
The Human Consequences of the Chernobyl Nuclear Accident A Strategy for Recovery
Final – 25.01.02 The Human Consequences of the Chernobyl Nuclear Accident A Strategy for Recovery A Report Commissioned by UNDP and UNICEF with the support of UN-OCHA and WHO 25 January 2002 Final: 25.01.02 Preface 0.01 This Report contains the findings of a study commissioned by agencies of the United Nations to obtain up-to-date and credible information on the current conditions in which people affected by the Chernobyl accident are living fifteen years after the explosion, and to make recommendations as to how their needs can best be addressed in the light of this information. 0.02 The Report is addressed in the first instance to the UN and its funds, programmes and specialised agencies and to the international donor community. The need to tackle the consequences of the Chernobyl nuclear accident has spurred the development of wide-ranging international co-operation in science, humanitarian assistance and technology. The primary role has, rightly, always been taken by the Governments of the countries directly concerned, initially the Soviet Union and, after 1991, Belarus, Russia and Ukraine. These countries have made an enormous commitment in addressing the consequences of the accident, the scale of which has never been fully appreciated by the outside world. The Report is also addressed to the three concerned Governments for their consideration in potential policies and actions related to the Chernobyl issue. A central role has been played by the voluntary movement and by scientists, health workers and other specialists. The Report addresses these interests too. 0.03 The study was conducted by a multidisciplinary international team in July and August 2001 on behalf of UNDP and UNICEF, with the support of the UN Office for the Coordination of Humanitarian Affairs (OCHA) and WHO. The assessment in the Report is based on rigorous analysis of evidence drawn from a wide range of interviews and observations conducted in the affected areas. It draws on discussions with senior officials in the three capitals and in the regions; on research papers commissioned from leading national experts; on a review of current reports, including the National Chernobyl Programmes of Belarus, the Russian Federation and Ukraine; and on scientific papers, legal documents and other publications. The Mission spent thirty-one days in the field, with approximately ten days in each country. 0.04 The Mission Team consisted of six specialists from three disciplines: ecology, health and economics. Three members of the team were recruited internationally, while the other three were national experts, recruited one from each of the three countries directly concerned (Annex 2). The Mission was supervised by a multiagency Steering Committee which included the UNDP Resident Representatives for the three countries, the UNICEF Representative for the Russian Federation, Ukraine and Belarus, and representatives of UN-OCHA and WHO. The Mission is confident that it was able to carry out its enquiries in all three countries in an independent manner and without undue influence. It thanks all of the many individuals who assisted it in its work. The Mission commends the Report and the recommendations that it contains to the international community, to the three governments, and to the other parties concerned. ii Final: 25.01.02 Table of Contents Page Preface ii Contents iii Part I: Executive Report Section 1: Summary of findings Recommendations Project concepts 1 15 22 Part II: Mission Findings Section 2: Background: the accident and the events that followed Section 3: Environmental consequences Section 4: Health Section 5: Economic development and household incomes 27 35 47 63 Annexes References The Mission Team 74 75 iii Final – 25.01.02 Part I: Executive Report Introduction 1.01 This Report contains the findings of a study conducted into the human consequences of the Chernobyl nuclear accident fifteen years after the explosion. The Mission explored the health, socio-economic and environmental effects of the accident and the events that followed. The Report contains an analysis of the current situation and the prospects for the future, focusing on aspects that are significant for the well-being of the people and communities directly affected. 1.02 The affected population - those exposed to radioactive fallout, remaining in the affected areas, or forced to relocate - continue to face disproportionate suffering in terms of health, social conditions, and economic opportunity. Hundreds of thousands of people have been evacuated from the most severely affected areas (see Section 2). Many have found it difficult to adapt and continue to face serious psychological, economic and social problems. The process of evacuation has now virtually ceased and only a small number of people continue to live in the most polluted areas. However, some tens of thousands remain in areas polluted to a level of between 15 and 40 curies per square kilometre. 1.03 The accident has also had a continuing impact on the opportunities and well-being of a much wider circle of the inhabitants of Belarus, Ukraine and Russia, through the negative image that it has created for large areas of these countries. It has imposed a heavy burden on the national budgets through the cost of clean-up, compensation and recovery. Ukraine, in addition, has had to carry much of the cost of closing and making safe the Chernobyl complex as well as the opportunity cost of the lost electrical output from the reactors concerned. These commitments have diverted resources away from other priorities, such as health, education and investment, at a time of profound economic crisis. 1.04 Fifteen years after the accident, and with the governments of the three most directly affected countries actively engaged, the question may reasonably be asked, why should the international community continue to fund measures to address the complicated cluster of human problems that were triggered by the explosion of 26 April 1986? Three strong reasons can be given in answer to this question. The first reason is that the rest of the world has an important practical interest in remaining involved with the issue of Chernobyl. This interest not only concerns the safety of the complex itself but also the knowledge that can be gained about the long-term effects of the radioactive fallout on health and about the difficult issues of disaster management involved in the post-accident response. 1.05 This consideration is not simply theoretical. Today there are over 400 nuclear reactors in operation around the world. Based on the experience of more than 10,000 years of operation, experts consider that the probability of a major 1 Final: 25.01.02 accident with significant contamination outside plant boundaries is very small. Future designs will doubtless be safer, but as for all technologies, even the best designs can never assure absolute safety from accident or attack. 1.06 But scientific interest in the lessons of Chernobyl cannot be satisfied in isolation from the question of the well-being of those whose lives have been altered for the worse by Chernobyl. In the spirit of the Helsinki Declaration on Biomedical Research on Human Subjects, the international community must accept a share in the responsibility for the well-being of those concerned if it is to expect to be able to learn from their predicament. Moreover, if active steps are not taken to resolve the human problems relating to the accident, the fate of the communities blighted by Chernobyl will continue to haunt discussions on energy generation for decades to come. In the context of global warming, governments around the world and the international energy industry share an interest in resolving these problems and promoting a debate on the future of nuclear power based not on emotion but on arguments and facts. 1.07 The second reason is that the international community has been intimately involved in the evolution of the issue of Chernobyl and its consequences. With the national authorities and the scientific community, it has helped to shape the experiences of many whose lives have been touched by the accident. It must not simply turn its back with the job half done. The moral case is obvious. The wellbeing of very large numbers of human beings, including children, is involved. Their prospects have been profoundly influenced by decisions over which they have had no say. These decisions have involved governments, but also, to a greater or lesser extent, the outside world. 1.08 The third reason why the international community must continue to cooperate in resolving the human problems linked to Chernobyl is more positive. It lies in the potential that such cooperation has to serve as a model for the future. In all the disruption and distress, the issue has become the focus for a unique experiment in international collaboration involving not just governments and international organisations, but doctors and scientists and ordinary people engaged in partnership activities designed to meet the needs of children and adults affected by Chernobyl. Many of the initiatives that are being developed have potential applications in other parts of the world where rural communities have been subjected to destructive shocks, whether technological in origin or resulting from war, civil disturbance, or economic change. 1.09 The Report argues that the environmental effects of Chernobyl cannot be considered in isolation from their socio-economic and health aspects or from the changing institutional context of the three countries concerned. It explores the links between environmental contamination, health risks and economic constraints. The Report finds that, while physical processes are gradually reducing the level of radioactive contamination in the environment, the most vulnerable groups of people in the affected areas are facing a complex and 2 Final: 25.01.02 progressive downward spiral of living conditions induced by the consequences of the accident and the events that followed. 1.10 1.11 The Report outlines a ten year strategy for tackling and reversing this downward spiral. It makes a series of recommendations designed to address the human needs resulting directly or indirectly from the accident. These aim to promote long-term recovery through a new consensus between the main parties involved, new partnerships and a new generation of initiatives designed to assist the individuals and the communities concerned to take their future in their own hands. On the basis of the assessment undertaken, the Mission identified the following five key principles which underlie the approach it recommends to tackling the consequences of the accident: * Chernobyl related needs should be addressed in the framework of a holistic view of the needs of the individuals and communities concerned and, increasingly, of the needs of society as a whole; * the aim must be to help individuals to take control of their own lives and communities to take control of their own futures; * efficient use of resources means focusing on the most affected people and communities, and on children. The response must be commensurate to the scale of the needs; * the new approach should seek changes that are sustainable and long-term, and based on a developmental approach; * the international effort can only be effective if it supports, amplifies and acts as a lever for change in the far larger efforts made by local and national government agencies and the voluntary sector in the three countries. Based on these principles and the results of the assessment, the Report proposes a new medium term strategy as a framework for relaunching the international community’s commitment to help address the human needs resulting from the accident. A small but important minority, those caught in the downward spiral, need substantial material assistance to rebuild their lives. This population probably numbers between one and two hundred thousand individuals. It includes those who continue to live in severely contaminated areas and who are unable to support themselves adequately, unemployed resettlers and those whose health is most directly threatened, including the victims of thyroid cancer. These people are right at the core of the cluster of problems created by Chernobyl. Resources should be focused on resolving their needs and on helping them to take control of their destinies in the circumstances that have resulted from the accident. 3 Final: 25.01.02 1.12 A second group consists of those whose lives have been directly and significantly affected by the consequences of the accident but who are already in a position to support themselves. This group, numbering some hundreds of thousands of individuals, includes resettlers who have found employment and many of the former clean up workers. The priority here should be to help these people to normalise their lives as quickly and as far as is possible. Over a period of time, they need to be reintegrated into society as a whole, so that their needs are increasingly addressed through mainstream provision and according to the same criteria as apply to other sections of society. 1.13 A third group consists of a much larger number of people, totalling several million in the three countries, whose lives have been influenced by the accident primarily in that they have been labelled as, or perceive themselves as, actual or potential victims of Chernobyl. Here the main need is for full, truthful and accurate information on the effects of the accident based on dependable and internationally recognised research, coupled with access to good quality mainstream provision in health care and social services; and to employment. 1.14 The approach of defining the most serious problems and addressing them with special measures, while pursuing an overall policy of promoting a return to normality, should apply to the affected territories as well as to the affected individuals and communities. Where in the light of the best scientific knowledge it is reasonably possible, measures should be adopted to integrate less severely affected areas back into productive use as soon as is practicable. This combination of measures – focusing resources on those most in need, while actively promoting integration with mainstream provision wherever possible – is not a second best. Within the available budgets it is really the only alternative to the progressive breakdown of the recovery effort, continuing haemorrhaging of scarce resources and continuing distress for the people at the centre of the problem. By fostering a process of healing, these measures will help to address the widespread psychosocial effects of the accident. They will protect the most vulnerable as the Chernobyl spend inevitably declines and will enable the authorities to promote an orderly process of recovery over the coming years. 1.15 This new strategy marks a clear break from the policies of the past fifteen years; it challenges widely held assumptions in the countries concerned and in the international community. Strong barriers to change exist in the fears and the patterns of behaviour of the affected population and the wider community, and powerful vested interests are involved. At first sight, there may seem little chance of building the consensus needed to make a success of the new approach. In practice, however, it was clear to the Mission that many of those most involved in addressing the consequences of the accident are aware that in future it will not be possible simply to carry on as before. A log-jam has developed of expectations and assumptions that no longer reflect the current realities. Breaking this log-jam is the key to resolving the continuing problems that have followed from the Chernobyl accident. 4 Final: 25.01.02 Towards a Sustainable Environment 1.16 The radioactive fallout from the Chernobyl accident contaminated large territories in all three countries affecting life in rural communities for decades to come (see Section 3). Agriculture and forestry are forbidden in wide areas. Poverty forces many people to eat contaminated berries, mushrooms, game and fish, to feed contaminated hay to their cattle and to burn radioactively contaminated firewood in their stoves. Many of those living in the affected areas are ignorant of the risks that they face, or have adopted an apathetic and fatalistic attitude. 1.17 Radioactive contamination resulting from the Chernobyl explosion and fire poses health risks to the rural population and constrains economic development. Serious concerns primarily relate to the so-called “highly contaminated territories” where contamination is between 15 and 40 curies per square kilometre. At present between 150 and 200 thousand people permanently reside in these areas. 1.18 Substantial doses of radiation were received by the general public and clean-up workers in the period immediately following the accident. The associated risks involved have already been incurred and cannot be influenced by environmental management measures. The main problem today relates to internal irradiation resulting from the consumption of contaminated foodstuffs, notably milk, meat and forest products such as game, berries and mushrooms. This threat can be controlled to a significant extent by the use of special fertilisers and fodder supplements and by changes in diet. However, those most at risk are the least able to protect themselves. The overall level of contamination is falling gradually as a result of natural radioactive decay. Certain high-risk groups, however, face stable, or even increased, exposure as a result of the decline in the use of protective soil treatments and changes in the structure of agriculture following the break up of the Soviet Union. Framework for action 1.19 The logic of these findings is that resources should be concentrated on those most at risk – country people who grow and gather their own food – and on efforts to revive the economies of the affected areas in ways which are compatible with the continuing radiation hazard (Project 5). Environmental policy development, planning, implementation and management needs to be improved at the national and local levels. This should include building on the lessons of the post-Chernobyl response in terms of disaster management and strengthening capacity to cope with a range of environmental hazards (Project 6). The concept of strategic environmental planning and transboundary co-operation should be promoted in the affected regions, with the participation of the communities concerned (Project 4). This should involve increased training for regional planning and environmental specialists and should reflect the reality that the impact of Chernobyl transcends the frontiers of the affected countries. 5 Final: 25.01.02 1.20 Innovative ways need to be developed to increase knowledge about how to live safely in environments which have suffered radioactive contamination. Important pilot studies have been carried out, often with international assistance. The lessons of these projects need now to be disseminated much more widely. Efforts should be made to strengthen the local capacity for sustainable development by establishing a small grant facility for voluntary organisations and local government interested in promoting sustainable development initiatives (Project 6). Continued efforts are also needed to develop and promote agricultural products that can be produced safely where radionuclides are present in the soil. 1.21 Continuing internationally accredited research is needed into the effects of radioactive contamination on the environment and on strategies for addressing problems such as the dispersal of radionuclides in water and into the atmosphere and the implications that this has for groups, such as forestry workers and hunters and their families, who are at risk because of their particular patterns of life. Efforts should be made to encourage the international scientific community to make fuller use of the unique natural laboratory constituted by the exclusion zone surrounding the Chernobyl Power Plant, in conjunction with the existing management and research centres which are responsible for monitoring and managing the zone (Project 7). 1.22 One way these research needs could be met would be through the creation of an International Chernobyl Foundation (ICF) charged with promoting high quality research on the environmental and health effects of the accident (Project 3). Consideration should be given to using the existing mechanism of the UN Chernobyl Trust Fund. The Foundation would act as a channel for long-term funding for research into the effects of the Chernobyl accident and into the best means to ensure the well being of the affected communities. It would need to be administered by an independent multinational body and would draw its resources from a variety of sources including parties standing to gain from knowledge generated by impartial research into the effects of the accident. 1.23 Consideration should be given to creating an International Chernobyl Research Board (ICRB) under the umbrella of the ICF. To keep administrative costs to a minimum, the Board could be established in the framework of an existing international institution such as the UN University. The Board would be made up of a panel of independent experts in health and environmental science. On presentation of a proposal relating directly or indirectly to the effects of the accident, the Board would convene an expert panel to investigate and report publicly on the issue. It would make recommendations as to priorities for research either generally or to the ICF, which would be empowered to support appropriate projects. A further role for ICRB would be to make available authoritative information on the effects of radiation on health and the environment directly to the public. 6 Final: 25.01.02 1.24 Efforts are needed to identify sustainable ways to make use of the most affected areas that reflect the radiation hazard, but also maximise the economic potential for the benefit of the community. Consideration should be given to organising a series of local reviews in each of the most severely affected districts. These would bring together members of the local community, local government representatives and national and international specialists to map out options for the future development of the areas concerned as radioactive contamination progressively declines. This would enable local people to contribute to forward planning for the affected areas. It would help to highlight the continuing dangers in a realistic way, while at the same time establishing a positive, constructive and forward looking attitude towards the areas concerned among those most directly affected. 1.25 The international community should explore with the governments concerned the possibilities for promoting specialised ecological tourism and for maximising the contribution that these areas can make to the preservation of international biodiversity. Little attempt had been made to exploit the reduction of human disturbance to the ecosystems and cultural landscape in a positive way and the current national plans for biodiversity protection and cultural preservation hardly refer to this potential. The territories could be used to fulfill the three countries' international obligations on the protection of biodiversity (Project 7). Health in the affected communities 1.26 Morbidity in the affected areas continues to reflect the pattern in other parts of the Former Soviet Union. Life expectancy, particularly of males, is substantially lower than in Western and Southern Europe, with heart disease and trauma the leading causes of death (see Section 4). Low household incomes, demoralisation, poor diet and high levels of alcohol and tobacco consumption are key factors. 1.27 Very considerable uncertainty remains over the possible long-term health effects of the accident. On the one hand, the nuclear industry acknowledges only very limited and closely defined consequences. On the other, some politicians, researchers and voluntary movement workers claim that the accident has had profound and diverse impacts on the health of many millions of people. This uncertainty is a cause of widespread distress and misallocation of resources and needs to be addressed though rigorous and adequately funded international efforts. 1.28 No reliable evidence has emerged of an increase in leukemias, which had been predicted to result from the accident. However, some two thousand cases of thyroid cancer have so far been diagnosed among young people exposed to radioactive iodine in April and May 1986. According to conservative estimates, this figure is likely to rise to 8-10,000 over the coming years. While thyroid cancer can be treated, all of these people will need continuing medical attention 7 Final: 25.01.02 for the rest of their lives. A significant number have potentially serious complications. It is likely that the coming decades will see an increase in other solid cancers resulting from exposure to radiation. However, there is no consensus over how many cases will occur. 1.29 As well as the direct effects of radiation on health, the accident led to enormous disruption to the lives of those who were evacuated from their homes and resettled. Many of these people have found it very difficult to adapt to their new circumstances and continue to suffer high levels of stress, in particular linked to unemployment and a feeling that they do not have adequate control over their lives. A significant proportion of, in particular older, re-settlers still express a desire to return to their old homes. Those who continue to live in contaminated areas appear to suffer lower levels of stress, but they too face high levels of unemployment and many of them face the problem of bringing children up in a polluted environment. Research suggests that recent years have seen a major change in attitudes among those remaining in the affected areas, with far fewer now wishing to leave. Framework for action 1.30 Efforts to address the health effects of the Chernobyl accident need to be undertaken in the context of a wider reform of health care provision in the three countries. Such reform should be based on a rigorous examination of the cost effectiveness of current practices and a determined effort to improve primary care and ensure that resources are allocated on the basis of medical need. Strong measures are needed to improve the level of care available to poor people living in rural areas. Particular attention needs to be paid to addressing the effects of social and environmental factors on health, including poverty, poor diet, alcoholism, tobacco abuse and poor living conditions including inadequate basic services such as sanitation and access to clean drinking water (Project 9). 1.31 Continuation of the present policies by the three affected States, the international community and charitable organisations will only serve to prolong the dependency culture that has developed over the past 15 years, and the associated negative aspects of health and well-being. If the health interests of the affected populations are to be addressed, the present emphasis on humanitarian aid, delivered to passive populations, has to be replaced, gradually, by assistance in developing economically and socially sustainable communities. Such efforts must involve tackling the constraints imposed by radioactive contamination in a positive and innovative way. 1.32 This is not in anyway to minimise the seriousness of the situation for health and well-being or the role played by the exposure to ionising radiation. However, the clear priority for health, both physical and psychological, is to improve basic primary health care, diet and living conditions, while at the same time helping those concerned to come to terms with living in a radioactively contaminated 8 Final: 25.01.02 environment. This, and improvement in the economic status of the population, is the key to reversing the downward spiral in health and well-being. 1.33 The health problems linked to the Chernobyl accident reflect complex interactions between health, ecology, economics and community development. The effects of radiation cannot be ring-fenced and treated in isolation from other aspects of the lives of the individuals concerned (Project 9). Priority should be given to those measures which can be most effective in extending healthy life and improving well-being. In practice this means that a strong emphasis should be put on efforts to improve household incomes, to strengthen primary health care and to rebuild the structures of society at the community level. These objectives can best be achieved through active collaboration between the communities concerned, government agencies, local and national, the international community and the voluntary sector (Project 8). 1.34 As far as the psychosocial dimension of health is concerned, two things are urgently needed. First, it is vital that those affected, and the population at large, be given clear advice on what, on the basis of the best evidence, are believed to be the real risks associated with the kinds of exposure to radiation that resulted from the Chernobyl accident. It is essential that this advice is honest and that areas of doubt are fully acknowledged. Where appropriate, political leaders should be encouraged to add their weight to the effort to encourage a more realistic and balanced attitude to the question of radiation and health in the affected countries. The second thing that is needed is a mechanism to provide authoritative opinions on these issues and ensure that properly designed and impartial research is carried out. 1.35 The history of the Chernobyl issue since the accident indicates the importance of continuing high-level research; both to meet the needs of the affected populations and also to address questions of importance for humanity. Major health and environmental issues remain unresolved and, if the evidence is not to be lost forever, it is essential that they be investigated according to internationally recognised protocols and in a timely manner. Concern for the effects on health of ionising radiation delivered in low doses and at low dose rates has grown over the past 15 years. These concerns reflect the fact that there is no direct basis for determining risks associated with exposures of the kind resulting from the Chernobyl accident. Further research needs to be undertaken on this issue to supplement work already undertaken by the International Radiation Protection Association and other bodies. 1.36 Over the past decade, progress in radiobiology and radiation epidemiology has been considerable. This research presents important challenges to existing concepts upon which risk estimation is based. In addition, little serious consideration has been given by the research community to ameliorating the psychosocial effects of accidents such as Chernobyl. The argument for a more systematic approach to Chernobyl related research is forcefully illustrated by the 9 Final: 25.01.02 unexpected appearance of early childhood thyroid cancer, the unexpected absence of leukaemia stemming from the accident, and the persistence of the psychosocial effect, all of which to some degree contradicted the accepted wisdom. 1.37 Specific health issues which need to be explored as a matter of priority include the question of a possible link between breast cancer in younger women and women who were lactating at the time of the accident, and radiation. Studies in Japan indicate that such a relationship is possible. It is particularly important to resolve this issue because early diagnosis through appropriate screening can be effective in reducing mortality from breast cancer (Project 12). 1.38 The question of thyroid cancer in those who were infants or children at the time of the accident and who lived in areas outside of the areas designated as contaminated by caesium and strontium should be investigated as a matter of priority. Claims have been made in Russia that meteorological conditions may have led to fallout of radioactive iodine affecting a wider area through so-called dry deposition. If that were the case, then the scope of the current monitoring effort would need to be extended. Other issues that should be followed up include the physical and psychological health of clean-up workers; an evaluation of the distribution of caesium in various body tissues and assessment of risk of tissue specific damage; a study of thyroid cancer in those who were adults at the time of the accident; the development of a strategy for screening that is cost effective; and an evaluation of the need for treatment and follow-up of young thyroid patients. A high priority should be given to tackling the problem of iodine deficiency through properly researched and designed iodine supplementation programmes, and, protection against iodine deficiency for the population at large through the universal iodisation of salt. 1.39 As far as the psychosocial dimension of health is concerned it is essential that the affected population and the population at large be given clear advice on what are believed to be the real risks associated with the kinds of exposure that resulted from the Chernobyl accident (Project 13). A mechanism, such as the proposed International Chernobyl Foundation, is needed to provide authoritative opinions on these issues and ensure that properly designed and impartial research is carried out where needed. Determined efforts need to be made at national and local level to promote a balanced understanding of the health effects of radiation among the public, many of whom at present suffer distress as a result of ill-founded fears. Economic development and household incomes 1.40 The Chernobyl accident has had profound effects, immediate and long-term, on the economy of the surrounding areas (see Section 5). The disruption caused by the radioactive contamination, the plant and farm closures and the resettlement of many of the inhabitants was amplified after 1991 by the effects of the break up of 10 Final: 25.01.02 the Soviet Union. The accident has also imposed a heavy burden on the national budgets through the cost of clean-up, compensation and recovery. A total of some seven million people are in receipt of Chernobyl-related welfare benefits of one kind or another. Many of these are of little financial value to the individuals concerned, but in total make up a very substantial burden on the exchequers of the three countries. The direct and indirect effects of the disaster on the affected population are enormously amplified by poverty and lack of opportunities for household income generation. Effective measures to promote economic and social recovery and to give the individuals and communities greater control over their own destinies must play a central role in any future response. 1.41 Poverty and unemployment blight the lives of people still living in the contaminated areas and of those who have been evacuated. While meaningful figures are not available for the level of employment specifically for the affected areas, unemployment and under-employment clearly constitute a major problem. The migration of skilled young people from the affected areas has hindered industrial recovery and deterred investment. In rural communities, where food production and food processing are the staple sources of income, radioactive contamination has severely reduced the opportunities for household income generation. Investment in the affected areas is constrained by mistaken perceptions of the nature and extent of the threat posed by the effects of the accident. Framework for action 1.42 The most important factor determining economic conditions in the affected communities is the overall performance of the national economies of the countries concerned. While all three countries have seen significant growth over the last year, they continue to lag behind not only the main industrial market economies, but also neighbouring transition countries such as Hungary, Poland and the Baltic States. Sound finances and the creation of an open competitive market economy and an investment-friendly business environment are preconditions for sustained recovery in the affected areas. Experience in the former Soviet Union and in other parts of the world, however, indicates that growth at the national level does not automatically solve the problem of severe local economic disadvantage. 1.43 The areas and communities blighted by the Chernobyl accident need massive investment if they are to break out of poverty and dependency. Appropriate national policies, therefore, need to be supplemented by a proactive approach to stimulating economic development at the local level (see Section 4, Box 4.2). Efforts should be made to build upon experience of the local economic development agencies already functioning in the Gomel Region (Belarus) and Slavutich (Ukraine) to build a network of intermediary organisations which are sensitive to local conditions and can act as an interface with national and international development bodies and donors (Project 14). 11 Final: 25.01.02 1.44 At the regional level, measures are needed to help integrate locally-based businesses into the world market (Project 18) and to promote inward investment, both national and international. The latter will involve a major change in approach by authorities and communities, which have become used to emphasising the problems and the special needs of their areas to the outside world rather than the opportunities they offer. Experience in other parts of the world shows that a concerted effort to attract inward investment can succeed even in very unfavourable conditions. Special institutions should be established to lead this drive as has been done in other parts of Europe, including in the CIS (Project 15). This effort will also help to break down the prejudices associated with the affected areas as far as food and other sensitive products are concerned. 1.45 Industrial companies can play an important role in the process of recovery by creating new opportunities for job seekers from rural communities. By processing agricultural produce bought from affected areas, they generate income for agricultural enterprises and rural families. Consideration should also be given to supporting good quality, locally appropriate, training (Project 20) and providing tax incentives or grants to businesses setting up in the less contaminated areas of the most severely affected districts as a complement to the existing special zones. 1.46 While promoting inward investment is an efficient way of creating employment and benefits the whole community, it will not be sufficient to solve the most serious social problems caused by the Chernobyl accident. It needs to be complemented by efforts to promote the development of indigenous businesses and by encouraging self-employment in rural communities to enable households to become self-sufficient. Active measures are needed to encourage the establishment and growth of small and medium sized enterprises in the affected areas and in the adjacent towns and cities using the whole range of business support techniques which have been tried and tested in other parts of the world. 1.47 In the meanwhile, the present Chernobyl budgets play a key role in supporting living standards and demand in the affected communities. It is important that this spend be maintained in the short run. However, it is equally important that it be redirected as quickly as possible towards measures to promote self-sufficiency, including training and support for income generating activity. This is important for the psychological welfare of the individuals concerned, and it is also the only way to secure their economic well-being on a sustainable basis (Project 16). 1.48 At the local level, a major drive is needed to support the trend towards household self-sufficiency. Country people in the affected areas already have many of the skills needed to support themselves. The lives of those who are left out of this process can only continue to deteriorate. Local self-help initiatives to address the need for small-scale finance and help with access to markets are needed (Project 19). Helping to establish such structures should be a priority for international assistance. Promising pilot projects have been carried out in these areas in recent years. These now need to be scaled up to a point where they can begin to have a 12 Final: 25.01.02 meaningful impact. The Mission found that the inhabitants of the affected districts were very interested in the idea of developing new locally appropriate forms of small-scale enterprise. This interest should be harnessed through developing local recovery strategies for the most severely affected districts. 1.49 Initiatives to tackle rural poverty and unemployment need to be appropriate to local conditions, which include an almost complete absence of experience of entrepreneurship and a very strong tradition of collectivism. They should concentrate on encouraging local clusters of particular types of small scale business so that the families involved can learn from each other and share some of the costs, for example in fields such as marketing, purchasing and transport (Project 17). Efforts should be made to explore the possibilities for encouraging other forms of business organisation which reflect the experience of country people. One possible format for this is credit unions, which are already being encouraged in some areas with support from UNDP and other donors (Project 19). The possible role of small scale worker and consumer cooperatives in contributing to economic development in the affected areas should also be explored. 1.50 To support this process, it is crucial that economic development skills and resources are mobilised at the regional and local levels. The local economic development agencies already functioning in the area provide an example of how this can be done. International Voluntary Partnerships (IVPs) such as community and town twinnings can play a useful part in the development of grass roots initiatives (Section 4, Box 4.5). As they have much lower costs than conventional technical assistance projects and are not tied to short-term budget cycles they can address the issue of sustainability in a meaningful way. The international community should help to multiply the benefits of IVP activity through small grants, and initiatives to encourage training and networking (Project 2). 1.51 Re-integrating areas formerly condemned as a result of pollution needs to be examined in the context of economic development. Progressively, natural processes are reducing the extent of territory that is blighted. The issue of how to deal with territories as restrictions are lifted requires careful consideration. In strictly economic terms, the merits of reversing these measures in the near future may be questioned. Proposals for developing timber resources on contaminated territories were submitted to the Mission, however, the opinion of forestry experts was that from a commercial point of view, resources would be better spent on timber extraction in cleaner areas. 1.52 On the other hand, bringing condemned land back into economic use would be a powerful marker of the process of recovery for potential investors and in terms of the psychology of the communities concerned. The issue needs to be carefully considered by these communities, working with appropriate specialists and local and national government agencies. Wherever possible, the assumption should be that local people should have the choice of where to live and work, provided the interests of vulnerable individuals, including children, can be properly protected. 13 Final: 25.01.02 1.53 Alongside measures to support employment generation at the village level, vigorous efforts are needed to promote the rebuilding of community structures to replace those which were lost in the process of evacuation and as a result of the break up of the Soviet Union. In the Soviet period small towns and rural communities were served by a range of institutions and organisations, including collective farms, local “houses of culture” and various Communist Party inspired social organisations such as the young pioneers. In general, these institutions have disappeared and have not been replaced by adequate alternatives. 1.54 The primary requirement for rebuilding the communities affected by the accident is the promotion of economic development and better household incomes. However, these steps need to be supplemented by initiatives specifically designed to strengthen social interactions and promote community leadership in towns and villages (Project 10). A variety of different models exist including the existing psychosocial centres and the various NGO and IVP based initiatives. Strengthening primary health care and the organisation of cultural activities and events in the affected areas will also contribute to community development. Conclusions 1.55 Enormous efforts have been made by the governments of the three countries concerned to address the effects of the Chernobyl accident. These efforts have been supplemented to a significant degree by assistance from international sources, public and voluntary. However, support from public international sources for programmes designed to address the needs of those directly affected by the accident has declined in recent years. Following the accident, the response was reactive in nature and focused on resettlement, urgent humanitarian assistance and monitoring of the effects of radiation on health. There is a widespread recognition that this approach is no longer adequate. 1.56 Fifteen years after the accident, governments in all three countries are reviewing their policies in response not only to economic constraints, but also to new priorities and a new perception of the kinds of measures that are needed to address the long-term consequences of the accident. The international community also needs to adopt a new approach to the needs of those affected. A concerted campaign is needed to remind the World of the on-going suffering of those affected by the disaster and of the continuing need for international support for efforts to promote recovery. 1.57 The Chernobyl complex is now closed, the process of resettlement almost complete, but the demands made by the communities involved have scarcely diminished. Indeed, for many of those in the villages and settlements directly affected by the accident, the needs are as acute as ever. In this perspective, the Report proposes a framework for the national and international response based on three successive phases. The first phase, covering the fifteen years following the accident from 1986 to 2001, could be described as the Emergency Phase. This 14 Final: 25.01.02 phase has been characterised by urgent measures to make the reactor safe, to resettle the population in immediate danger, to deliver humanitarian assistance to those in urgent need and to explore the best means to address longer-term issues through pilot projects and research. 1.58 The Report proposes a new approach to be embodied in a second, ten-year, Recovery Phase of initiatives. The new approach should focus on enabling the individuals and communities affected by the disaster to enter fully into society by taking control of their own lives and acquiring the means for self-sufficiency through economic and human development. Chernobyl related assistance, which was ring-fenced in the first phase, should increasingly be measured against a more holistic view of individual and community needs and, where possible, be progressively integrated into mainstream provision. It is suggested that at the end of this ten-year period, a further review of the issues should be carried out to define on-going Chernobyl related needs in areas such as health, ecology and research. Those exceptional needs that cannot be adequately addressed through mainstream provision should be carefully defined and be the subject of agreement between the governments concerned and the international community with regard to measures appropriate for a third, long-term Management Phase. 1.59 In order to ensure that the new campaign of initiatives is built on an agreed approach, workshops should be organised to launch the coming phase and to help the main parties to define the nature of their involvement over the coming ten years (Project 1). As far as is practicably possible, efforts should be made to promote consensus around a set of basic guiding principles. The international community should renew its commitment to helping to address the issues raised by Chernobyl through a medium term programme of development assistance and research. 1.60 Under this proposal, the governments of the countries concerned would reshape their post-Chernobyl programmes. While as far as possible maintaining their overall spend, they would concentrate special funding on those most in need, and progressively switch the majority of the resources involved from welfare assistance to mainstream provision, and to sustainable economic and social development. The communities concerned and the voluntary sector would be encouraged to enter into partnerships with donors to expand their role, while progressively directing their efforts towards measures designed to promote longterm sustainable development. The Recommendations and Project Concepts that follow translate these overarching principles into specific practical initiatives. Recommendations A new approach 1 The international community should adopt a new developmental approach to tackling the problems caused by the Chernobyl accident and the events that 15 Final: 25.01.02 followed. As far as is compatible with the continuing threat from radioactive pollution and the continuing need for appropriate humanitarian assistance, this approach should work towards normalising the situation of the individuals and communities concerned in the medium and long-term. 2 Rather than focusing narrowly on the issue of radioactivity, the approach should be holistic, integrating health, ecological and economic measures to address the needs of those concerned in the round. The approach should aim, as far as possible, to give individuals and communities control over their own futures. A high priority should be given to addressing the needs of children and young people in the affected communities. 3 The new approach should recognise that it is vitally important that the whole world learns the lessons of Chernobyl. The quest for understanding should be pursued in a manner that is of benefit not only to humanity as a whole, but also to those directly affected by Chernobyl and the events that followed. The international community must accept a share in the responsibility for the future well-being of those whose lives have been blighted by the accident. This shared responsibility should be expressed through a new generation of proactive initiatives to address the current and future needs of those affected by the Chernobyl accident. Institutional, policy and human resources framework 4 In a world of conflicting priorities, such a commitment cannot be open-ended. It is proposed that the international community adopt a set of priorities for a programme of assistance over the next ten years and that after that a further study be undertaken to review progress towards normalising life in the affected communities. 5 It is proposed that the UN calls a series of three national workshops involving governments and the donor community, one in each of the affected countries, to seek consensus on the new programme as soon as it practically can. The purpose of the workshops should be to mobilise all of the relevant parties around the objectives outlined in this report. 6 The international community, the governments of the countries concerned and the voluntary sector should engage in an open-minded dialogue over the focus and cost effectiveness of the main policies. So far as is practicable, the workshops should seek to promote consensus on the broad approach to be pursued in the forthcoming period. An important aim should be to discuss how the elements of the proposed new approach would fit in with the existing framework of strategy and national activities as set out in the respective National Programmes. Priorities should be agreed as a basis for pulling the various project concepts together into thematic action programmes. 16 Final: 25.01.02 7 It is proposed that a target of between 5% and 10% of the cost of the rebuilding of the Chernobyl Shelter, be set for this appeal. Consideration should be given to developing a programme implementation capacity (possibly based in the UNDP representative offices in the three countries). 8 Resources should be concentrated on services which have the greatest effect in improving life expectancy and well-being. In practice this means concentrating on primary health care, health education and economic development in the affected communities. A high priority should be given to improving access to clean water and other local services in rural communities, not only to address the specific problem of radioactive contamination, but also to improve the overall condition of life for those who continue to live in the affected areas. 9 To promote a proper understanding of the environmental and health effects of Chernobyl a long-term, independent, properly funded, internationally recognised programme of research is needed. To ensure that this is conducted according to internationally recognised procedures and provide a high degree of confidence in the quality and impartiality of findings, consideration should be given to establishing an independent international body to initiate and oversee research into the effects of Chernobyl, as was done in the case of Hiroshima. 10 It is proposed that to meet this need an International Chernobyl Foundation (ICF) be established. Consideration should be given to using the existing mechanism of the UN Chernobyl Trust Fund. The constitution of the Foundation should be designed to ensure that it is independent and seen to be independent. The Foundation would receive funds from donors, including bodies with an interest in the results of research into the health effects of radiation such as the nuclear energy industry. The Foundation would channel resources into health and ecological research relating to the effects of the Chernobyl accident. 11 Wherever possible, Chernobyl related initiatives, for example relating to education and health, should be integrated into mainstream provision to ensure sustainability, cost effectiveness and wide dissemination. Efforts should be made to study and systematically apply the lessons of the accident and the events that followed in terms of the principles of disaster management. Towards a sustainable environment 12 Resources need to be focused on the most affected individuals and communities, in particular on low income rural households who grow and gather their own food. Innovative ways need to be developed to increase knowledge about how to live safely in environments affected by radioactive contamination. Important pilot studies have been carried out, often with international assistance. The lessons of these pilot projects need now to be disseminated much more widely. 17 Final: 25.01.02 13 The concept of strategic environmental planning and transboundary environmental cooperation should be promoted in the affected regions, with the full participation of the communities concerned. This should involve support for the training of regional planning and environmental specialists. Such planning should, as far as possible, reflect the reality that the impact of Chernobyl transcends the frontiers of the affected countries. 14 Continuing research is needed into the effects of radioactive contamination on the environment and into how best to address problems such as the dispersal of radio-nuclides in water and into the atmosphere, particularly as they affect groups such as forestry workers and hunters and their families, who are especially at risk because of their particular patterns of life. 15 It is proposed that an International Chernobyl Research Board (ICRB) be set up under the umbrella of the proposed ICF. This would be an expert body, which would meet periodically to make recommendations to the ICF on the priorities for research in the fields of ecology and health. The ICRB would also be responsible for making the results of research accessible to the public. 16 Efforts are needed to identify positive and sustainable ways to make use of the most affected areas that reflect the radiation hazard, but also maximise the potential for the benefit of the community. In this context, the international community should explore with the governments concerned the possibilities for promoting specialised tourism and for maximising the contribution that these areas can make to the preservation of international biodiversity. Continued efforts are also needed to develop and promote agricultural products that can be produced safely where radionuclides are present in the soil. 17 Efforts should be made to strengthen the local capacity for sustainable development by establishing a small grant facility for voluntary organisations and local government interested in promoting sustainable development initiatives. Consideration should be given to involving local people in the development of local recovery plans for the most severely affected districts. Health in the affected communities 18 Efforts to address the health effects of the Chernobyl accident need to be undertaken in the context of a wider reform of health care provision in the three countries. Such reform should be based on a rigorous examination of the cost effectiveness of current practices and a determined effort to ensure that resources are allocated on the basis of medical need. Strong measures are needed to improve the level of care available to poor people living in rural areas. Particular attention needs to be paid to addressing the effects of social and environmental factors on health, including poverty, poor diet, alcoholism, tobacco abuse and poor living conditions including inadequate basic services such as sanitation and access to clean drinking water. 18 Final: 25.01.02 19 Increased attention needs to be paid to health education. This should be undertaken in way which is participative and as far as possible is channelled through local structures such as schools and parents’ groups. It should address the issue of how to minimise the hazard to health from radioactive contamination in the context of broader guidance on how to promote family health and wellbeing in the circumstances which prevail in the affected communities. 20 Continued efforts are needed in the field of medical research both as a basis for designing more effective care and as a means to reduce distress caused by illgrounded fears. The International Chernobyl Research Board should make recommendations on the priorities for research on issues relating to health and to make the results of research accessible to the public. Research issues to which particular attention needs to be paid include a possible link between radiation and breast cancer, adult thyroid cancer, and the health of clean-up workers who worked in the vicinity of the reactor during 1986 and 1987. 21 Special attention should be paid to the lifetime needs of the generation of people who were infants or children at the time of the accident, lived in the areas affected by the fallout of radioactive iodine and who may have contracted, or be at risk of, thyroid cancer. For these, elimination of iodine deficiency is a priority (as, for the population at large, is protection against iodine deficiency disorders through the iodisation of salt). The international community should explore the possibility of developing and funding a long-term strategy to support the special needs of these people, many of whom will need expensive medication and monitoring for the rest of their lives if they are to survive and enjoy good health. 23 The social, psychological and economic effects of the disaster should be properly studied and evaluated and appropriate responses developed. Efforts must be made to apply the lessons of successful interventions to address the psychological and social needs of the affected individuals and communities more widely. Careful consideration should be given to the results of research which indicates that the psychological welfare of people who remained in their homes in the affected areas after the accident is better than that of those who were evacuated. 24 A high and growing proportion of people who were evacuated from the affected areas wish to return to their old homes. As far as possible people should be allowed to take their own informed decisions about where they wish to live, even if those decisions may lead to them facing a measure of increased risk. Studies should be undertaken to establish how far the present regime of restrictions could responsibly be relaxed, taking into consideration the different needs and degrees of vulnerability of groups such as children, young people of child bearing age and older people. This review should also consider the issue of whether the policy of resettlement should be continued in its present form. 19 Final: 25.01.02 25 The new approach should fully reflect the vital role played by the voluntary sector both in terms of the scale of the effort and resources involved, and in exploring new initiatives and new forms of assistance. It should recognise that well run partnership initiatives, based for example on links between towns, communities, hospitals and children’s support groups, are a powerful means to promote cost effective and sustainable programmes. Voluntary initiatives should be supported with limited amounts of public funding from international sources to promote a much wider application of the good practice already developed through partnerships involving the affected communities. Such support should combine accountability and cost effectiveness with full respect for the independence of the voluntary groups concerned. 26 Efforts should be made to ensure that international initiatives supporting holidays for children from the affected areas in families abroad promote a positive image of the affected communities and that everything possible is done to ensure that the visits and the associated publicity promote mutual respect and individual development. The international community should promote the idea of a code of best practice, to be drawn up in conjunction with the voluntary organisations to ensure that parties involved in working with children from the affected communities follow recognised guidelines in all areas of their activities. Economic development and household incomes 27 Economic development aiming to make the affected communities economically and socially viable in the medium and long-term should play a central role in strategies to address the effects of Chernobyl. This should be done in such a way as to give the individuals and communities concerned control over their own futures, which is both efficient in terms of resources and crucial in addressing the psychological and social effects of the accident. 28 To address the needs of the affected population, economic interventions are needed at different levels. They need to reflect both the fact that very large resources are needed to promote the economic recovery in these communities effectively and also the reality that achieving economic self-sufficiency will free up large national resources, which are at present tied up in subsidies and special Chernobyl related assistance. 29 At the national level, sound finances and the creation of an open competitive market economy and an investment friendly business environment are preconditions for sustained recovery in the affected areas. Appropriate national policies need to be supplemented by a proactive approach to stimulating economic development at the regional and local levels. 30 It is important that national resources continue to be directed to the affected areas and communities. Because of the very low levels of income in the most affected rural areas, resources deployed under the national Chernobyl 20 Final: 25.01.02 programmes make a significant contribution to well being in these communities. A sudden withdrawal of such funding would increase distress and set back the process of recovery. As far as possible, however, these resources should be focused more closely on the individuals and communities most in need. Support needs to be sufficiently long-term realistically to bring about a change in expectations, by fostering self-sufficiency and initiative on a sustainable basis. 31 At regional level, initiatives are needed to promote inward investment, domestic and international, to promote employment and create a positive image for the areas concerned. The international community can play an important part in this by assisting in transferring experience from successful initiatives in other parts of the world, which have been blighted by economic restructuring, high levels of unemployment and environmental contamination. Efforts should be made to build upon experience of the local economic development agencies already functioning in the Gomel Region (Belarus) and Slavutich (Ukraine) to build a network of intermediary organisations which are sensitive to local conditions and can act as an interface with national and international development bodies and donors. 32 Active measures are needed to encourage the establishment and growth of small and medium size enterprises in the affected areas and in the adjacent towns and cities using the whole range of business support techniques which have been tried and tested in other parts of the world. Because of the nature of the local economies concerned, particular efforts are needed to promote indigenous agricultural and food processing businesses by supporting the growth of existing enterprises (whatever their ownership status), and through new ventures. 33 Examples of good practice in the three countries and abroad, including community based solutions such as credit unions and producer and consumer cooperatives should be adapted to the special circumstances that apply in the affected areas. An appropriate organisational framework should be developed to ensure that such businesses get the support that they need. 34 At local level, a high priority should be given to supporting very small-scale business development, including village level enterprise clusters to boost the incomes of the poorest households. Such initiatives must draw on the growing body of international experience in this area and be sensitive to the very special problems affecting communities which largely depend on food production in areas suffering from radioactive contamination. 35 Vigorous efforts should be made to promote the rebuilding of community structures to replace those which were lost in the process of evacuation and as a result of the break up of the Soviet Union. Initiatives specifically designed to strengthen social interactions and promote community and economic leadership in towns and villages are needed to underpin sustainable recovery. 21 Final: 25.01.02 Project Concepts A. Cross sectoral 1. Policy dialogue on new strategy for international Chernobyl co-operation * 2. Support for the development of local sustainable development initiatives through international voluntary partnerships. * 3. promoting consensus among governments, the donor community and the voluntary sector is crucial to the success of the new strategy for postChernobyl recovery. The project would involve organising a series of workshops, public hearings and media events at the national, regional and local levels in the affected countries. The aim would be to build a common approach based on the principles of international cooperation and sustainable development. since 1986, many community and institutional twinning links have developed between local authorities, schools and other bodies in the affected Regions and abroad. The project would encourage these to extend from humanitarian assistance to sustainable development initiatives, through promotion, training, and the operation of a small grants scheme and would encourage the development of new international twinning projects. Promoting understanding of the internationally validated research. * effects of the accident the project would address the need for a more systematic, independent and better-funded approach to research into the ecological and health effects of the Chernobyl accident through the establishment of an independent International Chernobyl Foundation served by an international board of experts in appropriate areas of environmental and health science. B. Towards a sustainable environment 4. Transboundary environmental co-operation in the affected areas. * through the project would seek to improve trans-boundary co-operation in dealing with environmental issues such as water contamination, fire protection and radiation protection standards, through joint projects, information exchange and training. 22 Final: 25.01.02 5. Promoting innovative radio-protective techniques in private agriculture. * 6. Strengthening capacity for primary environmental care and disaster management * 7. the project would seek to promote the use of soil and fodder additives, especially by small scale private farmers, which constitute the most at risk group. It would promote new techniques. The project would encourage long-term improvement in practices through training and example. The project would (1) develop capacity for addressing priority environmental issues at the local, community and household levels. It would provide small grants to NGOs and local government bodies initiating sustainable development initiatives, including activities aiming to reduce radiological hazards and promote environmental education and networking activities in the framework of UNICEF’s primary environmental care approach; (2) analyse the implications of the accident and the events that followed as a basis for strengthening local and national capacities in the field of disaster management. Conservation of the natural and cultural heritage of the affected areas. * The project would encourage long-term environmentally sustainable economic development in the affected territories by promoting unique features of the natural environment and culture of the area, develop the local capacity for natural resources management and elaborate a plan for conservation of biodiversity and cultural assets through economically and socially sustainable measures such as the developing a network of reserves and the promotion of scientific tourism. C. Health in the affected communities 8. Development of international voluntary partnerships (IVPs) involving hospitals and clinics in affected areas. * the project would promote, monitor and a provide a small grant facility to support the establishment of IVP links between hospitals and clinics serving the affected communities and similar institutions in other countries. The grants would be allocated on the basis of proposals through competitive selection. The project would provide a cost effective means of building links between health workers in the affected communities and in other parts of the world, promoting mutual understanding and disseminating best practice in health care. 23 Final: 25.01.02 9. Integrated health education through training of trainers, parents as educators in healthy living and schools of health * 10. Strengthening primary health care * 11. the project would raise awareness of, and implement integrated holistic approaches to, primary health care within the health care system; build capacity to address local infant and child health priorities; strengthen health surveillance; evaluate essential drugs and equipment and promote greater community involvement in primary health care delivery. Addressing the needs of children and youth from the affected areas * 12. the project would: (1) address life style problems at the root of high levels of heart disease and trauma in the affected areas, by training medical and nursing staff in health promotion, multi-skilling health workers, promoting internet access and encouraging women’s health initiatives and other targeted programmes; (2) assist parents to give children healthy living knowledge and habits from an early age. The project would involve participative training and learning based in schools, community centres and social and cultural centres in the affected areas; (3) promote UNICEF’s Schools of Health concept by preparing and implementing a programme in the affected areas to encourage schools to use methods which promote childrens’ health involving coordinated action by teachers, psychologists and physicians leading to this approach becoming part of the core curriculum. the project would: (1) develop the capacity of youth organisations and the media to promote young people’s health and development in the affected areas; and (2) evaluate the impact of youth health holidays and address the need for an agreed set of international guidelines covering the activities of NGOs and IVPs working with young people from the affected areas. Mutual respect and individual and community development should underlie work with young people. There is a risk that, in seeking host families, sponsoring organisations may sometimes inadvertently propagate inaccurate and negative images of life in the affected communities. The project would promote the concept of guidelines, organise consultation and endorsement and disseminate an agreed definition of good practice. Research on priority health issues. * This family of projects would promote research into: (1) the health of clean-up workers; (2) claims of excess breast cancer; possible excess incidence of thyroid cancer in adults; (3) distribution of caesium in body tissues and risk of specific damage; (4) cost effectiveness of screening for thyroid cancer; (5) treatment and follow-up needs of thyroid cancer 24 Final: 25.01.02 patients; (6) possible effects of radiation on intra-uterine development; (7) relative advantages of resettlement as compared to continued residence in (or return to) contaminated areas. 13. From psychosocial rehabilitation to development. * the project would support the existing Socio-Psychological Rehabilitation Centres; help to re-orient their focus from rehabilitation to development; strengthen links with local government and the NGO sector and develop their potential as instruments for promoting a wider understanding of issues relating to the risks and perceived risks of living in areas affected by radio-active contamination. D. Economic development and household incomes 14. A network of regional economic development agencies in the affected areas. * 15. Promoting inward investment in the affected areas. * 16. regional economic development agencies have proved their value in many parts of the world. The special problems and opportunities of the affected areas call for a locally rooted approach, built on partnership between public administration and the enterprise sector. Such agencies could encourage new small and medium size business ventures, help existing businesses to grow and provide an interface between international donors and the local community. large resources are needed to bring about the recovery of the affected areas. Specialist skills are needed to identify the comparative advantages; build positive images; actively seek national and foreign investors; facilitate the investment process; and maintain a relationship with investors. The project would support capacity building through existing structures and specialist inward investment promotion bodies. Reshaping regional and national budgets and commuting Chernobyl benefits into start-up finance for income generation. * (1) there is a continuing need in the three countries to promote better targeted use of public resources and to increase the effectiveness of social welfare spending while making resources available for local and regional economic development; (2) many families living in resettlement communities depend wholly on Chernobyl benefits. This drains scarce public resources and has created a multi-generational downward spiral of dependence. Such families have animal raising and horticultural skills, but lack capital to buy stock and equipment. The project would contribute 25 Final: 25.01.02 to buying out entitlement to benefits in return for start-up finance for household businesses and provide support in the initial stages. 17. Development of village level clusters of household businesses. * 18. Promotion of international enterprise partnerships through transfer of technology and business best practice * 19. the project would address the need to strengthen the commercial and technical basis of small and medium sized businesses in the affected Regions by promoting partnerships with businesses in other countries. The project would provide grants and would involve the transfer of technology and improved business practices linked to the establishment of a commercial relationship between the partners. The concept is based on a format successfully piloted in Romania through the EU Phare Programme. Creation of a network of credit unions in the affected areas. * 20. rural families in the affected areas traditionally depended on state and collective farms for their money incomes, but produced much of their food themselves. The project would assist households through advice and small grants to build income-generating activities on the basis of their domestic skills. Promoting village level clusters of household businesses would generate economies of scale in purchasing, transport and marketing and encourage technical and business skills at the local level pilot projects already successfully undertaken by UNDP and other agencies demonstrate the possibility of promoting household level businesses and self-sufficiency through credit unions. The project would extend this experience to a range of communities in the affected areas and in resettlement villages using proven methods involving the provision of advice, training, management support and small scale start-up finance. Slavutich Town customised training initiative. * the project would help to equip people made redundant from the Chernobyl Nuclear Power Plant with the skills to enable them to find employment in the construction of the new containment shelter and other civil works associated with decommissioning. It would offer a service to the construction companies in identifying and training potential local recruits to meet their specific needs. The industry would play a part in the management of the initiative and contribute human and material resources. The above concepts are developed more fully in Project Notes available from the UNDP and UNICEF offices in Kiev, Minsk and Moscow. 26 Final: 25.01.02 Part II: Mission Findings Section 2: The accident and the events that followed 2.01 The Chernobyl Nuclear Power Plant is located in the Kiev region in the north of Ukraine, 7 km south of the Ukrainian-Belarusian border in an area of forest and meadows near the point where the Prypiat river joins the Dneiper. It started producing power in 1977. The fourth reactor unit went into operation at the end of 1983. Between 1 and 2 am on the 26th of April 1986, an accidental explosion during a safety test destroyed the core of this unit and started a powerful fire, which lasted for about 10 days. A massive amount of radioactivity was released into the environment during the explosion and the fire. 2.02 Contamination was most intense around the stricken reactor, where lumps of the reactor core expelled by the explosion and large particles fell. However, the bulk of the radioactive material significant for the current environmental situation was initially released to the atmosphere. This material was carried by the wind and gradually fell out over large areas of Belarus, Russia, Ukraine and beyond. During the fire the wind and other climatic conditions changed several times. Initially the radioactive plume was blown westwards across northern Ukraine and southern Belarus. Subsequently fallout was carried in a northerly direction, affecting the eastern parts of Belarus and the western areas of the Russian Federation and then in a southerly direction towards Kiev. Evolution of the environmental situation 2.03 Reliable data regarding the composition and distribution of radioactive contamination during the first weeks after the accident is lacking. However, the released material certainly contained a wide variety of radioactive substances with various physical, chemical and biological properties. Of primary significance to human health during this period was radioactive iodine - the isotope 131I, which ultimately led to a large increase in the incidence of thyroid cancer in children born prior to the accident. This isotope has a half-life of 8.05 days, so the extent of its presence in the environment immediately after the accident can only be judged from historic data, mathematical models or expensive high-tech field research. All these sources point to the possibility of high initial 131I contamination even outside the areas currently designated as affected by the Chernobyl accident. 2.04 Radioactive particles were deposited on soil, vegetation, buildings, machinery and other objects. Gamma-radiation emitted by these particles was the major component of the so-called “external” dose received by the population during the first months after the accident. During the period of the fire, the weather in the western part of the Soviet Union was showery. The distribution of the fallout depended largely on where it happened to rain and hence was very patchy. As a 27 Final: 25.01.02 result, the level of contamination can vary greatly between one village and another and even between adjacent fields. 2.05 The radioactive fallout from the Chernobyl accident primarily affected rural areas largely occupied by forests and wetlands as well as arable land and pastures. Prior to the accident rural communities in the area traditionally relied on agriculture (mainly grain, potato and flax production and livestock farming) as well as on harvesting wild products such as mushrooms, berries, game and fish. The timber industry and peat extraction were also important components of the local economy. Immediate Response (1986 – 1991) 2.06 Immediate action to tackle the consequences of the accident focused on protecting the population from exposure to the already released radioactivity. This was achieved through urgent evacuation of the town of Pripyat and other nearby settlements, and by clean-up works. Evacuation was initially applied on an obligatory basis to the population of the Exclusion Zone (extending 30 km in all directions from the Chernobyl Plant). Later, the primary criteria became the density of contamination of the area by the radioactive isotope of caesium (137Cs) and the average individual doses for particular settlements. Clean-up works involved washing off buildings and streets, removing topsoil and burying contaminated equipment. To prevent further release of radioactivity, a structure the so-called shelter or sarcophagus - was fabricated around the stricken reactor. Highly contaminated soil in the vicinity was removed. A system of dams and other waterworks was erected to reduce the run-off from contaminated territories. 2.07 Restrictions on land-use were implemented and controls of radioactive contamination in foodstuffs and other produce strengthened. In the years following the accident, standards for contamination by radioactive substances were made progressively stricter. The restrictions on land use were supplemented by the application of agricultural countermeasures to prevent the migration of radio-nuclides from soil to food stuffs. A strong research and development capacity was created to achieve this purpose. Dozens of countermeasures were tested and some were introduced in routine practice. 2.08 A policy of compensation for various categories of Chernobyl victims was also introduced. The eligible groups included people who had been involved in the post accident clean-up, people who had been resettled and people who continued to live in areas with above a certain level of contamination. Compensation took the form of welfare payments and free and priority access to such things as medicine, travel and health recuperation holidays. The cost of these measures rapidly became a significant factor in the national budget. According to the Ukrainian national report “15 Years after the Chernobyl Catastrophe” the Soviet Union spent $18 billion on Chernobyl rehabilitation between 1986 and 1991. Of this, 35% went on “social assistance to affected people” and 17% on resettlement. 28 Final: 25.01.02 Chernobyl and the politics of transition 2.09 Important features of the policies adopted and continued by the Governments of Belarus, Russia and Ukraine, can only be properly understood in the context of Soviet conditions and practices and the politics of the transition. Soviet legislation gave high priority to the protection of the welfare of the citizen but, because of the absence of market based pricing, planners lacked the means to estimate opportunity costs effectively. Exchange of information and dissent were limited, while the State possessed very considerable powers of compulsion. 2.10 For example, mass resettlement had been used, in the comparatively recent past, as an instrument of public policy in the Second World War in the cases of the socalled Volga Germans and the Crimea Tartars and in the settlement of Kaliningrad after the War. Following the Chernobyl accident, the Soviet Government adopted a very cautious policy with regard to the level of radioactive contamination which was considered acceptable for inhabited areas. This meant that a large number of people were subject to compulsory or voluntary resettlement. Because of the political environment, the Soviet State, with its vast resources, was able to embark on resettling several hundred thousand people without serious challenge from the communities concerned. 2.11 After the Soviet Union broke up in 1991, Chernobyl became a key factor in domestic politics and in relations between the three new states. Belarus and Ukraine demanded compensation from Russia for the effects of the accident. Political institutions and procedures were immature. Politicians took up the issue of Chernobyl energetically on behalf of their constituents and in some cases parliaments agreed benefits without adequate regard to the resources available. As a result, some commitments could not be fully met. Especially in the case of Belarus and Ukraine, Chernobyl benefits came to represent a heavy burden on the national budgets and drained resources away from other areas of public spending. By the late 1990s, however, scaling them down, or exploring alternative strategies had become politically impossible. 2.12 Faced with limited resources, the three countries each adopted different priorities. In Belarus priority was given to improving conditions in communities situated in contaminated areas, or which received large numbers of resettlers. Substantial resources were also allocated to assisting collective farms to grow clean products. The Russian government continued to pay comparatively high allowances to Chernobyl victims, but in the late 1990s virtually stopped resettlement even from the most severely contaminated areas. Support for protective measures for pasture and arable land also declined steeply. The government of Ukraine spent heavily on resettling people and improving living conditions and also faced the burden of making the Chernobyl power plant safe and preparing it for closure. 29 Final: 25.01.02 National Programmes 1991-2001 2.13 Strategy for post-Chernobyl rehabilitation is spelt out in National Programmes. The first of these was adopted in 1990 by the Soviet parliament. Later each country produced its own programme. These are based on legislation passed by the national parliaments during the 1990s. While the programmes have a lot in common, each reflects particular national circumstances. The National Programmes take the form of action plans. They list tasks to be undertaken, with targets in terms of the number of flats, houses, schools, cultural centres, public baths and hospitals to be built. However, the way that they are prepared makes it difficult to assess the qualitative impact, and hence the cost effectiveness, of the expenditure involved. 2.14 Belarus has recently started implementing the “National Programme of the Republic of Belarus on Mitigation of Consequences of the Chernobyl NPP Catastrophe for 2001 – 2005 and until 2010”. The Russian Federation has Federal Programmes concerning protection of the population against the consequences of Chernobyl; “Children of Chernobyl”; and “Housing for Liquidators”. A new Ukrainian National Programme is expected to be adopted by the parliament this year. This will establish rehabilitation tasks for the period from 2001 to 2005. 2.15 The scale of rehabilitation actions undertaken by Belarus, Russia and Ukraine from 1986 to the year 2000, is indicated by the official statistics on the number of houses, schools and hospitals built, as shown in table 2.1. Very large investments were also made in physical infrastructure such as roads, water and electricity supply and sewerage. Because of the risk that was believed to be involved in burning locally produced wood and peat, many villages were provided with access to gas supplies for heating and cooking. This involved laying down a total of 8,980 kilometres of gas pipeline in the three countries in the fifteen years following the accident. Table 2.1 Housing and social provision Houses and flats Schools (number of places) Kindergartens (number of places) Outpatient health centres (visits/day) Hospitals (beds) Belarus 64,836 44,072 18,470 20,922 4,160 Russia 36,779 18,373 3,850 8,295 2,669 Ukraine 28,692 48,847 11,155 9,564 4,391 Total 130,307 111,292 33,475 38,781 11,220 Social Protection 2.16 The system of compensation payments established after the accident reflected a Soviet practice of, in effect, compensating exposure to risk rather than actual injury. Belarusian and Russian legislation provides more than seventy, and Ukrainian legislation more than fifty, different privileges and benefits for Chernobyl victims, depending on factors such as the degree of invalidity and the level of contamination. The system also guarantees allowances, some of which 30 Final: 25.01.02 are paid direct, while others take the form of, for example, free meals for schoolchildren. In all three countries, each family member is paid a monthly bonus for living on contaminated territory, but the size of the payment depends on circumstances. In Belarus these allowances vary from 2 to 20% of the minimum wage. In Russia, a family with two children can receive almost $40 per month, which is comparable to the average wage. However, such entitlements are unequally paid and in some cases people living in less affected areas get higher benefits, which feeds public discontent. Box 2.1: Categories of “Chernobyl victims” Those officially designated as Chernobyl victims include people who: • fell ill with radiation sickness or became invalids due to the consequences of the accident; • took part in clean-up activities on the Chernobyl site and in the evacuation zones in 1986 – 1987 (the so called “liquidators”); • participated in clean-up activities in 1988 – 1989; • continue to live in areas designated as contaminated; and, • were evacuated, or resettled, or left the affected areas on their own initiative. 2.17 Benefits for Chernobyl victims cover numerous aspects of life: health care, housing, travel, tax exemptions, access to university education, compensation for property and damage to health and monthly allowances for disabilities linked to Chernobyl. Some are implemented in full, while others can only be applied in part because of resource constraints. For example, invalids and liquidators are entitled to free medicines, though lack of cheap locally manufactured pharmaceuticals means that this is not always applied. Other privileges, such as priority access in hospitals, telecom offices, restaurants and car maintenance are in practice rarely claimed. Some other privileges, such as hors concours admission to universities and colleges would appear to be questionable in public policy terms. 2.18 Poverty caused by resettlement, restrictions on agriculture and the effect of the collapse of the Soviet Union led to more and more people claiming Chernobyl related benefits. With the economic crisis of the 1990s, registration as a victim of Chernobyl became for many the only means of access to an income and to vital aspects of health provision, including medicines. Several million people are now receiving pensions and special health care privileges as a result of being categorised as in some way affected (see Table 2.2). According to Ukrainian figures, the number of people designated as permanently disabled by the Chernobyl accident (and their children) increased from 200 in 1991 to 64,500 in 1997 and 91,219 in 2001. With inflation and increasing budget constraints, however, the value of the payments steadily fell. Thus in Belarus, the value of payments made to help people living in the affected areas to buy clean food is currently around $1.50 per person per month. The system has also created incentives that encourage potentially harmful or wasteful behaviour. The Mission spoke to people who had returned to the affected areas with their families in order to be able to claim a higher level of benefits. It met tractor mechanics in a 31 Final: 25.01.02 bankrupt farm in the Briansk Region of Russia who were not being paid, but who had turned down an opportunity to open their own workshop for fear of losing Chernobyl entitlements. Table 2.2 Number of people affected by the Chernobyl accident (to December 2000) Belarus Russia Ukraine Total Resettled people 135,000 52,400 163,000 350,400* People living on contaminated territories 1,571,000 1,788,600 1,140,813 4,500,413 Liquidators 1986/87 70,371 160,000 61,873 292,244 Liquidators 1988/89 37,439 40,000 488,963 566,402 Invalids ** 9,343 50,000 88,931 148,274 Total 1,823,153 2,091,000 3,189,477 7,103,630 * Includes voluntary resettlers ** Definitions vary between the three countries Health improvement 2.19 The initial response of the authorities to the medical aspects of the accident were those characteristic of the former Soviet Union. Registries of affected people were created and substantial resources were devoted to pensions and health care privileges, such as yearly medical examinations and extended visits to sanatoria for children. Epidemiology was poorly developed in the Soviet Union and much data relating to radiation was treated as secret. The amount of scientific information available to policy makers on the relationship between exposure to radiation and specific health conditions was therefore limited. As a result, a wide range of health conditions entitled an individual to be classified as a victim of Chernobyl. Ongoing uncertainty over the health consequences of exposure to radiation contributed to the pressure to register an ever-increasing number of people. This in turn further reduced the resources available for mainstream provision, both in the affected communities and beyond. 2.20 As the Soviet system of welfare provision has dwindled, the expansion of individual Chernobyl related benefits has led to a situation where scarce resources are allocated not primarily on the basis of medical need but rather on an individual’s ability to register as a victim. The system has promoted an exaggerated awareness of ill-health and a sense of dependency, which has prevented those concerned from taking part in normal economic and social life. This pattern of behaviour was described by the Kiev conference on the Health Effects of the Chernobyl Accident (organised with the participation of the Governments of Belarus, Russia and Ukraine in June 2001), as the “Chernobyl accident victim syndrome”. 2.21 Health holidays in sanatoria and summer camps are fully financed by the authorities for invalids, liquidators, people who continue to live in highly contaminated areas, children and adolescents. If the authorities cannot provide free holidays they are required to pay compensation. In Belarus almost 500,000 people, including more than 400,000 children, have the right to free holidays. 32 Final: 25.01.02 Children living in areas with contamination at a level above 5Ci/km2 (five Curies per square kilometre have the right to two months holiday. Disabled children and those under school age have to be accompanied by a parent, bringing the total entitlement to 700,000 holiday months a year. In practice, financial constraints limit the actual number of holiday months. In the year 2000, 293,895 Belarussian children and adults were provided with such holidays. A similar situation exists in Ukraine. Table 2.3 indicates the number of health holiday months taken per year in Ukraine in the period 1994 to 2000. Table 2.3 Health improvement holidays in Ukraine (1994 –2000) Adults Children 1994 57,000 340,000 1995 38,000 401,000 1996 49,000 453,000 1997 37,000 467,400 1998 41,900 482,200 1999 30,500 427,100 2000 25,400 347,500 Total 397,000 439,000 502,000 504,400 524,100 457,600 372,900 Pressure for change 2.22 This analysis of the Government response in the years following the accident is not intended to suggest that the policies concerned were necessarily inappropriate in the context of the transition period. Resettlement certainly reduced the collective dose and the number of individuals receiving unacceptably high doses. In the absence of alternatives, Chernobyl benefits became the key to survival for many of those whose lives were blighted by the accident. It does, however, explain how countries facing deep economic crisis became locked into a disruptive and expensive programme of resettlement and compensation without adequate examination of the costs and benefits involved. It also points to the need to examine whether the same results could not now be achieved by other means at a lower human and financial cost. 2.23 All three countries have seen a change in emphasis in their Chernobyl recovery programmes in the last few years. It is still not clear what direction policy will take in future. The pressure to find a new way forward has come about as a result of three main factors. First, the resettlement programmes are complete or virtually complete. Second, the seemingly inexorable rise in Chernobyl related welfare payments has forced policy makers to question whether the current pattern of expenditure is cost effective. Third, while nothing like a consensus yet exists, a clearer picture is beginning to emerge of the impact of exposure to Chernobyl-type radiation and health than was available previously. 2.24 The enormous scale of the effort currently being made by the three governments means that even small improvements in efficiency could significantly increase the resources available for those in need. Assessing the costs and benefits of 33 Final: 25.01.02 particular interventions more rigorously, and focusing resources more effectively, should be a high priority. This however, will take courage as reallocating resources is likely to face strong resistance from the many vested interests involved. 2.25 In practice, funding for the Federal Chernobyl programmes has declined steadily in recent years. This has left many projects half completed. Thus the Briansk Region in Russia has only been able to build 62% of the housing needed for relocation, 14% of the schools and 27% of outpatient centres. According to Briansk administration data, there are more than 1,200 uncompleted houses, water supply stations and other public buildings in the Region. The Mission saw many examples of abandoned half-built houses and facilities in resettlement villages in the course of its visits. Table 2.4 Chernobyl budget expenditures of the Ukraine, M$US Item 1. Social protection 2. Special medical care 3. Scientific research 4. Radiation control 5. Environmental recovery 6. Radiological rehabilitation & radioactive material disposal 7. Resettlement, housing and living conditions improvement 8. Exclusion zone maintenance 9. Other expenditures Total 1992 197.3 6.3 3.2 2.0 0.3 1993 196.5 3.0 4.4 1.6 .01 0.1 1994 478.1 8.8 5.0 2.3 0.4 0.2 1995 384.0 22.8 5.9 3.1 0.4 0.1 1996 545.6 19.0 7.0 4.4 0.2 0.2 1997 637.4 15.9 6.4 15.7 0.2 0.3 1998 429.1 8.2 8.9 8.7 0.2 0.2 1999 292.5 6.6 2.6 4.1 0.1 0.1 2000 290.1 6.4 1.8 2.7 .04 .05 276.1 197.8 205.3 167.4 194.1 193.8 86.5 39.50 13.7 19.7 17.7 510.8 25.8 15.9 436.0 46.4 25.9 755.7 44.9 41.9 638.3 52.1 43.4 835.2 56.1 13.2 939.0 42.5 0.3 584.7 25.6 0.7 371.8 17.4 0.4 332.7 2.26 In Ukraine, the overall Chernobyl budget has been declining since 1997 because of shortage of resources (Table 2.4). The proportion of expenses allocated to resettlement and living conditions improvement has gradually decreased while the proportion accounted for by social assistance, including medical care, welfare payments and health holidays, has increased - from 39% in 1992 to 87% in 2000. Some 4,600 people who agreed to be resettled are still waiting for new homes to be built. Budget constraints have meant that support for farmers to produce safe food has been cut back. The Republic of Belarus too has almost completed its resettlement programme, with 7,000 people still waiting for new homes. With a significant proportion of good agricultural land blighted by contamination, the Government decided to restore some land to crops in the mid-1990s. 2.27 Politicians and administrators generally expected the process of recovery to be over once resettlement was complete and the population were provided with jobs and proper services. To their deep disappointment, the gravity of the Chernobyl issue showed no sign of declining with the passage of time. As one public servant in the Gomel region of Belarus told the Mission: “We spent enormous sums of money in Chernobyl areas, but the number of complaints from people in the villages stays almost the same”. 34 Final: 25.01.02 2.28 The Mission found that government officials interviewed recognized that they could not simply continue with existing policies. They understood that a new approach would be needed which gave a higher priority to economic regeneration as the key to improvements in the affected rural communities, including improvements in health and ecology. Resources will be needed to create opportunities for people to support themselves and improve their own living conditions. The planning methods inherited from the old Soviet system will not be adequate to meet the challenges of the forthcoming phase. New concepts of social and economic rehabilitation will be needed based on qualitative as well as quantitative targets. The policy options for the coming years are discussed more fully in the following sections. Section 3: Environmental Consequences Current environmental situation 3.01 Radioactive contamination resulting from the Chernobyl explosion poses health risks to the rural population and constrains economic development. The significance of contamination for a particular location, community or household depends primarily on the level of Chernobyl fallout. The most widely used indicator is the density of contamination by radioactive caesium 137Cs. In Belarus, Russia and Ukraine, the territory is considered “contaminated” if this parameter exceeds 1 Ci/km2. So defined, there are 43 500 km2 of contaminated territory in Belarus, 59 300 km2 in Russia and 37 600 km2 in Ukraine. Contaminated territory is divided into five zones as shown in Table 3.1. It should be noted that 1Ci/km2 is a relatively low level of contamination. In substantial areas of Britain, France and Scandinavia, for example, natural background radiation, resulting in part from radon gas released from granite and other rocks, occurs at a level of between 1 and 5 Ci/km2. 3.02 Officially designated contaminated territories account for 23% of the surface area of Belarus, 5% of Ukraine and 1.5% of the Russian Federation. The population of these territories is around 6 million people: about 19% of the population of Belarus, 5% of the population of Ukraine and about 1% of the population of the Russian Federation. Serious concerns primarily relate to the so-called "highly contaminated territories" where contamination is between 15 and 40 ci/km2. At present between 150 and 200 thousand people permanently reside in these areas. The population of the zones with contamination exceeding 40 ci/km2 is insignificant and not precisely known. 35 Final: 25.01.02 Table 3.1: Zones of contamination in Belarus, Russia and Ukraine Contamination Official designation of zones density by 137Cs (Ci/km2 ) Belarus* Russia** Ukraine*** 1-5 Periodic radiation monitoring Privileged socioeconomic status Zone enhanced radiological control of 5-15 Zone with the Right to resettle Zone right to (if dose > 1 guaranteed resettle mSv/year) resettlement of 15-40 Zone of Mandatory Zone secondary resettlement (if obligatory 137Cs resettlement >40 resettlement 2 Ci/km or dose Zone of > 5mSv/year). priority Voluntary if resettlement below of >40 Territories adjacent to the Chernobyl NPP (including the 30km zone). Population evacuated 1986 1987 Zone of Resettlement Exclusion zone evacuation zone (exclusion (exclusion zone) zone) Sources: * - Goskomchernobyl 2001, ** - Russian Federation 1992, *** Ukraine 2001 3.03 Apart from the question of radioactive contamination caused by the Chernobyl accident, environmental trends on the affected territories are typical for rural areas of the former Soviet Union. The larger part of the affected areas was not significantly affected by industrial or urban pollution. Due to the recent economic decline, pollution from agricultural sources has also declined. The Mission found that, as in other rural areas, environmental services, such as drinking water supply, sewerage, waste water treatment, municipal solid waste collection and disposal are generally of a poor standard. Waste water was the most frequently mentioned local environmental problem. Gas heating systems had been provided extensively to the affected communities as a means to reduce the burning of 36 Final: 25.01.02 contaminated wood and peat. The Mission visited a number of locations, especially those initially designated for resettlement, where investment on local infrastructure had been frozen, leaving the situation with regard to basic environmental services worse than in comparable non-affected areas. Environmental contamination as a source of health risks 3.04 It is generally recognised that substantial doses of radiation were received by the general public and the clean-up workers in the period immediately following the Chernobyl accident (Table 3.2). According to some estimates (including UNSCEAR 2000) up to 90% of the total collective dose was received in the period between 1986 and 1995. Since risks that have already been incurred cannot be influenced by current or future environmental measures, the Report concentrates on future hazards. 3.05 Virtually all doses from environmental sources currently received by the general public on the affected territories are within the range of “low” doses. It should be noted that there is no universal scientific agreement on the nature and scale of the health risks of long-term exposure to so-called "low" levels of radiation. The ongoing medical debate on this issue is outside the scope of the current Report. According to mainstream scientific evidence, however, the health effects of individual lifetime doses well under one Sievert (1Sv) would not be statistically distinguishable from the pattern of disease in the population at large. Table 3.2. Average individual doses received 1986-1995 by population of affected territories in relation to current density of contamination by 137Cs Land Average individual doses* received in 1986-95 by contamination residents of affected territories, mSv 137Cs, by Ci/km2 Belarus Russia Ukraine 1-5 3.9 4.2 11.7 5-15 18.7 13.0 24.4 > 15 47.0 35.7 82.6 Source: derived from UNSCEAR 2000. Note: * - excluding doses to thyroid Radiation doses 3.06 The threshold for assigning settlements to the status of "contaminated by the Chernobyl accident" is an average annual dose of 1 mSv (milli Sievert). Ukrainian Chernobyl-related legislation aims to avoid individual doses exceeding 1 mSv/year or 70 mSv per lifetime (Ukraine 2001). The figure of 1 mSv/year is 37 Final: 25.01.02 also the current public dose limit recommended by the International Committee on Radiological Protection (ICRP). Thus, the annual average dose of 1 mSv (or an equivalent lifetime dose of 70 mSv) can be considered as a reference value for discussion of the actual doses of the affected population. Accurate measurement or calculation of doses is notoriously difficult and subject to many uncertainties and assumptions. This is one reason why the density of contamination per square kilometre rather than individual doses is primarily used as a criterion for compensation and counter-measures. It is even more difficult to forecast doses. 3.07 Generally speaking, doses of radiation depend upon three factors: (a) the level of contamination of a particular territory; (b) the nature of migration of radiation in the environment and into human bodies; and (c) the lifestyle and behaviour of the affected population. While (a) has been most generally used to describe the potential radiological hazard associated with particular areas, it is (b) and (c) that can be most easily influenced. The sources of doses to human beings are shown in Figure 3.1. The majority of the current collective dose results from contamination of the environment by 137Cs. A significant part of the dose derives from internal irradiation resulting from contamination of foodstuffs, most notably milk, meat and forest products (such as game, fish, berries and mushrooms). 3.08 Figure 3.1 also shows the various ways in which radioactive material can enter human beings. The dose received from foodstuffs, drinking water and inhalation, the so-called "internal dose", has decreased less sharply than the external dose and, at the moment, accounts for a large proportion of the total dose received by people in affected areas. Important sources are food and drink and the inhalation of radioactive particles, especially as a result of forest or peat bog fires or heating houses with contaminated wood. During forest or peat bog fires substantial amounts of radioactive material currently locked in soil or vegetation may be released into the atmosphere, and transported across large distances. In addition, most people on contaminated territories are subject to some external exposure. Figure 3.1. Key sources of radiation doses to humans resulting from the accident. Source: adapted from Ukraine 2001 38 Final: 25.01.02 Irradiation ofhum ans (doses) External Internal Ingestion Inhalation Eco- and agro-systems Vertical migration Fallout Wet and dry precipitation Transport in the atmosphere Radioactive cloud Fire atthe ChernobylNPP 3.09 As the Ukrainian National Report recognises, rural populations generally receive higher doses than urban populations. Table 3.3 shows the current and projected doses for the rural population of Ukraine, averaged for the officially designated contamination zones. It demonstrates that the average dose for about 11,600 people residing in the most contaminated territories (137Cs > 10 Ci/km2 ) will somewhat exceed 70 mSv in their lifetimes to 2055. However, only a small proportion of this dose (about 20 mSv) is likely to be incurred between 2000 and 2055. Table 3.3 also demonstrates that the major contribution to the collective dose occurs in highly populated areas with a low density of contamination, whereas significantly higher individual doses are received on largely depopulated but highly contaminated areas. Thus, reducing the collective dose and reducing the dose for high-risk groups require different approaches. Table 3.3: Past and projected doses of the rural population of Ukraine 137Cs/k m2 1 Populatio Number Average dose, mSv n, in of thousand settleme 19861986 s nts 2000 individual Collective person/Sv 19862055 198 19866 2000 19862055 21742,2 1,5 778 25357 5 32694 27523 0,36 1,2 39 dose, Final: 25.01.02 Average dose, mSv individual Collective person/Sv dose, 1-2 892,2 1153 2,1 12 14 190 10302 2 12485 2-5 423,4 669 4,5 20 25 190 8516 7 10542 5-10 39,6 120 11 34 44 426 1337 1737 10-15 8,4 22 21 54 73 176 457 614 15- 3,2 11 26 74 96 83 313 23109,0 29498 0,7 2,0 2,5 162 46210 51 Total 241 58385 Source: Ukraine National Report 2001 3.10 In particular villages and towns, the doses may be significantly higher than the average for a particular zone. There are currently more than 400 towns and villages in Ukraine where the average individual dose exceeds 1mSv/year. This number has declined significantly from the early 1990s, but has remained relatively stable in recent years. In 1996 in Russia, there were 307 villages (more than 48,000 people) where the average individual dose exceeded 1 mSv/year and 6 settlements (about 2,000 people) where the dose exceeded 5 mSv/year (Stepanenko 2001). 3.11 The variation of average doses between localities with the same degree of environmental contamination is determined by their environmental characteristics and by the effectiveness of the countermeasures. For example, radio-nuclides more readily migrate to vegetation (and hence to animals and ultimately to human bodies) on poor sandy and peaty soils and uncultivated pastures. Extensive peat bogs and mature forests present higher fire risks. Many of the pathways of radiation in the environment can be artificially controlled and managed to reduce the dose rates. Monitoring of foodstuffs, drinking water and other key environmental media can point to specific problem localities. 3.12 The doses may also vary widely within a particular town or village. In the same locality the variation of the doses to different individuals primarily depends upon lifestyle and the behavioural factors summarised in Box 3.1. At one end of the spectrum are well-educated and economically better-off urban dwellers who purchase their food. At the other end are the poorest and least educated groups of the rural population, who consume food from their own plots and from the forest. This conclusion is confirmed by numerous empirical measurements using whole body counters, which point to higher accumulated radioactivity among poor people from the countryside. 40 Final: 25.01.02 3.13 There are indications that radioactive substances such as as 137Cs and 90Sr may be migrating towards deep ground aquifers and accumulating in closed water bodies. This potentially presents a long-term threat to health the extent of which needs to be studied further (Germenchuk 2001). In one community visited by the Mission, a programme of laying down pipes to bring non-contaminated water to the community had been initiated. However, for budgetary reasons, the project had been stopped when the pipes were still several hundred metres from the village. A number of residents expressed concern over what they saw as a continuing threat to the health of their families. It was not possible for the Mission to establish how serious a problem radioactive contamination of drinking water supplies is in the affected areas. However, internationally accredited studies, including one recently sponsored by UNDP in Russia (UNDP 2001), indicate that the extent of contamination of aquifers is currently insignificant and only longterm monitoring is necessary. If this is indeed the case, it is important that steps be taken to reassure the public, as the issue is a cause for concern. High risk groups 3.14 There is some evidence that the doses received by high risk groups, as well as the number of people involved, may have been increasing in recent years, despite the overall reduction in radioactive contamination. This could result from increased poverty pushing people into switching to locally grown food, abandoning fertiliser-based countermeasures and consuming more forest products. Some of the recent economic changes, such as the disintegration of collective farms in Russia and Ukraine and the encouragement of private agricultural entrepreneurship, may have contributed to this trend. An increase in dose rates could also be linked to decreasingly effective protective policies. Banning the sale of products such as milk outside the affected areas (as has been done in Russia) may also have increased dose rates for the most at risk groups. 3.15 Foodstuffs that are certified as clean are widely available from commercial sources but at a higher price than home produced food. Much privately produced food, particularly milk, is not tested and may contain radioactivity above the control values. In addition, country people appear to be increasingly likely to ignore restrictions on consuming forest products. Thus, in spite of radioactive decay and other natural processes that are reducing the environmental radioactivity levels, doses for a proportion of the population may be increasing. While the majority of the affected population is receiving 1 mSv/year or less per year, a significant minority may be receiving annual doses of up to 5 mSv a year. Box 3.1: Major behavioural and lifestyle factors influencing exposure to radiation * Consumption of forest products: berries and mushrooms * Consumption of wild game and fish * Consumption of locally produced food, especially milk and meat 41 Final: 25.01.02 * Spending significant proportion of time outdoors * Using decentralised water supply systems, especially shallow wells * Decentralised house heating using firewood * Familiarity with, and attitude to, risk factors and local information on radioactive contamination Promoting Ecological Recovery 3.16 The underlying trends in environmental contamination can scarcely be influenced by policy measures; however, the influence of this contamination on humans can be controlled to a large extent. In the short and medium-term, the health and economic impacts of contamination depend more upon policy, and the capacity to implement policy, than on natural environmental processes. Current policies will also influence the long-term future of the region (after radioactivity has significantly declined) insofar as they affect the future human, environmental and economic capital of the region. In other words, the health and economic impacts of environmental contamination depend upon political and economic changes. 3.17 The effectiveness of any of these policies most critically depends upon the existing capacity at local, regional and national levels. At the national level, responsibility for dealing with the consequences of the Chernobyl accident has typically been spread between different agencies, with overall co-ordination in the hands of the Ministries for Emergency Situations. Special Chernobyl departments in the respective Region administrations are responsible for much of the delivery of Chernobyl related programmes such as resettlement and decontamination. 3.18 The capacity to address Chernobyl issues in all three countries has been significantly strengthened during the last fifteen years. A relatively strong capacity exists at the national level in monitoring, research and education with a strong build-up of instrumentation and skills. This has continued up to the present time with data, knowledge and experience accumulating in centres of excellence. Examples of this are the Kiev Radioecology Institute, the Science and Technology Division of the Exclusion Zone, and the Typhoon Institute in Obninsk. In contrast, many of the facilities created at the local level in the late 1980s and the early 1990s have shown signs of decline due to lack of funding and qualified personnel. Some have been closed down and others operate at less than full capacity. For example, the Mission visited out-stations involved in monitoring food products which lacked the resources to carry out their functions. Many of these have closed, making it difficult for local people to obtain the documents they need to sell produce in the towns. 42 Final: 25.01.02 Table 3.4. Environmental issues in different Zones affected by the Chernobyl Accident Contamination level by 137Cs, Ci/km2 The nature of environmental issues Major state policies 1-5 Radiation does not pose serious health risks to any particular group. Economic activities may be hindered by indirect association with Chernobyl. Additional radiation monitoring. Extended social protection of the population. 5-15 Radiation may pose risks to small high risk groups. Economic activities hindered by Chernobyl name and contamination of some products. Local capacity undermined by outmigration of skilled people Radiation monitoring. Social protection. Countermeasures in agriculture 15-40 Radiation may pose risks to small high risk groups while average individual doses more often exceed legal limits. Economic activities hindered by frequent contamination of products, association with Chernobyl, restrictions on forestry, agriculture and other activities. Local capacity suffers severely from socio-economic decline Resettlement. Radiation monitoring. Social protection. Countermeasures in agriculture and forestry. Forest and water resource management Exclusion zone Risk of forest and peat bog fires threatening radioactive contamination of larger areas. Security of waste disposal sites and abandoned villages Forest and water resources management. Restrict access. Research on migration and effects of radiation. Effectiveness of control measures 3.19 The initial radiation protection measures adopted in response to the Chernobyl accident in the USSR in the mid-1980s aimed to limit the individual life-time exposure to 350 mSv (1000 mSv = 1Sv). This would mean limiting the annual dose to under 5 mSv. Subsequently, this threshold was made stricter and a number of measures initiated to reduce the individual dose to under 1 mSv/year. This has led to the setting of control values for caesium and strontium in food products at quite low values. The target values are achieved by discarding products which do not meet the standard and by the use of various dose reduction techniques such as potassium fertiliser, and ferrocyanide fodder supplements for cattle. Enforcing these measures required a significant increase in the capacity for the radiological monitoring of food products. The measures undertaken appear to have gone some way to reducing individual doses and maintaining the confidence of urban dwellers in the safety of food products in the shops. Table 3.5: Technical measures for controlling radioactive contamination Policy area/objective Examples of countermeasures and notes Constraining presence of people in contaminated areas Resettlement (significantly scaled down in recent years); restriction of access to the exclusion zone (fencing, roadblocks, etc.) 43 Final: 25.01.02 Policy area/objective Examples of countermeasures and notes Land and water management Restriction of forestry and agriculture on contaminated lands; forest management and fire prevention; water and wetland management Countermeasures in agriculture Improving pastures; introduction of additional fertilisers and liming, where necessary; application of food additives absorbing radiation (e.g. ferrocyanides); selection of appropriate crops. Reduction of radioactivity in the immediate human environment Cleaning up houses, removal of upper level of soil in courtyards, installing connections to gas lines to reduce usage of firewood for heating, installing centralised water supply systems Control of radioactive contamination of foodstuffs Setting standards for radioactive contamination of foodstuffs; systematic monitoring at place of production and in distribution network; discarding contaminated products or using them for non-food purposes. Providing compensation to buy "clean" food Education and information Publication and dissemination of information materials (leaflets, brochures, etc.) with specific information on local contamination and advice on reducing exposure to radiation. Dissemination of information through the mass-media. Advice for households where members manifest accumulation of large amounts of radioactivity* Source: interviews and observations July-August 2001: * - e.g. in Narodichi, Zhitomir Region, Ukraine. 3.20 The policy of all three countries has been to relocate all people living on territories with contamination by 137Cs exceeding 15 Ci/km2 or dose exceeding 1 mSv/year. Priority resettlement was implemented for territories with contamination exceeding 40 Ci/km2 or doses of 5 mSv/year. Voluntary resettlement from less contaminated territories was also legally guaranteed. For example, according to the current Russian legislation, mandatory relocation is carried out for communities where the average individual annual dose exceeds 5 mSv. If this dose exceeds 1 mSv, the individuals are entitled to voluntary stateaided relocation. These policies and their subsequent development into a set of measures for land, water and natural resource management have been largely effective in reducing the collective dose. There seem to have been significant achievements in controlling forest fires in contaminated areas and in restricting unauthorised access to territories that are highly contaminated. 3.21 The resettlement policies, however, have never fully reached their objectives. Hundreds of thousands of people still live in territories officially designated as unsuitable for habitation. The majority of these people are not subject to 44 Final: 25.01.02 significant health risks from radioactive contamination. However, they may suffer severe socio-economic and psychological pressures. Evacuation and resettlement, especially immediately following the accident, probably very significantly reduced the collective dose. However, the effectiveness of the measure declines as time goes by and negative effects may start to outweigh the benefits, especially if other potential uses of the resources involved are taken into account. Resettlement appears to have been least successful when implemented inconsistently, leaving significant numbers of people behind in villages designated for evacuation. Currently, resettlement continues, though at a minimal scale. However, some of those most at risk (for example, the poorest sections of the rural population) often do not want to move. 3.22 While effective in reducing the collective dose, the restrictions on land use undermined the economies of agricultural communities and necessitated large additional subsidies from the centre to support the proper maintenance of abandoned land and forests. These strategies could be made more efficient and sustainable if alternative uses of the excluded territories were more systematically considered. For example, wetlands and forest ecosystems can be used for biodiversity conservation purposes and as a focus for scientific tourism. A similar argument applies to the unique and rich cultural landscape. 3.23 Sound strategic management of land and other natural resources requires a strong capacity for long-term planning and management at the regional level. By and large capacity is, at present, insufficient to deal with the complex set of problems involved. Certain environmental management issues, such as flood control on contaminated territories, require stronger trans-boundary co-ordination and cooperation. For example, seasonal flooding of pastures and meadows in Belarus benefits agriculture there, but leads to radioactivity leaching from the soil and causing contamination downstream in Ukraine. Agricultural countermeasures 3.24 The effectiveness of countermeasures in agriculture depends on the level and character of contamination (for example, uptake of 137Cs is controlled more easily than uptake of 90Sr) as well as the consistency with which a particular measure is applied. From the point of view of protecting critical groups, only a narrow range of countermeasures (such as improving private pastures and distributing fodder fortified with materials that absorb radioactive substances) are effective. From the point of view of overcoming environmental constraints to economic development, only those countermeasures which allow production at competitive costs can be considered effective. Unfortunately, many countermeasures require large subsidies or the final produce is too expensive to sell. 3.25 Many of the clean technologies were unsuitable for application in the private agricultural sector. Naturally, the situation in the private sector was not a major consideration under the centrally planned economy in the first five years after the 45 Final: 25.01.02 accident. However, private agriculture is a source of serious health risks and also the key to alleviating rural poverty. Its increasing importance today means that the use of countermeasures needs to be considered. The issue is not straightforward. Subsidies to encourage the use of clean technologies in the collective and state sectors have been falling in recent years. Reversing this trend is likely to be difficult, as can persuading country people to use food supplements and fertilisers. In addition, the question of which techniques are most appropriate for use by smallholders needs to be more fully explored. 3.26 The relevant research and development capacity is relatively strong and significant field experience exists in applying various countermeasures. However, the overwhelming majority of these have been subsidised and the capacity for evaluating their effectiveness in economic terms, promoting them and developing new measures seems to be lacking. Developing this capacity is becoming a priority as state subsidies decline. Not only have radiological controls failed to reduce the exposure of high-risk groups to radiation from privately grown food and forest products sufficiently, they have also meant that much produce from contaminated areas cannot be sold. This has further depressed economic activity and forced people to consume a larger share of contaminated products locally, increasing their exposure to radioactivity. Public information and the radiation hazard 3.27 Public information and education initiatives have been among the least consistently planned and least effective measures. Information campaigns have frequently been conducted in isolation from other activities and have generally involved a one-way top-down process. Information on radiological protection has often not been linked to explanation of the health effects of radiation. The result has been a confused perception of radiation and its effects among all sections of society. Widespread ignorance exists as to how best to minimise exposure to radiation. For example, one 10-year-old Belarusian boy, who had been taught about the dangers of radiation in school, told the Mission that the best way to avoid exposure was to “run and hide in the forest”. 3.28 Strong anxiety and fear of radiation exists, compounded by mistrust of official information and an inability to interpret the available data. In other words, people have an inadequate perception of radiation risks and an excessively pessimistic perception of their own capacity to control them. A well-educated resident of Slavutich in Ukraine told the Mission: “We’re afraid to check the contamination levels of berries and mushrooms that we pick. We don’t want to know!” 3.29 There is a strong capacity for public and school education in the environmental area at national level in all countries. For example, the National Centre for Environmental Education in Kiev has a world-class capacity in teaching children environmental knowledge and related skills. At the same time, the corresponding local capacity in the affected territories is declining. Thus, the Young Naturalists 46 Final: 25.01.02 Station in Narodichi, Ukraine, has been closed down following the decline in the population of the area resulting from the Chernobyl accident. 3.30 There have also been a number of successful non-governmental initiatives in the field of information and education. For example, the Radimichi-Chernobyl Children NGO from Novozybkov, in the Bryansk region of Russia, has been organising an educational and health summer camp for several years. This has attracted talented young teachers and students to work with disabled children and young people from the area. This activity has been supported by voluntary groups from Germany. Among donor funded initiatives, the European Community’s ETHOS and ENVREG projects provide an important model of how technical assistance can be used to promote community based programmes involving environmental education. Box 3.2: Successes and failures of environmental policy Achievements of the response to the Chernobyl accident have included: * * * * reducing collective dose by technical, administrative, and economic measures; Significantly improving scientific understanding of the possible causes, scenarios and consequences of accidents on nuclear power plants; Improving preparedness to deal with consequences of nuclear accidents, including understanding of the effectiveness of different protective measures. Building the national capacity in Belarus, Russia and Ukraine to deal with contamination of the environment by radioactive material, including development of expertise, instrumentation and institutions. Failures have included: * * * * * 3.31 a significant number of rural people in high risk groups are still exposed to substantial and, probably, increasing doses of radiation; environmental contamination still imposes significant economic constraints associated with a variety of protective measures, many of which are not effective in the new economic and political conditions; economies and social structures in affected communities are deteriorating, alongside an apparent increase in poverty; the activities undertaken so far have failed to increase trust and reduce anxiety. low local capacity to deal with health, economic and environmental challenges. Despite the natural process of radioactive decay, the major pollutants of Chernobyl origin will continue to pose a hazard to health for decades to come. However, some studies indicate that the area of territory with the highest level of contamination will decline fastest. For example (according to Vakulovsky 2001), while in 1986 580 km2 of the Russian Federation were contaminated by 137Cs in excess of 40 Ci/km2, there will be no territories with such a level of contamination by 2006 (see Table 3.6). Some long-lived isotopes such as plutonium 239 and Americium 241 will stay in the environment for many thousands of years, though 47 Final: 25.01.02 fortunately they are almost exclusively confined to the zone adjacent to the Chernobyl Plant (see Germenchuk 2001). Table 3.6: Projected changes in radioactive contamination of territories of Russia and Belarus in the period 1986-2046 Levels of contamination by 137Cs Projected decline in the area of the contaminated territory between 1986 and 2046, times Belarus* Russia** 1-5 Ci/km2 ≈ 1.8 ≈5 5-15 Ci/km2 ≈4 ≈4 >15 Ci/km2 >10 ≈ 26 Total > 1 Ci/km2 ≈ 2.4 ≈ 5.2 Source: * - Germenchuk 2001, ** - Vakulovsky 2001 supplemented by calculations by A. Cherp 3.32 In summary, therefore, it appears that the main threat to health from current and future exposure to radiation concerns a distinct group of country dwellers who in live in contaminated areas (see Table 3.4), produce their own milk and depend to a significant extent on wild mushrooms, berries and game. Many of these people have very low incomes and have little choice as to their diet. In these circumstances, education is likely to have little or no effect unless it is combined with measures to enable them to increase their household incomes and to adopt measures to reduce their intake of radio-nuclides, through soil treatment techniques and animal feed supplements. Section 4.0: Health Current health situation 4.01 The health and well-being of populations in the affected regions is generally very depressed. As is true throughout the Former Soviet Union, life expectancy is low not only as compared with Southern and Western Europe, North America and Japan, but also with a number of countries from the developing world. Life expectancy for men in Belarus, Russia and Ukraine, for example, is some ten years less than in Sri Lanka, which is one of the twenty poorest countries in the world and is in the middle of a long drawn out war. Overwhelmingly the most important reason for this is the combination of poverty, poor diet and living conditions, and lifestyle factors such as tobacco and alcohol use. These factors may also, to some degree, be reinforced in the affected areas and communities by the psychosocial effects of the accident. Cardiovascular disease and trauma 48 Final: 25.01.02 (accidents and poisonings) are the two most common causes of death followed by cancer (this situation is not confined to the Chernobyl affected regions). Most doctors when asked what measures would most improve the health of the population said improved diet and living conditions 4.02 A well-established increase in thyroid cancer diagnosed in children and adolescents poses a major problem for health services, particularly in Belarus and Ukraine. While the disease is not generally fatal, the treatment is expensive and demanding upon resources. The populations in the affected regions also suffer from endemic goitre (enlarged thyroid gland) ranging from mild to severe, due to a deficiency of iodine in the diet. Iodine deficiency (ID) as well as affecting the thyroid gland, diminishes the IQ. As well as its negative consequences for IQ, iodine deficiency is also known to increase the risk of absorption of radioactive iodine by the thyroid gland. The population’s exposure to radioactive iodine, especially in the months following the accident, was enhanced because iodine deficiency led to the uptake of the radioactive iodine, mainly through drinking contaminated milk. 4.03 In many settlements visited by the Mission living conditions were far from conducive to good health. Thus, the perception held by local doctors that there had been a general increase in morbidity from non-oncological conditions, such as cardiovascular and respiratory conditions, may be well-founded. Concerns expressed by doctors over specific health effects allegedly related to radiation exposure, either since the accident (such as congenital conditions in new births) or in comparison with trends before the accident were generally not based on statistical evidence but on subjectively perceived trends. This, however, is not a reason to dismiss these claims. 4.04 Healthcare provision in the affected communities suffers from many of the problems that affect care in other predominantly rural areas of the three countries. The mission met many dedicated and well-qualified doctors and health workers. In contrast, equipment and buildings, such as hospitals and clinics, were often old and in a poor state of maintenance. It was evident that access to appropriate medicines was an almost universal problem. Although those registered as victims of Chernobyl have the right to free medical treatment, for others, the cost of even simple medicines could be an insuperable barrier to treatment for a wide range of conditions. In addition, many of the medicines that were available were herbal remedies rather than internationally recognised pharmaceuticals. 4.05 Many districts experienced difficulties in attracting doctors to work in contaminated areas, mainly because of isolation and lack of suitable housing but allegedly also to some degree because of the perceived risks of living in such areas. However, patient to doctor ratios reported to the Mission were usually about 300 to 1, which is high by international standards. In the smaller, more remote, settlements the full range of specialists was not available. This was especially a problem for those too poor to travel to district or regional centres, which might be over a hundred kilometres distant. 49 Final: 25.01.02 4.06 In a number of centres, the Mission saw examples of sophisticated equipment which had been donated by international voluntary organizations and charities. In some cases the equipment was being used in inappropriate ways or in circumstances which were less than ideal. In one hospital, for example, bone marrow transplants were being carried out without due attention being paid to the overriding need to ensure a sterile environment. In several clinics and hospitals, donated equipment could not be used for lack of materials or appropriately trained staff. These examples illustrated a recurring problem with one-off donations of capital equipment: that without continuing support in the form of training, maintenance and consumables, much or all of the potential of the equipment is wasted. 4.07 Despite the strong tradition of primary health care in the Soviet Union, a large discrepancy appeared to exist between the resources available for a minority of prestigious clinics and hospitals, mainly in urban centres, and provision in rural areas and smaller communities. It appeared that the issue of Chernobyl had in certain respects distorted the pattern of spending on health. Resources sometimes appeared to be focused on high cost facilities concerned with the health effects of radiation, and on mass screening, rather than on preventative medicine and community based care which could arguably yield better results in terms of curing disease and promoting good health. 4.08 It is well established that the populations in the affected areas exhibit strongly negative attitudes in self-assessments of health and well-being and a strong sense of lack of control over their own lives. Associated with these perceptions is an enhanced perception of the dangers to health of exposure to radiation. On the question of psychological health, judgements are necessarily very subjective. However, there is clearly a strong concern in the affected populations for health and a widespread belief that exposed people are in some way condemned to a shorter life expectancy. The Mission spoke to one overweight woman in her late fifties who suffered from high blood pressure. When asked whether she had tried to reduce her consumption of salt and fatty food, she replied: “Why should I? I’m a liquidator, I will die soon whatever I do”. Such feelings also are linked to a loss of initiative to solve the problems of sustaining an income and to dependency on assistance from the state. 4.09 The system of Chernobyl related benefits has created expectations in terms of payments and advantages and has undermined the capacity of the individuals and communities concerned to tackle their own economic and social problems. Studies carried out by the Institute of Sociology in Kiev indicate that 80% of respondents living in areas with a guaranteed right to resettlement expect “financial assistance and special medical treatment”. Among resettlers, 84% expect “special medical treatment” and 71% claim unemployment allowance. 50 Final: 25.01.02 4.10 The health situation encountered in the populations living in the affected territories is thus a complex product of inputs ranging from radiation induced disease, through endemic disease, poverty, poor living conditions, primitive medical services, poor diet, and the psychological consequences of living with a situation that was frightening, poorly understood and over which there seemed to be little control. Claims and counter claims 4.11 In the aftermath of the Chernobyl accident many claims have been made of diverse health effects among people who were evacuated, those living in contaminated regions and among recovery workers. Most of these effects have not been associated in the past with radiation exposure and are treated sceptically by many experts in radiation medicine. These claims and counter claims are a cause of widespread confusion and distress in the affected communities and beyond. They also lead to resources being used in a less than optimal manner. It is important, therefore, that the evidence be appraised comprehensively and honestly and that, as far as possible, broad agreement be reached on which health effects are known to be linked to the accident. Box 4.1: Estimating radiation risks Exposure to ionising radiation is a part of everyday life through the natural background radiation from soil, air, food, water and the sun. Typically, the annual dose is 2mSv but can be substantially more in some places, for example, where the natural radioactive gas radon is present in dwellings or where the soil contains radioactive isotopes. The study of populations exposed to different levels of natural background has not enabled the risks of such exposures to be determined directly. It has been necessary to study populations exposed to much higher doses to determine risks to health. The exposure from Chernobyl can be regarded as similar to the component of natural radiation not due to radon and thus of carrying similar risks. The principal source of risk data has come from studies on the survivors of the atomic bombings in Japan. Here the doses were generally large (deriving from the “flash” rather than any fallout) and delivered in a fraction of a second. Nearly 100,000 exposed persons were recruited into the so called Life Span Study (LSS) and from their experience and a knowledge of the doses they received, the health risks of exposure to ionising radiation can be estimated. Initially an excess of leukaemias (blood cancers) was observed in Japan occurring only a few years after the exposure. Much later (in the early 1970s) an excess of solid cancers was seen and even more recently it has been noted that certain non-cancer disease (heart disease for example) are found to be related to the dose received. No association with hereditary disease in the children of the survivors has so far been detected. From these studies, the risk of fatal cancer is estimated to be about 10% per cent per Gray and that of noncancer disease about half this value. These risks are sufficiently well determined for the WHO to classify ionizing radiation as an established carcinogen. The risk values derived from the LSS are broadly supported by many other studies on, for example, patients exposed to radiation either for diagnosis or therapy. However, the exposure to natural background radiation is not exactly comparable to that in Japan because doses are much lower and delivered over much longer times. There is an international scientific consensus that such low dose and dose-rate exposures are not without risk, but that the risk is too low to be statistically detected. Thus, a factor is employed to interpret the risk of such exposures from the LSS data. This factor, called the dose and dose rate effectiveness factor (DDREF) is generally taken to be 2 although 51 Final: 25.01.02 the validity for this value has been challenged and a value of unity may be more realistic. Hence, the risk of fatal cancer from Chernobyl type radiations is assumed to be 5%/Gy. In this case 1Gy = 1 Sv. 4.12 An important step towards creating the basis for an international consensus on the health effects of the accident was taken by the international conference “Fifteen Years After the Chernobyl Accident. Lessons Learned”, which was held in Kiev in April 2001. This conference was organised by the relevant Ministries and Committees from the three affected countries together with the International Atomic Energy Agency (IAEA), the UN Office for the Coordination of Humanitarian Affairs, the European Commission and a number of international and national expert bodies. The Report of the Conference summarises an agreed view of the health effects of the accident. While reached by an entirely different route, the findings of the Conference are broadly in line with the findings of the present UN Mission as reflected in this Report. 4.13 Much is still not known about the biological effects of radiation. Ionising radiation is the direct cause of health detriment, both cancer and non-cancer morbidity and mortality, but there is little consensus in the scientific community as to the consequences, qualitative or quantitative, of exposures such as those arising from the Chernobyl accident. All that is certain is that some effects may be delayed in their appearance for up to several decades after the exposure. More research is needed, and it will only become possible to answer many important questions with the passage of time. With that proviso, however, it remains true that existing knowledge can throw a great deal of light on which health phenomena do, and which do not, result from the Chernobyl accident. In particular it is important to identify a number of factors that have contributed to the current confusion. For example, it has often been claimed that falling life expectancy, and indeed declining population, in the affected areas largely or entirely results from the effects of radioactive fallout from the accident. 4.14 Ukraine, Belarus and Russia for example, have declining populations, with death rates exceeding birth rates by a significant factor. These phenomena have occurred throughout the Former Soviet Union and therefore cannot be a result of Chernobyl. In reality, they are a consequence of factors such as emigration and the difficult economic circumstances facing these countries, which have led to increased ill-health and caused young couples to defer having children. Demographic factors have contributed strongly to the pattern of morbidity and mortality in the affected areas. Large numbers of young people, in particular, have moved away, leaving a population dominated by older people. This in turn has radically altered factors such as the ratio of births to deaths and the pattern of disease. Several of the chief doctors of the districts visited by the Mission pointed out this factor as the key to understanding the health statistics of their areas. 4.15 A further source of confusion is the so-called screening effect. Since the Chernobyl accident, health care resources have been focused on the affected communities. Large-scale screening programmes have been introduced for the main affected areas and groups, but not for the population of the rest of the 52 Final: 25.01.02 countries concerned. The result has been that cases of cancer and other medical conditions have been identified and included in the statistics, some of which would otherwise never have come to light. Box 4.2: The physiopathological effects of radiation exposure Ionising radiation absorbed by the body’s cells is capable of breaking chemical bonds, so causing damage to the genetic material contained in the cell. This damage may lead to loss of cells and early, so called deterministic, effects in the body’s tissues, or to changed genetic properties leading to so called stochastic effects such as cancer and inherited disease. In addition, other non-cancer diseases have been observed in irradiated populations, the causes of which are not understood. The most prominent deterministic effect following the Chernobyl accident was the death of 28 highly exposed individuals from acute radiation sickness within 4 months of exposure. (In addition, up to the end of 1998 eleven others have died). Some of the more highly exposed persons involved in clean-up after the accident may suffer from cataract of the eye, another deterministic effect. Less highly exposed populations will not be at risk of deterministic effects but may suffer late onset stochastic effects such as cancer, or pass damage to future generations. There is some, still controversial, evidence of inherited genetic damage, but the health consequences that might stem from it are not clear. Considerable controversy exists over the magnitude of the stochastic effects in relation to absorbed dose, of exposure to ionising radiation, especially where low doses and low dose-rates, as apply in the circumstances of the Chernobyl accident, are concerned. All that is certain is that some effects may be delayed in their appearance for up to several decades after the exposure. Specific health issues: thyroid cancer 4.16 First reports of an excess of thyroid cancer in children were published in The International Chernobyl Project, which was coordinated by the IAEA with the participation of other UN agencies including FAO and WHO. This was initiated in 1989 at the request of the Soviet Union to address the claims of ill health arising from the accident. This report was published in 1991 and reported that no link between the health status of the population and radiation had been found. The report however did refer to the fact that local physicians had identified 20 thyroid cancer cases in the period up to the end of 1990 and concluded that “there may be a statistically detectable increase in the incidence of thyroid tumours in the future”. Given the rarity of childhood thyroid cancer, this finding in Ukraine should have been a warning signal of what was to come. 4.17 In 1992 the European Regional Office of WHO visited Minsk to investigate claims of increased childhood thyroid cancer incidence, mainly in children from the Gomel region. Although these claims were initially greeted with scepticism it is now clear that there has been a very marked rise in thyroid cancer in those who were children at the time of the accident. A recent United Nations Scientific Committee on the Effects of Atomic Radiation report (UNSCEAR 2000) acknowledges 1,800 cases of thyroid cancer in children residing in the affected area up to the end of 1998, although others claim that this is an underestimate. A conservative estimate of the number of cases of thyroid cancer occurring over the lifetimes of those exposed in childhood in the affected areas is 6 to 8,000 in the 53 Final: 25.01.02 three countries. Claims have been made of higher numbers diagnosed but these include cases diagnosed in those exposed as adults. 4.18 This increase represents a unique situation in which a single cause, at a defined time, has resulted in such a large increase in a specific cancer. Much remains to be learned about the ultimate consequences, including the final number of cases. Previous experience of the irradiation of the thyroid gland indicates that cases related to the exposure will continue to occur for at least 50 years after exposure. The principal reason why the 1,800 cases can be unequivocally attributed to radiation exposure from the accident is the rarity of the disease in children, in whom most of the cases have occurred. For example, in some settlements in the Gomel region the incidence rates in the mid 1990s were up to 200 times that associated with the “sporadic” incidence rate. These cancers are associated with exposure to the radioactive isotopes of iodine, which concentrate in the thyroid gland, although this is still contested by some. Figure 4.1: Thyroid cancer in children under 15 years of age at diagnosis. Number of cases diagnosed 100 75 Russia Belarus Ukraine 50 25 0 1986 1987 1988 1989 1990 1991 1992 1993 1994 1995 1996 1997 1998 Year of Diagnosis 4.19 In response to the situation encountered in Minsk, namely a substantial (in relative terms) increase in a rare disease, the European Regional Office of WHO set up the International Thyroid Project to assist Belarus in dealing with monitoring, diagnosis and treatment issues. This increase in childhood thyroid cancer was not uncovered as a result of screening (except insofar as the iodine deficiency problem had resulted in surveillance through annual palpation of the thyroid). Under the Project, iodine status was regarded as crucial to the further development of thyroid cancer in the population. A survey of iodine status was 54 Final: 25.01.02 commenced in Belarus and subsequently in the other two countries, as a means to develop a policy for iodine supplementation. Other projects within the International Thyroid Project included a joint three-country database for thyroid cancer, the assessment of the cost effectiveness of screening for thyroid cancer and the development of locally produced thyroid hormone test kits. The Project closed in 2000 without having completed its work. A number of other international bodies have also supported thyroid cancer related projects. In 19992000, for example, IAEA supported a project to improve the diagnosis and treatment of radiation induced thyroid cancer in children in Ukraine. 4.20 There is a continuing need to treat thyroid cancer, especially in those who were under 18 at the time of the accident, and to provide clinical follow up with thyroid hormone treatment. Belarus still relies on assistance from abroad for up to 30% of its patients. A substantial number of these patients are being treated for metastases on the lung, which have proved refractory to treatment with 131I. For all patients who have had total thyroidectomy follow-up medication is required for the remainder of their lives. Fewer thyroid cancers have occurred in the Russian Federation than in Belarus and Ukraine, and accuracy of diagnosis has been questioned in a proportion of these cases. Nevertheless an extensive screening programme is operated in the contaminated territories by mobile units from Obninsk. This includes screening of adults as well as children. The Mission heard conflicting views on the adequacy of the support offered to victims of thyroid cancer. Further investigation is needed as a basis for a strategy to ensure the long-term well being of the people concerned. In view of their needs and the history of the issue, the international community should accept a share of responsibility for ensuring that the necessary resources are available to guarantee that they continue to receive proper care. 4.21 The issue of iodine deficiency is of great importance to the health of children in general because it depresses IQ, and for those exposed to radio-iodine in particular, as it is likely to accelerate the development of latent thyroid cancer. In 1991 it was clear that the affected regions contained areas of mild to severe iodine deficiency resulting in a high prevalence of goitre. As part of the International Thyroid Project, surveys were initiated in the three countries as the basis for a policy to correct iodine deficiency through dietary supplementation. The analysis of the data from the survey needs to be completed and evaluated so that it can be used to develop a policy on iodine supplementation in the affected territories. 4.22 UNICEF has been a strong advocate in all three countries of the elimination of iodine deficiency through universal salt iodisation. The overall situation is far from satisfactory. Universal salt iodisation has proved its effectiveness over decades in many countries. In the Russian Federation UNICEF has supported the development of a communication and social mobilisation strategy to achieve and sustain it. Since most salt comes from kitchen salt rather than processed food (consumption of processed food is relatively low in these countries), UNICEF has advocated the mandatory iodisation of kitchen salt. Current regulations only 55 Final: 25.01.02 promote voluntary use of iodised salt and penetration of iodised salt remains at only 15 to 30%. 4.23 A scheme initiated by the Radiology Research Centre in Obninisk is marketing an organic iodine compound, "iodo-casein", for incorporation into bread milk and even vodka. The bread is said to be widely available but it was not clear to what extent it is being bought, especially in rural areas. However, there are drawbacks to this initiative. Multiple sourcing of iodine could lead to over iodisation, which in an iodine deficient population can result in a transient adverse health effect. Additionally the Mission was told that as part of the marketing strategy for iodocasein, salt iodisation is being discredited. The promotion of this and other iodised substances constitute in UNICEF’s view barriers to the adoption of universal salt iodisation, the most efficient and cost-effective method of eliminating iodine deficiency disease. 4.24 In Belarus the focus of attention on thyroid disease following the Chernobyl accident has meant that iodine deficiency is a well recognised public health problem. However, the extent of penetration is unclear. Although estimates vary, some suggest that up to 50% of the population consumes iodised salt, mostly the better-educated population and those in affected areas. The Mission was assured that schools and hospital canteens used iodised salt exclusively. Management at the Mosyr salt plant (where the project is supported by the European Union) reported that they were currently expanding capacity, with assistance from UNICEF, and believed that the use of iodised salt would rise rapidly over the coming year. 4.25 Until 2000-2001, the main obstacle to implementation of effective measures to eliminate iodine deficiency disease in Ukraine was the obsolete concept that iodine deficiency in this country is limited to eight “Endemic Goitre” western mountain districts. In the Chernobyl affected regions distribution of iodised salt was also limited due to fears of inducing certain thyroid disorders. In 2000 UNICEF supported a small scale iodine deficiency disease survey in four districts that were previously thought to be not “endemic for goitre”. This survey helped to promote government regulation on universal salt iodisation. Ukraine still has one of the lowest levels of iodised salt use at the household level – less than 5%. Specialised registries and screening 4.26 The traditional Soviet approach to events such as the Chernobyl accident was to place the exposed populations on special epidemiological registries and offer the registrants health privileges, including annual medical examinations and population screening for health effects. In contrast, in the West, the approach adopted is to maintain country wide disease registries as a matter of routine and carefully assess the cost effectiveness of screening of population groups exposed to specific risks. The health risks associated with the average Chernobyl exposures to radiation (exposure of children’s thyroids to radioactive iodine 56 Final: 25.01.02 excepted) are most unlikely to be mitigated significantly by annual medical examinations. 4.27 The policy of mass screening, which is followed in all three countries, needs to be thoroughly reviewed. The issue is important both in terms of the resources involved and the well-being of the populations concerned. Broad-based screening of adults is not a part of mainstream medical provision in most parts of the world and it can be argued that it may be counter productive for those concerned. While it intuitively sounds a good idea, such screening consumes scarce financial and human resources and may reinforce the idea that ill-health is the norm. By revealing slow growing cancers in older people, which would in many cases never otherwise become manifest, it can heighten anxiety, lead to unnecessary operations and distort the health statistics which provide the basis for the planning of medical services. 4.28 Backed up by proper care, however, the screening of particular at risk groups, including children, plays an important part in preventing and curing disease. During the past 15 years considerable efforts have been made by the three countries, with international assistance (for example from the EU) to strengthen existing disease registries and initiate new ones. Efforts to assess the cost effectiveness of the present screening programmes have been made by the countries as part of the International Thyroid Project. The combined use of disease registries and a cost effective screening strategy should enable scarce resources to be redirected to more urgent needs. The psychosocial dimension 4.29 Over the last fifteen years, it has become increasingly apparent that the accident has had important psychosocial effects, which, interacting with the other effects, have had a profound impact on the well-being of the communities concerned. The origins of the psychosocial effects are complex and relate not only to the accident itself and the threats that it involved to the other aspects of health, but also to the impact of the process of resettlement. Uncertainty about the health consequences has been a key factor for those involved in the clean-up operation as well as those living in the areas affected by the accident. 4.30 Research carried out in Ukraine indicates that anxiety over the effects of radiation on health is the most important psychosocial effect of the accident, that such anxiety is very widespread and shows no sign of diminishing. It also shows that it is spreading beyond the affected areas and communities into a wide section of the population. The research suggests that parents are transferring their anxiety to their children through example and excessively protective care. Some 65% of adolescents from the affected communities manifested attitudes which the researchers categorised as pessimistic, far higher than in the population at large. 4.31 Releases of toxic substances, including radioactivity, are associated with stress that manifests itself in “illness behaviour”, alterations in reproductive behaviour 57 Final: 25.01.02 and changes in lifestyle factors, such as diet and tobacco and alcohol use. Such stress responses are known to be persistent. With time, people under such chronic stress make the transition from anxiety through depression, to a state of apathy and fatalism. The combined effect of the many sources of stress is a decline in the health and well-being of the affected populations, which many will attribute to the effects of exposure to radioactivity, further fuelling fears and raising stress levels. The situation encountered by the Mission in the affected territories is the result of 15 years of an unremitting downward spiral of health and well-being (see Fig 4.2). 4.32 The system of Chernobyl related benefits has created expectations of payments and advantages and has undermined the capacity of the individuals and communities concerned to tackle their own economic and social problems. Studies carried out by the Institute of Sociology in Kiev indicate that 80% of respondents living in areas with a guaranteed right to resettlement expect “financial assistance and special medical treatment”. Among resettlers, 84% expect “special medical treatment” and 71% claim unemployment allowance. Figure 4.2: The Downward Spiral in communities affected by Chernobyl Low tax base Unemployment Inadequate health/social facilities Poor nutrition Desperation due to lack of economic opportunities Weakened, ageing and outmigrating workforce Costs of medical treatment Costs of compensation Obstacles to economic development Environment has low priority Lack of funds to reduce exposure Withdrawal of land Pressure to use Restriction on agriculture contaminated products Negative image Costs of protective measures Constraints on economic activities Chernobyl accident, resettlement, compensation and other response Radiation-induced disease Psychological impact Social disruption Release of Radioactive Material Environment not a priority Poor awareness and education Poor coping capacity HEALTH AND SOCIAL CRISIS 4.33 Exposure to radiation Alteration of traditional lifestyles Contamination of the environment and foodstuffs The Institute of Sociology report argues that the Chernobyl accident led to a wide range of psychological problems including a sense of being a victim; a sense of social exclusion; lack of initiative, a low level of adaptation to the new environment and an expectation of external support. Significantly, the state of 58 Final: 25.01.02 mind of victims was not connected to their objective living conditions. This situation has produced a culture in which ill health is the expectation for many people, including doctors, nurses and teachers; a phenomenon particularly prevalent where children are concerned. 4.34 In 1990 the WHO conducted an expert group meeting in Kiev to consider the socalled psychosocial implications of the Chernobyl accident. The expert group found five dimensions of the psychosocial effect. These are listed in Box 4.3. Of particular significance in the development of the health situation following the Chernobyl accident were the first dimension (concerning the perception of radiation as a risk to health and the provision of information relating to those risks), and the fourth dimension (concerning illness behaviour and the doctor's response). All five dimensions of the psychosocial effect were clearly evident in the affected communities, making the psychosocial effect the most pervasive underlying cause of ill health and lack of well-being. The lack of a clear consensus on the link between health effects and radiation exposure, the failure of the scientific community to predict the very visible increase in childhood thyroid cancer, and the debate that followed, played an important part in creating the current situation. 4.35 Research carried out by the Institute of Sociology in Kiev highlights some very significant aspects of the psychology of the affected individuals. The Institute carries out twice-yearly surveys of different groups, including resettlers, inhabitants of the affected areas and clean-up workers, as well as control groups. It is, therefore, able not just to give a snapshot of responses at a particular moment, but also to track changes in attitudes. This research has produced some very interesting insights, which provide an important backdrop for policy making. Box 4.3: Factors involved in the interaction of radiation health risks and the psychosocial effect. 1. the sociopsychological dimension of the perception of risk involved in radiation and the part that information policy plays 2. the sociocultural dimension of displacement (through policies of relocation due to heavy contamination) and the consequent social disruption of communities 3. the general pathogenic factor relating to physiological stress reactions to change in lifestyle, such as dietary habits and the consumption of alcohol 4. the medical sociological dimension concerning changes in illness behaviour of the population and in the diagnostic behaviour of doctors 5. the socioeconomic dimension relating to large scale effects of the Chernobyl accident such as the closure of nuclear plants and the reversion to other sources of energy as well as the economic transition following the collapse of the USSR. 59 Final: 25.01.02 4.36 The Institute found that distress was highest among resettlers who had moved away from their original homes as a result of the accident. These people considered that their lives, and the lives of their children, had been dramatically changed for the worse by the accident. The passage of time appeared to have done little to blunt their distress. They had been subjected to a series of shocks: the accident itself; the discovery of its true extent and nature with Perestroika; resettlement; the effects of the break up of the Soviet Union, and the subsequent collapse of living standards and of much of the welfare state. They had developed an overwhelming sense of helplessness and victimisation. A minority of this population, mainly young people, reported that they considered that their health was the most important thing and that they did not wish to return to their villages. However, more that half of the resettlers stated that they would return to their homes if they were allowed to, and this proportion did not appear to be declining. Those over fifty years of age found it most difficult to adapt. 4.37 Somewhat better adapted to their situation were the group of people who remained in their homes in the affected areas. Six years ago, 80% of this group said that they wanted to leave. In the latest survey, this proportion had fallen to 20%, with 80% wishing to stay in their homes. Many of those who still wanted to leave were young people who were concerned about the risks involved in raising children in a contaminated area. Psychologically the best adapted group were the so called “self-settlers” who had been evacuated and had then returned despite the restrictions. These people asserted that the threat from radiation was not as bad as the authorities claimed. They argued that they wanted to be left in peace in their homes. The Institute found that economic considerations were not necessarily the over-riding factor. Cultural arguments, such as a desire to live in the traditional home near to where ancestors were buried, could be very important, especially for older people. 4.38 These findings were broadly reflected in what the Mission saw during its visits. Many of those who were spoken to appeared to have very little confidence in their own ability to improve their situation. While some, for example, among the selfsettlers were proud of their independence, others were clearly living in circumstances of deep distress, with little belief in their own or the authorities’ ability improve their circumstances. The Mission also saw much evidence of the way in which the infrastructure of community life had broken down. Community institutions from the Soviet era, such as the local houses of culture and organisations such as the young pioneers, had ceased to function and had not been replaced by any alternative. In rural areas, state and collective farms had previously played an important part in community life. In Russia and Ukraine, these organisations had largely disappeared, although in Belarus they continue to function albeit in difficult circumstances. 4.39 School and kindergarten education in the affected areas have come under pressure as infrastructure development has slowed down, particularly in communities designated for resettlement. In some of the resettlement villages houses had been 60 Final: 25.01.02 built, but community facilities such as social centres and clinics had been left unfinished because of lack of resources. Half finished buildings such as these must add to the sense of abandonment reported by many resettlers. Rehabilitation 4.40 On the positive side, the Mission also saw several examples of good practice, which could serve as models for future initiatives. In particular in Ukraine, the Psychosocial Rehabilitation Centres, originally established with support from UNESCO, were clearly playing an important role. They had become a focus for a range of development activities, including support for new voluntary organisations. One reservation about these centres was that they often gave great stress to the issue of Chernobyl in a way which would appear to conflict with their mission of promoting rehabilitation. In some centres large and potentially frightening pictures of the accident were prominently displayed, in one case dominating the entrance hall and in another taking the form of an altar. One worker explained that these were intended to appeal to donors, but it is hard to believe that they can contribute to the healing process, particularly since many of the users of the centres were not born at the time of the accident. 4.41 Local and international voluntary efforts were also well in evidence in some of the affected communities. One group had set up an innovative youth centre in a former pioneer camp working with young people with disabilities. They had an impressive record of activities and had established links with several parallel organisations in Germany. These links were very firmly rooted in the idea of mutual respect, rather than in the concept of victims and donors. The organisers had initiated genuine international exchanges, with young people from Germany staying in the camp and young Russians returning their visits. Box 4.4: Psychosocial Rehabilitation Centres In 1991 UNESCO initiated an extensive programme (with funds of $9,000,000 donated by European countries) to address the psychological and social aspects of the accident. An integral part of this programme was the setting up of nine Psychosocial Rehabilitation Centres, three in each country. The Centres seem to have been most successful and sustainable in Ukraine where five are now functioning with support from the National Ministry for Emergencies. UNESCO phased out the programme in 1998, but the rehabilitation centres in Ukraine are now receiving assistance from UNDP. The centre in Ivankiv in Ukraine, for example, serves a community with a population of 13,000. The number of people using the centre has continued to rise since it was opened, from 6,907 people in the first six months of 1996 to 9,878 in the first six months of 2000. Almost half of the people visiting the centre are children. A survey carried out in 1999 showed that 85% of the adult population of Ivankiv considered that the Centre had either a medium or a strong impact in the community. The Centres offer a range of services which bring together trained community workers and members of the public. For example, they work with groups of children, young mothers and old people and provide a focus for a variety of local social cultural and educational activities. The centres appear to have been most successful where local leadership has taken the initiative in developing new areas of 61 Final: 25.01.02 activity to meet local needs. They appear to have been effective in easing some of the psychological effects of the accident, promoting community cohesion, encouraging voluntary activities and contributing to better education and information. Their relevance could be enhanced through linking their activities to local government and directing them more clearly towards development objectives. 4.42 Also impressive was the work of some of the town twinnings, for example, the link between Svetlagorsk in Belarus and Mendip in the UK (see Box 4.5). Supporting the activities of initiatives such as these should be a high priority for the international community. Small amounts of additional resources, in the context of respect of the autonomy of the partnerships involved, could yield benefits which would be beyond the reach of conventional donor activities. 4.43 A unique feature of the response to the Chernobyl accident has been the voluntary initiatives supporting holidays for children from the affected areas in families abroad. These have become possibly the largest and most sustained international voluntary welfare programme in human history: a total of several hundred thousand children have taken part since the accident. Some 60,000 young people a year from Belarus alone visit countries in Western Europe each year under such schemes. While there is no consensus in the international health community as to the claimed benefits in terms of “detoxification”, the visits are undoubtedly popular in the affected communities. They support the large efforts of the governments concerned to offset the disadvantages facing these young people. Box 4.5: International Voluntary Partnerships (IVPs) The Mission came across many examples of good practice involving the voluntary movement. These included initiatives by conventional non-governmental organisations (NGOs) such as the larger children’s charities. They also included projects undertaken by community based international partnerships, such as town twinnings and links between hospitals and clinics in the affected areas and similar institutions in other parts of the world. These typically had no paid staff, and were sustained entirely through the commitment of the individuals concerned. The Mission labelled these initiatives International Voluntary Partnerships (IVPs). In recent years, the Gomel Regional Economic Development Agency, with support from UNDP and the Central European Initiative, has organised conferences of IVPs from the affected Region in Belarus every two years. Some thirty town and city twinnings have taken part in these meetings. The conferences have revealed that these partnerships have provided a sustainable and cost effective basis for a wide range of different forms of mutual support and assistance, including humanitarian and technical assistance, training and educational exchanges. An outstanding example is provided by the link between Svetlagorsk in the Gomel Region and Mendip District in the UK. This link is consciously based on the principles of mutual respect and sustainable development. Since it was established in 1996, it has involved over a thousand people from Svetlagorsk taking part in training or visiting the UK in connection with a variety of health, educational and civic development projects. These have included initiatives concerning environmental management, HIV awareness, cultural exchanges and support for the development of the voluntary sector. 62 Final: 25.01.02 4.44 The main downside of the visits is that they may perpetuate inaccurate and negative stereotypes about life in the affected areas, both in the minds of the young people and in the host communities. Research carried out by the Kiev Institute of Sociology suggests that the effects of the visits are beneficial in the long run. It is crucial, however, that, while maintaining their efforts to the full, the organisers do everything possible to ensure that the visits and the associated publicity promote mutual respect and individual development. 4.45 International exchanges are only one element in holiday provision for young people from the affected areas. In Belarus, for example, all children from the more severely affected districts are entitled to two months holiday a year provided by the state. The mission visited one holiday camp run by the Ministry of Emergencies in the Gomel Region which provided several thousand holiday months a year. The camp offered health services including dental services, medical check-ups and massage. It was well equipped and gave the impression of being a happy and well-organised place for young people to stay. Role of the international community 4.46 Activities by the international community have been intertwined with the issue of health in the affected communities since soon after the accident. On the positive side, very considerable assistance has been given by a range of international bodies, both public and private. This has not only contributed to resolving health care problems and to delivering improvements in provision, but has also helped to tackle the sense of abandonment that many of those affected by the disaster have described. The UN Office for the Coordination of Humanitarian Affairs has played an important role in encouraging this assistance. International voluntary efforts have also played an important part, especially in helping to tackle the psychosocial dimension of the problem and with the provision of medical equipment and training, as has the WHO’s International Project on the Health Effects of the Chernobyl Accident (IPHECA). A very important recent initiative is the International Thyroid Tissue Bank, which can serve as a model for future research co-operation involving the three countries. 4.47 There have also been a number of significant areas where the international community has failed to have a significant impact, or has in some cases even made things worse. First, it has often given very conflicting messages on the question of the nature and extent of the health effects of the accident. Particularly damaging was the delay in acknowledging the relationship between childhood thyroid cancer and radiation by a number of international bodies in the early 1990s. Second, there has been a lack of coordination, particularly on health issues, which has led to too much attention being focused on some aspects at the expense of others. Third, it is also the case that the international community has tended to concentrate assistance on high visibility projects such as donations of high technology equipment rather than on helping to improve primary health care, which is where the greatest need lies. Fourth, the international community has 63 Final: 25.01.02 sometimes been at risk of throwing away the potential benefits of its initiatives by failing to carry through projects to completion, as appears to be the case, for example, with the International Thyroid Project. Future projects need to take account of these experiences. Section 5.0: Economic Development and Household Incomes Current economic situation 5.01 After ten years of decline, the economies of Belarus, Russia and Ukraine, including the affected territories, are now showing clear signs of recovery. Industrial companies in the Zhitomir Region of Ukraine increased their output by 13% in 2000 and the rate of growth reached 25% during the first three months of 2001. In Russia, Briansk Region has also seen a steady growth in production since 1999. In the first six months of 2001 output was 20% higher than a year before. In the Gomel Region of Belarus industrial production rose by 12% in 2000 and further growth was expected in 2001, though at a slower rate. 5.02 Unfortunately, agricultural production has grown very little in the Gomel and Briansk Regions and farms, whether private as in Russia or publicly owned as in Belarus, appear unable to play a significant role in increasing rural incomes. In Novozybkov District in Russia, six former collective farms out of seventeen are bankrupt, and another seven are unprofitable. Many farms have abandoned cultivating part of their arable land because of a lack of working capital. Yields of grain at around 1.5 tons per hectare are very poor. 5.03 In Ukraine, however, the sector is going through a process of profound reform that is beginning to bringing positive results. Growth was 5% in the Zhitomir Region of Ukraine in 2000. Some 665 former collective farms in the Region have been transformed into 713 private farming enterprises and 1,177,700 ha of land have been distributed to 288,600 people. The number of unprofitable farms decreased from 98% to 66% in 2000 and regional authorities expect this figure to fall to below 20% this year. Economic impact of the Chernobyl accident 5.04 The Chernobyl nuclear accident affected the economies of the three countries and the regions concerned in many ways and at different levels. In terms of the impact at national level, it is not possible to estimate the scale of the losses accurately. Attempts were first made to calculate the financial cost in the early 1990s, but different methods were used. The Government of the Republic of Belarus estimates that losses over the 30 years following the accident will amount to $235 billion. The Ukrainian government estimates the loss as $148 billion over the period from 1986 to 2000. 5.05 Because of difficulties relating to exchange rates during a period of rapid inflation and other factors, these figures are open to question on a number of grounds. 64 Final: 25.01.02 What is clear is that the three countries suffered considerable direct costs in the form of buildings and equipment that had to be abandoned. They also suffered very large and on-going costs in terms of the recovery programme, together with opportunity costs resulting from the diversion of resources away from productive activities. In the case of Belarus and Ukraine, losses included the balance of payments cost of purchasing energy which otherwise would have been generated locally. Ukraine ultimately lost all of the output of the Chernobyl complex, while Belarus cancelled its nuclear generation programme as a result of the accident. The categories of losses suffered by the three countries are listed in Box 5.1. Box 5.1: Losses resulting from the Chernobyl accident * * * * Direct damage caused by the accident Expenditures related to a) Actions to mitigate the consequences in the exclusion zone b) Social protection and health care to affected population c) Research on environment, health and production of clean food d) Radiation monitoring of the environment e) Radioecological improvement of settlements and disposal of radioactive waste f) Resettlement of people and improvement of their living conditions. Indirect losses relating to the opportunity cost of removing agricultural land and forests from use and the closure of agricultural and industrial facilities. Opportunity costs, including the additional costs of energy resulting from the damage and eventual closure of the Chernobyl complex and the cancellation of Belarus’s nuclear power generation programme. 5.06 The 1990s was a period of great political, social and economic turmoil in the three countries. The collapse of the Soviet Union in 1991, the economic chaos of 1991 and 1992, social tensions in Russia and Ukraine, the growing economic crisis and hyper-inflation all exacerbated the effects of the Chernobyl accident in the countries concerned. One indication of the scale of the economic burden resulting from the accident is given by the cost of the recovery programmes to the national budgets. The statistics for Belarus are shown in Table 5.1. 5.07 In Belarus and the Ukraine these expenses have been met from a special Chernobyl emergency tax. In Belarus, the emergency Chernobyl tax was introduced in 1992. In 1994 it stood at a rate of 18% of wages for all nonagricultural firms. Even at this point receipts only accounted for 65 % of planned expenditure. The tax was constantly criticized by businesses for making Belarusian products uncompetitive. It was later reduced to 12 % and is currently levied at a rate of 5 %. In Ukraine the Chernobyl tax also faced strong opposition and was progressively reduced. In Russia, resources were mostly provided by assigning funds within the national and regional budgets. Environmental contamination as an economic constraint 65 Final: 25.01.02 5.08 The consequences of the Chernobyl accident have been addressed through a number of policies, most of which have had significant economic and social impacts. Restrictions on economic activities on contaminated areas, particularly the loss of agricultural land and timber production and restrictions on access were an important factor. Restrictions on agricultural production affected territories with contamination exceeding 40 Ci/km2 where all agricultural production was prohibited. Part of the abandoned land, however, was forested with a view to reducing migration of radio-nuclides and supplying timber in the distant future. Extraction of timber for commercial purposes was prohibited from forests on territories where contamination by 137Cs exceeds 15 Ci/km2. Due to the level of contamination and the high cost of remedial measures, some agricultural land and forests have been removed from service for the next 60 to 80 years. The number of small and medium sized enterprises (SMEs) per 10,000 inhabitants is markedly lower in the affected regions than nationally: in Zhitomir Region are 36 SMEs per 10,000 compared to 44 in Ukraine as a whole, while in Gomel Region are 19,compared to 32 per 10,000 in Belarus as a whole. Table 5.1: Chernobyl expenses as share of national budget in Belarus 1992 to 2000 Year % of national budget 1992 1993 1994 1995 1996 1997 1998 1999 2000 2001 19.9 16.1 10.1 11.5 10.9 9.9 8.9 8.1 6.4 5.3 5.09 As a result of compulsory and voluntary resettlement, 282 rural settlements were closed in Belarus alone, together with their cultural centres, libraries, schools, outpatient health care facilities and productive infrastructure. The list of closed facilities includes production units, houses, roads, heating, electricity and water supply and sewage networks. Table 5.2 indicates losses in the three countries in terms of closed agricultural and industrial enterprises and other economic resources. 5.10 Companies producing food were among the most disadvantaged. The Chernobyl stigma became a serious obstacle to sales. A Russian milk processing company told the Mission, for instance, that even if their products are in compliance with health standards, distributors are reluctant to buy them. More than one third of industrial output in the Gomel, Zhitomir and Briansk Regions is accounted for by food processing companies. Efforts will have to be made to overcome the fear of the Chernobyl label. Private investment can play an important part in this. There 66 Final: 25.01.02 are already examples proving that it is possible. For example, the Mission was told that after being taken over by private investors from Kiev, the Ivankiv milk processing factory stepped up its marketing effort and doubled production in less than eight months. Table 5.2: Agricultural land, forest, enterprises and resources removed from service Belarus Russia Ukraine Total Agricultural land (hectaires) 264,000 17,100 512,000 784,320 Forest (hectaires) 200,000 2,200 492,000 694,200 Agricultural and forest enterprises 54 8 20 82 Factories, transport and service enterprises 9 0 13 22 Raw material deposits 22 0 0 22 Demographic impact 5.11 Since the Chernobyl accident, more than 348,000 people have been relocated away from the most severely contaminated areas, some were evacuated immediately after the accident, others were resettled several years later. This completely distorted the demographic pyramid in the most affected regions and districts. For example, in Ivankiv District, immediately south of the exclusion zone, 16,500, or 43%, of the 38,000 inhabitants are now pensioners. Table 5.3 indicates the scale of evacuation and resettlement actions undertaken by the governments. 5.12 In Belarus, the worst affected districts of the Gomel and Mogilov Regions are among the worst in Belarus in terms of demographic indicators. This will severely handicap economic recovery in future. Tables 5.4a and 5.4b show that the population of the Gomel Region dropped by 8% between 1986 and 2000, while in Khoiniki District it fell by 43%. The rural population declined much more sharply than the urban population as a whole: by 27% in rural areas of the Gomel Region compared with a fall in the urban population of 3%. The birth rate also dropped sharply, almost halving in the Gomel Region between 1986 and 2000. Khoiniki District showed a sharp fall in the birth rate between 1985 and 1987, despite the fact that mass relocation was only launched in 1990/91. Table 5. 3: Evacuated and resettled people Evacuated people (1986/1990) Resettled people (1991 to 2000) Total Expecting resettlement 5.13 Belarus 24,000 111,000 135,000 7,000 Russia 3,400 49,000 52,400 Ukraine 91,000 72,000 163,000 4,600 Total 118,400 231,000 350,400 11,600 The lack of young people has had serious implications for the local economies. It has also had psychological effects. For example, the fact that there were many more deaths than births encouraged the belief that the areas concerned were dangerous places to live. District chief executives interviewed during the Mission 67 Final: 25.01.02 complained that schools, hospitals, agricultural co-operatives, utility companies and many other organisations were short of qualified specialists. In Nvozybkov, in Russia, the Mission was told that the district hospital was 40 % understaffed in terms of doctors. An entrepreneur in Ivankiv complained that he could not find wood processing engineers, even for comparatively high wages, despite widespread unemployment. The decline in the number of young, skilful and enthusiastic school teachers follows a trend in other rural areas but is more serious here because of fear of radiation and the lack of young people and social facilities in the affected areas. Table 5.4a Demographic indexes in Gomel Region (Belarus) in 1986 and 2000 1986 Inhabitants: 1,677,500 Including: - Rural population 653,600 - Town population 1,023,900 Birth rate 17.2 Mortality 9.2 Natural population growth + 8.0 Life expectancy, years 72.6 2000 1,535,000 475,200 1,059,800 9.7 14.8 - 5.1 67.6 Table 5.4b Demographic indexes Khoiniki District (Gomel Region) in 1986 and 1999 1986 1999* Inhabitants: 45,850 25,900 Including: - Rural population 29,450 11,100 - Town population 16,400 14,800 Birth rate 15.2 12.9 Mortality 11.8 19.4 Natural population growth + 3.4 - 6.5 Life expectancy 68.3 64.0 * latest available data 5.14 While many of those who remained are poorly skilled, lack of resources has meant that little has been done to improve their capacity. One exception is Slavutych, the town built to house the workers from the Chernobyl complex after the accident. A university in Chernigiv has established subsidiary departments here because standards of education are high and more than half of the population is young. Employment in the power plant complex will taper off over many years as decommissioning continues. This process will also generate new opportunities, for example in construction. However, retraining will be needed if local people are to take advantage. Recovery measures 68 Final: 25.01.02 5.15 Concerned with the growing social and economic disparities between contaminated and clean territories, governments started exploring new measures in the mid-1990s that would reduce the burden on their national budgets. Promoting inward investment into large formerly state owned companies became a priority. However, little progress was made with this policy, in part because of misinformation relating to the effects of the Chernobyl accident. Mass privatisation carried out by the governments of Russian Federation and Ukraine in the 1990s has not brought significant investment to the affected areas. In Belarus, there has been very little privatisation and only minimal inward investment. 5.16 To promote investment in affected areas, the Ukrainian government has established a special regime for nine districts and one city in Zhitomir Region covering 16,000 km2. In Belarus, special economic zones were implemented, including one in Gomel. Recently discussion has begun on promoting the rehabilitation of the six most blighted districts. These measures focus primarily on promoting investment in industries which are located in district centres rather than in rural communities. In Ukraine the 16 projects that have started are expected to bring investment of $25 million, saving 495 jobs and creating 1,332 new ones. In general, however, the governments have so far failed to attract significant amounts of foreign or national investment for the economic regeneration of the affected areas. 5.17 If an appropriate economic environment could be created, demands on the state budgets could be considerably reduced. However, until recently economic development of the affected districts has not been a high priority in Russia or Ukraine, where they only represent a small proportion of capacity in terms of industrial and agricultural output. Investment in industrial companies, which are mainly in the towns, would create new jobs and help to draw in labour from rural communities where unemployment and under-employment are endemic. Most of the jobs would go to young people as the majority of the rural population are older and likely to be unwilling to move, even within their own districts. A study by the Ukrainian Institute of Sociology indicates that older people in rural areas have a low capacity to adapt to new social and economic circumstances. Unemployment 5.18 Official statistics indicate unemployment of between 2 and 3% across the affected regions of Belarus, Russia and Ukraine, which is not higher that in other similar areas. Interviews during the Mission suggest a higher level of unemployment in areas where relocated people are concentrated than in contaminated districts, and widespread hidden unemployment in rural communities. Thus, Brusiliv District in Ukraine, which is not contaminated and has accommodated large numbers of resettlers, has 18,100 inhabitants and an active labour force of 7,600. In the District, 1,175 people are registered in the local job centre, representing an unemployment rate of 15%. A similar situation applies in other districts with large resettler populations in Russia and Belarus. 69 Final: 25.01.02 5.19 Lack of data makes it difficult to assess hidden unemployment in former collective farms. However, evidence from other parts of the Former Soviet Union and Eastern Europe suggest that agricultural reform will lead to a halving of employment, leaving one worker per 150 hectares of agricultural land instead of one worker per 25 to 40 hectares as at present. In the case of small rural districts like Narodichi or Khoiniki such a development could theoretically lead to up to 40% of the labour force becoming unemployed. Impact on the rural economy 5.20 The agricultural sector has been the area of the economy worst hit by the effects of the accident. Imposing radiological controls has closed the markets for foodstuffs and other products from the affected areas. This problem has been aggravated by the Chernobyl stigma, which has caused better educated urban consumers to reject products from these areas. As a result, revenues from agricultural activities have fallen, certain types of production have declined, and some facilities have closed altogether. In Belarus, where radioactive fallout removed some of the best arable land, the impact on agriculture has affected the whole economy. However, although the government has promoted the idea of the economic rehabilitation of contaminated territories, lack of understanding of how to conduct an active economic regeneration policy has meant that little has been done to develop an appropriate strategy. 5.21 The impact of the Chernobyl accident on many rural households in Belarus, Russia and Ukraine was catastrophic. In the first weeks many were evacuated with only their personal belongings. A few months later they were allowed to collect their property, but many of them found their houses plundered. Later when the process of resettlement started in a more organized way, families were allowed to take their property with them. They were also given a choice of where to settle. Even though they were compensated for their losses and were offered free houses, 75% of resettlers still complain that their “wishes were not taken into consideration” according to a survey by the Ukrainian Institute of Sociology. It appears that “the more time has passed since the Chernobyl disaster, the more people have become discontented with the consequences of relocation and the way it was carried out” (Prilipko, 2000). Resettlement not only affected the lives of the resettlers, but also in many cases of the residents of the communities into which they were moved. Tensions between new and old residents of resettlement villages was one of the reasons given to the Mission to explain why so many resettlers wanted to return to their original homes. 5.22 Those who decided to stay in contaminated areas, or were waiting for relocation, were often forbidden to keep cows because of the risk posed by contaminated milk. This was the case until recently in the eastern districts of the Briansk Region. The ban not only restricted their diets, but deprived them of income, led to them losing their livestock breeding skills and resulted in a decline in the productivity of their plots because they no longer had manure to serve as 70 Final: 25.01.02 fertilizer. The economic crisis of the 1990s made the financial situation of rural families extremely precarious. Heavily dependent on collective farms, they lost income and social and economic benefits. Average wages are now $20 per month and in many cases workers have not been paid in cash for several years. Instead they are paid with products such as straw and hay or with services such as ploughing and harvesting. National statistics show that farm workers are the poorest paid category in the affected countries: 87% of families in the rural Khoiniky District classified themselves as poor. 5.23 Historically rural households were involved in one main activity - growing agricultural products; but on two levels. Householders were employed in collective farms where they received benefits and wages, which constituted their main source of money income. They also produced food on small plots of land around their houses which they consumed, sent to relatives in the towns, or sold in the market. The household activity was never considered a major source of income. However, householders depended heavily on home production for their food. 5.24 Domestic animals, and specifically cows, are the basis of the whole household economy. There is a country saying in these areas that if a family has a cow, the children will never be hungry. A typical rural household has a small plot of land adjacent to the house and sometimes an additional plot of up to a hectare outside the village, together with a cow and a calf, and sometimes a pig and poultry. Nowadays, some families also keep horses for heavy work in the fields or, if they are better off, an old tractor. In the Soviet period the collective farms provided veterinarian services free of charge, and also helped families with ploughing and harvesting, but these benefits have now largely disappeared. In some resettlement villages the influx of new residents meant that there was insufficient land available to give every household an adequate plot on which to grow food. The Mission was told that this was having a serious effect on the ability of families to support themselves in some of the villages visited. Rural initiatives 5.25 Since the beginning of the 1990s, the authorities in Ukraine have encouraged households to support themselves by easing restrictions on individual plot size and on the number of domestic animals. These measures have led to an increase in cultivated land and in the number of farm animals. They have helped to increase output of some important food products. Households supply a considerable quantity of food to local markets in Zhitomir Region. They possess a quarter of agricultural land and produce more than 90% of potatoes and vegetables and 19% of grain. In Ovruch District, rural households account for 32% of cattle, but their share of production of meat and milk is two times higher than that of former collective farms. This indicates that in conditions of extensive agriculture, households are more efficient than collective farms. 71 Final: 25.01.02 5.26 This increase of agricultural production by households has also occurred in Belarus and the Russian Federation. In Khoiniki District in Belarus, the number of cattle possessed by families almost doubled in the last seven years. In most affected communities in Gomel Region more than three out of four households have at least one cow. In response to external economic, social and environmental pressures families have developed their own techniques for survival by setting up small scale agricultural production and exploiting local resources. 5.27 Once engaged in this process they start to act as family micro-businesses and look for ways to improve efficiency. Spontaneously, entire villages in Ukraine and Belarus have become specialised in one or two specific products. In Novi Ladizhichi (Ivankiv District, Ukraine) many inhabitants are involved in raising and supplying piglets for the local market, because pastures and agricultural land are scarce. In resettlement villages in Brusiliv District in Ukraine, family involvement in producing milk is rapidly expanding. This is due to the existence of large free pastures and meadows around the settlements. To create a market for their milk, households in Ladizhichi, a small village close to Ivankiv, invested in a dairy which enabled them to increase the number of cows from 135 in January 2001 to 143 in July. Alshani (Brest Region, Belarus) and the adjacent villages are also of great interest. In conditions of land shortage, the inhabitants have developed family micro-businesses growing spring vegetables and autumn flowers in small greenhouses on their land plots. These products are supplied to markets in Minsk, St Petersburg, Brest and Gomel. This activity now supports over a thousand families in an area where contamination is at the level of 7 ci/kmsq. 5.28 Outside support can play a part in initiating such developments. One example of how this could be done is provided by a project in a village in the Vetka District where the Gomel Regional Economic Development Agency is helping villagers to develop a business raising geese for the market with support from the UK Department for International Development (DFID). The geese feed themselves in the water meadows through the summer and can be sold in the autumn for $6 per head, yielding valuable cash income for the householders. The Gomel based Radiological Institute is providing advice on how to ensure that the geese are free from radioactive contamination when brought to market. If successful, this initiative should help a cluster of village households both to raise their money incomes and acquire new animal raising and business skills. Role of the international community 5.29 Economic development is probably the area where assistance from the international community has so far been least successful. As far as business development projects are concerned, investors and the main donors have concentrated on the capital cities and other areas with good growth prospects and have largely by-passed the affected Regions. In addition, because of difficult 72 Final: 25.01.02 political relations between Belarus and major donor countries, normal programmes of development cooperation have been limited, particularly those involving assistance to government activities. This has curtailed economic development projects in the affected areas, as in other parts of the country. 5.30 Such projects as have been undertaken in the affected areas of the three countries have often produced only disappointing results, for a number of very specific reasons. First and most obvious, they have often failed to reflect the profound differences between the pattern of economic life inherited from the Soviet Union and that which pertains in Western market economies. The belief that rapid privatisation would rapidly lead to the early emergence of a new class of market oriented business people led to projects that were not properly rooted in the local economic and administrative fabric. 5.31 A second problem was that for reasons relating to budget and project development cycles, donors tended to work to time scales that were far too short in terms of what they were trying to achieve. For similar reasons many pilot projects have been carried out, often at a high cost in terms of the benefits, but these have rarely been rolled out into substantive programmes. A third problem was that projects tended to be designed by administrators and consultants who knew a lot about macro-economics and western business practices, but little or nothing about local and regional economic and community development, even in their own countries. As a result, business support initatives were sometimes set targets in terms of achieving self-sufficiency which would have been quite unrealistic even in Europe or North America, let alone in the far more difficult circumstances of the Former Soviet Union. This has led to frustration on the donor side and disappointment and cynicism on the side of the intended beneficiaries. Box 5.2: International experience in local economic development To be effective, economic development policies need to be able to act at a number of different levels: national, regional and local. They also need to be able to mobilise resources on a substantial scale. While the response in the affected areas needs to be tuned to the particular local conditions, experience in other parts of the world which have faced economic collapse can provide useful insights into how recovery can be promoted in the affected areas. In essence the approach needs to build on a realistic assessment of local strengths and to foster the development of a local leadership spanning local government and the enterprise sector, which is committed to bringing about the economic development of the area. Effective support for business start ups and for small and medium size firms is crucial to this process. Experience in various parts of Europe suggests that an institutional framework including, for example, a network of local economic development agencies can be useful in promoting collaboration between the enterprise sector, public administration and potential donors. Such agencies can also serve as a local source of expertise in business development. 5.32 On the other hand, there have been some areas of real success among initiatives supported by the international community. Projects supported by a number of donors, including the European Union and the Central European Initiative, 73 Final: 25.01.02 offering training and mentoring for specialists and business leaders, have helped to break down barriers and provide new ideas for those taking part. Fostering international contacts is particularly important as far as the Chernobyl affected areas are concerned because of isolation resulting from fear of radiation. While several institution-building initiatives have failed completely, others have taken root. Examples of these are the economic development agencies based in Gomel (initiated on the basis of a study funded by UNIDO and supported by the EU and DFID) and in Slavutich (supported by the EU and USAID). These provide locally rooted expertise and a structure for the promotion of economic development on the basis of partnership between local government and the enterprise sector. The EU ETHOS project in the Brest Region of Belarus has explored environmentally appropriate community and economic development. IAEA and FAO have supported a large-scale project to develop rapeseed production in the Gomel and Mogilov Regions of Belarus. The project has demonstrated that good quality radio-nuclide free edible oil can be produced on contaminated land, creating an important potential source of income for farmers in the area. 5.33 The experience of the last fifteen years shows that a policy of propping up large enterprises that lost their markets through the break-up of the Soviet Union cannot provide a solution to the problems of the affected areas. Nor is simply privatizing state companies an adequate response. The new approaches that the governments of the three countries are beginning to explore, involving incentives for investors, are a step in the right direction. But these policies need to be developed and refined. 5.34 The areas and communities blighted by the Chernobyl accident need massive resources in the form of investment if they are to break out of their present state of poverty and dependency. Neither governments nor the international community can provide resources on the scale required. Future recovery of the affected areas will depend on inward investment and on indigenous small and medium sized businesses with the skills to identify and exploit local comparative advantages and progressively integrate their activities into wider national and international markets. The analysis and recommendations in Part I point to some of the ways that governments and the international community can help to promote this process. 74 Final: 25.01.02 Annex 1: References 1. European Communities and others. 1998. Atlas of Caesium Deposition on Europe after the Chernobyl Accident (on a CD-ROM). Luxembourg: Office for Official Publications of the European Communities. 2. Germenchuk, M. 2001. Radioecological Situation on the Territory of the Republic of Belarus after the Chernobyl NPP Disaster. Minsk: Special report to the UN Chernobyl Mission. 3. Goskomchernobyl, State Committee of the Republic of Belarus on the Consequences of the Disaster at the Chernobyl NPP. 2001. 15 Years after the Chernobyl Disaster: Consequences in the Republic of Belarus and Overcoming Them. Minsk: Trioleta. 4. Ministry of Education, Republic of Belarus. 2001. State of the Educational Systems on the Regions Affected by the Chernobyl Disaster. Minsk. 5. Russian Federation. 1992. The Law on the Social Protection of Population Affected by the Consequences of the Chernobyl Accident. Moscow. 6. Stepanenko, V. 2001. Reference Materials for the UN Chernobyl Mission. Obninsk. 7. Ukraine. 2001. Fifteen Years of the Chernobyl Disaster: the Experience of Overcoming: the National Report of Ukraine. Kyiv: Chernobyl Radioecological Center of the Ministry of Emergencies of Ukraine. 8. UNDP. 2001. Evaluation and Forecast of Water Quality in Districts Affected by the Chernobyl Accident (Bryansk Region). Final Project Report. Project RUS/99/004. Moscow. 9. UNSCEAR. 2000. Medical Effects of the Accident at the Chernobyl Power Plant. 10. Vakulovsky, S. 2001. Brief Information on the Radioactive Contamination of the Russian Federation as a Result of the Chernobyl NPP Accident 26.04.86. Moscow: Special report produced for the UN Chernobyl Mission. 75 Final: 25.01.02 Annex 2: Mission Team Dr Aleg Cherp Professor Dr Angelina Nyagu Fedor Fleshtor International Expert, Ecology. Assistant Professor, Central European University, Budapest: [email protected] National Expert, Ukraine, Health. President of the Association “Physicians of Chernobyl”. Editor-in-Chief: International Journal of Radiation Medecine: [email protected] National Expert, Belarus, Economy. Director, Gomel Regional Economic Development Agency: [email protected] Dr Keith Baverstock Dr Marina Khotouleva Patrick Gray (Team Leader) International Expert, Health. Regional Adviser, Environmental Radiation and Public Health, European Regional Office, WHO e-mail: [email protected] National Expert, Russia, Ecology; Director, Ecoline, Moscow: [email protected] International Expert, Economy; Director, Oxford Research Ltd: [email protected] The following specialists prepared commissioned papers for the Mission: Dr H G Germenchuk Dr Larissa Shevtchuk Dr Sergey Vakulovsky Dr Valery Stepanenko Dr Irina Abalkina Vasyl Kovalchuk Dr Valentina Prylpko Dr Yury Sayenko Mr Mykhailo Borycyuk Deputy Head, Centre for Radiation Control and Monitoring of the State Committee on Hydrometrology (Belarus) Health Specialist, Chernobyl Committee (Belarus) Deputy Director, Institute of Experimental Meteorology, NPO Typhoon (Russian Federation) Head of Medical and Ecological Dosimetry Laboratory, Russian Academy of Sciences (Russian Federation) Senior Research Fellow, Nuclear Safety Institute, Russian Academy of Science (Russian Federation) Head of Chornobyl Department, Ministry of Emergencies (Ukraine) Head of Sociological Laboratory, Scientific Centre for Radiation Medecine (Ukraine) Deputy Director, Institute of Sciology, Kiev (Ukraine) Head of Secretariat, Verhovna Rada Ecological Committee (Ukraine) The report was drafted by Patrick Gray, drawing on sector reports prepared by the sector specialists. Copies of these can be obtained from Dr A Cherp - Ecology; Dr K Baverstock - Health; Mr F Fleshtor – Economy (e-mail addresses above), or from Neil Buhne, the UN Resident Representative in Minsk ([email protected]). 76


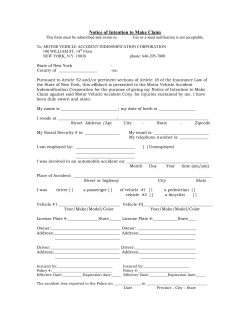









© Copyright 2026