
Arizona Kith and Kin Project The Invisible Child Care Provider:
Arizona Kith and Kin Project Year 1 Evaluation Report Arizona Kith and Kin Project The Invisible Child Care Provider: Findings from Arizona’s Kith and Kin Project 2010 Prepared by Eva Marie Shivers, J.D., Ph.D. Institute for Child Development Research & Social Change Indigo Cultural Center, Inc. Arizona Kith and Kin Project Year 1 Evaluation Report Acknowledgements This research was made possible through the generous support of First Things First. The conclusions and views presented in this report are those of the author only and not of the study’s funders or reviewers. Special thanks to: Susan Wilkins Jacobs, Vicki McCarty, and Sarah Ocampo-Schlesinger for the guidance and support on the design of the evaluation, and for the patience and openness to the process of evaluation. Toni Porter at Bank Street for her guidance, resources and enthusiasm for the work of those who serve Family, Friend and Neighbor child care providers throughout the country. All the ASCC Arizona Kith and Kin Project Specialists for their hard work as data collectors and for sharing their insights into the process. Cristal Byrne, Luiset Vargas, and Marcia Taplin for their assistance and amazing attention to detail in managing the database for this evaluation. Collective Designs for the fabulous layout and formatting of this report. All the Family, Friend and Neighbor child care providers in completing all the survey instruments, and for so graciously allowing us into their homes. 2 Arizona Kith and Kin Project Year 1 Evaluation Report Table of Contents Executive Summary . . . . . . . Page 4 Introduction . . . . . . . . Page 10 Methods . . . . . . . . Page 15 Findings . . . . . . . . Page 21 Discussion . . . . . . . . Page 48 References . . . . . . . . Page 54 Appendices . . . . . . . . Page 59 3 Arizona Kith and Kin Project Year 1 Evaluation Report Executive Summary Introduction The prevalence of child care provided by informal caregivers – also increasingly referred to as “Family, Friend and Neighbors” (FFN) – has been well documented by researchers over the past six years. This is a common child care arrangement for many young children in the U.S., especially those from low-income families, families of color, and infants and toddlers (Brandon, 2005; Porter, Paulsell, Del Grosso, Avellar, hass, Vuong, 2010a). The Arizona Kith and Kin Project was established in 1999 to provide ongoing early childhood training and support to exempt family, friend, and neighbor caregivers. The goals of the Arizona Kith and Kin Project are to (1) improve the quality of child care through training; (2) increase caregiver’s knowledge and understanding of early child development; and (3) increase caregiver’s knowledge and understanding of health and safety issues to provide a safer child care environment1. The Arizona Kith and Kin Project provides 14-week, two-hour support group training series for Spanish and English-speaking caregivers. Most training sessions are offered only in Spanish. The initiative provides transportation for caregivers who are located within a 5-mile radius of the training location and on-site child care by trained child care providers during each training session. All training sessions are offered during the day and sometimes the evening. In the 2010 funding year, The Arizona Kith and Kin Project offered training at 55 locations,including four sites in Coconino County and six sites in Yuma County. The following subjects are covered during the 14-week support group training series; some topics span multiple weeks: r Child Development / Ages and Stages r Daily Schedule Planning r Nutrition r Parent/Caregiver Relationships r Arranging the Environment r Language and Literacy (including a Reading Is Fundamental (RIF) book event and distribution) r Brain Development r Health and Safety r First Aid r CPR r Child Passenger Safety r Guidance and Positive Discipline In addition to First Things first, other funders include: Valley of the Sun United Way; Bank of America; the City of Tempe; Arizona Republic; Channel 12 Season of Sharing; and JP Morgan Chase. 1 4 Arizona Kith and Kin Project Year 1 Evaluation Report Purpose of Evaluation The purpose of this evaluation was to discover whether the Arizona Kith and Kin Project was successful in reaching its desired outcomes – that is, whether there were demonstrable changes in participants’ beliefs, practices with children, and environmental quality. Methods This evaluation had two main components – data collection with all participants (n = 827) and data collection with a smaller, targeted sample of participants (n = 55). Instrumentation included: Background questionnaires r Provider surveys » Beliefs about caregiving » Social, emotional, material well-being r Observational instruments (Baseline 2-hour visit in provider’s home; Second 2-hour visit after project completion) » Provider-child communication » Learning activities with children » Provider interactions with children » Materials and equipment » Health and safety r Pre and post tests » Knowledge about child development » Knowledge about health and safety r Feedback about project Results In 2010, the Arizona Kith and Kin Project served more than 900 Family, Friend and Neighbor (FFN) child care providers. This is one of the largest quality improvement initiatives for FFN providers in the country (Porter et al., 2010). By and large, the Arizona Kith and Kin Project was a success as measured by high participation rates, statistically significant increases on key quality indicators, and overwhelming positive feedback from providers. Key findings are summarized below. Conditions of Caregiving We found that providers in this sample (n = 827) care for an average of 2.02 children, and adult:child ratios were on average 2:1. These findings are consistent with other literature (Layzer & Goodson, 2003; Maxwell & Kraus, 2002; Porter, Rice, & Mabon, 2003). Contrary to most of the literature on FFN child care, the providers in this sample were mostly aunts and not the child’s grandparent (Brown-Lyons et al. 2001; Shivers & Wills, 2001; Susman-Stillman & Banghart, 2008). While the majority of providers were related to the children in their care, 20% of the providers were not. Providers’ motivations for providing care are largely based on wanting to help the child’s family be self-sufficient 5 Arizona Kith and Kin Project Year 1 Evaluation Report and feeling a sense of emotional investment in the child. This finding is also consistent with the literature (Anderson et al., Brandon et al., 2002; Bromer, 2005; Porter et al., 2010; Shivers, 2003). We also found that a provider’s relationship to the children in her care was significantly associated with her motivation for providing child care. For example, aunts were more likely to report providing care in order to help the family. Grandparents were more likely to report providing care because of their emotional investment in the child, and non-relatives were more likely to provide care because they viewed providing child care as a source of income. Community-based efforts to enhance the quality of FFN child care will be successful if they can build upon these unique features of FFN caregiving arrangements such as low group sizes, low ratios, and personal investment in children (Brandon, 2005). This group of child care providers demonstrated flexibility in both scheduling and payment arrangements. About half of the providers in this sample provided child care during “traditional” child care hours. About a quarter provided care during evenings and weekends. The remaining quarter had care arrangements that included both traditional and nontraditional hours. While almost 60% of providers in this sample do not get paid for the care they provide, the majority of these providers reported having arrangements that included providing child care in exchange for other services, such as groceries, getting other household bills paid, child care exchange with their own children, etc. These findings are consistent with other literature (Brandon, 2005; Shivers, 2003). It is also noteworthy that an overwhelming 98.5% of providers in this sample do not receive child care subsidy reimbursement. This finding is consistent with other research on child care providers from immigrant communities (Chase, 2008; Yoshikawa, 2011). Findings from demographic surveys (n = 827) revealed that 90% of the providers identify as Latino and of those, 96% report having Mexican-heritage. While we did not collect data on immigration or citizenship status, we know that the average amount of time providers have lived in the U.S. is 13 years, which indicates that this project has successfully recruited and served a largely immigrant population. In addition, the project included three sites, which were aligned with Somali, Nepali, and Bhutanese refugee communities. Obtaining high recruitment and participations rates for marginalized FFN providers is traditionally a concern with which many community agencies struggle (Powell, 2008). However the large numbers of providers who participated in this year’s program (more than 900) and the existence of waiting-lists at several sites in the South Phoenix Region indicate that this project has been successful at reaching a hard-to-reach population of child care providers. Increases in Key Quality Outcomes We found statistically significant increases on almost all of our key quality indicators: r r r r r r Health and safety scores Materials in the physical environment Provider-child communication patterns Provider engagement Learning activities (see tables below) Providers’ basic knowledge about child development. In addition, we found that those providers who started out with the lowest scores made the largest increases. We also found that providers who were younger and relatively new to the U.S. made most gains. 6 Arizona Kith and Kin Project Year 1 Evaluation Report Caregiver communication to child 100 90 80 70 60 50 40 59 36 41 34 36 30 20 10 0 26 26 18 Responds 22 51 Time 1 Time 2 19 18 Requests language Verbally directs Repeats or builds Names or labels "Other" talk Focus-child communication 100 90 80 70 60 49 54 Time 1 Time 2 50 40 30 23 13 20 10 0 16 22 4 With caregiver Self-talk Other children 6 Other adults Participant Feedback Feedback from participants was overwhelmingly positive. The most influential workshops were related to issues of health and safety. This finding is consistent with findings from observations of providers’ homes using the Health and Safety Checklist, where health and safety scores significantly increased. Providers reported many changes in their interactions with children. The most commonly reported changes were in the areas of positive discipline and more reading activities. 95% of providers reported that they kept coming back to the trainings week after week because of a desire for more knowledge. In fact, 65% reported that it was “very likely” that they would pursue additional training once the project ended. About half of the providers reported a desire to be connected to more formal systems such as licensing, the food program, or the child care subsidy program. 7 Arizona Kith and Kin Project Year 1 Evaluation Report Discussion For the past 15 years, the Arizona Kith and Kin Project through the Association for Supportive Child Care (ASCC) has been providing training and outreach to Family, Friend and Neighbor (FFN) child care providers. Not only is this project well noted among early childhood professionals in Maricopa County and the state of Arizona, but this project has also garnered national attention for the work they do. For the past ten years, project leadership staff at ASSC has worked with others across the country to raise awareness of FFN child care issues. In addition, the work of the Arizona Kith and Kin Project has been featured in nationally disseminated publications and national conference presentations. Despite this list of accolades, this is the first in-depth evaluation of the Arizona Kith and Kin Project that included pre and post observations as well as extensive data collection on the demographics, beliefs and motivations of its participants. Positive findings from this evaluation suggest that the Arizona Kith and Kin Project is an effective strategy for reaching Family, Friend and Neighbor providers and increasing their quality of care. As Arizona moves toward building a system where ALL children have access to high-quality, culturally responsive early care and education that promotes their development, many are considering whether providing support and training for Family, Friend and Neighbor– or Kith and Kin child care providers – fits into this vision. It is clear from this data and other data throughout the country that children are spending a considerable amount of time in these arrangements while parents work. In addition, we know that providers are paid, and receipt of payment makes this a serious employment activity. From a public policy, workforce, and social justice perspective it is imperative that we view this substantial portion of caregivers as part of our early care and education workforce and worthy of our investments in quality improvement (Brandon, 2005). 8 Arizona Kith and Kin Project Year 1 Evaluation Report References Anderson, S., Ramsburg, D., & Scott, J. (2005). Illinois study of license-exempt care. Urbana-Champaign, IL: University of Illinois at Urbana-Champaign. Brandon, R. N. (2005). Enhancing family, friend and neighbor caregiving quality: The research case for public engagement. Seattle, WA: University of Washington, Human Services Policy Center. Bromer, J. (2005). Ways of caring: How relative caregivers support children and parents. In R. Rice (Ed.), Perspectives on family, friend and neighbor child care: Research, programs and policy (pp. 14-21). New York: Bank Street College of Education. Brown-Lyons, M., Robertson, A., & Layzer, J. (2001). Kith and kin—informal child care: Highlights from recent research. New York: National Center for Children in Poverty. Chase, R. (2008). State policies for supporting family, friend, & neighbor care: BUILD initiative policy brief. Wilder Research. Layzer, J.I., & Goodson, B. D. (2006). National Study of Child Care for Low-Income Families – Care in the Home: A Description of Family Child Care and the Experience of Families and Children That Use It. Wave 1 Report. Cambridge, MA: Abt Associates. Maher, E. J. (2007). Measuring quality in family, friend, and neighbor care: Conceptual and practical issues. New York: Columbia University Mailman School of Public Health National Center for Children in Poverty, Child Care and Early Education Research Connections. Ocampo-Schlesinger, S., & McCarty, V. (2005). The Arizona kith and kin project. In R. Rice (Ed.), Perspectives on family, friend and neighbor child care: Research, programs and policy (pp. 22-25). New York: Bank Street College of Education. Paulsell, D., Porter, T., Kirby, G., Boller, K., Martin, E., Burwick, A., Ross, C., & Begnoch, C. (2010). Supporting quality in home based child care: Initiative design and evaluation options. Princeton, NJ: Mathematica Policy Research, Inc. Porter, T. (2007). Assessing initiatives for family, friend and neighbor child care: An overview of models and evaluations. New York: Columbia University Mailman School of Public Health, National Center for Children in Poverty, Child Care and Early Education Research Connections. Porter, T., Nichols, T., Del Grosso, P., Begnoche, C., Hass, R., Vuong, L., Paulsell, D. (2010a). A compilation of initiatives to support homebased child care. Washington, D.C.: Mathematica Policy Research. Porter, T., Paulsel, D., Nichols, T. Begnoche, C., Del Grosso, P. (2010b). Supporting quality in home-based child care: A compendium of 23 initiatives. Washington, D.C.: Mathematica Policy Research. Porter, T., Rice, R., & Mabon, S. (2003). Doting on kids: Understanding quality in kith and kin child care. New York: Bank Street College of Education. Powell, D. (2008). Who’s watching the babies? Improving the quality of family, friend and neighbor care. Washington, DC: Zero to Three. Shivers, E. M. (2003) Where the children are: Predicting provider-child relationships in informal (kith and kin) child care settings. Dissertation Abstracts International Section A: Humanities & Social Sciences. Vol. 65 (1-A), 64. Shivers, E., & Wills, S. (2001). License-Exempt Assistance Project Final Report – 2001. Los Angeles, CA: Crystal Stairs, Inc. Shivers, E. M., Ocampo-Schlesinger, S., & Wilkins, S. (2010). Findings from the Arizona Kith and Kin Project. Field presentation at Zero the Three’s National Training Institute, Phoenix, AZ. Sussman-Stillman, A., & Banghart, P. (2008). Demographics of family, friend and neighbor child care in the United States. New York: Child Care and Early Education Research Connections. Yoshikawa, H. (2011). Immigrants raising citizens: Undocumented parents and their young children. New York, NY: Russell Sage. 9 Arizona Kith and Kin Project Year 1 Evaluation Report Introduction Background The prevalence of child care provided by informal caregivers – also increasingly referred to as “Family, Friend and Neighbors” (FFN) – has been well documented by researchers over the past six years (Brandon & Matinez-Beck, 2006; Cappizzano & Adams, 2003; Kids Count, 2006; Sussman-Stillman, 2008). This is a common child care arrangement for many young children in the U.S., especially those from low-income families, families of color, and infants and toddlers (Brandon, 2005; Porter, Paulsell, Del Grosso, Avellar, hass, Vuong, 2010). FFN child care is usually defined as: any regular, nonparental child care arrangement other than a licensed center, program, or family child care home; this care thus includes relatives, friends, neighbors, and other adults (Brandon, Maher, Joesch, Battelle, & Doyle, 2002). Because of the informal nature of this type of child care, it is difficult to track the exact numbers of children in these types of care arrangements. National studies report that the number of children in child care provided by a relative range from 20% to 40% of all children under the age of five (Boushey & Wright, 2004; Capizzano, Adams, & Sonenstein, 2000; Johnson, 2005). Studies also report that six percent of children under the age of five are in child care provided by non-relatives (Cappizano et al., 2000; Tout, Zaslow, Papillo, Vandivere, 2001). Convenience, affordability, and access are often cited as the main reasons parents select this type of child care arrangement for their children (Brandon, 2005; Kids Count, 2006; Porter et al., 2010). However research also indicates that other factors such as preference, trust, personal comfort, culture, and relationships also have important influences on parents’ choices (Brandon, 2005; Porter et al., 2010; Susman-Stilman & Banghart, 2008). As researchers have discovered increasing links among children’s early experiences and early environments on concurrent and future developmental outcomes, there has been a corresponding increase in the number of statewide quality improvement initiatives (Child Trends, 2010). Unfortunately, even with strong research evidence about the benefits of high quality center-based care – particularly for low-income children, and visionary systems-building, we have still not attracted enough public financial support to make high quality center-based care available for all children who need it and all parents who want it (Kids Count, 2006). Policy makers have argued that while it is paramount that we expand the financial support required to scale up effective evidence-based quality child care programs and improve access for low-income families, it is also important to recognize that much can be gained by going to where the children are, and increasing training and support for family, friend and neighbor child care providers (Adams, Zaslow, & Tout, 2006; Brandon, 2005; Chase, 2008). Researchers have also documented the uneven and low quality present in many FFN child care settings that may have an adverse impact on children’s and families’ development (Fuller, Kagan, Loeb, & Chang, 2004; Maher, 2007; Polakow, 2006; Porter et al., 2010). Rather than viewing these concerns as an argument against greater support for FFN care, child advocates and policy makers argue that evidence of low quality in FFN settings underscores the need to pay even more attention to strategies that can improve it – particularly in light of the reality that FFN care will likely continue to play a significant role in the lives of children most at risk for not being ready for school (Chase, 2008; Emarita, 2007; Kids Count, 2006). Evaluation Rationale There is a great need for more research and evaluation on Family, Friend and Neighbor (FFN) child care (Paulsell et al., 2010; Porter et al., 2010). Despite the importance of quality child care experiences for children's present and future well being, relatively little research has explored practices that are effective with this group of caregivers. This is mostly due to the many challenges involved with conducting research and evaluations on FFN child care initiatives. Challenges may include sample variability, inadequate theoretical frameworks, recruitment issues, methodology concerns, and a limited ability to generalize results. Nevertheless, it is imperative that we gain a deeper understanding of the link between FFN child care quality and children’s developmental outcomes. While we have decades of research that has indicated which aspects of formal child care are predictive of children’s future and concurrent social and emotional outcomes, we have yet to discover components of FFN child care that are distinct from more formal care, as well as predictive of children’s current and future success. Our goal for this study was to pilot an evaluation that would attempt to meet several objectives: 1) inform the project’s 10 Arizona Kith and Kin Project Year 1 Evaluation Report ongoing design and implementation; 2) add to the field of literature on effective strategies for quality enhancement for FFN providers; and 3) provide findings that could guide our state’s efforts to build a comprehensive system of professional development for the entire continuum of child care providers. Description of the Arizona Kith and Kin Project The Arizona Kith and Kin Project is implemented under the auspices of the Association for Supportive Child Care (ASCC), a nonprofit child care agency that was founded in 1976 to improve the quality of care for Arizona children. ASCC oversees the Arizona Kith and Kin Project as well as 13 other programs. The project is funded primarily through a grant from First Things First, although there are six other sites that have received funding from other sources. The program was established in 1999 to provide ongoing early childhood training and support to exempt family, friend, and neighbor caregivers. The goals of the Arizona Kith and Kin Project are to (1) improve the quality of child care through training; (2) increase caregiver’s knowledge and understanding of early child development; and (3) increase caregiver’s knowledge and understanding of health and safety issues to provide a safer child care environment (See Appendix A for Logic Model). Format The Arizona Kith and Kin Project provides a 14-week, two-hour support group training series for Spanish and English-speaking and refugee caregivers. Most training sessions are offered only in Spanish. The initiative provides transportation for caregivers who are located within a five-mile radius of the training location and on-site child care by trained child care providers during each training session. Most training sessions are offered during the day and sometimes the evening. In the 2010 funding year, The Arizona Kith and Kin Project offered training at 55 locations, including four sites in Coconino County and six sites in Yuma County. The training sessions are held at various Head Start centers, faith-based organizations, public libraries, elementary schools, and local community centers that have an adjoining space for child care. Child care during the training sessions is offered by caregivers from community partner agencies, who regularly provide care for different groups of children for other activities such as Head Start parent meetings or policy councils, or by caregivers who have “graduated” from the Arizona Kith and Kin Project. These on-site child care providers receive 12 hours of annual training, and are supervised by a Specialist with a college degree and experience in early childhood education. The Arizona Kith and Kin Project holds a fall cycle and spring cycle at each site. Caregivers may join a cycle at any time during the first seven weeks. When the 14-week training session ends, participants receive a certificate that indicates the number of training hours they received. They are not required to return for the following cycle, but many participants do. Typical groups average 15 caregivers, but some can have up to 20. In the 2010 funding year the project served a total of 1,315 providers. Valley of the Sun United Way; Bank of America; the City of Tempe; Arizona Republic; Channel 12 Season of Sharing; JP Morgan Chase. There were two groups with refugee child care providers. One group was comprised of providers from Somalia. The other had refugee providers from Bhutan and Nepal. There were translators at both groups. 2 3 11 Arizona Kith and Kin Project Year 1 Evaluation Report Curriculum The following subjects are covered during the 14-week support group training series; some topics span multiple weeks: Child Development / Ages and Stages Daily Schedule Planning Nutrition Parent/Caregiver Relationships Arranging the Environment Language and Literacy (including a Reading Is Fundamental (RIF) book event and distribution) Brain Development Health and Safety First Aid CPR Child Passenger Safety Guidance and Positive Discipline financial as s is tance to low-to moderate income individuals to start a child care business in their homes and complete state certification. Interested providers also receive technical assistance to qualify and enroll in ASCC’s Food Program (Child and Adult Care Food Program). Injury Prevention The Arizona Kith and Kin Project includes a strong injury prevention component. As part of the 14-week sessions, participants attend a Car Seat Training with instructions on proper safety seat installation. After the training, participating caregivers can schedule an appointment with the program to receive free car seats. The program distributes an average of 2.5 car seats per caregiver. Similarly, there is also a separate Crib Safety/Safe Sleep Training class available to participants where providers learn about crib safety and creating a safe sleep environment. After completing the class, and if requested a Specialist delivers a crib to providers’ homes and safely assembles it. Every year, the Arizona Kith and Kin Project hosts an Annual Health and Safety Training Conference for family, friend, and neighbor caregivers. The conference is held on a Saturday in each county. During the conference, the project A workshop on conference, the project also provides outlet covers and smoke alarms, as well as other health and safety related items. In addition, community exhibitors are invited to set up tables displaying resources and information for other community events and opportunities. The Arizona Kith and Kin Project provides transportation to enable caregivers to attend. In the funding year for 2010, over 250 FFN providers attended the conference. Provider Recruitment: Strong Community Partnerships The Arizona Kith and Kin Project’s approach to participant recruitment is based on a history of developing strong partnerships with other community-based entities that are trusted by residents of those neighborhoods and communities. Examples of such partners include: local Head Start sites; elementary schools; faith-based organizations; children’s museums; and other community agencies. Another important strategy for recruitment is involving an individual community partner as a co-facilitator during the training. 12 Arizona Kith and Kin Project Year 1 Evaluation Report Staf ng responsible for providing training to the participants, a coordinator, an assistant coordinator, on-site child care Specialist, and administrative assistant. Part-time employees included 30 community co-facilitators and 43 on-site child care providers. Eight Arizona Kith and Kin Specialists served as facilitators for the training sessions. All the Specialists were female and bilingual. Their background quali cations included a four-year degree in child development, early childhood education, or related eld (AA degree and eight years of related work experience could be substituted for educational background). Upon being hired by the Arizona Kith and Kin Project, Specialists receive training in the areas of: Child passenger seat safety CPR and First Aid Brain development Attachment theory Language and literacy Group facilitation Adult learning theory Specialists receive on-going in-service training every six months – during winter break and summer break. They also attend trainings provided by ASCC on a variety of other topics related to early childhood development and education. They also have opportunities to attend conferences. Theory of Change Kin Project. Carol Weiss (1972) popularized the term "Theory of Change" as a way to describe the set of assumptions that explain both the steps that lead to the long-term goals of interest, and the connections between program activities 1. Quality child care positively impacts children’s school readiness. 2. Positive, nurturing relationships with caregivers help a child succeed in school and in life. 3. For home-based child care, much of what we consider to be “quality” resides within the control of the provider. 4. It takes more than mere exposure to child development content to impact child rearing practices. The Logic Model is displayed in Appendix A, and the conceptual model for the theory of change is displayed in Appendix B. It is considered to be a work in progress, and will likely be revisited at the end of each project year, as ndings from the evaluation prompt a deeper understanding of process and outcomes. Purpose of Evaluation The purpose of this evaluation was to discover whether the Arizona Kith and Kin Project was successful in reaching its desired outcomes – that is, whether there were demonstrable changes in participants’ beliefs, practices with children, and environmental quality. Speci c research questions are as follows: 13 Arizona Kith and Kin Project Year 1 Evaluation Report FULL SAMPLE Research Question 1: What are providers’ previous experiences with child care and personal investments in child care training and education? Research Question 2: What are providers’ conditions of caregiving (e.g., hours worked; group size; payment arrangements; etc.) Research Question 3: What are providers’ motivations for caring for children and their beliefs about children’s parents? Research Question 4: Is there an increase in child development knowledge after completing the training sessions? Research Question 5: What were participants’ experiences and ratings of their experiences in the Arizona Kith and Kin Project? FOCUSED SUB-SAMPLE Focused Sub-Sample: Research Question 1: What are the background characteristics of providers in the focused subsample? (e.g. demographics; conditions of caregiving; motivations and beliefs about parents) Focused Sub-Sample: Research Question 2: How do providers’ scores on various indices of well-being and support change after completing the Arizona Kith and Kin Project? Focused Sub-Sample: Research Question 3: How do providers’ scores on various indices of quality change after completing the Arizona Kith and Kin Project? Focused Sub-Sample: Research Question 4A: Are providers’ background characteristics associated with quality outcome scores at Time 2? Focused Sub-Sample: Research Question 4B: Are providers’ background characteristics associated with the amount of change in quality scores from Time 1 to Time 2? 14 Arizona Kith and Kin Project Year 1 Evaluation Report Methods Evaluation Design This evaluation is primarily a summative outcome evaluation, which used performance measures based on the project developers’ theory of change and child care research on effective professional development for infant and toddler caregivers. The purpose of this evaluation is three-fold: first and foremost, the goal is to determine whether the Arizona Kith and Kin Project met its stated objectives and outcomes. Second, the evaluation is designed to provide insight and feedback to the program’s developers as they move forward to bring the program to scale. Third, the research on effectiveness of Family, Friend and Neighbor professional development initiatives is sparse. Findings from this evaluation will likely point to many other research questions that researchers and future evaluations can explore in order to push the field toward a deeper understanding of FFN professional development models, provider outcomes, and ultimately, incorporating FFN initiatives into states’ larger professional development systems. Limitations of the Data There are several serious limitations in this evaluation. We cannot, with ultimate confidence, state that the observed changes are a direct result of the Arizona Kith and Kin Project. Limitations are listed below: r There is a self-selection bias insofar as the Arizona Kith and Kin Project was a service for which FFN providers volunteered. It may be that seeking out this type of experience is a characteristic of providers who are already offering a higher quality experience for children and families. r This is a non-experimental design, with the same group of providers serving as their own comparison group through the use of a pre-post design. There is no randomized control group, and participants were not randomly recruited, which makes causal and generalizeable statements harder to ascertain than when using randomized recruitment and an experimental design. r The same Specialists who facilitated the training sessions collected observational data in providers’ homes. One of the most challenging aspects of conducting research and evaluation with r FFN providers is gaining entry into providers’ homes (Porter & Paulsell, 2010). In order for us to successfully recruit a sample of providers who would allow us into their homes, we had to use data collectors whom they already knew and trusted. As a result, providers’ training facilitator collected all of the Time 1 observational data. As a rule, a different Specialist collected Time 2 observations. In some instances providers would only allow their training facilitator into the home at Time 2. Although we controlled for this potential bias in the analysis (Burchinal, 2010), there is a possibility that the results were impacted by this limitation in our data collection design. r Questionnaire responses are self-reported and not verified by observation. One assumes a response bias on the part of caregivers to provide socially desirable responses and present oneself in the best possible light. r The sessions provided by the Arizona Kith and Kin Project Specialists were designed to be adapted according to the ebb, flow and interests of the providers present at each session. The hallmark of effective adult learning strategies is tailoring the mix and intensity of activities, topic content and discussion to the unique needs of the providers present in each session (Speck, 1996). Consequently, the intervention was not identical in all sites. 15 Arizona Kith and Kin Project Year 1 Evaluation Report Description of Participants Providers 827 child care providers participated in the full sample evaluation. The demographic characteristics of this sample are detailed in the tables below. Table 1: First Things First Regions Frequency Percent Central Phoenix 352 42.6 South Phoenix 196 23.7 North Phoenix 68 8.2 Southwest Maricopa 116 14.0 Coconino County 43 5.2 Yuma County 48 5.8 4 .5 827 100.0 Other Total Table 2: Provider Age Frequency Percent 0-19 20-29 17 206 2.1 25.9 30-39 340 42.7 40-49 50-59 60-69 70+ 168 44 20 1 21.1 5.5 2.5 .1 Table 3: Provider Sex Male Female Frequency Percent 30 751 3.8 96.8 Table 4: Racial and Ethnic Background White, not Hispanic African American or Black, not Hispanic Hispanic American Indian or Alaska Native Asian or Pacific Islander Other 16 Frequency Percent 22 24 690 21 7 4 2.9 3.1 89.9 2.7 .9 .5 Arizona Kith and Kin Project Year 1 Evaluation Report Table 5: Ethnic Background – Country of Origin Frequency Percent 688 18 7 6 3 3 1 726 94.8 2.5 1.0 .8 .4 .4 .1 100 Mexico Guatemala Mexican American El Salvador South America Central America Puerto Rico Total Table 6: Number of years living in the U.S. Minimum Maximum Mean Std. Deviation .50 67.00 12.57 7.29 Number of years living in the U.S. Table 7: Provider Household Income* Frequency Percent 229 135 88 65 46 31 13 12 3 6 5 1 86 31.8 18.8 12.2 9.0* 6.4 4.3 1.8** 1.7 .4 .8 .7 .1 11.9 Less than $10,000 $10,000-$14,999 $15,000-19,999 $20,000-24,999* $25,000-29,999 $30,000-34,999 $35,000-39,999** $40,000-44,999 $45,000-49,999 $50,000-59,999 $60,000-74,999 $100,000 or more Decline to answer *71.6% of this sample is at 100% Federal Poverty Level for family of four. **84.1% of this sample is at 175% Federal Poverty Level for a family of four. Table 8: Work in addition to providing child care No Yes Frequency 640 118 Percent 84.4 15.6 Table 9: Providers’ Marital Status Single Married Living with significant other Divorced or separated Widowed Frequency Percent 91 437 169 55 10 11.9 57.3 22.2 7.2 1.3 17 Arizona Kith and Kin Project Year 1 Evaluation Report Evaluation Procedures This evaluation had two main components – data collection with all participants and data collection with a smaller, targeted sample of participants. All participants were asked to complete a background questionnaire at the beginning of the project, pre and post child development tests, and feedback surveys at the end of the project. For the smaller, targeted sample, Specialists asked for volunteers during the first week of classes. Providers were informed about the purpose of the focused evaluation, timeline for observations in providers’ homes, and incentives for participation. Upon agreeing to participate, the Specialist then collected their name and phone number and contacted them to make an appointment for the observation visit. (See Results section for attrition rate with targeted sample.) Once Specialists arrived to the home of the provider, they were instructed to read and complete a consent form. The baseline data (Time 1 data) was collected within three weeks of enrollment into the Arizona Kith and Kin Project. At the end of the project, providers were once again contacted by their specialist who informed them that a different observer would be completed the second observation (Time 2). In some instances, providers would not provide consent for the visit unless the visit was conducted with their original Specialist. In order to prevent attrition, we complied with their request. Incentives for participation included: a $20 gift certificate for Wal-Mart and a bag of toys and materials for the children. Toys and materials were from Lakeshore Learning Materials. These incentives were given only at the second data collection visit. Data Collection and Instrumentation Data were collected through questionnaires, observations, and surveys. A summary of the instruments used and the information collected is included below as Table 10. 18 Arizona Kith and Kin Project Year 1 Evaluation Report Table 10: Overview of Evaluation Measures* Instrument Citation Constructs Measured Respondent When Collected Child Care Assessment for Relatives (CCAT-R) Caregiver Interview (Porter et al., Institute for Child Care Continuum, 2003) Demographics Conditions of Care; Motivation for Providing Care; Beliefs About Parents (Structured questions) Full Sample Baseline Child Development Pre/ Post Test (Ocampo & Ortiz, 1999) Knowledge about basic elements of child development. Items correspond to content covered in workshops. Full Sample Completion of program (Shivers, 2010) Providers’ perceptions of effectiveness of training and Specialists (Likert rating). Open-ended responses probe for feedback on what providers learned and how project can improve. Full Sample Feedback Survey Baseline; Completion of program Measures used with sub-sample during data collection in providers’ homes CCAT-R Caregiver Interview (Porter et al., Institute for Child Care Continuum, 2003) Conditions of Care; Relationships With Parents; Routines With Children (Structured questions) Baseline; Sub-Sample CCAT-R Action and Communication Snapshot Time sampling methodology captures caregiver (Porter et al., Institute communication with focus child; caregiver action; child for Child Care language; child interactions with children and adults (ObservaContinuum, 2003) tion completed in provider’s home) CCAT-R Behavior Checklist Checklist completed after each snapshot page. Categories (Porter et al., Institute include: Location; caregiver tone; child tone; child learning for Child Care Conactivities; toileting/diapering; caregiver interaction with child; tinuum, 2003) behavior management; child safety (Observation conducted in provider’s home) Sub-Sample CCAT-R Health and Safety Checklist (Porter et al., Institute Checklist identifies the health and safety features of the home. for Child Care Main categories are: food preparation; environment; routines; Continuum, 2003) outdoor play (Observation completed in provider’s home) Sub-Sample CCAT-R Materials Checklist (Porter et al., Institute Checklist identifies play and learning materials/equipment for Child Care present in caregiving environment. Does not measure quantity. Continuum, 2003) Caregiver Interaction Scale (CIS/Arnett) Completion of program Baseline; Sub-Sample Completion of program Baseline; Completion of program Baseline; Completion of program Baseline; Sub-Sample Completion of program Baseline; (Arnett, 1987) Widely used observational tool capturing provider’s global relationships with children in care (26 items – 3 subscales: sensitivity; harsh; detached) (Observation in provider’s home) Sub-Sample Perceived Financial Needs (Dunst & Leet, 1994) Providers’ perceptions of how well their material needs are met (Likert rating; scale of 0-4) Sub-Sample Parent’s Use of Social Support (F-COPES) (McCubbin & Patterson, 1982) Providers’ ratings of how they solve problems and to whom they turn for emotional, social and instrumental support Sub-Sample Child Rearing Attitudes (Block, 1965; Kontos et al., 1995; Rickel & Biasatti, 1982) Providers’ ratings of child rearing practices they endorse (Likert rating; 1-7) Sub-Sample Completion of program Baseline; Completion of program Baseline; Completion of program Baseline; Completion of program *For more detailed information about individual measures, please contact the author of this report. 19 Arizona Kith and Kin Project Year 1 Evaluation Report Analyses Items in each of the data sets listed above were initially examined for accuracy and consistency. Problematic data in the electronic files were assessed against the original hardcopy forms. Summary scales were created for the standardized instruments (e.g., F-COPES, CIS/Arnett). Where applicable, measures were merged across data sets (e.g., Provider background characteristics; Feedback Surveys; Pre and Post-Tests). Analyses followed standard methods in applied social research. Item and scale frequencies were generated along with relevant summary statistics (counts, percentiles, means, medians and dispersion indexes). Bivariate procedures were selected based on levels of measurement. For example, with continuous measures Pearson’s moment correlations were performed; t-tests were used with two-category predictors and interval-level dependent variables. Where relevant, coded themes from open-ended, qualitative responses gleaned from surveys were integrated throughout the results section to highlight quantitative findings. Finally, based on a hypothesized theory of change, multivariate regression models were created and performed. Training and Reliability In the summer of 2009, Toni Porter from the Institute for a Child Care Continuum at Bank Street College of Education trained ASCC Specialists and the Program’s evaluator to use the Child Care Assessment Tool for Relatives (CCAT-R). The CCAT-R is a well-known assessment tool that measures various elements of child care quality, and was specifically developed for Family, Friend and Neighbor child care providers. Like other well-known time sampling measures, it measures the frequency of interactions between the caregiver and the focal child with time sampling. These interactions include talk within the caregiver-child dyad, as well as among the child, the caregiver, and other children and adults; the caregiver’s engagement with the child; and the child’s engagement with materials and other children or adults in the setting. In addition, the CCAT-R includes items related to affect of the caregiver and the child; the types of caregiver and child activities that occur; and disciplinary practices. The CCAT-R training consisted of one day of classroom work as well as practice on three videotaped observations. On the second day, two teams of a trained observer and three project members conducted reliability observations on home-based child care providers. Additional practice sessions on the videotaped observations were held in the afternoons. At the conclusion of the training, all but two of the staff had achieved the CCAT-R standard of reliability of .80 exact agreement on individual items. During the next two weeks, the program’s evaluator trained the other two staff with the practice videos as well as on-site observations to help them become reliable. The program’s evaluator conducted the same reliability training for all new staff that subsequently joined the Arizona Kith and Kin Program. After initial reliability training, every six months the principal investigator for the evaluation conducted reliability checks consisting of live visits with a caregiver and young child. Reliability observations are repeated until all program staff achieved .80 exact agreement on individual items. 20 Arizona Kith and Kin Project Year 1 Evaluation Report Results SECTION I: FULL SAMPLE (n = 827) Research Question 1: What are providers’ previous experiences with child care and personal investments in child care training and education? Research has demonstrated wide variability in the caregiving experiences of family, friend and neighbor child care providers (Porter et al., 2010). However, there is not as much variability in levels of education and formal training in the field of early childhood development and education. Levels of formal education are usually lower than regulated providers (Brown-Lyons et al., 2001; Sussman-Stillman, 2008). Eighty-one percent of providers have a high school diploma or less. Lower levels of education might be indicative of the large number of providers in this sample who grew up in other countries where economic conditions made education less accessible. Eighteen percent of providers had at least some exposure to college courses. Previous research has found positive associations between previous exposure to formal child care settings and positive provider and child outcomes (Shivers, 2003; Shivers, 2006). In this sample, 35% of providers reported previous exposure to formal settings. We hypothesized that here too we would discover positive associations between exposure to formal settings and materials and interactions with children. This analysis is described in Section II of the results. Table 11: Number of years as a child care provider How long have you taken care of other people's children in your home? (in years) Minimum Maximum Mean SD .00 37.00 4.89 6.09 Table 12: Provider education Frequency Percent 12 1.6 Elementary School 182 23.9 Middle/Junior High School 177 23.2 Some High School 118 15.5 High School diploma or equivalent 127 16.7 Some college courses 83 10.9 Two-year college degree 18 2.4 Four-year college degree 34 4.5 Some graduate school 3 .4 Graduate degree 8 1.0 762 100.0 No schooling Total 21 Arizona Kith and Kin Project Year 1 Evaluation Report Table 13: Previous exposure to training Frequency Percent No 388 50.4 Yes 382 49.6 Total 770 100.0 Table 14: Caregiver previous exposure to formal child care settings Frequency Percent No 498 64.8 Yes 271 35.2 Total 769 100.0 Table 15: Type of program for those caregivers with previous exposure Frequency Percent Head Start 97 36.1 Family Child Care Home 83 30.9 Child Care Center 39 14.5 Church Child Care 8 3.0 Elementary School Classroom 14 5.2 School Volunteer 12 4.5 Other 16 5.9 Total 269 100.0 22 Arizona Kith and Kin Project Year 1 Evaluation Report Research Question 2: What are providers’ conditions of caregiving (e.g., hours worked; group size; payment arrangements; etc.) Very little is known about family, friend and neighbor providers’ conditions of providing child care in Arizona. These descriptive analyses are meant to provide a snapshot of how and with whom providers are arranging their care with children. The variables examined in this section create a landscape for examining another context of children’s development. Knowing the characteristics of this group of providers is an important factor in guiding and informing the content and mode of delivery of the Arizona Kith and Kin Project. In addition, there are prevailing notions about FFN providers that have affected the ways in which child care policy in Arizona and around the country is constructed and implemented (Schulman & Blank, 2007; Susman-Stillman & Banghart, 2008). Understanding the diverse ways in which FFN providers organize their child care is paramount if equitable and effective decisions regarding the children experiencing this type of care are to be made. Tables 16-21 display details related to the conditions of caregiving. The average number of children (6 years and younger) cared for by providers in this study was 2.02 (SD = 1.23). This is slightly less than findings from several other national studies that examined unregulated care (Layzer & Goodson, 2003; Maxwell & Kraus, 2002; Porter, Rice, & Mabon, 2003), but slightly larger than some smaller studies (Anderson et al., 2003; Brandon et al., 2002; Shivers & Wills, 2001). Literature from other studies on non-regulated/relative care indicates that large numbers of parents select FFN care for their infants and toddlers (Brandon, 2005; Paulsell, et al., 2006). In this study 74.7% of providers reported having infants and toddlers in their care. This number is consistent with other studies (Anderson et al., 2003; Brandon, 2005; Maher & Joesch, 2005; Tout et al., 2001). Average child:adult ratios in this sample were 2:1. Research has demonstrated that ratios are consistently lower (usually better) for FFN than other types of early care settings. For example, an analysis of NHES 1999 data shows that for children between birth and age five, center-based care has an average child:adult ratio of 6.5:1, formal family child care of 3.5:1 and FFN care an average of 1.5:1. While ratios in centers increase greatly as children go from infant, to toddler, to preschool age, they increase only slightly for children in FFN care (Maher, 2005). These consistently low child:adult ratios are a measure of quality that is highly visible and important to many parents. Many have hypothesized that low ratios in FFN care is a strength upon which to build even more positive relationship building among providers, parents and children (Bowman, Donovan, Burns, 2001; Kids Count, 2006; Porter et al., 2010; Shivers, 2003). Research on FFN characteristics finds that grandmothers are the most common relative caregivers (Brown-Lyons et al. 2001; Shivers & Wills, 2001; Susman-Stillman & Banghart, 2008). However, in our sample we found that 40% of the caregivers were the Aunts of the children in their care. Grandmothers comprised only 14% of the caregivers. Consistent with the literature, the majority of caregivers were related to the children in their care – almost 59% (Porter et al., 2010). Interestingly, mere acquaintances or “conocidos” made up almost 20% of the caregivers in this sample. It would be important to explore the implications of this finding a little further. Are families placing their children in the care of conocidos because they do not have access to or trust other forms of child care? What are the implications for provider-parent communication when the parents do not know their providers very well? What are the implications for children when the parents do not know their providers very well? How can programs like the Arizona Kith and Kin Project work to forge effective communication between parents and their conocido providers? In our sample, the percent of providers caring for children during evening and weekend hours is 51.5%. This percentage is similar to reports from other states (Brandon et al., 2002; HSPC 2002-2004). We found that 58.7% of providers in this sample do not get paid for the care they provide. Nonrelatives were significantly more likely to receive payment from families for providing care. This pattern is consistent with other studies (Bromer, 2005; Brown-Lyons et al., 2001; Folk, 1994; Susman-Stillman, 2008). In our sample, the average amount of weekly pay a provider receives per child is $34.23. Research on FFN payment has determined that the payment rates are often a mixture of a market service rate and an understood family arrangement, which often involves bartering (trading of services like buying groceries, exchanging child care, or cleaning one’s house) (Brandon, 2005; Shivers 2003). It is also noteworthy that an overwhelming 98.5% of providers in this sample do not receive child care subsidy reimbursement. Although it is unclear what percentage of providers in this sample were eligible for subsidies, the rate of subsidy take-up in this sample is extremely low. Studies suggest that most states deliver child care subsidies between 15% and 30% of the eligible population (Herbst, 2008; U.S. GAO Report, 2010). 23 Arizona Kith and Kin Project Year 1 Evaluation Report Table 16: Numbers of children in care by age group Minimum Maximum Mean SD Number of infants in care (0-12 mo) .00 2.00 .26 .47 Number of toddlers in care (13-35 mo) .00 5.00 .65 .76 Number of pre-schoolers in care (3-5 yr) .00 5.00 1.11 .97 Number of school age children (6 and above) .00 7.00 1.63 1.29 Largest number of children in care (under the age of 6 including their own children) .00 7.00 2.02 1.23 Table 17: Relationship to children in care Frequency Percent Aunt/Uncle 325 40.3 Grandparent 113 14.0 Cousin 26 3.2 Sister/Brother 10 1.2 Parent (others’ children not in care at this time) 95 11.8 154 19.1 Close friend of family 57 7.1 Neighbor 26 3.2 806 100.0 Acquaintance / “Conocido” Total Table 18: Hours of Care Frequency Percent Traditional (7:00 am – 6:00 pm; M-F) 301 47.7 Non-traditional (evenings and weekends) 184 29.2 Varies/Both 141 22.3 3 .5 629 100.0 Caregiver lives with child Total Table 19: Payment received for providing child care Frequency Percent No 440 58.7 Yes 309 41.3 Total 749 100.0 24 Arizona Kith and Kin Project Year 1 Evaluation Report Table 20: Total weekly payment amount for full-time care What is the total weekly amount of payment for all children in your care? Minimum Maximum Mean SD 8.00 250.00 60.53 39.05 Minimum Maximum Mean SD 3.00 140.00 34.23 28.34 Table 21: Weekly payment per child for full-time care Weekly payment per child (Full-time care only) 25 Arizona Kith and Kin Project Year 1 Evaluation Report Research Question 3: What are providers’ motivations for caring for children and their beliefs about children’s parents? We measured providers’ motivations for caring for children by using questions and categories from the Child Care Assessment Tool for Relatives (CCAT-R) Caregiver Interview. Providers were asked to select their primary and secondary reasons for why they provide child care for young children. The results in Table 22 below indicated that the top two reasons for caring for children were: “I want to help my family,” and “I love the child(ren), and want to spend time with him/her.” These two categories accounted for 56% of all responses. This finding is consistent with almost all the literature on FFN providers. Studies show that especially for low-income families, providers want to help family members become self-sufficient (Anderson et al., Brandon et al., 2002; Bromer, 2005; Porter et al., 2010; Shivers, 2003). We conducted a chi-square analysis to determine whether patterns of motivation were differentiated by providers’ relationships to the children in their care (Susman-Stillman, 2008). We found that grandparents were the most likely to be motivated by their relationship with the child(ren). Aunts were the most likely to be motivated by a desire to help out the child’s family. Friends who were close to the family were the most likely to be motivated by needing an income. And mere acquaintances or “conocidos” were the most likely to be motivated by a desire to work with young children in general. This pattern of distinction in motivations could have implications for level of “intentionality,” and might be associated with children’s experiences in care. For example, one might hypothesize that providers who enjoy working with young children in general might be more inclined to intentionally organize stimulating activities for children and more likely to seek training in child development and early education (Kontos et al., 1995; Shivers, 2003). One might also hypothesize that providers who are primarily motivated by deep affection and love for the child might be more likely to work harder to co-construct a positive relationship with the child (Porter et al., 2010). Table 22: Primary motivation for caring for children Frequency Percent I want to help my family 171 29.0 I love the child(ren), and want to spend time with him/her 160 27.2 I don't have any other job 88 14.9 I need the money 72 12.2 I enjoy working with children 68 11.5 I can do a better job than a “stranger” 30 5.1 589 100.0 Total 26 Arizona Kith and Kin Project Year 1 Evaluation Report SECTION II: TARGETED SUB-SAMPLE Research on observed FFN child care provider outcomes such as practices and quality is scarce (Paulsell, et al., 2010). Our goal in this section of the evaluation is two-fold. First, we wanted to provide descriptive information about FFN child care providers’ observed practices and quality. Second, we wanted to test whether there would be a change in observed practices and quality after providers completed the 14-week session. This study represents one of only a handful to use standardized observational data to discover whether a FFN child care initiative had an impact on provider practices and quality (Maher, 2007; Paulsell et al., 2010) Theoretical Framework for the Comprehensive Evaluation The broad theoretical framework from which these research questions flow has been informed by a theoretical framework that places children's development within ethnic and social class contexts and within relationships with others (Howes, 2000). This framework draws from Bronfenbrenner’s theory of human ecology (1979) and from more recent work that interprets the development of all children within a cultural and class context (Garcia Coll et al., 1996). The model is bi-directional, wherein, each level is assumed to influence the adjacent one. We hypothesized that provider outcomes – that is, increased or enhanced practices and quality – would be associated with variables from other layers of the ecological model like: background characteristics, conditions of caregiving; motivations / beliefs; indices of well-being (Howes, 2000; Shivers, 2003). The framework and the specific layers and contexts of development that we examined are illustrated in Figure 1. Researchers, practitioners, and policy makers are well-aware of the myriad challenges involved with recruiting FFN providers to participate in research and evaluation (Paulsell et al., 2010; Powell, 2008; Susman-Stillman, 2008; Whitebook, Phillips, Bellm, Crowell, Almaraz, & Young, 2004). For this targeted sub-sample, we recruited providers to participate on the first day of their session. Specialists explained the study and offered incentives. Specialists then followed up by calling each provider who expressed interest in participating in this aspect of the evaluation, and scheduled an appointment to conduct a 2-3 hour observation in the provider’s home. Our goal was to recruit 10% of the larger sample, and we accomplished our goal by initially recruiting 88 providers. However, our retention rate fell to 63% at Time 1 observations and to 28% by Time 2 observations, which resulted in 55 providers in our sample at Time 1 and only 25 in the sample at Time 2. We suspect that reasons for low retention rates included: scheduling difficulties; providers’ fear and distrust during heated community debates on immigration; and children and providers leaving town for the summer. Once Specialists arrived to the home of the provider, they gave a consent form to the provider to read and sign. The baseline data (Time 1 data) was collected within 3 weeks of enrollment into the Arizona Kith and Kin Project. At the end of the project, providers were once again contacted by their Specialist who informed them that a different observer would complete the second observation (Time 2). In some instances, providers would not provide consent for the visit unless the visit was conducted with their original Specialist. In order to prevent attrition, we complied with their request. Incentives for participation included: a $20 gift certificate for Wal-Mart or target and a bag of Lakeshore art and materials for the children. These incentives were given at the second data collection visit. 27 Arizona Kith and Kin Project Year 1 Evaluation Report Figure 1. Theoretical Framework: Ecological model for children’s experiences in Family, Friend and Neighbor child care ECE Policy Context: Child care subsidy policies; Quality and access; First Things First program implementation; School readiness awareness Cultural Community Context: Cultural capital; migration patterns; oppression and fear Child Care Context: Provider background; Provider education; Conditions of caregiving; Provider beliefs; Practices; Environment 28 Child’s Experiences: Relationships with caregiver and peers; Learning activities Family Context: Child care arrangement; Relationship and communication with child care provider Arizona Kith and Kin Project Year 1 Evaluation Report Focused Sub-Sample: Research Question 1: What are the background characteristics of providers in the focused sub-sample? (e.g. demographics; conditions of caregiving; motivations and beliefs about parents) We used the CCAT-R’s full “Caregiver Interview” with the targeted sample. The main sections of the Caregiver Interview included: background characteristics; conditions of caregiving; motivations for providing child care; relationships with parents; and routines. Caregivers’ background characteristics The background characteristics of the targeted sample map onto those characteristics of the full sample. Providers in this smaller sample were all women, 98% of providers claimed a Mexican heritage, and the average number of years living in the U.S. is 12.6. The majority of the providers were under 40 years old and 82% were married or in a partnership with a significant other. Similar to the full sample, this targeted sample was very low-income, with 87% of providers living in households that were 175% below the federal poverty level. In regards to educational background, this targeted sample was slightly more educated than the full sample. Twenty percent (20%) had a high school diploma (vs. 17% of the full sample), 11% (5 providers) had a college degree (vs. 4.5% of the full sample). However, the targeted sample had slightly less training in child development than the full sample (49.6% -- full sample vs. 43% -- targeted sample, and less previous exposure to formal child care settings (35% -- full sample v. 28% -- targeted sample). Focus-child characteristics When Specialists arrived at providers’ homes to conduct the observations, they were instructed to randomly select one “focus-child” who was closest in age to 24 months and was not the provider’s own child. This focus-child was the focus of the CCAT-R communication and interaction observation. Whenever possible, Specialists conducted observations with the same child at Time 1 and Time 2, but due to fluctuations in children’s weekly child care schedules, and many families who left town during the summer, Specialists conducted observations with different children for 48% of their Time 2 observations. Based on other studies that involve observations of child care providers with randomly selected children over several time-points, we did not anticipate that this would negatively impact the design of our evaluation, as the instruments used in this evaluation focus on provider practices (Howes, Shivers, & Ritchie, 2004). However, it is noteworthy that there were some significant differences in the characteristics between the focus children at Time 1 and Time 2. The average age at Time 1 was 33.76 months, and 38.72 months at Time 2. There were more girls in the sample at Time 2. At baseline observations there were no parent-child dyads. By the second observation time-point, 16% percent of the observations were completed on parent-child dyads. See Table 23 for more details. Table 23: Focus child background characteristics Focus Child Characteristic Gender Female Male Provider’s relationship to child Aunt Grandmother Friend of family Parent Cousin Other Percent Time 1 Percent Time 2 34.8% 65.2% 70% 30% 38.9% 9.3% 48.1% 0 3.7% 0 36% 24% 20% 16% 0 4% 29 Arizona Kith and Kin Project Year 1 Evaluation Report Conditions of caregiving The conditions of caregiving in the smaller, targeted sample are very similar to the full sample. Notable differences between the two samples include: a higher average of total children in care (2.97 in targeted sample vs. 2.02 in full sample), and a higher percentage of providers in the targeted sample receive payment for providing child care (61.7% vs. 41.3% in full sample). Motivations The targeted sample’s primary motivations for caring for children were aligned with findings from the full sample. The top two reasons for caring for children were: “I want to help my family,” and “I love the child(ren), and want to spend time with him/her.” These two categories accounted for 53.8% of all responses. This finding is consistent with almost all the literature on FFN providers. Studies show that especially for low-income families, providers want to help family members become self-sufficient (Anderson et al., Brandon et al., 2002; Bromer, 2005; Porter et al., 2010; Shivers, 2003). Table 24: Primary motivation for caring for children Frequency Percent 13 31.7 I love the child(ren), and want to spend time with him/her 9 22.0 I don't have any other job 8 19.5 I enjoy working with children 5 12.2 I need the money 5 12.2 I can do a better job than a “stranger” 1 2.4 41 100.0 I want to help my family Total Relationships with parents Researchers have suggested that one of the most unique features of FFN child care is the nature of provider-parent relationships. This feature of FFN child care can be both a challenge to providers as well as a source of strength in promoting parent and child outcomes (Bromer, 2005; Bromer & Henley; Bromer, Paulsell, Porter et al., 2010; Porter et al., 2010; Shivers, 2009). Noted FFN researchers like Toni Porter have argued that there are several pathways through which a parent’s relationship with her FFN provider could ultimately promote child outcomes (See Bromer, Paulsell, Porter et al., 2010; Porter et al., 2010). This section describes findings on various features of provider-parent relationships in the targeted sample, such as communication frequency; beliefs about parents; and supporting parents in addition to providing child care. Table 25: Frequency of communication with parents (0=never; 1=sometimes; 3=often) Minimum Maximum Mean SD How often do you talk to parents about the child(ren) in your care? .20 2.00 1.55 .50 How often do you talk about what’s happening in parent’s life? .00 2.00 1.33 .71 How often do you talk about what's happening in your life? .00 2.00 1.29 .82 30 Arizona Kith and Kin Project Year 1 Evaluation Report Table 26: To whom do you talk the most about the child(ren) in your care? Frequency Percent Mother 45 84.9 Father 2 3.8 Both Other 4 2 53 7.5 3.8 100.0 Previous studies with child care teachers show that how providers feel and think about their work with children and families guides their observed behavior with children (Kagan & Smith, 1988; Nespor, 1987; Wishard et al., 2003; Shivers, 2006). Accordingly, we asked parents to rate their feelings and beliefs about their relationships with parents, and predicted that providers’ belief systems about how they feel about their relationship with parents would be associated to other outcomes in this study such as practices and quality. This section of the CCAT-R Caregiver Interview contained 10 questions related to providers’ perceptions of their relationships with parents. Providers rated their responses on a scale of 1 – 3 (1 = disagree; 2 = neither disagree nor agree; 3 = agree). We conducted a principal component factor analysis (with varimax rotation) to discover whether there were patterns of responses that hung together. We created two distinct factors, which are described in Table 27 below. We called the first factor “Conflict and Resentment,” and the second factor “Cooperation, Communication, Consistency.” In subsequent sections of this analysis, we used these factors to predict provider practices and quality (see Focused Sub-Sample: Research Question 4). 31 Arizona Kith and Kin Project Year 1 Evaluation Report Table 27: Factor Analysis – Provider-Parent Relationship Scale Factor 1 “Conflict & Resentment” (factor loading scores) I think the parent takes advantage of our relationship. .707 I think that the parent is worried that I am closer to the child than he/she. .672 I get upset because the parent doesn’t discipline the same way as me. .585 The parent and I really value our relationship with each other. (disagree) -.517 The parent takes delight in how close I am with his/her child (disagree) -.469 I’m willing to work with the parent to be flexible about his/her schedule. (disagree) -.491 I understand what the parent’s schedule is like. (disagree) -.562 Factor 2 “Cooperation, Communication, Consistency” (factor loading scores) The parent listens to my suggestions about taking care of the child. .787 I'm willing to work with the parent to be flexible about his/her schedule. .703 The parent gives me valuable suggestions about taking care of the child. .630 I understand what the parent’s schedule is like. .574 The parent and I really value our relationship with each other. .503 The parent’s approach for raising children matches mine. .470 Finally, 75.5% of providers in this targeted sample reported that they do things with the children and parents when they are not providing child care. This finding implies that parents and providers have relationships outside of their child care arrangement, which is not uncommon given the types of affiliation (i.e., grandmother; aunt; friend of family). Also, 50% of providers report that they do things – besides providing child care – to help out the parents. This includes taking on tasks such as: picking up prescriptions, taking children to their doctors’ appointments, buying clothes for the children. This finding is consistent with literature on family sensitive caregiving, which posits that one of the strengths of FFN child care arrangements is evidenced by the way FFN providers support parents. By supporting and helping parents – beyond providing child care, providers are easing parental stress, and in turn, indirectly supporting children’s optimal development (Bromer, 2005; Bromer & Henley, 2009; Bromer, Paulsell, Porter et al., 2010). 32 Arizona Kith and Kin Project Year 1 Evaluation Report Research Question 2: How do providers’ scores on various indices of well-being and support change after completing the Arizona Kith and Kin Project? This line of questioning and exploration is guided by family stress models, which suggest that adults’ expressions of negative emotion are associated with higher levels of exposure to poverty-related stressors (Conger, Ge, Elder, Lorenz, & Simons, 1994; McLoyd, 1990; McLoyd 1994). Therefore, we included several indices of support and well-being to determine to what extent providers’ psychosocial supports are associated with features of positive caregiving such as provider sensitivity, rich communication, and positive interactions. It is important to note that most studies involving poverty-related stressors and psychosocial functioning with caregivers have focused on the parent-child relationship (Grining, Raver, Champion, Sardin, Metzger, & Jones, 2010). This evaluation extends the findings from these studies to test if a provider’s perceived material well-being is associated with positive outcomes. The three dimensions of wellbeing and support we measured include: perceived material support, emotional support, and social support. Social support includes a vast array of different types of assistance including instrumental, informational, emotional, and caregiving support (McLoyd, 1994). We know that social support buffers feelings of psychological distress and depression in low-income adults (McLoyd, 1994), but little is known about the effects social support has on informal child care providers. The economic status of many FFN providers parallels that of the parents, and the providers in this study are no exception to this trend. As such, we inferred from a growing body of literature on parenting behavior that indicates that social support not only improves parents’ dispositions, but also, lessens their tendency toward insensitivity and coercive discipline. In fact, both poor and more affluent mothers’ receipt of higher levels of emotional support are positively associated with more sensitive and nurturing behavior towards their children (McLoyd, 1994; Crnic & Greenberg, 1987). Based on this literature, we believed the role of positive social support as a buffer for lowincome women could be expanded to include informal child care providers, and would contribute to optimal providerchild relationships. Table 28: Mean scores psycosocial well-being and support indices Mean SD Perceived Needs Time 1 30.76 6.45 Perceived Needs Time 2 29.00 5.70 Social Support Daily Responsibilities Time 1 9.00 6.54 Social Support Daily Responsibilities Time 2 8.16 4.42 Social Support Affiliations Time 1 6.64 5.58 Social Support Affiliations Time 2 7.36 6.18 Emotional Support Time 1 11.92 3.38 Emotional Support Time 2 12.88 1.83 It is notable that none of the support means scores significantly increased or decreased between Time 1 and Time 2. This means that for the most part, levels of support were held constant, and can be used in subsequent analyses to determine whether levels of psychosocial support and well-being are associated with other outcomes. 33 Arizona Kith and Kin Project Year 1 Evaluation Report Research Question 3: How do providers’ scores on various indices of quality change after completing the Arizona Kith and Kin Project? We measured various dimensions of quality outcomes by using the Child Care Assessment Tool for Relatives (CCAT-R; Porter, Rice, & Rivera, 2006). The CCAT R was developed specifically to assess quality of care provided by relatives, but it has been used to measure quality of care provided by friends and neighbors as well. Like other well-known time sampling measures, it measures the frequency of interactions between the caregiver and the focal child with time sampling. These interactions include talk within the caregiver-child dyad, as well as among the child, the caregiver, and other children and adults; the caregiver’s engagement with the child; and the child’s engagement with materials and other children or adults in the setting. In addition, the CCAT-R includes items related to affect of the caregiver and the child; the types of caregiver and child activities that occur; and disciplinary practices. Caregivers are rated on four factors—nurturing, engagement, and two factors that relate to language—that are based on the percentage of time that the related interactions occur. Ratings include poor, acceptable, and good and are based on the percentage of time that the related interactions occur. There is a range of percentages for each rating. We also reported scores on the basis of the proportion of time certain practices and interactions were observed, (Early, Iruka, Ritchie, Barbarin, et al., 2010; Early Head Start Enhanced Home Visiting Evaluation, Paulsell et al., 2006). The CCAT-R also includes checklists for health and safety and materials, and we reported those scores separately from the communication and interaction scores. The scores for the checklist are based on the percentage of items that were observed. We also used the Caregiver Interaction Scale (CIS/Arnett). The CIS/Arnett (Arnett, 1989) was completed at each time point. Three composite measures were yielded based on previous research findings (Kontos et al., 1995; Whitebook et al., 1990) three scores: sensitivity (e.g., warm, attentive, and engaged); harshness (e.g., critical, threatens children, and punitive); and detachment (e.g., low levels of interaction, interest, and supervision). Scores from this instrument have been found to predict caregiver’s involvement with children and children’s language development and attachment security (Whitebook, Howes, & Phillips, 1989). We calculated mean scores for each instrument’s subscales and conducted paired sample t-tests to discover whether there were statistically significant changes from Time 1 to Time 2. Results are displayed in Tables 29 and 30. 34 Arizona Kith and Kin Project Year 1 Evaluation Report Table 29: T-tests – observed environmental outcome scores at Time 1 and Time 2 Mean SD Total score (children under 3) Time 1 9.86 4.45 Total score (children under 3) Time 2 11.57 5.94 Total score (children 3 and over) Time 1** 10.55 3.75 Total score (children 3 and over) Time 2** 13.73 1.74 Total score (children 3 and over) Time 1* 18.00 1.43 Total score (children 3 and over) Time 2* 19.54 1.14 Food subscale (children 3 and over) Time 1 1.71 .76 Food subscale (children 3 and over) Time 2 1.57 .53 Indoor env. subscale (children 3 and over) Time 1** 11.23 2.05 Indoor env. subscale (children 3 and over) Time 2** 12.77 3.11 Routines subscale (children 3 and over) Time 1 3.92 1.44 Routines subscale (children 3 and over) Time 2 3.67 1.67 Outdoor env. subscale (children 3 and over) Time 1* 2.00 1.33 Outdoor env. subscale (children 3 and over) Time 2* 2.60 1.43 Materials Checklist Health & Safety Checklist * p < .05; ** p < .01 35 Arizona Kith and Kin Project Year 1 Evaluation Report Table 30: T-tests – observed interaction and communication scores at Time 1 and Time 2 Mean SD Arnett/CIS Detached Subscale Time 1 1.65 .80 Arnett/CIS Detached Subscale Time 2 1.48 .65 Arnett/CIS Harshness Subscale Time 1** 1.26 .12 Arnett/CIS Harshness Subscale Time 2** 1.44 .29 Arnett/CIS Sensitivity Subscale Time 1 2.85 .53 Arnett/CIS Sensitivity Subscale Time 2 2.90 .65 Nurturing Time 1+ .88 3.67 Nurturing Time 2+ 2.42 5.37 Caregiver Engagement Time 1 129.46 39.22 Caregiver Engagement Time 2 138.63 40.36 Bi-Directional Communication Time 1 220.54 106.10 Bi-Directional Communication Time 2 242.21 91.47 Unidirectional Communication Time 1 127.71 77.22 Unidirectional Communication Time 2 139.63 59.42 Interacts with books and printed materials Time 1** .63 1.35 Interacts with books and printed materials Time 2** 1.54 1.74 Encourages experimentation with object Time 1* 1.25 1.33 Encourages experimentation with object Time 2* 2.04 1.33 Tell stories, rhymes, sings Time 1* .21 .51 Tell stories, rhymes, sings Time 2* .75 1.39 Caregiver Interaction Scale Interaction and Communication Snapshot Behavior Checklist + < .10; * p < .05; ** p < .01 36 Arizona Kith and Kin Project Year 1 Evaluation Report Table 31: Caregiver communication to child 100 90 80 70 60 50 40 30 20 10 0 59 36 41 34 36 26 26 18 Responds 22 Time 1 Time 2 51 19 18 Requests language Verbally directs Repeats or builds Names or labels "Other" talk Table 32: Focus-child communication 100 90 80 70 60 49 54 Time 1 Time 2 50 40 30 23 13 20 10 0 16 22 4 With caregiver Self-talk Other children 6 Other adults Table 33: Focus-child interactions with people and objects 100 90 80 70 60 50 40 64 70 70 81 20 30 20 10 0 Caregiver Safe materials 27 33 9 Television Time 1 Time 2 6 Other children 8 Other adults Providers demonstrated improvements in almost all of the outcome categories. Most notably, gains were observed in regards to materials in the environment, health and safety environmental features and practices, learning activities, and caregiver-child interactions and communication. In regards to the qualitative aspect of observed caregiver interaction as measured by the Arnett/CIS, provider harshness unexpectedly increased from Time 1 to Time 2. We explore possible hypotheses for this increase in harshness in the Discussion Section. 37 Arizona Kith and Kin Project Year 1 Evaluation Report Research Question 4a: Are providers’ background characteristics associated with quality outcome scores at Time 2? There are several dimensions of process quality that are most often measured and discussed in the child care literature: environment, interactions, and activities (Shonkoff & Phillips, 2000; Vandell & Wolf, 2000). We chose instruments that were designed and/or adapted for use in Family, Friend and Neighbor child care settings. Specifically, our battery of quality outcome tools include the following: CCAT-R Health and Safety Checklist CCAT-R Materials Checklist CCAT-R Learning Activities from the Behavior Checklist rConcept learning rExperimentation with objects rEncouraging independence and autonomy rExplaining and demonstrating how to do something rUsing routines as learning opportunities rStories, rhymes, singing rInteracting with books and other print materials rMusical and rhythmic activities CCAT-R Interaction and Communication Snapshot rNurturing (positive affect; physical affection; responsive to child’s distress) rCaregiver Engagement (talking and interacting with child) rUni-directional communication (caregiver to child) rBi-directional communication (caregiver and child) Caregiver Interaction Scale (Arnett) rSensitivity rHarshness rDetachment A very common approach to describing child care quality is in terms of their structural and caregiver characteristics. Characteristics such as child:adult ratio, group size, caregiver formal education, and caregiver specialized training are viewed as more distal contributors to quality environments. Relations between structural and caregiver characteristics and process quality are well-documented in the research literature (Howes, 2000; NICHD Early Child Care Research Network, 1996, 2007; Phillipsen, Burchinal, Howes, and Cryer, 1997; Vandell & Wolff, 2000). In this evaluation, we consider background variables such as providers’ education levels; specialized training; numbers of children in care; etc. We conducted Pearson bi-variate correlational analysis to determine which provider variables such as background characteristics, conditions of care, and beliefs were associated with quality outcome scores at Time 2. 38 Arizona Kith and Kin Project Year 1 Evaluation Report Table 34: Associations among Provider Characteristics and Quality Outcome Indicators at Time 2 Quality Indicators T2 Health & Safety Checklist Background Characteristics More formal education (.44*) College child development courses (.44*) Conditions of Care Fewer preschoolers in care (-.57**) Beliefs Greater perception that material needs are met (.27*) Other Quality Indicators Higher detachment (-.40*) Less restrictive beliefs about raising children (.42*) Higher Sensitivity (CIS) (.56**) Older children in care (.46*) Materials Checklist Higher engagement (.66**) Higher communication (.56**) Learning Activities College child development courses (.44*) Older children in care (.49**) More Materials (.55**) More Learning Activities (.60**) More Materials (.56**) Higher Nurturing (.48*) Sensitivity (CIS) Fewer infants in care (-.50*) Higher Caregiver engagement (.69**) Higher Uni-directional communication (.67**) Higher Bi-directional communication (.71**) Less Sensitivity (-.56**) Harshness (CIS) More Detachment (.44*) Higher Harshness (.44) Higher perceived cooperation with parents (-.39*) Detachment (CIS) Nurturing (Snapshot) Caregiver Engagement (Snapshot) Lower Sensitivity (-.75**) Less Learning Activities (-.50**) Higher Sensitivity (.48*) College child development courses (.47*) Fewer adults living in household (-.48*) More Materials (.64**) Higher Sensitivity (.56**) Uni-Directional Communication (Snapshot) Fewer adults living in household (-.51*) Older children in care (.39*) Bi-Directional Communication (Snapshot) Fewer adults living in household (-.52*) Older children in care (.41*) More Materials (.56**) Higher Sensitivity (.67**) More Materials (.56**) Higher Sensitivity (.71**) * p<.05; **p<.01 In summary, the background characteristics that seemed to make a difference in quality outcome scores were number of adults living in the household and formal education – including experience with college early childhood education (ECE) courses. The conditions of caregiving that were most associated with quality indicators were number of children in care and the age of children in care. For example, providers who demonstrated higher sensitivity tended to have fewer infants in their care. Also providers who had older children in care tended to score higher on health and safety and had more learning materials in their environment. Contrary to our earlier hypotheses, we did not find many associations with providers’ intrinsic beliefs. However, it is interesting to note that greater perceptions of cooperation with parents was associated with less detachment with children. Finally, there were many associations among the quality indicators. Most notably, provider sensitivity was associated with learning activities, more communication with children, and more learning materials in the environment. 39 Arizona Kith and Kin Project Year 1 Evaluation Report Research Question 4b: Are providers’ background characteristics associated with the amount of change in quality scores from Time 1 to Time 2? We thought it was important to discover whether changes in providers’ quality outcome scores between Time 1 and Time 2 were associated with any other provider or child characteristics. We calculated a change score for each provider on each of the quality indicators, and then conducted Pearson bi-variate correlational analyses with quality outcome scores and change scores. The results are displayed in Table 35 below. Table 35: Associations among Provider Characteristics and Changes in Quality Outcome Scores from Time 1 to Time 2 Change in Quality Indicators Background Characteristics Conditions of Care Beliefs Health & Safety Checklist (increase) Materials Checklist (increase) Fewer adults in household (-.44*) Fewer infants in care (-.50*) Lower household income (-.55**) Learning Activities (increase) Sensitivity (CIS) (increase) Harshness (CIS) (decrease) Detachment (CIS) (decrease) Nurturing (Snapshot) (increase) Previous experience working in child care program (-.46*) More likely to endorse “nurturing” child rearing beliefs at T1 (.46*) Caregiver Engagement (Snapshot) (increase) Uni-Directional Communication (Snapshot) (increase) Fewer years living in the U.S. (-.70**) Lower perception of material needs met at T1 (-.45*) Bi-Directional Communication (Snapshot) (increase) Fewer years living in the U.S. (-.59**) Lower perception of material needs met at T1 (-.44*) The results in the above table indicate that there are very few provider characteristics that were associated with enhanced quality outcomes from Time 1 to Time 2. Implications for this finding is explored further in the Discussion section. In addition, we also found that providers who tended to have much lower scores at the beginning of the project (Time 1), were more likely to demonstrate greater gains at the end of the project (Time 2). This finding is consistent with literature on quality enhancement initiatives, which argues that there is more room to grow as a result of a professional development initiative when one starts with lower quality scores (Shivers, 2011). 40 Arizona Kith and Kin Project Year 1 Evaluation Report SECTION III: PROVIDER FEEDBACK Research Question 1: Was there an increase in child development knowledge after completing the training sessions? At the beginning of each session, providers were given a child development and child safety “Pre-Test” in order to gauge knowledge about basic aspects of child development and safety (e.g., “A 2 and 3 year-old should be able to sit quietly during story-time;” “All children should be potty-trained by 18 months;” “Harness straps on a child car-seat should be loose enough to slide your hand underneath.”) Please see Appendix C for complete list of questions. Providers were then given a “Post-Test” (the same questions) on the last day of their session. We discovered that there was an increase in participants’ child development knowledge after completing the training sessions. We compared scores on the Pre and Post-Tests and found that, on the whole, providers’ scores significantly increased from Time 1 (M= 75.90) to Time 2 (M=80.60) [t (2)= -5.84, p<.05]. We also found that on average, Englishspeaking providers had higher scores than Spanish-speaking providers [F (2, 342) = 3.27, p = .039], and younger providers tended to score higher than older providers (r = -.13, p < .05). Table 36 lists Pre-Test and Post-Test mean scores. Table 36 Pre and Post-Test Mean Scores Region Whole Sample Pre-Test Mean Post-Test Mean 75.90 80.60* * = p < .05 41 Arizona Kith and Kin Project Year 1 Evaluation Report Research Question 2: What were participants’ experiences and ratings of their experiences in the Arizona Kith and Kin Project? At the end of the session, during the last class, participants are asked to complete a “Feedback Survey.” The ASCC Specialist/facilitator asks for a participant to volunteer to collect all the surveys and mail them back to the agency (pre-addressed and pre-paid envelope provided). The Specialist then leaves the room, and providers are free to fill out the confidential surveys. The Feedback Survey is comprised of a combination of rating scales and open-ended questions. Items were grouped under two dimensions: 1) Knowledge and Skills and 2) Interpersonal Style. Ratings ranged from Strongly Disagree (score of 1) to Strongly Agree (score of 4). Specialists’ mean score for Knowledge and Skills was 3.86. Specialists’ mean score for Interpersonal Style was also 3.86. Table 37 provides a summary of responses on each of the items. Table 37: Feedback Survey Ratings “The lead facilitator in my group…” 1 strongly disagree 2 disagree 3 agree 4 strongly agree 11% 89% Knowledge and Skills our Trainer is well-versed in early childhood content our Trainer demonstrated respectful awareness of the unique cultural diversity in our community .3% -- 13% 86.7% our Trainer recommended appropriate strategies and resources .3% .3% 12.2% 87.2% our Trainer elicited information from others and is a good listener .3% .3% 13.9% 85.5% our Trainer demonstrated effective organizational skills (e.g., used time efficiently, was prepared for each meeting) .3% .3% 11.6% 87.8% our Trainer provided prompt feedback .3% .3% 13.5% 85.8% our Trainer was skilled in teaching adults .3% -- 12.6% 87.1% our Trainer was comfortable to talk with .3% -- 12.6% 87.1% our Trainer demonstrated flexibility and openness .3% .3% 11% 88.4% our Trainer was generally pleasant .3% -- 10.7% 89% our Trainer expressed ideas without being overpowering .3% -- 13% 86.6% our Trainer supported our active participation in the training process -- .3% 13.5% 86.2% our Trainer was respectful and caring -- .3% 15% 84.7% -- .3% 15.7% 84% Interpersonal Style 42 Arizona Kith and Kin Project Year 1 Evaluation Report Table 38: Which workshop was most useful for you? Percentage CPR & First Aid 79.9 Nutrition 76.8 Child passenger safety 72.9 Ages & Stages 71.9 Health & Safety 71.6 Brain development 67.7 Guidance and discipline 65.5 Daily schedule planning 59.8 Language and literacy 51.2 Parents and business practices Arranging the environment Community resources 50.9 43.3 39.9 Ninety-three percent (93%) of participants reported a change in their interactions with children as a result of participating in the Arizona Kith and Kin Project. We solicited open-ended responses prompting providers to describe what they have changed as a result of participating in the project. We transcribed verbatim each response, and then coded the responses according to themes. We found that their responses coalesced into three big themes: Engagement and Discipline; Learning Activities; Health and Safety Practices. Most providers’ responses included a combination of statements from each of these broad themes. For example: “We have more daily routines, we talk more to each other, we eat dinner together at the table.” 43 Arizona Kith and Kin Project Year 1 Evaluation Report Engagement and Discipline Themes (In order of most salient response) rMore patience with children rMore positive discipline strategies rBetter communication / I listen to children more rMore awareness of how to communicate in a developmentally appropriate way rI interact with children more, and spend more time with them Here are some examples of responses in these categories: “When I talk to [the children], I look them in the eyes. I praise them when they do things right.” “In regards to discipline, give them time to correct themselves, pay more attention and listen to them when they talk.” “I am more patient when I talk to them and when they don’t understand.” “I make them feel important.” “I have more patience, I understand that their behavior is normal for their age.” “I used to have a list of negative rules – for example: don’t run, don’t scream – but I’ve changed my rules to be more positive.” Learning Activities Themes: rMore time and opportunities for reading, songs, and stories rMore intentional learning activities rCreate and stick to a routine and schedule rPlay with the children more rLess TV / More interaction during TV watching rInvolve children in my chores and activities so they can learn Here are some examples of participants’ statements that were coded according to the above themes: “Less TV, more reading, visits to the library and park more often. More activities for them.” “I read to them more, I don’t yell at them and I play with them more.” “I started to do routines during the day, and they worked.” “I have a routine and rules, we read every day, we do learning activities.” “Be with them when they color, watch TV, and read. Give them quality time and don’t watch more than an hour of TV.” “Have a daily plan.” “I made my own library and I’ve done a lot of the leaps and bounds activities with the children.” 44 Arizona Kith and Kin Project Year 1 Evaluation Report Health and Safety Themes: rChanges in food and nutrition rCar and passenger safety rGeneral safety practices rChemical safety rCPR / First Aid rMore communication with parents about health and safety issues Here are some examples of statements that were coded as Health and Safety Practices: “I now have an agreement with the parents that includes rules about payment and medicine.” “I learned how to install and harness children in car seats.” “I know more about first aid and CPR.” “I don’t use a used car seat, I clean wounds with water, I don’t use bleach on the floors, I don’t give medicine without parents’ permission.” “I put dangerous objects away from children, and I don’t mix cleaning chemicals.” “I made smaller portions of food for children.” “We have an escape plan.” We were also curious to know their thoughts about improving their own quality of care. We asked: If there were one thing you could do to enhance the quality of the care you provide, what would it be? Percentage Get more training 66.2 Learn English 59.1 Get connected to the formal child care system (get licensed or certified; join the food program) 52.4 Go back to school 36.9 Obtain more materials for my child care 29.3 Create more space in my home for child care 20.1 45 Arizona Kith and Kin Project Year 1 Evaluation Report We also wanted feedback on other features of their involvement with the Arizona Kith and Kin Project such as recruitment, retention, level of difficulty, and the likelihood of continuing to seek training. How did you hear about the program? Percentage I saw a flyer or heard through someone at local elementary school 55.2 Invited by friend or family member 29.0 Word of mouth 23.2 Other 5.8 What kept you coming back week after week? Percentage Desire for knowledge and training 94.5 Relationship with trainers 21.6 Contact with other providers 17.7 Prizes and materials 10.1 What was the level of difficulty of the workshops? 100 Percent 80 60 60 40 26 13 20 0.3 0 too easy easy but interesting challenging too difficult What is the likelihood that you will continue to get training on child care and child development? 100 65 Percent 80 60 20 0 46 33 40 0.6 not likely kind of likely most definitely Arizona Kith and Kin Project Year 1 Evaluation Report Every year there are a percentage of providers who return from previous sessions. This year, 14% of providers reported that this was not their first time in the Arizona Kith and Kin Project. When we asked them what motivates them to keep returning, they gave us open-ended responses. Here are examples of the most common responses: (In order of most salient response) I want to keep learning I want to improve the care I give to children I want to open my own business 47 Arizona Kith and Kin Project Year 1 Evaluation Report Discussion For the past 15 years, the Arizona Kith and Kin Project through the Association for Supportive Child Care (ASCC) has been providing training and outreach to Family, Friend and Neighbor (FFN) child care providers. Not only is this project well noted among early childhood professionals in Maricopa County and the state of Arizona, but this project has also garnered national attention for the work they do. For the past ten years, project leadership staff at ASSC has worked with others across the country to raise awareness of FFN child care issues. In fact, nationally noted and respected researcher and leader of FFN child care awareness – Toni Porter – attended the 10-year anniversary of the Arizona Kith and Kin Project and delivered the keynote address. In addition, the work of the project has appeared in nationally disseminated publications (Ocampo-Schlesinger & McCarty, 2005; Porter, 2007; Porter et al., 2010a; Porter et al., 2010b) and national conference presentations (Shivers, Ocampo-Schlesinger, & Wilkins, 2010; Ocampo-Schlesinger & McCarty, 2006). Also, the project’s leaders have played a strong leadership role in the National Alliance of Family Friend and Neighbor Child Care; provided professional consultation on the development of the CCAT-R, and staff from this project participated in the CCAT-R’s validation study (Porter, Rice, & Rivera, 2006). Despite this long list of accolades, this is the first in-depth evaluation of the program that included pre and post observations as well as extensive data collection on the demographics, beliefs and motivations of its participants. Our goal was to pilot an evaluation that would attempt to meet several objectives: 1) inform the project’s ongoing design and implementation; 2) add to the field of literature on child care in general and FFN child care more specifically; and 3) provide findings that could guide our state’s efforts to build a comprehensive system of professional development for the entire continuum of child care providers. Highlighted Findings By and large, the Arizona Kith and Kin Project was a success as measured by high participation rates, statistically significant increases on key quality indicators, and overwhelming positive feedback from providers. Key findings are summarized below. Cultural Communities In 2010, the Arizona Kith and Kin Project served more than 900 Family, Friend and Neighbor (FFN) child care providers. This is one of the largest quality improvement initiatives for FFN providers in the country (Porter et al., 2010). Findings from our demographic surveys (n = 827) revealed that 90% of the providers identify as Latino/a and of those, 96% report having Mexican-heritage. While we did not collect data on immigration or citizenship status, we know that the average amount of time providers have lived in the U.S. is 13 years, which indicates that this project has successfully recruited and served a largely immigrant population. In addition, the project included three sites, which were aligned with Somali, Nepali, and Bhutanese refugee communities. Obtaining high recruitment and participations rates for marginalized FFN providers is traditionally a concern with which many community agencies struggle (Powell, 2008). However the large numbers of providers who participated in this year’s program and the existence of waiting-lists at several sites in the South Phoenix Region indicate that this project has been successful at reaching a hard-to-reach population of child care providers. Research demonstrates that when approaches for FFN training and support are flexible, voluntary, and tailored, and when they recognize and respect the inherent strengths of FFN care, the cultural differences, and the essential voluntary and personal relationships of FFN caregiving, agencies are more successful at engaging participation from marginalized cultural communities (Chase, 2008; Powell, 2008). This project used several proven culturally responsive strategies in its design. For example, the project did not expect the FFN caregivers to come to its offices, but rather, outreach was built on natural connections, going where FFN caregivers already congregate – schools, churches, libraries, and community centers. In addition, the Project’s specialists and co-facilitators had the same ethnic heritage and spoke the same language as the providers. This is a proven effective strategy in community-based programming (Powell, 2008; Yoshikawa, Wilson, Hsueth, Rosman, Chin, & Kim, 2003). It will be important to situate and examine current evaluation findings in a cultural context (Garcia-Coll et al., 1996; Golden & Fortuny, 2010; Johnson et al., 2003; Yoshikawa, 2011). 48 Arizona Kith and Kin Project Year 1 Evaluation Report Conditions of Caregiving We found that providers in this sample (n = 827) care for an average of 2.02 children, and adult:child ratios were on average 2:1. These findings are consistent with other literature (Layzer & Goodson, 2003; Maxwell & Kraus, 2002; Porter, Rice, & Mabon, 2003). Contrary to most of the literature on FFN child care, the providers in this sample were mostly aunts and not the child’s grandparent (Brown-Lyons et al. 2001; Shivers & Wills, 2001; Susman-Stillman & Banghart, 2008). While the majority of providers were related to the children in their care, 20% of the providers were not. Providers’ motivations for providing care are largely based on wanting to help the child’s family be self-sufficient and feeling a sense of emotional investment in the child. This finding is also consistent with the literature (Anderson et al., Brandon et al., 2002; Bromer, 2005; Porter et al., 2010; Shivers, 2003). We also found that a provider’s relationship to the children in her care was significantly associated with her motivation for providing child care. For example, aunts were more likely to report providing care in order to help the family. Grandparents were more likely to report providing care because of their emotional investment in the child, and non-relatives were more likely to provide care because they viewed providing child care as a source of income. Community-based efforts to enhance the quality of FFN child care will be successful if they can build upon these unique features of FFN caregiving arrangements such as low group sizes, low ratios, and personal investment in children (Brandon, 2005). This group of child care providers demonstrated flexibility in both scheduling and payment arrangements. About half of the providers in this sample provided child care during “traditional” child care hours. About a quarter provided care during evenings and weekends. The remaining quarter had care arrangements that included both traditional and nontraditional hours. While almost 60% of providers in this sample do not get paid for the care they provide, the majority of these providers reported having arrangements that included providing child care in exchange for other services, such as groceries, getting other household bills paid, child care exchange with their own children, etc. These findings are consistent with other literature (Brandon, 2005; Shivers, 2003). It is also noteworthy that an overwhelming 98.5% of providers in this sample do not receive child care subsidy reimbursement. This finding is consistent with other research on child care providers from immigrant communities (Chase, 2008; Yoshikawa, 2011). Increases in Key Quality Outcomes We found statistically significant increases on almost all of our key quality indicators: health and safety scores; materials in the physical environment; provider-child communication patterns; provider engagement; learning activities; and providers’ basic knowledge about child development. In addition, we found that those providers who started out with the lowest scores made the largest increases. We also found that providers who were younger and relatively new to the U.S. made most gains. Finally, contrary to our original hypothesis, we discovered that providers’ beliefs, perceptions and intrinsic values did not impact amount of growth on quality indicators as much as we originally thought based on our reading of the literature (Bromer et al., 2010; Kontos et al., 1995; Shivers, 2003; Shivers, 2007). There are several ways to interpret this finding. On one hand, few associations among provider beliefs and quality indicators might lead one to conclude that changes to provider practices are possible despite intrinsic values and beliefs providers bring with them to the training and support groups. Another might argue that there were few associations because belief findings were truncated, and there was not much variability in responses. However this argument falls apart in light of research, which demonstrates rich intracultural variability in the belief systems of Mexican-heritage caregivers (Howes, Wishard-Guerra, & Zucker, 2007), and the very wide distribution of findings in the targeted sample (see Table 28). Finally, and perhaps the most compelling interpretation of these findings is that perhaps we did not select the “right” set of provider-belief instruments that are sensitive to nuances in caregiving practices for this particular group of providers. 49 Arizona Kith and Kin Project Year 1 Evaluation Report Provider-Child Interactions – Sensitivity and Harshness Despite the salience of responses from providers reporting that they changed their interaction practices with children, we did not find an increase in provider sensitivity. Provider sensitivity scores as measured by the Arnett, remained constant. However, we found an increase in provider harshness from Time 1 to Time 2. When we contextualize our findings with the national literature on home-based providers, we find the sensitivity scores for the providers in this sample (M = 2.9) are a little lower than most other national samples (range 2.6 – 3.3). However, the harshness scores for providers in this sample (M = 1.4) are lower than national samples (range 1.5 - 1.6). So while harshness increased from Time 1 to Time 2, it was still lower than the national average for home-based child care (Administration for Children & Families, 2004; Kontos et al., 1995; Peisner-Feinberg & Burchinal, 1997). Nevertheless, it is important to explore possible explanations for the increase in provider harshness. We first must consider the community and cultural context in which we were conducting our observations. These providers face multiple risk factors such as few material resources, low cultural and social capital, and hostility from larger political forces. Observations for this study took place in the spring of 2010, a time when Arizona was experiencing the effects of a severe recession. Understandably, fear, uncertainty and chaos do not provide an optimal backdrop for high emotional availability (Capps, Casteaneda, Chaudry, & Santos, 2007), and these set of circumstances might have impacted providers’ relationships with the children in their care. A second explanation for this finding involves the very nature of observable changes in adults’ interactions with children. Research has demonstrated that the process for adult learning involves “head, heart, then hands.” In other words, the shift first happens in adults’ acquisition of new knowledge. It is then transferred, and manifests as changes in belief systems. And then finally, we see changes in actual behaviors and practices (Sipos, Battisti, & Grimm, 2008). It may conceivably take longer than 14 weeks to observe measurable change in providers’ qualitative interactions with children – especially in light of providers’ multiple risk factors (Capps et al., 2007; Rogers, Perreira, Beeber, & Schwartz, 2008). A more intense intervention may be needed to see measurable impact on the provider sensitivity and harshness. Perhaps it may not be reasonable for us to include “increases in provider sensitivity” as immediate outcome indicator – it may be more appropriately categorized as a more distal outcome. Finally, child care researchers have recently begun to question the cultural validity of the Harshness subscale on the Caregiver Interaction Scale (Arnett). Many researchers who conduct observations with low-income African American and Latino/a child care providers are opting not to include the Harshness subscale in their analyses (Johnson & NICHD ECCRN, 2003). We may want to reconsider its use in this study as well if it is not an accurate measure of levels of harshness in child care provided by low-income Latina providers. Feedback from Participants Feedback from participants was overwhelmingly positive. The most influential workshops were related to issues of health and safety. This finding is consistent with findings from observations of providers’ homes using the Health and Safety Checklist, where Health and Safety scores significantly increased. Providers reported many changes in their interactions with children. The most commonly reported changes were in the areas of positive discipline and more reading activities. 95% of providers reported that they kept coming back to the trainings week after week because of a desire for more knowledge. In fact, 65% reported that it was “very likely” that they would pursue additional training once the project ended. About half of the providers reported a desire to be connected to more formal systems such as licensing, the food program, or the child care subsidy program. Implications for Program Design and Implementation The current curriculum design seems to be effective at enhancing health and safety, materials in the environment, learning activities, and communication complexity and frequency. Admittedly, it is more difficult to impact provider sensitivity with children. However, a robust area for exploration would be implementation of professional development initiatives and curricula that focus on enhancing provider-child relationships and children’s social and emotional development. Given the limited number of sessions and a project curriculum that must cover a wide array of topics, it may be necessary to enhance the training and support Specialists receive. By enhancing training and support to Specialists, they in turn might be better equipped to weave social and emotional themes throughout the rest of 50 Arizona Kith and Kin Project Year 1 Evaluation Report the curriculum. This may be a worthy investment in Specialist training given the importance of children’s social and emotional development in their concurrent and future developmental outcomes. Indeed, provider–child relationships characterized by more warmth and responsiveness, and by less anger and harshness, are linked to children’s greater academic achievement and social competence, especially for children at risk (Burchinal, Peisner-Feinberg, Pianta, & Howes, 2002; Decker, Dona, & Christenson, 2007; Hamre & Pianta, 2005). Another finding that may inspire project expansion is related to the fact that over half of the participants reported a desire to be more connected with formal systems. Some ideas for intentionally helping providers get connected to systems include: more technical assistance getting licensed and certified; more intentional exposure to high quality early care and education programs in providers’ local communities such as Head Start and other subsidized programs; and giving providers detailed information about other First funded Things First programs in their communities, which they, in turn, can share with children’s parents. Implications for Policy As Arizona moves toward building a system where ALL children have access to high-quality, culturally responsive early care and education that promotes their development, many are considering whether providing support and training for Family, Friend and Neighbor– or Kith and Kin child care providers – fits into this vision. It is clear from this data and other data throughout the country that children are spending a considerable amount of time in these arrangements while parents work. In addition, we know that providers are paid, and receipt of payment makes this a serious employment activity. From a public policy and workforce perspective it seems reasonable to treat this substantial portion of caregivers as part of our early care and education workforce and worthy of our investments in quality improvement (Brandon, 2005). A related policy issue takes into consideration the specific cultural community that is served by and makes up this group of caregivers. In a socially stratified society, social position variables such as migration patterns and language acquisition, determine access to critical resources (Emarita, 2007; Garcia-Coll et al., 1996; Johnson et al., 2003, Yoshikawa, 2011). Critical resources as they pertain to this sample of providers might include access to formal education, materials and resources for children, information about caring for children, and information about how formal institutions and systems work in this state. Low-income immigrant mothers face formidable obstacles in locating good quality care when they have limited cultural and social capital, such as English language proficiency or the resources to pay market costs of high quality child care (Polakow, 2007). Currently, one in every five children in the U.S. has a foreign-born parent, with the majority of immigrant families experiencing high levels of poverty and restricted access to public benefits (Golden & Fortuny, 2010). As the fastest growing segment of the nation’s young child population, lowincome immigrant children are far less likely to gain access to quality child care, and are underrepresented in public Pre-k and Head Start programs (Polakow, 2010; Yoshikawa, 2011). A key aspect of Arizona’s vision is to build a system that does not leave children behind. In Minnesota, where the state legislature designated funding specifically targeted towards enhancing the quality of FFN care, policy makers argued that supporting FFN child care is a means to insure inclusion in developing an early childhood system that supports ALL children (Chase, 2008; Emarita, 2007). 51 Arizona Kith and Kin Project Year 1 Evaluation Report Next Steps Policy Considerations Clearly, the potential need and demand for quality improvement are quite large. A preponderance of evidence on structural and observational measures of quality suggests that a high percentage of FFN caregivers are below a desirable level of quality (Fuller et al., 2004; Maher, 2007; Porter et al., 2010). Although this study and a number of studies suggest that a high percentage of FFN caregivers would like voluntary training and support (Anderson et al., 2005; Brandon et al., 2002; Shivers 2010), and our own state’s efforts have been growing in recent years, they are currently still small in scale. A particular challenge for the policy community is that while there appear to be both substantial need and potential demand for training and support for FFN caregivers, there is no robust evaluation literature documenting either the conditions under which FFN caregivers will actually participate, or the degree to which various training or support activities can improve the quality of their interaction with children (Brandon, 2005; Porter et al., 2010). Gathering more data about this group of providers is therefore a critical priority for the early childhood policy agenda throughout the country (Chase, 2008). This evaluation report represents a move in this direction, but we need to continue funding and mandating additional efforts at robust evaluations and research studies. Researcher, Richard Brandon from the University of Washington, developed several critical criteria for determining the appropriate degree of public policy engagement with FFN caregiving (2005). He lists guiding questions such as: rHow much of young children’s experience in non-parental care is accounted for by FFN caregiving? rAre the children in FFN care also in formal arrangements where quality may be easier to track and enhance? rWhat portion of the early care and education workforce is comprised of FFN caregivers? rWhy do parents choose FFN care, and how stable are those patterns of choice likely to be if financial access to high quality formal ECE were to be substantially increased? rWhat is the current level of financial engagement by parents and public agencies with FFN care? rIs the quality of FFN care sufficiently high to assure children’s appropriate development, or low enough to pose a developmental threat? rAre FFN caregivers satisfied with their situation, or would they like training and support to improve their caregiving? rHow likely are they to participate in training and support activities? Lastly, findings from this evaluation move us closer to determining appropriate indicators for this child care population. As we build an early care and education system that relies upon heavily monitoring quality, we should be considering the entire continuum of child care – and the role FFN child care can play in bridging parents to quality programs. Indeed, other states are also discussing how FFN providers can be included in their professional development and quality initiatives. In fact, we can look to other states, like Illinois and Pennsylvania, as they grapple with the challenge of including FFN providers in their Quality Rating and Improvement Systems (QRIS) and professional development systems. Additional Research and Evaluation Considerations The early education field as a whole is challenged to draw conclusions about the effectiveness of different strategies for improving the quality of FFN child care because of the lack of rigorous methods to isolate the effects of the initiative (Paulsell et al., 2010). The majority of evaluations on FFN initiatives consists of provider-reports on experiences and satisfaction with the program, and reported change in knowledge and practices. Even those studies (including this current evaluation) 52 Arizona Kith and Kin Project Year 1 Evaluation Report that employ observational data can only infer causal connections between the intervention and provider and child outcomes. Most evaluations and studies lack a randomly assigned comparison group; thereby rendering it almost impossible to isolate the effects of the strategies and initiatives (Paulsell et al., 2010). And finally, sample sizes are too small to conduct rigorous analyses that are generalizeable to the broader population of FFN child care providers. For the purposes of continued evaluation of the Arizona Kith and Kin Project, we currently do not have the resources to conduct a randomized study; however, there are things we can do to make our evaluation more robust. First, we could implement new strategies to increase our sample size, such as developing flyers and other take-home material that further explain the study. Second, we can continue to refine the project’s logic model and make sure that the evaluation design and measurement tools align with intended outcomes. Finally, we can revisit our expectations about the intermediate and long-term outcomes, and determine whether we are specifying and testing a realistic pathway of change (Paulsell, 2010). For example, is it realistic for us to expect that we would be able to observe a change in provider sensitivity given the relatively short time-frame of 14 once-a-week sessions, and the myriad of stressors impacting providers’ lives? Another important next step would be to advocate for more funding to collect rigorous data on the effectiveness of FFN child care initiatives, such as the Arizona Kith and Kin Project. Given the amount of local, state and national resources that are used for FFN child care training and technical assistance initiatives that are springing up around the country, it is paramount that we understand how and for whom these strategies are impacting provider and child outcomes. Collecting rigorous outcome data can also help answer questions about which aspects of professional development initiatives are predictive of children’s concurrent and future developmental outcomes. These data are essential for future policy directions regarding the role of FFN child care in promoting school readiness. Conclusion In a recent presentation, the U.S. Secretary of Education, Arne Duncan, spoke about access to high quality child care programs (Race to the Top Early Learning Challenge Grants announcement, May 25, 2011). He spoke about the rich tradition of research that has clearly and undeniably demonstrated the long-lasting benefits of high quality child care – especially for low-income children and families. He cautioned that we must be careful to balance the tension between investing resources in improving center-based care, while not abandoning and neglecting the thousands of young children whose parents are neither selecting nor have access to high quality center-based care. Given critical importance of building early skills, we must reach vulnerable children where they are. An increasingly common approach used throughout the country is to boost the quality of care they receive in FFN settings. As long as parents continue to place their children with families, friends and neighbors – a choice they make for various reasons, it is our responsibility to reach out to those providers and help them enhance the quality of care they provide. 53 Arizona Kith and Kin Project Year 1 Evaluation Report References Adams, G., Zaslow, M., & Tout, K. (2006). Child Care for Children in Low-Income Working Families: Trends, Patterns, and Potential Policy Implications for Children’s Development. Paper prepared for The Urban Institute and Child Trends Roundtable on Children in Low-Income Families, January 12, 2006. Administration for Children and Families (2004). The role of Early Head Start programs in addressing the child care needs of low-income families with infants and toddlers: Influences of child care use and quality. Washington, DC: U.S. Department of Health and Human Services. Anderson, S., Ramsburg, D., & Scott, J. (2005). Illinois study of license-exempt care. Urbana-Champaign, IL: University of Illinois at Urbana-Champaign. Arnett, J. (1989). Caregivers in day-care centers: does training matter? Journal of Applied Developmental Psychology, 10, 541-552. Bowman, B., Donovan, S. & Burns, S. (eds.) (2001). Eager to Learn: Educating Our Preschoolers. Washington, DC: National Academy Press. Brandon, R. N. (2005). Enhancing family, friend and neighbor caregiving quality: The research case for public engagement. Seattle, WA: University of Washington, Human Services Policy Center. Bromer, J. (2005). Ways of caring: How relative caregivers support children and parents. In R. Rice (Ed.), Perspectives on family, friend and neighbor child care: Research, programs and policy (pp. 14-21). New York: Bank Street College of Education. Bromer, J., & Henly, J.R. (2009). The work-family support roles of child care providers across settings. Early Childhood Research Quarterly, 24, 271-288. Bromer, J., Paulsell, D., Porter, T., Weber, R., Henly, J., & Ramsburg, D., with Families and Quality Workgroup members (2010). Family-sensitive caregiving: A Key component of quality in early care and education. In M. Zaslow, K. tout, T. Halle, & I. Martinez-Beck (Eds.), Quality measurement in early childhood settings. Baltimore, MD: Brookes Publishing. Brown-Lyons, M., Robertson, A., & Layzer, J. (2001). Kith and kin—informal child care: Highlights from recent research. New York: National Center for Children in Poverty. Capps, R., Castaneda, R M., Chaudry, A., & Santos, R. (2007). Paying the price: The impact of immigration raids on America’s children (Report by the Urban Institute for the National Council of La Raza). Washington, DC: National Council of La Raza. Chase, R. (2008). State policies for supporting family, friend, & neighbor care: BUILD initiative policy brief. Wilder Research. Child Trends (2010). Quality Rating and Improvement Systems for Early Care and Education. Early Childhood Highlights, Vol. 1, Issue 1. Conger, R. D., Ge, X., Elder, G. H., Lorenz, F. O., & Simons, R. L. (1994). Economic stress, coercive family process, and developmental problems of adolescents. Child Development, 65, 541–561. Crnic, K. A., Greenberg, M., Ragozin, A., Robinson, N., & Basham, R. (1983). Effects of stress and social support on mothers and premature and full-term infants. Child Development, 54, 209-217. Early, D.M., Iruka, I., Ritchie, S., Barbarin, O., Winn D. M., Crawford, G., Frome, P., Clifford, R., Burchinal, M., Howes, C., Bryant, D., & Pianta, R. (2010). How do pre-kindergartners spend their time? Gender, ethnicity, and income as predictors of experiences in pre-kindergarten classrooms. Early Childhood Research Quarterly, 25, 177-193. 54 Arizona Kith and Kin Project Year 1 Evaluation Report Emarita, B. (2007). Family, friend, and neighbor care best practices: A report to Ready 4 K. St. Paul: Ready 4 K. Fuller, B., Kagan, S. L., Loeb, S., & Chang, Y. (2004). Child care quality: centers and home settings that serve poor families. Early Childhood Research Quarterly, 19, 505-527. Golden, O. & Fortuny, K. (2010). Young children of immigrants and the path to educational success: Key themes from an Urban Institute roundtable. Urban Institute. Grining, C., Raver, C., Champion, K., Sardin, L., Metzger, M., & Jones, S. (2010). Understanding and improving classroom emotional climate and behavior management in the “real world”: The role of Head Start teacher’ psychosocial stressors. Early Education and Development, 21, 65-94. Howes, C. (2000). Social-emotional classroom climate in child care, child-teacher relationships, and children's second grade peer relations. Social Development, 9, 191-204. Howes, C., Shivers, E. M., & Ritchie S. (2004). Improving social relationships in child care through a researcher- program partnership. Early Education & Development, 15, 57-78. Howes, C., Wishard Guerra, A., & Zucker, E. (2007). Cultural communities and parenting in Mexican-heritage families. Parenting: Science and Practice, 7, 1-36. Human Services Policy Center (2002-2004): summaries of state ECE utilization surveys conducted and analyzed by HSPC, available at www.hspc.org: Highlights of the Ohio Child Care Survey; Highlights of the South Carolina Child Care Survey; Highlights of the Illinois and Chicago Child Care Surveys; Highlights of the Mississippi Child Care Survey. Herbst, C., (2008). Who are the eligible non-recipients of child care subsidies? Children and Youth Services Review, 30, 1037–1054. Layzer, J.I., & Goodson, B. D. (2006). National Study of Child Care for Low-Income Families – Care in the Home: A Description of Family Child Care and the Experience of Families and Children That Use It. Wave 1 Report. Cambridge, MA: Abt Associates. Kontos, S., Howes, C., Shinn, M., & Galinsky, E. (1995). Quality in family child care and relative care. New York: Teachers College Press. Maher, E. J. (2007). Measuring quality in family, friend, and neighbor care: Conceptual and practical issues. New York: Columbia University Mailman School of Public Health National Center for Children in Poverty, Child Care and Early Education Research Connections. Maher, E. J., & Joesch, J. (2005). The prevalence and characteristics of child care provided by family, friends and neighbors. Paper presented at the biennial meeting of the Society for Research in Child Development, Atlanta, GA. Maher, E.J. & The Human Services Policy Center and the Center for the Child Care Workforce (2003). Determinants of State Child Care Utilization Patterns for Estimating the Size of the Child Care Workforce at the State Level. Seattle, WA. McLoyd, V. C. (1990). The impact of economic hardship on black families and children: Psychological distress, parenting, and socioemotional development. Child Development, 61, 311–346. McLoyd, V.C. (1994). Research in the service of poor and ethnic/racial minority children: Fomenting change in models of scholarship. Family and Consumer Sciences Research Journal, 23, 56-66. Ocampo-Schlesinger, S., & McCarty, V. (2005). The Arizona kith and kin project. In R. Rice (Ed.), Perspectives on family, friend and neighbor child care: Research, programs and policy (pp. 22-25). New York: Bank Street College of Education. Paulsell, D., Mekos, D., Del Grosso, P., Rowand, C., & Banghart, P. (2006). Strategies for supporting quality in kith and kin child care: Findings from the Early Head Start Enhanced Home Visiting Pilot Program evaluation final report. Princeton, NJ: Mathematica Policy Research, Inc. 55 Arizona Kith and Kin Project Year 1 Evaluation Report Paulsell, D., Porter, T., Kirby, G., Boller, K., Martin, E., Burwick, A., Ross, C., & Begnoch, C. (2010). Supporting quality in home based child care: Initiative design and evaluation options. Princeton, NJ: Mathematica Policy Research, Inc. Peisner–Feinberg, E. & Burchinal, M. (1997). Concurrent relations between child care quality and child outcomes: The study of cost, quality, and outcomes in child care center, Merrill-Palmer Quarterly, 43, 451–477. Pittard, M., Zaslow, M., Lavelle, B., & Porter, T. (2006). Investing in quality: A survey of state child care development fund initiatives (Washington, DC: American Public Human Services Association and Child Trends), 25. Polakow, V. (2007). Who cares for our children: The child care crisis in the other America. New York: Teachers College Press. Powell, D. (2008). Who’s watching the babies? Improving the quality of family, friend and neighbor care. Washington, DC: Zero to Three. Porter, T. (2007). Assessing initiatives for family, friend and neighbor child care: An overview of models and evaluations. New York: Columbia University Mailman School of Public Health, National Center for Children in Poverty, Child Care and Early Education Research Connections. Porter, T., Nichols, T., Del Grosso, P., Begnoche, C., Hass, R., Vuong, L., Paulsell, D. (2010a). A compilation of initiatives to support home-based child care. Washington, D.C.: Mathematica Policy Research. Porter, T., Paulsel, D., Nichols, T. Begnoche, C., Del Grosso, P. (2010b). Supporting quality in home-based child care: A compendium of 23 initiatives. Washington, D.C.: Mathematica Policy Research. Porter, T., & Rice, R. (2000). Lessons learned: Strategies for working with kith and kin caregivers. New York: Bank Street College of Education. Porter, T., Rice, R., & Mabon, S. (2003). Doting on kids: Understanding quality in kith and kin child care. New York: Bank Street College of Education. Porter, T., Rice, R., & Rivera, E. (2006). Assessing quality in family, friend, and neighbor care: The child care assessment tool for relatives. New York: Bank Street College of Education. Porter, T., & Vuong, L. (2008). Tutu and me: Assessing the effects of a family interaction program on parents and grandparents. New York: Bank Street College of Education. Powell, D. (2008). Who’s watching the babies? Improving the quality of family, friend and neighbor care. Washington, DC: Zero to Three. Rogers, J., Perreira, K., Beeber, L., & Schwartz, T. (2008). The ALAS project: Removing barriers to mental health care for Latina immigrant mothers. Journal of Zero to Three, 29, 39-44. Schulman, K., & Blank, H. (2007). Close to home: State strategies to strengthen and support family, friend and neighbor child care. Washington, DC: National Women’s Law Center. Shivers, E. M. (2004) Where the children are: Predicting provider-child relationships in informal (kith and kin) child care settings. Dissertation Abstracts International Section A: Humanities & Social Sciences. Vol. 65 (1-A), 64. Shivers, E. M. (2005). Predicting provider-child relationships from provider characteristics and conditions of care. Presentation at the Society for Research on Child Development Biennial Meeting, Atlanta, Georgia. Shivers, E. M. (2006). A closer look at kith and kin care: Exploring variability of quality within family, friend and neighbor care. Applied Developmental Psychology, 27, 411-426. 56 Arizona Kith and Kin Project Year 1 Evaluation Report Shivers, E. M. (2007). Ways of Caring: Examining Racial-Ethnic Socialization Practices and Emotional Availability among African American FFN Providers. National Alliance of Family, Friend and Neighbor Child Care Annual Meeting – Invited paper presentation, November 2007, Chicago, IL. Shivers, E.M. (2008). Exploring the Training Needs of Family Friend and Neighbor Child Care Providers. Technical Report: Prepared for Zero to Three with support from the Annie E. Casey Foundation and the Federal Child Care Bureau. Shivers, E. M. (2011). Evaluation of Tennessee’s Statewide Infant Toddler Credential Pilot Project. Technical Report: Prepared for Signal Centers, Inc. with funding from Tennessee Department of Health Services. Shivers, E. M., Ocampo-Schlesinger, S., & Wilkins, S. (2010). Findings from the Arizona Kith and Kin Project. Field presentation at Zero the Three’s National Training Institute, Phoenix, AZ. Shivers, E., & Wills, S. (2001). License-Exempt Assistance Project Final Report – 2001. Los Angeles, CA: Crystal Stairs, Inc. Shonkoff, J.P. & Phillips, D.A. (eds) (2000), From Neurons to Neighborhoods: The Science of Early Childhood Development, National Academy Press, Washington, DC. Sipos, Y., Battisti, B., Grimm, K. (2008). Achieving transformative sustainability learning: Engaging head, hands and heart. International Journal of Sustainability in Higher Education, 9, 68-86. Snyder, K. & Adelman, S. (2004), The Use of Relative Care While Parents Work: Findings from the 1999 National Survey of American Families. Washington, D.C., The Urban Institute (Discussion Paper 04-09). Sussman-Stillman, A., & Banghart, P. (2008). Demographics of family, friend and neighbor child care in the United States. New York: Child Care and Early Education Research Connections. Tout, K., Zaslow, M., Papillo, A. R., & Vandivere, S. (2001, September). Early child care and education: Work support for families and developmental opportunities for young children. (Occasional Paper #51.) Washington, DC: Urban Institute. U.S. Government Accountability Office (2010). Child Care: Multiple factors could have contributed to the recent decline in the number of children whose families receive subsidies. Report to Congressional Requesters, May 2010, GAO-10-344. Whitebook, M., Howes, C., & Phillips, D. (1990). Who Cares?: Child care and the quality of care in America. Final report of the National Child Care Staffing Study. Oakland, CA: Child Care Employee Project. Whitebook, M., Phillips, D., Bellm, D., Crowell, N. Almaraz, M., & Yong Jo, J. (2004). Two years in early care and education: A community portrait of quality and workforce stability – Alameda County, California. Berkeley: University of California at Berkeley, Center for the Study of Child Care Employment. Wishard, A. G, Shivers, E. M., Howes, C., Ritchie, S. (2003). Child care program and teacher practices: associations with quality and children’s experiences. Early Childhood Research Quarterly, 18, 65-103. Yoshikawa, H. (2011). Immigrants raising citizens: Undocumented parents and their young children. New York, NY: Russell Sage. Yoshikawa, H., Wilson, P.A., Hsueh, J., Rosman E.A., Chin, J., & Kin, J.H. (2003). What front-line community-based organization staff can tell us about culturally anchored theories of behavior change in HIV prevention for Asian/PacificIslanders. American Journal of Community Psychology, 32, 143-158. 57 Arizona Kith and Kin Project Year 1 Evaluation Report APPENDIX A Logic Model 58 APPENDIX A: Logic Model INPUTS Full-time bilingual employees. Videos, books, hands-on games, role playing kits and activities, reference materials, printed resources and community related information. Special skills utilized: Certi ed Child Passenger Safety Technicians, CPR and First Aid instructors, Registered Nurse volunteers, STRATEGIES Establish collaborations with community partners as point of contact for each site. Conduct outreach to participants. Provide transportation to and from the meetings. Provide on-site child care during meetings. Educate kith and kin providers on early childhood related topics. Create supportive relationships for kith and kin providers. Support the provider’s emotional and social well-being so that she can enhance the emotional climate of care. Educate kith and kin providers on resources and opportunities for future growth that are available. Provide the necessary safety devices to improve the safety of children. Enhance providers’ awareness of what it takes to prepare children for school. OUTPUTS Provide training-support groups sessions in Maricopa, Yuma and Coconino County. Deliver a 14 week training session in the Fall and Spring each year. Provide training and support to Impact the quality of child care provided to children in the care of family, friend and neighbor care providers. Make safety equipment including car seats, smoke alarms, outlet covers and cribs available to providers who complete the appropriate training. cation to providers enrolled in the 14 week training-support groups OUTCOMES Short-Term Participants will gain a better understanding and increased knowledge of quality child care by the end of the 14-week support- training. Participants receive the opportunity to get respite from their normal child care responsibilities and an opportunity to network with other providers in their community. Mid-Term Participants’ caregiving practices will be enhanced. The early childhood environment in which participants care for children will be enhanced. Participants’ emotional climate of care will be enhanced. Participants will be better equipped to provide a healthy and safe child care environment by the end of each 14-week session. Participants’ awareness of what it takes to prepare children for school will be enhanced. Long-Term Kith and Kin participants gain long-term peer support (social and emotional support) that continues beyond the 14-week training- support session. Kith and kin participants will increase the quality of care they provide for children. Kith and kin participants will be able to more successful at preparing children to succeed in school. INDICATORS Conduct recruitment and outreach activities. Host an annual health and safety training day, supply providers with smoke detectors, re extinguishers, car seats, outlet covers, rst aid kits and cribs. Child development knowledge gained from 14-week sessions. Measured by: Pre / Post Test Knowledge Survey Caregiving practices enhanced: engagement in learning activities with child; caregiver-child bidirectional communication; caregiver unidirectional use of language Measured by: CCAT-R: Action/Communication Snapshots and CCAT-R Behavior Checklist (Porter et al.)Quality of caregiving environment: Measured by: CCAT-R: Action/Communication Snapshots and CCAT-R Behavior Checklist; CCAT-R Materials Checklist Emotional climate of child care Measured by: Caregiver Interaction Scale (Arnett); CCAT-R: Nurturing subscale Home environmental safety Measured by: CCAT-R Health & Safety Checklist; Car-seat Safety Exam; CPR/First-Aid Certification Indices of support will increase: social support; child care affiliations; emotional support. Measured by: F-COPES Social Support Scale; Perceived Needs Survey (Dunst) Providers’ attitudes and beliefs about child care and child development will re ect more nurturing attitudes; re ect more awareness of developmentally appropriate pedagogy Measured by: Pre / Post Test Knowledge Survey; Child Rearing Attitudes Survey (Block & Block) Arizona Kith and Kin Project Year 1 Evaluation Report APPENDIX B Theory of Change Conceptual Map Children will be ready to succeed in school and in life Children will experience high quality child care Children will spend their early years in healthy and safe environments Children will spend their early years in nurturing environments Beliefs and attitudes about children Perceived needs Social support Children will spend their early years in cognitively stimulating environments Provider Self-Efficacy Knowledge about child development Resources for child care Cultural validation Emotional Well-being Child Development Training Curriculum; Supportive Relationships; Safety Mobile Van (materials & equipment for health & safety); Health & Safety Training; Information on other Community Resources ASCC’s Arizona Kith and Kin Activities and Steps Towards Desired Outcomes 60 Arizona Kith and Kin Project Year 1 Evaluation Report APPENDIX C Pre/Post Test SECTION I: Please rate your level of agreement with the following statements. Question Strongly Agree Agree Neither agree nor disagree Disagree Strongly Disagree Do not know 1.Punishing a child is the only way to get him or her to behave. 2.A good child care provider does not need to ask anyone else for help in caring for children. 3.The best way to get a child to take a medicine is to call it “candy”. 4.Children should be served smaller portions of food than adults. 5.Before a child is old enough to talk, it is not necessary for a child care provider to talk to the child. 6.If a child gets sick in the middle of the day while in your care, it is safe to give them medicine from your cabinet. 7.It is possible to spoil an infant one year of age or younger. 8.Snacks are an important part of a child’s daily intake of food and nutrition. 9.A 2 and 3-year-old child should be able to sit quietly during story time. 10.Children learn from helping with cooking and household chores. 11.It is important to praise young children for good behavior. 12.It is good for a child to know their numbers and letters by the time they enter Kindergarten. 13.All children should be potty trained by 18 months of age. 14.If I have made sure my home is free of hazards, it is safe for me to leave a child alone while I fix lunch or clean the house. 15.It is safe to hold a fussy/crying baby on my lap while traveling in a car. 16.Children should finish everything on their plate before being allowed to leave the table. 17.If my smoke detector is constantly beeping, it is time to replace the batteries. 18.Children learn best by doing things themselves rather than listening to others. 61 Arizona Kith and Kin Project Year 1 Evaluation Report SECTION II: Please check the answer below that best fits your situation Question Yes 19.Car seats purchased from a second-hand store or garage sale are safe to use. 20.Five servings of fruits and vegetables are an important part of a child’s daily diet. 21.It is important to have a smoke detector in each sleeping area/bedroom of my home. 22.Children should use a booster car seat while traveling in a car until they are 4 feet 9 inches tall and approximately 80 pounds. 23.It is important to read to children every day. 24.I have an escape plan for my house in case of emergencies like a fire. 25.It is safe to turn a car seat to forward-facing when a child turns one year old and weighs 20 pounds. 26.It is important to have a planned daily schedule for the children in my care. 27.A child can sit in the front seat of a car as soon as they are tall enough to safely use a seat belt regardless of the child's age. 28.Harness straps on a car seat should be loose enough to slide your hand underneath. 29.I have a written agreement with the parent of the children in my care that outlines fees, services and/or payment schedule. 30.I have a library card. If yes, which library? 31.Do you know about the Child and Adult Care Food Program? (CACFP) If yes, do you participate in CACFP? ___ Yes ___ No 32.I have an emergency contact phone number for the parents of the children in my care. 33.I have participated in the Kith and Kin program before. If yes, how many times _____ If yes, what motivates you to return to the Kith and Kin program again? 62 _____ _____ _____ _____ No Arizona Kith and Kin Project Year 1 Evaluation Report 63








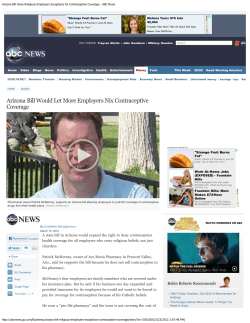
© Copyright 2026