an environment that supports sexuality education and responsible sexual decisionmaking by youth. Standard 6.7(a) The child’s social worker must make sure that children and youth in care receive ongoing, age-appropriate education about sexuality issues. In addition to healthy sexual development the risks associated with and prevention of sexually transmitted diseases must be reviewed. The date and summary of the discussions must be noted in the record. The social worker should: • provide children and youth in care with support, counselling, and other resources regarding sexuality issues • make sure that children and youth in care have access to inclusive sexual health services that are responsive to the diversity of the children and youth, regardless of their gender, age, sexual orientation, race, ethnicity, or ability • promote awareness of the importance of regular sexually transmitted infection testing for sexually active youth and annual pap smears for sexually active young women • respect the right to confidentiality of the youth with regards to sexual health services 6.7.1 Sexuality Education The goals of (sexuality education) are to help people achieve positive outcomes (e.g. self-esteem, respect for self and others...rewarding human relationships...) and to avoid negative outcomes (e.g. unwanted pregnancy, sexually transmitted disease, sexual coercion). (Canadian Guidelines for Sexual Health Education 1994) Canadian Guidelines for Sexual Health Education provides the framework for the provision of sexuality education to children and youth in care. Following these guidelines, ongoing sexuality education for children and youth in care will include developmentally appropriate information and resources, opportunities for skills development (e.g. communication, decision-making, media literacy, values clarification, critical thinking) and the promotion of positive self-esteem and other motivations for sexually healthy practices. Information for youth in care will include both the positive and negative components of sexual health outlined in the guidelines. Section 6 Services to Children in Care Caseworkers, foster parents, and/or residential staff should work collaboratively to provide sexuality education for children and youth in care. Members of this adult team must communicate that they are available and approachable if children and youth in care have any questions about sexuality and relationship issues. However, the adult team members should initiate discussion and learning rather than waiting until children and youth in care ask questions, as they may not ask out of fear or shame. There are many opportunities for the provision of sexuality education. Adults can use naturally occurring events as teachable moments. For example, a pregnant pet in a foster home is an opportunity to talk to young children about pregnancy and birth. With adolescents, adults could initiate a discussion by inquiring about what sexual health information they have received at school. In addition, caseworkers and residential staff might set up information sessions about sexual health topics for youth in care. There are also a number of books available on a variety of sexuality issues written for children and youth of all ages. Effective sexuality education is ongoing and comprehensive and the opportunities for its provision are likewise extensive. The child’s social worker needs to develop a basic comfort level with sexuality issues so that they are able to communicate in a positive, non-judgmental, and sensitive manner, affirming the importance of sexual health. Social workers, foster parents, and residential staff should be sensitized to the importance of sexuality education for children and youth in care. Social workers may be supported in their role as a sexuality education resource for children and youth in care through access to sexuality information, training opportunities, and the sharing of resources. 6.7.2 Access to Sexual Health Services Effective sexual health education...(goes) hand-in-hand with access to clinical services, counselling, and social services...and the physical resources that are required to support individual efforts to enhance sexual health and avoid sexual problems. (Canadian Guidelines for Sexual Health Education 1994) Procedures Sexual and reproductive health services are part of primary health care. The child’s social worker should endeavour to make sure that the child or youth in care have access to inclusive sexual health services. The social worker can facilitate access by keeping up to date on community resources for the purposes of referral, developing a working relationship with sexual health agencies, sharing sexual health resources with youth in care, and perhaps arranging transportation to appointments for sexual health services. The social worker should promote awareness of the importance of regular sexually transmitted infection testing for sexually active youth and annual pap smears for sexually active young women. The social worker can discuss this issue with the youth in care and encourage the youth to talk to their health care provider. This encourages the youth to assume responsibility for their sexual health and fosters independence. In addition, the Section 6 Services to Children in Care social worker may consult with the physician to make sure that these issues are raised by the health care provider during annual checkups. It is imperative that the social worker, foster parents, and residential staff respect the right to confidentiality of youth with regards to sexual health services. Medical records pertaining to the provision of sexual health services should not be accessed without the youth's consent. A violation of confidentiality, whether perceived or actual, may cause youth to conceal their sexual activity and/or to avoid accessing sexual health information and services, thereby placing them at risk of unhealthy outcomes. Results of sexually transmitted infection testing do not need to be included in case files. From a public health perspective, it is not necessary for residential facilities or foster homes to be informed of positive test results. As long as these facilities are following basic universal precautions, there is no risk of transmission of sexually transmitted infections from household contact. A local public health department can provide information on universal precautions. 6.7.3 Gay and Lesbian Youth Legislation In Canada there is legal protection from discrimination because of sexual orientation for gay, lesbian, and bisexual people in the majority of provinces, including Nova Scotia. It is important to make sure that gay, lesbian, and bisexual youth enjoy the same human rights as the rest of society. Even though this protection is mandated by our human rights legislation, prejudice and discrimination still exist. For information, contact the provincial Human Rights Commission or the Federal Human Rights Commission (see Resource Material for this section). It is the social worker’s responsibility to provide information, support counselling, and other resources to youth in care regarding sexuality and family planning. Youth require accurate information regarding sexual development and this is best provided by a caring parent or caregivers. In the case of children and youth in care, it is necessary for the caseworker, foster parents, or residential staff to decide who should provide this information. In the case of gay or lesbian youth, it is the social worker’s responsibility to help caregivers explore their own values and beliefs about sexuality and make sure that accurate information and proper confidential support services are available. It is the responsibility of the social worker to provide support for the youth who have questions about their own sexuality. Information is available on activities, outreach Section 6 Services to Children in Care programs, workshops, and referrals. These programs are available for youth in both urban and rural areas. 6.8 Assessment and Therapy Legislation The Act provides for children in care to have access to “child care services,” which means assessment, counselling, and referral services as stipulated under Clauses 3(1)(g)and (i) of the Act. The agency is responsible to assess and counsel the child in care the best they are able given the resources that are available to them. To assist a child in care with their future, an agency must have an understanding (as clear as possible) of the child’s past. Therefore, the agency must attempt to understand the interaction of family members: the relationships between adults, relationship between the adults and the child or children, and the patterns of parenting that have occurred in the past. The goal is to develop an understanding of the child that will result in a comprehensive report describing the psychological, biological, and social history of the child. 6.8.1 Contracting Services Policy Statement #75 Standard 6.8.1(a) Policy Statement #75 must be applied when contracting services for a child in care. A complete copy of this policy (and the contract) must be reviewed by the social worker before entering into any service agreement (see the appendix for this section). The following is a brief summary: Standard 6.8.1 (b) When directed by the courts to complete psychological, psychiatric, or other assessments, or where the child welfare agency requires an assessment/treatment of a child, and the agency is unable to provide the assessment and/or treatment, the agency must utilize existing mental health or other publically funded services when possible and appropriate. • When such services are not available, and the agency’s social workers are unable to provide the service, or when a special assessment or counselling service is required, an agency may use an approved practitioner. Any such service is subject to the availability of funds. Section 6 Services to Children in Care • There is an approved list of private practitioners that is made available to agency offices on a quarterly basis. • Any use of a private practitioner must be approved by a casework supervisor, agency executive director, district manager, or special needs committee. • A contract or agreement must be signed between the practitioner and agency that outlines the maximum number of hours and must specify what services are being offered. • There is a set rate for assessments and counselling. 6.8.2 Psychological Assessment and Testing It is important to distinguish between these two terms. Assessment is a set of statements about an individual and his/her circumstances in relation to some problem. Assessment, as a process, is the bringing together of relevant information from a variety of sources, that is the systematic collection, organization and interpretation of information about a person (child) and his/her situation. Assessments are never undertaken in isolation, they are investigated to solve a clinical problem which predetermines the form and goals of assessment.(Berger 1985) A psychological test is a device and/or a set of procedures for measuring psychological phenomena. The term ‘psychological test’ is usually associated with a narrow range of procedures to measure IQ, personality, educational attainments, or to diagnose ‘brain damage,’ ‘thought disorder,’ or deficits in language or perception. It is, however, more appropriate to regard a test as any systematic procedure for obtaining information about psychological functioning and describing it with the aid of a numerical scale or category system.(Berger 1985) Professionals: Psychiatry is a speciality of medicine concerned with the treatment of mental illness and emotional problems. There are many sub-specialties, e.g. child psychiatry. The social worker should consider using a psychiatrist if seeking a diagnosis of a possible mental disorder, or if there is an indication of an emotional condition that may require psychiatric attention. If the child has already been diagnosed as suffering a mental disorder, a psychiatrist will be able to comment on the probable outcomes of various treatment methods, as well as the implications that mental disorders and their treatment have for the lives of the youth as well as others involved. Section 6 Services to Children in Care Psychology is the study of mental processes, normal and abnormal. Many sub-specialties exist, e.g. developmental psychology. The social worker should consider using a psychologist if there is concern about the child’s intellectual level, if there is need for information by various recognized tests concerning developmental normalcy and learning functions, or if there is a need to compare personality structure and coping skills to norms in a measured way through projecture tests and personality tests. Couselling: Mental health professionals, e.g. psychiatrists, psychologists, social workers, nurses, all practise counselling at varying levels of expertise. Those who are licensed and trained in one or more of a variety of schools of thought in psychotherapy recognize the course of treatment is generally several years long. There are many others who claim expertise in counselling and are not licensed. There is no legal requirement to be licensed as a therapist or counsellor. Treatments include individual psychotherapy that assumes the need to gain insight into intra-psychic processes. Other forms of counselling include behavioural techniques which are based on learning principles, therapies that focus on the re-orientation of conscious thought processes, interventions designed to alter patterns of family interaction, methods that seek to improve a person’s skills to cope with social problems, and approaches that aim to influence the broader social environment. Psychotherapy is not generally appropriate for children in care. 6.8.3 Referral Criteria Being successfully involved in counselling requires certain prerequisites as outlined below: • The child has demonstrated an ability to form and sustain at least one meaningful relationship (must be capable of forging a relationship with a therapist). • The child has shown some ability to internalize psychological tension within themselves, rather than having to discharge it immediately via poorly controlled and outwardly directed behavioural explosions, technically referred to as ‘acting out.’ • The child must not only have serious psychological problems, but must recognize at least some of these as problems within themselves, rather than attributing them all to an unsympathetic family or environmental situation (motivation to change). • As a corollary to the above, a reasonable candidate for counselling should be able to reflect upon the part they play in perpetuating their unsatisfactory relationships (ability to reflect on personal contributions to the problems). Section 6 Services to Children in Care • The final and least negotiable criteria to be met before referring a child in care for counselling concerns the stability of that child’s environment. (Steinhauer 1991) In general, children in care are poor candidates for psychotherapy (Steinhauer 1991). The average child in care is more likely to benefit from and find a relationship within the child welfare system, e.g. specialized families, agency social worker, residential centre. 6.9 Education Legislation Education Act 5(2) Subject to this Act and the regulations and notwithstanding the Age of Majority Act, every person over the age of five years and under the age of twenty-one years has the right to attend a school serving the school district or school region in which he/she resides, as assigned by the school board. Standard 6.9(a) A child in care is entitled to have access to education. In compliance with the Education Act, a child in care over 5 and under 21 must be enrolled in public school in their local community unless: • the child is 5 and it is in the child’s best interests that enrolment be deferred for one year • the child is involved in an alternate education program offered or approved by the Department of Education • the child is over 16 and refuses to attend any school or any alternate education offered or approved by the Department of Education Procedures 6.9.1 Enrolment A child in care should be enrolled in school as soon as possible after placement in the local school district. Previous school records should be transferred accordingly and any steps necessary be put in place to make sure there is a smooth transition between schools. Section 6 Services to Children in Care 6.9.2 Additional Services Within the School Children in care with special needs have the entitlement under the Special Education Policy to additional services within the school. The costs of these services are the responsibility of the education authorities. (See Appendix 6) 6.9.3 Meetings: Parent/Teacher Consultations The social worker or the child’s caregivers should attend meetings with the educational authorities. Where the child’s caregivers attends these meetings, the child’s social worker should be kept informed of what transpired at the meeting as part of the case planning process. 6.9.4 Additional Services Outside of School The child should be encouraged and assisted in their education including establishment of regular study habits. Funding is provided by the agencies under Policy Statement 94 for the purchase of school supplies. If the services of a tutor after school are needed, compliance with Policy Statement 75 is required (see the appendix for this section 6). 6.9.5 Enrolment in Private School In exceptional circumstances, the executive director or district manager may approve a child in care to attend a private school if the following circumstances exist: • the public school system is unable to offer a suitable education program to the child and the Department of Education has approved funding, and • the child’s physical and emotional needs could best be met in the private school, and • the child’s level of development will likely be enhanced by the child’s attendance at the private school, and • attendance at the private school would provide continuity of education for the child 6.9.6 Post-Secondary Education - Educational Bursary Program Standard 6.9.6(a) Educational goals must be developed as part of the Comprehensive Plan of Care. Section 6 Services to Children in Care Where youth are in the care and custody of the agency, their care and custody may be extended to 21 if they are pursuing their education (see the appendix for Section 8). All children and youth in care should be encouraged to continue their education. Preparation for post-secondary education should begin several years in advance of the youth’s anticipated graduation from high school. Efforts directed towards supporting and preparing the youth for post-secondary education, including advising the youth in care about the Educational Bursary Program, should be documented in the youth’s Comprehensive Plan of Care. Under the Educational Bursary Program for Youth in Care, youth in permanent care and custody will receive funds to cover the actual costs of tuition, books and related expenses, in addition to regular maintenance. The following conditions apply: • the youth must be in permanent care and custody • the youth in care must be enrolled in a program offered at an accredited educational institution (university, community college or private vocational training) that is designated by or registered with the Canada Student Loan Program or registered as a Trade School under the Private Career Colleges Act (see www.ednet.ns.ca for complete listing) • the youth in care will attend an education institution within the Atlantic Provinces unless the program they wish to pursue is not available within the Atlantic Provinces • the youth in care must attend the program of study on a full-time basis and carry a full course load for the year • the youth must successfully complete a minimum of 80% of the courses per year. An exception can be made with the approval of the Regional Administrator. The request for an exception shall be forwarded in writing from the Executive Director/District Manager to the Regional Administrator. • the youth in care must provide an annual transcript to the youth’s social worker • the youth in care must contribute $500 towards the cost of the first year of post-secondary expenses and contribute $1000 in each year thereafter. These funds may be obtained through summer employment, part-time employment or loans. A reduction of the $1000 contribution may be approved by the Executive Director/District Manager, if the post secondary program extends beyond eight months each year. • the youth in care must apply for any available scholarships and bursaries, including the Ken Dryden Scholarships • this program will provide funding to support the completion of only one degree at university, one community college program or one private vocational program. • post-secondary programs whose tuition fees are greater than the most expensive Nova Scotia university tuition fees will require the approval of the Regional Administrator. The request shall be forwarded in writing from the Executive Director/District Manager to the Regional Administrator. • funds can be made available until the youth’s 21st birthday Section 6 Services to Children in Care Procedures Youth who are planning to attend a post-secondary educational institution should make their plans known to their social worker. The social worker will provide support and assistance to the youth as they complete application requirements and apply for available scholarships and bursaries. Once the youth receives confirmation of acceptance at a post-secondary institution, the youth and social worker will determine the costs of tuition, books and related expenses. The total funds provided will be reduced by the value of any scholarships or bursaries the youth is able to obtain and the $500 contribution from the youth. Prior to the beginning of each subsequent school year, the youth and social worker will determine the costs of tuition, books and related expenses for the upcoming year. The total funds provided will be reduced by the value of any scholarships or bursaries the youth is able to obtain and the $1000 contribution from the youth. The anticipated budget for each school year should be determined and recorded by the social worker, as completely as possible, in advance of any expenditures. For each year of the program, the agency/district office will pay tuition and other fees directly to the post-secondary institution. The youth will be provided with the funds to cover the costs of books, supplies and related expenses for each term or session and will be expected to provide receipts to the social worker. The social worker will be available to assist with these purchases. Maintenance payments and expenses covered under Policy 94 will continue to be paid by the agency/district office. A youth in care who is unsuccessful in completing the first year of any post-secondary program may, under exceptional circumstances, be considered for another program. The youth will be required to write a letter to their Executive Director/District Manager, outlining the reasons for not completing the first program, the reasons why the youth believes that he or she will be successful in the second program and requesting permission to obtain funds from the Education Bursary Program. The Executive Director/District Manager will forward the request to the Regional Administrator with respect to the release of funds for a second program. 6.9.6.1 Extension to the Educational Bursary Program The Extension to the Educational Bursary Program is intended to assist former youth in care who have begun post-secondary studies to continue their studies up to their 24th birthday. It is anticipated that the Extension will make it possible for these former youth in care to complete their post-secondary studies. With the approval of the Regional Administrator, former youth in care who had not begun post-secondary studies prior to exiting care and who wish to pursue their studies will also be eligible for this program. Section 6 Services to Children in Care The following conditions apply: • the youth must have been in permanent care and custody and be between the ages of 19 and 24 years • the youth must be enrolled in a program offered at an accredited educational institution (university, community college or private vocational training) that is designated by or registered with the Canada Student Loan Program or is registered as a Trade School by the Private Career Colleges Act (see www.pcc.ednet.ns.ca for complete listing) • the youth must attend an education institution within the Atlantic Provinces unless the program they wish to pursue is not available within the Atlantic Provinces • the youth must attend the program of study on a full-time basis and carry a full course load for the year • the youth must successfully complete a minimum of 80% of the courses per year. An exception can be made with the approval of the Regional Administrator. The request for an exception shall be forwarded in writing from the Executive Director/District Manager to the Regional Administrator. • the youth must provide an annual transcript to the youth’s social worker • the youth must contribute $1000 annually. These funds may be obtained through summer employment, part-time employment or loans. A reduction of the $1000 contribution may be approved by the Regional Administrator if the post-secondary program extends beyond eight months each year • the youth must apply for any available scholarships and bursaries, including the Ken Dryden Scholarships • this program will provide funding to support only one degree at university, one community college program or one private vocational program. • post-secondary programs whose tuition fees are greater than the most expensive Nova Scotia university tuition fees will require the approval of the Regional Administrator. The request shall be forwarded in writing from the Executive Director/District Manager to the Regional Administrator. • funds may be made available until the youth’s 24th birthday • in the event a young person’s 24th birthday falls during the course of the academic year, funding will be extended to allow the youth to complete the academic year • the youth must sign a Post Care and Custody Agreement (see Appendix for Section 6) which will outline the terms and conditions of the financial assistance Procedures Prior to their 21st birthday, youth in care who have attended post-secondary education must notify their social worker of their intention to continue their education. The youth will sign a Post Care and Custody Agreement (see Appendix for Section 6), indicating that he/she understands and accepts the terms of the Agreement. The Agreement will be signed by the youth’s social worker and the Executive Director/District Manager with the approval of the Regional Administrator, and must be renewed annually. Youth who were formerly in care and who received funds through the Educational Section 6 Services to Children in Care Bursary Program but who reached their 21st birthday prior to the introduction of the Extension to the Educational Bursary Program are eligible for funds under the Extension. They must apply in writing to the Executive Director/District Manager of the agency/district office that had been responsible for their care. The youth will sign a Post Care and Custody Agreement, indicating that he/she understands and accepts the terms of the Agreement. The Agreement will be signed by the youth’s former social worker (or another social worker assigned to provided support under the Extension) and the Executive Director/District Manager with the approval of the Regional Administrator and must be reviewed annually. Youth who were formerly in care but exited care prior to their 21st birthday must apply in writing to the Executive Director/District Manager of the agency/district office that had been responsible for their care, outlining their wish to pursue post-secondary education. If the Executive Director/District Manger agrees, the request will be forwarded to the Regional Administrator for approval. If approved, the youth will sign a Post Care and Custody Agreement, indicating that he/she understands and accepts the terms of the Agreement. The Agreement will be signed by the youth’s former social worker (or another social worker assigned to provide support under the Extension) and the Executive Director/District Manager with the approval of the Regional Administrator, and must be renewed annually. Prior to the beginning of each school year, the youth and social worker will determine the costs of tuition, books and related expenses for the upcoming year. The total funds provided will be reduced by the value of any scholarships or bursaries the youth is able to obtain and a $1000 contribution from the youth. The anticipated budget for each school year should be determined and recorded by the social worker, as completely as possible, in advance of any expenditures. For each year of the program, up to the youth’s 24th birthday, so long as the terms of the Post Care and Custody Agreement are met, the agency/district office will pay tuition and other fees directly to the post-secondary institution. The youth will be provided with the funds to cover the costs of books, supplies and related expenses for each term or session and will be expected to provide receipts to the social worker. The social worker will be available to assist with these purchases. Maintenance payments and expenses will continue to be paid by the agency/district office. The standards with respect to Children in Care do not apply to youth formerly in care but the social worker will provide supportive services to the youth, as required. All documentation concerning the Post Care and Custody Agreement is to filed in the Children In Care file. 6.9.7 Education: Aboriginal Children To determine source of funding for an aboriginal child’s education, the agency should Section 6 Services to Children in Care contact the individual band or First Nation for educational services. Eligibility for educational services is as follows: • jurisdiction at band levels • preschool, elementary, and secondary services are provided to members and non members who are residing in First Nation communities (on reserves) • post-secondary educational services or programs are provided to registered band members who may reside in and away from First Nation communities (on and off reserves) • agency must contact individual bands for advice on funding for educational services 6.9.8 Residential Child-caring Facilities Standard 3.3.2 of the Provincial Standards for Residential Child-caring Facilities should be applied. 6.10 Employment Any youth who is over 16 may apply for employment. Procedures A youth over 16 who wishes to apply for employment should do so in consultation with the caseworker and caregiver in the context of the youth’s comprehensive plan of care. Contributions to the youth’s maintenance from earnings should be determined in consultation with the youth, social worker, and caregivers. The social worker is responsible for making sure that the youth has the proper documentation, such as a birth certificate and social insurance number. For information on services and programs available under the Employment Support Services program, contact the Department of Community Services, Employment Support Services. 6.11 Inheritance and/or Insurance Settlements Section 6 Services to Children in Care Standard 6.11(a) Where a child is in the care and custody of an agency or district office by court order and the child is entitled to money from an estate or insurance settlement, and no guardian has been appointed in regard to that money, the agency or district office must consult with the office of the public trustee. Procedures If a child in care is entitled to money under the Public Trustee Act and there is no trustee for that sum of money established, either in the terms of the will or in the terms of the insurance settlement or other document which bestows the money upon the child, then any person can apply to the court under the Guardianship Act to become the guardian of the estate of the child. If the guardianship order is granted, the individual who is appointed by the order is entrusted with the child’s money and has the obligations of a trustee as prescribed under the Trustee Act and Guardianship Act. 6.12 Canada Pension Plan Benefits Standard 6.12(a) Where a child in care is entitled to Canada Pension Plan benefits, the agency or district office must take the necessary steps to make sure an application is made for those benefits and the benefits be used to contribute to the costs of maintaining the child. A child may be eligible for pension benefits if either of their parents are disabled or deceased and the contribution requirements have been met. Procedures The agency or district office should contact the nearest Human Resources Development Canada (HRDC) office to advise them that the child is in the care and custody of the agency or district office. HRDC will forward the appropriate application form for completion and take action to suspend payment to the previous payee. The Canada Pension Plan benefits for a child in care upon receipt should be placed in the maintenance budget to offset the costs of maintaining the child (see Policy Statement 62 in the appendix for this section). Section 6 Services to Children in Care SECTION 6 APPENDIX 1. Guidelines for Medical Treatment and Services 2. Letter of Medical Designation, Authority to Consent for Medical Treatment, Authorization for the Sharing of Medical Information about Children in Care 3. Policy Statement #62 Surpluses in the Children’s Services Agencies’ Operating Accounts 4. Policy Statement #64 i. Authority to sign Medical Consents for a Child Placed on Adoption Probation by a Child Placement Agency ii. Notification of Hospitals of Adoption Placement iii. Notification of MSI of order of Care & Custody or Adoption Placement 5. Policy Statement #75 A. Policy Statement regarding the process for contracting with private practitioners to provide private assessments or counselling for matters under the Children & Family Services Act; and B. Provision of other Contracted Services 6. Policy Statement #94 Maintenance Expenditures for Children in Care 7. Special Education Policy: Go to www.ednet.ns.ca/pdfdocs/studentsvcs/specialed/speceng.pdf 8. Post Care and Custody Agreement Section 6 Services to Children in Care - Appendix Department of Community Services GUIDELINES FOR MEDICAL TREATMENT AND SERVICES FOSTER CARE SERVICES POLICY DATE: March 2007 Children and Youth receive a variety of medical and mental health services as a result of their individual needs and as documented in the Child’s Comprehensive Plan of Care or within the Case Plan prepared for the courts. Within each type of care status, the legal responsibilities for guardianship and legal care may vary, and subsequently within the Health Care system, the roles and responsibilities for information sharing and medical consent with the Department of Community Services and/or the local Child Welfare agency may also vary depending upon the level of treatment, the type of medical service ,or consultation required for the child or youth in care. To enhance the process of information sharing and the determination of the level of medical consent required, the following Guidelines for Medical Treatment and Services have been developed for use with the IWK, and any other hospitals or medical services throughout the province. Medical Records Booklet The Medical Records Booklet is required for all Children and Youth in Care. • The Medical Records Booklet is provided through the Department of Community Services to assist social workers, foster parents, residential facilities and children and youth to track and manage medical services and needs. • The Medical Records Booklet is to accompany the child/youth to all medical appointments to ensure that the information regarding the medical services received are documented and maintained as part of the child/youth’s personal record. • All care providers responsible for ensuring that the child/youth receives medical services and treatment will be provided with the Medical Records Booklet • Responsibilities for maintaining the Medical Services Booklet and the subsequent Section 6 Page -29- Services to Children in Care - Appendix responsibilities for medical services is documented in the Child’s Comprehensive Plan of Care or the Case plan. Attendance for Medical Treatment and Services • Children should never attend clinics or any type of treatment facility without the support of the social worker or a designated care giver. (Child care worker, foster parent, or family member.) • Children require the support of their foster parent, their social worker, child care worker, or a family member when attending medical visits. The access facilitator, access driver, nor any other type of facilitator, do not have the authority to provide information, to receive information, nor to consent to medical services. Letter of Medical Designation and Care Giver Identification • A duly signed Letter of Medical Designation from the Child Welfare Agency/District Office will also accompany the Medical Records Booklet clearly stating the designation of authority to either receive and/or disclose information about the child/youth in care and where necessary to consent to a specific level of medical care. • All care givers from Residential and Foster Care Services, all relatives caring for children and youth on behalf of the Department of Community Services and/or local Child Welfare Agency are to be provided with the Letter Of Medical Designation from the social worker responsible for the child/youth in care (see form letter of medical designation). • All care givers are required to provide picture identification to the IWK and all other medical facilities and/or services when accompanying a child/youth for medical services . A driver’s license or work identification is preferred. • All care givers are also required to present the Letter of Medical Designation for the child or youth in care. Types of Child/Youth in Care Status as Defined in the Children and Family Services Act, 1991 The medical designation or the responsibilities of the care giver may vary depending upon the legal status of the child or youth in care. The following types of legal status may require varying degrees of designation. Children and Youth Taken Into Care - Section 33 Section 6 Page -30- Services to Children in Care - Appendix • During the initial stages of the Child Protection Investigation when children are being taken into care and the status of the child is before the courts, the children and youth are the full responsibility of the Department of Community Services or local Child Welfare agency. The social worker has the responsibility to advise the IWK, and any other hospitals or medical services of the status of the child or youth and the authority in which they are requesting services. • In circumstances where treatment is required, the Health Care system have consent procedures in place that are determined by the level of treatment required. • It is the responsibility of the Child Welfare Social Worker to advise whether there are safety or information sharing concerns that hospital personnel may be required to discuss with the Child Welfare Social Worker as the Child Protection Investigation proceeds and document it accordingly. Children and Youth In Care through Agreement (CRV7, CRV8) - Section 17 and Section 18 • Children and Youth in Care by Agreement through Section 17 and 18 of the Children and Family Services Act have entered into care through the parents and/or youths consent and agreement. Parties to the Agreement do address the issue of medical care and services as part of the Agreement documentation. Parental rights regarding medical treatment usually continue to rest with the parents. In some cases the parent may be unable to continue to maintain their parental rights and may wish to transfer medical responsibilities to the local Child Welfare Agency/District Office. • In all cases the Temporary Care Agreement has a specific section dealing with Medical Services and Consent. This section is to be photocopied and attached to the designation document for the IWK and any other hospitals or medical services as part of the notification of the designation process and documentation. Child and Youth in Care through Adoption Agreement (CRV6) - Section 68 • Children in Care through a Section 68 of the Children and Family Services Act have entered care as a result of the birth mother and/or birth parents actively developing an adoption plan for the child. Within the Section 68 Agreement, the responsibility and p a r e n ta l a u th o r i t y f o r m e d ic a l s e r v ic e s re s ts s o le ly w ith t h e Child Welfare Agency/District Office. However, once the Notice of Proposed Adoption has been signed the local Child Welfare Agency/District Office is required to designate legal control to the adopting parents. Section 6 Page -31- Services to Children in Care - Appendix Children in Temporary Care and Custody - Section 42 and 44 • Children and Youth in Care through a Temporary Care and Custody Order have been ordered into care through the court and full authority for parental responsibilities and consent usually rests solely with the local Child Welfare Agency/District Office, unless otherwise stated within the Temporary Care Order. • However, in many cases, the birth family may be actively involved with the child/youth in care and the local Child Welfare Agency and/or District Office and is working towards a plan for the child’s return home to parental care. • In these instances IWK, and any other hospitals or medical services require notification within the Designation document from the local Child Welfare Agency/District Office of the medical responsibilities of the birth family and care giver as stated within the Case Plan or the child/youth’s Comprehensive Plan of Care to determine where their responsibilities for information sharing is required. Children and Youth in Permanent Care and Custody - Section 42 (f) and 47 • Children and Youth in Care and Custody have been ordered into care by the courts and are the full responsibility of the local Child Welfare Agency/District Office. All parental responsibilities for parental care and custody and subsequent medical services rest solely with the Child Welfare Agency/District Office. Internal Medical Consent and Information Sharing Procedures and Policies within local Hospitals, Mental Health Services and the IWK Health Centre • All medical facilities and services have protocols, policies and procedures for consent to treatment and information sharing that are applied for all children and youth receiving services. In order for doctors and medical personal to accurately determine the level of consent, the type of information required for diagnosis, and the information required for treatment, all parties require full understanding of the legal status and subsequent responsibilities for gathering information ,as well as releasing information. • Internal Medical /Health Services Consent policies are developed and determined upon the level of treatment or intervention required by the child or youth in care . The letter of Medical Designation provides the Health profession with the information required to accurately assess who receives information ,who provides information, and who has the authority to determine the type or level of treatment required. For example: The level of treatment and the level of consent required for a bruised knee from a fall on a bicycle is different from the level of treatment and the level of consent required for ongoing therapeutic Section 6 Page -32- Services to Children in Care - Appendix treatment at a day clinic which may include medication and direction from a mental health or medical professional, versus treatment for cancer, juvenile diabetes, congestive heart failure, etc. The Letter of Medical Designation • Attached to the Guidelines for Medical Treatment and Services is the template that social workers will use and provide for the care givers that have responsibilities in ensuring that child and youth receive regular and ongoing medical check-ups, treatment and ongoing medical services . • Medical services include regular visits with the family doctor, all clinics at the IWK or any other medical or health centre, including Mental Health Services . • Medical designation may change as the child or youth’s health needs change ,or the legal care status may change. The medical designation may subsequently change and should be reviewed during the annual child in care comprehensive planning meeting or during any case conference where a revised case/family plan may result. Section 6 Page -33- Services to Children in Care - Appendix Department of Community Services LETTER OF MEDICAL DESIGNATION AUTHORITY TO CONSENT FOR MEDICAL TREATMENT AUTHORIZATION FOR THE SHARING OF MEDICAL INFORMATION ABOUT CHILDREN IN CARE I _______________________________ of (Name of Care Giver) (Address) have been designated by the Minister of Community Services of the Province of Nova Scotia, or his/her delegate, under the authority of the Children & Family Services Act, and the Freedom of Information and Protection of Privacy Act, as the Care Giver for: (Child/Youth’s Name) (HCN#) (Date) The type of care status of the said child/youth is the following (please check appropriate box): Q Q Q Q In care through agreement Taken into care (case before the courts) Temporary care and custody Permanent care and custody As the designated Care Giver, I am authorized to consent to the following medical services: Q Q Q Q Regular visits to family doctor Appointments at the hospital Routine dental work Other (specify if necessary) for tests or visits with specialists I am also authorized to consent to the release of patient information from the child/youth health records to another care provider. The Social Worker responsible for this child/youth in care is: ______________________________________________ (Social Worker responsible for Child/Youth in Care) _______________________ (Phone #) The Social Worker shall be contacted when: • • medical treatment or surgical interventions other than those identified above are required; for the release of patient information from the child/youth health record to a third party. Section 6 Page -34- Services to Children in Care - Appendix Page - 2 This designation is valid for one year from date of signing or as determined by the Department of Community Services or Child Welfare Agency. It is the responsibility of the social worker responsible for the child/youth in care to ensure that a current Letter of Medical Designation is presented at the time of requesting medical services. (Care Giver) (Witness) (Date) (Social Worker) (Agency/District Office) (Date) (MARCH 2007) Section 6 Page -35- Services to Children in Care - Appendix Policy # 62 Family & Children’s Services Division Policy Statement/Protocol NO: 62 DATE: May 1, 1997 RE: Surpluses in the Children’s Services Agencies’ Operating Accounts Any funds received on behalf of children being maintained by the Department of Community Services, e.g., parents’ contribution, Canada Pension benefits, shall be placed in the appropriate maintenance budget subject to offset the cost of maintaining the child. ___________________________________ Jane E. Fitzgerald, MSW, RSW Administrator Family & Children’s Services Page -36 Policy # 64 DEPARTMENT OF COMMUNITY SERVICES FAMILY AND CHILDREN’S SERVICES DIVISION Policy Statement DATE: July 21, 2003 No: 64 (revised) TO: District Offices, Department of Community Services Children’s Aid Societies Family and Children’s Services Child Placing Agencies RE: i)Authority to sign Medical Consents for a Child Placed on Adoption Probation by a Child Placement Agency ii)Notification to Hospitals of Adoption Placement iii)Notification of MSI of Order of Care and Custody or Adoption Placement i) At the time a child is placed with an adopting family and the Notice of Proposed Adoption is signed, the agency and adopting parents shall also sign the attached form giving the adopting parents authority to sign for any medical treatment the child may require. (Form A) Form A shall be completed for: • • all children now in adoption probation placements; all children being placed on adoption probation after this date. ii) In addition, the social worker’s responsibilities include: • • • checking to determine if the child was previously admitted to any hospitals; and if so, advising the Hospital Medical Records Department of each hospital of the child’s new status and new parent(s)’ name(s) and birth date(s). (Form B) providing adopting parents with Form A. ..../2 Page -37 Policy Statement No. 64 (revised) July 21, 2003 Page Two iii) When a child is placed in permanent care and custody, or placed for adoption, agencies must notify MSI. Where a child in care is placed for adoption the adoptive parents must apply for a new Health Card Number in the adoptive name. Form C must be completed and submitted within five (5) working days of the order of care and custody or placement of a child for the purposes of adoption. Sincerely, Jane E. Fitzgerald, M.S.W., R.S.W. Executive Director Family and Children’s Services Att. c Regional Administrators Regional Child Welfare Specialists Page -38 Form A WHEREAS a female/male child, born on the ____ day of ____________________ , 2____ and known as is under the legal control of the (adoptive name) by virtue of an Order of Care and Custody or a Voluntary Care Agreement Section 68, under the Children and Family Services Act, AND WHEREAS the agency, by virtue of its legal control of the child has been given all the rights of the parents of the child, AND WHEREAS the child known as has been (adoptive name) placed on an adoption basis with who are adoptive parents’ name(s) fully responsible for the care and maintenance of the child, This document authorizes the above named adoptive parent(s) to obtain medical treatment, surgery, anaesthetic, etc., necessary for the health of the above named child and to sign whatever forms are necessary for admission of the child to hospital in furtherance of any such medical treatment, surgery, anaesthetic, etc. ....................................................... DATED ...................................................................... (Executive Director/District Manager) Previous admission to hospital ................................................ New Health Card # ................................................................. We, Mr. and Mrs. confirm the placement with us on an adoption basis of the child, named born on day of day of , , who was placed with us on the , . .................................................... DATED SIGNED ................................................................ SIGNED ................................................................ Page -39 Form B CHANGE OF NAME - ADOPTIVE CHILDREN (In accordance with Policy #64) FROM: Children’s Services Agency: (i.e.: Children’s Aid Society, Family and Children’s Services or District Office, Child Placing Agency) TO: Name of the hospital(s) where the child was previously a patient: Complete the following cross reference information Child’s Previous Health Card # Child’s Date of Birth day month year first second surname first second surname Hospital Chart Number if known Child’s New Health Card # Child’s Adoptive Name Adoptive Parents’ Name and mailing address Send this completed form to the above named hospital(s). Date After the Medical Records Department at the Hospital has completed the cross-reference procedure, this form will be destroyed. Note: This form must be forwarded to all hospitals in Nova Scotia who have treated this child. Page -40 Form C NOTIFICATION OF CANCELLATION TO M. S. I. TO: M.S.I. P.O. Box 500 Halifax, NS B3J 2S1 FROM: or by fax: 481-3160 Name and Address of Agency Reason for cancellation: G Placement for Adoption Date of Placement or G Order of Permanent Care and Custody Date of Care and Custody Old Health Card # Child’s Date of Birth Page -41 Policy #75 Family & Children’s Services Division Policy Statement/Protocol NO: 75 (Revised) DATE: April 1, 1999 RE: Revised Policy Statement for: (A) Persons Wishing to Provide Private Assessments or Counselling Pursuant to the Children and Family Services Act and (B) Provision of Other Contracted Services (A) PersonsWishing to Provide Private Assessments or Counselling Pursuant to the Children and Family Services Act Mandate This directive provides for the preparation of court ordered psychological, psychiatric or other assessments by private practitioners for children or families pursuant to Children and Family Services Act. It also covers requests for private assessments or counselling services by child welfare. The following is subject to the availability of funds designated for this purpose as referenced herein. Background Staff receiving a Court order for assessment or counselling of a client(s) under the Children and Family Services Act shall utilize existing mental health or publicly funded services when possible and appropriate. In matters where existing mental health or publicly funded assessments or counselling services are not available nor appropriate or in matters where special assessments or counselling services are required that are not otherwise available except through private practitioners, then these services may be provided by a person who has been approved pursuant to this directive. This directive is further subject to the availability of funds for this purpose as noted herein. . . . /2 Page -42 Policy Statement 75, Effective Page 2 April 1, 1999 Assessments and Counselling Arranged Through Private Practitioners Assessments or counselling sessions by approved private practitioners under the Children and Family Services Act may be approved by the Regional Administrator, District Manager, Agency Executive Director or Casework Supervisor and charged to the agency or department office budget approved for that purpose. In either case, an agreement for assessment or counselling must be developed between the agency, district office and the service provider which shall indicate the maximum number of hours being agreed to by the agency, district office and the private assessment or counselling service. In addition, the specific services being agreed to shall also be outlined. A standard agreement, Services Agreement pursuant to Policy #75, is attached as Part A and Part B. Approved List of Private Practitioners Before a person is contacted to provide a counselling service or complete an assessment, pursuant to this policy, the person must be included on the approved list of private practitioners. This list, to be maintained by the Family and Children’s Services Division and updated on a regular basis, shall include the qualifications of the practitioner and the type of service they are offering to provide. This list shall be made available to departmental and agency offices on a quarterly basis. Requirements For a person to be considered for the list of private practitioners, the following must be provided: (a) A completed application (as provided in Appendix “A”) as well as a curriculum vitae. (b) Proof of educational credentials (i.e., copy of diploma, certificate, etc.). (c) The person must be licensed or certified by their professional body and approved for private practice. Documentation to this affect shall accompany the application and be updated and submitted on an annual basis. (d) The person shall carry appropriate liability insurance while in private practice and shall include a copy of their current liability insurance along with their application. This must be updated on an annual basis. (e) A letter of security clearance from the municipal police force or RCMP shall also be provided. The potential service provider shall report to their local municipal police detachment or RCMP and request a criminal records check be completed on them and a copy included with the application. Please note that there may be a charge for this criminal records check. . . . /3 Page -43 Policy Statement 75, Effective Page 3 April 1, 1999 (f) The person shall include a signed permission to check with the Child Abuse Register as provided in Appendix “B” and returned with your application. Please complete the second section on the form and be sure that it is sworn to before a Commissioner of Oaths and return the form with your completed application. (g) An Oath of Confidentiality, signed by a Commissioner of Oaths, as provided in Appendix “C”. (h) Three letters of references from professionals who have knowledge of the professional qualifications and capabilities of the person requesting to be listedmust be submitted (see Professional Reference Form - Appendix “D”). (i) In the application, related experience in the area of specialization, i.e,. assessment, counselling, custody assessment, etc., must be highlighted. All requested information must be received before a review of the application will be considered. The completed application and supporting documentation should be forwarded to: Director of Child Welfare Family and Children’s Services Department of Community Services PO Box 696 Halifax, Nova Scotia B3J 2T7 Please note where private organizations or firms are asking to provide these services, the persons who will be providing services for the purposes identified shall be listed and similar information as noted above shall be provided with respect to these individuals. Persons Not Eligible for Private Service Agreements The following persons are not deemed eligible for private service agreements: (a) former employees of the Department of Community Services within the first six months of their separation from the Department cannot perform private practice for the Department of Community Services. (b) Current employees of Children’s Aid Societies or Family & Children’s Service Agencies if the parties are residents within the territorial jurisdiction served by the agency. (c) Current employees who may or may appear to be in a conflict of interest to prepare assessments or conduct counselling for youth because of their performance of official duties. . . . /4 Page -44 Policy Statement 75, Effective Page 4 April 1, 1999 (d) Individuals unwilling to comply with the information requirements or rate structure noted in this directive. (e) Individuals who are deemed to be unqualified to provide the services offered. Rates - Assessments, Counselling The maximum approved rate for assessments or counselling services pursuant to the Children and Family Services Act for assessments and counselling is up to $65.00 per hour to a maximum total amount agreed to when services were discussed with the assessor/counsellor and permissible within budget allocations. (Please note - individuals may be contracted to provide services for less than that amount). Where services cannot be obtained for this rate, the Executive Director or District Manager, as appropriate, may approve a rate up to $85.00 per hour to a maximum total amount agreed to by the parties. Executive Directors, District Managers, or Casework Supervisors will be able to enter into agreements subject to the allocation of funds approved for this purpose in their budget. Psychological Assessments/Counselling Where psychological assessments or counselling services are required under the Children and Family Services Act, the maximum approved rate shall be up to $85.00 per hour. (Please note parties may charge less than the maximum rate). Psychiatric Services Where private psychiatric services or reports are ordered and/or approved payment should be in line with the MSI fee scale for private practice and specified in the Agreement of Service. Hourly Rate Charges The hourly rate may be charged for: (a) Interviews with agency, district office or court personnel making the assessment or counselling referral (b) Reviewing documentation related to the case (c) Interviewing the parties (d) Interviewing collateral contacts as necessary or appropriate (e) Report/assessment preparation (f) Attending court when ordered/or required for the purpose of giving evidence. . . . /5 Page -45 Policy Statement 75, Effective Page 5 April 1, 1999 (g) Travel time in situations where the total amount of travel exceeds 100 km per session. In these instances, the travel time for the period related to the travel in excess of 100 km will be paid for at the rate of 50% of the agreed hourly contracted rate. Expenses Included in the Rate The following are deemed to be covered in the approved rate and shall not be charged for additionally. These include: (a) (b) (c) (d) (e) (f) (g) the typing of the report; providing the minimum number of copies of the report required, i.e., original and two copies; long distance phone calls; meals; courier costs; the first 100 km of travel related to each client session; other costs related to the assessment not prior agreed to. Billing The Service Provider agrees to the terms set out in Part “C”, the Client Attendance Policy for Payment to Service Providers. As per the Service Agreement, a bill shall be forwarded to the designated staff person who contacted the private practitioner to prepare the report outlining, in detail, the time spent, by date relating to the service provided. Part “D” Client Confirmation of Service Provided Pursuant to an Established Purchase of Service Agreement must be completed and accompany each billing presented. (B) Provision of Other Contracted Services A listing of the Other Contracted Services is outlined on the Service Agreement Form, Part A, pursuant to Policy Statement #75. Requirements For a person to be considered to provide services listed on the Services Agreement Form other than counselling and assessments, the following must be provided: (a) A completed application for contracted services (as provided in Appendix “E”) as well as a curriculum vitae. (b) A letter of security clearance from the municipal police force or RCMP shall also be provided. . . . /6 Page -46 Policy Statement 75, Effective Page 6 April 1, 1999 The potential service provider shall report to their local municipal police detachment or RCMP and request a criminal records check be completed on them and a copy included with the application. Please note that there may be a charge for this criminal records check. (c) The person shall include a signed permission to check with the Child Abuse Register as provided in Appendix “B” and returned with your application. Please complete the second section on the form and be sure that it is sworn to before a Commissioner of Oaths and return the form with your completed application. (d) An Oath of Confidentiality, signed by a Commissioner of Oaths, as provided in Appendix “C”. (e) Three letters of references from professionals who have knowledge of the professional qualifications and capabilities of the person requesting to be listed must be submitted. (f) In the application, related experience in the area of the service to be provided etc., must be highlighted. (g) A valid driver’s licence, current vehicle inspection certificate and proof of current automobile insurance. All requested information must be received before a review of the application will be considered. The completed application and supporting documentation should be forwarded to the Agency/ District Office the applicant is applying to provide a service. Please note where private organizations or firms are asking to provide these services, the persons who will be providing services for the purposes identified shall be listed and similar information as noted above shall be provided with respect to these individuals. Persons Not Eligible for Private Service Agreements The following persons are not deemed eligible for private service agreements: (a) former employees of the Department of Community Services within the first six months of their separation from the Department cannot perform private practice for the Department of Community Services. (b) Current employees of Children’s Aid Societies or Family & Children’s Service Agencies if the parties are residents within the territorial jurisdiction served by the agency. . . . /7 Page -47 Policy Statement 75, Effective Page 7 April 1, 1999 (c) Current employees who may or may appear to be in a conflict of interest to conduct counselling for youth because of their performance of official duties. (d) Individuals unwilling to comply with the information requirements or rate structure set out by Policy #75. (e) Individuals who are deemed to be unqualified to provide the services offered. Rates and Billing The Service Provider agrees to the terms set out in Part “C”, the Client Attendance Policy for Payment to Service Providers. Rates will be paid as per the Service Agreement. A bill shall be forwarded to the designated staff person who contacted the private practitioner to prepare the report outlining, in detail, the time spent, by date relating to the service provided. Part “D” Client Confirmation of Service Provided Pursuant to an Established Purchase of Service Agreement must be completed and accompany each billing presented. _____________________________ George R. Savoury, MSW , RSW Acting Executive Director ps’75.cw (Feb 1//99) Page -48 Revised July 1, 2011 Policy #94 MAINTENANCE EXPENDITURES FOR CHILDREN IN CARE Babysitting Prior Approval** Up to a Max. $4.00 per hour*** Approvals are on a case-by-case basis and must be associated with the child’s Plan of Care. Board Dept. Rate* (Appendix A) Covers food, lodging and personal care items. Personal care items includes items such as toothpaste, soap, shampoos, deodorant, shaving supplies, etc. Camps, Club Memberships Prior Approval** Up to a Max $500 per year.*** Includes fees for registration and membership, associated costs i.e., brownie uniform, camping gear along with travel expenses, i.e., hockey practices outside local community. Recreation and items such as skates, bicycles. Child Care Children in Permanent Care and Custody: agency pays full costs. Children Taken into Care who are with their parents under supervision of the agency: subsidized child care costs are paid by the parents. Children Taken into Care and placed in foster care: Agency pays full costs. The agency has the discretion to cover the costs of the child care space for a period up to two weeks after the child is removed to hold the space for the child. Clothing Dept. Rate* (Appendix A) Guideline: Careful consideration of the parents views regarding clothing should fully be discussed at the time of placement. Evaluate with the family that there may be a possibility that their child(ren) will return home with a higher level expectation of dress than the parents can afford. If the initial contract is for less than (4) four months, the clothing subsidy shall be omitted. The only exception to this policy is in special circumstances where there is a demonstrated seasonal/or obvious need. In this case, workers have discretion up to $200 for the purchase of immediate clothing needs when a child first enters care. * ** *** Department rates are enclosed and must be adhered to. Prior Approval - bases on decision of worker and/or supervisor and/or Executive Director or District Manager upon review of the agencies maintenance budget. W here maximum are indicated, consideration to exceed these limits must be reviewed at a case planning meeting. Page -50 Damages When a child in care damages property in a licensed child caring facility outstanding costs not covered by the insurance shall be paid from the facility’s maintenance and repair budget. In the case of damage to a staff person’s personal property, outstanding costs not covered by a staff person’s personal insurance, may be submitted to the agency and any payments, with prior agency approval, shall be issued from the appropriate agency budget depending on the child’s care status. When a child in care damages property in a foster home, costs under $250. are to be submitted to the agency and may be reimbursed from the appropriate agency budget. Foster parents will first discuss property damages with agency staff and request approval for reimbursement. All damages over $250. and up to $25,000. are to be managed under the Foster Care Self-Funded Program. When appropriate, the child should make restitution for the damage, ie. from their spending money or doing chores. Dental Costs paid to a dentist for routine examinations, cleaning and preventative care including fillings not covered by provincial health care. Diapers/Infant formula Up to a Max. $200 per month per child*** To be paid by agency. There will be a straight reimbursable for items purchased upon receipt verification. Driver’s Education Requests to be reviewed at a case planning meeting. Driver’s License/Insurance Driver’s Ed. may be cost shared with child and agency. Any license or insurance costs are responsibility of the youth. Equipment, Furniture & Replacement of Bedding Crib, highchair, playpen, beds, dressers, etc. These items are expected to be provided by the foster parent and will only be covered in extraordinary circumstances with prior approval. If foster parents(s) do not have access to a safety approved car seat, the agency will provide one. If any items in this category are purchased, then they are considered to be the property of the agency. Foster parents will be required to complete an equipment and furniture request form (Appendix B). Agencies will be required to use the inventory system to track purchases and subsequent retrievals of these items (Appendix C). Replacement of bedding may be provided based on the special needs of the child. The cost of furniture to establish a child in an independent living situation requires prior approval. Consideration must be given to obtaining these furnishing in a cost effective manner. * ** *** Department rates are enclosed and must be adhered to. Prior Approval - bases on decision of worker and/or supervisor and/or Executive Director or District Manager upon review of the agencies maintenance budget. W here maximum are indicated, consideration to exceed these limits must be reviewed at a case planning meeting. Page -51 Glasses/Contacts Prior Approval** Up to a Max. $300 every other year*** Eye examinations (10 yrs. - 21 yrs.) Hair Care Prior Approval** Up to a Max. $150 per year*** Cuts, perms, straighteners, extensions, colouring and associated items. Independent Living Under Review. Medical Equipment Prior Approval** The cost of equipment not covered by MSI as recommended in writing by the appropriate specialist i.e., wheelchair, prosthesis, etc. Non-Prescription Items Prior Approval** The cost of non-prescription remedies associated with ongoing treatments as recommended by a doctor or required to treat common ailments, (cold, flu, e.g., common cold remedies, acne remedies, allergy medication or items such as menstrual discomfort remedies and sanitary supplies). Orthodontics Prior Approval** Only applies to long-term placements, children in permanent care and custody or Section 18. Post Secondary Education See Section 6 - Children In Care and Custody Manual for Department of Community Services Educational Bursary Policy and Extension to the Educational Bursary Policy. Prescriptions Prescriptions for children in care who are placed outside of their parents’ home will be covered by Pharmacare. Pharmacare provides prescription drug coverage for those drugs listed in the Nova Scotia Formulary. Pharmacare generally covers generic drugs. If there is a need for a drug that is not listed, the physician may be able to obtain approval by contacting Pharmacare. In extraordinary circumstances, and with supervisory approval, Pharmacare benefits may be extended to children in care whose placement is with a parent. * ** *** Department rates are enclosed and must be adhered to. Prior Approval - bases on decision of worker and/or supervisor and/or Executive Director or District Manager upon review of the agencies maintenance budget. W here maximum are indicated, consideration to exceed these limits must be reviewed at a case planning meeting. Page -52 School Activities & Items Prior Approval** Up to a Max $200 per year*** The cost of approved school related items such as class and school trips, school pictures, additional supplies, etc. School Supplies Prior Approval** Up to a Max $200 per year** The cost of approved school related items such as class and school trips, school pictures, additional supplies, etc. Special Occasion Costs Includes: Birthday, Christmas, Grading gifts, Graduation costs and other ethnic/religious events. Birthday: Up to a Max. $125*** Worker and caregiver discretion. Christmas: Dept. Rate* (Appendix A) Grading Gifts: Up to a Max. $50*** Worker and caregiver discretion. Should not be awarded to set up expectations of success or failure, however, should be provided if birth child(ren) in the home receive gifts. The child’s age and appropriateness of the gift must be considered. Graduation Costs: Prior Approval** Up to max. (Senior - $400, Junior - $200)*** Graduation photos, school ring, Prom outfit, etc. Clothing is cost shared from clothing allowance with certainty of a successful school completion. Other (Ethnic/Religious Events): Up to a Max. $20*** Worker and caregiver discretion. Spending Allowance for Children Dept. Rate* (Appendix A) Telephone Calls Prior Approval** Up to a Max. $30 per month*** May be used to maintain contact with birth family and significant others determined by child’s worker and caregiver. Whenever possible, use discount times. * ** *** Department rates are enclosed and must be adhered to. Prior Approval - bases on decision of worker and/or supervisor and/or Executive Director or District Manager upon review of the agencies maintenance budget. W here maximum are indicated, consideration to exceed these limits must be reviewed at a case planning meeting. Page -53 Transportation Transportation shall be reimbursed for the following only: • • • • • • • child’s medical appointments child’s mental health appointments child’s other counselling legal access visits case conferences recreational activities at the current provincial government rate Vacation Prior Approval** Up to a Max. $300 per year.*** Approvals are on a case-by-case basis and must be associated with the child’s Plan of Care. Procedure for Reimbursement Foster parent must use the claim form for reimbursement of expenses incurred on behalf of a child in their care (Appendix D). Receipts must be provided for purchased items. The form is forwarded to the child’s worker for approval who then forwards the cheque requisition and receipts to Financial Services/Agency Accounting Department for payment. * ** *** Department rates are enclosed and must be adhered to. Prior Approval - bases on decision of worker and/or supervisor and/or Executive Director or District Manager upon review of the agencies maintenance budget. W here maximum are indicated, consideration to exceed these limits must be reviewed at a case planning meeting. Page 1 Appendix A DEPARTMENT OF COMMUNITY SERVICES Foster Care Maintenance Rates for Children in Care Revised July 1, 2011 AGE RATE PER DIEM 0-9 $17.50 10+ $25.43 CLOTHING ALLOWANCE AGE MONTHLY QUARTERLY 3 TIMES/YEAR YEARLY 0-4 $39.20 $118.00 $157.00 $471.00 5-9 $64.75 $194.00 $259.00 $777.00 10+ $90.60 $272.00 $362.00 $1,088.00 Note: Slight variance in clothing allowance may occur depending on frequency of payment. SPENDING ALLOWANCE Effective March 1, 1999 AGE MONTHLY 0-5 $10.00 6 - 11 $15.00 12 - 15 $25.00 paid to child 16+ $40.00 paid to child Page 2 SCHOOL SUPPLIES RATES Effective March 1, 1999 AGE ANNUALLY Grades Primary to Six $120.00 Grades 7+ $150.00 CHRISTMAS ALLOWANCE Effective March 1, 1999 Revised July 1, 2011 AGE ANNUALLY 0-5 $100.00 6 - 10 $145.00 $125 to caregiver to purchase child’s gift and $20 for child to buy gifts) 11 - 20 $190.00 $150 to caregiver to purchase child’s gift and $40 for child to buy gifts) Appendix B Family and Children Services Agencies Furniture Request Form Foster Parent Name Request # Child’s/(children’s) Name (s) Care Status CRCC G CRTC G Vol. Care G Date of Placement Initial Placement at this home yes G no G Reason foster parent is unable to provide appropriate furnishings. Date furniture is required: Items Required Description Estimated/Actual Costs Total Foster Parent In completing and signing this request, I confirm that I do not have access to the described furnishings above in any other manner than direct purchase by the Agency. As well, I understand that these furnishings remain the property of the Agency and as such I will ensure they are returned in reasonable condition following the termination of a related foster care placement. Failure to return these furnishings may result in a garnishing of board payments. Foster Parent signature: Social Worker I have reviewed the above request and based on this support the provision of furniture by the Agency. In advance of approving a purchase of new equipment, I have reviewed the availability of existing furniture items not in use. Social Worker signature: Supervisor/District Office Manager Approval Family and Children Service Agencies Furniture Inventory Tracking Appendix C Item # Request # Description Price Purchase Date Placed at (Foster Parent) Date Moved to (Foster Parent) Date Moved to (Foster Parent) Date Moved to (Foster Parent) Date Appendix D Part 1 FOSTER HOM E TOTAL EXPENSE FORM Please forward the completed form, including any receipt information, to your agency/district office on a monthly basis. NOTE: Please attach all receipts when requesting reimbursement. ONE EXPENSE FORM PER CHILD Name of Foster Parent: Address: Name of Child: Postal Code: Telephone: Date From: DATE TRAVEL DESTINATION (From/To) M ILEAGE # OF KM S Date To: DESCRIPTION OTHER EXPENSES AM OUNT SUBTOTAL # OF KMS TOTAL KMS REIMBURSEMENT FOR THIS CHILD TOTAL OTHER EXPENSES TOTAL EXPENSE REIMBURSEMENT I hereby certify that the expenses claimed are correct and just in all respects and that the w hole expenditure w as incurred on behalf of the child in care. Signature of Foster Parent: Appendix D Part 2 FOSTER HOM E TRAVEL EXPENSE FORM 1. 2. 3. 4. 5. 6. 7. 8. 9. Complete a FOSTER HOM E EXPENSE FORM (Appendix D) for each of the children in your home during the past month. Complete your name, address, telephone number and postal code. Enter the appropriate dates, i.e., Date From: April 1, 2007 Date To: April 30, 2007. Total the numbers of Kms driven for all children and enter this figure in the This M onth’s Kms block . Add the figure in This M onth’s Kms block to the Year to Date Kms block and enter this figure in the Total Year to Date Kms. The figure in the Total Year to Date Kms. block will be the figure in the Year to Date Kms block next month. As your total Kms driven for all children reaches 16,001 kms and then 27,001 kms, the rate will be reduced, as shown. Place the number of Kms driven this month in the appropriate column, depending on the yearly total of Kms. driven. Calculate the Amount and the Total Amount. Foster Parent Name: Address: Telephone: Postal Code: Current Claim Summary This M onth’s Date Kms: Date From: Date To: Year to Date Kms. First 16,000 Provincial Government Rate 16.001 - 27,000 Over 27,000 Total Year to Date Kms: No. of Kms driven this month @ Kms claimed @ Kms Claimed @ Kms Claimed @ Rate Amount Amount for First Child Amount for Second Child Amount for Third Child Amount for Fourth Child Total Amount I hereby certify that the expenses claimed are correct and just in all respects and that the w hole expenditure was incurred on behalf of children in care. Signature of Foster Parent: Appendix E DEPARTMENT OF COMMUNITY SERVICES FAMILY AND CHILDREN’S SERVICES DIVISION ASSESSMENT OF CHILDREN IN FOSTER HOME CARE GUARDIAN AGENCY DATE OF ASSESSMENT NAME OF CHILD BIRTH DATE SIGNATURE OF FOSTER PARENT SIGNATURE OF WORKER INSTRUCTIONS: Read through the following lists checking in the space beside each statement only if it applies to the child. Go back over those statements you have checked off and make a further rating (1, 2 or 3) by putting a check mark in the appropriate space to the right of the line. (1) requires NO MORE time, energy or skill than would be spent caring for a child of his/her age not having this problem. (2) requires a MODERATE expenditure of time, energy and/or skill (quite a bit more than would be spent on a child of his/her age not having this problem). (3) requires a GREAT expenditure of time, energy and/or skill (much more than would be spent caring for a child of his/her age not having this problem). EXAMPLE: Mrs. Jones feels that Johnny is physically slow in getting around and a bit uncoordinated, that this does not require any more time, energy or skill from a supervising point. N/A #2 Child needs supervision and/or some help with mobility due to: (1) (2) (3) x NOTE: FOR RATING PURPOSES, THE CHILD ’S PHYSICAL AND /OR MENTAL AND /OR EMOTIONAL DISABILITIES - NOT AGE , ARE TO BE CONSIDERED AS THE DETERMINING FACTORS . I. PHYSICAL OR PERSONAL CARE THIS SECTION , NORMAL CARE INCLUDES THOSE CHILDREN WHO ARE BASICALLY SELF-CARING FOR THEIR AGE , BUT WHO MAY NEED SOME HELP WITH PUTTING ON BRACES OR PROSTHESIS , HELP WITH BUTTONS, LACES. N/A 1. Child needs help with dressing, bathing and general toilet (except infants). 2. Child needs supervision and/or some help with mobility due to: 3. a) being physically slow/uncoordinated b) being independent on a mechanical appliance to move around, eg., uses wheelchair, or braces, or walker. c) being unable to run and play as others do. Child has feeding problems that require attention and/or assistance due to: a) excessive intake of food, may require frequent small meals rather than three. b) excessive messiness or slow eating due to mental retardation, emotional or physical disability. c) need for tube or gavage feeding. 4. Child does not have complete bladder or bowel control because of illness or organic defect and requires attention. 5. Child has a medical appliance that requires attention, eg., for drainage or ileal conduit, colostomy. 6. Child cannot be left alone at any time, eg., in the yard, in a room watching T.V. Page -61 (1) (2) (3) 7. Child requires continuous supervision by a mature adult and cannot be left with a teenage babysitter. 8. Child requires continuous supervision by a skilled adult, eg., trained nurse. II THERAPEUTIC PHYSICAL CARE 9. Child requires regular program of prescribed medications requiring skill and training to administer. 10. Child requires extra care to skin. 11. Child requires special diets or supplements. 12. Child requires attention due to need for aspiration, suctioning, mist-tent. 13. Child requires attention due to need for allergyfree atmosphere, eg., for asthma. 14. Child requires assistance with: (a) physical therapy (b) speech therapy (c) occupational therapy to be done at home. 15. Child requires supervision of: (a) physical therapy (b) speech therapy (c) occupational therapy to be done at home. 16. Due to: (a) physical disability (b) mental disability (c) learning disability child requires extra attention and play to stimulate development. 17. Other (Specify) N/A (1) (2) (3) N/A (1) (2) (3) III SUPERVISION OF MEDICAL CARE 18. Child needs frequent hospitalization. 19. Child needs unusual or exceptional medical care at least monthly. 20. Child needs unusual or exceptional dental care at least monthly. 21. Child needs regular visits to allied health professionals. IV ANCILLARY CARE 22. Child requires excessive laundry. 23. Child is destructive to household goods, eg., tearing up sheets, chair covers, smearing and soiling. 24. Other (Specify) N/A (1) (2) (3) N/A (1) (2) (3) THERAPEUTIC EMOTIONAL CARE: IN THIS SECTION , NORMAL CARE INCLUDES CHILDREN WHOSE CARE IS ESSENTIALLY NORMAL ON A DAY -TO -DAY BASIS, BUT WHERE IRREGULAR LAPSES COULD OCCUR , EG ., DUE TO PARTICULARLY DIFFICULT SESSIONS AFTER VISITS WITH NATURAL FAMILY , OCCASIONAL PERIODS OF EXCESSIVE DEPENDENCY AND /OR CHILD IS PASSIVE , LACKING IN RESPONSE AND ABILITY TO RELATE . N/A 25. Child needs emotional support, encouragement and re-assurance because: a) is unusually withdrawn. b) has a low self-image, feels inferior/ rejected. c) is unusually dependent. d) is depressed. e) Other (Specify) (1) (2) (3) N/A 26. 27. Child needs extra attention from the foster parents, eg., extra time for discussion, special play periods, supervision of activities due to: a) attention seeking. b) night problems. c) need for constant repetition and followthrough on instructions. d) hyperactivity. e) encopresis (incontinence, not due to illness or organic defect). f) lies. g) Other (Specify) Child needs limit setting, firmness, some discipline because: a) is angry/defiant b) is manipulative c) is destructive d) is aggressive e) is a runner f) steals g) is dependent on drugs/sniffing h) is dependent on alcohol i) acts out sexually j) Other (Specify) (1) (2) (3) N/A 28. 29. Child’s behavior in the community requires that foster parents have frequent contact with community persons such as: neighbours, school authorities, law enforcement authorities and the Courts, in order to explain and deal with the child’s problems which are: a) academic/learning problems. b) regular truanting. c) inappropriate behaviour but non-delinquent. d) delinquent or deviant behavior. e) Other (Specify) Child needs help in finding and making use of satisfying recreational opportunities. TABULATION OF SCORE: #2's x 2 = #3's x 4 = TOTAL POINTS = (1) (2) (3) SPECIAL BOARD RATES (Regular Rate Plus Point Rating) Points Rating Points Rating 10 - 19 $1.50 80 - 89 $8.50 20 - 29 2.50 90 - 99 9.50 30 - 39 3.50 100 - 109 10.50 40 - 49 4.50 110 - 119 11.50 50 - 59 5.50 120 - 129 12.50 60 - 69 6.50 130 - 139 13.50 70 - 79 7.50 140 - 149 14.50 Post Care and Custody Agreement I, __________________________________________, wish to participate in the Extension to the Educational Bursary Program. I understand that I will receive funds to cover the actual costs of tuition, books and related expenses, in addition to regular maintenance, so long as I meet the following conditions: • I enroll in a program offered at an accredited educational institution (university, community college or private vocational training) that is designated by or registered with the Canada Student Loan Program or that is licensed by the Private Colleges Act • I attend an education institution within the Atlantic Provinces unless the program I wish to pursue is not available within the Atlantic Provinces • I attend the program of study on a full-time basis and carry a full course load for the year • I successfully complete a minimum of 80% of the courses per year. An exception can be made with the approval of the Regional Adminsitrator. The request for an exception shall be forwarded in writing from the Executive Director/District Manager to the Regional Administrator. • I provide an annual transcript to my social worker • I contribute $1000 annually. These funds may be obtained through summer employment, part-time employment or loans. I understand that a reduction of the $1000 contribution may be approved by the Executive Director/District Manager if the post-secondary program extends beyond eight months each year • I apply for any available scholarships and bursaries, including the Ken Dryden Scholarship • I understand that this program will provide funding to support only one degree at university, one community college program or one private vocational program. • I understand that post-secondary programs whose tuition fees are greater than the most expensive Nova Scotia university tuition fees will require the approval of the Regional Administrator. The request shall be forwarded in writing from the Executive Director/District Manager to the Regional Administrator. • I understand that funds can be made available until my 24th birthday _______________________________ Date ______________________________________ Signature I, _____________________________________________, Executive Director/District Manager of ____________________________________, agree to cover the costs of post-secondary tuition, books and related expenses in addition to regular maintenance for _________________________________, so long as the conditions of this agreement are met. This agreement is effective for one year but will expire on ______________________________________’s 24th birthday. ______________________________ Date ____________________________________ Signature SECTION 6 REFERENCE MATERIAL SEXUALITY RESOURCES Publications: 1. Agnes, M. (1996). Nova Scotia Sexual Health Needs and Resources Assessment: Just loosen up & start talking. Halifax, NS: The Nova Scotia Department of Supply & Services. 2. Early Childhood Education Task Force (1995). Right from the start: Guidelines for sexuality issues, birth to five years. USA: Sexuality Information and Education Council of the United States. 3. Health Canada (1994). Canadian Guidelines for Sexual Health Education. Ottawa: Health Canada. 4. McCullagh, J. & Simpson, B. (1995). “Accessible child welfare services for lesbian, gay and bisexual youth”, OACAS Journal, 39(3). 5. Planned Parenthood Federation of America (1986). How to talk with your child about sexuality. New York: Doubleday & Company, Inc. 6. Selverstone, R. (1996). Now what do I do? How to give your pre-teens your messages. USA: Sexuality Information and Education Council of the United States. Community Agencies with Sexual Health Information &/or Services: 1. 2. 3. 4. 5. 6. AIDS service organizations Gay, lesbian & bisexual youth groups Planned Parenthood affiliates Public health department Teen health centres Helpline Websites: 1. 2. 3. 4. 5. 6. American Social Health Association: www.ashastd.org Planned Parenthood Federation of America: www.plannedparenthood.org Planned Parenthood Federation of Canada: www.ppfc.ca Rainbow Classroom Network: www.dezines.com/rainbow/ Sexuality Information & Education Council of the United States: www.siecus.org Lesbian, Gay and Bisexual Youth Project: www.youthproject.ns.ca Resources/Books: Entitlement Books Frog Hollow Books - Street, Halifax One Teenager in Ten, Alyson Publications, Boston, 1983 Looking At Gay and Lesbian Life, Warren Blumfeld and Diane Raymond, Beacon Press, Boston, 1983 The New Loving Someone Gay, Don Clark, Celestial Arts, Berkeley, 1987 Young Gay and Proud, S. Alyson, ed, Alyson Publications, Boston, 1981 Reference Material: Steinhauer, Paul D., The Least Detrimental Alternative, 1991 Psychiatry: Provincial Medical Association Psychology: St. Mary’s University, Department of Psychology Dalhousie University, Department of Psychology Provincial Psychological Association SECTION 6 SERVICES TO CHILDREN IN CARE Summary of Standards For Services To Children In Care 6.1(a) The child’s social worker must have face to face contact with the child within the first seven days of placement, this must occur in the child’s placement. The social worker must have either phone or face to face contact at least every 30 days with the child. Face to face contact with the child must be at a minimum of once every 90 days for children and youth in care of the agency, and this contact must occur in the child’s placement. Each contact with the child must be recorded and documented on the case management system. When contact was not possible, the reasons why should also be documented. 6.1(b) Children and adolescents in care must have access to a telephone and a contact number for their social worker or how to reach another worker or the supervisor in an emergency. 6.2(a) Social workers responsible for a child in care must have regular and meaningful contact with the child’s care providers. The child’s social worker must have face to face contact with the caregiver within the first seven days of placement, this must occur in the child’s placement. The social worker must have either phone or face to face contact at least every 30 days with the caregiver. Face to face contact with the caregiver must be at a minimum of once every 90 days, and this contact must occur in the child’s placement. 6.2.3(a) Children over 12 must be consulted on whom they consider significant and who they would like contacted (see Section 2.19: Access Services). 6.3(a) When a social worker or other agency staff is transporting a child in care, the social worker or agency staff must make sure that the children are properly restrained, either by seatbelt or by child restraint system, as appropriate. 6.3(b) A child in care must not be transported by taxicab unless they are properly secured by either a child restraint system or a seatbelt, as appropriate, and as prescribed by the Motor Vehicle Act. 6.4(a) Parents have an obligation to contribute financially to the care of their children. Agencies are required to review the financial capacity of all parents who enter into a Section 17 or Section 18 Agreement regarding their ability to contribute toward maintenance of their children in care, using the Child Maintenance Guidelines. 6.4.1(a) A child in care must be provided with sufficient nourishing food to meet their individual needs for growth, development, and activity. Section 6 Services to Children in Care A child’s individual needs for growth, development, and activity must take the following into account: • • • • • general nutritional requirements of children the special nutritional requirements of the particular child, including any requirements or limitations diagnosed or prescribed by a health care provider the child’s views, including the child’s specific likes and dislikes the child’s culture and diet customs, if applicable any special requirements of the child relating to the manner in which food is served or prepared, if the child is young or has special needs 6.4.2(a) A child in care must be provided with clothes that are of comparable style, quality, and condition as those of other children in their community. 6.5(a) A medical must be completed within 30 days of a child entering care and annually thereafter while in care. (See Appendix Section 3 for forms) 6.5(b) A medical booklet must be provided and maintained for every child in care which must include the child’s health card number. 6.5.1(a) A child in care must receive dental care as required to maintain their oral health, safety, and well-being. A dental checkup must be completed within 90 days of a child entering care and annually thereafter while in care. 6.5.2(a) Where the child has the capacity to consent, the child’s consent to treatment must be obtained. 6.5.4(a) A valid Nova Scotia health care number must be documented for each child in care on the case management system and made available to those persons responsible for overseeing the medical care of the child. 6.5.5(a) Where the status of the child is not determined, the social worker must apply to Indian and Northern Affairs Canada to determine if the child is eligible for Indian status. For a child with Indian status, the social worker must clarify with Indian and Northern Affairs Canada which health care benefits the child may be entitled to receive. 6.7(a) The child’s social worker must make sure that children and youth in care receive ongoing, age-appropriate education about sexuality issues. In addition to healthy sexual development the risks associated with and prevention of sexually transmitted diseases must be reviewed. The date and summary of the discussions must be noted in the the record. 6.8.1(a) Policy Statement #75 must be applied when contracting services for a child in care. Section 6 Services to Children in Care 6.8.1(b) When directed by the courts to complete psychological, psychiatric, or other assessments, or where the child welfare agency requires an assessment/treatment of a child, and the agency is unable to provide the assessment and/or treatment, the agency must utilize existing mental health or other publically funded services when possible and appropriate. 6.9(a) A child in care is entitled to have access to education. In compliance with the Education Act, a child in care over 5 and under 21 must be enrolled in public school in their local community unless: • • • the child is 5 and it is in the child’s best interests that enrolment be deferred for one year the child is involved in an alternate education program offered or approved by the Department of Education the child is over 16 and refuses to attend any school or any alternate education offered or approved by the Department of Education 6.9.6(a) Educational goals must be developed as part of the comprehensive plan of care. 6.11(a) Where a child is in the care and custody of an agency or district office by court order and the child is entitled to money from an estate or insurance settlement, and no guardian has been appointed in regard to that money, the agency or district office must consult with the office of the public trustee. 6.12(a) Where a child in care is entitled to Canada Pension Plan benefits, the agency or district office must take the necessary steps to make sure an application is made for those benefits and the benefits be used to contribute to the costs of maintaining the child. A child may be eligible for pension benefits if either of their parents are disabled or deceased and the contribution requirements have been met. Section 6 Services to Children in Care



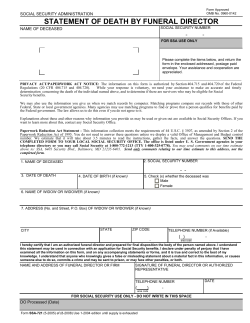








© Copyright 2026