
The MDM2 Oncogene Overexpression in Chronic
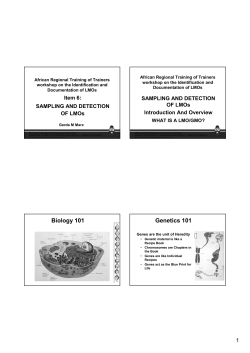
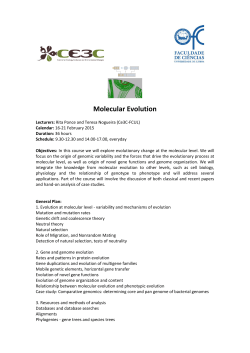
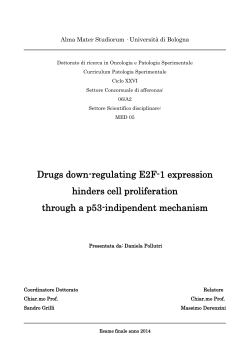
From www.bloodjournal.org by guest on February 11, 2015. For personal use only. The MDM2 Oncogene Overexpression in Chronic Lymphocytic Leukemia and Low-Grade Lymphoma of B-Cell Origin By Takashi Watanabe, Tomomitsu Hotta, Atsushi Ichikawa, Tomohiro Kinoshita, Hirokazu Nagai, Toshiki Uchida, Takashi Murate, and Hidehiko Saito The expression of the murine double minute-2 (MDMZ)gene, the product of which binds to and inactivates p53,was studied in 60 patients with B-cell chronic lymphocytic leukemia (B-CLL) or non-Hodgkin's lymphoma (B-NHL). Northern blot analysis showed that the level of MDMZ gene expression was low in normal human B-cells, whereas 17 theof patients (28.39/0)with B-CLLorNHL had more than 10-fold higher levels of MDM2 gene expressionthan that observed in norMDMZ mal B cells. Immunohistochemical analysis confirmed overexpression at the cellular proteinlevel. MDMZ gene overexpression was found more frequentlyin patients with the low-grade typeof lymphoma (56.5%)than in those with intermediate-/high-gradetypes(10.8%) (P = .M11). Moreover, MDMZ overexpression was found significantly more frequently in patients at advanced clinical stages. Simultaneous analysis of p53 gene mutation showed that three patients had both MDM2 gene overexpression and p53 gene mutation. Theresults of the presentstudysuggest that MDMZ gene overexpression may play an important role in the tumorigenicity and/or disease progression of CLL and low-grade lymphomasof B-cell origin. 0 1994 by The American Society of Hematology. A gene." Overexpression of this gene has been shown to confer tumorigenic properties on transfected murine cells: but thus far overexpression of human MDM2 gene has been reported only in sarcoma'' and breast carcinoma cell lines." Mutations of the p53 gene have been reported frequently in several types of However, in hematologic disorders, this mutation appears to be limited to blastic crisis of chronic myelogenous leukemia," some acute lymphocytic leukemias2' and lymphomas,2',22and a few cases of myelodysplastic syndrome.2' The human MDM2 gene is localized to chromosome 12q13-14"; chromosome 12 appears to be altered in many patients with ~ a r c o m a ~and ~ - *also ~ in some with chronic lymphocytic leukemia of B-cell origin (B-CLL) (21% to 62%)27-32 or low-grade lymphoma (8% to 25%).'3,34 We speculated that MDM2 gene alteration and/or overexpressionmayplay a role in the tumorigenicity of B-cell lymphoproliferative disorders. In the present study, we performed Southern blot analysis in patients with B-CLL and Bcell non-Hodgkin's lymphoma (B-NHL) to examine whether this gene was amplified or rearranged, and we performed Northern blot analysis and immunohistochemical analysis to examine the expression of the gene. We simultaneously analyzed p53 gene alterations of the same specimens by polymerase chain reaction-mediated single-strand conformation polymorphism (PCR-SSCP) and by a direct sequencing technique. CELLULAR phosphoprotein (apparent molecular mass, 90 kD), capable of forming specific complexes with p53,' has recently been characterized and identified as a product of the murine double minute-2 (MDM2) gene.2This gene was originally identified and cloned on the basis of its amplificationin a highly tumorigenic derivative of NIH3T3 cells.',4 Although the precise biochemical nature of the product remains to be determined, the deduced amino acid sequence contains a putative nuclear localization signal, as well as two zinc finger proteins, which suggests that it is a DNA binding protein. This gene also contains an acidic domain often found in transactivators and is evolutionarily conserved, as is the p53 gene." These findings suggest that this gene provides a fundamental cellular function. On the other hand, an excess of MDM2 protein can abrogate transcriptional activation by the transfected wild-type ~ 5 3Hence, . ~ the MDM2 product has been implicated as a functionally negative regulator of p53, the overexpression of which may mimic the effects brought about by mutational inactivation of the p53 gene. High levels of the MDM2 gene product can also bind and inactivate the p53 protein in ways similar to those shown by some DNA viral gene products, such as simian virus 40 T antigen, adenovirus ElB, and human papilloma virus E6.5-9However, the MDM2 protein can bind to both mutant- and wild-type p53 proteins.',* Thus, MDM2 gene overexpression may provide a mechanism of p53 inactivation that differs from p53 mutations in human cancers. The human homologue of the murine MDM2 gene has been cloned, and more than one third of 47 human sarcomas examined were found to exhibit amplification of the MDM2 From the First Department of Internal Medicine, Nagoya University School of Medicine, Nagoya, Japan. Submitted October 5, 1993; accepted July 1 1 , 1994. Supported in part by Grants-in-Aidfor Cancer Research from the Ministry of Health and Welfare of Japan. Address reprint requests to Takashi Watanabe, MD,First Department of Internal Medicine, Nagoya University School of Medicine, 65 Tsurumai-rho, Showa-ku, Nagoya 466, Japan. The publication costsof this article were defrayedin part by page chargepayment. This article must therefore be hereby marked "advertisement" in accordance with 18 U.S.C. section 1734 solely to indicate this jact. 0 1994 by The American Society of Hematology. 0006-4971/94/8409-07$3.00/0 31 58 MATERIALS AND METHODS Patient characteristics. We analyzed 60 consecutive patients, 17 with B-CLLkmall-cell lymphocytic lymphoma (SCL) and 43 with B-cell lymphoma other than SCL (follicular type, n = 8; diffuse type, n = 35). who were admitted to our hospital between April 1986 and March 1993, including nine patients with CLL who were treated in our affiliated hospitals, and whose RNA was available for Northern blot analysis. The diagnosis of CLL was based on the criteria proposed by the International Workshop on CLL?5 and three of the 17 B-CLL patients were histologically diagnosed as having SCL at lymph node biopsy. Histologic and surface marker studies using an immunohistochemical technique showed B-cell phenotype in all examined patients. The characteristics of these patients are listed in Table 1. Fifty of 60 patients were untreated, but 10 patients had received a variety of prior treatments. Patients with CLL were classified according to a revised prognostic staging system as proposed by the International Workshop on CLL, which encompasses features of boththe Rai and the Binet systems.16 The Modified Blood, Vol 84, No 9 (November l ) , 1994: pp 3158-3165 From www.bloodjournal.org by guest on February 11, 2015. For personal use only. 3159 MDMZ OVEREXPRESSION IN LOW-GRADELYMPHOMA Table 1. Characteristics of 60 Patients With B-CLL or B-NHL No. of Patients Age (yr) Median Range Sex (M/F) Untreated/treated Clinical stage of CLL A (0) A (1) B (1) c (111) c (IV) 60 51 15-86 40120 50/10 4 1 3 4 5 Clinical stage of N H L (except SCL) I I1 111 IV Histopathology for N H L (modified Working Formulation) Low grade Small lymphocytic (including CLL)' Follicular small cleaved Follicular mixed Intermediate/High grade Follicular large Diffuse small cleaved Diffuse mixed Diffuse large Diffuse larae, - . immunoblastic 0 9 11 23 17 4 2 2 7 4 23 1 The staging system of the International Workshop on CLL was applied to 17 patients withCLUSCL.Roman numerals in parentheses represent the Rai classification. The histopathologic categow of small lymphocytic consisted of three small lymphocytic lymphomas and 14 CLLs diagnosed according to the clinical criteria. Working Formulation Classification was applied for histologic classification ofthelymphomas."DNAand RNA samples were extracted from peripheral blood lymphocytes (PBL), lymph nodes (LN), extranodal tumors, or pleural effusions filled with lymphoma cells. Mononuclear cells isolated by Ficoll-Paque (Pharmacia, Piscataway, NJ) gradient centrifugation were substituted for PBL. LN and extranodal tumors were obtained at biopsy performed for diagnosis after informed consent was obtained. Control specimens. As normal controls, we used DNA and RNA obtained from the PBL of healthy volunteers, from the spleen excised from a patient with gastric cancer, and from the LN of patients with reactive lymphangitis. The excised spleen was depleted of monocytes/macrophages by incubation at 37°C for 1 hour with 10% silica particles (KAC-2; JIMRO, Takasaki, Japan), and subsequently mononuclear cells were isolated by Ficoll-Payue gradient centrifugation. B cells were then enriched by depleting T cells through rosetting with sheep erythrocytes (Kyokuto, Tokyo, Japan)," yielding splenic B-cells as a control. LN of reactive lymphangitis patients were obtained at biopsy performed for diagnosis. MDM2 probe. The MDMZ probe was produced by PCR,39 using cDNA from normal human PBL as a template. The DNA was amplified with the following primers: 5'-CCTGTGTGTCGGAAAGAT3' and 5'-CTGCTACTGCTTCTMl2A-3'. The 91l-bp MDM2 probe spanned nucleotides -273 to +638 of the published cDNA sequence of the human MDM2 gene." The oligonucleotide primers used were synthesized by the phosphoroamide method with a 391 DNA synthe- sizer (Applied Biosystems, Foster City, CA), and were purified with OPC columns (Applied Biosystems). Preparation of DNA and RNA. DNAwas prepared by the method reported previously.'"' Alltissues and cell samples used were homogenized in guanidine isothiocyanate, and total cellular RNA was extracted as described previously?' After phenol and chloroform extraction, RNA was precipitated in ethanol for storage. Southern blotting. Five micrograms of each DNA was digested with several different restriction enzymes such as EcoRI, BamHI, HindIII, and PvuII (Boehringer Mannheim, Mannheim, Germany), and then separated by 1% agarose gel electrophoresis and transferred to nylon membranes (Genescreen Plus, Biotechnology Systems, Boston, MA) as described previously!2 The membranes were hybridized to the human MDMZ probe; hybridization was performed as previously described.43 Northern blotanalysis. Denatured RNA samples (10 pg total cellular RNA per lane) were separated by electrophoresis in 3-(NMorpho1ino)propanesulfonic acid formaldehyde 1% agarose gels, transferred to Hybond N membranes (Amersham, Buckinghamshire, UK), and analyzed by Northern blot hybridization. Transfer and hybridization were performed as described previously,44except that Quickhyb (Stratagene, La Jolla, CA) wasused for hybridization. The quality of the RNA was verified by noting the integrity of the 28s and 18s ribosomal RNA stained by ethidium bromide. Hybridization was performed to the human MDM2 probe, andall blots were boiled and subsequently rehybridized to a @-actinprobe, which provided a qualitative and quantitative control for RNA preparations. Quantijcation of expression and amplification. To determine the levels of expression and amplification of the MDM2 gene, we exposed the blots to phosphor imaging plates (Imaging plate BAS 111, Fuji, Japan), which were subsequently studied with a laser image analyzer (FUJIX BAS2000, Fuji, Japan). We then calculated the intensity of phosphostimulated luminescence (PSL) of the bands on the blots, since PSL is proportional to the absorbed radioactive energy. These methods have been described in detail el~ewhere.~' Concerning gene amplification, the signal of each specimen was compared with that of the control splenic B cells. Zmmunohistochemical analysis. Immunohistochemical analysis was performed on cytospin preparations, using the IgGzb mouse monoclonal antibody (MoAb) IF2 (Oncogene Science, Uniondale, NY), which specifically recognizes the terminal epitope of human MDMZ protein.& We made the cytospin preparations with cytospin 2 (Shandon, Pittsburgh, PA), either immediately after sampling or thawing cell suspensions of peripheral blood and LN, which were frozen with20% fetal calf serum and 10% dimethyl sulfoxide (DMSO) in liquid nitrogen and stored at -80°C. The slides were fixed in 4% paraformaldehyde (PFA) in phosphate-buffered saline (PBS) overnight at 4°C following in 100% ethanol for more than 2 hours at -2O"C, and washed in PBS before labeling. After endogeneous peroxidase was quenched by a 2-hour incubation in 0.5% hydrogen peroxide, the slides were incubated first with goat normal serum for 30 minutes, then with the MoAb IF2 diluted in PBS (5 pg/mL) containing 1% bovine serum albumin overnight at 4"C, then with a goat antimouse immunoglobulin for 1 hour, andfinallywiththe peroxidase-antiperoxidase complex (Medical Biological Laboratories, Nagoya, Japan) for 1 hour. The enzymatic color reaction was developed with 3,3'-diaminobenzidine (Sigma, St Louis, MO). Peroxidase activity was visualized as a brown reaction product, and slides were counterstained with Mayer's hematoxylin. Analysis of the p53 gene by PCR-SSCP and direct sequencing. To detect whether p53 gene alterations were present in the60 patients in whomMDMZ expression was examined, we analyzed the genomic DNAof exons 5 through 9 by PCR-SSCP, andthen studied the sequences of the bands showing a mobility shift by a direct sequencing technique. Half of these cases were described in the previous From www.bloodjournal.org by guest on February 11, 2015. For personal use only. WATANABE ET AL 3160 A B 1 2 3 4 1 2 3 4 5 6 7 8 9 1011 1 2 1 3 V MDM2 --C m - 28s P-actin "c Fig 1. (A) Expression of MDM2 mRNA in normal human lymphocytes. Total cellular RNA (10 p g ) was size-fractionated by electrophoresis and analyzed by blot hybridization. (Lane 1) PBL of a normal healthy volunteer; (lane 2) normal splenic B-cells; (lanes 3 and 4) LN of reactive lymphangitis patients. Arrows show the position of the transcripts of MOM2 or of pactin. (B) Overexpression of the MDM2 gene in patients with B-NHL in relation to subgroup of the Working Formulation classification. Northern blot analysis of total cellular RNA (10 pg). (Lane 1) Positive control, MT-2 cells; (lane 2) normal splenic B cells; (lanes 3 to 9) NHL, diffuse type; (lanes 10 to 13) NHL, follicular type. report,*' and we added data from 30 new patients whose RNA was available for Northern blot analysis. PCR-SSCP and direct sequencing were performed as described previously." RESULTS MDM2 gene expression in normal B cells. To determine the extent of M D M 2 gene expression in normal and reactive lymphocytes, we performed Northernblot analysis of the PBL of healthy volunteers, the splenic B cells, and the reactive B cells separated from the LNof four patients with reactive lymphangitis. These cells showed a single 5.5-kb transcript, in accordance with previous reports,"'but their bands were all faint. The level of the transcript in splenic B cells was as low as that of the PBL from healthy volunteers. However, levels in reactive lymphangitis LN were1.2- to 1.8-fold higher than those in PBL or splenic B cells (Fig 1A). Overexpression of the MDM2 gene in neoplastic B cells. To our knowledge, no detailed data on the expression of the M D M 2 gene in human lymphoid cells have been reported to date. We first performed a preliminary study in which we examined the levels of M D M 2 RNA in several human cell lines; we found that the M D M 2 gene was overexpressed in MT-2 cells, a T-cell line derived from human cord leukocytes by cocultivation with T cells infected with human Tcell leukemia virus type I (HTLV-I)?' The level of MT-2 RNA expression was 15- to 20-fold higher than that in normal human B cells (Fig IB). We therefore used this cell line as a positive control. We next investigated whether the M D M 2 gene was expressed in neoplastic B cells of NHL (Fig 1B) and CLL (Fig 2). The expression of this gene in the 60 patients varied; 17 of 60 patients withNHL or CLL (28.3%) were found to overexpress the gene at levels more than IO-fold higher than that observed in normal splenic B cells, and 19 showed twofold to fivefold higher expression than that in normal B cells. Ampl8cation or rearrangement of the MDM2 gene. To whether overexpression Of the MDM2 gene from its amplification or its alteration. we analyzed the P o mic DNA of 60 patients by Southern blot analysis. However, none of the patients who showed M D M 2 gene overexpression appeared to have either amplification or rearrangement of the M D M 2 gene. MDM2 expression at the cellularprotein level. To evaluate M D M 2 expression at the cellular protein level, we first examined proteins derived from MT-2. the cell line which was shown to overexpress the M D M 2 gene by Northern blot analysis. A strong exclusively nuclear signal was observed in MT-2 cells immunostained with the IF-2 MoAb (Fig 3A). The nuclear localization of M D M 2 is consistent with previous studies of mouse cells4* and the previous reportthat human M D M 2 contains a nuclear localization signal."' This MoAb was then used to stain the specimens in which M D M 2 RNA was analyzed. Those specimens that showed levels of M D M 2 RNA lower than IO times those of normal B cells showed no or very weak staining of lymphoma cells (Fig 3B). We examined almost all specimens in which levels of M D M 2 RNA were more than IO-fold higher than those of normal splenic B cells, and found that leukemic or lymphoma cells with strong atypical nuclei .(ie, irregular shaped or accompanied with clear nucleoli) stained strongly in all cases (Fig 3C). Overexpression of the MDM2 gene in relation to sub- 1 2 3 4 5 6 7 8 Fig 2. Overexpression of the MDM2 gene in patients with B-CLL compared with normal splenicBcells. Northern blot analysisof total cellular RNA (10 *g) (Lane 1) Control splenic B cells; (lanes 2 to 8 ) PBL from patients with CLL. From www.bloodjournal.org by guest on February 11, 2015. For personal use only. MDMZ OVEREXPRESSION IN LOW-GRADE LYMPHOMA 3161 I Fig 3. Immunohistochemical detection of MDM2 protein in cytospin preparations. (A)MT-2 cells [positive control) steined with antiMDM2 entlbody. MDM2 was localized to the nucleus as expected (brown). (B) Absence of MDMstaining in a specimenwithout MDM2 RNA overexpression. Nuclei were counterstained with hematoxylin (light blue). (C) MOM2 staining of malignant cells in a specimen (case no. 2; PEL) with increased MDM2 RNA more than 10-fold thet in normal B cells. Note the localhation of positive staining within the atypical nuclei, irregular shaped or accompenied with clear nucleoli. (Original megnification x 400.1 groups of the Working Formulation cZassijication. Overexpression of the MDM2 gene was definedas levels more than 10-fold higher than those in normal human B cells; of 17 patients with MDM2 gene overexpression,eight were classi- fied as B-CLL/SCL (47.1%) and nine were B-NHL non-SCL (20.9%): five follicular type (62.5%) and four diffuse type (11.4%).Weexamined the relationshipbetween MDM2 of mature B-cell neoplasm; overexpression and the subtypes From www.bloodjournal.org by guest on February 11, 2015. For personal use only. WATANABE ET AL 3162 Table 2. Overexpression of the MDM2 Gene in Relationto Subgroups of the Modfiecl Working Formulation Classification Subgroup MOM2 Gene Overexpression* f Total Low Grade IntermediateIHigh Grade 13 (56.5%)t 10 4 ( 10.8%) 33 23 37 "+" for MDM2 gene overexpression indicates levels more than 10-fold higher than those in normal splenic B cells; "-"indicates levels of MDM2 expression lower than 10 times those observed in normal splenic B cells. t MDMZ overexpression was found in 13 of 23 patients with lowgrade type (56.5%)and in four of37 patients with intermediate-/highgrade type of lymphoma (10.8%).This difference was highly significant ( P = ,001). MDM2 gene overexpression was significantly more frequent in patients with the low-grade type (56.5%) than in those with the intermediate-high-grade types of lymphoma (10.8%) ( P = .001) (Table 2). Overexpression of the MDM2 gene in relation toadvanced clinical stage. We examined the relationship between MDM2 gene overexpression and the clinical stage of CLL and NHL. When the clinical stage classification proposed by the International Workshop on CLL was applied to the 17 patients with CLUSCL, overexpression of the MDM2 gene was found significantly more frequently in patients at stage C than in those at stages A or B ( P < .03). All but one NHL patient with MDMZ gene overexpression was at clinical stage IV. Overexpression of MDM2 gene was found significantly more frequently in patients at clinical stage IV than in those at clinical stages I1 or III ( P < .05) (Table 3). Overexpression of the MDM2 gene and p53 gene alterations. We analyzed the genomic DNA of the p53 gene by PCR-SSCP and a direct sequencing technique, and found that 11 of 60 patients showed p53 gene alterations. Of17 patients with MDM2 gene overexpression, 14 had the wildtype p53 gene and three had mutant-type. The histologic diagnosis of each case was SCL, diffuse mixed, and diffuse large-cell type. Among three patients with both MDM2 overexpression and the p53 mutation, two had the same mutation in exon 6 and the other had a mutation in exon 7. Codon 216 to 218 (Val) deletion was identified in two patients, while the third patient had a point mutation at codon 248 (CGG .-+TGG, Arg Trp) (Table 4). "f DISCUSSION The widespread expression of the MDM2 gene in many murine and human tissues was investigated, and it was shown that the level of expression appeared to be different in different tissues!'49 However, human lymphoid tissues were not examined in these previous studies. The present study showed that human splenic B cells, as well as normal PBL, expressed low levels of MDM2. In addition, the level of expression was slightly less than twofold enhanced in reactive B cells relative to that in normal splenic B cells. The levels of gene expression in the specimens from NI" and CLL patients were various. As there were no previous basic data concerning B cells, it remains unknown how much expression of the MDM2 gene in B cells is morbid state. It has only been demonstrated that the MDM2 gene induced tumorigenicity in MDM2 transfectants when overexpressed at levels 10- to 15-fold higher than those in NIH-3T3 cells before transfection! Therefore, we speculated that at least those B cells that had levels more than 10-fold higher than those of control B cells might be tumorigenic, and thus defined overexpression of the MDM2 gene tentatively as levels in excess of 10 times those in normal human B cells. If significant proportions of normal cells were present in the specimens, the levels of MDM2RNAmay be underestimated, so MDM2 might play arole in some of the 19 patients who showed twofold to fivefold higher MDM2 expression than normal B cells. A strong exclusively nuclear immunopositive signal was observed with the MoAb IF2 in leukemic or lymphoma cells in all cases in which levels ofMDM2 RNA were more than 10-fold higher than those of normal splenic B cells. However, strong staining of lymphoma cells was not found in those cases in which levels ofMDM2 transcript were lower than 10 times those of normal B cells. From the results of immunohistochemical analysis, levels of MDM2 RNA correlated well with levels of MDM2 protein. Thus, we hypothesized that overexpressed MDM2 protein may bind to p53, and consequently play a role in the pathogenesis andor disease progression of patients who overexpress the MDM2 RNA via inactivation of p53. Figure 3C shows thatmost leukemic cells are MDM2positive; however, it shows that a fair number of cells do not stain with the anti-MDM2 antibody. According to a morphologic examination, it may be true that some leukemic cells were very weak or negative in MDM2 expression. We can provide two reasons for these negative cells. First, the previous report showed that MDM2 levels increased in the late G1-phase of the cell cycle:* and so, if malignant cells have the diversity in their cell cycles, all malignant cells may not have to be strongly stained with the antibody. Second, we Table 3. Overexpreuion of the MDMZ Gene According to Clinical Stage Clinical Stage of NHL Clinical Stage of CLL MOM2 Gene Overexpression + - NB 1 8t 7 15 C 111111 7 2 l* 19 IV Patients with B-CLL were classified according to the staging system proposed by the International Workshop on CLL. MDM2 overexpression was found in one of eight patients (12.5%)at clinical stage A or B and in seven of nine patients (77.7%)at clinical stage C. This difference was highly significant ( P < .03).MDM2overexpression was found in one of 20 NHL patients (5.0%) at clinical stage II or 111 and in eight of 23 patients (34.8%)at clinical stage IV. This difference was also highly significant ( P < .05). * One patient with follicular lymphoma at clinical stage 111. t Eight consisted of fourpatients with follicular lymphoma and four patients with diffuse lymphomaat clinical stage IV. From www.bloodjournal.org by guest on February 11, 2015. For personal use only. MDM2 OVEREXPRESSION3163 IN LOW-GRADE LYMPHOMA Table 4. p53 Genetic Analysis in 17 Patients Wkh MDMP Overexpression p53 Gene Patient No. 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 Lymphoma Type Wild-type CLL CLL CLL CLL CLL CLL CLL CLL FSC FSC FM FM DM DL DL DL Stage 6 Clinical Exon c (IV) c (IV) c (IV) c (IV) c (111) c (111) c (111) A (0) IV IV IV IV 111 IV IV 248 IV IV 6 7 Codon Nucleotide Amino Acid 216-218 GTG deletion Val deletion 216-218 Wild-type Wild-type Wild-type Wild-type Wild-type Wild-type Wild-type Wild-type Wild-type Wild-type Wild-type GTG deletion CGG TGG Wild-type Wild-type -. Val deletion Arg -+ Trp Three patients (no. 1, 14, and 15) had both MDMZoverexpression and p53 gene mutation. Patient no. 15 had a point mutation at codon 248 of the p53 gene, known as a weaker mutant. Abbreviations: FSC, follicular small cleaved; FM, follicular mixed; DM, diffuse mixed; DL, diffuse large cell. found leukemic cells with strong atypical nuclei stained with the IF-2 MoAb. The tendency that nuclei of tumor cells with strong atypia were prone to be stained was seen in other lymphoma specimens in which MDM2 RNA was overexpressed. In accordance with these observations, we found that cells that stained for strongly positive for MDM2 might tend to appear and increase in CLL and low-grade lymphoma at advanced stages. Why MDM2 gene overexpression was more frequently observed in the low-grade type of B-NHL (including CLL) than in the intermediate-high-grade types is unknown. While a previous report has shown that the MDM2 gene was amplified five-fold to 50-fold in sarcomas," none of our 60 patients showed sufficient amplification or rearrangement to explain the more than 10-fold increase in expression of the MDM2 gene. We speculate that the observed abnormal expression of the MDM2 gene may result from aberrations in some as yet undetermined regions that control the expression, or from aberrations in some undefined protein that regulates the expression of the MDM2 gene. MDM2 overexpression was detected more frequently in patients in advanced clinical stages of these diseases (stage C of CLL and stage IV of NHL). Our data are consistent with previous reports that showed that p53 alterations were found more frequently in patients at advanced clinical stage of the disease,*' and p53 and MDM2 presumably affect the same pathway in B-cell neoplasms. The proportion of neoplastic B cells in the PBL of patients with B-CLL was 70% to 90%,and there were no differences between groups A/B versus C. Thus, it was clear that the difference in expression did not result from the proportion of tumor cells in PBL. Five of 17 patients who showed MDM2 overexpression had received previous treatments: all four patients with diffuse lymphoma and one of eight with CLL. In these cases, we were not able to exclude the influence of chemotherapy, which could cause DNA damage and subsequent alterations in the pathway of p53 to maintain genomic stability. As the result of high levels of MDM2 gene expression is known to be functionally synonymous with mutant-type p53 protein, and the p53 mutation is rarely observed in hematologic malignancies, we expected to find MDM2 overexpression in patients who lacked p53 alterations. A previous study showed that none of five sarcomas examined with MDM2 amplification had p53 gene mutations." However, in the present study, of 17 patients in whom wefound MDM2 overexpression, 14 had the wild-type and three the mutanttype p53 gene. Since different mutant alleles of p53 have different biologic properties, it is possible that MDM2 overexpression could also confer an added selective advantage on tumors with weaker mutant alleles, which do not bind to the cellular heat-shock protein, hsc70, and which are less efficient at forming transformed foci in culture. Indeed, one of three patients with both MDM2 overexpression and mutant-type p53 had a point mutation at codon 248, which was reported as a weaker mutant, as well as those for such residues as 273 and 281.',50 The results of the present study showed that the MDM2 gene was overexpressed in patients with some particular types of B-cell malignancies. It appears that MDM2 gene overexpression may play animportant role in tumorigenicity andor in disease progression in this type of neoplasia. However, the precise molecular mechanism underlying this overexpression is still unclear. In addition, whether MDM2 overexpression is a prognostic factor is now being investigated. Further studies will be needed before the clinical implications of these findings become clear. ACKNOWLEDGMENT We thank N. Hirabayashi, MD, and S . Goto, MD (Nagoya Second Red Cross Hospital), Y. Kagami, MD (Aichi CancerCenter), K. From www.bloodjournal.org by guest on February 11, 2015. For personal use only. 3164 Satake, MD,and H. Suito, MD (Toyohashi City Hospital) for allowing us to examine their patients with CLL. REFERENCES 1. Hinds PW, Finlay CA, Quartin RS, Baker SJ, Fearon ER, Vogelstein B, Levine A J : Mutant p53 DNA clones from human colon carcinomas cooperate with rus in transforming primary rat cells: A comparison of the “hot spot” mutant phenotypes. Cell Growth Differ 1571, 1990 2. Momand J, Zambetti GP, Olson DC, George D, Levine AJ: The mdm-2 Oncogene product forms a complex with the p53 protein and inhibits p53-mediated transactivation. Cell 69:1237, 1992 3. Cahilly-Snyder L, Yang-Feng T, Francke U, George DL: Molecular analysis and chromosomal mapping of amplified genes isolated from a transformed mouse 3T3 cell line. Somat Cell Mol Genet 13:235, 1987 4. Fakharzadeh S S , Trusko SP, George DL: Tumorigenic potential associated with enhanced expression of a gene that is amplified in a mouse tumor cell line. EMBO J 10:1565, 1991 5. Linzer DIH, Levine AJ: Characterization of a 54 K dalton cellular SV40 tumor antigen present in SV40-transformed cells and uninfected embryonal carcinoma cells. Cell 17:43, 1979 6. Lane DP, Crawford LV: T antigen is bound to a host protein in SV40-transformed cells. Nature 278:261, 1979 7. Sarnow P, Ho YS, Williams J, Levine AJ: Adenovirus Elb58kd tumor antigen and SV40 large tumor antigen are physically associated with the same 54 kd cellular protein in transformed cells. Cell 28:387, 1982 8. Werness BA, Levine AJ, Howley PM: Association of human papillomavirus types 16 and 18 E6 proteins with p53. Science 248:76, 1990 9. Vogelstein B, Kinzler KW: p53 function and dysfunction. Cell 70:523, 1992 10. Oliner JD, Kinzler KW, Meltzer PS, George DL, Vogelstein B: Amplification of a gene encoding a p53-associated protein in human sarcomas. Nature 358:80, 1992 11. Sheikh MS, Shao ZM, Hussain A, Fontana JA: The p53binding protein MDM2 gene is differentially expressed in human breast carcinoma. Cancer Res 53:3226, 1993 12. Nigro JM, Baker SJ, Preisinger AC, Jessup JM, Hostetter R, Cleary K, Bigner SH, Davidson N, Baylin S , Devilee P, Glover T, Collins FS, Weston A, Modali R, Harris CC, Vogelstein B: Mutations in the p53 gene occur in diverse human tumor types. Nature 342:705, 1989 13. Baker SJ, Fearon ER, Nigro JM, Hamilton SR, Preisinger AC, Jessup JM, van Tuinen P, Ledbetter DH, Barker DF, Nakamura Y, White R, Vogelstein B: Chromosome 17 deletions and p53 gene mutations in colorectal carcinomas. Science 244:217, 1989 14. Takahashi T, Nau MM, Chiba I, Birrer MJ, Rosenberg RK, Vinocour M, Levitt M, Pass H, Gazdar AF, Minna JD: p53: A frequent target for genetic abnormalities in lung cancer. Science 246491, 1989 15. Hollstein MC, Metcalf RA, Welsh JA, Montesano R, Harris CC: Frequent mutation of the p53 gene in human esophageal cancer. Proc Natl Acad Sci USA 87:9985, 1990 16. Hsu IC, Metcalf RA, Sun T, Welsh JA, Wang NJ, Harris CC: Mutational hot spot in the p53 gene in human hepatocellular carcinomas. Nature 350:427, 1991 17. Mashiyama S , Murakami Y, Yoshimoto T, Sekiya T, Hayashi K Detection of p53 gene mutations in human brain tumors by singlestrand conformational polymorphism analysis of polymerase chain products. Oncogene 6:1313, 1991 18. Hollstein M, Sidransky D, Vogelstein B, Harris CC: p53 mutations in human cancers. Science 253:49, 1991 19. Marshal R, Shtalrid M, Talpaz M, Kantarjian H, Smith L, WATANABE ETAL Beran M, Coek A, Trujillo J, Gutterman J, Deisseroth A: Rearrangement and expression of p53 in the chronic phase and blastic crisis of chronic myelogeneous leukemia. Blood 75: 180, 1990 20. Sugimoto K, Toyoshima H, Sakai R, Miyagawa K, Hagiwara K, Hirai H, Ishikawa F, Takaku F: Mutations of the p53 gene in lymphoid leukemia. Blood 77:1153, 1991 21. Gaidano G, Ballerini P, Gong JZ, Inghirami G, Neri A, Newcomb EW, Magrath IT, Knowles DM, Dalla-Favera R: p53 mutations in human lymphoid malignancies: Association with Burkitt’s lymphoma and chronic lymphocytic leukemia. Proc Natl Acad Sci USA 885413, 1991 22. Ichikawa A, Hotta T, Takagi N, Tsushita K, Kinoshita T, Nagai H, Murakami Y, Hayashi K, Saito H: Mutations of p53 gene and their relation to disease progression in B-cell lymphoma. Blood 79:2701, 1992 23. Sugimoto K, Hirano N. Toyoshima H, Chiba S, Mano H, Takaku F, Yazaki Y, Hirai H: Mutations of the p53 gene in myelodysplastic syndrome (MDS) and MDS-derived leukemia. Blood 81:3022, 1993 24. Mandahl N, Heim S, Willen H, Rydholm A, Eneroth M, Nilber TM, Kreicbergs A, Mitelman F Characteristic karyotypic anomalies identify subtypes of malignant fibrous histiocytoma. Genes Chrom Cancer 1:9, 1989 25. Turc-Carel C, Limon J, Dal Cin P, Rao U, Karakousis C, Sandberg AA: Cytogenetic studies of adipose tissue tumors. 11. Recurrent reciprocal translocation t(12;16) (q13;pll) in myxoid liposarcomas. Cancer Genet Cytogenet 23:291, 1986 26. Meltzer PS, Jankowski SA, Dal Cin P, Sandberg AA, Paz IB, Coccia MA: Identification and cloning of a novel amplified DNA sequence in human malignant fibrous histiocytoma derived from a region of chromosome 12 frequently rearranged in soft tissue tumors. Cell Growth Differ 2:495, 1991 27. Gahrton G, Robbrt K-H, Friberg K, Zech L, Bird AG: Nonrandom chromosomal aberrations in chronic lymphocytic leukemia revealed by polyclonal B-cell-mitogen stimulation. Blood 56:640, 1980 28. Han T, Ozer H, Sadamori N, Emrich L, Gomez GA, Henderson ES, Bloom ML, Sandberg AA: Prognostic importance of cytogenetic abnormalities in patients with chronic lymphocytic leukemia. N Engl J Med 310:288, 1984 29. Pittman S, Catovsky D: Prognostic significance of chromosome abnormalities in chronic lymphocytic leukaemia. Br J Haemato1 58:649, 1984 30. Juliusson G , RoMrt K-H, Ost A, Friberg K, Biberfeld P, Nilsson B, Zech L, Gahrton G: Prognostic information from cytogenetic analysis in chronic B-lymphocytic leukemia and leukemic immunocytoma. Blood 65:134, 1985 31. Juliusson G, Gahrton G: Chromosome aberrations in B-cell chronic lymphocytic leukemia. Cancer Genet Cytogenet 45:143, 1990 32. Juliusson G, Friberg K, Gahrton G : Consistency of chromosomal aberrations in chronic B-lymphocytic leukemia. A longitudinal cytogenetic study of 41 patients. Cancer 62:500, 1988 33. Yunis JJ, Oken MM,Kaplan ME, Ensrud KM, Howe RR, Theologides A: Distinctive chromosomal abnormalities in histologic subtypes of non-Hodgkin’s lymphoma. N Engl J Med 307:1231, 1982 34. Offit K, Wong G, Filippa DA, Tao Y, Chaganti RSK: Cytogenetic analysis of 434 consecutive ascertained specimens of nonHodgkm’s lymphoma; clinical correlations. Blood 77:1508, 1991 35. Binet E, Catovsky D, Dighiero G , Gale RP, Montserrat E, Rai KR: Chronic lymphocytic leukemia: Recommendations for diagnosis, staging, and response criteria. Ann Intern Med 110:236, 1989 36. Binet JL, Catovsky D, Chandra P, Dighiero G, Montserrat E, From www.bloodjournal.org by guest on February 11, 2015. For personal use only. MDM2 OVEREXPRESSION IN LOW-GRADE LYMPHOMA Rai KR, Sawitsky A: chronic lymphocytic leukaemia: Proposals for a revised prognostic staging system. Br J Haematol 43:365, 1981 37. Nathwani BN, Winberg CD: Non-Hodgkin’s lymphomas: An appraisal of the ‘Working Formulation” of non-Hodgkin’s lymphomas for clinical usage, in Sommers SC, Rosen PP (eds): Malignant Lymphomas: A Pathology Annual Monograph. Norwalk, CT, Appleton-Century-Crofts, 1983, p 1 38. Madsen M, Johnsen HE, Wendelboe-Hanser P, Christiansen SE: Isolation of human B and T lymphocytes by E-rosette gradient centrifugation. J Immunol Methods 33:323, 1980 39. Saiki RK, Gelfand DH, Stoffel S , Scarf SJ, Higuchi R, Horn GT, Mullis KB, Erlich HA: Primer-directed enzymatic amplification of DNA polymerase. Science 239:487, 1988 40. Blin N, Stafford DM: A general method for isolation of high molecular weight DNA from eukaryotes. Nucleic Acids Res 3:2303, 1976 41. Chomczynski P, Sacchi N: Single-step method of RNA isolation by acid guanidium thiocyanate phenol chloroform extraction. Anal Biochem 162:156, 1987 42. Reed KC, M m DA: Rapid transfer of DNA from agarose gels to nylon membranes. Nucleic Acids Res 13:7207, 1985 43. Ohashi H, Ichikawa A, Takagi N, Hotta T, Naoe T, Ohno R, Saito H: Remission induction of acute promyelocytic leukemia by all-trans-retinoic acid Molecular evidence of restoration of normal hematopoiesis after differentiation and subsequent extinction of leukemic clone. Leukemia 6:859, 1992 3165 44. Murate T, Yamashita K, Ohashi H, Kagami Y, Tsushita K, Kinoshita T, Hotta T, Saito H, Yoshida S , Mori K, Hayakawa T: Erythroid potentiating activity of tissue inhibitor of metalloproteinases on the differentiation of erythropoietin-responsive mouse erythroleukemia cell line, ELM-1-1-3, is closely related to its cell growth potentiating activity. Exp Haematol 21:169, 1993 45. Amemiya Y, and Miyahara J: Imaging plate illuminates many fields. Nature 336:89, 1988 46. Leach FS, Tokino T, Meltzer P, Burrell M, Oliner JD, Smith S , Hill DE, Sidransky D, Kinzler KW, Vogelstein B: p53 mutation and MDM2 amplification in human soft tissue sarcomas. Cancer Res 53:2231, 1993 47. Miyoshi I, Kubonishi I, Yoshimoto S , Akagi T, Ohtsuki Y, Shiraishi Y, Nagata K, Hinuma Y: Type C virus particles in a cord T-cell line derived by co-cultivating normal human cord leukocytes and human leukaemic T cells. Nature 294770, 1981 48. Olson DC, Mmchal V, Momand J, Chen J, Romocki C, Levine AJ: Identification and characterization of multiple mdm-2 proteins and mdm-2 p53 protein complexes. Oncogene 8:2353, 1993 49. Ladanyi M, Cha C, Lewis R, Jhanwar SC, Huvos AG, Healey JH: MDM2 gene amplification in metastatic osteosarcoma. Cancer Res 53:16, 1993 50. Zambetti GP, Levine AJ: A comparison of the biological activities of wild type and mutant p53. FASEB J 7:855, 1993 From www.bloodjournal.org by guest on February 11, 2015. For personal use only. 1994 84: 3158-3165 The MDM2 oncogene overexpression in chronic lymphocytic leukemia and low-grade lymphoma of B-cell origin T Watanabe, T Hotta, A Ichikawa, T Kinoshita, H Nagai, T Uchida, T Murate and H Saito Updated information and services can be found at: http://www.bloodjournal.org/content/84/9/3158.full.html Articles on similar topics can be found in the following Blood collections Information about reproducing this article in parts or in its entirety may be found online at: http://www.bloodjournal.org/site/misc/rights.xhtml#repub_requests Information about ordering reprints may be found online at: http://www.bloodjournal.org/site/misc/rights.xhtml#reprints Information about subscriptions and ASH membership may be found online at: http://www.bloodjournal.org/site/subscriptions/index.xhtml Blood (print ISSN 0006-4971, online ISSN 1528-0020), is published weekly by the American Society of Hematology, 2021 L St, NW, Suite 900, Washington DC 20036. Copyright 2011 by The American Society of Hematology; all rights reserved.









© Copyright 2026