
Homelessness and its Effects on Children FAMILY
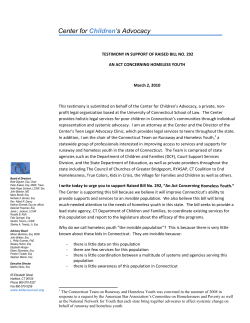
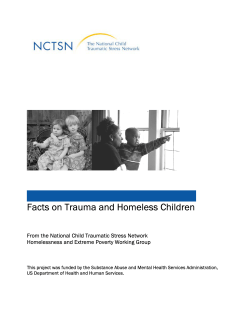
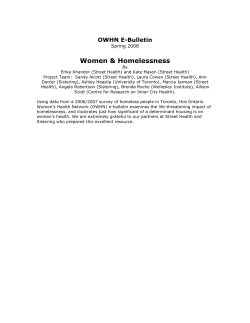
Homelessness and its Effects on Children FAMILY HOUSING FUND A Report Prepared for the Family Housing Fund December 1999 By Ellen Hart-Shegos Hart-Shegos and Associates, Inc. Editor: Anne Ray Table of Contents 1. Executive Summary — Homelessness and its Effects on Children …………………………………2 2. Homelessness and its Effects on Early Childhood Development ……………………………4 3. Homelessness and its Effects on School Age Children ………………………………………6 4. The Effects of Homelessness can be Minimized — Maybe Even Reversed ………………………10 5. Endnotes ……………………………………………………12 1 Executive Summary 1 Homeless children are not simply at risk; most suffer Homelessness influences every facet of a child’s life — from conception to young adulthood. The experience of homelessness inhibits the physical, emotional, cognitive, social, and behavioral development of children. specific physical, psychological, and Homelessness and its emotional damage. Effects on Early Childhood Development Before Birth Young children who are homeless are often separated from their parents, which can cause long-term negative effects. Homeless preschool age children also are more likely to experience major developmental delays and to suffer from emotional problems. Despite these developmental delays and emotional difficulties, homeless preschoolers receive fewer services than other children their age. Homelessness and its Effects on School Age Children The impact of homelessness begins well before a child is born. The overwhelming majority of homeless parents are single women, many of whom were homeless themselves as children. Homeless women face many obstacles to healthy pregnancies, such as chemical abuse, chronic and acute health problems, and lack of prenatal care. By the time homeless children reach school age, their homelessness affects their social, physical, and academic lives. Homeless children are not simply at risk; most suffer specific physical, psychological, and emotional damage due to the circumstances that accompany episodes of homelessness. Infants Physical Health Children born into homelessness are more likely to have low birth weights and are at greater risk of death. Homelessness also exposes infants to environmental factors that can endanger their health. Because homeless families often have little access to health care, many homeless infants lack essential immunizations. In general, homeless children consistently exhibit more health problems than housed poor children. Environmental factors contribute to homeless children’s poor health, and homeless children are at high risk for infectious disease. Homeless children are at greater risk for asthma and lead poisoning, often with more severe symptoms than housed children. Poor nutrition also contributes to homeless children’s poor health, causing increased rates of stunted growth and anemia. Despite these widespread health problems, homeless children generally lack access to consistent health care, and this lack of care can increase severity of illness. Toddlers Homeless children begin to demonstrate significant developmental delays after 18 months of age, which are believed to influence later behavioral and emotional problems. 2 Preschoolers Emotional and Behavioral Development: Homeless children are confronted with stressful and traumatic events that they often are too young to understand, leading to severe emotional distress. Homeless children experience stress through constant changes, which accumulate with time. These stressful changes result in a higher incidence of mental disorders, which become manifested in homeless children’s behavior. Despite significantly more incidences of mental illness, less than one-third of these children receive professional help. Academic Development: Homeless children’s academic performance is hampered both by their poor cognitive development and by the circumstances of their homelessness, such as constant mobility. Homeless children are more likely to score poorly on math, reading, spelling, and vocabulary tests and are more likely to be held back a year in school. As with physical and mental health care, homeless children’s greater needs do not lead to greater access to special services. The Effects of Homelessness With early and can be Minimized — Maybe consistent Even Reversed intervention, While research on homeless children paints an overwhelmingly bleak picture of their current and future status, there is hope that with early and consistent intervention strategies, children can learn to overcome many of the detrimental effects of their poverty and homeless experiences. One set of strategies is to ensure priority access for homeless families for services that can mitigate the effects of homelessness, such as supportive housing, drug and alcohol treatment, parenting support, afterschool programs, and nutritional support. A second set of strategies can be employed by emergency and supportive housing providers to assist their residents, including obtaining health screenings and prenatal care for women, assisting families in obtaining health and nutrition information, assessing and monitoring children’s development, and assisting children and parents in participating in school activities. children can overcome many of the effects of poverty and homelessness. These interventions give young children who have experienced the traumatic effects of homelessness the chance to build the resiliency and competence they need to break the detrimental cycle of homelessness. 3 Homelessness and Its Effects on 2 Early Childhood Development The impact of homelessness begins well before a child is born. Homelessness influences every facet of a child’s life — from conception to young adulthood. A review of a well-established body of research on childhood homelessness reveals a profound and accumulative negative effect on the development of children, leading many to repeat the cycle of homelessness as adults. Homelessness inhibits the physical, emotional, cognitive, social, and behavioral development of children. Before Birth The impact of homelessness begins well before a child is born. Homeless parents generally have had difficult starts in life. The overwhelming majority of homeless parents are single female heads of households, many of whom were homeless themselves as children and had lived in emergency shelters.1 Many of these parents were displaced as children from their families of origin, with nearly a quarter having lived in foster care.2 Today’s homeless parent is likely to be a young woman in her twenties who gave birth to her first child in her teens. She is likely to have never been married, have had multiple pregnancies resulting in at least two children under the age of six, have had an incomplete education, and have never been employed. Many homeless parents have experienced physical and sexual abuse, constant crisis, family and community violence, isolation, and the cumulative stress of persistent poverty. Nearly a third of all homeless women have been diagnosed and hospitalized for mental illnesses, such as depression. Despite these difficult circumstances, however, pregnancy rates among homeless women are high. Nationally, 35 percent of women coming into shelters are pregnant versus 6 percent of the general population, and 26 percent have given birth within a year of seeking shelter. 4 Homeless women face many obstacles to healthy pregnancies. First, many homeless women abuse alcohol or chemicals. Service providers report a 40 percent substance use rate among women in their programs, with approximately one-fifth of homeless women disclosing drug and alcohol abuse during pregnancy. There is overwhelming evidence that chemical abuse harms prenatal development and later cognitive and behavioral development of children. Second, homeless women tend to suffer from chronic and acute health problems that can affect the prenatal development of their children.3 Finally, homeless women are less likely to seek prenatal care. Fifty percent of homeless women versus 15 percent of the general population had not had a prenatal visit in the first trimester of pregnancy. Forty-eight percent of homeless women had not received medical assessment of their pregnancy before being admitted to the shelter. Infancy Children born into homelessness are more likely to have low birth weights. A child with a low birth weight and whose mother did not receive prenatal care is nine times more likely to die in the first 12 months of life. These risks are multiplied if the mother also abused drugs and/or alcohol.4 Homelessness also exposes infants to environmental factors that can endanger their health. Homeless women with infants often are forced to return to a shelter or an overcrowded home of a family member or friend after the birth. Overcrowded conditions expose babies to disease and illness, maternal stress, lack of sanitation, lack of refrigeration and sterilization for formula, and lack of a routine. The difficult surroundings often affects the mother’s feelings of adequacy and can interfere with critical maternal-child bonding.5 (ages 18 months to 3 years) Homeless pre-school age children are likely to demonstrate developmental delays. Most homeless children (75 percent) under age five have at least one major developmental delay or deviation, primarily in the areas of impulsivity or speech.8 Even more alarming, nearly half of homeless children (44 percent) have two or more major developmental delays. More than half of all homeless preschoolers tested were at or below the first percentile for their age in receptive verbal functioning. Nearly one-third of homeless preschoolers functioned only at the fifth percentile for age in visual-motor ability, and 38 percent exhibited emotional and behavioral problems.9 The more subtle developmental delays in homeless children begin to reveal themselves after 18 months of age. Then, as toddlers, homeless children often begin to demonstrate their reactions to stress. They may become markedly insecure, tearful, distrusting, and irritable, and they may regress in speech and toilet training. From this point on, homeless children begin to demonstrate significant developmental delays. These developmental delays are believed to influence later behavioral and emotional problems.6 Young children who are homeless often suffer from emotional problems. In general, homeless children cry more easily, react more intensely when upset, tend to overreact to small trials, and are easily distressed. One in five homeless children ages three to six years demonstrate extreme emotional distress warranting professional intervention. Twelve percent have clinically diagnosed problems with anxiety, depression and withdrawal, and 16 percent have behavior problems demonstrated by severe aggression and hostility. Finally, homeless families often have little access to health care. Research indicates that at least one-third of all homeless infants lack essential immunizations. Toddlers Preschoolers (ages 3 - 6) Young children who are homeless are often separated from their parents. As noted earlier, many homeless mothers have experienced foster care placement as children. Most homeless mothers (70 percent) who were in foster care as children will have at least on of their children placed in foster care. When children are separated from their mothers, particularly during the critical first five formative years, they are likely to suffer longterm negative effects. Foster care is so destabilizing for some children that its effects last well into adulthood.7 Homeless preschool age children are likely to demonstrate developmental delays. Despite these developmental delays and emotional difficulties, homeless preschoolers receive fewer services than other children their age. For example, significantly fewer homeless children of preschool age are enrolled in early childhood programs that could greatly aid them in their transition to school.10 5 Homelessness and its Effects on 3 School Age Children In general, homeless children consistently exhibit more health problems even than poor children who have housing. Illness Each Month Extended Care Post-birth Chronic Problems Infectious Diseases Respiratory Infections Hospitalized Asthma Stunted Growth Anemia 1x 2x 3x 4x 5x 6x Homeless children are many times more likely to experience By the time homeless children reach school age, their homelessness affects their social, physical, and academic lives. In each of the major areas surveyed—physical health, development, and academic performance— studies reveal that homeless children are not simply at risk; most suffer specific physical, psychological, and emotional damage due to the circumstances that accompany episodes of homelessness. health problems. Physical Health Homeless children face multiple, profound risks to their health.11 In general, homeless children consistently exhibit more health problems even than poor children who have housing.12 Half of homeless children experience two or more illnesses per month. 6 Homeless children are more likely to experience chronic health problems than are housed children. They are four times more likely to need extended health care immediately post-birth. Sixteen percent of older homeless children, versus nine percent of housed children, have one or more chronic health problems, such as cardiac disease, peripheral vascular disease, endocrine dysfunction, or neurological disorders.13 Homeless children also are at high risk of infectious disease. As compared with housed children, homeless children suffer from five times the rate of diarrheal infections as housed children; this is a serious, potentially fatal illness.14 Homeless children suffer from many respiratory infections at twice the rate of housed children, and they are twice as likely to have a positive skin test showing exposure to tuberculosis. Homeless children are confronted with stressful and traumatic events that they often are too young to understand, and this leads to severe emotional distress. Homeless children worry about where they will sleep on a given night, and if they have a place to sleep, they are afraid of losing it. Older children worry about being separated from friends and pets, and they fear that they will be seen as different among new peers at school. They also worry about their families: their parents, whose stress and tension is often shared with the children, and their siblings, for whom they see themselves as primary care givers. More than half of homeless children surveyed also said that they worried about their physical safety, especially with regard to violence, guns, and being injured in a fire. One-quarter of homeless children have witnessed violence in the family. homeless children between the ages of 6 and 17 have very high rates of mental disorders compared to their peers. 50% 40% 30% 20% 10% Homeless children Development stressful events, Other children Despite these widespread health problems, homeless children generally lack access to consistent health care, and this lack of care can increase severity of illness. Most other children in the United States receive routine medical care in a doctor’s office, visit a dentist regularly, and are covered by private health insurance. Homeless children are far more likely to receive poor preventative care and excessive emergency treatment. While approximately half of homeless families surveyed said they had received care from a community clinic, 60 percent stated they had visited the emergency room of a hospital at least once within the past 12 months, and 37 Emotional and Behavioral As a result of Homeless children Poor nutrition also contributes to homeless children’s poor health. Homeless children are six times more likely than other children to have stunted growth16 and seven times more likely to experience iron deficiencies leading to anemia.17 When found to be anemic, homeless children’s iron deficiency is 50 percent worse than anemia among housed poor children. two or more times in the past year. More than 10 percent surveyed stated that they or their child had been hospitalized in the past year. Moreover, nearly a third of homeless children have never visited a dentist.18 Other children Environmental factors also contribute to homeless children’s poor health. Asthma is common among homeless children and children living in poor quality housing. Indoor environmental conditions that aggravate asthma include cockroach infestations, molds, smoke, and overcrowding. When homeless children with asthma get sick with other ailments, their symptoms generally are more pronounced than those in housed children, and they are hospitalized for symptoms at three times the rate of the average asthma patient. Homeless children also are more apt to test positive for lead poisoning, with more severe symptoms. The symptoms of lead poisoning can include abdominal pain, constipation, fatigue, anemia, nerve damage, and altered brain functions. Lead poisoning’s effect on the brain can cause seizures, coma and even death in severe cases, and long term exposure can lead to kidney, brain, and reproductive organ damage.15 0% Homeless children also experience stress through constant change, and these stressful changes accumulate as these children grow older. The average homeless child moves as many as three times in a year. Homeless children are seven times more likely than other children to be placed in foster care. Twentytwo percent of homeless children experience foster care or living with relatives, compared with three percent of housed children. The likelihood of foster care placement increases with the child’s age: nine percent for infants and toddlers, 19 percent for three to six year olds, and 34 percent among school-agers.19 Anxiety Depression Aggressive Behavior Percentage of homeless children with emotional problems compared with other school age children. 7 Homeless children are four times more likely than other children to score at or below the tenth percentile in vocabulary and reading. Test Scores Reading Spelling Math 0 10% 20% 30% 40% 50% 60% 70% 80% Percentage of homeless children performing below grade level 8 As a result of these stressful events, homeless children between the ages of six and 17 have very high rates of mental disorders compared to their peers. One-third of homeless children have at least one major mental disorder that interferes with daily activity. Almost half (47 percent) have problems with anxiety, depression, or withdrawal, compared to 18 percent of other school age children. Thirty-six percent demonstrate delinquent or aggressive behavior, compared with 17 percent of other school age children.20 The stress of homelessness in children can lead to insecure attachments to others, poor self-esteem, and dysfunctional personality development. These conditions manifest themselves in the behavior of homeless children. Often, boys exhibit aggression, while girls exhibit depression and passive or withdrawn behavior. Most often, homeless children exhibit lethargy, extreme indifference at school, and overt anger with their parents. Despite significantly more incidents of mental illness, less than one-third of these children actually receive professional help.21 In fact, as the severity of the mental illness increases, homeless children are less likely to receive adequate health care. Academic and Cognitive Development Homeless children’s academic performance is hampered both by their poor cognitive development and by the circumstances of their homelessness. First, homeless children experience developmental delays that hamper academic success at four times the rate of other children.22 They suffer from emotional and behavior problems that affect learning at almost three times the rate of housed children. Homeless children experience twice the incidence of learning disabilities, such as speech delays and dyslexia, as other children. These developmental delays have multiple causes. All poor children are at higher risk for delayed cognitive development due to higher rates of perinatal complications, reduced access to resources that buffer the effects of these complications, increased exposure to lead, and less home-based cognitive stimulation.23 Homeless children are also subjected to the detrimental affects of pronounced and prolonged stress. These factors, often combined with lower teacher expectations, poor school readiness skills, and harsh and inconsistent parenting, conspire to negatively affect homeless children’s cognitive and intellectual development. Second, the circumstances of homelessness make it even more difficult for homeless children to perform well in school. In particular, constant mobility harms the academic progress of homeless children. Forty-one percent of homeless children attend two different schools in one year, and 28 percent of homeless children attend three or more schools. Frequent mobility leads both to poor performance, which is evident in lower math and reading test scores, and increased behavioral and emotional problems, such as peer disturbances, anxiety or depression, lower ratings of psychosocial development, difficulties in developing and maintaining peer relationships, and absenteeism and truancy. Negative impact on achievement due to mobility seems to be higher among children in elementary school. However, this may be because many homeless youth drop out of high school. Another circumstance of homelessness that compromises children’s ability to perform in school is poor physical health; in addition to the environmental effects of poverty and homelessness, these children must juggle academic expectations when they are not feeling well. These cognitive delays and circumstances have a clear, negative effect on homeless children’s school performance. Homeless children are four times more likely than other children to score at or below the tenth percentile in receptive vocabulary and reading.24 Nationally, 75 percent of homeless children perform below grade level in reading, 72 percent perform below grade level in spelling, and 54 percent perform below grade level in math. As with physical and mental health care, homeless children’s greater needs do not lead to greater access to special services. Even though homeless children are more in need of special education as compared to the general student population, they receive less. Thirtyeight percent of homeless children with learning disabilities receive treatment for their disabilities, compared to 75 percent of housed children with disabilities; nine percent are in special education classes, compared to 24 percent of housed children. While homeless children receive fewer services, they are more likely to be held back a year (36 percent of homeless children compared to 18 percent of other children). This is particularly disturbing because in general, children who are held back a year are more likely to repeat a grade in the future.25 Although many homeless children are held back because of academic failure, many others are held back because of circumstances that may relate to their homelessness: excessive absenteeism (21 percent of homeless children compared to five percent of other children) and because they moved (14 percent of homeless children compared to five percent of other children).26 A local study of homeless children conducted by the University of Minnesota’s Center for Urban and Regional Affairs (January 1999) bears out these trends. In 1995-96, 80 percent of homeless children surveyed fell into the bottom quartile of the Weschsler Individual Achievement Test. Another achievement test showed that more than half of these children had already fallen behind in elementary school by two or more years. CURA notes that children with such delays have high drop-out rates when they enter secondary school. Many of these children have poor academic performance before becoming homeless, and their homelessness exacerbates their academic difficulties. 9 4 The Effects of Homelessness Can Be Minimized—Maybe Even Reversed Many homeless children can benefit from a number of cost-effective, practical interventions. Parental Closeness Involvement in Education Caring Adults One-to-One Tutors Teachers Support Programs There is good news. While research on homeless children paints an overwhelmingly bleak picture of their current and future status, there is hope that with early and consistent intervention strategies, children can learn to overcome many of the detrimental effects of their poverty and homeless experiences. A local study of homeless children conducted by the University of Minnesota’s Center for Urban and Regional Affairs (CURA) noted that some homeless children were succeeding academically despite highly challenging situations. In their efforts to collect information directly from homeless parents, CURA found that parents typically are “quite concerned about their children and value education as the most important need of their children beyond the survival basics of shelter, food, and clothing.”27 When CURA analyzed what practices contributed to the success of these children, they noted: • • • • parental closeness with their children and involvement in children’s education; high-quality relationships with teachers in special intervention support programs; one-to-one relationships between tutors and children; and relationships with competent and caring adults. While it is true that most homeless children have been damaged significantly in their short lives, there is real hope that many homeless children can benefit from a number of cost-effective, practical interventions that 10 build their resiliency and competence. If these interventions are to be successful, however, homeless families must be placed in stable housing with appropriate services as soon as possible, and the parent must receive the support necessary to act as the primary caregiver.28 One set of strategies is to ensure priority access for homeless families for the services that can mitigate the detrimental effects of homelessness. Homeless parents and children should receive priority for the following services: • Long-term supportive housing; • Drug and alcohol treatment and sobriety support programs for mothers, particularly those who are pregnant; • Parenting education and support programming specifically designed for parents who did not experience a supportive childhood; • After-school tutoring and academic support programs; • Nutritional support programs, including WIC (Women, Infants and Children — a food supplement program), free-lunch programs at school, supplemental snacks in after-school programs, and other food support programs for families and children. In addition, there are a number of strategies that providers of emergency and supportive housing can employ to mitigate or reverse the negative effects of homelessness on children. These include: • • • • Ensuring that all homeless women receive an initial health screening at time of admission into emergency or supportive housing; Ensuring easy access to prenatal care for pregnant women. This may require advocacy regarding their entitlement to benefits, transportation, and child care for their other children; • • • • • Teaching each new mother about her child’s individual early development needs, especially if the child was born with health problems; Encouraging the use of WIC and other food supplement programs to meet the increased nutritional needs of pregnant and lactating mothers; Assisting parents in understanding their children’s nutritional needs; • Assisting families in obtaining supplemental food resources, either on-site or through advocacy and referral; • Ensuring that all children are screened for immunizations and receive ongoing immunizations; • Ensuring that preschoolers attend early childhood and learning readiness programs, which may include arranging for transportation to programs; Conducting an initial developmental screening of all children entering the housing programs, including physical, emotional and behavioral, cognitive, and academic assessments; Monitoring children to ensure that they receive the physical, mental, and special educational resources to which they are entitled; Assisting parents in supporting their children’s school attendance and performance. This might include helping parents to enroll their children in school, arrange for school transportation, and attend school functions and meetings associated with the child’s performance; Interventions give young children who have experienced the traumatic effects of homelessness the chance to build the resiliency and competence they need to break the detrimental cycle of homelessness. Assisting children in participating in after-school social and recreational activities. These various strategies begin with the earliest interventions in prenatal care and continue as the child grows and pursues his/her potential. These interventions give young children who have experienced the traumatic effects of homelessness the chance to build the resiliency and competence they need to break the detrimental cycle of homelessness. 11 Endnotes 5 1 Hausman, Bonnie and Constance Hammen. “Parenting in Homeless Families.” Amer. J. Orthopsychiat 63(3): 358-369, July 1993; “Tale of Two Nations” Homes for the Homeless. www.opendoor.com/hfh/ Sep. 2, 1998. 2 Roman, NP; Woffe PB. “Web of failure: the relationship between foster care and homelessness.” Washington, DC: National Alliance to End Homelessness, 1995; “Homeless Children: America’s New Outcasts.” Better Homes Fund, 1999; “Day to Day: Parent to Child.” Homes for the Homeless. www.opendoor.com/hfh/Jan. 1998; Ibid. “Tale of Two Nations.” 3 Bassuk, Ellen L. and Linda Weinreb. “Homeless Pregnant Women.” Amer. J. Orthopsychiat. 63(3): 348-356, July 1993. 4 Ibid. “Homeless Pregnant Women.” 5 Ibid. “Homeless Children: America’s New Outcasts”; Ibid. “Homeless Pregnant Women.” 18 Ibid. “Homeless Children: America’s New Outcasts.” 19 Ibid. 10 Rescorla, L: et al. “Ability, achievement, and adjustment in homeless children.” Amer. J. Orthopsychiat. 61(2): 210-220, April 1991. 20 Ibid. 11 Ibid. “Homeless Children: America’s New Outcasts.” 21 Zima, BT; et al. “Emotional and behavioral problems and severe academic delays among sheltered homeless children in Los Angeles County.” AJPH 84(2): 260-264, February 1994. 12 Wood, D. “Homeless children: their evaluation and treatment.” Journal of Pediatric Health Care 3(4): 194-199, July 1989; Wood, DL: et al. “Health of homeless children and housed, poor children.” Pediatrics 86(6): 858-866, December 1990; “Affordable Housing Shortage Threatens Children’s Health.” Family Housing Fund, June 1999. 13 Molnar, JM; et al. “Constantly Compromised: Impact of Homelessness on Children.” Journal of Social Issues 46(4): 109-124, 1990. 6 Ibid. “Homeless Children: America’s New Outcasts.” 14 Smith, LG. “Teaching treatment of mild, acute diarrhea and secondary dehydration to homeless parents.” Public Health Rep 102(5): 539-542, September 1987. 7 Mangine, SJ; et al. “Homelessness among adults raised as foster children: a survey of drop-in center users.” Psychology Rep 67(3 Pt 1): 739-745, December 1990. 15 Ibid. “Homeless Children: America’s New Outcasts.” 8 Grant, R. “The special needs of homeless children: early intervention at a welfare hotel.” Topics in Early Childhood Special Education 10(4): 76-91, 1990. 12 9 Eddins, E. “Characteristics, health status and service needs of sheltered homeless families.” ABNF J 4(2): 40-44, 1993. 16 Fierman, AH; et al. “Growth delay in homeless children.” Pediatrics 88(5): 918-925, November 1991. 17 Ibid. “Affordable Housing Shortage Threatens Children’s Health.” 22 Molnar, JM; et al. “Constantly compromised: the impact of homelessness on children.” Journal of Social Issues 46(4): 109-124, 1990. 23 McLoyd, VC. “Socioeconomic disadvantage and child development.” Am Psychology 53(2): 185-204, February 1998. 24 Parker, RM; et al. “A survey of the health of homeless children in Philadelphia shelters.” Am J Dis Child , 145(5): 520-526, May 1991; Ibid. “Homeless Children: America’s New Outcasts.” 25 Ibid. 26 Sandel, Megan; et al. “There’s No Place Like Home.” Housing America , 1999. 27 Masten, AS and Arturo Sesma. “Risk and Resilience Among Children Homeless in Minneapolis.” CURA Reporter 19(1), January 1999. 28 Helvie, CO and BB Alexy. “Using after-shelter case management to improve outcomes for families with children.” Public Health Rep 107(5): 585-588, September 1992. 13 FAMILY HOUSING FUND MIDWEST PLAZA WEST SUITE 1840 801 NICOLLET MALL MINNEAPOLIS, MINNESOTA 55402 Tel: 612-375-9644 Fax: 612-375-9648









© Copyright 2026