
Update on MS Internal Medicine Comprehensive Review and Update 2012
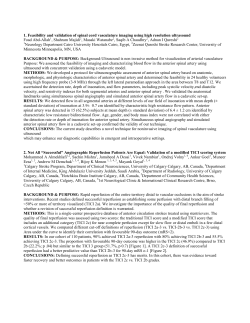
Update on MS Internal Medicine Comprehensive Review and Update 2012 June 7, 2012 Guy Buckle, MD, MPH Director of Clinical Care Partners MS Center Brigham & Women’s Hospital Assistant Professor Department of Neurology Harvard Medical School Boston, MA, USA Guy Buckle, M.D. Disclosures • • • • • • • • Acorda: Consultant/Advisor Bayer: Consultant/Advisor Biogen-Idec: Consultant/Advisor EMD-Serono: Consultant/Advisor Genzyme: Consultant/Advisor Novartis: Consultant/Advisor Questcor: Consultant/Advisor Teva Neuroscience: Consultant/Advisor Learning Objectives • The participant will be able to: – Discuss the epidemiology, possible etiology and risk factors for developing MS – Recognize common presenting signs and symptoms of MS – Discuss the development of diagnostic criteria for MS based on clinical presentation and MRI – Discuss the FDA-approved and newly emerging therapies for MS and their risks/benefits Overview • Epidemiology: Genetics and Risk Factors • MS Presentation: CIS, RIS, RRMS, SPMS, PPMS • Diagnostic Criteria: Old and new • FDA-Approved Therapies: Old drugs, new trials • Emerging Disease Modifying Therapies in Phase III: New drugs, new problems Epidemiology of MS • The most common chronic disabling disease affecting the CNS in young adults • Approximately 400,000 cases in the United States (1997). – Estimates range from 250,000 to 500,000 (probably higher). • The chances of developing MS are approx. 1:1000 in the general population • Incidence increases with distance from the equator • Estimated 2.5 million cases worldwide (probably more). • Highest incidence in Caucasians • Higher incidence in women (approximately 2.5:1) • MS strikes individuals between the ages 20-50, normally a time of peak productivity CNS = central nervous system. Compston A, et al. Lancet. 2002;359(9313):1221-1231. Frohman EM. Med Clin N Am. 2003;87(4): 867-897. Hogancamp WE, et al. Mayo Clin Proc. 1997;72(9):871-878. National Multiple Sclerosis Society. Who gets MS? http://www.nationalmssociety.org/about-multiple-sclerosis/who-gets-ms/index.aspx. Accessed January 8, 2009. Lage MJ, et al. Work. 2006;27(2):143-151. Economic Implications • Annual cost of MS in the United States is estimated at approximately $13.6 billion (in 1994 dollars) • Total lifetime direct and indirect costs per patient are estimated at approximately $2.4 million (in 1994 dollars) • Mean annual direct and indirect costs per patient total an estimated $47,215 (in 2004 dollars) • Mean direct healthcare costs incurred by insured patients with MS are 2 to 3 times higher than those without MS • Direct correlation between cost (direct and indirect) and severity of disease has been well-established • Therapeutics that modify MS activity and severity can result in both clinical and economic benefits Whetton-Goldstein K, et al. Mult Scler. 1998;4(5):419-425. Pope GC, et al. Neurology. 2002;58(1):37-43. Kobelt G, et al. Neurology. 2006;66(11):1696-1702. Patwardhan MB, et al. Mult Scler. 2005;11(2):232-239. O’Brien JA, et al. J Neurosurg Psychiatry. 2006;77:918-926. Age of Onset of MS Distribution of Patients According to the Decade of Life of MS Symptoms Onset 35 Patients (%) 30 25 20 15 10 5 0 0-10 11-20 21-30 31-40 Years Cardoso E, et al. Arq Neuropsiquiatr. 2006;64(3-B):727-730. 41-50 51-60 MS: Prevalence Pathogenesis of MS Infectious Agent Genetic Predisposition Abnormal Immunologic Response Cardoso E, et al. Arq Neuropsiquiatr. 2006;64(3-B):727-730. Environmental Factors MS Figure 1 The immunopathogenesis of the MS lesion. Overview of the components of the immune system that are involved in pathogenesis in MS, as discussed in the text. Dhib-Jalbut S , Marks S Neurology 2010;74:S17-S24 ©2010 by Lippincott Williams & Wilkins MS Genetics: Approximate Probability of Developing MS 1)Hauser SL, Goodin DS. Chapter 375. Multiple sclerosis and other demyelinating diseases. In: Harrison's Principles of Internal Medicine. Fauci AS, Braunwald E, Kasper DL, et al, eds. Available at: http://www.accessmedicine.com/content.aspx?aID=2906445. Accessed on: September 11, 2009. 2)Willer CJ, Dyment DA, Risch NJ, et al, and the Canadian Collaborative Study Group. Twin concordance and sibling recurrence rates in multiple sclerosis. Proc Natl Acad Sci U S A. 2003;100:12877-12882. Higher Vitamin D is Associated With Fewer T2 and Gd-Enhancing Lesions • • • • 469 subjects with clinically isolated syndrome or RRMS evaluated annually for 5 years by clinical evaluations, brain MRI, and blood draws Annual vitamin D (25-hydroxyvitamin D3) levels evaluated for association with subsequent development of: – New T2-weighted lesions – New Gd enhancing T1-weighted lesions – Clinical relapse of MS Each 10 ng/mL higher vitamin D level was associated with: – 15% lower risk of developing a new T2 lesion (P = 0.004) – 32% lower risk of developing a new Gd-enhancing lesion (P = 0.002) Higher vitamin D levels were associated with lower relapse rate (P not significant) Mowry E, et al. ECTRIMS/ACTRIMS 2011; Amsterdam, The Netherlands. Oral Presentation 129. Overview • Epidemiology: Genetics and Risk Factors • MS Presentation: CIS, RIS, RRMS, SPMS, PPMS • Diagnostic Criteria: Old and new • FDA-Approved Therapies: Old drugs, new problems • Emerging Disease Modifying Therapies in Phase III: New drugs, new problems Types of Multiple Sclerosis (MS) Relapsing-remitting Disability – Relapsing-remitting (RRMS) – Secondary Progressive (SPMS) – Primary Progressive (PPMS) – Progressive-relapsing (PRMS) Secondary Progressive Primary Progressive Progressive-relapsing Time Lublin FD, Reingold SC. Neurology. 1996;46(4):907-911 Clinical Manifestations • Fatigue • Bladder dysfunction • Pain • Bowel dysfunction • Depression • Cerebellar dysfunction • Numbness/paresthesias • Sexual dysfunction • Cognitive dysfunction • Gait abnormalities • Weakness/ Spasticity • Partial/complete paralysis • Visual loss/Optic neuritis National Multiple Sclerosis Society. http://www.nationalmssociety.org/about-multiplesclerosis/what-we-know-about-ms/symptoms/index.aspx. Accessed February 21, 2010. Natural History of MS Measures of brain volume Relapses and impairment MRI burden of disease MRI activity Preclinical RIS Secondary-Progressive Relapsing-Remitting CIS Time Comi. Opin Neurol. 2000;13:235; Munschauer. Clin Ther. 1997;19:868; Weinshenker. Brain. 1989;112:1422. Clinically Isolated Syndrome: Optic Neuritis • • 26 year-old woman with acute onset of monocular visual loss O.S. with pain on eye movement. Examination: Mild papilledema; Acuity of 20/200 w/ red desat. central scotoma and RAPD. Remainder of exam is normal. Clinically Isolated Syndrome: Optic Neuritis • Symptoms – Periocular pain (unilateral) on EOM – Monocular visual loss – Fading or blurring of vision – Uhthoff’s effect • Signs – Decreased visual acuity – Decreased color vision (red desaturation). – Decreased contrast sensitivity – Central scotoma – Relative afferent pupillary defect – +/-Disc swelling or pallor (chronic) Clinically Isolated Syndrome 1: Optic Neuritis Initial Findings on FLAIR MRI FLAIR = fluid-attenuated inversion recovery Clinically Isolated Syndrome 1: Discussion Points • • • • • Does this patient have MS? If not, what is her risk of developing CDMS? Would you perform a lumbar puncture? Would you treat with steroids? Would you recommend immunomodulatory treatment? – If yes, what type of treatment should be offered? – If no, how should this patient be followed? Clinically Isolated Syndrome 2: Transverse Myelitis • 23-year-old woman with gradual onset of tingling and numbness in her feet that ascends to the umbilicus over the next 4 days. • Exam shows a T8 sensory level to LT and temp. and reduced vibratory sensation with hyper-reflexia in the LE’s. The remainder of the neurological examination is normal. T2 T1 + Gd Clinically Isolated Syndrome 2: Transverse Myelitis • Patient is active and appears to be in good health. • No personal history of previous neurological disease. • There is no family history of neurological or autoimmune disease. • Patient c/o urinary frequency/urgency. • Unexplained fatigue since college. Basic Differential Diagnosis TM • Metabolic — Vit. B12, Copper deficiency • Infectious — Lyme, syphilis, HIV, HTLV-1 • Vascular — arteriovenous malformation (AVM) • Malignancy — intramedullary or extrinsic tumor • Inflammatory/autoimmune — SLE, Sjögren's, sarcoidosis, APLS, NMO • Structural — cervical spondylosis Clinically Isolated Syndrome 2: Initial Findings on Proton Density MRI Proton Density T1 w/Gd Sagittal FLAIR – Dawson’s Fingers Unlikely MS Perivenular Random Pathology of MS: Demyelination • Areas of demyelination • Followed by partial remyelination and gliotic scarring Used with permission from Florida State University College of Medicine. Axons Are Transected in MS Plaques and in NAWM SMI-32 (non-phosphorylated neurofilament) Trapp. N Engl J Med. 1998;338:278. Number of Transected Axons Increases With Level of Activity in MS Lesions 12,000 11,236 10,000 8,000 6,000 3,138 4,000 875 2,000 17 0.7 NAWM Control white 0 Active Chronic active edge Chronic active core (NAWM: normal-appearing white matter) Trapp BD, et al. N Engl J Med. 1998;338:278-285. Clinically Isolated Syndrome (CIS) Patients who present with clinically isolated syndrome (CIS) should be managed based on their risk of progression to MS: • In the Optic Neuritis Trial, risk at 10 years was: – 56% for patients with ≥1 lesion – 22% for patients with no lesions • In patients with CIS and no lesions, risk of MS at 14 years was: – 19% for clinically definite (CD) MS Brex et al. N Engl J Med. 2002;346:158-164. Optic Neuritis Study Group. Arch Ophthalmol. 2003;121:944-949. 12 EDSS Has Long Been a Standard Disability Measure accepted by FDA Expanded Disability Status Scale Death Normal neurological exam 0 0.5 1.0 Increased limitation in walking ability Minimal disability 1.5 2.0 2.5 3.0 3.5 4.0 4.5 5.0 Need for Restriction to walking wheelchair assistance 5.5 6.0 6.5 7.0 7.5 8.0 8.5 Helpless bed patient 10.0 9.0 9.5 Patient Disability Classification Expanded Disability Status Scale (EDSS): Rating system used by neurologists and clinical trial investigators to follow the progression of disability in MS. Kurtzke JF. Neurology. 1983;33(11):1444-1452. Median EDSS Score at Year 14 Number and Volume of T2 Lesions at Presentation Predict Disability 7 6 6 5 4 4 3 2 1.75 2 0 (0 cm3) 1 to 3 (0.6 cm3) 1 0 4 to 10 (0.9 cm3) >10 (5.6 cm3) Number (Median Volume) of T2 Weighted Lesions at Presentation Brex. N Engl J Med. 2002;346:158. Overview • Epidemiology: Genetics and Risk Factors • MS Presentation: CIS, RIS, RRMS, SPMS, PPMS • Diagnostic Criteria: Old and new • FDA-Approved Therapies: Old drugs, new problems • Emerging Disease Modifying Therapies in Phase III: New drugs, new problems Poser Criteria (1983) Define MS as “Clinically Definite” or “Probable” 8 • Clinically definite MS – A1: 2 attacks + 2 lesions – A2: 2 attacks + 1 lesion + 1 paraclinical lesion • Laboratory-supported definite MS – B1: 2 attacks + 1 lesion or 1 paraclinical lesion + abnormal CSF – B2: 1 attack + 2 lesions + abnormal CSF – B3: 1 attack + 1 lesion + 1 paraclinical lesion + abnormal CSF • Poser criteria also includes 2 additional categories – Clinically probable MS – Laboratory-supported probable MS Poser CM et al. Ann Neurol. 1983;13(3):227-231. McDonald Criteria (2001, rev. 2005) Incorporated MRI Measures Clinical (attacks) Objective lesions Additional requirements to make diagnosis 2 or more 2 or more • None; clinical evidence will suffice (additional evidence desirable but must be consistent with MS) 2 or more 1 1 2 or more 1 monosymptomatic 0 (progression from onset) 9 • Dissemination in space by MRI or positive CSF and 2 or more MRI lesions consistent with MS or further clinical attack involving different site • Dissemination in time by MRI or second clinical attack 1 • Dissemination in space by MRI or positive CSF and 2 or more MRI lesions consistent with MS AND • Dissemination in time by MRI or second clinical attack 1 • Positive CSF AND • Dissemination in space by MRI evidence of 9 or more T2 brain lesions or 2 or more cord lesions or 4–8 brain and 1 cord lesion or positive VEP with 4–8 brain lesions or positive VEP with less than 4 brain lesions plus 1 cord lesion AND • Dissemination in time by MRI or continued progression for 1 year McDonald WI et al. Ann Neurol. 2001;50(1):121-127. Diagnostic Criteria Vary Across DMD Pivotal Trials for Relapsing Forms of MS DMD Study group n IFN β-1b SC IFNB MS Study Group 372 Poser (“clinically definite” or “laboratory-supported definite” MS) IFN β-1a IM MSCRG 301 Poser (“clinically definite” MS) Glatiramer acetate Copolymer 1 MS Study Group 251 Poser (“clinically definite” or “laboratory-supported definite” MS) IFN β-1a SC PRISMS Study Group 560 Poser (“clinically definite” or “laboratory-supported definite” MS) Natalizumab AFFIRM Investigators 627 McDonald (17% in placebo arm met McDonald but not Poser definition of “clinically definite” MS) Only comparative, head-to-head studies allow evidence-based comparisons of efficacy and safety between drug products. 11 Diagnostic criteria used IFNB MS Study Group. Neurology. 1993;43(4):655-661. Jacobs LD et al. Ann Neurol. 1996;39(3):285-294. Johnson KP et al. Neurology. 1995;45(7):1268-1276. PRISMS Study Group. Lancet. 1998;352(9139):1498-1504. Polman CH et al. N Engl J Med. 2006;354(9):899-910. On-Treatment Annualized Relapse Rates Have Decreased Over Time Mean Event Rates in Major MS Clinical Trials 1.0 Mean Annualized Relapse Rate 0.91 0.9 0.87 0.84 McDonald criteria introduced 0.8 0.7 0.70 0.67 0.64 0.59 0.6 0.54 0.50 0.5 0.4 0.35 0.35 0.30 0.3 0.34 0.34 0.29 0.22 0.2 0.10 0.1 0.0 1992–2001 2002–2007 Only comparative, head-to-head studies allow evidence-based comparisons of efficacy and safety between drug products. A 32-year-old woman with left heminumbness and left leg weakness. No prior Patient Meets Criteria for MS Using the MAGNIMS medical history. Examination demonstrates diminished sensation in the left upper and lower extremities; 2010 mild weakness of the left leg with extensor Criteria plantar response and asymmetrically hyperreflexic. Brain MRI shows: Posterior fossa lesion Juxtacortical lesion Asymptomatic gadolinium-enhancing lesion Periventricular lesion Asymptomatic T2 lesion Images courtesy of Omar Khan, MD. Why Treat Early? • Relapses and impairment parallel the MRI burden of disease.1-3 • Axonal damage occurs early and may cause permanent neurological dysfunction.4 • Number of MRI lesions are predictive of future disability.5 • Preventing development of lesions may prevent progression of disability in patients.6 • Early treatment may delay mortality. 1. Comi. Curr Opin Neurol. 2000;13:235; 2. Munschauer. Clin Ther. 1997;19:868; 3. Weinshenker. Brain. 1989;112:1422; 4. Trapp. N Engl J Med. 1998;338:278; 5. Brex. N Engl J Med. 2002;346:158; 6. O’Riordan. Brain. 1998;121:495. Early Relapses Affect Long-Term Disability 100 Low (0―1 attacks in 2 years) Intermediate (2―4 attacks in 2 years) High (>5 in 2 years) Patients (%) 80 60 40 20 0 0 10 20 30 40 50 Time From Onset of MS (years) Actuarial analysis of disability: percentage of patients not having reached EDSS 6: difference between the groups significant (P<0.0001). Weinshenker. Brain. 1989;112:1422. Mortality for IFNβ-1b vs Placebo 21 Years After Randomization In Pivotal Trial 100 IFNβ-1b 250 µg Placebo Proportion of Patients Still Alive 95 90 85 80 78.3% of deaths MSrelated HR = 0.532 46.8% reduction in mortality risk P = 0.0173 75 70 65 0 At risk: INFβ-1b 250 µg 124 Placebo 123 5 10 124 120 121 117 15 Time (yrs) 118 109 Reder AT, et al. Presented at AAN; April 21-28, 2012; New Orleans, LA. Abstract P04.129. 20 104 88 25 Overview • Epidemiology: Genetics and Risk Factors • MS Presentation: CIS, RIS, RRMS, SPMS, PPMS • Diagnostic Criteria: Old and new • FDA-Approved Therapies: Old drugs, new trials • Emerging Disease Modifying Therapies in Phase III: New drugs, new problems FDA-Approved Therapies for MS: Immunomodulators Agents* Indications Doses and Administration 1996 Glatiramer acetate (Copaxone®) Relapsing-remitting MS 1st clinical episode and MRI consistent with MS 20 mg/d SC 1996 Low-dose IFNβ-1a (Avonex®) Relapsing forms of MS 1st clinical episode and MRI consistent with MS 30 mcg/wk IM 2002 High-dose IFNβ-1a (Rebif®) Relapsing forms of MS 1993 High-dose IFNβ-1b (Betaseron®, Extavia®) Relapsing forms of MS 1st clinical episode and MRI consistent with MS 22 mcg or 44 mcg tiw SC 250 mcg qod SC INFβ = interferon beta; SC = subcutaneous; IM = intramuscular; tiw = 3 times per week; qod = every other day *Trade names are included in this presentation to reduce confusion regarding medication formulations and in no way endorses the use of the product with the trade name. Copaxone. http://www.accessdata.fda.gov/drugsatfda_docs/label/2009/020622s057lbl.pdf Avonex. http://www.accessdata.fda.gov/drugsatfda_docs/label/2007/103628s5115lbl.pdf Rebif. http://www.accessdata.fda.gov/drugsatfda_docs/label/2005/103780s5062lbl.pdf Betaseron. http://www.accessdata.fda.gov/drugsatfda_docs/label/2003/103471s5032lbl.pdf Extavia. http://www.accessdata.fda.gov/drugsatfda_docs/label/2009/125290s0000lbl.pdf REGARD: Primary endpoint10 Survival distribution function 1.00 Rebif® (IFNβ-1a) 672 days (96 weeks) (n=386) 0.75 Hazard ratio: 0.94 95% CI: 0.74-1.21 P=0.643 0.50 0 100 200 COPAXONE® (glatiramer acetate injection) (n=378) 300 400 500 600 Time to first relapse (days) CI=confidence interval. A hazard ratio of 1 would indicate that the curves were exactly identical. 10. Mikol DD, et al. Lancet Neurol. 2008;7:903-914. No significant difference in: – Hazard rates for time to first relapse between the Rebif® and COPAXONE® groups – The proportion of patients who were relapse free over 96 weeks 0.25 0 • 700 REGARD: Safety and immunogenicity10 35 COPAXONE® (n=378) (glatiramer acetate injection) 30 Rebif® (IFNβ-1a) (n=386) Patients (%) 25 20 15 10 5 0 Injection site pruritis Injection site swelling Injection site Immediate induration post-injection drug reaction Flu-like illness Headache Adverse events 10. Mikol DD, et al. Lancet Neurol. 2008;7:903-914. Myalgia AAT elevation Dyspnea Depression BEYOND: Primary efficacy endpoint8,15 Relapse rate reduction vs pretreatment – There was no significant difference among the 3 treatment arms on the primary endpoint of risk for relapses – Relapse rate reductions during the study period of up to 3.5 years were similar in all 3 treatment groups ® 0 -20 -40 Betaseron 250 mcg (IFNβ-1b) COPAXONE® Betaseron® 500 mcg (glatiramer acetate injection) 79% 79% n=899 n=448 78% n=897 -60 -80 -100 During a double-blind, placebo-controlled pivotal trial, COPAXONE® reduced relapses by 29% vs placebo over 2 years (1.19 vs 1.68; P=0.055).4 4. Johnson KP, Brooks BR, Cohen JA, et al. Neurology. 1995;45:1268-1276. 8. Data on file, Teva Neuroscience, Inc. 15. BEYOND press release. Bayer HealthCare AG. Oct 29, 2007. FDA-Approved Therapies for MS: Immunosuppressive Agents* Indications Doses and Administration 2005 Natalizumab (Tysabri®)a Relapsing forms of MS 300 mg q4wk IV 2000 Mitoxantrone (Novantrone®)b SPMS, PRMS, worsening RRMS 12 mg/m2 over 5–15 min; q3mo IV infusion q4wk = every 4 weeks; q3mo = every 3 months *Trade names are included in this presentation to reduce confusion regarding medication formulations and in no way endorses the use of the product with the trade name. aCurrently used as 2nd-line therapy bOnly indicated for progressive and/or worsening disease; cumulative dose should not exceed 140 mg/m2 Natalizumab. http://www.accessdata.fda.gov/drugsatfda_docs/label/2008/125104s106lbl.pdf Mitoxantrone. http://www.accessdata.fda.gov/drugsatfda_docs/label/2009/019297s030s031lbl.pdf Natalizumab-Associated PML: Updated Incidence and Risk Stratification 3 2.77 Incidence per 1,000 patients 2.61 2.5 2.38 2.30 2 2.17 2.10 1.94 2.01 1.56 1.5 1.68 1.37 1 0.79 0.85 0.58 0.5 0.41 0.04 0 Post Marketing 1–12 13–24 25–36 37–48 49–60 Number of infusions PML risk lowest in anti-JCV Ab(-) pts: ≤ 0.10 cases/1,000 pts treated PML risk highest in pts with all 3 known risk factors (anti-JCV Ab(+), prior immunosuppressant use, and 25-48 months of tx): 10.6 cases/1,000 pts 232 cases of PML have been documented in patients treated with natalizumab as of May 3, 2012. Available at: http://chefarztfrau.de/?page_id=716 Bloomgren G, et al. Presented at AAN; April 21-28, 2012; New Orleans, LA. Abstract S41.001. Fingolimod (FTY720): Overview • Therapeutic class – Sphingosine-1-phosphate (S1P) receptor modulator • Molecular mechanism of action (MOA) – FTY720 binds to S1P receptors on lymphocytes – Circulating lymphocytes are sequestered in lymph nodes – Thought to reduce the infiltration of reactive effector T cells and macrophages into the CNS • Neurodegeneration/neuroprotection – Modulation of S1P receptors located within the CNS may lead to neuroprotective effects Mandala S, et al. Science. 2002;296:346-349. Kappos L, et al. N Engl J Med. 2006;355:1124-1140. Jaillard C, et al. J Neurosci. 2005;25:1459-1469. FREEDOMS: Key Efficacy Results Annualized Relapse Rate Disability Progression 0.4 30 - 60% versus placebo p < 0.001 FTY720 1.25 mg vs placebo HR = 0.68, p = 0.017 0.3 0.2 0.18 0.16 0.1 Placebo FTY720 0.5 mg vs placebo HR = 0.70, p = 0.024 25 % with 3-mo confirmed EDSS progression Annualized Relapse Rate 0.4 - 54% versus placebo p < 0.001 20 FTY 0.5 mg 15 FTY 1.25 mg 10 5 0 0 Placebo (n = 418) Fingolimod 0.5 mg (n = 425) Fingolimod 1.25 mg (n = 429) 0 90 180 270 360 450 Days on Study 540 630 http://www.novartis.com/downloads/investors/presentations-events/other-events/2009/20090930_fty720.pdf (accessed 2009-10-06) Adapted from Kappos L, et al. N Engl J Med. 2010;362(5):387-401. 720 TRANSFORMS: Primary Efficacy Endpoint Annualized Relapse Rate Annualized Relapse Rate at 12 months 0.4 0.33 -52% vs IFNβ-1a, P < 0.001 -38% vs IFNβ-1a, P < 0.001 0.3 0.20 0.2 0.16 0.1 0 IFNβ-1a 30 µg IM once weekly (n = 431) Oral fingolimod 0.5 mg (n = 429) Adapted from Cohen J, et al. N Engl J Med. 2010;362(5):402-415. Oral fingolimod 1.25 mg (n = 420) TRANSFORMS: Key Safety Data •Event, n (%) •Flu-like illness •IFNβ-1a 30 µg IM once weekly •(n = 431) •159 (36.9) •Oral fingolimod 0.5 mg (n = 429) •15 (3.5) •Oral fingolimod •1.25 mg (n = 420) •15 (3.6) •Pyrexia •77 (17.9) •18 (4.2) •15 (3.6) •Myalgia •44 (10.2) •14 (3.3) •14 (3.3) •Hepatic ALT elevation •8 (1.9) •28 (6.5) •24 (5.7) •Hypertension •8 (1.9) •16 (3.7) •21 (5.0) •Dyspnea •7 (1.6) •8 (1.9) •22 (5.2) •Malignancies •2 (0.5) •8 (1.9) •4 (1.0) •Bradycardia •0 (0.0) •2 (0.5) •10 (2.4) •Atrioventricular block •0 (0.0) •2 (0.5) •5 (1.2) •Herpes viral infections •1 (0.2) •1 (0.2) •3 (0.7)† ALT = alanine transaminase †Includes 2 fatal viral infections: primary disseminated varicella zoster and herpes simplex encephalitis Adapted from Cohen J, et al. N Engl J Med. 2010;362(5):402-415. Recent Additions to Fingolimod Prescribing Information • First Dose Monitoring: – Observe all pts for signs and symptoms of bradycardia for at least 6 hrs after first dose with hourly pulse and blood pressure measurement – Obtain ECG prior to dosing and at the end of the observation period – Pts who develop a heart rate < 45 bpm, or a new onset 2nddegree or higher AV block should be monitored until resolution – Pts at lowest post-dose heart rate at the end of observation period should be monitored until heart rate increases http://www.accessdata.fda.gov/scripts/cder/drugsatfda/index.cfm?fuseaction=Search.Label_ApprovalHistory#labelinfo http://www.msrc.co.uk/index.cfm/fuseaction/show/pageid/1309 Recent Additions to Fingolimod Prescribing Information • First Dose Monitoring (cont’d) – In pts experiencing symptomatic bradycardia, begin continuous ECG monitoring until symptoms have resolved; if pharmacological intervention is required for bradycardia, continuous ECG monitoring should continue overnight in a medical facility, and 1st-dose monitoring procedures should be repeated for the 2nd dose – Patients who may be less tolerant of fingolimod-induced bradycardia, are at higher risk of serious rhythm disturbance, or with prolonged QTc interval at baseline or at any time during the observation period should be observed overnight with continuous ECG monitoring • Patients who have stopped taking fingolimod and re-initialize treatment are advised to again follow these updated recommendations http://www.accessdata.fda.gov/scripts/cder/drugsatfda/index.cfm?fuseaction=Search.Label_ApprovalHistory#labelinfo http://www.msrc.co.uk/index.cfm/fuseaction/show/pageid/1309 Recent Additions to Fingolimod PI: Improving Patient Selection • Contraindications – Recent (within the last 6 months) occurrence of: myocardial infarction, unstable angina, stroke, transient ischemic attack, decompensated heart failure requiring hospitalization, or Class III/IV heart failure – History or presence of Mobitz Type II 2nd degree or 3rd degree AV block or sick sinus syndrome, unless patient has a pacemaker – Baseline QTc interval ≥ 500 ms – Treatment with Class Ia or Class III anti-arrhythmic drugs http://www.accessdata.fda.gov/scripts/cder/drugsatfda/index.cfm?fuseaction=Search.Label_ApprovalHistory#labelinfo http://www.msrc.co.uk/index.cfm/fuseaction/show/pageid/1309 Fingolimod Cardiac Effects and Safety in Clinical Practice – First dose observation (FDO) uneventful in 307/317 pts – 3 pts (0.9%) developed symptomatic sinus bradycardia • Seen only in pts with abnormal screening EKG • Those with low resting heart rate (HR) appear most at risk – 2 pts (0.6%) patients developed transient chest tightness – Significant decreases in HR, sBP, dBP, MAP observed 3 and 6 hrs after 1st dose • Average ∆ HR: -14.9%; maximal within first 3 hrs • 12 pts (3.8%) had HR drops of ≥ 30 bpm (all had baseline HR > 90 bpm) – Discontinuation rate at 3 months (9.5%) was higher than in clinical trials and mostly related to adverse events sBP = systolic blood pressure; dBP = diastolic blood pressure; MAP = mean arterial pressure Ontaneda D, et al. Presented at AAN; April 21-28, 2012; New Orleans, LA. Abstract P04.138. Ontaneda D, et al. Presented at AAN; April 21-28, 2012; New Orleans, LA. Abstract P04.130. New Therapies for MS • Oral Medications • Monoclonal Antibodies Teriflunomide*: TEMSO Efficacy Year Clinical Outcomes • Teriflunomide*1 – Parent compound used in treatment of RA (leflunomide) – Inhibits pyrimidine synthesis • Reversibly inhibits dihydro-orotate dehydrogenase, key enzyme in de novo pyrimidine synthesis – Inhibits T cell division • Alters tyrosine kinase activation of calcium mobilization • TEMSO (108-week, randomized, double-blind, placebo-controlled, parallelgroup, multicenter study)1,2 12-Week Confirmed Progression in Disability 23.7% – Inhibits EAE P = 0.084 27.3 0.54 2- 31.2% P = 0.0002 0.37 21.7 31.5% 29.8% P = 0.028 20.2 P = 0.0005 0.37 Placebo Teriflunomide Teriflunomide 14 mg 7 mg Placebo Teriflunomide Teriflunomide 14 mg 7 mg ARR TEMSO: Study of Teriflunomide in Reducing the Frequency of Relapses and Accumulation of Disability in Patients With MS *Investigational agent 1Tallantyre 2O’Connor E, et al. Int MS J. 2008;15:62-68. P, et al. ECTRIMS 2010; Gothenburg, Sweden. Abstract 79. Teriflunomide*: TEMSO Safety and Discontinuations AEs Placebo Teriflunomide 7 mg Teriflunomide 14 mg Any AE 87.5% 89.1% 90.8% Serious AE 12.8% 14.1% 15.9% Discontinuation AE 8.1% 9.8% 10.9% Serious Hepatic Disorders 2.5% 1.9% 2.5% ALT > 3 Times Upper Limit Normal 6.7% 6.3% 6.7% Serious Infections 2.2% 1.6% 2.5% n = 1088 patients randomized to teriflunomide (7 mg or 14 mg daily) or placebo 73.2% of patients completed treatment1 Leflunomide is pregnancy category X2 1O’Connor *Investigational agent P, et al. ECTRIMS 2010; Gothenburg, Sweden. Abstract 79. 2http://www.accessdata.fda.gov/drugsatfda_docs/label/2011/020905s022lbl.pdf. Accessed August 10, 2011. BG-12 CONFIRM: ARR (1o Endpoint) 44%*** 51%*** 29%* 0.401 0.224 0.198 0.286 Placebo (n = 363) BG-12 BID (n = 359) BG-12 TID (n = 345) GA (n = 350) 0.6 0.5 ARR 0.4 0.3 0.2 0.1 0 *P < 0.05; ***P < 0.0001 Fox R, et al. Presented at AAN; April 21-28, 2012; New Orleans, LA. Abstract S01.003. CONFIRM: MRI Outcomes (2° Endpoint) New or Enlarging T2 Hyperintense Lesions *** 71% *** 73% *** 54% 20 15 10 5 10 Adjusted Mean No. of Lesions Adjusted Mean No. of Lesions 25 New T1 Hypointense Lesions 5.1 4.7 8.0 *** 65% ** 41% 3.0 2.4 4.1 5 7.0 17.4 *** 57% 0 0 Placebo BG-12 BID BG-12 TID GA (n = 139) (n = 140) (n = 140) (n = 153) Placebo BG-12 BID BG-12 TID GA (n = 139) (n = 140) (n = 140) (n = 154) **P < 0.01; ***P < 0.0001 Miller D, et al. Presented at AAN; April 21-28, 2012; New Orleans, LA. Abstract S11.001. CONFIRM: Time to Disability Progression 12-wk Confirmed Progression of Disability Probability of Confirmed Disability Progression 0.2 24-wk Confirmed Progression of Disability 0.2 HR vs placebo BG-12 BID: 0.79, 21% reduction; P = 0.2536 BG-12 TID: 0.76, 24% reduction; P = 0.2041 Proportion progressed at 2 yrs 0.169 (Placebo) HR vs placebo BG-12 BID: 0.62, 38% reduction; P = 0.0630 BG-12 TID: 0.67,33% reduction; P = 0.1172 GA: 0.87, 13% reduction; P = 0.5528 Proportion progressed at 2 yrs 0.130 (BG-12 TID) 0.128 (BG-12 BID) 0.125 (placebo) 0.108 (GA) 0.1 0.1 0.086 (BG-12 TID) 0.078 (BG-12 BID) 0 0 BL 12 24 36 48 60 72 84 96 BL 12 24 36 48 60 72 84 96 Weeks Fox R, et al. Presented at AAN; April 21-28, 2012; New Orleans, LA. Abstract S01.003. Weeks CONFIRM: Safety – Flushing and gastrointestinal symptoms were common AEs reported more frequently in BG-12 groups vs placebo • Incidence of flushing and gastrointestinal symptoms decreased substantially after the first month of BG-12 – AEs reported more frequently with GA were injection-related – The incidence of serious infections was low and similar across groups (1–2%) • No opportunistic infections reported in any treatment arm – No malignancies reported in patients receiving BG-12 Philips JT, et al. Presented at AAN; April 21-28, 2012; New Orleans, LA. Abstract S41.005. Monoclonal Antibodies for MS in Late Stage Clinical Development Agent Mechanism of Action Alemtuzumab • Anti-CD52 • Depletes T and B lymphocytes Daclizumab • Anti-CD25 (IL-2 receptor α-chain) • Inhibits T lymphocyte activation and expansion Rituximab/ ocrelizumab • Anti-CD20 • Deplete B lymphocytes Rituximab Phase II data in MS Hauser et al. NEJM: 358 (7): 676, Figure 2 Reductions in MRI Lesions with Daclizumab Depend on Magnitude of Natural Killer (NK) Cell Expansion Mean No.New/Enlarged Gd + Lesions 87% reduction (P = 0.024) 4 3.8 75% reduction (P = 0.037) 3 2.0 2 1 0.5 0 IFN + Placebo (n = 17) IFN + DAC (n = 11) Lowest Quartile CD56tright NK IFN + DAC (n = 12) Highest Quartile CD56tright NK Sheridan JP, et al. Presented at ECTRIMS, Düsseldorf, Germany, September 9-12, 2009. Poster # 430. Alemtuzumab Alemtuzumab CAMMS223 Study: Key Efficacy Results Sustained Accumulation of Disability Time to First Relapse SC IFNβ-1a Alemtuzumab 12 mg/day Alemtuzumab 24 mg/day Alemtuzumab Pooled 40 SC IFNβ-1a Alemtuzumab 12 mg/day Alemtuzumab 24 mg/day Alemtuzumab Pooled 60 30 73% p < 0.0001 20 % Patients Relapsing % of Pts with Sustained Accumulation of Disability 50 40 72% p < 0.0001 30 20 10 10 0 0 0 6 12 18 24 Months 30 36 42 48 0 6 12 18 24 Months Coles A. Presented at ECTRIMS, Düsseldorf, Germany, September 9-12, 2009. Poster # 890. 30 36 42 48 Alemtuzumab CAMMS223 Study: Key Efficacy Results Annualized Relapse Rate 0.5 Years 0-3 (p < 0.0001) Years 0-4 (p < 0.0001) EDSS Change from Baseline to Year 4 Year 4 (p < 0.0001) 0.4 0.3 EDSS - Year 4 Change from Baseline Annualized Relapse Rate 0.4 0.3 0.2 0.1 0.2 0.1 -0 -0.1 -0.2 -0.3 -0.4 -0.5 -0.6 0 IFNβ-1a Alem Pooled IFNß-1a Alem Pooled IFNß-1a Alem Pooled IFNβ-1a Alem Pooled N = 30 N = 122 Coles A. Presented at ECTRIMS, Düsseldorf, Germany, September 9-12, 2009. Poster # 890. Alemtuzumab CAMMS223 Study: Safety • Principal AEs associated with alemtuzumab included: – Infusion reactions – Mild-to-moderate infections – Autoimmunity • Immune thrombocytopenia (ITP) • Thyroid disorders (28% vs 3% for IFNβ-1a) Coles A. Presented at ECTRIMS, Düsseldorf, Germany, September 9-12, 2009. Poster # 890. CARE-MS II: Phase III Study Design IFNβ-1a 44 mcg SC Randomized 2:1 Alemtuzumab 12 mg IV Alemtuzumab 24 mg IV 0 12 3 ×/week Daily ×5 Daily ×3 Daily ×5 Daily ×3 – 1 g methylprednisolone QD × 3 days at months 0 and 12 in all treatment arms – Blinded raters scored relapse, EDSS every 3 months, MSFC every 6 months, and MRI annually – Relapse Adjudication Panel – Randomization into 3rd treatment arm (24 mg/day alemtuzumab) was discontinued early and it was thereafter deemed “exploratory” for statistical purposes Cohen J, et al. Presented at AAN; April 21-28, 2012; New Orleans, LA. Abstract S01.004. 24 CARE-MS II: Relapses ARR (Co-Primary Endpoint) Proportion of Patients Relapse Free 0.9 SC IFNβ-1a 0.6 Alem 12 mg/day 0.5 0.4 0.3 0.2 0.1 0.26 0.52 0 Years 0–2 Percentage of Patients Without Relapse Adjusted ARR (95% CI) Reduction 49.4% 0.8 P < 0.0001 0.7 SC IFNβ-1a 100 Alem 12 mg/day 90 80 70 65% 60 50 47% 47% Risk Reduction 40 P < 0.0001 0 3 6 9 12 15 18 21 24 Follow-Up Month Cohen J, et al. Presented at AAN; April 21-28, 2012; New Orleans, LA. Abstract S01.004. CARE-MS II: 6-Month Sustained Accumulation of Disability (Coprimary Endpoint) Patinets with SAD (%) 30 SC IFNβ-1a Alem 12 mg/day HR = 0.58 Treatment Effect 42% P = 0.0084 25 20 21.1% 15 10 12.7% 5 0 0 3 6 9 12 15 18 Follow-Up Month Cohen J, et al. Presented at AAN; April 21-28, 2012; New Orleans, LA. Abstract S01.004. 21 24 CARE-MS II: EDSS Change from Baseline 3.25 SC IFNβ-1a Alem 12 mg/day Mean EDSS Score 3.00 0.24 P = 0.0064 2.75 -0.17 P = 0.0044 2.50 2.25 0 3 6 9 12 15 18 Follow-Up Month Cohen J, et al. Presented at AAN; April 21-28, 2012; New Orleans, LA. Abstract S01.004. 21 24 CARE-MS II: Safety SC IFNβ-1a n = 202 Alemtuzumab 12 mg/day n = 435 Alemtuzumab 24 mg/day n = 161 Infusion Reactions NA 393 (90.3) 156 (96.9) Serious Infusion Reactions 0 12 (2.8) 5 (3.1) 134 (66.3) 334 (76.8) 134 (83.2) 3 (1.5) 16 (3.7) 6 (3.7) 2 (1.0) 2 (0.46) 3 (1.9) 10 (5.0) 69 (15.9) 31 (19.3) 0 2 (0.5) 2 (1.2) 0 4 (0.9) 3 (1.9) 0 3 (0.7) 2 (1.2) Adverse Events N (%) Infections Serious Infections Malignancies Autoimmune Events N (%) Thyroid AEs Serious Thyroid AEs ITP AEs Serious ITP AEs Cohen J, et al. Presented at AAN; April 21-28, 2012; New Orleans, LA. Abstract S01.004. Alemtuzumab Effects on Immune Cells • Alemtuzumab induces a significant Treg and Th2 cell expansion and inhibits Th1 and Th17 cells – At day 7 post-therapy, depletion of CD4+ and CD8+ T-cells by 99.9% and 99.2%, respectively • CD4+ cells remained significantly decreased for 12 months – Predominant expansion of CD45RO+ memory cells at month 1 and decreased percentage of CD45RA+ naïve cells in both CD4+ and CD8+ T-cell populations – Significantly increased (4.1-fold) the percentage of CD4+CD25+CD127lowFOXP3 Treg cells at month 1 Zhang X, et al. Presented at AAN; April 21-28, 2012; New Orleans, LA. Abstract P02.119. Defining Immunomodulation and Immunosuppression • Immunomodulation* – Ability to alter immune function from its current state of activity without any cytotoxic activity or bone marrow suppression – Therapeutic manipulation of the immune system • Immunosuppression* – Ability to alter the immune system through a direct cytotoxic activity or bone marrow suppression – Immunosuppression can lead to immuno-modulation secondarily *Defined by Adil Javed, MD, PhD, University of Chicago. *Defined by Adil Javed, MD, PhD. University of Chicago. Risk-Benefit Assessment • Risk-Benefit assessments should include: – The benefits of therapies – The risks of those therapies – The risks of not treating or under-treating the disease itself • Quality of life • Long-term outcomes • Patient’s history of disease and disease activity • Costs Risk-Benefit information should be communicated to patients! Highest Priority Therapy Categories On a scale from 1 to 5, where 1=lowest priority and 5=highest priority, rate the priority to manage each drug category. EMD Serono Specialty Digest, 6th edition MS Cost Drivers Informal Care (12%) Sick Leave/Reduced Working Time (10%) Adaptations (5%) Services (2%) Other Drugs (6%) Early Retirement (34%) DMTs (22%) Tests (2%) Ambulatory Care (4%) DMT = disease-modifying therapy. Kobelt G, et al. Neurology. 2006;66(11):1696-1702. Hospital Inpatient Care (3%) Dramatic Price Increases for MS Agents $4,700 $4,500 Gilenya $4,300 $4,100 $3,900 $3,700 $3,500 $3,300 Copaxone Betaseron Avonex $3,100 Tysabri $2,900 Rebif Extavia $2,700 Sep-09 Oct-09 Nov-09 Dec-09 Jan-10 Feb-10 Mar-10 Apr-10 May- Jun-10 Jul-10 Aug-10 Sep-10 Oct-10 Nov-10 Dec-10 Jan-11 Feb-11 Mar-11 10 Per First DataBank , pricing information represents a 28 day supply of each medication MS Non-adherence Ranks High Compared to Other Diseases Patients not adhering, % 80 Non-adherence across chronic disease states 60 40 20 0 Cancer2 Asthma1 Renal Transplant4 Epilepsy1 HIV5 Hypertension1 MS3 Depression5 Diabetes1 Arthritis1 Note: If range is available, mean number is presented. 1. Berg JS, et al. Ann Pharmacother. 1993;27(Suppl 9):S1-S24. 2. Cuzick J, et al. Lancet. 1999;353:930. 3. Hadijmichael O, et al. Neurology. 1999;52(Suppl 2):A549. 4. Wells H. Hosp Pharmacist. 2004;11:69-71. 5. World Health Organization. Adherence to Long-term Therapies—Evidence for Action. 2003. 82 Compounds in development for Multiple Sclerosis MHC class II modulator Recombinant human alphafetoprotein T cell receptor vaccine CCR2 agonist Phase I MM-093 Integrin antagonist CCX140 Phase II TV 3606 Tovaxin NeuroVax MLN-1202 PI-2301 Unidentified Mechanism AMPA receptor antagonist TV-5010 Phase III R 1295 Immunomodulator INCB8696 Nrf2 activator BGC20-0134 IR 208 Reg. MCT125 anti CD52 Revimmune Laquinimod Heat shock protein BG-12 Launched E-2007 IL-27 agonist Alemtuzumab XToll Novantrone RPI-78M CDP323 Copaxone VLA-4 antagonist Elnd002/Elnd 004 Firategrast Estrogen agonist Estriol Tysabri DNA ntercalating Pixantrone agent T cell regulator ATXMS1467 Avonex LAS 186323 Teriflunomide ATL-1102 / TV-1102 Rebif Betaseron dihydro-orotate dehydrogenase Atacicept Extavia Ocrelizumab Biferonex BAF312 Asonep ONO-4641 CS-0777 S1P Pegylated Avonex ofatumumab Anti CD 20 Fingolimod Fampridine-sr MBP8298 BHT-3009 Cladribine AZD5904 Masitinib RTL1000 Baroferon LY2127399 T cell activation inhibitor Tyrosine kinase inhibitor Key Biological Antisense inhibitor of CD49d NCE Nerispirdine Daclizumab Pegylated IFN-β IFN-ß IL-23 antibody & anti-BAFF human antibody K Channel Blocker IL-2 Blocker 6 ribonucleotide reductase inhibitors B-lymphocyte stimulator modulators myeloperoxidas e inhibitor Thank you for your attention Questions ?










© Copyright 2026