
Autism Training - Massachusetts Behavioral Health Partnership
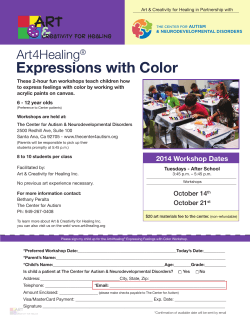
To gain a clearer understanding of the diagnoses of Autism, Asperger’s and Pervasive Development Disorder Not Otherwise Specified (PDD NOS). To learn about services and resources available through community agencies and how to successfully access and navigate these for children with autism. To learn about the most effective intervention strategies for providers, parents and families. Autism: ◦ Social language and communication deficits including both spoken and unspoken (pointing, eye contact, smiling) along with challenging behavioral traits Asperger’s Syndrome: ◦ Typically high intellect and verbal abilities, but still lack common social skills PDD NOS: ◦ Known as Pervasive Developmental Disorder-Not Otherwise Specified. Combination of traits from other categories such as trouble with social interaction, as well as difficulties in either communication or behavior Less frequently occurring disorders: Childhood Disintegrative Disorder: ◦ Complete loss of language at age 2 with little subsequent improvement Rett’s Syndrome: ◦ 90% affected are female who have multiple and severe disabilities Autism, Asperger’s Disorder, and Pervasive Developmental Disorder Not Otherwise Specified (PDD NOS) fall under the umbrella of Pervasive Developmental Disorders and are commonly referred to as ASDs. PDDs are called “spectrum” disorders because each child has different symptoms that can range from mild to severe. PDD NOS is a diagnosis that is given when a child exhibits only some of the criteria for autism, an atypical pattern of deficits, or if the onset of the disorder is later than age 3. In Massachusetts, the rate is estimated to be 1 in 122 children (Mass. DPH 12/05) ASDs affect 1 in 88 individuals nationally (CDC, 2012) a 23% increase since (2009). ASDs are 5 times more prevalent in boys than in girls and occur in all races, ethnicities, and social classes. The number of children identified with an ASD has been growing steadily in the last few decades. Some of this increase can be explained by: ◦ more comprehensive research methods (e.g., casting a wider net in health and educational settings and seeking out those who do not have a diagnosis) ◦ accounting for the entire spectrum (e.g., Asperger’s Disorder and PDD NOS were included in more recent studies) ◦ improved parent and professional awareness ◦ advanced parental age Researchers from the fields of genetics and environmental toxicology continue to investigate other reasons why the rate of autism has increased so significantly. More children will be diagnosed with ASD this year than AIDS, Cancer and Diabetes combined Social skills: Such as emotions Understanding how people are feeling Having a conversation Communication: Both spoken and unspoken (pointing, eye contact, smiling) Behaviors or interests: Such as repeating words or actions, Playing with things in an unusual way (spinning, lining up toys) Insistence on following routines and schedules ASDs are neuro-developmental disorders that are characterized by impairments in: Social Interaction, Communication, and Behavior. Specifically, individuals with ASDs have difficulty interacting with others and using language in conversation. They also have a restricted range of interests or engage in repetitive behaviors. These deficits are usually seen before the age of 3. Individuals with ASDs often have difficulty learning how to perform everyday activities, and some have intellectual impairments that cause them to learn more slowly than their peers. Asperger’s Disorder differs from autism because individuals with Asperger’s Disorder do not have a history of cognitive or language delays, yet they have significant difficulties in social interactions and communication. Asperger’s Disorder is often diagnosed later than autism since the deficits may not be observed until the child begins to interact with peers in more structured settings. PDD NOS: A diagnosis that is given when a child exhibits only some of the criteria for autism, an atypical pattern of deficits, or if the onset of the disorder is later than age 3. Currently, there is no known cause of ASD. Research suggests that ASD is caused by genetic factors, which may be triggered by environmental causes. Exposure to environmental causes may occur in the womb or during or after birth. Ongoing studies are primarily focused on genetic and environmental causes, such as maternal illnesses during pregnancy, conditions during childbirth, and chemical exposures in the individual’s environment. ASD is not linked to parenting skills or psychological issues. Given the many similarities and differences between individuals with ASDs, many researchers suggest that there is likely to be more than one cause of autism. Risk Factors that may be associated with Autism: Higher incidence in families with a member who has autism, Risk Factors in pregnancy and delivery, Fragile X Syndrome, Gene Mutation, and if you have noticed recent research is looking at causal factors of obesity and Type II Diabetes. No medical or blood tests available to detect ASD If an ASD is suspected, a multidisciplinary evaluation should be conducted as soon as possible. During these evaluations, the child and parents may meet with a number of specialists. Each professional will conduct part of the evaluation including a pediatric neurologist or developmental pediatrician, psychologist, speech-language pathologist, and occupational or physical therapist and the results will be summarized in a written report. ADOS is considered as the standard test for observations for diagnosing ASD◦ Autism Diagnostic Observation Schedule Although there is no diagnostic laboratory test for ASDs, tests are often recommended for the following reasons: ◦ 1) to search for a cause, ◦ 2) to find out if there are other medical problems that might look like autism (e.g., hearing loss), and ◦ 3) to detect additional medical problems that might be co-existing with an ASD. Audiologic testing is recommended for any child with delayed language or at risk for autism. A child who does not speak or respond to others’ speech may have autism, a hearing problem, or some other condition which interferes with speech. Neuroimaging, the process of capturing images of the brain, may be needed if there is an abnormal neurologic examination not explained by the diagnosis of autism (e.g., non-symmetrical motor examination, cranial nerve abnormalities, microcephaly). Hypopigmented or hyperpigmented skin lesions, in which the skin appears lighter or darker, may be examined by a Woods Lamp. Electroencephalograph (EEG), a test that measures the electrical activity of the brain, may be recommended if the child is demonstrating signs of seizure activity or language regression. Routine clinical neuroimaging, such as Magnetic Resonance Imaging (MRI), is not recommended as part of the diagnostic evaluation of autism at the present time. Metabolic testing (a blood test) should be considered when there is a history of lethargy, cyclic vomiting, early seizures, intellectual disability, or unusual facial features. Untreated phenylketonuria (PKU) is an example of a metabolic disorder. Additional blood tests may be recommended. Lead testing is recommended for children with pica (eating substances other than food). Individuals may also have their ferritin level checked if there are concerns of anemia (a lower than normal amount of red blood cells). Genetic testing may be used to rule out Fragile X or other genetic disorders. Girls who fail to progress and lose skills following typical development may be tested for a mutation in the MECP2 gene, indicating the presence of Rett’s Disorder. Physicians may also consider other genetic tests such as CGH (microarray). Further medical tests may be recommended by the team. Individual recommendations are based on the child's medical history and symptoms. Many individuals with autism do not spontaneously reach out to others to share information or feelings. They often do not know how to engage in simple social interactions, such as sharing an experience with another person. For example, a 3-year-old child with autism may not point to an animal so that his sister will notice it too. Social skill deficits can make the development of interpersonal relationships difficult. Some individuals with autism have difficulty understanding others’ perspectives, such as recognizing when other people do not share the same interests. Another hallmark of autism is a delay in or a lack of development of spoken language. While many individuals with autism develop speech, their communication may consist of single-word utterances or simple sentences. Common speech abnormalities include echolalia (immediate or delayed repeating of information), unconventional word use, and unusual tone, pitch, or inflection. Even if more complex vocabulary is acquired, individuals with autism may still have difficulties having conversations with other people. They also may not understand common nonverbal cues such as body language, facial expressions, and eye contact. Individuals with autism have a restricted range of interests. For example, a 6-year-old child with autism may play with his or her toy train to the exclusion of all other toys. Additionally, they may engage in repetitive play activities such as spinning the wheels on a toy car rather than pretending to drive it, or dangling a shoelace in front of their eyes for long periods of time. Other repetitive behaviors may include motor movements, such as hand flapping, spinning, or jumping. Individuals with autism can be very resistant to changes in routine or transitions between activities. Even a minor change could be a great upset to an individual with autism. Behavior that is aggressive to others Self-injurious behavior May have either extremely passive behavior or extremely anxious, active behavior Difficulty with transitions “Neophobia” fear of anything new ◦ Often food, may have very self-limiting diets Strict adherence to schedule or routines Desire to follow set patterns of behavior and interaction Limited interests and /or intense restricted interests Hypersensitivity ◦ Touch, lights, sounds, smells and other sensory stimuli may be overwhelming Hyposensitivity ◦ Little sense of pain, temperature Little sense of: ◦ Fear, danger, safety Prone to wandering or bolting Often seek out water sources Body movements ◦ May have unusual walking pattern or balance, walking on tip-toes repetitive actions such as rocking back and forth, flapping of hands, and pacing or constant movement Repetitive behavior (perseveration) will simply repeat words or phrases that have been spoken to them (known as echolalia) or memorized from songs, television shows , movies or books (known as scripting) Delayed echolalia: repeating something heard at an earlier time Confusion between pronouns “I” and “you” Lack of response to people Lack of eye contact Lack of pointing Approximately 50% of individuals with ASD are non-verbal or do not have functional speech People with ASD who are verbal often have far better receptive language skills compared to expressive skills People with Asperger’s Syndrome may appear verbally sophisticated but still lack comprehension skills First Domain-Impairment in ability to interact with others, lack of appreciation of social cues, social/emotional inappropriate behaviors Second Domain- narrow interest pattern leading to exclusion of activities (self or others) or relying on memory rather than underlying meaning Third Domain- repetitive routines or interests Fourth Domain- speech and language peculiarities- delayed onset of language; superficially perfect expressive language; odd prosody, impaired comprehension, often able to read before speaking, marked comprehension problems despite good expressive skills, semantic-pragmatic language difficulties, nonverbal learning disability (NLD) Fifth Domain-non verbal communication problems, limited use of gestures, body language and facial expressions Sixth Domain-motor clumsiness, odd posturing and odd motor behaviors, poor performance on neuro-developmental exam Drawing skills Musical skills Arithmetic Calendar arithmetic Memory Perfect pitch Normal to above normal intelligence Affinity for perseverating on subject matters which are of interest to them at the time-often passionate and obsessive on the subject Rule bound-limited ability to differentiate when rules should be applied or relaxed Tendency to being argumentative-especially about rules. If non verbal, the defiance is expressed physically, outwardly or inwardly Executive Function Disorder (EFD)- the ability to plan, to know when to start, shift, delay reactions Difficulty in maintaining friendships due to confusion about social, subtle cues Difficulty in modulating voice, and in establishing personal space and distance Difficulty in understanding another’s perspective- empathy, (theory of mind) Unrealistic expectation of one’s own abilities Difficulty in censoring comments; doesn’t realize the potential consequences Trouble with transitions Hypo or hypersensitive to touch, noise, smells Has difficulty keeping track of possessions Loses track of time and schedule Starts things but doesn’t complete them-distracted Has systems for organization but doesn’t use them Has difficulty with working memory-holding information in mind while processing and implementing it Feels challenged when trying to organize information and relating it to their knowledge Struggles with transitions e.g. getting dressed, waking Has a one track mind Seems to be the last to know what is going on Doesn’t know how to use an “inner voice” to problem solve Psychiatric diagnoses are more likely to be diagnosed or classified at a later age Among children with Autism up to 96% are reported to have a co-occurring developmental condition The most common conditions are: Learning disability, ADD/ADHD, mental retardation, and stuttering, many of which can delay or “Mask” a clinical diagnosis of ASD. ADHD can be found in up to 21% of children High frequencies of attentional difficulties in 94% of children Hyperactivity in 56% of children Impulse control in 35% of children Tic disorders in 22% of children Some studies say 40%-75% of children with ASD have ADHD. The most common are: Anxiety disorder, mood disorder (bi-polar disorder), obsessive compulsive disorder and oppositional defiant disorder. Early delays in communication skills, challenging behaviors or impaired social skills may be more general markers for conditions later diagnosed as more complex psychiatric or developmental conditions. The intensity and severity of psychiatric symptoms in individuals with ASD are influenced by a number of factors including: Severity of core deficits, Severity of cognitive impairments, Presence of co-morbid medical disorders, and Life experiences related to coping with a disability and or combination. Recent studies using standard psychiatric assessments indicate a majority of children with ASD ranging from 5-17 years meet criteria for DSM Axis I diagnoses at 72%-80% with: ◦ anxiety disorders, bi-polar disorder, ADHD, other disruptive behaviors and major depression most commonly reported. Oppositional defiant disorder may be related to core symptoms of Autism or may be consistent with a true ODD diagnosis and the prevalence rate is seen to be 25% 7.0% 6.0% 5.0% 4.0% 3.0% 2.0% 1.0% 0.0% 2008 National Health 2008 National Health Survey Study Survey Study General Population ASD Population 6.4% 25.0% 20.0% 21.0% 18.0% 15.0% 0.7% 10.0% 0.4% 0.5% 0.1% General Population 5.0% 0.0% 1.7% 1.7% 1.0% ASD Population The Autism Division at Department of Developmental Services oversees the management of the Autism Waiver Program. Autism Clinical Managers provide oversight, technical assistance and monitoring. There are seven DDS funded Autism Support Centers across the state. These Centers provide support brokerage services to assist families with service planning, identifying service providers and managing their budgets for this program. DDS/Respite Autism Support Centers Autism Resources TILL’s Autism Support Center Advocates: Autism Alliance of Metro West HMEA: Autism Resource Center NSARC: The Autism Support Center Community Autism Resources Community Resources for People with Autism The Family Autism Center An individualized planning process, resulting in an Autism Support Plan of Care, assists each family in identifying the assessed needs of their child and the specific waiver services available to address these needs. All services have limits on their frequency and scope. With the assistance from a Support Broker and oversight from an Autism Clinical Manager, each family develops and directs a plan of supports and services within the limits of an individual budget, up to $25,000 based on the child’s assessed needs. Families receive support in identifying, hiring and training providers who are qualified to deliver these services. Provides one‐to‐one behavioral, social and communication based interventions through a service called Expanded Habilitation. The service consists of one‐to‐one interventions developed and monitored by a trained clinician and is carried out in the child’s home and community. Expanded Habilitation includes, but is not limited to: ◦ Behavioral approaches such as Applied Behavioral Analysis (ABA). ◦ Developmental and Relational Models such as: Floor Time and Communication Models. ◦ Expanded Habilitation Services should help children develop basic adaptive skills, elementary verbal skills and appropriate interactive and play skills. Obtain a diagnosis that is documented in writing. For an individual in Massachusetts for whom the diagnosis of autism or a related developmental disability is being considered, a referral should be considered. A diagnosis by a Developmental Evaluation Clinic, school psychologist, or private clinician typically provides documentation of a disability. Documentation of a disability is necessary to access the services provided by public agencies for individuals with disabilities. Education Obtain a functional, educational assessment during the early adolescent years. Assure that the results of this assessment are integrated into goals of the IEP. Assure the IEP includes experiential, community based goals. Assure there is an annual evaluation of progress made on all goals. All students need to prepare themselves for the opportunities and challenges of adulthood. Such preparation is critical for individuals with autism because it is the key to a happy and productive life. Public Law 94-142 that guarantees a free and appropriate education for all school-aged children. Individuals with disabilities must maximize their abilities and opportunities in preparation for satisfactory occupation during their adult years. An educational assessment should measure the student’s ability to function independently in areas essential to daily living as an adult (e.g. communication, social, self care, independence, etc.). Teaching goals derived from the assessment should be included in the IEP and progress on those should be reviewed annually. Assure a written ITP (Individualized Transition Plan) is in place at age 16. Assure a referral to Vocational Rehabilitation has been made at age 16 or older if a work capability assessment is desired. Assure a referral to the Single Portal Agency / Local Management Entity has been made by the beginning of the final year of school unless your relative with autism is able to function independently. If the VR assessment or Transition Plan includes any form of employment, assure a referral is made for Long-Term Supported Employment. By the age of 14 the student with autism should have the above mentioned assessment and it should be reviewed annually to measure progress toward appropriate assessment-based goals. At the age of 16 a written Individualized Transition Plan, like the IEP, should be developed in conjunction with the family and reviewed annually until the transition from school to a future setting occurs. The process of transitioning to the next setting should be by the beginning of the final year of education, unless the student can function well without assistance. As part of the referral, all future needs should be listed, (e.g. vocational, recreational, residential, transportation, etc.) even if they are not needed immediately The Children’s Behavioral Health Initiative is an interagency initiative of the Commonwealth’s Executive Office of Health and Human Services whose mission is to strengthen, expand and integrate Massachusetts state services into a comprehensive, community-based system of care, to ensure that families and their children with significant behavioral, emotional and mental health needs obtain the services necessary for success in home, school and community. Standardized Behavioral Health Screening in Primary Care Standardized Behavioral Health Assessment, using the Child Adolescent Needs and Strengths tool (CANS) Intensive Care Coordination In-Home Therapy Mobile Crisis Intervention Family Support and Training In-Home Behavioral Services Therapeutic Mentoring Services These covered services can be accessed through: ◦ Outpatient therapy, ◦ In-Home therapy, or ◦ Intensive Care Coordination, as part of the youth’s Individual Care Plan (ICP) or treatment plan (for Outpatient or In-Home Therapy). Use calm, simple language Be literal and specific Avoid slang words Never try to stop a repetitive behavior unless it is self-injurious or dangerous to others Avoid touching or standing behind the person Always be aware of the possibility of bolting Allow the person to finish the behavior because this selfstimulating (stimming) can be self soothing Be aware of hypotonia-people with ASD often have underdeveloped trunk muscles and may be unable to support their airway when lying flat on their chest Remember that stressful or upsetting situations overwhelm people with ASD and can adversely affect them. They may struggle with tasks they could normally perform (regression) Sign language Pictures and visuals PECS – Picture Exchange Communication System Assistive technology All people can benefit from visual supports Visual cues may be easier to follow than auditory cues Visual cues stay in place after the auditory cue is gone Individuals with autism often have difficulty with auditory processing Assist in following routines/schedules Cue when there are changes in routines Cue us to follow rules Help remember directions Provide tangible concrete information Increase independence Remind us of significant events Provide concrete reminder of what to do or say Prepare-organize expectations Preview-teach skills prior to activity Prompt-provide instructional cues during an activity Review-reinforce skills through review after an activity May be related to difficulty processing the information their body receives through various senses. Disturbances can occur in any or all of the following areas: 1. Analysis: how the person interprets the 2. 3. sensation Memory: how (or if) the person remembers similar sensations and proper responses from the past Processing: how quickly (or if) the sensation reaches the central nervous system to be interpreted Many individuals with ASD already have difficulty with communicating, the added frustration of sensory challenges may result in: ◦ ◦ ◦ Negative behaviors like object or physical aggression Withdrawal from activities Self-stimming activities Recognize that everyone has some sensory issues Learn to distinguish between hyperactive and hypoactive sensory systems Make observations of individual’s behaviors in relationship to sensory input Make environmental changes if possible i.e., lights, fragrances, music, clothing tags ◦ ◦ ◦ ◦ ◦ Engage in an activity with the child Go to their level: Use calm simple language Avoid idioms or slang “You're pulling my leg.” Talk in short, direct phrases Be literal and specific Make eye contact Remain calm: Avoid overreacting to inappropriate behaviors as this could inadvertently reinforce this behavior Practice patience: Allow for delayed response to questions or commands Assist with transitions Utilize positive behavior reinforcement strategies when ever possible: ◦ (“Nice job getting out of the pool”) Model positive behaviors: ◦ Use calm body language ◦ No screaming ◦ Avoid negative phrases Utilize visuals as much as possible: ◦ ◦ ◦ ◦ Picture cards Written daily schedules Written rules or directions Simple phrase board Recommended ◦ ◦ ◦ More research needed and proceed with caution or use in conjunction with the recommended: ◦ ◦ ◦ ◦ ◦ ◦ ◦ ◦ Applied behavior analysis (ABA) Positive behavior supports (PBS) Medication – can help with symptoms and for serious behaviors Developmental therapies (DIR/Floor time or RDI) TEACH Social stories Animal therapies Art therapy Music therapy Herbs and Homeopathic treatments Most vitamin therapies Proven ineffective: ◦ ◦ ◦ ◦ Auditory integration training Facilitated communication Secretin Psychoanalysis Reinforcement Shaping Prompting Task analysis and chaining Discrete Trial Instruction Activity Schedules Verbal Behavior Pivotal Response Training Natural Environment Training Incidental Teaching Token Economy Generalization Maintenance Functional Behavior Assessment and Intervention www.wrongplanet.net -Wrong Planet is the web www.aspennj.org/ Asperger Syndrome Education Network www.autism.healingthresholds.com- Summarizes community designed for individuals (and parents / professionals of those) with Autism, Asperger's Syndrome, ADHD, PDDs, and other neurological differences. www.dotolearn.com –Do2Learn: Educational Resources for Special Needs -picture communication cards, songs, games and activities for autism and special needs children. Many free printables. (ASPEN) ASPEN provides families and individuals whose lives are affected by Autism Spectrum Disorders and Nonverbal Learning Disabilities with education, support and advocacy. current autism therapies, treatments, research and news ◦ www.tillinc.org -Towards Independent Living and Learning, Inc. ◦ www.fcsn.org - The Federation for Children with Special Needs ◦ www.aane.autistics.org - The Asperger’s Association of New England◦ www.autism-society.org/massachusetts Autism Society of America’s Massachusetts chapter ◦ www.autismspeaks.org - Autism Speaks ◦ www.autismconsortium.org -Autism Consortium The Autism Consortium The Federation for Children with Special Needs Asperger's Association of New England (AANE) Mass Advocates for Children The Lurie Center Boston Medical Center Children’s Hospital A psychologist ◦ A Psychologist will administer developmental and intelligence testing. These tests yield important information related to the child's abilities, limitations, and overall level of functioning compared to other children the same age. Behavior Therapists ◦ A Behavior Therapist will use behavioral assessments to design, implement, and evaluate procedures to help the child learn new skills and reduce challenging behaviors. Occupational Therapists ◦ An occupational therapist will assess the child's fine motor and self-help skills to determine if the child is able to complete age-appropriate activities such as getting dressed, using utensils, brushing teeth, or writing. Physical Therapists ◦ The physical therapist will evaluate the child’s gross motor skills and coordination (e.g., running, biking, throwing, catching). Speech Language Pathologists: ◦ A speech therapist will assess the child's communicative abilities, including the ability to understand and use language, articulate clearly, use language for different functions, and engage in conversations. The speech therapist’s evaluation should result in specific treatment recommendations for improving the child’s speech and communication. Joshua Lyons Autism Services Coordinator TILL’s Autism Support Center (781)302-4835 [email protected] Elizabeth Waters Director of Family Supports TILL’s Autism Support, PCA, IHBS, Children’s Services (781)302-4824 [email protected] Ann Cotter-Mack MS BCBA Director of Behavioral Services (781)302-4835 [email protected]








© Copyright 2026