
Document 6846
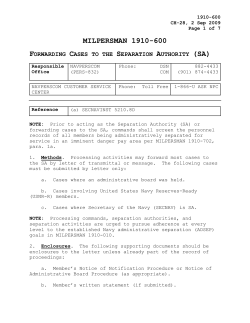
REVIEWS MINERVA ENDOCRINOL 2006;31:27388 alterutions Roleof endocrine ?fidinflammatory ln comorbidsomaticdiseases stressdisorder of post-traumatic N. ROHLEDER1.A. KARL2 Since its first description in the Diagnostic and Statistical Manual for Mental Disorders, posttraumatic stress disorder (PTSD) has been charact€rized as a disorder of altered affective functioning which causes tremendous distress. In is not addition, it has b€enrecognizedthatPTsD only accompanied by "poor health" but also by a number of specific and non-specific "sornatic" pathologies, such as cardiovascular, autoimpain. It mune and physical complaints/chronic has been hypothesized that alterations of the (HPA) axis, the hypothalamic-pituitary-adrenal (SAM) and the sympathetic-adrenal-medullary funrnune system may mediate or facilitate these somatic conditions. The aims of ttris review are to summarize studies that reporrt altered somatic functioning in PTSD andto reviewhow endocrine and irnmune function differentially affect PTSD-related somatic malfirnction. It is hypothestued that alterations of HPA axis and of inflamSAM system permit disinhibition matory mechanisms, which in turn foster the development of somatic diseases as well as selfreported physical complaints. - PostKey words: Inflammation-Comorbidities traumatic stress disorders. p ost-traumatic stress disorder (PTSD) and I its related comorbid somatic diseases are an important health problem. In the United States, about 70o/oof women and 5o/oof men Address reprint requests to: Dr. rer. nat. N. Rohleder, Department of Psychology, University of British Columbia, 2136 west Mall, Vancouver, B.C. V6T 724, Canada. E-mail: [email protected] V o l .3 1 ,N . 4 l Llniuersityof Britisb Columbia, Vancouuer British Columbia. Canada 2Schoolof Psycbotogy Soutbampton, UK of Soutbampton, Llniuersit.y have had PTSD once in their live. While a large number of original and review articles have been published since its first description in the Diagnostic and StatisticalManual for Mental Disorders(DSM), many questionsare still open. One important question is how the psychological disrurbancesin PTSDrelate to the fact that patients often suffer from somatic diseases,or even die earlier due to somatic conditions, such as cardiovascular disease. While the association of PTSD with somatic disease has been well documented (see below), the diseasemechanismsare unclear so far, especially since a large variety of somatic symptoms is reported by people with "medPTSD,and many symptoms are labeled ically unexplained". Thus, it has been assumedthat PTSDis associatedwith typical changes in the endocrine and the immune system that rnay be, at least in pafi, responsible for the somatic complaints seen in PTSD. One of these alterations is t|rat a component of the immune systemof PTSD patients appears to be over-active (while others are not or even suppressed).It appears that this over-active part is the unspecific or innate component of the immune systern. This is a MINERVA ENDOCRINOLOC ICA ENDOCRINEAND INFLAXI\{ATORYALTER{TIONSIN PTSf) ROHI,EDER rather important subsystem as it builcls the first defenseline of our bddies againstinvading pathogens from the environment. Hon'ever. this sub-systemhas a highly damaging potential for host itself. In the healthy organism, it is therefi)re to be kept under tight control. One of these controlling systems is tire hypothalamic-pituitary-adrenal (HPA) axis thrdugh its secretion of the glucocorticoiclhormone cortisol. Interestingly, in I'TSD the HPA axis is fiequently reported to be under-active,leaving the possibility of disinhibition of inflarnmatory responsesmediated by the innate component of the irnmune system.The theory of a hvoo-activeIIPA aris as a mediatorof disease bli.tirir-rninition of the inflammatory svstem is u'eil documentedin animal studiesr,rzrnd has been proposed for several human psychiatric and sornaticdiseasesj* and specifically fbr cardiovasculardiseasein PTSD.5 In this review. lve will discussthe role of changes in the endocrine and the innate immune systen-lin the incidence of somatic diseasesand phvsical complaints in PTSD. Therefore. u,'e n ill first describe the symptomatologr.ancl netrr:rlbasis of PTSD.then on somatic summarizethe current literatr-rre cliseasesin I'TSD. follou,ed Lryan analysisof enclocrineancl inflammatory-alterationsand a conclusive sllrrllnan'. r-na CueS111 . 2 a n d e x a g g e r a t e 6 l 5 1 x 1 1 1 9 . 1 t3. .i Personswith PTSD may also exhibit deficits in attention and working memory as well as difficulty encoding information and inhibiting distractingstimuli.l;,16They may also exhibit enhanced processing of threat stimuli and cues.ll an attentionalbias to trauma-relatecl Vhile on one hand intrusive recollections (e.g. flashbacks) are very vivid and under limited strategiccontrol, the episodic (contextual) memories of the trautnatic event are has lessverbally accessible.This cl1'5ft1nction been related to alterationsin a cortico-limbic network in n'hich amygdala, hippocarnpus and frontai cortical areas play a major role. Intrusive recollections,exaggerateclstartle and enhanced threat processing have Lreen relatedto enhancedamygdalaactivity,lswhile lack of strategiccontrol over the trauma memories, attentionalbias and limited inhibition of distracting stimuli have been reiated tcr poor frontal fr-rnctioning(prefrontal cortex,te anterior cingulate cortex2')).Altered episodic memory functioning has been relatedto profound structural2iand functional alterations22 in the hippocampal formation. Studieson functional br:rin asyrnmetriesll.23ancl functional neuroimagingstttdiesrlpoint to altered connectivityin this netvl'ork.Successfuipharmacological or cognitir.'ebehavioral treatment of PTSDl-rasbeen accotnpaniedby beneficial alterationsin the above describednety761[..]5 28 Post-traumatic stress disorder PTSDhas been obsen'ed as one possible c()nseqllenceof the exposLtreto a severe tratrmatic e\rent. PTSD is characterized Lry s.vmptomsof intrusive recollectionsof the avoidance of- trauma-relatedemotraur.nzi. tions and situations,emotional numbing ancl general hy'perarousal(DSM-IV6).The prevalcnce of PTSD is a function of trauma i.e,.interpersonal trautypc anci clr-rratior-r. rna slrch iis tortllre or serr-ralabutseresults in irigherplcl.alencerates(-, ,-64"u-s) as compareclto :rcciclents and naturaidisasters(101 5 ( . ) ( r ! rl 1. ) ) . PTSI) is relatecl to nLunerolrs cognitivea f i ' e c t i r . ' ep r o c e s s i n g a l t e r a t i o n s , s u c l ' r a s heiglrtenecl physielr*i.'ll respouses t() traLl- Thor-rghPTSD is observed subsequent to severe traumatic experience, its emergence has to be tl'reresult of a complex interaction between various pre-, peri- and post-traumatic fhctors.Processesof fear conditioning, sensitizationancllack of extinction hal'e been discussed,The highly al,ersitreeurotional expcriencemav enhancethe consolidationof tlre trzrumamemory t:ia adrenergic mechais nisms. Tl-rechronicity of the s.vtnpton-rs accornpanieclb,v alterations it-tthe HI)A axis (see belon''), lr'hich rnal' facilitate hip30Rccentl)-,the potenpocarnpalatroph.v.re. tiai contribution o1'pretraLrmaticrisk factors (/.e. pretraLlltlatic l-rasalso been cliscussecl hippocarnpaiatlophl',3tgenetic polytnor-, nhism that facilitate alterationsin neuroiransmitter fr:nctionJ-;. \ I I N I ] R \ - \ E \ I J ( J (- R I N I J L O C I ( . , Dicenrlxe -2006 tr\DOCRINEANI) INFI-AMMATORY ALlERATION*S lN P'lSD ROHI-EI)ER Prevalence of somatic diseases and physical complaints in post-traumatic stfess disorder Chernobyl area had significantly higher IES scores than comparison sr.rlrjects together with higher relative risks (RRs)for self-reporlecl heart disease (1.88 confidence interval Severalstudies.as well as clinical obser- [CI]:1.09-3.22). Furthermore,IESscoreswere vations, harre shourn that the psychiatric corelatecl (r:0.33) with number of self:reporlsymptom complex PTSDappearsto be asso- ed chronic conditions..lT ciated with somatic diseasesand ohvsical Ot 1 399 rnale Vietnam veterans investisymptoms.Tlresebecame especiallyappar- gated lry Boscarino,ss 332had lif'etirnePTSD ent in tJ.S. veterans returning from the as diagnoseclby tl-reDiagnostic Interview Vietnanr Var33 and also in lsraeli soldiers Schedule(DIS).4eAnalysesof self-reported However. as surn- disease symptoms revealed, alrlong others, after the Lebanon\7ar.3a.35 marized beiow and in Table I. somatic corrr- significantly higher odds ratios (ORs) for cirplaints and increased morbidity are not culatorydiseases(1.62).J8 Dobie et al.3einvesrestricteclto military veterans,but also oc--c-ur tigatecl 1 259 f'emzrleVietnarn veterans, 21%u in PTSD after natr-rraldisasters,physical and of wl-rich \\iere screened positive for PTSD sexuralabuse,intimate partner violence and using a PTSD Checklist (PTSD Checklist other trauma. Severaldiseasecategoriesare Civilian Version,PCL-C).50 Vomen with PTSD observed in people suffering from PTSD. reportecl significantly more strokes.-re Among them are cardiovascularcliseases, Sawcl-l,rkst 511.10 (2005) investigated1 41,1 inf-lammatorydiseasesancl a large range of Ar-nericanIndian participants. 750/o of which sornatic symptoms often describeclas mecl- u,ere di:rgnoseclwith lifetin-rePTSD, r-rsing iczrllyunerplained. Tw-elve the CIDI (\flHO version for PTSD51). percent of participantswith PTSD reported carcliovascr.rlar diseases,as corllpareclto only C'ardiouascttlar clisease participants.After correcof nor-r-PTSD 5% One of the rnajor somatic pathokrgies tion for Agc, sex, education,cardiovascular apparentlyassociatedwith PTSDare cardic)risk factors and comorbid deoression. the vascuiardiseases.In a recent revien'. Gancler u-as2 ( CI: 1.1OR for cardiovascularcliscrrse et al. surtmarize several stucliesthat shorv 3.8).i0 highel rates of cardiovascular cliseasesin In tu''o stuclies, self-reported symptons PTSI) patients.s sYx4P]'otis Sttt,-tigpoit'rED An increasednumber of self-reoortecl cardiol'ascr.riar diseaseol diseasesr'niotourswas fotrnclin scveralsttrtlies. Fonler Dtrltlr resistance figl-rtcrs\\'ere studieclb)' Falger et al.:r. Alrolrt 7/2 of then were diagnoseclr.vithPTSD using the StructuredClinical Inten'ien. for DSM-IV(SCID).1-Those ciiagnosedw-ithPTSI) reportecl rnore CVD risk factors inch-rding angina pectoli5.3r, Crvikel et al.J- assessecl P'fSD syn-rptor-ns cmploving thc Lnpact of Event Scale(lES) rs in Israeli imrnigrirntsu,.h<r previor-rsh,livecl in the area ir-npactecl by' the Chernobvinuciearacciclentrrnclcomp:rrison u'iro inrmigratedfi-orl othcr lrcas. sr-rlrlccts no separatL'anal\rsesurere Llnfortr,rnatelt,, maclecontrastingPf'SD and non-PTSDpart i c i p a n t s .I l o u e r e r . p a l t i c i p a n t sf r c i r l t h e \ ' < r l J. 1 . N . r \vere compared with physician-cliagnosecJ disease: Shaler,' et al. investigatecl 98 male combzrt ve'terans, half of wl-rich were diagnosed n ith PTSD using a clinical inten'iewaccording tl-re DSM-III. Veterans rvith PTSD reportecl significantlr' higl-rer rates of cardiovascplar sylnptolns. However, in a medical exarnination, inclucling an electrocardiogram ancl laboratory parameters, fe\\. dif'ferences iretrl,'een both groups of combat \,'eterans u,erc' folrncl. Unsurprisingly, r'eterans n'itl-r PTSD reportecl rnore aclverse health practices. strch as snr<lking ancl ;rlcohol abr-rse.*i Fort-\'-two months afier a catastr()phic l)Llsir fir-e in Ar-rstralia.N'lcFarlane el a/. investigatecl a sarnplc of 70 fire fighters u,'ho hacl clevelopecl PTSD (rs cliegnosccl b.v l)IS ancl IFIS) and comparecl thcm to 70 firc fighters *'itir()ut symptolns. The PTSD group rcportccl signiflcantlr. hishel' Latcs o1'carcliovasctrlarancl !II\F]R\,4 E\I)C)(]RINOI-O(;I(]A ENDOCRINEAND INFLAMMATORYALTERATIONSIN PTSD ROHLEDER Teerr I. - Self-repofied uspbltsician diagnosed cardktuascular cliseasesin PTSDpatients. Sample Stncly Self-reported cardiouascular Falger et a1.36 Results disease Dutch resistance fighters (\7\(/II) (.n=141)t n=82 (.57o/o)with PTSD Higher cardiovascular risk factors: angina pectoris, life stressors, vital exhaustion Cwlkel et a1.31 Immigrants into Israel from Chernobyl nuclear accident area (n:3Q4) vs immigrants from olher arers (n=JJ4): no distinct groups but higher IES in Chernobyl immigrants Higher RRs in Chernobyl groups for heart disease (1.88), anhritis/rheumatism (2.57), or having >3 chronic conditions; conelation of IES with number of symptoms (r=0.33) Boscarino3s Male Vietnam veterans (n:1 399); n=332 (63%) with PTSD In PTSD higher ORs for circulatory (1.62), digestive (7.47'), musculoskeletal (1.78), endocrine-metabolic (1.58), nervous system (2.47), respiratory (1.54) and infectious diseases (2.14) Dobre et orl.39 Female Vietnam veterans (n=1 259); v.tith PTSD n=266 (.270/o) More strokes, fibromyalgia, irritable bowel syndrome, chronic pelvic pain in PTSD Sawchuk et al.4o American Indians (.n=1 471): n:272 (15%) with PTSD OR 2 for cardiovascular disease, controlling for age, sex, CVD risk factors and depression Shelev e,I a/.al Male Israeli combat veterans (n:98); n=50 (510lo)with PTSD More self-reported cardiovascular, neurological, gastrointestinal and pain symptoms in PTSD group No differences in medical and laboratory examination Male Australian fire fighters (n:140) n:70 (50%) wirh PTSD More self-reported physical symptoms and doctor visits; More self-repofted cardiovasculaq respiratory, musculoskeletal a n d n e u r o l o g i c a ls y m p t o m s No differences in medical examination McFarlane et al.a2 Pb ysici an- diagn osed card iouasc u lar disease Boscarino43 Analysis of numbers and causes of death Male Vietnam "theater" veterans (n=7 "era" veterans (n=7 between 1985/1986 and 2000: higher 364); PTSD: 921) vs theater n:836 (rro/a); era: n:214 (2.9o/o) moftality of PTSD positive veterans; HR for all-cause mortalify: 2.1; cardiovascular mortality: 1.6; cancer mofiality: 1.5 Schnurr et a1.44 Older male Veterans (W-s7II/Korea); (n:605); n=6 (70/o)with PTSD PTSD symptoms predict arterial cardiovascular, gastrointestinal, dermatologic and musculoskeletal disease Boscarino et al.4i M a l e V i e t n a m v c t e r a n s( n : 4 4 6 2 t ; n = 1 4 (1%) with PTSD More ECG abnormalities indicative of conduction deficits and MI in PTSD Shemesh el a/,46 MI survivors (n:61); n=13 (20%) with PTSD OR 2.7 for a subsequent cardiovascular event in PTSD group. PTSD: post-traurnatic stress disorder; \W'!flI: \World ITar II; RR: relative risk; IES: Impact of Event Scale; ORr odds ratio; CVD: cardiovascular disease; HR: heart rate; ECG: electrocardiogram; MI: myocardial infarction. 276 MINERVA ENDOCRINOLOGICA Dicembre 2006 ENDOCRINE AND INFLAMMATORY ALTERATIONS IN PTSD ROHLEDER other symptoms. Interestingly, here again a dence of self-reported cardiovascularsympmedical examination revealed no higher rates toms and also physician-diagnosedcardioof these diseasesin fire fiqhters wiril pTSD.+z vascular morbidity and mortality. Oe.lncrvnrv ASSESSED cARDTovASCULAR DTsEASE Diseasesassociated witb inflamffiatory conclitions In 4 studies, cardiovasculardiseasewas diagnosed by a medical examination or In a re-analysesof data from the National review of medical records.In a recent paper, Comorbidity Survey (NCS),Kimerling invesBoscarino analyzed the causes of deltd of tigated medical condirions in a toral of 5 877 Vietnam veterans deceasedbetween 1986 parricipants. Using cIDI, 70.40/o of women and the end of 2000.About 770/o of 7 924 so- and 50/oof men where diagnosed with pTSD. called "theater" veterans,which had served in Self-reportedrates of arthritis and hypertenVietnam, had been diagnosed with pTSD sion were largely increased in both genders compared to 2.90/0of 7 361 "era" veterans, with PTSD, autoimmune diseaseswere sigwhich had served in other areas outside nificantly increasedin female PTSDpatients.:: Vietnam. Resultsshowed that PTSDveterans In a further analyses of a subsample of 2 490 Vietnam veterans'analyzedin earlier studies had a higher mortaliry: at the rime of followup, 11.8%of PTSDposiriveveteranshad died (see above), rates of autoimmune diseases in comparisonto 4.9o/o of PTSDnegativevet- were also significantlyincreasedin the study erans. Calculated hazard ratios (HRs) were by Boscarino on Vietnam veterans.Those 2.7 (CI 7.7-2.6)for all-causemortalityand 1.6 diagnosed with comorbid PTSD were more (:CII.1-2.4)for cardiovascularmoftalitv.'13 In likely to have rheumatoid arthritis, psoriasis or any other autoimmune disease.sa A higha stlldy of 605 olcler militarv veterans, who had served during the Word War II or the er RR for arthritis or rheumatism (2.57; CI 1.12-5.88)was also found in the study by Korea Conflict. Schnurr et al.+* found only Cwikel et al.3'7Dobie et al. also reported high1% with fullPTSD, and assessedPTSDsymper rates of fibromyalgia and irritable bowel toms with the Mississippi Scale for Combat syndrome in female Vietnam veterans with RelatedPTSD.52Despite these low numbers PTSD.39 of PTSD positive veterans, they found In some studies, the occurrence of diaincreased HRs for PTSD symptoms as predictors of arterial (not hypertensive or betes in patients with PTSD was investigated. ischemic)cardiovasculardiseases,lower gas- In both of the studies menrioned above, highHigher trointestinal, dermatologic, and muscu- er rates of diabetes were found.53,54 loskeletal disease.aaIn another study, rates of diabetes (I5o/o)were also reooltecl Boscarino et al. analyzed resting electrocar- in a group of tgS PTSDpatienrsby Weisberg diogram (ECG) data of 4 462 male veterans, et al., as compared to trauma (90/o)and no (6%) controls.5sElevated prevalence 54 of which were diagnosed with PTSDusing trauma of diabetes was furthermore found in anoththe DIS. Controlling for cardiovascular risk er sample of veteranswith PTSD(n:55;23%) factors, as well as anxiety and depression, in comparison with 38 patients with alcohol PTSDwas associatedwith ECG abnormalities dependenc e (80/o).56 In this study, prevalence indicativefor conduction deficits(OR 2.81:CI of heart disease and osteoarthritiswere also 1.03-7.65)and infarctions(OR 4.44: CI t.2increased. 16.43').45 Shemesh et al. investisated 55 myocardial infarction (MI) survivois 1 year after the cardiovascularevent. Twenfv Dercent Pby.sical symptoms and somatic complaints had IES scores higher than the cut-off and Most studies on physical complaints in were thus diagnosedwith PTSD.'Ihesewere PTSD appear to be in fact self,reported fwice as likely to be readmitted due to a car- insteadof physician-diagnoseddiseases,and diovascular event during follow-up.46In sum- some are therefore summarized as medicalmary, there appears to be an increasedinci- ly "unexplained" symptoms. V o l .3 1 .N . 4 MINERVA ENDOCRINOLOGICA IN PTSI) patients Jrtllammtrtctrfr;tutoimmune cliseasescotclselJ'-reporteclsymptoms ilt PTSD T,rnr.rII. - Sample KesUlts Participantsofthe NCS (n=5 877): PTSD of r'vomen; 50.4ol nlcn in 10-0,/o Higher self rcported clisc:rse.Iloth gcn clers: arthr-itts,cliabetes. ancl hypertension. \Vomen: alltoilnmltne diseases \{alc Vietnzrmvcter.lns (n=2 :i9O)l n=5+ (2%) u'ith PTSD; n:12'1 (5%) rvith comorbicl PTSD Highcr rates of self-rcportccl lut()i1'nmune diseasesin cllrrent and conlorbicl PTSL)l cr.rrrentPTSD: psoriasis, gl()me rr.rloncphritis:conlorbitl l)TSL):t'heulll:rt o i c l a r t h r i t i s . 1 ' r s o r - i : r s i sd. i a b e t e s . Stuclv I nflant mab t1t o r tu iritn m u ttt: diseases K r r T l r [ l r n g" hJ(rsclll lnO AI,TER{IIONS ENDOCRINF AND INILAI'{MATORY ROHLEDER '' h.vpothyroiclism \\'eisbrrg e/ a/.tt Dllrd et al.5(' Self' rn;,onn U s.ymptonl s atrl p h.vsi c a I complaints Lttz.et al.1- I)rimal"- care patients rvith PTSD (n=185) vs tratlma (n:233) ztncl non-tmrtnla (n:8,i ) control patients Nlor-ecliabetcs. arthritis. asthma. ecze m:r, back pain in PTSI) groLrP !-cterans n'ith P'fSD (n=i5) r"s pxtients t-ith alcohol clepenclcnce(n:J8) rs N{oreclialttes in PTSD veterans(2JLl'ir) alcohol clepenclentcolltl-ols ( 81rir) Vietnalr vcter:tns*'ith ancl s ithotrt PTSD slrllptollls: tinnittls. rapicl Selt'-r'eportecl bleething. tacittg heet-t.sextlal clisintcrest. buttetf-lies in the st<:rlllach. :rt-rcl n1t Ltseil \\olfc e,ra/.18 Female Victnam veterans (n:109)t I'TSD clepencling on cut-<>ff in 27 .501'tr'l ,1-0rb P'I'SDscore predrcecl sell-reporteclcar cLovascular,gastrointestin:ll, gynecokrgical. clcrmrtological, ophtalmologicel sVmptolns anct Paln Kirrcrling e/ a/.;e Fcrn:rle Vietnerll \eter:itls (n:51): (2J'r'tr) t'tlt PTqL) tlighel latcs of self'-rcportcclfirlgetfirlncss. flttiglrc. elt-lr :ts'ltkening. restless sieep. ston-rlchltrttltltttls. tttttsclt l e:tk- n=ll NCSS For:c\et al.6t) s/agner e1a/.('L Dolll'e et al.1') P-l \l): lr"'t-tr'f, tl LIl.llr( Culf \{'ar vetcrans (n=31i9): 237 of ri'hich s'erc diagnosecl :rs persistentlv ill ancl I12 l'ere he:rlthy PTSI) scolcs s tre higher in pel'sistentlv ill. n'ho reported gastr-ointestinal.ancl nltrscle shin/mr-tcottscourllllints. f :rtigr-le. or loint pain Gulf War vcLeret'rs( r-r:2 301: 8(i/0\\'()nlen); of \\'()tttcn :rncl f .3'l'irof PTSD in 7.1J0/o nlen PTSI) scores werc associated rvith kr*c-t' sclf rtportccl health F e n a i e V i e t n e r t . tv e t c r a n s ( n = l 2 5 9 ) n : 2 ( 1 6( l l r , i , ) \ ' i t h P T S D Loler scorc'son stlbiectilc phlsical health qtrestiollrtaife(gellcrlrl lrcaltll. r i t a l i t r ' .b o c l i l v P a i n ) strcss clisorclerr\CS: \lttionri Ctrllclrbiciin- Srrrvcr Lrt7.et al. founcl higher self reporled phvs- for PTSD 2rnclfouncl to preclictself-reported gynecological, gastrointestinai' icalcomplaintswhen cornparingsmall groups carcliovllscttlar, i' of veterans vn'ithand withor-tt P'fSf) In a dermatological,clphtalmologicaIs,vmptolns str-rclvon f'ernaleVietnam veterans (n=109). as well as pain.5sKirnerling e/ a/. inr''estigzrtvetPTSDrn'asassessedby the MississippiScelc ed another gr()Llpof 52 female Vietnatn 218 M]NI]R\A F]NI)OCRINOI-OLII(]A I )i(rernl)re 2006 ROHLEDI.]R ENDOCRINE ANI) INFLAMMATORY AI,1'I.]RATIONSIN PTSD erans,12 of which were diagnosedwith PTSD r-rsingSCID and Clinician-AdministeredPTDS Scale (CAPS).They found not only higher rates of self-repofied forgetfulness,fatigue, early awakening, restlesssleep, stomach problems, ancl muscle weakness, but also found that PTSD predicteclhealth perception. Further analyses revealed that more physical symptoms and lower health perception were primarily associatedwith the hyperarousal symptom cluster of PTSD.5q In another study gastrointestinaland other "unexplained" physical symptoms, such as fatigue, muscle or joint pain, skin/mucous comDlaints.were associatedwith scroreson In a cohort of the MississippiPTSD scale.6o 2301 Gulf War veteransof mixed gender (8% women), PTSD was assessedusing the Mississippi Scale.5zPTSD symptoms were associatedwith low follow-up scoreson selfreported health as assessedby a Health Symptom Checklist 2 years later.61The 266 ftmale veterans n-ith PTSD from the study bl' Dobie et al. adclitionallt' hacl lorver scores assessingsubiectivephyson a questionn2rire ical syrnptolrs in categoriessttch zlsgeneral health, boclily pain, and vitality:r (Table II). Interestingly,many of the symptoms repofied above, such zrsmllscle pain, joint pain, nallsea, fatigue, skin problems, and even decreasesin general well-being are typically found in stateswith heightened inflammatofor example during infections and ry activity, labeled "sicknessbehavior".('zIncreaseclconcentrati()nsof circulating inflammatory mediators are capable of lowering pain thresh"medolds63and may thus be able to explain ically unexplainecl" symptoms. autoimmune diseases,as well as diabetes "unexplained" physical comand so-called plaints, is that all of them are associatedwith or, at least in part, mediated by circulating Ingls2sed coninflammatoly mediator5.63-65 mediators, in inflaurmatory centrations of of alterations the conseqllence nray be turn, in the function of the endocrine stressresponse systems, i.e. the HIA axis and the (SAM) syssyrnpathetic-adrenal-medullary tem.3,1The following section will therefore be dedicated to the analyses of literature on endocrine alterationsin PTSD. Endocrine changes in post-traumatic stfess disorder PTSD is associated with Profound endocrine changes,most of which appear in the systems crttcial fbr the stress response, /.e. the HIA aris ancl the SAM system. Hypoth ala m usp itu it a4y adrenal axis The HPA axis is a complex hormone system and severalaspectsof its function can be altered. We will focus here on basal HPA axis activity and feedback sensitivity,as these are the aspectslnost relevant for somatic diseasesand innate immune function. Readers interested in comprehensive analysesof HPA axis function are directed to the excellent review by De Kkter et a1.66 R,qser HvpotHALAMIC-t'ITttITAItYAXISACTIVIT\- Basal HPA axis activity can be assesseclat several levels of this hierarchic hormone system. An interesting feature of PTSD is the Conclttsions cliscordance between increased activity of ln summary, PTSD appearsto be associrt- the HPA axis at a central level and lower ed with many diff'erentsomatic diseasesand activity in the periphery. In detail, cerephysical complaints. Best documented are brospinal fluicl levels of corticotropin releaselevated rates of carcliovasclllardiseases,5 ing l-rormone (CRH) have been found l)ut rates of diabetes and autoimmllne ()r increased in PTSD patients in 3 independent although in the latter stucly, the inf-lammatorydiseasesare also increased. stLldies,6T-6e was that cerebrospinal fluid finding main physirangle of self:reported a Furthermore, (CSF) are increased and correlated cortisol are detriments health ancl cal complaints with CSF CRH levels. reoortecl. In the periphery, findings are less clear. A common featurreof cardiovascr,tiarand V o l .3 1 .N . a . \ l t N L R \ A F N t ) O C t i l \ ( ) L () C T . \ ENDOCRINEAND INFLAMMATORYALTERATIONS IN PTSD ROHLEDER First resultswere obtained by measuringurinary cortisol excretion over periods of 12 or 24 h. These measurementsorovide an estimate of overall cortisol output over the timespan chosen and are a good marker for basal HPA axis activity. Lower urinary cofiisol concentrations of PTSD patients have been reported in the majority of studies, comparing PTSD patients with psychiatric controls,7o, 71traumatized patients without PTSD,uzor normal 661t161s.73-76 In contrast,urinary cortisol excretion was found increasedin PTSD patients in 3 studies.l-zq Several studies have reported on single time-point measurementsof plasma cortisol. However, as single measurementsat random time points arc of rather limited validity given the considerable variability of HPA axis activity throughout the day, we will only review studies in which cortisol measurements are obtained over severaltime-points of the day, with relation to the circadian rhythm of this hormone system. The first study reporting on alterations of circadian cortisol secretion in PTSD patients was published by Yehuda et al. They obtained plasma samples from combat veterans every 30 min over a total period of 24 h. Compared to healthy controls, veterans with PTSD had significantly lower plasma cortisol levels throughout the day.aoBremner et al. reported lower plasma cortisol levels in the first half of the day in abused women with PTSD as compared to abused and non-abused women without PTSD.81Through cortisol measurements in saliva, we were able to replicate these findings of low cortisol levels in a sample of civil war refugees from BosniaTaand in a sample of PTSD patients traumatizedby severeaccidents,violent crime or sexLlalassault.sz Most notably, in both studies we showed for the first time that the normal cortisol awakening response83of the HPA axis appears to be blunted in PTSD. In a recent study, Yehuda et al. investigated circadian salivary cortisol levels of Holocaust sulvivors with and without PTSD (mean age: 69 years) and found that those with PTSD had flattened cortisol trajectories.s4 Young et al. measured salivary coftisol levels in a larger community sample of 575 par- ticioants. In contrast to the studies summarized above, 56 indivicluals with PTSD had increasedevening cortisol levels, while morning levels were unchanged.asLindater et al. reported higher early morning and total (area under curue) salivarycofiisol levels in a group of 12 Dutch police officers with PTSD in relation to traumatized police officers without PTSD.86The authors' explanation for these differences is that the trauma in their study was relatively recent compared to rather long interuals between trauma and study in most of the other studies. This interoretation is consistentwith findings Froma rccent metaanalysisby Miller et al.,where time between trauma and assessmentwas negatively associated with daily cofiisol output.87This metaanalyses of HPA axis changes following diverse acute and chronic stressorsincluding trauma furlher revealed that daily corlisol output was reduced (d=-0.34) and evening cortisol levels were increased (d=0.47) in people with PTSD. FrEogacr SENSITIVITy In a comprehensive review of pharmacological and non-pharmacological challenge tests for the HPA axis, De Kloet et al. also summarize the results of the low-dose dexamethasone suppression test (DST).66Via oral ingestion of 0.5 mg of dexamethasonein the evening and assessmentof cofiisol levels the following morning, the sensitivity of the HPA axis towards the negative feedback effects of glucocorticoids can be tested.While early studies using the classical 1 mg DST were not successfulin detecting alterations in feedback sensitivity in PTSD, studies using the low-dose DST revealed a tvDical disturbance in PTSD patients, descrihed as supersuppression.The first study to report this finding was published by Yehuda et al.They showed that 2L combat veterans with PTSD had significantly lower plasma cortisol levels at 08:00h in the morning after ingestion of 0.5 mg dexamethasonecompared to 12 healthy controls.8sThese findings were subsequently replicated in several other studies from this group. The findings were also extended to patients traumatized by childhood sexual MTNERVAE\ DOCRINOLOCICA Dicembre2006 ENDOCRINEAND INFLAMMATORYALTERATIONSIN PTSD eoThe quantitative meta-analysisby abuse.8e, Miller et al. also revealed lower postdexamethasone cortisol levels @:-0.25) in PTSD patients.sT ROHLEDER hypoactive HPA axis and hyperactive SAM system) are theoretically compatible with such a disinhibition, we will in the following section review the literature on immune disturbances in PTSD with a focus on signs of overactive immune processes. Sympath etic-adrenal -medullary system Three aspectsof immune function in PTSD Similar to the HPA axis, the SAM system have been investigatedso far. The vast major' appears to be over-active at a central level, as ity of studies focused on numbers and perevident for example by the finding of centagesof circulating immune cells and their increased norepinephrine levels in CSF, subtypes. This is by far the easiest way to repofted by Geracioti et al. in 11 male com- obtain measures of immune function, but bat veterans with PTSD.elIn contrast to the also the one with the leastinformation about HPA axis, this increased central activity is the statusof the immune system.Some studaccompaniedby a higher peripheral activity. ies have employed functional assays,mainly Enhanced urinary excretion of epinephrine or by applying antigensto the skin and investinorepinephrine has been reported in sever- gating delayed type hypersensitivify responsal studies.For example, in women with PTSD es, while others have assessedthe ability of after childhood sexual abuse,78in mothers natural killer (NK) cells to fight tumor cells in with PTSD caused by a child suffering from uitro.whlle thesefunctional assaysprovided cancer,75and in Bosnian war refugees with better information about the ability of the PTSD (marginally significantra). However, immune system to fight infection,l+they are Pitman et aL reported unchanged urinary cat- less useful for predicting the negative outecholamine excretion in a sample of combat comes of immune over-activation.The most veteranswith PTSD.77 informative measure in this regard are conPlasmalevels of norepinephrine have been centrations of circulating inflammatory medireported to be elevated by Yehuda et al. in ators, such as interleukin-6 QL-6), tumor PTSDpatientswithout comorbid depression.ez necrosisfactor-cr(TNF-cr),IL-1, and the acute However, in the study by Geracioti et al. phase protein C-reactiveprotein (CRP),which despite higher concentrationsin CSF,norep- have proven useful in predicting inflammaineohrine did not differ between PTSD tory disease related morbidity and mortalipatlents and controls in plasma.er ty.e5 Interestingly, PTSD patients are further reported to show increased sympathetic and Immune cell numbers catecholaminergicresponsesto trauma cues In summary, PTSD and other stressors.93 Largely divergent findings have been patients are characterizedby a noradrenergic reported for immune cell counts and perhyperactivity, which appears to be associat- centages.Some studiesreport higher numbers ed with the hyperarousalsymptom complex of total leukocytes, lymphocytes and certain of the disorder. subtypes for example in combat veterans with PTSD,e6or in women tratmatized by childhood 2buse,e7where numbers of total leukocl'tes, as well as B and T lymphocytes Imrnune changes in post-traumatic were correlatedwith PTSDseverity.However, stfess disorder several other studies report unchanged or Based on the factthat many of the somat- lower numbers of the same immune cells. ic diseasesand physical complaints reported Ironson et al. fotnd that numbers of leukoby PTSD patients could potentially be medi- cytes did not differ between hurricane victims ated by a disinhibition of inflammatory medi- with and without PTSD,while NK cell numators, and further based on the fact that the bers, but not function, were higher in PTSD endocrinologic disturbancesin PTSD (i.e. victims.esLower T and B lymphocyes in peo- V o l .J l , N . 4 MINER\A ENDOCRINOLOGICA ENDOCRINE AND INFLA}I\,IMORY ROHLEDI]R ALI'ER{TIONS IN PTSL) of I'TSD patients. One group of researchers f o u n d l o w e r c o n ( e n t r a t i o n so f C R P i n refugeesfrom the Iraq suffering from PTSD10e In contrast to this result, 5 other studiesreport increased plasma concentrations of inflammatory/mediators. Higher concentrationsof IL-1, were found by Tucker et al. in 58 PTSD patients,110 and by Spivak et aL in 19 Israeli combat veteranswith PTSDrll in contrast to healthyvolunteers.In the latter sample,PTSD duration was associatedwith IL-18,levels. Increasedconcentrationsof IL-5 have been reoorted in accident victims with PTSD as and in comcompared to healthy controls,112 Immune cell.function bat veteranswith PTSD.It-rIn this latter str-rdy, Six studies have investigatedthe ability of higher IL-6levels were found only in the secNK cells to lyse specified target cells in uitro, ond half of the day, which is interesting as again with inconsistent results. Four studies cofiisol levels are relatively low at this time of found that PTSD Datients'NK cells were less day in healthy controls and even more so in efficient ccrmpa.edto the respective control PTSD patients.Ta Furthermore, Baker et al. groups without PTSD or participants with IL-6 concentrations in increased also found 103 Jqle less severe PTSD symptoms.es9e,102' cerebrospinal fluid of their PTSD sample, studiesreported contrary results, i.e. increased possibly show.inga central disinhibition of NK cell cytotoxicity in combat veteranswith inflammation.r1J PTSD,to+and a sample of rescue workers Further information about inflammatory with varying I'TSD severity.to5 processescan be obtained by in uitro stimuThree stlrdies assessedthe efficacy of the lation of whole blood with mitogens and meacellular immune response by applying antisuring inflammatory cytokines. Such assays gens to the skin and measuring the local provide information of the potential responirnmune resDonse. \7hile Boscarino et al. sivity of the individual's inflammatory system were not ablb to detect differencesbetween in the presenceof respectivestimuli, such as PTSD patients and controls,e6the remaining pathogens,allergens,or other danger signals. studies found increases in cell mediated Two srudiesmeasuredthe T helper 1 cyokine 106 immunity in combat veterans with PTSD interferon-y (IFN-, after stimulation of whole and in abusedwomen with PTSD.1o7 blood with lipopolysaccharideand phytohemagglutinin. The results are inconclusive: Inflammatory,t mecliators while Kawamura et al. found lower in uitro As noted above, the peripheral concentra- IFN-y secretion in 12 traumatized men with tions of inflammatory mediators are of central PTSD, \Woodset al. found the opposite, i.e. interest for predicting long-term health out- increasedconcentrationsof IFN-A in abused 11:tJlg5e divergent comes. Inflammatory mediators such as IL-6, women with PTSD.ee. to results may be explained by gencler differIL-18,TNF-o and CRPare now reco5anized stimulate atherosclerosis,the main cause of ences.As we have shown earlier,ll' large sexdiseases.6a to foster insulin differences exist in ex uiuo inflammatory cardiovascr-rlar 1e responseswith generally higl-rercytokine proresistanceand thus callsetype 2 diabetes,65 lower pain thresholds6:and, thus, increase duction levels in women. In a third study the likelihood of experiencing any physical assessingthe potential to mount an inflammatory response,we \\,'ereable to show that symptoms. In fact, as summarized inTable III, 6 stud- Civii \Warrefugeeswith PTSD(mlred gender) ies have measured the concentration of dif- producedsignificantlymore lL-6 and TNF-o irz f-erentinflammatory mediators in the plasma uitro compared to healthy controls.Ta ple with PTSD were also reported by Kawamura et al.e9 of immune In summary,simple assessment cell numbers in PTSD has not yet revealed a consistent pattern. More promising may be the results by Dekaris et al. anclWllson et al. Both groups of authors report higher nurnbers of immune cells that show a phenotype indicative of immune activation in PTSDusing 101flsv/svsr, these results flow cytometry.100, warrant replication, befbre further conclusions can be drawn. \4I\FR\A F\I)O'.RI NOLOCTCA Dicembre 2006 ROHLEDER IN PTSI) ENI)OCRINEAND INFLAMMATORYALTE}G-TIONS Ts,ztu lll.-Inflammatotl) mediators in PTSDpatients. Results Sample Stucly Circulating inflammatory Miller et al.1o8 mediators Accident or assault victims (n=15) ers No llroup differences in CRP and sIL-6R comelation of CRP and SIL-6Rwith PTSD tlauma controls (n:8) severity Sonclergaarde/ a/.109 Refugees from lraq (n:tl6); partial PTSD: n=24; full PTSD: n:32 Lower CRP and serum amyloicl A in PTSD Ttcker et al.l\t) Outpatients with PTSD (mixed trauma; n=58) erstrauma controls (n=21) Higher It-1p ancl lower sIL-ZR in PTSD Spltrk et ctl.111 Israeli combat veterans with PTSD (n:19) vs healthy controls (n=19) Highcr lL-1B in PTSD; correlation of ILlB t\irh PTSD duration (r=0.54) Maes et a\.112 Acciclent victims with PTSD (n:13) z,s Higher IL-(r and sIL-6R in PTSD; r-rodiff'erence in additional inflammatory healthy controls (n=32) r n e d i a t o r s( s g p 1 3 0 , I L 1 R A , C C 1 6 , a n d sCDB) Btker et al.IlJ Combat veterans with PTSD (n=11) tr.s Higher IL-6 in samples befbre 14:00 h; no IL 6 differences in the afternoon; healthy controls (n:8) higher IL-6 in CSF In L'itr() stimuldted ntetlicttrtrs Kan'anrura e/ a/.')') inJlantntator.y Trauniltizecl workcrs rvith PTSD (n=12) z'-s trauma cor-rtrols(n:48) Lo.ver LPS- .rncl PHA-stimulated ploduction of interi'eron-1 (IFNY) and IL-,1 \(oods e/a/.ir' intimate partner violence victirns (n:62; ri'ith PT'SD: n=39) rs non-abused controls (n:39) Highel LPS- ancl PHA-stimulated IFNY in abused v!'omen r'vith PTSD Rol-rleder eI a/.; i Civil war refugees with PTSI) (n=72) us hcalthy controls (n:13) Higher LPS-stimulatedproduction of IL6 and TNF; incrcascd GC sensitivity of IL-6 and TNF-cr P r t r e n t su i t h r r p i d l r p l o g r e s . i v c p e r i o dontitis (n=20, all with PTSD) r.sheaithy controls Increased incidence of rapidly progressive periodontitis; higher salivaly IL-6 in perioclontitis patients Patients admitted to the emergency roon afier a life-threatening e'vent (n:24; n= tl n-ith PTSI) afier ,i rnonths) Gene chip/microarray: reducecl expression of genes involvecl in transcriptio nal activation; distinct expression of genes involved in inmune activation Ot h er in llamm.ttotry markers Ltrer et a1.115 Segm:rn e/ a/.1l6 PHA: phyttthemag stressclisofder;CRP:C-reactir.eproteini CSF:celebrospinalfluicl;LPS:lipopolysaccharider P'lSl): post-trllrnatic 'l'NF: glutininl tr.rmornecrosislactor;GC; glucocorticoicl. 'I'wo other studieshave investigatedinflarnmatory parametersin PTSDpatientsutilizing a nor.'elapproach. Aurer et al. found higher periodontal inflammation in PTSD patients corrpared to controls.lls tJsing microarray technique, Segman et aL investigated gene erpression of peripheral Lrloodmononuclear cells that were obtained imrnediatelyas well \ i , 1 .a i . N . 4 as 'i rrronths after l'reumatization. They were able to demonstratethat gene profiles could distinguish those with PTSD from those without PTSD. Interestingly, those with PTSD (n=13) and higher IES scores showed overexpression of genes that signify immune activation.116 In summary, it appearsthat PTSDpatients MINERVA ENDOCRINOLOGICA )Rt ENDOCRINEAND INFLAMMATORYALTERATIONSIN PTSD ROHLEDER response system. Although some of these data are preliminary and thus have to be interpreted with caution, we conclude that in PTSD, all three assumptionsare met. PTSD Datientsshow more somatic diseasesthat may be caused or acceleratedby peripheral inflammation, have a disturbed endocrine system that may foster inflammation, and show increased inflammatory activity. Unfortunately, no study has investigated all assumptionsin the same sample of subjects. Therefore, it remains unknown whether the Conclusions . endocrine changes are the consequence of In the present review, we set out to find PTSD, and whether the endocrine changes evidence for the hypothesis that the increased are the main cause of inflammatory disinhiincidence of somatic diseasesand physical bition. Detrimental health behaviors, in turn, could complaints in PTSD may be mediated by typbe an additional or alternative mediating facin the system, ical disturbances endocrine tor befween PTSD and inflammatory disininflamwhich in turn foster disinhibition of hibition. PTSD patients repofi more drug and mediators. matory In this we regard, we first reviewed stud- alcohol abuse, and are more often smokies reporting that PTSD patients show high- ers.rle Deleterious health behaviors are not er rates of cardiovascular,autoimmune, and only independent cardiovascular risk factors, inflammatory diseases,including diabetes. but also foster disinhibition of the inflammaMost of these data stem from self-reportsof tory response, thus being able to increase PTSD patients, together with many studies the risk of all diseasesreported for PTSD.120, evidencing a large array of physical com- r21 In eonclusion, the association of somatic plaints. Interestingly,all of these diseases, including so-called "medically unexplained" disease,endocrine alterations and inflamsyffrptoms could be explained by assuming a matory disinhibition in PTSD appears promisdisinhibition of the inflammatory response ing in supporting the hypothesisthat inflamwith heightened plasma concentrations of matory disinhibition mediated by endocrine inflammatorymediatorssuch as IL-6, [-18, or alterations foster the heightened incidence 65Cardiovasculardiseasescan alter- in somatic diseasesin PTSD. However, to CRP.63 native be explained by the hyperarousal substantiatethis hypothesis, clearly more evisymptom complex mediating damage to the dence is needed, optimally assessingimmune heart and circulatory system by increasing and endocrine parametersas well as health heart rate and blood Dressure.llOur review outcomes in longitudinal designs. of the literature furthermore supported the assumption that PTSD is characterizedby typical alterationsin the endocrine systems. Riassunto Most, but not all, studies show a hypoactive HPA axis with lower cortisol levels, which Disturbo post-traumatico da stress: ruolo delle alterazioni enelocrine e infiammatorie nei rJisturbi somacould be the main factor for disinhibition of inflammatory response,together with height- tici comorbosi A partire dalla sua prima descrizione nel Diagnostic ened activity of the SAM system,which can and StatisticalManual for Mental Disorders (DSM), il stimulate inflammation uia activation of the disturbo post-traumatico da stress (post-traumatic 1 18 transcription factor NF-r<B. stressdisorder, PTSD) e stato carattertzzatocome un In summarizing, studies investigating disturbo del funzionamento affettivo resposabile di immune functioning in PTSD,we found evi- notevole sofferenza. Inoltre, d stato riconosciuto che dence for an over-active inflammatory il PTSD non d solamente accompallnato da una compresent with increased circulating levels of inflammatory mediators. F{owever, these results have to be interoreted with caution at this point. as most of the studiesinvestigated a rather low number of subjects. Furthermore,measurementsof unstimulated inflammatory mediators in plasma are somewhat troubled by concentrationsclose to the detection limit of most assaysavailable. MINERVA ENDOCRINO],OCICA Dicembre 2006 ROHLEDER ENDOCRINE AND INFLAMMATORY ALTER{TIONS IN PTSD promissione generale dello stato di salute, ma anche da un numcro pii o meno specifico di patologie somatiche di natura cardiovascolare, autoimtnune, di disturbi fisici e dolore cronico. E stato. inoltre. ipotizzato che queste condizioni somatiche possano esseremediate o facilitate da alterazioni dell'asseipotalamo-ipofisario, del sistema simpatico e aclrenomedullare e del sistema immunitario. Gli obiettivi di questa revisione sono: 1) esarninare gli studi che riportano alterate funzioni somatiche nel PTSD e 2) discutere le rnodaliti con cui le funzioni endocrine e immunologiche incidono in modo differenziale sulle alterazioni somatiche PTSD-correlate. Si ipotizza che alterazioni dell'asse ipotalamo-ipoflsario e del sistema simpatico e adreno-medullare t'isultino in r-rna disinibizione dei meccanismi infiammatori, che, a loro volta, scatenano lo sviluppo di disturbi somatici e dei sintomi fisici lamentati dal paziente. Parole chiave: Infiammazione - Comorbiditi Disordini post-traumatici da stress. References 1. Stcrnberg EM, Hill JM, Chrousos GP, Kamilaris T, Listwak SJ, Gold Plilr et al. Inflammatory mediatorinduced hypothalamic-pituitary-adrenal axis activati()n is defective in streptococcal cell wall arthritis surjccptilrle Lewis rats. Proc Natl Acad Sci U S A 1989;86: 2374 8. 2. Sternberg EM, Young WS 3Ld, Bernardini R, Calogero AE, Clrrousos GP, Gold P'il/ et al. A central nervolls systeln defect in biosynthesis of corticotropin-relea sing honnone is associated with susceptibility b strept()coccal cell wall-induced arthritis in Lewis rats. Proc Natl Acacl Sci U S A 7989:86:4771-5. 3. Heim C, Ehlert U, Hellhammer DH. The potential role of hypocortisolism in the pathophysiokrgy of stressrelated bodily disorders. Psychoneurocndocrinology 2000;2i:1-35. .1. Raison CL, Miller AH, When not enough is too much: the role of insufficientglucocorticoid signaling in the pathophysiology.of stress related disorders. Am .l Psvchiatry 2003:760:7i5 4 6i. 5. Gancler ML, von Kanel R. Myocardial inf'arction and post-traLlffratic stress clisorclcr: frequency, outcome. :rncl atherosclerotic mechanisms. EurJ Cardiovasc Prev Rehabil 2006:13 :1.65-7 2 (r. APA. Diasnostic and statisticalmanual of mental disorclers. Washington, DC: Arnerican Psychiatric Association; 1991. 7. Bichescu D, Schauer M, Saleptsi E, Neculau A, Elbert T, Neuncr F. Long-term consequences of traumatic experiences: an asscssrnentof former political detainccs in Romania. Clin Pract Eoidemol Ment Health 2005:1:17. | { . 5 o l () m () n : D . D . r v i c l . o nj R . T r a r r n a : p r ( v a l ( n ( ( . i r n p J i r rnent. service use, ancl crrst..JClin Psychiatry 791)7;58 S r , r p p9l r i - 1 1 . 9. Kr-rchK. Cox BJ. Evans R.J.Posttrallmatic stress disorder and motor vchicle accidents: a multidisciplinary r ) \ ( n i c \ ^ . t . a n J l ' s y t h i a t r yl ' ) ( ) 6t l t 2 q - J - l 10, Kohn R, Levav 1, Garcia ID, Machuca ME. Tamashiro R. Prevalence. risk factors and aging r,'ulnerabiliry fcrr psychopathology following a n:rttrral disaster in a cleve loping country. Int I Cleriatr Psychiatry 2005;20: 835-11. \ b l . 3 1 .N . 4 11. Buckley TC, Kaloupek DG. A meta-anal1'ticexamination of basal carcliovascular activity in p()sttraumatic stress disorder. Psychosom Med 2001;61;585-94. 12. Karl A, Malta LS, Maercker A. Meta analytic review of event-related potential studies in post-traLrmatic stress rli'ordcr. Biol Psychol2006;-l: l2J- r-. 13. Shalev AY, Peri T, Orr SP,Bonne O, Pitman RK. Auditory startle responses in. helpseekingtrauma survivors. Psychiatry Res 1997;69:1-7. 14. Metzger L.j, Orr SP, Berry NJ, Ahcrn CE, Lasko NB, Pitman RK. Physiologic reactivity to startling tones in women with posttrallmatic stress clisorder. J Abnorm Psychol 1999;108:347-52. 15. VasterlinglJ, Brailey K, ConstansJI, Sutker Pts. Attention and memory dysfunction in posttraLlmatic stress disorder. Neuropsychology 1998;12:725-33. 16. Vasterling lJ, Duke LM, Brailey K, Constans JI, All.rin ANJ, Sr-rtkerPB. Attention, learning, and memory perfbr mances ancl intellectual resollrces in Vietnam veterans: PTSD and no disorder comparisons. Ncuropsychology 2002:16:5-11. 17. BuckleyTC, Blanchard EB, Neill WT. Information processing and PTSD: a review of the empirical literature. C l i n P s y c h u l R e v 2 0 0 0 : 2 0 l:0 r I - 6 s . 18. Protopopescu X, Pan H, Tuescher O, Cloitre M, Goldstein M, Engelien rW et al. Differential time courses and specificity of amygdala activity in posttraumatic stress disorder subjects and normal control subiects. Biol l'sychiatry 2005;57:461-73. 19. Matsuo K, Taneichi K, Matsumoto A. Ohtani T, \'amastte H. Sakano Y et al. Hypoactivation of tfre prefrontal cortex dllring verbal fluency test in PTSD: a near infrarecl spectrosc<.rpystlldy. Psychiatry Res 2003;12'i: 1-10. 20. Shin LM, Wl'ralen l' J, Pitman RK, Bush G, Macklin ML, Lasko NB et al. An fMRI study of anterior cingulate function in posttraumatic stress disorder. Biol Psychiatry 2001:i0:932-42. 27. Karl A, Schaefer M, Malta LS, Dorfel D, Rohleder N, rJilerner A. A meta-analysis of structural brain abnorrnalities in PTSD. Neurosci Biobehav Rev 2006 [Eputr aheacl of printl. 22. Shin LM, Shin PS, Heckers S, Krangel TS, Macklin ML, Orr SP et al. IJippocarnpal function in posttraumatic stress disorcler. Hippocarrrpus 2004;1'I:292-3Q0. 23. Rabe S, Beauducel A, Zollner T, Maercker A, Karl A. Regional brain electrical activity in posttraumatic stress disorder after motor vehicle accident. J Abnorm Psvchol. In oress 2006. 24. Lanius RA, \izilliamson PC, Densmore M, Boksman K. Neufelcl RW, Gati JS et al. The nature of traurnatic mernories: a 4-T FMRI functional connectivity analysis. Arn J Psychiatry 2001,161:36-44. 25. Fernanclez M, Pissiota A, Frans O, von Knorring L, Fischer H, Fredrikson M. Brain function in a patient with torture related post traumatic stress disorder before and after flLx)xetine treatment: a positron emission provocation study. Neurosci Lctt tomography 2007:297:101-1. 26. Karl A, Maita LS, Alexander J, tslanchard EB. Starile responses in motor vehicle accident sLul.ivors:a pilot :223-37. stucly. Appl Psychop\siol Biofeedlrack 2O04;21) 27. Karl A, Itabe S. Zollner T, Maercker A. Psychophysrological corrclates of PTSD symptom rcchrction induced by psychotherapy. Psychophysiology 2005;50: 28. Vermetten E, Vythilingam M, Southwick SM, Charney DS. BremnerJD. Long{erm treatmcnt w'ith paroxetine increases verbal declarative memory and hippocampal r'olurne in posttraumatic stress clisorcler.Biol Psychiatry 2003:54:693-7O2. 29. McEwen BS. Thc neurobiokrgy and nelrroendocrino- . \ 4 I N F R V AF N I ) O C R I\ U L O C I C A 285 ROHLEI)ER EN])OCRINE AND INI.'I,AMMATORY AI,TF]RA'I'IONSIN PTSD logy of stress. Implications for posttraumatic stress disorcler from a basic science perspective. Psychiatr Clin N<rrth Am 2002;25:469-94,ix. 30. Sapolsky RM. Atrophy of the hippocampus in posttraumatic stress disorder: how and when? Hippocampus 2 0 0 1 ; 1 1 : 910. Gilbertson MW Shcnton NIE, Ciszewski A. Kasai K, Lasko NB, Orr SP et al. Smaller hippocampal volume pre dicts pathologic vulnerability to psychological traurna. N a t N e r r r o s c i2 O O 2 ; 5 : 7 2 172. Lee HJ, Lee MS. Kang RH, Kim H. Kim SD, Kee BS et al. Influence of the serotonin tfanspofier pfomoter gene polyrnorphisrh on susceptibility to posttrallmatic stress disorcler. f)epress Anxiety 2005;27:735-9. 33. Control Cfl). Health statlrs of Vietnam veterans. II. Physical flealth. The Centers for Disease Control Vietnam Experience Str-rcly.JAMA 7988;259:2708 I1+. 3z+.Solomon Z. Mikulincer M. Combat stress reactions, p()st traumatic stress disorder ancl somatic complaints a m o n g I s r a e l i s o l c l i e r s .J P s y c h o s o m l i c s 1 9 8 7 : 3 1 : 131-7. J5. Solon'ronZ, Mikulincer M, Kotler MI.A rwo year tbllorvr-rpc.rfsomatic complaints among Israeli comllat stress r e a ( t j ( ) n c a s u a l t i e s . .P l s y c h o s o r nR e s 1 9 l l 7 ; 3 I: 4 6 3 - 9 . F-alger-PR.Op dcn Velde W, Hovens JE, Schouten EG, De Crocn.fH. \'an l)uijn H. Cr:rrent posttraumatic stress c l i s o r c l e ra n d c a r d i o v a s c u l e r c i i s c a s e r i s k i a c t o r s t n Dutch Resistance veterans from \7<rrlcl War II. Ps1-c'll,),1r.r Psvchosom 1992ai7J.61-17. Cwikel J, Abclelgani A. GoJdsmithJR, Quastel M, Yevelson II. Ts.'o year fbllorv up study of strcss-rclatcrl clisorclers among imlnigrants to Isr-aclfrom thc Chernobyl :rrea. llnr.'iron Hcalth i)erspect 1997:105 Suppl 6r 15 , i 5 - 5 0 . Bosc:rrino JA. Diseases rmong rlren 20 ycars afier erposr-r fe t() sevefc stress: implications firr clinical research anrl rneclical c.rrc. Psvchosonr Nlecl 1997:59:605-1.i Doirie D_J.Kirlahan DR. \laynarcl C. liush KR. Davis TM, IJlacllct KA. Posttratrmatic stress clisorclcr in female l e t e f : l n s : e s s ( ) c i : r t i ( ) nr v i t h s e l t r e p o r t e c l h e a l t h p r o blems :rntl firnctionel inrpairment. Arch Intern NIed 200,i:16.i:.19+-+00. i 0 . S a r v c h r - r kC N , R o y - I l y r n c P . C l o i c l b e r gJ , M a n s o n S . Noonan C. BealsJ et al. The rclationship between posttl'aumatic stress disordcr, cltltrcssion and carcliovascuIar discasc in an American Inclian tribe. Psychol Nlecl 2 0 0 5 ; J 5 : 1 7 t 395' + . : i l . S h e l e v A . I l l c i c h A . { I r s a n o R - 1P . o s t t r a r r m a t i cs t f e s s .iisorclcr': sornatic i'omorbiciity ancl cfkrrt tolerance. P s yc h o s o r n a t i c s19 9 0 ; 31: 1 9 7 - 2 0 3 . 42. Mr:Ferllnc AC, Atcllis()n M, Ilafakrwicz E, P:rpav P. Ph,vsiceisyllpt()rns in p()sttralll]r:rtic stress disorcler..[ P s y c i t < ; s o mR e s 1 9 9 / + : 3 t t r 7 I 2 56 . Soscarino .jA. 1)()sttrallmaticstress clisorcier ancl mortelity :rmong tl.S. Army veterans l0 years after militarv ser."'ice.Ann Epiclen'riol2006;1(r:2+tl-56. Schnr"rrrI)l). Spiro Ar'. i)aris AH. Phvsician-cliagnoseclnrcdicrl tlisorct:rs in relation to PTSI) symptolns rn olcler rnele rnilikrry vetLrrans.Heelth [)s_vcht.rl l(Xl0: I!):9l-7. lloscarino .fA. Ohang.J. Electrocardiogrem;rbnormalitics rnen qith strcss reiatecl psychiatri<:rlisorders: Jr.r.r()ng in-r1.llic:rtions firr coronarv heart clise:rseencl clirrical resealr'h. Ann tJellav l\{ccl 19!9;2I :221-a.+. Shernesh E, Ychtrda i{, Mikr O. Dinr,rr-I, Rrrclnick A, \'crccl Z et al. P()sttrarrrlr:ltic stl'css.nonaclherence..rncl aclverse ()utcolnc ir.t survivors of a rnyocarcli:rl inferction. Psvchosom X4ed 200'1;66:i21-(r. 'l'he 'Williams.lR. Stnrctr.rrecl Ciibbon NI, First N{B. Spitzel RL, (.linrcel lntervic'"r fbr DSMllIlt (SCII)). l: Historl'. ratitrrralt. :rncl descriptit>rr. Arch (]en Psychiatry 1992:+\): 6'24,9. 286 Hor<x'itz M, \l(/ilncr N. Alvarez ]W. Impact of Evcnt Scalc: a measrlre of subjectivc strcss. Psychosom Mecl 1979:1I:201)-78. Robins L, Helzer.J, Cottler L, Goldring\ u. NIMH Diagnostic Interview SchecluleVersion III tlevisecl (DIS-lll-R). St. Louis. MO: Washington University School of Meclicrne; 1989. rWeathers F, Forcl J. Psvchomctric Properties of the P'I'SD Checklist (PCL-C, PCIL-S.PCL-M, PCL-PR). In: Stamm BH, cclitor. Measurernent of stress, trallma. and adap tation. Lutherville, Ml): SiclranPress; 1996. lrittchen HLr. Relialrility and validity studies of the \XrHO: Cornposite lntern:ltional I)iagnostic Interview (CIDI): a critical rcview. J Psychiatr Res 1994;28:57-84. Keanc TM, Cadclell JM, Taylor KL. Mississippi Scale for Cornbat-Related Posttrar.rmaticStress Disorder: three stuciiesin reliability and validity..l Consult Clin Psychol 1988;56:85-90. 51. Kirnerling R. An investigation of sex cliflerences in nonpsychiatric morbiclity associate.l with posttralLmatic strcss clisorcler..f Am Mecl Wcrmens Assoc 2004:59: /+3-7. 5,i. BoscarinoJA. Posttraumaticrstress clisorder and physical illness: resr.rltsfrom clinical ancl epiclemiologic stu c l i e s .A n n N Y A c a d S c j 2 0 0 , i r 1 0 3 2 : 1 4 1 - 5 3 , 55. Veisberg RB. Brtrcc Sts, Machan JT, Kessler RC, Culpepper L. Kellcr MB. Nonpsychiatric illness among prirnary care patients rvith trauma histories and posttraumatic stressclisorcler.Psychiatr Sen 2002:53:8,18-5,i. 5 6 . D a v i c i D . W o o c l r v a r c lC . E s < l t t e n a z -i [ . M e l l t n a n T A . Comparison of comorbici physicai illnesses among vctcrans rvith PTSI) ancl veterans l'ith alcohol depeni l e n c e . P s y c h i a t rS e n ' 2 0 0 i 1 5 5 : 8 25 . t 1 . 1 . 1 t 2B T . K e a n c T V t . F i s h e r L . N ' l a r x B . N l o n a c o l V . Phvsical healtli conrplaints in <ornbat-relateclpost-traur.natic stress clisorcler: A orelin-rinary repolt. .i Traum S t r e s s1 9 9 2 ; 5I: 3 1 - +L 5tt. \l,krlfeJ, Schnurr PP. fJron'n I' .]. F-urcy.l. Posttr,run'ratic str-cssdisolclcl lncl n':Lr-zone exp()srlre as cclrrclatcs lrf pelceivccl hcaitlr in fenralc \,-ietnam \far veterrns. J 22 : 35,i0. C o n s u l t C l i n I ' s v c h o l 1 9 t ) . i : 6 .1 59. Kinrerling R. (lh.rrnGA, '.)iblfe.l. Relationships among tl-autnlrexp()slrre, chronic p()sllrtumxtic str-cssclisorcler svlnptoms. and self-reportecl health in q'omen: r e p l i c a t i o n a n d e x t e n s i o n . - JT r a u n r a S t r e s s 2 0 0 0 : 1 3 : l l i,18. /r0. Ford _ll), (irrlpbcll KA. Storzbach D. Rincler LNI. Anger WK. Rohlman DS. l)osttrar.rnraticstress symptornato krgv is asstriatrd $'1th unexplainecl illness attributeclto P e r - s i a nt i r r l f \ V a r -r n i l i t a r y s e r v i c e . P s y c h o s o m M e c l 2001:ti3:rl'129. tr1. \X/agnerAW, \Xtrlfc.J.Rotnitsky A, Proctor SP,Erickson D-J.An in!rstigation of the irnpact of posttraumatic s t r c s s d i s o r c l c r o n p h y s i c a i h e a l t h . . J T r z r u n r aS t r e s s 2000;13:41-i5. ,.'-rl.i)antzcr R. (lytokine-inclr.rcecisickness behavior: r'vhere ckr we stancl?IJlain fJehav Imrnun 2007;75:1-21. 53. Watkins l-R. iVlaier SF. imrnunc rcglrlation of ccntral ncrvolrs systenr iirnr:tions: fiom sickness responses t() p a t h o k r g i c a l p a i n . - [ I n t c r n N l e c l2 0 0 5 ; 2 5 r : 1 3 9 - 5 5 . 6'+. Hensson GK, Libby P. ['lrc inrrnrrnc responsc in atlrtrosclcrosisr a dor.rble e'clgctisworci. Nat Rev lmrntrno] 200('r:(r:50819. ir5. Slohrrhn A. Nystr'<xn l'. intlamnntion and the etiolog,v oi type 2 rliabetes. l)ialrctcs Nlctelr Res Rer- 2006;22: .ri-i 0. 56. rie Kloet CS. VcrmLrttenE, (leuzc E, Kavcluars A. Heijnen C.f. \Vestr:nbcrg FI(1. Asscssmcnt of HIA-exrs firnction in posttraumatic stress clisorder: pharrnacr:r Iogical rncl non-pliarmacological challenge tests. a revies-. -l l)svchi'rtr Rcs 2005 [Fipub ahcacl of printl \ I T \ F R \ - \ F \ T ) L X R T \ . ) T T ) (i T ( \ Diccmhre 2006 tsNDOCRINEANI) INFLA\'{MA'I'ORY ALI'ERAI'IONSIN PTSL) 67. tsrenrnerJD. Licinkr.f, I)arnell A, KrystalJH, Owens M.f, Southlvick SM et al. ElevateclCSF corticotropin-relea sing factor concentrations in posttrallmatic stress disorclcr. Arn J Psychiatry 7997 t754:621-9. 68. Baker DG, lVest SA, Nicholson \l/E. Bkhator NN. Kasckow-J\il, Hill KK et al. Serial CSF corticotropinrclc:rsing hormonc lcvcls and aclrenocortical lctivity in combat vetefans s'ith posttraumatic stress disor' der. Arn J Psychiatry 1999ri56:5U5-fJ.Erratum in: Am .J l,sychiatry 1999:1i6:986. 69. Raker lXl, Ekhator NN, Kasckor'.1\17.I)ashevsky B. Horn PS, Reclnarik L et al. Higher levcls of basal scrial CSIr cortisol in combat vctcrans with posttranmatic stress clisorcler. Am J I'sycl'riatry 2005:162:992-1. 70. N{ason.lSil.Giller EL, Kosten TR, Ostroff RLl, Podcl L. lJrinary fiee-cortisol lcvcls in posttraumatic stress disorcler patients. J Nen Mcnt l)is i98(i117:i:1.15-9. 71. Ychucla R. Boisonc:ru I), Mason JW. Giller EL. Cilucocorticoicl receptor number and cofiisol excfetion in moocl. anriety. and psychotic disorclers. Biol Psychiatry 791)3:31tt18-25. 7 2 . Y e l ' t r c l aR . K : r h a n a B , R i n d e r - R r y n e s K , S o r - r t h w i c k SM, MasonJW, Gillci EL. Lo.nvlrrinarl, cortisol cxcretion in Holocaust slrrf ivors v'ith posttraumatic stress disorder. Am J Psychiatr\' 7995:752:982-6. 7J. Yehuda ll, Southu'ick SM, Nussbaum G, \ilahby V. Giller FILJ,MasonJW. Lon'urinary cortrsol excrction rn patients \\'ith posttraumatic strcss disordcr. .f Nerv M e n t D i s 1 9 9 0 ; 1 7 8 : 3 6 69 . 7.i. Rohlcclct N,joksimovic L, Wcrlf JM, Kirschbaunr C. tlypocortisolism ancl increirse'dgh,rcocorticoiclscn>itivitl of pro Inflammatory cytokine proclrrction in Bosnian u'ar re f lrgees n-ith posttratrrnaticslrcss clisorc l e r .B i o l P s v c h i a r n ,2 0 0 a : 5 5 : 7 i 5 - 5 1 . 75. Glover I)A. Polancl RFl.L'rinan cortisol ancl catech<> lamines in mothers of chiltl cJnLtrr sur\-i\ ors Nith .rnd n i t h o u t P T S D . P s v c h o n e u r o e n c l o c r i n o l o g l2 0 0 2 ; 2 7 : 8 0 5 - t9 . 76. Thaller \'. Vrkljan M, Hotulac L, Thakore.J. The pote ntial rolc of hypocortisolism in the pathophysiokrgy of PTSD and psoriasis. Coll Antropol 7999:23677 9. 77. Pitman RK, Orr SP.Twcnty-fbur hotu-lrrinary cortisol and catecholamine excretion in combat-related posttralrmatic strcss clisorder. Biol Irsychratry 1990;2r-: 2tt5 7. 78. Lemielrx AM. Coe CL. Abuse-relatecl posttraumatic stress disordcr: cvidence fbl chronic neuroenclocrirrc activation in nomen. Psychosorn N{ccl 1995t57: 105-1i. 79. Macs M. Lin A. Bonaccorso S, van Hunsel F. Van Gastel A, Dclmcirc L ct al. Increasecl 2,i hour urinary cortisol excretion in patients with post-traumatic strcss clisorcler and patients \\,ith nraior clcprc'ssion, bllt not rn patients $'ith fibl'omyalgia. Acta Psychiatr Scancl 19 9 8 : 9 8 : 1 2 8 - 3 5 . 80. \ehucla R, Teicher MH, Trcstman ItL. Lcvcngoocl RA, Sicver LJ. Cortisol regulation in posttraumatic stress c l i s o r c l c ra n d m a j o r c l e p r e s s i o n :a c h r o n o b i o l o g i c a l analvsis. Riol I)sychiatry 1996;40:79-ulJ. 81. tlrernnc'r-fD. Vythilingarn M. Anclerson Ci. Vermetten E. \{c(il:rshan T, Heninger (} et al. Assessrlent of the l'rvpothalarnic-pituitary uclrenal axis r>r.ere 2:i hour cliurnal pet'iocl ancl in rcsponsc to ncurocnclocrine cliallenges in r''o1nen rvith and \\,ithout chilclhcxrcl sexual abuse rncl posttrallmatic stress clisordcr. Biol Psr,chiatry2003:5,1:710-8. Rctraction in: 13iolPsychiatry 2 0 0 i : 5 5 : 12 0 2 . 82. V'essa NI. Rohlecler N, Kirschbaum C. Fkrr II. Altcrccl cortisol arvakcning rcsponsc in posttlaLlmali(' stress clisorcler.Psvchoneuroencloclinology 2{i06:31:209-15. u 3 . P n r c s s n e r i C . w o t f O T . H c l l h a r r i r i - r c rL ) H , B t r s k e \bl. t1. N. + ROHI,F]DI.]R Kirschlraum A, r'on Auer K,.Job.it S et al. Free coftisol levels aftcr :rwakening: a re|able biological mart<cr fbr the assessment of adrenocrrrtical activitv. l,ife Sci 1997.67:2i39-4c). 84. Ychucla R, Golier.iA, Kaufman S. Circadian rhythm of s a l i r . a r v c o r t i s o l i n H o l o c a r , r s ts u r v i v o r s w i t h a n c l withoui PTSI). Am J Psychiatry 2005:i62:99ti-1000. 85. Young EA, Brcslau N. Saliva cortisol in posttrallmatic strcss disorder: a community epiclemiokrgic' study. I3iol Psychiatry 2004:56:2059U6. Lindauer R.l,()lff M, van Meijel EI' , Carlier IV Gersons B]'. Cortisol, learning, memory. in.l attenti()n in rela tion to smaller hippocampal rroluure in police ofli cers n'ith posttrallmatic stress clisorcler. 13iol I'sychiatry 2006:51):771-7. 87: Millcr GE. Chen E, Zhor.rE. If it goes up, must it come dor"n? Chronic stress ancl the hypothalamic pituitery aclrcnocortical axis in humans. I)sychol Rull. In press 2006 88. \'ehuda R. Sor,rthn'ick SM. Krystal ,JH, Rremner l), Charney I)S, MasonlV. Enhanceclsuppresskrn ofcortisol follon'ing clexarncthasonc administration in posttralrmatic stress disorder. Am .f Psychiatry 1993;150: 83 6. U9. Stein MB. Yehuda R. Koverola C, Hanna C. Flnhancecl dexamethasone suppression of plasma coltisol in adult lliol wornen traumatized bv chilclhoocl sexual abr,rser. Psychiatl 1997\42:680-6. 90. Newport D.l. Heirl C, I}rnsall R. Nliller AH. Nerncroff responses to stanclard :rncl low' CB. 1)rtr-ritary-aclrenal close cle'ramethas()nesuppressi()n tc-stsin aclult survivors of ctrilcl elluse. Bkrl l)s-vchiatry20()1;55:7O-20. 91. Ccracioti TI).fr-.Baker l)G. Ekhator NN. West SA. Hill KK. Bmce AR et al. CSFnorcpinephrine c()nccntrati()ns in posttraunratic stress clisorder. Am J Psychiatrv 2 0 0 1 : 15 f 3 : 1 227-30. 92. Yel'ruda R. Siever LJ, Teicher MH, Levengood fuA., Ccrber DK, Schn-reidlerJet al. Plasma norepinephri ne ancl 3 rnethoxy-4J-rydroxyphcnylglycol conccntr2rtions ancl severity of clepression in combat posttraumatic strcss disorder' :rncl major depressive disordcr. Biol Psychiatry 7998:41:56 63. 93. O'Donnell T. Hegadoren KM, Coupland NC. Noreclrenergic mcchanisms in the pathophysiology of post-traunatic stress clisorcler-.Neuropsychobiology 200.i;50:273-f13. 9.1. VeclhrrraK, Fox.fD, Vang EC. The measurcment of str-css-r'elatedimmune dysfunction in psychonetr roimmunology. Ncurosci Biobcliav Rcv 1999;23: 699-77i. 95. Krabbe KS. Peclcncn M, Brr:unsgaarclH. Inflarnmatory rnccliatom in the elderly. Erp (lerontol 20O1;39:68799. 96. Boscarino .JA, Cheng J. Higher abnormal leukocytc ancl lymphocyte collnts 20 ,vears after exposure to sLrvcrestress: research and clinical irnplications. Psychosom Mecl I999r(rl:37U ti6. 97. \Woods S.f, $ilinenran NM. Pagc GG, Hall RJ, Alexancler TS, Campbell JC. Prcclicting immunc status in r''omcn frc.rmPTSD ancl childhcxrci ancl aclult vurlen<:e.ANS Aclv Nttrs Sci 2005;2ll:306-19. 98. l'onson C;. Vynings C, Schncidcrman N, Baurn A. RoclriguezM. Grccnw-ooclD ct al. t'osttrarrmaticstrcss symptolns, intrusive thougl'rts.loss, ancl in-rmunefunc tion afte r I Itrrric ane Anclren'. Psychosorn 1\4ecl 1 9 9 7 r 5 9 :2 1 8 - ' l1i . 99. Kalvamr.u'aN. Krm Y, Asukai N. Suppression of cellu l:Lr imrnunity in r.nen n,ith a past I'ristory of posttraulnatic stressclisolder'.Arn .f Ps.vchiatry2001l 158:.i84-6. 100. I)ekaris l), Sabionccllo A. Mazuran ll, l{alratic S. S l o b o c l a B e u s a n I . R n c u n i c aN L e t a l . M u l t i p l c c h a n ges of imnrunologic pararneters in prisoners of u,'ar. NIINER\A ENI)OCRINOI,O(}I(]A 281 ALTERATIO\5I\ PT\I) tsNDOCRINIA\D INFLA\4l\,IATORY ROHLEDER Assessrnents after release from a camp in Manjaca, Bosnra. JAMA 1993:270:5959. 101. Wilson SN, van der Kolk B, Burbridge J, Fisler R, Kradin R. Phenorype of blood lymphocytes in PTSD suggests chronic immune activation. Psychosomatics 7L)99:40:222-5. 102. Mosnaim AD, Wolf ME, Maturana P, Mosnaim G, Pllente J, Kucuk O et al. In vitro studies of natural killer cell activity in post traumatic stress disorder patients. Response to methionine-enkephalin challenge. Immunopharmacokrgy 1993;25:7O7-76. 103. Inoue-Sakurai C, Maruyama S, Morimoto K. Posttraumatic stress and lifestyles are associated with natural killer cell activity in victims of the HanshinAwaji earthquake inJapan. Prev Med 2000t37i61-73. 104. Laudenslager ML, Aasal R, Adler L, Berger CL, Montgomery PT, Sandberg E et al. Elevated cytotoxicity in combat veterans with long-term post-tralrmatic stress disorder: preliminary obseruations. Brain Behav Immun 1998;12:74-9. 105. I)elahanty DL, Dougall AL, Craig KJ,.lenkins FJ, Baum A. Chronic stress and natural killer cell activity after exposllre to trallmatic death, Psychosom Med 199-:i9:16---6. 106. Vatson IP, Muller HK, Jones IH, Bradley AJ. Cellmediated immunity in combat veterans with posttraumatic stress disorder. MedJ Aust 1993;159:513-6. 107, Altemus M, Cloitre M, Dhabhar FS. Enhanced cellular immune resDonse in women with I'TSD related to childhood a6use. AmJ Psychiatry 2003;160:170i 7. 108. Miller R.J,Sutherland AG, Hutchison.jD, Alcxander DA. C-reactive protein and interleukin 6 receptor in post-traumatic stress disorder: a pikrt study. Cytokine 2001t73:253-5. 109. Sondergaard HP, Hansson LO, Theorell T. The inflammatory markers C-reactive protein and serum amyloid A in refugees with and without p()sttraumatic stress disorder. Clin Chim Acta 2004:342:938. 110. Tr-rcker P, Ruwe \WD, Masters B, Parker DE, Hossain A, Trautman RP et al. Neuroimmune and coftisol changes in selective serotonin reuptake inhibitor and pla ccbo treatment of chronic posttrallmatic stress clisorder. Biol Psychiatry 20O4:56:7278. 111. Spivak B, Shohat B, Mester R, Avraham S, Gil-Ad I, Bleich A et al. Elevated levels of serun interleukin 1 beta in combat-related posttraumatic stress disorder. Biol Psvchiatrv 191)7;12:315-8. 288 112. Maes M, Lin AH, Delmeire L, Van Gastel A, Kenis G, De.]ongh R et al. Elevated serum interleukin-6 (IL-6) and IL-6 receptor concentrations in posttraumatic stress disorder following accidental man-made tratlmatic events. Biol Psychiatry 1999;45:833-9. 113. Baker DG, Ekhator NN, Kasckow J\(, Hill KK, Zoumakis E, Dashevsky tsA et al. Plasma and cerebrospinal fluid interleukin-6 concentrations in posttraLlmatic stress disorder. Neuroimmunomodulati<;n 2001:9:209-77. 11,1.Voods AB, Page GG, O'Campo P, Pugh LC, Forcl D, Campbell JC. The mediation effect of posttraum2rtic stress disorder symptoms on the relationship of intimate partner violence and IFN-gamma levels. Am J Community Psychol 2005:36:759-7 5. 115. Aurer A, Aurer-KozeljJ, Stavljenic-Rukavina A, Kalenic S, Ivic-Kardum M, Haban V. Inflammatory mediators in saliva of patients with rapidly progressive periodontitis clurins war stress induced incidence increase. Coll Antropol 7999:23:717-24. 116. Segman RH, Shefi N, Goltser-Dubner T, Friedman N, Kaminski N, Shalev AY. Peripheral blood mononuclear cell gene expression profiles identify emergent post-traLlmatic stress disorder among traLlma survivors. Mol Psychiatry 2005;i0:500-13, 425. Erratr-rmin: Mol Psychiatry 2005:10:514. 117. Rohleder N, Schommer NC, Hellhammer DH, Engel R, Kirschbai-rmC. Sex differences in glucctcorticoid sensitivity of proinflammatory cytokine prodtrctitrn after 72. psychosocial stress. Psyr'hosom Med 2OO1:63:966 118. Bierhaus A, \ilolf .1,Andrassy M, Rohleder N, Humpcrt PM, Petrov D et al. A mechanism converting psychosocial stress into mononuclear cell activation. Proc Natl Acad Sci U S A 20031100:1920-5. 119. Vlahov D, Galea S, Resnick H, AhernJ, BoscarinoJA, Bucuvalas M et al. Increased use of cigarettes, alcohol, and marijuana among Manhattan, New York, resiclents after the September 11th terrorist attacks. AmJ Epiclemiol 2002;155:988 96. I20. I4az.z.anoLA, He J. Mlrntner P, Virpputuri S, Whelton PK. Relationship between cigarcttc stttoking ancl novel risk f:rctors for cardiol'ascular cli.t.tst in the United S t a t e s .A n n I n t e r n M e d 2 0 0 3 ; 1 3 8 : f l (l -) 7 . 121. SfannametheeSG, Lowe GD, Vl-rinctrp PH, Rumley A, 'Walker M, Lennon L. Physical activity and hemostatic and inflammatory variables in elderly men. Circulation 2002:105:7785-90. 1\ItNERVAEN DOCRINOIOCT(,A Dicembre 2006











© Copyright 2026