
Student Safety
Student Safety n Safe Environment – Protection of Students n Safe Environment – Emergency Procedures n Physical Restraint of Students ÿ Documentation of Physical Restraint (ECP-S31) ÿ Significant Incident Report (ECP-S32) n Use of Protective and Restraint Devices ÿ Documentation for Use of a Protective Device (ECP-S42) Durham Public Schools Programs for Exceptional Children SAFE ENVIRONMENT – PROTECTION OF STUDENTS 1. Students in Exceptional Children’s Programs are often vulnerable due to physical, emotional and/or cognitive limitations. Therefore, ECP staff is obligated to provide a safe environment for these students. 2. Each student has a right to be free from abuse, neglect, and exploitation. 3. Staff shall not abuse a student by intentionally inflicting any emotional or physical harm. 4. Staff shall provide sufficient supervision to avoid the infliction of any emotional or physical harm by other adults or students. 5. Staff shall not knowingly divulge confidential information about a student, or allow other staff to do so. Staff shall not borrow or accept money or gifts of substantial value from a student or his/her family, or allow other staff or students to do so. 6. In emergency situations only the minimum degree of force necessary, and no more, shall be used to re-establish a safe environment (see physical restraint procedure). 7. A Significant Incident Report shall be used to document any situation in which a student was subjected to abuse, neglect, exploitation, or potential harm, or was put in a situation of high risk for such to occur. For situations involving a student put at high risk, the report shall be delivered to the building administrator by the end of the school day. In situations where abuse, neglect, or exploitation actually occurred, the report should be delivered to the building administrator as soon as is practical but no later than the end of the school day. Both the teacher and building administrator should keep a copy of this report on file. The building administrator should forward a copy of this report within three days to the Exceptional Children’s office for review by the school’s ECP Coordinator. [The DPS district-wide Student Accident Report (RC 28-97) and/or NCIC Form 19 (for employee injury) must also be filed when otherwise required under Board Policy or Administrative Procedures.] Related Procedures: “Safe Environment – Emergency Procedure” “Physical Restraint of Students” Related Forms: Documentation of Physical Restraint (ECP-S31) Significant Incident Report (ECP-S32) 11-1 Durham Public Schools Programs for Exceptional Children SAFE ENVIRONMENT – EMERGENCY PROCEDURES 1. If a student in the Exceptional Children’s Programs becomes violent or aggressive, it is the responsibility of teachers in these situations to provide for both the safety of the student who is aggressive as well as the safety of the rest of the students in the classroom. 2. If emergency procedures are included in the student’s Behavior Intervention Plan, these procedures should be followed to the maximum extent possible under the circumstances. 3. If emergency procedures are not included in the student’s Behavior Intervention Plan, the following procedures should be followed: A. The other students in the room should be moved to another location under the supervision of an adult whenever possible. B. If the student with the behavioral emergency can be physically restrained safely, the teacher or assistant should follow the procedure for physical restraint (see “Physical Restraint of Students”). C. If the student cannot be physically restrained safely (after the other students have been moved) an administrator should be summoned for assistance. D. If necessary to restore a safe environment, the administrator may request assistance from the School Resource Office (SRO) to remove the student from the setting. C. In emergency situations only the minimum degree of force necessary, and no more, shall be used to re-establish a safe environment (see “Physical Restraint of Students”). D. In any situation where physical restraint was used or the SRO has physically intervened with a student, the school’s EC Coordinator should be notified by the building administrator and a Documentation of Physical Restraint form (ECP-S31) should be completed by the staff members involved in the incident. Related Procedures: “Safe Environment – Protection of Students” “Physical Restraint of Students” Related Forms: Documentation of Physical Restraint (ECP-S31) Significant Incident Report (ECP-S32) 11-2 Durham Public Schools Programs for Exceptional Children USE OF PHYSICAL RESTRAINT 1. When a student is in imminent danger of causing injury to him/herself or another person, or when the student is causing substantial property damage, staff must take immediate action to re-establish a safe environment. 2. DPS authorized intervention techniques for physical restraint include PIC (Preventive Intervention Course) and C.P.I (Crisis Prevention Institute - Non-Violent Crisis Intervention). 3. If no trained and currently PIC- or CPI-certified staff members are present, the building administrator should be notified before any student is physically restrained unless there is an immediate threat of injury. Non-trained staff members may physically restrain a student only under genuine emergency circumstances and only until such time as a true emergency no longer exists. They should immediately defer to and follow the directions of a trained staff member should one arrive to assist. 4. If staff are present who have been trained in PIC or CPI, they may use these techniques to re-establish a safe environment. Only the minimal amount of physical control and/or the least intrusive technique that is sufficient to re-establish a safe environment shall be used. Only staff who have been trained and who have current certification may use PIC or CPI techniques to physically remove a student to another location. 5. When physical restraint is used two staff people should be present. If only one person is available at the time of an emergency, another person should be summoned immediately. 6. After the use of any physical intervention technique, a Physical Intervention Report shall be completed and submitted to the building administrator before the end of the school day. If the physical intervention lasted more than fifteen minutes, resulted in any injury to the student, or was conducted by a staff member not trained in physical restraint techniques, the documentation of physical restraint form (ECP-S31) should be turned in to the building administrator as soon as possible after the incident, but no later than the end of the school day. (It is not necessary to also complete the “Significant Incident Report). A copy of this report should be kept on file by both the teacher and the building administrator. The building administrator should forward a copy within three days to the Exceptional Children’s office for review by the PIC/CPI trainers. 7. The use of restraint as punishment, the use of restraint in non-emergency situations, and the intentional infliction of pain are always prohibited under any circumstances, as is the use of corporal punishment (see DPS Board Policy 4310). Related Procedures: “Safe Environment – Emergency Procedures” “Safe Environment – Protection of Students” Related Forms: Documentation of Physical Restraint (ECP-S31) Significant Incident Report (ECP-S32) 11-3 DURHAM PUBLIC SCHOOLS Exceptional Children’s Program DOCUMENTATION OF PHYSICAL RESTRAINT Student ____________________________________________ Teacher _____________________________________________ Date of incident _________________ Type of classroom _______________ Location of incident ____________________________________________________________________ Time restraint began ________________________ Time restraint ended ______________________ Staff involved in restraint ________________________________________________________________ Staff witnessing restraint ________________________________________________________________ Which staff were trained in PIC? _________________________________________________________ Which staff were trained in CPI? _________________________________________________________ Were authorized techniques used? Yes ______ No _______ If no, describe how the student was physically restrained. _____________________________________________________________________________________ _____________________________________________________________________________________ _____________________________________________________________________________________ Give a brief description of the circumstances leading up to this incident. _____________________________________________________________________________________ _____________________________________________________________________________________ _____________________________________________________________________________________ What specific behavior necessitated the use of physical restraint? _____________________________________________________________________________________ _____________________________________________________________________________________ _____________________________________________________________________________________ Briefly describe the behavior of the student during the restraint. _____________________________________________________________________________________ _____________________________________________________________________________________ _____________________________________________________________________________________ ECP-S31 Rev. 8/01 p.1 of 2 Name: Date: DOCUMENTATION OF PHYSICAL RESTRAINT (Continued) Briefly describe the student's behavior after the restraint. _____________________________________________________________________________________ _____________________________________________________________________________________ _____________________________________________________________________________________ After the restraint, what interventions or other types of resolutions were used? _____________________________________________________________________________________ _____________________________________________________________________________________ _____________________________________________________________________________________ After the restraint, did staff discuss ways to reduce identified behavior? Explain. _____________________________________________________________________________________ _____________________________________________________________________________________ _____________________________________________________________________________________ Signature of staff members involved in restraint: _______________________________________ _______________________________________ _______________________________________ Signature of staff members witnessing restraint: _______________________________________ _______________________________________ _______________________________________ ________________________________________ Signature of building administrator: ________________ Date Building administrator must forward copy of this form to EC Office at Fuller Building. Reviewed by PIC or CPI instructor __________________________________________ Date_________ c: ECP-31 Rev. 8/01 Confidential File p. 2 of 2 DURHAM PUBLIC SCHOOLS Exceptional Children’s Program SIGNIFICANT INCIDENT REPORT This form should be used to document any event that is out of the ordinary and requires a unique response by staff to ensure safety and security or to prevent the abuse, neglect, or exploitation of a student, e.g. runaways, student injury, situations of physical danger, etc. Name of Student ______________________________________________________________________ Name of Staff ________________________________________________________________________ Date ____________ Time ____________ School ______________________________________ Description of Significant Incident: _____________________________________________________________________________________ _____________________________________________________________________________________ _____________________________________________________________________________________ _____________________________________________________________________________________ _____________________________________________________________________________________ _____________________________________________________________________________________ _____________________________________________________________________________________ Staff Response: _____________________________________________________________________________________ _____________________________________________________________________________________ _____________________________________________________________________________________ _____________________________________________________________________________________ _____________________________________________________________________________________ _____________________________________________________________________________________ _____________________________________________________________________________________ _____________________________________ Signature of person completing report / Date _______________________________________ Signature of Building Administrator / Date Completed form must be forwarded to the EC office within three days of the incident. ____________________________________ Signature of EC Coordinator / Date received c: ECP-32 Rev. 8/01 Student confidential folder Durham Public Schools Programs for Exceptional Children USE OF PROTECTIVE AND RESTRAINT DEVICES Definitions Protective Device: A protective device is an intervention that is used to promote proper positioning and safety to assist in providing the student with a free appropriate public education. Protective devices may consist of physical or occupational therapy equipment or other tools that have been agreed upon by the IEP Team (including the parent), to be used under specified circumstances. Restraint: A restraint is any intervention, agreed upon by the IEP Team (including the parent) that is used to restrict the student’s movement or normal access to his/her own body, to be used under specified circumstances. A restraint is used to prevent the student from causing injury to self or others, or to the classroom environment, and may consist of equipment or other tools. Physical restraint techniques used by school personnel, such as NCI, PIC or CPI, are not addressed here. Refer to the policy entitled “Use of Physical Restraint” in this section for more information on the use of these techniques. Use of Protective and Restraint Devices The use of protective devices should be limited to situations in which the device is needed for positioning and/or safety. The Physical Therapist and/or Occupational Therapist should be consulted when there appears to be a need for a protective device. In some cases, rather than a true need for positioning support or safety, there is very likely a behavioral issue that needs to be addressed in the IEP, or an issue of lack of classroom support and personnel/supervision. Positioning equipment should not be used to alleviate behavior problems. Instead, behavior problems should be addressed through the IEP and/or Behavior Intervention Plan. If the behavior problem is anticipated to require the use of a restraint, the circumstances under which the restraint may be used should be discussed and documented by the IEP team. Use of PT and OT Equipment 1. PT/OT equipment is specially designed to address positioning and/or supportive seating, standing and mobility issues and, accordingly, is frequently used as a protective device. 2. PT/OT equipment is NOT designed to restrain students and should NOT be used for that purpose. 3. Members of the Physical and Occupational Therapy staff are the only individuals who are qualified to make decisions about the appropriate use of positioning/safety devices. Therefore, PT/OT equipment may be used only with students who are receiving PT and/or OT services. 4. Educational staff may NOT make independent decisions about the use of PT/OT equipment. 5. Seatbelts, whether attached to a chair or added to the chair, may be used as a protective device ONLY under the supervision of the OT or PT staff with appropriate documentation as described below. Documentation of Use of Protective Devices The use of a protective device must be documented in the IEP, using form ECP-S42, “Documentation for the Use of a Protective Device.” The Physical or Occupational Therapist must approve the use of the device. The documentation must include at least the following: 7/02 11-7 Durham Public Schools Programs for Exceptional Children 1. Identification of physical issues that affect the student’s ability to independently position self for classroom activities (e.g., the student is unable to sit or stand independently) 2. Identification of physical issues that could impact the student’s ability to participate in classroom activities safely (e.g., poor balance, poor muscle control) 3. Statement that a protective device is necessary for the student to benefit from his/her program of special education (i.e., without this device, the student would be unable to participate in classroom activities appropriately and safely). 4. Description of the student’s activities that prompt the need for a protective device. 5. Type of protective device to be used. 6. Activities for which it will be used. 7. When, and for how long the protective device will be used during the day. 8. Timeline for use of the protective device to be reviewed (at least annually, at the IEP review). 9. Signature of the IEP Team. 10. If the parent is not present at the meeting, the protective device may not be used until 5 school days after the parent has been notified (via the DEC-5, “Prior Written Notice”). A copy of the ECP-S42 should be sent with the DEC-5. The use of the protective device(s) should be documented on the IEP, DEC 4, p.3 under “Appropriate supplementary aids, services, and modifications. . .” The IEP may refer to the documentation contained in the ECP-S42, as described above. For example, the Team may state: “The protective device identified on the attached form ECP-S42 will be used as described therein.” The documentation form MUST be attached to the IEP. Related Procedures: “Use of Physical Restraint” “Related Services Referrals” “Development of the IEP” “Procedural Safeguards” Related Forms: Documentation of Need for a Protective Device (ECP-S42) Prior Written Notice 7/02 11-8 DURHAM PUBLIC SCHOOLS Exceptional Children’s Programs DOCUMENTATION FOR USE OF A PROTECTIVE DEVICE This form must be completed by the IEP Team and approved by the Physical/Occupational Therapist when a protective device is needed. The device may not be used until approved by the therapist and notification is given to the parent. Student’s Name: ___________________________ Exceptionality: _______ Circle Related Services: PT OT 1. Describe any physical issue which affects the student’s ability to be independent when positioning him/herself for classroom activities. (e.g., unable to sit or stand independently) 2. Describe any physical concerns that could impact on the student’s ability to participate safely in classroom activities. (e.g., poor balance, poor muscle control) 3. Does the IEP team agree that a protective device is the most appropriate way for this student to benefit from his/her education (without this device, the student would be unable to participate in classroom activities appropriately and safely)? Yes No Explain: (What is happening that prompts the need for a protective device?) 4. Specify the type of protective device to be used: 5. State the particular activities which require this student to use a protective device: 6. Length of time or time periods during the day when the device is to be used: 7. How often will the use of this protective device be reviewed? Signatures of IEP Team: Name Title Date Parent LEA Rep EC Teacher Reg. Ed Teacher Therapist * If the parent is not present at the meeting, the protective device may not be used until 5 school days after the parent has been notified (via the DEC-5, “Prior Written Notice”). A copy of this form should be sent with the DEC-5. Approval of the Physical/Occupational Therapist I agree that use of the specified protective device in the manner described above is appropriate for this student. _____________________________________ __________________ Signature of PT / OT (circle one) Date Copy to parent ____/____/____ ECP-S42 7/02 Durham Public Schools Programs for Exceptional Children BEHAVIORAL SUPPORT ASSISTANTS The Office of Exceptional Children’s Programs offers the services of a limited number of Behavioral Support Assistants to help students experiencing a sudden, unexpected behavioral crisis. The Behavioral Support Assistants work under the direction of the Behavior Support Liaison and are provided as a short-term intervention designed to allow personnel within the school to develop a long-term plan to address the student’s needs. As a condition of this service, it is expected that school personnel will meet regularly with the Behavioral Support Assistant, Behavior Support Liaison, and/or other members of the ECP administrative team during the period of service. School personnel will be expected to follow through with the recommendations of ECP personnel working with the student. The following procedure applies to the assignment of a Behavioral Support Assistant to assist a school. 1. If the teacher has problems with a student, the (BST) Behavior Support Team at the school will assess the situation and recommend strategies to address the problem. 2. If strategies recommended by the BST are not working, the teacher should contact the SAP team if the student is a regular education student. If the student is an exceptional education student, a FBA (Functional Behavioral Assessment) and a BIP (Behavioral Intervention Plan) must be developed by the IEP team. 3. If the student is still having problems following the SAP interventions or FBA/BIP, an administrator at the school should assess the situation to determine if all required procedures have been followed and new ideas explored. 4. Administrator should contact EC Coordinator to request a Behavioral Support Assistant. Form ECP-F10, “Behavior Support Assistant Request Form,” should be complete by the school team and given to the Coordinator. 5. The EC Coordinator should review the request form for the following, as applicable: Referral form Cumulative Folder Data Grades EOG/EOC Retention History Attendance Discipline History List of outside agencies involved SAP History ECP Folder FBA BIP Before and After School Data List of school staff involved Other relevant information 6. An EC Coordinator will assess the above information and do a classroom observation. 7. EC Coordinator will ask the BST to try other strategies and/or meet with Behavioral Support Liaison to determine if a Behavior Support Assistant is needed. 8. EC Coordinator and the Behavior Support Liaison will meet with the principal to discuss and plan meeting of Behavioral Support Team at the school. 9. Behavioral Support Assistants are subject to immediate reassignment to intervene with a student in imminent danger of hurting self or others. Related Forms: Behavior Support Assistant Request Form (ECP-F10) 7/02 11-10 DURHAM PUBLIC SCHOOLS Exceptional Children’s Programs BEHAVIOR SUPPORT ASSISTANT REQUEST FORM Student’s Name ______________________________________________ Date of Birth __________________ Grade _____________________________ Race __________________________ Sex _____________________ School _________________________________________ Primary Disability __________________________ Teacher's Name ____________________________________________________________________________ Please give reasons why the above student is being referred. Please describe specific behaviors. ____________________________________________________________________________________________ ____________________________________________________________________________________________ ____________________________________________________________________________________________ Please include the following information with this form: ____ ____ ____ ____ Referral Form EOG/EOC Discipline History FBA ____ Cumulative Folder Data ____ Before/After School Data ____ SAP History ____ BIP _____ _____ _____ _____ Grades Attendance ECP Folder Retention History List of school staff involved: ____________________________________________________________________ List of outside agencies involved: ________________________________________________________________ Other relevant information: _____________________________________________________________________ Do not write below this line Behavioral Support Team reviewed and tried other strategies. Yes_____ No _____ If yes, what strategies were tried?________________________________________________________________________________________________ ______________________________________________________________________________ EC Coordinator reviewed and suggested other strategies. Yes_____ No _____ If yes, what strategies were suggested?____________________________________________________________________________________________ ____________________________________________________________________________________________ Received Date _________________________________ Referred By__________________________________ Accepted Date ___________ Rejected Date ____________ Behavior Assistant __________________________ ******************************************************************************************** Comments: __________________________________________________________________________________ ____________________________________________________________________________________________ _____________________________________________________________________________________________________ ECP-F10 7/02 Occupational Course of Study n n Student Enrollment Parent and Student Notification Letter (ECP-S33) ÿ Student Enrollment Form (ECP-S34) Durham Public Schools Programs for Exceptional Children THE OCCUPATIONAL COURSE OF STUDY -- STUDENT ENROLLMENT Overview The Occupational Course of Study, available only for students with an IEP, is a program that focuses on the acquisition of functional academic and work readiness skills. It is not a separate diploma, but one of four courses of study leading to a regular diploma. Successful completion of the OCS requirements, which include school and community-based training as well as competitive employment, results in graduation with a North Carolina Diploma. According to the North Carolina Department of Public Instruction, students meeting the following guidelines should be considered for the Occupational Course of Study: (1) students who are being served in the Exceptional Children’s Program, (2) who have a post-school outcome goal for employment (not college) after graduation, (3) whose post-school needs are not being met by the NC Standard Course of Study and (4) who wish to pursue a course of study that provides functional academics and hands-on vocational training. The Occupational Course of Study is not: (1) an appropriate curriculum for all students who cannot obtain a high school diploma through one of the other courses of study; (2) a program designed to remove certain students from the accountability standards; or (3) a “classroom-textbook” driven course of study. The IEP Team must consider enrollment of students into the Occupational Course of Study on a case by case basis. Students should not be recommended based solely on their disability classification. However, all members of the IEP Team should recognize that the curriculum objectives were designed for students functioning intellectually, academically, and socially in the mild mentally handicapped range. In most cases the decision to enroll a student into the Occupational Course of Study will be made when the student is in the 8th grade. Students who enroll during their 9th or 10th grade year may have to spend an extra year in high school in order to complete all the requirements. Procedure for Enrolling a Student in the Occupational Course of Study If an EC teacher or IEP Team believes that this program is appropriate for a student they should follow these steps: q Contact the parent to discuss enrollment. Send them the DPS parent letter that describes the OCS (Occupational Course of Study Parent & Student Notification, ECP-S33), along with an Invitation to Conference. q Hold an IEP meeting to discuss enrollment and other high school options (for example, the Career Prep. Course of Study). This may occur at the same time as the annual IEP meeting. Review the requirements as listed on the parent letter and notification. The team should include at least one of the student’s EC teachers, one of his/her regular education teachers, an LEA representative, a guidance counselor, the parent, and the student. q If the IEP Team, including the parent and student, agree that this pathway is appropriate, the team should sign the OCS Student Enrollment Form (ECP-S34). Give a copy to the parent and keep the original in the front of the confidential folder. Rev. 7/02 12-1 Durham Public Schools Programs for Exceptional Children q Review the student’s IEP and transition plan. The student’s EC placement should be marked as “Separate” and the goals aligned with the OCS curriculum objectives. For example, math goals might include, “The learner will demonstrate an understanding of financial management skills necessary for independent living and employment.” If the student does not have a transition plan, this is a good time to write one. q Check the “Separate Setting” database. If the student is not listed on it, (possibly because the student has been in a resource setting) or the address is incorrect, send a SIMS Update Form (ECP-S40) to the Elementary/Secondary EC Administrator at the Central Office. Indicate on the form that the student is OCS and the date that the student will begin the separate setting. q Enlist the counselor’s assistance in registering the student for the correct OCS classes for the next school year. q Keep a list of students who are being enrolled. You will be asked to send this to the central office and/or to the appropriate high school. Note: If, after “reasonable” IEP meeting notification, the parent does not respond or attend the meeting, the IEP Team may sign the enrollment form. In these cases it is particularly important that the student understands this Course of Study, agrees to participate, and signs the enrollment form. Related Forms: Rev. 7/02 OCS Parent and Student Notification (ECP-S33) OCS Student Enrollment Form (ECP-S34) 12-2 DURHAM PUBLIC SCHOOLS Exceptional Children’s Programs OCCUPATIONAL COURSE OF STUDY PARENT AND STUDENT NOTIFICATION Date: Dear Parent/Guardian and Student: The Occupational Course of Study is a new high school program approved by the North Carolina State Board of Education for certain students who receive services from the Exceptional Children’s Program. It is one of four courses of study leading to a regular diploma. This program focuses on the acquisition of functional academic and work readiness skills and prepares students to enter competitive employment. Successful completion of the Occupational Course of Study requirements results in graduation with a North Carolina Diploma. Course requirements include: • 4 courses in Occupational English • 3 courses in Occupational Mathematics • 2 courses in Occupational Science • 2 courses in Occupational Social Studies • 4 courses in Occupational Preparation which include 300 hours of school-based training, 240 hours of community-based training, and 360 hours of paid employment. • 1 course in Health/Physical Education • 4 courses in Career/Technical Courses in this program cannot be substituted for courses in other programs of study (for example, Occupational English I cannot be substituted for English I) and occupational courses will not be accepted for credit by most colleges. Parents of students enrolled in the Occupational Course of Study will be expected to do the following: • Provide copies of the student’s birth certificate, social security card, and medical insurance information • Sign and return all forms as needed • Sign referral forms to Vocational Rehabilitation when their child reaches the age of 16 • Participate in IEP meetings and transition planning for their child. We would like to discuss enrolling your child in this course of study at the date and time noted on the enclosed Invitation to Conference. If you have any questions, please call me at 560-_______ . Sincerely, EC Facilitator c: confidential folder ECP-S33 Rev. 8/01 DURHAM PUBLIC SCHOOLS Exceptional Children’s Programs OCCUPATIONAL COURSE OF STUDY STUDENT ENROLLMENT FORM Student: _____________________________________________________________________________ Name of Parent or Guardian: _____________________________________________________________ Address: _____________________________________________________________________________ Current School: _______________________________________________________________________ Student’s area of exceptionality: ___________________________________ School: _______________________________________________________ Date of Meeting: _______________________________________________ The IEP Team recommends that the above named student be enrolled in the Occupational Course of Study to begin on ________________________________ (date). Participants in meeting: Name Position ________________________________________ Parent ________________________________________ Student ________________________________________ LEA Representative ________________________________________ ECP Teacher ________________________________________ ________________________________ ________________________________________ ________________________________ Comments: _____________________________________________________________________________________ _____________________________________________________________________________________ _____________________________________________________________________________________ Distribution: Place the original of this form in the EC file, give a copy to the parent, and mail a copy to the Transition Specialist. ECP-S34 Rev. 7/02 Closing the School Year n Promotion and Retention n End of Year IEP Procedures n End of Year Folder Exchange Durham Public Schools Programs for Exceptional Children PROMOTION AND RETENTION The school principal makes promotion and retention decisions in accordance with State regulations and school board policy 3225.6 3225.6 Promotion/Retention of Students with Exceptional Learning Needs The decision regarding the retention/promotion of exceptional children will be determined by the IEP Team in consultation with the principal. Factors to consider if a student fails to meet promotion standards: The IEP Team should reconvene immediately with the principal to consider the following: • Is the current IEP appropriate? • Is the manner of assessment appropriate and does it include any accommodations and/or modifications identified in the IEP? • Were all the services required by the student to make progress in the general education curriculum appropriately identified in the student’s IEP? • Did the student receive all the services identified in the IEP? • If ESL, were the linguistic needs of the student appropriately identified? Minutes are to be kept of the discussion and the decision. Minutes should reflect that all of the above questions were discussed. Place minutes in the confidential folder and give parents their copy. 13-1 Durham Public Schools Programs for Exceptional Children END OF YEAR IEP PROCEDURES Exit of seniors who are graduating with a diploma: 1. Send parents a Handbook on Parents’ Rights and Invitation to Conference letter marked “change of placement” and “exit from the program”. 2. Review the student’s goals and progress and be sure the parents understand the student is graduating from Exceptional Children’s services. 3. IEP Team signs Prior Written Notice form, exiting student from Exceptional Children’s services. 4. All other seniors should have an IEP that continues into the next year, as they are eligible to receive Exceptional Children’s services until the age of 21 or upon graduating with a diploma. 5th/8th graders moving to middle and high school: 1. IEPs should be reviewed for any changes needed at the receiving school. 2. The IEP Team must amend any changes in time/meeting dates. 3. If the student’s needs in the receiving school result in a change of placement on the IEP, the following must be done: • Send Invitation to Conference and Handbook on Parents’ Rights. • Amend the IEP to reflect the change of placement. • Complete the Prior Written Notice form. • Complete SIMS/4 GL Data update. 4. IEPs that expire prior to September 15th should be rewritten before the end of the school year. 13-2 Durham Public Schools Programs for Exceptional Children END OF YEAR FOLDER EXCHANGE The confidential folders of rising K, 6th and 9th grade students must be transferred to the students' new schools at the end of the school year. Folder exchange usually takes place sometime during or near the last week of school and is announced in advance. The Case Manager is responsible for ensuring that his/her folders are prepared for transfer at any time, i.e., they should be kept current and complete throughout the year. In the spring, the Case Manager must carefully review each transferring folder to confirm that all required components of the folder are present and in proper order. Not later than 5 school days before the end of the school year for students, the Case Manager should attach the final progress report of the year to the IEP. Folders to be transferred must be in correct folder order. (See "Guidelines for Uniform Folder Order -EC Active Folder (Green Dot).") In addition to the folder order, the following components of the folders will be checked at the time of folder exchange: 1. 2. 3. 4. IEP – must be current 3 yr. reevaluation – must be current Progress Reports – must be present for entire year SIMS sheet – must be present Folders brought to the folder exchange that are not in folder order or that are missing required components will be returned to the Case Manager for immediate correction. Graduating Seniors: Folders of graduating seniors must be forwarded to the DPS Records Center, using the form “Records Transfer For Graduating Seniors” (ECP-F7). Related Forms: Records Transfer For Graduating Seniors (ECP-F7). 13-3 DURHAM PUBLIC SCHOOLS Exceptional Children’s Programs RECORDS TRANSFER FOR GRADUATING SENIORS At graduation time each spring, every EC Facilitator or designee in the senior high schools should indicate on this form in alphabetical order those exceptional education students who will graduate. Please make three (3) copies of this form and send to the following by June 1: (1) Records Center; (2) ECP Central Office, Fuller Building; and (3) School File. Signature of Person Completing Form: ____________________________________________________ High School: ____________________________________________________ Last Name, First Name MI Date Completed ECP-F7 Rev. 8/01 Date of Birth Last Name, First Name MI ___________________________________ Date of Birth Job Descriptions n Case Manager ß Facilitator ß Coordinator ß Specialist ß Teaching Assistant Durham Public Schools Programs for Exceptional Children JOB DESCRIPTION – CASE MANAGER The Case Manager is usually the teacher of the student with a disability or a suspected disability. In the event the student has speech as the primary category; the speech pathologist is the Case Manager. If the student is served by a specialist, i.e. autistic, blind visually impaired, etc. on a consultative basis, the special teacher in the school to which the student is assigned is the Case Manager. The Exceptional Children’s Facilitator (EC Facilitator) or the principal is responsible for assigning students to the Case Manager. Responsibilities of the Case Manager (This is not an exhaustive list.) Compliance: The Case Manager is responsible for compliance of the special education folder of a student with a disability. This includes: - Organizing and keeping the confidential folder in proper folder order; - Ensuring that IEPs are kept current; - Ensuring that 3-year reevaluations are kept current; - Working with EC Facilitator to correct problems in the folder; and - Ensure compliance with students’ designated methods of participating in State Testing Program.* * For students participating through the Alternate Academic Assessment Inventory or the Alternate Assessment Portfolio, baseline data must be collected during the first 3 weeks of the school year and regularly thereafter. Communication: - Advise students’ regular education teacher(s) about students’ IEP, modifications, and accommodations; - Communicate student progress via regular progress reports to parents; - Advise EC Facilitator of students’ testing modifications as required;* and - Collect data as required by the Central Office. *For third-grade students, this information must be communicated within the first 3 weeks of the school year so that modifications will be provided for the EOG Pre-Test. Referral: After receiving assignment as Case Manager or receiving referral from EC Facilitator: - Serve on SAP Team when requested to do so by school administrator; - Begin special folder for student, organizing the order according to DPS directions; - Notify staff members who must be present at pre-evaluation meeting; - Schedule pre-evaluation meeting; - Send Invitation to Conference to parents (all blanks must be filled) and Handbook on Parent’s Rights. Request parent bring any information, i.e. privately obtained evaluations, parental concerns, etc., to the meeting; and - Send 2nd and (when appropriate) 3rd notice to parent when there is no response. Pre-evaluation Meeting: - Gather information that will be needed at the pre-evaluation meeting, i.e., information from SAP; - Chair the meeting; - Arrange for someone at the meeting to take minutes; - Notify EC Facilitator of need for an interpreter for a parent with limited English proficiency or who is deaf or hard of hearing; and - Obtain written consent for evaluation and provide copy of consent for parent. 14-1 Durham Public Schools Programs for Exceptional Children Following the Pre-evaluation meeting: - Notify EC Facilitator of need for psychological testing; - Complete educational testing; - Notify EC Facilitator of need for other required testing: e.g., occupational therapy, physical therapy, medical evaluations including vision and hearing, adapted physical education, adaptive behavior, assistive technology, social history, behavioral assessment, etc.; and - Provide psychologist with completed test information along with copy of permission to test. Eligibility Meeting: - Schedule meeting; - Notify persons who must be in attendance; - Send Invitation to Conference with adequate notice to allow parents to attend. Send 2nd and 3rd notices if no response is received from parent; - Ensure that all evaluation material required by pre-evaluation meeting participants is completed and available for the meeting; - Notify EC Facilitator if any interpreters are needed; - Arrange for someone at the meeting to take minutes; and - Ensure the Summary of Evaluations has been completed. Eligibility Meeting That Includes IEP Development and Placement Decision: - Chair the meeting unless the EC Facilitator has been assigned to do so; - Following the determination of eligibility ensure that the eligibility statement on the Summary of Evaluations is completed; - Facilitate the IEP development process; (See DPS procedures on IEPs) - See that appropriate signatures are obtained on the IEP signature page; - Ensure that parent receives copy of completed IEP along with minutes as appropriate; - Obtain written parent permission to place; - Ensure that any teacher or other staff who has responsibility for any part of the IEP receives a copy of the IEP or a copy of the parts for which he/she is responsible; and - Give parent the Handbook on Parents’ Rights Separate IEP Meeting From Eligibility Meeting: - Same as above except the meeting focuses only on IEP development and placement. Annual Review and Reevaluation: - Same responsibilities and process as above except for annual review, which is the review and development of the IEP on an annual basis. - Refer to section of DPS procedures on reevaluation. 14-2 Durham Public Schools Programs for Exceptional Children JOB DESCRIPTION – EXCEPTIONAL CHILDREN’S FACILITATOR The Exceptional Children’s Facilitator (EC Facilitator) is a teacher who is assigned responsibilities at a designated school to: • • • • • • • • • • • • • • • • • Chair IEP Team meetings as appropriate. Ensure that all mandated timelines are adhered to in processing student referrals and service delivery (i.e., annual reviews and reevaluations). Ensure that EC folders are complete, accurate, and compliant, including all required documentation in folder order. Serve as liaison between school and administrative staff for Exceptional Children’s Programs. Address parent concerns and ensure that parents are informed of parental rights and are given maximum opportunity to participate in all educational decisions. Assist with training and orienting new Exceptional Children’s teachers. Audit records to ensure compliance. Receive and transfer confidential records. Arrange for data input. Assign and assist Case Managers as needed with initial eligibility, reevaluation and annual review meetings. Help provide training and support for regular and special education staff. Consult with principal regarding exceptional children’s needs and assist with the evaluation of building level programs. Monitor statewide testing program for students with disabilities. Obtain accurate teacher schedules and class loads and monitor EC teachers’ caseloads for State compliance. Assist with behavioral issues, i.e., manifestation meetings, suspension records, etc. Coordinate psychological and other required assessments. Serve on the Oversight Committee when appropriate. 14-3 Durham Public Schools Programs for Exceptional Children JOB DESCRIPTION – EXCEPTIONAL CHILDREN’S COORDINATOR The Exceptional Children’s Coordinator is a Central Services special education staff person who provides leadership to personnel in the schools, assists the Assistant Superintendent for Exceptional Children’s Programs and responds to parents. Duties and responsibilities of this position are varied and complex. Persons in this position must possess a high level of knowledge and expertise in the area of education of students with disabilities, as well as possess excellent communication and interpersonal skills. A list of the types of activities in which the coordinator is involved follows: • Plans staff development; • Assists with personnel allotments for the schools; • Plans and assists with programming at the building based sites; • Acts as liaison between teacher and principal; • Acts as liaison between principal and central office staff; • Assists with personnel interviews; • Assists with recruitment of teachers, assistants, and related service personnel; • Assists with teacher observations and evaluation of school level personnel; • Approves final assignment to self-contained classes; • Makes decisions about program locations at particular schools; • Works to maintain compliance at the school level with State, federal and local procedures; • Attends manifestation meetings as requested; • Responds to emergencies; • Works with court counselors as appropriate; • Attends court as required (due process hearings, etc.); • Gives depositions as required; • Orchestrates response to parent complaints; • Develops and works with corrective action plans responding to parent complaints; • Responds to requests for and schedules independent educational evaluations; • Coordinates the scheduling of related services and transportation; • Works with the transfer of folders within the school system; • Assists with the tracking of students; • Works with budgets; and • Assists with headcount. 14-4 Durham Public Schools Programs for Exceptional Children JOB DESCRIPTION – EXCEPTIONAL CHILDREN'S SPECIALIST The specialist is a teacher who is assigned responsibilities in a particular category of disability or a particular area of expertise. The specialist may have direct teaching responsibilities, but usually serves students on a consultative or outreach basis. The specialist is available to regular and special education teachers who may require assistance in working with a particular child. The assistance may include direct instruction of the student in order to provide models for the regularly assigned teacher. It may include observation of the student and the regularly assigned teacher, followed by recommendations that will improve instruction and services to the student. It may include providing information on different types of techniques or methodologies that might be more appropriate for the student. It may include the specialist meeting with the parent. It may include assisting with determining the requirement of assistive technology and instruction for the teacher, as well as the student, in how to use it. There are specialists in the following areas: - Blind and visually impaired - Autism - Assistive technology - Speech-language - Physical therapy - Occupational therapy - Audiology - Transition Note: Teachers who are employed in specialist positions do not act as Case Managers. 14-5 Durham Public Schools Programs for Exceptional Children DURHAM PUBLIC SCHOOLS Exceptional Children’s Programs JOB DESCRIPTION – EC TEACHING ASSISTANT The EC Teacher Assistant works under the supervision of the classroom teacher and/or principal. A wide variety of tasks to support the teacher and students may fall within the scope of the job. The specific tasks that are required will vary according to the particular needs of the EC students in the class. The EC Teacher Assistant may be asked to perform any of the following duties: Supervision of Students and Behavior Monitoring: • Meet the buses in the morning and escort students to the classroom daily* • Accompany students from separate to regular education inclusion classes or other classes, activities, or events during the school day* • Assist in transition times: bus lot, cafeteria, etc.* • Supervise students during breakfast and lunch and on the playground* • Assist in dismissal and supervise students during departure, including escorting students to the bus as needed* • Discipline misbehavior through approved methods, at the direction of the teacher • Report discipline problems to teacher or other supervisory personnel* • Report to teacher or other supervisory personnel significant change or lack of change in student behavior* • Model appropriate social skills and respect for others* Academic Assistance: • While in the class, assist students with understanding directions, beginning and completing assignments, or as otherwise directed by the teacher* • Provide follow-up from class instruction* • Work with small groups of student under the direction of the classroom teacher* • Occasionally cover classroom while teacher attends EC or other meetings (lead teacher plans and leaves assignments and activities)* Student Support • Assist with personal/physical care of student based on child’s needs, including, but not limited to any of the following:* - tube feedings - catheterization - assisting with transfers of physically impaired students from wheelchair to toilet, desk, etc. and back - changing soiled clothing - changing diapers - assisting with toileting • Assist with implementation of modifications and accommodations on student IEPs* 7/02 14-6 Durham Public Schools Programs for Exceptional Children Communication and Record Keeping • • • • • • Maintain confidentiality of student records, performance and medical/disability-related information* Communicate observations, information, etc., regarding students, classroom activities, etc. to the classroom teacher and/or parents as directed by the teacher* Participate in data collection for student IEPs as directed by the teacher* Participate in IEP meetings, discussions, etc. upon request of teacher/principal* Assists in data collection for behavioral intervention plans, contracts, reward systems, etc.* Take attendance, prepare materials,* and file student work Other • Other duties as assigned by supervisory personnel • Participate in available training for the duties listed above* *Denotes essential function of the job Knowledge, Skills and Abilities Required • • • • • • • • • • 7/02 Working knowledge of the core subjects at the grade level to which employment assignment is made Ability to read, speak and write the English language sufficiently to be clearly understood by school personnel and parents Ability to lift and/or transfer students or materials weighing up to 50 pounds without assistance and up to 100 pounds with assistance Ability to establish and maintain positive relationships with students, staff and parents. Ability to record data accurately Ability to maintain safe environment for students during activities and mealtime Ability to follow minimally detailed written and oral instructions without constant supervision Ability to independently solve minor problems Ability to maintain confidentiality of student information Ability to follow prescribed procedures to maintain sanitary environment 14-7 Additional Local Forms Durham Public Schools Programs for Exceptional Children ADDITIONAL LOCAL FORMS 1. IEP Team Meeting Minutes Form (ECP-S35) Used to record minutes of all IEP meetings. 2. Exceptional Student Information Sheet (ECP-S36) Completed by Case Managers. The form serves to share class schedules and modifications with regular teachers. 3. Acknowledgement of Receipt of EC Information (ECP-S37) Completed by regular education teachers to verify that they have received a copy of their students' IEPs and/or modifications and accommodations. 4. Confidential Social Developmental History (ECP-S38) Usually completed during the SAP process. 5. Confidential Social Developmental History Update (ECP-S38A) Used to update the social developmental history for a reevaluation. 6. Surrogate Referral (ECP-S39) Completed by Facilitator and sent to EC Central Office personnel in charge of assigning Surrogate Parents. 7. Special Education Class Enrollment Form (Class Schedule) (ECP-DPI1) Completed by each EC teacher at the request of EC Central Office to indicate daily schedule of the number of students served by category each period of the day. Directions included. 8. Separate Data Base Codes and Explanations Used to manually update the EC Central Office database of EC separate students. 9. SIMS Update Form (ECP-S40) Used to record information necessary for updating the Student Information Management System (SIMS) database. 10. Health Screening Report (ECP-S41) Used in evaluation/reevaluation and eligibility determinations for disabilities that require a health screening. Requires review and signature of school nurse. 11. Modified Textbook Order Form (ECP-F9) Used to record requests for modified textbooks that are necessary to meet IEP requirements. 12. Records Center Transfer Form for Confidential Records To be affixed to boxes of confidential records transferred to the Records Center Rev. 7/02 15-1 p. ___ of ___ DURHAM PUBLIC SCHOOLS Exceptional Children’s Programs IEP TEAM MEETING MINUTES Name of Student:_____________________________________ Meeting Date: ____/_____/____ DOB:____________________________ School: ________________________________________ Present for meeting: ______________________________________________________________ ________________________________________________________________________________ ________________________________________________________________________________ ________________________________________________________________________________ Purpose of meeting: ______________________________________________________________ ________________________________________________________________________________ Parent received copy of Parents’ Rights Handbook prior to meeting: Yes q No q If no, explain____________________________________________________________________ Presentation: ____________________________________________________________________ _______________________________________________________________________________________ _______________________________________________________________________________________ _______________________________________________________________________________________ _______________________________________________________________________________________ _______________________________________________________________________________________ _______________________________________________________________________________________ _______________________________________________________________________________________ _______________________________________________________________________________________ _______________________________________________________________________________________ _________________ Decision/Recommendation: ______________________________________________________ _______________________________________________________________________________ Follow-up: _____________________________________________________________________ ______________________________________________________________________________________ ________________________________________________________________________ Report Submitted By: _________________ ECP-S35 Rev. 8/01 Copy Given to Parent____________ p. ___ of ___ DURHAM PUBLIC SCHOOLS Exceptional Children’s Programs IEP TEAM MEETING MINUTES (Continued) Student Name _________________________________ Meeting Date:_____/_____/____ DOB:____________________________School:________________________________________________ _______________________________________________________________________________________ _______________________________________________________________________________________ _______________________________________________________________________________________ _______________________________________________________________________________________ _______________________________________________________________________________________ _______________________________________________________________________________________ _______________________________________________________________________________________ _______________________________________________________________________________________ _______________________________________________________________________________________ _______________________________________________________________________________________ _______________________________________________________________________________________ _______________________________________________________________________________________ _______________________________________________________________________________________ _______________________________________________________________________________________ _______________________________________________________________________________________ _______________________________________________________________________________________ _______________________________________________________________________________________ _______________________________________________________________________________________ _______________________________________________________________________________________ _______________________________________________________________________________________ _______________________________________________________________________________________ _______________________________________________________________________________________ _______________________________________________________________________________________ _______________________________________________________________________________________ _______________________________________________________________________________________ _______________________________________________________________________________________ _______________________________________________________________________________________ _______________________________________________________________________________________ _______________________________________________________________________________________ _______________________________________________________________________________________ _______________________________________________________________________________________ _______________________________________________________________________________________ _______________________________________________________________________________________ ECP-S35 Rev. 8/01 DURHAM PUBLIC SCHOOLS Exceptional Children’s Programs EXCEPTIONAL STUDENT INFORMATION SHEET For School Year 200__ – 200__ Student's Name Date of Birth School Grade Parents' Names Home Phone Work Phone IEP Review Date Re-Eval Date Case Manager ECP Teacher(s) Exceptionality Areas Related Services Behavior Intervention Plan ? Notes: Student's Schedule* FIRST SEMESTER CLASSES SECOND SEMESTER TEACHERS CLASSES TEACHERS HR 1 2 3 4 5 6 7 *Optional for elementary students p. 1 of 2 ECP-S36 Rev. 8/01 DURHAM PUBLIC SCHOOLS Exceptional Children's Programs EXCEPTIONAL STUDENT INFORMATION SHEET For School Year 200__ – 200__ Student's Name Case Manager Classroom services: (indicate none, consult (con), inclusion (inc), or resource (res) ) LA or English Social Studies Math Science Copy of IEP goals and objectives attached: Yes ____ No____ Student has a behavior intervention plan: No ____ Yes____ Copy attached _____ Standardized Testing Modifications (check all that apply) Separate setting Extended time Read aloud Scribe Mark in book Multiple sessions 1 Test item per page Other: Classroom Modifications (Check all that apply) Instructional Presentation Instructional Materials Assignments Testing Physical Environment Interpreter Audio Tapes Alternate Read Aloud Seated near Teacher Teacher Notes Demo Teaching Student Notes Tape Recorder Large Print Simplified Larger Desktop Models Oral Extended Time Separate Setting Sequential Modified Large Print Captioned Films Regraded Dictation Adapted Text Completion Timeline Self-paced Projects Cooperative Group Proj. Multiple Choice Short Answer Highlight Text Graphic Organizer Course Outline Study Guide Review Materials Portfolio Demonstration Nonglare Lights Away from Windows Classes on 1st Floor Supplemental Aides Braille/ Braillewriter CrammerAbacus Magnification Devices Computer/ Word Proc. p. 2 of 2 ECP-S36 Rev. 8/01 DURHAM PUBLIC SCHOOLS Exceptional Children’s Programs ACKNOWLEDGMENT OF RECEIPT OF EC INFORMATION TO: All Teachers of EC Students FROM: RE: Verification of receipt of modification sheets and/or IEP for the following students: 1. ______________________________________ 2. ______________________________________ 3. ______________________________________ 4. ______________________________________ 5. ______________________________________ 6. ______________________________________ Please initial students' names and sign below indicating you have received these items. Return memo in this folder/envelope to ______________________________________. Thank you. Signature _________________________________________ Date _______________________ ECP-S37 Rev. 8/01 DURHAM PUBLIC SCHOOLS Exceptional Children’s Programs CONFIDENTIAL SOCIAL DEVELOPMENTAL HISTORY Completed by __________________________________ Date ______________________ Relationship to Student _____________________________ I. Student Information Name ____________________________________________________ School ___________________ Age ___________ Date of Birth ____/____/____ Gender ______ Grade ______________ Address _______________________________________________ Telephone _________________ II. Parent Information (If relevant, also provide information for stepparent or guardian.) Mother ________________________________ Father _________________________________ Age _____ Education ____________________ Age _____ Education ____________________ Place of Birth ___________________________ Place of Birth __________________________ Marital Status: Married ______ Separated ______ When __________________ Divorced ______ When __________________ Custody arrangements __________________________________________________________________ _____________________________________________________________________________________ Remarried? Mother _____ When ________ Father _____ When ________ Deceased? Mother _____ When ________ Father _____ When ________ III. Employment Information (circle parents with whom the child lives) Mother / Step-Mother / Guardian Father / Step-Father / Guardian Employer ______________________________ Length of Employment ___________________ Work Telephone ________________________ Employer ______________________________ Length of Employment ___________________ Work Telephone _________________________ IV. Family Composition List brothers and sisters and/or members of stepfamilies: Name Relationship ____________________________ ___________ ____________________________ ___________ ____________________________ ___________ ____________________________ ___________ ____________________________ ___________ Gender ______ ______ ______ ______ ______ ECP-S38 Rev. 8/01 Age _____ _____ _____ _____ _____ Lives in the Home yes ____ no ____ yes ____ no ____ yes ____ no ____ yes ____ no ____ yes ____ no ____ p. 1 of 4 Name: Date: CONFIDENTIAL SOCIAL DEVELOPMENTAL HISTORY (Continued) V. Medical History Pregnancy: Mother’s age at delivery ______________ Father's age ______________________ Complications: Premature_____ Number of weeks early _______ Number of week's late____________ Urinary Infection ______ Toxemia ____ High Blood Pressure _________ Other _________________________________________________________________ Illnesses ________________________________________ Medications ______________________ Smoking _______ How Much? ___________________________________________________________ Alcohol ________ How Much? ___________________________________________________________ Any unusual stress during the pregnancy which has not been addressed :___________________________ _____________________________________________________________________________________ _____________________________________________________________________________________ VI. Neonatal Period Birthplace _______________________________________ Birthweight ______________________ Breech ____ Cesarean ____ Why? _____________________________________________________ VII. Early Development When did the child: Sit _________ Crawl _________ Stand _________ Walk __________ Say single words __________ Use sentences __________ Feed self ________________ Complete Toilet training ___________ Did she/he eat well? _________________________ Sleep well? ______________________ Describe his/her disposition (e.g., active, passive, loud, quiet, happy, etc.) _________________________ _____________________________________________________________________________________ _____________________________________________________________________________________ _____________________________________________________________________________________ VIII. Diseases/Illnesses (indicate age when contracted) Measles _________________ Mumps _________________ Pneumonia _________________ Spinal Meningitis ___________________ Scarlet Fever ______________________________ Rheumatic Fever ___________________ Anemia __________________________________ Heart Problems _________________________ Kidney Problems ______________________ High fevers ________________ Describe _________________________________________ Serious injuries __________ Describe ____________________________________________ Allergies ___________________________________________________________________ History of seizure activity _____________________________________________________ Vision ________________ Hearing ________________ Ear Infections _________________ IX. Hospitalization (include age, length of stay, reason, etc.) ____________________________________________________________________________ ____________________________________________________________________________ ____________________________________________________________________________ ____________________________________________________________________________ ECP-S38 Rev. 8/01 p. 2 of 4 Name: Date: CONFIDENTIAL SOCIAL DEVELOPMENTAL HISTORY (Continued) X. Current Health Present health condition is: ____ Excellent _____ Good _____Satisfactory ______Poor Child has problems with: ____ Speech ____ Hearing ____ Vision ____Asthma ____ Headaches ____ Stomach Aches ____ Diabetes ____ Hyperactivity ____ Bed Wetting ____ Tubes in Ears ____ Ear Aches/Infections Other ________________________________________________________________________________ Does the child have good eating habits? ____________________________________________________ Child’s weight: ____ Underweight ____ Normal ____ Overweight Is the child on medication? _____ Yes ____ No Condition being treated: __________________________________________________________ Name of medication:_____________________________________________________________ Dosage: _______________________________________________________________________ XI. Family History (Include relationship to child.) Epilepsy _________________ Seizure _________________ Convulsions _________________________ Diabetes ______________________________ Mental Handicap _______________________________ Cerebral Palsy _________________________ Physical Disabilities ____________________________ Mental Illness __________________________ Behavior Difficulties ____________________________ Learning Difficulties ____________________ Other ________________________________________ XII. Behavioral/Emotional Information Parent’s perspective concerning child’s problem(s) __________________________________________ ___________________________________________________________________________________ Parent/Child Relationship: Mother (Stepmother) __________________________________________________________________ ___________________________________________________________________________________ Father (Stepfather) ___________________________________________________________________ ___________________________________________________________________________________ Sibling relationships __________________________________________________________________ ___________________________________________________________________________________ Relationship with peers _______________________________________________________________ ___________________________________________________________________________________ Behavior(s) of most concern to parents __________________________________________________ ___________________________________________________________________________________ Discipline Techniques/Results __________________________________________________________ ___________________________________________________________________________________ Family moves _______________________________________________________________________ Deaths or losses _____________________________________________________________________ Family problems _____________________________________________________________________ ___________________________________________________________________________________ Specific behaviors observed in the home (include ages and any comments) ___________________________________________________________________________________ ___________________________________________________________________________________ ___________________________________________________________________________________ ___________________________________________________________________________________ Do the parents feel the child is under any peer pressure? _____________________________________ ___________________________________________________________________________________ ECP-S38 Rev. 8/01 p. 3 of 4 Name: Date: CONFIDENTIAL SOCIAL DEVELOPMENTAL HISTORY (Continued) XIII. Preschool/School Experiences Child’s primary care person ______________________________________________________________ Have there been others? (grandparent, babysitter, daycare, preschool, etc.) Please list who and for how long: ________________________________________________________________________________ _____________________________________________________________________________________ What is your child’s attitude toward school? _________________________________________________ _____________________________________________________________________________________ What school problems are you are aware of?_________________________________________________ _____________________________________________________________________________________ _____________________________________________________________________________________ How does your child do his/her homework? ___ independently ___ with help ___ not at all Attitude towards homework is: ___ good ___ poor XIV. Community Agency Involvement Which community agencies have been involved with the child/family, how did they become involved, what was the outcome, is contact with family ongoing, if not, when was contact terminated? ___________________________________________________________________________________ ___________________________________________________________________________________ ___________________________________________________________________________________ XV. General Comments What do you regard as your child’s greatest strengths or assets? _______________________________ ___________________________________________________________________________________ ECP-S38 Rev. 8/01 p. 4 of 4 DURHAM PUBLIC SCHOOLS Exceptional Children’s Programs CONFIDENTIAL SOCIAL DEVELOPMENTAL UPDATE Note: For Reevaluations only. Not to be used for Initial Placement Completed by: ________________________________ Relationship to Student: _________________________ Date: ________________________________________ Student Information Name: _________________________________________ School: _________________________ Age: ____ Gender: __________ Grade: _______ Date of Birth: ______________________ Address: ____________________________________________________________________________ Phone: _______________________________ Medical Describe the child’s health: Describe any recent physical/medical problems: List medications the child takes and reasons taken: Describe any severe illnesses, injuries, or accidents that have occurred within the last three years: Parental Information Mother / Step-Mother / Guardian (circle) Father / Step-Father / Guardian Name: ________________________________ Name: ________________________________ Employer: _____________________________ Employer: _____________________________ Length of Employment: __________________ Length of Employment: __________________ Are the child’s parents (circle one) married / divorced / separated / never married? Child lives with __________________________________. If parents divorced/separated, please explain current custody or visitation and source of this information: Family Composition List brothers and sisters and/or members of stepfamilies: Name Relationship Gender ____________________ ____________________ ______ ____________________ ____________________ ______ ____________________ ____________________ ______ ____________________ ____________________ ______ ____________________ ____________________ ______ ECP-S38A Rev. 7/02 Age ___ ___ ___ ___ ___ Lives in the Home? yes____ no_____ yes____ no_____ yes____ no_____ yes____ no_____ yes____ no_____ p. 1 of 2 Name: Date: CONFIDENTIAL SOCIAL DEVELOPMENTAL UPDATE (Continued) Describe any different living/family arrangements during the past three years: Describe how the child gets along with family members: Describe anything in the family that may be worrying your child (deaths, sickness, moves, separations, divorces, financial trouble, etc.) School How does your child feel about school? What are the child’s favorite/least favorite things about school? Describe the child’s study and homework habits: Behavioral/Emotional Describe the child’s current behavior at home: How is the child disciplined for misbehavior? How often does the child need discipline? On an additional page, please add any additional information about the child or the family that you feel may be helpful to the school. Thank you. ___________________________________________ Signature of person completing form ECP-S38A Rev. 7/02 p. 2 of 2 DURHAM PUBLIC SCHOOLS Exceptional Children’s Program REQUEST FOR ASSIGNMENT OF SURROGATE PARENT This form should be completed when a surrogate is needed because (1) no natural parent or legal guardian can be located; and (2) there is no other adult who, with the permission of the parent, is acting in the place of the parent, e.g., a grandmother, aunt or adult sibling. The surrogate may not be an employee of DPS or any other school district or State agency. Send completed form to EC Central Office personnel in charge of assigning Surrogate Parents. Name __________________________________________ DOB ____________________________ Address ________________________________________ City_____________________________ State __________ Zip Code ____________ Phone Number ( Grade _________ Ethnicity ____________ Sex ____________ )_______________ School ________________________________________ Primary Disability _________________ Foster Parents __________________________________ Work Number(s)___________________ Address ______________________________________________________________________________ D.S.S. Case Worker _______________________________ Phone Number____________________ Guardian ad Litem ________________________________ Phone Number ____________________ Referred by ______________________________________ Date Sent ________________________ Comments ___________________________________________________________________________ _____________________________________________________________________________________ _____________________________________________________________________________________ _____________________________________________________________________________________ _____________________________________________________________________________________ This section to be completed by Central Office Personnel Surrogate Assigned ____________________________________________ Date _____________ Address __________________________________________________________________________ ___________________________________________________ Phone _______________________ ECP-S39 Rev. 7/02 Special Education Class Enrollment LEA: Durham Public Schools School: _________________________________________ Elem ________ MS ________ HS _________ Non-Duplicated Class Load by Disabilities (school wide caseload): AU _______ SLD _______ SPD _______ DD _______ BED _______ OHI _______ TMD _______ SI _______ EMD _______ OI _______ TBI _______ HI _______ MU _______ VI _______ *Total ______ Regular _______ Resource _______ Separate _______ Inclusion ______ Consult _______ *Total ______ Teacher:_______________________________________ EC Certification Area(s):_________________________ Percent employed by Regular Education/Exceptional Ed.: ______%Regular ______%EC Classroom Assistant(s) (1)____________________________________________ SPEECH THERAPISTS ONLY FILL IN SHADED BLOCK Do not complete rest of form Show Total Served: ________ (2)____________________________________________ (3)____________________________________________ Inclusion Class Periods:______ *Totals must be the same 1) Indicate number of students by category Daily Schedule Period 1 MONDAY 1) 2) 2) Total per period TUESDAY 3) 1) _____ 3) Number of assistants WEDNESDAY 2) 3) 1) 2) *highlight period(s) you are requesting to exceed class size THURSDAY 3) 1) ______ ______ ______ FRIDAY 2) 3) 1) Time: Period 2 Time: Period 3 Time: Period 4 Time: Period 5 Time: Period 6 Time Period 7 Time Teacher’s Signature/Date : ____________________________________________________ EC Facilitator/Date: __________________________________________________________ DPI USE ONLY Approval is requested to exceed maximum recommended class size, as highlighted above, based on a review of teacher’s workload and the assurance that each student’s IEP can be met. pApproved Principal’s Signature/Date: _____________________________________________________ Assistant Superintendent of Exceptional Children Signature/Date: _______________________________________________________________ __________________________________________ ___________ Fred J. Baars, Consultant Date ECP-DPI1 Rev. 8/01 pNot Approved 2) 3) Durham Public Schools Programs for Exceptional Children SEPARATE DATABASE CODES AND EXPLANATIONS Column Title Explanation School Present school assignment Teacher Current EC teacher Name Student’s legal name (Last, First, MI) Date of Birth Year, day, month (e.g., 86/27/03) Age As of today’s date Ethnicity Use SIMS codes Sex Male or Female Exceptionality Area of eligibility as checked on IEP Setting Level of service Street number Street Apartment number Zip code Most current home address available Class Type of classroom where the student is receiving EC services (BED, EMD, AU, MU, SP, TMD, MC, SLD, HI) 0_- 0_ Grade level for this school year Home School To be completed by EC Central Services Grade 0_- 0_ Projected grade level for next school year Last Column* Note whether student is due to graduate or age out of the program *This column to be completed by high school teachers only! PLEASE COMPLETE ANY MISSING INFORMATION! FILL IN ALL BLANKS EXCEPT FOR “HOME SCHOOL” 15-15 WORKSHEET E C A D D / C H A N G E S T U D E N T I N F O R M A T I O N STUDENT NAME:__________________________ YEAR___/___ EXIT DATE ___/___/___ STUDENT # ____________________ EXIT CODE_________________________ REFERRAL/RE-EVALUATE DATE ___/___/___ THIRD YEAR RE-EVALUATION (Y/N) ? ___Y___ N PERMISSION/NOTICE EVALUATE ___/___/___ (Parent Permission to Eval. Or Re-Eval.) SCREENINGIEVALUATION: S-Procedures/EH ___/___/___ E-Educational ___/___/___ S-Procedures/LD ___/___/___ E-IQ/Aptitude %ile ___/___/___ S-Health ___/___/___ E-Medical ___/___/___ S-Hearing ___/___/___ E-Ophthal/Optometric ___/___/___ S-Multidisc. Team ___/___/___ E-Otological ___/___/___ S-Psychomotor ___/___/___ E-Performance on Grades ___/___/___ S-Speech-Language ___/___/___ E-Psychological ___/___/___ S-Vision ___/___/___ E-Psychomotor ___/___/___ E-Adaptive Beh. ___/___/___ E-Review Early History ___/___/___ E-Audiological ___/___/___ E-Social/Dev. Hist ___/___/___ E-Beh/Emotional ___/___/___ E-Speech-Language ___/___/___ E-Cognitive ___/___/___ ___________________________________________________________________________________ WRITTEN SUMMARY OF EVALUATION TO PARENT/S ___/___/___ SBC DETERMINATION OF ELIGIBILITY ___/___/___(Date of eligibility determination)* APC DECISION FOR PLACEMENT ___/___/___(Date of IEP completion) INITIAL PLACEMENT (Y/N) ? ___Y___ N ___/___/___ PARENTAL CONSENT FOR PLACEMENT ___/___/___ PRIMARY EXCEPTIONALITY _______ SERVED DATE ___/___/___(Date IEP service begins in each LEA) STUDENT SETTING _______ BEGIN DATE END DATE FIRST IEP ___/___/___ ___/___/___ SECOND IEP ___/___/___ ___/___/___ THIRD IEP ___/___/___ ___/___/___ ___________________________________________________________________________________ EC IDENTIFIER CODE [computer]__ EC TEACHER [blank]__ IDENTIFICATION MATRIX _________ STATE OPERATED PROGRAM _________ COMPLIANCE OVERRIDE ___S___ ENTITLED (Y/N)? ___Y ___N LEGALLY BLIND (Y/N) ___Y ___N VISUAL ACUITY L _____ (Do Not complete R _____ if answer is "no") VISUAL ACUITY CODE L _____ R _____ READING MEDIUM CODE _____ (S-System, C-Compliant, N-Not Compliant) CODE BEGIN DATE END DATE _____ ___/___/___ ___/___/___ (Date related service _____ ___/___/___ ___/___/___ began/Date exited _____ ___/___/___ ___/___/___ from related service) _____ ___/___/___ ___/___/___ ___________________________________________________________________________________ DO YOU WANT TO ADD WILLIE M DATA? (Y/N) N ----------------------------------------------------------------------------------F1 PROCESS SBC: ______________ DATE: ___/___/___ SIMS: ______________ ___/___/___ FOLDER: ________________ ___/___/____ ___________________________________________________________________________________ RELATED SERVICES *This will be: (1) date of Re-Evaluation Determination Report if no additional assessment was needed to determine continuing eligibility; or (2) date of the Summary of Evaluation Results and Eligibility Determination if additional assessment was required to determine eligibility. ECP-S40 Rev. 8/01 DURHAM PUBLIC SCHOOLS Exceptional Children’s Programs Health Screening Report Child’s Name: ___________________________________________ Date of Birth: ___________________ Name of Interviewer: _________________________________ Date: _______________________ Name of Person Interviewed: _______________________________ Relationship: ____________________ I. Health History Has the child had problems in any of the areas below? Explain “yes” answers. Yes No ___ ___ Frequent Earaches/Infections _______________________________________________ ___ ___ Frequent Headaches ______________________________________________________ ___ ___ Diabetes _______________________________________________________________ ___ ___ Asthma ________________________________________________________________ ___ ___ Seizures _______________________________________________________________ ___ ___ Sickle Cell Disease/Trait ___________________________________________________ ___ ___ Allergies (List) __________________________________________________________ ___ ___ Complications with Childhood Illnesses ______________________________________ ___ ___ Serious Illness __________________________________________________________ ___ ___ Serious Accident ________________________________________________________ ___ ___ Hospitalization _________________________________________________________ ___ ___ Surgery _______________________________________________________________ Other Pertinent Medical Information Medication List all medication taken on a regular basis. Name of Medication Date Prescribed Dosage ________________________________________________________________________________ ________________________________________________________________________________ ________________________________________________________________________________ ________________________________________________________________________________ ECP-S41 7/02 p.1 of 2 Name: Date: Health Screening Report (Continued) II. Developmental Milestones List approximate age at which child did the following: Sat Alone ______________________ Fed Self __________________________ Crawled ______________________ Toilet Trained _____________________ Walked ______________________ Dressed Self ______________________ Talked ______________________ Peddled Tricycle ___________________ III. Dietary Habits Approximately how many times a week does the child eat: Breakfast: _________ Lunch: __________ Dinner: ___________ Does child eat foods from the following food groups? Yes No ___ ___ Dairy products ___ ___ Meat ___ ___ Fruits and vegetables ___ ___ Breads and cereals ___ ___ Does your child eat sweets frequently? ___ ___ If yes, does it interfere with or substitute for meals? IV. Physical Condition (To be completed by school nurse) Height _____________________ Blood Pressure ___________________________ Weight _____________________ Pulse ___________________________________ Teeth Respirations _____________________________ _____________________ General Physical Condition _____________________________________________________ Referral for a medical evaluation (circle one): Yes No ___________________________________ Nurse’s Signature and Date ECP-S41 7/02 p.2 of 2 Durham Public Schools Programs for Exceptional Children SEPARATE DATABASE CODES AND EXPLANATIONS Column Title Explanation School Present school assignment Teacher Current EC teacher Name Student’s legal name (Last, First, MI) Date of Birth Year, day, month (e.g., 86/27/03) Age As of today’s date Ethnicity Use SIMS codes Sex Male or Female Exceptionality Area of eligibility as checked on IEP Setting Level of service Street number Street Apartment number Zip code Most current home address available Class Type of classroom where the student is receiving EC services (BED, EMD, AU, MU, SP, TMD, MC, SLD, HI) 0_- 0_ Grade level for this school year Home School To be completed by EC Central Services Grade 0_- 0_ Projected grade level for next school year Last Column* Note whether student is due to graduate or age out of the program *This column to be completed by high school teachers only! PLEASE COMPLETE ANY MISSING INFORMATION! FILL IN ALL BLANKS EXCEPT FOR “HOME SCHOOL” 15-15 WORKSHEET E C A D D / C H A N G E S T U D E N T I N F O R M A T I O N STUDENT NAME:__________________________ YEAR___/___ EXIT DATE ___/___/___ STUDENT # ____________________ EXIT CODE_________________________ REFERRAL/RE-EVALUATE DATE ___/___/___ THIRD YEAR RE-EVALUATION (Y/N) ? ___Y___ N PERMISSION/NOTICE EVALUATE ___/___/___ (Parent Permission to Eval. Or Re-Eval.) SCREENINGIEVALUATION: S-Procedures/EH ___/___/___ E-Educational ___/___/___ S-Procedures/LD ___/___/___ E-IQ/Aptitude %ile ___/___/___ S-Health ___/___/___ E-Medical ___/___/___ S-Hearing ___/___/___ E-Ophthal/Optometric ___/___/___ S-Multidisc. Team ___/___/___ E-Otological ___/___/___ S-Psychomotor ___/___/___ E-Performance on Grades ___/___/___ S-Speech-Language ___/___/___ E-Psychological ___/___/___ S-Vision ___/___/___ E-Psychomotor ___/___/___ E-Adaptive Beh. ___/___/___ E-Review Early History ___/___/___ E-Audiological ___/___/___ E-Social/Dev. Hist ___/___/___ E-Beh/Emotional ___/___/___ E-Speech-Language ___/___/___ E-Cognitive ___/___/___ ___________________________________________________________________________________ WRITTEN SUMMARY OF EVALUATION TO PARENT/S ___/___/___ SBC DETERMINATION OF ELIGIBILITY ___/___/___(Date of eligibility determination)* APC DECISION FOR PLACEMENT ___/___/___(Date of IEP completion) INITIAL PLACEMENT (Y/N) ? ___Y___ N ___/___/___ PARENTAL CONSENT FOR PLACEMENT ___/___/___ PRIMARY EXCEPTIONALITY _______ SERVED DATE ___/___/___(Date IEP service begins in each LEA) STUDENT SETTING _______ BEGIN DATE END DATE FIRST IEP ___/___/___ ___/___/___ SECOND IEP ___/___/___ ___/___/___ THIRD IEP ___/___/___ ___/___/___ ___________________________________________________________________________________ EC IDENTIFIER CODE [computer]__ EC TEACHER [blank]__ IDENTIFICATION MATRIX _________ STATE OPERATED PROGRAM _________ COMPLIANCE OVERRIDE ___S___ ENTITLED (Y/N)? ___Y ___N LEGALLY BLIND (Y/N) ___Y ___N VISUAL ACUITY L _____ (Do Not complete R _____ if answer is "no") VISUAL ACUITY CODE L _____ R _____ READING MEDIUM CODE _____ (S-System, C-Compliant, N-Not Compliant) CODE BEGIN DATE END DATE _____ ___/___/___ ___/___/___ (Date related service _____ ___/___/___ ___/___/___ began/Date exited _____ ___/___/___ ___/___/___ from related service) _____ ___/___/___ ___/___/___ ___________________________________________________________________________________ DO YOU WANT TO ADD WILLIE M DATA? (Y/N) N ----------------------------------------------------------------------------------F1 PROCESS SBC: ______________ DATE: ___/___/___ SIMS: ______________ ___/___/___ FOLDER: ________________ ___/___/____ ___________________________________________________________________________________ RELATED SERVICES *This will be: (1) date of Re-Evaluation Determination Report if no additional assessment was needed to determine continuing eligibility; or (2) date of the Summary of Evaluation Results and Eligibility Determination if additional assessment was required to determine eligibility. ECP-S40 Rev. 8/01 DURHAM PUBLIC SCHOOLS Exceptional Children’s Programs Health Screening Report Child’s Name: ___________________________________________ Date of Birth: ___________________ Name of Interviewer: _________________________________ Date: _______________________ Name of Person Interviewed: _______________________________ Relationship: ____________________ I. Health History Has the child had problems in any of the areas below? Explain “yes” answers. Yes No ___ ___ Frequent Earaches/Infections _______________________________________________ ___ ___ Frequent Headaches ______________________________________________________ ___ ___ Diabetes _______________________________________________________________ ___ ___ Asthma ________________________________________________________________ ___ ___ Seizures _______________________________________________________________ ___ ___ Sickle Cell Disease/Trait ___________________________________________________ ___ ___ Allergies (List) __________________________________________________________ ___ ___ Complications with Childhood Illnesses ______________________________________ ___ ___ Serious Illness __________________________________________________________ ___ ___ Serious Accident ________________________________________________________ ___ ___ Hospitalization _________________________________________________________ ___ ___ Surgery _______________________________________________________________ Other Pertinent Medical Information Medication List all medication taken on a regular basis. Name of Medication Date Prescribed Dosage ________________________________________________________________________________ ________________________________________________________________________________ ________________________________________________________________________________ ________________________________________________________________________________ ECP-S41 7/02 p.1 of 2 Name: Date: Health Screening Report (Continued) II. Developmental Milestones List approximate age at which child did the following: Sat Alone ______________________ Fed Self __________________________ Crawled ______________________ Toilet Trained _____________________ Walked ______________________ Dressed Self ______________________ Talked ______________________ Peddled Tricycle ___________________ III. Dietary Habits Approximately how many times a week does the child eat: Breakfast: _________ Lunch: __________ Dinner: ___________ Does child eat foods from the following food groups? Yes No ___ ___ Dairy products ___ ___ Meat ___ ___ Fruits and vegetables ___ ___ Breads and cereals ___ ___ Does your child eat sweets frequently? ___ ___ If yes, does it interfere with or substitute for meals? IV. Physical Condition (To be completed by school nurse) Height _____________________ Blood Pressure ___________________________ Weight _____________________ Pulse ___________________________________ Teeth Respirations _____________________________ _____________________ General Physical Condition _____________________________________________________ Referral for a medical evaluation (circle one): Yes No ___________________________________ Nurse’s Signature and Date ECP-S41 7/02 p.2 of 2 DURHAM PUBLIC SCHOOLS Exceptional Children’s Programs MODIFIED TEXTBOOK ORDER FORM For Use by VI Staff Only Date Submitted: _______________________________ School: _____________________________________ School Contact*: _______________________________ Student’s Name: _______________________________ Student’s EC Placement: _______________________________ Date order placed: _________________________ Date order sent to school: _________________________ Modifications Available: A = Audio Cassette, B = Braille, L = Large Print Quantity Textbook Title Grade Level Publisher * The School Contact is responsible for receiving and returning these materials. ECP-F9 7/02 Copyright Date ISBN # Mod. Needed FOR DELIVERY TO THE RECORDS CENTER, HAMLIN ROAD BOX ______ OF ______ CONTENTS: Confidential Files for Students: FROM: _________________ TO: ____________________ (Last name) (Last name) FROM (school):___________________________ ___Alpha order ___List enclosed (or previously sent by e-mail) (This form must be affixed to each box of records transferred to the records center) &&&&&&&&&&&&&&&&&&&&&&&&&&&&&&&&&&&&&&&& FOR DELIVERY TO THE RECORDS CENTER, HAMLIN ROAD BOX ______ OF ______ CONTENTS: Confidential Files for Students: FROM: _________________ TO: ____________________ (Last name) (Last name) FROM (school):___________________________ ___Alpha order ___List enclosed (or previously sent by e-mail) (This form must be affixed to each box of records transferred to the records center) State Forms State Forms and Directions for Use DEC/Prior Notice Invitation to Conference/Prior Notice DEC 1/Prior Notice Exceptional Children Referral DEC 2/Prior Notice Prior Notice and Parent/Guardian Consent for Evaluation/Reevaluation DEC 3/Prior Notice Summary of Evaluation Results and Eligibility Determination DEC 3(a)/Prior Notice Eligibility Report/Specific Learning Disabilities (Revised 8/01) DEC 3(a) –alt/Prior Notice Eligibility Report/Specific Learning Disabilities Alternative Discrepancy Revised (8/01) DEC 3(b)/Prior Notice Eligibility Report – Behaviorally Emotionally Disabled DEC 3(c)/Prior Notice Eligibility Report – Other Health Impaired DEC 4 Individualized Education Program (IEP) NCTP/Table 1 NC Testing Program: Tests Required for Graduation NCTP/Table 2 NC Testing Program: Grades 3-8 NCTP/Table 3 NC Testing Program: Grades 9-12 DEC 5/Prior Notice Prior Written Notice DEC 6/Prior Notice Prior Notice and Consent for Initial Placement for Special Education Services DEC 7/Prior Notice Reevaluation Determination Report Note: Copies of Spanish-language forms can be obtained from the EC Facilitator. Rev. 7/02 16-1 Directions for DEC 3(a)/Prior Notice Eligibility Report/Specific Learning Disabilities This form must be completed by the LD Eligibility Team as part of (and at the same time as) the Eligibility Determination (DEC 3/Prior Notice) whenever Specific Learning Disabilities (SLD) is being considered as an area of eligibility. This form must be completed under the following circumstances: • Initial placement in LD • Reevaluation resulting in change of label to LD from another area of identification (e.g., SI) • Change in area of eligibility is considered (e.g., adding reading comprehension) • Reevaluation when new ability and achievement testing are obtained (it is not good practice to use data more than one year old to calculate discrepancies) The date on the DEC3(a) must be the same as the date on the corresponding DEC3. The DEC3(a) is to be attached to the DEC 3. A copy of the DEC 3(a) must be given to the parent along with the DEC 3. This revised DEC 3(a) (effective August 2001) represents changes to the prior version in order to reflect federal law that requires identification in one or more of the seven areas of learning disabilities (e.g., reading comprehension and basic reading but not broad reading). There is also an increased emphasis on documenting information processing difficulties which reflects current research and thought. Although there is no separate specific section to describe observational data, the team’s written report must include “the relevant behavior noted during the observation of the child” and “the relationship of that behavior to the child’s academic functioning.”(300.543) This information can be included in Sections A, C, and/ or D. Section A: Information Processing Section A allows the team to determine if there is evidence of a processing difficulty. The team considers each of the three items (#1-2-3) related to processing difficulties. If a processing difficulty is not found, document this by writing “none found.” If a processing difficulty is found, describe the learning behaviors associated with that processing difficulty. Sources of evidence of a processing difficulty include, but are not limited to, observations of the student engaged in learning, data from evaluations, outcomes from focused interventions, and work samples. Section B: Ability-Achievement Discrepancy Write the name of the general ability instrument and the ability standard score (e.g., Full Scale IQ, General Cognitive Abilities, Broad Cognitive Abilities, etc.) in this section. When there is a Verbal/Performance IQ discrepancy of at least 20 points on the Wechsler scale, the higher scale IQ may be used to determine the ability/achievement discrepancy if evidence is documented that the higher score accurately reflects the student’s intellectual functioning. Section C: Alternative Discrepancy If the team determines that the standardized assessment data do not accurately reflect a substantial discrepancy, place a check mark at C and complete the DEC 3(a)-alt/Prior Notice. Any time an alternative discrepancy is used there must be compelling documentable justification. Section D: Substantial Learning Difficulties The evidence may address observational data, grades, learning rate, basic skills for learning and concept development. Appropriate interventions should reflect interventions designed to address the concerns noted in the SAP referral. Section E: Other Impacting Factors These factors may exist concomitantly with a Specific Learning Disability. However, if the team determines that a factor is the primary cause of the student’s disability, the student may not be identified as having SLD. Section F: SLD Eligibility Check each SLD area that the student meets eligibility criteria. Each member of the LD Eligibility Team indicates whether he/she agrees or disagrees on the DEC 3. If the student is not found to be eligible in any area, check ( ) not eligible. For more information, see “Specific Learning Disabilities Eligibility” in Section 2 of this manual.







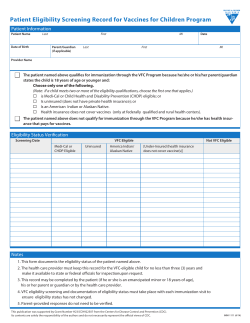


© Copyright 2026