
Recognition for a Job Well Done!
1 City College San Francisco RadTimes July 2014 | Volume 3, Issue 4 DIAGNOSTIC IMAGING PROGRAM NEWSLETTER CONTENTS 1 Student Life 3 How we survived second semester 4 First Day San Francisco General 5 Graduation Photos 6 Tuberculosis: A Newbie’s Guide on How to Protect Yourself and Others 8 Inter-Professional Education: DMI and RN’s New Frontier 9 Children or School 10 #studentradiographer 11 My Clinical Rotation Experience 12 A Lesson Learned 13 Let’s go BACK to the FUTURE! 14 HOLD YOUR BREATH ... BREATHE 15 Migration South for Vacation 16 Diary of a 4th Semester Student 18 MRI Contrast Complications 19 Student Meets Incident 20 Why DMI? Graduation Day: Members of the December, 2014 class joined the July, 2014 class for a day of celebration and ceremony Recognition for a Job Well Done! Recognition For a Job Well Done! This issue is dedicated to the DMI instructors and students for working together to achieve success. The student success rate which had decreased below 70% in recent years, increased to 76%. Included in this figure are the seven graduates of July, 2014. Don't miss their class picture on page 5 of this issue. This program does not involve luck. It requires hard work. The staff and students have proven that they are motivated to do what it takes to progress to the next level. Way to go! 21 Second Semester Students Explore the 15% Rule Student Life By Kenny Yip As an immigrant to the United States without too much educational background, there weren’t many opportunities for me to choose what I wanted to do once I arrived here. Moreover, education wasn’t an option for me previously because of my financial situation and therefore, I went to work in a restaurant shortly after moving to the United States. After working in the restaurant business for over fifteen years, everything in my life was pretty much on track, however, I felt lost. I kept asking myself if I was destined to work in a restaurant for the rest of my life. Should I be doing something else? Should I be doing something more meaningful? With my limited education and skills, I Continued on page 2 4 2 3 didn’t know what I could do besides working in food service. Fortunately, a friend of mine is a radiologic technologist and he guided me into this field and I discovered the Diagnostic Medical Imaging program at City College of San Francisco. In order for me to apply to the DMI program, I needed to take some prerequisite classes so I embarked on my educational journey in 2007. It took me three years to finish all the prerequisites while I was still working full time and in 2010 I was finally qualified to submit an application for the program. However, spaces are limited due to the number of students who apply to the program. For this reason, not every applicant is accepted despite having fulfilled all of the prerequisites. Instead, everyone has to go through the lottery process. Unfortunately, my name didn’t get chosen in the first round so I had to wait for another year and resubmit my application. Luckily, I was accepted to the program the second time around and this is how my story starts. Since the DMI program is a full time program, I was unable to work full time. I had to change my life style and change my spending habits because I would now have to live on my savings plus a limited income for the next three years. It was a little difficult at first since I had to reduce expenditures on just about everything. Fortunately, I was able to lower the monthly mortgage on my house which helped. I had to make sure that I didn’t gain or lose more than a few pounds because that would mean buying new clothes which wasn’t an option. My eating habits had to change a bit and some of my favorite foods wouldn’t be on the menu anymore. For instance, I wouldn’t be dining out as much, but rather cooking at home. Finally, I had to sell my six cylinder car and exchange it for a smaller four 2 cylinder car in order to save money on the gas and insurance. These lifestyle changes are just one piece of the puzzle that would now define my life. After squaring away the financial changes and lifestyle changes, I then needed to work on the emotional changes. After the program started, I was no longer able to spend much quality time with my wife and my family. My time was occupied by class, clinical, and work. Even when I had a day off I would still need to keep up with studying and homework. I felt like nobody could understand how stressful my life had become including my wife. Furthermore, the program required a 75% passing grade in every class. If I received a grade lower than 75% in a class I would need to start all the program over from the beginning assuming I could even get into the program again. A spot was not guaranteed. For this reason, I felt incessantly anxious and worried. As the saying goes, “I’m not getting any younger” so I had to make sure I passed all the classes because I don’t have time to start all over again. I don’t want to waste six years of hard work. After all, I am nearing the end of this program. Besides the didactic activities, the clinical component is the other part of the DMI program. Everything went well for the first two clinical semesters until the third clinical semester. The third semester is the rotation semester where students rotate to a new hospital. Everything is so different from the hospital that I was based at and it took me a little over a month to get used to new equipment and new protocols. I also had to get used to new people including the technologists and the types of patients. I was so nervous at the beginning when I rotated to the new hospital because of the new surroundings. Meanwhile, I was also trying to prove myself and gain the trust of those around me. I found out that the more I pushed myself, the more mistakes I made. Luckily, one of the technologists noticed my honest efforts and told me to slow down and not try to rush everything because this is how we make mistakes. In all honesty, that was the best advice I had received so far because I didn’t realize I was pushing myself so hard. In short, the DMI program at CCSF is a great program for people who want to work in the medical field because of the bright future; moreover, it is also great for people like me who want to change their career and do something more challenging. As a final suggestion for those who want to be a future technologist, be prepared financially and emotionally as you enter the program. You won’t be able to work full time and you won’t see your friends or family often. One final thought for future students is that I can attest to the fact that we are most certainly not just “button pushers”! CCSF RadTimes July 2014 1 2 3 NEWSLETTER SPOTLIGHT: How We Survived Second Semester By Michael Ng Since the 2nd semester of (DMI) Diagnostic Medical Imaging Program has been touted as one of the most difficult of all the semesters, I thought it would be interesting to do a survey of my class to share how so many of us are progressing through. The objective was to figure out the study habits and the different ways people were coping with the workload while trying to de-stress and maintain some sort of sanity. Kyle Thornton, Department Chair, and Diane Garcia, Clinical Coordinator, have stated that as a group, this class, in particular, has been one of the most stressed out classes in a while. Kyle has also stated that he expects a larger than usual number of students to continue on to the 3rd semester, making it more challenging for Diane to place us in clinical sites. I conducted this survey with various questions such as educational background, work balance, study habits, and stress management. The first couple of questions were aimed at trying to understand the background of the class to see if there was any 3 correlation between previous schooling and our success. Of the thirteen people in the class, most were working and held jobs that varied from bartending, retail, and even graphic design. Some of the younger classmates were still in school doing prerequisites for the DMI program or trying to finish their degrees. Seven students in the class already had degrees that varied from kinesiology, fine arts, microbiology, and even business. Three students had no degrees and three others had associate degrees. Most felt that their degrees have not helped much with the program since they were in different subjects, but some feel that the study habits that they obtained while in school have been useful. Because the workload for the second semester is significantly more than the first, it was important to inquire about the number of hours per week the working students were putting in. It would be difficult to study three hours for every one hour of class recommended by our teachers if we were working too much. The results found that nine out of thirteen classmates worked an average of 12 hours per week. Ricky Ng shockingly worked the most during the week with about 33-36 hours. Working during this semester can be done, however making it much more challenging. My classmates said they would consider cutting back hours if necessary. Also, because the workload has increased I wanted to find out if my classmates were doing anything different compared to the first semester to compensate. The results were quite varied here but the most common accommodations that took place 2nd semester were studying harder, not procrastinating, and working less. Some also suggested having more study group sessions or giving up Saturdays to practice positioning at school. Vanessa Aycock's answer was interesting because she "treated school like a full time job" during the 2nd semester. No doubt the study time has increased but everyone studies differently. It was important to know how people were studying and to see what is working for our class. The majority of the class said their preferred method of studying was a combination of individual time mixed with study groups. Most everyone preferred to study by themselves until they grasped the information and understood it before joining study groups. However, some preferred only doing study groups, for constant dialogue to help understand the information as well as an opportunity to ask questions. Group study also provided a forum for testing one another. Because meeting up isn't always easy and convenient for everyone, a common tool used by my peers was Skype. Studying individually is essential, but studying in groups is essential as well. For example, you can't practice positioning by yourself. Other tools that were useful throughout the semester were the notes and study guides that classmates passed around. We were lucky enough to have students who made PowerPoints and Quizlettes that were used to test each other. Not only is the workload immense, but the stress that goes along with it is evident as well. Everyone will have their own way of coping and dealing with stress. My peers all had different ways of coping. Some said that keeping up with the work helped them feel less stressed because they didn't feel behind in their studies. Others went out with CCSF RadTimes July 2014 4 1 friends once in awhile to get away from the daily grind. Some listened to music while others ate food to distract themselves. Another common answer was to empathize with your peers. Luis Moran utilizes a light hearted method of stress relief by tuning into Comedy Central everyday because "laughter cures all". In the end, the best advice we can give to anyone coming into this program is to take ownership of your learning and do what works for you. Don't fall behind and have fun with the opportunity you have been given! Talk to the classes ahead of you and let them instill some fear in you. Hearing all the horror stories made us work that much harder. Another key component is that cooperation is vital. Every Remember that “laughter cures all” for students during second semester! person in the class was a key contributor to the success of the group. Even though we, unfortunately, lost a couple of people, our class is tight knit. We have each other's back and are each other's motivators. No one else understands the stress you go through but the people who fill those classroom chairs each and every day. So, be there for each other and support one another. Lastly, ENJOY THE RIDE! FIRST DAY: San Francisco General Hospital By Jalil Kawas It was the last week of our finals after a brutal second semester in the Diagnostic Medical Imaging Program at City College of San Francisco and with just a couple days to unwind, the grind of internship consisting of 8 hours a day for 5 days a week was just around the corner for my classmates and me at San Francisco General Hospital (SFGH). We had often talked about where we wanted to be placed even though the decision was out of our hands. I was one that said, “I hope I go to the General. I want to be a part of that mayhem”. When the day came that we got our clinical placement e-mail, my placement was at SFGH. The day after Memorial Weekend 2013 was the first day of clinical at SFGH. I started to prepare for what would be my daily routine for the next seven weeks of “summer school”, as I thought of it. I was as nervous as a child on his first day of school. SFGH requires us to start at 7:30am. My classmates and I arrived at different times but all of us arrived at the radiology department by 7:30. As I entered, I started to introduce myself to the radiologic technologists that were also arriving to start the day. Some were approachable and some gave you the feeling that they were thinking, “great, a new batch of students to babysit”. Since this was my first clinical assignment, I felt like I was coming in “wearing diapers”. Not too long after introductions, we met our assistant clinical instructor whom we followed to the break room for our orientation to our new home for the summer. We were given an introduction to the hospital and what was expected of us while we were here. During my second week at SFGH I was shadowing the different techs and accompanying them during exams to observe and assist so that I could become acclimated to the radiology department. One afternoon a tech approached me and asked if I wanted to “check something out.” I was all about being busy and I didn’t want to stand around so I took a walk with the tech. As we walked I asked him where we were going and what was going on. He turned and told me, “gunshot victim”. My eyes, at that moment lit up with excitement, this was my first trauma patient. We entered Room 64 which connected to Trauma 2. Each x-ray room is connected to a trauma room. There are windows to observe not only the patient but whatever medical emergency happens to come through the hospital. Looking through the window, the victim was a male who was shot in the chest. Most of the personnel in the emergency department converged on the room like a swarm to help this individual who was lying on the gurney in a motionless state. They cut his clothes off, started IV’s, and intubated him with the quickness of a cheetah chasing down its prey. I couldn’t move away from where I was standing because my eyes were glued to the action. Continued on page 5 4 CCSF RadTimes July 2014 2 Looking at the victim, I could see where the bullet penetrated him in the chest. The hospital staff was relentless in their efforts to keep this person alive. After a few minutes of chest compressions and other life saving techniques, the chief surgeon showed up with two other doctors to assess and assist in trying to save this man’s life. As I studied the scene, the doctor made a lengthy incision down the side of the victim’s chest. In the brief moment that I turned my head away to sneeze, the patient’s chest had been cracked open with rib splitters. The scene was surreal; one second his chest looked normal and the next second his ribs were protruding through his skin. The doctors then proceeded to work their hands, one at a time, into the victim’s chest. The tech explained that “the doctors were in the chest cavity massaging the heart to keep it beating while they tried to save him.” After another few minutes of doing everything they could to revive the patient, the medical team’s actions came to a halt. The patient was pronounced dead. I then saw others entering the trauma room. It didn’t dawn on me at first why these people came in, but then I remembered that SFGH is a teaching hospital for new residents. These people were doctors in training and they were in the trauma room getting a lesson from the seasoned doctors. You could see them examining the victim from every aspect as if experiencing something fascinating for the first time. After all the residents left, I remained transfixed on the patient. I stayed and watched a female doctor stitch the victim’s chest back together. Looking at the aftermath, my eyes fell upon the victim’s dead stare. This made me reflect on how precious life is how easily life can be cut short in the face of a tragedy. I finally peeled myself away from the trauma window with a whole new perspective and respect for what I would be experiencing in my daily life as a tech. Later that night I received an e-mail from my clinical coordinator asking us how our day in the hospital went. I summarized the shocking scene that unfolded before my eyes earlier that day. She responded back by explaining that situations like the one I witnessed are a part of life and not to let it bother me into the night. I wrote back and told her that it didn’t bother me. The events of the day made me think about my own life. I thought about the patient as well. He will never see his family again and his family will be grieving the loss of their loved one indefinitely. All of the lives he touched would be affected by his passing. It was an important reminder that death is a part of life. I would never have imagined that my first day in the clinical environment would begin with that experience. Though shaken, I was equally excited to get back to SFGH the next morning and continue my education. I want to be a technologist who makes a difference by performing my job well. I have always taken my education seriously but now I have a new appreciation for the role of radiographer. This is serious work and I am determined to do the very best I can to aid the healthcare team in our mission to care for patients … and perhaps even save a life. 5 Congrats to our Grads!!! Did you know that you can support patient safety and help to protect the future of your career at the same time? Join the CSRT today! It’s your future. CCSF RadTimes July 2014 1 TUBERCULOSIS: A Newbie’s Guide on How to Protect Yourself and Others By Chelsea Christopher Tuberculosis.... I remember before I lived in San Francisco, I had learned about tuberculosis in school. I vividly remember the image of the Iron Lung shown in class and I remember mentally categorizing tuberculosis with other diseases, such as polio, as a condition of 1950s America; a thing of the past. I knew that tuberculosis was rampant in other areas of the world, but I never thought I would have to worry about this “old” disease in my lifetime. That all changed when I started my clinical rotation at a major San Francisco hospital as a student technologist. The first time I encountered a patient’s requisition that read “TB+,” I panicked. I had no idea what to do or how to protect myself. I realized I knew very little about the disease and what to do when performing an examination on a patient with suspected or confirmed tuberculosis. After talking with some seasoned technologists and doing a little research on my own, I now feel confident as to what to do when encountering this type of patient demographic. In this article, I hope to provide a background and a simple how-to guide as to what to do to protect yourself and others against the spread of tuberculosis. Chances are, if you work in the health profession, you have encountered a patient with suspected or confirmed tuberculosis. This is especially true in the city of San Francisco. According to San Francisco Health Partnership (SFHIP), 13.1 cases of tuberculosis per 100,000 people were recorded in 2011. This makes San Francisco County the highest of all tuberculosis rates in California, with 118 new recorded cases in 2011 alone. San Francisco is also home to a number of tuberculosis care facilities, making the possibility of exposure that much more probable to health care workers in this area. Since radiologic exams are often used to diagnose or rule out tuberculosis, technologists are often subjected to the potential tuberculosis infection. Since the likelihood of coming into contact with tuberculosis is high, it is important to recognize when a potential exposure is likely to occur in order to reduce the possibility of infectious transmission. So how can you recognize a situation where you might be exposed to tuberculosis? Unfortunately, these situations are not always obvious. A person with tuberculosis may or may not be showing any signs of infection and might not be wearing a mask to avoid infectious transmission. Luckily, in the world of radiology, a patient’s requisition can tell us a lot about the patient before we come within contact. This gives us an opportunity to prepare for potential exposure to tuberculosis and other infectious diseases requiring special protective measures. A patient’s requisitions may state that the patient has a history of positive (+) PPD or QFT. These two abbreviations stand for purified protein derivative, also known as the tuberculin skin test, and the QuantiFERON tuberculosis blood test respectively. Although a positive test finding does not always mean the patient actually has the disease, the same precautions should be exercised as if the patient had tuberculosis to minimize potential infection. Other indications of potential tuberculosis exposure include a requisition that reads “R/O TB,” or “positive (+) TB.” As a health care employee, knowing what tuberculosis is and how it spreads will help you to take the appropriate precautions in protecting yourself and others from potential infection. So, what is tuberculosis and how does it spread? Mycobacterium tuberculosis is the bacteria responsible for tuberculosis. Once a person is infected with mycobacterium tuberculosis, they will always possess the disease in either an active form or a dormant form. This bacterial disease predominantly affects the lungs, but can spread to affect other areas of the body. When this bacterium enters the lungs it wreaks havoc on the delicate lung tissues. The body attempts to protect itself by walling off the infiltrative organism, limiting its spread to adjacent tissues in a process that results in necrosis of lung epithelial, and eventually scarring. Scarring can lead to further respiratory complications in an infected person. Although primary tuberculosis occurs in the apices of the lungs, secondary infections and other types of tuberculosis can occur in any part of the lungs. When a person is infected with mycobacterium tuberculosis, he can spread the disease to others by transmission through air. This disease is considered airborne and a person can catch the disease by being in close proximity to an infected individual when they cough, sneeze, or even talk. According to San Francisco Health Partnership (SFHIP), a person with tuberculosis is contagious until she has been on the appropriate treatment and has completed the intended course of medications. One thing that makes tuberculosis especially dangerous is that research on its transmission is incomplete. The CDC states on their website ( HYPERLINK "http://www.CDC.org" www.CDC.org) that, “... the smallest infectious dose of M. tuberculosis nor the highest level of exposure to M. tuberculosis From left: Hui Shan Su, Jalil at which transmission will not occur has been defined conclusively.... Furthermore, Kawas, and Chelsea Christopher the size distribution of droplet nuclei and the number of particles containing viable chill out before a tour of the MRI Continued on page 7 6 CCSF RadTimes July 2014 2 M. tuberculosis that are expelled by infectious TB patients have not been defined adequately, and accurate methods of measuring the concentration of infectious droplet nuclei in a room have not been developed.” This statement should raise significant concern. What is to be done to limit the spread of tuberculosis if the means of infectious transmission are not well defined? It is crucial to use standard precautions when working with all patients. Standard precautions assume every patient is infectious and requires health care providers to exercise minimum infection prevention measures with all patients, regardless of suspected or confirmed infection (www.CDC.org). Hand washing is of particular importance. Although standard precautions minimize the risk of infection for most communicable diseases, tuberculosis requires efforts beyond the use of gloves and frequent hand washing due to its aerosol, or airborne nature. In the case of tuberculosis, transmission-based precautions should be used. Under the larger umbrella of transmission-based precautions, tuberculosis is considered an airborne communicable disease, and requires the use of airborne precautions. This means that when coming within contact with an infected patient, we follow the following guidelines according to the CDC: Try to isolate the patient as much as possible. This means not placing the patient within close contact with yourself, health care workers, or other patients. Provide a procedure or surgical face mask to the patient. Obtain an exam room as soon as possible and instruct the patient to keep their mask on for the entire exam, or while visiting the hospital, and to avoid close contact with other individuals. Ideally, an airborne infection isolation room (AIIR) should be used to perform the exam in, if available at your care facility. If at any time you need to leave the room, make sure the exam room door is closed, and personnel are notified of the patient’s condition if they attempt to enter the exam room. Make sure to wear personal protective equipment appropriate for airborne precautions before coming within contact with a suspected or confirmed tuberculosis patient. This included the use of an N-95 respirator or higher (i.e. N-99 or N-100 respirator) to be worn by the health care worker. According to the FDA and CDC, N-95 respirators are approved for use, and measure over 95% effective against the spread of tuberculosis, when properly used. The effectiveness is a measurement of filter efficiency of the respirator’s ability to filter particles of a size of 1 µm at a rate of 50 L/min. Fit testing is necessary for the N-95 respirator to be considered effective. Proper fitting requirements will be explained later in this article. The N-95 respirator should be removed promptly whenever exiting an exam room. Proper disposal of the N-95 respirator is crucial to contain any potentially infectious particles that might be present on the respirator. All FDA-cleared N-95 respirators are designed for single-use only, and are considered disposable devices. If your N-95 respirator becomes damaged, wet, soiled, or if breathing becomes difficult, the N-95 respirator should be replaced immediately. Make sure to wash your hands before and after coming into contact with an infected patient or contaminated objects. Properly dispose of contaminated objects such as gloves, masks, respirators, and other materials. Finally, proper cleaning of the exam room should be done once the patient has left. This includes any surfaces the patient may have touched or been near (i.e. chest stand for chest x-ray, etc). The room should be well ventilated and left vacant for as long as possible to reduce the risk of inhaling residual mycobacterium tuberculosis particles. As stated above, proper N-95 respirator fitting is required to ensure protection against tuberculosis. Without proper fit testing, an N-95 respirator is considered ineffective. So, how do you go about getting fit tested? Check with your facility to see where to get fit tested. They must provide the means to do so as part of their infection control program. The goal of fit testing is to provide an adequate seal and this is achieved when there is a N-95 respirator leakage under 10% (NIOSH guidelines). In general, a proper fitting N-95 respirator should fit tight to the face without feeling uncomfortable. It should provide a seal to the wearer’s face to improve protection from mycobacterium tuberculosis particles. It is important to note that fit testing is model specific and whenever switching from model to model, you must be fit tested again to ensure protection. An improperly fitted N-95 respirator poses the risk of infectious particles being inhaled and this is particularly of concern around the periphery of the respirator where there is poor contact or lack of a seal to the wear’s face. N -95 respirators are not designed for children and are not appropriate for people who have facial hair or wear excess makeup, because a proper seal cannot be achieved. Once you have been fit tested and the make/model and size has been determined appropriate for you, you can now follow the guidelines detailed above when coming into contact with patients that have suspected or confirmed tuberculosis to reduce the spread of infection. Reducing the spread of mycobacterium tuberculosis through the use of airborne precautions allows a technologist to provide a safe environment for all patients. Knowing what to do in the case of potential tuberculosis infection will enable a technologist to perform the necessary diagnostic images while maintaining professional. A professional technologist should concentrate on providing exceptional patient care without showing signs of anxiety or fear that might otherwise alarm a patient. It is our responsibility as technologists to support to our patients in times of uncertainty. Personal confidence in caring for patients with suspected or confirmed tuberculosis and other communicable disease not only allows patient care to become a priority, but enables a technologist to protect themselves and others from the spread of tuberculosis. References: "TB Respiratory Protection Program In Health Car Facilities- Administrator's Guide." Centers for Disease Control and Prevention. DHHS (NIOSH) Publication Number 99-143 . (1999): n. page. Web. "Basic Infection Control and Prevention Plan for Outpatient Oncology Settings." Centers for Disease Control and Prevention. (2011): n. page. Web. 26 Feb. 2014. 7 CCSF RadTimes July 2014 1 2 3 Inter-Professional Education: DMI and RN’s New Frontier By Kyle Thornton Registered nurses and imaging technologists must often collaborate in order to conduct imaging studies on patients. Communication is an essential element to ensure the success of the students. Interaction, collaboration, and professional conduct in a stressful and rapidly changing environment are also key factors. The DMI students participating in the activity were fourth semester students. Many of them had observed technologists and other medical professionals caring for a trauma patient, but had not actively participated in the event. Thus, the objective of this skills laboratory activity was to create a situation as true to an actual clinical experience as possible. Using a patient simulator, the skills lab was set up to resemble a trauma room. The patient was involved in an explosion. He sustained severe burns to most of his body, along with an open, compound femoral fracture. Upon arrival to the trauma center, RN students were required to assess his condition, stabilize him, and provide appropriate care. Part of their assessment and care included ordering a number of appropriate diagnostic procedures. Among them were X-ray studies of the chest and femur. DMI students were requested to provide an X-ray examination of the affected areas in the trauma room, with mobile imaging equipment. DMI Intern Natalia House assesses the trauma patient while DMI Intern Harry Jufri moved the portable X-ray machine in place. The examination was conducted by students, Natalia House and Harry Jufri, while the other members of the class observed. Prior to the event, These skills are often learned in the “real-time” clinical environment in which there is not always time for evaluation, comment and reflection. Therefore, the Registered Nursing and DMI programs collaborated to implement a skills laboratory activity in which the two disciplines could interact and participate in a simulated environment with guidance and feedback before students encountered the experience in “real-time.” DMI Intern Natalia House discusses the examination with the RN students. 8 the students were briefed on expectations of what they might encounter, and what their duties would be once they entered the trauma room. When the students entered the environment, the atmosphere was one of managed chaos. The patient was screaming in pain, nurses were rushing to stabilize him, and the DMI students had to determine where they fit in to this scenario. For a simulated environment, the stress level was high, but that was to be expected. The purpose was to create as true a scenario as possible. Natalia and Harry communicated their needs with the RN student in charge, and proceeded to conduct the examination. For a first time effort, this event was considered successful. Following the event, the group of students indicated this activity had educational value, and felt more confident in their ability to participate in the imaging needs of a trauma patient, as well as their ability to communicate with other personnel while conducting an exam. Effective patient care is the result of a collaborative effort of multiple individuals, each providing their own level of expertise. Interdisciplinary activities such as these have excellent potential to improve the educational experiences of students and their ability to provide better patient care. Dr. Kyle R. Thornton, RT(R), (CT), CRT Radiologic Sciences Department Chairperson, Diagnostic Medical Imaging Program Director CCSF RadTimes July 2014 1 2 Children or School By Hui Shan Su I feel so lucky that I could start the Diagnostic Medical Imaging (DMI) program in Fall of 2012. The education system in the United States will lead me to a better way of life. My dream, to be a radiologic technologist, will come true with this treasured chance. I have two sons who are four and two years old and a one-month old daughter. As a full time student and part time employee, my biggest fear is that I won’t have the time to give my children the care they need. I really want my children to have the best upbringing possible. I love my children without any reservation but I also enjoy my student life very much. This paradox causes me to ponder whether I should drop school and stay home with my children or continue. After thoroughly pondering this burdensome decision, I strongly believe that I should not drop out of the program. I am eager to be a radiographer one day soon. I am ready to reach my dream so I must complete the Diagnostic Medical Imaging Program. The decision has been made. Students entering this field of study need strong mathematics and communication skills. They need a background in chemistry, physics, english, and health education. Luckily, I am good at science but I am struggling with my English skills as I am an ESL student which adds an extra burden to my learning. One challenge I have is convincing my friends that I want to continue in school because they are trying to convince me to drop. They think that I should spend some more time with my children. I agree that it is not easy to take care of three children as a full time student. My daughter is only one-month old! She is demanding much of my attention. She does not always sleep when I need to sleep and cries during the night and I have to comfort her. Her needs come first so I must often sacrifice sleep for myself. She sleeps during the daytime, but I cannot. I have to go to school and go to work. My sons are also very young and demanding of my attention. They are at an age where they fight with each other, often over toys. I must be there to help them learn. On top of the daily pressures, I must also squeeze in enough time to take my children to the doctor for checkups and other issues. I must also have time to see the counselor of the Women, Infants & Children Supplemental Nutrition Program……and there is so much housework that is always waiting for me. The fact that English is not my native language causes me to spend a lot of time reading and understanding what is required before I can even begin doing the work. To communicate well, I have to have time to talk in English with my classmates and teachers in order to understand the information to pass all of the courses. My friends fear that I will be too tired and not have enough energy to effectively and successfully care for so many things at the same time. I understand that it is extremely difficult for me to be a radiology student as well as to care for my children and also have a part-time job but everything in life is a choice and these are the choices I have made. I know I can take care of them all. This is how I do it….. I have a wonderful husband who supports me. He cares for the children in the early morning so I can leave by 6:00 am for the hospital. He takes our eldest son to preschool from 9-5 pm and my mother helps by taking care of the younger boy and my baby girl during the afternoon so my husband can go to work. My sister helps me by picking up my son from preschool and brings him back home. She then gives the children a bath so that I can attend the evening courses that are required. My husband finishes his job and gets home around 7:30pm. He takes care of the kid’s dinners, teeth brushing, storytelling, and more. Family support is so important. It would be impossible for me to be a full time student without help from my family. The trick to juggling all of my responsibilities is my ability to manage my time well. Time management is one of my specialties! I arrange all appointments with the doctor and counselor in the same afternoons. I do my homework in the evenings after my family goes to sleep. I write down all of my appointments and school assignments on the calendar and check it every day so I will not miss any of them. If you have responsibilities that demand your time the way I do, you become an expert in time management very quickly! I have a part-time job as a medical clerk at a clinic eight hours per week. This only allows me to earn a few hundred dollars per month to supplement the household income. My husband also has a parttime job. The amount of money that we earn is barely enough for our daily living and educational expenses but I am grateful for what we have and especially grateful for the W.I.C. program and food stamp programs that help us. This help is instrumental in helping me to finish the DMI program. So, as I think about this more clearly as I am writing, I absolutely will not drop out of the radiology program, it is my dream and I will make it come true. My educational goals are important to me and I will not let anything get in my way. I will follow my dreams for a higher paying career, better benefits and the opportunity to be financially independent. Along with this, I vow to give my children the best education and upbringing that our lives will allow. Thinking about this choice I realize that to be a DMI student doesn’t mean that I love my children less, on the contrary, being a DMI student means that I love them more and without any reservation! 1 2 #studentradiographer By Steve Carreon I can still remember receiving my letter of acceptance to the DMI program at CCSF. It seemed too good to be true after not being accepted the previous year. It took a moment for me to realize that I was, in fact, accepted this time around and I needed my wife to reread the acceptance letter for me. Upon DMI program commencement, the director, Kyle Thornton, gave us clear expectations as to what lies ahead. He provided us with meaningful advice to help us succeed. Congruently, our clinical coordinator, Diane Garcia, provides the similar advice up to the present day. When you’re listening to the advice given, you hear everything that is being said but, you really need to experience the program in full swing to put the advice into action. It seems that when you reach a certain age, your ability to evolve tends to diminish. I know that I have the capacity to change and adapt, but sometimes I’m unsure of how to implement that change. My perception of myself isn’t quite realized yet. This experience is quite different compared to previous learning situations. So, this road is definitely not an easy one. That truth doesn’t hit you until later while immersed in the program. Summer of 2009, our first child, Addison was born while I hammered out my prerequisites in a timely manner. I say “timely manner” because I wasn’t getting any younger and my wife doesn’t want to be the sole bread winner. Nor did I want her to be. I was already practicing how to have a young child, but not be fully present with him because I was studying. Thank you, Grandmas and Grandpa. A year later, while achieving the completion of my volunteer hours, we had our second child, Bryce Marie. Unfortunately, we had to make a decision that I wish no parent should have to make. We withdrew life support. She was born almost four months premature and suffered an injury to the blood vessels of her brain. So, when the program acceptance letter came, it was a blessing to my family and me after a very difficult few months subsequent to the loss of our second child. Maybe someone “up there” was advocating for me. I figured that this experience would allow me to become a true professional in the healthcare field. We shall see. We did receive an additional blessing with our third child. Grayson was born a year after Bryce’s passing. I know what you’re thinking … and yes, I was told not to have any major life events during the program. But again, my wife and I are not getting any younger and, for now, they have grandparents to partake in their upbringing. Later that fall (of 2012), I began the rigorous DMI program at CCSF. 10 As the first semester began, my family and I grappled with the uncertainty of my father’s health. He was cared for in a rehab facility after suffering from multiple strokes. We still regularly checked on the quality of his care. But, his condition became increasingly bleak as the semester drew on. Ultimately, he passed away half way through the first semester. I needed to mourn quickly and get back on track. I heard some feedback from students ahead of me about the challenges of the second semester. It seemed as if my dad sensed that. Apparently, he was determined that his poor health would not be a burden to me while I was in the DMI program. He was leaving that duty to his grandkids that are now age four and two. With my wife working twelve-hour shifts at the hospital and additional per diem shifts at a clinic, it leaves me to pick up the balance of the household duties. Despite my packed schedule, I’ve found myself thinking about our personal losses and they sometimes weigh heavy on me. There are no extravagant birthday parties for the kids. We are content with small family gatherings to celebrate the milestones. Weekly ballet practice for my daughter takes up a little valuable study time. Every now and then a parent or teacher will dole out some guilt to my already heavy conscience. Preschools do their part in helping to develop some important skills, but parents are leaned on to fill in the blanks and work with their children when they are not in school. I have to pick and choose what’s most important for my family and me. In other words, I don’t read books to my daughter EVERY night but, dinner is on the table. My son’s speech was described as “underdeveloped” compared to other kids his age. So what? He’s two! He doesn’t have to take the SAT’s for a little while longer. Sometimes, my brat pack would be lucky to have as many as three baths in the same week. I was fortunate enough to be present for their first steps, first words, and first acts of defiance. Otherwise, that is what smart phones with cameras are for. My Minions tax me for the energy that I wish I had. I’ve managed to still stop and wipe a few runny noses and then continue studying. I am not saying that the road I have traveled is more difficult than the next student’s but, it has not been one of the easiest either. I am only one shade of gray from a box that contains many more shades. There are benefits of embracing these challenges. There are no excuses for the poor exam results or missed homework assignments. Sometimes it is necessary for me to have a longer exposure time to a particular subject before achieving the desired knowledge. Pun intended. But the instructions are clear. Do the work. Put in the time. The goals are in plane sight. The “goals” being to graduate, become licensed, become employed, and make the family proud. Allow me to introduce myself… Steve Carreon, student radiographer. CCSF RadTimes July 2014 1 2 3 My Clinical Rotation Experience by Dallas Fair First day on the job is always nerve wracking and my first day of clinical rotation was no different. I tried not to let the butterflies in my stomach get the best of me. I gave myself extra time to get to the clinical site, as I was not familiar with the location of the hospital and the surrounding area. I also wanted to allow myself time to look for parking. I did a trial drive through a few days before, but I was completely lost and had to rely on my GPS to guide me. My trial drive was during the afternoon and the scenery was different compared to the 6:00am darkness. I drove back and forth on one particular road a few times and thought I had better call the radiology department at the hospital to inform them that I got lost and will be late. Then I saw the hospital’s emergency sign. I managed to get to the radiology department at the hospital fifteen minutes before my start time. I felt like a wreck but managed to put on a brave, smiling face and I introduced myself to some hospital employees. I received lukewarm hellos following awkward moments of silence and the technologists went on with their routines. It seemed like everybody had a job to do and I had better find one quick if I was going to be a part of the team. Since I was a new student, I was expecting an orientation around the radiology department and maybe a description of the hospital layout upon my arrival, it seemed a tour might not happen today. It was every clinical student’s nightmare, standing around not knowing what to do or where to go or who to talk to. It was only 7:30 in the morning and I could not wait until 3:30pm when I would get to go home. I decided right at that moment that if I was going to make it through that day, I had better attach myself to a technologist and shadow him/her 11 during exams. I asked to shadow one of the technologists who was about to do the morning portable rounds. We made small talk as we wheeled the portable x-ray machines to the patient rooms. When we got to the first patient’s room, I went into this automatic mode of introducing myself as well as the other technologist, asked the patient for her birthday, and reconfirmed her last name for identification. I proceeded by letting the patient know that we were there to take her chest x-ray. Next, I continued on by positioning the patient upright for an AP Landscape portable chest x-ray. The other technologist assisted me and we took the exposure. It was not until we had finished the portable round while heading back to the radiology department that the technologist made a comment that I was not new to doing portable x-rays and my work was good. I had forgotten that I was a new student and had not earned the trust of the technologists yet. At least I had earned the trust of one technologist that morning. One tech down and how many more to go? When we arrived back in the radiology department, my clinical instructor welcomed me with open arms. She was just arriving at the hospital. There were more employees arriving now and I was introduced to all who were there. As it turned out, the staff I encountered earlier were from Ultrasound and Interventional Radiography. The technologists I was now meeting turned out to be very nice and friendly people. My clinical instructor was called into surgery so the assistant clinical instructor gave me an orientation tour of the radiology department, the emergency room, and the general hospital floor plans. He was extremely helpful in explaining department procedures and protocols. We got called back to radiology as the cases were piling up. The technologists were busy taking exams and I offered to help but was told to just stand aside and observe. Observe I did. Standing aside and observing the orderly chaos of the activities around me, I noticed a lot of foot traffic between of the x-ray room and the cassette reader which is located in the hallway. That’s when I realized the system they use at this hospital is the CR system and not the digital system. I thought of the inconvenience of having to run out of the x-ray room to process a CR cassette after each exposure, not to mention the inconvenience of having the patient wait in the x-ray room alone while the cassette is being processed. It took longer to finish one study in my new clinical site than at my home base hospital because of digital system efficiency. With the digital system the technologist does not need to leave the room because the image is displayed on the screen shortly after the exposure is taken. The technologist is in the exam room with the patient the entire time, which is important for patient safety. In spite of having to process each cassette in between, the technologists moved quickly and efficiently. I was very impressed with how well the technologists set manual techniques. Their exposures always fell within the acceptable exposure range. I cannot say the same for me. As I was observing, I took out the technique chart that I previously made for myself and would try and remember the techniques for the study of a body part at a certain kVp and a certain mAs. To my surprise, the levels that rendered diagnostic quality images at my home hospital were far less Continued on page 12 CCSF RadTimes July 2014 4 1 2 3 than what was used at my current hospital. My setting for kVp was always acceptable but my setting for mAs would have consistently been underexposed had an exposure been taken. I was told I would need to use more mAs. It was not uncommon to see a lateral L-spine study with 80kVp at 250mAs. The thought of using a technique with such high mAs scared me, but the image came out within the acceptable exposure range. I had to train myself to change my way of thinking about utilizing more mAs. Within the first week I was given studies to do on my own. I made another technique chart to use on the machines for this hospital. They said that every machine has its own personality. I soon found out what they meant. The center marked line of the x-ray field is not always in the center. The detent track squeaks loudly and the detent indicator light is not always illuminated. These are just a few quirks of the machines that I had to learn to maneuver. Now one month later, I still feel uneasy sometimes when setting a higher mAs when I know that much less mAs can still render diagnostic quality at other hospitals. I kept reminding myself that I am working with the CR system, which requires more mAs than the digital system. The technologists all seem to be comfortable with higher techniques. I’m still learning to be a technologist, so for now I just have to put my apprehensions aside and follow their lead. My CT and MRI rotation is not for another four weeks. With what I have learned so far in CT class, I feel that I will understand more when I do my CT rotation at clinical. For now, the workload is more than enough for me to handle as I’m only in clinical two days a week. I’m still trying to learn about the hospital billing and processing computer system. I’m in a whole new hospital with a whole new computer system to learn. Although I am stressed out at clinical, I am grateful for the opportunity to work with the CR system, which requires me to master my manual techniques. I am not there yet but each day at clinical brings me closer to a working confidence level. 12 A Lesson Learned By: Sandy Zhou It all happened so fast. I stood there, not knowing what to do. I just stood there. “Call a code,” the anesthetist shouted. Someone, I can’t remember who, asked, “What’s the code number?” “555… dial 555, code blue,” the attending technologist answered. “Go get the crash cart, the pediatric crash cart. Location of code blue at XXX hospital XXX campus, CT department, first floor, 8 month old male.” On the overhead: “Code blue, CT.” Again, “Code blue, CT.” A doctor rushed in, asking, “What happened?” Then the anesthetist shouted, “Cancel code, cancel code. He’s breathing.” I started to tear up - tears of joy, of course! What an experience! I never thought I would actually experience a code blue. As a student, I learned what a code blue is and what needed to be done when a code is called, but I never paid too much attention when these lessons were given. On the first day at the clinical site, the lead technologist gives the new students a tour of the radiology department. The location of the crash cart is always highlighted during the tour. Now I know, being familiar with the location of the crash cart is much more important that one would think. It is not something to just acknowledge and then forget. The students really need to pay attention. This is serious business. I am a 4th semester radiologic technology student at City College of San Francisco (CCSF). After this semester ends I will become an Intern. At CCSF that means that my didactic education is complete and I will then be in the hospital 40 hours per week for 6 months. By the end of this semester I will have been in the program for almost two years but I will not be done. CCSF is longer than all the other programs in the Bay Area and I’m sure glad that it is. I have so much more to learn. By the end of this semester I will have completed about 810 clinical hours. I still have about 1000 hours left but it will be concentrated on perfecting radiographic procedures not bookwork. Finishing up my 4th semester, I should be a confident clinical student at any hospital. Yet, when the code blue was called, I stood there, not knowing what to do. The code lasted less than 10 minutes, but it was one of the longest 10 minutes of my life. This is how it started. A head CT scan was ordered, and the child, a boy, was to be sedated. When the boy’s mother carried him into the CT room, his eyes grew large as he looked around the room. He must have been wondering about the big, scary-looking machines. His mom then placed him on the CT table, and a mask was placed over his face by the anesthetist. He went to sleep within seconds. After his mother kissed him good night, she went to the waiting room with the child life support assistant. What is amazing to me is how, within a matter of minutes, everything can change. Most people who enjoy hospital themed television shows have probably seen a code blue on television. However, unless you have actually experienced one in real life, you can never really understand the intense stress and desperation that is present during a code. I certainly feel lucky that my first experience was at a hospital with a dedicated and intelligent team of health care providers. They brought the patient, a beautiful baby boy, back to life and earned my utmost respect. Wow! I am actually part of this team. I just learned a very valuable lesson…..to be present at every moment – in class, during orientation, and every moment that I am in the clinical environment – to pay attention to every detail no matter how small. There could be a life depending on me and I intend to be sure I give the best care possible. My advice to all students is to PAY ATTENTION to what you are learning. Everything being taught is important to your new career and to quality patient care. Your patients are depending on you to know what to do. PAY ATTENTION! CCSF RadTimes July 2014 1 2 Let’s go BACK to the FUTURE! By Diane R. Garcia, MS, RT(R)(CT),CRT The latest Radiologic Technology Certification Committee (RTCC) Meeting was held in Los Angeles on Wednesday, April 2, 2014. After approval of the previous meeting’s minutes the agenda included the following: • • • • • • • • • Status of Prior RTCC Motions Legislative and Regulatory Updates Whole Body Composition & Scope of X-ray Bone Densitometry Permit Fluoroscopy Examination Update QA/QC Regulation Inspection Experiences Consideration of Eliminating Fluoroscopy Permit for CRTs Radiation Protection in the Cath Lab: 1950s Technology Jeopardizes Today’s Medical Professional Agenda for RTCC Subcommittee Scope of Practice for Radiologic Technologists Consideration of RCIS Regulatory Fluoroscopy Exception The minutes of this meeting will not be available until after they have been approved at the October, 2014 meeting. The most important part of this meeting, from my point of view, was the part of the agenda that had to do with allowing non-radiology personnel the ability to operate fluoroscopy equipment without being CRTs. Deregulating radiologic technology is very disturbing to me and many others including the radiologists on the RTCC as evidenced by the way they voted on the motions made at this meeting. An important motion was made by Radiologist, Dr. Bonna Rogers-Nuefeld, which was voted on and passed by the RTCC to rescind the previous motion that was passed in the October 23, 2013 meeting. This previous motion made by committee member Dr. Dale Butler (non-radiologist physician) and seconded by committee member Dr. Todd Moldawer (non-radiologist physician) stated the following: “The committee members approved that the RTCC support the development of a limited permit, or an exception to existing regulation, that would allow an individual, with specific education and experience to be defined or determined, the ability to position the patient or the equipment under the personal immediate supervision of the S & O, while x-rays are not being generated.” (Oct. 23,2013 RTCC meeting minutes) Though this motion states, “…while x-rays are not being generated,” it is well known that once the barrier is lowered, operating the equipment with the beam on will become common practice of those who obtain said permit. It has even been said at the last few RTCC meetings that currently Cath Lab personnel, specifically Registered Cardiovascular Invasive Specialists (RCIS), have been defying California Laws and operating fluoroscopy equipment in many facilities. I am aware of a few in the San Francisco Bay Area that, at present time, do not even employ any CRTs in Cath Labs so who do you think is operating fluoroscopy equipment (illegally) in those departments? I wonder if the patients know that they do not have qualified personnel potentially setting technical factors and operating fluoroscopy during their procedures. As a matter of fact, it is widely known that most RCIS personnel have only on the job training with little to no radiology education at all. Even those from an accredited program have only minor questions on their board examination regarding radiation or fluoroscopy and a person taking that exam can get all of those questions wrong and still be qualified as an RCIS. Are they qualified to operate and understand fluoroscopy equipment? Back in 1969, the Radiation Health Branch (RHB) made the enlightened decision to create the Radiologic Technology Act which specified that only those educated in a particular way could operate radiology equipment for the purpose of irradiating human beings. To be exact, “The Legislature finds and declares that the public health interest requires that the people of this state be protected from excessive and improper exposure to ionizing radiation. It is the purpose of this chapter to establish standards of education, training, and experience for persons who use X-rays on human beings and to prescribe means for assuring that these standards are met.” This comes from the Health and Safety Code (HSC), Division 104. Environmental Health, Part 9. Radiation, Chapter 6. Radiologic Technology, Article 1 Declaration of Policy, Section 114840. (RegsToday.com) At the latest RTCC meeting on April 2, 2014, a motion was passed to consider non radiologic technology personnel to possess the ability to operate fluoroscopy equipment in the surgical suite and the cardiac catheterization laboratory (Cath Lab). During the discussion that ensued, it was even suggested (though the motion did not include this) that any person in the IR suite should also be allowed to operate the fluoroscopy equipment. This motion was voted on by the committee. The nonradiologist physicians all voted in favor of this motion while the radiologic technologists and the radiologists all voted against it. Unfortunately the non-radiologist physicians outnumbered those of us (Radiologists and CRTs) whose entire education revolves around radiology. I now fear that the non-radiologists are trying to bring the state of California back to 1969 when anyone was allowed to operate radiology equipment with little to no Continued on page 14 13 CCSF RadTimes July 2014 1 3 2 education at all. The argument made by the non-radiologists is that the physicians who supervise in fluoroscopy are capable of monitoring all aspects of the fluoroscopy procedure and the other personnel do not need to be licensed CRTs. The physician will have complete control over verifying all technical factors and other important elements of the procedure. In theory, this may be true, but in my 35 years of experience working in surgery, general fluoroscopy, and IR, this is absolutely not true in practice. Though the Cath Lab traditionally does only cardiac procedures, this is not the case any longer. They are also doing interventional procedures which makes the deregulation even more concerning. To conclude, do we really want to return to 1969 or do we want to go back to the future? Do we want to join the other states that have no regulations regarding radiology? As a technologist of vast experience both in practice and in education, I personally understand the risks involved. Are we going to allow this deregulation of our profession or are we going to fight for our patients? AND I remind you that YOU may also become a patient one day! Let’s go BACK to the FUTURE! Diane encourages you to get involved today! Resources: Approved RTCC meeting minutes of October 23, 2013 RegsToday.com; California Law http://ca.regstoday.com/law/hsc/ca.regst oday.com/laws/hsc/calawhsc_DIVISION104_PART9_CHAPTER6.aspx 14 HOLD YOUR BREATH ... BREATHE Eric Holmgren There is a moment in many x-ray exams when you ask the patient to stop breathing. Preparation is complete: you have identified the patient, confirmed the order and its clinical indication, set the technique, shielded, angled, and positioned. Now, just before you make an exposure, there is a pause as breathing is suspended. Full stop in this moment allows you to capture a clear image without motion. As I complete the City College of San Francisco Diagnostic Medical Imaging Program, I find myself in a similar moment. In a scant six weeks internship ends for me and my cohort. Our education will be completed and then evaluated via the ARRT exam. Of course, we hope to soon be working as radiologic technologists and we know that our education will be ongoing. HOLD YOUR BREATH ... pausing in this moment to mark, celebrate and reflect on this accomplishment - full stop before moving forward - can add clarity to the picture of the path and our place on it. Personally, it is clear that this accomplishment is not mine alone. Though I dedicated myself and my hard work to this program, I know that the success I enjoy is also due to the opportunities I have been afforded, the support I have received and the friends I have made as a result. It is difficult to imagine a more comprehensive preparation for this career than that which the CCSF Diagnostic Medical Imaging Program provides. I am grateful to the entire faculty for not just teaching radiologic science and technical proficiencies, but also illuminating a more complex and integrated picture of modern health care and compassionate patient care, all while shouldering the stress and uncertainty of CCSF accreditation in a manner that minimized its impact on students. At City College, I was encouraged to acquaint myself with two of our professional societies. My participation as a student member of the CSRT and the ASRT has deepened my appreciation of the world I am entering, how much there still is (and will always be) to learn, and issues that affect our profession and our patients in an evolving health care environment. Being able to attend meetings of the Radiologic Technology Certification Committee, I witnessed lobbying to issue fluoroscopy permits to personnel other than CRTs to operate fluoroscopy in the operating room, catheterization lab and interventional radiology suite, without formal diagnostic medical imaging education. The RTCC is the advisory body to the Radiologic Health Branch of the California Department of Public Health. Their recommendations will affect the value of our education and expertise, the necessity of RTs, and - most critically - the safety of patients and health care workers. The CSRT is a countervailing voice in California on this issue and it lobbies for educational and patient safety standards locally. CSRT joins the efforts of the ASRT on a national level through support of measures like the CARE bill. HOLD YOUR BREATH ... I know my future includes ongoing membership in these two important organizations. Whether or not we attend their continuing education conferences, our membership dues support the work they do on our behalf. Finally, my clinical education has been rich and diverse. The encouragement and mentoring that I received from scores of techs, radiologists and others at the various campuses of my two clinical hospitals have been profound. All have helped me hone my skills as I developed them. The tech I have become is a reflection of their skill and innovation. In addition to general x-ray, my internship has included rotations in surgery, trauma, ultrasound, fluoroscopy, MR and IR. This has given me a clear sense of the profession and the opportunities that await me. HOLD YOUR BREATH … I am fortunate that throughout this journey I have remained certain that this is the right path for me. I embrace the transition from student to colleague, knowing that my education continues and we all can learn from one another. I welcome the day that I find myself working with a new clinical student practicing their fledgling skills. ... AND BREATHE. CCSF RadTimes July 2014 1 Migration South for Vacation by Rhonda Boulland There’s no hiding from the truth. My friend and classmate, Dallas Fair, and I took our chances on scoring two standby seats on a packed jet headed for LAX one Friday evening in early May of this year. We were after one thing: vacation days to use during our internship. The deal presented to our class was three vacation days in exchange for making the journey down to southern California for the CSRT Spring Seminar. I don’t know about you, but I’ve never worked for six months straight without a vacation so I knew what needed to happen. Honestly, our chances of getting seats on the airplane were not much better than finding parking in Union Square, but we headed into the pandemonium of SFO to try our luck. Score! Big thanks to my travel partner for a trip down to the land of palm trees and Botox. The next day after a mere four and a half hours of sleep, we fueled up on Starbucks and made our way to Northridge Hospital. I couldn’t stop thinking about my only reference to Northridge. Earthquakes! Dallas and I arrived and tried to prepare ourselves to sit and listen for the balance of the day. We were in the company of about fifty other attendees. Dallas and I were the only ones representing CCSF. The first speaker discussed how multiple regulatory agencies had visited his hospital and how unnerving their visits were. A few of the agencies that dropped in were the FDA, RHB, and JCERT. And what do these agencies want radiology managers to fill out? Surveys. After several lengthy questionnaires, the speaker was happy to report that there were no findings. The entire department could breathe easy and get on with their busy workload. Next we broached the incredibly relevant subject of overexposure in CT, particularly in perfusion scans done using a head CT. This type of scan would be common for a stroke patient for example. At one particular hospital 40% of the patients receiving this type of scan on a repeat basis had hair loss in the shape of a ring around their head. The overexposure occurring with this particular type of scan went unnoticed for 20 months before changes were made. The “Ring Effect” is happening to patients all over the country. Senate bill 1237 and Assembly bill 510 were passed to address dose reporting in CT, but this is not an official policy that must be followed by all radiographers yet. The discussion moved to adjusting protocols in CT for pediatric and pregnant patients and how the dose limits are not always followed. There were some real life examples given of pregnant women and children being given dozens more times the dose they needed. One baby boy, in particular, was given hundreds more times the necessary dose and his doctor anticipates that the boy will develop cataracts as well as other unfortunate manifestations due to the high exposure of ionizing radiation. I could see everyone in the room shaking their heads and shuddering at the thought of being the tech that made such a grave error. This is likely the number one concern for most radiographers; making a mistake that has a negative impact on a patient. For the hundredth time since I started this program, I vowed to be super-duper-exceptionally-unbelievably-astonishingly careful both in my internship and beyond. Dallas and I had not yet had the opportunity to give each other feedback about our thoughts on the seminar, but as the speakers were making their presentations and sharing their ideas about how to help us become more accountable and more knowledgeable techs, Dallas and I exchanged approving glances. I could see the element of delight and surprise on Dallas’ face and he witnessed the same on mine. Maybe we would get more out of this jaunt to SoCal than a few vacation days. The next subject was about the dangers of an MRI quench. A quench is often signaled by a loud bang and a hissing sound from escaping gas. It occurs when the liquid cryogens that cool the magnet coils boil off rapidly, which results in helium escaping very rapidly from the cryogen bath. The quench duct can reach temperatures of 470° below zero and will freeze anything around it, including you or me. Techs need to be aware of where the quench duct is located at their hospital. If the scanner quenches it is very dangerous to be within a few feet of the duct because the extreme low temperatures of the helium gas could cause frostbite or burns. Hospital employees should be able to identify the duct’s location and what type of barrier, if any, is around it. The white smoke-like gas that comes out of the vent could prompt a visit from the fire department. If proper signage isn’t present near the quench duct then fire department employees could be hurt if they go beyond the barrier. How does your hospital handle this potential hazardous situation? As the day progressed I was increasingly able to identify with Pooh Bear and his rumbling tummy when my attention was again turned to CT. It came as surprising news to me that CT techs don’t necessarily have to be certified or licensed at present time in the state of California (aside from their diagnostic license), but that will be changing soon. CT scanners have to be “accredited” in each location that they reside in because of the law passed in July of 2012 mandating dosage reporting. It would follow that techs be required to pass a board exam and hold a license in order to run an accredited scanner. The only appropriate response to the aforementioned next level of laws around CT licensing should be favorable by the radiographer community. Why? Because nurses and physician’s assistants want to take over certain aspect of our jobs. With every law that’s passed requiring CRT’s to obtain a specific license to run a specific piece of equipment then hopefully we are solidifying the fact that education is paramount when working with ionizing radiation. Maybe one day California will require CRT licensure to accompany a bachelor’s degree. Can you see why that would be a move in the right direction for our industry? The speaker also discussed the Image Gently Campaign (imagegently.org) and how educating radiology staff about how “one size does not fit all” can lead us to true patient care. Can we adopt the philosophy that we are our patient? When we become every patient’s advocate than we, as a whole, are becoming respected professionals that will not let other hospital employees take over our jobs. Continued on page 16 15 CCSF RadTimes July 2014 1 2 Migration South for Vacation CONTINUED Break time! Dallas and I took a few minutes to talk about the day’s topics and we were both brimming with enthusiasm. Every speaker had made an impact on us. We were furiously taking notes and trying to absorb every nugget of information that was presented. This seminar was turning out to be a rich surprise that fueled ideas and chatter amongst all who attended. As a testament to how important dose management is, we welcomed a new set of speakers to the podium and continued the discussion about using appropriate protocols to avoid overdosing the patient. One of the speakers, Tim Gustafson, was so determined to purchase a CT scanner for his department that administered the lowest possible doses to patients that he brought a phantom torso on a business trip to visit various CT manufacturers. Mr. Gustafson showed up at companies such as GE, Siemens, Zeam, OEC, and Toshiba with the phantom in tow. Like a teacher who administers a pop quiz, he sparked quite a stir when he asked if he could do an unscheduled abdomen scan at each of the companies being considered. One brand of scanner stood out as the low dose leader. For the type of scanner that he was in the market for, let’s just say the winner’s name rhymes with “Neiman’s”. Enough said. There were many more speakers, each with the background and devotion to their subject to keep the group fully engaged. We learned about the ABC’s of a chest x-ray, acromegaly, Cushing’s syndrome, legislative trends that affect our future, acute CT brain imaging, and finally cultural diversity within imaging departments. The diversity discussion ruffled a few feathers and sparked more input from the group than any other subject. The speaker was trying to make a case that the U.S. isn’t a melting pot, but a fruit salad and we should treat one another according to the type of fruit we are. In other words: don’t treat every patient the same. Hmmmmmm. Doesn’t the fruit in a fruit salad always remain firmly an apple or firmly an orange in salad after salad? From my perspective, with each generation we combine the characteristics and traditions of far-away lands to unite and fuse into a new family unit. With all due respect, we are a melting pot and not a fruit salad. That being said, I do agree that every patient should be treated differently, but always with one idea in mind: I am my patient and I will do everything in my power to protect my patient. The afternoon wrapped up and Dallas and I headed to LAX to try our luck at once again scoring a standby seat. We both felt like the seminar was a total bonus and an unexpected bounty of pertinent information. And just when we felt like our luck may have run out, we received a couple more gifts … the last two standby seats on the airplane. ☺ Diary of a 4th Semester Student by Rhonda Boulland It’s Thursday and my alarms both sound at 5:45am. I turn them both off and I’m surprised that my alarms wake me up and not my kids. My hospital shift is 8:00am to 4:30pm and I’ve rotated to a new hospital this semester so I’m learning new exam protocols, new equipment, and trickiest of all I’m learning how to work with a new set of radiographers. I’m tired on this particular Thursday because my four year old son is sick and woke me up several times during the night. I wonder how my husband can sleep through the coughing, night terrors, and crying from my kids?! No time to ponder such absurd questions; I need to get ready and go. An hour later as I’m packing my lunch and getting ready to leave, my sons both emerge from their bedroom. I’m overjoyed that I can spend a minute and thirty seconds with them before I race out the door. I ignore their fussing and pleas for milk and television as I pat their thin, blonde hair that’s sticking out in all directions. At one and four years old, they both still view me as someone who can meet their every need at every moment. At this moment I view them as the two most precious little bundles of love I could ever imagine that are about to make me late. Now my husband is emerging, eyes squinting, and still half asleep. I tell him “we’re out of vegetables because I made a salad for lunch so you’ll have to go to the store before dinner tonight. Don’t forget, I have class tonight so you have to pick up the kids. Wait … Levi was up all night coughing and he feels feverish. On second thought, you need to stay home from work because Levi’s preschool director will flip out if you drop him off in that condition. Oh, and when you’re getting Henry ready for the nanny-share can you give her more diapers. She’s out. And don’t forget to put applesauce in Henry’s lunch, he’s been constipated for two days. Also, check out Levi’s eyes. They look so red. I think he has pink eye. Okay, bye babe, love you”. My husband gets back in bed and pulls the covers over his head and pretends to cry as I walk out the door. (continued on page 17) “When the stress becomes overwhelming I exchange it for gratitude.” 16 CCSF RadTimes July 2014 2 It’s now 7:05am and I’m out the door a few minutes later than I’d like. I debate whether to listen to NPR on my way to work or to listen to a recording of my instructor’s voice to prepare for an upcoming quiz. I can feel my anxiety level rise. I know I have a quiz coming up that I haven’t studied for so I listen to NPR for 10 minutes then listen to my instructor for the remainder of the drive. I park 7 blocks from the hospital to save $7 on parking, but the $13 per day charge is another small added stress to the huge financial burden of living off of loans and one income while in the program. I stuff the financial worries in a mental file that I try not to open very often. I arrive at the hospital and after cleaning and stocking are complete it’s time for the first x-ray. The tech on duty tells me to get the order and the patient. I position the patient for an AP knee x-ray by angling the tube 5 degrees cephalad. Collimation, marker, and lead are all in order. As I turn to dart behind the lead wall, I realize that my clinical instructor and two senior techs have been watching my every move. Clearly, I’ve done something wrong. I’m staring at two puzzled faces and one slightly annoyed face. Note to self: this hospital doesn’t want an angle on the AP knee. I erase from my memory nine months of clinical instruction at my previous hospital along with what I’ve learned in my positioning class and replace it with this new nugget of information. My mental hard drive is being reformatted with every move I make today and for the rest of the semester. It’s 9:00am now and I head over to fluoroscopy where I’m scheduled to be for the remainder of the day. I love fluoro because it feels like I’m part of a little clinic. I enjoy working with the radiology residents who are also on a rotation as well as the speech pathologists who come in for swallow studies. I always pick up new tidbits of information listening to the residents talk to the patients. Our first patient will have a barium swallow study and an esophagram. The tech sets up while I watch and I notice the similarities and differences in the set up procedure to my base hospital. The chatty speech pathologist comes in and makes small talk with the tech while she sets up. Our patient comes in and the study begins. I try to take in every detail in hopes of getting a competency signed off the next time this type of exam comes up during my rotation. At this point I’m just trying to figure out when to put lead on, where to stand, and how not to be annoying to the tech, resident, and speech pathologist. The esophagram is over and the doctor fills the patient in on what he has just witnessed. I’m wondering if there will be overheads, but the tech motions for me to help the patient off the table and clean the room. I guess the study is over! Our last exam of the day is a hysterosalpingogram. A female tech comes in from the x-ray department to take over. I have been signed off on this competency so I set up the room accordingly. The tech makes a few adjustments and we’re ready to get the patient. I have a list of questions ready to ask the patient and I get her consent forms in order while she’s changing into a gown. The patient nervously sits down. I make notes for the resident as I ask the patient several pointed questions that will give the doctor some clues as to the patient’s condition when he arrives. I explain the exam and I’m extra calm and warm in my demeanor in hopes that the patient will feel a little less anxious. During the exam I ask her where she’s from and about her job to get her mind off the catheter that’s being inserted into her cervix. I rest my hand on her shoulder and tell her to remember to breathe at certain times during the exam. At the end of the study the patient thanks me profusely and tells me that I made the exam a “piece of cake”. This makes my day and is the equivalent of a friendly reminder about why I went into this field. The clinical portion of my day ends at 4:30pm and it’s time to commute to school for my night class. I’m exhausted. I call my husband to check in. As soon as our kids realize that they don’t have dad’s undivided attention they begin to fuss. Trying to talk is futile. I realize that I have a quiz in my class tonight. The wave of dread washes over me. I know this feeling all too well. I’ve reviewed fifty pages of the hundred page chapter. For the remainder of the drive my thoughts vacillate between my odds of passing the quiz and what I can find to eat at Whole Foods for less than $6. With no time to change out of my scrubs, I arrive at 6pm on the dot for class. Two and a half hours go by and it feels like ten. Now it’s time for the quiz. Why does the vascular system of the liver need to be so complicated? The quiz is significantly more difficult than I anticipated, but the “I’m always end of the quiz means the end of class. It’s time to go home at last. heartbroken when another day has gone by and I haven’t done any of the things a parent longs to do with their children.” My husband is asleep on the couch when I walk in at 9:30pm. The house smells like the dinner he prepared. There are clothes, shoes, toys, sippy cups, art projects, and pieces of mail everywhere. I go into my son’s room. They are sleeping so perfectly. I miss them so much it hurts. I kiss their foreheads and watch them breath. I’m always heartbroken when another day has gone by and I haven’t done any of the things a parent longs to do with their children. My husband is awake now and I fall onto the couch next to him. He asks how my day was. I’m too tired to speak. He already knows this and doesn’t press me for a response, but just rests his hand on mine. I simply could not be in this imaging program without his support. He is the reason it all works. When the stress becomes overwhelming I exchange it for gratitude. Gratitude has never failed me during this journey. I could say that I’m lucky, but luck doesn’t lend itself to the work that has been done so I’m just thankful each and every day for my incredible husband, my two boys, and the strength to get up and do all over again tomorrow. ☺ 17 CCSF RadTimes July 2014 1 2 Benjamin Franklin once said, MRI Contrast Complications "The only things certain in life are death and taxes." Although some people try to avoid taxes, death is inevitable. Early death, however, can be avoidable, by Roel Atanacio particularly the ones caused by diagnostic procedures. Like anything else that enters our bodies (food, water, drugs), contrast used in MRI can also cause our body to have some unkind reactions. The most widely used contrast for MRI is Gadolinium based contrast agents (GBCA). Gadolinium is specifically used for MRI because of its magnetic properties. This agent is introduced intravenously but can cause side effects and reactions ranging from mild to severe. In fact, GBCA has been linked to many adverse reactions such as headache, nausea, and dizziness and in rare occasion anaphylactic shock [8]. An even more rare but very severe adverse reaction, one that effects people with impaired renal function and is a potentially fatal complication is called Nephrogenic Systemic Fibrosis or NSF for short. Nephrogenic systemic fibrosis is a rare disease that causes fibrosis of the skin and multiple internal organs such as the heart, kidneys, and lungs. NSF causes patches of thick and hardened tissue [1]. Patients with NSF have also experienced joint pains, tight muscles and yellow spotting in the whites of their eyes. This illness only affects those with weak renal function and is usually paired with the introduction of gadolinium for MRI [2]. NSF starts in the lower extremities and makes its way up through the thigh muscle, then to the abdomen and all the way up to the thorax. Within weeks, many patients affected by NSF find themselves dependent on a wheelchair. This disease has no cure and is progressive and can cause death. The most effective method in controlling NSF is trying to improve the patient’s renal function [4]. Although introduction of gadolinium is not the only way patients end up with NSF, through the increasing number of uses and requests for MRI studies, gadolinium has become one of the most common ways of contracting NSF in patients with impaired renal function [3]. Patients who have had liver transplants in the past are also at risk of developing NSF when given GBCA. The Food and Drug Administration has approved the use of five GBCA’s and all five have been linked to reports of NSF. Although approved, the FDA does warn the public of the risks [4]. It is important to note that although this is a very severe, life changing and potentially life ending complication of this particular MRI contrast, it is very rare and uncommon for a patient to contract this disease from GBCA due to lab screening and questionnaires that the patient must complete before they are deemed acceptable to proceed with an MRI study with use of GBCA [6, 5,7]. Just like in many decisions that we make in life, we must weigh the risks and benefits. Gadolinium does come with many complications including a major one in NSF; however, these complications including the minor ones are not common. There are many tests patients must pass that limit risks of such reactions. As a student in diagnostic imaging, I am learning that there are many things that can go wrong… especially in the hospital setting. We, as technologists, have the responsibility to double and triple check everything that we need to know about each patient before proceeding with an exam whether it is MRI or general x-ray because even if we do not spend a lot of time with each patient we can still have a major impact on their future. Work Cited [1] Mayo Clinical Staff. June 17, 2013. Diseases and Conditions: Nephrogenic Systemic Fibrosis. Retrieved Feb. 23, 2014. From http://www.mayoclinic.org/diseases-conditions/nephrogenicsystemic-fibrosis/basics/definition/con-20036311 [2] Marie Cheour. Oct. 11, 2013. Side Effects of MRI with Contrast. Retrieved Feb. 23, 2014. From http://www.livestrong.com/article/178926-side-effects-of-mri-with-contrast/ [3] Jeffrey Schlaudecker MD. And Christopher Bernheisel MD. Oct. 1, 2009. Gadolinium-Associated Nephrogenic Systemic Fibrosis. Retrieved Feb. 23, 2014 http://www.aafp.org/afp/2009/1001/p711.html [4] Questions and Answers on Gadolinium-Based Contrast Agents. May 2007. Retrieved Feb. 23, 2014. http://www.fda.gov/Drugs/DrugSafety/DrugSafetyNewsletter/ucm142889.htm [5] Todd DJ, Kagan A, Chibnik LB, Kay J. Cutaneous changes of nephrogenic systemic fibrosis: predictor of early mortality and association with gadolinium exposure. Arthritis Rheum. Oct 2007;56(10):3433-41. [6] Guidelines on the Administration of Intravenous Gadolinium-containing Contrast Media. Sept. 9, 2011. Retrieved Feb. 26, 2014 http://www.radiology.ucsf.edu/patient-care/patientsafety/contrast/gadolinium-policy [7] Noah S Scheinfeld MD. Feb. 7, 2014. Nephrogenic Systemic Fibrosis. Retrieved Feb 22, 2014 http://emedicine.medscape.com/article/1097889-overview#showall [8] Dr. Maurice Molan, Prof. Stacy Goergen. May 1, 2009. Gadolinium Contrast Medium (MRI Contrast Agents). Retrieved Feb. 23, 2014. http://www.insideradiology.com.au/pages/view.php?T_id=38#.Uw6I__RdWFB 18 CCSF RadTimes July 2014 1 2 Student Meets Incident by Joseph Carlisle The life of a student in any medical imaging program is likely to be full of obstacles and stress that must constantly be dealt with and overcome. Murphy’s Law basically states, “if anything can go wrong, it will, accidents happen, that’s life as we know it no matter how careful we are in avoiding them.” When we are in the hospital that rule has no exception. Despite knowledge, training, practice and even the watchful eye of a supervising technologist, accidents involving patients happen. As a student, there are few situations more stress inducing than having an incident involving a patient. However, it is immensely important that one takes responsibility for these accidents, learn from them and continue to work after the fact. As students, we cannot let incidents negatively affect our performance while in the hospital. My personal experience with this circumstance was minor according to the supervising technologist, but the patient didn’t think so and this ultimately caused me grief. Imagine a clinic site in an orthopedic / sports medicine facility with some of the latest equipment you could imagine. The site is an outpatient clinic and as one would expect, it is extremely busy from day to day. Over the short span of time I was there, I could see just how great the pressure is that radiographers are under. The many physicians at the facility have high demands from a small department of technologists. These doctors expect their radiographs to be done quickly and given promptly back to them. While this concept is not uncommon at other clinics, I could see that these RTs were stretched a bit too far. During one such day, I was working in the sports medicine side of the clinic, and as expected, it was a busy day and everyone was rushed to some degree trying to get patients in and out as quickly as humanly possible. A female patient comes in with a history of bilateral knee replacement. She had surgery about a year prior to this exam. The appointment was just a standard follow up before seeing her physician. After obtaining the standard patient information, I proceeded with the known protocol in the department for a bilateral knee examination. The last view done for this protocol is a Merchant View (Modified Knutsson method) to see the patient’s patella. The position requires a supine patient on the table with both knees flexed, the CR is angled and directed through the patellofemoral joint space 19 towards the IR which is placed at the end of the table beyond flexed knees and just in front of patient’s feet in a lateral cassette holder. As I previously stated, the entire staff and I were moving patients in and out of the clinic at a pace that is faster than safely recommended. In the course of placing the image receptor (IR) into the lateral cassette holder and securing it in place, I didn’t properly ensure that the top bracket engaged. The IR seemed as if it was secure and it didn’t move until the patient moved slightly which shook the table and caused the top of the cassette to fall forward and onto the patient’s shins. The patient reacted instantly complaining of great pain. The injury looked like a minor contusion, a small bump and bruise was present, but the patient began to claim that the bone had been broken and she wanted to see her physician as well as have additional images taken to prove it. Both the tech and I stopped everything and immediately assisted the patient, apologizing for this accident and assuring her that the bone was most likely not broken. The IR that fell forward was a GE wireless digital cassette which weighs about nine pounds. The full force didn’t seem to hit her shins however she still continued to complain. The tech and I both felt that the injury was minor and that the IR didn’t even hit her shins all that hard, certainly not enough to break a bone but that wasn’t for us to decide. We proceeded with filing the patient incident report as is required. As it is with most service industry jobs, the customer is always right and in the hospital the patient is the customer. In short order, the tech and I filled out the incident reports, explained everything to the supervisor, the sports medicine supervisor, and the patient’s physician then demonstrated what had happened. This is the point at which my nerves started getting to me because the stress and concern about the situation grew. Not knowing the outcome of what was to come felt overwhelming. While we were filling out the reports, I could hear the patient in the other room going on and on about how the bone must be broken and that it was the student (also saying my full name) who made the error. I could hear the endless ranting and raving about the whole mishap, which heightened my anxiety. My heart was racing with concern. Luckily, after the physician cleared the patient of serious injury, he said, “the bone was not broken, it’s a minor bruise and any further imaging is entirely unnecessary”. The patient left the clinic shortly following the physician’s verdict. Continued on page 20 CCSF RadTimes July 2014 3 The entire situation took over an hour to resolve and it wasn’t until the end of the ordeal that those in charge could finally speak to me about the incident. In my mind, I expected a scolding. Much to my surprise, that didn’t happen. Instead I was told by everyone not to worry about it. The error was an accident that had happened to other techs in a similar fashion. All that was requested of me was to learn from it, not to think much about it, and to move on from the incident. I was also advised to slow down a bit. In fact, everyone was extremely pleasant and understanding about the calamity and not at all concerned with my abilities. As much of a relief as this all was, I still had my own anxiety about the whole situation. In the back of my mind I was now worried about how the staff perceived me and my aptitudes. Will they trust me for indirect supervision or are they going to require me to go back to direct supervision on exams that I have been deemed competent to perform? What kind of example did I just make of myself? I felt terrible that I injured the patient even though it was a minor incident. The events started eating at me. The remainder of that day was difficult mentally, to say the least, but I did proceed with my job as was expected in spite of it all. The rest of this day, I moved a little slower and more deliberately but that was accepted and everyone understood. What an extreme learning experience this was and one that I had not expected to learn. Later that day, the weight of the incident still on my mind, I tried to do things that personally relieve stress for me. Then after a good night’s sleep, I found myself feeling better. I woke up with a new realization of what had happened. I followed all the proper procedures and took care of everything that was required and requested of me. I had learned a valuable lesson. "Why DMI?" by John Bates --Many people choose health care as a profession because of the satisfaction they get from helping others. From what I have seen, many of those same people gravitate toward nursing or various forms of therapy rather than diagnostic medical imaging. For me, DMI seems a better fit. I have previously done volunteer work with people recovering from addiction. From that I learned that I invested a lot of my own psyche in patient’s outcomes. That’s not a good thing, especially when a large majority of those patients don’t recover from their disease. Their failure to get well is often messy for them as well as their loved ones. I also have a friend who left her career in Respiratory Therapy because so many of her patient’s bleak prognoses took such an emotional toll on her. I can identify with her situation all too easily. So that is why I am pursuing a career in diagnostic medical imaging. It is fulfilling to know that I am part of a team that helps people have a better quality of life. I usually won’t see the final outcome. I am content to know in my heart that I play a small role in the recovery of every patient with whom I come in contact. I find that life as a student is filled with studying, homework, exams, and practicing positioning. This doesn’t leave us much time to reflect on the bigger picture. Dwelling upon the things we cannot change is useless. We just have to take responsibility for our actions and learn from our mistakes. We must be confident that we will learn from our blunders and not repeat them. In the end, it is the collection of experiences that will make us better techs. Though this seems like something straight forward and simple, not everyone can do it. Some students let their stress and nerves shake them to the core and dwell on their mistakes. Not advisable. I will leave you with the moral of this story from my point of view. Everything is a learning experience - the good and the bad. As a student, I must learn from both and advance to my goal of becoming a productive part of the health care team. Though this was a difficult lesson to learn, I am a better student because of it and will take this part of my education with me into the future and not make the same mistake twice! 20 DMI 62 Students prepare for summer clinical during an all day orientation in May. CCSF RadTimes July 2014 1 2 3 Second Semester Students Explore the 15% Rule By Vanessa Aycock One of the things that I find special about the Radiography program at City College of San Francisco is the hands-on labs regarding the physics behind x-rays. It’s one thing for a student to read about a law in a book and it’s a very different thing to be able to create an experiment and see the results of that law. In our case, eight students in the second semester Physics Class (50B) wondered if the 15% Rule could be used as a dose reduction tool. This rule is a guideline used by technologists for their technique. It states that in the diagnostic value range, as kVp is raised 15%, you can then reduce mAs by half in order to maintain the same overall exposure for a radiograph. This rule is often employed as a way to reduce time when the reciprocity law has reached its limit, but it can also be used to reduce patient dose by halving the mAs value since mAs controls the quantity of radiation being emitted by the x-ray tube. Our group project was inspired by the work of Dennis Bowman, educator and radiographer in Monterey, CA who advocates the use of technique charts with higher kVp ranges for CR and Digital Radiography in order to reduce patient dose. His findings state that such techniques can reduce dose by 66%. Intrigued by his research, our group created an experiment to compare patient dose as kVp was increased for both film and CR systems. At first, the task seemed daunting since we had to create an experiment that was achievable. I have to admit that our enthusiasm made it hard for us to limit the experiment to the one question, “Would we be able to reduce patient dose and still create images of diagnostic quality?” Initially, our biggest challenge was the complexity of getting 8 radiography students to take 25 x-rays in one hour. Our team 21 was comprised of four DMI students: Allison Correia, Luis Moran, John Bateman and Vanessa Aycock as well as four Radiation Therapy students: Liz Gonzalez, Charles Li, Antony Appedu and Michaela Nekovarova. For the experiment, each student had an assignment of either data keeping, film exposures, CR exposures or reading the dosimeter for the patient dose. Our key tool in our experiment was our beloved phantom, who proved to be an excellent patient as we took our 25 AP Abdominal x-rays during our experiment. Being novices as both radiography students and as researchers, our experiment did teach us to keep perspective as we encountered hiccups in our experiment. Some of these included learning how to correctly use the dosimeter, figuring out the best technique to create an optimal radiograph despite our phantom only having “some” of its abdominal viscera, and lastly, our natural ability to recreate almost every film artifact known to radiographers in our school darkroom. We also had some ideas about the outcome of our experiment. First, we expected a visual difference with our film series of exposures verses our computed radiography exposures. We expected both to become gradually underexposed due to decreased mAs but expected the film to produce a smaller number of diagnostic images as we increased kVp. We also expected that patient dose would decline as kVp increased due to the increased penetrating power of the beam, however, we did not think we could recreate Dennis Bowman’s results of 66% reduction in dose. Our experiment produced both visual and numerical data. As a group, we were able to analyze the images for their diagnostic quality and we were able to calculate the absorbed patient dose for each exposure. We produced five images each for film and CR, starting with our baseline of optimal image and increasing the kVp by 15% while halving the mAs for each successive exposure. Our results were surprising to us — in the end both film and CR produced diagnostic images for the first three “steps” of exposures in the experiment and then the fourth and fifth exposures were both underexposed and nondiagnostic. Additionally, both film and CR had a similar decrease in patient dose, which was a 57% decrease from the first exposure, to the third exposure. In a nutshell, a 30% increase in kVp resulted in almost a 60% decrease in dose. For our group, this exercise became more than a school project, it became a way to actually see that the guidelines and science behind x-rays really exist. This is a great way to gain understanding about the foundations of our field as student radiographers. Due to the extended capabilities of postprocessing in CR and digital systems, it has become easier for radiographers to overexpose their patients and not have the tell-tale sign of an overly darkened film. Recently, in starting my own clinical rotation, I am very fortunate to work with a group of technologists who passionately support ALARA. Even in the last week, I had the real-world experience of adjusting my hand technique charts to utilize a higher kVp with a lower mAs resulting in a new technique chart that helps me create diagnostic images while lowering patient dose. Without the opportunity at school to be able to test the physics behind the x-ray beam, I wouldn’t have gained the knowledge of how being smart about your technique can make you a better technologist for your patient. CCSF RadTimes July 2014







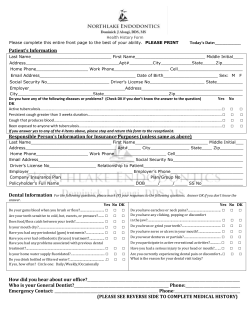




© Copyright 2026