
Final Report on Engagement Findings
‘Right Care, Right Time, Right Place’ Report of Findings - Engagement Phase April – July 2014 1 Contents Page 1. Purpose of the report 4 2. Background 2.1: The case for change 2.2: The Providers’ response 2.3: NHS Calderdale and Greater Huddersfield Clinical Commissioning Group (CCG) Commissioning Intentions – the commissioners’ response 2.3.1: NHS Calderdale CCG – five year strategic plan 2.3.2: NHS Greater Huddersfield – two year operational plan and five year strategy 4 4 5 5 3. Legislation 7 4. Principles of Engagement 8 5. Methodology 5.1: How did we deliver the engagement plan? 5.2: What did we do to deliver the engagement plan? 8 9 10 6. Findings from the engagement process 12 7. Findings from the Providers’ engagement process 7.1: Findings from the SOC survey 7.2: Findings from the wider stakeholder meetings and events 7.3: Other findings 7.3.1: Staff engagement 7.3.2: Stakeholder event: locality and community services key messages 7.3.3: Stakeholder event: specialist hospitals key messages 7.3.4: Stakeholder event: self-managed care key messages 7.3.4: Stakeholder event: emergency and urgent care key messages 7.3.6: Letter from Barry Sheerman 7.4: Equality findings 14 14 30 8. Findings from the Commissioners’ engagement process 8.1: Findings 8.2: Findings from the community assets 42 42 46 6 6 32 32 33 34 34 34 34 36 2 8.2.1: Responses from Mixenden, Illingworth and Ovenden area in Calderdale 8.2.2: Cornhome and Walsden residents, Calderdale 8.2.3: Calderdale Basement project 8.3: Findings from Greater Huddersfield CCG ‘Care Closer to Home’ 8.4: Equality monitoring 46 48 58 49 52 9. Equality and Diversity 9.1: Equality recommendations 56 57 10. Overall findings and common themes 57 11. How the findings will be used to inform our plans 58 Appendices Appendix 1: CCG, Communication and Engagement Strategy Appendix 2: Provider, Communication and Engagement Strategy Appendix 3: Joint engagement Plan Appendix 4: Providers engagement document – SOC summary Appendix 5: Providers engagement document – SOC easy read version Appendix 6: CCG engagement document – 5 year plans Appendix 7: CCG engagement document – easy read versions Appendix 8: Comments cards Appendix 9: Providers stakeholder engagement Appendix 10: Letter from Barry Sheerman Appendix 11: Equality Monitoring from SOC respondents Appendix 12: Cornholme and Portsmouth Old Library focus group Appendix 13: Equality Monitoring from Commissioning Strategy respondents 59 76 89 96 96 96 96 96 97 124 125 128 132 3 1. Purpose of the Report The purpose of this report is to present the findings from the recent engagement activity for ‘Right Care, Right Time, Right Place’. This report describes both the Providers’ and Commissioners’ response to the case for change and the engagement process we followed to gather public, staff and stakeholder views. The engagement was delivered through a ‘Communication, Engagement and Equality Strategy’ and action plan, these plans were written to describe the process required for each of the engagement processes; this included one for the Providers and Commissioners (see appendix 1 and 2). The report provides feedback on: The engagement process delivered, including methods and approaches and the target audience reached Findings from the Providers’ engagement activity Findings from the Commissioners’ engagement activity Specific findings relating to equality, and Overall findings and key themes The background to the engagement activity and the ‘Case for Change’, is described to set the context. This includes a brief introduction to the Providers’ response to ‘Right Care, Right Time, Right Place’ and Calderdale and Greater Huddersfield commissioning intentions. The report also sets out the legal obligations for engagement and the principles by which the Commissioners’ want to engage, which forms part of their organisational strategy. 2. Background 2.1 The Case for Change (Right Care, Right Time, Right Place) The case for change sets out the way we deliver health and social care services and the need to change if we are to make sure we can meet current and future needs. Huge advances in medicine have changed the way we treat illness and injury; we have a growing and an ageing population; our illnesses are different and people’s expectations of health care are growing. We know people want care closer to, or at, home and a choice about how, when and where they’re treated. The cost of health and social care across Calderdale and Huddersfield is now more than £600 million a year. Growing demand, price inflation and the costs of new drugs and treatments mean we need to look at how we spend budgets to get maximum benefit for everyone. We need to ask some serious questions; Can we do things differently but maintain high quality services? Can we keep people out of hospital for everything but the most serious illness by improving the way we care for them at home? All seven organisations involved in health and social care in Calderdale and Huddersfield are working together on the ‘Right Care, Right Time, Right Place’: 4 2.2 Calderdale and Huddersfield NHS Foundation Trust (CHFT) NHS Calderdale Clinical Commissioning Group (CCCG) Calderdale Council NHS Greater Huddersfield Clinical Commissioning Group (GHCCG) Kirklees Council Locala Community Partnerships South West Yorkshire Partnership Foundation Trust (SWYPT) The Providers’ response to ‘Right Care, Right Time, Right Place’ A Strategic Outline Case (SOC), prepared by three providers: Calderdale and Huddersfield Foundation Trust, Locala Community Partnerships and South West Yorkshire Partnership NHS Foundation Trust (SWYPFT) set out a response to ‘Right Care, Right Time, Right Place’ which included a review by the National Clinical Advisory Team (NCAT) in spring 2013. The Providers’ response describes a new model for the provision of hospital and community services across Calderdale and Greater Huddersfield. Under this model, the three providers would work together and closely with general practice, social care and voluntary organisations to deliver integrated care and support services in the community. This would include including moving current hospital-based services closer to where people live. The response states that: integrated community services would work seamlessly with acute and emergency services based on one specialist hospital site and with planned and elective care on a second specialist planned care hospital site. It also identified significant benefits to patients, services users, local people and service providers and commissioners. However, it is important to note that a decision will not be made about significant changes to the future of services in Calderdale and Greater Huddersfield without a period of formal consultation. Any decision of this significance will be made by the Commissioners’ and not by the Providers’. 2.3 NHS Calderdale and Greater Huddersfield CCGs Commissioning Intentions – the Commissioners’ response Calderdale and Greater Huddersfield Clinical Commissioning Groups (CCG’s) are responsible for commissioning a range of services in Calderdale and Greater Huddersfield. The CCG’s need to ensure their commissioning intentions meet the needs of the local community to deliver these intentions, each CCG has a five year strategy based on what they already know about the community and the health needs in the area. 5 2.3.1 NHS Calderdale CCG – five year strategic plan NHS Calderdale CCG set out a five year ambition which includes a vision for the future. This vision is the Commissioners’ contribution to the delivery of change as a partner for ‘Right Care, Right Time, Right place’. The plan builds on the organisational aims, intelligence gathered from previous engagement and patient experience activity and clinical insights. The aim is to ensure changes needed to deliver the outcomes for local people are safe and of high quality. The focus over the next five years is to continue the shift of services and resources from unplanned hospital care to integrated health and social care - delivered in community and primary care settings. In addition a number of improvement programmes will drive delivery over the next three to five years. These programmes are: Cardiovascular Diabetes Respiratory Alcohol conditions Musculoskeletal Cancer & tumours Mental health Strategic Review Better Care Fund Each programme is described in more detail in the strategy and the aim is to ensure any plans reflect the needs of the local community. 2.3.2 NHS Greater Huddersfield CCG – two year operational plan and five year strategic plan Greater Huddersfield CCG has developed a two year operational plan and a five year strategic plan. The vision for the larger health and social care system in the next five years has been developed in partnership with North Kirklees CCG and Kirklees Council. The geographical footprint has been important when bringing together the partners to develop proposals for transformational change. The two year strategic plan is based on the contribution to ‘Right Care, Right Time, Right Place’. Greater Huddersfield Clinical Commissioning Group’s operational plan sets out a unique and innovative vision of health and social care service delivery for the next two years in the area. The focus of this change programme is to continue the shift of services and resources from unplanned hospital care to integrated health and social care - delivered in community and primary care settings. The outcomes delivered by these aspirations can be characterised into a number of themes: Increasing opportunities for self-care, especially for people with long term conditions Making best use of technology and innovation 6 Optimising delivery in primary and community care by providing secondary care services or hospital services, in the community and thinking about innovative ways of doing this Optimising delivery in secondary care Building community capacity to deliver better health and wellbeing As a result of this, local people can expect: Services delivered as close to home as possible Improved health and wellbeing Opportunities to have a say in the design of health and social care provision Accessible, non-discriminatory service provision Integrated services Services that maximise dignity and respect for vulnerable groups The plan sets out the pathway for the organisation to navigate a course through external change and uncertainty towards stable, responsive and sustainable health and social care services for Greater Huddersfield now and in the future. 3. Legislation Health and Social Care Act 2012 The Health and Social Care Act 2012 makes provision for Clinical Commissioning Groups (CCGs) to establish appropriate collaborative arrangements with other CCGs, local authorities and other partners. It also places a specific duty on CCGs to ensure health services are provided in a way which promotes the NHS Constitution – and to promote awareness of the NHS Constitution. Specifically, CCGs must involve and consult patients and the public: In their planning of commissioning arrangements In the development and consideration of proposals for changes in the commissioning arrangements where the implementation of the proposals would have an impact on the manner in which the services are delivered to the individuals or the range of health services available to them, and In decisions affecting the operation of the commissioning arrangements where the implementation of the decisions would (if made) have such an impact The Act also updates section 244 of the consolidated NHS Act 2006 which requires NHS organisations to consult relevant Overview and Scrutiny Committees (OSCs) on any proposals for a substantial development of the health service in the area of the local authority, or a substantial variation in the provision of services. The Equality Act 2010 The Equality Act 2010 unifies and extends previous equality legislation. Nine characteristics are protected by the Act, age, disability, gender reassignment, marriage and civil 7 partnership, pregnancy and maternity, race, religion and belief, sex and sexual orientation. Section 149 of the Equality Act 2010 states all public authorities must have due regard to the need to a) eliminate discrimination, harassment and victimisation, b) advance ‘equality of opportunity’, and c) foster good relations. All public authorities have this duty so the partners will need to be assured that “due regard” has been paid. The NHS Constitution The NHS Constitution came into force in January 2010 following the Health Act 2009. The constitution places a statutory duty on NHS bodies and explains a number of patient rights which are a legal entitlement protected by law. One of these rights is the right to be involved directly or through representatives: 4. In the planning of healthcare services The development and consideration of proposals for changes in the way those services are provided In the decisions to be made affecting the operation of those services Principles for Engagement NHS Calderdale and NHS Greater Huddersfield CCG both have ‘Patient and Public Engagement and Experience Strategies’. These strategies have been developed alongside key stakeholders. The strategies set out an approach to engagement which describes what the public can expect from any engagement activity. The principles in both strategies state that the CCG will; Ensure that the CCG engage with public, patients and carers early enough throughout any process Be inclusive in all engagement activity and consider the needs of the local population Ensure engagement is based on the right information and good communication so people feel fully informed Ensure that the CCG are transparent in their dealings with the public and discuss things openly and honestly Provide a platform for people to influence thinking and challenge decisions Ensure any engagement activity is proportionate to the issue and that feedback is provided to those who have been involved in that activity The strategy sets out what the public can reasonably expect the CCG to do as part of any engagement activity and the process required to preserve these principles to ensure public expectations are met. 5. Methodology Both the Providers and Commissioners undertook engagement activity to identify if the SOC and the five year strategies were capable of delivering service improvements and meeting the needs of the local population now and into the future by gathering public, staff and stakeholder views. 8 The process involved two conversations taking place simultaneously, one on the Providers’ response and one on the Commissioners’ response. The Commissioners’ responsibility is to ensure they commission services from providers that will ensure the health and wellbeing of the local population of Calderdale. The Providers are commissioned to provide services that support that vision. The engagement activity for both the Providers’ and Commissioners’ was supported by a joint delivery plan (see appendix 3) which was delivered during an eight to 12 week period. The Providers commenced engagement prior to Commissioners’ and the process involved a number of planned engagement activities aimed at a variety of target audiences. The process followed is described in diagram one. Diagram One Case For Change Providers’ Strategic Outline Case Commissioning Intentions Existing Mechanisms Drop in Sessions Asset Based Approach Stakeholder Events Development of Joint Report of findings Stakeholder Event Commissioners’ Service Change Proposals 5.1 How did we deliver the engagement plan? The purpose of all the engagement activity was to capture the views of local people with a specific focus on key stakeholders. Both the Providers’ and Commissioners’ engagement required different activities but both were brought together at 10 drop in sessions which took place in eight locations in Calderdale and Greater Huddersfield. The methods of engagement used were supported by a number of documents: A summary (see appendix 4) and easy read version (see appendix 5) of the SOC which contained a feedback and equality monitoring from A summary (see appendix 6) and easy read version (see appendix 7) of the commissioning intentions for each CCG and a feedback and equality monitoring form 9 Comments cards used in both drop in sessions and as part of the asset based approach (see appendix 8) The methods of engagement set out in the diagram are described below in more detail, which describe what we did. 5.2 What did we do to deliver the engagement plan? Existing Mechanisms: Calderdale and Greater Huddersfield CCG both have a ‘relationship matrix’ which enables the CCG to engage with a number of key organisations. The matrix is a list of voluntary and community organisations which are willing to work with us to engage their clients and staff. These organisations are mapped by the target audience they reach and the protected characteristics they cover. Calderdale CCG also work closely with the third sector and have invested in ‘health connections’ a third sector hub which ensures they can engage with third sector colleagues providing support to health. Greater Huddersfield CCG work closely with third sector leaders and local authority colleagues to target specific communities. Third sector organisations were targeted using ‘North Bank Forum’ which has a regular e-newsletter and Voluntary Action Kirklees (VAK). Close working relationship with staff and member practices, including patient reference groups and work with the Calderdale Health Forum and Greater Huddersfield Patient Network have been utilised. Membership of the three provider organisations and the Right Care, Right Time, Right Place reference group were engaged through electronic or postal surveys. Drop in sessions: 10 Drop in sessions were set up in 8 locations across Calderdale and Greater Huddersfield to ensure all members of the community had an opportunity to have their say. Each session was delivered on a different day to give as many people as possible the chance to attend. The drop-in sessions provided a platform for the public to talk about commissioning intentions, the provider response and ‘Right Care, Right Time, Right place’. The sessions were delivered between 2pm-7pm. Comments cards – These were available at the drop-in sessions and in other service areas for people to write down any comments, issues or concerns they may have. Asset Based Approach: Calderdale CCG use an ‘asset based approach’ to engaging with the local population, this means they train and fund local groups to talk to the public on their behalf using the methods and approaches appropriate to that community. The CCG work with over 40 groups in varying localities representing some of the most seldom heard residents in our area. 10 A similar approach took place in Greater Huddersfield utilising community development workers from Kirklees Council to have conversations at a community level with existing groups and organisations who already have a good working relationship with staff in the area. Provider Stakeholder Events: A number of stakeholder meetings and events were arranged by the Provider organisations to gather views. These activities took place over a number of weeks and included conversations with the voluntary and community sector. To ensure the views gathered were a representative sample all engagement activity was equality monitored. This will help the engagement team further understand if we have reached protected groups who may have different experiences of health and social care services. In addition to the engagement activity there was a number of other mechanisms operating in order to gather views, these are below: Dedicated website which contained information on how to contact the programme management office and also opportunities to post comments. This includes the use of social media such as Twitter. PALS and complaints service who were asked to capture public views as part of their customer facing role. Close working relationship with Healthwatch colleagues to ensure we listen to people’s views through consumer champions. Existing consumer websites were reviewed including those attached to the local media, patient opinion and NHS Choices to gather feedback. A variety of communication channels were used to disseminate information and provide opportunities for patients and the public to give their views. The methods below were supported by the communication leads for each organisation and centrally managed by the Programme Management Office. All communications have been centrally logged. Target Audience Service users, general public, third sector OSC/Health and Wellbeing boards Staff Delivery Method Partners’ intranets, websites and social media platforms Relationship matrix Patient reference groups Third sector umbrella organisations. Patient groups and Carers groups Meetings/ briefings Internal bulletins Staff Intranets Cascades at meetings through managers. 11 Healthwatch Elected members / Councillors Media 6. Email and personal discussions Newsletter articles Information to be circulated electronically – explanatory email with a link to web survey Proactive media releases Social media Findings from the engagement process The engagement process took place between April and July 2014. These were a number of activities taking place throughout this period and the responses we received are as follows: Method Drop in Sessions Calderdale and Greater Huddersfield Asset based approach Calderdale Contact / attendance 202+ attendees Asset based approach Greater Huddersfield Existing networks Calderdale and Greater Huddersfield: postal, email, social media Stakeholder activities Calderdale and Greater Huddersfield 477 contacts 1,263 contacts 18,000+ contacts 20,500 contacts Responses received 153 responses received 1,244 responses received 57 responses received 215 responses received 806 + responses received ( not all numbers recorded) (Figures including + mean we did not always count the numbers attending therefore the target audience was greater than the numbers recorded) In total we received 2,475 responses with the majority of these responses 85% on the Strategic Outline Case (SOC) and the remaining 15% on the CCGs commissioning intentions. 1,306 equality monitoring forms were completed (this comprises; 1091 from the SOC engagement, 126 from the 5 Year Strategy engagement and 89 form the drop in sessions) and from these we know +we received the majority of our responses from residents in Calderdale who provided 51% of the total responses, Greater Huddersfield 3% and 46% where there was no postcode provided. It is worth noting however that this does not take into account the remaining 891 responses where some may have come from residents in the Greater Huddersfield area. As well as our planned engagement activities a number of meetings were held with key stakeholders. These contacts have not been counted in the contact or response figures in the table above. However, feedback from these organisations can be found in the findings for both the CCGs and Providers’. The meetings attended by both the Providers’ and the CCG are tabled below: Target Audience: Meetings attended Overview and Scrutiny Committee – Calderdale Overview and Scrutiny Committee – Kirklees Monthly Monthly 12 Health and Well Being Boards - Calderdale Health and Well Being Boards - Kirklees Local councillors and MPs - Calderdale Local councillors and MPs - Kirklees Local Medical Committee GPs Healthwatch - Calderdale Healthwatch - Kirklees Yorkshire Ambulance Service Community Pharmacy Local Care Direct Unions Voluntary and Community Sector Monthly Monthly Regular briefings and information exchange Regular briefings and information exchange 26.03.14, 30.04.14 and 28.05.14 01.04.14, 03.04.14 and 03.06.14 01.04.14, 07.04.14 and 15.05.14 19.03.14 03.04.14 15.04.14 20.06.14 27.02.14 10.04.14, 27.05.14 and 28.05.14 We have evaluated the process we followed to deliver the engagement on both the Providers SOC and the CCG commissioning intentions using the feedback we received from community assets, members of the public and the drop in sessions. The key learning points are: People found the SOC and commissioning intentions information too much, it was a lot to take in and people found it complicated to understand. There was a lot to consider and people did not know how to provide feedback resulting in a lower response rate in some areas. People in Greater Huddersfield were harder to engage than those in Calderdale, this can have been for a number of reasons including the perception that changes may not affect people in that area. The equality monitoring form was not attached to the commissioners’ engagement questionnaire and therefore whilst many people completed it, it was not possible to align the responses to the equality detail. This meant we were not able to comment on views held by those with particular protected characteristics. The evaluation from the drop in sessions found that from those completing the form (77 in total), 47% stated the drop in was what they expected with only 8% stating it wasn’t. Comments received were that the Information provided was vague and the drop in could have been better set out and publicised and appeared to be poorly attended. However the positive comments were that it gave people time to talk to people at length and for some it exceeded their expectations and they found it informative. There were suggestions that the drop in sessions should be more formal and that we should go to community groups. 13 7. Findings from the Providers’ engagement process The focus of the Providers’ engagement was to gather views on the ideas set out in the SOC. The full SOC document was made public on the Right Care, Right Time, Right Place website. The content of the document was then developed into a summary format (see appendix 4) and an easy read version (see appendix 5). The document was circulated to the community assets in both Calderdale and Greater Huddersfield along with comments cards, at the drop in sessions and via the website. In addition the providers hosted a number of conversations to engage stakeholders (see appendix 9). The findings from the engagement process are reported below. It is worth noting that not everyone replied to every question so 100% is based on the total number responding to that question not 100% of the total responses received. 7.1 Findings from the SOC survey The providers asked: Q1. Do you think we have reflected the things people have already told us? Those responding told us: From the 1,039 responses we received to this question 82% stated that they felt providers had considered the things that they had already been told during previous engagement exercises and other forms of feedback. The 18% responding No have provided a response to their answer in the additional questions highlighting some of their concerns or ideas. Those people who chose not to respond may account for people who had not previously been engaged or people who have not previously given their views. 14 The providers asked: Q2.What do you think about the ideas described in this leaflet? The feedback received was grouped into positive (green), negative (red) and neutral comments (amber). The chart above shows that the majority of comments are neutral with all the feedback we received falling into the following themes: Hospital services Travel and transport Care and services in the community Delivering the model Engagement process and information provided The weighting of those responses as positive, negative or neutral against each theme are highlighted below: The table suggests that the majority of negative comments received relate to the providers ideas about the hospital model with travel transport highlighted as an area that had not been properly considered. 15 Whilst the majority of people provided positive responses to looking at care in the community and delivering the model people felt the information provided described the ideas in a way they could understand and welcomed the opportunity to respond. Those responding told us: Hospital services: Positive comments included: Some people liked the plans and the idea of a specialist hospital with planned care on one site. People like the idea of cottage hospitals and services closer to home. Negative comments included: The majority of negative comments related directly to the plans to create one A&E and the message came very clearly from the population of Calderdale that they did not want to lose their A&E. People expressed worry and concern if this happened. Neutral comments included: People did not understand how it works now so felt unable to comment fully, there were a number of comments about keeping things as they are and that it currently works. There were a lot of people who stated they needed more information on the A&E plans and wanted more detail, that language like minor injuries needed describing and was confusing. Care in the community: Positive comments included: People welcomed the idea of more services in the community and closer to home. There were comments that GP practices would be a better option than going to A&E and there were some requests for more walk in facilities. Negative comments included: People felt that the plans were not diverse enough and would suit only a sector of the population. Access issues for people who are deaf, and those who have a first language that is not English requires addressing. There were comments about current poor appointment systems and whether community services could cope with demand. Care is not coordinated and there is concern that older people may deteriorate through lack of support. Neutral comments included: People wanted more services from the GP i.e. health checks but there was concern that GPs were already busy. Appointment and waiting times are a concern and need to be addressed; people would like more face to face contact such as home calls. Streamlining and coordinating services better were mentioned and more links to the third sector to support delivery. Travel and transport: Positive comments included: There were few positive comments on transport and travel but those that were related to encouraging walking to appointments and positive experience of the ambulance service. 16 Negative comments included: Too far to travel for those who are unwell and the cost of travel were both common themes. Longer journey times are more stressful, particularly for those visiting and for parents/carers. Car parking was also a big issue and concerns about the dual carriageway and Ainley Top with a focus on peak travel times and congestion which would increase journey times or slow down access to services which could be serious. For those who can’t drive taxi journeys would be expensive including the cost of travelling from rural areas. Neutral comments included: People stated that current transport arrangements needed to be improved such as the shuttle bus. Delivering the model: Positive comments included: The ideas were good and well thought through. People commented that the model would make a difference and needed to be implemented or put into action straight away. More joined up thinking and a solid structure would help with delivery. Negative comments included: People stated that the plans were about cuts not spending more and that the plans would be a waste of money. There was a view that plans had not been thought through properly and people wanted things left as they are. There was no consideration for specific groups like BME or people living in rural areas and some people felt that plans would just not work. A few stated the plan to move/close A&E would cost lives and that services would not be able to manage certain health conditions as effectively. Neutral comments included: The majority of neutral comments were that the ideas looked good on paper or in theory but would they work in practice. There were comments that any changes should not be at the cost of quality and that more detail was needed to help people understand how the model will work and that vulnerable and diverse groups are considered. People wanted to know the cost of the changes and how money would be spent in the future and for the commissioners and providers to be honest and transparent about this. There was a general feeling that the plans could be too ambitious, a comment that pharmacy services are not mentioned and that prevention needed to be more of a focus. Engagement process and information provided: Positive comments included: The majority of comments received about the information provided were positive. This included comments that the information was good, clear, informative, and people were able to understand the content. There were comments that the information helped people to understand the ideas for future services and it was good to keep people informed. Some respondents felt solutions were described and people stated there were lots of good ideas which were to the point if not a lot to digest. The easy read version was described as easy to understand and very useful. Negative comments included: The negative comments referred to the information being provided was a ‘smoke screen’, the ideas were a done deal and that the leaflet 17 was about convincing people of what will happen. In addition there were some comments that the information was hard to understand, too complicated and too much information for the average person to understand or to take in. There were a few requests for future information to be available in Urdu. Calderdale residents felt their views would be ignored and we needed to listen to the public more. Neutral comments included: The neutral comments related to the information being reasonable but not enough detail with more information needed to have an informed view. Some people stated they did not know what to believe as there had been too many conflicting messages and there were a number of comments with people wanting to know what it meant for them. There was a request for more engagement to help people understand this further. Quotes: ‘I agree that you need to reorganise healthcare to reflect changing needs of the population but I share the concerns of many that concentrating emergency care in HX or HD will make it much harder to access particularly for those that do not have access to a car. I think there needs to be a minimum level of A&E provision at both hospitals’. ‘I can see for and against for several options! I do not want to travel to hudds or Bradford for tests which can be done in my local community and I want easy access to A&E. However it’s Catch 22 and will get very costly which has to be addressed wisely’. ‘The proposals are really good. I would like more diabetes services.’ ‘I think moving A&E care from Halifax to Huddersfield is a bad idea, people from this area needing a+e care could be at’ Community teams may have improved 24/7 reactive service but decentralised services can create silos with breakdown ‘They don’t deal with how people can contact health and social services and I am deaf and don’t use the telephone’. ‘I would be very concerned if the only emergency / A&E were in Huddersfield, I have a child with asthma and getting to’ ‘Ideas are ok, but getting people to actually care about the health care service, community teams and services sound’ ‘GOOD, like idea of specialist units’ I want to have a hospital in Halifax with A&E and planned care because I have 2 children. I can’t afford to travel to Huddersfield. I speak little English so I feel more confident if I can see a doctor face to face. I think moving A&E care from Halifax to Huddersfield is a bad idea, people from this area needing A&E care could be at risk as it takes much longer to arrive at hospital, also once they are there it is much more difficult to get home if you don’t have transport 18 It’s about making existing services more effective, making them more widely available. It's all about improving access to effective services - all providers in community to work together ‘Don't like them I am dyslexic and moving services makes it worse’ ‘Ideas are good if followed through; however need more details on how it will affect us on the ground’ ‘Good to read about what is happening and it's important to involve the community in hospital and community services and listen to their views’. ‘Smoke Screen. Decisions have already been made so why consult’. ‘They are reassuring but I feel they are slightly ambiguous. The justification has not been put across why is this change happening’ ‘There’s too much information and I don't know which bit concerns me’ The providers asked: Q3. Do you have any other suggestions for changing health and community services? The feedback received was grouped into positive (green), negative (red) and neutral comments (amber). The chart above shows the feedback we received was again predominantly neutral with all the feedback we received falling into the following themes: Access and waiting times Supported self-care/management Community care Hospital services Staff care and treatment 19 The weighting of those responses as positive, negative or neutral against each theme are highlighted below: The table suggests that the majority of negative comments received related to staff care and treatment and access and waiting times. There were a lot of positive comments relating to hospital services and positive suggestions about how care could be provided in the community. There were lots of ideas about how we could improve services in the neutral comments across all the themes. Those responding told us: Access and waiting times Positive comments included: People stated that same day appointments worked well and longer opening times for some GP practices were working well. There was a comment that out of hours mental health services were liked and home visits for the vulnerable. Some comments supporting the need to share patient information out of hours and a move towards 24/7 community care. Negative comments included: The main comments were about travel times to get to Huddersfield, these were raised by Calderdale residents and included comments that people can’t get there, transport is inadequate and the travel times are too long even for planned appointments. This followed comments that parking needed to be improved on hospital sites, patient transport and public transport systems if changes were to be made. The other main theme was to improve GP services which consisted of a better appointment system and many examples were given of not getting an appointment. Having to contact the practice to make an appointment was problematic including ringing at a set time and the need to further consider the working age population with more out of hour appointments. More work needed to be done to reduce appointment cancellations and do not attends. Some people wanted more time to talk once they had an appointment. 20 Neutral comments included: The suggestions included more walk in facilities and improved access in the evening and weekends to community services with better appointment systems, again working people were mentioned as requiring better options for accessing services. Suggestions were made that more urgent care and diagnostics could be provided at a GP practice level and that we should have more GPs. Screening and testing it was suggested could take place in other venues such as schools, workplaces and wider community facilities and there was a suggestion about developing a 24 hour emergency clinic for the upper valley. Some stated we needed access to more BME appropriate services and reduce waiting times at A&E. The community want to be kept informed at each stage of developments and want more information on services. Transport was raised as an issue that needed solving and there were requests that services were in walking distance and that frail elderly services were local. Supported self-care/ management Positive comments included: More help is needed for people to look after themselves at home, things like phone chats and on line facilities would help. More emotional support for families in the same way that cancer services help. People stated they would like more care in a variety of settings such as schools, community venues and youth groups. More health information in schools and healthier lifestyle programmes. A number of people did state that people should take responsibility for their own health and education was needed to support this. Negative comments included: Responses included comments that there was not enough done on the preventative agenda and we needed to stop people becoming unwell. More frequent checks for people who may be subject to conditions such as diabetes and more help for people with mental health issues. People stated there was not enough help to use technology to support health and patients needed to be involved in the design of services for self-care to work. There were a number of responses that stated not enough is done to train and provide support to carers. Neutral comments included: People put forward a number of ideas relating to the delivery of self-care, these included: Specialist local community hubs which could manage local need Extending the minor ailments scheme to more products Community awareness days which focussed on prevention Regular health checks for the elderly and those with conditions Leaflets in a more reader friendly format More education and training for the patient, families, friends and carers More local support groups Subsidised or free activities such as gym memberships and access to gyms, swimming and keep fit classes for specific groups i.e. older people in community settings More advice on diet, weight management and links into existing schemes such as slimming world which are subsidised After surgery clinics run by trained volunteers on healthy lifestyle 21 A focus on the young and part of the schools, youth clubs approach to working with young people In addition people wanted better trained receptionists who could sign post people for appropriate support and treatment. More ownership of the self-care approach in the local community, including services run by VCS groups and local people using local facilities. Community care and services Positive comments included: Positive community suggestions were that GPs should be given more of a role in delivering different services with the opportunity to open longer. More district nurses were favoured and more home help and social care services to keep people well in their own home. Negative comments included: Negative comments included more help for those people who cannot get to a GP surgery and more podiatry services in practices. Also barriers to accessing services in the community need to be addressed particularly for BME groups. More investment is needed in the community to support community services including projects funded for longer terms and less dependency on grants. More support should be given to community involvement including representation on decision making forums with local communities represented, and targeted discussions with communities about their individual needs and services assessed. Neutral comments included: There were lots of suggestions on the model for community services, these included: Ensuring services keep people well in their own home More targeted support for specific groups such as young people, BME communities, people with mental health issues and those with dementia or who have had a stroke People wanted to see specialist GPs and nurses for certain conditions including those with skills to work with particular groups i.e. deaf people Community services need to respond over a 24/7 period including bank holidays and using more support systems though phone lines There needs to be more services for elderly people and women and some separate services for men People liked the idea of services you can walk into to get advice, support and treatment rather than via referrals or appointments More services to be placed in community settings and buildings such as mosques, youth groups, supermarkets and the places people go and can walk to There were comments requesting that commissioners and providers work more closely with the community to plan and assess services but to deliver them too More social groups, support networks and informal places to go to get peer support, Brighouse was cited by a few as being under resourced in this area There were a few suggestions that some services should charge people who misuse them, whilst others did not want services to charge as they could not use them if they had to pay 22 Hospital Services Positive comments included: The majority of respondents stated they did not have any further suggestions relating to the hospital. The few responses we received related to elderly care being best placed in the community to ensure beds were not taken up and 24/7 GP services to prevent people attending A&E. There were a lot of positive comments about the current service and suggestion we should not fix that which is not broken. Negative comments included: The majority of suggestions were to improve hospital waiting times and to improve both hospitals, some believed they were in the process of being shut down and that any more changes would adversely affect people. There were comments that services were already fragmented and needed consolidating to work including information systems to share data which were outdated and more training was needed for staff on things like mental health. Some did not like the idea of community hospitals and there were suggestions to charge people for using A&E. A few comments about getting the basics right first before changing and a few comments about the coroners not being trained appropriately to support those of a Muslim faith. Neutral comments included: The majority of suggestions were to keep A&E in Calderdale and to keep a facility in both hospitals. Most people wanted things to stay as they are and services not to change. The suggestions were to improve waiting times in A&E and keep both A&E and maternity services at both sites with a partial facility in Todmorden and refer to specialist hospitals when required. There was a lot of support for community hospitals with a few dislikes, and a request to increase transport which is flexible and free and increase ambulance services and crews. Some suggested that improved access to a GP and better prevention work in the local community would decrease attendance at the hospital and if attending to treat in order of priority to stop people dropping in to the service. There were a few requests for improved services for mental health including more psychiatric beds in the community. Staff care and treatment Positive comments included: That respondents wanted to see their GP and community nurses and wanted to see more of these and other well trained staff in the community. There were a number of comments relating to staff needing to share information to work better. Negative comments included: The need for more staff and less managers and improved standards of care for the vulnerable. There were concerns that staffing levels in the community were low and that in particular social care staff need more time to spend with the person they care for. Respondents want to see the same staff, this includes GPs and staff who can communicate clearly in the right language and be understood. There were concerns that there is a lack of qualified nursing staff and a need for more out of hours GP cover and that there may not be enough staff to work in the community. Staff attitude was a also a problem and that people were not treated as a whole. 23 Neutral comments included: Suggestions that more consultants needed to hold community clinics and that health professionals needed to work together to look at the person as a whole. That paperwork needs to be reduced to enable busy nurses and more suitable qualified staff to work more effectively with services needing to be staffed properly to work, including admin teams. There were a number of requests for more female GPs and, more doctors in A&E and the chance to see the same doctor at each appointment. There were comments that GPs could get overstretched and that whilst community care sounded good that it may not work in practice . Quotes: ‘Should be able to get doctor appointment on the day you need it not in 2 weeks’ time. Doctors surgeries need to have more appointments and more doctors need to be available to accommodate the patients’. ‘Each Doctors surgery should have a few available slots on that day which work on a first come first serve basis. As it is very difficult to get an appointment within 1-5 days.’ ‘I would like there to be more community groups for people with physical & mental health issues’. ‘Make more services available to patients nearer where they live to make transport easier and reduce the stress of travelling on patients and their family’ ‘Don’t’ discharge patients at 4.30am in the morning Will there be more beds for mental health to stop patients having to be transported 100s of miles More and better care in the community for people with mental health illness would be welcomed’ ‘More community services for me to attend, I would like to be able to get a carer when I’m bad instead of going to hospital, I hate it!’ ‘I am in favour of more GP openings I support community hubs I feel there needs to be a proactive approach to include BME VCS a real and meaningful partners’ ‘Easier access to GP appointments, out of hour GP care not to go through 111 - to be direct to out of hour number’ ‘Less worried about accidents more focus on mental health and maybe down size both hospitals but don’t change the areas for different treatment’. ‘There should be health check-ups particularly for older people as prevention, for early detection of ailments is better, more efficient, and economic that treatment of advanced conditions and it should be easier for people to see their doctors’. Continue to develop a secure system allowing health professional the chance to access the same relevant information’ ‘I noticed the comment around staff training and attitude my response to that is that staff should be given the time and support to train properly. not just video training. The government needs to realise you can’t cut back in care’. 24 ‘Although patient care is obviously the priority some thought should be given to the visitors to the patient which has a great support to the wellbeing of patient recovery. Additionally, public transport and certainly more car parking need to be addressed. Personally I would be prepared to attend either Calderdale or Huddersfield as a long term patient of specialist’. ‘It’s a long way to HRI from the other side of Holmfirth. We need more local services and the thought of A&E moving to Calderdale is totally unthinkable. Even planned appointments would be difficult for many people. For planned operations where a stay in hospital is required it would make visiting for many impossible’ We need to educate people more to take charge of their own lives. I do think we are improving with fitness classes etc. but I still think there is a need to educate families on better eating habits. Without NHS my husband would have died years ago, and my two sons wouldn’t be here today’. ‘provision of services seems to be becoming a very fragmented thing with different groups supplying differing services, there needs to be greater consolidation of services’ The providers asked: Q4. Do you want to tell us anything else about hospital and community services in Calderdale and Greater Huddersfield? The feedback received was again grouped into positive (green), negative (red) and neutral comments (amber). The chart above shows the feedback we received was again predominantly neutral although the negative comments increased on this question. The feedback received followed a number of themes: The care people received Hospital services Access and waiting times Community care and services Quality and safety 25 The weighting of those responses as positive, negative or neutral against each theme are highlighted below: The table suggests that the negative comments were related more to access and waiting and quality and safety. There were a lot of positive comments relating to the care people received and once again lots of neutral comments across all the themes. Those responding told us: The care someone received Positive comments included: There were a number of comments which related to the care people received and they were all positive. Comments to staff that were described as caring and helpful, second to none and professional. Quite a number of people described particular examples where they were grateful for the care they received. Negative comments included: A number of comments relating towards being understaffed, particularly A&E and the need for matrons. There were comments that staff do not listen, or communication is limited and there is more paperwork than care. Staff using phones on wards and not staying focussed or being caring or sympathetic were also highlighted. In addition there were a number of comments which suggested there is a lack of understanding of mental health, addiction, BME and Learning disability. There was also a few comments about the care over 65s receive which was deemed as poor in comparison. Neutral comments included: Respondents told us that we need to look at the whole person when we care for them and that included more training on elderly care, mental health, BME and young people. There was a request for more bilingual workers, advocacy and female GPs, trained staff to keep people in their own homes and more staff in A&E. There were a few respondents who wanted to see happy staff with vocational interests and to stop nursing degrees. Poor communication by consultants needed improvement and so did discharge arrangements. 26 Hospital Services Positive comments included: There were a number of positive comments relating to hospital care received in the community including services received at Broad Street and Todmorden Health centre both in Calderdale. Respondents wanted to feedback the positive experiences of hospital services, there were comments that it was well run, it was clean and people received good care and treatment. There were also comments from some that they understood the financial challenges. Negative comments included: There were quite a few patient stories about how care has deteriorated, that food was not good, some wards were not clean and that the discharge lounge at HRI was unpleasant. There were concerns that moving A&E to Huddersfield would cost lives, that transport systems were not in place and travel and parking would be difficult and journeys too long. In particular Calder valley residents felt that access was poor already and that those in rural areas had not been considered. Current hospital appointment and waiting times required improvement and there were a number of examples of appointments not being on time. There were quite a few comments from elderly people that they were frightened, worried and scared about the plans. In addition there were some comments about being discharged too early and a lack of cultural awareness or staff speaking community languages. Neutral comments included: The majority of neutral comments were from Calderdale residents requesting that A&E services remained open and a few from Greater Huddersfield residents about keeping services local. There were a few comments about keeping ‘walk in’ facilities and a number of requests for more female GP’s. We also received some comments about maternity services which varied from people wanting more support to give birth at home to concerns about maternity arrangements in the future. Access and waiting times Positive comments included: People wanted to see more community services, open for longer. There were a few comments that people would be willing to travel for the best treatment and lots of examples of services people had used where access was good. Negative comments included: The majority of negative comments were related to travel and transport and came particularly from Calderdale residents who do not want to travel to Huddersfield. Respondents told us that isolated communities had not been considered and that longer journeys may increase mortality rates. Huddersfield parking was poor and expensive and there were issues with disabled parking too, there were worries that Huddersfield would become too crowded. Those on a low income or without their own transport wanted services closer to home although some would welcome improved and even free transport services. A lot of comments relating to the need to improve appointment systems and waiting times in both a hospital and community setting. 27 Neutral comments included: There were lots of comments that people wanted to see longer opening hours in the community (i.e. 8am-8pm GP services 7 days a week) and services that are accessible and convenient. The issues were described as appointment systems which do not work and access to a GP decreasing. The solutions were more telephone based consultations and shorter waiting times to see a GP of choice. More local pharmacy services in some areas and less waiting time for procedures such as operations. Community care and services Positive comments included: There were lots of comments about current community services working well and these included continence services, ophthalmology and cardiology. A number of people were in favour of the model and services being placed closer to people’s home. There were some positive stories of how patients had been trained by staff to look after themselves in for example dialysis. There were requests to keep working with schools and educating young people about their health. Negative comments included: Current community services work but are disjointed and systems need to work better. There were concerns that mental health was not supported as well in the community including through GP services and mental health beds, the suggestion was for more training and a focus on improving services in this area. People were still concerned that the GP may prevent referrals and so people will not receive the services they need and that some may be out of touch with patients’ needs. There was criticism that the health gap had not been closed and services needed to be expanded to meet the needs of poorer communities. More information on services for the elderly and a stronger focus on isolation were needed. There were comments that discharge from hospital was sometimes too soon and the waiting time for mid midwifes was too long, there were a few comments that were concerned that services will close or be lost. Neutral comments included: Improved opening times and out of hour’s access to a GP and other services was the key message. People wanted more time with the GP, access to female GP’s and more walk in services. There were some comments relating to improvements to home help services. There was a strong message that the community wanted to help find the solutions to community care, be trained to deliver the model and that VCS organisations should be used to ensure services remain near to people’s homes and in local community settings. Quality and safety Positive comments included: Positive comments related to suggestions to use more voluntary help to improve services already provided by hard working and dedicated staff. There were a number of comments that facilities were cleaner and some services were described as excellent. Negative comments included: There was a concern that moving A&E to Huddersfield will result in deaths. That staff were not patient focussed enough and some required training to improve quality particularly in elderly care and for those 28 with dementia. There were examples of misdiagnosis and not enough follow up after discharge. BME communities felt they received inconsistent care and that coroners arrangements were inadequate. There were a few comments that maternity care had deteriorated and that in general care was worse. Neutral comments included: There were a number of suggestions that included a need for joined up specialist services in the community to improve quality. Longer opening hours and more weekend services. There was a need for better information and communication and an improvement in staff attitude. Respondents felt that sign posting to services was vital that more work needs to be done with the community to improve quality for individuals by understanding each community and its particular need. Quotes: ‘I have recently suffered from a badly fractured leg and have received very good care over the 5 months from Calderdale royal and the local physios. This is also true of my general health care, eye clinic at Huddersfield inf, and Beachwood medical centre’ ‘When you go in walk-in centres they are always very busy we are sent to A&E. So more walk in services should be available and more staff should be recruited’ ‘my experience have led me to wonder if paperwork has to take priority over face to face contact and care’ ‘I feel the standard of care has deteriorated in some hospitals and the food served is in some cases appalling, People need good nutrition to recover successfully mentally and physically’. ‘Huddersfield RI has given us fantastic support over the past 30 years. We are want to keep our local NHS service’ ‘Will minor injuries unit have doctors? What will be the opening hours of the minor injuries probably to 10pm what happens if an elderly patient falls out of hours? or in hours? Falls team, telehealth etc. etc. Elderly lady - fall out of bed, staff couldn’t pick her up, had to wait 2 hours for an ambulance’ ‘I am full of praise and confidence with CRH in them. They treated my husband with his near death experience’ ‘Following an explanation about the proposals people were generally understanding and supportive of proposals - 7 people attending a focus group’ ‘Cardiology and ophthalmology at Tod is used well’ ‘I know of two lives saved because of being close to Halifax hospital. One an unborn baby another a heart attack victim. It is a definite possibility if services are moved they may not have survived. Having the NHS open to valid criticism.’ 29 ‘Totally against moving accident and emergency from Calderdale. Access is already poor for the Calder Valley’ ‘The Halifax emergency dept. should be kept open but it should be better organised with perhaps a minor injury unit’. ‘I have had experience at the Halifax hospital and think it is well run and doing a great service for its community’ ‘Stand in the patient shoes more often’ ‘We closed Hx Infirmary, St Johns, Northowram just in this area - where are the savings. Bring Matrons back. Simple clean hospital standards with discipline and good quality nursing care’. ‘My experiences have not been good. Long waiting times, passing information on and being examined by 3 different doctors. No pillow or bedding offered .Not sure if we were staying the night or going home’. Remove smoking shelters and have an outright ban on smoking on NHS premises, applicable to all staff and patients. Invest in renewable energy to reduce costs in long term Provide covered cycling parking close to entrances What is the future role for home valley memorial hospital?’ Care was only available in one of the hospitals. I understand financial implications and the best care is a priority, Having recently had experience of A&E department in Calderdale I cannot speak highly enough of the care I was given.’ ‘As many insulin pump users live in the Hebden Bridge/Tod area we should have consultant services at Todmorden Medical Centre. When I fractured my knee I spent 2/3 weeks in Huddersfield hospital. It was very difficult for my husband to visit because he has Parkinson's disease. He found public transport too difficult to use because of too many changes to get to Huddersfield from Hebden Bridge (up at Dodd Naze) The distances to both hospitals need better public transport for older people’. ‘I think we shouldn't have to wake up in the morning just to book an appointment, and this still does not guarantee an appointment’. 7.2 Findings from the wider stakeholder meetings and events Target Audience: Key messages: Overview and Scrutiny Committee – Calderdale Overview and Scrutiny Committee – Kirklees Health and Well Being Boards - Calderdale Updates received – no key messages Need to clarify what minor injuries means Concern about loss of beds at CRH Updates received – no key messages 30 Health and Well Being Boards - Kirklees Local councillors and MPs - Calderdale Need to demonstrate topic 2 has a wider benefit for the wider geography. Developments at Todmorden would be welcome. Good communication is key Updates received – no key messages Local councillors and MPs - Kirklees Local Medical Committee GPs Positive about proposals; Anxious about impact on primary care Factor in workforce issues Need to clarify Trust and CCG boundaries re proposed visits to practices Agreed with the direction of travel Wanted to know how to involve primary care contractors further Why has old primary care models been dismantled and cut? Concerns about Social Services capacity Strong support for self-care models The need to understand and factor in changes in in patient flows as a result of changes e.g. possible increased flow to Barnsley The importance of effective and integrated IM and T to enable new ways of working The need for more community beds as a result of changes in hospital bed base Agreed the system would benefit from some re-design Pressures in both primary and secondary care Keen to bring primary and secondary care clinicians together to have conversations How do we convince decision makers of the clinical evidence base? Could PHH become a 4th partner in the process? Healthwatch - Calderdale Healthwatch - Kirklees Yorkshire Ambulance Service Need to clarify what minor injuries means Very concerned about the possibility of no A & E in Calderdale Want to see more info re what a Minor Injuries Unit would look like – the conditions/injuries it deals with. The importance of provision of additional services out of hospital Overall, constructive dialogue which highlighted the importance Healthwatch place on providing care out of hospital and reducing the need for hospital admissions Be honest about budget reductions What’s the cost of the PFI at Calderdale If both A & Es close how will we get home once treated How will we address gaps in services, e.g. continence What will happen if the M62 is shut Is losing 100 beds safe Will our-patients services be on both sites? Moving services into the community is great but we have to 31 Royal College of Midwives Community Pharmacy CHFT membership Council and councillors Local Care Direct Unions Third Sector 7.3 ensure we have resources in the community to manage them How will cultural changes be managed – previously clinics held at Todmorden were never that busy RCM seeing these changes up and down country Would we still be giving women the choice of service model Role of Community Pharmacy in helping to build confidence in self-care and prevention Push boundaries on dealing with complex patients Pharmacy could be developed into an intermediate service We need to look at the bigger West Yorkshire picture in terms of provision across the region Location of individual services not important, but infrastructure is Important to have assurances that funding provided for community services is used for that service LCD would like to be part of discussions. Want to be engaged further as part of the engagement process People less interested in big strategic plan – but whether they will have a job at the end! It’s a fait a complait /staff side concerned about the connectivity in the community The 3rd Sector are/can be the ‘champions of prevention. Need to consider how this is made a reality in the model Self-care model is understood by some, but not all – we need to find ways of describing it better Consider ‘digital inclusion’ so that people aren’t disadvantaged by digital developments Statutory partners need to be more inclusive of third sector, with the potential for partners. Attendees generally supported the proposals in the SOC document Discussion about a “super ambulance/ mobile hospital” Consider wheelchair/guide dog access to ambulances. High quality care is key Transport issues need addressing. Strong emphasis to Improve communications across voluntary sector and hospital boundaries Other findings 7.3.1 Staff Engagement: The feedback received from staff is as follows; Generally, staff are supportive of our preferred topic Staff recognise the longer-term benefits of changing the way services are delivered for both patients and staff Staff want to work with us on the design of new services 32 Staff recognised that this is one Trust with two hospitals – patients and staff are already familiar with the two hospitals CHFT Medical Division, had concerns over capacity and fit if HRI is unplanned site but in general a positive response and a good understanding of the need to change Estates staff in HRI stated spending capital in a building we own (if HRI) is good but were concerned that A&E waiting times will get worse if there is only one A&E Staff wanted to know if their jobs were secure Nursing staff wanted to see more District Nursing staff CHFT Nursing staff asked if A & E waiting times will get worse if there is only one and thought it was good to spend capital building on a building the Trust own (if HRI) Examples of poor service in community (poor palliative care) What will happen to ISS staff if HRI is the unplanned hospital. Will they transfer? What will be the impact on jobs at CRH if HRI is main site? Conscious that more people will choose to call 999 for an ambulance due to distance to travel from Calderdale(when maternity services moved to Halifax there was a worry that more women in labour would call 999) but that has proved not the be the case) What are GPs doing about appointments and increased number of A&E attendances because patients can’t get a GP appointment? Staff understand the rationale behind the proposed changes, but want to know more about how it might work in practice Staff wanted to better understand the thinking behind the Trust’s stated preference The services proposed would need extensive new build on the current HRI site and wanted to understand PFI arrangements more, there was a suggestion for one big hospital in Elland Senior consultant presence was needed outside daytime hours Staff wanted to know if the shuttle service will improve Staff asked if beds in the hospital would be reduced Social Care staff stated that a 7-day provision of Social Services is implicit in the new Care Bill and Urgent Care Agenda Community resources governed and managed by us, but not owned by us Learn from Locala example. Staff want to come back into Hospital setting as they feel isolated Significant Consultant presence in the community is needed to show investment of the current model The intermediate care teams wanted to know if Dewsbury had been factored into the A&E plans but were generally supportive of the plans 7.3.2 Stakeholder Event: Locality and Community services key messages: Single Info system or shared record essential Single assessment – build on through shared record Is it affordable? 33 7.3.3 Stakeholder Event: Specialist Hospitals key messages: There needs to be an unplanned site to meet all demands Public education is needed on the revised health and social care system Ensure proposals fit with a wider West Yorkshire plan 7.3.4 Stakeholder Event: Self-Managed Care key messages: Change of culture is needed for both staff and patients Not enough sharing of best practice currently to understand self-care 7.3.5 Stakeholder Event: Emergency and Urgent Care key messages: Attendees generally supportive of service models described in SOC 7.3.6 Letter from Barry Sheerman: Barry Sheerman MP, sent in a letter and a petition containing over 1,000 signatures opposing plans to the closure of the A&E department in either Calderdale or Huddersfield (see appendix - 10). The petition also came with 141 public comments relating to A&E services. The comments covered the following key themes: Keep A&E services in both Calderdale and Huddersfield, both local areas are large enough to require their own services. One A&E service will become overcrowded, services are already overcrowded. Travel and transport for people particularly in rural areas will not be possible because of the cost, time to travel and parking, if they have their own transport, will not be sufficient to cope with demand. The Elland by pass is gridlocked and will cause problems for emergency vehicles. Ambulance response times were a concern, including the time it would take to reach the hospital destination. There were a number of concerns that lives would be lost. Services were being cut as part of a cost cutting exercise. Current services were valued and there were lots of examples to support this. Local people want easy access to local facilities and there were a number of comments that services may go to Leeds. People want a say on what happens to ‘their’ services. Services work perfectly well as they are and people do not want them to change. 34 Quotes: ‘The whole idea is ridiculous. The point of Accident and Emergency is to give rapid, often life-saving access, help in a crisis. Increasing the distance of travel is plain daft, especially for the very young, the elderly, and the infirm.’ ‘No closure of life saving services, regardless of cost’. ‘The bypass between Huddersfield and Halifax is by no means free flowing. There is very little room for vehicles to manoeuvre to allow emergency services through’. ‘My 16 month old grandson has quite a rare congenital illness (congenital Adrenal Hyperplasia) and would not be alive if it were not for the A&E departments at both HRI and Calderdale. When his condition is acute he does not have time to travel far; his condition is critical and life threatening and he needs his local A&E department’. ‘The A&E in Huddersfield offers a fast and very satisfactory service in the community at present and should stay a vital part of Huddersfield!’ ‘One of the major reasons for living in towns the size of Huddersfield and Halifax is to have services in the locality without having to travel outside the town you live in. This was also my reason for supporting both towns having maternity wards several years ago’. ‘we need to keep the A&E our little boy Jake attended the A&E several times when he was a youngster unfortunately he passed away when he was 2 and a half in Leeds but it was Huddersfield who dealt with him first and they did a great job. Regards Carl (Jakes Dad)’ ‘We Need and A&E in Huddersfield. Can you imagine taking a child on two buses to Halifax when they have an accident…or will there be more ambulances and paramedics to meet demand as people can’t access A&E easily’ ‘Both these towns are large enough to warrant their own A&E units. The Elland bypass is gridlocked at peak periods, patients will die in the back of ambulances in the rush hour times.’ ‘I find this totally unacceptable, the NHS belongs to the people not management or government, leave our services alone!’ ‘In the past my husband has been taken to A&E by ambulance – each time he has been looked after with dignity, compassion and medical care…’ ‘How on earth are people who live in Todmorden going to get to HRI in an emergency. It is a joke!’ ‘How can you possible move emergency services to Leeds. Emergencies need highly skilled and specialist care within minutes not after a long arduous journey to Leeds. Where’s the common sense and compassion gone!’ 35 7.4 Equality Findings 1091 people partially or fully completed the equality monitoring form. The full detail is reported in (see appendix 11). To initially understand the validity of the data a comparison was undertaken with the local demographics of the population. Calderdale CCG is co-located with the local authority do the data is compared to the 2011 census. For Greater Huddersfield CCG the data (in the most part) comes from the census 2011 which covers the Kirklees local authority area. This mean the data cannot be a direct comparison. Any notable or expected variations will be noted. For some equality groups we do not have local data available for comparison so national data will be referred to. Sex There was no significant difference to the local demographics. Age groups The data for age was sourced from the mid 2011 population estimates for CCGs based on the 2011 census, so reflects the most accurate picture for Greater Huddersfield. There is significant difference in the under 18’s category with only 3% of survey respondents compared to a population of 22-23%. This is to be expected as the under 11s were not specifically engaged in this exercise. The 26-45 group was over represented 38% compared to 27% for both Calderdale and Greater Huddersfield CCG. Ethnicity There is a reasonable match to the local demographics with a couple of notable anomalies. There is a significant over representation of Pakistani populations at 33% compared to 7% (Calderdale) and at 10% (Kirklees). There is a commensurate under representation of White British at 56.2% compared to local populations of 87% (Calderdale) and 78% (Kirklees). Other less significant, but still notable differences are; the under representation of Indian people, this may be due to the majority of respondents coming from Calderdale; the underrepresentation of Other White people; there is a 1% ‘other’ ethnic group and an increase in the number of Arab people compared to the local population; there are fewer mixed White and Black Caribbean people, but more mixed White and Asian people. Population Calderdale % Kirklees % Respondents % White: English/Welsh/ Scottish/ Northern Irish/British 2.1 Mixed/ multiple ethnic group: White and Black Caribbean 0.5 Mixed/ multiple ethnic group: White and Black African 0.1 0.0 1.8 1.2 0.2 0.3 0.6 0.1 0.1 White : Irish White: Gypsy or Irish Travell er White : Other White 86.7 0.9 0.0 76.7 0.6 56.2 0.8 36 Population Calderdale % Kirklees % Mixed/ multiple ethnic group: White and Asian Mixed/ multiple ethnic group: Other Mixed Asian/ Asian British: Indian Asian/ Asian British: Pakistani Asian/ Asian British: Banglad eshi Asian/ Asian British: Chinese Asian/ Asian British: Other Asian 0.4 0.3 0.6 6.8 0.3 0.2 0.4 0.6 0.3 4.9 9.9 0.2 0.3 0.7 1.2 0 0.3 33.0 0.2 0.2 1.6 Respondents % Population Black/African/ Caribbean/ Black British: African Black/African/ Caribbean/Black British: Caribbean Black/African/ Caribbean/ Black British: Other Black Other ethnic group: Arab Other ethnic group: Any other ethnic group 0.2 0.2 0.0 0.1 0.2 0.6 1.1 0.2 0.3 0.4 0.5 0.2 0 0.7 0.9 Calderdale % Kirklees % Respondents % Religion Of those who stated they had a religion the data showed an over representation of Muslim people 36% compared to 7.3% (Calderdale) and 14.5% (Kirklees), Buddhists and ‘other’ were also over represented but to a much lesser extent. There was a significant gap in respondents of a Christian faith 25% compared to 56% (Calderdale) and 53% (Kirklees). Disability There is limited data available about the local population of disabled people the census has 2 measures; ‘day to day activity limited a lot’ and ‘day to day activity limited a little’. The survey respondents were asked ‘do you consider yourself to be disabled’ and 23% responded yes. The data from the census recorded 17.9% (Calderdale) and 17.7% (Kirklees). This was made up of people limited a lot, 8.2% (Calderdale) and 8.4 (Kirklees) and limited a little 9.7 (Calderdale) and 9.3% (Kirklees). In relation to the types of impairments; the majority of respondents had a long term condition (42%) or mental health condition (29%). Sexual orientation Of the respondents only 2% identified as lesbian (0.8%), gay man (0.5%) or bisexual (0.8%) (LGB). Sexual orientation is not included in the census so it is difficult to demonstrate a 37 local picture, but in the Integrated Household Survey, (Office of National Statistics), gave the following figures for the period April 2011 to March 2012: 1.1 per cent of the surveyed UK population, approximately 545,000 adults, identified themselves as Gay or Lesbian. 0.4 per cent of the surveyed UK population, approximately 220,000 adults, identified themselves as Bisexual. 0.3 per cent identified themselves as "Other". 2.7 per cent of 16- to 24-year-olds in the UK identified themselves as Gay, Lesbian or Bisexual compared with 0.4 per cent of 65-year-olds and over. There is a perception that many people chose ‘prefer not to say’ to this question for a variety of reasons reducing the number of respondents identifying as LGB. Of the people who stated ‘other’, two described themselves as ‘past it’ and widow’. Gender reassignment One of the greatest difficulties in measuring or estimating the size of the Trans population is that no systematic or reliable data has been collected through the Census or through other Government-sponsored surveys. However in 2011 research by GIRES* concluded, organisations should assume that 1% of their employees and service users may be experiencing some degree of gender variance. At some stage, about 0.2% may undergo transition. The number who have so far sought medical care is likely to be around 0.025%, and about 0.015% are likely to have undergone transition. (*Gender Identity Research and Education Society, 2011) of the respondents to the survey 0.2% said their gender identity was different to the sex they were assumed to be at birth. Pregnancy and maternity Of the respondents 2% said they were pregnant or had given birth in the last 6 months. Carers Of the respondents 10.4 identified themselves as carers, the 2011 census found 10.5% (Calderdale) and 10.4% (Kirklees). Reponses to Question ‘what do you think of the ideas in this leaflet’ An analysis was undertaken comparing responses to the question ‘What do you think about the ideas described in the leaflet’ to understand whether there were any different views dependent on protected characteristics. The responses were themed into positive, negative and neutral with 5 areas emerging which capture the comments made. These are; Hospital services Travel and transport Care and services in the community Delivering the model Engagement process and information provided Analysis of the themes has been undertaken compared to some of the protected characteristics, where there was a sufficient sample. This will be detailed below. 38 Sex There is no significant difference in responses from the sexes. Women Men Positive 53% 53% Negative 21% 17% Neutral 24% 30% When comments were broken down into the 5 themes and analysed (positive, negative, neutral) it became apparent that there was very limited differences in the views of men and women. Women were more negative about the hospital services (women, 50.4% men, 41.5%) and women were more positive about care and services in the community (women, 61.9% men, 45.7%). Quotes Women care and services in the community – positive quotes The idea that more services are nearer patients (providing the correct diagnoses and care programmes are in place and regular visits happen, treating patients in their own home and friendly surroundings would be ideal, particularly for the elderly. realistic, easily understood putting needs at heart localizing service can understand need for local hubs I think the ideas are good, especially the specialist community centres, bring services more local for people will help them access the healthcare they need easier and making these services accessible seven days a week is good too I feel community based services are an excellent idea however there must be the resources to deliver them gender specific services should be offered at places like the well womans centre Women and hospital services negative quotes Some of the views I find contradictory. Outlining plans for more community based care and then suggesting the relocation of hospital services to Huddersfield, Bradford and Leeds There are a selection of options but they fail to address a and e issue. Emergency care needs to be close to communities. I am dubious as to whether or not the decision about the future of a and e services has already been made. Halifax needs a and e department and gp surgeries should be open longer to alleviate the pressure on hospitals 39 Age The youngest group were the most positive, with the 46-65 coming next. In terms of negativity the oldest group were the most negative, although this is based on a small number of respondents (29). Under 18 18-25 26-45 46-65 66-80 81+ Positive 73% 50% 53% 59% 42% 38% Negative 14% 23% 20% 13% 21% 46% Neutral 14% 26% 27% 28% 36% 15% In terms of age groups analysed by theme the comments related to hospital services were mostly negative (31.5-55.7%) and neutral with no group giving a majority of positive comments. The most negative were the 26-45s (55.7%) with 18-25s (51.9%). In relation to care and services in the community the majority of age groups were positive (50-60%) however the 66-80s were much less positive (27.8%), similarly they had the most negative comments (22.2%). For delivering the model the majority of comments were positive (57.4-69.2%). Comments made by people over 81and under 18 have not been considered as the sample size is too small. Quotes Age 66-80 care in community negative quotes Supporting people to look after themselves at home. This hasn't worked the elderly who I have worked with for thirty Years deteriorate quite quickly when in their own. All ages positive care in community quotes like the idea of more community services, its good to empower people to take greater responsibility and their own health care. Agree with the specialist community centres and hubs. (46-65) Putting patients at the centre of services is an excellent idea and one that would definitely benefit the community (26-45) living out in Todmorden having services locally will be a huge benefit. i work in stroke early supported discharge and so i have seen the benefits of supporting people as they leave hospital. this could benefit other conditions especially orthopaedics/ surgery falls (26-45) Age 26-45 hospital negative quotes good ideas but not much attention paid to how deaf people can contact the NHS all based on centred services or telephone - needs rethinking. not good people will die if services are moved 40 Ethnic Group Only two ethnic groups have sufficient respondents to consider the themes raised by the data, these are the White British and Pakistani groups. The numbers for other groups would be too low to present an accurate picture. There is no significant difference in the opinions of these two groups. White British Asian Pakistani Positive Negative Neutral 53% 18% 29% 59% 17% 23% When the comments were analysed in relation to theme (comparing only White British and Pakistani groups) there were no significant differences, however Pakistani groups commented more positively on care and services in the community (Pakistani, 67.9% White 48.2%) and the engagement process and information provided (Pakistani, 72.5% White 63.6%). Quotes Pakistani – care in community positive quotes like ideas for community services and care and specialist centres positive ideas for older people for dementia Its making services less complicated its giving people choice and capabilities to have services nearer to home I think the ideas will help members of the community feel more confident in using the services by having local easy to access walk in centres and ability to get advice when needed. Disabled There does not seem to be a significant difference in views from disabled people to people without impairments. Yes No Positive 55% 53% Negative 19% 20% Neutral 26% 27% In considering the themes disabled people made more negative comments on hospital services (yes, 70.9% no, 43.0%) and less positive ones (yes, 6.4% no, 15.2%). When commenting on care and services in the community the differences were much less pronounced negative (yes, 9.7% no, 10.5%) but in contrast disabled people were more positive (yes, 64.5% no, 52.6%) 41 Religion Given the sample size it is only reasonable to consider Christianity and Islam for potential difference in opinion. Islam Christianity Positive 57% 47% Negative 18% 21% Neutral 25% 32% While Muslims are more positive about the ideas in the leaflet, Christians are more neutral. Carers Carers are more negative about the ideas within the leaflet. Yes No Positive 47% 55% Negative 27% 18% Neutral 26% 27% Other groups There are insufficient respondents to consider themes for sexual orientation, pregnancy and maternity and gender reassignment, although the participation is not considerably different than what would be expected compared to national demographics. 8 Findings from the Commissioners’ engagement process The focus of the Commissioners’ engagement was to gather views on the commissioning intentions as part of the five year plan. NHS Calderdale and Greater Huddersfield CCGs each have their own strategy these documents including a questionnaire were circulated to existing networks for comment and views gathered at the local drop in sessions for each CCG. A summary and easy read version of the commissioning intentions, were developed to ensure information was accessible (see appendix 6 and 7). 8.1 Findings The commissioners asked: Q1. Do you understand what we plan to do? 42 From the responses we received on this question 65% understood the plans definitely or to some extent and 16% thought they did. This left 19% who did not understand what the plans were describing which may have some bearing on the responses that follow. The commissioners asked: Q2.Do you agree with our plans? From those responding 59% did agree with our plans and those responding no or not really came in at 31% those who were unsure formed 10% or respondents. The questionnaire asked those responding to no or don’t know to describe their response and the following themes were identified: Those responding with no or don’t know (31%) told us: The plans were too vague or abstract and there was not enough detail to allow for comment The information was complex and hard for some people to understand The plans need to be better communicated to local people People want to know what it all means for them Some people wanted us to describe what we mean by planned and unplanned care and community care and what this means for A&E There were concerns that the plans are to reduce cost There were comments that we needed more focus on current appointment and waiting times More focus on keeping people healthy 43 Quotes You state, in effect, a member of deliverable objectives, but given no indication of priorities or how any of these objectives may either be obtained or delivered, or that they can’. ‘Plans as set out are very vague - just a wish list’. ‘Of the people who said not really and no not really the reasons were that the document does not offer enough information for anyone to make a decision. Writing a document can look good on paper, but it does not explain how and where the proposed changes would take place. Also when it talks about community services, what does this mean? These decisions will make a massive impact on people’s lives, their health and that of their families. Instead of writing flashy documents, GPs and these commissioners should hold public events regularly across Calderdale to explain and face up to people and take the real questions not hide behind websites and emails’. ‘Because your documents do not state clearly what may happen. Referring to planned and unplanned care means nothing to much of the population. We only know that a&e dept. is likely to close because others have translated for us. It looks like using jargon is a way to hide the facts’ Could be rationalised -Travel is big issue - people who need care are older/disabled - less likely to be able to travel visiting more difficult, agree with development of local services, increased availability of GPs It sounds as if you are piously relying on unpaid workers rushing in to replace paid ones but there is nothing to say that this must happen. ‘I don’t know if these plans cover enough of teaching us how to be healthy’ Not really/ no not at all - the plans look good on paper and if they are plans it suggests you have already made a decision. The commissioners asked: Q3. Is there anything missing in our plans that you think we should be doing to help improve the health of people living in Calderdale and Greater Huddersfield? 44 The feedback received was grouped into positive (green), negative (red) and neutral comments (amber). The chart above shows that the majority of comments received were neutral and negative, there were some positive comments and the feedback received formed the following categories: Those responding told us: There needs to be more engagement on the CCGs plans Better communication and more information Focus on diet and health That the CCG need to be able to adapt as local needs change More plans on dementia and dementia care Quotes Lack of consultation - limited events, poorly publicised Todmorden representation on CCG board and broader engagement Better more robust consultation on proposals ‘diet so very important but you know all this’ ‘Other health problems - you seem to have the right priorities here but we can only say be aware things change so how will you adapt and include any future health problems as they arise? Where care is provided this is not a good idea. If care is changed and moved to other providers who will monitor and check these. there are plenty of examples over the past few years of bad practice and as people who already suffer poor health and poor services this will only get worse with cuts kicking in’. ‘Dementia is a pressing problem and not specifically mentioned’. Yes. Why is there a "no change" option? We pay our taxes and so we should be able to say "no" to any changes. If you want to make change, start by providing proper service rather than sending people all over the place over and over again and then back to square one. Agree with more care in the community, but what do you mean by that? You don't say what they are. Can you provide services in the Youth Club? (Group of 15 young people) The Commissioners asked: Q4. Is there anything else you would like to tell us? Those responding told us: They want more plans to be publicised and more about the CCG and who you are They want to see a reduction in paperwork for GP’s but an improvement in GP opening times and appointments When dealing with people who are unwell we need to ensure the appropriate amount of time and care is given That they want to help find solutions and spend resources together Work more with young people and educate them at a young age 45 Use community groups to deliver plans Find more innovative solutions to delivering services like exercise classes and incentives to lose weight, relaxation classes etc. Quotes Publicise more with plans and meetings. Does not feel closing A&E is acceptable. We want to be informed of future consultation meetings. Good experience of ambulance treatment’ ‘Yes improve GP appointments times longer opening times, open a GP practice 24/7 to reduce minor injuries to a&e’. ‘I am a teenager with psoriasis and apart from creams I have not been given help with stress relief or relaxation though these have all been proven to help my condition why do I get creams’ 8.2 Findings from the Calderdale community assets not included in the analysis. The findings were a late submission so all the data captured is reported separately. 8.2.1 Responses from Mixenden, Illingworth and Ovenden area in Calderdale We received 44 responses from residents living in this area. Residents comments about the plans: 36 people understood the plan, 3 thought they did and 4 did not, we had 1 no response. From this 31 agreed with the plans with 10 not at all and 3 others stating they thought they did. The respondents understood the ‘what’ but needed to know the ‘how’ There was not enough detail in the plans to make an informed decision about what should be delivered People wanted to know what was meant by local delivery for them, where would it be centred and what do we mean by local, more things are needed in the local community More detail is needed about what services would like in this area. This needed to describe so that people could understand Concerns that one A&E would mean an overcrowded service Tougher on those who do not look after themselves i.e. alcohol related conditions The plans read as a move towards privatisation, with the plans not being workable More say in these plans for local people, more help form local people to design services Be honest about what is driving the change, the media portray things differently What was missing from the plans, residents told us: The areas described needed to be more specific in how they would support an individual, what would it mean for me 46 Improved access to GP services, improved appointment system was needed There were concerns about how services will be staffed People wanted to know plans for things such as opening times More focus on local communities and listen to local communities more Look at longer investment in projects and provide adequate budgets to community services such as Upbeat More focus on incentives and preventative services than treatment More services to support people with mental health problems, services like CAMHS need more staff and funding Need to consider transport and travel as part of your plans and improve patient transport services which are often slow and running late and people cannot travel to Huddersfield for services, concerns about ambulance transfer times More drop in services in other areas which can link to your GP practice for people working away from home More help for rough sleepers and the homeless who use A&E because they have nowhere else to go More services for people with a Learning Disability such as annual health checks Anything else people wanted to tell us: What is the case for moving A&E and what would replace it, keep the A&E as it is How will your plans affect me? GP appointment systems need improving Less focus on paperwork Loneliness and isolation is a huge problem and small groups and informal community activities can support this Sessions to help people who are in debt, which can cause depression Volunteer networks to support residents Schemes to help people just out of hospital, gardening, shopping, cleaning and people to have a chat More choice of places to go when we need help other than healthcare settings Local support for people with diabetes, groups that can advise on diet. Lifestyle help people go the gym and back to work More services that operate as a drop in – informal places for a coffee and chat Concerns that older people may not receive the treatment they need to save costs More education in schools about health, first aid and managing minor health issues Better coordination of services from hospital to community i.e. physiotherapy stopped on discharge from hospital and patients are often discharged too soon without any help or support All the care has gone out of the NHS Look at funding play therapy 47 8.2.2 Cornhome and Walsden Residents, Calderdale Residents in Cornholme and Walsden held a focus group with residents to discuss the commissioning intentions and provide feedback. This document was received in the form of a report and the following summarises the findings from this exercise. The full report can be found in appendix 12. The main themes emerging from conversations with residents in this area were the distance from hospital and the lack of public transport at night, leaving costly transport such as a taxi the only solution; most were unable to afford this option. Residents stated they would like to see: GP communication and information systems need to be improved, more facilities such as Skype and use of email for the deaf Patient information shared between hospitals and GPs needed to be handled more effectively Enough GPs to cover the work described in the plan and to play a stronger role they need to sort out their own services A better transport system to get people back home if they are transferred to a hospital far away More community services in Cornholme including more GP nurse services, a baby clinic and other services closer to home More investment in preventative medicine particularly massage and physiotherapists. More emphasis on a good diet with the healthcare system leading by example More information and involvement for families and carers if a patient has a sensory disability so they can support communication and care of the patient Early detection of mental health and better care and treatment, more information in schools People with mental health problems and dementia treated better as currently they are treated as second class citizens and the care they receive is not appropriate 8.2.3 Calderdale Basement Project: Calderdale Basement project provided 24 responses to the CCG plans. The project supports people with substance misuse and is a third sector organisation based in Halifax town centre. Respondents comments about the plans: 10 people understand the plan, 11 thought they did and 5 did not. From this 9 agreed with the plans with 7 not at all and 10 others stating they thought they did. Services should be left alone There is not enough information about what you do and why Why change something that works? Why do it now? I don’t understand the plans As long as it improves things I agree You will do what you want anyway why ask our opinion 48 What was missing from the plans, respondents told us: More home care from CPNs and more CPNs More medication reviews, reviews completed more often More home help and less focus on services in health settings or hospitals Access to better psychiatrists Anything else people wanted to tell us: 8.3 No one will listen to what I say anyway or we can’t influence anything Stop messing with systems that are in place We should know about your plans sooner, more information, more often Listen to our suggestions Decisions should be well thought out if money is an issue More help and training for those carers who care at home Keep the things that work that we have now and create more accessible services. More holistic therapy on offer Employ Doctors who care about us Findings from Greater Huddersfield ‘Care Close to Home’ engagement activity In January 2014, Greater Huddersfield CCG engaged with the public, key stakeholders, providers and voluntary and community sector organisations in Kirklees to gain views and ideas on their intentions to deliver care as part of Right Care, Right Time, Right Place. The views of 202 people were gathered over this period including 60 people who attended a stakeholder event, 112 people completing a survey and 30 people attending a Primary Care event, all activity took place between January and February 2014. The main themes taken from the engagement and the key points are highlighted below: Supported self-care and prevention To be supported in being healthy and to be encouraged to self-care by providing access to information, advice and support with regards to diet, exercise, support groups / networks and who to contact for on-going support Individuals supported to take responsibility for their own health and wellbeing Provision of local, affordable gym and exercise / sport Early intervention through better identification of patients at risk and targeted support Diagnosis and care planning specific themes Individualised care plan held electronically that can be accessed by patient and professionals – plan needs to be outcome focused not just based on medical needs, refreshed regularly and with a holistic approach to care while improving safety and quality 49 Preventing admission to hospital specific themes Ensuring patients are fully involved in the development of their care plan and informed, so they know what to expect, who to contact, provision of ongoing care / support and regular reviews to help reduce the chance of a crisis occurring. Improve staffing at Care homes – increase staffing, ensure staff receive appropriate training and support to improve care and prevent high turnover of staff. Consider an increase in bed provision. Greater innovation and use of technology to improve outcomes and transformation Discharge planning specific themes To involve patients and their families throughout the planning of their discharge. To enable them to make an informed choice, they should be advised on what services are available and what their options are. The approach needs to be holistic and flexible to meet the individual needs of the patient. This should be done early enough, to ensure that the appropriate services can be put in place. Upon discharge, patients need to know what to expect and who to contact should they require any further advice or support. Greater integration of care across pathways which break down traditional barriers in primary, community, secondary and social care Terminology needs to change from discharge to transfer of care. It was felt that discharge implies that no longer receiving care; however, in most cases the care transfers to another provider, this transfer needs to be seamless. Overarching themes that emerged across more than one area Regular reviews, follow ups and ongoing support and for this to be provided at home or closer to home. Ongoing involvement of patients and their families / carers throughout their care. Enabling them to make informed choices and ensuring that they are provided with information that they are able to understand. Patients need to know about their diagnosis, what to expect, how to manage their condition, what their treatment options are, what ongoing support or care is available and who to contact for further support. Doing the right thing for patients and their families Provision of care navigators To be able to access the right services at the right time and for more services to be available in the evening and at the weekend. Ability for services and patients to access their patient record Provision of a seamless / integrated service staffed by a skilled and flexible workforce that wraps around the needs of the patient. Improve and increase the use of technology, such as telemedicine, self-care hub, assistive technology 50 In May 2014, a follow up event was held which further focussed on the development of an integrated community-based service model (Care closer to home), which had been developed using the feedback from the engagement undertaken in January 2014. 32 people attended the stakeholder event and the key themes are listed below: The need for care and support that is co-ordinated and planned What is needed to regain independence Core Community Team Functions and stakeholder views on what this could look like Ongoing Care and what this means for patients Specialist in-reach / Out-reach and the functions of this service Rapid response And how to support discharge Some of the general comments were: Where is prevention and self-care in the model? Care co-ordinator needs skills and experience to direct patients – anti natal, post natal, children, and older patients – when they need it A Single point of access needs to have access to a wide range of information (using integrated systems) to ensure appropriate next steps/onward referral. Specialist functions should be part of this. For example, a lot of antenatal care should lead to higher need around postnatal depression – need access to specialist services Need to take into account the needs of the population and the localities – it may differ between areas as there will be pockets of various needs Referral to be changed to access. Role of pharmacy in prevention. How do they interact with social services care needs based on patient feedback Concerns – follow up appointments for procedures need to be adhered to as sometimes they are lost in the system and forgotten about e.g. bone density scans, MRI scans How are services going to join and be accessible 24/7 across health & social care? There are gaps at the moment Sharing information across agencies is key to ensuring the care navigator and anyone else involved in the care/support of an individual Concerns: how will Joe Public without up to date technology know where to go for help in the first place? And get through the maze of info available? Concerns: timetable for e.g. Occupational therapies, physiotherapy appointments, pain management – at present this is inadequate ALL services should be available via Choose & Book / NHS E-referral Need to speak to deaf people/hard of hearing people/blind & visually impaired people who all have different needs and will have some suggestions 51 8.4 Equality Monitoring 126 people partially or fully completed the equality monitoring form (see appendix 13). The equality monitoring form was not attached to the questionnaire so unfortunately it has not been possible to compare views held by particular protected groups. To initially understand the validity of the data a comparison was undertaken with the local demographics of the population. As Calderdale CCG is co-located with the local authority the data is accurate to the 2011 census. For Greater Huddersfield CCG the data (in the most part) comes from the census 2011 which covers the Kirklees local authority area. This mean the data cannot be a direct comparison. Any notable or expected variations will be noted. For some equality groups we do not have local data available for comparison so national data will be referred to. Sex Of the respondents 65% were women and 28% men, this means many more women responded compared to the population locally. % Calderdale Kirklees Respondents Men 48.9 49.4 28.0 Women 51.1 50.6 65.0 Age groups The data for age was sourced from the mid 2011 population estimates for CCGs based on the 2011 census, so reflects the most accurate picture for Greater Huddersfield. There is significant difference in the under 18’s category with only 9.4% of survey respondents compared to a population of 22-23%. This is to be expected as the under 13s were not specifically targeted in this exercise. There was a slight over-representation of 18-25s, 26-45 and 46-65, with reduced numbers of the 66-80 and no over 81 year olds. 52 Age Place % 0-17 Calderdale Greater Huddersfield Calderdale Greater Huddersfield Calderdale Greater Huddersfield Calderdale Greater Huddersfield Calderdale Greater Huddersfield Calderdale Greater Huddersfield 22% 18-25 26-45 46-65 66-80 81+ Respondents No % 22% 12 9.4 18 14 40 31.4 40 31.4 9 7 0 0 9% 11% 27% 27% 27% 26% 11% 11% 4% 4% Ethnicity There is a significant over representation of Pakistani populations at 19.7% compared to 7% (Calderdale) and at 10% (Kirklees). There is a commensurate under representation of White British at 41% compared to local populations of 87% (Calderdale) and 78% (Kirklees). The other groups with less prominent over representation are; white other, mixed, white and Black African and mixed, white and Asian. All other groups are under-represented. The sample size, however was quite small at 127 people so this could be expected to some extent, with the most notable under representation is that of Indian people. Calderdale % Kirklees % Respondents% White: English/ Welsh/ Scottish/ Northern Irish/British White: Irish White: Gypsy or Irish Traveller White: Other White Mixed/ multiple ethnic group: White and Black Caribbean Mixed/multiple ethnic group: White and Black African 86.7 0.9 0.0 2.1 0.5 0.1 76.7 0.6 0.0 1.8 1.2 0.2 41.0 0 0 4.7 0 0.78 53 Mixed/ multiple ethnic group: White and Asian Mixed/ multiple ethnic group: Other Mixed Asian/ Asian British: Indian Asian/ Asian British: Pakistani Asian/ Asian British: Banglad eshi Asian/ Asian British: Chinese Asian/ Asian British: Other Asian Calderdale % 0.4 0.3 0.6 6.8 0.3 0.2 0.4 Kirklees % 0.6 0.3 4.9 9.9 0.2 0.3 0.7 0.78 0 0 19.7 0 0 0 Other ethnic group: Arab Other ethnic group: Any other ethnic group Respondents % Calderdale % Kirklees % Respondents % Black/ African/ Caribbean/ Black British: African Black/African/ Caribbean/Black British: Caribbean Black/ African/ Caribbean/ Black British: Other Black 0.2 0.2 0.0 0.1 0.2 0.6 1.1 0.2 0.3 0.4 2.4 0 0.78 0.78 0 Religion Of those who stated they had a religion the data showed an over representation of Muslim people 23.6% compared to 7.3% (Calderdale) and 14.5% (Kirklees), Buddhists were also over represented but to a much lesser extent. There was a significant gap in respondents of a Christian faith 25% compared to 56% (Calderdale) and 53% (Kirklees). Christianity Islam Buddhist 0.3 Calderdale % 56.3 7.3 Kirklees 0.2 53.4 14.5 % Respondents 0.78 25 23.6 % Disability There is limited data available about the local population of disabled people the census has 2 measures; ‘day to day activity limited a lot’ and ‘day to day activity limited a little’. The survey respondents were asked ‘do you consider yourself to be disabled’ and 21.3% responded yes. The data from the census recorded 17.9% (Calderdale) and 17.7% 54 (Kirklees). This was made up of people limited a lot, 8.2% (Calderdale) and 8.4 (Kirklees) and limited a little 9.7 (Calderdale) and 9.3% (Kirklees). In relation to the types of impairments; of those defining an impairment the majority of respondents had a mental health condition (40%). Calderdale Kirklees Day-to-day Day-to-day Respondents activities activities ‘do you limited a limited a consider lot little yourself to be disabled’ 21.3 8.2 9.7 8.4 9.3 Sexual orientation Of the respondents 7.9% identified as lesbian (3.1%), gay man (3.93%) or bisexual (0.8%) (LGB), this could be an over representation, however sexual orientation is not included in the census so it is difficult to demonstrate a local picture, but in the Integrated Household Survey, (Office of National Statistics), gave the following figures for the period April 2011 to March 2012: 1.1 per cent of the surveyed UK population, approximately 545,000 adults, identified themselves as Gay or Lesbian. 0.4 per cent of the surveyed UK population, approximately 220,000 adults, identified themselves as Bisexual. 0.3 per cent identified themselves as "Other". 2.7 per cent of 16- to 24-year-olds in the UK identified themselves as Gay, Lesbian or Bisexual compared with 0.4 per cent of 65-year-olds and over. Gender reassignment One of the greatest difficulties in measuring or estimating the size of the Trans population is that no systematic or reliable data has been collected through the Census or through other Government-sponsored surveys. However in 2011 research by GIRES concluded, organisations should assume that 1% of their employees and service users may be experiencing some degree of gender variance. At some stage, about 0.2% may undergo transition. The number who have so far sought medical care is likely to be around 0.025%, and about 0.015% are likely to have undergone transition. (Gender Identity Research and Education Society, 2011) of the respondents to the survey none said their gender identity was different to the sex they were assumed to be at birth. Pregnancy and maternity Of the respondents 0.78% said they were pregnant or had given birth in the last 6 months. 55 Carers Of the respondents 18.1% identified themselves as carers, the 2011 census found 10.5% (Calderdale) and 10.4% (Kirklees). 9. Equality and diversity The majority of the engagement activity has been equality monitored to assess the representativeness of the communities reached during the engagement process. The monitoring is optional and some people chose not to participate, other methods of engagement such as the comments cards did not include equality monitoring. Once data had been gathered it was analysed, this allowed for comparison with the local demographic data and where possible trends in responses identified. This information is presented in this report and will be used to contribute to the equality impact assessment for the Right Care, Right Time, Right Place programme. Equality monitoring is an essential part of our legal requirement to ensure we have given due consideration to protected groups. However, as they are optional, not all equality forms are completed fully and some not at all. Overall through the various engagement activities 1306 equality forms were gathered. The majority of these were through the 2 questionnaires that considered the SOC and the 5 year strategy. The results of these is described earlier in this report. The drop in sessions utilised a shorter equality monitoring form to understand who had attended. This gave us the following data from the attendees who completed the form. 89 people completed the form, of which; 55% women, 43% men 91% White British, 3.4 % Asian 18% were disabled In terms of ages; Under 18 18-45 46-65 66-75 75+ % 1 16 39 31 8 In terms of a comparison to local demographics the drop in sessions were not well attended by people from Black and Minority Ethnic communities or by younger people. 56 Considering the reach of the engagement activity there are a number of themes; There was no significant difference in views on the ideas in the SOC leaflet for different equality groups Most protected groups were represented; where there was over representation this was of a group who usually have less of a voice so it benefited the programme to hear them; where there was under representation this was of young people under 18 and some ethnicities (see recommendations) Drop in sessions did not attract a diverse population, possibly due to the appeal of such activities, venue choice, timing or a perception that it does not affect them 9.1 Equality recommendations The engagement activity has mostly met a representative sample of the majority of the local population. It would not seem necessary to repeat the exercise to target any particular communities to address the gaps that have emerged through the analysis. There would however be learning for future activity; 10. reaching the Indian population and other ethnic groups reaching young people considering the methodologies utilised to attract different groups Overall findings and common themes The engagement process carried out on behalf of the Providers and Commissioners in the response to the case for change jointly produced findings which highlighted some common themes. It is clear that the public see one health system and views relating to primary and secondary care were contained in each of the engagement exercises. The areas or aspects of care which were highlighted as being of highest importance to the public when redesigning a health care system are as follows (these are not cited in any order of importance): People wanted to see more care closer to home and in a variety of community settings The public in Calderdale do not want to lose their A&E as part of services changing Travel and transport needed further consideration as people could neither afford the time to travel; the cost, or find suitable parking on premises. People want services to be based locally Access to services in the community needed to be 24/7 including bank holidays and there was a strong message that GP access in particular needed to be addressed if the system was to change. People also wanted services they could drop in to People wanted more focus on prevention and innovative opportunities to keep themselves well or be educated, particularly at a young age Appropriate staff are needed in the community and this included more GP’s, district nursing staff and those with a particular focus on a specialism or to meet the needs of diverse communities 57 There were concerns that the model looked good on paper but would it work in practice, this included comments relating to capacity to deliver including social care, how information is shared and how services are coordinated People did not understand the detail of any of the plans and wanted to understand this further People wanted the community to be part of the solution including design, delivery and estates with greater community participation being the key to delivering services for each community Mental health services were not working and there was a need to look at services further in both primary and community care Hospital services were poor on waiting times and needed to improve in addition there were a number of comments that people are discharged too early There needs to be more consideration for vulnerable groups, protected groups, carers and those with a disability These themes reflect on the whole the things that people have already told us they would like to see in the planning of future health and social care services. Whilst staff training had been mentioned previously it was not reflected as a priority in these engagement findings although people did want to see the right staff with the right skills in the community model. Education and information was not described as a theme on this occasion although the details regarding ideas for supported self-care included these areas. Technology was cited as telephone access and sharing information in this instance and managing risk and safeguarding were reflected in people’s experiences which varied. 11. How the findings will be used to inform our plans With the information we already have, the findings from the recent engagement activity and the information we gather at the stakeholder event we will: Further develop a ‘Community Model’ for Calderdale. Further develop a ‘Community Model’ for Greater Huddersfield. Inform the specification we have developed for the ‘In Hospital Model’ In addition: The CCG governing bodies will make a decision about the next steps. NHS England will look at our plans along with the ‘Yorkshire and Humber Clinical Senate’ as part of the NHS England ‘Strategic Change Assurance Process’. We will provide a full document containing all our findings and the feedback from the engagement activity on the Right Care, Right Time, Right Place website. In addition we will inform people of any further decisions or updates on the website. The website address is. http://www.rightcaretimeplace.co.uk/ 58 Appendix 1: CCG, Communication and Engagement Strategy ‘Right Care, Right Time, Right Place’ Communication, Engagement and Equality Strategy and Action Plan Commissioners’ NHS Calderdale and Greater Huddersfield Clinical Commissioning Groups 59 1. Introduction The purpose of the Communication, Engagement and Equality Strategy and Action Plan is to describe our proposals for engaging with staff, the public, patients and carers on the commissioning intentions for Calderdale and Greater Huddersfield service reconfiguration as part of our response to the Calderdale and Huddersfield Health and Social Care Strategic Review, ‘Right Care, Right Time, Right Place’. The plan does this by describing the background to the review and the ‘Case for Change’, a brief introduction to the Providers’ response to ‘Right Care, Right Time, Right Place’, Calderdale and Greater Huddersfield commissioning intentions and our plans for delivering engagement activity; this includes what we already know. 2. The Case for Change The way we deliver health and social care services needs to change to make sure it can meet current and future needs. Huge advances in medicine have changed the way we treat illness and injury; we have a growing and an aging population; our illnesses are different and people’s expectations of health care are growing. We know people want care closer to, or at, home and a choice about how, when and where they’re treated. The cost of health and social care across Calderdale and Huddersfield is now more than £600 million a year. Growing demand, price inflation and the costs of new drugs and treatments mean we need to look at how we spend budgets to get maximum benefit for everyone. We need to ask some serious questions; Can we do things differently but maintain high quality services? Can we keep people out of hospital for everything but the most serious illness by improving the way we care for them at home? All seven organisations involved in health and social care in Calderdale and Huddersfield are working together on the review, ‘Right Care, Right Time, Right Place’: Calderdale and Huddersfield NHS Foundation Trust (CHFT) Calderdale Clinical Commissioning Group (CCCG) Calderdale Metropolitan Borough Council Greater Huddersfield Clinical Commissioning Group (GHCCG) Kirklees Metropolitan Borough Council Locala Community Partnerships South West Yorkshire Partnership Foundation Trust (SWYPT) The review consists of four working groups attended by staff, managers and clinicians from each of the partner organisations; each group has been tasked with identifying proposals which will ensure we can meet the future needs of our population. The four working groups are: 60 Integration and Personalisation - ‘Integrating services delivered in the community and integrated commissioning and personalisation’. The vision is to improve efficiency by removing duplication, streamlining management of services and providing specialist care in community settings where appropriate. Working together to change the health and care system by shifting resources towards early intervention and prevention of health conditions while reducing duplication. Children - ‘Taking forward the proposals from the Children’s Care Stream’ The Children’s Care Stream has developed a 10 year vision for the transformation of children's services: every child will have a healthy start and continue to lead a safe, happy life with every opportunity to achieve their potential within their families and communities. Capacity and Capability - ‘To deliver best in class care and support through existing capability and capacity ‘ The working group wants to enable individuals and their families to make informed choices about their lifestyle and management of health conditions and improve the effectiveness and responsiveness of services so that care providers ‘do it once’ and ‘do it well’. Digitisation - ‘To digitise the health and social care economy’ The working group wants to improve efficiency and to support people to live independent lives for longer but making best use of information technology, changing the way services are delivered and driving additional efficiency by joining up IT systems across the health and social care economy. 3. The Providers’ response to ‘Right Care, Right Time, Right Place’ Alongside the work taking place within the review, a Strategic Outline Case (SOC) has been prepared in collaboration by three provider partner organisations; Calderdale and Huddersfield Foundation Trust, Locala Community Partnerships and South West Yorkshire Partnership NHS Foundation Trust (SWYPFT). This outline case is a response to ‘Right Care, Right Time, Right Place’ and a review by the National Clinical Advisory Team (NCAT) in spring 2013. The Providers’ response describes a new model for the provision of hospital and community services across Calderdale and Greater Huddersfield. Under this model, the three providers would work together and closely with general practice, social care and voluntary organisations (the third sector) to deliver integrated care and support services in the community. This will include including moving current hospital-based services closer to where people live. The response states that: integrated community services would work seamlessly with 61 acute and emergency services that would be based on one specialist hospital site and with planned and elective care on a second specialist planned care hospital site. It also identifies significant benefits to patients, services users, local people and service providers and commissioners. The scenarios included in the document have been drawn from a significant local, national and international evidence base and are recommended and supported by senior doctors and other health and social care professionals from all three providers. It is important to recognise that the response is underpinned by a strong patient, service user, public and stakeholder voice which will be refined and change following further discussions and deliberations amongst the seven Strategic Review partners and the public. The response will be subject to a separate engagement process which will be published on the Right Care, Right Time, Right Place website. This process will describe how the Providers’ will engage with staff, key stakeholders, public, patients and their representatives to strengthen their proposal. Once the findings from the Providers’ engagement have been evaluated, a report of findings will be produced and this will further inform our commissioning intentions. We will use the information to enable us to assess the extent to which the Providers’ response is in line with staff, key stakeholders, public, patients and their representatives’ views and how we deliver future services. Until this process is complete, no decision can be taken about significant changes to the future of services in Calderdale and Greater Huddersfield. Any decision of this significance will be made by the commissioning organisation and not the provider and can only be made after a period of formal consultation. 4. NHS Calderdale and Greater Huddersfield CCG Commissioning Intentions – the Commissioners’ response NHS Calderdale and Greater Huddersfield Clinical Commissioning Groups (CCG’s) are responsible for commissioning a range of services in Calderdale and Greater Huddersfield. Using the information already held on the local areas using the JSNA and working with partners in the Health and Well Being Board, CCG’s need to ensure that their commissioning intentions meet the needs of the local community. In order to deliver these intentions each CCG has a five year strategy based on what they already know about the community and the health needs in the local area. NHS Calderdale CCG – five year strategic plan We have developed a plan for Calderdale which sets out our five year ambition. This ambition includes a vision for the future, which is the Commissioners’ contribution to the 62 delivery of change as a partner in the Calderdale and Huddersfield Strategic Review, ‘Right Care, Right Time, Right place’. Our system has recognised that significant change is essential in order to ensure that everyone gets the right care at the right time and in the right place, whilst responding to the challenges it faces. The plan builds on our organisational aims, which are: To Commission high quality services that are evidence based and make the most of available resources Seek to ensure that all Calderdale residents have access to appropriate clinical care at all times Encourage and enable the development of care closer to home Continue to tackle variation in the quality of services provided to ensure improved experience and outcomes Improve access to and choice of services Enhance integration and collaboration for service delivery Improve infrastructure to support delivery Encourage the development of supportive learning environments In developing this plan we have maintained the integrity of our aspirations for Calderdale, whilst ensuring we respond to the need to change the system around us. We have developed our plans using information from The Joint Strategic Needs Assessment (JSNA) and the Health and Well-Being Strategy for Calderdale together with information and intelligence gathered from previous engagement and patient experience activity. In addition we have used clinical insights and refreshed our outcomes and design principles to ensure we will make the changes needed to deliver the outcomes for local people, ensuring services are safe and of high quality. The focus of our change programme over the next 5 years is to continue the shift of services and resources from unplanned hospital care to integrated health and social care delivered in community and primary care settings. The first 3 years of our plan will be heavily focused on work already started to create and deliver new models of unplanned and urgent care. We have developed a number of improvement programmes which will drive the delivery of our ambition over the next 3-5 years. These programmes are: Cardiovascular Diabetes Respiratory Alcohol conditions Musculoskeletal Cancer & tumours Mental health Strategic Review 63 Better Care Fund Each programme is described in more detail and we want to ensure that our plans reflect the needs of our local community. The engagement activity will enable us to have more detailed conversations on our plans and help us to understand how we can deliver these over the next five years. NHS Greater Huddersfield CCG – two year operational plan and five year strategic plan NHS Greater Huddersfield CCG has developed a two year operational plan and a five year strategic plan. The Vision for our larger health and social care system in the next five years has been developed in partnership with NHS North Kirklees CCG and Kirklees local authority. The strategic planning footprint has a pivotal role in bringing together the partners to develop proposals for transformational change. The development of the vision for our larger health and social care system in the next five years has also been greatly influenced by our proactive collaboration in the Calderdale and Huddersfield Strategic Review, Right Care, right time, right Place. As a CCG, our two year strategic plan is based on our contribution to delivery of this change. Our system has recognised that significant change is essential because we want to ensure that everyone gets the right care at the right time and in the right place, whilst responding to the challenges it faces. We know that to meet current challenges, service delivery will need to change on an unprecedented scale. Delivering care across existing systems will be a key development for the future of service delivery and evidence suggests that a “systems thinking approach” will be required to understand the environment and the complex interactions within it. NHS Greater Huddersfield Clinical Commissioning Groups (GHCCG) operational plan sets out a unique and innovative vision of health and social care service delivery for the next two years in this locality. GHCCG has set the development of its two year plan within the context of the footprints in which we plan and deliver services. In developing this Plan we have maintained the integrity of our aspirations for GHCCG. We have aligned ambitions across our units of planning (particularly those of our economy-wide change programme) to ensure synergy in delivery and maximise the opportunities to make large scale, sustainable change: The focus of our change programme over the next two years is to continue the shift of services and resources from unplanned hospital care to integrated health and social care delivered in community and primary care settings. The first two years of our plan will be heavily focused on work already started to create and deliver new models of unplanned and urgent care and on our intention to provide a new model to deliver high quality, safe care out of hospital. 64 GHCCG recognise that transformational change is most likely to be achieved through the implementation of this medium term plan and our whole system long-term commissioning plans. Taking this longer-term perspective is crucial, as commissioners we need to develop bold and ambitious strategies for future service delivery. Benefits and Outcomes The outcomes delivered by these aspirations can be characterised into a number of themes: Increasing opportunities for self care Making best use of technology and innovation Optimising delivery in primary care Optimising delivery in secondary care Building community capacity to deliver better health and wellbeing The direction of commissioning for the CCG is fully contextualised within the local area and takes account of the holistic landscape of public sector service provision across the patch. The innovative approaches to community engagement and involvement developed in Greater Huddersfield provide a unique platform upon which to build locally steered and designed services, based on the real input from local people. As a result of this, local people can expect: Services delivered as close to home as possible Improved health and wellbeing Opportunities to have a say in the design of health and social care provision Accessible, non-discriminatory service provision Integrated services Services that maximise dignity and respect for vulnerable groups The plan sets out the pathway for the organisation to navigate a course through external change and uncertainty towards stable, responsive and sustainable health and social care services for Greater Huddersfield now and in the future. What will GHCCG health economy look like in two years’ time? In line with the strategic vision and the priorities arising from the needs assessment, the GHCCG health and social care economy in two years’ time will have the following characteristics: Improved outcomes and performance Improved safety and quality 65 Greater integration of care across pathways in primary, community, secondary and social care Clinical leadership at all levels Financial stability for all organisations, across the commissioning and provider health and social care economy Individuals supported to take responsibility for their own health care, through an integrated self-care programme Meaningful engagement of patients and communities in decision making and active use of patient experience to improve care Greater innovation and use of technology to drive improved outcomes and further support transformation Earlier intervention through better identification of patients at risk and targeted support (Risk stratification) Innovative forms of contracting which incentivise integration and joint delivery of better outcomes and quality The CCG recognises the importance of ensuring a good quality of care; this is reflected in both the approach to quality, with a focus on clinical leadership and embedding quality from strategic objectives to the point of care delivery. We understand that each of our residents within Greater Huddersfield will have different health needs now and in the future and so each and every patient journey through our services will be different. We have created a number of models for each of these areas; Self-management Primary Care Hospital Care Community and Mental Health Each model is described in more detail in the plan and we want to ensure that our plans reflect the needs of our local community. The engagement activity will enable us to have more detailed conversations on our plans and help us to understand how we can deliver these over the next five years. 5. The purpose of the strategy and action plan The purpose of the strategy and action plan is to provide information on our intention to engage with the following target audiences: Public, patients, carers and their representatives Local Councillors and MP’s Member practices and staff The strategy sets out why we need to engage with the target audience on our plans – this includes the legislation each CCG has to work from and our local approach to engagement. 66 The action plan sets out the activity people can expect to take place as part of our delivery of the engagement, the timelines involved and who will be leading on the work. This will help people to understand what to expect from an engagement exercise, how they can be involved and how long the process will take. 6. What have public, patients and carers already told us? Engagement activity delivered as part of ‘Right Care, Right Time, Right place’ took place from October 2012 to February 2013. This activity provided us with insight on a number of key themes. The insights were supported by from three years of data collection using information stored in PALS (Patient Advice and Liaison Service), Complaints, Patient Opinion, NHS Choices, local and national surveys and dedicated engagement events. During this time and to date we have been able to reach; 44 members of the public through planned care focus groups 1, 653 people via a survey about unplanned care – this included 97 web based responses, 247 location interviews and 1,313 hard copy survey returns 50 members of the public participated in a long term care event, and 254 children and young people were directly engaged on unplanned care The total number of people directly engaged in conversations was 2,002 people and we have an engagement reach using the Clinical Commissioning Group (CCGs) relationship matrix. The relationship matrix is a list of organisations that are willing to circulate information to their own members. We have a profile of each organisation on the matrix which means we can reach of 24,440 people from various localities and protected characteristics. In addition we combined all the data held by all seven partners’ organisations using Patient Advice and Liaison Service (PALS), complaints, local and national surveys over the past three years. This intelligence captured an estimated combined reach of approximately 12,000 people. This year (2013/2014) we have directly engaged with approximately 5,000 people on a variety of service areas. All this information has been combined together to provide the programme office for the Calderdale and Huddersfield Strategic Review, Right Care, Right Time, Right Place with some common themes and has provided us with real insight into how services should be provided in the future. The common themes were: Timely and consistent access to services Coordinated and integrated care Services closer to home Involve us in decisions about our care and in planning care Better use of technology. 67 In addition we have delivered the NHS national “Call to Action’ and received the views of 487 people who told us what was important to them. The public identified 13 themes, in order of importance the themes were: Education and information Invest in the community National solutions and campaigns Self Care Improve access to health services Staff and training Working together Regular check ups Discharge planning and better hospitals Manage risk and safeguarding More services in the community Invest in technology Accountability Each of themes has been presented to the Strategic Review Programme Board in more detail. The commissioners have captured all this feedback and have used it as a basis for describing their commissioning intentions. 7. Aim and objectives of the engagement activity The aim of the engagement exercise will be to talk to key stakeholders, which includes staff, public, patients, carers and their representatives using a series of activities to ensure our commissioning intentions have been properly discussed and considered, and any additional views are taken into account. This information will help us to understand our approach to delivering the commissioning intentions and inform any future plans. In addition, we will use the information to further inform the providers response to the way services can be provided in the future and ensure as CCG’s we have considered the needs of our local population from a commissioner’s perspective. We want to describe our commissioning intentions to local people by making sure our two strategies are available for people to read, by producing a summary document, which includes a version in an accessible format. Using these aims, the objectives will be: To ensure any engagement activity is delivered in line with current legislation 68 To listen to a representative sample of public views on the proposals using a variety of mechanisms to engage with people and capture views To communicate clearly and simply the messages in an accessible format, how we intend to commission services in the future and receive feedback on these should be delivered To use the information from the engagement exercise to assess the extent to which the Providers response will deliver services in line with your views To ensure we meet with a representative sample of the population to understand if there are any particular impacts on the nine protected groups as defined by the Equality Act 2010 To analyse results and identify potential trends – including those relevant to protected groups To provide a report of findings on the engagement process. This report will be used to inform our plans to deliver services in the future To provide feedback to staff, public, patients and carers on the findings of the engagement activity To ensure that adequate engagement has been undertaken The engagement activity taking place to inform our plans will be delivered in conjunction with the commissioners. Diagram below describes the process we will use: Case For Change Providers’ Strategic Outline Case Commissioning Intentions Existing Mechanisms Drop in Sessions Asset Based Approach Stakeholder Events Development of Joint Report of findings Stakeholder Event Commissioners’ Service Change Proposals Stakeholder Event CCGs’ Governing Body Decision on Proposals 69 8. Principles for Engagement NHS Calderdale and Greater Huddersfield CCGs both have ‘Patient and Public Engagement and Experience Strategies’. These strategies have been developed alongside key stakeholders. The strategies set out the approach to engagement and what the public can expect when we deliver any engagement activity. The principles in both strategies state that we will; Ensure that we engage with our public, patients and carers early enough throughout any process Be inclusive in our engagement activity and consider the needs of our local population Ensure that engagement is based on the right information and good communication so people feel fully informed Ensure that we are transparent in our dealings with the public and discuss things openly and honestly Provide a platform for people to influence our thinking and challenge our decisions Ensure that any engagement activity is proportionate to the issue and that we provide feedback to those who have been involved in that activity The strategy sets out what the public can reasonably expect us to do as part of any engagement activity and the process we need to deliver needs to preserve these principles to ensure public expectations are preserved. 9. Legislation Health and Social Care Act 2012 The Health and Social Care Act 2012 makes provision for Clinical Commissioning Groups (CCGs) to establish appropriate collaborative arrangements with other CCGs, local authorities and other partners. It also places a specific duty on CCGs to ensure that health services are provided in a way which promotes the NHS Constitution – and to promote awareness of the NHS Constitution. Specifically, CCGs must involve and consult patients and the public: in their planning of commissioning arrangements in the development and consideration of proposals for changes in the commissioning arrangements where the implementation of the proposals would have an impact on the manner in which the services are delivered to the individuals or the range of health services available to them, and In decisions affecting the operation of the commissioning arrangements where the implementation of the decisions would (if made) have such an impact. 70 The Act also updates Section 244 of the consolidated NHS Act 2006 which requires NHS organisations to consult relevant Overview and Scrutiny Committees (OSCs) on any proposals for a substantial development of the health service in the area of the local authority, or a substantial variation in the provision of services. The Equality Act 2010 The Equality Act 2010 unifies and extends previous equality legislation. Nine characteristics are protected by the Act, age, disability, gender reassignment, marriage and civil partnership, pregnancy and maternity, race, religion and belief, sex and sexual orientation. Section 149 of the Equality Act 2010 states that all public authorities must have due regard to the need to a) eliminate discrimination, harassment and victimisation, b) advance ‘equality of opportunity’, and c) foster good relations. All public authorities have this duty so the partners will need to be assured that “due regard” has been paid through the delivery of this strategy and in the review as a whole. The NHS Constitution The NHS Constitution came into force in January 2010 following the Health Act 2009. The constitution places a statutory duty on NHS bodies and explains a number of patient rights which are a legal entitlement protected by law. One of these rights is the right to be involved directly or through representatives: In the planning of healthcare services The development and consideration of proposals for changes in the way those services are provided, and In the decisions to be made affecting the operation of those services 10. Engagement The engagement activity will be planned to capture views of local people with a specific focus on patients currently using services, protected groups and carers. A plan proposing the engagement activity is attached as an action plan (appendix 1). What we already have in place We currently have a number of mechanisms in place to capture the views of the public. These mechanisms have already informed our commissioning intentions and will continue to be utilised throughout this process. The current engagement mechanisms we have in place are: A dedicated website which will contain information on how to contact us and also opportunities to post comments. This includes the use of social media such as Twitter and Facebook. 71 PALS and complaints services who regularly capture public views as part of their customer facing role. We work closely with Healthwatch colleagues to ensure we listen to people’s views. We work closely with our staff and member practices, including Patient Reference Groups. We review existing consumer websites including those attached to the local media, patient opinion and NHS Choices to gather feedback. We gather the views and opinions through national and local surveys on specific service areas or topics. We have a ‘Relationship Matrix’ which enables to engage with a number of key organisations. These organisations are mapped by the target audience they reach and the protected characteristics we cover. In Calderdale we work closely with the third sector and have invested in ‘Health Connections’ a third sector hub which ensures we can engage with third sector colleagues providing support to health. Greater Huddersfield work with third Sector leaders. In addition Calderdale use an ‘Asset Based Approach’ to engaging our local population, this means we train and fund local groups to talk to the public on our behalf using the methods and approaches appropriate to that community. We work with 44 groups in varying localities representing some of the most seldom heard residents in our area. Greater Huddersfield work closely with local authority colleagues to deliver similar activities. What else do we need to do? In order to enable the public to engage on our commissioning priorities we will need to provide further platforms for discussion, offer stakeholders the chance to host conversations and directly target those groups who we need specific feedback from. This will include any groups who may have been underrepresented in any previous engagement activity. The engagement activity will be delivered using a number of mechanisms; these are: Drop in sessions - To ensure all members of the community we serve have an opportunity to have their say, we will need to deliver drop in sessions in each local area. Each session will be on different days to give as many people as possible the chance to attend. The drop in sessions will provide a platform for the public to talk to us about our commissioning intentions, the provider response and ‘Right Care, Right Time, Right place’. There will also be an information stand displayed about the ideas we have in easy to understand and accessible formats. We recommend that we deliver 12 drop in sessions across Calderdale and Greater Huddersfield. Comments cards – Comments cards will be available at the drop in sessions and in other service areas for people to write down any comments, issues or concerns they may have. 72 A comments box will also be made available for the comments cards to be posted to provide anonymity. Media and communications - The communication channels identified in section 10 will be used to disseminate information about the drop in sessions and will describe any other opportunities for involvement. In addition a contact name and number will be provided for members of the public to contact should they need more information. The media support required includes: Sign-post people to websites where they can receive more information and provide comment Provide a contact point for anyone requesting a presentation or discussion on our commissioning intentions Social media feeds Media releases and liaison Existing networks - In addition we need to capture people’s view through engagement and conversation and we can use our networks and existing platforms to host conversations and ensure comments and views are captured on the proposals by circulating a summary document and attaching a short questionnaire. We can use third sector organisations and membership networks to deliver this. Stakeholder events – Two joint stakeholder events will be organised following the engagement with wider target audiences. These events are displayed in the diagram on page 12. The events will form part of the engagement process and ensure that key stakeholders are engaged in the development of any proposals. The first stakeholder event will be set up to consider the information we have collected jointly, the second event will be to present the proposals we have developed following the first event. To ensure we capture a representative sample of community views we will equality monitor at all engagement activity intervention. This will enable us to reach protected groups who may have different experiences of health and social care services, where we do not reach those protected groups we will specifically target engagement to reach them. 11. Communication Communication channels identified in this section will be used to disseminate information and will provide opportunities for patients and the public to provide their views. The methods below will also be supported by the communication leads for each organisation using a central team within the Programme Management Office to produce press releases, content for social media, intranet and internet sites and staff engagement. We will use the following delivery methods to reach each of the named target audiences: 73 Target Audience Service users, general public, third sector OSC/Health and Wellbeing boards Staff Healthwatch Elected members / Councillors Partners’ intranets, websites and social media platforms Relationship matrix Patient Reference Groups Third Sector umbrella organisations. Patient groups Carers groups Meetings/ briefings Internal bulletins Staff Intranets Cascades at meetings through managers. Media 12. Delivery Method Email and personal discussions Newsletter articles Information to be circulated electronically – explanatory email with a link to web survey Proactive media releases briefings Social media Equality All engagement activity will be equality monitored to assess the representativeness of the views gathered during the engagement process. Where there are gaps in gathering the views of specific groups relating to the protected characteristics, this will need to be addressed. The engagement activity is required to identify trends in opinion and these will form part of the engagement process with findings feeding directly into the Equality Impact Assessment. To ensure we have given due consideration to equality issues we will undertake a full Equality Impact Assessment (EQIA) on the results of our engagement and detail the process we have undertaken to ensure we are full informed about any adverse impact or consequence for any group. This will ensure we have the potential to improve equality outcomes. 13. Non pay budget required We have already identified a budget, which will deliver the engagement on the Providers’ response. We will work together on the drop in sessions and these have already been accounted for in the Providers’ engagement plan. The budget set out below highlights the additional costs required. 74 Engagement Phase Budget Commissioning Intentions Summary document to be developed and accessible formats created £2,000.00 Events display materials and presentations Maximum additional total budget required £2,000.00 £4,000.00 14. Analysis of data and presentation of findings We will fully utilise all existing engagement intelligence and ensure that we have gathered and considered previous information to inform the process. Once the proposed engagement activity has taken place we will ensure that all recent and existing intelligence is captured into one report, this will include engagement activity delivered as part of the Providers’ response. This report will provide an overview of the views of staff, public, patients and carers. This report will be received through internal reporting mechanisms and a decision will be made on the next steps. The report and decision will be shared with providers. 15. How the findings will be used to inform our plans With the information we already have, the findings from the recent engagement activity and the information we gather at the stakeholder event we will: Further develop a ‘Community Model’ for Calderdale. Further develop a ‘Community Model’ for Greater Huddersfield. Inform the specification we have developed for the ‘In Hospital Model’ In addition: The CCG governing bodies will make a decision about the next steps. NHS England will look at our plans along with the ‘Yorkshire and Humber Clinical Senate’ as part of the NHS England ‘Strategic Change Assurance Process’. We will provide a full document containing all our findings and the feedback from the engagement activity on the Right Care, Right Time, Right Place website. In addition we will inform people of any further decisions or updates on the website. The website address is. http://www.rightcaretimeplace.co.uk/ 75 Appendix 2: Provider, Communications and Engagement Strategy Right Care, Right Time, Right Place Communication, Engagement and Equality Strategy and Action Plan Providers’ 76 Introduction The purpose of the Communication, Engagement and Equality Strategy and Action Plan is to describe our proposals for engaging with staff, the public, patients and carers on the Providers’ response to ‘Right Care, Right Time, Right Place’. The strategy does this by describing the background to the Strategic Review through the Case for Change, The Strategic Outline Case and the CCG’s intentions. The document tells you about our plans for delivering engagement activity which includes a brief summary of what people have already told us. The Case for Change The way we deliver health and social care services needs to change to make sure it can meet current and future needs. Huge advances in medicine have changed the way we treat illness and injury; we have a growing and an aging population; our illnesses are different and people’s expectations of health care are growing. We know people want care closer to, or at, home and a choice about how, when and where they’re treated. The cost of health and social care across Calderdale and Huddersfield is now more than £600 million a year. Growing demand, price inflation and the costs of new drugs and treatments mean we need to look at how we spend budgets to get maximum benefit for everyone. We need to ask some serious questions; Can we do things differently but maintain high quality services? Can we keep people out of hospital for everything but the most serious illness by improving the way we care for them at home? All seven organisations involved in health and social care in Calderdale and Huddersfield are working together on the review, ‘Right Care, Right Time, Right Place’: Calderdale and Huddersfield NHS Foundation Trust (CHFT) Calderdale Clinical Commissioning Group (CCCG) Calderdale Metropolitan Borough Council Greater Huddersfield Clinical Commissioning Group (GHCCG) Kirklees Council Locala Community Partnerships South West Yorkshire Partnership Foundation Trust (SWYPT). The review consists of four working groups attended by staff, managers and clinicians from each of the partner organisations; each group has been tasked with identifying proposals which will ensure we can meet the future needs of our population. The four working groups are: Integration and Personalisation - ‘Integrating services delivered in the community and integrated commissioning and personalisation’. The vision is to improve efficiency by removing duplication, streamlining management of services and providing specialist care in community settings where appropriate. Working together 77 to change the health and care system by shifting resources towards early intervention and prevention of health conditions while reducing duplication. Children - ‘Taking forward the proposals from the Children’s Care Stream’ The Children’s Care Stream has developed a 10 year vision for the transformation of children's services: every child will have a healthy start and continue to lead a safe, happy life with every opportunity to achieve their potential within their families and communities. Capacity and Capability - ‘To deliver best in class care and support through existing capability and capacity ‘ The working group wants to enable individuals and their families to make informed choices about their lifestyle and management of health conditions and improve the effectiveness and responsiveness of services so that care providers ‘do it once’ and ‘do it well’. Digitisation - ‘To digitise the health and social care economy’ The working group wants to improve efficiency and to support people to live independent lives for longer but making best use of information technology, changing the way services are delivered and driving additional efficiency by joining up IT systems across the health and social care economy. Calderdale and Greater Huddersfield Commissioning Intentions – The Commissioners’ response Calderdale and Greater Huddersfield CCG are the commissioners for the local area. The commissioners buy services on behalf of the local population of Calderdale and Greater Huddersfield from providers. Providers include Calderdale and Huddersfield Foundation Trust, Locala and South West Yorkshire Foundation Trust. The CCG also work with the local authority to ensure services are provided in partnership. Each CCG has a five year strategy in place, this strategy takes into account national and local priorities. These priorities need to be delivered using the finances allocated whilst achieving the necessary outcomes and improvements. The strategic review takes account of these priorities and supports delivery in a partnership approach. The CCG are responsible for engagement on their commissioning intentions and this activity will also take place at the same time as the provider engagement on ‘Right Care, Right Time, Right Place’. The Providers’ response to ‘Right Care, Right Time, Right Place’ Alongside the work taking place within the review, as Providers’ we have prepared a Strategic Outline Case (SOC) in collaboration with our three provider partner organisations; Calderdale and Huddersfield Foundation Trust, Locala Community Partnerships and South West Yorkshire Partnership NHS Foundation Trust (SWYPFT). This outline case is a response to ‘Right Care, Right Time, Right Place’ and a review by the National Clinical Advisory Team (NCAT) in spring 2013. 78 The Providers’ response describes a new model for the provision of hospital and community services across Calderdale and Greater Huddersfield. Under this model, the three providers would work together and closely with general practice, social care and voluntary organisations (the third sector) to deliver integrated care and support services in the community. This will include including moving current hospital-based services closer to where people live. The response states that: integrated community services would work seamlessly with acute and emergency services that would be based on one specialist hospital site and with planned and elective care on a second specialist planned care hospital site. It also identifies significant benefits to patients, services users, local people and service providers and commissioners. The scenarios included in the document have been drawn from a significant local, national and international evidence base and are recommended and supported by senior doctors and other health and social care professionals from all three providers. It is important to recognise that the response is underpinned by a strong patient, service user, public and stakeholder voice which will be refined and change following further discussions and deliberations amongst the seven Strategic Review partners and the public. The response will be subject to a separate engagement process which will be published on the Strategic Review website. This process will describe how the Providers’ will engage with staff, key stakeholders, public, patients and their representatives to strengthen their proposal. Once the findings from the Providers’ engagement have been evaluated, a report of findings will be produced and this will further inform our commissioning intentions. We will use the information to enable us to assess the extent to which the Providers’ response is in line with staff, key stakeholders, public, patients and their representatives’ views and how we deliver future services. Until this process is complete, no decision can be taken about significant changes to the future of services in Calderdale and Greater Huddersfield. Any decision of this significance will be made by the commissioning organisation and not the provider and can only be made after a period of formal consultation. The purpose of the Strategy and Action Plan The purpose of the Communication, Engagement and Equality strategy and action plan is to provide information on our intention to engage with the following target audiences: Key stakeholders including partner organisations 79 Staff Public, patients, carers and their representatives Local Councillors and MP’s The strategy sets out why we need to engage with the public on our plans - which includes the legislation we need to work within. We want to involve as many people as possible to strengthen our plans. The action plan sets out the activity people can expect to take place as part of our delivery of the strategy, the timelines involved and who will be leading on the work. This will help people to understand what to expect from an engagement exercise, how they can be involved and how long the process will take. What have public, patients and carers already told us? We have used information already gathered from staff, public, patient’s carers and their representatives from the last 18 months. This engagement activity delivered as part of the ‘Right Care, Right Time, Right Place’ took place from October 2012 to February 2013 and has been used to inform our response. This activity reports provided us with insight on a number of key themes. These insights were supported by from three years of data collection using information stored in PALS (Patient Advice and Liaison Service), Complaints, Patient Opinion, NHS Choices, local and national surveys and dedicated engagement events. During this time and to date the review reached; 44 members of the public through planned care focus groups. 1, 653 people via a survey about unplanned care – this included 97 web based responses, 247 location interviews and 1,313 hard copy survey returns. 50 members of the public participated in a long term care event, and 254 children and young people were directly engaged on unplanned care. The total number of people directly engaged in conversations was 2,002 people and an engagement reach using the Clinical Commissioning Group (CCGs) relationship matrix. The Relationship Matrix is a list of organisations that are willing to circulate information to their own members. The matrix has a profile of each organisation on the which means we can reach of 24,440 people from various localities and protected characteristics. In addition we combined all the data held by all seven partner organisations using Patient Advice and Liaison Service (PALS), complaints, local and national surveys over the past three years. This intelligence captured an estimated combined reach of approximately 12,000 people. This year (2013/2014) we have directly engaged with approximately 5,000 people on a variety of service areas. All this information has been combined together to provide us with some common themes and real insight into how services should be provided in the future. The common themes were: 80 Timely and consistent access to services Coordinated and integrated care Services closer to home Involve us in decisions about our care and in planning care Better use of technology. In addition the local NHS national “Call to Action’ engagement activity received the views of 487 people across Calderdale and Greater Huddersfield. The public identified 13 themes, in order of importance the themes were: Education and information Invest in the community National solutions and campaigns Self Care Improve access to health services Staff and training Working together Regular check ups Discharge planning and better hospitals Manage risk and safeguarding More services in the community Invest in technology Accountability We have captured all this feedback and it has been used as a basis for describing the landscape of health and social care services in the future from a provider perspective. Aim and objectives of the engagement activity The aim of the engagement exercise will be to communicate and engage with key stakeholders on our response to ‘Right Care, Right Time, Right Place’. The target audiences will include professionals, clinicians, staff, public, patients, carers and their representatives and we will use a number of mechanisms and key activities to deliver this. We want to share what people have already told us and listen to people’s views so we can ensure we have captured as many views as possible. By engaging in this way we can ensure any plans have been properly discussed and everyone’s views have been considered. We need to ensure that we give ‘intelligent consideration’ to our findings to ensure we can evidence how the intelligence has informed our plans. Using these aims, the objectives will be: 81 To communicate clearly and simply the messages in an accessible format, how our plans will deliver services for residents, staff and service users living in both Calderdale and Greater Huddersfield. To listen to public views on the plans using a variety of mechanisms to engage with people and capture views. To actively engage with current service users and staff to understand in more detail their views and the direct impact they may have on those currently working for, and using a service. To ensure we meet with a representative sample of the population to understand if there are any particular impacts on the nine protected groups as defined by the Equality Act 2010. To analyse and identify key themes from what residents, staff and service users have told us so - including those relevant to protected groups. To provide a report of findings on the engagement process, which will help inform the development of proposals, which will be subject to a formal consultation. To provide feedback to staff, public, patients and carers on the findings of the engagement activity. To ensure any engagement activity is delivered in line with current legislation. To ensure that adequate engagement has been undertaken . The engagement activity taking place to inform our plans will be delivered in conjunction with the commissioners. The diagram describes the process we will use: Case For Change Providers’ Strategic Outline Case Commissioning Intentions Existing Mechanisms Drop in Sessions Asset Based Approach Stakeholder Events Development of Joint Report of findings Stakeholder Event Commissioners’ Service Change Proposals Stakeholder Event CCGs’ Governing Body Decision on Proposals 82 Legislation Health and Social Care Act 2012 The Health and Social Care Act 2012 makes provision for Clinical Commissioning Groups (CCGs) to establish appropriate collaborative arrangements with other CCGs, local authorities and other partners. It also places a specific duty on CCGs to ensure that health services are provided in a way which promotes the NHS Constitution – and to promote awareness of the NHS Constitution. Specifically, CCGs must involve and consult patients and the public: in their planning of commissioning arrangements in the development and consideration of proposals for changes in the commissioning arrangements where the implementation of the proposals would have an impact on the manner in which the services are delivered to the individuals or the range of health services available to them, and in decisions affecting the operation of the commissioning arrangements where the implementation of the decisions would (if made) have such an impact. The Act also updates Section 244 of the consolidated NHS Act 2006 which requires NHS organisations to consult relevant Overview and Scrutiny Committees (OSCs) on any proposals for a substantial development of the health service in the area of the local authority, or a substantial variation in the provision of services. The Equality Act 2010 The Equality Act 2010 unifies and extends previous equality legislation. Nine characteristics are protected by the Act, age, disability, gender reassignment, marriage and civil partnership, pregnancy and maternity, race, religion and belief, sex and sexual orientation. Section 149 of the Equality Act 2010 states that all public authorities must have due regard to the need to a) eliminate discrimination, harassment and victimisation, b) advance ‘equality of opportunity’, and c) foster good relations. All public authorities have this duty so the partners will need to be assured that “due regard” has been paid through the delivery of this strategy and in the review as a whole. The NHS Constitution The NHS Constitution came into force in January 2010 following the Health Act 2009. The constitution places a statutory duty on NHS bodies and explains a number of patient rights which are a legal entitlement protected by law. One of these rights is the right to be involved directly or through representatives: In the planning of healthcare services The development and consideration of proposals for changes in the way those services are provided, and In the decisions to be made affecting the operation of those services. 83 Engagement The engagement activity will be planned to capture views of staff and local people with a specific focus on protected groups and carers. A plan proposing the engagement activity is attached as an action plan (appendix 1). What we already have in place We currently have a number of mechanisms in place to capture the views of the public. These mechanisms will continue to be utilised throughout this process. The current engagement mechanisms are: Local councillors and MP’s have been kept up to date with briefings and a log of all conversations and contact has been established. Overview and Scrutiny Committees and Health and Well Being Boards are being kept up to date with our plans through presentations and briefings. PALS and complaints services have been fully briefed and they will capture public views as part of their customer facing role. We are working closely with Healthwatch colleagues to ensure we provide consistent messages to the public and capture views on a day to day basis. We will trawl existing consumer websites including those attached to the local media, patient opinion and NHS Choices to gather feedback. What else do we need to do? In order to enable the public to engage with us we will need to provide further platforms for discussion, offer stakeholders the chance to host conversations and directly target those groups who we need specific feedback from. This will include any groups who may have been underrepresented in any previous engagement activity. The engagement activity will be delivered using a number of mechanisms and will need full commitment from all partners to providing staffing and appropriate key speakers as required. The engagement mechanisms will be: Drop in sessions - To ensure all members of the community we serve have an opportunity to have their say, we will need to deliver drop in sessions in each local area. Each session will be on different days and dates to give as many people as possible the chance to attend. The drop in sessions will provide a platform for the public to talk to us about the proposals and for staff to listen to peoples’ views. There will also be an information stand displayed in easy to understand and accessible formats. We recommend that we deliver 12 drop in sessions across Calderdale and Greater Huddersfield to cover a number of geographical locations. Comments cards – comments cards will be available at the drop in sessions and in other service areas for people to write down any comments, issues or concerns they may have. A comments box will also be made available for the comments cards to be posted to provide anonymity. 84 Media and communications - The communication channels identified in section 10 will be used to disseminate information about the drop in sessions and will describe any other opportunities for involvement. In addition a contact name and number will be provided for members of the public to contact should they need more information. The media support required includes: Posters in key locations to promote the engagement and advertise the drop in sessions Sign-post people to websites where they can receive more information and provide comment Social media feeds Media releases and liaison Existing networks - In addition we need to capture people’s view through engagement and conversation and we can use our networks and existing platforms to host conversations and ensure comments and views are captured on the proposals by circulating a summary document and attaching a short questionnaire. We can use third sector organisations and membership networks to deliver this. To be able to ensure we capture a representative sample of community views we will equality monitor at each engagement activity intervention. This will enable us to ensure we reach protected groups who may have different experiences of health and social care services, and where we do not we will specifically target engagement to reach them. Staff engagement – we will be using the same material to engage staff. We will build on existing platforms in organisations and utilise notice boards, websites, staff briefings, local intranets through partner organisations. Political stakeholders – We will write to core MPs to offer monthly informal briefings to keep them abreast of progress with the strategic review and address any specific questions they may have. In this letter we will also inform them in advance of any new material being posted on our website. In addition we will write to the elected members of each council via the appropriate officers offering a similar approach. This will be in addition to reacting as appropriate to any suggestions for alternative approaches the MPs and/or elected members may suggest. Staff, clinicians and professionals – We will engage with key stakeholders through a number of key stakeholder events which will focus on key themes. The key themes will be: Locality and community model Specialist hospital sites How will self-care work Emergency and urgent care Community hubs Non-financial appraisal criteria Stakeholder events – Two joint stakeholder events will be organised following the engagement with wider target audiences. These events are displayed in the diagram on page 12. The events will form part of the engagement process and ensure that key stakeholders are engaged in the development of any proposals. The first stakeholder event 85 will be set up to consider the information we have collected jointly, the second event will be to present the proposals we have developed following the first event. To ensure we capture a representative sample of community views we will equality monitor at all engagement activity intervention. This will enable us to reach protected groups who may have different experiences of health and social care services, where we do not reach those protected groups we will specifically target engagement to reach them. Communication Current communication channels will be utilised to reach service users, the public and stakeholders to distribute information and to raise awareness of the activity taking place so this will support the engagement process. In addition a communication plan will be developed which supports future communications with key stakeholders. This will include a number of activities including: Development of a media release to let people know how we intend to engage with patients, public and other stakeholders. Build messaging about our approach to engagement into on-going media liaison opportunities Supporting the production and distribution of the engagement document for use in engagement meetings and events including any supporting media like Q&A documents. Work with communications colleagues to develop further collateral to explain the Providers’ response. The methods below will also be supported by the communication leads for each organisation that will collectively agree content for social media, intranet and internet sites and staff engagement. In summary we will use the following delivery methods to reach each of the named target audiences; these will be described in more detail in the communication plan: Target Audience Service users, general public, third sector OSC/Health and Wellbeing boards Staff Healthwatch Delivery Method Partners’ intranets, websites and social media platforms Partners’ membership forums Relationship matrix Patient Reference Groups Third Sector umbrella organisations. Patient groups Carers groups Meetings/ briefings Internal bulletins Staff Intranets Cascades at meetings through managers. Briefing meeting 86 Elected members / Councillors Local Professional Committees Media Email and personal discussions Newsletter articles Information to be circulated electronically – explanatory email with a link to web survey Information to be circulated electronically. Face to face discussions to be offered to LMCs etc. Proactive media releases briefings Social media Equality All engagement activity will be equality monitored to assess the representativeness of the views gathered during the engagement process. Where there are gaps in gathering the views of specific groups relating to the protected characteristics, this will need to be addressed prior to any formal consultation. The engagement activity is required to identify trends in opinion and these will form part of the engagement process with findings feeding directly into the Equality Impact Assessment for the Full Business Case. To ensure we have given due consideration to equality issues we will undertake a full Equality Impact Assessment (EQIA) on the results of our engagement and detail the process we have undertaken to ensure we are full informed about any adverse impact or consequence for any group. This will ensure we have the potential to improve equality outcomes. Non pay budget required Engagement Phase Budget Providers’ response to ‘Right Care, Right Time. Right Place’ Item Community Champions/Community Assets - KMBC Community assets – Calderdale CCG Children and Young People specific engagement - KMBC Children and Young People specific engagement - Calderdale Venue Hire – 4 for Calderdale (upper and lower valley, central and north) – 5 for Greater Huddersfield (town centre, Denby Dale, Holmfirth, Slaithwaite, Salendine Nook) including refreshments Interpreters Engagement document (low key) – Leaflet, summary document, questionnaire, design, printing, electronic format. Accessible formats – language, large print, Braille and easy read Posters in GP practices and localities Events display materials and presentations Estimated Cost £10,000.00 £7,500.00 £ 2,000.00 Funded £5,000.00 £500.00 £4,000.00 £500.00 £1,000.00 £2,000.00 87 Press adverts Radio Phoenix £2,000.00 Free Maximum total budget required 34,500.00 Analysis of data and presentation of findings We will fully utilise all existing engagement intelligence and ensure that we have gathered and considered previous information to inform the process. Once the proposed engagement activity has taken place we will ensure that all recent and existing intelligence is captured into one report. This report will provide an overview of the views of staff, public, patients and carers on the proposals. This report will be received through internal reporting mechanisms and a decision will be made on the next steps which may include a formal consultation process. A Communications, ‘Engagement and Equality Formal Consultation Plan’ will then be developed to accompany this process. How the findings will be used to inform our plans We have already used the views of the staff, public, patients, carers and stakeholders to inform our plans. This information is identified in section 6, ‘What have staff, the public, patients and carers already told us?’ The next stage of engagement will be to help us to understand if what people have already told us is all we need to consider when developing further plans. We need to ensure that we provide platforms for engagement to test out our thinking and identify if there is anything else we should consider. This information will be used to further inform the development of future proposals. The process for ensuring we intelligently consider views is highlighted in the stages listed below: Stage 1 – (Autumn 2013) Develop scenarios based on what we already know and what staff, public, patient’s carers and stakeholders have already told us. This will be achieved through analysing the information we already have. Stage 2 – (April – June 2014) Engage further with staff, the public, patients, carers and stakeholders to understand if we have considered everything. Stage 3 – (June –July 2014) Test our proposals using two stakeholder events and assurance from the Consultation Institute. 88 Appendix 3 Calderdale and Huddersfield Strategic Review - Engagement Stage April, May and June 2014. Drop in sessions – Calderdale and Greater Huddersfield Catchment Area Drop in Location Date of meeting Time of meeting North Halifax New Beginnings @Threeways Thursday 10th April 2014 2pm - 7pm Fartown Fartown Village Hall Tuesday 8th April 2014 2pm – 7pm Catchment Area Drop in Location Date of meeting Time of meeting Salendine Nook Salendine Nook YMCA Wednesday 28th May 2pm - 7pm Slaithwaite Slaithwaite Civic Hall Friday 30th May 2pm -7pm Upper Valley Mytholmroyd Community Centre Monday 2nd June 2014 2pm – 7pm Fartown Fartown Village Hall Tuesday 3rd June 2014 2pm – 7pm Lower Valley Brighouse Civic Hall Wednesday 4th June 2014 2pm-7pm Denby Kirkburton “The Hub” Thursday 5th June 2014 2pm – 7pm Central Halifax Hanson Lane Enterprise Centre Monday 9th June 2014 2pm – 7pm North Halifax New Beginnings @Threeways Tuesday 10th June 2pm – 7pm Holmfirth Holmfirth Civic Hall Wednesday 11th June 2pm-7pm Todmorden Todmorden Health Centre Thursday 12th June 2pm – 7pm 89 Asset Based Approach – Planned Activities - Greater Huddersfield from 1st April – 31st May Group / Forum Contact Existing / New Description Location Protected Characteristics Engagement Officer Best Time To Engage Estimated numbers Sister Shout Existing Lesbian Support Group Town Centre Yes Carmen- Tuesday Eve 10 HUGG Existing Huddersfield Gay Group Town Centre Yes Carmen Wednesday Eve 22 Chinese Community Centre Existing Social Hub for Chinese Community in South Kirklees Town Centre Yes Carmen Awaiting response 10 APNA Health Existing South Asian community Health Support Group Springwood Temple Yes Carmen with Sally Awaiting date 50 Kurdish School Existing Women and children South Kirklees Yes Carmen 9th April – 12 noon 10 Huddersfield Deaf Community Existing Huddersfield Centre for the Deaf Huddersfield Town Centre Yes Carmen with Sally 1st May at 6pm 20 Huddersfield African Caribbean Cultural Trust Existing Huddersfield Caribbean Carnival/promotion of Caribbean culture in schools and amongst young people and the community. Huddersfield Town Centre Yes Rebecca Evening 7 Ahmadiyya Muslim Association Existing Faith Group and Health Focus Birkby Yes Both male and female groups Rebecca and Laila Friday Daytime 70 REACH project Existing Support for Asylum Seekers and Refugees New North Baptist Church New North Parade Huddersfield Sarli 15 April 2014 11.30am 15-20 Moldgreen United Reformed Church Yes Jeremy Tuesday morning end April/Early May 2014 10 Kirklees Volunteer Centre Huddersfield town centre Yes Rebecca Flexible Huddersfield town centre Pack Horse Centre Polish Parish Huddersfield Thornton Lodge Yes Rebecca and Carmen Once a month on a Thursday evening Up to 70 Yes Rebecca and Sally Up to 20 Yes Sarli Tues lunch time every fortnight Monday Lunchtime Crosland Moor Yes Sarli To be confirmed 15 Yes Sarli Tbc 12 Moldgreen United Reformed Church Friendship Centre Existing Kirklees Visually impaired network Existing Womens Institute Central Huddersfield Existing Polish Elderly group Existing Huddersfield Pakistani Association Friends of Beaumont Park Existing Friendship and Support group for individuals and family with mental health issues KVIN is run by and for visually impaired people. To improve the health and well being of blind and partially sighted people Membership organisation for womens involvement and learning Luncheon group and support group Older people luncheon group Existing Park Support Volunteers Together Existing Asylum support group Kirklees-wide Yes 10-20 90 Group / Forum Contact Existing / New Description Location Protected Characteristics Engagement Officer Best Time To Engage Estimated numbers Agewell Existing Fartown Yes Jeremy and Nisar Existing Birkby Yes Jeremy and Habi April 8th May 2014 April th 7 May 2014 25 Birkby Croft Older peoples support group mixed ethnicity Sikh and South Asian Women support group Jigsaw / Young Adults with Physical Disabilities Hillhouse Gurdwara Existing Employment support for people with disabilities South Kirklees Yes Jeremy 7th may 1.30pm hudds mission 15 Existing Sikh Temple involved in T.B focus group. Interest in health work identified Hillhouse Yes Jeremy and Sarli Women’s Sewing Group – South Asian Women Existing Sewing – Peer support emotional health and wellbeing Birkby Yes Linda Monday a.m April/May 2014 10 One stop shop, Birkby Existing South Asian Women attending one stop shop Birkby Yes Linda Thursday PM April/May 2014 10 Birkby/Paddock Family Forum Existing Birkby/Paddock Yes Linda Wednesday AM April/May 2014 12 Sahaylees Netball Existing Diverse group of parents wishing develop activities for the community Sport Fitness. South Asian Women Birkby Yes Linda Flexible April/May 2014 10 35 25 15 91 Asset Based Approach Planned Activities – Calderdale from 1ST April – May 2014 Group / Forum Contact Existing / New Description Location Forum 50+ Northowram over 50’s Southowram over 50’s WAC Women’s Centre Crisis Pregnancy Care British Muslim Association Integrate Interfaith Council C COM Carers project Existing Existing Network of older people Group meeting Existing St Augustines Centre Existing Pennine Magpie Existing Disability Partnership Existing Disability Support Calderdale Dialogue Groups SWYFT Existing Ver di Gris Engagement Officer Best Time To Engage Estimated numbers Calderdale Town ward Protected Characteristics Age - older Age – older Soo Hanif Asset to decide Tuesday Morning tbc tbc Group meeting Town Ward Age-older Hanif Thursday afternoon tbc Existing Existing Existing Day care centre Drop in centre Drop in centre Central Halifax Calderdale Calderdale Age- older/BME Women/gender Women/gender Sajid Helen Val Asset to decide Asset to decide Asset to decide 50 tbc 10 Existing Day care centre Central Halifax Religion/ethnicity Rahoof Asset to decide 50 Existing Existing Existing Existing Group meeting Network of faith groups Network of mosques Support groups for carers in Calderdale Central drop in facility with community cafe. Day care for young people with a learning/physical disability Network of people with a disability. Support group for people with a disability Monthly meeting for mental health service users and carers. Arts group for older people with Dementia Youth club for young people Todmorden Calderdale Calderdale Calderdale BME Religion – all faiths Religion – muslim faith Carer Nadeem Hanif Sail Wendy 50 100 tbc tbc Calderdale Asylum seekers & refugees Disability – Young people Laura Asset to decide Asset to decide Asset to decide Various support groups in April Cafe Wednesday – 12 noon Asset to decide Calderdale Disability - all Hanif tbc Calderdale Disability - all David 2nd Tuesday evening in May Asset to decide Calderdale Mental Health/carers Aboo Monthly – April/May tbc Calderdale Mental Health/Age Jeff Asset to decide tbc Pye Nest / Sowerby Bridge Young People Rod Asset to decide 50 Calderdale Young People Asad Asset to decide 50 North Halifax Young People Sarah Asset to decide tbc Calderdale Young people Anne Gomersall Asset to decide tbc Calderdale Young People Rahat Asset to decide tbc Calderdale Substance misuse Mary Asset to decide 30 Calderdale Substance misuse Hanif Asset to decide tbc Existing Existing Pavilion in the Park Existing Calderdale Reds Existing St Georges Youth Club CY3P Existing Himmat Existing Project Colt Existing Basement Project Existing Existing Youth club for young people Youth club for young people Engagement project for young people Youth provision for excluded young people Drop in support group for people with substance misuse. Drop in support group for people with substance misuse. Calderdale Jill tbc tbc 60 92 Asset Based Approach Planned Activities – Calderdale from 1ST April – May 2014 Group / Forum Contact Existing / New Description Location Protected Characteristics Geographical representation Geographical representation Geographical representation Geographical representation Geographical representation Engagement Officer Best Time To Engage Estimated numbers NBCC Existing Community Hub Rastrick CC Existing Community Hub North Halifax Ovenden Lower Valley Colin/Roy Asset to decide 50 Jason Asset to decide 50 Halifax Opportunities Trust Boothtown Partnership Mixenden Resource Centre Existing Community Hub Central Halifax Abrar Asset to decide 50 Existing Community Hub Town Vicky Asset to decide tbc Existing Community Hub North Halifax Liz Asset to decide 50 Old Library Cornholme BME Network Existing Cafe and community Hub Upper Valley Hanif Asset to decide tbc Calderdale Geographical representation BME/Geographical Existing Healthy Living Partnership Elland and District Partnership Halifax Central Initiative Advancement of Community Empowerment Existing Network of diverse organisation and groups. Community Hub Rahoof Asset to decide 100 Park Ward BME/Geographical Safdar Asset to decide 30 Existing Community Hub Lower Valley Geographical Jo Asset to decide tbc Existing Community Hub Central Geographical Hanif Asset to decide tbc Existing BME hub Central Geographical BME Riaz Asset to decide 50 Chiraag People Existing BME hub Central Geographical BME/All ages Waseem Asset to decide 50 93 Existing networks – Calderdale and Greater Huddersfield Group / Forum Contact Existing / New Description Location Mechanism Engagement Officer Best Time To Engage Estimated numbers Membership - Locala Existing Locala have a membership database of x amount of people Greater Huddersfield wide Sent out an engagement document to each member via the newsletter Amanda Thomas April 2014 tbc Sent out an engagement document to each member via the newsletter Bronwyn Gill April 2014 tbc Send out the engagement document to each member Sabrina Armstrong April 2014 tbc Send out an electronic engagement document to each member Send out an electronic engagement document to each member Send out an electronic engagement document to be included in the newsletter. Send out an electronic engagement document to be included in the newsletter. Send out an electronic engagement document to be used at focus groups. Tracey Robson April 2014 tbc Emma Tasker April 2014 tbc Dawn Pearson April 2014 700 groups Dawn Pearson April 2014 500 groups Dawn Pearson April 2014 tbc Send out an electronic engagement document to be used at focus groups. Richard Kennedy April 2014 14,000 people Membership - SWYFT Existing SWYFT have a membership database of x amount of people Calderdale wide Greater Huddersfield wide Calderdale wide Membership CHFT Existing CHFT have a membership database of x amount of people Patient Reference Groups - calderdale Existing Patient Reference Groups – Greater Huddersfield Third Sector Networks - Calderdale Existing Most practices have patient reference groups and a central group. Most practices have patient reference groups and a central group. North Bank Forum provide support to over 700 local groups Third Sector Networks – Greater Huddersfield Existing Healthwatch Existing Relationship Matrix Existing Existing Voluntary Action Kirklees and Third Sector Leaders provide support to local VCS groups. Calderdale and Greater Huddersfield both have a Healthwatch Calderdale CCG and Greater Huddersfield CCG have a relationship matrix of 60 groups Greater Huddersfield wide Calderdale wide Calderdale wide Greater Huddersfield wide Calderdale wide Greater Huddersfield wide Greater Huddersfield wide Calderdale wide Greater Huddersfield wide Calderdale wide 94 Stakeholder Activities – clinicians, staff and professionals Event 1. Locality/community model Julie Barlow Bev Walker 2. Specialist hospital sites Julie Barlow Kathryn Aldous Julie O’Riordan (TBC) 3. How will self-care work Julie Barlow Kathryn Aldous Pravin (TBC) 4. Emergency & Urgent Care Rachel and Mark D (TBC) 5. Community Hubs Andrew and Simon Sturdee (TBC) 6. Non-financial appraisal criteria Clare Lead Jim Barwick Jackie Ramsey Anna Basford Catherine Riley Alex Farrell James Drury Anna Basford Catherine Riley Alex Farrell James Drury Alex Farrell Anna Basford Date (All sessions take place 13.30pm) th 11 April 2014 Venue Parent craft room, CRH 15th April 2014 Bankfield meeting room, Dean Clough 17th April 2014 Medium training room, CRH 22nd April 2014 Board Room, Broad Lea House 25th April 2014 Board Room, Broad Lea House 28th April 2014 Large Training Room, CRH 95 Appendix 4: Providers engagement document – SOC summary http://www.rightcaretimeplace.co.uk/wp-content/uploads/2014/08/StrategicOutline-Case-summary.pdf Appendix 5: Providers engagement document – SOC easy read http://www.rightcaretimeplace.co.uk/wp-content/uploads/2014/08/StrategicOutline-Case-summary-easy-read-version.pdf Appendix 6: CCG engagement document – 5 year plans http://www.rightcaretimeplace.co.uk/wp-content/uploads/2014/08/GreaterHuddersfield-Plain-English-5yr-Strategy-.pdf http://www.rightcaretimeplace.co.uk/wp-content/uploads/2014/08/CalderdaleCCG-Plain-English-Strategy-Calderdale.pdf Appendix 7: CCG engagement document – easy read versions http://www.rightcaretimeplace.co.uk/wp-content/uploads/2014/08/GreaterHuddersfield-CCG-Easy-Read-Strategy-Calderdale.pdf http://www.rightcaretimeplace.co.uk/wp-content/uploads/2014/08/CalderdaleCCG-Easy-Read-Strategy-Calderdale.pdf Appendix 8: comments cards 96 Appendix 9: Providers stakeholder engagement - SOC – ENGAGEMENT EVENTS – CHFT / LOCALA Key CHFT Staff Public Key Stakeholders Calderdale and Huddersfield NHS Foundation Trust Calderdale Clinical Commissioning Group Greater Huddersfield Clinical Commissioning Group Event cancelled South West Yorkshire Partnership NHS Foundation Media Interviews Trust Locala Key Date Time Week commencing Monday 3 February (3 – 9 February) 7.2.14 Week commencing Monday 17 February (17-23 February) 20.2.14 Venue Speakers (Clinicians/ Directors/ ADD) Briefing to Linda Riordan, MP Owen Williams Briefing to Membership Councillors Andrew Haigh Owen Williams Nos Attended Date Mtg Reques ted (If known) Key Issues Raised Information exchange Discussion re the Trust’s preferred option ‘2’ We need to demonstrate that topic 2 has wider benefits for a large scale geographic area, eg M62 corridor and changes in mid-Yorks Developments at Todmorden would be welcomed 97 Date Time Venue 21.2.14 Briefing to Craig Whittaker, MP 22.2.14 Written Staff Briefing - CHFT Week commencing Monday 24 February (24 Feb -2 March) 24.2.14 24.2.14 25.2.14 1 pm 6 pm Locala Executive Directors and Senior Management Briefing - electronic Locala staff - electronic Kirklees HWB Calderdale OSC Speakers (Clinicians/ Directors/ ADD) Nos Attended Good communications is key Information exchange Owen Williams/ Barbara Crosse Carol Hirst Catherine Riley Jim Barwick Jim Barwick 1300 Locala staff Anna Basford Barbara Crosse Martin Carter Briefing to Workforce and OD Directorate 25.2.14 Locala Partnership Forum (Unions) 27.2.14 Week commencing Monday 3 March (3-9 March) Kirklees OSC 4.3.14 Calderdale HWB Locala Board 6.3.14 Date Mtg Reques ted (If known) Key Issues Raised Julie Hull Jim Barwick Anna Basford /Owen Williams Robert Flack Jim Barwick 60 staff Presentation/ discussion of SOC Need to clarify what ‘minor injuries’ means Concerns about loss of beds at CRH Staff information exchange Presentation/discussion of SOC 98 Date Time Venue 7.3.14 Briefing to Jason McCartney, MP 7.3.14 Briefing to Barry Sheerman, MP Week commencing Monday 17 March (17-23 March) CHFT Staff Meetings 17/18/19 (x 2 sessions per day - 1 each at HRI and March 2014 CRH) 17.3.14 17.3.14 Face-to-Face Interview – Halifax Courier (Calderdale CCG) Alan Brook, Steve Cleasby, Nigel Taylor Briefing to CHFT Medical Division Consultant Management Forum Speakers (Clinicians/ Directors/ ADD) Nos Attended Owen Williams/Helen Thomson Owen Williams/David Birkenhead Catherine Riley, CHFT Barbara Crosse, CHFT Keith Griffiths, CHFT Martin Debono, CHFT Julie Hull, CHFT 150 staff over 6 events Date Mtg Reques ted (If known) Key Issues Raised Information exchange Information exchange Generally, staff are supportive of our preferred topic; Staff recognise the longer-term benefits of changing the way services are delivered for both patients and staff; Staff want to work with us on the design of new services; Staff recognise that we are one Trust with two hospitals – our patients and staff are already familiar with our two hospitals “Response Time more vital than A & E Department” Saj Azeb 20 staff Concerns over capacity and fit if HRI is unplanned site Generally, positive and a good understanding of the need to change 99 Date Time 19.3.14 10.00am Venue Speakers (Clinicians/ Directors/ ADD) Kirklees Healthwatch Board Meeting Catherine Riley, CHFT Carol McKenna Steve Ollerton (GHCCG) 19.3.14 20.3.14 Locala Members’ Council Lynn Galvin Full-time Officer Royal College of Midwives 20.3.14 Membership Council Development Session Robert Flack Ann-Marie Henderson, CHFT Jason Eddlestone, CHFT Catherine Riley, CHFT Andrew Haigh Ruth Mason 20.3.14 Good Shepherd Church Mytholmroyd “An Introduction to your local FT” Ruth Mason Nos Attended Date Mtg Reques ted (If known) Key Issues Raised Be honest about budget reductions What’s the cost of the PFI at Calderdale If both A & Es close how will we get home once treated How will we address gaps in services, e.g. continence What will happen if the M62 is shut Is losing 100 beds safe Feeling from staff is “here we go again” RCM seeing these changes up and down country We would still be giving women the choice of service model We need to look at the bigger West Yorks pic in terms of provision across the region There is a need to explain the rationale for preferred scenario Priority need to be given to making sure Todmorden is up and running Are you planning redundancies. Have staff been consulted? Concerns about moving A & E, e.g. Heptonstall, and distance to 100 Date Time Venue Speakers (Clinicians/ Directors/ ADD) Nos Attended Date Mtg Reques ted (If known) Key Issues Raised CRH Trust News Article – front page 23.3.14 Week commencing Monday 24 March (24-30 March) Face-to-face Interview – (CHFT) Halifax 25.3.14 Courier (featured on 28 March) Calderdale LMC 26.3.14 27.3.14 Week commencing (31 March – 6 April) 31.3.14 8-9.30 Available in paper and electronic format – 6,000 staff “Trust say changes will lead to better level of care for all” Owen Williams Barbara Crosse (supported by Carol Hirst) Catherine Riley, CHFT Barbara Crosse, CHFT Jim Drury, SWYFT Jim Barwick, Locala 16 Positive about proposals; Anxious about impact on primary care Factor in workforce issues Locala Partnerhsip Forum (Unions) Monday 31 March CHFT – Estates Staff - HRI Lesley Hill, CHFT 20 staff It’s good we’re spending capital in a building we own (if HRI) A & E waiting times will get worse if only one A & E Are our jobs secure? 101 Date Time Venue Speakers (Clinicians/ Directors/ ADD) 31.3.14 Peta Clarke – full-time RCN officer 31.3.14 Chairman’s Information Exchange With Membership Councillors Nos Attended Jason Eddlestone, CHFT Catherine Riley, CHFT Jackie Murphy, CHFT Andrew Haigh Membership Councillors How does this fit in with retendering of Locala services Will skill-mix and staffing ratios change People feel it’s a ‘done deal’ MC’s feedback from discussions at staff sessions Location of individual services not important, but infrastructure is Important to have assurances that funding provided for community services is used for that service Very concerned about the possibility of no A & E in Calderdale Want to see more info re what a Minor Injuries Unit would look like – the conditions/injuries it deals with We want to see more District Nursing staff Will A & E times get worse if there is only 1? Its good that we are spending on a capital building we own (if HRI) Briefing on process so far 1.4. 14 6.45 pm start Calderdale Healthwatch Upper Valley – Ward Forum Hebden Bridge Town Hall Entrance via George Street Entrance from 6.15pm Dawn Pearson, wybscu Lesley Hill, Director of Planning, Performance, Estates & Facilities, CHFT 1.4.14 4-6pm CHFT Staff Meetings – Nursing Lecture Theatre - HRI Jackie Murphy, CHFT Ajay Sharma Barbara Crosse, 1.4.14 ) Date Mtg Reques ted (If known) Key Issues Raised 102 31.3.14 26.3.14 Date Time Venue Dil Ashraf David Hughes Speakers (Clinicians/ Directors/ ADD) ) GPs ) Nos Attended CHFT Catherine Riley, CHFT CHFT Staff Side reps 3.4.14 Catherine Riley (CHFT) Julie Hull (CHFT) Yorkshire Ambulance Service Catherine Riley, CHFT 3.4.14 3.4.14 Calderdale Ward Forum Ripponden Junior and Infant School Halifax Road Ripponden evening Greater Huddersfield GPs Broad Lea House 6.45 pm They agreed our direction of travel How to involve primary care contractors Request for us to speak to LMC People less interested in big strategic plan – but whether they will have a job at the end! It’s a fait a complait /staff side concerned about the connectivity in the community Will our-patients services be on both sites? Moving services into the community is great but we have to ensure we have resources in the community to manage them How will cultural changes be managed – previously clinics held at Todmorden were never that busy, and staff were bored, 3.4.14 Date Mtg Reques ted (If known) Key Issues Raised Not yet confirmed/provisional Event cancelled by CCG - Alex Farrell, SWYFT Anna Basford, CHFT All GPs present supported direction of travel 31.3.14 103 Date Time Venue Speakers (Clinicians/ Directors/ ADD) Nos Attended Jim Barwick, Locala Ashwin Verma, CHFT 4.4.14 8-9.30 CHFT ISS and Leaselend staff CRH Week commencing Monday 7 April (7 – 13 April) CHFT Staff Meetings – Nursing 7.4.14 2pm Lecture Theatre - HRI 7.4.14 4 pm CHFT Staff Meetings – Nursing Parentcraft Room, CRH Lesley Hill, CHFT 40 staff Clare Brearley, CHFT Catherine Riley, CHFT 15 staff Janet Powell, CHFT Catherine Riley, CHFT 23 staff Date Mtg Reques ted (If known) Key Issues Raised Why has old primary care models been dismantled and cut? Concerns about Social Services capacity Strong support for self-care models Examples of poor service in community (poor palliative care) We need more District Nurses What will happen to ISS staff if HRI is the unplanned hospital. Will they transfer? Will senior decision making be 24/7? Does the decision have to be a unanimous vote? Do the CCGs have a preferred option? Who will sit on the consultation panel? What will be the impact on jobs at CRH if HRI is main site? Conscious that more people will choose to call 999 for an ambulance due to distance to travel from Calderdale(when maternity services moved to 104 1.4.14 26.3.14 26.3.14 Date Time Venue Speakers (Clinicians/ Directors/ ADD) Nos Attended Date Mtg Reques ted (If known) Key Issues Raised Halifax there was a worry that more women in labour would call 999) but that has proved not the be the case) What are GPs doing about appts and increased number of A & E attendances because patients can’t get a GP appointment? 7.4.14 8.4.14 6.30 pm 2-7pm Calderdale Heathwatch Lower Valley Bailiff Bridge Community Centre 1 Victoria Road Baliff Bridge West Yorkshire HD6 4DX Drop-In Session Fartown Village Hall Ballroyd Road Penny Woodhead CCCG David Birkenhead CHFT Alan Brook CCCG Anna Basford CHFT Jim Barwick Locala Dawn Pearson wybcsu Alex Farrell, SWYFT Amanda Thomas, Locala Rationale for A & E changes and the scope of minor injuries The importance of provision of additional services out of hospital Receiving the presentation provided a more balanced picture than current media coverage Overall, constructive dialogue which highlighted the importance Healthwatch place on providing care out of hospital and reducing the need for hospital admissions Members commented that they found the presentation very helpful. Praise about the Trust’s eye dept at CRH, and the fact that 105 Date Time Venue Fartown HD2 1AN Membership Council Development Session Written Staff Briefing - CHFT 8.4.14 8.4.14 8.4.14 11pm12am CHFT Discussion – for Night Staff Southside Restaurant, HRI Speakers (Clinicians/ Directors/ ADD) Nos Attended Carol Hirst, CHFT Date Mtg Reques ted (If known) Key Issues Raised many patients already travel from Huddersfield to Halifax and vice-versa Need to clarify what a minor injuries unit will be like Personal experience of a patient requiring neuro surgery travelling to Leeds for in-patient care Catherine Riley Carol Hirst Available as a written briefing and electroni cally for 6,000 staff Owen Williams, CX, CHFT 8 staff Staff understand the rationale behind the proposed changes, but want to know more about how it might work in practice Staff wanted to better understand the thinking behind the Trust’s stated preference The services proposed would need extensive new build on the current HRI site Maintaining the status quo is not an option (a point raised at both 106 Date Time Venue Speakers (Clinicians/ Directors/ ADD) Nos Attended Date Mtg Reques ted (If known) Key Issues Raised HRI and CRH meetings) 9.4.14 12.30 am1.30 am 2-7pm 10.4.14 10.4.14 3pm Clarity around rumours circulating re A & E closure Staff wanted to better understand the current PFI arrangements Staff placed significant emphasis of senior consultant presence, particularly outside daytime hours. Staff questioned finances and savings of £50m and how this might relate to job security. A belief from staff that if the proposed changes in community and close to home do not materialise, the chance of these proposals working would be reduced (a point made at both CRH and HRI meetings) (Nothing to record due to low footfall at session) CHFT Discussion – for Night Staff Ingleton Falls Restaurant, CRH Owen Williams, CX, CHFT 30 staff Drop-In Session New beginnings@ 3ways Nursery Lane Ovenden Halifax HX3 5 SX CHFT – Staff Meeting - Nursing Keith Griffiths, CHFT Debbie Graham, CCCG Tracey Hollis. GHCG 2 Jackie Murphy, CHFT 24 staff 26.3.14 Will the shuttle service improve? 107 Date Time Venue Speakers (Clinicians/ Directors/ ADD) Nos Attended Date Mtg Reques ted (If known) Key Issues Raised Stroke services – would acute care be on one site and rehab on the other? Could we not have one big new build hospital in Elland? Will there be a reduction in bed capacity? 10.4.14 Greater Huddersfield GPs Textile Centre of Excellence Anna Basford, CHFT Jim Barwick, Locala James Drury, SWYFT Barbara Crosse, CHFT 10.4.14 Third Sector/Voluntary Organisations – Greater Huddersfield Anna Basford, Jim Barwick, Alex Farrell 15 Implications of National Policy and Keogh report an recognition that this is the way forward across England The need to understand and factor in changes in in patient flows as a result of changes e.g. possible increased flow to Barnsley The importance of effective and integrated IM and T to enable new ways of working The need for more community beds as a result of changes in hospital bed base The 3rd Sector are/can be the ‘champions of prevention. Need to consider how this is made a reality in the model Self-care model is understood 108 Date Time Venue Speakers (Clinicians/ Directors/ ADD) Nos Attended Date Mtg Reques ted (If known) Key Issues Raised by some, but not all – we need to find ways of describing it better Consider ‘digital inclusion’ so that eole aren’t disadvantaged by digital develoments Statutory partners need to be more inclusive of third sector, with the potential for parterships Locala Board briefing 10.4.14 11.4.14 1-3.30 Stakeholder Event Locality/Community Services Parent Craft Room, CRH Week commencing Monday 14 April (14-20 April 15.4.14 1-3.30 Stakeholder Event Specialist Hospitals Bankfield Meeting Room, Dean Clough discuss planned and unplanned sites 17.4.14 1-3.30 Robert Flack Jim Barwick Helen Frain, Peter Horner, Carol Atkin, Jill Adams, Melanie Giles, Caroline Mullins (Locala) (panel complete) Stakeholder Event Self-Care Medium Training Room CRH to Anna Basford, Catherine Riley, (CHFT) Jackie Ramsay, Peter Horner, Carol Atkin, Jill Adams (Locala) (panel complete) Alex Farrell, James Drury (panel complete) 27 22 Single Info system or shared record essential Single assessment – build on through shared record Is it affordable? Sufficient capacity on unplanned site for all demand Public education in revised health and social care system Ensure proposals fit with a wider West Yorkshire plan Change of culture for staff and patients Not enough sharing of best practice currently 109 Date Time Venue Week commencing Monday 21 April (21-27 April) Rowen Health Federation (GP Federation 22.4.14 in Greater Huddersfield) 22.4.14 1-3.30 24.4.14 25.4.14 10- Speakers (Clinicians/ Directors/ ADD) Barbara Crosse Anna Basford Catherine Riley Stakeholder Event Emergency and Urgent Care Board Room, Broad Lea House Anna Basford, Catherine Riley, CHFT (panel complete) CHFT Staff Meeting - Community Mandy GibbsonsPhelan CHFT, Lesley Hill, CHFT CHFT Staff Meeting – Estates Nos Attended 23 Date Mtg Reques ted (If known) Key Issues Raised Opportunities of provider collaboration across primary and secondary care Support for the strategic direction of travel an scope for providers to offer integrated care Mutual benefits for working together was recognised and agreed as essential to deliver more effective models of care Explore opportunities for provider collaboration re minor injuries/illnesses in OBC Explore opportunities around specific LTCs The possibility of GPs having remote access to SKYPE to access advice of senior physicians Attendees generally supportive of service models described in SOC An opportunity to share views and ideas - 110 Date Time Venue 11.30 1-3.30 Stakeholder Event The Community Hubs Board Room, Broad Lea House Week Commencing Monday 28 April (28 April-4 May) 28.4.14 1-3.30 Stakeholder Event Prioritisation of Criteria Large Training Room, CRH 25.4.14 Speakers (Clinicians/ Directors/ ADD) Alex Farrell, SWYFT Anna Basford, CHFT (panel complete) 30.4.14 Jim Barwick Catherine Riley Jim Barwick Jackie Ramsey Kirstie Scott 30.4.14 Calderdale LMC Barbara Crosse Mags Barnaby Date Mtg Reques ted (If known) Key Issues Raised General support for service models described in SOC Alex Farrell, James Drury (panel complete) Locala Executive Directors Meeting with Social Care Provider Staff Huddersfield 28.4.14 Nos Attended 19 Public education/marketing “where we go for? Needed Recognise ‘home’ as the default – ensure hubs don’t absorb community resources Need social care presence, access and phone numbers Ambulance access required at all levels in building * A detailed report of 6 Stakeholders Events has been produced 8 social care represe ntatives 7-Day provision of Social Services is implicit in new Care Bill and Urgent Care Agenda All agreed it is a shared direction of travel Concerns from Council we are focussed on adult services OBC Briefing – well received Need to clarify Trust and CCG boundaries re proposed visits to practices 111 Date Time Venue Speakers (Clinicians/ Directors/ ADD) 30.4.14 Locala Members’ Newsletter - update Amanda Thomas (Locala) 30.4.14 Locala Integrated Children’s Service Team Leaders briefing CHFT Staff Meeting Intermediate Care and Community Directorate Jim Barwick 1.5.14 CR Nos Attended 1500 Membe rs 20 staff Week commencing Monday 5 May (5 May-11 May) (Bank Holiday 5th May) Meeting with Leader/CX of Calderdale 8.5.14 Council Written Staff Briefing - CHFT 8.5.14 9.5.14 Halifax Courier - Owen Williams Andrew Haigh Carol Hirst Catherine Riley Date Mtg Reques ted (If known) Key Issues Raised Community resources governed and managed by us, but not owned by us GPs in Calderdale were engaged in the process Learn from Locala example. Staff want to come back into Hospital setting as they feel isolated Significant Consultant presence in the Community needed to show investment of the current model Information Exchange Available as a written briefing and electronic ally for 6,000 staff Article following Calderdale H 112 Date Time Venue Speakers (Clinicians/ Directors/ ADD) “Bust up at A & E” – Halifax Courier – 9.5.14 “Message is Clear – Hands Off our A & E” Week commencing Monday 12 May (12 May-18 May) 13.5.14 14.5.14 14.5.14 14.5.14 15.5.14 Locala Health Visitor Team Leaders Briefing Community Pharmacy West Yorkshire Staff Jim Barwick Workshop to understand the Clinical Voice – Dean Clough Locala Members’ Council briefing Meeting with Calderdale Healthwatch Jackie Murphy Karen Taylor (SWYMHT) Jim Barwick OOwen Williams Anna Basford Catherine Riley Catherine Riley James Drury John Yorke Bash Fazlee Nos Attended Date Mtg Reques ted (If known) Key Issues Raised & WB Board Meeting on 8.5.14 Article following march through Halifax Town Centre 20 community pharmacy staff Role of Community Pharmacy in helping to build confidence in selfcare and prevention Push boundaries on dealing with complex patients Pharmacy could be developed into an intermediate service People accept the views outlined in the SOC when it is explained The SOC doc isn’t easy to find, easy to read, or easy to follow Perception that the 113 Date Time Venue Speakers (Clinicians/ Directors/ ADD) Nos Attended Date Mtg Reques ted (If known) Key Issues Raised Acre Mill development means that the decision has already been made Specific questions raised at the meeting and responses – see central SOC file (date to be confirmed) Meeting with Kirklees Healthwatch 16.5.14 Briefing to Linda Riordan, MP 16.5.14 Briefing to Craig Whittaker,MP 16.5.14 Briefing to Jason McCartney, MP 16.5.14 Briefing to Barry Sheerman, MP -- Update/Information Exchange Update/Information Exchange Update/Information Exchange Update/Information Exchange Owen Williams James Drury Owen Williams James Drury Owen Williams Barbara Crosse Owen Williams Barbara Crosse Week commencing Monday 19 May (19 May-25 May) CHFT Staff – Estates 20.5.14 2.30 Lecture Theatre, HRI Face-to-face interview (CHFT) with Nick 22.5.14 Lavigueur, Huddersfield Examiner (Featured on 26th and 27th May 2014) Face-to-Face Interview (Matt Walsh 23.5.14 CCCG) Lesley Hill Barbara Crosse (supported by Caroline Wright) Interview with Matt Walsh – Supported by Rosemary Cook 40 New Twist : Threat to both A & E Units – but health plan will lead to better care Health Chief joins call to save NHS 114 Date Time Venue Locala Exec Directors and Senior Management Team Briefing Week commencing 26 May (26 May-1 June) 5.30 Voluntary Action Calderdale 27.5.14 pm Calderdale Disability Centre Kings Centre Park Road Halifax 23.5.14 Speakers (Clinicians/ Directors/ ADD) Nos Attended Jim Barwick Jim Barwick (Locala) James Drury (SWYFT) Janet Powell (CHFT) 20 27.5.14 27.5.14 27.5.14 28.5.14 28.5.14 10-12 2-7 pm Date Mtg Reques ted (If known) Key Issues Raised Locala OBC Action Team Lync debrief/update Locala Health Visitor Team Leader Briefing Locala District Nursing/Community Matrons Intermediate Care – South Operational Meeting Voluntary Action Calderdale Resource Centre Hall Street (on corner of Lister Lane) Halifax HX1 5AY All/Jim Barwick Anna Basford Allan Hart-Thomas Clare Brearley 17 Drop-In Session YMCA Salendine Nook Steve Ollerton David Birkenhead Carol Hirst Janet Powell James Drury 20 (approx.) Attendees generally supported the proposals in the SOC document Discussion about a “super ambulance/ mobile hospital” Consider wheelchair/guide dog access to ambulances Jim Barwick Caroline Mullins individuals representing 17 groups High quality care is key Transport issues Strong emphasis to Improve communications across voluntary sector and hospital boundaries Concerns expressed by one gentleman re how/where drop-in sessions had been advertised/timing and location of meetings 115 Date Time 29.5.14 29.5.14 30.5.14 28.5.14 2-7pm Venue Speakers (Clinicians/ Directors/ ADD) Locala District Nursing North Operational Mtg Locala Partnership Forum (Unions) Drop In Session Slaithwaite Village Hall Slaithwaite Huddersfield Caroline Mullins Calderdale LMC Rob Aitchison Jim Barwick Barbara Crosse Jackie Murphy Nos Attended Date Mtg Reques ted (If known) Key Issues Raised Praise re food provided by CHFT Concerns by a number of people following “New Twist” headline by the Huddersfield Examiner The majority of people supportive of the need to change how some services are to be delivered Some concern whether community services can support the proposals (Locala) TBC Implications of YAS issues – and the fact that they are downgrading some services Most people only recognise CHT as a provider and A & E seems to be the biggest concern More information/ communications needed – on GP screens and door knocking LMC value being kept informed and involved in the 116 Date Time Venue Speakers (Clinicians/ Directors/ ADD) Nos Attended Date Mtg Reques ted (If known) Key Issues Raised process Week commencing 2 June (2-6 June) Meeting with Leader/CX of Kirklees 2.6.14 Council 2-7pm Drop-in Session 2.6.14 Mytholmroyd Community Centre 3.6.14 7-8pm GP Federation PHH (Huddersfield) Broad Lea House Owen Williams Andrew Haigh Juliet Cosgrove (2-7) Clare Brearley (24) Julie O’Riordan (3.30 – 6pm) Ashwin Verma Julie O’Riordan Martin Debono David Birkenhead Catherine Riley Anna Basford Mark Davies Jim Barwick 25 30 GPs Update/ Information Exchange Visiting patients at HRI will be difficult and costly This is politically motivated with no real evidence base behind it Concerns at the prospect of closing A & E and “running down” the Calderdale site A plea for wider/improved communications (events and developments/issues) Support for improving community services – but this needs to be in place before making changes to the hospitals Agreed the system would benefit from some re-design Pressures in both primary and secondary care Keen to bring primary and secondary care clinicians together to have conversations How do we convince 117 Date Time Venue Speakers (Clinicians/ Directors/ ADD) Nos Attended 3.6.14 2-7pm Drop-in-session Fartown Village Hall Catherine Riley (2-4pm) Heather McClelland (2-4 pm) Juliette Cosgrove (4-7pm) Janet Powell (5.30-7pm) TBC Date Mtg Reques ted (If known) Key Issues Raised decision makers of the clinical evidence base? Could PHH become a 4th partner in the process? Some cynicism about proposed changes Some support of proposed changes and offer of involvement Don’t want A & E to go to Leeds Emma Gothard and Melanie Giles (LOCALA) 4.6.14 2-7 pm Drop-in Session Brighouse Civic Hall Brighouse Emma Livesley (2-7) Colin Welsh (3pm) Barbara Schofield (4-7 pm) TBC Travel issues for people travelling from remote areas of Calderdale to HRI without a car Need to explain more about Minor Injuries Unit in community locations Other ‘not SOC related’ issues – Parking/disability access at CRH Issues raised/ addressed within division by EL 118 Date 5.6.14 Time 2-7 pm Venue Drop-in session The Hub Kirkburton Speakers (Clinicians/ Directors/ ADD) Catherine Riley (2-5) Lesley Hill (2-6) Carol Hirst (5-7) Nos Attended TBC Jim Barwick Carol Atkin and Kirsty Shepherd (LOCALA) 5.6.14 8.6.14 Locala Board Briefing Written Staff Briefing - CHFT Week commencing 9 June (9-15 June) 2-7pm Drop-in session 9.6.14 Hanson Lane Enterprise Jim Barwick Catherine Riley Caroline Wright Rob Aitchison (27pm) Catherine Riley (2-3.30pm) Colin Welsh (27pm) Date Mtg Reques ted (If known) Key Issues Raised Transport Concerns, particularly for elderly Practice based anticoagulation is very good. High praise re services provided from Kirkburton Health Centre. Agree with topics in principle, but not sure care in the community is feasible due to lack of money and staff “Very informative day” – awoken my thought processes Available as a written briefing and electronically for 6,000 staff Public feel we need to get the message across – they want to understand the evidence base Some worried about emergency care Travel concerns, especially the elderly 119 Date Time Venue Speakers (Clinicians/ Directors/ ADD) Nos Attended Date Mtg Reques ted (If known) Key Issues Raised People keen to understand proposal in more detail and engage in a constructive way We need to explain where plans like ours have worked and benefitted the public, eg Torbay Public sceptical about planned improvements to community services 9.6.14 10.30am 9.6.14 10.6.14 2-7pm DATS Staff Engagement session Discussion Room 1, HRI Intermediate Care Team St John’s, Halifax Drop-in session New Beginnings (Halifax) 26 staff Catherine Riley Mandy Gibbons Phelan 30 staff Catherine Riley (2-5pm) Lindsay Rudge TBC (2-5pm) David Birkenhead (4.30-7pm) Lesley Hill (4- TBC Have you factored Dewsbury A&E demand? Following the presentation, staff feel excited about the future and about the Trust as a whole Staff feel able to discuss the proposals with their patients, families, relatives “It all makes sense really” Don’t close our A & E! – strong feelings/passion from 3 people “If” we go ahead the MI Unit should have the ability to stabilise critically ill pts 120 Date Time Venue Speakers (Clinicians/ Directors/ ADD) Nos Attended 7pm) Melanie Giles (Locala) Jim Barwick (Locala) 10.6.14 10.6.14 11.6.14 11.6.14 2-7pm 12.6.14 2-7pm Locala OBC Action Team Lync debrief/update Locala Health Visitors Team Leaders Children’s Business Unit Professional Forum Briefing Drop-in session Holmfirth Civic Hall All/Jim Barwick Drop-in session Todmorden Health Centre Rob Aitchison (27) Vicky Pickles (2- Emma Gothard Richard Palfreeman Jan Giles David Hughes, GP Janet Youd (2-5) David Birkenhead (2.30-7) Date Mtg Reques ted (If known) Key Issues Raised prior to transfer Event poorly attended – but no suggestions as to how this could be improved Poor experience of end of life care (hospital) (15 years ago and 3 years ago) More/improved community support needed TBC ?80 (tbc) Generally supportive of proposals Some concerns about A&E topics Transport concerns – particularly for elderly visitors Support for specialist paediatrics Support for a MI Unit at HVMH Concerns re ambulance response times Events not well advertised. Need to get the clinical 121 Date Time Venue Speakers (Clinicians/ Directors/ ADD) Nos Attended 6) Lesley Hill (3.305.30) Sal Uka (3.30 pm) Janet Powell (3.30-7) 12.6.14 8pm Meeting for the Deaf Community Locala Transformation Team - briefing DATS Staff Engagement Session Medium Training Room, CRH Week commencing 16 June (16-22 June) Locala Quality/Governance Team 16.6.14 Meeting District Nurse/Team Leader Cabinet 18.6.14 12.6.14 13.6.14 19.6.14 11am 20.6.14 12 – 1pm DATS Staff Engagement Session Board Room, HRI Local Care Direct Bradley, Huddersfield benefits across to the public with case studies, eg the role of paramedics in assessing where a patient should be treated Improve pharmacy access out of hours in Todmorden People interested in having a community hub at Todmorden, and having a say in future developments - Community Health Workers (on behalf of the CCGs/WSYCSU) Jackie Ramsay 11.00am Date Mtg Reques ted (If known) Key Issues Raised 20 Jim Barwick Carol Atkin Kirsty Shepherd 18 Catherine Riley Jim Barwick LCD want to be part of our conversations – frustrated 122 Date Time Venue Speakers (Clinicians/ Directors/ ADD) Nos Attended Week commencing 23 June (23-29 June) 26 June 11am DATS Staff Engagement Session Week commencing 30 June (30 June-6 July) Waterhouse McIntosh Homes 2.7.14 Halifax Contact: George Pickles 01422 831878 Date Mtg Reques ted (If known) Key Issues Raised that they weren’t involved earlier in the engagement process. Further session to be arranged for clinical teams 10 staff Clare Brearley Catherine Riley The group provides warden supported homes They are strongly supportive of locality model, and feel they could work better with NHS, on admission and discharge planning Communications could be better managed The group are keen to become more involved in engagement/service model planning /CH/Y: ENGAGEMENT EVENTS – 21 JULY 2014 123 Appendix 10: Letter from Barry Sheerman Barry Sheerman MP, sent in a letter and a petition containing over 1,000 signatures opposing plans to the closure of the A and E department in either Calderdale or Huddersfield (see appendix - ?). The petition also came with 141 public comments relating to A and E services. The comments covered the following key themes: Keep A and E services in both Calderdale and Huddersfield, both local areas are large enough to require their own services. One A and E service will become overcrowded, services are already overcrowded. Travel and transport for people particularly in rural areas will not be possible because of the cost, time to travel and parking, if they have their own transport, will not be sufficient to cope with demand. The Elland by pass is gridlocked and will cause problems for emergency vehicles. Ambulance response times were a concern, including the time it would take to reach the hospital destination. There were a number of concerns that lives would be lost. Services were being cut as part of a cost cutting exercise. Current services were valued and there were lots of examples to support this. Local people want easy access to local facilities and there were a number of comments that services may go to Leeds. People want a say on what happens to ‘their’ services. Services work perfectly well as they are and people do not want them to change. 124 Appendix 11: Equality monitoring of respondents on SOC 1091 completed whole or part, of whom; Sex Women 590 Men 478 Prefer not to say/blank 23 Under 18 36 129 26-45 414 46-65 334 66-80 117 81-100 28 100+ 1 Blank 32 Afghanistan 3 Austria 1 Bangladesh 6 Britain 28 Canada 1 China 2 Czech Republic 3 D R Congo 1 England 411 Germany 3 Hong Kong 2 India 4 4 Iran 6 Iraq 7 Ireland 6 Israel 1 Kuwait 1 Northern Ireland 2 Pakistan 126 Poland 1 Romania 1 Scotland 5 Singapore 1 Slovakia 1 South Africa 2 Turkey 1 UK 270 Yemen 1 Vietnam 2 Wales 5 Zaire 1 Zimbabwe 1 Blank 167 Age 18-25 Country of birth 125 Ethnic group Arab 8 Chinese 2 Indian 3 Pakistani 360 African 5 Caribbean 3 Mixed white and Asian 13 0 Mixed white and black Caribbean 1 White British 614 White Gypsy 3 White Irish 9 Other mixed 2 Prefer not to say/blank 30 Other white 7 Other Asian 20 Other 10 Polish 1 Bangladeshi 2 Vietnam 2 Bengali 1 D.R.Congo 1 Vietnam 2 Iraqi 2 Afghan 3 Bangladesh 3 Bengali 1 Jewish 1 Mixed white and black African Disability No 778 Yes 261 Prefer not to say/blank 28 Hearing 19 18 Physical or mobility 44 Long standing illness 110 Mental health 75 Learning Disability 29 Prefer not to say 22 Other 11 MS 1 Diabetes 1 Stroke - COPD 1 Over active thyroid 1 Addiction 2 Stroke - Slight mobility problem 1 Type of impairment Visual 126 Addict on recovery 1 Parkinson's 1 Epilepsy 1 Spinal stenosis 1 Sexual orientation Bisexual 8 Gay Man 5 Heterosexual 888 Lesbian 9 Prefer not to say/blank 93 Other 2 Past it 1 Widow 1 Religion and belief No religion 317 Yes 676 Prefer not to say/blank 46 Buddhism 9 Christianity 276 Islam 397 Hinduism 1 Judaism 1 Other 16 Roman Catholic 8 If yes, which religion? Non declared 1 Sunni Muslim 1 Atheist 1 Rastafarian 1 Agnostic 1 Church of England 1 Other 1 Gender reassignment Transgender 2 Pregnant/Had a baby within the last 6 months Yes 26 Are you a carer? Yes 114 Open minded (awaiting 1 proof) 127 Appendix 12: Cornholme and Portsmouth Old library focus Group 128 129 130 131 Appendix 13: Equality monitoring on Commissioners 5 year strategy leaflet 127 completed whole or part, of whom; Sex Women 83 Men 36 Prefer not to say/blank 6 Under 18 12 18-25 18 26-45 40 46-65 40 66-80 9 Blank 8 England 34 Iraq 1 Kenya 1 New Zealand 1 Nigeria 2 Pakistan 8 Poland 5 Scotland 1 Somalia 1 UK 45 Unknown/blank 23 Age Country of birth Ethnic group Asian/Asian British Pakistani 25 White Black and Black British Mixed African 3 White and Asian 1 Other 1 White and Black African 1 Other White British – Scottish/Welsh/NI/England 53 Arab 1 White other 6 Prefer not to say/blank 34 132 Disability No 94 Yes 27 Prefer not to say/blank 8 Hearing 2 Visual 1 Physical or mobility 5 Long standing illness 7 Mental health 10 Other 0 Autism spectrum 0 Heterosexual 10 7 Type of impairment Sexual orientation Bisexual 1 Gay Man 5 Lesbian 4 Prefer not to say/blank 13 34 Yes 65 Prefer not to say/blank 26 1 Christianity 32 Islam 30 Gender reassignment Transgender 0 Pregnant/Had a baby within the last 6 months Yes 1 Are you a carer? Yes 23 Religion and belief No religion If yes, which religion? Buddhism 133

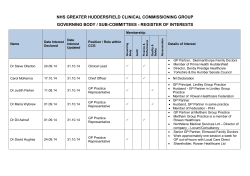







© Copyright 2026