
Form - World Health Organization
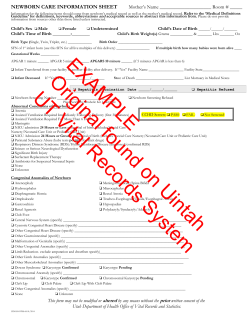
Database on Newborn Health and Birth Defects Center Name Baby’s Hospital Record No. Mother’s Hospital Record No. Inborn live birth 1. i. ii. iii. iv. v. vi. vii. viii. ix. x. NNPD Number Outborn live birth Basic information Mother’s Name * Date of Delivery * d d m m y y y y Time of Delivery (24 hr format) h h m m Baby’s Gender * Male / Female / Ambiguous Birth weight (g) Head Circumference (in cm) Mode of delivery * Vaginal / Cesarean section / Instrumental Multiple birth Single / Twin / Triplet / Higher order Gestation (in weeks) Delivery attended by Doctor / Nurse / ANM / Midwife For Out Born babies only d d m m y y y y i. Date of admission * Home / Hospital / Others ii. Place of delivery Doctor / Nurse / ANM / Midwife / Traditional birth attendant / Others iii. Delivery attended by Pre Term (< 37 weeks)/ Term (>37 weeks) iv. Gestation (in weeks) * v. Weight at admission (g) * 2. i. iii. v. vii. 3. i. ii. Maternal Details: Para Antenatal Care 5. i. 6. i. iii. 7. ii. Severe Anaemia iv. Gestational Diabetes Y / N Y / N vi. Eclampsia Y / N Y / N viii. Y / N (at least 4 antenatal check-up) Antepartum Hemorrhage Cord Prolapse 4. Labor/Delivery: Oxytocin/other drug for induction Y / N * Antenatal steroids * $ Complete Y / N Obstructed Labour Y / N At Birth Care: I. Bag and mask ventilation II. Birth defects Y / N $ None / IC / CC (For gestation <35 weeks) * Incomplete course I. Newborn (NB) Form Y/N If yes; fill BD Form at the end of this form course Newborn Morbidities: Birth trauma Y/N Hypoglycemia Y / N iii. Meconium aspiration Y / N iv. Hypothermia Y / N ii. Pneumonia Y / N Seizures Y / N ii. (If yes specify) Respiratory Distress: RDS (HMD) Y / N Transient tachypnea of newborn Y / N CNS Disorders: HIE stage 3 / stage 2 / stage 1 / None II. Supported by WHO-SEARO and CDC Atlanta 8. Systemic Infections: Systemic sepsis I. Y / N If ‘Yes’, Please fill the following fields; otherwise skip to ‘9’. Episode No. 9. Name of organism* Onset Culture Early / Late + ve / - ve Early / Late + ve / - ve Early / Late + ve / - ve Select from the list Mandatory if + ve Other: Hyperbilirubinemia I. Y / N (Need for phototherapy) II. Rh isoimmunization Y / N III. ROP requiring Laser Y / N IV. Any other morbidity Y / N If ‘Yes’, specify 10. Therapy provided: I. Intravenous fluids Y / N II. CPAP Y / N III. IMV Y / N IV. Surfactant Y / N V. Antibiotic(s) * Antibiotics Y / N If ‘Yes’, fill the followings items; otherwise skip to ‘11’. Codes Codes Codes Codes Codes Codes Name Duration (days) 11. Outcome of newborn * $ Fill Discharged / Died$ / Referred / Left against medical advice (LAMA) the following fields up to 14 if died option is selected otherwise skip to ‘15’ 12. Neonatal death * i. Date of death (dd/mm/yyyy) ii. Time of death (24 hrs) d d h m m h y y y m y m 13. Causes of Neonatal / Death* i. Asphyxia Y / N ii. Infection Y / N iii. Prematurity Y / N iv. Birth Defect(s) Y / N 14. What was the single most important cause of neonatal death? v. Others vi. Unknown Y / N If ‘Yes’, Specify Y / N Asphyxia /Infection/ Prematurity/ Birth Defect(s)/ Others/ Unknown 15. Maternal Death: Y / N Name of professional filled the physical form Date: * Mandatory Fields Supported by WHO-SEARO and CDC Atlanta





© Copyright 2026