
Document 62473
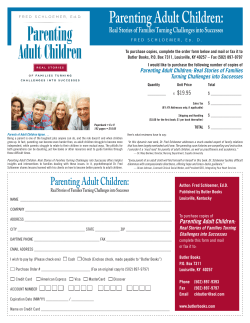
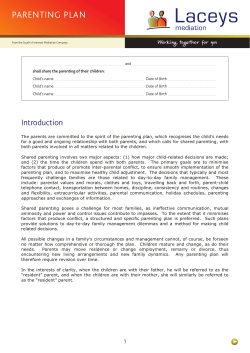
Child and Adolescent Mental Health Volume **, No. *, 2012, pp. **–** doi:10.1111/j.1475-3588.2011.00643.x Review: The contribution of mindfulness-based therapies for children and families and proposed conceptual integration Paul H. Harnett1 & Sharon Dawe2 1 School of Psychology, University of Queensland, St Lucia, Brisbane, Queensland 4072, Australia. E-mail: [email protected] 2 School of Psychology, Griffith University, Brisbane, Queensland, Australia Background: Mindfulness is the development of a nonjudgmental accepting awareness of moment-bymoment experience. Intentionally attending to oneÕs ongoing stream of sensations, thoughts, and emotions as they arise has a number of benefits, including the ability to react with greater flexibility to events and sustain attention. Thus the teaching of mindfulness-based skills to children and their carers is a potential means of improving family relationships and helping children achieve more positive developmental outcomes through increased ability to sustain attention and manage emotions. We provide a review of recent studies evaluating mindfulness-based interventions targeting children, adolescents, and families in educational and clinical settings. Method: Searches were conducted of several databases (including Medline, PsychINFO and Cochrane Reviews) to identify studies that have evaluated mindfulness-based interventions targeting children, adolescents or families published since 2009. Results: Twenty-four studies were identified. We conclude that mindfulnessbased interventions are an important addition to the repertoire of existing therapeutic techniques. However, large-scale, methodologically rigorous studies are lacking. The interventions used in treatment evaluations vary in both content and dose, the outcomes targeted have varied, and no studies have employed methodology to investigate mechanisms of change. Conclusions: There is increasing evidence that mindfulness-based therapeutic techniques can have a positive impact on a range of outcome variables. A greater understanding of the mechanisms of change is an important future direction of research. We argue that locating mindfulness-based therapies targeting children and families within the broader child and family field has greater promise in improving child and family functioning than viewing mindful parenting as an independent endeavor. Key Practitioner Message: • Mindfulness-based interventions hold promise for improving outcomes for children and adolescents • The number of mindfulness-based interventions being developed and evaluated is increasing rapidly • There is a need for greater methodological rigor in studies evaluating mindfulness-based therapies targeting children and adolescents • Understanding the mechanisms of change is important in the future development of mindfulness-based family interventions • Models of mindful parenting have been proposed to guide both research and the clinical application of mindfulness-based family interventions Keywords: Mindfulness; child development; parenting; intervention; mechanisms of change Mindfulness has been described as a process of developing a nonjudgmental accepting awareness of moment-by-moment experience (Bishop et al., 2004; Kabat-Zinn, 2005). This involves intentionally attending to oneÕs ongoing stream of sensations, thoughts, and emotions as they arise, without evaluating these phenomena as good or bad, true or false, healthy or sick (Baer, 2003). The practice of mindfulness is integral to Eastern spiritual, philosophical traditions, most notably Buddhism from which much of the understanding and practice of mindfulness within Western psychotherapies has derived (Kang & Whittingham, 2010). When integrated into Western psychotherapies, mind- ful awareness and an accepting attitude toward moment-to-moment experience is taught as a way of helping people tolerate psychological and physiological distress. Insofar as mindfulness can also raise an individualÕs awareness of positive experiences that otherwise may not be attended to, mindfulness training has been used as a means of enhancing emotional well being and life satisfaction (Harnett et al., 2010). The turn of the century has seen a growing interest in mindfulness as evidenced by a comprehensive search of the research literature with the term ÔmindfulnessÕ. In 1990, a search of 30 databases across multiple disciplines resulted in 27 hits, when all publication types 2012 The Authors. Child and Adolescent Mental Health 2012 Association for Child and Adolescent Mental Health. Published by Blackwell Publishing, 9600 Garsington Road, Oxford OX4 2DQ, UK and 350 Main St, Malden, MA 02148, USA 2 Paul H. Harnett & S. Dawe (journal articles, book reviews, and dissertations) were included. For the year 2010 the same search resulted in 1060 hits. Of particular interest for the current article was the increase in the number of peer-reviewed articles on mindfulness focusing on children, adolescents or families. Seven were found in 1990 compared to 55 in 2009 and 116 hits one year later (see Figure 1). With this rapid escalation of interest in mindfulness, it is timely to consider how the concept of mindfulness can contribute to efforts to improve child and family functioning. In this article, we first provide a review of intervention studies published since 2009. We then consider whether the teaching of mindfulness skills has the potential to contribute to the treatment of child and family functioning more broadly than has been attempted to date. We do so by considering the potential role of mindfulness in the light of an integrated theoretical framework for working therapeutically with families. Method The review builds upon a preliminary review of 15 studies on mindfulness-based approaches with children and adolescents written by Burke (2009). Searches were conducted in the following electronic data bases: PsychINFO, PSYarticles, Medline, Web of Science, and the Cochrane Library. Search terms included ÔÔmindfulnessÕÕ, ÔÔmeditationÕÕ ÔÔMBCTÕÕ, ÔÔMBSRÕÕ, ÔÔchildrenÕÕ, ÔÔadolescentsÕÕ, ÔÔyoung peopleÕÕ, ÔÔfamiliesÕÕ, and ÔÔschoolsÕÕ. Dissertation studies and conference papers were excluded and only articles written in English were considered. In examining the quality of the research evidence we focused on the following: (i) research design, including descriptive studies such as single-case designs, nonrandomized designs, studies that had a wait list control group and finally, as the design with the most rigorous support, randomized controlled designs; (ii) the extent to which the measures reflected the theoretical foundation of the intervention; and (iii) the dose of treatment and the extent to which the treatment was manualized or had a published description that addressed treatment fidelity (Mercer & Pignotti, 2007). Results of the literature review We identified 24 studies published since BurkeÕs review (2009) targeting children and adolescents that had been 1200 all disciplines-peer reviewed 1000 all disciplines-all publication types Number of hits child & family all disciplines-peer reviewed 800 child & family all disciplines-all publication types 600 400 200 0 1990 1992 1994 1996 1998 2000 2002 2004 2006 2008 2010 Year Figure 1. Number of hits from database searches of the term ÔmindfulnessÕ from 1990 to 2010 Child Adolesc Ment Health 2012; *(*): **–** conducted both in educational settings and with clinical groups either in the home or in clinical settings. The school-based studies tended to have a preventative focus and were generally delivered by teachers specifically trained in mindfulness procedures. The interventions evaluated in the school setting included programs for the children themselves and programs aimed at improving child outcomes by teaching mindfulness skills to teachers, carers or parents (e.g., Coatsworth, Duncan, Greenberg, & Nix, 2010; Duncan, Coatsworth, & Greenberg, 2009b). Two studies focused on reducing psychological distress of the teachers rather than children (Franco, Manas, Cangas, Moreno, & Gallego, 2010; Gold et al., 2010). A second group of studies used mindfulness-based strategies within clinical settings where children and young people were referred with an existing psychological disorder or identified as high risk for a stress-related physical disorder. While we have grouped the review into school-based and clinical settings, many of the techniques used to improve child outcomes were common to both types of studies. Mindfulness-based interventions delivered in educational settings Mindfulness-based interventions have been delivered in educational settings with both pupils and teachers (see Table 1). When considering those with a focus on improving emotional well being in children, Joyce, Etty-Leal, Zazryn, Hamilton, and Hassed (2010) report pre- and post-group differences in children aged 10– 13 years on measures of behavior problems and depression. The 10-week program delivered by teachers lead to a significant reduction in self-reported behavioral problems and depression scores at post-treatment. However, the gains were mainly limited to students showing clinically significant scores at preintervention. Targeting older adolescents, Broderick and Metz (2009) reported a study that involved a curriculum-based program delivered over six lessons. Using a non-randomized design with a small comparison group of younger school children, the authors reported a decrease in negative affect and an increase in feeling calm, relaxed, and self-accepting. Notably, however, there were no changes in any of the other measures including rumination, somatization and a well-established measure of emotional regulation – a key construct targeted in mindfulness interventions. Mixed findings were also reported by Schonert-Reichl and Lawlor (2010) in a study that included both a wait list control and measures of treatment fidelity in a large sample of fourth to seventh grade children. The mindfulness-based program, delivered by teachers, involved 10 lessons and three times daily practice of mindfulness meditation. Overall, there was a significant increase in scores on self-report measures of optimism (part of a larger scale focusing on resilience) and a trend toward an increase in positive emotions. There was no change in self-reported negative affect. An unusual finding was that students in the preadolescent group showed an improvement in self-concept, while students in the early adolescent group showed deterioration relative to controls. Teacher reports showed an improvement in social and emotional competence for children in the intervention group, and a decrease in aggression and oppositional behavior, although the lack of 2012 The Authors. Child and Adolescent Mental Health 2012 Association for Child and Adolescent Mental Health. N Participant Type 120 246 97 Broderick & Metz, 2009 Schonert-Reichl & Lawlor, 2010 Mendelson et al., 2010 Fourth and fifth grade students 4th–7th grade students All students of a senior high school class Studies targeting school students Joyce et al., 2010 175 Year 5 and 6 primary school students Study 9–10 years 11.4 years 17.4 years 10–13 years Age(years) School Classroom Classroom Classroom Study Setting 2 group RCT pre test post-test Quasi-experimental control group pre test post-test 2 group pre test post-test Pre test post-test Research design Table 1. Summary of mindfulness-based intervention studies in educational settings None Junior school students (n = 17) Wait list No treatment 6 · 30 min sessions (3 hr) of the Learning to BREATHE based on MBSR 10 · 40–50 min weekly sessions (7.5 hr) :mindfulness, selfregulation, goal setting, learned optimism; plus 3 · 3 min daily mindfulness practice 12 · 45 min sessions (9 hr) of mindfulness and yoga Control group 10 · 45 min sessions (7.5 hr) based on MBSR Treatment group Self-report: involuntary responses to stress; depression; peer and school relationships; affect Self-report: affect; emotional regulation; rumination; somatization Self-report: optimism; school and general self-concept; positive and negative affect. teacher report: social and emotional competence Self-report: child behavior problems; depression; DV < in child behavior problems for high and low scorers; < in depression for high scorers only; > in prosocial functioning for low scorers only. < in negative affect; > in feeling calm/relaxed/ self-accepting; No change in emotional regulation, rumination or somatization. > in self-reported optimism and positive affect for all students; no change in negative affect; > in self-reported general self concept for pre adolescents only. > in teacher report of attention, emotional regulation, social and emotional competence; < in teacher report of aggression and oppositional behavior. Good retention and acceptability of program to students and teachers; < in rumination, intrusive thoughts and emotional arousal; no change in positive or negative affect, depression, or relationships with peers and teachers; trend toward greater trust in friends. Results doi:10.1111/j.1475-3588.2011.00643.x Mindfulness-based therapies for families 2012 The Authors. Child and Adolescent Mental Health 2012 Association for Child and Adolescent Mental Health. 3 18 25 166 Liehr & Diaz, 2010 Semple et al., 2010 Gregoski et al., 2011 Afro-American adolescents at risk of cardio-vascular disease Children struggling academically Minority children Participant Type Duncan et al., 2009b 5 Families of nine children in 6th grade 11.5 years Care-givers own children aged 9–16 15 years 9–13 9.5 years Age(years) School Home School and home School School Study Setting Uncontrolled pilot study Multiple-baseline across participants 3 group RCT pre test post-test RCT 2 group RCT pre test post-test Research design Heath education; life skills training 12 · weekly (10 min weekdays, 20 mins weekends; 14 hr total; BAM) taken from MBSR None None Waitlist 12 · 90 min weekly sessions (18 hr) MBCT for children 7 session mindfulness training provided to carers to work with individuals in their care 7 · 2-hr sessions (14 hr; MSFP) Health education Control group 10 · 15 min sessions daily for 2 weeks (2.5 hr) of attention to breath, mindful movement and generosity. Treatment group Parent report: qualitative feedback Number of noncompliant responses made by children Physiological: ambulatory diastolic blood pressure; overnight sodium excretion; self-report: perceived stress Attention; anxiety; behavior Self-report: depression; anxiety DV Training carers in mindfulness in group home setting lead to < in non-compliant responses in carers own children. Qualitative feedback showing usefulness and acceptability of MSFP to parents. < in depression in intervention group only; < in anxiety in both intervention and control group. < in attention problems; < in anxiety, but no group differences; < in behavior problems, but no group differences. BAM group showed greatest improvement in systolic blood pressure; BAM group showed greater reduction in diastolic blood pressure and heart rate compared to LST; No change in perceived stress. Results Paul H. Harnett & S. Dawe Studies targeting parents, carers or teachers Singh et al., 2010 3 African American caregivers N Study Table 1. Continued 4 Child Adolesc Ment Health 2012; *(*): **–** 2012 The Authors. Child and Adolescent Mental Health 2012 Association for Child and Adolescent Mental Health. 2012 The Authors. Child and Adolescent Mental Health 2012 Association for Child and Adolescent Mental Health. 11 68 31 & 39 Gold et al., 2010 Franco et al., 2010 Jennings et al., 2011 - reported 2 studies th Teachers working in a high-poverty urban setting (study 1) and student teachers working in a semi-rural/ suburban college town setting (study 2) Secondary school teachers Qualified teachers teaching assistants Families of 5 –7 grade students transitioning from elementary school th Participant Type Pre test post-test Study 1: pre test post-test Study 2; waitlist control School Mean age teachers was 40 (study 1); mean age of student teachers was 21 (Study 2) Pre test post-test School School 20–50 years 3-group RCT (stratified by school district) pre test post-test Research design 24–58 years School Study Setting Child 11.7 years; mother 39.4 years Age(years) Two day weekend workshop, phone coaching and one day workshop - The Cultivating Awareness and Resilience in Education (CARE) professional development program None 8 · 2.5 hr weekly sessions (25 hr) of a mindfulness course taught by MBSR teacher 10 · 1.5 hr sessions (15 hr) of mindfulness program Listening to relaxing music Study 1: none Study 2: waitlist 1)7 · 2-hr 2) wait list control Control group 7 · 2-hr sessions (14 hr) of (MSFP) - parents and youth both involved in sessions Treatment group Teacher self-report: well being; depression; time urgency; physical symptoms; motivation orientation; teacher efficacy; mindfulness. Observations: classroom climate (study 2 only) Psychological distress Parent report: mindful parenting; Child management strategies; Maternal anger and affect toward child Youth report: discipline consistency Psychological distress, mindfulness DV Results Study 1 < in time urgency; > in mindfulness. No change in wellbeing, depression, physical symptoms, motivation orientation or teacher efficacy. Study 2 > in motivation orientation (support student autonomy); > in teacher efficacy. No difference in wellbeing, depression, physical symptoms, mindfulness or classroom climate. < in depression, stress, but not anixety; > in Ôaccept without judgmentÕ scale, but not other scales of the KIMS. < in psychological distress > in parental report of mindful parenting in MSFP group; > use of effective child management practices in both SFP and MSFP groups. > in youth report of parental discipline consistency in MSFP group. MBSR, Mindfulness Based Stress Reduction; MBCT, Mindfulness Based Cognitive Therapy; BAM, Breathing Awareness Meditation; MSFP Mindfulness-Enhanced Strengthening Families Program; KIMS, Kentucky Inventory of Mindfulness Skills. < indicates decrease in outcome; > indicates increase in outcome. 65 N Coatsworth et al., 2010 Study Table 1. Continued doi:10.1111/j.1475-3588.2011.00643.x Mindfulness-based therapies for families 5 6 Paul H. Harnett & S. Dawe independent ratings raises concerns about the reliability of these findings. Mendelson et al. (2010) employed a mindfulness-based intervention to improve self-regulatory capacities in fourth and fifth grade children from disadvantaged backgrounds. The current intervention included yoga-based physical activity, breathing techniques and guided mindfulness practice designed to help children manage arousal and stress levels. Randomization occurred at the school level with two schools receiving the intervention four days per week for 12 weeks while the other two schools served as wait list controls. The treatment was acceptable to both students and teachers and some significant reductions were found in the subscales and total score on a measure of involuntary response to stress. No effects were found on negative or positive affect, depression or peer relationships, although a trend was noted for greater trust in friends. There has been one small randomized trial in which a mindfulness-based intervention was compared to an active intervention focusing on improving depression and anxiety (Liehr & Diaz, 2010). In this study involving 18 children, minority and disadvantaged children recruited from a summer camp were randomly assigned to either a mindfulness-based intervention or to heath education. Children attended ten 15 min classes of mindful breathing and mindful movement over two weeks. There was a significant reduction in depression symptoms for those in the mindfulness group and a reduction in anxiety for both groups, in the immediate post-treatment follow up. Using a waitlist control, Semple et al. (2010) assessed the impact of a 12-week group program based on mindfulness-based cognitive therapy in children who were struggling academically. The authors proposed that anxiety influences attention, which in turn impacts academic performance. Significant improvements were found on measures of attention compared to the wait list. There were reductions in anxiety and behavior problems, although no group differences at posttest or follow-up. While the authorÕs suggestion that mindfulness served to enhance selfmanagement of attention and emotion regulation was supported, whether this, in turn, influenced academic performance was not tested. One randomized study investigated the impact of mindful breathing meditation on 166 Afro-American adolescents at risk of cardiovascular disease (Gregoski, Barnes, Tingen, Harshfield, & Treiber, 2011). Three-month interventions were offered in two high schools during regular health education classes. The interventions were delivered by teachers who were each randomly assigned to deliver one of the interventions. The teachers were provided with training in an intervention and treatment fidelity measures assessed adherence to treatment. Breathing awareness meditation produced greater reductions in systolic blood pressure compared to Life Skills Training (LST) or the usual Health Education program. Participants taught breathing meditation also showed greater reductions for 24 hr diastolic blood pressure and heart rate compared to LST. Six studies reported interventions that targeted the parents, carers or teachers of children. Singh et al. (2010) investigated the transfer of mindfulness skills following mindfulness training of carers in a group home for individuals with severe physical and intellec- Child Adolesc Ment Health 2012; *(*): **–** tual disabilities. Records were kept of non-compliant responses by the carersÕ own children. Results showed that the mindfulness training they received in the work context transferred to the home context, demonstrated by a reduction in noncompliant responses by the carers children. A small pilot study involving five families reported by Duncan et al. (2009b) described a modification of the Strengthening Families Program (SFP), an evidence-based, universal, family focused intervention designed to reduce risk factors and enhance protective factors as a means of preventing adolescent substance use and problem behaviors. The modifications included teaching the principles of mindfulness and specific mindfulness practices such as mindful breathing. Results were limited to positive qualitative feedback. However, in a larger scale study, Coatsworth et al. (2010) found the addition of the mindfulness component in MSFP resulted in improvements on a newly developed measure of mindful parenting, while the youths reported their parents to be more consistent in their use of discipline. Two studies targeting teachers found that a course in mindfulness lead to reduced psychological distress for those who participated (Franco et al., 2010; Gold et al., 2010). Jennings et al. (2011) found mixed support for the Cultivating Awareness and Resilience in Education (CARE) professional development program designed to reduce teachersÕ distress and promote improvements in teachersÕ well being, motivational orientation/efficacy, and mindfulness. A significant increase in mindfulness was found in only one of the two studies reported. One study found a decrease in teacherÕs sense of time urgency, suggesting that teachers experienced less stress associated with time demands after participating in the program. The increase in mindfulness was found when CARE was offered to a group of experienced teachers working in an urban district with high levels of poverty, a high proportion of at-risk students and a context of limited institutional support. CARE was designed for teachers working in the context of high emotional stress that can lead to emotional reactivity in the classroom. The program did not appear to be relevant to a group of student teachers and mentors working in a less stressful semirural setting with few at risk students and effective institutional support. On balance there is reasonable cause for optimism when considering whether to include mindfulnessbased approaches within an existing school curriculum and targeting both students and teachers. Positive mood does appear to be increased while more traditional measures of mood symptoms in particular depression, show reductions. What is clearly needed, however, is a clearer understanding of what treatment should consist of and the dose of treatment that is necessary to effect change given the considerable variability noted across the studies reviewed above. Variability in outcome measures and methodological limitations of studies, which are discussed in more detail below, limit conclusions that can be drawn. Mindfulness-based interventions delivered in clinical settings Single case studies have been conducted by Singh and colleagues using meditation-based strategies to reduce aggressive behavior in young people with autism or 2012 The Authors. Child and Adolescent Mental Health 2012 Association for Child and Adolescent Mental Health. doi:10.1111/j.1475-3588.2011.00643.x Asperger syndrome (Singh, Lancioni, Manikam, et al. 2011; Singh, Lancioni, Singh, et al. 2011). In these studies mothers, after being trained in a meditative procedure, taught their children to redirect attention from an aggression-triggering event to a neutral body part – the soles of their feet. In both studies parents and siblings reported a decrease in the frequency of aggressive incidents suggesting that the adolescents with developmental disorders can learn, and effectively use, a mindfulness-based procedure to self-manage their physical aggression. Several studies reported on the effectiveness of mindfulness-based treatments incorporated into either an existing treatment process or delivered as a standalone treatment in clinical populations. Britton et al. (2010) conducted a prospective uncontrolled clinical trial of 55 adolescents who had been recent inpatients receiving substance abuse treatment. Six 90 min group sessions based on MBSR aimed to improve sleep with the rationale that poor sleep contributes to mood problems, which in turn may increase the risk of relapse to substance use. Outcomes were emotional distress, relapse and substance use measured across 60 weeks. Completion (defined as attendance at 4 of 6 sessions) was poor (42%) and substance use increased across the group. There were, however, significant improvements on measures of emotional distress with a trend favoring those who were classified as completers and a reduction in daytime sleepiness for those who completed the program. A study of youth who were either HIV infected or Ôat riskÕ who were attending a pediatric primary care clinic investigated the impact of an MBSR program on health-related quality of life and psychological distress. Youth self-reports found a statistically significant decrease in hostility and general and emotional discomfort. However, significant improvement was found on only three of 18-subscales. A small-scale uncontrolled trail of a mindfulness-based program for adolescents diagnosed with ADHD found little change on a variety of measures (van de WeijerBergsma, Formsma, Bruin, & Bögels, 2011). While there was some improvement in the adolescentsÕ behavior and attention, and some reduction of parenting stress in fathers and overreactivity in mothers, these changes were not reported by all informants and were generally not sustained at follow-up. However, the study was very small, with data from only eight participants available for analysis. Thus, the statistical power to detect change was very low. Two randomized controlled trials compared mindfulness-based treatment with an active alternative treatment. In a small study of depressed adolescents, Hayes, Boyd, and Sewell (2011) found that an adaptation of Acceptance and Commitment Therapy for adolescents produced greater decreases in a measure of depression compared to treatment as usual (cognitive behavioral therapy). There were also decreases in behavior problems, although this difference was not significantly greater for the ACT condition. Finally, Catani and colleagues investigated the effectiveness of meditation-relaxation compared to narrative exposure therapy in traumatized children living in refugee camps in Sri Lanka (Catani et al., 2009). The latter treatment protocol was designed specifically for people who have been exposed to enduring trauma associated with war Mindfulness-based therapies for families 7 and torture. Treatment was delivered by local therapists trained in the two models. Treatment duration was of equal length (six 60–90 min sessions over two weeks). Follow up occurred 4–5 weeks and again 6 months later by interviewers blind to the treatment condition. While there were no differences between the two treatments, the reductions in post-traumatic symptoms were striking, with recovery rates of 81% for the narrative exposure group and 71% for the meditation relaxation group post-treatment. The improvements were maintained at 6 months. Oord, Bögels, and Peijnenburg (2011) reported on a randomized controlled trial with a short (8 weeks) follow-up period. The study evaluated an 8-week mindfulness course for children displaying symptoms of ADHD that included a parallel course for parents. Statistically significant changes between preand post-intervention included a decrease in both child and parent ADHD symptoms and an increase in parental mindfulness as measured by the Mindfulness Attention and Awareness Scale. No changes were observed in parenting stress or parenting style. At follow-up, the reduced levels of ADHD symptoms remained for both children and parents. A reduction was found in over-reactive parenting and parental stress between the pre-intervention and follow-up assessment. However, mindfulness scores did not vary between pre-intervention and follow-up. Our own work in this area has involved the evaluation of an intensive home visiting program focusing on multiproblem families characterized by emotional dysregulation, maternal psychopathology, and substance abuse. The program, Parents Under Pressure (PuP), is based on the premise that sensitive and responsive parenting requires emotional regulation skills that are generally dysfunctional in parents with a history of trauma or psychopathology, including substance misuse and mood disorders. Thus the program draws from the recent literature on emotional regulation with an explicit adaption of mindfulness strategies integrated with parenting skills. The PuP program has been evaluated in three separate case studys (Dawe, Harnett, Rendalls, & Staiger, 2003; Frye & Dawe, 2008; Harnett & Dawe, 2008) and one randomized controlled trial (Dawe & Harnett, 2007). These studies found a reduction in child abuse potential as well as reductions in maternal mood difficulties and parenting stress. Notably, the studies did not directly measure mindful parenting or parental emotional regulation capacity. As in other studies, measures of mood were used as proxy measures of this. Overall, the studies carried out in clinical settings, like those in educational settings, justify optimism for the potential of mindfulness based therapies to improve child, adolescent and family functioning. In addition to the efficacy of programs that deliver interventions directly to children and adolescents, programs that target parents and carers appear to be effective in improving parental functioning, and in turn, promote positive child outcomes. Methodological limitations While the majority of the studies reviewed were pilot studies that had a range of methodological problems, a small number of studies have been randomized control trials. Thus, some caution needs to be exercised when 2012 The Authors. Child and Adolescent Mental Health 2012 Association for Child and Adolescent Mental Health. 33 10 Sibinga et al., 2011 van de WeijerBergsma et al., 2011 55 3 3 Singh, Lancioni, Singh et al., 2011a Lancioni, Manikam, Singh et al., 2011a Britton et al., 2010 N Study Adolescents with ADHD Adolescents with sleep problems following substance abuse treatment HIV-infected and at-risk youth Adolescents with Asperger Syndrome Adolescents with Autism Participant Type Academic treatment center Pediatric primary care hospital clinic 13–21 11–15 Outpatient Home Home Location of intervention 16.4 (SD = 1.2) 14–17 13–18 Age Pre-post with 8 week followup Pre-post Pre-post Multiple-baseline across participants Multiple-baseline across participants Research design Table 2. Summary of mindfulness-based intervention studies in clinical settings None None None None 6 · 90 min weekly group sessions (9 hr) modified (MBSR) and CBT 8 · ? weekly sessions based on MBRS. 8 · 90 min weekly group mindfulness sessions for adolescents. Eight parallel sessions with parents. None Comparison treatment 5 days of training in Meditation on the Soles of the Feet 17–24 weeks of ÔMeditation on the Soles of the FeetÕ Treatment group Adolescent report: behavior; executive functioning; mindfulness; fatigue; happiness; attention. Mother and father report: behavior; mindfulness; parenting style; parenting Stress. Teacher report: behavior Self-report: health related quality of life; psychological distress Self-report: emotional distress; relapse resistance; substance use Number of aggressive incidents Number of aggressive incidents DV < in one of nine domains of psychological distress (hostility); > in two of nine domains of quality of life (general and emotional discomfort). < in externalizing behavior problems reported by fathers only; < in executive functioning problems reported by fathers only; > in some aspects of attention, but overall no change; no change in adolescent internalizing, attention problems. fatigue or happiness; no change in adolescent or parent mindfulness; < in parenting stress for fathers but not mothers at post but nor follow-up; < in mothers overreactivity at post but not follow-up > in substance use; < in emotional distress;< in daytime sleepiness for completers only. < in aggressive incidents maintained over 3 years. < in aggressive incidents maintained over 4 years. Results 8 Paul H. Harnett & S. Dawe Child Adolesc Ment Health 2012; *(*): **–** 2012 The Authors. Child and Adolescent Mental Health 2012 Association for Child and Adolescent Mental Health. 12 Families on methadone maintenance In home, 4 years In home, parents referred by community methadone clinic 12 sessions · 1.5 hr/per session DV 6 sessions Narrative Exposure Therapy None None < in depression greater for ACT than TAU; greater proportion of ACT condition showed clinically significant change in depression; no change in behavioral problems. < PTSD symptoms at 1 month for both groups. Results Pre-post change: < parent reported child ADHD symptoms; < parent ADHD symptoms; > Mindful awareness of parents; no change in parenting stress or parenting style. Pre-Follow-up change: < child ADHD symptoms; < parent ADHD symptoms; < parenting stress; < in over-reactive parenting style; no change in parental mindful awareness. Parent report: parenting 9 of 12 completed stress, child program, reduction in abuse potential, child behavior variables measured problems, drug use, alcohol use, found for 6/7 of the Risk taking behavior families except risk behaviors where only three showed a decrease Parent report: parenting stress, All 10 families were mood, child abuse potential, followed up. Significant child behavior problems, social < on all measures support pre-post, 2 of 10 families showed no change on any domain. Parent report: parenting stress; parenting style; mindful awareness; parent ADHD symptoms. Parent & teacher report: child ADHD symptoms; child behavior problems. PTSD symptoms TAU-manualized Depression, Emotional and CBT provided by behavioral functioning the psychiatric service Comparison treatment 8 · 90 min weekly group none sessions for parents based on MBCBT and MBSR.Parallel sessions with children. 6 sessions Meditationrelaxation ACT -individual sessions using published treatment manuals Treatment group Single case study, Mean number of pre postsessions 11.5 measures (range 9–13) Single case study, pre post-measures Outpatient Waitlist mental control; 8 health clinic week follow-up 8–12 RCT RCT Research design Community transitory camp Outpatient psychiatric clinic Location of intervention 8–14 12–18 Age Harnett & 10 Families <8 Dawe, 2008 referred by child protection services Dawe et al., 2003 Catani et al., 31 Children 2009 affected by tsunami in northeastern Sri Lanka Oord et al., 22 Children with 2011 ADHD and their parents 38 Adolescents experiencing moderate to severe depressive symptoms Hayes et al., 2011 Participant Type N Study Table 2. Continued doi:10.1111/j.1475-3588.2011.00643.x Mindfulness-based therapies for families 2012 The Authors. Child and Adolescent Mental Health 2012 Association for Child and Adolescent Mental Health. 9 Child Adolesc Ment Health 2012; *(*): **–** MBSR, Mindfulness Based Stress Reduction; ACT, Acceptance and Commitment Therapy; TAU, treatment as usual. < indicates significant decrease in outcome; > indicates significant increase in outcome. 12 Women offenders 5.6 years In home or in low in low security or security just released prison Frye & Dawe Dawe & 64 Families on Harnett, 2007 methadone maintenance DV Comparison treatment Treatment group Research design Location of intervention Participant Type Age N Study Table 2. Continued Single case Mean number of None Parent report: parenting stress, 8 remained in treatment, mood, child abuse potential, Significant < on all study, pre sessions for treatment post- & 3-month completers 20 child behavior measures at 3 month (range 11–38) follow up follow up measures Mean number of sessions TAU, 2 sessions Parent report: parenting stress, Significant < on all Randomized 3.5 years In home, measures for PuP controlled for PuP group clinic based mood, child abuse potential, parents 10.5 (SD = 2.9) on parenting child behavior Methadone dose, group, significant < trial referred on child abuse information by community potential for brief methadone intervention, > on clinic child abuse potential in TAU group Paul H. Harnett & S. Dawe Results 10 considering the balance of evidence for including mindfulness into interventions for children and families. The heterogeneity of the populations in which studies have been conducted makes it difficult to build a consistent picture of efficacy, although arguably does speak to the issue of generalizability. Related to the issue of diversity in populations studies is the range of outcome measures adopted, again leading to little consistency to allow for a more measured appraisal of the benefits of mindfulness. The dimensions of functioning measured included behavioral (internalizing and externalizing problems), emotional (psychological distress, emotional regulation), cognitive (rumination, attention, self concept) social (peer functioning, relationship with parents), child abuse potential and health (blood pressure). Only a small number of studies measured the construct of mindfulness itself, which is largely explained by the lack of a suitable instrument to measure mindfulness in young people over the period the studies were conducted. Only recently has a promising measure been described in the literature (Greco, Baer, & Smith, 2011). While the interventions being evaluated can be classified as Ômindfulness-basedÕ, there was in fact a large variation in both the content and dose of the interventions evaluated. In around half of the studies, the intervention involved an adaptation of the Mindfulness Based Stress Reduction program (Kabat-Zinn, 2003), although there was no single agreed adaptation of this program. Other programs adapted included Mindfulness Based Cognitive Therapy and Acceptance and Commitment Therapy – programs that have differing theoretical underpinnings and were developed for adults. The adaptations described for use with children and adolescents were generally practical concerns (e.g., shorter duration sessions for children with limited attention spans) rather than adaptations informed by models of child development and family functioning. In general, the sample size of the studies reviewed was small, compromising the power to detect changes in participant functioning. Most studies assessed only the short-term impact of interventions using pre-post designs. When follow-up assessments were included they were generally short (around 8 weeks). Thus it is not possible to determine how enduring the treatment effects may be both in the presence and absence of ongoing meditative practice. A primary concern was the lack of focus on evaluation mechanisms of change, a point we turn to next. Parental mindfulness and proposed mechanisms of change Despite the methodological limitations, sufficient studies showed evidence that mindfulness-based techniques led to positive changes to justify optimism for the inclusion of mindfulness-based techniques as part of a practitionerÕs therapeutic repertoire for treating children and families. However, we see a problem for the field to be the proliferation of Ômindfulness-basedÕ interventions targeting children and families that vary both in content and dose, as well as their theoretical underpinnings. Kazdin has persuasively argued that the emphasis of research in the child and family field should be on developing a greater understanding of the 2012 The Authors. Child and Adolescent Mental Health 2012 Association for Child and Adolescent Mental Health. doi:10.1111/j.1475-3588.2011.00643.x active ingredients of programs if any are to be optimally effective (Kazdin, 2007; Kazdin & Nock, 2003). While ÔmindfulnessÕ as a psychological construct is assumed to be responsible for improved outcomes, this was not systematically investigated in any of the studies above. One obstacle for research on mechanisms of change is the lack of psychometrically sound measures of the construct of ÔmindfulnessÕ as it relates to parents and children. We note that two measures are in development that will help to facilitate such research in the future (Coatsworth, Duncan, Greenberg, & Nix, 2009; Greco et al., 2011). However, another obstacle has been the lack of an agreed model of mindful parenting to guide research on mechanisms of change. An important development, then, are recent attempts to identify the mechanisms that change as a consequence of improved parental mindfulness. Duncan, Coatsworth, and Greenberg (2009a) describe a model of mindful parenting that focuses on the benefits of mindfulnessbased interventions to enhance the parent-child relationship. Specifically, the authors suggest that parents who acquire mindfulness skills will have an enhanced capacity to listen with full attention (increased sensitivity to the childÕs cues); will adopt a more nonjudgmental acceptance of self and child (a balance between parent-orientated, child-orientated, and relationship orientating goals); have greater emotional awareness of self and child (acknowledgment of the childÕs emotional state and responding to the childÕs needs with less negative emotions); be better able to self-regulate in the parenting relationship (maintaining a focus on long term parental goals and values and avoidance of shortterm automated reactive responses); and display more compassion for self and child (the expression of more positive affect toward the child and avoidance of self-blame in the parenting role). More recently Bögels, Lehtonen, and Restifo (2010) have argued that mindfulness-based interventions improve aspects of attention, in particular the ability to disengage from unexpected and emotionally charged stimuli. Integrating findings from the experimental literature on mindfulness, the authors suggest mindfulness-based parenting interventions may exert their effects by: (a) reducing parental stress; (b) reducing parental preoccupation resulting from parental and/or child psychopathology; (c) improving parental executive functioning (in particular reduced impulsivity); (d) reducing the impact of dysfunctional upbringing schemas and habits; (e) increasing self-nourishing attention; and (f) improving marital functioning and co-parenting. In a recent cross-sectional study of Duncan et al.Õs (2009a) model, Parent et al. (2011) investigated the relationship between parental mindfulness, parental depression, positive and negative parenting practices (based on observations of parent-child interactions) and child outcomes (internalizing and externalizing problems). Correlational analyses carried out on the results of 180 families involving 242 children aged 9–15 showed that parental mindfulness was associated with both internalizing and externalizing problems of the children. Regression analyses failed to find that parental depressive symptoms or positive or negative parenting behaviors acted as intervening variables to explain the significant association. While this might suggest mindfulness has a direct effect on child outcomes, the Mindfulness-based therapies for families 11 authors speculated that other variables not measured in their study, possibly parental emotion regulation or adaptive coping skills, might be candidates to explain the relationship. This conclusion is consistent with the model of mindful parenting put forward by Duncan et al.Õs (2009a) and the mechanisms proposed by Bögels et al. (2010); specifically that heightened parental awareness of their own and their childÕs emotional states and enhanced parental emotional regulation skills allow the parent to respond more flexibly to the child, as opposed to responding with a ÔmindlessÕ automated negative reactivity. Placing mindfulness within a broader context While the ÔmindfulnessÕ of children and parents is a variable that may prove to be a key factor in adaptive functioning, there is a danger that a focus on mindfulness in isolation from other variables influencing the development of children and functioning of families could limit consideration of the full range of variables that potentially mediate outcomes in treatment. We suggest the benefits of mindfulness-based interventions targeting families would be better considered within the context of an integrated framework of family functioning, one that is itself informed by existing models of child development and family functioning (Cicchetti & Cohen, 2006; Sameroff, 2010). That is, we suggest that mindfulness-based interventions may be better considered as one strategy for obtaining positive outcomes when working with children and their families rather than an endeavor in its own right. We present here an integrated framework (Figure 2) for working with families and consider below how mindfulness-based interventions can sit within and complement other intervention strategies. Indeed an important implication of the integrated framework is that changes in mindfulness can be tested as mediators and moderators of change across multiple domains of functioning. The integrated framework we propose takes, as its starting point, the aim of promoting positive child developmental outcomes across multiple domains of a childÕs functioning and across time. This is achieved by targeting both proximal and more distal domains of family functioning. Those influences most proximal to a child are (a) the quality of the parent child relationship and (b) how the parent behaves in their parenting role. In regards to the quality of the parent child relationship, the framework draws on BiringenÕs work on emotional availability (Biringen, 2000, 2004). This model delineates the dimensions of the parent-child relationship that predict the quality of parent-child attachment and other child developmental outcomes. Four dimensions describe the behavior of the parents – the ability to respond sensitively to the child (sensitivity), provide structure to help the child manage their emotions and behaviors (structuring), promote autonomy (non-intrusiveness); and minimize angry and hostile interactions (non-hostility). In addition to being emotionally available, the integrated framework highlights the importance of parental values and expectations of the child as major influences on the choices a parent make about issues such as their style of discipline, level of child monitoring and importance of family routines. 2012 The Authors. Child and Adolescent Mental Health 2012 Association for Child and Adolescent Mental Health. 12 Paul H. Harnett & S. Dawe Child Adolesc Ment Health 2012; *(*): **–** Figure 2. Integrated framework Critically, however, and an area that typically receives less focus in many traditional family focused interventions, the integrated framework suggests that the extent to which the parentsÕ capacity to be emotionally available and ability to consistently implement parenting practices based on fair and reasonable values and expectations is directly influenced by the parentÕs emotion regulatory capacities. Parents create a social and emotional climate to which children must learn to self-regulate, as well as provide the safety net when selfregulation fails (Sameroff, 2010). High levels of parental emotional dysregulation results in a high stress environment and impairs the parentÕs capacity to be emotionally available. Thus a significant contribution that mindfulness can make is to provide a therapeutic approach that may directly enhance this self-regulatory capacity. However, the integrated framework acknowledges parental functioning and a childÕs development are affected by multiple influences, including the resources (or lack of) available to the family, schools, neighborhoods, culture and economic and political climate (e.g., Bronfenbrenner, 1986; Sameroff, 2010). Thus, the ecological context in which the family is embedded is an important target for therapy – by helping parents manage those aspects of the social ecology that are amenable to change, such as managing life stressors and engaging support. Mindfulness and the integrated framework A common theme of the articles reviewed was that mindfulness leads to greater acceptance of problem child behavior by parents, carers and teachers that leads to an increase in the quality of the relationship with the children in their care. For example, Singh et al. (2010) speculated that mindfulness training might produce a transformational change in carers that does not occur following training in contingency management and specific methods of behavior management. On the contrary, mindfulness training leads to nonjudgmental acceptance of problem behavior that is responded to more favorably by the children in their care, improving the quality of the carer–child interactions. This was echoed by Coatsworth et al. (2010) who found changes in parental discipline and monitoring by mothers in the standard Strengthening Families Program was not received well by the youth in their study. Children whose mothers received mindfulness training in addition to SFP reported their mothers to be more consistent in their use of discipline and more likely to monitor where they were and who they were with. Children from the SFP group reported slight increases in motherÕs negative affect directed toward them, while MSFP children reported a decrease in negative affect (despite positive affect remaining high throughout). Mothers in the MSFP condition perceived their children to display more positive and less negative affect, whereas mothers in the SFP condition perceived less positive affect and more negative affect from their children. The authors suggested that when disciplinary strategies are taught in conjunction with mindful parenting, parents are able to modulate their emotional reactivity to their childrenÕs behavior and this may have contributed to building a closer and more loving relationship between parent and children (Coatsworth et al., 2010). Within the school environment Gold et al. (2010) noted that teachers described the intervention to be helpful in controlling their stress because they became more accepting and nonjudging. The authors report that ÔResponding, not reacting, teaches us to take controlÕ (p. 188). There is some empirical support for this suggestion. Two studies by Bluth and Wahler (2011a,b) tested the hypotheses that mothersÕ everyday mindfulness would covary inversely with the effort they put into parenting, that mothersÕ mindfulness will covary inversely with their reports of their childrenÕs problem behavior, and that mindfulness would mediate or moderate the correlation between their effort and their reports of their childrenÕs problem behavior. Parenting effort was described as emotionally taxing 2012 The Authors. Child and Adolescent Mental Health 2012 Association for Child and Adolescent Mental Health. doi:10.1111/j.1475-3588.2011.00643.x struggles parents have when trying to handle challenging situations with their children, such as reacting emotionally in the moment rather than disciplining in a manner more in line with their values. Bluth and Wahler found that mothers reporting high mindfulness were less intrusive and more able to avoid the escalation of conflicts with their adolescents (Bluth & Wahler, 2011a) and pre-schoolers (Bluth & Wahler, 2011b) compared to mothers who were classified as low mindfulness. The authors argued that parental mindfulness has the potential to interrupt or de-escalate a chaotic or emotionally charged situation. Mindful parents can be more aware of their habitual patterns of parent-child interaction, leading to a less reactive and more nuanced responses, that requires less effort. Our integrated framework acknowledges the important influence of the social ecology within which the family is embedded. At this level mindfulness-based therapeutic techniques have a potentially important role to play. Duncan and Bardacke (2010) in a study of pregnant women reported that mindfulness training helped the women cope with stressful aspects of pregnancy and family life post-intervention, expanding their repertoire of skills to cope with contextual demands such as poverty, major life events, work related stress and interpersonal tensions (Duncan & Bardacke, 2010). The ability to employ mindfulness skills to protect against such adversity is worthy of increased attention given the negative impact of stressors associated with low SES on individual and family functioning (McEwen & Gianaros, 2010). In a recent study Sturge-Apple, Skibo, Rogosch, Ignjatovic, and Heinzelman (2011) found that mothers facing the stress of extremely low social economic status displayed abnormal sympathovagal activity (hyporarousal). This physiological reaction, the result of the need to adjust to chronic stress, was associated with disengaged and insensitive interactions with their children during observations of free play. Importantly, Ganzel, Morris, and Wethington (2010) have presented evidence pointing to the potential of mindfulness-based therapies to significantly influence the physiological processes associated with individuals physiological adjustment to ongoing stress – raising the hope that mindfulnessbased therapies can potentially promote improved family functioning and child outcomes in socially and economically disadvantaged families (see Repetti, Robles, & Reynolds, 2011). Conclusion The results of the research conducted thus far suggest that mindfulness-based techniques have the potential to improve aspects of individual and family functioning that are associated with better developmental outcomes for children and families. However, we argue that the outcomes of interventions targeting children, adolescents, and families will be most informative if the mindfulness-based therapeutic techniques are integrated into existing programs that address multiple domains of family functioning rather than pursued as an independent endeavor. It is important that the field avoids continued proliferation of programs and focuses more on understanding the mechanisms responsible for change. ÔMindfulnessÕ is emerging as an active Mindfulness-based therapies for families 13 ingredient of interventions, but is unlikely to be the sole variable responsible for the changes in outcome. Acknowledgement This review article was commissioned by the Editors of the journal, for which the first author received a small honorarium towards expenses. The authors have both declared that they have no competing or potential conflicts of interest arising from the publication of this article. References Baer, R.A. (2003). Mindfulness training as a clinical intervention: A conceptual and empirical review. Clinical Psychology: Science & Practice, 10, 125–143. Biringen, Z. (2000). Emotional availability: Conceptualization and research findings. American Journal of Orthopsychiatry, 70, 104–114. Biringen, Z. (2004). Raising a secure child: Creating emotional availability between parents and your children. New York: The Berkley Publishing Group. Bishop, S.R., Lau, M., Shapiro, S., Carlson, L., Anderson, N.D., Carmody, J., et al. (2004). Mindfulness: A proposed operational definition. Clinical Psychology: Science Practice, 11, 230–241. Bluth, K., & Wahler, R.G. (2011a). Does effort matter in mindful parenting? Mindfulness, 2, 175–178. Bluth, K., & Wahler, R.G. (2011b). Parenting preschoolers: Can mindfulness help? Mindfulness, 2, 282–285. Bögels, S.M., Lehtonen, A., & Restifo, K. (2010). Mindful parenting in mental health care. Mindfulness, 1, 107–120. Britton, W.B., Bootzin, R.R., Cousins, J.C., Hasler, B.P., Peck, T., & Shapiro, S.L. (2010). The contribution of mindfulness practice to a multicomponent behavioral sleep intervention following substance abuse treatment in adolescents: A treatment-development study. Substance Abuse, 31, 86–97. Broderick, P.C., & Metz, S. (2009). Learning to breathe: A pilot trial of a mindfulness curriculum for adolescents. Advances in School Mental Health Promotion, 2, 35–46. Bronfenbrenner, U. (1986). Ecology of the family as a context for human development: Research perspectives. Developmental Psychology, 22, 723–742. Burke, C.A. (2009). Mindfulness-based approaches with children and adolescents: A preliminary review of current research in an emergent field. Journal of Child and Family Studies, 19, 133–144. Catani, C., Kohiladevy, M., Ruf, M., Schauer, E., Elbert, T., & Neuner, F. (2009). Treating children traumatized by war and tsunami: A comparison between exposure therapy and meditation-relaxation in North-East Sri Lanka. BMC Psychiatry, 9, 22. Cicchetti, D., & Cohen, D.J. (2006). Developmental psychopathology: Theory and method (2nd edn). New York: John Wiley and Sons. Coatsworth, J.D., Duncan, L.G., Greenberg, M.T., & Nix, R.L. (2009). changing parentÕs mindfulness, child management skills and relationship quality with their youth: results from a randomized pilot intervention trial. Journal of Child and Family Studies, 19, 203–217. Coatsworth, J.D., Duncan, L., Greenberg, M., & Nix, R. (2010). Changing parentÕs mindfulness, child management skills and relationship quality with their youth: Results from a randomized pilot intervention trial. Journal of Child and Family Studies, 19, 203–217. Dawe, S., & Harnett, P.H. (2007). Reducing potential for child abuse among methadone-maintained parents: Results from a randomized controlled trial. Journal of Substance Abuse Treatment, 32, 381–390. Dawe, S., Harnett, P.H., Rendalls, V., & Staiger, P. (2003). Improving family functioning and child outcome in methadone maintained families: The parents under pressure program. Drug and Alcohol Review, 22, 299–307. 2012 The Authors. Child and Adolescent Mental Health 2012 Association for Child and Adolescent Mental Health. 14 Paul H. Harnett & S. Dawe Duncan, L.G., & Bardacke, N. (2010). Mindfulness-based childbirth and parenting education: promoting family mindfulness during the perinatal period. Journal of Child and Family Studies, 19, 190–202. Duncan, L.G., Coatsworth, J.D., & Greenberg, M.T. (2009a). A model of mindful parenting: Implications for parent-child relationships and prevention research. Clinical Child and Family Psychology Review, 12, 255–270. Duncan, L.G., Coatsworth, J.D., & Greenberg, M.T. (2009b). Pilot study to gauge acceptability of a mindfulness-based, family-focused preventive intervention. Journal of Primary Prevention, 30, 605–618. Franco, C., Manas, I., Cangas, A.J., Moreno, E., & Gallego, J. (2010). Reducing teachersÕ psychological distress through a mindfulness training program. Spanish Journal of Psychology, 13, 655–666. Frye, S., & Dawe, S. (2008). Interventions for women prisoners and their children in the post-release period. Clinical Psychologist, 12, 99–108. Ganzel, B.L., Morris, P.A., & Wethington, E. (2010). Allostasis and the human brain: Integrating models of stress from the social and life sciences. [Research Support, N.I.H., Extramural Review]. Psychological Review, 117, 134–174. Gold, E., Smith, A., Hopper, I., Herne, D., Tansey, G., & Hulland, C. (2010). Mindfulness-based stress reduction (MBSR) for primary school teachers. Journal of Child and Family Studies, 19, 184–189. Greco, L.A., Baer, R.A., & Smith, G.T. (2011). Assessing mindfulness in children and adolescents: Development and validation of the child and adolescent mindfulness measure (CAMM). Psychological Assessment, 23, 606–614. Gregoski, M.J., Barnes, V.A., Tingen, M.S., Harshfield, G.A., & Treiber, F.A. (2011). Breathing awareness meditation and LifeSkills Training programs influence upon ambulatory blood pressure and sodium excretion among African American adolescents. Journal of Adolescent Health, 48, 59–59. Harnett, P.H., & Dawe, S. (2008). Reducing Child abuse potential in families identified by social services: Implications for assessment and treatment. Brief Treatment and Crisis Intervention, 8, 226–235. Harnett, P.H., Whittingham, K., Puhakka, E., Hodges, J., Spry, C., & Dob, R. (2010). The short-term impact of a brief groupbased mindfulness therapy program on depression and life satisfaction. Mindfulness, 1, 183–188. Hayes, L., Boyd, C.P., & Sewell, J. (2011). Acceptance and commitment therapy for the treatment of adolescent depression: A pilot study in a psychiatric outpatient setting. Mindfulness, 2, 86–86. Jennings, P.A., Snowberg, K.E., Coccia, M.A., & Greenberg, M.T. (2011). Improving classroom learning environments by cultivating awareness and resilience in education (CARE): Results of two pilot studies. Journal of Classroom Interaction, 46, 37–48. Joyce, A., Etty-Leal, J., Zazryn, T., Hamilton, A., & Hassed, C. (2010). Exploring a mindfulness meditation program on the mental health of upper primary children: A pilot study. Advances in School Mental Health Promotion, 3, 17–17. Kabat-Zinn, J. (2003). Mindfulness-based stress reduction (MBSR). Constructivism in the Human Sciences, 8, 73–107. Kabat-Zinn, J. (2005). Full catastrophe living: Using the wisdom of your body and mind to face stress, pain, and illness: Fifteenth anniversary edition. New York: Delta Trade Paperback/Bantam Dell. Kang, C., & Whittingham, K. (2010). Mindfulness: A dialogue between Buddhism and clinical psychology. Mindfulness, 1, 161–173. Kazdin, A.E. (2007). Mediators and mechanisms of change in psychotherapy research. Annual Review of Clinical Psychology, 3, 1–27. Kazdin, A.E., & Nock, M.K. (2003). Delineating mechanisms of change in child and adolescent therapy: methodological issues and research recommendations. Journal of Child Psychology & Psychiatry & Allied Disciplines, 44, 1116–1129. Child Adolesc Ment Health 2012; *(*): **–** Liehr, P., & Diaz, N. (2010). A pilot study examining the effect of mindfulness on depression and anxiety for minority children. Archives of Psychiatric Nursing, 24, 69–71. McEwen, B.S., & Gianaros, P.J. (2010). Central role of the brain in stress and adaptation: Links to socioeconomic status, health, and disease. Annals of the New York Academy of Sciences, 1186, 190–222. Mendelson, T., Greenberg, M.T., Dariotis, J.K., Gould, L.F., Rhoades, B.L., & Leaf, P.J. (2010). Feasibility and preliminary outcomes of a school-based mindfulness intervention for urban youth. Journal of Abnormal Child Psychology: An official publication of the International Society for Research in Child and Adolescent Psychopathology, 38, 985–994. Mercer, J., & Pignotti, M. (2007). Shortcuts cause errors in systematic research syntheses: Rethinking evaluation of mental health interventions. The Scientific Review Of Mental Health Practice, 5, 59–77. Oord, S., Bögels, S.M., & Peijnenburg, D. (2011). The effectiveness of mindfulness training for children with ADHD and mindful parenting for their parents. Journal of Child and Family Studies, doi:10.1007/s10826-011-9457-0 Parent, J., Garai, E., Forehand, R., Roland, E., Potts, J., Haker, K., et al. (2011). Parent mindfulness and child outcome: The roles of parent depressive symptoms and parenting. Mindfulness, 1, 254–264. Repetti, R.L., Robles, T.F., & Reynolds, B. (2011). Allostatic processes in the family. Development and Psychopathology, 23, 921–938. Sameroff, A. (2010). A unified theory of development: A dialectic integration of nature and nurture. Child Development, 81, 6–22. Schonert-Reichl, K.A., & Lawlor, M.S. (2010). The effects of a mindfulness-based education program on pre- and early adolescentsÕ well-being and social and emotional competence. Mindfulness, 1, 137–151. Semple, R.J., Lee, J., Rosa, D., & Miller, L.F. (2010). A randomized trial of mindfulness-based cognitive therapy for children: Promoting mindful attention to enhance socialemotional resiliency in children. Journal of Child and Family Studies, 19, 218–218. Sibinga, E.M., Kerrigan, D., Stewart, M., Johnson, K., Magyari, T., & Ellen, J.M. (2011). Mindfulness-based stress reduction for urban youth. Journal of Alternative and Complementary Medicine, 17, 213–218. Singh, N.N., Lancioni, G.E., Manikam, R., Winton, A.S.W., Singh, A.N.A., Singh, J., & Singh, A.D.A. (2011a). A mindfulness-based strategy for self-management of aggressive behavior in adolescents with autism. Research in Autism Spectrum Disorders, 5, 1153–1158. Singh, N.N., Lancioni, G.E., Singh, A.D.A., Winton, A.S.W., Singh, A.N.A., & Singh, J. (2011b). Adolescents with Asperger syndrome can use a mindfulness-based strategy to control their aggressive behavior. Research in Autism Spectrum Disorders, 5, 1103–1109. Singh, N.N., Lancioni, G.E., Winton, A.S.W., Singh, J., Singh, A.N., Adkins, A.D., & Wahler, R.G. (2010). Training in mindful caregiving transfers to parent–child interactions. Journal of Child and Family Studies, 19, 167–174. Sturge-Apple, M.L., Skibo, M.A., Rogosch, F.A., Ignjatovic, Z., & Heinzelman, W. (2011). The impact of allostatic load on maternal sympathovagal functioning in stressful child contexts: Implications for problematic parenting. Development and Psychopathology, 23, 831–844. van de Weijer-Bergsma, E., Formsma, A.R., Bruin, E.I., & Bögels, S.M. (2011). The effectiveness of mindfulness training on behavioral problems and attentional functioning in adolescents with ADHD. Journal of Child and Family Studies, published online 22 September 2011, doi:10.1007/ s10826-011-9531-7 Accepted for publication: 9 November 2011 2012 The Authors. Child and Adolescent Mental Health 2012 Association for Child and Adolescent Mental Health.










© Copyright 2026