
25th Annual Meeting program and abstracts
Program and abstracts 25th Annual Meeting 12 - 14 February 2015 Geilo, Norway www.ssrcts.org 1 SSRCTS 2015 Table of contents Welcome! .............................................................................................................. 3 Committee ............................................................................................................. 4 Program at a glance ............................................................................................... 5 Scientific program .................................................................................................. 6 Thursday, 12 February ...................................................................................... 6 Friday, 13 February ........................................................................................... 9 Saturday, 14 February ..................................................................................... 11 Abstracts - Oral presentations ............................................................................. 13 Abstracts - Poster presentations ......................................................................... 44 Authors’ index...................................................................................................... 55 2 SSRCTS 2015 Welcome! Dear Colleagues and Friends, th We welcome you to the 25 Annual Scientific Meeting of SSRCTS! This is a jubilee meeting showing that “the little rebellion” has proven its independency and become a true and proud offspring of the Scandinavian Association of Thoracic Surgery, hosting around 60 participants every year. The last year’s meeting proved that the new location at Bardøla Høyfjellshotell was a success. We also hope to continue the success of the meeting this year with interesting abstracts from both inside and outside of Scandinavia. Our aim is to give a “voice” to every participating scientist, so there will be mainly oral presentations. We hope to succeed in our work to combine basic and clinical research within the field of cardiothoracic surgery and give our young scientists a thorough overview of ongoing research in Scandinavia. th The invited guests for the 25 anniversary meeting in 2015 are renowned international scientists and surgeons: Professor Johan Pillgram-Larsen from Oslo will lecture on cardiothoracic trauma, Professor RJ Cusimano from Toronto will add on with a talk on training of cardiothoracic surgeons in Canada. He will also lecture on the treatment of cardiac tumors. Professor Pascal Dohmen from Berlin will guide us through the latest in tissue engineering and heart surgery in his Main Basic Topic lecture: The decellularized homograft. In the same symposium the mechanisms of valvular calcifications will be clarified by Dr. Arkady Rutkovskiy from Oslo. The Clinical Main Topic lecture will focus on heart- and lung-transplantation and Dr. Göran Dellgren from Gothenburg will give this State-of-the-Art lecture. There will also be some surprises and for sure, “pompous” speeches at the Anniversary Dinner on Saturday. I hope your days in Geilo will be memorable ones. Sincerely, Tómas Guðbjartsson President of SSRCTS n 3 SSRCTS 2015 Committee President SSRCTS Program Director SSRCTS Professor Tómas Guðbjartsson, MD, PhD Department of Cardiothoracic Surgery Landspitali - University Hospital IS-101 Reykjavik, Iceland Mobile: +354 825 5016 [email protected] www.ssrcts.org Mari-Liis Kaljusto, MD, PhD Department of Cardiothoracic Surgery Oslo University Hospital, Ullevål 0407 Oslo, Norway Tel: +47 99727991 [email protected] www.ssrcts.org Scientific Secretariat SSRCTS Gunnhildur Jóhannsdóttir, Office Manager Landspitali - University Hospital IS-101 Reykjavik, Iceland [email protected] Conference venue Bardøla Høyfjellshotell Tlf: +47 32 09 45 02 www.bardola.no 4 SSRCTS 2015 Program at a glance Thursday 12 February Friday 13 February Saturday 14 February 14:0014:50 Arrival and registration 14:0015:00 Oral Session III Abstracts A12-A16 14:5015:00 Welcome 15:0015:10 Coffee break 15:0016:00 Oral Session I Abstracts A01-A05 15:1016:34 16:0016:15 Coffee break 16:3517:20 16:1517:30 Oral Session II Abstracts A06-A11 17:3018:00 Coffee break 17:2017:50 Coffee break 17:1517:45 Coffee break 18:0018:50 Invited lecture 17:5018:35 Main topic, basic science Arkady Rutkovskiy: The basic mechanism of valvular calcification 17:4518:35 Postgraduate course Robert James Cusimano: 14:3016.00 Oral Session V Abstracts A24-A29 Oral Session IV Abstracts A17-A23 15:4516:15 Coffee break Main topic, clinical 16:1517:15 Invited lecture Pascal Dohmen: The decellularized homograft Cardiac tumors Johan PillgramLarsen: Thoracic trauma and the cardiothoracic surgeon Robert James Cusimano: Education of cardiothoracic surgeons in Canada 18.5019.00 Coffee break 18:3518:50 Coffee break 18:3519:00 Beer and Business 19:0020:10 Poster Session Abstracts P01-P10 18:5019:50 State-of-the-art lecture 19:30 Awards 20:00 Presidential dinner with pompous speeches Göran Dellgren: Heart and lung TX 20:10 Dinner 20:00 Dinner (buffet) 5 SSRCTS 2015 Scientific program Thursday, 12 February 14:00-14:50 Arrival and registration 14:50-15:00 Welcome Mari-Liis Kaljusto, Oslo, Norway Tómas Guðbjartsson, Reykjavík, Iceland 15:00-16:00 Oral session I Chairman: Anders Jeppsson, Gothenburg, Sweden 9+3 minutes for each presentation 15:00 A01 Functional and biomechanical performance of stentless extracellular matrix tricuspid tubegraft in pigs DM Røpcke, C Ilkjær, T Hejslet, AV Sørensen, H Jensen, MOJ Jensen, VE Hjortdal, SL Nielsen 15:12 A02 Impedance aggregometry for quality assessment of platelet concentrates S Singh, C Hesse, A Jeppsson 15:24 A03 A validation study of near infrared fluorescence imaging of lymphatic vessels in humans J Grønlund, N Telinius, SN Skov, M Ølgaard, VE Hjortdal 15:36 A04 Primary adenocarcinoma in the lung re-classified – histological subtypes and outcome GN Oskarsdottir, J Bjornsson, S Jonsson, HJ Isaksson, T Gudbjartsson 15:48 A05 Bronchial basal cells acquire mesenchymal traits in idiopathic pulmonary fibrosis and in culture HR Jonsdottir, AJ Arason, R Palsson, SR Franzdottir, T Gudbjartsson, HJ Isaksson, G Gudmundsson, Th Gudjonsson, MK Magnusson 16:00-16:15 Coffee break 6 SSRCTS 2015 16:15-17:30 Oral session II Chairman: Theis Tønnessen, Oslo, Norway 9+3 minutes for each presentation 16:15 A06 Preoperative measurement of platelet aggregability identifies ticagrelor-treated CABG patients with increased risk of perioperative bleeding complications CJ Malm, E Hansson, CS Hakimi, A Jeppsson 16:27 A07 Design of custom-made TAVI valve for low-cost valve concept testing D Bruus, I Lindhardt, PBS Weng, R Galsgaard, P Johansen 16:39 A08 Children with ASD – long-term follow-up using registries Z Karunanithi, C Nyboe, VE Hjortdal 16:51 A09 Novel assessment of strain distribution with high spatiotemporal resolution on aortic valve leaflets S Heide-Jørgensen, SK Krishna, J Taborsky, T Bechsgaard, JL Hønge, R Zegdi, P Johansen 17:03 A10 Dual antiplatelet therapy with ticagrelor or clopidogrel and the risk for bleeding complications after CABG V Fröjd, A Jeppsson 17:15 A11 Tissue engineering and cell therapy – novel therapeutic approaches for thoracic diseases P Jungebluth, S Sjöqvist, ML Lim, P Macchiarini 17:30-18:00 Coffee break Invited lecture Chairwoman: Mari-Liis Kaljusto, Oslo, Norway 18:00-18:50 Cardiac tumors Robert James Cusimano, MD, Toronto, Canada 18:50-19:00 Coffee break 7 SSRCTS 2015 19:00-20:00 Poster session Chairman: Vibeke Hjortdal, Århus, Denmark 3+3 minutes for each presentation 19:00 P01 The in-vivo comparison of a new semi flexible mitral annuloplasty ring to rigid, flat- and fully flexible mitral annuloplasty rings in a porcine model 19:06 P02 Development of a new valve prosthesis concept for infant cardiac surgery 19:12 P03 The effect of TAVI oversizing on valve tissue stresses MJ Tjørnild, DM Røpcke, SN Skov, C Ilkjær, SL Nielsen MB Jensen, MH Smerup, P Johansen SK Krishna, R Galsgaard, S Heide-Jørgensen, T Bechsgaard, R. Zegdi, L Bräuner, JV Nygaard, P Johansen 19:18 P04 Comparison of the aortic root remodeling techniques - with and without a supporting annular ring. An vitro evaluation TS Lading, DM Røpcke, T Lindskow, T Bechsgaard, P Johansen, H Nygaard, JM Hasenkam, SL Nielsen 19:24 P05 Are all flexible mitral annuloplastic rings the same? An in vivo study 19:30 P06 Giant right atrial myxoma presenting as chronic obstructive pulmonary disease 19:36 P07 Metachronous metastatic hepatocellular carcinoma to the right ventricle 19:42 P08 Cavitation in patiens with bileaflet mechanical heart valves 19:48 P09 Major ischemic stroke caused by air embolism from a ruptured giant pulmonary bulla J Rasmussen, MJ Tjørnild, DM Røpcke, SN Skov, C Ilkjær, SL Nielsen S Kumar, C Howes, A Delvecchio, PN Bonde S Kumar, AA Mangi P Johansen, TS Andersen, JM Hasenkam, H Nygaard, PK Paulsen JF Gudmundsdottir, BL Thorarinsson, G Myrdal, P Hannesson, T Gudbjartsson 19:54 P10 David versus Yacoub aortic root repair: Assessment and comparison of stress distribution in the aortic root - a clinical porcine experimental study T Lindskow, MJ Tjørnild, T Bechsgaard, DM Røpcke, SL Nielsen 20:10 Dinner (buffet) 8 SSRCTS 2015 Friday, 13 February 14:00-15:00 Oral session III Chairman: Arnar Geirsson, Reykjavík, Iceland 9+3 minutes for each presentation 14:00 A12 Ischemic preconditioning in advance of segmental arteries sacrificing protects the spinal cord J Herajärvi, T Anttila, H Haapanen, H Sarja, C Mustonen, T Laukka, T Starck, M Kallio, H Tuominen, K Kiviluoma, P Karppinen, V Anttila, T Juvonen 14:12 A13 Design, calibration and preliminary results of force transducers for aortic root repairs T Bechsgaard, S Laugesen, JL Hønge, H Nygaard, SL Nielsen, P Johansen 14:24 A14 Carbonic anhydrase 9 deposits are associated with increased ascending aortic dilatation E Niinimaki, P Muola, S Parkkila, H Haapasalo, T Paavonen, A Mennander 14:36 A15 The persistence and significance of acute aortic dissection: Incidence and mortality derived from a nationwide population study in Iceland 1992-2013 IH Melvinsdottir, SH Lund, B Agnarsson, T Gudbjartsson, A Geirsson 14:48 A16 Physical modeling studies of vibration transmittance to assess healing after sternotomy A Joutsen, J Hautalahti, A Paldanius, J Hyttinen, J Laurikka 15:00-15:10 Coffee break 15:10-16:34 Oral session IV Chairman: Philipp Jungebluth, Heidelberg, Germany 9+3 minutes for each presentation 15:10 A17 New concept for quantifying two-dimensional forces acting on an implanted mitral annuloplasty ring SN Skov, DM Røpcke, AW Siefert, C Ilkjær, MJ Tjørnild, A Yoganathan, H Nygaard, SL Nielsen, M Jensen 15:22 A18 Living arrangements of octogenarians after isolated coronary artery bypass surgery. A nationwide study K Thorsteinsson, JJ Andreasen, C Torp-Pedersen, G Gislason, K Fonager 15:34 A19 Retrograde lung perfusion in the treatment of massive pulmonary embolism. A randomized porcine study B Kjærgaard, JL Hønge, SO Magnusdottir, BS Rasmussen, UTh Baandrup, JM Hasenkam, SR Kristensen 9 SSRCTS 2015 15:46 A20 Clinical presentation of native mitral valve infective endocarditis determines outcome after surgery S Ragnarsson, J Sjögren, M Stagmo, P Wierup, S Nozohoor 15:48 A21 Surgery for active infective endocarditis in Iceland 1997-2013 RM Johannesdottir, T Gudbjartsson, A Geirsson 16:10 A22 Short and long-term outcome of mitral valve repair in Iceland JF Gudmundsdottir, S Ragnarsson, A Geirsson, R Danielsen, T Gudbjartsson 16:22 A23 Common sequence variants associated with coronary artery disease correlate with the extent of coronary atherosclerosis E Bjornsson, DF Gudbjartsson, A Helgadottir, Th Gudnason, T Gudbjartsson, K Eyjolfsson, RS Patel, N Ghasemzadeh, G Thorleifsson, AA Quyyumi, U Thorsteinsdottir, G Thorgeirsson, K Stefansson Main topic, clinical Chairman: Jarle Vaage, Oslo, Norway 16:35-17:20 The decellularized homograft Pascal Dohmen, MD, PhD, Leipzig, Germany 17:20-17:50 Coffee break Main topic, basic sciences Chairwoman: Mari-Liis Kaljusto, Oslo, Norway 17:50-18:35 The basic mechanism of valvular calcification Arkady Rutkovskiy, MD, PhD, Oslo, Norway 18:35-18:50 Coffee break State-of-the-art-lecture Chairman: Tómas Guðbjartsson, Reykjavík, Iceland 18:50-19:50 Heart and lung TX Göran Dellgren, MD, PhD, Gothenburg, Sweden 20:00 Dinner (buffet) 10 SSRCTS 2015 Saturday, 14 February 14:30-15:42 Oral session V Chairman: Ari Mennander, Tampere, Finland 9+3 minutes for each presentation 14:30 A24 Osteogenic potential of valvular interstitial cells is increased in patients with calcific aortic valve disease M Bogdanova, A Malashicheva, J Vaage, A Rutkovskiy 14:42 A25 Single center surgical experience of native aortic valve infective endocarditis: Preliminary results S Ragnarsson, P Timane, J Sjögren, M Stagmo, P Wierup, S Nozohoor 14:54 A26 Acute kidney injury is an independent risk factor for morbidity and mortality following aortic valve replacement for aortic stenosis D Helgason, SA Viktorsson, AW Orrason, IL Ingvarsdottir, S Helgadottir, A Geirsson, T Gudbjartsson 15:06 A27 Remote ischemic preconditioning protects spinal cord after segmental arteries cutoff H Haapanen, J Herajärvi, O Arvola, T Anttila, T Starck, M Kallio, V Anttila, H Tuominen, K Kiviluoma, T Juvonen 15:18 A28 Early statin treatment dampens recovery after experimental cardiac arrest A Mennander, V Vuohelainen, M Hämäläinen, T Paavonen, E Moilanen 15:30 A29 Acute volume-overload impacts early on intramyocardial arteries; an experimental rat study C Huuskonen, R Bolkart, T Soininen, M Hämäläinen, T Paavonen, E Moilanen, A Mennander 15:45-16:15 Coffee break Invited lecture Chairman: Theis Tønnessen, Oslo, Norway 16:15-17:15 Thoracic trauma and the cardiothoracic surgeon Johan Pillgram-Larsen, MD, Oslo, Norway 17:15-17:45 Coffee break Postgraduate course Chairman: Tómas Guðbjartsson, Reykjavík, Iceland 11 SSRCTS 2015 17:45-18:35 Education of cardiothoracic surgeons in Canada Robert James Cusimano, MD, Toronto, Canada 18:35-19:00 Beer and business 19:30 20:00 Awards Presidential dinner with pompous speeches 12 SSRCTS 2015 Abstracts - Oral presentations A01 Functional and biomechanical performance extracellular matrix tricuspid tubegraft in pigs 1,2 2 1 3 1,2 of stentless 1 1 DM Røpcke , C Ilkjær , T Hejslet , AV Sørensen , H Jensen , MOJ Jensen , VE Hjortdal , 1,2 SL Nielsen 1 2 Department of Cardiothoracic and Vascular Surgery, Department of Experimental & 3 Clinical Research and Department of Cardiology, Aarhus University Hospital, Aarhus, Denmark [email protected] Objectives: A stentless porcine extracellular matrix tricuspid tubegraft has been developed for tricuspid valve reconstruction. This study purpose was to compare biomechanical and functional performance of native and tubegraft tricuspid valves in an acute porcine model. Material / methods: Fourteen 65 kg pigs were randomized to a tubegraft (n=7) or control with native valve preservation (n=7). Anterior papillary muscle force was measured with a dedicated force transducer implanted on the papillary muscle tip. Microtip pressure catheters were placed in the right atrium and right ventricle. To assess dynamic 3D valve geometry and leaflet motion, thirteen sonomicrometry crystals were implanted: Six in the tricuspid annulus, one on each leaflet free edge, one on each papillary muscle tip and one in the right ventricular apex. The level of significance was p <0.05. Results: No tricuspid regurgitation was observed after tricuspid tubegraft implantation. No significant differences in intracavitary pressures, annular motion or leaflet excursion angles were observed between groups. Tricuspid annulus and leaflet orifice area, annular diameters and the septal segment of the annulus were significantly smaller in the tubegraft group. Accordingly, anterior papillary muscle force was significantly lower in the tubegraft group, despite the fact that anterior leaflet and -tenting areas were significantly larger. Discussion: An extracellular matrix tubegraft was implanted in the tricuspid position, producing a competent valve with physiological biomechanical and functional performance compared with native valves. We anticipate that annulus-remodelling effects following tubegraft implantation reduce leaflet stress distribution, which may protect repair durability. 13 SSRCTS 2015 A02 Impedance aggregometry for quality assessment of platelet concentrates 1 2 S Singh , C Hesse , A Jeppsson 1 1,3 2 Department of Cardiothoracic Surgery, Department of Clinical chemistry and 3 Transfusion Medicine and Department of Molecular and Clinical Medicine, Institute of Medicine, Sahlgrenska Academy, University of Gothenburg, Gothenburg, Sweden [email protected] Objectives: Transfusion of platelet concentrates is used to improve hemostasis in patients with ongoing bleeding. Storage impairs the quality of the concentrate. We have previously shown that platelet aggregability attenuates over time in platelet concentrates and in vitro platelet aggregometry may thus be a quick and simple method for quality assessment. The aim of the present study was to describe the association between in vitro aggregability and other biomarkers of platelet storage lesion. Materials and methods: Eight apheresis platelet concentrates were investigated 1, 4, and 7 days after preparation. Collagen-induced platelet aggregation was assessed with impedance aggregometry (Multiplate®). The expression of three markers of platelet activity; the granule proteins CD62p and CD63 and phosphatidylserine exposure was determined with flow cytometry. In addition, lactate and glucose levels, platelet count, and pH were analyzed in the concentrate. Results: A significant and gradual reduction in collagen-induced platelet aggregation during storage was observed. Storage significantly increased the expression of CD62p and phosphatidylserine from day 1 to day 4 and further increased phosphatidylserine expression to day 7. Lactate levels increased while glucose levels, platelet count and pH decreased over time. Collagen-induced platelet aggregation correlated significantly with phosphatidylserine expression (r = −0.67, p<0.001), pH (r = 0.68, p<0.001), glucose level (r = 0.53, p<0.001) and lactate level (r = −0.82, p<0.001). Discussion: Collagen-induced platelet aggregation correlates strongly with other markers of platelet storage lesion. The results support the use of impedance aggregometry for in vitro quality assessment of platelet concentrates. 14 SSRCTS 2015 A03 A validation study of near infrared fluorescence imaging of lymphatic vessels in humans J Grønlund, N Telinius, SN Skov, M Ølgaard, VE Hjortdal Department of Cardiothoracic and Vascular Surgery, Aarhus University Hospital, Denmark [email protected] Objectives/Aims: The aim of this study is to validate and gain experience of near infrared fluorescence (NIRF) imaging of human lymphatic vessels. The study will examine the inter and intraindividual variability, and furthermore how time, temperature and muscle activity will alter the parameters measured. This study will shed light on the strengths and weaknesses of the technique, as well as the considerations that are necessary when using it. Materials and methods: Ten healthy volunteers were included in the study. Lymph propulsion in lymphatic vessels on the lower leg was visualized using 3 intradermal injections of the fluorescent dye Indocyanine green. A custom built camera setup consisting of a EM-CCD camera with appropriate filters and a 785 nm laser was used to visualize the fluorescent dye. Each test subject was examined twice with 14 days between each examination. Lymphatic activity and changes in activity over time were examined. Lymphatic activity was defined as a contraction frequency and lymph packet velocity. Tests to quantify the vessel activity such as pumping pressure and refill time were also performed. Lymphatic activity before and after two interventions, physical activity and local hyperthermia, were examined. Sequences were analyzed by plotting “regions of interests” on the vessels, where a contraction is seen as a significant decrease in the differentiated intensity curve. Results: All 10 subjects have completed the study. The collected data have been blinded and are currently being analyzed. Discussion: This study provides valuable insight in regard to the viability of NIRF imaging of lymphatic vessels in humans. The technique has the potential to become an important tool in research and diagnostics of diseases with a lymphatic component, by providing real time visualization and quantification of the lymphatic vasculature system. 15 SSRCTS 2015 A04 Primary adenocarcinoma in the lung reclassified – histological subtypes and outcome 3,5 4 3,4 2 1,5 GN Oskarsdottir , J Bjornsson , S Jonsson , HJ Isaksson , T Gudbjartsson 1 2 3 Departments of Cardiothoracic Surgery, Pathology and Pulmonology, Landspitali 4 5 University Hospital. Department of Pathology, Akureyri Hospital, Faculty of Medicine, University of Iceland, Reykjavik, Iceland [email protected] Objective: Non-small cell lung cancer (NSCLC) comprise 85% of primary lung cancer, where adenocarcinoma, squamous cell and large cell carcinoma are the most common histological types. Our previous data have indicated that adenocarcinoma histology predicts improved survival compared to other histological types in patients operated with lobectomy for NSCLC in Iceland. Recently a new classification of primary adenocarcinomas of the lung was published. The aim of this study was to review the histology of all primary lung adenocarcinomas operated on in Iceland during a 20 year period, 1991-2010, using the new criteria and assess the impact of histology on survival. Materials and methods: This retrospective nationwide study included 312 patients with primary lung adenocarcinoma (mean age 65.6 yrs., 56% female) that underwent resection in Iceland between 1991-2010. Tumors were reclassified according to the current IASLC/ATS/ERS pulmonary adenocarcinoma classification system. Overall survival was estimated by the Kaplan-Meier method. Results: Preliminary results for the first 277 cases show that acinar predominant adenocarcinoma (APA) was the most common subtype (46%), solid predominant (SPA) with mucin production comprised 25% of the cases, lepidic predominant (LPA) 17% and papillary predominant (PPA) 8%. There were two cases of preinvasive adenocarcinoma and 3 cases of minimally invasive adenocarcinoma. Overall survival at 1 year for all histological subtypes of adenocarcinoma was 79% and 42% at 5 years. A statististically significant difference in survival between the histological subtypes was not seen (log-rank test, p=0.55) (Fig. 1). Conclusions: Acinar and solid predominant adenocarcinoma are the most common histological subtypes followed by mucin production subtype and lepidic predominant adenocarcinoma. Overall survival at 5 years is 42% which is in the lower range compared to other studies with no apparent diffence between subtypes. These findings suggest that other factor than histologic subtype explain the higher survival of adenocarcinoma in recently pubished data. 16 SSRCTS 2015 Fig 1. Overall survival according to adenocarcinoma subtype A05 Bronchial basal cells acquire mesenchymal traits in idiopathic pulmonary fibrosis and in culture 1,2 1,2 1,2,4 1,2 3,7 HR Jonsdottir , AJ Arason , R Palsson , SR Franzdottir , T Gudbjartsson , HJ 4 5,6 1,2 1,2,6 Isaksson , G Gudmundsson , Th Gudjonsson , MK Magnusson 1 Stem Cell Research Unit, Biomedical Center, Faculty of Medicine, University of Iceland, 2 3 4 Department of Laboratory Hematology, Cardiothoracic Surgery, Pathology and 5 6 Respiratory Medicine and Sleep, Landspitali University Hospital, Department of 7 Pharmacology and Toxicology, Faculty of Medicine, University of Iceland, Faculty of Medicine, University of Iceland [email protected] Idiopathic pulmonary fibrosis (IPF) is a progressive interstitial lung disease with high morbidity and mortality. The cellular source of the fibrotic process is currently under debate with one suggested mechanism being epithelial-tomesenchymal transition (EMT) in the alveolar region. In this study we show that bronchial epithelium overlying fibroblastic foci in IPF contains a layer of p63 positive basal cells while lacking ciliated and goblet cells. This basal epithelium shows increased expression of CK14, Vimentin and N-cadherin while retaining Ecadherin. The underlying fibroblastic foci showed both E- and N-cadherin positive cells. To determine if p63 positive basal cells were able to undergo EMT 17 SSRCTS 2015 in culture we treated VA10, a p63 positive basal cell line, with the serum replacement UltroserG™. A subpopulation of treated cells acquired a mesenchymal phenotype, including an E- to N- cadherin switch. After isolation, these cells portrayed a phenotype presenting major hallmarks of EMT (loss of epithelial markers, gain of mesenchymal markers, increased migration and anchorage independent growth). This phenotypic switch was prevented in p63 knockdown cells. In conclusion, we show that bronchial epithelium overlying fibroblastic foci in IPF lacks its characteristic functional identity, shows increased reactivity of basal cells and acquisition of a partial EMT phenotype. This study suggests that some p63-positive basal cells are prone to phenotypic changes and could act as EMT progenitors in IPF. A06 Preoperative measurement of platelet aggregability identifies ticagrelor-treated CABG patients with increased risk of perioperative bleeding complications 1,2 1,2 1,2 CJ Malm , E Hansson , CS Hakimi , A Jeppsson 1 1,2 2 Department of Cardiothoracic Surgery, Sahlgrenska University Hospital, Department of Molecular and Clinical Medicine, Institute of Medicine, Sahlgrenska Academy, University of Gothenburg, Gothenburg, Sweden [email protected] Background: The ADP-receptor inhibitor ticagrelor reduces risk of thrombotic advents in patients with acute coronary syndrome but increases the risk for nonsurgical and surgical bleeding complications. Current guidelines recommend that ticagrelor should be discontinued at least 5 days prior to surgery but this cannot always be achieved. We investigated if preoperative measurement of platelet aggregability in CABG patients with ticagrelor treatment <5 days before surgery, identifies patients with increased risk of perioperative bleeding complications. Methods: Seventy-seven CABG patients with ticagrelor treatment within 5 days of surgery were included in a prospective observational study. Median time from last ticagrelor dose was 30 hours (interquartile range 24-72 h). Preoperative platelet aggregability was assessed with the Multiplate® instrument. Poor ADP-dependent platelet aggregability was defined as <30 aggregation units as previously suggested. Bleeding complications were registered using the new universal definition of perioperative bleeding (UDPB). In addition, pre- and perioperative variables factors univariately associated with bleeding complications were identified. 18 SSRCTS 2015 Results: Poor preoperative ADP-dependent platelet aggregability was detected in 52/77 (68%) of the patients. Bleeding complications occurred in 28/77 (36%) patients. Twenty-four of the 28 (86%) bleeding complications occurred in patients with poor ADP-dependent platelet aggregability. Accordingly, the risk of bleeding complications was significantly higher in patients with poor aggregability compared with patients with acceptable aggregability (46% vs 16%, p=0.012). The only factors univariately associated with an increased risk of bleeding complications were cardiopulmonary bypass (CPB) time (p=0.01) and poor ADP-dependent platelet aggregability (p=0.002). Conclusions: Preoperative measurement of ADP-dependent platelet aggregability identifies patients with high risk of bleeding complications. In nonurgent cases, surgery can be postponed until tests are satisfactory. In acute cases, poor ADP-dependent platelet aggregability may motivate early use of procoagulant drugs or blood products. A07 Design of custom-made TAVI valve for low-cost valve concept testing 1 1 1 1 12 D Bruus , I Lindhardt , PBS Weng , R Galsgaard , P Johansen , 1 2 Dept. of Engineering, Faculty of Science and Technology, Aarhus University, Dept. of Cardiothoracic Surgery, Aarhus University Hospital, Skejby, Aarhus, Denmark [email protected] Objectives: Transcatheter aortic valve implantation is an alternative to the conventional open-heart surgery for patient suffering from aortic valve dysfunction. This technique is used in patients with high operative risk and is appealing because of the reduced hospitalization and comparable outcome to surgical valve implantation. However, there are still circumstances where the deployed valve does not reach the optimal geometries that it was designed for (e.g. as a non-circular deployment or size mismatch (oversizing)). During such conditions the valve function may be impaired, and the stress in the leaflets may be increased, potential leading to accelerated non-calcific tissue degradation, hence reduced valve longevity. To further investigate these events it will be beneficial to establish an in vitro setup at which detailed analyses can be performed. To increase the precision and reproducibility at various valve alteration scenarios it could be beneficial to develop a model of a TAVI valve which can be produced incorporating such alterations. 19 SSRCTS 2015 Therefore, the aim of this study is to design a low cost 3D-printed TAVI stent with attached bovine pericardial tissue leaflets initially in a circular fitted geometry and later in various altered configurations based on clinical data. Materials and methods: The design of the custom-made stent is inspired by the Edwards Sapiens 3 valve. The stent will not be crimped nor designed for catheter insertion. It will be optimized for installment in a pulsatile mock circulatory in vitro flow loop. The stent is designed as a 3D CAD model and printed in stainless steel (316L). However, as the stent is manufactured using 3D print it must meet some restrictions concerning angles and thickness of material. The leaflets and skirt are made of bovine pericardial tissue and GoreTex and sutured to the stent frame, as seen on Figure 1. The valve will initially be evaluated hemodynamically and biomechanically in its non-altered configuration. Results: Pending Discussion: The opportunity to 3D print a custom-made TAVI valve on location is useful to provide flexible and reproducible test protocols for TAVI valve concept models and also to keep future in vitro TAVI valve experiments on a low-cost level. Figure 1. a: 3D CAD model of stent. Dimensions, h: 20mm, id: 24,8 mm od: 26 mm. b: First version of the stent with a pulmonary artery from a heart of a pig sutured to the stent frame. A08 Children with ASD – long-term follow-up using registries Z Karunanithi, C Nyboe, VE Hjortdal Dept. of Cardiothoracic and Vascular Surgery, Aarhus University Hospital, Denmark [email protected] The objective of the study is to estimate the risk of developing atrial fibrillation and stroke in adult patients with atrial septal defects (ASD), by investigating if 20 SSRCTS 2015 adult patients with ASD closure during childhood have an increased use of antiarrhythmic or anticoagulation medicine in adulthood compared with the general population. Adult patients with ASD diagnosed in childhood but without closure have increased risk of atrial fibrillation, stroke and atrial fibrillation related medicine use in adulthood compared with the general population. The data originates from hospital records, The Danish Civil Registration Registry, The Danish National Patient Registry (DNPR) and The Danish National Prescription Registry. By using specific ICD codes we will include Danish patients diagnosed between 1963 and 1994, before the age of 18 and born before 1994, with or without closure. Patients with other concomitant heart disease or no sign of ASD in the hospital record upon review were excluded. For each patient included in the study we match 10 controls by age- and gender. The outcomes (defined by ICD codes) are atrial fibrillation, stroke, vitamin K antagonist, digitalis glycosides and antiarrhythmic drugs. The risk of atrial fibrillation and stroke will be estimated using Cox regression analysis with age as an underlying time scale and entry at 18 years. The analyses are adjusted for hypertension, ischemic heart disease, pulmonary disease and diabetes. Cumulative incidences are performed for 10 and 20 years and compared with the control group with death as a competing risk. A total of 2111 patients have the ASD diagnosis and are currently being validated. Of the 1815 patients validated, 926 are included in the study population at present. Of these patients the mean age at operation is 9.29 years [8.77; 9.81]. When the validation finishes and the study population is fully defined, we connect to the database in Statistics Denmark to obtain more data on each individual patient, after which we start performing the statistical analyses. The results obtained at the beginning of the year will be presented at the meeting. A09 Novel assessment of strain distribution with high spatio-temporal resolution on aortic valve leaflets 1 1 1 1,2 2 3 S Heide-Jørgensen , SK Krishna , J Taborsky , T Bechsgaard , JL Hønge , R Zegdi , P 1,2 Johansen 21 SSRCTS 2015 1 2 Dept. of Engineering, Faculty of Science and Technology, Dept. of Cardiothoracic 3 Surgery, Aarhus University Hospital, Skejby, Aarhus, Denmark, Hôpital Européen Georges Pompidou, Service de Chirurgie Cardiovasculaire, Paris, France [email protected] Objectives: In order to estimate the wear and tear of the tissue valves, mainly prosthesis, assessment of valve stress and strain is warranted. The traditional approaches for strain measurements are using strain gauges. However, this is not a feasible approach for heart valves as the size, mass, and application of the strain gauge may interfere with the dynamics of the valve. The aim of this study is to develop a platform for non-contact heart valve deformation analysis with high spatio-temporal resolution. Materials and methods: Deformation analyses are performed in a pulsatile in vitro system using ARAMIS (GOM), which offers means of acquiring strain analyses with high temporal and spatial resolution, enabling the material independent pattern recognition software to apply frame-by-frame cross correlation based strain estimates. The images are acquired at 2000 frames per second through two high speed cameras for 3D analyses. Evaluation of this platform is done using homemade TAVI valves. Results: The study showed that ARAMIS was able to recognize stochastic pattern and estimate strain on the TAVI leaflets. Both major and minor strain along with deformation was successfully assessed for all leaflets from the analysis. The spatio-temporal development of a very detailed strain pattern was revealed with a 0.5 msec time resolution. 22 SSRCTS 2015 A10 Dual antiplatelet therapy with ticagrelor or clopidogrel and the risk for bleeding complications after CABG V Fröjd, A Jeppsson Dep of Cardiothoracic Surgery, Sahlgrenska University Hospital, Gothenburg, Sweden [email protected] Background: Dual antiplatelet therapy reduces the risk for thrombotic complications in patients with acute coronary syndrome but increases the risk for perioperative bleeding complications. It is therefore recommended that the ADP-inhibitor is discontinued five days before elective surgery. Ticagrelor reduces the risk for thrombotic events further compared to clopidogrel, without increasing the overall risk for CABG-related bleeding complications. It is unclear if this holds true if the ADP-receptor inhibitor cannot be discontinued in time. We compared the risk for major bleeding between clopidogrel and ticagrelor when the ADP-receptor inhibitor was discontinued <5 days before surgery. Methods: 1960 CABG patients (mean age 67±9 years, 78 % men) were included in a retrospective case control study. 421/1960 (21%) were treated with dual antiplatelet therapy <5 days before surgery, 327 with clopidogrel and 94 with ticagrelor. Major bleeding was defined according to the BART–criteria (postoperative blood loss >1500 ml/12 h, or re-exploration, or red blood cell transfusion >10 units, or death because of bleeding). Independent predictors for major bleeding were identified with logistic regression. Results: 205 (10.5%) of the patients suffered a major bleeding complication. Dual antiplatelet therapy with clopidogrel or ticagrelor <5days before surgery was an independent predictor of major bleeding (odds ratio 1.83 (95% confidence interval 1.29-2.59), p=0.001) together with EuroSCORE, intraoperative bleeding >0.5 l, preoperative eGFR and age. The risk for bleeding complications was higher with ticagrelor (OR 2.61, CI 1.50-4.53, p=0.001) than with clopidogrel (OR 1.63, CI 1.11-2.39, p=0.012) after adjustment for all other independent risk factors. When ticagrelor was compared to clopidogrel, the odds ratio was 1.79 (1.06-3.04, p=0.030). The risk for major bleeding decreased with 28 % for each day of discontinuation with ticagrelor (OR 0.72, CI 0.56-0.92, p=0.008) and with 19 % for clopidogrel (OR 0.81, 0.69-0.95, p=0.011). Conclusions: Treatment with dual antiplatelet therapy <5 days before surgery increases the risk for major bleeding complications. The risk is significantly higher with ticagrelor than with clopidogrel. The bleeding risk is markedly reduced for each day the ADP-inhibitor can be withdrawn before surgery. 23 SSRCTS 2015 A11 Tissue engineering and cell therapy – novel therapeutic approaches for thoracic diseases 1,2 1 1 P Jungebluth , S Sjöqvist , ML Lim , P Macchiarini 1 1 2 Karolinska Institutet, Stockholm, Sweden; Thoraxklinik at Heidelberg University Hospital, Heidelberg, Germany [email protected] Objectives/aims: Regenerative medicine, including tissue engineering and cell therapy, is a promising and growing field for the treatment of both acute and chronic diseases affecting thoracic tissues and organs. Materials and methods: Various tissue engineering approaches using both decellularized (DNase, deoxycholate, SDS) tissues and synthetic (molding technic, electrospinning, 3-D-printing) scaffolds seeded with different cell types (MSCs, MNCs, epithelial cells, chondrocytes) have been applied to investigate regenerative mechanisms and functionality both in vitro and in vivo. Small and large animals models have been utilized to generate tissue engineered grafts for the trachea, lungs, esophagus, heart, heat valves and the diaphragm. Initial clinical transfer has been performed for the trachea. Cell therapy has been examined in experimental disease models and initial clinical transfer realized in patients suffering from acute lung disease. Results: the decellularized scaffolds of the different tissues/organs have been approved to be biocompatible and non-immunogenic. The generated grafts mimic the native architecture, resist mechanical stress and induce angiogenesis. Seeded allogeneic mesenchymal stromal cells spontaneously differentiate (proven by gene-, protein and functional evaluations) on particular decellurized scaffolds. Both the reseeded biological and synthetic scaffolds are used to heterotopically investigate their immunogenicity and orthotopically replace the native tissue. Tissue engineered scaffolds for the trachea, the esophagus and the diaphragm have been demonstrated their functionality in animal models. Early clinical data (5-year follow-up) provide initial evidence for successful tracheal replacement using tissue engineered solutions. Cell-based therapy resulted in significant improvement in acute and chronic lung diseases both in experimental studies and clinical setting. Discussion: Regenerative medicine may represent a promising therapeutic alternative in the future. However, further efforts are necessary to detect underlying mechanisms and investigate the real impact of these new approaches for the treatment of thoracic diseases. 24 SSRCTS 2015 A12 Ischemic preconditioning in advance of segmental arteries sacrificing protects the spinal cord 1 1 1 1 1 5 2 J Herajärvi , T Anttila , H Haapanen , H Sarja , C Mustonen , T Laukka , T Starck , M 2 3 4 5 1 1 Kallio , H Tuominen , K Kiviluoma , P Karppinen , V Anttila , T Juvonen 1 2 3 4 Departments of Surgery, Clinical Neurophysiology, Pathology and Anesthesiology, 5 Oulu University Hospital, Department of Medical Biochemistry and Molecular Biology, University of Oulu, Oulu, Finland [email protected] Objectives: Following the repair of thoracic and thoracoabdominal aortic aneurysms (TAA/A) paraplegia remains one of the most serious complications. Strategies in order to prevent paraplegia are still inconsistent. Preconditioning has shown to be a promising method to mitigate neurological damage. In this study we focus on the mechanism of ischemic preconditioning preserving spinal cord function following segmental arteries sacrificing. Materials and methods: Sixteen female piglets are randomized into an ischemic preconditioning, group (n=8) and a control group (n=8). The intervention group undergoes 4 cycles of 5-minute left iliac artery occlusion ischemia-reperfusion episodes. The left subclavian artery and step-by-step segmental arteries sacrificing procedure is identical for both groups. Motor evoked potential (MEP) monitoring is performed from both hind limbs. Peripheral nerve stimulation is carried out to ensure no irreversible disadvantage occurring while using ischemic preconditioning. Continuous electrocardiogram and hemodynamics are monitored peri-, intra- and postoperatively to assess autonomic nerve system responses. Pulmonary artery blood samples are collected in several time points. After a 2-hour follow up period piglets are extubated and transferred to a recovery room. Postoperatively 24 hours the neurological assessment is carried out. At the end of the experiment thoracolumbar spinal cord is harvested for histopathological analysis. Results and discussion: Results are pending but preliminary data will be presented at the meeting. A13 Design, calibration and preliminary results of force transducers for aortic root repairs 1,2 2 2 2 2 T Bechsgaard , S Laugesen , JL Hønge , H Nygaard , SL Nielsen , P Johansen 25 1,2 SSRCTS 2015 1 Department of Engineering, Faculty of Science and Technology, Aarhus University, Department of Cardiothoracic & Vascular Surgery, Aarhus University Hospital, Aarhus, Denmark 2 [email protected] Objectives: Patients with aortic regurgitation secondary to ascending aortic dilation or aneurism can be treated with valve sparing techniques such as the David reimplantation or the Yacoub remodeling technique. In order to quantify the impact of these two repair procedures, new force transducers have been developed and tested. Materials and methods: Two transducers have been developed. The first transducer is an annulus transducer which can be placed subvalvular to the aortic valve to measure the in plane forces of the aortic annulus. The second transducer is a commissural transducer which can be placed extravascular to the aortic root at the commissural level in order to measure the forces in the valve commissures. The force transducers have been manufactured using rapid prototyping techniques in titanium. Micro strain gauges have been meticulously mounted on the transducer and sealed with two-component epoxy glue. The transducers were calibrated under static conditions using loads applied to the transducer. The output was recorded and plotted as a function of the input load. For the experiments aortic roots were excised from pig hearts collected at a local slaughterhouse and installed in a pulsatile in vitro model mounted with the developed force transducers. Results and discussion: A linear fit was made to the static calibration of the commissural transducer (R-squared value of 0.99) with a sensitivity of 184mV/N. Preliminary results from the porcine aortic roots tested in our in vitro model, using the newly developed force transducers showed a force of about 1.2N at the commissural points at fluid pressures of 130mmHg (Figure 1). Fig 1: Preliminary commissural force data acquired at 130 mmHg fluid pressure. 26 SSRCTS 2015 A14 Carbonic anhydrase 9 deposits are associated with increased ascending aortic dilatation 2 2 3 2 2 E Niinimaki , P Muola , S Parkkila , H Haapasalo , T Paavonen , A Mennander 1 1 2 Heart Center, Tampere University Hospital, Department of Pathology, Tampere 3 University Hospital and Tampere University, Department of Anatomy, Tampere University,Tampere, Finland [email protected] Objectives: Inflammatory factors defining ascending aortic wall stiffness attribute to aortic wall dilatation. Arterial wall carbonic anhydrase 9 (CA9) deposits during inflammation indicate local hypoxia. We studied whether CA9 deposits are associated with inflammatory remodeling of the ascending aorta in patients undergoing surgery for aortic dilatation. Material and methods: Aortic wall histology and immunohistochemistry for CA9, leukocytes, T- and B-lymphocytes, plasma cells, macrophages, endothelial cells, smooth muscle cells, cell proliferation, elastase and Van-Gieson-staining were performed to 30 selected patients that underwent surgery for ascending aorta, and the samples were grouped according to presence of CA9 deposits. Results: 20 out of 30 patients had CA9 deposits mainly within the adventitia, whereas 10 patients lacked CA9 deposits. Adventitial inflammation, mainly consisting of macrophages and plasma cells, were increased in CA9 positivity as compared with CA9 negativity (p < 0.01). The mean diameter of the ascending aorta at the sinotubular junction was 59 ± 2 mm for all patients, and was significantly increased in patients with CA9 positivity as compared with CA9 negativity (63 ± 3 vs 53 ± 2, mm, p < 0.02). Receiver operating characteristic curve analysis confirmed the association of CA9 positivity with increased ascending aortic dilatation (AUC 0.766; S.E. 0.090; p = 0.020; 95% C.I. 0.5900.941). However, root dilatation was equally present in CA9 positive and CA9 negative patients (50% and 60%, respectively). Discussion: Positive CA9 suggests carbonic anhydrase activity during ascending aortic dilatation. Intervening with CA9 may add an armament against aortic dilatation and extension of surgery. 27 SSRCTS 2015 A15 The persistence and significance of acute aortic dissection: Incidence and mortality derived from a nationwide population study in Iceland 1992-2013 1 1 2,3 1,3 IH Melvinsdottir , SH Lund , B Agnarsson , T Gudbjartsson , A Geirsson 1 2 3 3 University of Iceland, Department of Pathology and Department of Cardiothoracic Surgery, Landspitali University Hospital, Reykjavik, Iceland [email protected] Objectives: Acute thoracic aortic dissection is a life threatening disease where correct diagnosis and management is essential in order to modulate the high morbidity and mortality associated with the condition. Utilizing a nationwide data comprising the whole Icelandic population we determined the true incidence, mortality and the time-dependent mortality risk of acute aortic dissection. Material and methods: In order to capture all diagnosis of aortic dissection in Iceland from 1992-2013 the diagnosis databases of all regional hospitals in Iceland and Landspitali University Hospital as well as clinical and forensic autopsies databases of the Medical Examiner Office were queried for aortic dissection codes (ICD-9 and ICD-10). Demographics, medical history, risk factors and clinical symptoms variables were collected for all patients. Incidence was calculated using age and gender specific information derived from the National Statistics Iceland. Cox proportional hazards model was used to estimate hazards ratios. Results: A total of 148 individuals were diagnosed with acute aortic dissection resulting in age and gender adjusted yearly incidence of 2.55 per 100,000 person. There was no significance change in incidence during the study period. The mean age was 66.4±13.4 years and 62% were male. Of all cases 16% died outside of hospital settings while for the patients that arrived alive to a hospital, 29% died within 24 hours and the 30-day mortality was 45%. The 10-year overall survival was 37.6%. During the course of the study the short-term mortality rate decreased by 0.96, per year, (95% CI: 0.923- 0.996) and the 10-year survival improved significantly. Discussion: Acute thoracic aortic dissection remains a significant medical problem associated with high mortality. The incidence remained unchanged over the course of 23 years. We observed significant decline in short- and longterm mortality during the course of the study indicating improved overall outcome in patient diagnosed with acute aortic dissection. 28 SSRCTS 2015 A16 Physical modeling studies of vibration transmittance to assess healing after sternotomy 1,2 1 1,2 2 A Joutsen , J Hautalahti , A Paldanius , J Hyttinen , J Laurikka 1 1 2 Heart Center, Tampere University Hospital, Department of Electronics and communications engineering, Tampere University of Technology, Tampere, Finland [email protected] Objectives: Sternal instability following a sternotomy is a risk factor in the early postoperative period for mediastinitis causing morbidity and mortality. A device measuring vibration transmittance has been developed to assess sternal healing. To learn how the measuring geometry affects the transmittance, a bench test using artificial physical models was conducted. Materials and methods: The developed device includes two units, an actuator and a sensor, that are placed in contact with the measured object. The actuator emits a 3 s long 20 Hz – 2 kHz vibration stimulus and an accelerometer inside the sensor measures the transmittance of the vibration. Three simple block models and one anatomical model based on CT images were built to simulate sternal anatomy. Synthetic ballistic gel, 3D printed polylactate and polyurethane rubber modeled thoracic soft tissue, bone and cartilage respectively. Results: The three block models simulated intact (A), split (B) and steel wire bound (C) sternums. The actuator – sensor distance was 6 cm. Ten repeated measurements were made on the block models to assess the vibration transmittance. The measured power of the transmitted vibration was was A > C > B. All the comparisons between the conditions were statistically significant (p<0.001). The anatomical model simulated intact sternum (D), intact sternum with soft tissue incision (E), split sternum (F), loose closure (G) and tight closure (H) using steel sutures. The actuator and sensor were placed bilaterally on the 2nd, 3rd, 4th and 5th costal cartilages, 6 cm apart. 20 repeated measurements were made on each costal level 2-5 and condition (D-H). The results showed very high variance between the costal levels and conditions with no trend, contrary to what was found in the block model conditions A-C. Discussion: Our results show that in the simple block models the vibration transmittance is behaving as expected: intact > bound > split. However, the more elaborate anatomical model failed to give consistent results, possibly due to gel separation from the 3D printed frame during the model manipulation, 29 SSRCTS 2015 surface unevenness below the measuring device and manual holding of the device during a long measurement session. The device may be useful in assessing sternal healing, but further work is needed to discover the most suitable mode of operation. A17 New concept for quantifying two-dimensional forces acting on an implanted mitral annuloplasty ring 1,2 1 3 1 1 3 1 SN Skov , DM Røpcke , AW Siefert , C Ilkjær , MJ Tjørnild , A Yoganathan , H Nygaard , 1 3 SL Nielsen , M Jensen 1 2 Dept. of Cardiothoracic and Vascular Surgery, Aarhus University Hospital, Dept. of Engineering, Faculty of Science and Technology, Aarhus University, Aarhus, Denmark, 3 Dept. of Biomedical Engineering, Georgia Institute of Technology and Emory University, Atlanta, USA [email protected] Objectives: The objective of this study was to assess the feasibility of quantifying in-plane and out-of-plane forces acting on an implanted annuloplasty ring. Materials and methods: The design of an X-shaped transducer in the present study was optimized for simultaneous in- and out-of-plane force measurements. The force transducer was implanted in two groups with five 80 kg porcine animals in each group. The native group received the transducer implanted only. A second group had the transducer attached to a rigid Edwards Lifesciences Classic Annuloplasty Ring size 32 that was subsequently implanted in the annulus (Figure 1A). Transducer and ring dimensions were chosen to be truesized when implanted in an 80 kg porcine model to evaluate the impact of the healthy mitral valve force balance on the annuloplasty ring. Results: Calibrated out-of-plane forces in the native group were found to be 0.83 ± 0.6 N and 0.42 ± 0.3 N in the anterior and posterior segments respectively. The commissural segments were found to be 1.10 ± 0.7 N and 0.60 ± 0.5 N in the anterior and posterior commissural segments respectively. The calibrated in-plane forces were found to be 1.29 ± 0.7 N in the septal-lateral direction and 1.95 ± 1.1 N in the commissure-to-commissure direction (Figure 1B). Measurements with the force transducer attached to the Classic Annuloplasty Ring indicated a significant decrease in amplitude. Discussion: Measuring the forces in clinical mitral valve annuloplasty rings was demonstrated. Experiment results indicated a change of the force balance with and without a stiff annuloplasty ring. Further experimentation with this 30 SSRCTS 2015 transducer will provide a detailed and refined insight into the impact of these devices on mitral annular and device force distribution. A B Fig 1: (A) Transducer attached to annuloplasty ring prior to insertion (B) Selected force curves from the native group demonstrates the cyclic forces. ACOM, Anterior commissure; SL, Septal-lateral. 31 SSRCTS 2015 A18 Living arrangements of octogenarians after isolated coronary artery bypass surgery. A nationwide study 1,2 1,2 3 4 K Thorsteinsson , JJ Andreasen , C Torp-Pedersen , G Gislason , K Fonager 3,5 1 Department of Cardiothoracic Surgery, Center for Cardiovascular Researdh, Aalborg 2 3 University Hospita;, Department of Clinical Medicine, Aalborg University, Department of 4 Health Science and Technology, Faculty of Medicine, Aalborg University, Department of 5 Cardiology, Copenhagen University Hospital, Gentofte, Department of Social Medicine, Aalborg University Hospital, Aalborg, Denmark [email protected] Background: Proportion of octogenarians undergoing isolated coronary artery bypass surgery (CABG) is rapidly increasing. Data on living arrangements after surgery are scarce. The purpose of this study was to evaluate living arrangements in a nationwide cohort of octogenarians one year after isolated coronary artery bypass surgery. Methods: All patients who underwent isolated CABG between January 1996 and December 2012 in Denmark were included. All patients living in a nursery home previous to surgery were excluded. Patients were identified through nationwide administrative registers. Aalen Johansen estimator was used for the cumulative incidence of moving to a nursery home. A multivariate cox model was constructed to identify predictors for living in a nursery home one year after isolated CABG. Survival at 30 days and1 year was estimated by Kaplan-Meier estimates. Results: A total of 38,487 patients were included. Number of octogenarians was 1,455 (3.8%), median age was 65.4 ± 9.5 years. Males comprised 80% of the patients. 30-day mortality was 2.8%, increasing with age (1.2% in patients < 60 years, 7.6% in octogenarians). Long-term mortality at 1 year was 2.2% (age < 60 years) and 13.9% (age > 80 years). Proportion of patients living at a nursery home at 1, 5 and 10 years after surgery were 0.1%, 0.2% and 0.9% (<60 years),0.2%, 1% and 3.1% (60-69 years), 0.4%, 2.5% and 7% (70-74 years), 0.5%, 3.1% and 9% (75-79 years),1.5%, 7.7% and 17% (>80 years) respectively. Main predictors for living at a nursery home one year after surgery were: alcohol abuse (HR 2.47, 95% CI 1.9-3.2), stroke prior to surgery (HR 1.59, 95% CI 1.381.8), stroke < 30 days after surgery, female sex (HR 1.44, 95% CI 1.29-1.6), diabetes (HR 1.58, 95% CI 1.39-1.8), chronic renal insufficiency (HR 1.62, 95% CI 1.27-2.1) and heart failure (HR 1.28, 95% CI 1.13-1.5). Neither preoperative myocardial infarction, urgent or emergency surgery were significant predictors for living at a nursery home 1 year after surgery. 32 SSRCTS 2015 Conclusion: Octogenarians live at home in years to come after CABG. The risk of moving to a nursery home seems to be more dependent on the patient’s preoperative comorbidities than the surgical procedure itself. A19 Retrograde lung perfusion in the treatment of massive pulmonary embolism. A randomized porcine study 1,2 2 3 4 5 B Kjærgaard , JL Hønge , SO Magnusdottir , BS Rasmussen , UTh Baandrup , JM 2 6 Hasenkam , SR Kristensen 1 Department of Cardiothoracic Surgery, Cardiovascular Research Centre, Aalborg 2 University Hospital, Aalborg, Institute of Clinical Medicine, Aarhus University, Aarhus, 3 4 Biomedical Research Laboratory and Department of Anaesthesiology and Intensive 5 Care, Cardiovascular Research Centre, Aalborg University Hospital, Center for Clinical Research, Vendsyssel Hospital, Hjoerring, Department of Medicine, Aalborg University, 6 Department of Clinical Biochemistry, Cardiovascular Research Centre, Aalborg University Hospital, Aalborg, Denmark [email protected] Background: The treatment of massive pulmonary embolism with an associated cardiac arrest is controversial; however, surgical thrombectomy with extracorporeal circulation (ECC) is an option for treatment. It is difficult to remove all thrombembolic material. Theoretically, retrograde blood perfusion through the lungs may be beneficial. The purpose of the study was to investigate whether retrograde blood perfusion through the lungs during a thrombectomy is beneficial. Methods: Twelve pigs were prepared for ECC. Repetitive injections of preformed blood trombi into the right atrium resulted in cardiac arrest. ECC was established after 10 minutes of cardiac arrest, and after a sternotomy, the main pulmonary artery was incised as much thrombotic material as possible was removed from the pulmonary arteries. The pigs were randomized to ECC for one hour either with or without retrograde perfusion in the pulmonary circulation. After one hour, the released material was removed from the pulmonary arteries, and the incision was sutured. The pigs were weaned from the ECC. After sacrificing the pigs, they were autopsied with a special attention to the amount of remaining thrombi. Additional histologic analyses were performed with special attention to microembolisms, atelectases, and signs of tissue damages. Results: All of the pigs were weaned from the ECC. The amount of the embolic material removed varied considerably, as did the amount removed after the 33 SSRCTS 2015 retrograde or antegrade perfusion, and there was no significant difference between the two treatment modalities. There were no signs of tissue damage in the lungs. Conclusion: Retrograde lung perfusion was not generally beneficial in the treatment of massive pulmonary embolism in this setup; however, it may be an option if only modest amount of material is accessibly in the pulmonary artery. A20 Clinical presentation of native mitral valve infective endocarditis determines outcome after surgery 1 1 2 1 S Ragnarsson , J Sjögren , M Stagmo , P Wierup , S Nozohoor 1 1 2 Department of Cardiothoracic Surgery and Department of Cardiology, Lund University and Skåne University Hospital, Lund, Sweden [email protected] Objective: To examine the effect of the preoperative clinical presentation on long-term survival of patients undergoing surgery for isolated native mitral valve infective endocarditis (IE). Methods: A retrospective study was carried out on 100 patients who had undergone mitral valve surgery from 1998 to 2014 for ongoing isolated infective endocarditis. Patients were stratified depending on presenting symptoms: clinical stroke due to septic cerebral embolism, congestive heart failure, and uncontrolled sepsis. Group A had none of the clinical symptoms, Group B had one of the above clinical symptoms, and Group C had ≥2 symptoms. Follow-up was performed in March 2014 and was 100% complete for survival (median 3.8 years, IQR 0.8-7.7). Event rates were estimated with the Kaplan-Meier method and Cox-regression was performed. Results: Overall 30-day mortality was 5% (n=5); 0% in Group A; 8% in Group B (n=4); and 8% in Group C (n=1) (p=0.24). Five-year survival was 87.0±6.1% in Group A, 62.6±7.1% in Group B, and 33.8±15.2% in Group C. Grouping by clinical presentation was found to be an independent predictor of mortality (Group B, HR 2.37, 95% CI: 1.02-5.50; Group C, HR 4.07, 95% CI: 1.56-10.6). Other independent predictors of mortality were age (HR 1.04 per 1-year increment, 95% CI: 1.01-1.07, p=0.014), diabetes mellitus (HR 4.31, 95% CI: 2.28-8.51, p<0.001), preoperative renal failure requiring dialysis (HR 4.58, 95% CI: 1.5014.0, p=0.008), and Staphylococcus aureus infection (HR 3.43, 95% CI: 1.71-6.87, p=0.001). 34 SSRCTS 2015 Conclusions: Survival after surgery for native mitral valve IE was independently influenced by the presence of preoperative embolic stroke, congestive heart failure or uncontrolled bacteremia alone or in combination. Delaying surgical treatment may increase the probability and severity of preoperative complications and consequently postoperative mortality. A21 Surgery for active infective endocarditis in Iceland 1997-2013 1 1,2 RM Johannesdottir , T Gudbjartsson , A Geirsson 1 1 2 Department of Cardiothoracic Surgery, Landspitali University Hospital, Faculty of Medicine, University of Iceland, Reykjavik, Iceland [email protected] Introduction: Endocarditis is a serious infection of the heart valves and often needs operation for cure. Common risk factor for endocarditis are bicuspid aortic valve, intravenous drug abuse and immune compromised patients. Symptoms include fever, weight loss and general weakness and if the infection gets severe enough can consist of sepsis, embolic events, complete insufficiency of the infected valve, heart block and severe heart failure. 35 SSRCTS 2015 Materials and methods: This is a retrospective study in the years 1997-2013. Information was retrieval from medical records. Over these years 307 patients were admitted to the Lanspitali University Hospital with the diagnosis of endocarditis of which 38 (12.3%) patients underwent surgery for active endocarditis. Results: The aortic valve was most commonly infected or in 26 (68%) cases. The most common pathogens cultured from blood were gram positive cocci, Staphylococcus aureus overall 26 patients had positive blood cultures. Most common antibiotics to be used were 3rd generation Cephalosporins and Penicillin. Complications following the procedures were myocardial injury, respiratory failure and reoperation due to bleeding. Conclusion: Infective endocarditis remain a serious disease and can be very difficult to manage. Relatively few patients diagnosis of endocarditis require operative treatment. Complications following these operation are common with moderately high operative mortality. A22 Short and long-term outcome of mitral valve repair in Iceland 1 4 1 2 JF Gudmundsdottir , S Ragnarsson , A Geirsson , R Danielsen , T Gudbjartsson 1 1,3 2 Departments of Cardiothoracic Surgery & Cardiology, Landspitali University Hospital, 4 Faculty of Medicine, University of Iceland, Department of Cardiothoracic Surgery, Anesthesiology and Intensive Care, Lund University Hospital, Lund, Sweden 3 [email protected] Objectives: To study, for the first time, the outcome following mitral valve repair (MVR) in Iceland. Material and methods: All MVR-patients (average age 64 yrs, 74% males) operated in Iceland 2001-2012. All 125 patients had mitral regurgitation; either due to myxomatous degeneration (group M, 56%) or functional regurgitation (group F, 44%). Reoperations and mitral insufficiency due to endocarditis, or acute MI were excluded. Results: The number of MVRs increased two-fold for the later 6 yrs of the study. The mean EuroSCORE was 12.9% and 10% had history of previous cardiac surgery. A ring annuloplasty was performed in 98% of cases and posterior leaflet resection in 41%, 28 patients received artificial chordae and 7 Alfieri-stitch. Concomitant heart surgery was performed in 83% of cases, most often CABG or Maze-procedure. Major complications occurred in 56% of the cases; peri-op. MI and re-operation for bleeding being the most common. Two patients later 36 SSRCTS 2015 required mitral valve replacement. Eight patients died within 30 days (6%) and 5-year overall survival was 79%; 84 and 74% for the M and F-groups, respectively (p=0.08). Conclusions: Mitral valve repairs in Iceland have increased significantly. Complications are common but operative mortality and long-term survival is similar to contemporary studies. A23 Common sequence variants associated with coronary artery disease correlate with the extent of coronary atherosclerosis 1,2 2 1,2 3 1,3 E Bjornsson , DF Gudbjartsson , A Helgadottir , Th Gudnason , T Gudbjartsson , K 3 4,5 4 2 4 Eyjolfsson , RS Patel , N Ghasemzadeh , G Thorleifsson , AA Quyyumi , U 1,2 1,3 1,2 Thorsteinsdottir , G Thorgeirsson , K Stefansson 1 2 3 Faculty of Medicine, University of Iceland; deCODE Genetics; Landspitali University 4 Hospital; Reykjavik, Iceland, Emory University School of Medicine, Atlanta, Georgia USA, 5 University College London, London, United Kingdom [email protected] Objective: Single nucleotide polymorphisms predisposing to coronary artery disease (CAD) have been shown to predict cardiovascular risk in healthy individuals when combined into a genetic risk score (GRS). We examined whether the cumulative burden of known genetic risk variants associated with risk of CAD influences the development and progression of coronary atherosclerosis. Approach and results: We investigated the combined effects of all known CAD variants in a cross-sectional study of 8,622 Icelandic patients with angiographically significant CAD (≥50% diameter stenosis). We constructed a GRS based on 50 CAD variants and tested for association with the number of diseased coronary arteries on angiography. In models adjusted for traditional cardiovascular risk factors, the GRS associated significantly with CAD extent -17 (difference per SD increase in GRS, 0.076; P=7.3x10 ). Compared to the bottom GRS quintile, patients in the top GRS quintile were roughly 1.67x more likely to have multivessel disease (odds ratio, 1.67; 95% confidence interval, 1.45-1.94). The GRS significantly improved prediction of multivessel disease over traditional 2 cardiovascular risk factors (χ likelihood ratio 48.1, P<0.0001) and modestly improved discrimination, as estimated by the C-statistic (without GRS vs. with GRS, 64.0% vs. 64.8%) and the integrated discrimination improvement (0.52%). Furthermore, the GRS associated with an earlier age at diagnosis of angiographic CAD. These findings were replicated in an independent sample from the Emory 37 SSRCTS 2015 Biobank study (n=1,853). Conclusions: When combined into a single GRS, known genetic risk variants for CAD contribute significantly to the extent of coronary atherosclerosis in patients with significant angiographic disease. A24 Osteogenic potential of valvular interstitial cells is increased in patients with calcific aortic valve disease 1,2 2 3,4 M Bogdanova , A Malashicheva , J Vaage , A Rutkovskiy 1,3 1 Department of Physiology at the Institute of Basic Medical Sciences, University of Oslo, 2 Norway; Almazov Federal Heart Centre, Institute of Molecular Biology and Genetics, Saint 3 Petersburg, Russian Federation; Department of Emergency and Critical care, Oslo 4 University Hospital, Ullevål, and Institute of Clinical Medicine, University of Oslo, Oslo, Norway [email protected] Background: Calcific aortic valve disease (CAVD) is caused by changes in the cell biology of valve leaflets leading to calcification of the valve and aortic stenosis. The dominant cell type in aortic valves is interstitial cells (VICs). VICs may transform into osteoblast-like cells causing calcification, but the mechanisms of this process are unclear. Our hypothesis was that the osteogenic potential of VICs is increased in valves from patients with CAVD. Methods: Primary VICs were isolated from the aortic valves of five patients. Valves from two patients had no calcification whereas valves from three patients displayed calcification from moderate to extremely severe (ossification). The cells were isolated following the removal of endothelium using 24-hour enzymatic digestion. The phenotype of cells was confirmed by staining for desmin, vimentin and alpha-amooth muscle actin. The VICs were subjected to treatment with osteogenic medium supplemented with betaglycerophosphate, dexamethasone and ascorbic acid. After a 21-day treatment the cells were stained with Alizarin Red to visualize calcification. Expression of mRNA of bone morphogenetic protein 2 and osteopontin was evaluated by PCR Results: VICs from all donors differentiate into osteoblast-like cells over the course of 21 days when subjected to the osteogenic medium. Expression of BMP2 and osteopontin as well as calcification increased in the cultured VICs. The osteogenic potential of VICs was proportional to the degree of calcification in the harvested valves. 38 SSRCTS 2015 Conclusions: We established a cellular model of osteogenic differentiation with human aortic valve interstitial cells. Even VICs from non-calcified valves produced calcium deposits when subjected to the osteogenic medium, suggesting high plasticity of the phenotype of VICs. The osteogenic potential of VICs correlated with the degree of calcification of the aortic valve, indicating a change in basic cellular biology of these cells during the development of the disease. A25 Single center surgical experience of native aortic valve infective endocarditis: Preliminary results 1 1 1 2 1 S Ragnarsson , P Timane , J Sjögren , M Stagmo , P Wierup , S Nozohoor 1 1 2 Department of Cardiothoracic Surgery and Department of Cardiology, Lund University and Skåne University Hospital, Lund, Sweden [email protected] Objective: Surgery for active infective endocarditis (IE) is performed in up to half of all IE cases but the associated mortality remains high. We describe the single center experience of patients undergoing surgery for isolated native aortic valve infective endocarditis (IE) and report short-term and long-term mortality. Methods: A retrospective study with 72 of the 120 patients that underwent aortic valve surgery at Skane University Hospital in Lund from 1998 to 2014 for ongoing isolated infective endocarditis. Data was extracted from the department’s surgical database and patient records. Follow-up on survival was performed in January 2015 and was 100% complete (median follow up 8.5 years, IQR 5.1-11.2.). Event rate was estimated with the Kaplan-Meier method. Results: The mean age was 57.7±16.8 years and 21% (n=15) were females. Preoperatively, 41 patients (57%) had congestive heart failure with NYHA class III or IV, 22 (31%) had septic embolism including 3 (4%) with embolic stroke. The most common pathogens were oral Streptococci (n=24, 33%), Staphylococcus aureus (n=11, 15%), and Enterococcus faecalis (n=11, 15%). Intraoperative inspection revealed a large vegetation (>10 mm) in 42 (58%) and annular involvement in 19 (26%). Biological prostheses were used in 30 (42%), mechanical prostheses in 27 (38%), a homograft in 11 (15%), pulmonary autograft (Ross procedure) in 3 (4%) and a biological Bentall procedure in 1 (1.4%). Overall 30-day mortality was 2.7% (n=2) and 90-day mortality 4.2% (n=3). The one-year survival was 94.3±2.8%, five-year survival was 83.8±4.5%, and 10-year survival 71.8±6.0%. 39 SSRCTS 2015 Conclusions: The short term mortality was low despite the high number of patients with congestive heart failure, septic embolism and annular involvement. The five-year survival was similar to that of patients that underwent surgery for isolated mitral IE at our institution. A26 Acute kidney injury is an independent risk factor for morbidity and mortality following aortic valve replacement for aortic stenosis D Helgason, SA Viktorsson, AW Orrason, IL Ingvarsdottir, S Helgadottir, A Geirsson, T Gudbjartsson Departments of Cardiothoracic Surgery, Landspitali University Hospital. Faculty of Medicine, University of Iceland, Reykjavik, Iceland [email protected] Objective: Acute kidney injury (AKI) is a common complication after cardiac surgery. So far most AKI-studies have focused on short-term outcome following CABG. We reviewed the incidence and risk factors for AKI after aortic valve replacement (AVR) in a population based cohort, and studied its effects on short-term outcomes and long-term survival. Materials and methods: Retrospective review of 366 patients undergoing AVR for aortic stenosis between 2002 and 2011. AKI was defined according to the RIFLE criteria. All patients requiring dialysis were followed-up in a centralized registry. Risk factors for AKI were analyzed with uni- and multivariate analysis and survival estimated with the Kaplan-Meier method. Results: The incidence of AKI following surgery according to RIFLE was 83/366 (22.7%). Forty patients fell in the RISK-; 29 in the INJURY-; and 14 in the FAILURE-group. Preoperative reduction in kidney function (GFR<60 mL/min/1.73m2) was present in 37 (44.6%) of patient who suffered AKI. Postoperative dialysis was required in 17 patients (4.6%), including one patient who required permanent dialysis. Major postoperative complication, such as perioperative MI (24/83, 29% vs. 25/283, 9%), multi organ failure (34/83, 41% vs. 4/283, 1%), and reoperation due to bleeding (24/83, 29% vs. 31/283, 11%) were more common in the AKI group (p<0.01). In multivariate analysis female sex (OR=1.10), high BMI (OR=1.02) and prolonged CPB-time (OR=1.03) were independent risk factors for AKI. 30-day mortality in the AKI group was 18% (15/83) vs. 2% (6/283) in the non-AKI group (p<0.001). Five-year survival of the AKI group was 66% compared to 87% in the non-AKI group (p<0.001). AKI was an 40 SSRCTS 2015 independent predictor of operative mortality in multivariate analysis (HR=1.69, 95% CI=1.01-2.79) but not for long-term survival (HR=1.11, 95% CI= 0.59-2.12). Conclusions: One out of every four patients undergoing AVR developed AKI postoperatively. Complications were significantly increased in the AKI-group and mortality increased 9-fold. AKI following AVR is an independent risk factor for operative mortality but does not determine long-term survival. A27 Remote ischemic preconditioning protects spinal cord after segmental arteries cutoff 1 1 1 1 2 2 1 H Haapanen , J Herajärvi , O Arvola ,T Anttila , T Starck , M Kallio , V Anttila , H 3 4 1 Tuominen , K Kiviluoma , T Juvonen 1 2 3 4 Departments of Surgery, Clinical Neurophysiology, Pathology and Anesthesiology, Oulu University Hospital, Oulu, Finland [email protected] Objective: Thoracoabdominal aneurysm procedures jeopardize the vascularization of the spinal cord and therefore, in spite of the improvement of surgical techniques and adjuncts the risk of paraplegia still remain. The neuroprotective ability of the remote ischemic preconditioning (RIPC) has been proven in several studies. This study aimed to demonstrate the effect of RIPC to the preservation of spinal cord function after segmental arteries (SA) sacrificed. Materials and methods: Twenty native stock piglets were randomized into the RIPC group (n=10) and the control group (n=10). The RIPC group underwent transient left hind limb ischemia prior to intermittent left subclavian artery and SAs cut off to the level of diaphragm. Motor evoked potential (MEP) monitoring was performed from the hind limbs. Afterwards, thoracic and lumbar spinal cord was harvested and analysed. Results: The elevation of the MEP amplitude after RIPC was significant whereas amplitude was constantly decreased in the control group. Additionally, the onset latency was significantly shorter after RIPC during the SA cut off. The control group achieved sooner the fifty per cent decrease of MEP amplitude in the right hind limb. Histological analysis is pending and the results will be presented in the conference. Conclusions: The remote ischemic preconditioning seems to preserve spinal cord function after the left subclavian artery and SAs sacrifice as indicated by the MEP amplitudes. Simultaneously, the effect can be seen more clearly in the 41 SSRCTS 2015 right hind limb confirming the blood supply of the spinal cord being regulated by vascular network. A28 Early statin treatment dampens recovery after experimental cardiac arrest 1 1 2 3 A Mennander , V Vuohelainen , M Hämäläinen , T Paavonen , E Moilanen 1 2 2 Heart Hospital, Cardiac Research, The Immunopharmacology Research Group, Department of Pathology, Fimlab; University of Tampere School of Medicine and Tampere University Hospital, Tampere, Finland 3 [email protected] Objectives: Statin treatment after cardiac arrest is controversial. Myocardial infarction (MI) is a devastating entity after cardiac arrest due to permanent ischemia-reperfusion injury. We experimentally investigated the impact of early statin treatment on myocardial recovery after cardiac arrest and MI. Materials and methods: 28 syngeneic Fisher rats underwent heterotopic cardiac transplantation to induce reversible ischemia reperfusion after cardiac arrest (Controls). 56 rats also underwent permanent ligation of the left anterior descending coronary artery (LAD) to yield MI after cardiac arrest, of which 12 rats received Lipitor 10 mg/kg subcutaneously. Histology and qRT-PCR for endothelial nitric oxide synthase (eNOS), induced nitric oxide synthase (iNOS) and vascular cell adhesion molecule 1(VCAM-1) were performed to investigate for myocardial recovery and induction of inflammation. Results: 1 hour after reperfusion, the relative ischemia of remote intramyocardial arteries decreased temporarily in MI treated with Lipitor as compared with Controls and untreated MI (0.12±0.05 vs 2.69±1.35 and 3.50±3.58, PSU, p=0.032). After 1 day, the relative ischemia of intramyocardial arteries of the left ventricle increased in MI treated with Lipitor as compared with Controls and untreated MI (6.20±3.82 vs 0.33±0.10 and 0.95±0.42, PSU, p=0.025). Indicating myocardial ischemia, eNOS and VCAM-1 expressions increased in MI treated with Lipitor vs Controls and MI alone (3.67 vs 1.43 and 2.20, FC, p=0.040 and 9.57 vs 1.78 and 3.85, FC, p=0.028, respectively). At 1 day, no differences were observed in eNOS, iNOS or VCAM-1 expressions among the groups. Discussion: The initial temporary decrease of ischemic remote intramyocardial arteries after MI and cardiac arrest subsides soon during statin treatment; early statin intensifies ischemic myocardial response after MI and cardiac arrest. 42 SSRCTS 2015 A29 Acute volume-overload impacts early on intramyocardial arteries; an experimental rat study 1 1 1 2 3 2 C Huuskonen , R Bolkart , T Soininen , M Hämäläinen , T Paavonen , E Moilanen , A 1 Mennander 1 2 Heart Hospital, Cardiac Research, The Immunopharmacology Research Group, Department of Pathology, Fimlab; University of Tampere School of Medicine and Tampere University Hospital, Tampere, Finland 3 [email protected] Objectives: Acute volume-overload (AVO) leads to a devastating cardiac entity after surgery, often resulting in increased cardiac oxygen consumption; the histological outcome may reveal myocardial cellular destruction. We investigated whether acute AVO impacts on intramyocardial arteries early after experimental rat arterial-venous fistula. Material and methods: 27 syngeneic Fisher rats underwent surgical abdominal arterial-venous fistula to induce AVO. One day after surgery, the hearts were procured for regional and quantitative histology. 6 hearts without AVO served as Controls. Results: 23 rats survived until day 1 after AVO, while 4 rats were lost due to acute cardiac failure. Presence of subendocardial and myocardial edema, hemorrhage, inflammation and ischemia of the left and right ventricles did not differ in hearts with AVO as compared with Controls. Instead, ischemic intramyocardial arteries were abundant in the septum of the hearts with AVO as compared with Controls (0.32±0.04 vs 0.12±0.05, PSU, p=0.011), while did not differ in the right and left ventricles (0.22±0.04 vs 0.17±0.06, PSU, p=0.384 and 0.22±0.07 vs 0.19±0.05, PSU, p=0.473, respectively). Discussion: Early susceptibility of the septum is eminent after AVO; aiming treatment towards protecting intramyocardial arteries may provide novel insight against global cardiac detrition after AVO. 43 SSRCTS 2015 Abstracts - Poster presentations P01 The in-vivo comparison of a new semi flexible mitral annuloplasty ring to rigid, flat- and fully flexible mitral annuloplasty rings in a porcine model 1 1,2 1 1 1,2 MJ Tjørnild , DM Røpcke , SN Skov , C Ilkjær , SL Nielsen 1 2 Institute of Clinical Medicine and Department of Cardiothoracic and Vascular Surgery, Aarhus University Hospital, Denmark [email protected] Objectives: The aim of this study is to conduct an integrated in-vivo experimental evaluation of a newly developed semi-rigid mitral annuloplasty ring. The new ring will be compared a well-known annuloplasty rings used in today´s clinical practice: The Carpentier Edwards Classic Annuloplasty Ring, and the native heart. The evaluation and comparison of the rings will be based on, 3D geometry of the mitral annulus, leaflet coaptation geometry and leaflet curvature during heart cycle. Materials and methods: The two ring types will be implanted and tested in an acute experimental porcine model, where series of seven pigs will be randomized to receive one of the two rings. Before and after ring implantation, the dynamic 3D geometry and leaflet coaptation will be assessed by sonomicrometry and by 2D echocardiography, respectably. The recordings of the 3D leaflet geometry will be used for description of the leaflet curvature, commissure-commissure and septal-lateral mitral annular dimensions. Dedicated force transducers attached directly to the annuloplasty rings will measure annular deformational forces in the septal-lateral and commissural dimensions. A comprehensive analysis of the impact of flexible properties of the annuloplasty rings on mitral leaflet motion and stress distribution will be performed from simultaneous recordings and calculations of the mentioned parameters throughout the cardiac cycle. Results: Preliminary resultants are shown in Table 1 but more will be reviled at the conference. Conclusion: With this study, the hope is to expand the current knowledge of the complex issues concerning mitral annuloplasty. In particular, a semi-rigid annuloplasty ring might show advantages in comparison to today´s annuloplasty rings. The perspectives of the current study are to increase the number of repair 44 SSRCTS 2015 strategies in mitral annuloplasty surgery for long term valvular support and contribute to the development of future innovative annuloplasty ring designs. Type/Forces New-ring Classic Native ANT [N] POST [N] ACOM [N] PCOM [N] SL [N] CC [N] -0.09 ± 0.22 0.27 ± 0.79 -0.18 ± 0.78 -0.04 ± 0.10 0.01 ± 0.23 -0.29 ± 0.51 0.12 ± 0.18 0.30 ± 0.24 0.62 ± 0.69 0.07 ± 0.27 -0.10 ± 0.60 0.04 ± 0.27 0,30 ± 0.49 -0.38 ± 0.52 -0.37 ± 1.35 -0.13 ± 0.22 0.97 ± 1.14 -0.12 ± 2.41 Table 1. Data stated as mean ± STD and as mid diastolic - mid systolic. ANT: Anterior Segment, POST: Posterior Segment, ACOM: Anterior Commissure, PCOM: Posterior Commissure, SL: Septal-Lateral, CC: Commissure-Commissure. P02 Development of a new valve prosthesis concept for infant cardiac surgery 1 2 MB Jensen , MH Smerup , P Johansen 1,2 1 Cardiovascular Experimental Lab (CAVE Lab), Dept. of Engineering, Aarhus University, Dept. of Cardiothoracic Surgery, Aarhus University Hospital, Denmark 2 [email protected] Background: Congenital heart disease is the most common form of birth defect and are the leading cause of death from birth abnormalities in the first year of life. Approximately 8 in 1000 live births are affected by these conditions. While some conditions need immediate treatment, others might not affect the child for many years. Severe cases might need interventional catheterization, valve surgery or valve replacement. The size of an infant varies very much depending on its age. Hence, the cases where heart valve substitution is needed, it would be of great help, to be able to design a heart valve on the bench that exactly suits the individual infants. A new developed technique may be able to present such new paradigm in infant cardiac surgery. Through direct anatomical valve measures the surgeon can make an artificial heart valve based on fixated bovine pericardium and predefined templates in such a short time, that it can be done during cardiopulmonary bypass. However, initial design concept tests of the infant valve should be carefully caried out. Method: Initial experiments are conducted using upscaled heart valve designs. With a pulsatile left heart in vitro model the heart valve will be tested, to see 45 SSRCTS 2015 how it function and operate under various physiological conditions. Tests for hemodynamic properties will be carried out to investigate the transvalvular pressure gradient along with instantaneous flow recordings. Moreover, highspeed visualization of the valve will be carried out. These measures will present the hemodynamic characterization (pressure gradient, vascular impedance, valve leakage, geometric and effective orifice areas). The results will be compared to results found from identical testing with a native aortic root from a pig. Biomechanical testing will determine the stresses and strain in the various valve structures through high speed cameras and digital image correlation. This tissue load information may provide information that can be extrapolated to estimate the durability of the valve. Results: Pending. Discussion: We expect that the initial in vitro testing will result in further development of the design concepts of the infant valvesubstitute, which subsequently will be further tested with proper infant heart valve dimensions in vitro and in vivo at our animal experimental facilities. P03 The effect of TAVI oversizing on valve tissue stresses 1 1 1 1,2 3 1 SK Krishna , R Galsgaard , S Heide-Jørgensen , T Bechsgaard , R. Zegdi , L Bräuner , JV 1 1,2 Nygaard , P Johansen 1 2 Dept. of Engineering, Faculty of Science and Technology, Aarhus University, Dept. of 3 Cardiothoracic Surgery, Aarhus University Hospital, Skejby, Aarhus, Denmark, Hôpital Européen Georges Pompidou, Service de Chirurgie Cardiovasculaire, Paris, France [email protected] Objectives: Patients who suffer from aortic stenosis are most often treated with valve replacement. Traditionally, this requires an invasive procedure involving open-heart surgery and cardiopulmonary bypass. Not all patients are eligible for such treatment, and may therefore instead benefit of insertion of percutaneous valves through transcatheter aortic valve implantation (TAVI). Pre-procedural, the TAVI patients undergo CT-scanning for planning the access path and to determine the size of the TAVI valve. The TAVI valve is often selected a size larger than the aortic circumference of the patient, for better secure deployment of the valve and to minimize paravalvular leakage. The oversizing may lead to inappropriate deformations of the leaflets, altering their dynamic stress fields and reduce longevity. 46 SSRCTS 2015 The aim of this study is therefore to develop a Finite Element model to analyse the stress and strain fields on the TAVI valve leaflets during different sizing conditions. Materials and methods: CT images of a 26 mm TAVI valve, deployed in a fitted diameter tube will be obtained. This will be used to establish a 3 dimensional shell geometry CAD model. Surface smoothing and convenient mesh will be accomplished in SolidWorks. The diameter of the TAVI valve will be reduced from 26 mm to 24 mm, 22 mm, 20 mm and 18 mm, and the same aforementioned procedure will be accomplished for every TAVI valve size. Stress and strain analyses will be performed using COMSOL multi-physics, under different hemodynamic conditions. Results: Pending. P04 Comparison of the aortic root remodeling techniques - with and without a supporting annular ring. An vitro evaluation 1 1 1 2 2 2 TS Lading , DM Røpcke , T Lindskow , T Bechsgaard , P Johansen , H Nygaard , JM 1 1 Hasenkam , SL Nielsen 1 Department of Cardiothoracic & Vascular Surgery, Aarhus University Hospital, Department of Engineering, Faculty of Science and Technology, Aarhus University, Denmark 2 [email protected] Objectives: The aim of this study is to characterize the CAVIAAR technique (Conservative Aortic Valve surgery for aortic Insufficiency and Aneurysm of the Aortic Root) in vitro, comparing biomechanics of the native aortic root and valve to the root and valve after a Yacoub and a David repair technique. All three groups (native, Yacoub and David aortic roots) will be analyzed with and without a supportive external annular ring. The measurements used for comparison are leaflet dynamics, annular and aortic force distribution and hemodynamics. The CAVIAAR technique is based on wellknown repair techniques of the aortic root (David and Yacoub) adding an external subvalvular aortic annuloplasty ring, combining advantages of the original remodeling technique with the advantages of a supportive annuloplasty ring. Materials and methods: Fifteen porcine aortic roots (80 kg) will be prepared and randomized to either no aortic remodeling (n=5) or to a David (n=5) or a Yacoub (n=5) repair technique, which will be performed ex vivo before mounting the aortic root in the in vitro model.Two circular force transducers will be placed in 47 SSRCTS 2015 the aortic annulus and at the sinotubular junction, respectively, These transducers will measure annular contraction and dilation of the root. The annulus transducer consists of six strain gauges allowing individual force measuremets at each strain gauge point of the ring. The forces at each commisure of the aortic valce will be measured by attachment of three strain gauges mounted on the transducer ring at the sinotubular junction. Microtip pressure catheters will be used for pressure measurements, and a highspeed camera will be used for digital imaging of the leaflet motion and -dynamics throughout heart cycle. Results: Pending Discussion: Biomechanical and hemodynamic analysis of the CAVIAAR technique will hopefully provide knowledge for optimizing surgical procedures for aortic root repair in the relevant patient groups. This will lead to longer-lasting treatment results, lowering of costs related to re-operation, and hopefully improve the quality of life for each patient, since further knowledge allows a optimized and individualized surgical treatment of patients with aortic root pathologies. P05 Are all flexible mitral annuloplastic rings the same? An in vivo study 1 1 1,2 1 1 1,2 J Rasmussen , MJ Tjørnild , DM Røpcke , SN Skov , C Ilkjær , SL Nielsen 1 2 Institute of Clinical Medicine and Department of Cardiothoracic and Vascular Surgery, Aarhus University Hospital, Denmark [email protected] Objectives: The purpose of this experimental study is to assess the individual characteristics and different biomechanical properties of two different flexible TM TM mitral annuloplasty rings (Medtronic Simulus and Medtronic Duran ). This will be done with special emphasis on the rings different impact on mitral annular dynamics and force distribution and also the remodeling effect on the entire mitral valve apparatus. The evaluation and comparison of the rings will be based on 3D geometry of the mitral annulus, leaflet coaptation geometry and leaflet curvature during the heart cycle. Force quantification and distribution on the valve will also be evaluated. Material and methods: The two different types of annuloplasty rings will be surgically implanted and tested in an acute porcine model. To establish a TM reference, a completely rigid mitral annular plastic ring (Medtronic Classic ) 48 SSRCTS 2015 and the native heart without any implant, will be tested using the exact same procedures. Twenty animals (80 kg) will be used for testing, equally distributed amongst the four groups of either a ring or the native heart. Before and after ring implantation, the dynamic 3D geometry and leaflet coaptation will be assessed by sonomicrometry and by 2D echocardiography, respectably. The recordings of the 3D leaflet geometry will be used for description of the leaflet curvature, commissure-commissure and septal-lateral mitral annular dimensions. Force transducers attached directly to the annuloplasty rings will measure annular deformational forces. A comprehensive analysis of each rings impact on the mitral valve and its leaflets motion and stress distribution will be performed from simultaneous recordings of the mentioned parameters throughout the cardiac cycle. Results: Pending. TM Conclusion: We hypothesize that the Medtronic Simulus ring, compared to TM the Medtronic Duran ring, provide better support of the mitral annulus by reducing annular motion and the resulting deformational forces of mitral TM annulus during the cardiac cycle. We anticipate that the Medtronic Simulus ring, hereby, possess the ability to reshape the mitral annulus in specific regions, a feature usually associated with the more rigid annuloplasty rings, while allowing physiological motion of the annulus and leaflets due to its flexible properties. P06 Giant right atrial myxoma presenting as chronic obstructive pulmonary disease 1 2 3 S Kumar , C Howes , A Delvecchio , PN Bonde 1 1 2 Section of Cardiac Surgery and Section of Cardiology, Yale University School of Medicine, 3 New Haven, Connecticut, Department of Cardiology, Greenwich Hospital, Greenwich, Connecticut, USA [email protected] Background: Myxomas are the commonest benign tumour of heart with upto 20% located in the right atrium (RA). This rare case of giant RA myxoma presented as chronic obstructive pulmonary disease. Material and methods: 47 years old female was being followed for increasing dyspnea for 6 months duration. She gave a history of polysubstance abuse using cocaine and marijuana. Her shortness of breath started insidiously with moderate efforts and gradually progressed with mild efforts. She had dry cough 49 SSRCTS 2015 and progressive edema of lower extremities for 1 week associated with fatigue. There was no associated history suggestive of fever, chills, palpitation, chest pain, syncopal episodes, dizziness and orthopnea or paroxysmal nocturnal dyspnea. She had been treated as chronic obstructive pulmonary disease with Albuterol and Salmeterol /Fluticasone without any response to treatment. Result: The echocardiogram revealed 6.5x5.5 cm RA mass prolapsing through the tricuspid valve into right ventricle. She made an uneventful recovery following excision of RA myxoma through median sternotomy under cardiopulmonary bypass. Discussion: The dyspnoea should not be a real cardiac symptom when there is a right atrial occupation like in this case, but dyspnoea can also be present in right-sided pathology. P07 Metachronous metastatic hepatocellular carcinoma to the right ventricle S Kumar, AA Mangi Section of Cardiac Surgery, Yale University School of Medicine, New Haven, Connecticut, USA [email protected] Background: We present a very rare case of isolated metastasis to the right ventricle (RV) from hepatocellular carcinoma (HCC) for which he underwent a left hepatectomy a few years earlier. Material and methods: 71 year old gentleman presented with an episode of atypical chest pain. He had extended left hepatectomy with caudate lobectomy for hepatocellular carcinoma 3 years earlier, with no evidence of recurrence on restaging scans 1 year ago. ECG revealed sinus rhythm with new right bundle branch block and stress test with anterior ischemic, affixed inferoseptal defect and inferior ischemia. TTE showed a normal EF but a large RV mass. His hepatitis panel, CEA and AFP were negative. CT chest showed a 8x5x4.5 cm mass involving the anterior wall of the RV, extending from the level of the outflow tract to the apex. CT abdomen/pelvis showed no evidence of recurrent or metastatic disease. Cardiac catheterization showed right coronary artery (RCA) with ostial and proximal 80% lesions just prior to a large saccular aneurysm arising from the proximal vessel. MRI revealed a large hypervascular 7x5x4.5 cm enhancing RV mass involving approximately 50% of the RV free wall and the entire anterior wall. There was 50% invasion of the interventricular septum with 50 SSRCTS 2015 slight narrowing of the RV outflow tract without hemodynamically significant obstruction. Result: The patient underwent debulking of RV mass, intracardiac excisional biopsy of RV mass, plication of RCA aneurysm, and coronary artery bypass grafting x1 with reverse saphenous vein graft to the distal RCA. The tumor was only debulked because it was of metastatic origin on frozen section and occupied approximately two thirds of the anterior wall of the right ventricle, straddled the intraventricular septum and encased the midportion of the left anterior descending coronary artery for a length of about 8 cm, and extended onto the left ventricle for about 2 cm. He had uncomplicated recovery and was discharged home on post-operative 7 in good condition to follow up with his oncologist for further treatment of the residual RV tumor. Discussion: HCC tend to metastasize to the lungs, bones, and abdominal organs much more frequently. There is no reported case in literature of HCC metastasizing to the heart in association with RCA aneurysm. P08 Cavitation in patiens with bileaflet mechanical heart valves 1,2 2 2 2 2 P Johansen , TS Andersen , JM Hasenkam , H Nygaard , PK Paulsen 1 2 Dept. of Engineering, Faculty of Science and Technology, Aarhus University, Dept. of Cardiothoracic Surgery, Aarhus University Hospital, Skejby, Aarhus, Denmark [email protected] Objectives: Today, the quality of mechanical heart valves is quite high, and implantation has become a routine clinical procedure with a low operative mortality (< 5%). However, patients still face the risks of blood cell damage, thromboembolic events, and material failure of the prosthetic device. One mechanism found to be a possible contributor to these adverse effects is cavitation. In vitro, cavitation has been directly demonstrated by visualization and indirectly in vivo by registering of high frequency pressure fluctuations (HFPF). Tilting disc valves are thought of having higher cavitation potential than bileaflet valves due to higher closing velocities. However, the thromboembolic potential seems to be the same. Further studies are therefore needed to investigate the cavitation potential of bileaflet valves in vivo. The post processing of HFPF have shown difficulties when applied on bileaflet vavles due to asynchronous closure of the two leaflets. The aim of this study was therefore to isolate the pressure 51 SSRCTS 2015 signature from each leaflet closure and perform cavitation analyses on each component. Materials and methods: Six patients were included in the study (St. Jude Medical (n=3) and CarboMedics (n=3); all aortic bileaflet mechanical heart valves). HFPFs were recorded intraoperatively through a hydrophone at the aortic root. The pressure signature relating to the first and second leaflet closure was isolated and cavitation parameters were calculated (RMS after 50 kHz highpass filtering and signal energy). Data were averaged over 30 heart cycles. Results: For all patients both the RMS value and signal energy of the second leaflet closure were higher than for the first leaflet closure. Discussion: These results indicate that the second leaflet closure is most prone to cause cavitation. Therefore, quantifying cavitation based on the HFPF related to the second leaflet closure may suggest that the cavitation potential for bileaflet valves in vivo may be higher than previous studies have suggested. P09 Major ischemic stroke caused by air embolism from a ruptured giant pulmonary bulla 1 2 1 3 JF Gudmundsdottir , BL Thorarinsson , G Myrdal , P Hannesson , T Gudbjartsson 1 2 1,4 3 Departments of Cardiothoracic Surgery, Neurology, and Radiology, Landspitali 4 University Hospital. Faculty of Medicine, University of Iceland, Reykjavík, Iceland [email protected] Introduction: Giant pulmonary bullae (GPB) occupy more than one third of the hemithorax. They often cause complications, such as pneumothorax, hemorrhage or lung infections. We report a case of major ischemic stroke in a patient with giant pulmonary bulla, that ruptured during a commercial flight. Case: A 58 year old non-smoking male, previously healthy, suddenly experienced aphasia and right hemiplegia during a flight over the North Atlantic. After an emergency landing he was transported to our hospital in Reykjavik. On admission he complained of left-sided chest pain with dyspnea and a chest tube was inserted for a left sided pneumothorax. An acute CT scan and MRI of the head showed signs of acute ischemic cerebral infarction. Furthermore, air bubbles consistent with air emboli could be identified in his left sided intracerebral arteries. A chest CT then revealed a 15x13cm thin-walled GPB in the left upper lobe. One month after admission the GPB was removed with upper left lobectomy. Pathologic examination showed a benign thick-walled bulla and emphysematous lung tissue. He was discharged 2 weeks later after an 52 SSRCTS 2015 uneventful post-operative recovery and flew back to England where he is recovering from his stroke. Discussion. Giant pulmonary bullae are uncommon, especially in non-smokers. Ischemic stroke caused by air embolism due to ruptured bulla is very rare, but so far a couple of cases have been reported during a flight. P10 David versus Yacoub aortic root repair: Assessment and comparison of stress distribution in the aortic root - a clinical porcine experimental study 1,3 1,3 2,3 1,3 T Lindskow , MJ Tjørnild , T Bechsgaard , DM Røpcke , SL Nielsen 1,3 1 Department of Cardiothoracic and Vascular Surgery, Aarhus University Hospital, 3 Department of Biomedical Engineering and Clinical Institute of Medicine, Aarhus University Hospital, Denmark 2 [email protected] Objectives: Recent years of research has showed that aortic valve repair is superior to valve substitution in patients with aortic regurgitation due to aortic dilatation if the valve cusps themselves are normal. The aim of this study is to assess and compare stress distribution in the aortic root after aortic root repair using two of the most commonly accepted techniques developed by Dr Tirone E. David (The David valve re-implantation procedure) and Sir Magdi Yacoub (The Yacoub re-modelling procedure), respectively. Materials and methods: Fifteen pigs (90 kg) will be randomized to either a David repair (n=5), a Yocoub repair (n=5) or no repair at all (n=5). A median sternotomy will be performed and cardiopulmonary bypass will be established followed by cardioplegia and resection of the aortic root including freedissection of the coronary buttons. Hereafter a force transducer will be sutured to the aortic annulus just below the valve. This will enable measuring of stress distribution both in plane (annulus dilation/contraction) and out of plane (annulus bending). Fifteen piezoelectric crystals for sonomicrometric measurements will be implanted at four levels around the circumference of the aortic root (three at the annular level, three at each commissure tip, three at the sinotubular junction, three in the ascending aorta, and one on each free edge of the three aortic cusps). The sonomicrometric crystals will display 3D geometry of the changes in the aortic root. Two microtip pressure catheters will be inserted in the left ventricle and atrium for direct pressure measurements. After weaning from cardiopulmonary bypass and hemodynamic stabilization, data will be collected over 10 cardiac cycles. 53 SSRCTS 2015 Force distribution and 3D configuration/behavior of the aortic root will be described and compared between groups. Results: Results are pending. Conclusion: With this study we hope to gain more knowledge about the normal aortic root and also gain insight into different repair techniques, hopefully enabling surgeons to choose the right repair technique for each patient, depending on pathology and aortic root anatomy. 54 SSRCTS 2015 Authors’ index Agnarsson B ................................ A15 Andersen TS ................................ P08 Andreasen JJ ............................... A18 Anttila T .............................. A12, A27 Anttila V .............................. A12, A27 Arason AJ .................................... A05 Arvola O ...................................... A27 Baandrup UTh ............................. A18 Bechsgaard T ..................... A09, A13, .....................................P03, P04, P10 Bjornsson E ................................. A23 Bjornsson J .................................. A04 Bogdanova M.............................. A24 Bolkart R ..................................... A29 Bonde PN .................................... P06 Bräuner L .................................... P03 Bruus D ....................................... A07 Danielsen R ................................. A22 Delvecchio A ............................... P06 Eyjolfsson K................................. A23 Fonager K .................................... A18 Franzdottir SR ............................. A05 Fröjd V ........................................ A10 Galsgaard R ......................... A07, P03 Geirsson A...........A15, A21, A22, A26 Ghasemzadeh N.......................... A23 Gislason G ................................... A18 Grønlund J .................................. A03 Gudbjartsson DF ......................... A23 Gudbjartsson T .......... A04, A05, A15, .................... A21, A22, A23, A26, P09 Gudjonsson Th ............................ A05 Gudmundsdottir JF ............. A22, P09 Gudmundsson G ......................... A05 Gudnason Th .............................. A23 Haapanen H ........................ A12, A27 Haapasalo H ................................ A14 Hakimi CS .................................... A06 Hämäläinen M .................... A28, A29 Hannesson P ............................... P09 Hansson E ................................... A06 Hasenkam JM ............. A18, P04, P08 Hautalahti J ................................. A16 Heide-Jørgensen S .............. A09, P03 Hejslet T ...................................... A01 Helgadottir A............................... A23 Helgadottir S ............................... A26 Helgason D .................................. A26 Herajärvi J ........................... A12, A27 Hesse C ....................................... A02 Hjortdal VE ..................A01, A03, A08 Howes C ...................................... P06 Huuskonen C ............................... A29 Hyttinen J .................................... A16 Hønge JL ......................A09, A13, A18 Ilkjær C ................ A01, A17, P01, P05 Ingvarsdottir IL ............................ A26 Isaksson HJ .......................... A04, A05 Jensen H ...................................... A01 Jensen M ..................................... A17 Jensen MB................................... P02 Jensen MOJ ................................. A01 Jeppsson A ..................A02, A06, A10 Johannesdottir RM ..................... A21 Johansen P .................A07, A09, A13, ............................ P02, P03, P04, P08 Jonsdottir HR .............................. A05 Jonsson S..................................... A04 Joutsen A .................................... A16 Jungebluth P ............................... A11 Juvonen T ............................ A12, A27 Kallio M ............................... A12, A27 Karppinen P ................................ A12 Karunanithi Z............................... A08 Kiviluoma K ......................... A12, A27 Kjærgaard B ................................ A18 Krishna SK ........................... A09, P03 Kristensen SR .............................. A18 Kumar S ............................... P06, P07 Lading TS ..................................... P04 Laugesen S .................................. A13 Laukka T ...................................... A12 Laurikka J .................................... A16 Lim ML ........................................ A11 Lindhardt I................................... A07 Lindskow T .......................... P04, P10 Lund SH ....................................... A15 Macchiarini P .............................. A11 55 SSRCTS 2015 Magnusdottir SO ........................ A18 Magnusson MK ........................... A05 Malashicheva A........................... A24 Malm CJ ...................................... A06 Mangi AA .................................... P07 Melvinsdottir IH .......................... A15 Mennander A .............. A14, A28, A29 Moilanen E .......................... A28, A29 Muola P ...................................... A14 Mustonen C ................................ A12 Myrdal G ..................................... P09 Nielsen SL .................. A01, A13, A17, .............................P01, P04, P05, P10 Niinimaki E .................................. A14 Nozohoor S ......................... A20, A25 Nyboe C ...................................... A08 Nygaard H ........... A13, A17, P04, P08 Nygaard JV .................................. P03 Orrason AW ................................ A26 Oskarsdottir GN .......................... A04 Paavonen T ................. A14, A28, A29 Paldanius A ................................. A16 Palsson R..................................... A05 Parkkila S .................................... A14 Patel RS ....................................... A23 Paulsen PK .................................. P08 Quyyumi AA ................................ A23 Ragnarsson S............... A20, A22, A25 Rasmussen BS ............................. A18 Rasmussen J................................ P05 Rutkovskiy A ............................... A24 Røpcke DM ........................ A01, A17, .............................P01, P04, P05, P10 Sarja H ........................................ A12 Siefert AW .................................. A17 Singh S ........................................ A02 Sjögren J ............................. A20, A25 Sjöqvist S..................................... A11 Skov SN ............... A03, A17, P01, P05 Smerup MH................................. P02 Soininen T ................................... A29 Stagmo M ........................... A20, A25 Starck T ............................... A12, A27 Stefansson K ............................... A23 Sørensen AV ............................... A01 Taborsky J ................................... A09 Telinius N .................................... A03 Thorarinsson BL .......................... P09 Thorgeirsson G ............................ A23 Thorleifsson G ............................. A23 Thorsteinsdottir U....................... A23 Thorsteinsson K .......................... A18 Timane P ..................................... A25 Tjørnild MJ .......... A17, P01, P05, P10 Torp-Pedersen C ......................... A18 Tuominen H ........................ A12, A27 Vaage J ........................................ A24 Viktorsson SA .............................. A26 Vuohelainen V............................. A28 Weng PBS.................................... A07 Wierup P ............................. A20, A25 Yoganathan A .............................. A17 Zegdi R ................................ A09, P03 Ølgaard M ................................... A03 56 SSRCTS 2015 57


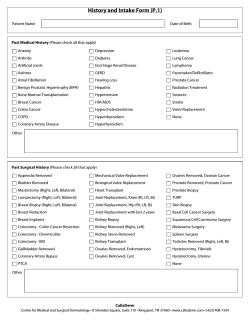







© Copyright 2026