
Reducing caregiver stress with internet
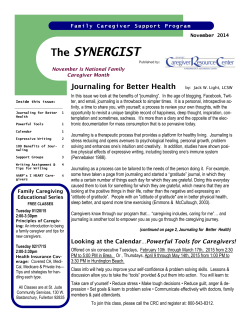
Review Reducing caregiver stress with internet-based interventions: a systematic review of open-label and randomized controlled trials Chunling Hu, Simon Kung, Teresa A Rummans, Matthew M Clark, Maria I Lapid Department of Psychiatry and Psychology, Mayo Clinic, Rochester, Minnesota, USA Correspondence to Dr Simon Kung, Department of Psychiatry and Psychology, Mayo Clinic, 200 First St SW, Rochester, MN 55905, USA; [email protected] Received 24 March 2014 Revised 4 June 2014 Accepted 25 July 2014 ABSTRACT Objective The high level of stress associated with caring for others with medical conditions has been recognized for some time. Reducing caregiver stress can improve caregiver quality of life as well as improve the care they provide to loved ones. This systematic review assesses the effectiveness of internet-based interventions to decrease caregiver stress. Materials and methods A comprehensive literature search of Ovid MEDLINE (1946–2013), Embase (1988– 2013), PsycINFO (1987–2013), and CINAHL was conducted using terms related to caregiver and internetbased interventions. Internet-based interventions involving informal caregivers in an open-label or randomized controlled trial setting were included. A pair of raters independently reviewed all published abstracts. Data regarding participants, interventions, and outcomes were extracted and, for randomized trials, methodology quality was also reviewed. Results Eight open-label trials met the review criteria: three showed positive benefit in reducing caregiver stress, four were partially positive (some outcomes positive, others negative), and one was a negative study. Sixteen randomized trials met the review criteria: six showed positive benefit, five were partially positive, and five were negative. There were no clear patterns as to the variables (such as study duration and complexity of intervention) associated with better outcomes, although earlier studies typically had more negative outcomes. Discussion Internet-based interventions were mostly effective in reducing aspects of caregiver stress and improving their well-being. Further studies to assess outcomes for caregivers and their recipients’ health, different technology delivery methods, and the cost of such interventions are needed. more apparent that caregiving for loved ones is burdensome, associated with fatigue, and impacts the health of the caregivers, therefore interventions are being designed to help address those concerns.3–7 Training and educational programs have been developed to provide support for the caregiver. These interventions have reduced caregiver burden and depression and improved well-being.6 8 However, due to the demands of caregiving, many of these face-to-face programs are inaccessible to caregivers. Therefore, technology-based interventions utilizing telephones, mobile phones, videophones, computers, and the internet are being developed to try to improve the caregiver’s ability to access help.4 In 2012 it was estimated that there were 2.4 billion internet users worldwide, with 274 million in North America.9 Internet usage, which provides people with abundant information and convenient ways of communicating, has become a regular activity of daily life. Internet-based programs have been shown to help people make health improvements such as smoking cessation or weight loss.10 11 Such programs have the advantage of being accessible 24 h a day and 7 days a week. Given that internet-based applications have been used to benefit patients with chronic illness, our research question was to find similar applications but with the target audience being caregivers. Surveying this field can help guide future application development. In this systematic review we identify open-label trials and randomized controlled trials (RCTs) of internet-based interventions to reduce caregiver burden. MATERIALS AND METHODS OBJECTIVE To cite: Hu C, Kung S, Rummans TA, et al. J Am Med Inform Assoc Published Online First: [ please include Day Month Year] doi:10.1136/amiajnl-2014002817 Non-professional caregivers, also known as informal caregivers who are usually family members, play an important role in caring for people who cannot care for themselves. There were an estimated 65.7 million informal caregivers in the USA in 2009, of which 66% (43.5 million) took care of an adult older than 50 years.1 It is expected that informal caregiving will be the largest source of long-term care services in the USA, increasing by 85% from 2000 to 2050.2 The roles and responsibilities of caregivers are complicated. Caregiving responsibilities are usually financially uncompensated, require the caregiver to juggle the responsibilities with other demands on their time, and often leave the caregiver exhausted and at risk for health problems. It is becoming Hu C, et al. J Am Med Inform Assoc 2014;0:1–11. doi:10.1136/amiajnl-2014-002817 The Cochrane Handbook for Systematic Reviews of Interventions guidelines was used.12 Inclusion criteria We included studies which met the following predetermined criteria: (1) non-professional (informal) caregivers of patients with chronic health problem; (2) internet-based technology delivering interventions to caregivers; (3) interventions designed to address caregiver stress, burden, or quality of life (QOL); and (4) open-label trials or RCTs published in peer-reviewed English language journals. Studies which did not incorporate formal measurement of caregiver stress, burden, or QOL were excluded from the summary tables but noted in the text. Studies which were not truly internet-based or web browser-based were also excluded, such as the older studies which used videophone technology or 1 Review older telephone modem connections, or studies which used only videoconferencing technology which was not internetbased. Studies which provided online education or information only, without any component of interactivity such as a discussion forum, were excluded because we wanted to assess internetbased studies which incorporated features of interaction. Two reviewers screened abstracts and, for those abstracts which appeared to meet the inclusion criteria, the full-text article was obtained and reviewed. Disagreements regarding whether an article met our inclusion criteria were resolved by applying the inclusion criteria again to the article and the two reviewers arriving at a consensus decision after further discussion. No numerical methods such as inter-rater scores were used. Search strategy The Ovid MEDLINE (1946 to September 2013), Embase (1988 to September 2013), PsycINFO (1987 to September 2013), and CINAHL databases were used. Search terms were caregivers AND evaluation/intervention AND technology OR blogging OR electronic mail OR internet OR software OR user-computer interface OR web based OR mobile OR cellular phone OR social media OR smartphone OR interactive OR Facebook OR twitter OR Tablet OR iPad OR distance learning OR Ehealth OR Online OR on-line OR Skype OR webcam OR Videophone OR Telemedicine OR Wireless OR wi-fi. Two reviewers (CH and SK) independently screened the article abstracts obtained from the search, and articles meeting the inclusion criteria were retrieved for full-text review. (performance and detection bias); (d) whether incomplete outcome data might affect the true study outcomes (attrition bias); (e) whether there was selective reporting (reporting bias); and (f ) the possibility of other bias. As recommended by the Cochrane Collaboration, we avoided the use of an overall summary category such as ‘high quality’ or ‘low quality’ to describe each study. Data extraction We extracted the following data: (1) participants (type of health problem of the care recipient, the number of participants in the intervention and control and other groups, caregiver mean age and gender; (2) intervention description (the intervention and comparison group(s) and study duration); (3) outcome measures and measurement timeline; and (4) study results (the effectiveness of intervention). RESULTS Two authors (CH and SK) independently screened 1474 article abstracts obtained from the search. Eleven abstracts were identified through bibliography and other search techniques. Of these combined 1485 abstracts, 162 reported on the same intervention and were excluded and a further 1014 did not meet the inclusion criteria. Three hundred and nine articles were retrieved for full-text review, resulting in 8 open-label trials and 16 RCTs included in the final analysis (figure 1). Table 1 presents the open-label studies which evaluated an intervention without a comparison group while table 2 contains those open-label studies which included a comparison group. Tables 3–6 summarize the RCTs. Risk of bias assessment The Cochrane Risk of Bias Tool was used for RCTs as we felt it has less meaning for open-label trials.12 Two reviewers (CH and SK) assigned ratings of ‘low,’ ‘high,’ and ‘unclear’ risk of bias for the following categories: (a) the adequacy of the sequence generation and randomization (selection bias); (b) the concealment of the treatment allocation (selection bias); (c) the adequacy of blinding of participants and research staff Participants The medical conditions of the care recipient ( patient) included cancer,30–32 dementia/neurodegenerative disease,13 16 22–24 28 pediatric traumatic brain injury,18–20 stroke,25 27 anorexia nervosa,34 35 schizophrenia,21 33 heart transplantation,17 frail elderly,14 hip fracture,15 infant/toddler sleep problem,36 and fetal alcohol spectrum disorders.37 Due to the nature of the Figure 1 Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) flow diagram. RCT, randomized controlled trial. 2 Hu C, et al. J Am Med Inform Assoc 2014;0:1–11. doi:10.1136/amiajnl-2014-002817 Review Table 1 Summary of open-label studies of internet-based interventions without a comparison group for caregivers Year/study Participants Interventions Outcome measures Results Comments 2004/Glueckauf et al13 21 caregivers of dementia patients. Mean age 64.4; 86% female. Two groups were analyzed as one large group: 15 received internet-based class instruction, 6 received telephone-based instruction 2008/Torp et al14 19 caregivers of frail elderly people. Mean age 73; 42% female Alzheimer’s Caregiver Support Online website including information, webcast sessions, discussion board, and chat room. Duration: 16 weeks Caregiving Self-Efficacy Scale, Stress-related Growth Scale, Caregiver Appraisal Inventory. Timeline: pretest, post-test Positive results. Significant increases in self-efficacy, decrease in caregiver burden Webcast sessions were designed to reduce caregiver stress. Telephone-based instruction provided as a backup to internet-based instruction or when caregivers did not have internet access. Both groups were similar for baseline measures so were combined for data analysis Online classes, discussion board, educational information, videophone. Duration: 18 months Social contacts, burden of care, knowledge, stress and mental health. Timeline: baseline, 7, 12 months 2012/Nahm et al15 27 dyads of hip fracture caregiver and care recipient. Caregivers mean age 55.5; 67% female Web-based Online Hip Fracture Resource Center (OHFRC) with learning modules and discussion board. Duration: 8 weeks 2012/Lorig et al16 60 family caregivers of dementia patients. Mean age 57.2; 81.7% female Intervention: Building Better Caregivers, an internet-based skills enhancement workshop including interactive learning center, bulletin boards, individualized problem behavior diaries and exercise logs, communications. Duration: 6 weeks Mixed results. No significant improvement in stress and mental health but significantly improved contact with family and friends and improved social support and knowledge Caregiver Strain Index, Negative results for mental Rhode Island Stress and health outcomes. Improvement Coping Inventory, care in caregiver stress, coping, and recipient outcomes, computer-mediated social eHealth literacy, website support was not statistically usability. significant. However, there was Timeline: pre- and improvement in knowledge post-intervention about caring for patients Health indicators, health Positive study. Significant reduction in caregiver burden, behaviors, healthcare utilization, including Zarit depression, pain, stress Burden Inventory, Caregiver Strain Index. Timeline: baseline, 3 months Somewhat difficult to recruit caregivers and resulting participants tended to be younger caregivers Successfully able to reach rural caregivers Table 2 Summary of open-label studies of internet-based interventions with a comparison group for caregivers Year/study 2004/Dew et al 17 2009/Wade et al18 Participants Interventions Outcome measures Results Comments Intervention group: 20 patients and caregivers of heart transplant patients. Mean age 45; 85% female. Control: Historic control group of 40 patients and caregivers. Mean age 65; 85% female Nine families of children aged 3–8 with traumatic brain injury. Mean age and gender unspecified Intervention: Online discussion group, stress and medical regimen management, communication with transplant team, educational information as well as usual care. Control: Usual care. Duration: 4 months Depression, anxiety, anger-hostility (using Symptom Checklist-90), quality of life (Short Form-36), medication compliance. Timeline: baseline and post-test Mixed results. Caregiver anxiety and hostility symptoms declined significantly, but not depression. Only the social functioning domain of QOL significantly improved Intervention for patients and caregivers. Seems to be an ideal/model design. Modules included working at user’s own pace and homework Intervention: web-based video education and coaching to increase positive parenting skills and to improve caregiver stress Duration: 10 core session Intervention: online multifamily group program including discussion board, online chat, and educational materials. Control: usual care. Duration: 1 year Dyadic Parent-Child Interaction Coding System-III (DPICS-III), Eyberg Child Behavior Inventory (ECBI) Mixed results. Significant improvements in parenting behaviors and no significant improvement (but a trend noted) for reducing problem behaviors Mixed results. No significant improvement of caregiver distress in online versus control group. Significant improvement of relationship stress in online group over time Also refer to related randomized interventions by Wade et al19 20 2010/Glynn et al21 42 caregivers of schizophrenia. 26 in intervention group (mean age 57, 77% female), 16 in control group (mean age 53.8, 94% female) 2011/Marziali and Garcia22 91 caregivers of dementia patients, 40 in chat group, 51 in video group. Mean age 65.5; 72% female Internet-based chat support group, duration: 6 months. Internet-based video conferencing support group, duration: 10 weeks Caregiver distress measured by Brief Symptoms Inventory, relationship stress between patient and caregiver, perceived social support Timeline: baseline, 6, and 12 months Caregiver distress, health status, social support, service utilization. Timeline: pretest, post-test Hu C, et al. J Am Med Inform Assoc 2014;0:1–11. doi:10.1136/amiajnl-2014-002817 Recruitment was challenging, with resulting small number of participants Positive results. Video group showed significantly greater improvement in mental health status, self-efficacy, neuroticism, social support, and lower stress response 3 4 Review Table 3 Summary of randomized controlled trials of internet-based interventions for caregivers of patients with neurodegenerative disease or stroke Hu C, et al. J Am Med Inform Assoc 2014;0:1–11. doi:10.1136/amiajnl-2014-002817 Year/study Participants Interventions Outcome measures Results Comments 2005/Beauchamp et al23 299 family caregivers of patients with dementia (150 in intervention group, 149 in control group). Mean age 46.9; 73% female 66 caregivers of patients with neurodegenerative disease (Alzheimer’s, stroke-related dementia, Parkinson’s): 34 in intervention group and 32 in control. Mean age 67.8; 76% female Caregivers had an average exposure of 32.2 min (SD 43.5, range 1–368) to the website program over the 30-day study duration Provided a qualitative analysis of group discussion themes 2009/Pierce et al25 73 caregivers of patients with stroke (36 in intervention group and 37 in control group). Mean age 55; 75% female Stress (primary outcome), self-efficacy, intention to get support, ways of coping, caregiver strain, caregiver gain, depressive symptoms, state anxiety. Timeline: baseline and post-intervention Health Status Questionnaire 12 (HSQ-12), Center for Epidemiologic Studies-Depression (CES-D), stress related to activities of daily living (ADL), Revised Memory and Behavior Problems Checklist, Multidimensional Scale of Perceived Social Support. Timeline: baseline and 6 months Depression (measured by CES-D), Satisfaction with Life Scale, and healthcare utilization. Timeline: baseline and every 3 months Intervention significantly improved 7 of 8 outcomes (all except ways of coping) 2006/Marziali et al24 Caregiver’s Friend website with text and video modeling positive caregiving strategies. Control: usual care. Duration: 30 days Caring for Others website and 22 weeks of videoconferencing support groups. Control: no intervention. Duration: 6 months 2012/Smith et al27 32 spouse caregivers of stroke survivors (15 dyads in intervention group and 17 dyads in control group). Mean age 55.3 in intervention group and 54.9 in control group; 100% female 2013/Kajiyama et al28 150 dementia caregivers (75 in intervention group, 75 in control group). Mean age 55 in intervention group, 57 in control. Gender: 83% female in intervention group, 86% in control group 201 family caregivers of adult patients with traumatic brain injury (104 in intervention group, 97 in control group). Mean age not specified; 86.4% female in intervention group, 88.4% female in control group 2013/McLaughlin et al29 Caring∼Web with informational and email forum for questions or discussion, accessed by internet TV. Control: no internet access. Duration: 1 year Website with professional guide, educational videos, online chat sessions, email and message board, and resource room. Control: resource room only. Duration: 11 weeks + 1 month follow-up iCare Stress Management e-Training Program; Control: Education/information only Duration: 3 months Brain Injury Partners (BIP) website for advocacy, improving communication skills with patients, and resources for families. Control: Similar website but more passive information and focused on legislative advocacy. Duration: 3 months Depression (primary outcome, measured by CES-D), Patient Health Questionnaire-9 (PHQ-9), Mastery Scale, Self-Esteem Scale, Social Support Survey, Credibility/Expectancy Questionnaire. Timeline: baseline, post-intervention (11 weeks), and 1 month follow-up No differences in any measure between intervention and control from baseline to follow-up. However, within the intervention group (not comparing to control), there was a greater reduction (change from baseline to follow-up) of two stress measures (related to ADLs and managing difficult behaviors) No significant differences in depression or life satisfaction between the two groups or over time. However, patient emergency department visits and hospital readmissions were significantly fewer in the intervention group Caregivers in the intervention group reported significantly lower depression at both post-intervention and 1 month follow-up compared with control group Perceived Stress Scale, level of bother due to disruptive behaviors, CES-D (depression), Perceived Quality of Life. Timeline: 3 months Change in perceived stress was significant for the iCare intervention group but not for the other outcome measures Satisfaction with Life Scale. Likert scales for knowledge, skill application, and behavioral intention. Timeline: pretest, post-test, and 3 months No significant improvement with life satisfaction but intervention group had significantly increased application, knowledge and attitudes A related 2008 study by Steiner using the same Caring∼Web system and a control group found no significant difference between intervention and control for caregiver emotional support26 Negative study Review Table 4 Summary of randomized controlled trials of internet-based interventions for caregivers of patients with cancer Year/study Participants Interventions Outcome measures Results Comments 2002/Farnham et al30 49 caregivers of bone marrow transplant patients and 35 patients: 21 in intervention group, 25 in control. Mean age 49; 60% female Computer usage patterns and quality of life. Timeline: baseline and 28, 56, 84 days (56 and 84 days results not reported) No change in quality of life (life satisfaction, stress, and social support) Participants were living up to 1 month in the Hutch outpatient housing facility and, at baseline, 60% overall had internet access 2012/Namkoong et al31 246 non-small cell lung cancer patient-caregiver dyads, 124 in intervention group, 122 in control. Mean age 55.6, 68.3% female Bonding (5-item scale) with other caregivers; coping strategies (active behavior, positive reframing, and instrumental support). Timeline: baseline and every 2 months, with 6-month outcomes reported Intervention had a significant positive effect on caregivers’ perceived bonding and coping strategies Secondary analysis 2013/Chih et al32 235 advanced stage lung, breast, and prostate cancer patient-caregiver dyads: 118 in intervention group, 117 in comparison group.Mean age 56, 64% female HutchWorld social interactive community and internet information access. Control: could use any self-provided computer facilities. Duration: 3 months Comprehensive Health Enhancement Support System (CHESS) website for information, communication, and support such as discussion groups. Control: laptop computer with internet access if needed, list of cancer care websites. Duration: 6 months Intervention group: CHESS with online clinician report (CR) to alert clinicians to severe patient symptoms. Comparison group: CHESS only. Duration: 12–24 months Caregiver preparedness (subscale of Family Care Inventory), Caregiver Physical Burden (subscale of Caregiver Burden Inventory), and Caregiver Negative Mood (subset of Profile of Mood States). Timeline: 6 and 12 months Less negative mood in CHESS+CR compared with CHESS only; no significant differences on caregiver preparedness or physical burden This study combined two randomized trials which had three comparison groups but did not use the control comparison group which did not use CHESS medical conditions such as dementia or stroke, or sometimes to the age of the patient such as for the pediatric population, many of the studies targeted only the caregiver. However, some of the studies were able to include the patient and caregiver in trying to improve outcomes for both.15 17 19 20 27 30–33 In the eight open-label studies 289 caregivers and patients were enrolled and, in the 16 RCTs, 1882 caregivers were enrolled with 10 studies having fewer than 100 caregivers and six having more than 100. Interventions The internet interventions included interactive modules with study investigator assistance or community interactions. Five of the RCTs compared an internet intervention with standard care,23–25 28 33 six compared an internet intervention with unguided computer use or internet resources,19 20 27 30 31 34 three compared an internet intervention with added features to the same internet intervention,29 32 35 and two RCTs used a three-group design comparing the internet intervention with a control group and a third group of either higher or lower intensity than the intervention.36 37 About half of the RCTs had durations of 3 months or less.23 27–30 33 35–37 Outcome measures The included studies used formal rating scales to measure the outcomes related to caregiver stress, mood, anxiety, well-being, life satisfaction, or QOL. Secondary outcomes included internet program usage and satisfaction. A few studies measured patient healthcare utilization.25 34 36 Outcomes Of the eight open-label studies, three reported positive benefit in reducing caregiver stress as measured by their selected rating Hu C, et al. J Am Med Inform Assoc 2014;0:1–11. doi:10.1136/amiajnl-2014-002817 scales,13 16 22 four reported mixed results,14 17 18 21 and one reported a negative result.15 Of the 16 RCTs, six reported positive or mostly positive results,19 23 27 31 34 36 five reported mixed results with some of the outcome measures showing improvement28 32 35 37 or when taking into account factors such as socioeconomic status,20 and five reported negative results in the primary outcomes.24 25 29 30 33 These negative studies comprised most of the earlier studies with publication years 2002, 2005, 2006, 2009, and 2013. Risk of bias for RCTs A summary of the risk of bias for RCTs is shown in table 7. Keep in mind that the Cochrane Risk of Bias Tool is better suited to assessing the fidelity of randomized double-blind trials more along the lines of medication interventions. Also, these internet intervention studies were likely not designed with the Cochrane guidelines in mind (such as to describe the details of randomization), so there are many resulting ‘unclear’ conclusions. However, we include this assessment as it is recommended when evaluating randomized trials. Due to the nature of internet use, a careful control group and rigorous blinding are usually not possible. Participants in several studies in which the control group received usual care or no internet support still had their own computer and/or access to internet.30 33 For participants in the intervention groups there could be a wide range of times that they spent on the intervention. Several studies did not record internet usage factors such as time and frequency, making compliance difficult to assess, also resulting in potential bias.25 31 Another risk of bias relates to incomplete data and drop-out rates which might affect the true outcome of the study. Using criteria from a different set of guidelines, acceptable drop-out rates were based on the study duration: <20% for studies less 5 Review Table 5 Summary of randomized controlled trials of internet-based interventions for caregivers of patients with mental illness (schizophrenia or anorexia nervosa) Year/study Participants Interventions Outcome measures Results Comments 2005/Rotondi et al33 21 support persons and their patients with schizophrenia or schizoaffective disorder: 11 in intervention group and 10 in control. Mean age 51.5; 66.7% female 63 caregivers of patients with anorexia nervosa: 33 in intervention group, 30 in control. Mean age 48.2 Schizophrenia Guide website providing information and bulletin board therapy groups. Control: usual care. Duration: 3 months Perceived social support and perceived stress. Timeline: baseline and 3 months No significant differences in perceived social support or stress from baseline to 3 month follow-up The intervention’s primary focus was to improve patient support and stress, but also included support person outcomes Overcoming Anorexia Online (OAO) website delivering a cognitive behavioral therapy (CBT) intervention and clinician guidance. Control: standard support resource with telephone hotline, email support, message board and, where available, support group. Duration: 4 months Overcoming Anorexia Online (OAO) website + clinician guidance. Control group: OAO alone. Duration: 3 month Hospital Anxiety and Depression Scale (HADS; primary outcome). Secondary outcomes consisted of caregiver experience, impact of illness, expressed emotion, and accommodation/ enabling scale. Timeline: baseline, 4 months (end of treatment) and 6 months Intervention significantly decreased anxiety and depression (primary outcome HADS, p=0.033) compared with control group. No significant improvements in the secondary outcomes The researcher assessing outcomes was adequately blinded to the intervention vs control group Primary outcome: Caregiver Level of Expressed Emotion (LEE), rated by caregiver and patient. Secondary outcomes: General Health Questionnaire-28, Medical Outcomes Study Short Form Scale, Depression Anxiety Stress Scales-21, Eating Disorder Symptom Impact Scale, Experience of Care Giving Inventory. Timeline: baseline, post-intervention, and 3-month follow-up Intervention group had a larger significant decrease in the intrusiveness subscale of the LEE 2011/Grover et al34 2013/Hoyle et al35 37 caregivers of patients with anorexia nervosa: 19 in intervention group, 18 in control group. Mean age not reported. Gender: 83% female than 3 months and <30% for studies more than 3 months.38 With these criteria, six of the short-term studies had acceptable drop-out rates19 20 23 27 33 36 and four did not.28 30 35 37 All five of the longer-term studies had drop-out rates >30%,24 25 31 32 34 with one study reporting >50% loss to follow-up.31 Most studies reported that the loss to follow-up was similar between groups except one study which reported more drop-outs in the control group24 and one study reporting more drop-outs in the intervention group.37 One study included intent-to-treat analysis27 and one study described the intention-to-treat analysis but did not report the resulting data.33 with providers or other caregivers.50 53–59 Some tested whether an in-person educational workshop could be equally effective when converted to an online format.47 60 Studies which were not internet web-based, such as purely videoconferencing or videophone-based, or those using older technology such as telephone dial-up modems, were also excluded.61–69 One study was excluded because the target audience was professional caregivers (ie, nursing home staff ) and the intervention was e-learning modules only.70 Overall, these studies showed a wide range of technologies and patient populations (dementia, cancer, brain injury, frail elderly patients, developmentally disabled patients, chronic illness, heart transplant, and schizophrenia). Excluded studies DISCUSSION Thirty-two open-label studies were not included in the tables because of our stringent inclusion criteria, but will be presented here in the text because they still demonstrate useful applications of computer-based technology for assisting caregivers. Several of these studies were proof-of-concept feasibility studies which measured usability, usage, and/or user satisfaction.39–43 We also excluded studies which did not measure outcomes related to reducing caregiver stress or improving caregiver QOL but instead might have measured caregiver knowledge, for example.39 44–52 Some of the interventions were only informational or educational without any interactive component such as a discussion forum or a method for the caregiver to interact In this systematic review of eight open-label trials and 16 RCTs of internet interventions to improve caregiver stress, we identified moderate evidence of benefit: nine trials were positive (three open-label studies and six RCTs), nine were partially positive (four open-label studies and five RCTs), and six were negative (one open-label study and five RCTs). Despite inherent differences in assessing the risk of bias for internet behavioral trials versus the traditional medication-based double-blind RCT, the quality of the RCTs was acceptable given the nature of the interventions. The evidence of benefit increases if the ‘partially positive’ category was reassigned to the positive category. In that case, 18 6 Hu C, et al. J Am Med Inform Assoc 2014;0:1–11. doi:10.1136/amiajnl-2014-002817 Hu C, et al. J Am Med Inform Assoc 2014;0:1–11. doi:10.1136/amiajnl-2014-002817 Table 6 Summary of randomized controlled trials of internet-based interventions for caregivers of patients with medical illness (traumatic brain injury, sleep disturbance, fetal alcohol syndrome) Year/study Participants Interventions Outcome measures Results Comments 2006/Wade et al19 46 families of children with moderate-to-severe traumatic brain injury: 26 in intervention group and 20 in control group.Mean caregiver age not reported Social Problem-Solving Index, Symptoms Checklist-90-Revised (SCL-90-R), CES-D, Anxiety Inventory. Timeline: baseline and follow-up Parents in the intervention group reported significantly less depression, anxiety, and general psychiatric symptoms at follow-up. However, problem-solving skills did not significantly improve Therapist assisted family in completing the sessions with webcam videoconferencing if family had not completed the content on their own 2011/Mindell et al36 264 mothers and their children (ages 6– 36 months) with sleep problems: 96 in internet intervention group, 84 in internet intervention plus bedtime routine group, and 84 in control group. Mean maternal age: 59% in the 30–39 year-old age category Brief Infant Sleep Questionnaire (BISQ), Pittsburg Sleep Quality Index (PSQI) regarding maternal sleep, Profile of Mood States (POMS) regarding maternal mood states. Timeline: baseline, weeks 2 and 3 Both intervention groups showed significant improvement of maternal sleep and mood state compared with control group The intervention’s primary outcome was to improve patient (child) symptoms (sleep) instead of caregiver symptoms, however, the study also measured caregiver (maternal) response to the intervention 2012/Wade et al20 41 families of adolescents with moderate-to-severe traumatic brain injury: 20 in intervention group and 21 in control group.Mean age 41.58 in intervention group and 40.81 in control Social Problem-Solving Index, Symptoms Checklist-90-Revised (SCL-90-R), CES-D, moderated by socioeconomic status (SES). Timeline: baseline and follow-up Lower SES families using TOPS improved on depression scale and two problem-solving items compared with lower SES in the control group Therapist reviewed website content with family via webcam videoconferencing in the second part of each session 2012/Kable et al37 59 families of children with fetal alcohol spectrum disorders (FASD): 18 in intervention internet group, 23 in workshop group, 18 in community standard of care group Online family problem-solving therapy website including 14 sessions. Control: internet resources comparison group. Duration: variable, depending on session completion, overall >3 months Group 1 received the internet Customized Sleep Profile (CSP) algorithm-based advice on how mothers can improve child’s sleep. Group 2 received CSP + instructions on a nightly 3-step bedtime routine for the child. Group 3 (control) received no intervention. Duration: 3 weeks, of which first week was baseline observation and intervention was 2 weeks Teen Online Problem Solving (TOPS) website including 9–13 sessions. Control: internet resources comparison group with links to TBI information. Duration: 8 months Community group received an informational packet. Workshop group had two in-person workshops. Internet group presented web-based parent education paralleling the workshops. Duration: unspecified, probably <3 months Child Behavior Checklist, Caregiver Advocacy Knowledge Questionnaire, Behavioral Regulation Knowledge Questionnaire. Timeline: baseline and post-intervention Internet group had no significant improvement in child behavior while community and workshop groups had improvement. Internet group had improvement in knowledge of FASD Some baseline differences among group characteristics TBI, traumatic brain injury. Review 7 8 Review Table 7 Risk of bias and quality assessment for randomized controlled trials Hu C, et al. J Am Med Inform Assoc 2014;0:1–11. doi:10.1136/amiajnl-2014-002817 Blinding? Incomplete outcome data addressed? Free of selective reporting? Free of other bias? ? H H L H ? ? H L L L Rotondi et al33 ? ? ? H ? H Marziali et al24 ? ? H H L L Wade et al19 L ? L L L H Pierce et al25 L ? H L L H Grover et al34 L L L H L L Mindell et al36 ? ? L L L H Namkoong et al31 L ? ? H L L Smith et al27 L ? L L L L Wade et al20 L H H H L L Kable et al37 Chih et al32 ? ? ? ? ? ? H ? L H L H Kajiyama et al28 ? ? ? H L L Hoyle et al35 ? ? ? ? L L McLaughlin et al29 ? ? ? L L L Reference Adequate sequence generation? Allocation concealment? Farnham et al30 ? Beauchamp et al23 ?, unclear; H, high risk of bias; L, low risk of bias. Comments Did not describe dropout or sample size at the end of the intervention. Participants in the control group could still access the internet Low dropout rate. Reported that baseline measures and demographic characteristics of patients who dropped out were not significantly different between the two groups Unclear regarding dropout rate. Unclear regarding exact questions used to rate stress and social support. A few participants in the control group had access to the internet Research staff were not blinded to the groups. High and unequal dropout rate between intervention and control groups, with 28/66 patients (42%) lost to follow-up Participants and research staff were not blinded to group assignments, but ratings were made by parents and thus not vulnerable to influence by research staff. Dropout rates were different in intervention vs control, but not statistically significant. Families were allowed to keep computer equipment at treatment completion as an incentive for participation Dropout rates were high but equal between the intervention and control groups, and dropout reasons were adequately explained. Participants were offered the computer equipment for free at the end of the study, regardless of whether they were in the intervention or control group Dropout data were not clearly explained. In the intervention group there were 24/33 (72.7%) completers and in the control group there were 21/30 (70%) completers, approximately 30% dropout rate Caregivers (mothers) were not aware of the other groups. Significant sleep differences at baseline. Study sponsored by a commercial entity. Participants were paid $90–$175 depending on number of visits. Low dropout rate (3%) but unequal among the three groups Secondary analysis. Use of the intervention system was not mandated. Laptop and internet access were provided if needed. High dropout rate of 58%, 75 in intervention and 67 in control The researcher assessing outcomes was blinded to the intervention vs control group. Dropout information was adequately explained. Data analyzed with per-protocol and intent-to-treat Participants and research staff aware of group assignments (no blinding). Ratings were made by parents and thus not vulnerable to influence by research staff. Dropouts had higher depression and distress than completers but was adequately explained High dropout rate 20–40% similar across the three groups and adequately explained Secondary analysis: the study combined two randomized trials and the original randomized three-group design was reduced to two groups because of low recruitment. For data analysis the relevant groups were selected. Participants were supplied with a laptop if needed and allowed to keep it High dropout rate of 31%, with 29 in the intervention and 18 in the control. Caregivers with severe depression as measured by CES-D >30 were screened out 37 caregivers entered, 27 completed time 2 questionnaires but 30 (81%) completed the intervention. Of the 27, 5 did not access the website. Of the 7 who withdrew from the study, did not describe how many were from the intervention versus control Incomplete assessments were low (6–14%) and not statistically different between the two groups. Missing data were imputed Review trials (7 open-label studies and 11 RCTs) would be positive and 6 trials (1 open-label study and 5 RCTs) would be negative. The ‘partially positive’ results indicate that the study authors chose several measures to analyze, and some of the measures showed positive benefit while others did not. In newer study methodologies the authors frequently chose one primary outcome measure and several secondary outcomes measures, and declare the success of the study based on the primary outcome. Some of the articles reviewed defined a primary outcome, but we did not categorize those as a negative outcome if the primary outcome was negative but some of the secondary outcomes were positive. While our rigorous inclusion criteria regarding the type of trial (open-label studies and RCTs), the level of internet-based technology with some component of interactivity, and the need for formal outcome measures resulted in only 24 included trials, we explained in the Results section why we excluded 32 openlabel studies. Most of these excluded studies reported favorable outcomes in terms of feasibility, satisfaction, and benefit. Thus, in looking beyond the strict level of evidence that we used, we also found optimism that internet-based interventions can help caregivers. There were no clear factors such as duration or complexity to suggest what intervention approach might be more effective. The earlier studies tended to be negative, possibly related to older internet technology (some of these studies used internet TV) and less general comfort level with internet use. As technology improves, its access, ease of use, and acceptance increases. A few of the studies incorporated videoconferencing, which was a novel approach, especially in the earlier studies.19 20 24 Our findings are similar to those of other reviews of technology-based interventions. In a meta-analysis of 28 studies spanning 12 different illnesses, computer-mediated support group interventions increased social support and QOL and decreased depression.71 In a systematic review of patients with dementia in 15 studies, networked information and communication technology interventions showed moderate effects on improving caregiver stress and depression, although outcomes were inconsistent.72 In a newer systematic review which reported that internet-based interventions can improve aspects of the well-being of dementia caregivers, it was also noted that the overall level of evidence was low and lacked methodologic quality and that more randomized controlled studies are needed.73 one in cancer caregivers which identified needs as selfmanagement of distress and fostering of supportive family relationships75—can help developers design the content of internet-based interventions. Some of the elements can be used for both patient and caregivers and across different health conditions. For example, one such module might allow for selfassessment of mood using interactive questionnaires and subsequent multimedia education and management of mood, distress, and QOL. Other considerations in designing caregiver interventions would be whether the target audience should include patients. In a study delivering an in-person multidisciplinary group intervention targeting QOL of cancer patients, caregivers were also invited to some of the sessions.76 From this study, an analysis of the QOL of patients and caregivers showed that, when patients had better QOL, caregivers also had better QOL.77 It is intriguing to consider whether internet-based videoconferencing delivery of such an intervention might similarly benefit patients and caregivers. A recent review of consumer health information technology to support caregivers of patients with chronic illnesses identified several considerations for future study.4 Online modalities which promoted caregiver interactions, such as peer support groups and chat rooms, were found to be highly used and valued. These technologies can overcome barriers such as distance, travel logistics and cost, and limited caregiver time availability. There are still many gaps in our knowledge about best evidence for future technology-based interventions to help the caregiver. For example, exploration of age, gender, ethnic, and socioeconomic differences in responding to such interventions; inclusion of patient and caregiver dyads versus caregivers only; and use of technologies such as mobile devices, videoconferencing, or social media. One of our findings from this review is the diversity of methodologies used and patient illnesses addressed. To help improve comparability across studies, future trials can try to incorporate more widely used caregiver rating scales and be clearer about choosing a primary outcome measure and secondary measures. Involving the appropriate psychology and QOL researchers can help with measurement and methodology issues. Many of the studies we reviewed were already of high quality. As this field needs more exploration, open-label studies are beneficial but, in the future, more RCTs would help to answer the research question of whether caregivers actually benefit from these internetbased interventions. Future considerations There is currently a wide variety of caregiver internet-based interventions, as evidenced by our review findings and also the studies we excluded. Our opinion is that these interventions should take advantage of the interactivity possible through internet technologies, such as discussion forums and group videoconferencing, to connect caregivers with the medical team as well as peer support. In designing internet interventions for caregivers, the technology elements are similar to those for patients. A systematic review of web-based interventions for cancer patient empowerment identified commonly used elements such as education, self-monitoring, feedback/tailored information, self-management training, personal exercise program, and communication tools.74 In the caregiver interventions we reviewed, common elements also included education, information, self-management, and communication. Of course the target audience is different, so the content will be different, such as information relevant to the patient (eg, regarding diagnosis and treatment) versus relevant to the caregiver (eg, how to support the patient). Caregiver needs assessments—for example, Hu C, et al. J Am Med Inform Assoc 2014;0:1–11. doi:10.1136/amiajnl-2014-002817 CONCLUSION Internet-based interventions were mostly effective in reducing aspects of caregiver stress and improving their well-being. This systematic review of open-label studies and RCTs identified 24 such trials, with nine trials reporting positive benefits in the outcome measures, nine reporting partially positive outcomes, and six reporting no benefit of the internet-based intervention. With continued population acceptance of internet use, there are opportunities to use this platform to improve the lives of caregivers. Further studies are needed to assess outcomes for caregivers and their recipients’ health, different technology delivery methods, and the cost of such interventions. Contributors All authors meet the criteria for authorship and agree to be accountable for all aspects of the work in ensuring that questions related to the accuracy or integrity of any part of the work are appropriately investigated and resolved. All authors were involved in the conception of the work, design of the search strategy and methodology, review of articles, data collection, data analysis and interpretation; initial manuscript draft and subsequent revisions; final approval of version for submission and publication; manuscript revision and resubmission. 9 Review Funding This work was supported by the Linse Bock Foundation. Competing interests None. 29 Provenance and peer review Not commissioned; externally peer reviewed. 30 REFERENCES 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 10 Adelman R, Tmanova L, Delgado D, et al. Caregiver burden: a clinical review. JAMA 2014;311:9. US Department of Health and Human Services. The future supply of long term care workers in relation to the aging baby-boom generation. Washington, DC, 2003. http://www.aspe.hhs.gov/daltcp/reports/ltcwork.pdf Biegel D, Sales E, Schulz R. Family caregiving in chronic illness: heart disease, cancer, stroke, Alzheimer’s disease, and chronic mental illness. Newbury Park, CA: Sage Publications, 1991. Dyer EA, Kansagara D, Mclnnes DK, et al. Mobile applications and internet-based approaches for supporting non-professional caregivers: a systematic review [Internet]. Washington, DC: Department of Veterans Affairs, 2012. Gallagher DE. Intervention strategies to assist caregivers of frail elders: current research status and future research directions. Annu Rev Gerontol Geriatr 1985;5:249–82. Thompson CA, Spilsbury K, Hall J, et al. Systematic review of information and support interventions for caregivers of people with dementia. BMC Geriatr 2007;7:18. Vachon ML. Care for the caregiver. Can Nurse 1980;76:28–33. Schulz R, Lustig A, Handler S, et al. Technology-based caregiver intervention research: current status and future directions. Gerontechnology 2002;2:15–47. Pingdom. Internet 2012 in numbers. Pingdom, 2012. Cavallo DN, Tate DF, Ries AV, et al. A social media-based physical activity intervention: a randomized controlled trial. Am J Prev Med 2012;43:527–32. Webber KH, Tate DF, Michael Bowling J. A randomized comparison of two motivationally enhanced Internet behavioral weight loss programs. Behav Res Ther 2008;46:1090–5. Higgins JPT, Green S. Cochrane Handbook for Systematic Reviews of Interventions, version 5.1.0. The Cochrane Collaboration, 2011. Glueckauf RL, Ketterson TU, Loomis JS, et al. Online support and education for dementia caregivers: overview, utilization, and initial program evaluation. Telemed J E Health 2004;10:223–32. Torp S, Hanson E, Hauge S, et al. A pilot study of how information and communication technology may contribute to health promotion among elderly spousal carers in Norway. Health Soc Care Community 2008;16:75–85. Nahm ES, Resnick B, Orwig D, et al. A theory-based online hip fracture resource center for caregivers: effects on dyads. Nurs Res 2012;61:413–22. Lorig K, Thompson-Gallagher D, Traylor L, et al. Building better caregivers: a pilot online support workshop for family caregivers of cognitively impaired adults. J Appl Gerontol 2012;31:5. Dew MA, Goycoolea JM, Harris RC, et al. An internet-based intervention to improve psychosocial outcomes in heart transplant recipients and family caregivers: development and evaluation. J Heart Lung Transplant 2004;23:745–58. Wade SL, Oberjohn K, Burkhardt A, et al. Feasibility and preliminary efficacy of a web-based parenting skills program for young children with traumatic brain injury. J Head Trauma Rehabil 2009;24:239–47. Wade SL, Carey J, Wolfe CR. An online family intervention to reduce parental distress following pediatric brain injury. J Consult Clin Psychol 2006;74:445–54. Wade SL, Walz NC, Carey J, et al. A randomized trial of teen online problem solving: efficacy in improving caregiver outcomes after brain injury. Health Psychol 2012;31:767–76. Glynn SM, Randolph ET, Garrick T, et al. A proof of concept trial of an online psychoeducational program for relatives of both veterans and civilians living with schizophrenia. Psychiatr Rehabil J 2010;33:278–87. Marziali E, Garcia LJ. Dementia caregivers’ responses to two Internet-based intervention programs. Am J Alzheimers Dis Other Demen 2011;26:36–43. Beauchamp N, Irvine A, Seeley J, et al. Worksite based internet multimedia program for family caregivers of persons with dementia. Gerontologist 2005;45:793–801. Marziali E, Donahue P. Caring for others: Internet video-conferencing group intervention for family caregivers of older adults with neurodegenerative disease. Gerontologist 2006;46:398–403. Pierce LL, Steiner VL, Khuder SA, et al. The effect of a web-based stroke intervention on carers’ well-being and survivors’ use of healthcare services. Disabil Rehabil 2009;31:1676–84. Steiner V, Pierce L, Drahuschak S, et al. Emotional support, physical help, and health of caregivers of stroke survivors. J Neurosci Nurs 2008;40:48–54. Smith GC, Egbert N, Dellman-Jenkins M, et al. Reducing depression in stroke survivors and their informal caregivers: a randomized clinical trial of a web-based intervention. Rehabil Psychol 2012;57:196–206. Kajiyama B, Thompson LW, Eto-Iwase T, et al. Exploring the effectiveness of an internet-based program for reducing caregiver distress using the iCare Stress 31 32 33 34 35 36 37 38 39 40 41 42 43 44 45 46 47 48 49 50 51 52 53 54 55 56 Management e-Training Program. [Erratum appears in Aging Ment Health. 2013;17 (5):c1]. Aging Ment Health 2013;17:544–54. McLaughlin KA, Glang A, Beaver SV, et al. Web-based training in family advocacy. J Head Trauma Rehabil 2013;28:341–8. Farnham S, Cheng L, Stone L, et al. Hutchworld: Clinical study of computer-mediated social support for cancer patients and their caregivers. In: Proceedings of the SIGCHI conference on Human factors in computing systems: Changing our world, changing ourselves. Terveen L, Wixon D, Comstock E, Sasse A, eds. 2002:375–82. Namkoong K, DuBenske LL, Shaw BR, et al. Creating a bond between caregivers online: effect on caregivers’ coping strategies. J Health Commun 2012;17:125–40. Chih MY, Dubenske LL, Hawkins RP, et al. Communicating advanced cancer patients’ symptoms via the Internet: a pooled analysis of two randomized trials examining caregiver preparedness, physical burden, and negative mood. Palliat Med 2013;27:533–43. Rotondi AJ, Haas GL, Anderson CM, et al. A clinical trial to test the feasibility of a telehealth psychoeducational intervention for persons with schizophrenia and their families: intervention and 3-month findings. Rehabil Psychol 2005;50:325–36. Grover M, Naumann U, Mohammad-Dar L, et al. A randomized controlled trial of an Internet-based cognitive-behavioural skills package for carers of people with anorexia nervosa. Psychol Med 2011;41:2581–91. Hoyle D, Slater J, Williams C, et al. Evaluation of a web-based skills intervention for carers of people with anorexia nervosa: a randomized controlled trial. Int J Eat Disord 2013;46:634–8. Mindell JA, Du Mond CE, Sadeh A, et al. Efficacy of an internet-based intervention for infant and toddler sleep disturbances. Sleep 2011;34:451–8. Kable JA, Coles CD, Strickland D, et al. Comparing the effectiveness of on-line versus in-person caregiver education and training for behavioral regulation in families of children with FASD. Int J Mental Health Addict 2012;10:791–803. van Tulder M, Furlan A, Bombardier C, et al. Updated method guidelines for systematic reviews in the Cochrane Collaboration back review group. Spine (Phila Pa 1976) 2003;28:1290–9. Astell AJ. Using a touch screen computer to support relationships between people with dementia and caregivers. Interact Comput 2010;22:9. Buono S, Citta S. Tele-assistance in intellectual disability. J Telemed Telecare 2007;13:241–5. Chang BL. Internet intervention for community elders: process and feasibility. West J Nurs Res 2004;26:461–6. Pierce LL, Steiner V, Govoni AL, et al. Internet-based support for rural caregivers of persons with stroke shows promise. Rehabil Nurs 2004;29:95–9, 103. Rotondi AJ, Sinkule J, Spring M. An interactive web-based intervention for persons with TBI and their families: use and evaluation by female significant others. J Head Trauma Rehabil 2005;20:173–85. Brennan PF. Computer networks promote caregiving collaboration: the ComputerLink Project. Proceedings of the Annual Symposium on Computer Application [sic] in Medical Care Symposium on Computer Applications in Medical Care. 1992:156––60. Brennan PF. Differential use of computer network services. Proceedings of the Annual Symposium on Computer Application [sic] in Medical Care Symposium on Computer Applications in Medical Care. 1993:5. Hayden LJ, Glynn SM, Hahn TJ, et al. The use of Internet technology for psychoeducation and support with dementia caregivers. Psychol Serv 2012;9:215–18. Kuhn D, Hollinger-Smith L, Presser J, et al. B. N. Powerful tools for caregivers online: an innovative approach to support employees. J Workplace Behav Health 2008;23:19. Marziali E, Donahue P, Crossin G. Caring for others: internet health care support intervention for family caregivers of persons with Alzheimer’s, stroke, or Parkinson’s disease. Fam Soc 2005;86:9. Savolainen L, Hanson E, Magnusson L, et al. An Internet-based videoconferencing system for supporting frail elderly people and their carers. J Telemed Telecare 2008;14:4. Smith T, Richardson K, Crammer C, et al. Theory-based evaluation of an online cancer fatigue class. J Cancer Educ 2010;25:422–30. Strozier AL, Elrod B, Beiler P, et al. Developing a network of support for relative caregivers. Child Youth Serv Rev 2004;26:16. Torp S, Bing-Jonsson PC, Hanson E. Experiences with using information and communication technology to build a multi-municipal support network for informal carers. Inform Health Soc Care 2013;38:265–79. Dow B, Moore K, Scott P, et al. Rural carers online: a feasibility study. Aust J Rural Health 2008;16:221–5. Edgar L, Greenberg A, Remmer J. Providing internet lessons to oncology patients and family members: a shared project. Psychooncology 2002;11:439–46. Jang J. Randomized trial of an eLearning program for training family members of children with autism in the principles and procedures of applied behavior analysis. Res Autism Spectrum Disord 2012;6:5. Krishna S, Francisco BD, Balas EA, et al. Internet-enabled interactive multimedia asthma education program: a randomized trial. Pediatrics 2003;111:503–10. Hu C, et al. J Am Med Inform Assoc 2014;0:1–11. doi:10.1136/amiajnl-2014-002817 Review 57 58 59 60 61 62 63 64 65 66 Lam L, Lam M. The use of information technology and mental health among older care-givers in Australia. Aging Ment Health 2009;13:6. Moore CD, Cook KM. Promoting and measuring family caregiver self-efficacy in caregiver-physician interactions. Soc Work Health Care 2011;50:801–14. van der Roest HG, Meiland FJ, Jonker C, et al. User evaluation of the DEMentia-specific Digital Interactive Social Chart (DEM-DISC). A pilot study among informal carers on its impact, user friendliness and, usefulness. Aging Ment Health 2010;14:461–70. Lai CK, Wong LF, Liu KH, et al. Online and onsite training for family caregivers of people with dementia: results from a pilot study. Int J Geriatr Psychiatry 2013;28:107–8. Bass DM, McClendon MJ, Brennan PF, et al. The buffering effect of a computer support network on caregiver strain. J Aging Health 1998;10:20–43. Brennan PF, Moore SM, Smyth KA. The effects of a special computer network on caregivers of persons with Alzheimer’s disease. Nurs Res 1995;44:166–72. Demiris G, Parker Oliver D, Wittenberg-Lyles E, et al. A noninferiority trial of a problem-solving intervention for hospice caregivers: in person versus videophone. J Palliat Med 2012;15:653–60. Eisdorfer C, Czaja SJ, Loewenstein DA, et al. The effect of a family therapy and technology-based intervention on caregiver depression. Gerontologist 2003;43:521–31. Finkel S, Czaja SJ, Schulz R, et al. E-care: a telecommunications technology intervention for family caregivers of dementia patients. Am J Geriatr Psychiatry 2007;15:443–8. Grover M, Williams C, Eisler I, et al. An off-line pilot evaluation of a web-based systemic cognitive-behavioral intervention for carers of people with anorexia nervosa. Int J Eat Disord 2011;44:708–15. Hu C, et al. J Am Med Inform Assoc 2014;0:1–11. doi:10.1136/amiajnl-2014-002817 67 68 69 70 71 72 73 74 75 76 77 Haney T, Tufts KA. A pilot study using electronic communication in home healthcare: implications on parental well-being and satisfaction caring for medically fragile children. Home Healthc Nurse 2012;30:216–24. Parker Oliver D, Demiris G, Wittenberg-Lyles E, et al. Caregiver participation in hospice interdisciplinary team meetings via videophone technology: a pilot study to improve pain management. Am J Hosp Palliat Care 2010;27:465–73. Van Ast P. Supporting community carers via videoconferencing. J Telemed Telecare 2005;11(Suppl 2):S96–7. MacDonald CJ, Walton R. E-learning education solutions for caregivers in long-term care (LTC) facilities: new possibilities. Educ Health (Abingdon) 2007;20:85. Rains SA, Young V. A meta-analysis of research on formal computer-mediated support groups: examining group characteristics and health outcomes. Hum Commun Res 2009;35:309–36. Powell J, Chiu T, Eysenbach G. A systematic review of networked technologies supporting carers of people with dementia. J Telemed Telecare 2008;14:154–6. Boots L, de Vugt M, van Knippenberg R, et al. A systematic review of Internet-based supportive interventions for caregivers of patients with dementia. Int J Geriatr Psychiatry 2014;29:13. Kuijpers W, Groen W, Aaronson N, et al. A systematic review of web-based interventions for patient empowerment and physical activity in chronic diseases: relevance for cancer survivors. J Med Internet Res 2013;15:e37. Kim Y, Kashy D, Spillers R, et al. Needs assessment of family caregivers of cancer survivors: three cohorts comparison. Psychooncology 2010;2010:14. Clark M, Rummans T, Atherton P, et al. Randomized controlled trial of maintaining quality of life during radiotherapy for advanced cancer. Cancer 2013;119:8. Shahi V, Lapid M, Kung S, et al. Do age and quality of life of patients with cancer influence quality of life of the caregiver? J Geriatr Oncol 2014;14. 11









© Copyright 2026