
Microbiome may drive the course of diabetes, obesity
VOL. 9 NO. 5 MAY 2015 Microbiome may drive the course of diabetes, obesity I N S I D E Bacterial balance may afect metabolism. News from the AGA BY MICHELE G. Fairbanks s chool oF Public h ealth at iuPu ® Dr. Hongmei Nan and colleagues found that aspirin/NSAIDs’ protection against colon cancer is based on 3 polymorphisms. NSAIDs’ ca protection tied to gene variations BY MARY ANN MOON Frontline Medical News T he well-documented protective efect that aspirin and nonsteroidal anti-infammatory drugs exert against colon cancer has been linked to three genetic variations at chromosome 12 and 15, according to a report published online in JAMA. In a genome-wide investigation of the interrelationship between genetic markers and the regular use of aspirin/NSAIDs, researchers found that the drugs were diferentially associated with colorectal cancer risk according to variations at single-nucleotide polymor- phisms (SNPs) on chromosome 12p12.3 (rs2965667 and rs10505806) and chromosome 15q25.2 (rs16973225). These fndings “can help to identify population subgroups defned by genetic background that may preferentially beneft from chemopreventive use of these agents and ofer novel insights into underlying mechanisms of carcinogenesis,” said Dr. Hongmei Nan of the department of epidemiology at Indiana University and the Bren Simon Cancer Center, both in Indianapolis, and her associates. To obtain a large population for the genome-wide See Colon cancer · page 24 SULLIVAN Frontline Medical News E merging research suggests that the complex microbial gut communities – which interact fuidly not only with their human host, but also with each other – play important roles in health and disease. They appear to confer both protection from and risk for many chronic illnesses, from asthma and allergies to obesity and diabetes. And what we don’t know about them dwarfs what we do know, said Dr. Robert Ratner, the chief medical ofcer of the American Diabetes Association, at the annual advanced postgraduate course held by the ADA. The microbiome is as individual as every person who carries it. The diferences are myriad, in the amount and variety of species, and in the sheer numbers of microbes that make up each community. Each region of the gut, from mouth to rectum, hosts a completely diferent population. Two main phyla populate the gut: Bacteroidetes, which are involved in protein and carbohydrate breakdown, and Firmicutes, which promote the absorption of fat. The ratios See Microbiome · page 30 News Stage 3 meaningful use CMS says all should be ready by 2018. • 4 Strategic Plan 2015-2020 Dr. John I. Allen outlines a vision for AGA’s future. • 17 Liver Diseases Are the new HCV drugs cost effective? Two complex studies examine the issue. • 18 IBD and Intestinal Disorders Stem cells for Crohn’s fstula Long-term relief reported in small study. • 30 SGR repeal refocuses CMS on value BY GREGORY TWACHTMAN Frontline Medical News I t’s value over volume for Medicare now that the Medicare Access and CHIP Reauthorization Act of 2015 is law. “AGA is pleased that the SGR repeal has fnally happened and puts physicians on a pathway toward value-based care,” said Dr. John I. Allen, MBA, AGAF, president, AGA Institute. “AGA will continue to work with Medicare and private payers on developing bundled payment models and other alternative payment models that demonstrate the value of GI services that we provide.” “There are a lot of evolv- ing issues to take care of in this migration toward models of payment delivery that work positively toward impacting quality of care,” Dr. James Madara, CEO of the American Medical Association, said April 15, the day after the Senate passed H.R. 2, the Medicare Access and CHIP Reauthorization See SGR repeal · page 41 2015 JAMES W. FRESTON CONFERENCE A RENAISSANCE IN THE UNDERSTANDING AND MANAGEMENT OF IBS AUG. 29 & 30, 2015 • CHICAGO, IL Learn what advances in IBS can help improve care for your patients at www.gastro.org/frestonibs. Funded by the Takeda Endowment in support of the James W. Freston Single Topic Conference. 125-134EDU_15-1 GI & HepatoloGy News 151 Fairchild Ave., Suite 2, Plainview, NY 11803-1709 CHANGE SERVICE REQUESTED Presorted Standard U.S. Postage PAID Permit No. 384 Lebanon Jct. KY NEWS 2 MAY 2 0 1 5 • G I & HEPATO LO G Y NEW S CLINICAL CHALLENGES AND IMAGES What’s your diagnosis? A 70-year-old man presented to the emergency department because of abdominal pain with vomiting for 1 day. The patient had a past history of peptic ulcer disease and underwent subtotal gastrectomy > 20 years ago; he was afebrile and his blood pressure was 181/110 mm Hg. He reported no bloody or tarry stool in recent days. However, after nasogastric tube The patient had a past history of peptic ulcer disease and underwent subtotal gastrectomy > 20 years ago. decompression, some cofee-ground material was observed. Physical examination showed a midline scar at the epigastric region. Severe tenderness and distention of the upper abdomen with hyperactive bowel sounds were noted. The laboratory values of liver functions and lipase were within normal limits, but there was leukocytosis with a white blood count of 11,440/mcL. His hemoglobin was 13 g/dL (normal, 13-17). Computed tomography (CT) was then carried out (Figure A). AGA InstItute By Dr. Shih-Ming Huang, Dr. ShihWen Chang, and Dr. Yeu-Sheng Tyan. Published previously in Gastroenterology (2012;143;29, 272, 273). The diagnosis appears on page 40. U.S. experiencing drug-resistant shigellosis outbreak BY DEEPAK CHITNIS Frontline Medical News T he United States is currently experiencing an outbreak of shigellosis caused by a strain of the Shigella sonnei bacteria that is resistant to ciprofoxacin, the most commonly prescribed antimicrobial treatment for shigellosis. In its Morbidity and Mortality Weekly Report, the Centers for Disease Control and Prevention revealed that 243 individuals in 32 states and the territory of Puerto Rico have come down with shigellosis between May 2014 and February 2015. Of those 243 cases, 126 isolates were tested and 109 (87%) of those were found to be nonsusceptible to ciprofoxacin. The largest clusters of the disease were found in Massachusetts (45 cases), in ChiEf Colin W. Howden, M.D., AGAF Editor AssoCiAtE Editors Joel V. Brill, M.D., AGAF Barbara H. Jung, M.D. Bryson Katona, M.D., Ph.D. John A. Martin, M.D. Kevin D. Mullen, M.D., FRCPI David T. Rubin, M.D., AGAF Editor EmEritus Charles J. Lightdale, M.D., AGAF AGA institutE stAff Managing Editor Brook A. Simpson Special Content Editor Lindsey M. Brounstein Publications Coordinator Jillian L. Schweitzer Vice President of Publications Erin C. Dubnansky offiCErs of thE AGA institutE President John I. Allen, M.D., MBA, AGAF President-Elect Michael Camilleri, M.D., AGAF Vice President Timothy C. Wang, M.D., AGAF Secretary/Treasurer Francis M. Giardiello, M.D., AGAF AGA Research Foundation Chair Martin Brotman, M.D., AGAF Past President Anil K. Rustgi, M.D., AGAF ©2015 by the AGA Institute. All rights reserved. No part of this publication may be reproduced or transmitted in any form or by any means, electronic or mechanical, including photocopy, recording, or any information storage and retrieval system, without permission in writing from the publisher. California (25 cases), and Pennsylvania (18 cases). Ninety-fve of the cases associated with the current outbreak were traced back to the homeless population of San Francisco; about half of the remaining cases were attributed to international travelers – specifcally, those visiting the Dominican Republic and India – who contracted the bacteria while abroad and unknowingly brought it to the United States. The disease is known to spread quickly in populations of children who attend child care facilities, homeless individuals, and men who have sex with men. “These outbreaks show a troubling trend in Shigella infections in the United States,” Dr. Thomas Frieden, CDC director, said in a statement. “Drug-resistant infections are harder to treat and because Shigella spreads so easily between people, Gi & hEpAtoloGy nEws is the offcial newspaper of the American Gastroenterological Association (AGA) Institute and provides the gastroenterologist with timely and relevant news and commentary about clinical developments and about the impact of health care policy. Content for Gi & hEpAtoloGy nEws is developed through a partnership of the newspaper’s medical board of editors (Editor in Chief and Associate Editors), Frontline Medical Communications Inc. and the AGA Institute Staff. “From the AGA” is provided exclusively by the AGA, AGA Institute, and FDHN. All content is reviewed by the medical board of editors for accuracy, timeliness, and pertinence. To add clarity and context to important developments in the feld, select content is reviewed by and commented on by external experts selected by the board of editors. The ideas and opinions expressed in Gi & hEpAtoloGy nEws do not necessarily refect those of the AGA Institute or the Publisher. The AGA Institute and Frontline Medical Communications Inc. will not assume responsibility for damages, loss, or claims of any kind arising from or related to the information contained in this publication, including any claims related to the products, drugs, or services mentioned herein. Advertisements do not constitute endorsement of products on the part of the AGA Institute or Frontline Medical Communications Inc. POSTMASTER Send changes of address (with old mailing label) to GI & Hepatology News, Subscription Service, 151 Fairchild Ave., Suite 2, Plainview, NY 118031709. The AGA Institute headquarters is located at 4930 Del Ray Avenue, Bethesda, MD 20814, [email protected]. Editorial Offces 5635 Fishers Lane, Suite 6100, Rockville, MD 20852, 240-221-2400, fax 240-221-2548 Gi & hEpAtoloGy nEws (ISSN 1934-3450) is published monthly for $230.00 per year by Frontline Medical Communications Inc., 7 Century Drive, Suite 302, Parsippany, NJ 07054-4609. Phone 973-206-3434, fax 973-206-9378 Scan this QR Code to visit gihepnews.com the potential for more – and larger – outbreaks is a real concern. We’re moving quickly to implement a national strategy to curb antibiotic resistance because we can’t take for granted that we’ll always have the drugs we need to fght common infections.” Shigellosis causes an estimated 500,000 cases of diarrhea in the United States each year. To help curb the growing number of shigellosis cases, the CDC recommends that international travelers wash their hands meticulously while abroad, and follow strict dietary precautions, such as eating hot foods and drinking beverages only from sealed containers, especially when consuming water. [email protected] frontlinE mEdiCAl CommuniCAtions soCiEty pArtnErs VP/Group Publisher; Director, FMC Society Partners Mark Branca Editor in Chief Mary Jo M. Dales Executive Editors Denise Fulton, Kathy Scarbeck Managing Editor Lora T. McGlade Creative Director Louise A. Koenig Print Production Manager Rebecca Slebodnik Display Advertising Sales Representative James G. Pattis, 201-767-4170, fax 201-767-2784, [email protected] Senior Director of Sales Tim LaPella, 484-921-5001, [email protected] Classifed Sales Representative Linda Wilson 973-290-8243, [email protected] Advertising Offces 7 Century Drive, Suite 302, Parsippany, NJ 07054-4609 973-206-3434, fax 973-206-9378 FRONTLINE MEDICAL COMMUNICATIONS Stephen Stoneburn, Chairman Douglas E. Grose, EVP Digital Business Development/CFO Alan J. Imhoff, President/CEO JoAnn Wahl, President, Custom Solutions, 973-206-8989 [email protected] Dennis Quirk, VP, Finance Jim Chicca, Executive Director, Operations Jim McDonough, VP, Marketing & Customer Advocacy Carol Nathan, VP, Custom Programs Lori Raskin, Corporate Director, Research & Communications Donna Sickles, VP, Audience Development Subscription Inquiry Line 1-800-480-4851 In affliation with Global Academy for Medical Education, LLC. Sylvia H. Reitman, MBA, Vice President, Medical Education & Conferences David J. Small, MBA, Vice President, Events 1 MOST PRESCRIBED, # BRANDED BOWEL PREP KIT1 A CLEAN SWEEP EFFECTIVE RESULTS IN ALL COLON SEGMENTS >90% no residual stool in all colon segments compared to Standard 4-Liter Prep2*†‡ · These results were statistically significant in the cecum (P=.010)2*§ · Significantly more subjects in SUPREP® group had no residual fluid in 4 out of 5 colon segments2*‡ Help meet Gastroenterology Quality Improvement Consortium (GIQuIC) benchmarks for 85% quality cleansing3 with the split-dose efficacy of SUPREP ® Bowel Prep Kit.4 *This clinical trial was not included in the product labeling. †Standard 4-Liter Prep [sulfate-free PEG electrolyte lavage solution]. ‡Based on investigator grading. §Statistically significant difference. References: 1. IMS Health, NPA Weekly, March 2015. 2. Rex DK, Di Palma JA, Rodriguez R, McGowan J, Cleveland M. A randomized clinical study comparing reduced-volume oral sulfate solution with standard 4-liter sulfate-free electrolyte lavage solution as preparation for colonoscopy. Gastrointest Endosc. 2010;72(2):328-336. 3. Rex DK, Schoenfeld PS, Cohen J, et al. Quality indicators for colonoscopy. Gastrointest Endosc. 2015;81(1):31-53. 4. SUPREP Bowel Prep Kit [package insert]. Braintree, MA: Braintree Laboratories, Inc; 2012. ©2015 Braintree Laboratories, Inc. GIHEP_3.indd 1 16-00590 March 2015 4/14/2015 4:30:57 PM NEWS 4 MAY 2 0 1 5 • G I & HEPATO LO G Y NEW S CMS: Stage 3 meaningful use by 2018 Frontline Medical News A ll physicians and hospitals would need to meet stage 3 meaningful use beginning in 2018, according to a recent proposal by the Centers for Medicare & Medicaid Services. In the agency’s Stage 3 proposed rule, there would be no transition period from earlier stages for those just starting or those who were in an earlier stage. CMS said that this is “expected to be the fnal stage” and will incorporate elements of the previous two stages. That change comes along with the proposal beginning in 2017 to permanently make the attestation period a full year, with a few exceptions. A full-year attestation period was supposed to go into efect for 2015 with Stage 2, but CMS announced that it would reduce attestation to a 90-day period because of low participation. The fnal year in which participants in the EHR Incentive Programs can receive bonus payments for meeting meaningful use criteria is 2017; pen- K oKouu /IstocKphoto . com BY GREGORY TWACHTMAN IMPORTANT SAFETY INFORMATION SUPREP® Bowel Prep Kit (sodium sulfate, potassium sulfate and magnesium sulfate) Oral Solution is an osmotic laxative indicated for cleansing of the colon as a preparation for colonoscopy in adults. Most common adverse reactions (>2%) are overall discomfort, abdominal distention, abdominal pain, nausea, vomiting and headache. Use is contraindicated in the following conditions: gastrointestinal (GI) obstruction, bowel perforation, toxic colitis and toxic megacolon, gastric retention, ileus, known allergies to components of the kit. Use caution when prescribing for patients with a history of seizures, arrhythmias, impaired gag refex, regurgitation or aspiration, severe active ulcerative colitis, impaired renal function or patients taking medications that may affect renal function or electrolytes. Use can cause temporary elevations in uric acid. Uric acid fuctuations in patients with gout may precipitate an acute fare. Administration of osmotic laxative products may produce mucosal aphthous ulcerations, and there have been reports of more serious cases of ischemic colitis requiring hospitalization. Patients with impaired water handling who experience severe vomiting should be closely monitored including measurement of electrolytes. Advise all patients to hydrate adequately before, during, and after use. Each bottle must be diluted with water to a fnal volume of 16 ounces and ingestion of additional water as recommended is important to patient tolerance. BRIEF SUMMARY: Before prescribing, please see full Prescribing Information and Medication Guide for SUPREP® Bowel Prep Kit (sodium sulfate, potassium sulfate and magnesium sulfate) Oral Solution. INDICATIONS AND USAGE: An osmotic laxative indicated for cleansing of the colon as a preparation for colonoscopy in adults. CONTRAINDICATIONS: Use is contraindicated in the following conditions: gastrointestinal (GI) obstruction, bowel perforation, toxic colitis and toxic megacolon, gastric retention, ileus, known allergies to components of the kit. WARNINGS AND PRECAUTIONS: SUPREP Bowel Prep Kit is an osmotic laxative indicated for cleansing of the colon as a preparation for colonoscopy in adults. Use is contraindicated in the following conditions: gastrointestinal (GI) obstruction, bowel perforation, toxic colitis and toxic megacolon, gastric retention, ileus, known allergies to components of the kit. Use caution when prescribing for patients with a history of seizures, arrhythmias, impaired gag refex, regurgitation or aspiration, severe active ulcerative colitis, impaired renal function or patients taking medications that may affect renal function or electrolytes. Pre-dose and post-colonoscopy ECG’s should be considered in patients at increased risk of serious cardiac arrhythmias. Use can cause temporary elevations in uric acid. Uric acid fuctuations in patients with gout may precipitate an acute fare. Administration of osmotic laxative products may produce mucosal aphthous ulcerations, and there have been reports of more serious cases of ischemic colitis requiring hospitalization. Patients with impaired water handling who experience severe vomiting should be closely monitored including measurement of electrolytes. Advise all patients to hydrate adequately before, during, and after use. Each bottle must be diluted with water to a fnal volume of 16 ounces and ingestion of additional water as recommended is important to patient tolerance. Pregnancy: Pregnancy Category C. Animal reproduction studies have not been conducted. It is not known whether this product can cause fetal harm or can affect reproductive capacity. Pediatric Use: Safety and effectiveness in pediatric patients has not been established. Geriatric Use: Of the 375 patients who took SUPREP Bowel Prep Kit in clinical trials, 94 (25%) were 65 years of age or older, while 25 (7%) were 75 years of age or older. No overall differences in safety or effectiveness of SUPREP Bowel Prep Kit administered as a split-dose (2-day) regimen were observed between geriatric patients and younger patients. DRUG INTERACTIONS: Oral medication administered within one hour of the start of administration of SUPREP may not be absorbed completely. ADVERSE REACTIONS: Most common adverse reactions (>2%) are overall discomfort, abdominal distention, abdominal pain, nausea, vomiting and headache. Oral Administration: Split-Dose (Two-Day) Regimen: Early in the evening prior to the colonoscopy: Pour the contents of one bottle of SUPREP Bowel Prep Kit into the mixing container provided. Fill the container with water to the 16 ounce fll line, and drink the entire amount. Drink two additional containers flled to the 16 ounce line with water over the next hour. Consume only a light breakfast or have only clear liquids on the day before colonoscopy. Day of Colonoscopy (10 to 12 hours after the evening dose): Pour the contents of the second SUPREP Bowel Prep Kit into the mixing container provided. Fill the container with water to the 16 ounce fll line, and drink the entire amount. Drink two additional containers flled to the 16 ounce line with water over the next hour. Complete all SUPREP Bowel Prep Kit and required water at least two hours prior to colonoscopy. Consume only clear liquids until after the colonoscopy. STORAGE: Store at 20°-25°C (68°-77°F). Excursions permitted between 15°-30°C (59°-86°F). Rx only. Distributed by Braintree Laboratories, Inc. Braintree, MA 02185 For additional information, please call 1-800-874-6756 or visit www.suprepkit.com ©2015 Braintree Laboratories, Inc. 16-00590 March 2015 alties for failing to meet criteria have already begun. The proposed rule also contains a number of more stringent requirements. On the patient engagement front, the proposed rule calls for 25% of patients to access their data, although it also allows for third-party providers to access a patient’s account as a means of satisfying the requirement. Patient-generated data also are highlighted, with a proposed requirement that physicians collect information via mobile devices or apps from 15% of their patients. Under the proposed Stage 3 of meaningful use, physicians and eligible hospitals must meet two of three criteria: that more than 50% of referrals or transitions of care involve the passing of information by the referring provider; that more than 40% of transitions or referrals received by a provider seeing a patient for the frst time include information imported into that new provider’s EHR; or that for more than 80% of those new patients seen in transition or by referral for the frst time, a clinical reconciliation be done on the information received during the health information exchange, including a review of current medications, medication allergies, and current and active diagnoses. The proposed rule is scheduled to be published in the Federal Register on March 30; comments will be accepted at www.regulations.gov until May 29. [email protected] Pages 4a—4b u NEWS GIHEP NEW S. COM • M AY 2015 5 Mongersen has 55%-65% remission rates in Crohn’s BY MARY ANN MOON Frontline Medical News M ongersen, an oral SMAD7 antisense oligonucleotide formulated to deliver its active ingredient primarily into the lumen of the terminal ileum and right colon, induced remission rates as high as 55%-65% in a small, brief, manufacturer-sponsored, phase II clinical trial, according to a report published online in the New England Journal of Medicine. In Crohn’s disease, gut infammation is characterized by abnormal reductions in a particular immunosuppressive cytokine caused by increased levels of SMAD7. Mongersen (formerly GED0301) downregulates SMAD7 using a classic antisense mechanism, which in turn restores the proper cytokine function and suppresses infammation, said Dr. Giovanni Monteleone of the department of systems medicine, University of Tor Vergata, Rome, and his associates. They assessed a 2-week course of mongersen in 166 adults with active, moderate to severe Crohn’s disease who were treated and followed for PERSPECTIVE Clinical versus biologic remission T he clinical response reported by Monteleone et al. is impressive, but it was not confrmed by endoscopic evidence of mucosal healing and it did not correlate with normalization of biomarkers such as fecal calprotectin or C-reactive protein. In short, there is a lack of congruence between clinical remission and biologic remission, an issue that must be addressed in future studies of this agent. Also intriguing was the fnding that clinical response was maintained for the duration of follow-up even though mongersen was only administered for 2 weeks and is thought not to linger in tissues. This is a stark contrast to the rapid recurrence of symptoms that characterizes withdrawal of existing anti-infammatory drugs. Severine Vermeire, M.D., Ph.D., is in the department of gastroenterology at Leuven (Belgium) University Hospital. She reported receiving grant support and personal fees from AbbVie, Merck Sharp & Dohme, Pfzer, Genentech/ Roche, Takeda, and Mundipharma. Dr. Vermeire made these remarks in an editorial accompanying Dr. Monteleone’s report (N. Engl. J. Med. 2015 March 19 [doi:10.1056/NEJMe1415053]). approximately 3 months at 17 medical centers in Italy and Germany. The study participants were randomly assigned to receive one of three doses of the agent or a matching placebo in a double-blind fashion. The study’s primary endpoint was the percentage of patients in remission at day 15 who remained in remission for at least 2 more weeks. Remission was defned as a Crohn’s Disease Activity Index (CDAI) score of < 150. Rates of remission were 65% in the 43 participants who received 160 mg of mongersen, 55% in the 40 who received 40 mg, 12% in the 41 who received 10 mg, and 10% in the 42 who received placebo. Thus, remission rates at the two highest doses of mongersen exceeded those achieved in other phase II trials for Crohn’s therapies, which ranged from 16% to 48%, the investigators said (N. Engl. J. Med. 2015 March 19 [doi:10.1056/ NEJMoa1407250]). Rates of attaining the secondary endpoint of “clinical response,” defned as a decrease of 100 or more points in the CDAI score at day 28, also were signifcantly higher at the two highest doses of mongersen – 72% and 58% – than with the lowest dose (37%) or with placebo (17%). No safety issues related to mongersen were identifed in this study, but a 2-week course of treatment in such a small group of patients likely is not adequate to determine safety. Adverse events occurred in 65% of the active-treatment groups and 64% of the placebo group and were mild. The nine serious adverse events that occurred were unrelated to study treatment, Dr. Monteleone and his associates said. Further study is needed to assess longer durations of treatment and to judge the efectiveness of the drug based on endoscopic analyses of mucosal healing rather than on CDAI score. It also will be important to determine whether higher doses or longer treatment courses of mongersen raise the risk of fbrosis, given that the targeted cytokine plays a profbrogenic role in many organs, they added. This study was sponsored by Giuliani, under contract to Nogra Pharma. Dr. Monteleone reported ties to Giuliani, Novo Nordisk, Teva, and others, and holds a patent on the use of SMAD7 antisense oligonucleotides in Crohn’s disease. His associates reported fnancial ties to numerous industry sources. [email protected] AGA Resource Review the AGA IBD Clinical Service Line to learn more about managing Crohn’s disease at www.gastro.org/practice/ clinical-service-line/ibd-clinicalservice-line New reprocessing instructions for TJF-Q180V duodenoscope BY ELIZABETH MECHCATIE Frontline Medical News O lympus, the manufacturer of the TJF-Q180V duodenoscope, has issued new, validated instructions for reprocessing this particular model, as part of the response to recent reports of a possible association between multidrug-resistant bacterial infections and improperly processed duodenoscopes, according to the Food and Drug Administration. The new instructions, which replace the manual reprocessing instructions included in the original labeling, and validation data have been reviewed by the FDA as part of its ongoing review of the device. The agency “recommends that any facilities that are using Olympus’ TJF-Q180V duodenoscope train staf on the new instructions and implement them as soon as possible,” according to an FDA statement. The instructions are provided in letters sent by Olympus to health care and other facilities that use this particular model. “Key changes” have been made to the procedures for precleaning, manual cleaning, and manu- al high-level disinfection reprocessing procedures, the FDA said. The TJF-Q180 V duodenoscope was the model used in four patients who had undergone an endoscopic retrograde cholangiopancreatography (ERCP) procedure between August 2014 and January 2015 with the same duodenoscope at Cedars-Sinai Medical Center in Los Angeles and had been infected with carbapenem-resistant Enterobacteriaceae (CRE). This outbreak was announced by the medical center in early March in a statement that said the infections occurred “despite the fact that Cedars-Sinai meticulously followed the disinfection procedure for duodenoscopes” recommended in instructions provided by Olympus and the FDA. In February, the FDA frst announced that the agency had received reports of multidrug-resistant bacterial infections in patients who had undergone ERCP procedures with duodenoscopes, despite proper cleaning and disinfection of the devices and that the “complex design of ERCP endoscopes (also called duodenoscopes) may impede efective reprocessing.” In the latest statement, the FDA said it “is closely monitoring the possible association between reprocessed duodenoscopes and the transmission of infectious agents,” including multidrug-resistant bacterial infections caused by CRE. If they are not properly reprocessed, the statement adds, “residual body fuids and organic debris may remain in microscopic crevices of the device following an attempted cleaning and high-level disinfection. If these residual fuids contain microbial contamination, subsequent patients may be exposed to serious infections.” Adverse events associated with duodenoscopes should be reported to the FDA’s MedWatch Program at 800-3321088 or www.accessdata.fda.gov/scripts/medwatch. [email protected] AGA Resource Read more about AGA’s eforts and recommendations to stop duodenoscope infections at www.gastro.org/practice/patient-safety/ recommendations-to-stop-duodenoscopeinfections 6 NEWS MAY 2 0 1 5 • G I & HEPATO LO G Y NEW S FROM THE AGA JOURNALS Oxidized LDL predicted HCV interferon response BY AMY KARON Frontline Medical News O xidized low-density lipoprotein prevented hepatitis C virus from entering liver cells and predicted interferon response among patients with chronic HCV infection, researchers reported online in the May issue of Cellular and Molecular Gastroenterology and Hepatology (2015 March 14 [doi:10.1016/j.jcmgh.2015.03.002]). “Even as all-oral regimens begin to reach the market, interferon-based treatment will continue to be used in cost-restrained settings. Thus, there is a need for predictors of who is likely to respond to interferon and who will require a more expensive direct-acting antiviral combination regimen,” said Dr. Philipp Solbach of Medizinische Hochschule Hannover and the German Center for Infection Research and his associates. Combinations of interferon and viral entry inhibitors might beneft patients with chronic HCV infection (CHC), the investigators added. Hepatitis C virus spreads between hepatocytes with the help of several cell surface receptors, including scavenger receptor class B type 1 (SR-BI). Research has shown that oxidized low-density lipoprotein (oxLDL) noncompetitively inhibits the interaction between SR-B1 and HCV. To further study the role of oxLDL in CHC pathology, the investigators used a commercial enzyme-linked immunosorbent assay test to measure serum levels in 379 patients with genotype 1 CHC from the INDIV-2 study. Patients in that study received a pegylated interferon-ribavirin (pegIFN/RBV) combination for 24-72 weeks, depending on baseline viral load. Dr. Solbach and his associates also studied the efects of oxLDL on HCV replication in hepatoma cells. Average serum oxLDL levels were signifcantly higher among patients who achieved SVR on peg-IFN/RBV than in those who did not (7.1 mU/L [standard deviation, 3.2] vs. 5.9 mU/L [SD, 2.6]; P < .001), the researchers reported. In the multivariate analysis, oxLDL levels independently predicted SVR, but were not associated with increased ALT or ferritin levels, both of which point to liver infammation. Increased serum oxLDL also was linked to decreased infected cell loss rate, further supporting the idea that oxLDL helps inhibit cell-to-cell spread of HCV in chronically infected patients. Area under the receiver operative curve (AUROC) values were similar for LDL and oxLDL, indicating that one value was a good clinical indicator of the other, the investigators said. The optimal cutof points to predict SVR in their model were 8.85 mU/L for oxLDL and 3.6 mmol/L for LDL. In the in vitro study, oxLDL did not afect the sensitivity of HCV replication to interferon, but strongly inhibited the spread of HCV between adjacent hepatocytes, the investigators reported. “We found that oxLDL but not LDL potently inhibits cellto-cell spread between neighboring cells,” they noted. “Cell-to-cell spread is thought to be the dominant route of new cell infection within the chronically infected liver.” Taken together, the fndings suggest that HCV needs to interact with SR-BI in order to spread between hepatocytes, that oxLDL can impede that interaction and thereby limit infection of naive cells, and that oxLDL D espite the fact that signifcant advances in the treatment of hepatitis C have been made, it is still a major global health burden. In order to follow up on their previous observation that oxLDL acts as a hepatitis C virus (HCV) entry inhibitor by disrupting the interaction between HCV and one of its entry factors, scavenger receptor type B class I (SR-BI), Dr. Solbach and his associates analyzed the oxLDL levels of 379 patients from the INDIV-2 study chronically infected with HCV genotype 1. The authors demonstrated that baseline oxLDL serum levels were an independent predictor of a sustained virologic response in interferon-based treatment regimens and that LDL is a sufcient surrogate marker. Clinicians, especially in resource-limited environments, may take oxLDL or LDL serum levels into consideration for treatment is neither an infammatory marker nor a modulator of interferon response, Dr. Solbach and his associates said. “The slower second-phase decline of viral load during interferon-based therapy is thought to refect a declining pool of infected hepatocytes, and the slope of second-phase decline and even more the estimated viral kinetic parameter describing the infected cell loss rate is predictive of eventual SVR,” they added. “The decisions, although these predictors are unlikely to broadly afect treatment decisions in real-world settings. The signifcance of this study lies more in adding to our understanding of the pathophysiology of HCV. The data presented here indicate that the observed efect of oxLDL is possibly due to an oxLDL-mediated inhibition of HCV cell-to-cell spread. Taken together with their previous observation that oxLDL interferes with the interaction of HCV and its entry factor SR-BI, the authors provide additional evidence that SR-BI may be needed for cell-to-cell spread of HCV and might thereby have implications for the further development of HCV entry inhibitors. Dr. Markus von Schaewen and Dr. Alexander Ploss are in the department of molecular biology, Princeton University, Princeton, N.J. They had no conficts of interest. presence of an agent reducing the rate at which naive cells get infected might thus be benefcial.” The Germany Center for Infection Research partially funded the study. Five coauthors reported having served as clinical researchers, consultants, or speakers for MSD/Merck and Roche. The other authors declared no conficts of interest. [email protected] Acid exposure time most useful in pH-impedance testing BY AMY KARON Frontline Medical News P H-impedance testing best predicted response to refux treatment when patients were of proton pump inhibitors, and abnormal acid exposure time was the single most useful testing parameter, a prospective study has found. “Impedance-based refux parameters complement but do not replace acid-based parameters in predicting symptom outcome from both medical and surgical antirefux therapy,” wrote Dr. Amit Patel and his associates at the Washington University at St. Louis School of Medicine. The study ap- pears in the May issue of Clinical Gastroenterology and Hepatology (doi:10.1016/j.cgh.2014.08.02). “Because abnormal acid refux time and symptom-refux correlation parameters are detected more often when testing is performed of therapy, pH-impedance testing of antisecretory therapy maximizes prediction of symptomatic outcome from GERD [gastroesophageal refux disease] therapy,” the researchers wrote. Clinicians continue to debate the role of pH-impedance testing in management of GERD, whether testing should be performed on or of antisecretory therapy, and which testing parameters are most useful for predicting treatment response, the investigators noted. Therefore, they followed 187 adults with persistent GERD symptoms who underwent pH-impedance testing at their center during a 5-year period. Average age of patients was 54 years, almost 71% were female, and none had histopathologic evidence of esophageal motor disorders. Almost half had been of proton pump inhibitors for 7 days when tested, and 68% were managed medically as opposed to surgically. Global symptom assessment (GSAS) and dominant symptom intensity (DSI) scores both improved signifcantly during an average of 40 months of follow-up, the researchers said. After Continued on following page NEWS GIHEP NEW S. COM • M AY 2015 7 FROM THE AGA JOURNALS Capsule colonoscopy improved, but limitations persist BY AMY KARON Frontline Medical News W hen compared with conventional colonoscopy, capsule colonoscopy had a sensitivity of 88% and a specifcity of 82% for detecting adenomas of at least 6 mm in asymptomatic subjects, a multicenter prospective study showed. But the capsule detected only 29% of subjects who had sessile serrated polyps of at least 6 mm, and required more extensive bowel preparation than did conventional colonoscopy, Dr. Douglas K. Rex, AGAF, at Indiana University Hospital in Indianapolis and his associates reported in the May issue of Gastroenterology (2015 [doi:10.1053/j. gastro.2015.01.025]). “Given these considerations ... colonoscopy remains the gold standard for the detection of colorectal polyps,” said the researchers. “The capsule is a good test for the detection of patients with conventional adenomas 6 mm or larger in size and appears to be an appropriate imaging choice for patients who cannot undergo colonoscopy or had incomplete colonoscopy.” Capsule endoscopy is useful for small-bowel imaging, but adapting the technology for colorectal studies has been difcult. A frst-generation capsule detected only 74% of advanced adenomas in one prospective multicenter trial. Since then, the PillCam COLON 2 capsule has been updated with motion detection, variable frame speed, and a wider angle view. In smaller studies, it detected up to 89% of subjects with polyps of at least 6 mm, but its specifcity was as low as 64%. To further investigate the technology, researchers at 16 centers in the United States and Israel compared the second-generation capsule with conventional colonoscopy in an average-risk screening population of 884 asymptomatic subjects. Endos- copists were blinded as to technique, but performed unblinded follow-up colonoscopies in subjects who were positive on capsule but negative on conventional colonoscopy. The capsule’s sensitivity was 81% (95% confdence interval, 77%-84%) and its specifcity was 93% (91%95%) for detecting subjects who had polyps of at least 6 mm, the researchers reported. Sensitivity was 80% (74%-86%) and specifcity was 97% (96%-98%) for detecting subjects with polyps of at least 10 mm. For conventional adenomas of at least 6 mm, sensitivity was 88% (82%-93%) and specifcity was 82% (80%-83%), I adenomas,” the researchers reported. Prior studies of the capsule did not look for serrated lesions; in the current study sensitivities were only 29% and 33% for 6-mm and 10-mm lesions, respectively. The software used to measure polyps during capsule colonoscopy had a 40% error range when tested on balls of known size, the researchers said. Therefore, there is a strict location-matching rule within the colon, but a liberal size rule that only required measurements to fall within 50% of one another to be considered a match. “Any set of matching rules for polyps detected by the capsule and n the United States, colonoscopy is the primary screening test for colorectal cancer. However, because of issues with colonoscopy uptake, costs, and the small but fnite risk of complications, the concept of a relatively noninvasive structural examination of the colon that can detect colorectal neoplasia is appealing to both patients and physicians. Although capsule colonoscopy has emerged as a potential noninvasive tool for examining the entire colon, there are limited data on its accuracy for detecting conventional adenomas or sessile serrated polyps, particularly in an average-risk screening population. In the May issue of Gastroenterology, Dr. Rex and colleagues report their results from a large, multicenter, prospective study evaluating the new second-generation capsule colonoscopy (PillCam COLON 2, Given Imaging) for detecting colorectal neoplasia in an average-risk screening population. Using optical colonoscopy as the reference standard, the capsule colonoscopy performed well for detecting conventional adenomas 6 mm or larger with a sensitivity and specifcity of 88% and 82%, respective- and for adenomas of 10 mm or larger, sensitivity was 92% (82%-97%) and specifcity was 95% (94%-95%). “Lesions in the serrated class were not detected well by the capsule in this study, compared with conventional Continued from previous page the researchers controlled for demographics, symptoms at presentation, use of proton pump inhibitors (PPI), and parameters that predicted treatment response in the univariate analyses, only abnormal acid exposure time (AET) predicted linear improvement in DSI scores (P =.027), while abnormal AET (P =.002) and symptom association probability (P =.026) predicted significant improvements in linear and dichotomous GSS, they reported. Abnormal AET and being of PPIs during testing also more than doubled the ly seen on capsule were not visualized on regular colonoscopy. “In these cases, a polyp that should be a true positive for the capsule was counted as false,” they added. “Both colonoscopy and capsule are inferior for localization, compared with CT colonography. Inaccurate localization by one or both tests in this study could have reduced the sensitivity of the capsule.” The investigators had to exclude 77 patients because of inadequate cleansing and short transit times related to using sodium phosphate as a boost. The Food and Drug Administration label for the capsule is expected to refect those limitations, they added. ly. In addition, the sensitivity and specifcity of capsule colonoscopy for conventional adenomas 10 mm or larger were 92% and 95%, respectively. However, despite the high performance characteristics for detection of conventional adenomas, the capsule colonoscopy had limited accuracy for detecting sessile serrated polyps 10 mm or larger, with a sensitivity of 33%. Furthermore, nearly 10% of the enrolled subjects were excluded from the analysis due to poor bowel preparation and rapid transit time. These issues aside, the Rex study provides important information about alternative screening modalities for detection of colorectal neoplasia, particularly for gastroenterologists who may be hesitant or unwilling to perform an optical colonoscopy in high-risk patients with signifcant comorbidities or in patients who had an incomplete colonoscopy. Dr. Jefrey Lee, MAS, is assistant clinical professor of medicine, division of gastroenterology, University of California, San Francisco. He has no conficts of interest. colonoscopy might operate to increase or decrease the calculated sensitivity of the capsule incorrectly,” they added. Also, the adenoma detection rate for conventional colonoscopy was only 39%, and some polyps that were clear- odds of at least a 50% improvement in GSS. In contrast, dichotomous refux exposure time did not predict response in any of the analyses, said the investigators. “Established thresholds for the total number of refux events did not predict linear or dichotomous global symptom severity improvement,” they added. “Our data therefore suggest that performing pH-impedance testing of PPI therapy increases the yield of abnormal AET and symptom-refux association with refux events, facilitating predicting value for symptom improvement with both medical and surgical antirefux therapy.” The researchers could not corroborate patients’ Given Imaging funded the study and paid consulting or other fees to Dr. Rex and six coauthors. The other authors reported no relevant conficts of interest. [email protected] compliance with antisecretory therapy, assess the reasons physicians chose medical or surgical management, or evaluate the impact of the placebo effect or other factors unrelated to refux, they said. The study was partly funded by the National Institute for Diabetes and Digestive and Kidney Diseases, the National Institutes of Health, and the Washington University Department of Medicine Mentors in Medicine and Clinical Science Training and Research programs. The authors declared no relevant conficts of interest. [email protected] 8 NEWS MAY 2 0 1 5 • G I & HEPATO LO G Y NEW S FROM THE AGA JOURNALS Cirrhosis mortality has dropped, except with sepsis BY AMY KARON Frontline Medical News ulation’s increasing age and medical complexity. Hospital mortality rates were higher for subgroups of cirrhosis patients with hepatorenal syndrome, hepatocellular carcinoma, variceal bleeding, and spontaneous bacterial peritonitis, but independent mortality risks for each of these conditions fell progressively over time. H ospital mortality among patients with cirrhosis fell by 41% in the United States between 2002 and 2010, far outpacing improvements in survival among inpatients who did not have cirrhosis, researchers reported in the May issue of Gastroenterology (2015 [doi:10.1053/j.gastro.2015.01.032]). The drop occurred even though cirrhosis inpatients were older and had more comorbidities by the end, compared with the beginning of the study, said Monica Schmidt at the University of North Carolina Liver Center and the Gillings School of Global Public Health in Chapel Hill, N.C., and her associates. The fnding was “remarkably consistent across several cirrhosis complications, and [suggested] improving cirrhosis care that may extend beyond general improvements in inpatient care,” the researchers added. “On the other hand, sepsis had an increasing mortality risk, suggesting that cirrhotic patients may need a more tailored approach to sepsis,” they said. New treatments have emerged in the past 10-15 years for several complications of cirrhosis, including hepatorenal syndrome, variceal bleeding, spontaneous bacterial peritonitis, ascites, and hepatocellular carcinoma, Ms. Schmidt and her associates noted. To study the extent to which these advances and updated guidelines have entered hospital practice, they examined 781,515 hospitalizations with a diagnosis of cirrhosis, and equal numbers of hospitalizations without cirrhosis or with congestive heart failure. Data were from the National Inpatient Sample of the Healthcare Cost and Utilization Project, which includes 46 states and is the single largest all-payer inpatient database in the country. Cohorts were matched by age, sex, and year of hospital discharge from 2002 through 2010. Hospital mortality among cirrhosis patients dropped by 41% (from 9.1% to 5.4%) during the 8 years of the study, compared with declines of 44% for inpatients with congestive heart failure and 19% for inpatients without cirrhosis, the investigators said. Furthermore, the independent risk of dying in the hospital among cirrhosis patients declined steadily to 0.50 by the end of the study (95% confdence interval, 0.48-0.52), despite the pop- The person depicted is a model used for illustrative purposes only. IMPORTANT SAFETY INFORMATION FOR SIMPONI® (golimumab) SERIOUS INFECTIONS Patients treated with SIMPONI® are at increased risk for developing serious infections that may lead to hospitalization or death. Most patients who developed these infections were taking concomitant immunosuppressants such as methotrexate or corticosteroids. Discontinue SIMPONI® if a patient develops a serious infection. Reported infections with TNF blockers, of which SIMPONI® is a member, include: • Active tuberculosis (TB), including reactivation of latent TB. Patients frequently presented with disseminated or extrapulmonary disease. Patients should be tested for latent TB before SIMPONI® use and during therapy. Treatment for latent infection should be initiated prior to SIMPONI® use. NEWS GIHEP NEW S. COM • M AY 2015 In contrast, cirrhosis inpatients with sepsis were 22% more likely to die in the hospital in 2010 than in 2002 (relative risk in 2002, 3.6; 95% CI, 3.3-3.95; RR in 2010, 4.6; 95% CI, 4.4-4.8), the researchers found. The increase in mortality risk related to sepsis in 2010 exceeded even that for hepatorenal syndrome, they said. The unexpected fnding contradicted a report of declining overall sepsis-related mortality, which was based on the same data source and a similar time period, the investigators noted. “Cirrhosis patients have particularly poor hemodynamic reserve, with wider perturbations in immune infammatory and compensatory responses that could hinder survival,” they commented. “The Surviving UC IS OVERWHELMING TREATMENT SHOULDN’T BE The injection experience she wants, proven e�fcacy she needs1* Most common adverse reactions are upper respiratory tract infection, nasopharyngitis, and injection-site reactions. SIMPONI® (golimumab) is indicated in adults with moderately to severely active ulcerative colitis (UC) for inducing and maintaining clinical response, improving endoscopic appearance of the mucosa during induction, inducing clinical remission, and achieving and sustaining clinical remission in induction responders who have demonstrated corticosteroid dependence or who have had an inadequate response to or failed to tolerate oral aminosalicylates, oral corticosteroids, azathioprine, or 6-mercaptopurine. For more information, visit www.injectionexperience.com *The safety and e�fcacy of SIMPONI® in UC were established in a Phase 2/3 induction study and a Phase 3 maintenance study.2,3 • Invasive fungal infections, including histoplasmosis, coccidioidomycosis, candidiasis, aspergillosis, blastomycosis, and pneumocystosis. Patients with histoplasmosis or other invasive fungal infections may present with disseminated, rather than localized, disease. Consider empiric anti-fungal therapy in patients at risk for invasive fungal infections who develop severe systemic illness. • Bacterial, viral, and other infections due to opportunistic pathogens, including Legionella and Listeria. The risks and benefits of treatment with SIMPONI® should be carefully considered prior to initiating therapy in patients with chronic or recurrent infection. Do not start SIMPONI® in patients with clinically important active infections, including localized infections. Closely monitor patients for the development of signs and symptoms of infection during and a�ter treatment with SIMPONI®, including the possible development of TB in patients who tested negative for latent TB infection prior to initiating therapy, who are on treatment for latent TB, or who were previously treated for TB infection. (CONTINUED ON THE NEXT PAGE) 9 Sepsis campaign may need guidelines that specifcally target cirrhosis patients.” The National Institutes of Health partly funded the study. The authors reported having no relevant conficts of interest. [email protected] 10 NEWS MAY 2 0 1 5 • G I & HEPATO LO G Y NEW S FROM THE AGA JOURNALS Probiotics showed slight promise in postresection Crohn’s BY AMY KARON Frontline Medical News A mixture of eight probiotic bacterial strains only somewhat outperformed placebo for preventing endoscopic recurrence after ileal resection in Crohn’s disease patients, according to a multicenter, randomized trial. After 90 days of treatment, 9.3% of patients who received the probiotic mixture (VSL#3) had developed IMPORTANT SAFETY INFORMATION FOR SIMPONI® (golimumab) (CONTINUED) Risk of infection may be higher in patients greater than 65 years of age, patients with co-morbid conditions and/or patients taking concomitant immunosuppressant therapy. Other serious infections observed in patients treated with SIMPONI® included sepsis, pneumonia, cellulitis, abscess and hepatitis B infection. MALIGNANCIES Lymphoma and other malignancies, some fatal, have been reported in children and adolescent patients treated with TNF blockers of which SIMPONI® is a member. Approximately half the cases were lymphomas, including Hodgkin’s and non-Hodgkin’s lymphoma. The other cases represented a variety of malignancies, including rare malignancies usually associated with immunosuppression and malignancies not usually observed in children or adolescents. Malignancies occurred after a median of 30 months after the frst dose of therapy. Most of the patients were receiving concomitant immunosuppressants. In the controlled portions of clinical trials of all TNF-blocking agents including SIMPONI®, more cases of lymphoma have been observed among patients receiving TNF-blocking treatment compared with control patients. In the Rheumatoid Arthritis (RA), Psoriatic Arthritis (PsA), and Ankylosing Spondylitis (AS) clinical trials, the incidence of lymphoma per 100 patient-years of follow-up was 0.21 (95% CI: 0.03, 0.77) in the combined SIMPONI® group compared with an incidence of 0 (95% CI: 0, 0.96) in the placebo group. In clinical trials, the incidence of malignancies other than lymphoma was not increased with exposure to SIMPONI® and was similar to what would be expected in the general population. In controlled and uncontrolled portions of the Phase 2/3 studies in ulcerative colitis (UC) with a mean follow-up of approximately 1 year, there were no cases of lymphoma with SIMPONI®. Cases of acute and chronic leukemia have been reported with postmarketing TNF-blocker use. The risks and benefts of TNF-blocker therapy should be considered prior to initiating therapy in patients with a known malignancy or who develop a malignancy. Postmarketing cases of hepatosplenic T-cell lymphoma (HSTCL), a rare type of T-cell lymphoma, have been reported in patients treated with TNF blockers. These cases have had a very aggressive disease course and have been fatal. Nearly all reported cases have occurred in patients with Crohn’s disease or UC, and the majority were in adolescent and young adult males. Almost all of these patients had received treatment with azathioprine or 6-mercaptopurine concomitantly with a TNF blocker at or prior to diagnosis. A risk for the development for HSTCL in patients treated with TNF blockers cannot be excluded. Melanoma has been reported in patients treated with TNF-blocking agents, including SIMPONI®. Merkel cell carcinoma has been reported in patients treated with TNF-blocking agents. Periodic skin examination is recommended for all patients, particularly those with risk factors for skin cancer. HEPATITIS B REACTIVATION The use of TNF-blocking agents including SIMPONI® has been associated with reactivation of hepatitis B virus (HBV) in patients who are chronic hepatitis B carriers. In some instances, HBV reactivation occurring in conjunction with TNF-blocker therapy has been fatal. The majority of these reports have occurred in patients who received concomitant immunosuppressants. All patients should be tested for HBV infection before initiating TNF-blocker therapy. For patients who test positive for hepatitis B surface antigen, consult a physician with expertise in the treatment of hepatitis B before initiating TNF-blocker therapy. Exercise caution when prescribing SIMPONI® for patients identifed as carriers of HBV and closely monitor for active HBV infection during and following termination of therapy with SIMPONI®. Discontinue SIMPONI® in patients who develop HBV reactivation, and initiate antiviral therapy with appropriate supportive treatment. Exercise caution when considering resumption of SIMPONI®, and monitor patients closely. HEART FAILURE Cases of worsening congestive heart failure (CHF) and new-onset CHF have been reported. Exercise caution and monitor patients with heart failure. Discontinue SIMPONI® if new or worsening symptoms of heart failure appear. NEWS GIHEP NEW S. COM • M AY 2015 severe endoscopic recurrence, compared with 15.7% of the placebo group (P = .19), reported Dr. Richard Fedorak of the University of Alberta, Edmonton, and his associates. The recurrence rate for the placebo group was about two-thirds lower than what the researchers had expected based on the sample size calculation, they noted. But the probiotic blend was linked to signifcant decreases in colonic mucosal levels of proinfammatory cytokines, they reported in the May issue of Clinical Gastroenterology and Hepatology (doi:10.1016/j.cgh.2014.10.031). Probiotics have been tested as a preventive therapy for Crohn’s disease because patients with active disease have less diverse intestinal microbiota, compared with those with quiescent disease or healthy controls. Past studies of single-strain probiotics have shown them to be no better than placebo for preventing endoscopic recurrence. But in one small study, rifampin followed by VSL#3 outperformed me- DEMYELINATING DISORDERS TNF-blocking agents, of which SIMPONI® is a member, have been associated with rare cases of new-onset or exacerbation of demyelinating disorders, including multiple sclerosis (MS) and Guillain-Barré syndrome. Cases of central demyelination, MS, optic neuritis, and peripheral demyelinating polyneuropathy have rarely been reported with SIMPONI®. Exercise caution in considering the use of SIMPONI® in patients with these disorders. Consider discontinuation if these disorders develop. HEMATOLOGIC CYTOPENIAS There have been reports of pancytopenia, leukopenia, neutropenia, and thrombocytopenia in patients receiving SIMPONI® in clinical trials. Additionally, aplastic anemia has been reported in patients receiving TNF-blocking agents, of which SIMPONI® is a member. Exercise caution when using SIMPONI® in patients who have or had signifcant cytopenias. USE WITH OTHER DRUGS The concomitant use of a TNF blocker and abatacept or anakinra was associated with a higher risk of serious infections; therefore the use of SIMPONI® in combination with these products is not recommended. Care should be taken when switching from one biologic to another since overlapping biological activity may further increase the risk of infection. A higher rate of serious infections has also been observed in RA patients treated with rituximab who received subsequent treatment with a TNF blocker. The concomitant use of SIMPONI® with biologics approved to treat RA, PsA, or AS is not recommended because of the possibility of an increased risk of infection. VACCINATIONS/THERAPEUTIC INFECTIOUS AGENTS People receiving SIMPONI® can receive vaccinations, except for live vaccines. Use of live vaccines could result in clinical infections, including disseminated infections. Administration of live vaccines to infants exposed to SIMPONI® in utero is not recommended for 6 months following the mother’s last SIMPONI® injection during pregnancy due to an increased risk of infection. It is recommended that therapeutic infectious agents not be given concurrently with SIMPONI® due to the possibility of clinical infections, including disseminated infections. HYPERSENSITIVITY REACTIONS Serious systemic hypersensitivity reactions (including anaphylactic reaction) have been reported with SIMPONI®, some occurring after the frst dose. If an anaphylactic or other serious allergic reaction occurs, discontinue SIMPONI® immediately and institute appropriate therapy. 025952-141204 ADVERSE REACTIONS The most serious adverse reactions were serious infections and malignancies. Upper respiratory tract infection and nasopharyngitis were the most common adverse reactions reported in the combined Phase 3 trials through Week 16, occurring in 7% and 6% of patients treated with SIMPONI® as compared with 6% and 5% of patients in the control group, respectively. The rate of injection-site reactions was 6% with patients treated with SIMPONI® compared with 2% of patients in the control group. In the Phase 2/3 trials in UC evaluating SIMPONI®-treated patients, no new adverse drug reactions were identifed, and the frequency of adverse drug reactions was similar to the safety profle observed in patients with RA, PsA, and AS. Please see the Brief Summary of Prescribing Information on the following pages. References: 1. SIMPONI® (golimumab) Prescribing Information. Janssen Biotech, Inc. 2. Sandborn WJ, Feagan BG, Marano C, et al; PURSUIT-SC Study Group. Subcutaneous golimumab induces clinical response and remission in patients with moderate-to-severe ulcerative colitis. Gastroenterology. 2014;146:85-95. 3. Sandborn WJ, Feagan BG, Marano C, et al; PURSUIT-Maintenance Study Group Subcutaneous golimumab maintains clinical response in patients with moderate-to-severe ulcerative colitis. Gastroenterology. 2014;146:96-109. © Janssen Biotech, Inc. 2015 03/15 029681-150213 11 salamine at 1 year (Gastroenterology 2000;118:A781), the researchers noted. “This mixture could confer protective efects where single-strain or lactobacillus-only formulations had failed,” they hypothesized. To test that theory, the investigators randomized 120 patients with Crohn’s Continued on following page 12 NEWS Continued from previous page disease who had undergone ileal resection to twice-daily VSL#3 or placebo. Treatment began within 30 days after surgery and continued for 90 days, after which all patients received open-label VSL#3 for another 9 months. Among patients who had nonsevere MAY 2 0 1 5 • G I & HEPATO LO G Y NEW S endoscopic lesions at day 90, 1-year rates of severe endoscopic recurrence were 10% for the early VSL#3 group, compared with 26.7% for the late VSL#3 group (P = .09), said the researchers. Likewise, combined rates of severe recurrence on days 90 and 365 were not signifcantly diferent, they reported. But the early VSL#3 group had lower mucosal levels of 13 proinfammatory cytokines than the patients who received placebo until day 90 (P < .05). Measures of Crohn’s disease activity and disease-related quality of life scores were similar for both groups. “Future larger studies will be needed to confrm the efect of VSL#3 in prevention of postoperative recurrence.” Brief Summary of Prescribing Information for SIMPONI® (golimumab) SIMPONI® Injection, solution for subcutaneous use See package insert for full Prescribing Information. WARNING: SERIOUS INFECTIONS AND MALIGNANCY SERIOUS INFECTIONS Patients treated with SIMPONI® are at increased risk for developing serious infections that may lead to hospitalization or death (see Warnings and Precautions). Most patients who developed these infections were taking concomitant immunosuppressants such as methotrexate or corticosteroids. Discontinue SIMPONI if a patient develops a serious infection. Reported infections with TNF-blockers, of which SIMPONI is a member, include: • Active tuberculosis, including reactivation of latent tuberculosis. Patients with tuberculosis have frequently presented with disseminated or extrapulmonary disease. Test patients for latent tuberculosis before SIMPONI use and during therapy. Initiate treatment for latent TB prior to SIMPONI use. • Invasive fungal infections including histoplasmosis, coccidioidomycosis, candidiasis, aspergillosis, blastomycosis and pneumocystosis. Patients with histoplasmosis or other invasive fungal infections may present with disseminated, rather than localized, disease. Antigen and antibody testing for histoplasmosis may be negative in some patients with active infection. Consider empiric anti-fungal therapy in patients at risk for invasive fungal infections who develop severe systemic illness. • Bacterial, viral, and other infections due to opportunistic pathogens, including Legionella and Listeria. Consider the risks and benefits of treatment with SIMPONI prior to initiating therapy in patients with chronic or recurrent infection. Monitor patients closely for the development of signs and symptoms of infection during and after treatment with SIMPONI, including the possible development of tuberculosis in patients who tested negative for latent tuberculosis infection prior to initiating therapy (see Warnings and Precautions). MALIGNANCY Lymphoma and other malignancies, some fatal, have been reported in children and adolescent patients treated with TNF blockers, of which SIMPONI is a member (see Warnings and Precautions). INDICATIONS AND USAGE: Rheumatoid Arthritis SIMPONI, in combination with methotrexate, is indicated for the treatment of adult patients with moderately to severely active rheumatoid arthritis. Psoriatic Arthritis SIMPONI, alone or in combination with methotrexate, is indicated for the treatment of adult patients with active psoriatic arthritis. Ankylosing Spondylitis SIMPONI is indicated for the treatment of adult patients with active ankylosing spondylitis. Ulcerative Colitis SIMPONI is indicated in adult patients with moderately to severely active ulcerative colitis who have demonstrated corticosteroid dependence or who have had an inadequate response to or failed to tolerate oral aminosalicylates, oral corticosteroids, azathioprine, or 6-mercaptopurine for: • inducing and maintaining clinical response • improving endoscopic appearance of the mucosa during induction • inducing clinical remission • achieving and sustaining clinical remission in induction responders (see Clinical Studies). CONTRAINDICATIONS: None. WARNINGS AND PRECAUTIONS: Serious Infections Patients treated with SIMPONI are at increased risk for developing serious infections involving various organ systems and sites that may lead to hospitalization or death. Opportunistic infections due to bacterial, mycobacterial, invasive fungal, viral, or parasitic organisms including aspergillosis, blastomycosis, candidiasis, coccidioidomycosis, histoplasmosis, legionellosis, listeriosis, pneumocystosis, and tuberculosis have been reported with TNF-blockers. Patients have frequently presented with disseminated rather than localized disease. The concomitant use of a TNF-blocker and abatacept or anakinra was associated with a higher risk of serious infections; therefore, the concomitant use of SIMPONI and these biologic products is not recommended (see Warnings and Precautions and Drug Interactions). Treatment with SIMPONI should not be initiated in patients with an active infection, including clinically important localized infections. Patients greater than 65 years of age, patients with co-morbid conditions and/or patients taking concomitant immunosuppressants such as corticosteroids or methotrexate may be at greater risk of infection. Consider the risks and benefits of treatment prior to initiating SIMPONI in patients: • with chronic or recurrent infection; • who have been exposed to tuberculosis; • with a history of an opportunistic infection; • who have resided or traveled in areas of endemic tuberculosis or endemic mycoses, such as histoplasmosis, coccidioidomycosis, or blastomycosis; or • with underlying conditions that may predispose them to infection. Monitoring Closely monitor patients for the development of signs and symptoms of infection during and after treatment with SIMPONI. Discontinue SIMPONI if a patient develops a serious infection, an opportunistic infection, or sepsis. For a patient who develops a new infection during treatment with SIMPONI, perform a prompt and complete diagnostic workup appropriate for an immunocompromised patient, initiate appropriate antimicrobial therapy and closely monitor them. Serious Infection in Clinical Trials In controlled Phase 3 trials through Week 16 in patients with RA, PsA, and AS, serious infections were observed in 1.4% of SIMPONI-treated patients and 1.3% of control-treated patients. In the controlled Phase 3 trials through Week 16 in patients with RA, PsA, and AS, the incidence of serious infections per 100 patient-years of follow-up was 5.7 (95% CI: 3.8, 8.2) for the SIMPONI group and 4.2 (95% CI: 1.8, The study was funded by VSL Pharmaceuticals, the Canadian Institutes of Health Research, and Crohn’s and Colitis Foundation of Canada. Dr. Fedorak reported serving on a speakers bureau for VSL Pharmaceuticals. The other authors declared no conficts of interest. [email protected] SIMPONI® (golimumab) 8.2) for the placebo group. In the controlled Phase 2/3 trial through Week 6 of SIMPONI induction in UC, the incidence of serious infections in SIMPONI 200/100 mg-treated patients was similar to the incidence of serious infections in placebo-treated patients. Through Week 60, the incidence of serious infections was similar in patients who received SIMPONI induction and 100 mg during maintenance compared with patients who received SIMPONI induction and placebo during the maintenance portion of the UC trial. Serious infections observed in SIMPONI-treated patients included sepsis, pneumonia, cellulitis, abscess, tuberculosis, invasive fungal infections, and hepatitis B infection. Tuberculosis Cases of reactivation of tuberculosis or new tuberculosis infections have been observed in patients receiving TNF-blockers, including patients who have previously received treatment for latent or active tuberculosis. Evaluate patients for tuberculosis risk factors and test for latent infection prior to initiating SIMPONI and periodically during therapy. Treatment of latent tuberculosis infection prior to therapy with TNF-blockers has been shown to reduce the risk of tuberculosis reactivation during therapy. Prior to initiating SIMPONI, assess if treatment for latent tuberculosis is needed; an induration of 5 mm or greater is a positive tuberculin skin test, even for patients previously vaccinated with Bacille Calmette-Guerin (BCG). Consider antituberculosis therapy prior to initiation of SIMPONI in patients with a past history of latent or active tuberculosis in whom an adequate course of treatment cannot be confirmed, and for patients with a negative test for latent tuberculosis but having risk factors for tuberculosis infection. Consultation with a physician with expertise in the treatment of tuberculosis is recommended to aid in the decision whether initiating anti-tuberculosis therapy is appropriate for an individual patient. Cases of active tuberculosis have occurred in patients treated with SIMPONI during and after treatment for latent tuberculosis. Monitor patients for the development of signs and symptoms of tuberculosis including patients who tested negative for latent tuberculosis infection prior to initiating therapy, patients who are on treatment for latent tuberculosis, or patients who were previously treated for tuberculosis infection. Consider tuberculosis in the differential diagnosis in patients who develop a new infection during SIMPONI treatment, especially in patients who have previously or recently traveled to countries with a high prevalence of tuberculosis, or who have had close contact with a person with active tuberculosis. In the controlled and uncontrolled portions of the Phase 2 RA and Phase 3 RA, PsA, and AS trials, the incidence of active TB was 0.23 and 0 per 100 patient-years in 2347 SIMPONI-treated patients and 674 placebo-treated patients, respectively. Cases of TB included pulmonary and extra pulmonary TB. The overwhelming majority of the TB cases occurred in countries with a high incidence rate of TB. In the controlled Phase 2/3 trial of SIMPONI induction through Week 6 in UC, no cases of TB were observed in SIMPONI 200/100 mg-treated patients or in placebo-treated patients. Through Week 60, the incidence per 100 patient-years of TB in patients who received SIMPONI induction and 100 mg during the maintenance portion of the UC trial was 0.52 (95% CI: 0.11, 1.53). One case of TB was observed in the placebo maintenance group in a patient who received SIMPONI intravenous (IV) induction. Invasive Fungal Infections If patients develop a serious systemic illness and they reside or travel in regions where mycoses are endemic, consider invasive fungal infection in the differential diagnosis. Consider appropriate empiric antifungal therapy and take into account both the risk for severe fungal infection and the risks of antifungal therapy while a diagnostic workup is being performed. Antigen and antibody testing for histoplasmosis may be negative in some patients with active infection. To aid in the management of such patients, consider consultation with a physician with expertise in the diagnosis and treatment of invasive fungal infections. Hepatitis B Virus Reactivation The use of TNF-blockers including SIMPONI has been associated with reactivation of hepatitis B virus (HBV) in patients who are chronic hepatitis B carriers (i.e., surface antigen positive). In some instances, HBV reactivation occurring in conjunction with TNF-blocker therapy has been fatal. The majority of these reports have occurred in patients who received concomitant immunosuppressants. All patients should be tested for HBV infection before initiating TNF-blocker therapy. For patients who test positive for hepatitis B surface antigen, consultation with a physician with expertise in the treatment of hepatitis B is recommended before initiating TNF-blocker therapy. The risks and benefits of treatment should be considered prior to prescribing TNF-blockers, including SIMPONI, to patients who are carriers of HBV. Adequate data are not available on whether anti-viral therapy can reduce the risk of HBV reactivation in HBV carriers who are treated with TNF-blockers. Patients who are carriers of HBV and require treatment with TNF-blockers should be closely monitored for clinical and laboratory signs of active HBV infection throughout therapy and for several months following termination of therapy. In patients who develop HBV reactivation, TNF-blockers should be stopped and antiviral therapy with appropriate supportive treatment should be initiated. The safety of resuming TNF-blockers after HBV reactivation has been controlled is not known. Therefore, prescribers should exercise caution when considering resumption of TNF-blockers in this situation and monitor patients closely. Malignancies Malignancies, some fatal, have been reported among children, adolescents, and young adults who received treatment with TNF-blocking agents (initiation of therapy ≤ 18 years of age), of which SIMPONI is a member. Approximately half the cases were lymphomas, including Hodgkin’s and non-Hodgkin’s lymphoma. The other cases represented a variety of malignancies, including rare malignancies that are usually associated with immunosuppression, and malignancies that are not usually observed in children and adolescents. The malignancies occurred after a median of 30 months (range 1 to 84 months) after the first dose of TNF blocker therapy. Most of the patients were receiving concomitant immunosuppressants. These cases were reported post-marketing and are derived from a variety of sources, including registries and spontaneous NEWS GIHEP NEW S. COM • M AY 2015 S tudies from the last decade implicate aberrant immune response to gut bacteria in susceptible hosts as a trigger of mucosal infammation in Crohn’s disease and ulcerative colitis. It therefore seems plausible to be able to “reset” the mucosal immune response by manipulating intestinal fora with probiotics. A formulation of eight diferent strains of probiotic bacterial species called VSL#3 has been shown to alleviate symptoms and maintain remission in UC and pouchitis. Prior studies assessing efcacy of probiotics in the treatment of CD used formulations with individual strains of bacteria (Saccharomyces, lactobacillus, and Escherichia coli Nissle 1971) and failed to show any beneft over placebo. In the recent study by Fedorak SIMPONI® (golimumab) SIMPONI® (golimumab) postmarketing reports. The risks and benefits of TNF-blocker treatment including SIMPONI should be considered prior to initiating therapy in patients with a known malignancy other than a successfully treated non-melanoma skin cancer (NMSC) or when considering continuing a TNF-blocker in patients who develop a malignancy. In the controlled portions of clinical trials of TNF-blockers including SIMPONI, more cases of lymphoma have been observed among patients receiving anti-TNF treatment compared with patients in the control groups. During the controlled portions of the Phase 2 trials in RA, and the Phase 3 trials in RA, PsA and AS, the incidence of lymphoma per 100 patient-years of follow-up was 0.21 (95% CI: 0.03, 0.77) in the combined SIMPONI group compared with an incidence of 0 (95% CI: 0., 0.96) in the placebo group. In the controlled and uncontrolled portions of these clinical trials in 2347 SIMPONItreated patients with a median follow-up of 1.4 years, the incidence of lymphoma was 3.8-fold higher than expected in the general U.S. population according to the SEER database (adjusted for age, gender, and race).1 Through Week 60 of the UC trials, there were no cases of lymphoma with SIMPONI. Patients with RA and other chronic inflammatory diseases, particularly patients with highly active disease and/or chronic exposure to immunosuppressant therapies, may be at higher risk (up to several fold) than the general population for the development of lymphoma, even in the absence of TNF-blocking therapy. Cases of acute and chronic leukemia have been reported with postmarketing TNF-blocker use in rheumatoid arthritis and other indications. Even in the absence of TNF blocker therapy, patients with rheumatoid arthritis may be at a higher risk (approximately 2-fold) than the general population for the development of leukemia. Rare postmarketing cases of hepatosplenic T-cell lymphoma (HSTCL) have been reported in patients treated with TNF-blocking agents. This rare type of T-cell lymphoma has a very aggressive disease course and is usually fatal. Nearly all of the reported TNF-blocker associated cases have occurred in patients with Crohn’s disease or ulcerative colitis. The majority were in adolescent and young adult males. Almost all these patients had received treatment with azathioprine (AZA) or 6-mercaptopurine (6–MP) concomitantly with a TNF blocker at or prior to diagnosis. The potential risk with the combination of AZA or 6-MP and SIMPONI should be carefully considered. A risk for the development for hepatosplenic T-cell lymphoma in patients treated with TNF-blockers cannot be excluded. During the controlled portions of the Phase 2 trial in RA, and the Phase 3 trials in RA, PsA and AS, the incidence of malignancies other than lymphoma per 100 patient-years of follow-up was not elevated in the combined SIMPONI group compared with the placebo group. In the controlled and uncontrolled portions of these trials, the incidence of malignancies, other than lymphoma, in SIMPONI-treated patients was similar to that expected in the general U.S. population according to the SEER database (adjusted for age, gender, and race).1 In the 6-week placebo-controlled portions of the SIMPONI Phase 2/3 clinical trials in UC, the incidence of non-lymphoma malignancies (excluding non-melanoma skin cancer) was similar between the SIMPONI and the placebo group. Through Week 60, the incidence of non-lymphoma malignancies (excluding non-melanoma skin cancer) was similar to the general U.S. population according to the SEER database (adjusted for age, gender, and race).1 Short follow-up periods, such as those of one year or less in the studies above, may not adequately reflect the true incidence of malignancies. It is not known if SIMPONI treatment influences the risk for developing dysplasia or colon cancer. All patients with ulcerative colitis who are at increased risk for dysplasia or colon carcinoma (for example, patients with long-standing ulcerative colitis or primary sclerosing cholangitis), or who had a prior history of dysplasia or colon carcinoma should be screened for dysplasia at regular intervals before therapy and throughout their disease course. This evaluation should include colonoscopy and biopsies per local recommendations. In patients with newly diagnosed dysplasia treated with SIMPONI, the risks and benefits to the individual patient must be carefully reviewed and consideration should be given to whether therapy should be continued. Melanoma has been reported in patients treated with TNF-blocking agents, including SIMPONI. Merkel cell carcinoma has been reported in patients treated with TNF-blocking agents. Periodic skin examination is recommended for all patients, particularly those with risk factors for skin cancer. In controlled trials of other TNF-blockers in patients at higher risk for malignancies (e.g., patients with COPD, patients with Wegener’s granulomatosis treated with concomitant cyclophosphamide) a greater portion of malignancies occurred in the TNF-blocker group compared to the controlled group. In an exploratory 1-year clinical trial evaluating the use of 50, 100 and 200 mg of SIMPONI in 309 patients with severe persistent asthma, 6 patients developed malignancies other than NMSC in the SIMPONI groups compared to none in the control group. Three of the 6 patients were in the 200 mg SIMPONI group. Congestive Heart Failure Cases of worsening congestive heart failure (CHF) and new onset CHF have been reported with TNFblockers, including SIMPONI. In several exploratory trials of other TNF-blockers in the treatment of CHF, there were greater proportions of TNF-blocker treated patients who had CHF exacerbations requiring hospitalization or increased mortality. SIMPONI has not been studied in patients with a history of CHF and SIMPONI should be used with caution in patients with CHF. If a decision is made to administer SIMPONI to patients with CHF, these patients should be closely monitored during therapy, and SIMPONI should be discontinued if new or worsening symptoms of CHF appear. Demyelinating Disorders Use of TNFblockers, of which SIMPONI is a member, has been associated with rare cases of new onset or exacerbation of central nervous system (CNS) demyelinating disorders, including multiple sclerosis (MS) and peripheral demyelinating disorders, including Guillain-Barré syndrome. Cases of central demyelination, MS, optic neuritis, and peripheral demyelinating polyneuropathy have rarely been reported in patients treated with SIMPONI (see Adverse Reactions). Prescribers should exercise caution in considering the use of TNF-blockers, including SIMPONI, in patients with central or peripheral nervous system demyelinating disorders. Discontinuation of SIMPONI should be considered if these disorders develop. Use with Abatacept In controlled trials, the concurrent administration of another TNF-blocker and abatacept was associated with a greater proportion of serious infections than the use of a TNF-blocker alone; and the combination therapy, compared to the use of a TNF-blocker alone, has not demonstrated improved clinical benefit in the treatment of RA. Therefore, the combination of TNF-blockers including SIMPONI and abatacept is not recommended (see Drug Interactions). Use with Anakinra Concurrent administration of anakinra (an interleukin-1 antagonist) and another TNF-blocker, was associated with a greater portion of serious infections and neutropenia and no additional benefits compared with the TNF-blocker alone. Therefore, the combination of anakinra with TNF-blockers, including SIMPONI, is not recommended (see Drug Interactions). Switching Between Biological Disease Modifying Antirheumatic Drugs Care should be taken when switching from one biological product to another biological product since overlapping biological activity may further increase the risk of infection. Hematologic Cytopenias There have been post-marketing reports of pancytopenia, leukopenia, neutropenia, aplastic anemia, and thrombocytopenia in patients receiving TNF-blockers. In clinical trials, cases of pancytopenia, leukopenia, neutropenia, and thrombocytopenia have also occurred in SIMPONI-treated patients. Caution should be exercised when using TNF-blockers, including SIMPONI, in patients who have or have had significant cytopenias. Vaccinations/Therapeutic Infectious Agents Live Vaccines Patients treated with SIMPONI may receive vaccinations, except for live vaccines. In patients receiving anti-TNF therapy, limited data are available on the response to live vaccination, or on the secondary transmission of infection by live vaccines. Use of live vaccines could result in clinical infections, including disseminated infections. Therapeutic Infectious Agents Other uses of therapeutic infectious agents such as live attenuated bacteria (e.g., BCG bladder instillation for the treatment of cancer) could result in clinical infections, including disseminated infections. It is recommended that therapeutic infectious agents not be given concurrently with SIMPONI. Non-live Vaccines In the Phase 3 PsA trial, after pneumococcal vaccination, a similar proportion of SIMPONI-treated and placebo-treated patients were able to mount an adequate immune response of at least a 2-fold increase in antibody titers to pneumococcal polysaccharide vaccine. In both SIMPONI-treated and placebo-treated patients, the proportions of patients with response to pneumococcal vaccine were lower among patients receiving MTX compared with patients not receiving MTX. The data suggest that SIMPONI does not suppress the humoral immune response to the pneumococcal vaccine. Hypersensitivity Reactions In post-marketing experience, serious systemic hypersensitivity reactions (including anaphylactic reaction) have been reported following SIMPONI administration. Some of these reactions occurred after the first administration of SIMPONI. If an anaphylactic or other serious allergic reaction occurs, administration of SIMPONI should be discontinued immediately and appropriate therapy instituted. ADVERSE REACTIONS: Clinical Trials Experience Because clinical trials are conducted under widely varying conditions, adverse reaction rates observed in the clinical trials of a drug cannot be directly compared to rates in the clinical trials of another drug and may not reflect the rates observed in clinical practice. The safety data described below are based on 5 pooled, randomized, double-blind, controlled Phase 3 trials in patients with RA, PsA, and AS (Trials RA-1, RA-2, RA-3, PsA, and AS) (see Clinical Studies). These 5 trials included 639 controltreated patients and 1659 SIMPONI-treated patients including 1089 with RA, 292 with PsA, and 278 with AS. The safety data in 1233 SIMPONI-treated patients with ulcerative colitis from 3 pooled, randomized, double-blind, controlled Phase 2/3 trials are also described below (Trials UC-1, UC-2, and UC-3) (see Clinical Studies). The proportion of patients who discontinued treatment due to adverse reactions in the controlled Phase 3 trials through Week 16 in RA, PsA and AS was 2% for SIMPONI-treated patients and 3% for placebo-treated patients. The most common adverse reactions leading to discontinuation of SIMPONI in the controlled Phase 3 trials in RA, PsA and AS through Week 16 were sepsis (0.2%), alanine aminotransferase increased (0.2%), and aspartate aminotransferase increased (0.2%). The most common adverse drug reactions leading to discontinuation through Week 60 of the UC trials in patients who received SIMPONI induction and 100 mg during maintenance compared with patients who received SIMPONI induction and placebo during maintenance were tuberculosis (0.3% vs 0.6%) and anemia (0.3% vs 0%), respectively. The most serious adverse reactions were: • Serious Infections (see Warnings and Precautions) • Malignancies (see Warnings and Precautions) Upper respiratory tract infection and nasopharyngitis were the most common adverse reactions reported in the combined Phase 3 RA, PsA and AS trials through Week 16, occurring in 7% and 6% of SIMPONI-treated patients as compared with 6% and 5% of control-treated patients, respectively. Infections In controlled Phase 3 trials through Week 16 in RA, PsA, and AS, infections were observed in 28% of SIMPONI-treated patients compared to 25% of control-treated patients. For serious infections, see the Warnings and Precautions section (see Warnings and Precautions). In the controlled Phase 2/3 trial of SIMPONI induction through Week 6 in UC, the rates of infections were similar in SIMPONI 200/100 mg-treated patients and placebo-treated patients, or approximately 12%. Through Week 60, the incidence per patient year of infections was similar in patients who received SIMPONI induction and 100 mg during maintenance compared with patients who received SIMPONI induction and placebo during the maintenance portion of the UC trial. Demyelinating Disorders In the controlled Phase 2/3 trial of SIMPONI induction through Week 6, no cases of demyelination were observed in SIMPONI 200/100 mg-treated patients or placebo-treated patients. Through Week 60, there were no cases of 13 and colleagues, the probiotic formulation VSL#3 did not decrease the likelihood of developing severe endoscopic lesions (Rutgeert’s grade 3 or 4) at 90 days following surgery for CD, when compared to placebo. Continued on following page 14 NEWS Continued from previous page Patients in the VSL#3 arm demonstrated lower levels of infammatory cytokines in the colonic mucosal biopsies; however, this did not translate to a signifcant diference MAY 2 0 1 5 • G I & HEPATO LO G Y NEW S over placebo in the rates of severe endoscopic recurrence at 3 and 12 months following surgery. While probiotics are safe and well tolerated, data supporting efcacy in CD are sparse at best. This may in part be due to variations in the bacte- rial communities found in the colon and small bowel, and following loss of the ileo-cecal valve postoperatively. Until larger studies are undertaken to investigate the potential for probiotics in the management of CD, immune modulators and biologic therapies remain the mainstay of treatment. Dr. Manreet Kaur is assistant professor, department of medicine, division of gastroenterology and hepatology, Baylor University, Houston. She has no conficts of interest. SIMPONI® (golimumab) SIMPONI® (golimumab) demyelination in the SIMPONI 100 mg group during maintenance. One case of CNS demyelination was observed in the placebo maintenance group in a patient who received SIMPONI 400/200 mg during induction. Liver Enzyme Elevations There have been reports of severe hepatic reactions including acute liver failure in patients receiving TNF-blockers. In controlled Phase 3 trials of SIMPONI in patients with RA, PsA, and AS through Week 16, ALT elevations ≥ 5 x ULN occurred in 0.2% of control-treated patients and 0.7% of SIMPONI-treated patients and ALT elevations ≥ 3 x ULN occurred in 2% of control-treated patients and 2% of SIMPONI-treated patients. Since many of the patients in the Phase 3 trials for RA, PsA, and AS were also taking medications that cause liver enzyme elevations (e.g., NSAIDs, MTX), the relationship between SIMPONI and liver enzyme elevation is not clear. In Phase 2/3 UC trials, the incidence of ALT elevations ≥ 5 x ULN was similar in SIMPONI-treated patients and placebotreated patients, or approximately 1%, with an average duration of follow-up of 46 weeks and 18 weeks, respectively. ALT elevations ≥ 3 x ULN occurred in 2.0% of SIMPONI-treated patients compared with 1.5% of placebo-treated patients with an average duration of follow-up of 46 weeks and 18 weeks, respectively. Autoimmune Disorders and Autoantibodies The use of TNF-blockers, including SIMPONI, has been associated with the formation of autoantibodies and, rarely, with the development of a lupus-like syndrome. In the controlled Phase 3 trials in patients with RA, PsA, and AS through Week 14, there was no association of SIMPONI treatment and the development of newly positive anti-dsDNA antibodies. In Phase 3 trials in RA, PsA, and AS through 1 year of follow up, 4.0% of SIMPONI-treated patients and 2.6% of control patients were newly ANApositive (at titers of 1:160 or greater). The frequency of anti-dsDNA antibodies at 1 year of follow up was uncommon in patients who were anti-dsDNA negative at baseline. Through Week 60 of the UC trials, 3.5% of patients who received SIMPONI induction and 100 mg during maintenance were newly ANA-positive (at titers of 1:160 or greater) compared with 3.5% of patients who received SIMPONI induction and placebo during the maintenance portion of the UC trial. The frequency of anti-dsDNA antibodies at 1 year of follow up in patients who were anti-dsDNA negative at baseline was 0.5% in patients receiving SIMPONI induction and 100 mg during maintenance compared with 0% in patients who received SIMPONI induction and placebo during maintenance. Injection Site Reactions In controlled Phase 3 trials through Week 16 in RA, PsA and AS, 6% of SIMPONI-treated patients had injection site reactions compared with 2% of control-treated patients. The majority of the injection site reactions were mild and the most frequent manifestation was injection site erythema. In the controlled Phase 2/3 trial through Week 6 in UC, 3.4% of SIMPONI-treated patients had injection site reactions compared with 1.5% in control-treated patients. The majority of the injection site reactions were mild and moderate and the most frequent manifestation was injection site erythema. In controlled Phase 2 and 3 trials in RA, PsA, AS, and Phase 2/3 UC trials, no patients treated with SIMPONI developed anaphylactic reactions. Immunogenicity Antibodies to SIMPONI were detected in 57 (4%) of SIMPONI-treated patients across the Phase 3 RA, PsA, and AS trials through Week 24. Similar rates were observed in each of the three indications. Patients who received SIMPONI with concomitant MTX had a lower proportion of antibodies to SIMPONI than patients who received SIMPONI without MTX (approximately 2% versus 7%, respectively). The presence of serum concentrations of golimumab can interfere with the detection of antibodies to SIMPONI leading to inconclusive results. In UC trials, 34 (3%), 341 (28%) and 823 (69%) of SIMPONI-treated subjects were positive, negative and inconclusive for antibodies to SIMPONI, respectively. Treatment with concomitant immunomodulators (AZA, 6-MP and MTX) resulted in a lower proportion of patients with antibodies to SIMPONI than patients receiving SIMPONI without immunomodulators (2% versus 4%, respectively). Of the patients with a positive antibody response to SIMPONI in the Phase 2 and 3 trials, most were determined to have neutralizing antibodies to golimumab as measured by a cell-based functional assay. The small number of patients positive for antibodies to SIMPONI limits the ability to draw definitive conclusions regarding the relationship between antibodies to golimumab and clinical efficacy or safety measures. The data above reflect the percentage of patients whose test results were considered positive for antibodies to SIMPONI in an ELISA assay, and are highly dependent on the sensitivity and specificity of the assay. Additionally, the observed incidence of antibody positivity in an assay may be influenced by several factors including sample handling, timing of sample collection, concomitant medications, and underlying disease. For these reasons, comparison of the incidence of antibodies to SIMPONI with the incidence of antibodies to other products may be misleading. Other Adverse Reactions The adverse drug reactions that occurred at a rate of at least 1% in the SIMPONI ± DMARD group and with a higher incidence than in the placebo ± DMARD group during the controlled period of the 5 pooled Phase 3 trials through Week 16 in patients with RA, PsA, and AS are summarized below. Patients may have taken concomitant MTX, sulfasalazine, hydroxychloroquine, low dose corticosteroids (≤ 10 mg of prednisone/day or equivalent), and/or NSAIDs during the trials). The numbers (percentages) of adverse drug reactions for SIMPONI ± DMARDs-treated patients (n=1659) and Placebo ± DMARDs-treated patients (n=639), respectively, were: Infections and Infestations: Upper respiratory tract infection (nasopharyngitis, pharyngitis, laryngitis, and rhinitis) 16%, 13%; Viral infections (such as infuenza and herpes) 5%, 3%; Bronchitis 2%, 1%; Superfcial fungal infections 2%, 1%; Sinusitis 2%, 1%; General disorders and administration site conditions: Injection site reaction (injection site erythema, urticaria, induration, pain, bruising, pruritus, irritation, paresthesia) 6%, 2%; Investigations: Alanine aminotransferase increased 4%, 3%; Aspartate aminotransferase increased 3%, 2%; Vascular disorders: Hypertension 3%, 2%; Nervous system disorders: Dizziness 2%, 1%; Paresthesia 2%, 1%; Gastrointestinal Disorders: Constipation 1%, <1%. Less common clinical trial adverse drug reactions Adverse drug reactions that occurred <1% in SIMPONI-treated patients during the SIMPONI clinical trials that do not appear in the Warnings and Precautions section included the following events listed by system organ class: Infections and infestations: Septic shock, atypical mycobacterial infection, pyelonephritis, arthritis bacterial, bursitis infective Neoplasms benign, malignant and unspecified: Leukemia Skin and subcutaneous tissue disorders: Psoriasis (new onset or worsening, palmar/ plantar and pustular), vasculitis (cutaneous) Vascular disorders: Vasculitis (systemic) Other clinical trial adverse drug reactions in ulcerative colitis clinical trials In the Phase 2/3 trials in UC evaluating 1233 SIMPONI-treated patients, no new adverse drug reactions were identified and the frequency of adverse drug reactions was similar to the safety profile observed in patients with RA, PsA and AS. Post-marketing Experience The following adverse reactions have been identified during post-approval use of SIMPONI. Because these reactions are reported voluntarily from a population of uncertain size, it is not always possible to reliably estimate their frequency or establish a causal relationship to SIMPONI exposure. Immune System Disorders: Serious systemic hypersensitivity reactions (including anaphylactic reaction) (see Warnings and Precautions), sarcoidosis Neoplasms benign, malignant and unspecified: Melanoma (see Warnings and Precautions) Respiratory, thoracic and mediastinal disorders: Interstitial lung disease Skin and subcutaneous tissue disorders: Skin exfoliation, rash, bullous skin reactions DRUG INTERACTIONS: Methotrexate For the treatment of RA, SIMPONI should be used with methotrexate (MTX) (see Clinical Studies). Since the presence or absence of concomitant MTX did not appear to influence the efficacy or safety of SIMPONI in the treatment of PsA or AS, SIMPONI can be used with or without MTX in the treatment of PsA and AS (see Clinical Studies and Clinical Pharmacology). Biological Products for RA, PsA, and/or AS An increased risk of serious infections has been seen in clinical RA trials of other TNF-blockers used in combination with anakinra or abatacept, with no added benefit; therefore, use of SIMPONI with abatacept or anakinra is not recommended (see Warnings and Precautions). A higher rate of serious infections has also been observed in RA patients treated with rituximab who received subsequent treatment with a TNF-blocker. The concomitant use of SIMPONI with biologics approved to treat RA, PsA, or AS is not recommended because of the possibility of an increased risk of infection. Live Vaccines/Therapeutic Infectious Agents Live vaccines should not be given concurrently with SIMPONI (see Warnings and Precautions). Therapeutic infectious agents should not be given concurrently with SIMPONI (see Warnings and Precautions). Infants born to women treated with SIMPONI during their pregnancy may be at increased risk of infection for up to 6 months. Administration of live vaccines to infants exposed to SIMPONI in utero is not recommended for 6 months following the mother’s last SIMPONI injection during pregnancy (see Use in Specific Populations). Cytochrome P450 Substrates The formation of CYP450 enzymes may be suppressed by increased levels of cytokines (e.g., TNFα) during chronic inflammation. Therefore, it is expected that for a molecule that antagonizes cytokine activity, such as golimumab, the formation of CYP450 enzymes could be normalized. Upon initiation or discontinuation of SIMPONI in patients being treated with CYP450 substrates with a narrow therapeutic index, monitoring of the effect (e.g., warfarin) or drug concentration (e.g., cyclosporine or theophylline) is recommended and the individual dose of the drug product may be adjusted as needed. USE IN SPECIFIC POPULATIONS: Pregnancy Pregnancy Category B – There are no adequate and well-controlled trials of SIMPONI in pregnant women. Because animal reproduction and developmental studies are not always predictive of human response, it is not known whether SIMPONI can cause fetal harm when administered to a pregnant woman or can affect reproduction capacity. SIMPONI should be used during pregnancy only if clearly needed. An embryofetal developmental toxicology study was performed in which pregnant cynomolgus monkeys were treated subcutaneously with golimumab during the first trimester with doses up to 50 mg/kg twice weekly (360 times greater than the maximum recommended human dose-MRHD) and has revealed no evidence of harm to maternal animals or fetuses. Umbilical cord blood samples collected at the end of the second trimester showed that fetuses were exposed to golimumab during gestation. In this study, in utero exposure to golimumab produced no developmental defects to the fetus. A pre- and post-natal developmental study was performed in which pregnant cynomolgus monkeys were treated with golimumab during the second and third trimesters, and during lactation at doses up to 50 mg/kg twice weekly (860 times and 310 times greater than the maximal steady state human blood levels for maternal animals and neonates, respectively) and has revealed no evidence of harm to maternal animals or neonates. Golimumab was present in the neonatal serum from the time of birth and for up to six months postpartum. Exposure to golimumab during gestation and during the postnatal period caused no developmental defects in the infants. IgG antibodies are known to cross the placenta during pregnancy and have been detected in the serum of infants born to patients treated with these antibodies. Since SIMPONI is an IgG antibody, infants born to women treated with SIMPONI during their pregnancy may be at increased risk of infection for up to 6 months. Administration of live vaccines to infants exposed to SIMPONI in utero is not recommended for 6 months following the mother’s last SIMPONI injection during pregnancy (see Warnings and Precautions). Nursing Mothers It is not known whether SIMPONI is excreted in human milk or absorbed systemically after ingestion. Because many drugs and immunoglobulins are excreted in human milk, and because of the potential for NEWS FROM THE AGA GIHEP NEW S. COM • M AY 2015 15 Consensus statement on dysplasia in IBD patients A GA and ASGE have issued updated recommendations for the surveillance and management of dysplasia in patients with IBD. The consensus statement represents an efort to unify consensus recommenda- tions to address two primary issues: 1) how should surveillance to detect dysplasia be performed; and 2) how should dysplasia be managed. The consensus statement addresses the optimal types of endoscopic pro- cedures and equipment to be used, recommended practices for removal of lesions, or referral for the more invasive surgical procedure, colectomy. In particular, the updated recommendations refect a shift to chromoendoscopy for SIMPONI® (golimumab) SIMPONI® (golimumab) adverse reactions in nursing infants from SIMPONI, a decision should be made whether to discontinue nursing or to discontinue the drug, taking into account the importance of the drug to the mother. In the pre- and post-natal development study in cynomolgus monkeys in which golimumab was administered subcutaneously during pregnancy and lactation, golimumab was detected in the breast milk at concentrations that were approximately 400-fold lower than the maternal serum concentrations. Pediatric Use Safety and effectiveness of SIMPONI in pediatric patients less than 18 years of age have not been established. Geriatric Use In the Phase 3 trials in RA, PsA, and AS, there were no overall differences in SAEs, serious infections, and AEs in SIMPONI-treated patients ages 65 or older (N = 155) compared with younger SIMPONI-treated patients. In UC, there were insufficient numbers of patients aged 65 and over to determine whether they respond differently from patients aged 18 to 65. Because there is a higher incidence of infections in the geriatric population in general, caution should be used in treating geriatric patients with SIMPONI. OVERDOSAGE: In a clinical trial, 5 patients received protocol-directed single infusions of 10 mg/kg of intravenous SIMPONI without serious adverse reactions or other significant reactions. The highest weight patient was 100 kg, and therefore received a single intravenous infusion of 1000 mg of SIMPONI. There were no SIMPONI overdoses in the clinical trials. PATIENT COUNSELING INFORMATION: See FDA-approved patient labeling (Medication Guide and Instructions for Use) Patients should be advised of the potential benefits and risks of SIMPONI. Physicians should instruct their patients to read the Medication Guide before starting SIMPONI therapy and to read it each time the prescription is renewed. Infections Inform patients that SIMPONI may lower the ability of their immune system to fight infections. Instruct the patient of the importance of contacting their doctor if they develop any symptoms of infection, including tuberculosis, invasive fungal infections, and hepatitis B reactivation. Malignancies Patients should be counseled about the risk of lymphoma and other malignancies while receiving SIMPONI. Allergic Reactions Advise latexsensitive patients that the needle cover on the prefilled syringe as well as the prefilled syringe in the prefilled SmartJect autoinjector contains dry natural rubber (a derivative of latex). Other Medical Conditions Advise patients to report any signs of new or worsening medical conditions such as congestive heart failure, demyelinating disorders, autoimmune diseases, liver disease, cytopenias, or psoriasis. Instructions for Safe Administration The first self-injection should be performed under the supervision of a qualified healthcare professional. If a patient or caregiver is to administer SIMPONI, he/she should be instructed in injection techniques and their ability to inject subcutaneously should be assessed to ensure the proper administration of SIMPONI. Advise the patient to read the FDA-approved Instructions for Use and provide the following instructions to patients: • Prior to use, remove the prefilled syringe or the prefilled SmartJect autoinjector from the refrigerator and allow SIMPONI to sit at room temperature outside of the carton for 30 minutes and out of the reach of children. • Do not warm SIMPONI in any other way. For example, do not warm SIMPONI in a microwave or in hot water. • Do not remove the prefilled syringe needle cover or SmartJect autoinjector cap while allowing SIMPONI to reach room temperature. Remove these immediately before injection. • Do not pull the autoinjector away from the skin until you hear a first “click” sound and then a second “click” sound (the injection is finished and the needle is pulled back). It usually takes about 3 to 6 seconds but may take up to 15 seconds for you to hear the second “click” after the first “click”. If the autoinjector is pulled away from the skin before the injection is completed, a full dose of SIMPONI may not be administered. • A puncture-resistant container for disposal of needles and syringes should be used. Patients or caregivers should be instructed in the technique of proper syringe and needle disposal, and be advised not to reuse these items. REFERENCES: 1. SEER [database online]. US Population Data – 1969-2004. Bethesda, MD: National Cancer Institute. Release date: January 3, 2007. Available at: http//seer.cancer.gov/popdata/. © Janssen Biotech, Inc. 2014 Horsham, PA 19044 1-800-JANSSEN (1-800-526-7736) US License No. 1864 Revised: 12/2014 025953-141204 patients with IBD during screening and surveillance to better visualize the tissue. Chromoendoscopy involves the use of dye sprayed onto the mucosa during the procedure. The new recommendations were developed by an international group of experts and stakeholders in IBD surveillance, in accordance with suggested standards from the Institute of Medicine. Existing guidelines on this topic, which were written by numerous expert groups, were considered, and in some cases, accepted in the new consensus statement. The consensus statement was published in the March issues of Gastroenterology and GIE: Gastrointestinal Endoscopy. [email protected] Fellows application period open: 2016 A GA honors superior professional achievement in clinical private or academic practice and in research with fellowship in the organization. Fellowships are awarded to members whose accomplishments and contributions demonstrate personal commitment to the feld of gastroenterology. AGA Fellows will be acknowledged in several ways, including a certifcate and the privilege of using the prestigious designation “AGAF” in professional activities. Learn more and complete the online application today at www.gastro.org/about/aga-fellows-program. The deadline for submissions is Friday, July 24, 2015. [email protected] New AGA guideline: pancreatic cysts A new AGA guideline provides direction to GIs and their patients with pancreatic cysts identifed during abdominal imaging. The guideline recommends that most patients with asymptomatic pancreatic cysts should be conservatively monitored with a longer surveillance period and more consideration of risks and benefts to patients before moving to surgery. To view this guideline, as well as the accompanying technical review and clinical decision tool, visit www.gastro.org/guidelines. [email protected] NEWS FROM THE AGA 16 MAY 2 0 1 5 • G I & HEPATO LO G Y NEW S Innovation to help patients with chronic liver disease T he American Gastroenterological Association (AGA) Research Foundation is pleased to announce that Ashish Nimgaonkar, MBBS, MTech, MS, from John Hopkins University, has received the inaugural AGA–Boston Scientifc Career Development Technology & Innovation Award. This award is graciously supported by a grant from Boston Scientifc, a leading innovator of medical solutions. “Dr. Nimgaonkar’s research represents a potential breakthrough in the treatment of patients with chronic liver disease,” said Dr. Martin Brotman, AGAF, chair, AGA Research Foundation. “The AGA Research Download the new AGA Publication Apps! Delivering convenient and interactive news and features on the go. P R E M I E R E The I S S U E NEW GASTROENTEROLOGIST INSIGHTS FOR FELLOWS & YOUNG GIs A Quarterly Supplement to GI & Hepatology News | Spring 2015 16 Postfellowship Pathways Advanced Endoscopy Fellowship 26 Protecting Your Future A Discussion About Disability Insurance for GIs HCV Update The Current State of Hepatitis C Therapy 8 The NEW GASTROENTEROLOGIST INSIGHTS FOR FELLOWS & YOUNG GIs A Quarterly Supplement to GI & Hepatology News Full interactive digital editions. FREE download available for iOS, Android, and Amazon Kindle. GIHEPNEWS.COM Foundation is proud to support Dr. Nimgaonkar as he works to enhance this technology and bring it one step closer to clinical practice.” Dr. Nimgaonkar’s research focuses on developing technology to manage patients with refractory ascites – a condition in which fuid builds up in the abdomen. This fuid accumulation eventually becomes resistant to medical therapy and the only defnitive treatment at this stage is liver transplantation, which is limited by organ availability. Patients with refractory ascites experience considerable deterioration in quality of life from abdominal discomfort and difculty breathing. The only option for them is removal of this fuid every few weeks in a hospital or clinical setting. Dr. Nimgaonkar and his colleagues have developed a wireless implantable shunt technology to pull the fuid from the peritoneal space into the stomach. With this approach, patients can manage their fuid drainage needs at home – signifcantly improving their quality of life, as well as reducing the cost of care associated with frequent hospital visits. Dr. Nimgaonkar and colleagues have demonstrated proof-of-concept for this approach in animal models and built shunt prototypes. The AGA–Boston Scientifc Career Development Technology & Innovation Award will enable Dr. Nimgaonkar to continue to refne and test this newly developed technology. “This award enables young investigators to develop their research careers and ensures that their valuable time is spent researching unique and novel technology for clinical care,” said David Pierce, senior vice president and president, endoscopy, Boston Scientifc. “We are pleased to support this project and wish Dr. Nimgaonkar much success in his endeavors.” The AGA–Boston Scientifc Career Development Technology & Innovation Award provides Dr. Nimgaonkar with $180,000 over 2 years – ensuring that a major proportion of his time is protected for research. AGA announced its partnership with Boston Scientifc in September 2013. In addition to funding this award, Boston Scientifc’s grant provides ongoing support to AGA’s central initiatives in technology and research, including the AGA Center for GI Innovation and Technology, the annual AGA Technology Summit, and the AGA Research Foundation Corporate Roundtable. [email protected] Pages 16a—16b u NEWS FROM THE AGA GIHEP NEW S. COM • M AY 2015 17 AGA Strategic Plan 2015-2020: Something that matters Publications Lead the GI/hepatology category of scientifc journals in rank, reach and accessibility while meeting the readership needs of basic and clinical investigators, practitioners, young GIs and trainees. • Achieve and maintain high-impact factors for all journals. • Rank highest in the feld for meeting the readership needs of basic and clinical investigators, practitioners, young GIs and trainees. • Expand journals’ reach via new content dissemination technologies. • Increase usage of the journals’ digital platforms. BY JOHN I. ALLEN, M.D., MBA, AGAF, PRESIDENT, AGA INSTITUTE Overview of the plan Two words describe each of the 3 fundamental AGA areas as illustrated in the triangular portion of the plan (Figure 1). For example practice and quality were paired intentionally to emphasize their close connection and the AGA’s increasing commitment to increasing the “value” (defned as quality per unit cost) of our GI and liver care. Research is critical to our advancing science, but needs to be coupled with AGA’s commitment to promote innovation in medical device and therapeutic advances, through the AGA Center for GI Innovation and Technology and the AGA Center for Diagnostics and Therapeutics. Finally, education must be paired with training our physician and provider workforce in new and emerging technologies. The plan includes specifc reference to patients. Throughout the four goals and supporting strategies, patient engagement, patient voice and patient experience all are emphasized. AGA Strategic Plan at a glance Practice & quality Defne optimal clinical practice and help gastroenterologists provide high-quality, high-value care. • Within the framework of the Triple Aim, defne high-value care for GI disorders. • Increase the number of gastroenterologists reporting on quality of care. • Build and engage an active grassroots network to communicate and advise AGA of emerging practice issues and trends. • Address evolving practice and reimbursement models in all practice settings. AGA InstItute I ’m proud to share with you the new strategic plan of the American Gastroenterological Association (AGA). Thanks to the hundreds of members who worked to ensure that the plan is responsive to the needs of thousands in the gastroenterology community. Throughout the process of developing the strategic plan, the phrase “start something that matters1” echoed through my head. In 1897, a group of physicians started the AGA to make a diference in the lives of their colleagues and their patients. Since that time, AGA has been the driving force behind advances that matter in gastroenterology and Hepatology research and practice. We have made staggering scientifc discoveries and applied them to improve patient care. However, we still have so much more to learn, and that’s why the AGA Strategic Plan matters. AGA, at our heart, is a learning organization. This new strategic plan will lead us to new discoveries in GI science, new tools to improve patient care, new ways to educate ourselves and the gastroenterologists of the future. Together we will shape a bright future for gastroenterology and our patients. Ultimately, the AGA Strategic Plan will mobilize the resources of our organization to fulfll our mission of advancing the science and practice of gastroenterology. Figure 1. Diagrammatic representation of the AGA Strategic Plan. Key sections are linked together (such as Practice and Quality) to represent the need to coordinate them organizationally. Research & innovation Foster scientifc discovery and the application of new knowledge to improve care of patients with digestive disease. • Target junior faculty engaged in research for special support. • Increase strategic innovation and research collaborations to promote high-value clinical care. • Support promising advances in research and innovation. Education & training Engage members and other GI health providers through personalized education across the continuum of their careers. • Help members satisfy requirements for certifcation, recertifcation, continuing medical education and licensure. • Educate members about emerging technologies, procedures and scientifc discoveries to improve patient care. • Help members and other learners develop their careers and navigate transitions. • Use state-of-the-art and innovative technology platforms for learning. AGA section Advocacy Infuence public policies to support quality patient care, improve the practice of gastroenterology, and advance digestive disease research and education. • Pursue policies that ensure patients have access to appropriate, afordable, high-value GI care. • Increase opportunities for funding digestive disease research. • Develop a grassroots network to advocate for improvements in patient care, increased research funding and the viability of GI practice. • Strongly advocate for sufcient federal funding of academic training programs. Organizational vitality Maintain a robust and diverse membership, develop society leaders, foster strategic collaborations, and maintain an infrastructure that supports AGA’s mission and goals. • Increase AGA’s membership. • Develop a sustainable global strategy. • Conduct leadership development and prepare members to serve in volunteer leadership positions within AGA. • Strive for diversity at all levels within the association, including governance, committee structure, stafng and program development. Diversity is an inclusive concept that encompasses race, ethnicity, national origin, religion, gender, age, sexual orientation and disability. The planning process In revising the plan, AGA leadership decided to focus in some interesting and innovative ways. Before Digestive Disease Week (DDW) 2014, Anil Rustgi (immediate past president) and I appointed 4 task forces each composed of scientists, academic clinicians, community practitioners, and AGA staf. The task forces were assigned to consider 1 of 3 topics, refected in the triangular fgure of our plan (Figure 1): research and innovation, practice and quality, and education and training. We also assigned AGA leadership and staf to focus on additional AGA areas including advocacy, publications, communications and organizational vitality. The task forces identifed key goals and strategies at meetings during DDW and subsequent teleconferences. Input from more than 75 members and staf helped shape the initial plan. In July 2014, the AGA Governing Board met for a 3-day retreat during which ideas were distilled into the plan we have today. Reference 1. Mycoskie B. Start something that matters. New York, NY: Spiegel and Grau, 2011. Acknowledgements Thanks to everyone who contributed to this plan and those who will use it and improve upon it in the future. We all look forward to a bright future for gastroenterology. This article appeared previously in Gastroenterology (2015;148:1053–4). The author discloses no conficts. [email protected] 18 LIVER DISEASES MAY 2 0 1 5 • G I & HEPATO LO G Y NEW S New hepatitis treatments cost effective for some BY KARI OAKES Frontline Medical News F or individuals infected with hepatitis C virus (HCV), new regimens are highly efective, but also very expensive, at approximately $28,000 for 4 weeks of treatment. However, the treatment is cost efective for HCV patients with cirrhosis and for those without cirrhosis who have failed other treatments, according to a new study. In an analysis of the cost efectiveness of sofosbuvir-based treatments for patients with HCV genotypes 2 and 3, Dr. Benjamin Linas of Boston Medical Center reported that when compared with pegylated interferon and ribavirin therapy, treatment regimens based on the new direct-acting antiviral are only cost efective for select groups (Ann. Intern Med. 2015 [doi:10.7326/M15-0674]). Cure rates with sofosbuvir are higher than rates with the previous standard of care, and sustained virologic response (SVR) “is associated with a greatly reduced lifetime risk for AGA Resources Review the AGA Hepatitis C Clinical Service Line to learn more about managing the disease at www.gastro.org/practice/ clinical-service-line/hcv-clinicalservice-line liver-related morbidity and mortality,” noted Dr. Linas and his colleagues. Using sophisticated statistical modeling to compare HCV treatment with pegylated interferon and ribavirin – the previous standard of care – to the newly Food and Drug Administration–approved sofosbuvir-ribavirin regimen, Dr. Linas explored clinical outcomes and costs for several diferent patient groups, including treatment-naive and treatment-experienced HCV genotype 2 and 3 patients with and without cirrhosis. Clinical outcomes, modeled from clinical trial and observational cohort data, were expressed as life expectancy in quality-adjusted life-years (QALYs) and lifetime medical costs. Investigators then calculated the incremental cost-efectiveness ratio (ICER) for each treatment strategy, dividing any additional cost for a more expensive treatment by the QALYs gained from this regimen. Using the commonly accepted ICER threshold of $100,000 per QALY, Dr. Linas and colleagues concluded that sofosbuvir-based HCV therapy for treatment-naive patients without cirrhosis was not cost efective, with ICERs of $238,000-$266,000. Interferon-based treatments, they noted, still achieve an approximately 80% rate of cure in this population. In the constrained resources of the real world, Dr. Linas and his associates noted that this analysis is import- ant. “Treatment strategies that do not use limited resources where they are likely to have the greatest impact may result in unequal access to interferon-free regimens, thereby limiting the population-level benefts of new HCV treatments,” they said. The National Institute on Drug Abuse and the National Institute of Allergy and Infectious Disease provided funding. Dr. Milton Weinstein reported compensation from OptumInsight; Dr. Arthur Kim received grants and compensation from Gilead, AbbVie, and Bristol-Myers Squibb. The other authors reported no relevant disclosures. [email protected] PERSPECTIVE HCV cost-effectiveness analysis raises tough questions for payers I n an editorial accompanying Dr. Linas’ study, Dr. Etzion and Dr. Ghany placed this analysis of the cost-efectiveness of sofosbuvir in the context of payer and clinician priorities. They noted that “from the patient and physician perspective, the benefts of new treatment are evident.” For payers, however, resources are constrained and tough decisions will have to be made. This cost-efectiveness analysis is needed to inform resource allocation decisions, since the cost of using direct-acting antivirals to treat all those infected in the United States alone would exceed $300 billion. In that context, the editorial noted, quality-of-life assessments become important. HCV infection causes relatively little diminution of quality of life until the stage of cirrhosis is reached; in this analysis, therefore, interferon-based regimens are still a reasonable choice for treatment-naive HCV patients without cirrhosis. Though Dr. Linas’ study also models incremental cost-efectiveness ratios for various lower price points for sofosbuvir, the editorial authors point out that the price point for the public’s willingness to eradicate HCV has not been established. Dr. Ohad Etzion and Dr. Marc G. Ghany are at the National Institute of Diabetes and Digestive and Kidney Diseases, National Institutes of Health, Bethesda, Md. Dr. Ghany reported nonfnancial support from Bristol-Meyers Squibb. Novel HCV therapies found cost effective, with caveats BY MARY ANN MOON Frontline Medical News T wo diferent statistical models found that novel therapies for chronic HCV infection, particularly the combination of sofosbuvir and ledipasvir, are cost efective in most patients, according to separate reports published online in Annals of Internal Medicine. The novel therapies, which typically contain sofosbuvir in combination with ledipasvir, simeprevir, or daclatasvir, substantially reduce the length of treatment, achieve much higher rates of sustained viral response (SVR), and ofer interferon-free alter- natives for patients who can’t tolerate or don’t respond to standard interferon-based treatments. Both statistical models were developed to examine this issue, but from diferent perspectives. In one study, investigators constructed a model that simulated 120 possible clinical courses of HCV-infectContinued on page 20 PERSPECTIVE Is the price of treatment too high? To whom? T he development and widespread use of highly efcacious direct-acting antiviral agents (DAAs) represent a paradigm shift in which the retail cost of treatment is now the most signifcant barrier to hepatitis C virus (HCV) eradication. We have begun to learn the medical value of curing HCV in the context of the staggering burden of chronic liver disease, but less is known about the economic value of the cost of therapy. There has been public outcry over the $1,000 per pill price tag of sofosbuvir, but demand for the medications remains high as nearly all HCV-infected patients are now treatment eligible. These studies collectively demonstrate a favorable incremental cost-efectiveness ratio per adjusted life-year relative to interferon-containing regimens in most patients with HCV: genotype 1, treatment experienced, and cirrhotic. And these studies illustrate the paradox at the crux of the issue: How can the novel HCV therapies be both cost efective for most HCV patients but simultaneously unafordable for payers? Although the price of achieving a sustained virologic response is reduced with the DAA reg- imens, the cost of treating all infected patients in the U.S. could exceed $300 billion, which greatly outweighs the short-term cost of the annual HCV-related burden (about $6.5 billion [Hepatology 2013;57:2164-70]). Treatment of other chronic illnesses such as HIV may incur greater costs but they are distributed over a lifetime. Ultimately, value depends on perspective; payers may balk at the price for the same cure that our patients consider invaluable. Dr. J.P. Norvell is assistant professor of medicine, Emory University, Atlanta. He has been a consultant to Gilead Sciences. Hepatic Encephalopathy (HE) EPISODES CAUSE COGNITIVE DYSFUNCTIONS. by 2014 SOME MAY BE IRREVERSIBLE Supported AASLD/EASL HE guidelines 1 Xifaxan® (rifaximin) 550 mg tablets are indicated for reduction in risk of overt hepatic encephalopathy (HE) recurrence in patients ≥ 18 years of age. Manage HE patients continuously with a Xifaxan 550 mg tablet twice daily The most common adverse reactions occurring in ≥10% of patients and at a higher incidence than placebo in the clinical study were peripheral edema (15%), nausea (14%), dizziness (13%), fatigue (12%), and ascites (11%). Important Safety Information about XIFAXAN 550 mg XIFAXAN® (rifaximin) 550 mg tablets are contraindicated in patients with a hypersensitivity to rifaximin, any of the rifamycin antimicrobial agents, or any of the components in XIFAXAN. Hypersensitivity reactions have included exfoliative dermatitis, angioneurotic edema, and anaphylaxis. Clostridium difficile-associated diarrhea (CDAD) has been reported with use of nearly all antibacterial agents, including XIFAXAN, and may range in severity from mild diarrhea to fatal colitis. Treatment with antibacterial agents alters the normal flora of the colon which may lead to overgrowth of C. difficile. If CDAD is suspected or confirmed, ongoing antibiotic use not directed against C. difficile may need to be discontinued. There is increased systemic exposure in patients with more severe hepatic dysfunction. The clinical trials were limited to patients with MELD scores < 25. Therefore, caution should be exercised when administering XIFAXAN to patients with severe hepatic impairment (Child-Pugh C). Xifaxan 550 mg is licensed by Alfa Wassermann S.p.A. to Salix Pharmaceuticals, Inc. Concomitant administration of drugs that are P-glycoprotein (P-gp) inhibitors with XIFAXAN can substantially increase the systemic exposure to XIFAXAN. Caution should be exercised when concomitant use of XIFAXAN and a P-gp inhibitor such as cyclosporine is needed. In patients with hepatic impairment, a potential additive effect of reduced metabolism and concomitant P-gp inhibitors may further increase the systemic exposure to XIFAXAN. Based on animal data, XIFAXAN may cause fetal harm. Discontinue in nursing mothers after taking into account the importance of the drug to the mother. The most common adverse reactions occurring in ≥10% of patients and at a higher incidence than placebo in the clinical study were peripheral edema (15%), nausea (14%), dizziness (13%), fatigue (12%), and ascites (11%). Please see brief summary on reverse. Web site: www.salix.com 8510 Colonnade Center Drive, Raleigh, NC 27615 Tel. 866-669-SLXP (7597) ©2015 Salix Pharmaceuticals, Inc. All rights reserved. Printed in USA. XIFH-US-0073-v1 GIHEP_19.indd 1 References: 1. Vilstrup H, Amodio P, Bajaj J, et al. Hepatic encephalopathy in chronic liver disease: 2014 practice guideline by the American Association for the Study of Liver Diseases and the European Association for the Study of the Liver. Hepatology. 2014; 60(2):715-735. 2. Xifaxan [prescribing information]. Raleigh, NC: Salix Pharmaceuticals, Inc; 2014. *Over a 6-month period in a double-blind, placebo-controlled clinical trial; P<0.0001 vs placebo.2 Prescribe. Protect. Repeat. 3/23/2015 10:28:44 AM 20 LIVER DISEASES Continued from page 18 ed adults of diferent ages and sexes, treatment histories, HCV genotypes, fbrosis scores, and interferon tolerances. For each of these patient profles, they ran simulations in which patients received either “the old standard of care” (peginterferon and ribavirin, with The following is a brief summary only. See complete Prescribing Information on www.Xifaxan550.com or request complete prescribing information by calling 1-800-508-0024. MAY 2 0 1 5 • G I & HEPATO LO G Y NEW S or without boceprevir and telaprevir) or sofosbuvir plus ledipasvir. The per-patient cost of standard care ranged from $15,000 to $71,000, depending on the patient profle; that of sofosbuvir-ledipasvir ranged from $66,000 to $154,000, said Jagpreet Chhatwal, Ph.D., of the University of Texas MD Anderson Cancer Center, Table 1: Adverse Reactions Occurring in ≥ 5% of Patients Receiving XIFAXAN and at a Higher Incidence Than Placebo Number (%) of Patients INDICATIONS AND USAGE To reduce the development of drug-resistant bacteria and maintain the effectiveness of XIFAXAN and other antibacterial drugs, XIFAXAN when used to treat infection should be used only to treat or prevent infections that are proven or strongly suspected to be caused by susceptible bacteria. When culture and susceptibility information are available, they should be considered in selecting or modifying antibacterial therapy. In the absence of such data, local epidemiology and susceptibility patterns may contribute to the empiric selection of therapy. Hepatic Encephalopathy XIFAXAN 550 mg is indicated for reduction in risk of overt hepatic encephalopathy (HE) recurrence in patients ≥ 18 years of age. In the trials of XIFAXAN for HE, 91% of the patients were using lactulose concomitantly. Differences in the treatment effect of those patients not using lactulose concomitantly could not be assessed. XIFAXAN has not been studied in patients with MELD (Model for EndStage Liver Disease) scores > 25, and only 8.6% of patients in the controlled trial had MELD scores over 19. There is increased systemic exposure in patients with more severe hepatic dysfunction. CONTRAINDICATIONS MedDRA Preferred Term XIFAXAN Tablets 550 mg TWICE DAILY N = 140 Placebo N = 159 Edema peripheral Nausea 21 (15%) 20 (14%) 13 (8%) 21 (13%) Dizziness 18 (13%) 13 (8%) Fatigue 17 (12%) 18 (11%) Ascites 16 (11%) 15 (9%) Muscle spasms 13 (9%) 11 (7%) Pruritus 13 (9%) 10 (6%) Abdominal pain 12 (9%) 13 (8%) 12 (8%) Abdominal distension 11 (8%) Anemia 11 (8%) 6 (4%) Cough 10 (7%) 11 (7%) Depression 10 (7%) 8 (5%) Insomnia 10 (7%) 11 (7%) Nasopharyngitis 10 (7%) 10 (6%) Abdominal pain upper 9 (6%) 8 (5%) Arthralgia 9 (6%) 4 (3%) Back pain 9 (6%) 10 (6%) Constipation 9 (6%) 10 (6%) WARNINGS AND PRECAUTIONS Dyspnea 9 (6%) 7 (4%) Travelers’ Diarrhea Not Caused by Escherichia coli Pyrexia Rash 9 (6%) 7 (5%) 5 (3%) 6 (4%) Hypersensitivity XIFAXAN is contraindicated in patients with a hypersensitivity to rifaximin, any of the rifamycin antimicrobial agents, or any of the components in XIFAXAN. Hypersensitivity reactions have included exfoliative dermatitis, angioneurotic edema, and anaphylaxis. XIFAXAN was not found to be effective in patients with diarrhea complicated by fever and/or blood in the stool or diarrhea due to pathogens other than Escherichia coli. Discontinue XIFAXAN if diarrhea symptoms get worse or persist more than 24-48 hours and alternative antibiotic therapy should be considered. XIFAXAN is not effective in cases of travelers’ diarrhea due to Campylobacter jejuni. The effectiveness of XIFAXAN in travelers’ diarrhea caused by Shigella spp. and Salmonella spp. has not been proven. XIFAXAN should not be used in patients where Campylobacter jejuni, Shigella spp., or Salmonella spp. may be suspected as causative pathogens. Clostridium diffcile-Associated Diarrhea Clostridium diffcile-associated diarrhea (CDAD) has been reported with use of nearly all antibacterial agents, including XIFAXAN, and may range in severity from mild diarrhea to fatal colitis. Treatment with antibacterial agents alters the normal fora of the colon which may lead to overgrowth of C. diffcile. C. diffcile produces toxins A and B which contribute to the development of CDAD. Hypertoxin producing strains of C. diffcile cause increased morbidity and mortality, as these infections can be refractory to antimicrobial therapy and may require colectomy. CDAD must be considered in all patients who present with diarrhea following antibiotic use. Careful medical history is necessary since CDAD has been reported to occur over two months after the administration of antibacterial agents. If CDAD is suspected or confrmed, ongoing antibiotic use not directed against C. diffcile may need to be discontinued. Appropriate fuid and electrolyte management, protein supplementation, antibiotic treatment of C. diffcile, and surgical evaluation should be instituted as clinically indicated. Development of Drug Resistant Bacteria Prescribing XIFAXAN for travelers’ diarrhea in the absence of a proven or strongly suspected bacterial infection or a prophylactic indication is unlikely to provide beneft to the patient and increases the risk of the development of drug-resistant bacteria. Severe (Child-Pugh C) Hepatic Impairment There is increased systemic exposure in patients with severe hepatic impairment. Animal toxicity studies did not achieve systemic exposures that were seen in patients with severe hepatic impairment. The clinical trials were limited to patients with MELD scores <25. Therefore, caution should be exercised when administering XIFAXAN to patients with severe hepatic impairment (Child-Pugh C). Concomitant Use With P-glycoprotein Inhibitors The following adverse reactions, presented by body system, have also been reported in the placebo-controlled clinical trial in greater than 2% but less than 5% of patients taking XIFAXAN 550 mg taken orally two times a day for hepatic encephalopathy. The following includes adverse events occurring at a greater incidence than placebo, regardless of causal relationship to drug exposure. Ear and Labyrinth Disorders: Vertigo Gastrointestinal Disorders: Abdominal pain lower, abdominal tenderness, dry mouth, esophageal variceal bleed, stomach discomfort General Disorders and Administration Site Conditions: Chest pain, generalized edema, infuenza like illness, pain NOS Infections and Infestations: Cellulitis, pneumonia, rhinitis, upper respiratory tract infection NOS Injury, Poisoning and Procedural Complications: Contusion, fall, procedural pain Investigations: Weight increased Metabolic and Nutritional Disorders: Anorexia, dehydration, hyperglycemia, hyperkalemia, hypoglycemia, hyponatremia Musculoskeletal, Connective Tissue, and Bone Disorders: Myalgia, pain in extremity Nervous System Disorders: Amnesia, disturbance in attention, hypoesthesia, memory impairment, tremor Psychiatric Disorders: Confusional state Respiratory, Thoracic, and Mediastinal Disorders: Epistaxis Vascular Disorders: Hypotension Postmarketing Experience The following adverse reactions have been identifed during post approval use of XIFAXAN. Because these reactions are reported voluntarily from a population of unknown size, estimates of frequency cannot be made. These reactions have been chosen for inclusion due to either their seriousness, frequency of reporting or causal connection to XIFAXAN. Infections and Infestations Cases of C. diffcile-associated colitis have been reported. General Hypersensitivity reactions, including exfoliative dermatitis, rash, angioneurotic edema (swelling of face and tongue and diffculty swallowing), urticaria, fushing, pruritus and anaphylaxis have been reported. These events occurred as early as within 15 minutes of drug administration. DRUG INTERACTIONS Effects of Rifaximin on Cytochrome P450 Enzymes ADVERSE REACTIONS In vitro studies have shown that rifaximin did not inhibit cytochrome P450 isoenzymes 1A2, 2A6, 2B6, 2C9, 2C19, 2D6, 2E1 and CYP3A4 at concentrations ranging from 2 to 200 ng/mL. Rifaximin is not expected to inhibit these enzymes in clinical use. An in vitro study has suggested that rifaximin induces CYP3A4. However, in patients with normal liver function, rifaximin at the recommended dosing regimen is not expected to induce CYP3A4. It is unknown whether rifaximin can have a signifcant effect on the pharmacokinetics of concomitant CYP3A4 substrates in patients with reduced liver function who have elevated rifaximin concentrations. Clinical Studies Experience Concomitant P-glycoprotein Inhibitors Because clinical trials are conducted under widely varying conditions, adverse reaction rates observed in the clinical trials of a drug cannot be directly compared to rates in the clinical trials of another drug and may not refect the rates observed in practice. An in vitro study suggested that rifaximin is a substrate of P-glycoprotein. Co-administration of cyclosporine, a potent P-glycoprotein inhibitor, with rifaximin resulted in 83-fold and 124-fold increases in rifaximin mean Cmax and AUC∞ in healthy subjects. The clinical signifcance of this increase in systemic exposure is unknown. Concomitant administration of drugs that are P-glycoprotein inhibitors with rifaximin can substantially increase the systemic exposure to rifaximin. Caution should be exercised when concomitant use of rifaximin and a P-glycoprotein inhibitor such as cyclosporine is needed. In patients with hepatic impairment, a potential additive effect of reduced metabolism and concomitant P-glycoprotein inhibitors may further increase the systemic exposure to rifaximin. Hepatic Encephalopathy The data described below refect exposure to XIFAXAN 550 mg in 348 patients, including 265 exposed for 6 months and 202 exposed for more than a year (mean exposure was 364 days). The safety of XIFAXAN 550 mg taken two times a day for reducing the risk of overt hepatic encephalopathy recurrence in adult patients was evaluated in a 6-month placebo-controlled clinical trial (n = 140) and in a long term follow-up study (n = 280). The population studied had a mean age of 56.26 (range: 21-82) years; approximately 20% of the patients were ≥ 65 years old, 61% were male, 86% were White, and 4% were Black. Ninety-one percent of patients in the trial were taking lactulose concomitantly. All adverse reactions that occurred at an incidence ≥ 5% and at a higher incidence in XIFAXAN 550 mg-treated subjects than in the placebo group in the 6-month trial are provided in Table 1. (These include adverse events that may be attributable to the underlying disease). USE IN SPECIFIC POPULATIONS Pregnancy Pregnancy Category C There are no adequate and well controlled studies in pregnant women. Rifaximin has been shown to be teratogenic in rats and rabbits at doses that caused maternal toxicity. XIFAXAN tablets should be used during pregnancy only if the potential beneft justifes the potential risk to the fetus. Administration of rifaximin to pregnant rats and rabbits at dose levels that caused reduced body weight gain resulted in eye malformations in both rat and rabbit fetuses. Additional malformations were observed in fetal rabbits that included cleft palate, lumbar scoliosis, brachygnathia, interventricular septal defect, and large atrium. Houston, and his associates. Compared with standard care, treating 10,000 patients with sofosbuvir-ledipasvir was projected to prevent 600 cases of decompensated cirrhosis, 310 cases of hepatocellular carcinoma (HCC), 60 liver transplantations, and 550 liver-related deaths. Compared with standard care, the in- The fetal rat malformations were observed in a study of pregnant rats administered a high dose that resulted in 16 times the therapeutic dose to diarrheic patients or 1 times the therapeutic dose to patients with hepatic encephalopathy (based upon plasma AUC comparisons). Fetal rabbit malformations were observed from pregnant rabbits administered mid and high doses that resulted in 1 or 2 times the therapeutic dose to diarrheic patients or less than 0.1 times the dose in patients with hepatic encephalopathy, based upon plasma AUC comparisons. Post-natal developmental effects were not observed in rat pups from pregnant/lactating female rats dosed during the period from gestation to Day 20 post-partum at the highest dose which resulted in approximately 16 times the human therapeutic dose for travelers’ diarrhea (based upon AUCs) or approximately 1 times the AUCs derived from therapeutic doses to patients with hepatic encephalopathy. Nursing Mothers It is not known whether rifaximin is excreted in human milk. Because many drugs are excreted in human milk and because of the potential for adverse reactions in nursing infants from XIFAXAN, a decision should be made whether to discontinue nursing or to discontinue the drug, taking into account the importance of the drug to the mother. Pediatric Use The safety and effectiveness of XIFAXAN 200 mg in pediatric patients with travelers’ diarrhea less than 12 years of age have not been established. The safety and effectiveness of XIFAXAN 550 mg for HE have not been established in patients < 18 years of age. Geriatric Use Clinical studies with rifaximin 200 mg for travelers’ diarrhea did not include suffcient numbers of patients aged 65 and over to determine whether they respond differently than younger subjects. In the controlled trial with XIFAXAN 550 mg for hepatic encephalopathy, 19.4% were 65 and over, while 2.3% were 75 and over. No overall differences in safety or effectiveness were observed between these subjects and younger subjects, and other reported clinical experience has not identifed differences in responses between the elderly and younger patients, but greater sensitivity of some older individuals cannot be ruled out. Renal Impairment The pharmacokinetics of rifaximin in patients with impaired renal function has not been studied. Hepatic Impairment Following administration of XIFAXAN 550 mg twice daily to patients with a history of hepatic encephalopathy, the systemic exposure (i.e., AUCt) of rifaximin was about 10-, 13-, and 20-fold higher in those patients with mild (Child-Pugh A), moderate (Child-Pugh B) and severe (Child-Pugh C) hepatic impairment, respectively, compared to that in healthy volunteers. No dosage adjustment is recommended because rifaximin is presumably acting locally. Nonetheless, caution should be exercised when XIFAXAN is administered to patients with severe hepatic impairment. PATIENT COUNSELING INFORMATION Persistent Diarrhea For those patients being treated for travelers’ diarrhea, discontinue XIFAXAN if diarrhea persists more than 24-48 hours or worsens. Advise the patient to seek medical care for fever and/or blood in the stool. Clostridium diffcile-Associated Diarrhea Clostridium diffcile-associated diarrhea (CDAD) has been reported with use of nearly all antibacterial agents, including XIFAXAN, and may range in severity from mild diarrhea to fatal colitis. Treatment with antibiotics alters the normal fora of the colon which may lead to C. diffcile. Patients can develop watery and bloody stools (with or without stomach cramps and fever) even as late as two or more months after having taken the last dose of the antibiotic. If diarrhea occurs after therapy or does not improve or worsens during therapy, advise patients to contact a physician as soon as possible. Administration With Food Inform patients that XIFAXAN may be taken with or without food. Antibacterial Resistance Counsel patients that antibacterial drugs including XIFAXAN should only be used to treat bacterial infections. They do not treat viral infections (e.g., the common cold). When XIFAXAN is prescribed to treat a bacterial infection, patients should be told that although it is common to feel better early in the course of therapy, the medication should be taken exactly as directed. Skipping doses or not completing the full course of therapy may (1) decrease the effectiveness of the immediate treatment and (2) increase the likelihood that bacteria will develop resistance and will not be treatable by XIFAXAN or other antibacterial drugs in the future. Severe Hepatic Impairment Patients should be informed that in patients with severe hepatic impairment (Child-Pugh C) there is an increase in systemic exposure to XIFAXAN. You are encouraged to report negative side effects of prescription drugs to the FDA. Visit http://www.fda.gov/medwatch or call 1-800-FDA-1088. To report adverse events, a product complaint, or for additional information, call: 1-800-508-0024. Manufactured for: Salix Pharmaceuticals, Inc. 8510 Colonnade Center Drive, Raleigh, NC 27615 http://www.salix.com XIFAXAN® is a trademark of Alfa Wassermann S.p.A., used under license by Salix Pharmaceuticals, Inc. Copyright © Salix Pharmaceuticals, Inc. cremental cost-efectiveness ratio of sofosbuvir-ledipasvir was $55,400 per additional quality-of-life-year (QALY) gained, which falls well within the accepted range (Ann. Intern. Med. 2015 [doi:10.7326/M14-1336]). But there was an important caveat: More patients are eligible because the novel therapies are much more easily tolerated. Compared with standard care, giving these novel HCV therapies to all eligible patients “would cost an additional $65 billion in the next 5 years,” which would not be counterbalanced by the estimated $16 billion saved by preventing cirrhosis, HCC, and transplantations. Therefore, “despite the cost-efectiveness of [novel] HCV treatments, our analysis shows that it is unafordable at the current price,” Dr. Chhatwal and his associates said. In the other study, researchers developed a discrete-event simulation model of the progression of liver disease in treatment-naive patients, categorized by whether they were infected with HCV genotype 1, 2, or 3. Several treatment regimens were considered for each genotype, and the SVR rates they were projected to attain were derived from those reported in clinical trials, said Mehdi Najafzadeh, Ph.D., of the division of pharmacoepidemiology and pharmacoeconomics, Brigham and Women’s Hospital and Harvard Medical School, Boston, and his associates. “The newly approved PEG-free regimen of sofosbuvir-ledipasvir for 12 weeks could be very cost-efective relative to usual care (costing $12,825/ QALY gained) for patients with HCV genotype 1.” This treatment proved to be the optimal strategy in the greatest number of simulations involving genotype 1. For genotype 3, sofosbuvir-ledipasvir plus ribavirin for 12 weeks cost $73,000/QALY gained, compared with usual care. This represents “relatively good value.” However, for genotype 2 the most cost-efective novel therapy, sofosbuvir-ribavirin, was $110,168/ QALY gained, which is not considered cost efective, Dr. Najafzadeh and his associates said (Ann. Intern. Med. 2015 [doi:10.7326;M14-1152]). Dr. Chhatwal’s study was supported by the National Center for Advancing Translational Sciences and the VA Health Services Research and Development Center for Innovations in Quality, Efectiveness, and Safety. Dr. Najafzadeh’s study was supported by an unrestricted grant from CVS Health to Brigham and Women’s Hospital and by a Canadian Institutes of Health Research fellowship. Both groups’ disclosures are available at www.annals.org. [email protected] Know the difference. Make a difference. a potent probiotic medical food VSL#3 provides clinically proven benefts in the dietary management of UC and an ileal pouch.Recognized by the ACG Practice Parameter Committee1 and the Cochrane Library2 as an effective tool for the management of pouchitis. VSL#3 adds billions of bacteria to the microbial barrier restoring balance and diversity in the GI tract.3 The research of the Human Microbiome Project [http://hmpdacc.org/] is investigating key links between human health and the balance of specifc microbes in the human gut. Knowing the difference makes all the difference when it comes to probiotic health. References: 1. Kornblut A, et al. Am J Gastroenterol. 2004;99(7):1371-1385. 2. Holubar SD, et al. The Cochrane Library. 2010, Issue 6. 3. Gionchetti P, et al. Gastroenterology, 2000;119(2):305-309. VSL#3 is a high potency probiotic medical food that must be used under medical supervision. www.vsl3.com Made in U.S.A. Distributed by Sigma-Tau Pharmaceuticals, Inc. Gaithersburg, M.D. ©2014 Sigma-Tau Pharmaceuticals. All rights reserved V1166 03/15 GIHEP_21.indd 1 3/24/2015 1:47:56 PM 22 LIVER DISEASES MAY 2 0 1 5 • G I & HEPATO LO G Y NEW S Obeticholic acid for NASH improves markers, fbrosis BY KARI OAKES Frontline Medical News F or patients with nonalcoholic steatohepatitis (NASH), a bile acid derivative that acts on a nuclear receptor reduced liver fat and fbrosis, but patients taking the drug also had worsening in serum lipid values and increased insulin resistance. The lipophilic bile acid obeticholic acid showed promise in the FLINT trial (Farnesoid X Receptor Ligand Obeticholic Acid in NASH Treatment) for NASH patients whose liver disease improved but did not resolve. Dr. Brent Neuschwander-Tetri of Saint Louis University, and coinvestigators in the National Institute of Diabetes and Digestive and Kidney Diseases’ NASH Clinical Research Network, conducted the multicenter, randomized, placebo-controlled study. The fndings were published in the Lancet. Obeticholic acid, a farnesoid X nuclear receptor agonist, works at a site whose activation promotes increased insulin sensitivity and decreased serum triglycerides. Serum lipids may also be improved by increased peripheral clearance of VLDL, increased reverse cholesterol transport, and reduced lipid synthesis in the liver. Currently, the only other treatments for NASH, aside from diet and lifestyle modifcations, are thiazolidinediones and vitamin E. Long-term safety and efcacy of these medications are unknown, especially in NASH patients with diabetes (Lancet 2015;385:956-65 [doi:10.1016/S0140-6736(14)61933-4]). Study participants were adults with biopsy-con- VITALS Key clinical point: The farnesoid X nuclear receptor agonist obeticholic acid improved clinical markers of nonalcoholic steatohepatitis (NASH) but increased serum cholesterol. Major fnding: Of patients assigned to receive liver biopsies, 50/110 (45%) receiving obeticholic acid showed improvement in liver histology compared with 23/109 (21%) in the placebo group (P = .0002). Data source: The Farnesoid X Receptor Ligand Obeticholic Acid in NASH Treatment (FLINT) study, a 72-week multicenter, double-blind, placebo-controlled trial of obeticholic acid for treatment of 283 patients with noncirrhotic NASH. Disclosures: Dr. Neuschwander-Tetri disclosed ties with Genentech/Roche, Nimbus Discovery, Boehringer Ingelheim, and Bristol-Myers Squibb. Several coinvestigators disclosed ties with various companies, including Intercept Pharmaceuticals, which provided partial funding for the trial under a Collaborative Research and Development Agreement with the National Institute of Diabetes and Digestive and Kidney Diseases. frmed NASH or borderline NASH with histologic steatosis, ballooning, and lobular infammation, but without cirrhosis. The study excluded heavy consumers of alcohol. Baseline and fnal assessments included liver biopsy and demographic and anthropometric information, as well as metabolic and lipid markers and liver enzymes. FLINT’s primary outcome measure was improved liver histology, defned as a decrease of two or more points on a nonalcoholic fatty liver disease Correction In the January 2015 issue (page 1, “Screen baby boomers, treat all hepatitis C”), Dr. Zobair Younossi’s conficts of interest were noted incorrectly. He is a consultant to AbbVie, BMS, Gilead, GSK, and Intercept. None of the other study authors had any relevant conficts of interest. The study was not supported by any pharmaceutical company. (NAFLD) pathology scoring system, without a worsening of liver fbrosis. Resolution of NASH was a secondary outcome, as were changes in liver enzymes, body measurements, and homeostasis model of assessment of insulin resistance (HOMA-IR) levels. The study’s Data Safety Monitoring Board recommended stopping biopsies after about half the patients had received biopsies and the primary histologic outcome measure was met, in order to avoid unnecessary patient risk. An intention-to-treat analysis found that 50 (45%) of 110 patients receiving obeticholic acid had improved liver histology, compared with 23 (21%) of 109 patients receiving placebo (relative risk 1.9, 95% CI: 1.3-2.8, P = .0002). This diference did not change with prespecifed subgroup analyses. Serum AST and ALT measures decreased signifcantly for the treatment group. The medication was generally well tolerated, though pruritis developed in 33 (23%) of 141 patients in the intervention group and 9 (6%) of the placebo group. Total serum cholesterol and LDL cholesterol, however, increased for the obeticholic acid group, while HDL cholesterol decreased. Insulin resistance as measured by HOMA-IR increased slightly for the treatment group, an unexpected efect. Study authors noted that this class of medication’s efect on cholesterol transport is complex. “Future studies of farnesoid X nuclear receptor agonists,” they noted, “will need to address the consequences of these changes on cardiovascular outcomes.” [email protected] Quick Quiz Q1: As compared to patients who acquire C. difcile infection in the hospital setting, individuals with community-associated C. difcile infection are more likely to have which of the following characteristics: A. Male sex B. Older age C. On PPI therapy D. Cancer patients E. Recent antibiotic exposure Q2: A 29-year-old man with a history of moderate ulcerative colitis diagnosed at the age of 22 has been in remission while on 6-mercaptopurine and sulfasalazine for approximately 3 years. He was started on sulfasalazine at diagnosis with improvement of his symptoms. At the age of 26 he required multiple courses of steroids for UC fares. As a result, 6-mer- captopurine was added at a dose of 1.5 mg/kg. Three months after initiation of 6-mercaptopurine he was in remission with one formed bowel movement daily. He got married about 2 years ago but he and his wife have been unable to have children despite unprotected intercourse. As his gastroenterologist, what would you suggest? A. Stop the 6-mercaptopurine and the sulfasalazine. B. Continue the 6-mercaptopurine and the sulfasalazine. C. Continue the 6-mercaptopurine. Switch the sulfasalazine to Asacol® (mesalamine). D. Continue sulfasalazine. Switch the 6-mercaptopurine to infiximab. E. Ask him to consult an in vitro fertilization specialist. The answers are on page 47. Now, less is an option. l Introducing GaviLyte™-H • Compare to HalfLytely®* • Now available as a generic • 2 liters and 1 Bisacodyl tablet GaviLyte-H Now, patients, prescribers and pharmacists have a choice – with GaviLyte-H. This 2-liter volume PEG-3350 with bisacodyl tablet provides an alternative pre-colonoscopy prep and is now available as a value-branded generic. GaviLyte-H is part of our complete family of generic PEG-3350 products, and is just one more example of how GAVIS Pharmaceuticals is listening – and delivering – what patients, physicians and pharmacists want: a choice. Learn more at gavilyte.com. *HalfLytely is a registered trademark of Braintree Laboratories, Inc. GIHEP_23.indd 1 4/14/2015 4:46:44 PM 24 GI ONCOLOGY MAY 2 0 1 5 • G I & HEPATO LO G Y NEW S BUN and Khorana score predict pancreatic ca death BY JENNIFER KELLY SHEPPHIRD Frontline Medical News U sing parameters routinely collected in patients with pancreatic cancer, the Khorana score and the blood urea nitrogen (BUN) level were signifcantly associated with early mortality in patients with pancreatic cancer who underwent surgical resection, according to a report published in the journal Cancer. VITALS Key clinical point: High Khorana score and elevated blood urea nitrogen predicted early mortality in patients after surgical resection for pancreatic cancer. Major fnding: For patients with elevated blood urea nitrogen, the early mortality hazard ratio was 4.34 (95% CI, 1.84-10.25), and for high-risk Khorana scores, this was 2.32 (1.04-5.13). Data source: The retrospective cohort study used medical chart data from 334 consecutive patients who underwent surgical resection at the Cleveland Clinic from 2006 to 2013. Disclosures: Dr. Sohal reported having no disclosures. Dr. Khorana has received fees from several industry sources for work outside of the current study. Dr. Davendra P.S. Sohal, an oncologist at Cleveland Clinic, and his colleagues stated that by identifying patients with resectable pancreatic adenocarcinoma who are at high risk of early mortality, the parameters “may be used to stratify patients, and ultimately may be used to select high-risk patients for more aggressive therapies in prospective studies” (Cancer 2015 [doi:10.1002/ cncr.29298]). Multivariate analysis showed the risk for early mortality (before 6 months) increased with highrisk Khorana score (hazard ratio, 2.32; 95% confdence interval, 1.04-5.13; P = .039) and elevated blood urea nitrogen (HR, 4.34; 95% CI, 1.84-10.25; P < .001). The authors noted that other key variables, such as TNM classifcation of malignant tumor staging, were not associated with early mortality. The study evaluated 334 patients, median age 67 years, who underwent surgical resection of pancreatic adenocarcinoma during 2006-2013 at the Cleveland Clinic. With a median follow-up time of 39.4 months, there were 205 deaths (61%), and median overall survival was 21.3 months. Within 30 days after surgery, 3 (0.9%) deaths occurred, and within 6 months of surgery, 29 (8.7%) deaths occurred. Most tumors were located in the head of the pancreas (73%); most pathologic stages were T3 (67%) and N1 (63%); median Khorana score was 2; 47% of patients had a score ≥ 3; 59% had comorbidities. Some of the patients received preoperative anticancer therapy, making the study population heterogeneous in that respect. The Khorana score, a measure of venous thromboembolism risk, combines fve items: cancer site, platelet count > 350/nL, white blood cell count > 11/nL, hemoglobin <100 g/L, and body mass index (BMI) ≥ 35 kg/m2; Khorana scores of 3 or greater indicate high risk. A novel fnding in patients with pancreatic cancer, elevated BUN levels have been previously linked to poorer prognosis for patients with non– small cell lung cancer and advanced malignancies Variants near pathogenesis genes Colon cancer from page 1 VITALS Key clinical point: The protective effect of aspirin and NSAIDs against colon cancer was linked to three genetic variants on chromosomes 12 and 15. Major fnding: The prevalence of colon cancer was 28% among regular users of aspirin/NSAIDs, compared with 38% among nonusers, for an odds ratio of 0.69. Data source: A genome-wide analysis of gene and environment interactions using data from 17,187 participants in 10 case-control studies conducted over a 40-year period in Australia, Canada, Germany, and the United States. Disclosures: The National Cancer Institute and the National Institutes of Health supported the study. Dr. Nan reported having no fnancial disclosures. One of her associates reported holding a patent for aspirin as a colorectal chemopreventive agent and two others reported ties to Arctic Dx, Bayer Healthcare, Pfzer, and Pozen. study, the investigators pooled data from 10 observational studies conducted between 1976 and 2003 in Australia, Canada, Germany, and the United States, which enrolled 8,634 colon cancer case subjects and 8,553 control subjects matched for age, sex, and race/ethnicity. Regular use was defned for the pooled studies and all of the study subjects were of European descent. Compared with nonuse of aspirin, NSAIDs, or both, regular use was associated with a lower risk of colorectal cancer: The overall prevalence of the disease was 28% among regular users, compared with 38% among nonusers, for an odds ratio of 0.69. The regular use of aspirin alone also was associated with a lower risk of colorectal cancer: The prevalence was 24% among regular users and 31% among nonusers, for an odds ratio of 0.71. This protective efect, however, and thus an NSAID user’s risk who were receiving palliative care. Elevated BUN levels may indicate subclinical renal dysfunction or other comorbidities that infuence survival. Univariate analysis in the current study did not fnd an association between early mortality and BMI, which may be due to the timing of the mea- The parameters ‘may be used to stratify patients, and ultimately may be used to select highrisk patients for more aggressive therapies in prospective studies.’ surement. Patients may experience cancer-induced weight loss that renders BMI measures falsely low. The association between BMI and decreased survival after pancreatic cancer diagnosis was found previously to be strongest when BMI was taken 1820 years prior to diagnosis. The authors note that although perioperative mortality has improved considerably in recent years, there exists a subgroup of patients who experience early recurrence. “These patients may not beneft from the current standard of care but to our knowledge, little is known regarding how best to identify such patients at high risk of early mortality,” wrote Dr. Sohal and his associates. The current study identifes a simple set of baseline parameters that may allow for “easy targeting of high-risk patients for specifc interventions aimed at improving clinical outcomes.” for colorectal cancer, varied by whether patients carried the genetic variants and how many copies of the risk alleles they carried, Dr. Nan and her associates said ( JAMA 2015;313:1133-42). All three genetic variants are located near genes known to be involved in the pathogenesis of colon cancer, including genes that regulate [email protected] the production of proinfammatory prostaglandins and interleukins, particularly within the gut. This proximity supports the idea that aspirin and NSAIDs exert their gut-protective efects through these infammatory mediators, the investigators said. [email protected] PERSPECTIVE Aspirin/NSAIDs to prevent colon cancer T hese fndings add complexity to, but do not answer, the longstanding clinical question of whether healthy adults should take aspirin regularly to reduce their risk of colon cancer. In the not-too-distant future, it will become afordable and practical to conduct genetic testing routinely in healthy people. At that time, primary care clinicians will need to understand genetic risks and to have informed, clear, literacy-adjusted, culturally competent discussions with their patients about how to use this information. Dr. Richard C. Wender is with the American Cancer Society, Atlanta, and the department of family and community medicine at Thomas Jeferson University, Philadelphia. He reported having no fnancial disclosures. Dr. Wender made these remarks in an editorial accompanying Dr. Nan’s report (JAMA 2015;313:1111-2). Albert Einstein used with permission of the HUJ/GreenLight. INDICATION HARVONI is indicated for the treatment of chronic hepatitis C (CHC) genotype 1 infection in adults. Please see Brief Summary of full Prescribing Information adjacent to this ad. GIHEP_25.indd 1 4/14/2015 4:51:18 PM HARVONI is the only HCV treatment offering an 8-week course of therapy1 % SVR12 among treatment-naïve HCV GT 1 subjects without cirrhosis who had baseline HCV RNA <6 million IU/mL1 100 90 Percent (%) Subjects 80 97% 70 60 50 40 30 20 10 0 n=119/123 HARVONI 8 weeks ION-3 • Overall SVR12 was 94% (n=202/215) in subjects receiving HARVONI for 8 weeks1,a • In treatment-naïve subjects taking HARVONI for 12 weeks, 96% (n=208/216) achieved SVR12 in the ION-3 trial and 99% (n=210/213) achieved SVR12 in the ION-1 trial1,a • The recommended treatment duration for treatment-naïve patients is 12 weeks1 • HARVONI for 8 weeks can be considered in treatment-naïve patients without cirrhosis who have pre-treatment HCV RNA <6 million IU/mL1 Study Designs ION-11: a randomized, open-label trial evaluating HARVONI with or without ribavirin (RBV) in GT 1 treatment-naïve subjects (N=865) with or without cirrhosis. Subjects were randomized in a 1:1:1:1 ratio to receive HARVONI for 12 weeks, HARVONI + RBV for 12 weeks, HARVONI for 24 weeks, or HARVONI + RBV for 24 weeks, and stratified by presence or absence of cirrhosis and HCV genotype (1a vs 1b). ION-31: a randomized, open-label trial in GT 1 treatment-naïve subjects (N=647) without cirrhosis. Subjects were randomized in a 1:1:1 ratio to receive HARVONI for 8 weeks, HARVONI + RBV for 8 weeks, or HARVONI for 12 weeks, and stratified by HCV genotype (1a vs 1b). a SVR12 was the primary endpoint and was defined as HCV RNA <25 IU/mL at 12 weeks after the end of treatment.1 Achieving SVR is considered a virologic cure.2 RBV was not shown to increase the response rates observed with HARVONI in ION-1 or ION-3. Therefore, the HARVONI + RBV arms are not presented.1 IMPORTANT SAFETY INFORMATION WARNINGS AND PRECAUTIONS • Risk of Serious Symptomatic Bradycardia when Coadministered with Amiodarone: Amiodarone is not recommended for use with HARVONI due to the risk of symptomatic bradycardia, particularly in patients also taking beta blockers or with underlying cardiac comorbidities and/or with advanced liver disease. In patients without alternative, viable treatment options, cardiac monitoring is recommended. Patients should seek immediate medical evaluation if they develop signs or symptoms of bradycardia. • Risk of Reduced Therapeutic Effect of HARVONI Due to P-gp Inducers: Rifampin and St. John’s wort are not recommended for use with HARVONI as they may significantly decrease ledipasvir and sofosbuvir plasma concentrations. • Related Products Not Recommended: HARVONI is not recommended for use with other products containing sofosbuvir (SOVALDI®). GIHEP_26&27.indd 2 4/14/2015 4:55:53 PM HARVONI is the only once-daily single-tablet regimen for HCV GT 1 patients1 Recommended treatment duration1 1 HARVONI TABLET ONCE DAILY WITH OR WITHOUT FOOD Can be considered in treatmentnaïve patients without cirrhosis who have pre-treatment HCV RNA <6 million IU/mL 8 weeks Treatment-naïve patients with or without cirrhosis Treatment-experienced patientsb without cirrhosis 12 weeks 12 weeks Treatment-experienced patientsb with cirrhosis 24 weeks Treatment-experienced patients who failed treatment with either peginterferon (Peg-IFN) alfa + ribavirin (RBV) or an HCV protease inhibitor + Peg-IFN + RBV.1 b • HARVONI is interferon- and RBV-free for GT 1 treatment-naïve and treatment-experienced patients with or without cirrhosis, regardless of GT 1a or 1b subtype1 • Each HARVONI tablet contains 90 mg of ledipasvir and 400 mg of sofosbuvir1 • Relapse rates are affected by baseline host and viral factors and differ between treatment durations for certain subgroups1 • No dose adjustments are required based on advanced age, mild or moderate renal impairment, or mild, moderate, or severe hepatic impairment. The safety and efficacy of HARVONI have not been established in patients with decompensated cirrhosis1 • No dose recommendations can be given for patients with severe renal impairment (estimated glomerular filtration rate [eGFR] <30 mL/min/1.73m2) or with end stage renal disease (ESRD) due to higher exposures (up to 20-fold) of the predominant sofosbuvir metabolite1 IMPORTANT SAFETY INFORMATION ADVERSE REACTIONS Most common (≥10%, all grades) adverse reactions were fatigue and headache. DRUG INTERACTIONS • In addition to rifampin and St. John’s wort, coadministration of HARVONI is also not recommended with carbamazepine, oxcarbazepine, phenobarbital, phenytoin, rifabutin, rifapentine, and tipranavir/ritonavir. Such coadministration is expected to decrease the concentration of ledipasvir and sofosbuvir, reducing the therapeutic effect of HARVONI. • Coadministration of HARVONI is not recommended with simeprevir due to increased concentrations of ledipasvir and simeprevir. Coadministration is also not recommended with rosuvastatin or co-formulated elvitegravir/cobicistat/emtricitabine/tenofovir disoproxil fumarate due to increased concentrations of rosuvastatin and tenofovir, respectively. Consult the full Prescribing Information for HARVONI for more information on potentially significant drug interactions, including clinical comments. Please see Brief Summary of full Prescribing Information on the following pages. Visit harvoni.com/hcp GIHEP_26&27.indd 3 4/14/2015 4:56:31 PM HARVONI® (ledipasvir 90 mg and sofosbuvir 400 mg) tablets, for oral use Brief Summary of full Prescribing Information. See full Prescribing Information. Rx Only. INDICATIONS AND USAGE: HARVONI is indicated for the treatment of chronic hepatitis C (CHC) genotype 1 infection in adults. CONTRAINDICATIONS: None WARNINGS AND PRECAUTIONS: Serious Symptomatic Bradycardia When Coadministered with Amiodarone: Postmarketing cases of symptomatic bradycardia, as well as fatal cardiac arrest and cases requiring pacemaker intervention, have been reported when amiodarone is coadministered with HARVONI. Bradycardia has generally occurred within hours to days, but cases have been observed up to 2 weeks after initiating HCV treatment. Patients also taking beta blockers, or those with underlying cardiac comorbidities and/or advanced liver disease may be at increased risk for symptomatic bradycardia with coadministration of amiodarone. Bradycardia generally resolved after discontinuation of HCV treatment. The mechanism for this effect is unknown. Coadministration of amiodarone with HARVONI is not recommended. For patients taking amiodarone who will be coadministered HARVONI and patients taking HARVONI who need to start amiodarone, who have no other alternative, viable treatment options; and due to amiodarone’s long half-life for patients discontinuing amiodarone just prior to starting HARVONI: Counsel patients about the risk of serious symptomatic bradycardia; and cardiac monitoring in an in-patient setting for the frst 48 hours of coadministration is recommended, after which outpatient or self-monitoring of the heart rate should occur on a daily basis through at least the frst 2 weeks of treatment. Patients who develop signs or symptoms of bradycardia should seek medical evaluation immediately. Symptoms may include near-fainting or fainting, dizziness or lightheadedness, malaise, weakness, excessive tiredness, shortness of breath, chest pains, confusion or memory problems. Risk of Reduced Therapeutic Effect Due to P-gp Inducers: Concomitant use may signifcantly decrease ledipasvir and sofosbuvir concentrations and may lead to a reduced HARVONI effect. Use of HARVONI with P-gp inducers (e.g., rifampin or St. John’s wort) is not recommended. Related Products Not Recommended: Use of HARVONI with products containing sofosbuvir (SOVALDI®) is not recommended. ADVERSE REACTIONS: The safety assessment of HARVONI was based on pooled data from three Phase 3 clinical trials in subjects with genotype 1 CHC with compensated liver disease (with and without cirrhosis) who received HARVONI for 8 (N=215), 12 (N=539) and 24 (N=326) weeks. Adverse events led to permanent treatment discontinuation in 0%, <1% and 1% of subjects receiving HARVONI for 8, 12 and 24 weeks, respectively. Adverse Reactions (adverse events assessed as causally related by the investigator): The most common adverse reactions (≥10%; all grades) were fatigue and headache. Adverse reactions (all grades; majority Grade 1) observed in ≥5% of subjects by treatment duration were: GIHEP_28.indd 1 • HARVONI for 8 weeks: fatigue (16%); headache (11%); nausea (6%); diarrhea (4%); and insomnia (3%) • HARVONI for 12 weeks: fatigue (13%); headache (14%); nausea (7%); diarrhea (3%); and insomnia (5%) • HARVONI for 24 weeks: fatigue (18%); headache (17%); nausea (9%); diarrhea (7%); and insomnia (6%) Direct comparison across trials should not be made due to differing trial designs. Laboratory Abnormalities: Bilirubin Elevations: Bilirubin elevations of greater than 1.5x ULN were observed in 3%, <1% and 2% of subjects treated with HARVONI for 8, 12 and 24 weeks, respectively. Lipase Elevations: Transient, asymptomatic lipase elevations of greater than 3x ULN were observed in <1%, 2% and 3% of subjects treated with HARVONI for 8, 12 and 24 weeks, respectively. Creatine Kinase: Creatine kinase was not assessed in Phase 3 trials of HARVONI. Isolated, asymptomatic creatine kinase elevations (Grade 3 or 4) have been previously reported in subjects treated with sofosbuvir in combination with ribavirin or peginterferon/ribavirin in other clinical trials. Postmarketing Experience Cardiac Disorders: Serious symptomatic bradycardia has been reported in patients taking amiodarone who initiate treatment with HARVONI during post approval use of HARVONI. Because postmarketing reactions are reported voluntarily from a population of uncertain size, it is not always possible to reliably estimate their frequency or establish a causal relationship to drug exposure. DRUG INTERACTIONS: Ledipasvir is an inhibitor of the drug transporters P-gp and breast cancer resistance protein (BCRP) and may increase intestinal absorption of coadministered substrates for these transporters. Ledipasvir and sofosbuvir are substrates of P-gp and BCRP while the inactive sofosbuvir metabolite GS-331007 is not. P-gp inducers (e.g. rifampin or St. John’s wort) may decrease ledipasvir and sofosbuvir concentrations leading to reduced HARVONI effect; use of HARVONI with P-gp inducers is not recommended. Established and Potentially Signifcant Drug Interactions: The drug interactions described are based on studies conducted in healthy adults with either HARVONI, the components of HARVONI as individual agents, or are predicted drug interactions that may occur with HARVONI. This list includes potentially signifcant interactions but is not all inclusive. An alteration in dose or regimen may be recommended for the following drugs when coadministered with HARVONI: • Acid Reducing Agents: Ledipasvir solubility decreases as pH increases. Drugs that increase gastric pH are expected to decrease ledipasvir concentration. • Antacids: Separate HARVONI and antacid administration by 4 hours. • H2-receptor antagonists: Doses comparable to famotidine 40 mg twice daily or lower may be administered simultaneously with or 12 hours apart from HARVONI. • Proton-pump inhibitors: Doses comparable to omeprazole 20 mg or lower can be administered simultaneously with HARVONI under fasted conditions. 4/14/2015 5:00:10 PM Brief Summary (cont.) USE IN SPECIFIC POPULATIONS: • Antiarrhythmics (amiodarone; digoxin) Amiodarone: Coadministration of amiodarone with HARVONI may result in serious symptomatic bradycardia and is not recommended. Mechanism of effect is unknown. If coadministration is required, cardiac monitoring is recommended. Digoxin: Increased digoxin concentration. Monitor digoxin therapeutic concentration during coadministration with HARVONI. Pregnancy: HARVONI is Pregnancy Category B; there are no adequate and well-controlled studies in pregnant women. HARVONI should be used during pregnancy only if the potential beneft justifes the potential risk to the fetus. • Anticonvulsants (carbamazepine; phenytoin; phenobarbital; oxcarbazepine): Decreased ledipasvir and sofosbuvir concentrations leading to reduced HARVONI effect. Coadministration is not recommended. • Antimycobacterials (rifabutin; rifampin; rifapentine): Decreased ledipasvir and sofosbuvir concentrations leading to reduced HARVONI effect. Coadministration is not recommended. • HIV Antiretrovirals • Regimens containing tenofovir disoproxil fumarate (DF) and an HIV protease inhibitor/ritonavir (emtricitabine/tenofovir DF plus atazanavir/ritonavir, darunavir/ritonavir or lopinavir/ ritonavir): The safety of increased tenofovir concentrations has not been established. Consider alternative HCV or antiretroviral therapy. If coadministration is necessary, monitor for tenofovirassociated adverse reactions. Refer to VIREAD or TRUVADA prescribing information for renal monitoring recommendations. • Efavirenz/emtricitabine/tenofovir DF: Monitor for tenofovirassociated adverse reactions. Refer to VIREAD, TRUVADA or ATRIPLA prescribing information for renal monitoring recommendations. • Elvitegravir/cobicistat/emtricitabine/tenofovir DF: The safety of increased tenofovir concentrations has not been established. Coadministration is not recommended. • Tipranavir/ritonavir: Decreased ledipasvir and sofosbuvir concentrations leading to reduced HARVONI effect. Coadministration is not recommended. Nursing Mothers: Studies in rats have demonstrated that ledipasvir and GS-331007 are secreted in milk but had no effect on nursing pups. It is not known if HARVONI and its metabolites are secreted in human breast milk. The developmental and health benefts of breastfeeding should be considered along with the mother’s clinical need for HARVONI and any potential adverse effects on the nursing child from the drug or from the underlying maternal condition. Pediatric Use: Safety and effectiveness of HARVONI have not been established in pediatric patients. Geriatric Use: Clinical trials of HARVONI included 117 subjects aged 65 and over. No overall differences in safety or effectiveness were observed between these subjects and younger subjects, and other reported clinical experience has not identifed differences in responses between the elderly and younger patients, but greater sensitivity of some older individuals cannot be ruled out. No dosage adjustment of HARVONI is warranted in geriatric patients. Renal Impairment: No dosage adjustment of HARVONI is required for patients with mild or moderate renal impairment. The safety and effcacy of HARVONI have not been established in patients with severe renal impairment (eGFR <30 mL/min/1.73m2) or end stage renal disease (ESRD) requiring hemodialysis. No dosage recommendation can be given for patients with severe renal impairment or ESRD. Hepatic Impairment: No dosage adjustment of HARVONI is required for patients with mild, moderate or severe hepatic impairment (Child-Pugh Class A, B or C). Safety and effcacy of HARVONI have not been established in patients with decompensated cirrhosis. • HCV Products (simeprevir): Increased ledipasvir and simeprevir concentrations. Coadministration is not recommended. • Herbal Supplements (St. John’s wort): Decreased ledipasvir and sofosbuvir concentrations. Coadministration is not recommended. • HMG-CoA Reductase Inhibitors (rosuvastatin): Signifcant increase in rosuvastatin concentrations and risk of rosuvastatin associated myopathy, including rhabdomyolysis. Coadministration is not recommended. Drugs without Clinically Signifcant Interactions with HARVONI: Based on drug interaction studies conducted with HARVONI or its components, no clinically signifcant drug interactions have been observed or are expected when used with the following drugs individually: abacavir, atazanavir/ritonavir, cyclosporine, darunavir/ritonavir, efavirenz, emtricitabine, lamivudine, methadone, oral contraceptives, pravastatin, raltegravir, rilpivirine, tacrolimus, tenofovir DF or verapamil. Consult the full Prescribing Information prior to and during treatment with HARVONI for potential drug interactions; this list is not all inclusive. GIHEP_29.indd 1 References: 1. HARVONI US full Prescribing Information. Gilead Sciences, Inc. Foster City, CA. March 2015. 2. US Department of Health and Human Services, Center for Drug Evaluation and Research. Draft Guidance for Industry. Chronic Hepatitis C Virus Infection: Developing Direct-Acting Antiviral Drugs for Treatment. October 2013. HARVONI, the HARVONI logo, SOVALDI, TRUVADA, VIREAD, GILEAD and the GILEAD logo are trademarks of Gilead Sciences, Inc., or its related companies. ATRIPLA is a trademark of Bristol-Myers Squibb & Gilead Sciences, LLC. ©2015 Gilead Sciences, Inc. All rights reserved. HVNP0241 04/15 4/14/2015 5:02:04 PM 30 IBD AND INTESTINAL DISORDERS MAY 2 0 1 5 • G I & HEPATO LO G Y NEW S Stem cells may relieve Crohn’s fstula BY DOUG BRUNK Frontline Medical News T hree-quarters of Crohn’s fstula patients who were treated with one or two doses of autologous mesenchymal stem cells derived from adipose tissue achieved complete closure at 2 years of follow-up, a retrospective analysis showed. “Crohn’s fstula is one of the most distressing diseases because it decreases patient’s quality of life and frequently recurs,” South Korean researchers led by Dr. Yong Beom Cho wrote in a study published online March 31, 2015, in Stem Cells Translational Medicine. “It has been reported to occur in 13%-38% of patients with Crohn’s disease and a proctectomy is required in 10%-18% of Crohn’s patients over the course of the disease.” To date, they continued, treatment with antibiotics and biological agents remain unsatisfactory “because they fail to achieve complete closure, lower recurrence, and limit adverse efects.” Over the past several years, researchers have been evaluating the efcacy of stem cell therapy for treating Crohn’s fstula, including those derived from bone marrow and adipose tissue. An earlier phase II trial conducted by Dr. Cho of the de- partment of surgery at Samsung Medical Center, Seoul, South Korea, and associates found that using mesenchymal stem cells derived from adipose tissue (ASCs) resulted in favorable efcacy and complete healing in 82% of 43 patients at 1 year (Stem Cells Trans. Med. 2013;31:2575-81). The purpose of the current trial was to evaluate the outcome of this approach by following the patients for an additional year. For the current phase II trial, the researchers followed 41 of the 43 patients from the initial trial, which took place at fve hospitals in South Korea from January 2010 to August 2012 and involved one or two injections of ASCs into the tract of fstulae associated with Crohn’s disease (Stem Cells Trans. Med. 2015 March 31 [doi:10.5966/ sctm.2014-0199]). At baseline the mean age of patients was 26 years, 68% were male, the mean fstula length was 4.6 cm, and the average duration of Crohn’s disease was 58 months. Modifed intention-to-treat (mITT) and modifed per protocol (mPP) analysis were used to assess efcacy. Patients who received other surgical procedures or operations involving the injection site were excluded from the mPP analysis, while the mITT analysis included patients who received ASC treat- Whose metabolism is it? Microbiome from page 1 of these communities, however, has changed over the last 30 years, diverging along a path that mirrors global spikes in obesity, diabetes, and allergic and infammatory disorders. “We have seen dramatic increases worldwide in these disorders,” Dr. Ratner said. “We’ve also seen decreased diversity of the microbiome, with a progressive change in density from Bacteroidetes to Firmicutes. These are associations – not causations – but I think the time has come to ask ‘What are we doing to change these bacteria?’ ” The use of antibiotics is the frst place suspicion falls – and it’s no wonder, since the epidemiologic changes Dr. Ratner described began to appear shortly after World War II. Antibiotics could exert their fora-changing efects in a couple of ways, he noted. They directly alter the composition of communities in the person who consumes the drug, even if just in the short term. There is some evidence that early-life antibiotics, though changing the microbiome only temporarily, can change fat metabolism for the entire lifespan (Cell 2014;158:705-21). The association between an altered gut microbiome and long-term health is unproven. But a picture does seem to emerge when viewed in light of the exponential increases in obesity and its attendant rise in diabetes. The Type 1 Diabetes Prediction and Prevention Project (DIPP) is an efort to predict and search for means to delay or prevent type 1 diabetes. Launched in 1994, it’s following a cohort of children who had genetic risk factors for type 1 diabetes. Data have consistently shown that those who develop the disease have signifcantly lower diversity in their gut fora, Dr. Ratner said. Certain species of Bacteroides increased the risk of autoimmunity by up to 20 times. ment and had efcacy data at month 24. At 24 months, complete fstula healing was observed in 81% of patients in the mPP analysis and 75% of patients in the mITT analysis. Furthermore, 83% of patients who showed complete closure at week 8 after ASC injection still showed complete closure at 24 months. No adverse events related to the administration of ASCs were observed. “ASCs represent a novel therapeutic option for Crohn’s fstulae with a high risk of recurrence, showing durable efcacy with low recurrence, even in cases in which healing cannot be achieved with biologics or in which conventional surgical procedures cannot be performed,” the researchers concluded. “Such refractory patients should be referred to tertiary centers where optimal therapy, including stem cell implants, can be ofered.” The work was supported by the National Institutes of Health Clinical Trials. Two of the study authors are employees of Anterogen Co. The remaining researchers reported having no relevant fnancial conficts. York University show for the frst time that a specifc bacterium, Ralstonia, can cause diabetes, and removing it cures the disease. The bacterium is a gram-negative pathogen that contaminates drinking water. Mice engineered for prediabetes gained much more weight when they consumed live Ralstonia than when they got a heat-inactivated version. They also developed insulin resistance and hyperglycemia with the live version. But when the same mice were given a Ralstonia antibody, they lost weight and their glycemic profle normalized. “This is the frst direct evidence we have of causality,” Dr. Ratner said. Mice engineered as prediabetic gained much more weight when they consumed live Ralstonia. Benefcial Firmicutes increased in mice that underwent vertical sleeve gastrectomy. DR. BLASER DR. SEELEY “It does now appear that our microbes are actually controlling our metabolism,” he said. “Some of these species liberate lipopolysaccharides, which function as endotoxins. These cross the mucosal barrier in the intestine, enter the interstitial space, and set up an infammation that impacts the liver and adipocytes, potentially decreasing insulin sensitivity.” Unpublished data from the laboratory of Dr. Martin J. Blaser at New Strong evidence of causation is also emerging in the surgical realm. Rouxen-Y gastric bypass seems to change the microbiome in a way that facilitates weight loss, beyond caloric intake. Randy Seeley, Ph.D., of the University of Michigan, Ann Arbor, theorizes that the physical manipulation of the gut induces what he calls “enteroplasticity” – a fuid adaptation of both the gut’s structure and its bacterial communities to the altered physical [email protected] On Twitter @dougbrunk and chemical environment. “There’s more going on during postsurgical weight loss than just food restriction and malabsorption,” Dr. Seeley said in an interview. “It’s logical to think that when you do this kind of surgery, the microbes in the intestine will change.” Roseburia intestinalis is a Firmicute that typically increases after bariatric surgery. It’s also defcient in people who have diabetes. Dr. Seeley coauthored an article showing that Roseburia and other benefcial Firmicutes increased signifcantly in mice that underwent vertical sleeve gastrectomy (Nature 2014;509:183-8). These mice lost weight after surgery, as would be expected, but then showed a preference for the high-protein and carbohydrate-rich foods that Firmicutes need. Their microbiome also showed decreases in fat-loving Bacteroides species. But weight loss and microbiome improvement happened only in mice that had a normal bile acid–signaling system. Immediately after surgery, mice engineered to lack bile acid receptors did eat less and lose weight. But a week later, their appetites came back full force, and they actually seemed driven to eat fat. They returned to their presurgical weight and their microbiome didn’t show the same improvement as their cousins with normal signaling pathways. Dr. Seeley disclosed receiving fnancial support from Johnson & Johnson, Novo Nordisk, and Eisai. [email protected] IBD AND INTESTINAL DISORDERS GIHEP NEW S. COM • M AY 2015 31 Colonoscopy follow-up varied after positive FOBT BY SHARON WORCESTER Frontline Medical News BIRMINGHAM, ALA. – The time to colonoscopy after a positive fecal occult blood test varied widely between health systems and also varied based on age and comorbidity score, in a study of more than 62,000 patients from four health systems. Both individuallevel factors as well as health care system were associated with follow-up. DR. CHUBAK The median time to colonoscopy after a positive fecal occult blood test (FOBT) in 62,384 patients in the Population-based Research Optimizing Screening through Personalized Regimens (PROSPR) Network ranged from 41 to 174 days. Most of those who received a follow-up colonoscopy did so within 3-6 months of their positive FOBT. The percentage of patients fol- lowed up with colonoscopy within 12 months ranged from 58.1% to 83.8%, with lowest percentages occurring in the two systems with the longest median time to follow-up, Jessica Chubak, Ph.D., of Group Health Research Institute and her colleagues reported in a poster at the American Society of Preventive Oncology annual meeting. The rate of colonoscopy follow-up within 12 months also decreased with advancing age and increasing Charlson comorbidity score. For those aged 55-59 years, 60-64 years, 65-69 years, or 70-75 years, the hazard ratios for follow-up were 1.02, 0.98, 0.98, and 0.90, respectively, compared with the youngest age group (50-54 years). But for those patients aged 76-84 years or 85-89 years, the hazard ratios were 0.65 and 0.34, respectively. For those with a Charlson comorbidity score of 1, 2, or 3 or more, the adjusted hazard ratios for follow-up were 0.93, 0.87, and 0.70, respectively, compared with those with a score of 0, the investigators said. No signifcant diferences in follow-up were seen based on gender, body mass index, or race/ethnicity. The investigators used administrative and clinical data to estimate the VITALS Key clinical point: Increasing age and comorbidities reduce the likelihood of colonoscopy follow-up for a positive fecal occult blood test. Major fnding: The percentage of patients followed up with colonoscopy within 12 months ranged from 58.1% to 83.8%. Data source: An analysis of administrative and clinical data from four health systems with more than 62,000 patients in the PROSPR Network. Disclosures: The National Cancer Institute funded the study. time to follow-up and probability of follow-up for all persons with a positive FOBT in 2011 and 2012. The fndings have implications for future research on improving follow-up in older patients and those with comorbidities, the study authors said. The diferences between health care systems may be due to varying practices. The two organizations with the best time to colonoscopy follow-up in the network are health maintenance organizations with targets for time to colonoscopy and monitored appointment supply. In contrast, the organization with the second longest time to follow-up was an HMO that contracted with external providers for about 60% of colonoscopies. The organization with the longest time to follow-up was a safety-net system with limited colonoscopy capacity that served socioeconomically disadvantaged patients who may have faced more barriers to colonoscopy completion. Colorectal cancer is the fourth most common cancer in the United States, and FOBT is an important screening strategy that relies on follow-up in the event of a positive fnding. “Our fndings that both individual-level factors as well as health care system were associated with follow-up strengthens the rationale for investigating multilevel interventions to improve follow-up after abnormal screening tests,” the researchers concluded. [email protected] GIHEP_32.indd GIHEP_33.indd BRIEF SUMMARY: Consult the Full Prescribing Information for complete product information. LIALDA® (mesalamine) Delayed Release Tablets Rx only INDICATIONS AND USAGE LIALDA is indicated for the induction of remission in patients with active, mild to moderate ulcerative colitis and for the maintenance of remission of ulcerative colitis. CONTRAINDICATIONS LIALDA is contraindicated in patients with known hypersensitivity to salicylates or aminosalicylates or to any of the ingredients of LIALDA . WARNINGS AND PRECAUTIONS Renal Impairment Renal impairment, including minimal change nephropathy, acute and chronic interstitial nephritis, and, rarely, renal failure, has been reported in patients given products such as LIALDA that contain mesalamine or are converted to mesalamine. It is recommended that patients have an evaluation of renal function prior to initiation of LIALDA therapy and periodically while on therapy. Exercise caution when using LIALDA in patients with known renal dysfunction or a history of renal disease. In animal studies, the kidney was the principal organ for toxicity. Mesalamine-Induced Acute Intolerance Syndrome Mesalamine has been associated with an acute intolerance syndrome that may be difficult to distinguish from an exacerbation of ulcerative colitis. Although the exact frequency of occurrence has not been determined, it has occurred in 3% of patients in controlled clinical trials of mesalamine or sulfasalazine. Symptoms include cramping, acute abdominal pain and bloody diarrhea, and sometimes fever, headache, and rash. Observe patients closely for worsening of these symptoms while on treatment. If acute intolerance syndrome is suspected, promptly discontinue treatment with LIALDA. Hypersensitivity Reactions Some patients who have experienced a hypersensitivity reaction to sulfasalazine may have a similar reaction to LIALDA tablets or to other compounds that contain or are converted to mesalamine. Mesalamine-induced cardiac hypersensitivity reactions (myocarditis and pericarditis) have been reported with LIALDA and other mesalamine medications. Caution should be taken in prescribing this medicine to patients with conditions predisposing them to the development of myocarditis or pericarditis. Hepatic Impairment There have been reports of hepatic failure in patients with preexisting liver disease who have been administered mesalamine. Caution should be exercised when administering LIALDA to patients with liver disease. Upper GI Tract Obstruction Pyloric stenosis or other organic or functional obstruction in the upper gastrointestinal tract may cause prolonged gastric retention of LIALDA which would delay mesalamine release in the colon. Interference With Laboratory Tests Use of mesalamine may lead to spuriously elevated test results when measuring urinary normetanephrine by liquid chromatography with electrochemical detection because of the similarity in the chromatograms of normetanephrine and mesalamine’s main metabolite, N-acetylaminosalicylic acid (N-Ac-5-ASA). An alternative, selective assay for normetanephrine should be considered. ADVERSE REACTIONS The most serious adverse reactions seen in Lialda clinical trials or with other products that contain or are metabolized to mesalamine are: • Renal impairment, including renal failure • Mesalamine-induced acute intolerance syndrome • Hypersensitivity reactions • Hepatic impairment, including hepatic failure Clinical Trials Experience Because clinical trials are conducted under widely varying conditions, adverse reaction rates observed in the clinical trials of a drug cannot be directly compared to rates in the clinical trials of another drug and may not reflect the rates observed in practice. LIALDA has been evaluated in 1368 ulcerative colitis patients in controlled and open-label trials. Induction of Remission In two 8-week placebo-controlled clinical trials involving 535 ulcerative colitis patients, 356 received 2.4 g/day or 4.8 g/day LIALDA tablets and 179 received placebo. The most frequent adverse reaction leading to discontinuation from LIALDA therapy was exacerbation of ulcerative colitis (0.8%). Pancreatitis occurred in less than 1% of patients during clinical trials and resulted in discontinuation of therapy with LIALDA in patients experiencing this event. Adverse reactions occurring in LIALDA or placebo groups at a frequency of at least 1% in two 8-week, double blind, placebocontrolled trials are listed in Table 1. The most common adverse reactions with LIALDA 2.4 g/day and 4.8 g/day were headache (5.6% and 3.4%, respectively) and flatulence (4% and 2.8%, respectively). GIHEP_34.indd Table 1: Adverse Reactions in Two Eight-Week Placebo-Controlled Trials Experienced by at Least 1% of the LIALDA Group and at a Rate Greater than Placeboa LIALDA 2.4 g/day (n = 177) 10 (5.6%) 7 (4%) LIALDA 4.8 g/day (n = 179) 6 (3.4%) 5 (2.8%) Placebo Adverse Reaction (n = 179) Headache 1 (0.6%) Flatulence 5 (2.8%) Liver Function Test Abnormal 1 (0.6%) 4 (2.2%) 2 (1.1%) Alopecia 0 2 (1.1%) 0 Pruritus 1 (0.6%) 2 (1.1%) 2 (1.1%) a: Adverse reactions for which the placebo rate equalled or exceeded the rate for at least one of the LIALDA treatment groups were abdominal pain, dizziness, dyspepsia, and nausea. The following adverse reactions, presented by body system, were reported infrequently (less than 1%) by LIALDA-treated ulcerative colitis patients in the two controlled trials. Cardiac Disorder: tachycardia Vascular Disorders: hypertension, hypotension Skin and Subcutaneous Tissue Disorders: acne, prurigo, rash, urticaria Gastrointestinal Disorders: abdominal distention, colitis, diarrhea, pancreatitis, rectal polyp, vomiting Investigations: decreased platelet count Musculoskeletal and Connective Tissue Disorders: arthralgia, back pain Nervous System Disorders: somnolence, tremor Respiratory, Thoracic and Mediastinal Disorders: pharyngolaryngeal pain General Disorders and Administrative Site Disorders: asthenia, face edema, fatigue, pyrexia Ear and Labyrinth Disorders: ear pain Maintenance of Remission of Ulcerative Colitis The dose evaluated in three studies of LIALDA given for the maintenance of remission in patients with ulcerative colitis was 1.2 g twice daily or 2.4 g once daily. One of these studies was a 6-month double-blind comparator study while two were 12- to 14-month open-label studies. The most common adverse reactions with LIALDA in the maintenance arms of long-term trials were colitis ulcerative (5.8%), headache (2.9%), liver function test abnormal (2.3%), and abdominal pain (2.2%). Of the 1082 subjects in the all maintenance studies pooled, 1.9% had severe adverse reactions. The most common severe adverse reactions were gastrointestinal disorders; these were mainly symptoms associated with ulcerative colitis. Table 2: Adverse Reactions in Three Maintenance Trials Experienced by at Least 1% of the LIALDA Group (maintenance phases of trials) All LIALDA (n=1082) Adverse Reaction Colitis ulcerative Headache Liver function test abnormal Abdominal pain Diarrhea Abdominal distension Abdominal pain upper Dyspepsia Back pain Rash Arthralgia Fatigue Hypertension n 63 31 25 24 18 14 13 13 13 13 12 11 10 % (5.8%) (2.9%) (2.3%) (2.2%) (1.7%) (1.3%) (1.2%) (1.2%) (1.2%) (1.2%) (1.1%) (1.0%) (1.0%) The following adverse reactions, presented by body system, were reported infrequently (less than 1%) by LIALDA-treated ulcerative colitis patients in the three long-term maintenance trials (maintenance phases of these trials): Cardiac Disorder: tachycardia Skin and Subcutaneous Tissue Disorders: acne, alopecia, pruritus, urticaria Gastrointestinal Disorders: colitis, flatulence, nausea, pancreatitis, rectal polyp, vomiting Nervous System Disorders: dizziness Respiratory, Thoracic and Mediastinal Disorders: pharyngolaryngeal pain General Disorders and Administrative Site Disorders: asthenia, pyrexia Ear and Labyrinth Disorders: ear pain Postmarketing Experience In addition to the adverse reactions reported above in clinical trials involving LIALDA, the adverse reactions listed below have been identified during post-approval use of LIALDA and other mesalamine-containing products. Because these reactions are reported voluntarily from a population of uncertain size, it is not always possible to reliably estimate their frequency or establish a causal relationship to drug exposure. Body as a Whole: lupus-like syndrome, drug fever Cardiac Disorders: pericarditis, pericardial effusion, myocarditis Gastrointestinal: pancreatitis, cholecystitis, gastritis, gastroenteritis, gastrointestinal bleeding, perforated peptic ulcer Hepatic: jaundice, cholestatic jaundice, hepatitis, liver necrosis, liver failure, Kawasaki-like syndrome including changes in liver enzymes Hematologic: agranulocytosis, aplastic anemia Immune System Disorders: anaphylactic reaction, angioedema, Stevens-Johnson syndrome (SJS), drug reaction with eosinophilia and systemic symptoms (DRESS) Musculoskeletal and Connective Tissue Disorders: myalgia Neurological/Psychiatric: peripheral neuropathy, Guillain-Barre syndrome, transverse myelitis Renal Disorders: interstitial nephritis Respiratory, Thoracic and Mediastinal Disorders: hypersensitivity pneumonitis (including interstitial pneumonitis, allergic alveolitis, eosinophilic pneumonitis) Skin: psoriasis, pyoderma gangrenosum, erythema nodosum Urogenital: reversible oligospermia DRUG INTERACTIONS No investigations of interaction between LIALDA and other drugs except for certain antibiotics have been performed. However, the following drug-drug interactions have been reported for products containing mesalamine: Nephrotoxic Agents, Including Non-Steroidal Anti-Inflammatory Drugs The concurrent use of mesalamine with known nephrotoxic agents, including non-steroidal anti-inflammatory drugs (NSAIDs) may increase the risk of renal reactions. Azathioprine or 6-mercaptopurine The concurrent use of mesalamine with azathioprine or 6-mercaptopurine may increase the risk for blood disorders. USE IN SPECIFIC POPULATIONS Pregnancy Pregnancy Category B. Reproduction studies with mesalamine have been performed in rats at doses up to 1000 mg/kg/day (1.8 times the maximum recommended human dose based on a body surface area comparison) and rabbits at doses up to 800 mg/kg/day (2.9 times the maximum recommended human dose based on a body surface area comparison) and have revealed no evidence of impaired fertility or harm to the fetus due to mesalamine. There are, however, no adequate and well-controlled studies in pregnant women. Because animal reproduction studies are not always predictive of human response, this drug should be used during pregnancy only if clearly needed. Mesalamine is known to cross the placental barrier. Nursing Mothers Low concentrations of mesalamine and higher concentrations of its N-acetyl metabolite have been detected in human breast milk. The clinical significance of this has not been determined and there is limited experience of nursing women using mesalamine. Caution should be exercised if LIALDA is administered to a nursing woman. Pediatric Use Safety and effectiveness of LIALDA in pediatric patients have not been established. Geriatric Use Reports from uncontrolled clinical studies and postmarketing reporting systems suggested a higher incidence of blood dyscrasias, i.e., neutropenia and pancytopenia in patients who were 65 years or older who were taking mesalamine-containing products such as LIALDA. Caution should be taken to closely monitor blood cell counts during mesalamine therapy. Clinical trials of LIALDA did not include sufficient numbers of patients aged 65 and over to determine whether they respond differently from younger patients. Other reported clinical experience has not identified differences in responses between the elderly and younger patients. Systemic exposures are increased in elderly subjects. In general, dose selection for an elderly patient should be cautious, usually starting at the low end of the dosing range, reflecting the greater frequency of decreased hepatic, renal, or cardiac function, and of concurrent disease or other drug therapy in elderly patients. OVERDOSAGE LIALDA is an aminosalicylate, and symptoms of salicylate toxicity may include tinnitus, vertigo, headache, confusion, drowsiness, sweating, seizures, hyperventilation, dyspnea, vomiting, and diarrhea. Severe intoxication may lead to disruption of electrolyte balance and blood-pH, hyperthermia, dehydration, and end organ damage. There is no specific known antidote for mesalamine overdose; however, conventional therapy for salicylate toxicity may be beneficial in the event of acute overdosage. Fluid and electrolyte imbalance should be corrected by the administration of appropriate intravenous therapy. Adequate renal function should be maintained. DOSAGE AND ADMINISTRATION The recommended dosage for the induction of remission in adult patients with active, mild to moderate ulcerative colitis is two to four 1.2 g tablets taken once daily with a meal for a total daily dose of 2.4 g or 4.8 g. The recommended dosage for the maintenance of remission is two 1.2 g tablets taken once daily with a meal for a total daily dose of 2.4 g. Store at room temperature 15°C to 25°C (59°F to 77°F); excursions permitted to 30°C (86°F). Manufactured for Shire US Inc., 725 Chesterbrook Blvd., Wayne, PA 19087, USA by Cosmo S.p.A., Milan, Italy. By license of Nogra Pharma Limited, Dublin, Ireland. U.S. Patent No. 6,773,720. © 2014 Shire US Inc. Rev. 06/2014 S03025 GIHEP NEW S. COM • M AY 2015 IBD AND INTESTINAL DISORDERS 35 Alternatives to colonoscopy are ‘works in progress’ BY DOUG BRUNK Frontline Medical News SAN FRANCISCO – Colonoscopy may be the most commonly used technique to screen for colorectal cancer in the United States, but it’s far from perfect, according to Dr. David A. Lieberman, AGAF. For one thing, serious complications occur in 3-5 per 1,000 procedures at 30 days of follow-up, “and if you look at individuals over 65, the rates almost double in terms of serious complications,” Dr. Lieberman, chief of the division of gastroenterology and hepatology at Oregon Health and Science University, said at the 2015 AGA Tech Summit, which was sponsored by the AGA Center for GI Innovation and Technology. “The rate of perforation over age 65 is about 1 per 1,000,” he said. Colonoscopy is invasive, “and it would never be conceived of as the ideal test for population-based screening,” he added. “It’s expensive, and [clinicians] in many countries simply do not have the resources and expertise to do it.” Compared with current screening rates in the United States for cervical and breast cancer, a “screening gap” exists in the percentage of adults who are up to date in tests for colorectal cancer, he said. “If you look at what’s been accomplished with cervical cancer screening and mammography, we see that there’s a ways to go for colonoscopy,” he said. The ideal screening test for colorectal cancer would accurately identify individuals at risk for colon cancer at an early, preventable stage, Dr. Lieberman said. That prevention element “really averts the downstream colon cancer care costs, which would be very attractive in a single-payer health care system,” he said. “If we had a system that took care of us for life, that system would be very invested in trying to prevent colon cancer, because [it would] be worried about those downstream costs.” One potential alternative to colonoscopy is fecal immunochemical testing (FIT). A recent meta-analysis suggested that FIT detected cancer with a 79% sensitivity (Ann. Intern. Med. 2014;160:171-81), and a separate, recent prospective study found a 74% sensitivity rate in detecting cancer, but a 24% sensitivity rate in detecting advanced adenoma (N. Engl. J. Med. 2014;370:1287-97). “So in terms of early detection, FIT is pretty good,” Dr. Lieberman said. “In terms of cancer prevention? Maybe not so good. There are also issues around the testing program, which requires adherence to both positive and negative tests. Some of these behavioral factors play a major role in the actual efectiveness. So you can have a great test, but if it’s not getting done properly then there’s going to be an issue. There is some potential for CRC prevention, but it’s going to be less than for some others.” What about stool DNA? A landmark study found that stool DNA detected cancer with a sensitivity of 92%, compared with FIT at 74% (N. Engl. J. Med. 2014;370:1287-97). However, the sensitivity for detecting adenomas was rela- per second before it reaches the small bowel,” Dr. tively low for both methods (42% for stool DNA, Ladabaum said. compared with 24% for FIT). Stool DNA testing In an early study of the second-generation sys“appears to be an efective screening test [but] the tem, the device achieved a sensitivity of 89% and a appropriate interval for testing is still uncertain,” specifcity of 76% in detecting polyps of 6 mm in Dr. Lieberman said. “The recommendation is a size or larger and a sensitivity of 88% and a speci3-year interval.” fcity of 89% in detecting polyps 10 mm in size or He characterized serum testing as the “holy grail” of screening for colorec- larger (Endoscopy 2009;41:1026-31). More recently, researchers examined consecutive tal cancer, “because it would ‘Colonoscopy patients who had incomplete colonoscopy and be ideal to have a noninvasive would never be compared a follow-up with either second-generatest. You’d come in, get a conceived of as tion CCE or CT colonography (Gut 2015;64:272blood draw, and get risk stratthe ideal test for 81). The diagnostic yield of CCE and CT ifed. There are a number of population-based colonography was 25% and 12%, respectively, for diferent possible pathways, screening.’ one looking at specifc genetic polyps 6 mm or larger and 5% vs. 3% for polyps 10 mm or larger. markers, others looking at DR. LIEBERMAN In a larger, multisite study, researchers examined genetic fngerprinting: in oththe efcacy of the second-generation PillCam as er words, seeing a pattern of a primary screening tool (Gastroenterology 2015 genes that are associated with colon cancer versus patients who do not have colon cancer. Proteomics [doi:10.1053/j.gastro.2015.01.025). Of 884 subjects is another fngerprinting technique, as is metabolo- enrolled, 85 were excluded from the analysis for a variety of reasons. Of these, 12 were excluded bemics: looking at a variety of metabolites that may cause the capsule did not reach the colon within 12 be altered by the presence of having neoplasia. hours and 8 were excluded because the capsule did This is an intriguing area but so far there hasn’t not pass the cecum within 12 hours. “So if used in been a lot of data.” practice, we’ll see this – [incomplete capsule studTo date, the most progress involved in this area ies],” Dr. Ladabaum said. involves molecular tests of DNA or proteins. In addition, 77 were excluded for inadequate “These studies are all relatively small and somecleansing and capsule transit time through the what promising in terms of cancer sensitivity, but colon in less than 40 minutes. “Maybe that’s due not so great for adenoma sensitivity,” he said. “It’s to the booster regifair to say that this is men,” he said. “There still a work in progTo date, the most progress involved in this are still some things to ress.” area involves molecular tests of DNA or work out in the bowel Dr. Lieberman reportprep. Overall, there ed having served on the proteins. ‘These studies are all relatively were a good number of scientifc advisory board small and somewhat promising in terms people [in this study] of Exact Sciences. of cancer sensitivity, but not so great who didn’t really have In a separate prethe exam [completed sentation, Dr. Uri for adenoma sensitivity.... It’s fair to say as intended]. Is that Ladabaum updated atgoing to pan out as a tendees on the status of that this is still a work in progress.’ big problem in clinical PillCam, also known as practice? That remains to be seen.” colon capsule endoscopy (CCE), for detecting coThe study found that the second-generation lon cancer. The PillCam is cleared by the Food and Drug Administration for detection of colon polyps PillCam achieved a sensitivity of 87% and a specin patients after an incomplete optical colonoscopy ifcity of 94% in detecting polyps 6 mm or larger with adequate preparation, or if a complete evalu- and a sensitivity of 85% and a specifcity of 97% in detecting polyps 10 mm in size or larger. “Is this ation of the colon was not technically possible. In good enough for this kind of technology?” Dr. a large meta-analysis, the frst-generation PillCam Ladabaum asked. “There’s lots of room for debate achieved a sensitivity of 71% and a specifcity of here. Interestingly, the numbers for sessile serrated 75% in detecting polyps of any size and a sensipolyps didn’t look that good” (a sensitivity of 29% tivity of 68% and a specifcity of 82% in detecting polyps 6 mm in size or larger (Clin. Gastroenterol. for polyps 6 mm in size or greater and 33% for polyps 10 mm in size or greater). Hepatol. 2010;8:515-22). “The results were someDr. Ladabaum disclosed that he has served as a what disappointing for a test like this, not hitting consultant for Given Imaging and Exact Sciences. the bar that we would want,” said Dr. Ladabaum, He has also served on the advisory board for Mauprofessor of medicine in the division of gastroenna Kea Technologies. terology and hepatology at Stanford (Calif.) UniIn conclusion, according to Dr. Lieberman, there versity. are several feasible alternatives to colonoscopy for The second-generation PillCam features an imprimary colon cancer screening in average-risk proved angle of the imagers, from 156 degrees to individuals. Each has advantages and limitations 172 degrees, “so you get a bigger view all the way and ofers a less invasive approach to screening. around,” he said. Another new feature is an adapThe bar for screening has been raised from early tive imaging rate. The frst-generation device captured 4 images per second regardless of where the cancer detection alone to both early detection and prevention. capsule was moving. The new system “goes at 4 images per second when stationary, goes as fast as [email protected] 35 images per second while moving, and 14 images INTRODUCING A New Face of * Cure in HCV For the treatment of chronic genotype 1 (GT1) hepatitis C virus (HCV) infection—an all-oral, interferon-free regimen with 3 distinct direct-acting antivirals *Cure (virologic cure): sustained virologic response (SVR12); HCV ribonucleic acid (RNA) below the lower limit of quantifcation (<25 IU/mL) 12 weeks after the end of treatment. INDICATION1 VIEKIRA PAK™, with or without ribavirin (RBV), is indicated for the treatment of adult patients with genotype 1 chronic hepatitis C virus infection, including those with compensated cirrhosis. Limitation of Use: VIEKIRA PAK is not recommended for use in patients with decompensated liver disease. IMPORTANT SAFETY INFORMATION for which elevated plasma levels are associated with serious and/ or life-threatening events; strong inducers of CYP3A or CYP2C8, which may lead to reduced effcacy of VIEKIRA PAK; and strong CYP2C8 inhibitors, which may increase dasabuvir levels and the risk of QT prolongation. • with the following drugs: alfuzosin HCL; carbamazepine, phenytoin, phenobarbital; gemfbrozil; rifampin; ergotamine, dihydroergotamine, ergonovine, methylergonovine; ethinyl estradiol-containing medicines, such as many oral contraceptives; St. John’s wort (Hypericum perforatum); lovastatin, simvastatin; pimozide; efavirenz; sildenafl (when dosed as Revatio‡ for pulmonary arterial hypertension); triazolam and oral midazolam. Risks Associated with RBV Combination Treatment If VIEKIRA PAK is administered with RBV, the contraindications, warnings and precautions (particularly pregnancy avoidance), and adverse reactions for RBV also apply to this combination regimen. Refer to the RBV prescribing information. • in patients with known hypersensitivity (e.g., toxic epidermal necrolysis or Stevens-Johnson syndrome) to ritonavir. CONTRAINDICATIONS WARNINGS AND PRECAUTIONS VIEKIRA PAK is contraindicated: • in patients with severe hepatic impairment due to risk of potential toxicity. • with drugs that are highly dependent on CYP3A for clearance and Increased Risk of ALT Elevations • Elevations of ALT to >5x the ULN occurred in 1% of all subjects in clinical trials and were signifcantly more frequent in females using ethinyl estradiol-containing medications. In female patients, GIHEP_36.indd 2 2/20/2015 5:13:11 PM VIEKIRA PAK +/- ribavirin (RBV) cured* chronic HCV in multiple GT1 patient types, including compensated cirrhotics VIEKIRA PAK +/- RBV was studied in 6 phase III clinical trials that included >2300 adult patients with chronic GT1 HCV1 Across patient populations, pooled by recommended treatment regimen† (n=1084), VIEKIRA PAK +/- RBV delivered consistently high cure* rates ranging from 95%–100%1,2 SVR12 rates Overall GT1 Patients Cured1,2* (n=1053/1084) VIEKIRA PAK / RBV (12 OR 24 WEEKS) Learn more at viekiraHCP.com † Recommended regimen=ombitasvir, paritaprevir, ritonavir (25/150/100 mg QD) and dasabuvir (250 mg BID) +/- ribavirin (1000 or 1200 mg determined by body weight; divided BID).1 discontinue ethinyl estradiol-containing medications prior to starting therapy and use alternative methods of contraception during therapy (e.g., progestin only or non-hormonal contraception). Use caution when co-administering VIEKIRA PAK with estrogens other than ethinyl estradiol, such as estradiol and conjugated estrogens. • Perform hepatic lab testing on all patients during the frst 4 weeks of treatment and as clinically indicated thereafter. If ALT is elevated above baseline levels, repeat testing and monitor closely. Patients should be instructed to consult their doctor without delay if they have onset of fatigue, weakness, lack of appetite, nausea and vomiting, jaundice, or discolored feces. Consider discontinuing VIEKIRA PAK if ALT levels remain persistently >10x the ULN. Discontinue VIEKIRA PAK if ALT elevation is accompanied by signs or symptoms of liver infammation or increasing conjugated bilirubin, alkaline phosphatase, or INR. Risk of Adverse Reactions or Reduced Therapeutic Effect Due to Drug Interactions • The concomitant use of VIEKIRA PAK and certain other drugs may result in known or potentially signifcant drug interactions, some of which may lead to loss of therapeutic effect of VIEKIRA PAK and possible development of resistance, or adverse reactions from greater exposures of concomitant drugs or components of VIEKIRA PAK. GIHEP_37.indd 3 HCV/HIV-1 Co-infected Patients: Risk of HIV-1 Protease Inhibitor Drug Resistance • The ritonavir component of VIEKIRA PAK is an HIV-1 protease inhibitor and can select for HIV-1 protease inhibitor resistance. To reduce this risk, HCV/HIV-1 co-infected patients should also be on a suppressive antiretroviral drug regimen. ADVERSE REACTIONS • In subjects receiving VIEKIRA PAK with RBV, the most commonly reported adverse reactions (>10% of subjects) were fatigue, nausea, pruritus, other skin reactions, insomnia, and asthenia. In subjects receiving VIEKIRA PAK without RBV, the most commonly reported adverse reactions (≥5% of subjects) were nausea, pruritus, and insomnia. ‡ Revatio® is a trademark of its respective owner and not a trademark of AbbVie Inc. The makers of this brand are not affiliated with and do not endorse AbbVie Inc. or its products. References: 1. VIEKIRA PAK [package insert]. North Chicago, IL. AbbVie Inc. 2. Data on file. AbbVie Inc. Please see Brief Summary of Prescribing Information on the adjacent page(s). ©2014 AbbVie Inc. North Chicago, IL 046-1574501 December 2014 Printed in U.S.A. 2/20/2015 5:14:00 PM PROFESSIONAL BRIEF SUMMARY CONSULT PACKAGE INSERT FOR FULL PRESCRIBING INFORMATION VIEKIRA PAKTM (ombitasvir, paritaprevir, and ritonavir tablets; dasabuvir tablets) INDICATIONS AND USAGE VIEKIRA PAK with or without ribavirin is indicated for the treatment of patients with genotype 1 chronic hepatitis C virus (HCV) infection including those with compensated cirrhosis. Limitation of Use: VIEKIRA PAK is not recommended for use in patients with decompensated liver disease [see Use in Specifc Populations]. CONTRAINDICATIONS • If VIEKIRA PAK is administered with ribavirin, the contraindications to ribavirin also apply to this combination regimen. Refer to the ribavirin prescribing information for a list of contraindications for ribavirin. • VIEKIRA PAK is contraindicated in patients with severe hepatic impairment due to risk of potential toxicity [see Use in Specifc Populations]. • VIEKIRA PAK is contraindicated with: ° Drugs that are highly dependent on CYP3A for clearance and for which elevated plasma concentrations are associated with serious and/or life-threatening events. ° Drugs that are strong inducers of CYP3A and CYP2C8 and may lead to reduced effcacy of VIEKIRA PAK. ° Drugs that are strong inhibitors of CYP2C8 and may increase dasabuvir plasma concentrations and the risk of QT prolongation. Table 1 lists drugs that are contraindicated with VIEKIRA PAK [see Drug Interactions]. Table 1. Drugs that are Contraindicated with VIEKIRA PAK Drug Class Alpha1adrenoreceptor antagonist Anticonvulsants Drug(s) within Class that are Contraindicated Alfuzosin HCL Clinical Comments Potential for hypotension. Carbamazepine, phenytoin, phenobarbital Ombitasvir, paritaprevir, ritonavir and dasabuvir exposures may decrease leading to a potential loss of therapeutic activity of VIEKIRA PAK. Antihyperlipidemic Gemfbrozil Increase in dasabuvir exposures by 10-fold which may increase agent the risk of QT prolongation. Antimycobacterial Rifampin Ombitasvir, paritaprevir, ritonavir and dasabuvir exposures may decrease leading to a potential loss of therapeutic activity of VIEKIRA PAK. Ergot derivatives Ergotamine, Acute ergot toxicity characterized by vasospasm and tissue dihydroergotamine, ischemia has been associated with co-administration of ergonovine, methylergonovine ritonavir and ergonovine, ergotamine, dihydroergotamine, or methylergonovine. Ethinyl estradiolEthinyl estradiol-containing Potential for ALT elevations containing products medications such as combined [see Warnings and Precautions]. oral contraceptives Herbal Product St. John’s Wort (Hypericum Ombitasvir, paritaprevir, ritonavir and dasabuvir exposures perforatum) may decrease leading to a potential loss of therapeutic activity of VIEKIRA PAK. HMG-CoA Reductase Lovastatin, simvastatin Potential for myopathy including rhabdomyolysis. Inhibitors Neuroleptics Pimozide Potential for cardiac arrhythmias. Non-nucleoside Efavirenz Co-administration of efavirenz based regimens with paritaprevir, ritonavir plus dasabuvir was poorly tolerated and reverse transcriptase inhibitor resulted in liver enzyme elevations. There is increased potential for sildenafl-associated adverse Phosphodiesterase-5 Sildenafl when dosed as (PDE5) inhibitor REVATIO for the treatment events such as visual disturbances, hypotension, priapism, and syncope. of pulmonary arterial hypertension (PAH) Sedatives/hypnotics Triazolam Triazolam and orally administered midazolam are extensively Orally administered midazolam metabolized by CYP3A4. Coadministration of triazolam or orally administered midazolam with VIEKIRA PAK may cause large increases in the concentration of these benzodiazepines. The potential exists for serious and/or life threatening events such as prolonged or increased sedation or respiratory depression. • VIEKIRA PAK is contraindicated in patients with known hypersensitivity (e.g. toxic epidermal necrolysis (TEN) or Stevens-Johnson syndrome) to ritonavir. WARNINGS AND PRECAUTIONS Increased Risk of ALT Elevations During clinical trials with VIEKIRA PAK with or without ribavirin, elevations of ALT to greater than 5 times the upper limit of normal (ULN) occurred in approximately 1% of all subjects [see Adverse Reactions]. ALT elevations were typically asymptomatic, occurred during the frst 4 weeks of treatment, and declined within two to eight weeks of onset with continued dosing of VIEKIRA PAK with or without ribavirin. These ALT elevations were signifcantly more frequent in female subjects who were using ethinyl estradiolcontaining medications such as combined oral contraceptives, contraceptive patches or contraceptive vaginal rings. Ethinyl estradiol-containing medications must be discontinued prior to starting therapy with VIEKIRA PAK [see Contraindications]. Alternative methods of contraception (e.g, progestin only contraception or nonhormonal methods) are recommended during VIEKIRA PAK therapy. Ethinyl estradiol-containing medications can be restarted approximately 2 weeks following completion of treatment with VIEKIRA PAK. Women using estrogens other than ethinyl estradiol, such as estradiol and conjugated estrogens used in hormone replacement therapy had a rate of ALT elevation similar to those not receiving any estrogens; however, due to the limited number of subjects taking these other estrogens, caution is warranted for coadministration with VIEKIRA PAK [see Adverse Reactions]. Hepatic laboratory testing should be performed during the frst 4 weeks of starting treatment and as clinically indicated thereafter. If ALT is found to be elevated above baseline levels, it should be repeated and monitored closely: • Patients should be instructed to consult their health care professional without delay if they have onset of fatigue, weakness, lack of appetite, nausea and vomiting, jaundice or discolored feces. • Consider discontinuing VIEKIRA PAK if ALT levels remain persistently greater than 10 times the ULN. • Discontinue VIEKIRA PAK if ALT elevation is accompanied by signs or symptoms of liver infammation or increasing conjugated bilirubin, alkaline phosphatase, or INR. Risks Associated With Ribavirin Combination Treatment If VIEKIRA PAK is administered with ribavirin, the warnings and precautions for ribavirin, in particular the pregnancy avoidance warning, apply to this combination regimen. Refer to the ribavirin prescribing information for a full list of the warnings and precautions for ribavirin. Risk of Adverse Reactions or Reduced Therapeutic Effect Due to Drug Interactions The concomitant use of VIEKIRA PAK and certain other drugs may result in known or potentially signifcant drug interactions, some of which may lead to: • Loss of therapeutic effect of VIEKIRA PAK and possible development of resistance • Possible clinically signifcant adverse reactions from greater exposures of concomitant drugs or components of VIEKIRA PAK. See Table 4 for steps to prevent or manage these possible and known signifcant drug interactions, including dosing recommendations [see Drug Interactions]. Consider the potential for drug interactions prior to and during VIEKIRA PAK therapy; review concomitant medications during VIEKIRA PAK therapy; and monitor for the adverse reactions associated with the concomitant drugs [see Contraindications and Drug Interactions]. Risk of HIV-1 Protease Inhibitor Drug Resistance in HCV/HIV-1 Co-infected Patients The ritonavir component of VIEKIRA PAK is also an HIV-1 protease inhibitor and can select for HIV-1 protease inhibitor resistance-associated substitutions. Any HCV/HIV-1 co-infected patients treated with VIEKIRA PAK should also be on a suppressive antiretroviral drug regimen to reduce the risk of HIV-1 protease inhibitor drug resistance. ADVERSE REACTIONS If VIEKIRA PAK is administered with ribavirin (RBV), refer to the prescribing information for ribavirin for a list of ribavirin-associated adverse reactions. The following adverse reaction is described below and elsewhere in the labeling: • Increased Risk of ALT Elevations [see Warnings and Precautions] Clinical Trials Experience Because clinical trials are conducted under widely varying conditions, adverse reaction rates observed in clinical trials of VIEKIRA PAK cannot be directly compared to rates in the clinical trials of another drug and may not refect the rates observed in practice. The safety assessment was based on data from six Phase 3 clinical trials in more than 2,000 subjects who received VIEKIRA PAK with or without ribavirin for 12 or 24 weeks. VIEKIRA PAK with Ribavirin in Placebo-Controlled Trials The safety of VIEKIRA PAK in combination with ribavirin was assessed in 770 subjects with chronic HCV infection in two placebo-controlled trials (SAPPHIRE-I and -II). Adverse reactions that occurred more often in subjects treated with VIEKIRA PAK in combination with ribavirin compared to placebo were fatigue, nausea, pruritus, other skin reactions, insomnia, and asthenia (see Table 2). The majority of the adverse reactions were mild in severity. Two percent of subjects experienced a serious adverse event (SAE). The proportion of subjects who permanently discontinued treatment due to adverse reactions was less than 1%. GIHEP_38.indd 103-B026 Viekira Pak PB 10.5x13 (1.25).indd 1 Table 2. Adverse Reactions with ≥5% Greater Frequency Reported in Subjects with Chronic HCV GT1 Infection Treated with VIEKIRA PAK in Combination with Ribavirin Compared to Placebo for 12 Weeks SAPPHIRE-I and -II VIEKIRA PAK + RBV Placebo 12 Weeks 12 Weeks N = 770 N = 255 % % Fatigue 34 26 Nausea 22 15 Pruritus* 18 7 16 9 Skin reactions$ Insomnia 14 8 Asthenia 14 7 *Grouped term ‘pruritus’ included the preferred terms pruritus and pruritus generalized. $Grouped terms: rash, erythema, eczema, rash maculo-papular, rash macular, dermatitis, rash papular, skin exfoliation, rash pruritic, rash erythematous, rash generalized, dermatitis allergic, dermatitis contact, exfoliative rash, dermatitis, photosensitivity reaction, psoriasis, skin reaction, ulcer, urticaria. VIEKIRA PAK with and without Ribavirin in Regimen-Controlled Trials VIEKIRA PAK with and without ribavirin was assessed in 401 and 509 subjects with chronic HCV infection, respectively, in three clinical trials (PEARL-II, PEARL-III and PEARL-IV). Pruritus, nausea, insomnia, and asthenia were identifed as adverse events occurring more often in subjects treated with VIEKIRA PAK in combination with ribavirin (see Table 3). The majority of adverse events were mild to moderate in severity. The proportion of subjects who permanently discontinued treatment due to adverse events was less than 1% for both VIEKIRA PAK in combination with ribavirin and VIEKIRA PAK alone. Table 3. Adverse Events with ≥5% Greater Frequency Reported in Subjects with Chronic HCV GT1 Infection Treated with VIEKIRA PAK in Combination with Ribavirin Compared to VIEKIRA PAK for 12 Weeks PEARL-II, -III and -IV VIEKIRA PAK + RBV VIEKIRA PAK 12 Weeks 12 Weeks N = 401 N = 509 % % Nausea 16 8 Pruritus* 13 7 Insomnia 12 5 Asthenia 9 4 *Grouped term ‘pruritus’ included the preferred terms pruritus and pruritus generalized. VIEKIRA PAK with Ribavirin in Subjects with Compensated Cirrhosis VIEKIRA PAK with ribavirin was assessed in 380 subjects with compensated cirrhosis who were treated for 12 (n=208) or 24 (n=172) weeks duration (TURQUOISE-II). The type and severity of adverse events in subjects with compensated cirrhosis was comparable to non-cirrhotic subjects in other phase 3 trials. Fatigue, skin reactions and dyspnea occurred at least 5% more often in subjects treated for 24 weeks. The majority of adverse events occurred during the frst 12 weeks of dosing in both treatment arms. Most of the adverse events were mild to moderate in severity. The proportion of subjects treated with VIEKIRA PAK for 12 and 24 weeks with SAEs was 6% and 5%, respectively and 2% of subjects permanently discontinued treatment due to adverse events in each treatment arm. Skin Reactions In PEARL-II, -III and -IV, 7% of subjects receiving VIEKIRA PAK alone and 10% of subjects receiving VIEKIRA PAK with ribavirin reported rash-related events. In SAPPHIRE-I and -II 16% of subjects receiving VIEKIRA PAK with ribavirin and 9% of subjects receiving placebo reported skin reactions. In TURQUOISE-II, 18% and 24% of subjects receiving VIEKIRA PAK with ribavirin for 12 or 24 weeks reported skin reactions. The majority of events were graded as mild in severity. There were no serious events or severe cutaneous reactions, such as Stevens Johnson Syndrome (SJS), toxic epidermal necrolysis (TEN), erythema multiforme (EM) or drug rash with eosinophilia and systemic symptoms (DRESS). Laboratory Abnormalities Serum ALT Elevations Approximately 1% of subjects treated with VIEKIRA PAK experienced post-baseline serum ALT levels greater than 5 times the upper limit of normal (ULN) after starting treatment. The incidence increased to 25% (4/16) among women taking a concomitant ethinyl estradiol containing medication [see Contraindications and Warnings and Precautions]. The incidence of clinically relevant ALT elevations among women using estrogens other than ethinyl estradiol, such as estradiol and conjugated estrogens used in hormone replacement therapy was 3% (2/59). ALT elevations were typically asymptomatic, generally occurred during the frst 4 weeks of treatment (mean time 20 days, range 8-57 days) and most resolved with ongoing therapy. The majority of these ALT elevations were assessed as drug-related liver injury. Elevations in ALT were generally not associated with bilirubin elevations. Cirrhosis was not a risk factor for elevated ALT [see Warnings and Precautions]. Serum Bilirubin Elevations Post-baseline elevations in bilirubin at least 2 x ULN were observed in 15% of subjects receiving VIEKIRA PAK with ribavirin compared to 2% in those receiving VIEKIRA PAK alone. These bilirubin increases were predominately indirect and related to the inhibition of the bilirubin transporters OATP1B1/1B3 by paritaprevir and ribavirin-induced hemolysis. Bilirubin elevations occurred after initiation of treatment, peaked by study Week 1, and generally resolved with ongoing therapy. Bilirubin elevations were not associated with serum ALT elevations. Anemia/Decreased Hemoglobin Across all Phase 3 studies, the mean change from baseline in hemoglobin levels in subjects treated with VIEKIRA PAK in combination with ribavirin was -2.4 g/dL and the mean change in subjects treated with VIEKIRA PAK alone was -0.5 g/dL. Decreases in hemoglobin levels occurred early in treatment (Week 1-2) with further reductions through Week 3. Hemoglobin values remained low during the remainder of treatment and returned towards baseline levels by post-treatment Week 4. Less than 1% of subjects treated with VIEKIRA PAK with ribavirin had hemoglobin levels decrease to less than 8.0 g/dL during treatment. Seven percent of subjects treated with VIEKIRA PAK in combination with ribavirin underwent a ribavirin dose reduction due to a decrease in hemoglobin levels; three subjects received a blood transfusion and fve required erythropoietin. One patient discontinued therapy due to anemia. No subjects treated with VIEKIRA PAK alone had a hemoglobin level less than 10 g/dL. VIEKIRA PAK in HCV/HIV-1 Co-infected Subjects VIEKIRA PAK with ribavirin was assessed in 63 subjects with HCV/HIV-1 co-infection who were on stable antiretroviral therapy. The most common adverse events occurring in at least 10% of subjects were fatigue (48%), insomnia (19%), nausea (17%), headache (16%), pruritus (13%), cough (11%), irritability (10%), and ocular icterus (10%). Elevations in total bilirubin greater than 2 x ULN (mostly indirect) occurred in 34 (54%) subjects. Fifteen of these subjects were also receiving atazanavir at the time of bilirubin elevation and nine also had adverse events of ocular icterus, jaundice or hyperbilirubinemia. None of the subjects with hyperbilirubinemia had concomitant elevations of aminotransferases [see Warnings and Precautions and Adverse Reactions]. No subject experienced a grade 3 ALT elevation. Seven subjects (11%) had at least one post-baseline hemoglobin value of less than 10 g/dL, and six of these subjects had a ribavirin dose modifcation; no subject in this small cohort required a blood transfusion or erythropoietin. Median declines in CD4+ T-cell counts of 47 cells/mm3 and 62 cells/mm3 were observed at the end of 12 and 24 weeks of treatment, respectively, and most returned to baseline levels post-treatment. Two subjects had CD4+ T-cell counts decrease to less than 200 cells/mm3 during treatment without a decrease in CD4%. No subject experienced an AIDS-related opportunistic infection. VIEKIRA PAK in Selected Liver Transplant Recipients VIEKIRA PAK with ribavirin was assessed in 34 post-liver transplant subjects with recurrent HCV infection. Adverse events occurring in more than 20% of subjects included fatigue 50%, headache 44%, cough 32%, diarrhea 26%, insomnia 26%, asthenia 24%, nausea 24%, muscle spasms 21% and rash 21%. Ten subjects (29%) had at least one post-baseline hemoglobin value of less than 10 g/dL. Ten subjects underwent a ribavirin dose modifcation due to decrease in hemoglobin and 3% (1/34) had an interruption of ribavirin. Five subjects received erythropoietin, all of whom initiated ribavirin at the starting dose of 1000 to 1200 mg daily. No subject received a blood transfusion. DRUG INTERACTIONS See also Contraindications and Warnings and Precautions. Potential for VIEKIRA PAK to Affect Other Drugs Ombitasvir, paritaprevir, and dasabuvir are inhibitors of UGT1A1, and ritonavir is an inhibitor of CYP3A4. Paritaprevir is an inhibitor of OATP1B1 and OATP1B3 and paritaprevir, ritonavir and dasabuvir are inhibitors of BCRP. Co-administration of VIEKIRA PAK with drugs that are substrates of CYP3A, UGT1A1, BCRP, OATP1B1 or OATP1B3 may result in increased plasma concentrations of such drugs. Potential for Other Drugs to Affect One or More Components of VIEKIRA PAK Paritaprevir and ritonavir are primarily metabolized by CYP3A enzymes. Co-administration of VIEKIRA PAK with strong inhibitors of CYP3A may increase paritaprevir and ritonavir concentrations. Dasabuvir is primarily metabolized by CYP2C8 enzymes. Co-administration of VIEKIRA PAK with drugs that inhibit CYP2C8 may increase dasabuvir plasma concentrations. Ombitasvir is primarily metabolized via amide hydrolysis while CYP enzymes play a minor role in its metabolism. Ombitasvir, paritaprevir, dasabuvir and ritonavir are substrates of P-gp. Ombitasvir, paritaprevir and dasabuvir are substrates of BCRP. Paritaprevir is a substrate of OATP1B1 and OATP1B3. Inhibition of P-gp, BCRP, OATP1B1 or OATP1B3 may increase the plasma concentrations of the various components of VIEKIRA PAK. Established and Other Potential Drug Interactions If dose adjustments of concomitant medications are made due to treatment with VIEKIRA PAK, doses should be re-adjusted after administration of VIEKIRA PAK is completed. Dose adjustment is not required for VIEKIRA PAK. Table 4 provides the effect of co-administration of VIEKIRA PAK on concentrations of concomitant drugs and the effect of concomitant drugs on the various components of VIEKIRA PAK. See Contraindications for drugs that are contraindicated with VIEKIRA PAK. Refer to the ritonavir prescribing information for other potentially signifcant drug interactions with ritonavir. Table 4. Established Drug Interactions Based on Drug Interaction Trials Concomitant Drug Class: Drug Name ANTIARRHYTHMICS amiodarone, bepridil, disopyramide, fecainide, lidocaine (systemic), mexiletine, propafenone, quinidine ANTIFUNGALS ketoconazole Effect on Concentration ↑ antiarrhythmics Caution is warranted and therapeutic concentration monitoring (if available) is recommended for antiarrhythmics when coadministered with VIEKIRA PAK. ↑ ketoconazole voriconazole ↓ voriconazole When VIEKIRA PAK is co-administered with ketoconazole, the maximum daily dose of ketoconazole should be limited to 200 mg per day. Co-administration of VIEKIRA PAK with voriconazole is not recommended unless an assessment of the beneft-to-risk ratio justifes the use of voriconazole. CALCIUM CHANNEL BLOCKERS amlodipine ↑ amlodipine CORTICOSTEROIDS (INHALED/NASAL) futicasone ↑ futicasone DIURETICS furosemide ↑ furosemide (Cmax) HIV-ANTIVIRAL AGENTS atazanavir/ritonavir once daily ↑ paritaprevir Clinical Comments Consider dose reduction for amlodipine. Clinical monitoring is recommended. Concomitant use of VIEKIRA PAK with inhaled or nasal futicasone may reduce serum cortisol concentrations. Alternative corticosteroids should be considered, particularly for long term use. Clinical monitoring of patients is recommended and therapy should be individualized based on patient’s response. When coadministered with VIEKIRA PAK, atazanavir 300 mg (without ritonavir) should only be given in the morning. darunavir/ritonavir ↓ darunavir (Ctrough) Co-administration of VIEKIRA PAK with darunavir/ritonavir is not recommended. lopinavir/ritonavir ↑ paritaprevir Co-administration of VIEKIRA PAK with lopinavir/ritonavir is not recommended. rilpivirine ↑ rilpivirine Co-administration of VIEKIRA PAK with rilpivirine once daily is not recommended due to potential for QT interval prolongation with higher concentrations of rilpivirine. HMG CoA REDUCTASE INHIBITORS rosuvastatin ↑ rosuvastatin When VIEKIRA PAK is co-administered with rosuvastatin, the dose of rosuvastatin should not exceed 10 mg per day. pravastatin ↑ pravastatin When VIEKIRA PAK is co-administered with pravastatin, the dose of pravastatin should not exceed 40 mg per day. IMMUNOSUPPRESSANTS ↑ cyclosporine When initiating therapy with VIEKIRA PAK, reduce cyclosporine cyclosporine dose to 1/5th of the patient’s current cyclosporine dose. Measure cyclosporine blood concentrations to determine subsequent dose modifcations. Upon completion of VIEKIRA PAK therapy, the appropriate time to resume pre-VIEKIRA PAK dose of cyclosporine should be guided by assessment of cyclosporine blood concentrations. Frequent assessment of renal function and cyclosporine-related side effects is recommended. tacrolimus ↑ tacrolimus When initiating therapy with VIEKIRA PAK, the dose of tacrolimus needs to be reduced. Do not administer tacrolimus on the day VIEKIRA PAK is initiated. Beginning the day after VIEKIRA PAK is initiated; reinitiate tacrolimus at a reduced dose based on tacrolimus blood concentrations. Typical tacrolimus dosing is 0.5 mg every 7 days. Measure tacrolimus blood concentrations and adjust dose or dosing frequency to determine subsequent dose modifcations. Upon completion of VIEKIRA PAK therapy, the appropriate time to resume pre-VIEKIRA PAK dose of tacrolimus should be guided by assessment of tacrolimus blood concentrations. Frequent assessment of renal function and tacrolimus related side effects is recommended. LONG ACTING BETA-ADRENOCEPTOR AGONIST salmeterol ↑ salmeterol Concurrent administration of VIEKIRA PAK and salmeterol is not recommended. The combination may result in increased risk of cardiovascular adverse events associated with salmeterol, including QT prolongation, palpitations and sinus tachycardia. NARCOTIC ANALGESICS buprenorphine/naloxone ↑ buprenorphine ↑ norbuprenorphine No dose adjustment of buprenorphine/naloxone is required upon co-administration with VIEKIRA PAK. Patients should be closely monitored for sedation and cognitive effects. PROTON PUMP INHIBITORS omeprazole ↓ omeprazole Monitor patients for decreased effcacy of omeprazole. Consider increasing the omeprazole dose in patients whose symptoms are not well controlled; avoid use of more than 40 mg per day of omeprazole. SEDATIVES/HYPNOTICS alprazolam ↑ alprazolam Clinical monitoring of patients is recommended. A decrease in alprazolam dose can be considered based on clinical response. The direction of the arrow indicates the direction of the change in exposures (Cmax and AUC) (↑ = increase of more than 20%, ↓ = decrease of more than 20%, ↔ = no change or change less than 20%). Drugs without Clinically Signifcant Interactions with VIEKIRA PAK No dose adjustments are recommended when VIEKIRA PAK is co-administered with the following medications: digoxin, duloxetine, emtricitabine/tenofovir disoproxil fumarate, escitalopram, methadone, progestin only contraceptives, raltegravir, warfarin and zolpidem. USE IN SPECIFIC POPULATIONS Pregnancy Pregnancy Category B Pregnancy Exposure Registry There is an Antiretroviral Pregnancy Registry that monitors pregnancy outcomes in women who are HCV/HIV-1 co-infected and taking concomitant antiretrovirals. Physicians are encouraged to register patients by calling 1-800-258-4263. Risk Summary Adequate and well controlled studies with VIEKIRA PAK have not been conducted in pregnant women. In animal reproduction studies, no evidence of teratogenicity was observed with the administration of ombitasvir (mice and rabbits), paritaprevir, ritonavir (mice and rats), or dasabuvir (rats and rabbits) at exposures higher than the recommended clinical dose [see Data]. Because animal reproduction studies are not always predictive of human response, VIEKIRA PAK should be used during pregnancy only if clearly needed. If VIEKIRA PAK is administered with ribavirin, the combination regimen is contraindicated in pregnant women and in men whose female partners are pregnant. Refer to the ribavirin prescribing information for more information on use in pregnancy. Data Animal data In animal reproduction studies, there was no evidence of teratogenicity in offspring born to animals treated throughout pregnancy with ombitasvir and its major inactive human metabolites (M29, M36), paritaprevir, ritonavir, or dasabuvir. For ombitasvir, the highest dose tested produced exposures approximately 28-fold 2/17/2015 12:23:33 PM (mouse) or 4-fold (rabbit) the exposures in humans at the recommended clinical dose. The highest doses of the major, inactive human metabolites similarly tested produced exposures approximately 26-fold the exposures in humans at the recommended clinical dose. For paritaprevir, ritonavir, the highest doses tested produced exposures approximately 98-fold (mouse) or 8-fold (rat) the exposures in humans at the recommended clinical dose. For dasabuvir, the highest dose tested produced exposures approximately 48-fold (rat) or 12-fold (rabbit) the exposures in humans at the recommended clinical dose. Nursing Mothers It is not known whether any of the components of VIEKIRA PAK or their metabolites are present in human milk. Unchanged ombitasvir, paritaprevir and its hydrolysis product M13, and dasabuvir were the predominant components observed in the milk of lactating rats, without effect on nursing pups. The developmental and health benefts of breastfeeding should be considered along with the mother’s clinical need for VIEKIRA PAK and any potential adverse effects on the breastfed child from VIEKIRA PAK or from the underlying maternal condition. If VIEKIRA PAK is administered with ribavirin, the nursing mothers information for ribavirin also applies to this combination regimen (see prescribing information for ribavirin). Pediatric Use Safety and effectiveness of VIEKIRA PAK in pediatric patients less than 18 years of age have not been established. Geriatric Use No dosage adjustment of VIEKIRA PAK is warranted in geriatric patients. Of the total number of subjects in clinical studies of VIEKIRA PAK, 8.5% (174/2053) were 65 and over. No overall differences in safety or effectiveness were observed between these subjects and younger subjects, and other reported clinical experience has not identifed differences in responses between the elderly and younger subjects, but greater sensitivity of some older individuals cannot be ruled out. Hepatic Impairment No dosage adjustment of VIEKIRA PAK is required in patients with mild hepatic impairment (Child-Pugh A). VIEKIRA PAK is not recommended in HCV-infected patients with moderate hepatic impairment (ChildPugh B). VIEKIRA PAK is contraindicated in patients with severe (Child-Pugh C) hepatic impairment [see Contraindications]. GIHEP_39.indd 03-B026 Viekira Pak PB 10.5x13 (1.25).indd 2 Renal Impairment No dosage adjustment of VIEKIRA PAK is required in patients with mild, moderate or severe renal impairment. VIEKIRA PAK has not been studied in patients on dialysis. For patients that require ribavirin, refer to the ribavirin prescribing information for information regarding use in patients with renal impairment. Other HCV Genotypes The safety and effcacy of VIEKIRA PAK has not been established in patients with HCV genotypes other than genotype 1. OVERDOSAGE In case of overdose, it is recommended that the patient be monitored for any signs or symptoms of adverse reactions and appropriate symptomatic treatment instituted immediately. PATIENT COUNSELING INFORMATION Advise the patient to read the FDA-approved patient labeling (Medication Guide). Inform patients to review the Medication Guide for ribavirin [see Warnings and Precautions]. Risk of ALT Elevations Inform patients to watch for early warning signs of liver infammation, such as fatigue, weakness, lack of appetite, nausea and vomiting, as well as later signs such as jaundice and discolored feces, and to consult their health care professional without delay if such symptoms occur [see Warnings and Precautions and Adverse Reactions]. Pregnancy Advise patients to avoid pregnancy during treatment with VIEKIRA PAK with ribavirin. Inform patients to notify their health care provider immediately in the event of a pregnancy. Inform pregnant patients that there is an Antiretroviral Pregnancy Registry that monitors pregnancy outcomes in women who are HCV/HIV-1 co-infected and taking concomitant antiretrovirals [see Use in Specifc Populations]. Drug Interactions Inform patients that VIEKIRA PAK may interact with some drugs; therefore, patients should be advised to report to their healthcare provider the use of any prescription, non-prescription medication or herbal products [see Contraindications, Warnings and Precautions, and Drug Interactions]. Inform patients that contraceptives containing ethinyl estradiol are contraindicated with VIEKIRA PAK [see Contraindications and Warnings and Precautions]. Hepatitis C Virus Transmission Inform patients that the effect of treatment of hepatitis C virus infection on transmission is not known, and that appropriate precautions to prevent transmission of the hepatitis C virus during treatment should be taken. Missed Dose Inform patients that in case a dose of ombitasvir, paritaprevir, ritonavir is missed, the prescribed dose can be taken within 12 hours. In case a dose of dasabuvir is missed, the prescribed dose can be taken within 6 hours. If more than 12 hours has passed since ombitasvir, paritaprevir, ritonavir is usually taken or more than 6 hours has passed since dasabuvir is usually taken, the missed dose should NOT be taken and the patient should take the next dose as per the usual dosing schedule. Instruct patients not to take more than their prescribed dose of VIEKIRA PAK to make up for a missed dose. Manufactured by AbbVie Inc., North Chicago, IL 60064. VIEKIRA PAK and NORVIR are trademarks of AbbVie Inc. All other brands listed are trademarks of their respective owners and are not trademarks of AbbVie Inc. The makers of these brands are not affliated with and do not endorse AbbVie Inc. or its products. Ref: 03-B026-R2-Revised December, 2014 046-1658504 MASTER 046-1574501 2/18/2015 4:43:02 PM 40 UPPER GI TRACT MAY 2 0 1 5 • G I & HEPATO LO G Y NEW S CLINICAL CHALLENGES AND IMAGES Answer to “What’s your diagnosis?” on page 2: Retrograde jejunogastric intussusception etrograde jejunogastric intussusception ( JGI) is a rare complication of gastric surgery with an unknown mechanism; the lapse of time between surgery and occurrence has been reported as being from 2 days to 30 years.1 There are three anatomic types of JGI that have been previously described by Shackman:2 Type I, aferent loop intussusception; type II, eferent loop intussusception; and type III, a combined form. In this case, type II JGI was present; this form has been reported most commonly (80%). The presence of a tender mass with vomiting and pain in a patient with a history of prior gastric surgery is the typical presentation. However, most reported cases have not been diagnosed preoperatively. The current state-of-the-art CT allows for the detection of the characteristic target-shaped soft-tissue mass with adjacent mesenteric vessels within the stomach; this is pathognomonic for JGI.3 The treatment of acute retrograde JGI is prompt surgery with reduction and resection of the gangrenous bowel and revision of the anastomosis, depending on the patient’s condition during the operation. In this case, contrast-enhanced CT scan showed retrograde jejunojejunal (Figure B, black arrow) and jejunogastric intussusception (Figure B, white arrow) via the gastrojejunostomy anastomosis (Figure B, dashed arrow). An emergency exploratory laparotomy showed AGA InstItute R an eferent loop jejunum of 25 cm long herniating into the stomach leading to the retrograde intussusception (Figure C). The intussuscepted loop had gangrenous changes and was resected; an end-to-end jejunojejunal anastomosis was performed. The postoperative recovery was uneventful, and the patient was discharged after 22 days of hospitalization. The pathology report showed hemorrhagic necrosis of the resected bowel, but no malignant changes were found. References 1. Conklin E.F., Markowitz A.M. Intussusception, a complication of gastric surgery. Surgery 1965;57:480-8. 2. Shackman R. Jejunogastric intussusception. Br. J. Surg. 1940;27:475-80. 3. Azar T., Berger D.L. Adult intussusception. Ann. Surg. 1997;226:134-8. [email protected] PRACTICE ECONOMICS GIHEP NEW S. COM • M AY 2015 41 Value-based payment: Time to start getting ready BY WHITNEY McKNIGHT Frontline Medical News WASHINGTON – Are physicians ready for the shift toward value-based compensation? A report from the American Medical Association and the RAND Corp. aims to get physicians thinking about what investments they should expect to make and what obstacles they may encounter as they prepare for the federal government’s switch from fee-forservice to value-based medicine in 2018. “There is a lot of enthusiasm for change,” Dr. Mark W. Friedberg, senior natural scientist at RAND in Boston and lead researcher on the report, said in an interview. “There is a lot of hope this will result in better patient care and physician success. It’s a matter of the details.” The report is based on survey data from 34 practices across the country, all of which have some form of alternative payment structure in place, whether it be accountable care or bundled services. Practices were located in rural and urban settings ranging from hospital- to physician-owned or corporately managed, all with varying sizes of patient panels. The top concern that practice managers faced was matching the appropriate alternative payment model to their particular patient population, researchers found. Other concerns included how best to use incentives without adversely afecting patient care and how to avoid physician burn-out. These concerns, Dr. Friedberg said, point to a need for payers to ofer guidance about what makes sense when and why. “We got the message that more communication between payers and physician practices tends to be a good thing.” Many of the coming changes will require updated technology. Finding the money for such an overhaul is a universal preoccupation of many practice man- agers, and another reason some practices have yet to switch. “Some of the time, practices can get a loan, or have the reserves to do it on their own, but sometimes they don’t and they need to partner with a large organization like a hospital or a large physician group,” Dr. Friedberg said. Payers are not likely to help foot the bill, according to Susan DeVore, president and chief executive ofcer of Premier Health, a performance improvement alliance of hospitals and other providers. “It would be wonderful if the health plans would ‘There is a lot spend hundreds of millions of hope this will of dollars for the technology result in better enablement of the physician patient care practices and the health sysand physician tems,” Ms. DeVore said at the success.’ press conference. “The truth is, health systems and physiDR. FRIEDBERG cians are [already] spending the billions to build these technology infrastructures, and they need to do that together.” She called for more systemwide transparent collaboration in how cost is determined and in how quality and outcomes are measured. “It’s not fair to say we need a coordinated system of care, but then we can’t do it for lots of regulatory reasons,” she said, noting that ultimately, she believed such information sharing would be determined by Congress. Payers should make sure that physicians and other providers have a seat at the table when performance metrics are determined, Dr. Friedberg said. “Some of the concerns we heard were that, in Value-based transition SGR repeal from page 1 Act of 2015 (MACRA). “Anytime a complex bill as helpful as this one is passed, there are implementation problems that sometimes arise, so one of the areas that we will be strongly attentive to at the AMA is keeping our fnger on the pulse of the implementation and working with the federal government to make sure that this tracks in a correct way.” President Obama signed the bill into law on April 16. The new law repeals the Medicare Sustainable Growth Rate formula, negating the 21% physician fee cut that was to go into efect April 1. In its place, the law provides a 0.5% pay increase yearly for 5 years as the Medicare program makes the transition away from fee-for-service and to val- ue-based payment. To help get to a point of value over volume, the bill consolidates existing quality programs – including those addition to the number of measures, was also whether individual measures are clinically valid, and do they really refect true diferences in the quality of the patient care. Is it possible that the measure isn’t really reliable and not adequately risk MS. DEVORE adjusted, and therefore might not be ready for prime time in a payment contract?” Although the report did not ofer specifc time frames practice managers could expect before a new structure would take hold, Ms. DeVore said she was aware of some practices that realized more than a third more profts within 3 years of switching to value-based care models. Chet Burrell, president and CEO of CareFirst BlueCross BlueShield, said his group’s experience was that overall, physicians were not ready for the change to value-based care. This, despite the insurer’s announcement that $1 in every $5 it spends on reimbursement is now tied to quality care. For physicians who are ready to make the shift to value-based payment, Mr. Burrell said an average of 5 years was necessary to fully integrate. “Each practice is its own ecosystem. Some physicians catch on very ‘Some physicians quickly, but some are hostile.” catch on very Through our Roadmap to quickly, but some the Future of GI Practice, AGA are hostile.’ has been developing resources to prepare you for value-based MR. BURRELL reimbursement systems. If you haven’t started to demonstrate and measure quality, it’s more important than ever to put processes in place. Learn more at www.gastro. org/roadmap-to-the-future-of-gi. Systemwide collaboration is needed in how cost is determined and quality is measured. and our House of Delegates, and the conclusion was that this was not just an improvement, but a signifcant improvement, over the current set of measurements,” Dr. Madara said. The new law also incentivizes physicians to use alternate payment models that focus on care coordina- This is a signifcant improvement over the current set of measurements. The bill ‘ensures that these federal rules are not misused for purposes for which they were never intended.’ DR. MADARA MR. ATCHINSON regarding the meaningful use of electronic health records – into a single value-based performance program. “We studied that, along with some of the other physician organizations tion and preventive care with a 5% payment bonus. It pushes for more transparency of Medicare data for physicians, providers, and patients. MACRA also includes funding to [email protected] On Twitter @whitneymcknight help smaller practices participate in alternative payment models or the streamlined quality measurement program, as well as funding to help in the development of quality measures. “The provisions that allow for continued funding of the quality measurement enterprise in H.R. 2 are a key building block of this important transition and will also facilitate work to continue advancing measurement science,” the National Quality Forum said in a statement. “Ultimately, these eforts will not only help people get better healthcare, but also will reduce costs that strain patients, purchasers, and the system overall.” Other important provisions in the new law include the reauthorization of several key programs. CHIP (the Children’s Health Insurance Program), the Community Health Center program, the National Health Continued on following page 42 PRACTICE ECONOMICS Continued from previous page Service Corps, and the Teaching Health Centers program were all reauthorized for 2 years; they had been scheduled to expire later this year. Additionally, the law continues a partial delay of the Medicare two-midnights rule until Sept. 30. Physicians also cheered provisions of the new law that allay malpractice concerns. The law specifes that the development, recognition, or implementation of any federal health care guideline or standard does not establish a duty of care in medical malpractice claims. The provision helps distinguish government quality guidelines and payment rules from medical liability standards, according to Brian K. Atchinson, president and CEO of PIAA, a national trade association for medical malpractice liability insurers. “None of these rules or guidelines were created with the intent to establish a legal standard for negligence, and so it makes sense for Congress to clarify that fact,” Mr. Atchinson MAY 2 0 1 5 • G I & HEPATO LO G Y NEW S said in an interview. “The standard of care provision in the SGR fx bill does just that, and nothing more. It does not shift the playing feld to either plaintifs or defendants. Instead, it ensures that these federal rules are not misused for purposes for which they were never intended.” H.R. 2 ran into some trouble in the Senate because it does not have a dedicated funding mechanism to cover its full cost. The Congressional Budget Ofce estimated that enactment of the law will increase the defcit by $141 billion over 10 years. The CBO’s score also found that the legislation would save money, compared with the price of continued patches. A total of $73 billion of the $214 billion cost of the package is ofset through spending reductions and revenue increases included in the bill, the CBO found. These include income-related premium adjustments for Medicare Parts B and D, Medigap reforms, an increase of levy authority on payments to Medicare providers with delinquent tax debt, adjustments to inpatient hospital payment rates, a delay of Medicaid Disproportionate Share Hospital changes until 2018, and a 1% market basket update for postacute care providers. Enactment of the law also looked a bit shaky when the Ofce of the Actuary for CMS released a report April 9 that suggested physicians would see future payment cuts under the law. “Physician payment rates under H.R. The provisions that allow for continued funding of the quality measurement enterprise in H.R. 2 are a key building block of this important transition and will also facilitate work to continue advancing measurement science. GICareerSearch com Looking for a new career or a new staff member? Job Seekers: Search jobs, fnd career advice and post your resume. Employers: Access qualifed candidates in the GI feld. Start your search today at GICareerSearch.com. 2 would be lower than scheduled under the current SGR formula by 2048 and would continue to worsen thereafter,” according to the report. “Absent a change in the method or level of update by subsequent legislation, we expect access to Medicare-participating physicians to become a signifcant issue in the long term under H.R. 2.” However, the AMA’s Dr. Madara said that he was not concerned about the projections because the report assumes no changes in coming years. “One does not make linear trajectories over a period of decades or more and assume that that’s where we are going to end up because that assumption is that nothing happens in the interim and, as we all know, that’s just simply not the way life works,” he said. AMA President Robert Wah noted that the report “fails to take into account the long-range impact such a drastic payment cut [due to the SGR] would have on quality and access for Medicare benefciaries, or the many options H.R. 2 will make available to physicians for avoiding onerous penalties under current law and the signifcant positive updates that high performers can earn.” 525-500COM_14-4 [email protected] PRACTICE ECONOMICS GIHEP NEW S. COM • M AY 2015 43 PRACTICE MANAGEMENT TOOLBOX: ACOs can be an opportunity for gastroenterologists BY G. ANTON DECKER, MBBCH, MRCP, FACG, CPE, MHA This month’s article comes from Dr. G. Anton Decker. Dr. Decker is one of the few board-certifed gastroenterologists who is in a leadership position of a functioning accountable care organization (ACO). As such, his insights into ACO workings and funds fow are especially important. As we continue to note health system consolidation and changes in the formulas by which reimbursements are distributed, gastroenterology has a lot at stake. We are fortunate to have several gastroenterologists in leadership positions within large integrated delivery networks. John I. Allen, M.D., MBA, AGAF, Special Section Editor A s a practicing gastroenterologist and chief medical ofcer of a large medical group participating in the Pioneer Accountable Care Organization (ACO) program, I have an encouraging view of health care transformation. Banner Medical Group (BMG), Banner Health’s employed medical group, has a presence in six states and employs more than 1,000 physicians. BMG is part of Banner Health Network (BHN), Banner Health’s ACO. Banner Health chose to form an ACO to maintain its competitive advantage and improve patient health and experience by providing coordinated and cost-efective care. My journey from a clinical gastroenterologist to a chief medical ofcer immersed in the challenges and opportunities of health care reform has been exciting and educational. From gastroenterologist to chief medical offcer I enjoyed clinical gastroenterology but became equally fascinated by more global health care challenges; the United States spends an unsustainable $8,402 per capita on health care,1 far higher than any other developed country, and yet it does not achieve superior outcomes or life expectancies. To obtain a seat at the table where health care delivery decisions are made, I sought out oppor- tunities to expand my knowledge and credibility in the science of health care delivery: I volunteered for committees such as Quality, Electronic Medical Record, and Practice Operations. I read books and journals on health care economics, business, leadership, and management. Finally, I pursued a master’s degree in health administration and became a certifed physiDR. DECKER cian executive through the American College of Physician Executives Program. Although a radical career move, the position of chief medical ofcer of BMG provided me the opportunity to be on the forefront of health care reform. Before my arrival, BHN received approval from the Centers for Medicare & Medicaid Services (CMS) to be a Pioneer ACO, 1 of 32 such ACOs in the country. I had to rapidly learn the rules of CMS ACOs and position the medical group to succeed as a component of BHN. A failed attempt at reading through the Patient Protection and Afordable Care Act (ACA)2 led me to search for articles and books on ACOs; however, most were outdated and based on 1990s managed care programs. My most useful sources of information were the administrative leaders of health plans and BHN, who had frsthand knowledge of and literature on the “rule book” because they had communicated directly with CMS during the application and formation of Banner’s Pioneer ACO. My eyes were opened to the true costs of health care and the complexity of an uncoordinated health care system riddled with stakeholders. Accountable care organizations A common misconception is that an ACO is a government invention or designation. An ACO is simply a group of providers who agree to be accountable for the quality, cost, and overall care Continued on page 46 44 MAY 2 0 1 5 • G I & HEPATO LO G Y NEW S CLASSIFIEDS Also available at MedJobNetwork.com PROFESSIONAL OPPORTUNITIES WHERE A LANDSCAPE OF OPPORTUNITIES AWAITS A GASTROENTEROLOGIST Large GI GROUP PRACTICE SEEKS NEW PHYSICIAN for Reno and Carson City, NV: Te largest and premier Northern, NV Gastroenterology group practice of nineteen (19) gastroenterologists plus three (3) PA’s is recruiting a new physician at our Reno and Carson City, NV ofce locations. Our physician owned practice includes facilities at fve (5) locations within the Reno, Carson City and Gardnerville areas. Our Reno ofces are located in beautiful buildings, which include state of the art endoscopy centers. We are on the cutting edge of technological and industry advances with our practice management system, electronic healthcare record, EUS, pediatric services, anesthesia services, and a Pathology Lab. Our city is adjacent to the breath taking Lake Tahoe area and at the base of the beautiful snowcapped Sierra Nevada Mountains. Boasting 300 days of sunshine, our area provides both summer and winter recreational activities with skiing, kayaking, hiking, boating and biking among the most popular. We are within forty-fve minutes of ffeen world class ski resorts and 90 minutes of thirty golf courses. In addition to our location to the Sierra’s, we are only a four (4) hour drive to San Francisco. We ofer an attractive compensation and beneft package to our new associate physicians, plus the opportunity for practice and ancillary service ownership. Candidates must be board eligible or board certifed in gastroenterology. Gundersen Health System in La Crosse, Wisconsin is seeking a BC/BE Gastroenterologist to join its established medical team. Practice in our state-of-the-art Endoscopy Center and modern outpatient clinic. Outreach services are provided at our satellite clinics located within an easy drive from La Crosse. In addition, you will have opportunities for clinical research and will be actively involved in teaching our Surgical, Transitional, and Internal Medicine residents. You’ll join a physician-led, not-for-proft health system with a top-ranked teaching hospital and one of the largest multi-specialty group practices with about 700 physicians and associate medical staf. Visit gundersenhealth.org/MedCareers Send CV to Kalah Haug Medical Staf Recruitment Gundersen Health System [email protected] or call (608)775-1005. DIRECT CONTACT INFORMATION If you are interested in joining our team, please contact our Chief Operating Ofcer, Mr. Tomas Klim at 775-284-4620 or send your CV directly by fax to 775-327-8868 or email at [email protected]. To learn more about our organization, please refer to our website at www.giconsultants.com GASTROENTEROLOGY OPPORTUNITY Cape Fear Center for Digestive Diseases growing Gastroenterology practice in Fayetteville, NC, is seeking a full-time BC/BE Gastroenterologist. Join a busy practice with 5 physicians and four mid-level providers that offer outpatient care at our practice owned endoscopy center, Digestive Health Endoscopy Center. Inpatient care is provided at Cape Fear Valley Health System, the 9th largest health system in the state with 765 patient beds, serving more than 935,000 patients annually. ABOUT THE PRACTICE • Practice established since 1984 • Full range of endoscopy including ERCP and capsule endoscopy • Practice owned endoscopy center ABOUT THE POSITION • ERCP/EUS experience necessary • Desirable call arrangement with one hospital • Partnership track with strong, reputable group • State of the art infrastructure • Outstanding quality of life in a family oriented community, with excellent schools and low cost of living. • Easy access to beach and mountains For more information about this great opportunity contact: Rita Graves, Practice Administrator [email protected] (910) 323-2477 EEO/AA/Veterans/Disabilities FIND YOUR NEXT JOB AT MEDJOBNETWORK com Physician NP/PA Career Center The frst mobile job board for Physicians, NPs, and PAs Mobile Job Searches—access MedJobNetwork.com on the go from your smartphone or tablet Advanced Search Capabilities—search for jobs by specialty, job title, geographic location, employers, and more Scan this QR code to access the mobile version of MedJobNetwork.com For Deadlines and More Information, Contact: Linda Wilson Tel: (973) 290-8243, Email: [email protected] 45 GIHEP NEWS. COM • M AY 2015 CLASSIFIEDS Also available at MedJobNetwork.com PROFESSIONAL OPPORTUNITIES If contributing to a team with an expectation for excellence and creating a balanced and fulfilling life are important to you, St. Vincent Healthcare in Billings, Montana has the opportunity and community for you! St. Vincent Healthcare in Billings, Montana seeks U.S. trained BE/BC certified physicians for our Gastroenterologist Clinic • • • • • • • • • • • • Full time employed position Physician will practice the full scope of general gastroenterology Skills in ERCP and/or EUS would be a plus. State of the art GI Diagnostic Center: Call responsibilities are 1:3 Hospital is staffed for 220 beds and is a Level II Trauma Center SVH is a regional destination hospital with a full complement of medical specialties available. Thriving medical community in a family-oriented suburban location Excellent School Systems Abundant recreational activities year round – hiking, skiing, fishing, biking and camping Competitive salaries with productivity incentives Start date bonus, Moving Allowances and CME reimbursement For more information, please contact Therese Teske, Physician Recruiter at (406) 237-4017 [email protected] or visit our website at www.svh-mt.org ************ Billings, Montana listed 4th in cities with highest satisfaction – Business Insider, Gallup 2014 Additional Gastroenterologist Wanted for Established Group Full or Part-Time Our Gastroenterology group of 4 Board Certified GIs, located in Palos Heights, IL, just 25 miles from downtown Chicago is seeking a full or part time BE/BC gastroenterologist. This well respected practice has enjoyed an excellent reputation in the community for many years and maintains a close relationship with our local hospital—Palos Community Hospital. The group also performs GI procedures at two ambulatory surgical centers in the area. The demand for GI services has remained strong in our area and we anticipate an industrious physician will be immediately able to fill an office schedule, a surgical schedule as share in weekend call among 3 other gastroenterologists. Our salary and benefits package are very competitive, and the opportunity exists to own shares in a surgical center. Send CV to Maura O’Reilly at [email protected] or call (708) 361-4089 PRESBYTERIAN HEALTHCARE SERVICES Albuquerque, NM Presbyterian Healthcare Services is seeking Board Certified Gastroenterology trained physicians to join our established practice of 11 physicians, 2 Gastroenterology Hospitalists and 7 midlevels. Our medical group employs more than 600 primary care and specialty providers and is the fastest growing employed physician group in New Mexico. Presbyterian Healthcare Services is a locally owned, not-for-profit organization based in Albuquerque. Our integrated healthcare system includes eight hospitals in seven New Mexico cities, a medical group, multispecialty clinics and a health plan (over 400,000 members). We have been proudly providing care to New Mexicans for 105 years. In addition to a guaranteed base salary we also offer a sign on bonus, incentive bonus, malpractice, relocation, house hunting trip, health, dental, vision, 403(b) w/ contribution from PHS 457(b), short & long term disability, CME allowance, etc. Albuquerque thrives as New Mexico’s largest metropolitan center with a population of 700,000. Albuquerque has been listed as one of the best places to live in the United States by Newsweek, U.S. News & World Report, Money and Entrepreneur Magazines! Albuquerque is considered a destination city for most types of outdoor activities with 310 days of sunshine. A truly diverse and multicultural city, Albuquerque offers you and your family a great variety of activities and entertainment including national theater productions, sporting events, golf courses ranked among the best in the country, the largest hot air balloon festival in the US, American Indian Cultural activities and much more. For more information, e-mail Kelly Herrera at [email protected] or call 1-505-923-5662. Visit our website at www.phs.org EOE EXCELLENT OPPORTUNITY Well established, successful hospital owned GI group in Cincinnati, Ohio is seeking a gastroenterologist due to growth and expansion. Our twenty one member physician group needs a general gastroenterologist to work in Northern Cincinnati, beautiful Oxford, Ohio, home to Miami University. Candidates should be board certifed or board eligible, able to work in a team atmosphere, possess an excellent bed-side manner, goal oriented with strong clinical endoscopic skills. Our practice ofers expertise in the clinical realm through performing diagnostic and therapeutic endoscopy, ERCP, EUS and dedicated Hepatologists. Within our system we also are doing research and training of primary care residents. Despite being a large group, we still maintain small group camaraderie. We ofer a very competitive starting salary with benefts and opportunities for performance bonuses, retirement plans, group insurance plans (health, dental, malpractice, disability), and an equal voice from the beginning. The group has a very favorable call schedule which means working only 14-15 weekends a year. Our ideal candidates will have outpatient and inpatient clinical responsibilities. If you are looking to join a reputable, fnancially stable and well-established practice, please give us a call. Please contact: Greg Bush via email at [email protected] or by phone at 513-569-6661 or Dr. Allan Peck via email at [email protected] or by phone at 513-853-9321. 46 PRACTICE ECONOMICS Continued from page 43 of their benefciaries. An ACO may have diferent ACO programs, which generally fall into two categories: commercial ACO programs, initiated by private payers; and government ACO programs, initiated by CMS. Government ACOs After the passing of the ACA, CMS initiated two ACO pilots: the Medicare Shared Saving Program (MSSP), administered by CMS; and the Pioneer ACO program, administered through the Center for Medicare & Medicaid Innovation, a CMS subsidiary.2 The goal for these ACO programs is to achieve the Triple Aim, as defned by the Institute for Healthcare Improvement: improving the patient experience, improving the health of populations, and reducing the per capita cost of health care.3 Participation in either of these programs is voluntary and requires application to and approval by CMS. The Pioneer program was designed for organizations experienced with taking fnancial risk for a population and capable of providing coordi- MAY 2 0 1 5 • G I & HEPATO LO G Y NEW S nated care. Thirty-two organizations participated in the Pioneer program beginning January 2012. Starting in year 3 of the initiative, those organizations that have earned savings during the frst 2 years are eligible to move to a population-based payment arrangement and full-risk arrangements that can continue through optional years 4 and 5. Pioneer ACOs are required to develop similar outcomes-based payment arrangements with other private payers by the end of the second year. A Medicare benefciary (patient) is aligned by CMS with an approved ACO on the basis of the benefciary’s pattern of utilization during a 3-year alignment period. It is the ACO’s decision on how to attribute the benefciary to a primary care provider. After CMS aligns a benefciary with an ACO, the ACO is required to notify the benefciary of their participation. Benefciaries aligned with an ACO maintain full benefts under the Medicare fee-forservice system and do not need a referral to see a specialist inside or outside the ACO. One of the key features that diferentiate these modern ACOs from managed care programs in the 1990s is CLASSIFIEDS Also available at MedJobNetwork.com CONTINUING EDUCATION MASTER YOUR GI BOARDS with the latest, most extensive GI prep book Diagnostic Gastroenterology by Perry Hookman, M.D. Now available on Amazon.com Give to the American Cancer Society. ® Disclaimer GI & HEPATOLOGY NEWS assumes the statements made in classified advertisements are accurate, but cannot investigate the statements and assumes no responsibility or liability concerning their content. The Publisher reserves the right to decline, withdraw, or edit advertisements. Every effort will be made to avoid mistakes, but responsibility cannot be accepted for clerical or printer errors. For Deadlines and More information, Contact: Linda Wilson Tel: (973) 290-8243 Email: [email protected] Moving? Look to Classified Notices for practices available in your area. Take-away points: 1. Accountable care organizations provide new opportunities for gastroenterologists to be successful and to provide the best care for their patients. 2. Gastroenterologists and their practices should become leaders of payment reform and accurate quality reporting within their local health systems. 3. Gastroenterologists should seek out opportunities for fnancial risk sharing with payers so that they are rewarded for taking the best care of their patients. that patient movement is not restricted. Thus, a Pioneer ACO assumes responsibility for the total health care cost of the benefciaries attributed to its providers, even though these patients may choose to see providers outside of that ACO. At frst glance this seems unjust; however, it encourages the ACO to build relationships of trust with their patients on the basis of a strong primary care base and an integrated delivery model. By default, CMS shares benefciary claims data with the ACO. The ACO must give the benefciary written notifcation and the option of opting out of data sharing. Even when claims data are not shared with the ACO, the ACO is still responsible for that benefciary’s total spending and quality outcomes. In the Pioneer program, the percentage of fnancial savings (up to 75%) shared with the ACO is dependent on how the ACO performs against benchmarks for each quality measure. There are 33 quality measures in the domains of patient experience, care coordination and safety, preventative health, and at-risk populations. Only one measure, ACO 19, directly applies to gastroenterology: the percentage of patients aged 50-75 years who receive appropriate colorectal cancer screening (fecal occult blood test during the last 12 months, fexible sigmoidoscopy during the reporting period or the 4 years prior, or colonoscopy during the reporting period or 9 years prior). The door opener for performance points that contribute to a composite score for all measures is the 30th percentile (19.91%). After this, performance points are awarded according to a sliding scale. Reasons for exceptions, such as terminal illness, total colectomy, or colorectal cancer, must be documented. Patient noncompliance is not an acceptable exception. A percentage of CMS fnancial savings for the benefciaries in the ACO, with a predetermined cap, are distributed to the ACO. The ACO reimburses itself for administrative overheads and then distributes the remaining money with the providers on the basis of any prearranged agreement. CMS does not prescribe how the ACO distributes the savings to its providers. For example, an ACO may choose to reinvest the savings in infrastructure or distribute the savings with all its providers, or only the primary care providers. In the Pioneer model, the ACO is also at risk for fnancial loss up to a maximum of 15%. Pioneer and Medicare shared saving program ACO results to date By the end of year 2, ACOs in the CMS Pioneer ACO Model and MSSP generated over $372 million in program savings. In total, ACOs qualifed for shared savings payments of $445 million. Pioneer ACO year 1 and 2 results have been published. In year 1 the cost of care for Medicare benefciaries aligned with Pioneer ACOs grew by 0.3% in 2012, compared with 0.8% for non–Pioneer ACO–aligned benefciaries during the same period.4 Pioneer ACO benefciaries outperformed the control group in 15 clinical quality measures for which comparable data are available. At the end of year 1, nine organizations chose to leave the Pioneer Program, seven going over to the MSSP and two leaving the ACO programs entirely. During the second performance year, Pioneer ACOs generated estimated total savings of over $96 million and qualifed for shared savings payments of $68 million.5 The per capita growth in spending for the Pioneer ACO program was 1.4%, which is approximately 0.45% lower than traditional Medicare fee-for-service. At the end of year 2, Pioneer ACOs showed improvements in 28 of the 33 quality measures and experienced average improvements of 14.8% across all quality measures. BHN distributed Pioneer ACO savings at the end of year 1 and 2 to the networks in the ACO. The MSSP ACO results from year 1 only have been published. Fifty-three MSSP ACOs reduced spending $652 million below their targets and earned performance payments of more than $300 million. What do ACOs mean for gastroenterologists? Quality and payment data are becoming increasingly transparent not only to patients but also between providers, payers (including CMS), and health systems, which function like payers in an ACO model. CMS, private payers, and ACOs are highly motivated to meet the Triple Aim to remain fnancially viable and to attract new benefciaries.6,7,8 When viewed from the vantage point of the ACO or payer, this undertaking Continued on following page PRACTICE ECONOMICS GIHEP NEW S. COM • M AY 2015 Continued from previous page is daunting, and limited attention can be spent on each specialty because of the lack of resources. This creates the opportunity for gastroenterologists, gastroenterology groups, and their representative societies to be proactive in setting quality standards and putting forward bundled payment options.9 Quality measures Gastroenterology quality measures should be determined by gastroenterology societies. The appropriate use of quality data is dependent on the accuracy of the structured felds in the electronic medical record (EMR). Gastroenterologists must take a leading role in ensuring that the correct data are recorded in the EMR where they practice and that the data are recorded in a timely manner. By using colorectal cancer screening as an example, there are logistical details that must be agreed on: 1. Who is responsible for recording the performance of colon cancer screening in the EMR, whether that is the primary care doctor, the gastroenterologist, or someone else? 2. How and where is it documented when the screening was performed at another institution? 3. Is there an automatic feed from the endoscopy reporting software into the EMR after the performance of the colonoscopy, or is this a manual process; if so, by whom? Content from this column was originally published in the “Practice Management: The Road Ahead” section of Clinical Gastroenterology and Hepatology (2014;12:1769-72). “Practice Management Toolbox” provides key information and resources necessary for facing the unique challenges of today’s clinical practices. Resources for Practical Application: To view additional online resources about this topic and to access our Coding Corner, visit www/cghjournal.org/content/practice_management. Bundled payments Bundled payments are appealing to payers and ACOs not only because they potentially lower expenses but, more importantly, they make expenses predictable and improve ability to manage fnancial risk and to share this risk with providers. As an additional beneft to the health care system and patients, bundled payments require coordination of care. The American Gastroenterological Association convened a physician work group in 2012 that developed a framework for a colonoscopy bundled payment that includes the preprocedure, procedure, and postprocedure periods. Specifc payment for the bundle was not recommended but left to the local physicians and payers to negotiate. A recent publication in this journal by Minnesota Gastroenterology reports the deployment of a colonoscopy bundle with three local self-insured employers; however, specifcs of the fnancial arrangement and outcomes are not presented.8 BHN is presently working with AGA on colonoscopy and Crohn’s disease bundled payment options. Conclusion Gastroenterology societies have been successful lobbying for their members’ and patients’ interests. Individual gastroenterologists and their practices should also become leaders of payment reform and quality reporting within their local health systems. If they do not, quality measures and payment methodologies will be developed for gastroenterologists by payers who do not have the same knowledge of what should be measured and rewarded in the care of patients with digestive diseases. References 1. Centers for Disease Control and Prevention. Healthcare Expenditure. 2010. Available at: www.cdc. gov/nchs/fastats/hexpense.htm. Accessed Nov. 11, 2013. 2. Patient Protection and Afordable Care Act, 42 U.S.C. § 18001 et seq. (2010). H.R. 3590 (2010). 3. Berwick, DM, Nolan, TW, and Whittington, J. The triple aim: care, health, and cost. Health Af. (Millwood). 2008;27:759-69. 47 4. Centers for Medicare & Medicaid Services. Pioneer Accountable Care Organizations succeed in improving care, lowering costs. 2013. Available at: www.cms.gov/Newsroom/MediaReleaseDatabase/ Press-Releases/2013-Press-Releases-Items/2013-07-16.html. Accessed Nov. 11, 2013. 5. Centers for Medicare & Medicaid Services. Medicare ACOs continue to succeed in improving care, lowering cost growth. 2014. Available at: www.cms.gov/Newsroom/MediaReleaseDatabase/Fact-sheets/2014Fact-sheets-items/2014-09-16.html. Accessed Sept. 28, 2014. 6. Kislof, B. Accountable care organizations. Clin. Gastroenterol. Hepatol. 2012;10:442. 7. Rustgi, AK, Allen, JI. The house of gastrointestinal medicine: how academic medical centers can build a sustainable economic clinical model. Clin. Gastroenterol. Hepatol. 2013;11:1370-3. 8. Taylor, IL. Clinchy, RM. The Affordable Care Act and academic medical centers. Clin. Gastroenterol. Hepatol. 2012;10:828-30. 9. Ketover, SR. Bundled payment for colonoscopy. Clin. Gastroenterol. Hepatol. 2013;11:454-7. Dr. Decker is president of Mercy Health Physicians, Cincinnati. He has no relevant conficts of interest. [email protected] Quick Quiz Answers Q1: ANSWER: C Critique A recent Olmstead County, Minn., study was undertaken to understand the epidemiology of community-acquired C. difcile infections. In the cohort of 385 proven C. difcile infections, 41% were community acquired. Compared to cases acquired in the hospital, community C. difcile infections were observed in younger (B) females (A) who had lower comorbidity scores and fewer chronic illnesses (D). Also, these outpatient cases were less likely to have recent antibiotic exposure (E) and fortunately had less severe clinical courses. A large population-based study and several others have confrmed that the use of gastric acid–suppressive agents such as PPIs (C) increases the risk of C. difcile–associated disease (adjusted risk ratio 2.9, 95% CI: 2.4-3.4). References 1. Khanna S., Pardi D.S., Aronson S.L., et al. The epidemiology of community-acquired Clostridium difcile infection: a population-based study. Am. J. Gastroenterol. 2012;107:89-95. 2. Dial S., Delaney J.A., Barkun A.N., Suissa S. Use of gastric acid–suppressive agents and the risk of community-acquired Clostridium difcile-associated disease. JAMA 2005;294:2989. Q2: ANSWER: C Critique Sulfasalazine can cause reversible azoospermia and infertility. About 80% of patients taking sulfasalazine have semen abnormalities and 72% have oligospermia. Only one case of azoospermia has been reported in patients taking pure mesalamines. The sperm abnormalities are thought to be caused by the sulfapyridine moiety in the sulfasalazine molecule. Therefore, a switch from sulfasalazine to Asacol® or any other pure mesalamine is indicated. Sulfasalazine inhibits dihydrofolate reductase and can cause folate defciency. As a result, it should always be given along with oral folic acid supplementation. There is no clear evidence that 6-mercaptopurine afects male fertility. Holding both medications in a patient with UC would put him at increased risk of recurrence and should not be recommended. Withdrawal of an immunomodulatory agent such as 6-mercaptopurine or azathioprine in patients who are in remission can lead to rapid relapse in up to one-third of patients in 1 year and two-thirds within 5 years. Since 6-mercaptopurine is maintaining remission, there is no need for a switch to infiximab. An in vitro fertilization specialist might be required if there is no conception despite sulfasalazine withdrawal. References 1. Nielsen O.H., Munck L.K. Drug insight: aminosalicylates for the treatment of IBD. Nat. Clin. Pract. Gastroenterol. Hepatol. 2007;4:160-70. 2. Cassinotti A., Actis G.C., Duca P., et al. Maintenance treatment with azathioprine in ulcerative colitis: outcome and predictive factors after drug withdrawal. Am. J. Gastroenterol. 2009;104:2760-7. [email protected] Add the defnitive treatment for hemorrhoids to your practice. (And smiles to your patients’ faces.) It’s also now being performed by more than 1,900 physicians at 700 practices across the country. Join your colleagues and get started today. For more information, call 888.599.7949 x 1023 or visit www.crhmedicalproducts.com Your patients will thank you. GIHEP_48.indd 1 4/14/2015 4:49:03 PM



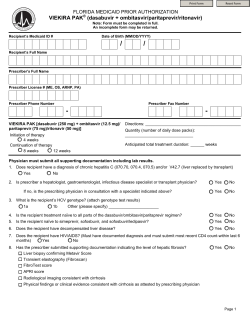






© Copyright 2026