
TUMORS AANS/CNS SECTION ON TENTH BIENNIAL SATELLITE TUMOR SYMPOSIUM PROGRAM BOOK
AANS/CNS SECTION ON TUMORS TENTH BIENNIAL SATELLITE TUMOR SYMPOSIUM PROGRAM BOOK APRIL 26–27, 2013 Hilton New Orleans Riverside New Orleans, LA This Program Book is sponsored by Arbor Pharmaceuticals. Jointly Sponsored by the AANS JOIN THE AANS/CNS SECTION ON TUMORS IN NEW ORLEANS Dear Colleagues, It is a great pleasure to welcome you to the 2013 Biennial Satellite Tumor Symposium of the AANS/CNS Section on Tumors. This year is particularly special as it marks the 10th Anniversary of the inception of this flagship Tumor Section meeting. The primary goal of the meeting is to present and discuss the most recent advances in clinical, translational, and basic science neuro-oncology research. Therefore, we have focused the meeting on peer reviewed oral and poster presentations selected from over 200 abstracts submitted by your colleagues. We have tried to provide ample time for discussion of the novel work that is presented. We also look forward to exciting keynote lectures by Eric Holland, MD, PhD, on “Molecular Targeting of Gliomas Using Mouse Models” and by Linda Liau, MD, PhD on “Imaging Paradigms to Characterize Tumor Genetics.” Both these lectures should provide critical updates on the paradigm shifting work of these two neurosurgical leaders. We thank Drs. Holland and Liau for their participation in the meeting. In addition, we have organized a comprehensive seminar on the “Multi-disciplinary Management of Meningiomas.” Co-sponsored by the Society of Neuro-Oncology (SNO), this seminar will explore all aspects of meningiomas, including pathology and molecular genetics, animal models, imaging, surgery, radiotherapy, stereotactic radiosurgery, medical therapies, quality of life and clinical trial opportunities. This symposium represents the continued effort of the Section on Tumors to partner with our neuro-oncology colleagues in SNO. We hope this will be the first of many events co-sponsored by the Section and SNO. We also invite everyone to attend the evening seminars to be held on Friday night. The first will focus on the “Latest Advances in Immunotherapy,” and the second will discuss “Surgical Adjunct to Optimize Tumor Resection.” These seminars will provide opportunities to meet with panels of experts in their respective fields. To celebrate the occasion of the 10th Anniversary of the Satellite Symposium, we have organized a reception on Saturday evening. We invite everyone to attend this reception to help us celebrate this important milestone, to learn about the history of this meeting, and to honor our Charles B. Wilson Awardee. On behalf of the Executive Committee of the AANS/CNS Section on Tumors, we thank you for participating in this 10th Biennial Satellite Tumor Symposium. We acknowledge the generous support of our corporate sponsors without whom this meeting would not be possible. We especially thank the staff at the AANS, particularly Rhonda Foss, who did yeoman’s work, while also making sure the organizing of this meeting was an enjoyable and fun experience. Sincerely, Frederick F. Lang Jr., MD, FAANS Chair, AANS/CNS Section on Tumors Nader Sanai, MD Scientific Program Co-Chair, AANS/CNS Section on Tumors 2 Isaac Yang, MD Scientific Program Co-Chair, AANS/CNS Section on Tumors TABLE OF CONTENTS Joint Sponsorship Disclaimer The material presented at the AANS/CNS Section on Tumors 10th Biennial Satellite Tumor Symposium has been made available by the AANS/CNS Section on Tumors and the AANS for educational purposes only. The material is not intended to represent the only, nor necessarily the best, method or procedure appropriate for the medical situation discussed, but rather it is intended to present an approach, view, statement or opinion of the faculty, which may be helpful to others who face similar situations. Continuing Medical Education Credit......................... 3 Disclaimer................................................................... 3 Learning Objectives.................................................... 3 Officers and Standing Committees of the AANS/CNS Section on Tumors................................... 4 Keynote Speakers....................................................... 5 Hotel Floor Plans........................................................ 6 Neither the content (whether written or oral) of any course, seminar or other presentation in the program, nor the use of specific product in conjunction therewith, nor the exhibition of any materials by any parties coincident with the program, should be construed as indicating endorsement or approval of the views presented, the products used, or the materials exhibited by the AANS/CNS Section on Tumors and jointly sponsored by the AANS, or its Committees, Commissions, or Affiliates. Exhibit Hall Floor Plan................................................ 7 Commercial Support.................................................8 Exhibitor Listing.......................................................... 8 Program Schedule.................................................... 10 Disclosures............................................................... 14 Scientific Program.................................................... 17 Oral Presentation Abstracts Scientific Program.................................................... 32 Electronic Poster Abstracts Neither the AANS nor the AANS/CNS Section on Tumors makes any statements, representations or warranties (whether written or oral) regarding the Food and Drug Administration (FDA) status of any product used or referred to in conjunction with any course, seminar or other presentation being made available as part of the AANS/CNS Section on Tumors 10th Biennial Satellite Tumor Symposium. Faculty members shall have sole responsibility to inform attendees of the FDA status of each product that is used in conjunction with any course, seminar or presentation and whether such use of the product is in compliance with FDA regulations. Learning Objectives: Upon completion of the CME activity, participants should be able to: n n n U pdate the audience on new neurosurgical techniques for brain tumors. R eview recent knowledge gained from neuro-oncology clinical trials. E valuate progress in the adjuvant therapy of brain tumors. Claim CME Credit the Easy Way Meeting attendees will self-report CME credit for the programs they attend by going online to MyAANS.org. PLEASE HAVE YOUR USERNAME [e-mail address] AND PASSWORD HANDY during and after the meeting for convenient completion and submission. Once logged in, click on “Self Reporting” on the left and choose AANS/CNS Section on Tumors 10th Biennial Satellite Tumor Symposium. Continuing Medical Education Credit This activity has been planned and implemented in accordance with the Essential Areas and policies of the Accreditation Council of Continuing Medical Education through the joint sponsorship of the AANS and AANS/CNS Section on Tumors. The AANS is accredited by the ACCME to provide continuing medical education for physicians. Designation Statement The AANS designates this live activity for a maximum of 13 AMA PRA Category 1 CreditsTM. Physicians should claim only the credit commensurate with the extent of their participation in the activity. 3 AANS/CNS TENTH BIENNIAL SATELLITE TUMOR SYMPOSIUM CONFERENCE COMMITTEE Scientific Committee Scientific Advisory Committee Nader Sanai, MD, Scientific Co-Chair Isaac Yang, MD, Scientific Co-Chair Frederick F. Lang, Jr., MD, FAANS Andrew Thomas Parsa, MD, PhD, FAANS Michael A. Vogelbaum, MD, PhD, FAANS, Society of Neuro-Oncology Representative Michael Lim, MD, FAANS Jonathan Harris Sherman, MD Gordon Ho-Wan Li, MD Gabriel Zada, MD William T. Curry Jr., MD, FAANS Theodore H. Schwartz, MD, FAANS Ricardo Jorge Komotar, MD James Bradley Elder, MD OFFICERS OF THE AANS/CNS SECTION ON TUMORS Chair.......................................................... Frederick F. Lang Jr., MD, FAANS Past-Chair. ...................................................... Jeffrey N. Bruce, MD, FAANS Secretary-Treasurer. .......................Frederick G. Barker II, MD, FAANS Advisory Board................................... Gene H. Barnett, MD, MBA, FAANS Mitchel S. Berger, MD, FAANS Ennia Antonio Chiocca, MD, PhD, FAANS William T. Couldwell, MD, PhD, FAANS Roberta P. Glick, MD, FAANS James M. Markert Jr., MD, FAANS Joseph M. Piepmeier, MD, FAANS Mark L. Rosenblum, MD, FAANS James T. Rutka, MD, PhD, FAANS Raymond Sawaya, MD, FAANS Ronald E. Warnick, MD, FAANS Journal of Neuro-Oncology. .............. Linda M. Liau, MD, PhD, FAANS Medical Neuro-Oncology. .......................................... Susan M. Chang, MD Matrix........................................... Ennio Chiocca, MD, PhD, FAANS (Chair) Membership......................................................................... Allen E. Waziri, MD Newsletter................................................... Jonas M. Sheehan, MD, FAANS NeuroPoint Alliance..................... Mark E. Linskey, MD, FAANS (Chair) James Bradley Elder, MD Nominating...................................................... Jeffrey N. Bruce, MD, FAANS Pediatrics............................................................. George I. Jallo, MD, FAANS Programs................................................ Daniel P. Cahill, MD, PhD, FAANS Christopher M. McPherson, MD, FAANS Viviane S. Tabar, MD, FAANS Ricardo Jorge Komotar, MD Michael A. Vogelbaum, MD, PhD, FAANS Radiosurgery.................................... Jason P. Sheehan, MD, PhD, FAANS Research. ...................................... Howard L. Weiner, MD, FAANS (ABTA) William T. Curry Jr., MD, FAANS (BrainLAB) Skull Base................................................... Nicholas B. Levine, MD, FAANS Spine. .......................................................... Laurence D. Rhines, MD, FAANS SANS MOC.......................................................................... Sarah C. Fouke, MD Washington...................................................... Andrew E. Sloan, MD, FAANS Young Neurosurgeons.........................................................Brian Nahed, MD Committee Chairs Awards...................................... Andrew Thomas Parsa, MD, PhD, FAANS Bylaws......................................................Isabelle M. Germano, MD, FAANS Clinical Trials. ................................................... Manish K. Aghi, MD, FAANS John A. Boockvar, MD, FAANS Constantinos G. Hadjipanayis, MD, PhD, FAANS CCI...........................................................Aaron A. Cohen-Gadol, MD, FAANS Brian T. Ragel, MD, FAANS Guidelines...................................................Steven N. Kalkanis, MD, FAANS Timothy C. Ryken, MD, FAANS Jeffrey J. Olson, MD, FAANS History.......................................................Anthony D’Ambrosio, MD, FAANS Information Technology.................................. Jason A. Heth, MD, FAANS International.................... Daniel Monte-Serrat Prevedello, MD (Chair) Randy L. Jensen, MD, PhD, FAANS (Chair) 4 KEYNOTE SPEAKERS ERIC C. HOLLAND, MD, PHD Dr. Holland is a board-certified neurosurgeon who specializes in the treatment of patients with gliomas — the most common malignant brain tumor in adults — and metastatic brain tumors. He is an attending physician in the Departments of Neurosurgery, and Neurology as well as a laboratory head in the Sloan-Kettering Institute's Cancer Biology and Genetics Program. He is also Vice Chair for Translational Research in the Department of Surgery. In the laboratory, his research team is seeking to understand the molecular mechanisms underlying the development of central nervous system tumors and developing models of these cancers in mice. Dr. Holland, along with his colleagues, have developed mouse models of many subtypes of gliomas, including the first truly lifelike model of glioblastoma — the most lethal brain tumor in people. These animal models are essential for making the transition from a scientific concept to understanding the behavior of a human tumor. Over the years, Dr. Holland has received several awards, including the American Brain Tumor Association Research Award, the Bittner, Bressler, Farber Award, Searle Scholar Award, Seroussi, the Steck Award and the Voynick Awards. In addition, he is a member of the National Academies’ Institute of Medicine. LINDA M. LIAU, MD, PHD, FAANS Dr. Linda M. Liau is Professor and Vice Chair of Academic Affairs in the Department of Neurosurgery at the David Geffen School of Medicine at UCLA, and Director of the UCLA Brain Tumor Program. She received her B.S. degree in Biochemistry and B.A. degree in Political Science, both with honors, from Brown University. She then received her M.D. degree from Stanford University and a Ph.D. degree in Molecular Neuroscience from UCLA. After completing her residency and fellowship training in neurosurgery and neurosurgical oncology at UCLA, she joined the faculty at the UCLA School of Medicine as an Assistant Professor in 1997, and is now a tenured Professor of Neurosurgery at UCLA. She is currently a boardcertified neurosurgeon with both an active research laboratory and a busy clinical practice in the field of brain tumors and neurosurgical oncology. She is currently ranked as one of the top 1% of neurosurgeons in the country by U.S. News Top Doctors. Dr. Liau currently serves on the Scientific Advisory Council of the National Brain Tumor Society, as well as the Scientific/ Medical Advisory Boards of the Musella Foundation for Brain Tumor Research, the Brad Kaminsky Foundation for Brain Tumors, the Miles for Hope Foundation, and Voices Against Brain Cancer. She has been the Principal Investigator on several NIH R01 research grants over the past 15 years, and is the mentor for several NIH training grants (R25, K01, K12, T32) for neurosurgical residents, fellows, and postdoctoral researchers in her laboratory. Her research interests include translational experimental therapeutics of cell-based therapies for brain tumors and characterization of molecular targets involved in brain tumor pathogenesis and progression. She is the principal investigator on various clinical trials of brain cancer vaccines and immunotherapy for patients with brain tumors and has published extensively in the field. She has authored over 100 peer-reviewed research articles, along with several book chapters and a textbook entitled Brain Tumor Immunotherapy. She is on the editorial boards of several scientific/medical journals and is the current Editor-inChief of the Journal of Neuro-Oncology. 5 HILTON NEW ORLEANS RIVERSIDE FLOOR PLAN Second Floor Third Floor 6 EXHIBIT FLOOR PLAN 7 COMMERCIAL SUPPORT The AANS/CNS Section on Tumors wishes to thank the following companies for their generous support of this year’s meeting. GOLD SUPPORT LEVEL SILVER SUPPORT LEVEL NEUROSURGICAL Rethinking Possibilities, Reshaping Lives EXHIBITOR LISTING Agenus 3 Forbes Road Lexington, MA 02421 Phone: (781) 674-4711 Fax: (781) 674-4200 www.agenusbio.com Booth #302 Brainlab 600 W. Van Buren, Suite 510 Chicago, IL 60607 Phone: (312) 257-0118 Fax: (708) 409-1619 www.brainlab.com Booth #304 Agenus is a biotechnology company focused on developing cancer immunotherapies, which includes Prohage G Series Vaccines currently being tested in clinical trials of newly diagnosed and recurrent GBM. Prophage Series contain HSPPC-96, which comprises heat shock protein, gp96, and associated peptides that are purified from the patients’ own tumor tissue. Brainlab develops, manufactures and markets software-driven medical technology, enabling access to improved, more efficient, less-invasive patient treatments. Arbor Pharmaceuticals, Inc. 980 Hammond Drive Building Two, Suite 1250 Atlanta, GA 30328 Phone: (866) 516-4950 Fax: (678) 334-2433 www.arborpharma.com Booth #100 Brainlab technology currently powers treatments in the fields of neurosurgery, radiation oncology, orthopedics, ENT, CMF, spine, and trauma. Core products revolve around less-invasive image guided surgery technology, more accurate and effective radiation therapy, and integration through planning and collaboration systems that bring patient data and physicians together. Privately held since its formation in Munich, Germany in 1989, Brainlab has more than 5,000 systems installed in about 80 countries. Brainlab employs 1,070 people in 17 offices worldwide, including 280 Research & Development engineers, who form a crucial part of the product development team. Arbor Pharmaceuticals, a specialty pharmaceutical company headquartered in Atlanta, GA, is pleased to announce the recent acquisition of the U.S. rights for GLIADEL® Wafer (polifeprosan 20 with carmustine implant) from Eisai Inc. Gliadel® is manufactured by Eisai Inc. for Arbor Pharmaceuticals, LLC. Gliadel® is a registered trademark of Eisai Inc. Learn more at www.brainlab.com. 8 Elekta 400 Perimeter Center Terrace, Suite 50 Atlanta, GA 30346 Phone: (770) 670-2592 Fax: (770) 448-6338 www.elekta.com Booth #202 NeuroBlate System®, a neurosurgical ablation device providing controlled therapy for difficult-to-treat brain tumors. Monteris also offers the AXiiiS® Stereotactic Miniframe; a single use platform for image-guided, stereotactic brain biopsy; and the AtamA® Head Coil and Stabilization System form MRI-guided neurosurgical procedures requiring head fixation. Elekta pioneers significant innovations and clinical solutions for treating cancer and brain disorders. The company develops advanced tools and treatment planning systems for radiation therapy, radiosurgery and brachytherapy, as well as workflow enhancing software systems. Through its products and services, Elekta aims to improve, prolong and save patient lives. Novocure 195 Commerce Way Portsmouth, NH 03801 www.novocure.com Booth #104 Novocure is an oncology company pioneering a novel treatment modality for solid tumors called NovoTTF™ Therapy. In patients with recurrent glioblastoma, treatment with NovoTTF Therapy has been shown to provide patients with efficacy outcomes comparable to chemotherapy with fewer side effects and a better quality of life. NovoTTF Therapy is delivered by a portable, non-invasive medical device designed for continuous use by the patient. For full prescribing information please visit www. novottftherapy.com. Integra LifeSciences 311 Enterprise Drive Plainsboro, NJ 08536 Phone: (609) 275-0500 Fax: (609) 275-5363 www.integralife.com Booth #102 Integra LifeSciences, a world leader in medical devices, is dedicated to limiting uncertainty for surgeons, so they can concentrate on providing the best patient care. Integra offers a vast portfolio of implants, devices, instruments and systems used in neurosurgery and neuro critical care. Osteomed 3885 Arapaho Rd Addison, TX 75001-4314 Phone: (800) 456-7779 Fax: (972) 677-4731 www.osteomed.com Booth #206 Medtronic 6743 Southpoint Drive N Jacksonville, FL 32216 Phone: (800) 876-3133 Fax: (901) 332-3920 www.medtronic.com Booth #208 OsteoMed is a leading global innovator, developer, manufacturer and marketer of specialty medical devices, surgical implants and powered surgical instruments. Stryker 750 Trade Centre Way, Suite 200 Portage, MI 49002 Phone: (800) 962-6558 Fax: (269) 324-5484 www.stryker.com Booth #204 Medtronic is the global leader in medical technology – alleviating pain, restoring health and extending life for millions of people around the world. During the past year, Medtronic provided medical professionals with products and therapies to improve the lives of nearly six million patients. Today, every five seconds another person, somewhere in the world, is alive or living a fuller life as a result of a Medtronic product or therapy. Since the beginning, Stryker has taken pride in developing innovative equipment and technology that helps medical professionals perform their jobs better and more efficiently. Our products include joint replacements, trauma, spine and micro implant systems, biologics, powered surgical instruments, surgical navigation systems, endoscopic products, patient handling and emergency medical equipment. Monteris Medical Inc. 16305 36th Avenue N, Suite 200 Plymouth, MN 55446 Phone: (763) 253-4710 Fax: (763) 746-0084 www.monteris.com Booth #300 Formed in 1999, Monteris Medical is a privately held medical device company dedicated to the development of innovative MRI guided, laser-based brain cancer treatments. Monteris Medical markets 9 PROGRAM SCHEDULE Friday, April 26, 2013 2:14–2:24 PM Rapid, Label Free Detection of Microscopic Brain Tumor BoundPerrs with Coherent Raman Scattering Microscopy Presenting Author: Daniel Orringer, MD 10:00 AM–7:00 PM Registration Hilton Exhibition Center Foyer, Second Floor 3:00–6:30 PM Exhibit Hall Open E-Poster Abstract Viewing Hilton Exhibition Center Hall B&C, Second Floor 2:25–2:35 PM Improving Functional Preservation in Acoustic Neuroma Surgery Presenting Author: Hirofumi Nakatomi 1:00-3:20 PM General Session I Hilton Exhibition Center Hall A, Second Floor Supported by an Educational Grant Provided by OsteoMed 2:36–2:46 PM Morbidity of Repeat Transsphenoidal Surgery Assessed in Over 1000 Operations Presenting Author: Arman Jahangiri 2:47–2:57 PM Comparative Integrated Analysis of Brain Tumor Initiating Cells and Their Parent Tumors Presenting Author: Candice Poon, MD NEUROSURGICAL Rethinking Possibilities, Reshaping Lives 1:00–1:10 PM Opening Remarks Frederick F. Lang Jr., MD, FAANS Nader Sanai, MD 2:58–3:08 PM MicroRNA 100 Targets the ‘Silencing Mediator for Retinoid Receptors’ (SMRT) Gene, Reduces Tumor Proliferation, and Improves Survival in Glioblastoma Presenting Author: John S. Kuo, MD, PhD, FAANS 1:10–1:40 PM Keynote Address I Molecular Targeting of Gliomas Eric C. Holland, MD, PhD 3:09–3:19 PM Prediction of Outcomes After Surgical Resection of Glioblastoma Using Contrast Enhancing and FLAIR Residual Tumor Volume Presenting Author; Matthew M. Grabowski Selected Abstract Presentations Moderators: Nader Sanai, MD; Isaac Yang, MD 1:41–1:51 PM Epileptic Seizures in Adult Diffuse Low Grade Gliomas. A Multicentre Study of 1544 Cases Presenting Author: Johan Pallud, MD 3:20–3:40 PM Beverage Break in Exhibit Hall Hilton Exhibition Center Hall B&C, Second Floor E-Poster Abstract Viewing 1:52–2:02 PM Periostin Induces Glioblastoma MRI T2/FLAIR Signal, Cellular Invasion, and Angiogenesis Presenting Author: Pascal Zinn, MD, PhD 3:00–7:00 PM Exhibit Hall Open E-Poster Abstract Viewing Hilton Exhibition Center Hall B&C, Second Floor 2:02–2:12 PM Surgery for Primary Supratentorial Brain Tumors in the United States, 2000 to 2009: The Effect of Provider Caseload on Complication Rates Presenting Author: Victoria Trinh 3:40–6:00 PM General Session II Hilton Exhibition Center Hall A, Second Floor Supported by an Educational Grant Provided by OsteoMed NEUROSURGICAL Rethinking Possibilities, Reshaping Lives 10 3:40–4:10 PM Keynote Address II Imaging Paradigms to Characterize Tumor Genetics Linda M. Liau, MD, PhD, FAANS 5:38–5:48 PM Delay of GBM Adjuvant Therapy Does Not Decrease Overall and Progression Free Survival: A Retrospective Analysis Presenting Author: Matthew Z. Sun Selected Abstract Presentations Moderators: Nader Sanai, MD; Isaac Yang, MD 6:00–7:00 PM Opening Reception in Exhibit Hall Hilton Exhibition Center Hall B&C, Second Floor 4:10–4:20 PM miR 124 Systemically Enhances Antitumor Clearance by Inhibiting STAT3 Signaling and Reversing Glioma Associated Immune Suppression Presenting Author: Amy B. Heimberger, MD, FAANS 7:00–8:00 PM Evening Symposium I–Immunotherapy for the Treatment of Glioma Patients Belle Chasse, Third Floor Andrew Thomas Parsa, MD, PhD, FAANS Isaac Yang, MD Michael Lim, MD, FAANS Ian Parney, MD, PhD This Evening Symposium is Supported by an Educational Grant Provided by Agenus 4:21–4:31 PM Intracranial Therapy of Glioblastoma by CED With a Novel Bispecific Ligand Directed Diphtheria Toxin Targeting EGF and uPA Receptors Presenting Author: Yan Michael Li, MD 4:32–4:42 PM MRI Based High Resolution Maps for Guiding Surgical Procedures in Brain Tumor Patients Presenting Author: Yael Mardor, MD 7:00–8:00 PM Evening Symposium II–Surgical Adjuncts To Optimize Tumor Resection: Applying Advanced Imaging And Navigation Techniques To Maximize Resection And Minimize Morbidity Melrose, Third Floor Alessandro Olivi, MD, FAANS Michael Edward Sughrue, MD Andrew Thomas Parsa, MD, PhD, FAANS This Evening Symposium is Supported by an Educational Grant Provided by Brainlab 4:43–4:53 PM Post Transcriptional Regulation of O6 Methylguanine DNA Methyltransferase (MGMT) by miR 603: A Step Toward Personalized Glioblastoma Treatment Presenting Author: Clark C. Chen, MD, PhD, FAANS 4:54–5:04 PM Distinct Roles for Histone Methyltransferase Ezh2 in Epigenetically Promoting Adult Neural Stem Cell Proliferation and Differentiation Presenting Author: Ryan Salinas Saturday, April 27, 2013 7:00 AM–6:00 PM Registration Hilton Exhibition Center Foyer, Second Floor 5:05–5:15 PM High Field Intraoperative MRI and Endoscopy Provide Complementary Extent of Transsphenoidal Resection Improvements for Pituitary Adenoma Presenting Author: Ralph Dacey Jr., MD 7:00–8:00 AM Continental Breakfast served in Exhibit Hall Hilton Exhibition Center Hall B&C, Second Floor 5:16–5:26 PM Tumor Derived Vasculogenesis in von Hippel Lindau Syndrome Associated CNS Hemangioblastoma Presenting Author: Jason Michael Frerich 7:00 AM–4:00 PM Exhibit Hall Open E-Poster Abstract Viewing Hilton Exhibition Center Hall B&C, Second Floor 5:27–5:37 PM Advanced MRI is Accurate and Cost Effective for Predicting Recurrent Glioma versus Treatment Related Necrosis Presenting Author: Jackson D. Hamilton, Jr. 11 7:45 AM–9:00 AM General Session III Hilton Exhibition Center Hall A, Second Floor Supported by an Educational Grant Provided by OsteoMed 9:00–9:10 AM Introductory Remarks Michael A. Vogelbaum, MD, PhD, FAANS 9:00–10:10 AM Meningioma Session I Hilton Exhibition Center Hall A, Second Floor NEUROSURGICAL Rethinking Possibilities, Reshaping Lives 7:45–7:55 AM Opening Remarks Issac Young, MD 9:10–9:30 AM Pathology and Molecular Genetics of Meningiomas Arie Perry, MD Selected Abstract Presentations Moderators: Nader Sanai, MD; Isaac Yang, MD 9:30–9:50 AM Mouse Models of Meningiomas Michel Kalamarides, MD, PhD 7:55–8:05 AM Radiographic Predictors of Functional Recovery in Adult Posterior Fossa Ependymomas Presenting Author: Zaman Mirzadeh, MD 9:50–10:10 AM Imaging Michael A. Vogelbaum, MD, PhD, FAANS 8:06–8:16 AM Continuous Dynamic Mapping of Corticospinal Tract during Surgery of Motor Eloquent Brain Tumors: Prospective Study Presenting Author: Andreas Raabe 10:10–10:30 AM Beverage Break in Exhibit Hall Hilton Exhibition Center Hall B&C, Second Floor 10:30 AM-12:35 PM Meningioma Session II Hilton Exhibition Center Hall A, Second Floor 8:17–8:27 AM Radical Resection Plus Radiation Therapy for Central Nervous System Hemangiopericytoma Presenting Author: Adam M. Sonabend Wothalter, MD 10:30–10:50 AM Surgery for Meningiomas Frederick G. Barker II, MD, FAANS 8:28–8:38 AM SapC DOPS Nanovesicles Selectively Target Externalized Phosphatidylserine and Identify Metastatic Brain Tumors Presenting Author: Xiaoyang Qi 10:50–11:10 AM Fractionated Radiation Therapy of Meningiomas Leland Rogers, MD 8:39–8:49 AM Utilizing PVI Z CCL21 Vault Nanoparticles as a Novel AntiTumor Therapy for Glioblastoma Presenting Author: Isaac Yang, MD 11:10–11:30 AM Radiosurgery of Meningiomas Jason P. Sheehan, MD, PhD, FAANS Selected Abstract Presentations Moderators: Patrick Wen, MD; William T. Curry, Jr, MD, FAANS 8:50–9:00 AM Importance of Extent of Resection in the Treatment of GBM: How Much is Enough? Presenting Author: Lauren Elana Rotman 11:30–11:40 AM A Molecular Predictor of Meningioma Recurrence Presenting Author: Erik P. Sulman 9:00 AM–5:00 PM Symposium on Multidisciplinary Management of Meningiomas Hilton Exhibition Center Hall A, Second Floor Co-Sponsored by Society for Neuro-Oncology 11:41–11:51 AM The Novel Neoplasia Genes, TRAF7 and KLF4, Along with SMO and AKT1, Define Clinically Distinct Meningiomas Presenting Author: Murat Gunel, MD, FAANS 12 11:52 AM–12:02 PM Genomic and Transcriptomic Analysis Reveals an Oncogenic Functional Module in Meningiomas Presenting Author: Gabriel Zada, MD 3:15-3:25 PM Autologous Vaccine Therapy to Control Invasive Canine Meningioma Presenting Author: Grace Elizabeth Pluhar 12:03–12:13 PM Trends in Centralization of Meningioma Surgery in the United States, 1988–2010: A Population Based Study Presenting Author: Frederick G. Barker II, MD, FAANS 3:26-3:36 PM Expression of CD163 Prevents Apoptosis Through the Production of Granulocyte Colony Stimulating Factor in Meningioma Presenting Author: Hiroshi Nishihara 12:14–12:24 PM Preclinical Studies of Intratumoral Cellular Immunotherapy for Recurrent Meningiomas with Alloresponsive Cytotoxic T Lymphocytes Presenting Author: Richard George Everson, MD 3:37-3:47 PM Increased [68Ga] DOTATOC Uptake in PET Imaging Discriminates Meningioma and Tumor Free Tissue Presenting Author: Jörg Christian Tonn, MD 12:25–12:35 PM mTOR Inhibition as a Reasonable Strategy for Meningioma Treatment Presenting Author: Christian Mawrin 3:48-3:58 PM Imaging and Clinical Factors Predictive of Atypical Meningiomas Presenting Author: Le (Lucy) He, MD 12:35–1:35 PM Lunch in Exhibit Hall Hilton Exhibition Center Hall B&C, Second Floor 3:59–4:09 PM Development of Atypical and Anaplastic Meningioma Cell Resources: Results From Three Years Experience at UCSF Presenting Author: Charles David James 1:35–4:20 PM Meningioma Session III Hilton Exhibition Center Hall A, Second Floor 4:10-4:20 PM Progression of Atypical Meningiomas Irrespective of Adjunctive Radiation Presenting Author: Heather M. Kistka 1:35–1:55 PM Medical Therapies of Meningiomas Patrick Wen, MD 4:20–5:00 PM Meningioma Session IV Hilton Exhibition Center Hall A, Second Floor Moderator: Michael A. Vogelbaum, MD, PhD, FAANS 1:55–2:15 PM New Therapeutic Targets of Meningiomas Rameen Beroukhim, MD, PhD 2:15–2:35 PM Quality of Life of Patients with Meningiomas Susan M. Chang, MD 4:20–5:00 PM Point to Counter Point Should Radiation Be Used for Newly Diagnosed or Recurrent WHO Grade II Meningiomas? Yes: Ricardo Jorge Komotar, MD No: Franco de Monte, MD 2:35-2:55 PM Clinical Trial Opportunities in Meningioma Thomas J. Kaley, MD 5:00-7:00 PM 10th Biennial Satellite Tumor Symposium Celebration Versailles Ballroom, Third Floor This reception is supported by 2:55-3:15 PM Beverage Break in Exhibit Hall E-Poster Abstract Viewing Hilton Exhibition Center Hall B&C, Second Floor Selected Abstract Presentations Moderators: Leland Roger, MD; James Bradley Elder, MD 13 DISCLOSURES The AANS controls the content and production of the CME activity and attempts to ensure the presentation of balanced objective information. In accordance with the Standards for Commerical Support established by the Accreditation Council for Continuing Medical Education, speakers, paper presenters/authors and staff (and the significant others of those mentioned) are asked to disclose any relationship they or their co-authors have with commercial companies which may be related to the content of their lecture. DISCLOSURES REPORTED Rameen Beroukhim, MD, PhD Novartis, Consultants J. Bryan Iorgulescu Aesculap, Inc., Consultants AstraZeneca, Stock Shareholder (Directly purchased) Randy Lynn Jensen, MD, PhD, FAANS Medtronic, Consultants Li Bie, Grant/Research Support Vivian Capilla-Gonzalez NIH, Grant/Research Support Pharmokinesis, Honorarium Ricardo Jorge Komotar, MD Osteomed, Consultants Susan M. Chang, MD Novartis, Grant/Research Support Medtronic, Consultants Schering, Grants/Research Support Linda M. Liau, MD, PhD, FAANS Northwest Biotherapeutics, Inc., Grant/Research Support William T. Curry, Jr., MD, FAANS Stryker CMF, Consultants NIH, Grants/Research Support Yael Mardor, MD Zach, Guez, Last, Daniels and Mardor are authors on a pending patent titled ‘vessel function maps’ Franco De Monte, MD, FAANS, FACS Medtronic, Consultants, Honorarium Murat Gunel, MD, FAANS NIH, Grant/Research Support Christian Mawrin Pfizer Inc., Grant/Research Support, Other Financial or Material Support Gregory M. Kiez and Mehmet Kutman Foundation, Grants/Research Support Jackson D. Hamilton, Jr. JDH—Travel expenses (‹$3000) were paid by Anatom-e information systems for travel expenses associated with a speaking engagement. Honorarium LAH is owner of Anatom-e Information Systems, whose program was used during some of the analysis. Other Financial or Material Support 14 Ziaoyang Qu, PhD Inventor on the patent (SapC-DOPS) Michael A. Vogelbaum, MD, PhD, FAANS Merck, Consultants Development and Commercialization has been licensed to Bexion Pharmaceuticals, LLC Pharmaco-kinesis, Consultants Patrick Wen, MD Novartis Consultants, Grant/Research Support, Honorarium Inventor of Scientific Research in the Pre-clinical Stage for Bexion Pharmaceuticals Genentech, Consultants, Grants/Research Support, Honorarium Bexion Pharmaceuticals does not offer any marketable treatments or drugs Merck, Grants/Research Support, Honorarium Theodore H. Schwartz, MD, FAANS Wellcome Trust, Grant/Research Support Pfizer, Grants/Research Support Sanofi-Aventis, Grants/Research Support Integra,Consultants Fumio Yamaguchi, MD, PhD Ministry of Education, Culture, Sport, Science, and Technology, Japan (MEXT), Grant/Research Support Visionsense, Honorarium Andrew E. Sloan, MD, FAANS Genentech, Consultants, Other Financial or Material Support Zaitun Zakaria Consultants Roche Pharmaceuticals, Inc, Consultants Corinna C. Zygourakis, MD Meningioma Mommas Surgical Theatre, Consultants Lentigen Inc., Grants/Research Support, Other Financial or Material Support Ruth Halperin Endowed Chair in Meningioma Research (McDermott), Grant/Research Support Erik P. Sulman GlaxoSmithKline, Consultants Reza and Georgianna Khatib Endowed Chair in Skull Base Tumor Surgery (Parsa), Grants/Research Support Jorg-Christian Tonn, MD Merck Serono, Consultants, Honorarium Roche, Consultants, Honorarium 2013 15 NON-DISCLOSURE INFORMATION Speakers, paper presenters/authors and staff (and the significant others of those mentioned) who have reported they do not have any relationships with commercial companies: Amjad Anaizi, MD Charles David James Walter Rachinger Patricia Anderson Michel Kalamarides, MD, PhD Shervin Rahimpour Khaled M. A. Aziz, MD, PhD, FAANS Farrukh Karimov, MD Maryam Rahman, MD El Mustapha Bahassi Yasutaka Kato Alexander Ramos Frederick G. Barker II, MD, FAANS Robert Givens Kellogg, MD Leland Rogers, MD Ernest Barthelemy Kartik Kesavabhotla Lara K. Ronan Maria Blagia Heather M. Kistka Lauren Elana Rotman Christian Andrew Bowers, MD John S. Kuo, MD, PhD, FAANS Ryan Salinas Clark C. Chen, MD, PhD, FAANS Frederick F. Lang Jr., MD, FAANS Nader Sanai, MD Felipe Goncalves de Carvalho, MD Christine Lauro Christopher Ian Sanders Taylor, MD Philip C. de Witt Hamer, MD Gordon Ho-Wan Li, MD Kenneth Schott James Bradley Elder, MD Yan Michael Li, MD Lucia Schwyzer, MD Sam Eljamel, MD, FRCS Mohammad Arif Malik, MBBS, FCPS Jason P. Sheehan, MD, PhD, FAANS Richard George Everson, MD Emmanuel Mandonnet Leslie Smith Javier Figueroa Salvador Manrique, MD Adam M. Sonabend Wothalter, MD Elena Fomchenko John M. McGregor, MD T. Barrett Sullivan Rhonda F. Foss Zaman Mirzadeh, MD Matthew Z. Sun Jason Michael Frerich Jennifer Moliterno Gunel, MD Peter Sylvester Matthew M. Grabowski Jeffrey Murray Yuzo Terakawa Sanjeet Singh Grewal Hirofumi Nakatomi Nam D. Tran, MD Puneet Gulati, MD Hiroshi Nishihara Victoria Trinh William C. Gump, MD Verrad Kwasi Nyame, MD Stephanie Elizabeth Weiss, MD John Franklin Hamilton, MD, PhD, FAANS Joseph Orinya Obande, MD Anna Magdalena Wilk Carl Irwin Odom Jing Wu Le (Lucy) He, MD Sacit Bulent Omay, MD Chunzhang Yang Amy B. Heimberger, MD, FAANS Mark E. Oppenlander, MD Isaac Yang, MD Tadashi Higuchi Daniel Orringer, MD Gabriel Zada, MD Allen L Ho Quinn T. Ostrom Zaitum ZaKaria Eric C. Holland, MD, PhD Johan Pallud, MD Pascal Zinn, MD, PhD Peleg Moshe Horowitz, MD Abdel Nasser Hosein Andrew Thomas Parsa, MD, PhD, FAANS Anwar Hossain Arie Perry, MD Namath Hussain, MD Grace Elizabeth Pluhar Michael Edward Ivan, MD Candice Poon, MD Arman Jahangiri Andreas Raabe 16 2013 AANS/CNS SECTION ON TUMORS SCIENTIFIC PROGRAM ORAL PRESENTATION ABSTRACTS 1. A Molecular Predictor Of Meningioma Recurrence 2. Advanced MRI Is Accurate And Cost Effective For Predicting Recurrent Glioma Versus Treatment Related Necrosis Erik P. Sulman; Lindsey Goodman, BS; Khalida Wani, PhD; Albert Lai, MD, PhD; Franco DeMonte, MD; Kenneth Aldape, MD (Houston, TX) Jackson D. Hamilton, Jr.; Edward Jackson, PhD; Norman Leeds, MD; Leena Ketonen, MD, PhD; David Schellingerhout, MD; Jessica Jones; LaToi Tatum; Ping Hou, PhD; David Evans; Michelle Underwood; Jerell Jones; Brandy Reed; Stacy Hash; Joseph Steele, MD; Heidi Albright; Ashok Kumar, MD (Houston, TX) Introduction: More than 20% of patients with meningioma suffer from tumor recurrence, leading to aggressive surgical and radiotherapeutic interventions that add to patient morbidity. Neither grade nor extent of surgical resection/Simpson grade fully account for recurrence risk. Adjuvant radiation may decrease this risk in some patients but comes with increase toxicity. We hypothesized that tumors at risk for recurrence would exhibit a unique gene expression signature that could be used to assign patients to adjuvant treatment. Introduction: Treatment related brain necrosis (TRN) mimics recurrent high grade glial tumor but can often be managed non surgically. Methods: Glioma patients radiated ‹6 months prior with a new enhancing lesion were prospectively imaged to determine recurrent glioma versus TRN. The protocol began in 2009, adding dynamic contrast enhanced and susceptibility contrast perfusion, diffusion tensor and multivoxel spectroscopy to conventional imaging. In 2011, multiple refinements occurred based on review of earlier results. Radiologist reports were considered accurate if within a point of pathology reports on a scale from pure tumor (1) to pure treatment effects (5). The cost of all care (surgery, chemotherapy, etc.) for patients beginning from imaging through 90 days was tabulated from baseline and after refinements, with inflation adjustment and outliers censored. Fisher exact test compared group differences. Methods: We performed expression profiling (Affymetrix HG U133Plus2.0) on previously untreated tumors resected at first diagnosis and correlated expression to clinicopathologic features (age, WHO grade, Simpson grade, sex, tumor location) and outcome [recurrence free (RFS) and overall survival (OS)]. Results: We evaluated 62 patients treated between 1991 2007. Median age was 57y. Forty three were female, 19 male. Median follow up was 3.9y with 8 deaths and 13 recurrences. WHO grading was as follows: grade I, 30 (48%); grade II, 31 (50%); grade III, 1 (2%). 46 resections were coded as Simpson I or II. Adjuvant radiation was given to 8 patients. Unsupervised clustering identified two predominant molecular subtypes with 25% of cases belonging to group 1 (meningioma recurrence risk group 1, MRRG1) and 75% to group 2 (MRRG2). Analysis by grade revealed that MRRG2 contained more higher grade tumors: 82% of grade II and 100% of grade III tumors. All but 1 recurrence belonged to MMRG2. Survival analysis revealed a 5yr RFS of 94% vs. 59% for MRRG1 vs. MRRG2. The 5yr OS was 100% vs. 82% (p=NS). We validated this signature using a published meningioma dataset (GSE16581) and found a similar association between MRRG group and recurrence with 100% of recurrent cases belonging to MRRG2 (p=0.0056). Results: In the baseline group, 33 of 110 had biopsy/surgery within 60 days of imaging and 11 had only treatment effects. After the protocol was refined, 29 of 103 had biopsy/surgery and 1 had only treatment effects (p=0.003). The radiology reports accuracy increased from 72% (24/33) to 97% (28/29). The average total cost for the 110 baseline imaged patients was $28,447 and for the 103 patient after the refinements $24,507, a savings of $3,900/patient. Conclusions: Improved diagnostic accuracy may decrease unnecessary surgical intervention for treatment effect and reduce overall care costs. This required an experienced team (technologists, physicists and neuroradiologists) with little additional scanning/post processing time (‹1 hour more than conventional imaging), justifying a prospective multicenter clinical trial. Conclusions: Our data suggest that gene signature can accurately segregate patients at risk for recurrence. This accurate classification would be a powerful tool for assigning patients for appropriate adjuvant therapy. 17 3. Autologous Vaccine Therapy To Control Invasive Canine Meningioma 4. Comparative Integrated Analysis Of Brain Tumor Initiating Cells And Their Parent Tumors Grace Elizabeth Pluhar; Matthew Hunt, MD; Brian Andersen, BS; John Ohlfest, PhD (St. Paul, MN) Candice Poon, MD; Wei Wu, PhD; Carly Pontifex; Mohammad Al Najjar; H. Luchman; Charles Chesnelong; Samuel Weiss, PhD; Jennifer Chan; J. Cairncross, MD, PhD; Michael Blough, PhD (Calgary, Canada) Introduction: Canine and human meningiomas have similar neuroimaging characteristics, gross and histological appearance, and expression of growth factors and cell surface receptors. However the biological behavior of tumors in dogs is more aggressive compared to human tumors. Median survival times in dogs after standard surgical excision has been reported to be 6 7.5 months and the prevalence of grade II meningiomas (40%) is high compared to humans. These characteristics make dogs a more meaningful model of high grade meningioma compared to mice for testing new strategies. To that end, we assessed safety and efficacy of tumor lysate vaccines to treat spontaneous meningioma in pet dogs. Introduction: Glioblastoma (GBM) is a uniformly fatal intra axial neoplasm that carries a dismal prognosis. It is speculated that brain tumor initiating cell (BTIC) cultures derived from resected GBM better captures its molecular heterogeneity and clinical features than traditional cell lines. As the effect of cell culture stresses on genomic alterations in BTICs has yet to be elucidated, we sought to inspect the genetic fidelity of BTICs compared to their parent tumors (PTs) by performing a comparative genomic and genetic analysis. Methods: Using the Affymetrix 6.0 SNP array and the Illumina HT12 beadarray, we acquired data on genome wide copy number alterations (CNAs), loss of heterozygosity (LOH), and gene expression patterns from 12 BTIC lines and their matched PTs. Methods: Dogs had surgical resection followed by six vaccinations with autologous tumor lysate and toll like receptor ligand adjuvant. Toxicities were monitored by examinations and blood tests, disease status by MRI, and immune response in peripheral blood mononuclear cells (PBMC) by ELISpot and flow cytometry and in sera by Western blot. Results: Although BTICs acquired more amplifications and deletions than their PTs, statistical significance was not achieved. However, the magnitude of amplifications with and without LOH in coding regions of the genome were significantly different. Expression analysis revealed that differentially expressed genes in BTICs were chiefly involved with metabolism, while an integrated analysis demonstrated chromosomal alterations in BTICs were most commonly associated with chromosome 7 amplifications, a location connected to putative oncogenes. Results: Gross total resection was achieved 17 of 19 cases; grade I (11), grade II (5), grade III (3). Adverse effects were rare, primarily pain and erythema at injection sites. Median survival time = 401 days (5 dead with NED; 1 alive 921 days) with CpG treated dogs, 865 days (2 euthanized @ 343 and 733 days) with imiquimod (n=6). Median survival is 155 days in a new trial with triziquimod (n=7); 2 dogs euthanized @130 and 200 days (NED) and 1 recurrence after 290 days. CD8+ T cells were increased post vaccination in two dogs. Polyclonal antibodies to tumor specific antigens were detected in all dogs and also triggered antibody dependent cell mediated cytotoxicity against autogolous and allogeneic cells. Conclusions: BTICs maintain their ancestor’s core genome structure, with many changes appearing to be "passenger" alterations.However, statistically significant changes did occur in the form of enhancement of existing genomic modifications. Notably, novel recurring genomic alterations were not observed in BTICs. Conclusions: Immunotherapy using autologous tumor lysate/ TLR agonists elicits antibody and T cell responses and increases survival compared to reported survival in dogs treated by surgery alone. Since dogs tend to have more aggressive disease, this may be a treatment for humans with meningiomas that have failed other standard therapies or those at high risk of recurrence. 5. Continuous Dynamic Mapping Of Corticospinal Tract During Surgery Of Motor Eloquent Brain Tumors: Prospective Study Andreas Raabe; Juergen Beck, MD, PhD; Philippe Schucht, MD; Kathleen Seidel, MD (Koenigstein, Germany) Introduction: We recently reported that the subcortical mapping motor threshold (MT) where irreversible DCS MEP changes and motor deficits regularly occur is lower (&lt;2mA) than previously thought. However, mapping at MTs of 1 5mA is hampered by insufficient temporal and spatial coverage of the surgical site with conventional monopolar fingerstick mapping probe (MFMP). A new continuous and dynamic mapping technique is described. 18 Methods: We prospectively studied 41 patients with tumor surgery adjacent to the CST with simultaneous subcortical monopolar motor mapping (train of five stimuli). Continuous and dynamic (spatial coverage) mapping was achieved by integrating the stimulation probe at the tip of a new suction device. MTs obtained with the new device and MFMP at the same site were analyzed. Motor function was assessed one day after surgery, at discharge, and after 3 months. additional adjuvant chemotherapy, delay was also significant but only when categorized into quartiles(p=0.042). Unexpectedly, delay was associated improved PFS(HR: 2nd quartile:0.515; 3rd quartile:0.608; 4th quartile:0.732). Conclusions: We demonstrated that delay to adjuvant therapy is not associated with decrease in either PFS or OS. This suggests that, when necessary, delay of adjuvant therapy may not negatively affect patient prognosis. Results: A 1:1 correlation of motor MTs for stimulation sites simultaneously mapped with the suction device and MFMP was found (74 stimulation points, r = 0.996, p&lt;0.001). All procedures were technically successful. Lowest individual MTs were: >5mA, n=12; 4 5mA, n=13; 1 3mA, n=16 patients. At 3 months, one patient had a persisting postoperative motor deficit (2.4%). Surgeons using continuous dynamic mapping unanimously reported a higher confidence regarding the exact location and safe distance from the CST compared to the MFMP. 7. Development Of Atypical And Anaplastic Meningioma Cell Resources: Results From Three Years Experience At UCSF Charles David James; Rintaro Hashizume, MD, PhD; Yu Jen Lu, MD, PhD; Arie Perry, MD; Andrew Parsa, MD, PhD; Michael McDermott, MD (San Francisco, CA) Introduction: The primary objective of this study is to assess the feasibility of establishing xenografts from surgical cases diagnosed as atypical or anaplastic menigioma. The long term purpose of this study is to develop preclinical models for therapeutic testing. Conclusions: Continuous dynamic mapping is a feasible technique for localizing the exact site and distance to the CST. It may increase the safety of motor eloquent tumor surgery by providing better temporal and spatial coverage compared to mapping with the fingerstick probe. Methods: Tumor specimens, classified as atypical WHO grade II (n = 9) or anaplastic WHO grade III meningioma (n = 10) were collected over a three year period from surgical cases at UCSF. Athymic mice were engrafted directly with 50 100 mm3 of tumor tissue in the subcutaneous space. Remaining tissue from surgical resection was minced in serum free media, then mechanically disrupted by repetitive pipetting to generate cell suspensions from which we attempted to establish cell cultures. 6. Delay Of GBM Adjuvant Therapy Does Not Decrease Overall And Progression Free Survival: A Retrospective Analysis Matthew Z. Sun; Orin Bloch, MD; Aaron Clark, MD, PhD; Michael Ivan, MD; Michael Safaee, BS; Taemin Oh, BA; Andrew Parsa, MD, PhD (San Francisco, CA) Results: Twelve of 19 cell cultures have proven sustainable (7 atypical and 5 anaplastic). Athymic mice, receiving subcutaneous implantation of patient surgical specimen, and that have been monitored for as long as one year for indication of subcutaneous tumor growth, have yielded transplantable tumor tissue, for successful serial propagation in 5 of 12 instances (42%: two atypical and three anaplastic); 7 mice receiving subcutaneous injection of patient surgical specimen remain under observation for the growth of tumor that can be serially propagated. Four of the tumorigenic meningiomas have been modified with a luciferase reporter, to enable in vivo bioluminescence imaging of tumor growth and response to therapy. Introduction: The effect of delaying concurrent chemotherapy and radiotherapy after GBM surgery remains unclear. Current literature on the subject lacks modern cohorts in the Stupp protocol era. Methods: We retrospectively analyzed GBM patients in the Stupp protocol era (2005 2011). Delay to adjuvant therapy after surgery was reclassified into 3 categorical variables:1) Binary(>28 or &;lt;28 days), 2)Quartiles (1st, 2nd, 3rd, or 4th quartile in time), and 3) bi weekly(<2, 2 4, 4 6, 6 8, or >8 weeks). Survival analysis was performed by constructing Kaplan Meier curves assessed by logrank test, and by multivariate Cox proportional hazards models. Conclusions: Our results demonstrate the feasibility of establishing a meningioma xenograft panel that can be used to test experimental therapies for treating patients whose meningiomas are not surgically curable. Results: There were 352 patients; median age was 59.88. Median delay, follow up, progression free survival(PFS), and overall survival(OS) were 28, 292, 172, and 356 days, respectively. Kaplan Meier Analysis showed no statistically significant differences with either OS or PFS when delay was analyzed as binary, quartile, or bi weekly categorical variables. Unexpectedly, those in the longest quartile had better PFS compared to the shortest quartile(p=0.04). Cox proportional hazards model incorporating delay, age, concurrent chemotherapy, additional adjuvant chemotherapy, and KPS revealed that only age and additional adjuvant chemotherapy remained significant for OS(age,p=0.003,HR:1.023; additional chemotherapy,p=0.04,HR:0.659). For PFS, in addition to age and 19 8. Distinct Roles For Histone Methyltransferase Ezh2 In Epigenetically Promoting Adult Neural Stem Cell Proliferation And Differentiation Methods: On data obtained on 1544 adult patients with supratentorial hemispheric diffuse low grade gliomas from multicentre French cooperative study groups, we addressed the relationships among seizures and clinical, imaging, pathological, molecular, treatment related parameters and outcomes. Ryan Salinas; William Hwang, PhD; Daniel Lim, MD, PhD (San Francisco, CA) Results: 89.8% of patients had seizures at diagnosis. Male gender, long time to diagnosis, temporal and parietal locations, and tumor close to functional areas were independent predictors of a history of seizures at diagnosis. Tumor volume, growth velocity, cortical location, histological subtype or molecular markers did not affect seizure occurrence probability. Long history of seizures and insular location were independent predictors of uncontrolled seizures at diagnosis, while history of seizures at diagnosis, tumor parietal and insular locations were independent predictors of uncontrolled seizures after oncological treatment. Subtotal and total surgical resections were independent predictors of seizure control after oncological treatment. History of seizures at diagnosis was associated with longer survival without malignant transformation and with longer overall survival. Introduction: The molecular mechanisms underlying the stem cell nature of glioblastoma are poorly understood. Aberrant overexpression of EZH2, a histone methyltransferase normally required to maintain stem cell populations in other tissues, likely contributes to this oncogenic transformation. Understanding EZH2 genomic targets in subventricular zone neural stem cells (SVZ NSCs), where many brain tumors potentially arise, would advance our understanding of oncogenesis and identify novel therapeutic targets. Methods: SVZ NSCs with conditional Ezh2 deletion were analyzed in vitro and in vivo. Neurosphere formation assays, chromatin immunoprecipitation (ChIP), reverse transcriptase quantitative PCR, immunocytochemistry, and immunohistochemistry (IHC) were used to identify molecular targets of Ezh2. Lentiviral Olig2 overexpression and Olig2 shRNA knockdown assessed Ezh2 mediated neuronal differentiation. Results: Ezh2 deletion in vitro greatly impairs both proliferation and neurogenesis. ChIP and mRNA analysis indicate EZH2 specifically binds and represses the tumor suppressor Ink4a/Arf locus in SVZ NSCs. Co deletion of Ink4a/Arf restored proliferation, but not neurogenesis. Co deleted cells had increased expression of basic helix loop helix transcription factor, OLIG2. ChIP analysis identified Olig2 as a direct and functional target of EZH2. Transient overexpression of Olig2 profoundly inhibited neurogenesis and intriguingly, knockdown of Olig2 enhanced neurogenesis in Ezh2 deleted but not WT NSCs. IHC revealed Ezh2 deletion greatly impairs SVZ neurogenesis in vivo. Conclusions: Ezh2 epigenetically represses Ink4a/Arf in SVZ NSCs, potentially contributing to SVZ NSC derived oncogenesis. However, Ezh2 mediated repression of Olig2, commonly expressed in gliomas, is required for neuronal progression. Rather than solely maintaining self renewal and anaplasticity, Ezh2 has a dual role in epigenetically regulating both self renewal and progressive lineage restriction in SVZ NSCs. 9. Epileptic Seizures In Adult Diffuse Low Grade Gliomas. A Multicentre Study of 1544 Cases. Johan Pallud, MD; Etienne Audureau, MD; Nader Sanai; Marie Blonski; Luc Bauchet; Denys Fontaine; Emmanuel Mandonnet; Jacques Guytotat; Philippe Peruzzi; François Xavier Roux; Luc Taillandier; Gilles Huberfeld; Laurent Capelle; Hugues Duffau (Paris, France) Introduction: The natural history of seizures, the predictors of seizure control and their prognostic significance have not been clearly defined in diffuse low grade gliomas, although seizures are known to be the most frequent symptom in glioma and deeply impact quality of life. Conclusions: Epileptic seizures occurrence depends on specific tumor characteristics and independently affect glioma prognosis. Patients with a history of seizures and those with a complete surgical resection have better outcomes. Thus, in addition to the oncological benefit, early and maximal surgical resection could help in achieving seizure control of patients harboring a diffuse low grade glioma. 10. Expression Of CD163 Prevents Apoptosis Through The Production Of Granulocyte Colony Stimulating Factor In Meningioma Hiroshi Nishihara; Hiromi Kanno, MD, PhD; Lei Wang, PhD; Hiroyuki Kobayashi, MD, PhD; Sunsuke Terasaka, MD, PhD; Kiyohiro Houkin, MD, PhD; Shinya Tanaka, MD, PhD (Sapporo, Japan) Introduction: CD163 is a 130 kDa transmembrane protein expressed in human monocytes and macrophages, while the aberrant expression of CD163 in breast and colorectal cancer associated with patients poor prognosis was reported. Here we analyzed the expression of CD163 in meningioma, a common intracranial tumor, and its molecular mechanism in association with meningioma progression. Methods: First, we performed immunohistochemical analysis using 50 human meningioma specimens. Next, we established CD163 overexpressing human meningioma cell lines and investigated its roles on tumor progression in vitro and in vivo. Results: Immunohistochemically, 26 out of 50 human meningioma specimens (52.0%) were positive for CD163 in tumor cells, including benign Grade I (48.5%) and Grade II (71.4%) cases. Furthermore, CD163 expression was correlated with histological atypical parameters which directly predict the prognosis of meningioma patients. CD163 overexpressing meningioma cells showed significant suppression of apoptosis and accelerated tumor growth in nude mice. In addition, unexpected splenomegaly affiliated with the xenograft predicted to us the tumor derived 20 12. High Field Intraoperative MRI And Endoscopy Provide Complementary Extent Of Transsphenoidal Resection Improvements For Pituitary Adenoma granulocyte colony stimulating factor (G CSF) production, which was confirmed by RT PCR and ELISA. Conclusions: To our knowledge, this is the first report which demonstrates CD163 expression in meningioma not only by immunohistochemistry but also by RT PCR using primary culture cells, and provides the novel molecular function of CD163 to prevent apoptosis through the production of G CSF in meningioma. Peter Sylvester; John Evans, BS; Feng Gao, PhD; Richard Chole, MD; Anne Getz, MD; Bruce Haughey, MD; Ravindra Uppaluri, MD; Keith Rich, MD; Gregory Zipfel, MD; Ralph Dacey, MD; Michael Chicoine, MD (St. Louis, MO) Introduction: Advanced operative techniques (AOTs; endonasal approach, stereotactic neuronavigation, and endoscopy) and intraoperative MRI (iMRI) are replacing traditional operative techniques (TOTs) for pituitary adenoma resection. The study objective was to evaluate the impact of AOTs and iMRI on extent of resection (EOR). 11. Genomic And Transcriptomic Analysis Reveals An Oncogenic Functional Module In Meningiomas Gabriel Zada, MD; Xiao Chang; Lingling Shi; Fan Gao; Jonathan Russin; Liyun Zeng; Shuhan He; Thomas Chen; Steven Giannotta; Daniel Weisenberger; Kai Wang; William Mack (Los Angeles, CA) Methods: Review of 184 iMRI and 298 conventional post operative MRI only (coMRI) cases (mean follow up=17.3 and 39.6 months, respectively), and the impact of AOTs. Case matching based on propensity scores yielded 133 matched iMRI/coMRI pairs. The EOR gross, near, or sub total resection (GTR, NTR, or STR) was determined, and progression free survival (PFS) assessed. Introduction: Meningiomas are among the most common primary adult brain tumors. Although typically benign, roughly 3 5% display malignant pathological features. The key molecular pathways involved in malignant transformation of meningiomas remain to be determined. Methods: A systematic analysis of genomic and transcriptomic differences between benign, atypical, and malignant meningiomas (n=19 total) was performed using DNA SNP array, DNA methylation sequencing, and gene expression array in an effort to provide insight into the tumor biology governing malignant transformation. Results: Patients who received no post operative radiation or hormone suppression had an increased PFS if post operative MRI revealed GTR or NTR versus STR (p=.049). Multivariate analysis showed that surgeries performed with all AOTs resulted in improved EOR compared to surgeries with TOTs (p=.041). Surgeries performed with AOTs without endoscopy did not show improved EOR compared to surgeries with TOTs (p=.932), indicating an EOR benefit specific to endoscopy. Of 49 patients with additional resection after iMRI, 14 improved to a higher level of EOR (28.6%). Improvement in EOR post iMRI was equivalent for cases performed with or without endoscopy (p=.674), indicating an iMRI benefit distinct from endoscopy. The absolute risk reduction and number needed to treat to improve EOR after iMRI usage were 6.8% and 14.8, respectively. Results: At the genomic level, malignant and atypical meningiomas had more chromosomal losses (average length in malignant: 528 Mb, atypical: 203Mb, benign: 34Mb) than their benign counterparts. Monosomic loss of chromosome 22 was identified as one of the primary chromosomal level abnormalities in all subsets of meningiomas, particularly in malignant samples. At the transcriptomic level, a weighted gene co expression network was constructed, 23 co expression modules were identified. Gene functional enrichment analysis identified a module with 356 genes that was highly related to tumorigenesis. Four intramodular hub genes (GAB2, KLF2, ID1, CTF1) were oncogenic and are related to leukemia. A meningioma related gene (MN1), which is also associated with leukemia, was also identified in this module and shown to demonstrate differential expression between malignant and benign meningiomas. Conclusions: For patients undergoing transsphenoidal surgery for pituitary adenomas, increased EOR led to increased PFS. Endoscopy and iMRI led to increased EOR compared to TOTs. Conclusions: DNA copy number variation analysis confirmed the high frequency of chromosome 22 monosomy and the association between WHO grade and chromosomal abnormalities. Transcriptome analysis identified several genes with highly differential expression between the benign and malignant groups, including a meningioma candidate gene, MN1. Genomic and transcriptomic analysis of surgical meningioma samples provides novel insight into the malignant transformation of meningiomas, with implications regarding molecular heterogeneity. 21 13. Imaging And Clinical Factors Predictive Of Atypical Meningiomas 14. Importance Of Extent Of Resection In The Treatment Of GBM: How Much Is Enough? Le (Lucy) He, MD; Megan Strother, MD; Roopa Vemireddy, MD; Lola Chambless, MD (Nashville, TN) Lauren Elana Rotman; Quinn Ostrom; Benjamin Kuhns, BS; Paul Farah; Jaime Vengoechea, MD; Carleton Johnson; Lisa Rogers, DO; Jill Barnholtz Sloan, PhD; Andrew Sloan, MD (Cleveland Heights, OH) Introduction: The World Health Organization (WHO) classifies meningiomas as WHO I (88 94%), WHO II (5 7%) and WHO III (1 2%). Grade II meningiomas have an aggressive clinical course with increased risk of post treatment recurrence. Distinguishing Grade II meningiomas from Grade I meningiomas preoperatively could affect surgical planning and improve treatment outcomes for patients. In this study, we examined whether clinical and magnetic resonance imaging (MRI) features could distinguish between Grade I and Grade II meningiomas. Introduction: Glioblastoma multiforme (GBM) is the most common malignant brain tumor and contributes disproportionately to mortality. Previous studies demonstrate that maximal extent of resection (EOR) is associated with increased survival. This prospective study assesses survival advantages of EOR in light of advancements in postoperative therapy. Methods: Clinical data and MRI imaging from 128 patients with Grade I or II meningiomas was retrospectively evaluated and correlated with histological grade to determine which features were predictive of more aggressive meningiomas. Imaging factors analyzed included peritumoral edema, presence of a draining vein, tumor necrosis, and tumor location. Methods: One hundred thirty four (134) newly diagnosed GBM patients were identified as part of the Ohio Brain Tumor Study. Tumor volume and eloquent location were determined based on preoperative and postoperative (‹ 48 hours following surgery) MRIs. Kaplan Meier and Cox Proportional Hazards models were used to determine the relationship between EOR and other prognostic factors on median survival (MS). Results: The 128 meningioma patients studied included 94 females and 34 males. Mean age at the time of meningioma diagnosis was 54.7 years (range 18 to 87 years). On histological grading at surgical resection, 94 patients had WHO I tumors and 34 patients had WHO II tumors. Imaging features associated with increased risk for atypical meningioma in univariate analysis included tumor necrosis by imaging (p=0.025), increased peritumoral edema (p=0.022) and convexity location (p=0.026). Neither male sex nor patient age were significant. In multivariate analysis, there was a trend towards increased risk of higher grade in patients with peritumoral edema (p=0.072), but this finding did not meet our criteria for statistical significance. Results: Mean patient age was 64, median post operative Karnofsky Performance Status (KPS) was 70. 65% underwent standard radiation and temozolomide following surgery. Median preoperative tumor volume was 34.68cm3 and median postoperative tumor volume was 4.42cm3. Mean EOR was 84.8% (range 26.8 100%). MS was 10.88 months from the date of surgery. KPS, age, eloquent location, and postoperative concomitant chemoradiation were significant predictors of survival. Significant survival benefit was observed with as minimal EOR as 83% (p ‹ 0.001) in both unadjusted and adjusted models. However, MS incrementally increased with EOR of ‹90%; ‹95% or ‹99% to 12.33, 13.48, 14.07 months respectively. Conclusions: Grade II meningiomas, are highly aggressive tumors that generally require early surgical resection and consideration of adjuvant radiation. Observation of these cases, may lead to the development of neurologic symptoms and may complicate future resections. We have identified three factors that are associated with increased risk of higher grade: convexity location, peritumoral edema, and presence of tumor necrosis. Future studies including larger numbers of patients may allow us to build a useful multivariate model that clinicians can use to predict meningioma grade accurately prior to treatment. Conclusions: Though EOR ‹99% is associated with the greatest survival benefit, significant survival advantage accrues with EOR as low as 83% in patients undergoing surgery for newly diagnosed GBM. This supports the survival advantage of debulking GBM ‹83% even when complete resection is not feasible or safe. 15. Improving Functional Preservation In Acoustic Neuroma Surgery Hirofumi Nakatomi; Hirofumi Nakatomi (Tokyo, Japan) Introduction: To restore nerve functions during acoustic neuroma (AN) surgery, we focused on minimizing the injury period and maximizing the recuperation period. Methods: Ninety consecutive patients underwent retrosigmoid unilateral AN surgery, and postoperative hearing and facial nerve function were evaluated. A novel application of continuous direct brainstem evoked potentials (CDBEPs) that visualized and tracked these neural functions was used to analyze the factors affecting same grade functional preservation: auditory evoked dorsal cochlear nucleus action potentials (AEDNAPs) for cochlear nerve (CN) and continuous facial nerve root evoked muscle action potentials (FREMAPs) for facial nerve (FN). Of the 90 patients, 23 underwent continuous direct AEDNAP and FREMAP 22 monitoring alone without intraoperative recuperation treatment (the monitoring alone group), and 67underwent both types of monitoring with intentional intraoperative extended recuperation treatment (IERT) (the IERT strategy group). Whenever these responses declined to 40% and 65% of initial responses, respectively, intentional IERT was performed up to every 30 min for AEDNAP and every 15 min for FREMAP until the determined level was restored. Conclusions: Increased [68Ga] DOTATOC uptake in PET allows a spatially precise discrimination between SRII expressing meningioma and tumorfree tissue, valuable both for surgery and radiation planning. Results: Logistic analysis revealed that the final AEDNAP/ FREMAP % and undertaking IERT were contributing factors for same grade functional preservation. Patients in the IERT strategy group had a significantly better functional preservation rate than those in the monitoring alone group (the adjusted hazard ratio for cochlear nerve same grade preservation in IERT strategy group relative to monitoring alone group, 0.173 [95% confidence interval (CI), 0.036 to 0.831], p =0.028 and the adjusted hazard ratio for facial nerve same grade preservation, 0.103 [95%CI, 0.027 to 0.398], p <0.0001). Yan Michael Li, MD; Daniel Vallera, PhD; Walter Hall, MD (Syracuse, NY) Conclusions: Visualizing neural function and rescuing reversible injury by IERT with continuous AEDNAP and FREMAP improved functional preservation in AN surgery. 16. Increased [68Ga] DOTATOC Uptake In PET Imaging Discriminates Meningioma And Tumorfree Tissue Walter Rachinger; Niklas Thon, MD; Alexander Haug, MD; Ulrich Schüller, MD; Jörg Christian Tonn, MD (Munich, Germany) Introduction: The somatostatin receptor II (SRII) analogue [68Ga] DOTATOC has been used for positron emission tomography (PET) imaging of meningiomas. However, no correlative analysis of increased [68Ga] DOTATOC uptake, SRII expression and histology has been published so far. This prospective study offers a spatially precise histopathological analysis of SRII expression using [68Ga] DOTATOC PET guided biopsies in primary and recurrent meningioma patients. Methods: Adult patients with suspected intracranial meningiomas and without prior radiotherapy were included. PET analysis included SUVmax within areas of biopsy inside and outside of the tumor. Magnetic resonance imaging (MRI), [68Ga] DOTATOC PET integrated into neuronavigation and intraoperative computed tomography (iCT) were used for a neuronavigated tissue sampling procedure. Histopathological analysis included SRII expression. Results: 12 patients (8x de novo and 4x recurrent meningiomas; median age 49 years) were included. Overall, 59 specimens were collected. 48 samples displayed tumor, 11 samples showed tumorfree scar tissue or dura. A SUVmax ‹2.3 was significantly associated with meningioma tissue. Sensitivity, specificity and positive predictive value of SUVmax ‹2.3 to detect meningioma tissue was 95.8%, 81.8%, and 95.8%, respectively. SRII expression was exclusively found in tumor specimens. Less than 25% SRII positive tumor cells were found in 20, 25 50% positive cells in 10, 50 75% positive cells in 13, and more than 75% in 16 samples. A significant correlation was found between SUVmax and quantitative SRII expression (p=0.001). Results did not significantly differ between primary and recurrent tumors. 17. Intracranial Therapy Of Glioblastoma By CED With A Novel Bispecific Ligand Directed Diphtheria Toxin Targeting EGF And uPA Receptors Introduction: Recombinant protein toxins that specifically target tumor cells appear to be a promising therapy for GBM. We aimed to broaden the receptor recognition by immunotoxins (IT) to a wider range of GBM by incorporating two totally unrelated ligands uPA and EGF that recognize common GBM and neovascular antigens and determinate whether this immunotoxin could inhibit the growth of aggressive human GBM in our mouse intracranial model via convection enhanced delivery (CED). Methods: We tested this new recombinant bispecific cytotoxin, called DTATEGF, against GBM lines using assays for cell proliferation, cytotoxicity, and flow cytometry. We established aggressive brain tumors intracranially (IC) in nude mice with U87 Luc and LN229 Luc glioma cells genetically marked with a firefly luciferase reporter gene. DTATEGF was delivered intracranially to treat mice with GBM via CED by a microosmotic pump. Results: DTATEGF was highly potent and selective in killing malignant glioblastoma cells lines, which is receptor specific since cytotoxicity could be blocked with antibodies and accompanied by increased apoptotic population. In vivo, DTATEGF significantly inhibited the tumor growth volume of the IC GBM shown by In Vivo Imaging System, compared to irrelevant control IT (P‹ 0.01). The mice with IC GBM treated with DTATEGF delivered by osmotic pump survived longer than the control animals (P‹0.01). No obvious local and systemic toxicity was seen at a dose of 1 µg via CED. Conclusions: A new co targeting agent that simultaneously recognizes EGFR and uPAR is more effective for anti glioblastoma therapy due to simultaneously targeting glioblastoma cells and the neovasculature. DTATEGF delivered by CED has effective therapeutic advantages for glioblastoma and low toxicity in an intracranial mouse model. Keywords: Glioblastoma, EGF, uPA, Diphtheria toxin, Cytotoxin, Convection enhanced delivery. 23 18. Morbidity Of Repeat Transsphenoidal Surgery Assessed In Over 1000 Operations Arman Jahangiri; Arman Jahangiri; Jeffrey Wagner; Liane Miller, BS; Mai Tran; Maxwell Tom, BS; Sandeep Kunwar, MD; Lewis Blevins, MD; Manish Aghi, MD, PhD Introduction: While transsphenoidal surgery has low morbidity, the degree of morbidity increase during reoperation remains unclear. We investigated morbidity of repeat transsphenoidal surgery in 946 consecutive patients. Methods: Five year retrospective review of the first 946 patients treated at our center since being named a pituitary center of expertise. Results: Of 946 patients, 104 had reoperation(s) (93 second operations, 9 third; 1 fourth; 1 fifth) a mean of 7 months after the first operation (range 1 55 months), with diagnoses including endocrine inactive (29%) or active (22%) adenomas, craniopharyngioma (15%), and Rathke’s cleft cysts (12%). Morbidity of reoperation versus initial surgery included transient diabetes insipidus (DI;24%vs.5%; P‹0.001), postoperative hyponatremia (14%vs.16%; P=0.6), CSF leak requiring repair (10%vs.3%; P=0.1), meningitis (4%vs.2%; P=0.4), length of stay (2.9 vs. 4.9 days; P=0.001), and new postoperative hypopituitarism (18% vs. 13%; P=0.1). Three category analysis comparing first, second, and third fifth operations revealed increased meningitis (1.5%/4.3%/10%; P‹0.01), length of stay (2.9/4.3/6.9 days; P‹0.001) and DI (5%/11%/80%; P‹0.0001). There was an insignificant trend towards more frequent reoperations for CSF leaks (2%/6%/9%; P=0.08), while new postoperative pituitary deficits did not occur more frequently (18%/11%/20%; P=0.6). Morbidity for reoperation was comparable amongst pathologies. No carotid artery injuries occurred. Conclusions: The benign nature of pituitary disease meant that reoperations were rarely needed in these 946 patients undergoing 1153 operations. However, when needed, repeat transsphenoidal had more frequent postoperative DI and meningitis and greater length of stay, with morbidity increasing with each subsequent operation. Our findings underscore the importance of repeat transsphenoidal surgery being performed by experienced neruosurgeons working with endocrinologists to reduce morbidity. 19. MRI Based High Resolution Maps For Guiding Surgical Procedures In Brain Tumor Patients Yael Mardor, MD; Zvi Cohen; David Guez; David Last; Dianne Daniels; Chen Hoffmann; Dvora Nass; Alisa Talianski; Leor Zach; Roberto Spiegelmann; Yuval Grober; Ouzi Nissim (Tel Hashomer, Israel) Introduction: Conventional MRI is currently unable to differentiate tumor from non tumoral tissues which show enhancement on conventional T1 MRI (such as radionecrosis). We have applied delayed contrast extravasation MRI for calculating high resolution maps clearly differentiating tumor from non tumoral tissues. Here we demonstrate the feasibility of applying these maps for improved targeting of stereotactic biopsies. Methods: 23 patients with primary/metastatic brain tumors post chemoradiation/radiosurgery were scanned by delayed contrast extravasation MRI prior to surgery. High resolution maps were calculated and used for planning stereotactic biopsies. Histological assessment was then compared with the pre surgical maps. Results: The maps showed two primary enhancement populations: the slow population where contrast clearance from the tissue was slower than contrast accumulation and the fast population where clearance was faster than accumulation. In all cases, biopsies obtained from regions of the fast population consisted of morphologically active tumor while biopsies obtained from regions of the slow population consisted of non tumoral tissues. According to our maps, in this cohort of patients 48.4±1.9%;1.9% (on average) of the enhancing lesion volume on T1 MRI did not represent morphologically active tumor. Conclusions: The fact that 50% of the enhancing volume on T1 MRI represents non tumoral tissues emphasizes the need for improved targeting of surgical procedures. The excellent correlation between our pre surgical maps and histology suggests that the maps may be applied for planning of diagnostic stereotactic biopsies thus improving targeting to regions of morphologically active tumor and for improved resection planning especially in the case of close proximity to functionally eloquent brain regions. 20. MicroRNA 100 Targets the 'Silencing Mediator For Retinoid Receptors' (SMRT) Gene, Reduces Tumor Proliferation, And Improves Survival In Glioblastoma John S. Kuo, MD, PhD, FAANS; Bahauddeen Alrfaei, MS; Raghu Vemuganti, PhD (Madison, WI) Introduction: Improved therapeutic approaches are needed for the most common primary adult brain cancer, glioblastoma (GBM) because of the current dismal median survival of less than two years. We identified and tested the differentially expressed microRNA 100 (MiR 100) as a candidate "tumor suppressor" in GBM. Methods: Standard molecular biology methods were used. GBM specimens were obtained with patient consent via IRB approved protocols to establish cell lines. Results: Quantitative PCR validated differential microRNA array results showing high miR100 expression in normal cells and low expression in multiple GBM lines. MiR100 overexpression via transfection of 4 GBM lines with miR 100 precursor (U87, U251, patient derived 22T and 33T) reduced proliferation on MTS assays (average 50%+15; p ‹ 0.05). TUNEL assays showed that transient transfection of 15 pmole of miR 100 per 500K GBM tumor cells triggered apoptosis 70% more than scrambled control miR after 24 hrs (p ‹ 0.01). SMRT was identified as a candidate miR100 target in multiple miRNA databases, and validated with miR100 specific inhibition in a luciferase SMRT 3’UTR reporter assay. In addition, a single dose of pre mir 100 (60 pmol) injected directly into intracranial GBM xenografts significantly extended survival 30% more than mice injected with control scrambled miRNA (p ‹ 0.01; n=8). GBM lines that stably overexpressed miR 100 two fold 24 22. Post Transcriptional Regulation Of O6 Methylguanine DNA Methyltransferase (MGMT) By miR 603: A Step Toward Personalized Glioblastoma Treatment over similar control transfected GBM lines were created for in vivo studies: 10x6 cells were implanted for tumor xenograft histology and survival analysis. Significantly reduced Ki 67 proliferation index was observed compared to control (mir 100 vector: 18 +14% Ki 67+; empty vector: 100+11% Ki 67+; p ‹ 0.01). Two fold over expression of miR 100 in vivo showed an average of 70% reduction in Ki 67 proliferation index. Furthermore, miR 100 overexpressing cells was associated with significantly smaller xenografts than injection of sibling control GBM cells. Clark C. Chen, MD, PhD; Valya Ramakrishnan, PhD; Deepa Kushwaha, PhD; Kimberly Ng, MD; Diahnn Futalan; David Gonda, MD; Tyler Steed, MD; Jann Sarkaria, MD; Bob Carter, MD, PhD (La Jolla, CA) Introduction: Approximately 10% of glioblastoma patients derive long term benefit from temozlomide (TMZ). As such, there is a critical need to develop predictive biomarkers to identify this patient subset. Patients unlikely to benefit from TMZ should be enrolled in novel therapeutic trials. The DNA repair enzyme O6 methylguanine DNA methyltransferase (MGMT) is the major mechanism by which cells detoxify TMZ induced DNA damage. The observation that the transcription of MGMT is suppressed by methylation of its promoter has led one set of predictive biomarkers. However, these biomarkers fail to assess the effect of post transcriptional regulation by micro RNAs. This study aims to identify critical MGMT regulating miRNAs that would help to predict clinical response to TMZ. Conclusions: These studies establish the tumor suppressor activity of miR 100 in GBM, which may lead to further development of miR 100 related cell mechanisms as novel GBM therapies. 21. Periostin Induces Glioblastoma MRI T2/FLAIR Signal, Cellular Invasion, And Angiogenesis Pascal Zinn, MD, PhD; Pascal Zinn, MD, PhD; Pratheesh Sathyan, PhD; Frederick Lang, MD; Raymond Sawaya, MD; Rivka Colen, MD; Sadhan M, PhD (Houston, TX) Introduction: The search for an effective therapy of Glioblastoma Multiforme (GBM) continues. Imaging Genomics, a newly emerged field, links gene expression profiles with MRI phenotypes (Zinn et al, 2011, 2012). MRI FLAIR was found to correlate with cellular invasion in GBM, thus, whole genome quantitative imaging analysis can reveal functional microRNA gene regulatory networks as novel targets for cellular invasion in GBM. Methods: Laboratory study. Results: A biochemical screen transfecting 885 known miRNAs into MGMT expressing T98 glioblastoma cells was performed to identify those miRNAs suppressing MGMT expression. Top candidates were confirmed using multiple adherent and neurosphere glioblastoma lines. We found that miR 603 consistently down regulated both MGMT protein and mRNA expression. Injection of miR 603 into murine glioblastoma xenografts down regulated MGMT expression in vivo. Importantly, antagomir introduction into cell lines that natively express high levels of miR 603 restored MGMT expression and TMZ resistance. MGMT mRNA preferentially affinity precipitated with biotinylated miR 603 and the predicted miR 603 binding region in the MGMT 3’UTR was necessary for suppressing luciferase activity in a luciferase 3’UTR assay. Finally, high expression of miR 603 correlated with low MGMT expression in clinical specimens and clinical response to TMZ. Methods: We performed radiogenomic mapping of MRI and corresponding genomic data in 78 TCGA patients. The top microRNA gene regulatory network was biologically validated by luciferase reporter assays, gain and loss of function using tet inducible lentiviral microRNA expression systems, as well as si/ shRNA, small molecule inhibitor/recombindant protein in vitro experiments and in vivo orthotopic xenograft models. Small animal 7T MRI T2/FLAIR was used for imaging genomic validations. Results: The top up regulated gene in high invasion MRI phenotypes was PERIOSTIN (POSTN). The top down regulated microRNA (miR 219) was validated to bind to POSTN. Glioblastoma derived stem cells (GSCs) from high FLAIR GBM patients correlated with levels of POSTN and increased invasion in vitro and in orthotopic xenograft tumor models on histological sections and MRI. Functionally, miR 219 overexpression reduced POSTN protein levels, while recombinant POSTN, neutralizing antibody, and shRNA experiments significantly altered cellular invasion in vitro and in vivo. MRI T2/FLAIR signal highly correlated with POSTN levels and the degree of cellular invasion in orthotopic xenograft models. Furthermore, high POSTN and a high POSTN/ miR 219 signature resulted in decreased survival and shorter time to progression. Conclusions: miR 603 is a MGMT regulating miRNA and a potential predictive biomarker for response to TMZ. Conclusions: In this study, we validated a novel noninvasive diagnostic method to screen for functional networks of cellular invasion. POSTN inhibition can be a novel therapeutic approach to target invasion in GBM. Furthermore, targeted individualized molecular therapies can be based on diagnostic imaging genomics and can be monitored through out the treatment period. 25 23. Preclinical Studies Of Intratumoral Cellular Immunotherapy for Recurrent Meningiomas With Alloresponsive Cytotoxic T Lymphocytes 24. Prediction Of Outcomes After Surgical Resection Of Glioblastoma Using Contrast Enhancing And FLAIR Residual Tumor Volume Richard George Everson, MD; Horacio Soto, MS; Edward Ha, BS; Kate Erickson, BS; Colin Malone, BS; Rudi Scharnweber, MD, PhD; Emma Young, NP; Neil Martin, MD; Isaac Yang, MD; Bob Shafa, MD; Marvin Bergsneider, MD; Robert Prins, PhD; Linda Liau, MD, PhD; Carol Kruse, PhD (Los Angeles, CA) Matthew M. Grabowski; Pablo Recinos, MD; Michael Vogelbaum, MD, PhD (Cleveland, OH) Introduction: Approximately one third of primary brain tumors are meningiomas and a third of those will display aggressive behavior, leading to recurrence. Since few experimental therapies are available for this subset of patients, we explored a cellular immunotherapeutic approach for the treatment of recurrent atypical meningiomas. Methods: We generated alloresponsive cytotoxic T lymphocytes (alloCTL) against atypical meningioma surgical explants by mixed lymphocyte tumor reactions (MLTRs). We measured alloCTL viability, growth and anti meningioma cytotoxicity and evaluated to what degree this antitumor activity was HLA specific. Results: We found that nearly all low passage atypical meningioma cells (P1 3 explant cultures of UC LH and UC CB derived from surgically resected material) displayed high levels of class I human leukocyte antigen (HLA), which could be upregulated upon exposure to interferon gamma (IFN γ). Thus, we prepared alloCTL with IFN γ incubated, radiation inactivated (70 Gy) tumor cells using one way MLTRs, which led to a 8 14 fold alloCTL expansion over a 25 33 day period after their culture. At 2 weeks, the alloCTL cultures were ‹70% CD3+ and 80 85% viable. They displayed cytotoxic function toward the meningioma cells in 4 hr calcein AM cytotoxicity assays, i.e., specific lysis of 54% ± 2% SEM at a 30:1 effector to target ratio; the cytotoxicity could be inhibited between 24 50% with anti HLA A,B,C blockade, indicating alloCTL specificity for meningioma cell HLA. Conclusions: These preclinical data were used to support the inclusion of patients with recurrent meningiomas to our Phase I dose escalation clinical study (www.clinicaltrials. gov, NCT 01144247), which is predicated upon high levels of HLA expression by tumor cells that are not expressed on normal neuroglia. Multiple intratumoral adoptive transfers of alloCTL will be performed after they are made by one way mixed lymphocyte reaction, where only patient lymphocytes are needed to accomplish alloCTL generation. Thus, a personalized immunotherapeutic approach is approved and open to enrollment for patients with recurrent meningioma. Supported by NIH R01 CA125244 and the Joan S Holmes Memorial Research Fund. Introduction: Currently, contrast enhancing tumor volume is used to delineate tumor burden in patients with glioblastoma (GBM). However, the enhancing tumor volume may underestimate the full extent of tumor burden, as tumor infiltration into normal brain has been observed in non enhancing areas, which are characteristically hyperintense on T2 weighted sequences. The relationship of post surgical FLAIR residual tumor volume (RTV) to clinical outcome is not well understood. We hypothesized that contrast RTV and FLAIR RTV may be individually predictive of survival. Methods: We retrospectively analyzed patients who underwent primary surgical resection of a supratentorial GBM followed by standard radiation/chemotherapy. Patients were excluded if ‹18 years old, had preoperative chemotherapy/radiotherapy, other intracranial malignancies, or were without post operative imaging within 48 hours of surgery. A semi automated volumetric analysis tool was used to quantitatively measure RTV using contrast enhanced and FLAIR MRI. Clinical and outcome data were compared to contrast RTV and FLAIR RTV. Results: One hundred twenty eight patients met study entry criteria. Median age was 60 years (range, 23-86), with a median KPS score of 90 (range, 30-100) at diagnosis. Median overall survival was 13.75 months (range, 1-84.2). After separately adjusting each volume measurement for age and Karnofsky performance score (KPS), both log contrast RTV (p=0.039) and log FLAIR RTV (p=0.018) were individually predictive of overall survival. Conclusions: Individually, contrast RTV and FLAIR RTV may be predictive of survival in patients with GBM, supporting the concept that post operative evaluation of GBM resection should incorporate both enhancing and non enhancing components of tumor. 25. Progression Of Atypical Meningiomas Irrespective Of Adjunctive Radiation Heather M. Kistka; Jessica Bassett, BS; Cheryl Kinnard, RN; Allen Redmond, RN; Allen Sills, MD (Nashville, TN) Introduction: Atypical meningiomas(AM) are rare tumors with a heterogeneous natural history. Their varying growth rates and resistance to conventional therapies render them challenging to treat. This has led to dispute over the role of radiation in treatment. Methods: We retrospectively reviewed the medical records of 78 surgically treated AM at our institution from 2002 to 2011. Overall survival(OS) and time to progression(TTP) were analyzed using univariate and multivariate Cox regression analyses. 26 Results: There were an equal number of males and females with a mean age of 52 years. Average follow up was 58 months (range 12 192). Gross total resection was achieved in 64(82%) patients. Nineteen patients (24.4%) received adjuvant radiation. Seventeen patients (21.8%) experienced disease recurrence/progression following resection with a median TTP of 31.5 months. Univariate analysis revealed female sex(p=0.006), age at diagnosis(p=0.023), and preoperative tumor size(p=0.020) as predictors of increased TTP. Neither extent of resection nor adjuvant radiation significantly prolonged TTP(p=0.693 and p=0.374 respectively) or OS(p=0.330 and p=0.084 respectively). Multivariate analysis did not reveal any independent predictors of increased TTP or OS. Conclusions: This series describes outcomes of CNS hemangiopericytomas from a nationwide patient population. In this study, overall survival benefit is only found when gross total resection can be accomplished, and it is combined with radiation therapy. 27. Radiographic Predictors Of Functional Recovery In Adult Posterior Fossa Ependymomas Zaman Mirzadeh, MD; Peter Nakaji, MD; Randall Porter, MD; Robert Spetzler, MD; Nader Sanai, MD (Phoenix, AZ) Introduction: Adult posterior fossa ependymomas have a relatively favorable prognosis compared with other intraparenchymal brain tumors. Following gross total resection and adjuvant radiation therapy, 10 year survival rates now approach 83%, emphasizing the importance of preserving neurological function. Here, we identify predictors of functional outcome following microsurgical resection. Conclusions: A subset of AM in our analysis were prone to progression irrespective of initial treatment. The use of adjuvant radiotherapy did not significantly prolong TTP or OS in our sample. As radiation introduces risk to patients without benefit, it should not be used as a first line treatment. Given the uniquely aggressive nature of a fraction of AM, further research should be aimed at identifying factors that render those tumors more prone to growth. Methods: We identified patients with newly diagnosed grade II posterior fossa ependymomas surgically treated at the Barrow Neurological Institute between 1996 and 2011. Pediatric patients were excluded. Routine clinical and radiographic variables were retrospectively collected, including volumetric extent of resection, cystic changes, peritumoral T2 signal changes, progression free survival, and overall survival. 26. Radical Resection Plus Radiation Therapy For Central Nervous System Hemangiopericytoma Adam M. Sonabend Wothalter, MD; Brad Zacharia, MD; Hannah Goldstein, BS; Samuel Bruce, BS; Dawn Herschman, MD; Alfred Neugut, MD; Jeffrey Bruce, MD (New York, NY) Results: Forty five patients were identified with median follow up of 72 months. Median progression free survival and overall survival were 5.2 and 6.0 years, respectively. Greater extent of resection and the adjuvant radiotherapy were both associated with improved survival. In univariate analyses, tumor size (p=0.016), cystic changes (p<0.001), and post operative T2 signal (p<0.001) predicted the rate of neurological recovery. Interestingly, multivariate regression analysis identified cystic changes (p=0.009) and post operative T2 signal (p=0.015) as independent predictors of slower neurological recovery. Specifically, patients with cystic changes and increased peritumoral T2 signal recovered their baseline KPS by 1 year, while those without these features improved by 6 weeks. Introduction: Central nervous system (CNS) hemangiopericytomas are relatively uncommon and are unique among CNS tumors as they can originate or develop metastasis outside the CNS. Most of the literature on this disease consists of single institution case series collected over long periods of time, and thus may reflect selection bias and might not be representative of the outcomes of current treatment paradigms. Methods: We queried the Surveillance Epidemiology and End Results (SEER) database to investigate the clinical behavior and prognostic factors for hemangiopericytomas originating within the CNS during the years 2000 2009. Results: We identified 227 patients with a diagnosis of CNS hemangiopericytoma. Age, radiation therapy, and gross total resection plus adjuvant radiation were significantly associated with survival on univariate analysis. On the multivariable model, age, location and adjuvant radiation therapy were significantly associated with prolonged overall survival. Older patients had a hazard ratio of 1.90 (95% CI: 1.28 2.83, p=0.001) of mortality from hemangiopericytoma. Patients with supratentorial lesions were found to have prolonged survival, with infratentorial tumors associated with a hazard ratio of 2.89 (95% CI: 1.03 8.06, p=0.043). The only treatment paradigm to confer a survival advantage was gross total resection plus radiation therapy. Patients undergoing this combination therapy were found to have significantly better survival, with a hazard ratio of 0.031 (95% CI: 0.01 0.95, p=0.04). Conclusions: Following microsurgical resection of posterior fossa ependymomas, cystic changes and increased peritumoral T2 signal are independent predictors of the rate of neurological recovery. Further study should examine the biological correlates underlying these radiographic features of adult posterior fossa ependymomas. 27 28. Rapid, Label Free Detection Of Microscopic Brain Tumor Boundaries With Coherent Raman Scattering Microscopy Daniel Orringer, MD; Minbiao Ji, PhD; Christian Freudiger, PhD; Shakti Ramkissoon, MD; Sandro Santagata, MD, PhD; Oren Sagher, MD; Sunney Xie, PhD (Ann Arbor, MI) Introduction: Surgery is an essential component in the treatment of brain tumors. However, delineating tumor infiltrated tissue from normal brain remains a challenge. Here we describe the use of Coherent Raman scattering (CRS) microscopy for differentiating healthy brain from tumor infiltrated brain based on histologic and biochemical differences. Unlike traditional histopathology, CRS is a label free technique that can be rapidly performed in situ. Methods: All experiments were performed using an established system for CRS microscopy. We started by comparing the ability of CRS and H/E to differentiate tumor from normal brain in frozen tissue sections from infiltrative human glioblastoma xenograft models. To demonstrate the ability of CRS to detect tumor infiltration in unprocessed tissue specimens we imaged fresh 2mm thick tissue sections from normal and tumor bearing mice. Finally, to simulate the in vivo use of CRS during surgery, we imaged superficial human tumor xenografts implanted in SCID mice. Results: In our experiments there was excellent correlation between CRS and H/E based tumor detection (K=0.98, (95% CI 0.96 0.99). Frozen and fresh tissue CRS imaging demonstrated both normal brain structures and and tumor infiltrated brain with excellent clarity and accuracy. We also demonstrated, that tumor detection with CRS is possible in vivo, revealing tumor margins that are invisible under the standard operative conditions. Methods: Using annexinV FITC labeling, we assessed the correlation between phosphatidylserine expression and SapC DOPS mediated death in human brain cancer and normal cells. Fluorescently labeled nanovesicles [SapC DOPS CVM (CellVue Maroon)] were used to test PS specific binding in vivo. To evaluate selective targeting of metastatic brain tumors induced with the luciferase expressing cell line MDA MB 231 luc D3H2LN, SapC DOPS CVM were systemically injected and colocalization assessed by luminescence/fluorescence in tumor bearing animals. Results: PS expression in cultured tumor cells correlated positively with SapC DOPS induced death. SapC DOPS CVM binding to tumor regions was seen in brain tumor tissues from patients. Selective targeting of brain tumor cells by SapC DOPS was observed in astrocyte Gli36 co cultures, a model that better resembles the in vivo tumor environment. Synergistic anticancer effects were observed after co treatment of glioma cell lines with SapC DOPS and chemotherapeutic drugs that promote PS externalization. Providing strong evidence that SapC DOPS targets PS, masking cell surface PS in U87EGFR Luc glioma cells with lactadherin C2 or beta 2 glycoprotein 1 inhibited binding by SapC DOPS CVM in vivo. Additionally, selective targeting of brain metastatic tumors was evidenced by colocalization of bioluminescent (MDA MB 231 luc D3H2LN) and fluorescent (SapC DOPS CVM) signals using animal models. Conclusions: These results support SapC DOPS as promising diagnostic and therapeutic agents for primary and metastatic brain tumors. Conclusions: By providing the surgeons with rapid histologic assessment of the operative field, CRS microscopy may ultimately improve the safety and accuracy of tumor surgeries where tumor boundaries are visually indistinct. FIGURE LEGEND: In vivo CRS microscopy imaging in an acute cranial window preparation in mice 24 days post implantation of human GBM xenografts. CRS microscopy demonstrates a clear distinction between tumor infiltrated areas (T) and non infiltrated brain (N) (a). Brightfield microscopy demonstrates no gross differences within the same FOV (b). High magnification views within the tumor (c), at the tumor/brain interface (d), and within normal brain (e) demonstrate the ability of SRS to image the architectural differences between tumor and normal brain. 30. Surgery For Primary Supratentorial Brain Tumors In The United States, 2000 To 2009: The Effect Of Provider Caseload On Complication Rates 29. SapC DOPS Nanovesicles Selectively Target Externalized Phosphatidylserine And Identify Metastatic Brain Tumors Victor Blanco, PhD; Zhengtao Chu, MD, MS; Ashley Stevens, BA; Ady Kendler, MD, PhD; Ronald Warnick, MD; Xiaoyang Qi, PhD (Cincinnati, OH) Results: Several complications of biopsy and craniotomy occurred less frequently for high volume centers. Patients treated by high volume surgeons (‹=20 cases/year) were 47% less likely to have a postoperative neurological complication, including infarction or hemorrhage (p=0.013). Patients treated in high volume hospitals (‹= 75/year) were less likely to develop hematoma (p‹0.001), hydrocephalus (p=0.006), and require placement of a ventriculostomy (p=0.013). Patients treated by high volume surgeons and hospitals were also less likely to experience renal (p=0.005), pulmonary (p‹0.001), and infectious complications (p‹0.001), including pneumonia (p=0.002). In the multivariate analysis adjusting for age, sex, race, tumor grade, medical Introduction: Though research into the pathogenesis of primary and metastatic brain tumors has advanced, current therapies still show limited efficacy. Saposin C dioleoylphosphatidylserine (SapC DOPS) nanovesicles are a novel antitumor agent that selectively target exposed phosphatidylserine (PS) on brain tumor cell membrane surface and induces cell death. We evaluate SapC DOPS in binding PS exposing cancer cells and its ability to target tumors. Victoria Trinh; Jason Davies, MD, PhD; Mitchel Berger, MD (San Francisco, CA) Introduction: Prior studies have suggested a volume outcome relationship for surgical resection or biopsy of primary brain tumors. The authors present analysis of these procedures between 2000 2009 to evaluate how procedural volume impacts complication rates. Methods: The authors performed a retrospective cohort study using data from the Nationwide Inpatient Sample (NIS) for 62,514 admissions for biopsy or resection of supratentorial primary brain tumors from 2000 to 2009. 28 comorbidity score, teaching status, weekend admission, and year of admission, low volume hospital (‹=25 cases/year) was significantly correlated with the presence of one or more of these complications (OR 1.6, 95% CI 1.3 1.9). The presence of one or more complications was significantly correlated with increased mortality (OR 6.5, p‹0.001) and delayed functional return (OR 0.29, p‹0.001). Median length of stay (LOS) was shortest at hospitals with ‹=100 cases/year (p‹0.001), and for surgeons with ‹=20 cases/year (p‹0.001). In the multivariate analysis, treatment by high volume hospitals and surgeons correlated with decreased mortality (p‹0.001, p=0.01) and more frequent routine discharge (p‹0.001, p=0.021). chromosomal instability and malignancy, anatomical location, histological appearance, gene expression and acetylation pattern. The mutational profile of a meningioma can largely be predicted based on its anatomical position, serving as the basis for targeted therapeutics. Conclusions: Consistent with the previous decade, the number of high volume hospitals and surgeons performing craniotomies and needle biopsies for primary brain tumor increased over the study period. Analysis of outcomes demonstrate that high surgeon and hospital volumes correlate with decreased risk of adverse outcome and support a shift towards regionalization of care. Introduction: Studies have suggested better outcome after complex surgery at hospitals with larger treatment volume, including meningioma craniotomy. We investigated whether previously reported US national trends toward neurosurgical centralization, as for intracranial aneurysm treatment, affected meningioma craniotomy practice patterns from 1988 2010. 32. Trends In Centralization Of Meningioma Surgery In The United States, 1988–2010: A Population Based Study Frederick G. Barker II, MD, FAANS, FACS; Pamela Jones, MD; William Curry, MD; Brian Nahed, MD; Daniel Cahill, MD, PhD (Boston, MA) Methods: Retrospective cohort study using the Nationwide Inpatient Sample (HCUP, AHRQ, Rockville, MD), 1988 2010. 31. The Novel Neoplasia Genes, TRAF7 And KLF4, Along With SMO And AKT1, Define Clinically Distinct Meningiomas Murat Gunel, MD, FAANS; Victoria Clark; Zeynep Erson Omay, PhD; Akdes Serin, PhD; Jennifer Günel, MD; Luis Kolb, MD; Ryan Hebert, MD; Bulent Omay, MD; Eric Holland, MD, PhD; Kaya Bilgüvar, MD; Joachim Baehring, MD; Philip Gutin, MD; Joseph Piepmeier, MD; Alexander Vortmeyer, MD; Cameron Brennan, MD; M. Pamir, MD; Türker Kilic, MD; Katsuhito Yasuno, PhD; _ Meningioma Genomics Group (New Haven, CT) Introduction: The genetic architecture of meningiomas, other than loss of NF2, is poorly understood. We aimed to comprehensively characterize the genomics of meningiomas. Methods: We performed genome wide genotyping, exome sequencing, ChIP seq and gene expression analyses of 50 tumors, followed by targeted resequencing of an independent cohort of 250 meningiomas. We correlated the genomic analyses with clinical findings. Results: Somatic mutations in just 5 genes, NF2, TRAF7, KLF4, AKT1 and SMO, explain the genetic basis of majority of benign meningiomas. Among the novel neoplasia genes, TRAF7, a pro apoptotic E3 ubiquitin ligase, is mutated in one fourth of all meningiomas. Mutations in TRAF7 co exist either with a recurrent K409Q mutation in another novel neoplasia gene, KLF4, a transcription factor known for its role in inducing pluripotency, or with the recurrent E17K mutation in AKT1. Hedgehog pathway activating SMO mutations are found in another 5%. These non NF2 meningiomas are nearly always benign, show chromosomal stability, include secretory and meningothelial histology, and mostly originate from the anterior and medial skull base with SMO mutants localizing to midline. In contrast, the vast majority of NF2 mutant tumors show genomic instability, localize to the cerebral and cerebellar hemispheres and are more likely to be malignant. Results: 31,921 adult craniotomy admissions to 1350 hospitals were studied; median age 59yr; 70% female. In hospital mortality was 1.8%, decreasing from 3.3% (1988 90) to 1.1% (2008 10). Annual US meningioma craniotomy caseload increased from 4300/yr (‘88 90) to 10100/yr (‘01 10). The number of US hospitals performing meningioma craniotomies remained largely stable: 1060 hospitals (1990), 1150 (2010). After multivariate adjustment (age, sex, race, payer, surgery year and admission type), larger hospital volume significantly predicted lower mortality both in 1988 2000 (OR 0.72 for tenfold larger volume, P=0.007) and in 2001 2010 (OR 0.64,P=0.001). Median hospital craniotomy volume (per patient analysis) increased from 7 cases/hospital/year (‘88 90) to 20 cases/hospital/yr (‘08 10). In 1988 90, 23% of meningioma craniotomies were at hospitals with ‹4 cases/yr, compared with 9% (2008 10). In 1988 90, 5% of meningioma craniotomies were at hospitals with 50+ cases/yr, compared to 38% (2008 10). Larger hospitals grew fastest in a per hospital analysis: median hospital volume increased from 3 cases/yr (1990) to 4/yr (2010), 90th percentile volume from 10/yr (1990) to 23/yr (2010), and 98th percentile volume from 23/yr (1990) to 58/yr (2010). Conclusions: Higher hospital volume continues to predict lower mortality after meningioma craniotomy. An increasing proportion of meningioma craniotomies in the US are being performed at high volume centers. Conclusions: Our results clearly identify clinically relevant meningioma subgroups, distinguishing them based on their mutually exclusive distribution of mutations, distinct potential for 29 33. Tumor Derived Vasculogenesis In von Hippel Lindau Syndrome Associated CNS Hemangioblastoma 34. Utilizing PVI Z CCL21 Vault Nanoparticles As A Novel Anti Tumor Therapy For Glioblastoma Jason Michael Frerich; Chunzhang Yang, PhD; Kristin Huntoon, PhD; Marsha Merrill, PhD; Russell Lonser, MD; Zhengping Zhuang, MD, PhD (Bethesda, MD) Isaac Yang, MD; Winward Choy, BA; Heather Garcia, BS; Andy Trang; Brittany Voth, BA; Nicole Cremer, BA; Linda Liau, MD, PhD; Robert Prins, PhD; Jian Yang, PhD; Leonard Rome, PhD (Los Angeles, CA) Introduction: von Hippel Lindau disease (VHL) patients develop a multitude of highly vascular tumors. It has been proposed that the vascular nature of these tumors is the product of reactive angiogenesis. Recent studies have shown that the characteristic islands of erythrocytes in VHL associated CNS hemangioblastomas develop from tumor cells. We hypothesized that a subset of vascular structures within VHL associated lesions are a result of tumor derived vasculogenesis. Methods: Tumor endothelial markers within CNS hemangioblastomas were visualized by immunofluorescence and three dimensional immunohistochemistry. Additionally, identified vascular elements from human vHL deficient murine xenografts were micro dissected and analyzed for loss of heterozygosity, as well as visualization by co localization immunofluorescence and fluorescence in situ hybridization (FISH). Results: Immunofluorescence showed small CD31 positive vascular elements that did not express Factor VIII. Three dimensional immunohistochemistry identified isolated islands of CD31 expressing structures. Micro dissected vascular structures demonstrated marked allelic imbalance after amplification with VHL gene flanking primers, indicating a loss of VHL and a somatic second hit deletion of the wild type allele. Co localization by immunofluorescence for HLA and CD31 further confirmed the presence of tumor derived vascular tissue. Moreover, FISH analysis of CD31 positive endothelial cells confirmed consistent loss of one copy of either chromosome 3 or VHL. Conclusions: The hemangioblast cell was identified as the embryologic progenitor cell for both endothelial cells and erythrocytes. We established that some VHL associated tumor cells differentiate into endothelial cells, confirming that developmentally arrested vHL deficient hemangioblast cells are responsible for VHL associated tumorogenesis, and maintain the potential to develop into endothelial cells. Introduction: While immunotherapy has demonstrated promise in clinical studies, overcoming immunosuppression within the tumor microenvironment remains a challenge. Naturally occurring ribonucleoproteins known as vault nanoparticles have been found capable of enclosing, protecting and delivering various antigens and drugs. In this study, we assay a bioengineered PVI Z vault containing CCL21, a potent lymphocyte chemoattractant, inducing antitumor immunity in glioblastoma in vivo. Methods: Using INT fusion proteins, CCL21 cDNA was integrated into PVI Z vaults. C57BL/6 mice 6 10 weeks old were injected with 1x10 6 GL261 cells into the left flank and given a single intratumoral injection/week for 3 weeks of either 5ug of recombinant PVI Z CCL21 vaults or 50uL PBS (control). Mice were euthanized if tumors were ulcerating or larger than 15mm in diameter. Survival and tumor growth rate were analyzed and compared. Results: GBM was successfully injected into our animal model. Tumor size was measured weekly, and continual tumor growth was present in 100% of untreated mice at each weekly interval. In the treatment group with CC21 vault nanoparticles, 33% of mice demonstrated tumor regression and decrease in size. For the other cohort, tumor size decreased on average by day 25, and stabilized until the conclusion of the study on day 38. Conclusions: PVI Z CCL21 vault nanoparticles can be bioengineered efficiently, and treatment with recombinant vaults demonstrated the potential for tumor control. This study demonstrates the in vivo efficacy of CCL21 vault nanoparticles, and its potential to be used as a potential novel therapy for high grade gliomas. 30 35. mTOR Inhibition As A Reasonable Strategy For Meningioma Treatment 36. miR 124 Systemically Enhances Antitumor Clearance By Inhibiting STAT3 Signaling And Reversing Glioma Associated Immune Suppression Christian Mawrin; Doreen Pachow; Elmar Kirches (Magdeburg, Germany) Amy B. Heimberger, MD, FAANS; Jun Wei, PhD; Fei Wang, PhD; Ling Yuan Kong, PhD; Shuo Xu, PhD; Tiffany Doucette, PhD; Sherise Ferguson, MD; Frederick Lang, MD; Ganesh Rao, MD; Gregory Fuller, MD; George Calin, PhD (Houston, TX) Introduction: Meningiomas are frequent intracranial tumors. Increased morbidity due to aggressive tumor growth and/ or recurrence is a significant problem. Because the mTORC1 (mammalian target of rapamycin complex 1) pathway is activated in many tumors, we explored the usefulness of mTORC1 inhibition as therapeutic strategy in meningioma cell lines and mouse models. Introduction: MicroRNAs (miRs) have been shown to modulate critical gene transcripts involved in tumorigenesis, but their role in tumor mediated immune suppression is largely unknown. Methods: On the basis of miRNA gene expression in gliomas using tissue microarrays, in situ hybridization, and molecular modeling, miR 124 was identified as the lead candidate for modulating signal transducer and activator of transcription 3 (STAT3) signaling, a key pathway mediating immune suppression of the tumor microenvironment. Methods: Tissue microarrays (53 meningiomas of all WHO grades) were used for immunohistochemical evaluation of mTOR related proteins. Expression of proteins and mRNAs was assessed by western blotting and real time PCR in 25 tumors. Meningioma cell lines including pairs of merlin positive or negative cells were used to assess sensitivity towards mTORC1 inhibitors by MTT and BrdU assays. Nude mice were either inoculated subcutaneously and the effect of systemic temsirolimus treatment (20 mg/kg daily) was monitored by measuring tumor weight and MRI estimated tumor volume, respectively. Results: MiR 124 is down regulated in all grades and pathological types of gliomas. Upon up regulating miR 124 in glioma cancer stem cells (gCSCs), the STAT3 pathway was inhibited, and miR 124 reversed gCSC mediated immune suppression of T cell proliferation and induction of Foxp3+ regulatory T cells (Tregs). Treatment of T cells from immunosuppressed glioblastoma patients with miR 124 induced marked effector response including up regulation of IL 2, IFN-Y, and tumor necrosis factor (TNF)-a. Both systemic administration of miR 124 or adoptive miR 124 transfected T cell transfers exerted potent anti glioma therapeutic effects in clonotypic and genetically engineered murine models of glioblastoma and enhanced effector responses in the local tumor microenvironment. These therapeutic effects were ablated in both CD4+ and CD8+ depleted mice and nude mouse systems, indicating that the therapeutic effect of miR 124 depends on the presence of a T cell mediated antitumor immune response. Results: The mTORC1 pathway was activated in most meningiomas independent of their WHO grade. A significant dosage dependent growth inhibition by temsirolimus was observed in all cell lines which was also affected by NF2 status. In xenograft models, temsirolimus treatment resulted in about 70% growth reduction of tumors (p‹0.01), which was paralleled by reduction of Ki67 mitotic index (p‹0.05) and reduction of mTORC1 activity (p70S6K phosphorylation) within the tumors. Conclusions: Preclinical data suggest usefulness of mTORC1 inhibitors to treat human meningiomas. Conclusions: Our findings highlight the potential application of miR 124 as a novel immunotherapeutic agent for neoplasms and serve as a model for identifying miRNAs that can be exploited as immune therapeutics. 31 2013 AANS/CNS SECTION ON TUMORS SCIENTIFIC PROGRAM ELECTRONIC POSTER ABSTRACTS 100. Pineal Region Tumours: Management Challenges Revisited Joseph Orinya Obande, MD; Abdullahi Jimoh, MD; Sunday Adewuyi, MD (Zaria/Kaduna State, Nigeria) Introduction: Pineal region tumours may affect only a relatively small subset of neurosurgical patients, they present enormous surgical challenge to the neurosurgeon; worse still in a resource poor setting, due to thier deep location, almost equidistant from all access points and surrounding neurovascular structures. We present a case report of a patient who had combination chemotherapy without histological diagnosis and had complete tumour regression. Methods: The patient's case folder was retrieved and information relating to presentation, the working diagnosis and supporting investigations were sought. She had pre chemotherapy ventriculo peritoneal shunt insertion for obstructive hydrocephalus. After due consultation with the Radio oncolgist, she had cyclical combination chemotherapy with cisplatin, etoposide and bleomycin. Results: The patient's clinical condition improved following the ventriculo peritoneal shunt insertion. Post chemotherapy Brain CT scan showed complete tumor regression. Conclusions: Tissue diagnosis may allow for precise, targeted management of pineal region tumours, however, in the absence of facilities which enable safe neurosurgery, resorting to the traditional chemo radiation is still a viable alternative. 101. A Nomogram For Individualized Estimates Of Survival Outcomes For Patients With Brain Metastasis Andrew E. Sloan, MD, FAANS; Jaime Venoechea, MD; Changhong Yu, PhD; Meihua Wang, PhD; James Dignam, PhD; Michael Vogelbaum, MD; Paul Sperduto, MD; Minesh Mehta, MD; Mitchell Machtay, MD; Michael Kattan, PhD; Jill Barnholtz Sloan, PhD (Cleveland, OH) Introduction: Brain metastases, which develop in 24 45% of cancer patients, account for 20% of cancer deaths annually, and are the most common intracranial mass lesions, with an incidence of 98,000 170,000 cases each year in the US. There are several therapeutic options, but selection of the optimal treatment for individual patients remains controversial. Classification schemes such as recursive partitioning analysis (RPA), and diagnosis specific graded prognostic assessment (DS GPA) have been validated, but these provide group, rather than individualized estimates of outcome. The purpose of this study was to develop and validate a nomogram for individualized patient prognosis which could be used for counseling patients. Methods: De identified data from 7 randomized controlled trials of brain metastasis in 2367 patients was obtained from the RTOG database. Overall survival was estimated using the Cox proportional hazards regression, RPA, and random survival forests (RSF) methods, and a nomogram was built using a concordance index to identify the best approach for each variable. Results: The Cox analysis outperformed other methods thus the nomogram was built to estimate survival probabilities and median survival based on the Cox model. The predicted values approximated the observed value within a 95% confidence interval. Conclusions: The nomogram based on the Cox model enabled better and more refined survival predictions than those based on RPA, DS GPA or RSF models. This predictor of outcome could be readily applicable to clinical practice in enabling patients and their physicians to make informed decisions regarding treatment options and will be provided as free software application. Future directions include external validation in a prospective dataset. 102. A Personalized Genetic Approach Using Circulating Mutant DNA To Monitor GBM Tumor Dynamics El Mustapha Bahassi; John Furgason, BS; Emily Cross; Ya Qin Li; Wenge Li, PhD; Jan Vrijg, PhD; Christopher McPherson, MD; Ronald Warnick, MD; Peter Stambrook, PhD; Olivier Rixe, MD, PhD; El Mustapha Bahassi, PhD (West Chester, OH) Introduction: Malignant gliomas are the most frequent and lethal cancers originating in the central nervous system. The most biologically aggressive subtype is the glioblastoma multiforme (GBM), a tumor associated with dismal prognosis. The current standard of care for GBM patients; surgical resection followed by adjuvant radiation therapy and chemotherapy with the oral alkylating agent temozolomide; produces a median survival of only 15 months. Even with the addition of the last generation of imaging studies, clinical assessment of tumor progression versus pseudo progression remains difficult. This, combined with the high cost of these imaging modalities, can pose serious delays in treatment decisions and result in harm to the patient. Hence, there is urgent need for a sensitive, specific, noninvasive and low cost biomarker which could be used routinely to monitor disease status in patients on treatment. Methods: It is now well established that circulating mutant DNA (cmDNA) that originates in the tumor can be detected in the peripheral blood. We used next generation, paired end sequencing to analyze several GBM genomes and their isogenic controls and identified tumor specific mutations. These mutations were detected by polymerase chain reaction (PCR) in the patients; plasma and were used to follow disease progression over time. 32 Results: Here, we show that the amount of cmDNA detected in the plasma of 10 GBM patients on treatment correlates with the tumor status. Conclusions: Mutation associated biomarkers offer a reliable measure that would be useful for monitoring tumor response to specific therapies, detecting residual disease after surgery, and for long term clinical management. 103. Altered Expression Of The Endoribonuclease Dicer Has Prognostic Significance In Meningiomas Felipe Goncalves de Carvalho, MD; Sanjay Singh, PhD; Shahrzad Jalali, PhD; Gelareh Zadeh, MD, PhD (Toronto, Canada) Introduction: Meningiomas are the most common primary brain tumors and, although usually benign, they may also present malignant behavior. The endoribonuclease Dicer is crucial for microRNA biogenesis. Low expression of Dicer has been associated with cancer, even though there are no studies in meningiomas. Methods: We used tissue microarray (TMA) slides containing 59 samples of meningiomas from patients that underwent surgical resection. We performed immunohistochemistry for Dicer and scored its expression according to the following criteria: (0) no staining; (1+) less than 25% of positive cells; (2+) less than 50%; (3+) between 50% and 75%; and (4+) more than 75%. We considered the range from 0 to 2+ as low and 3+ to 4+ as high Dicer expression. Clinical correlation was made between WHO grade classification, tumor recurrence, post operative radiation therapy, cavernous sinus invasion, Mib1 index and Dicerexpression. Results: From the total of 59 patients studied, 42 (71.2%) had high Dicer expression and 17 (28.8%) low Dicer. In the high Dicer group, the WHO grade distribution was: 34 (81.0%) grade I and 8 (19.0%) grade II, with no grade III. The low Dicer group revealed: 7 (41.2%) grade I, 8 (47.1%) grade II and 2 (11.8%) grade III. In addition, the low Dicer group had higher percentage of tumor recurrence (47.1% vs 26.2%), post operative radiation (54.5% vs 19.0%), cavernous sinus invasion (45.5% vs 24.3%), and Mib1 index (4.05% vs 1.50%) when compared to the high Dicer group. 104. Withdrawn 105. Case Presentation: Atypical Presentation Of Cervical Meningioma Presenting With Acute Epidural Hematoma John Franklin Hamilton, MD, PhD, FAANS; James Boddu, BS; Joseph Watson, MD; Ernest Roos, MD (Great Falls, VA) Introduction: Meningiomas can present anywhere along the cranio spinal axis. The clinical signs and symptoms of spinal meningiomas are typical of slow growing space occupying lesions of the spinal canal. Clinical symptoms are normally indolent, gradual in presentation, and dependent on the tumor level and breadth. Spinal epidural hematomas are normally associated with coagulopathy and/or trauma. These lesions have the potential to rapidly expand and cause acute neurological decline, often requiring emergent surgical intervention. There is ample literature on the more common causes of epidural bleeds, but sparse data describing spinal epidural hematomas presenting secondary to cervical meningiomas. This study describes a patient lacking the common risk factors for a spinal epidural hemorrhage, who presented clinically with acute paraparesis from a spontaneous cervical spinal hemorrhage. Methods: The patient physical examination was most notable for dense paraparesis. Clinical workup was unremarkable for any typical causes of an acute epidural hematoma. A cervical spine MRI revealed a meningioma at the C1 2 level, at the proximal portion of the epidural hematoma. We hypothesized the pathogenesis of the meningioma as the causative agent of the acute epidural hematoma. Results: The patient’s C2 T1 laminectomy revealed an epidural hematoma compressing the cal sac from C3 T1 with an extra/ intradural mass lesion from C1 3 compressing the friable posterior epidural venous plexus, and therefore causing the hemorrhage. Conclusions: This case provides evidence that, though not previously considered, spinal meningiomas should be included in the differential diagnosis of spinal hematomas. This is especially the case when long term indolent pain is followed by acute symptoms without the commonly reported risk factors. Conclusions: Therefore, low Dicer expression in meningiomas can be related to tumor aggressiveness and a worse clinical course. 33 106. Case Presentation: Management Of Subacute Complete Paralysis Secondary To Intraspinal Neuroblastoma In The Pediatric Patient John Franklin Hamilton, MD, PhD, FAANS; James Boddu, BS (Great Falls, VA) Introduction: Neuroblastomas are the most commonly encountered extracranial pediatric neoplasms. Prognosis of affected patients is dependent on age, staging, and the pathology of the neoplasms, and this in turn affects treatment. A review of the literature reveals a constant debate between surgical or non surgical management of these types of neoplasms. However, the literature unanimously reveals a poor prognosis in patients with severe acute progressive neurological deficits, regardless of treatment type. The novel case herein reports a 3 month old patient with full resolution of a 4 day history of complete lower extremity paralysis status post neurosurgical intervention. Methods: Magnetic resonance imaging showed complete spinal cord compression by a thoracolumbar intracanal extradural mass that was contiguous with a paraspinal mass. Further pathological and radiological analysis, including MIBG and bone scintigraphy, showed that the mass was consistent with a non metastatic neuroblastoma. The patient subsequently underwent a multilevel laminectomy that allowed for resection of the intraspinal mass and decompression of the spinal cord.This was followed by adjuvant therapy on a delayed basis. Results: Fortunately, despite their prolonged lower extremity paralysis the patient regained full neurological function with resolution of spinal cord compression on radiographic imaging at 6 months follow up. Conclusions: Currently, research states that patients with prolonged severe neurological deficits secondary to an intraspinal neuroblastoma have a very slim chance in regaining neurological function, irrespective of surgical or non surgical management. This novel case seems to suggest that prompt surgical intervention followed by adjuvant therapy is the best treatment for these patients, given the potential benefit of rapid recovery of neurological function. 107. Withdrawn 108. Comparison Of Coagulation Activation In Malignant Primary Brain Neoplasms And Meningioma Lara K. Ronan; Brett Gourley, MD; Deborah Ornstein, MD; Camilo Fadul, MD (Lebanon, NH) Introduction: Patients with malignant gliomas have a venous thromboembolism (VTE) risk of up to 30% over the course of the disease and are associated with systemic coagulation activation as assessed by increased blood levels of certain surrogate markers of coagulation activation. Meningiomas are benign brain tumors that are also associated with an increased VTE risk. Whether the presence or resection of meningiomas leads to systemic coagulation activation has not been clarified. Methods: We hypothesize that patients with glioblastoma multiforme (GBM) demonstrate increased systemic coagulation activation compared to healthy individuals. We further hypothesize that meningiomas are not associated with a significant increase in systemic coagulation activation and that this may account for the difference in VTE risk. We will test this hypothesis by measuring surrogate markers of systemic coagulation activation in patients with GBM and meningiomas before and after treatment and in age and sex matched healthy control blood donors. Markers of coagulation activation assayed for this study will include plasma D dimers, P selectin, tissue factor pathway inhibitor (TFPI), thrombin generation via calibrated automated thrombography and tumor tissue factor and TFPI expression by immunohistochemistry. Results: We are currently actively recruiting to this study and expect to complete arcual by the end of 2014. Conclusions: We expect this work to lead to clarification of coagulation abnormalities in patients with primary brain tumors and may result in identification of novel markers of VTE risk in these patients. 109. Concurrent Glioblastoma With Primary CNS Lymphoma Zaitun Zakaria; Eoin Fenton, MD; Ayman Khalil, MD; Muhammad Taufiq Sattar, MD (Dublin 9, Ireland) Introduction: The standard treatment of Glioblastoma(GBM) includes maximal surgical resection,followed by radiotherapy and concomitant and adjuvant chemotherapy. This however does not exclude the immunocompromising effect,which includes risks of lymphomatous disease. Methods: A 69 year old male underwent right temporal craniotomy and debulking of the lesion, confirmed to be GBM with positive MGMT promoter. He was commenced on Stupp prorocal with concurrent Temozolomide. His treatment completed 2 months after his initial presentation and a month later, he proceeded with first cycle of adjuvant chemotherapy. This was complicated with large pulmonary embolism and left lower limb deep vein thrombosis. Follow up MRI Brain revealed a recurrence of his tumour. There was also a new enhancing lesion in the left frontal lobe, measuring 1.5cm in dimension, thought likely to be a multifocal disease. He subsequenly underwent further debulking of his original tumour and stereotactic biopsy of the contralateral lesion. His debulking specimen revealed Astroctoma Grade III. Histopathologic evaluation from the left side showed primary CNS B cell Lymphoma. He deteriorated during chemotherapy and died 10 months after his original presentation. Results: We describe herein an interesting case of primary GBM with concurrent primary CNS lymphoma diagnosed 2 months after completion of Temozolomide treatment. To best of our knowledge, this is the first case reported in literature. This was observed on his surveillance MRI Brain 2 months after completion of treatment, therefore, the suspicion exists that the lesion may have developed while he was on treatment. To best of our knowledge, this is the first case reported in literature. 34 Conclusions: Regular follow up of glioma patients who recieve Temozolomide is recommended, particularly with risk for secondary malignancy from treatment associated immunosuppression. 111. Cortical GABAergic Excitation Contributes To Epileptic Activities Around Human Glioma. An Electrophysiological Study Johan Pallud, MD; Laurent Capelle; François Xavier Roux; Gilles Huberfeld (Paris, France) Introduction: Brain gliomas induce seizures in a majority of patients. Excitatory glutamatergic mechanism are shown to be involved in the generation of epileptic activities in the cortex surrounding gliomas. However, the contribution of defective Chloride homeostasis and paradoxical excitatory GABAergic mechanisms, crucial in other epilepsies, is unknown. 110. Correlation Of Histopathology To ALA Induced Fluorescence in Meningiomas Sam Eljamel, MD, FRCS; Tan Hon, MBBS; Carol Goodman, RN (Dundee, United Kingdom) Introduction: Meningiomas comprise 13 30% of primary intracranial tumors and are only less frequent than intracranial gliomas. They can occur anywhere in the cranium and the spine and have varied pathology. Removal of meningiomas in certain locations can be challenging, we explored the use of ALA induced fluorescence to guide intracranial meningiomas; resection and its corrolation to histopathology. Methods: We studied in neocortical slices from the security margin resected around human brain gliomas, the occurrence, networks, cells, signaling and origin of epileptic activities. Results: Postoperative glioma tissues of 69% patients spontaneously generated interictal like discharges. These events were synchronized in superficial layers of cortical columns in the neocortex surrounding glioma areas that presented a tumor infiltration and had a high frequency oscillation signature. Interictal like events depended on glutamatergic transmission but also on depolarizing GABAergic signaling. Up to 65% pyramidal cells were depolarized by GABA released by interneurons. This effect was related to perturbations in Chloride homeostasis, due to an abnormal load by the co transporter NKCC1. Ictal like activities could be exclusively generated in these epileptogenic areas. Methods: Twenty nine consecutive lesions with MRI differential of meningiomas were included in this analysis, including 17 supratentorial, 10 infratentorial and one thoracic. Twenty three were females, the mean age was 55.4 years and the final diagnosis was meningioma in 21 (72.4%). All these patients received 1.5 g 5 aminlevulinic acid (ALA) orally about 3 hours before surgery. Surgical resection was aided by using the blue light of the microscope (Pentero, Zeiss, Germany). The fluorescence was graded into strong (very red fluorescent), faint (pink) and moderate (in between red and pink). Conclusions: These activities sustained by excitatory effects of GABA, as those reported in human temporal lobe epilepsies, suggest that cellular Chloride regulation processes affecting oncogenesis are involved in the excitatory/inhibitory imbalance causing epileptic activity in peri tumoral tissue. Results: Fluorescence was detected in 22 (78.6%), of which twenty were intracranial meningiomas. Strong fluorescence signal was observed in nine of all lesions (32%) all of which were intracranial meningiomas (45%). Moderate fluorescence was noted in seven lesions (25%) all of which were intracranial meningiomas (35%). Faint signal was observed in six (14.3%) four of which were meningiomas (20%). Seventeen of intracranial meningiomas were WHO grade I (85%) and three (15%) were grade II. Total excision (Simpson grade 1) was achieved in all meningiomas. There was no correlation between histological type, ALA dose, or time to fluorescence and the intensity of fluorescence. Only two patients developed significant drop in their blood pressure (7.1%). Conclusions: Intracranial meningiomas fluoresce after oral ALA at a dose of 12 35 mg/kg body weight. ALA induced fluorescence is safe and helpful in intracranial meningioma surgical resection, but there was no correlation to histology. 35 112. Defining The Target For Radiation Therapy Of Meningiomas: A Multidisciplinary Study Of Interobserver Variability day to under 100 cc/day by the 11th day of radiation therapy. On postoperative day #22 the EVD was clamped, and the patient remained asymptomatic the following day. A new brain MRI showed significantly decreased size of the germinoma along with flow artifact across the floor of the third ventricle, and his EVD was removed. The patient's hydrocephalus did not recur over the following month. Stephanie Elizabeth Weiss, MD; Paul Kelly, MD; Edward Mannarino, BS; Fred Hacker, PhD; John Lewis, PhD (Philadelphia, PA) Introduction: We hypothesize significant inter observer variability exists in GTV and CTV for meningioma radiation planning. We undertook a multidisciplinary study among brain tumor experts to test this hypothesis. Methods: The expert group included 2 CNS radiation oncologists, 3 tumor neurosurgeons, and 2 neuro radiologists. De identified contrast enhanced MR/CT datasets of 2 cases of meningioma were co registered in the treatment planning system. Each observer received tutorials on GTV/CTV concept and contouring tools. Each was asked to define GTV and CTV for two cases, blinded to the delineations of other participants. CERR Matlab tool was used to compare volumes. Kappa statistics measured of corrected overlap agreement: 0= poor, 0.01; 0.20 slight, 0.21; 0.40 fair, 0.41; 0.60 moderate, 0.61; 0.80 substantial, and 0.80; 1.00 almost perfect agreement. CCC measured inter observer reproducibility. Results: Case 1, Grade 1 sphenoid meningioma: kappa=GTV 0.56, CTV 0.53 (<0.001); Case 2, atypical parasagittal meningioma: kappa = GTV 0.37, CTV 0.27 (GTV 0.41 (95% CI: 0.375 0.852, p<0.001) indicating poor reproducibility. CCC for CTV was not computed due to extreme variation. Conclusions: In this pilot substantial inter observer variability exists in meningioma target definition. Over contouring increases normal tissue exposure. Under contouring increases recurrence risk. Radiosurgery effectively reduces margins to zero (GTV=CTV), an approach counter conceptual to the maxim of maximal safe resection. Our findings suggest lack of physician consensus regarding target volume. We suggest a large scale study to confirm these findings and consideration of a multidisciplinary consortium to standardize target volumes. 113. Delayed Patency Of Endoscopic Third Ventriculostomy With Radiation Induced Reduction In Mass Effect: Case Illustration William C. Gump, MD; Ian Mutchnick, MD (Louisville, KY) Introduction: Endoscopic third ventriculostomy (E3V) is an established option for treatment of obstructive hydrocephalus and is often performed concurrently with biopsy of an obstructing mass lesion. Delayed failure is a known complication. We report the case of a patient whose E3V became functionally patent in a delayed fashion, three weeks postoperatively, when mass effect on the brainstem had been adequately relieved. Methods: A 13 year old boy presented to the emergency department with symptomatic obstructive hydrocephalus from a pineal region tumor. He underwent endoscopic biopsy, E3V, and external ventricular drain (EVD) placement. Results: Pathology was consistent with pure germinoma. The patient returned to surgery four days later for a secondary E3V. He remained drain dependent, and initiated radiation therapy on postoperative day #7. EVD output declined from over 300 cc/ Conclusions: Resolving mass effect from a rapidly shrinking pineal region tumor can delay relief of hydrocephalus from E3V, but has the potential to ultimately result in shunt independence. 114. Development Of A Three Dimensional Cell Culture Of Glioblastoma And Characterization Of A Novel Anti Tumoral Metabolic Treatment Anna Magdalena Wilk; Jennifer Mullinax, MD; Luis Del Valle, MD; Frank Culicchia, MD; Krzysztof Reiss, PhD (New Orleans, LA) Introduction: Because of the rapid growth, rate of recurrence, heterogeneity and resistance to therapies, Glioblastomas constitute one of the most aggressive human cancers. Therefore, advancements in research tools, including cell culture and animal models represent a challenge for basic research and are necessary for the development of more effective treatments. Methods: We are developing the 3 Dimensional cell culture model in which primary Glioblastoma cells are forced to form multi cellular Glio Spheres. This approach allows cells to grow for several months without losing their glial phenotype, the main problem with Glioblastoma culture. We use Seahorse Analyzer to characterize metabolic properties of Glio Spheres by measuring Extracellular acidification and Oxygen consumption rates; We also evaluate mitochondrial membrane potential, cell survival and response to a common lipid lowering drug, fenofibrate. Results: 1) Glio Spheres utilize both glycolysis and oxidative phosphorylation to sustain their metabolism, but unexpectedly, they do not show glycolytic reserve; 2) Fenofibrate induces acute inhibition of mitochondrial respiration which was partially compensated by glycolysis and/or glutaminolysis; 3) Fenofibrate compromises mitochondrial potential, accompanied by a G0/G1 cell cycle arrest, which was followed by massive apoptosis. Conclusions: Here, we demonstrate a new approach to develop 3 dimentional cell culture system for primary Glioblastoma (Glio Spheres) and present their metabolic profiles. We also include studies on fenofibrate, which has strong anti tumoral effect with low systemic toxicity, and could be introduced as a supportive regimen to the conventional therapies. The Glio Spheres can be also implanted into the brains of immunodeficient mice, providing a clinically relevant model for testing anti tumoral regiments against Glioblastoma. 36 115. Discovery Of Novel Oncogenic SMO And AKT1 Mutations In Meningiomas 116. Dynamic Susceptibility Contrast And Dynamic Contrast Enhanced MR Imaging Characteristics Distinguish Microcystic Meningiomas From Traditional Grade I Meningiomas And High Grade Gliomas Peleg Moshe Horowitz, MD; Priscilla Brastianos; Sandro Santagata; Robert Jones; Aaron McKenna; Gad Getz; Keith Ligon; Paul van Hummelen; Emanuele Palescandolo; Matthew Ducar; Laura MacConaill; Anat Stemmer Rachamimov; David Louis; William Hahn; Rameen Beroukhim; Ian Dunn, MD (Boston, MA) Namath Hussain, MD; Bart Keogh, MD, PhD; Steven Rostad, MD; David Newell, MD; Ryder Gwinn, MD; Gregory Foltz, MD; Marc Mayberg, MD; Brian Aguedan; Valerie Good; Sarah Fouke, MD (Bloomfield Hills, MI) Introduction: Meningiomas are the most common primary tumor of the central nervous system. Although most are cured by surgery, 20%recur and tend to be minimally responsive to systemic therapy. The tumor suppressor NF2 is disrupted in approximately half of meningiomas, but the complete spectrum of genetic changes remains undefined. Introduction: Microcystic meningioma is a variant of meningioma with a multicystic appearance that can mimic intrinsic primary brain tumors, hemangioblastomas, and other non meningiomatous tumor types. Dynamic susceptibility contrast (DSC) and Dynamic Contrast Enhanced (DCE) imaging have been developed to differentiate such tumors types. Methods: We performed whole genome or whole exome sequencing of 17 Grade I meningiomas and focused sequencing of an additional 48 tumors to comprehensively identify mutations, insertion deletions, copy number alterations, and genetic rearrangements contributing to oncogenesis. A mutational significance algorithm was used to distinguish driver and passenger events. Methods: 18 subjects with histopathological diagnosis of microcystic meningioma and a cohort of 12 subjects with grade I meningioma and 54 subjects with grade IV primary glioma were considered. Clinical variables including patient sex, age, extent of resection, surgical blood loss and need for adjunctive therapy were considered. DSC images were acquired at a temporal resolution of either 1500ms (3T) or 2000 ms (1.5T). Parameters including nCBV and kTrans were calculated with ROIs corresponding to enhancing tumor volume. Results: Overall, the tumors showed few somatic genetic events, consistent with their benign clinical status, but underscoring the potential importance of each individual event. Several tumors harbored more complex patterns of copy number changes and rearrangements including one tumor with chromothripsis. As expected, the NF2 gene was identified as the most frequently altered, with over half of tumors harboring NF2 disruptions. One sample had a novel translocation affecting the NF2 gene and a nearby region of chr22. In addition, several known cancer driver mutations including in SMO and AKT1 were seen primarily in NF2 wildtype tumors. Results: Preoperative DSC analysis demonstrated mean enhancing tumor nCBV values of 1.66 (+/ 0.60) for grade I meningiomas (meningoepithelial subtype), 5.74 (+/ 2.24) for Grade IV Astrocytomas, and 12.32 (+/ 3.81) for grade I meningiomas (microcystic subtype). nCBV measured within the enhancing portion of the tumor is significantly elevated in the microcystic meningioma subtype when compared with typical meningiomas (p<0.001) and Grade IV astrocytomas (p<0.0001). Preoperative DCE analysis demonstrated kTrans values of 0.49 min(e 1) (+/ 0.20) in grade I meningiomas (meningoepithelial subtype), 0.27 min(e 1) (+/ 0.12) for Grade IV Astrocytomas, and 1.35 min(e 1) (+/ 0.73 ) for grade I meningiomas (microcystic subtype). kTrans measured within the enhancing portion is significantly elevated in microcystic meningioma when compared with corresponding typical meningiomas (p<0.05) and Grade IV astrocytomas (p<0.0001). Intraoperative blood loss tended to increase with nCBV (R= 0.45) but was not statistically significant (p=0.085). Conclusions: This study begins to define the spectrum of genetic alterations in meningiomas. The discovery of novel drivers of meningiomagenesis with existing targeted therapeutics has the potential to rapidly transform the clinical management of meningiomas. Conclusions: An enhancing cystic lesion with elevated nCBV (‹10.3) or kTrans (0.49 min(e 1)) should lead surgeons to consider the diagnosis of microcystic meningioma, versus high grade glioma. Higher nCBV values are associated with a trend to increased intraoperative blood loss. 37 117. Endocrinological Outcomes Of Pure Endoscopic Transsphenoidal Surgery: An Uzbek Endocrine Center Experience 118. Endonasal Endoscopic Anatomy Of The Clinodial (C5) And Proximal Ophthalmic (C6) Internal Carotid Arteries Amjad Anaizi, MD; Almaz Kurbanov, MD; Vincent DiNapoli, MD, PhD; Jeffrey Keller, PhD; Lee Zimmer, MD, PhD; Philip Theodosopoulos, MD (Cincinnati, OH) Farrukh Karimov, MD; AM Akbutaev; RB Fayzullaev; SI Ismailov (Taskent, Uzbekistan) Introduction: Aim To analyze early remission, complications, and pituitary function recovery after pure endoscopic endonasal transsphenoidal surgery (PEETS), a novel method in pituitary adenoma treatment. Introduction: Increasing use of endoscopic approaches for the treatment of various intracranial pathology has necessitated neurosurgeons have a thorough understanding of the anatomy from an endoscopic endonasal perspective. We present a cadaveric anatomic study of the clinoidal and ophthalmic ICA from an endonasal endoscopic perspective. Methods: Testing of all basal hormone values and magnetic resonance imaging (MRI) were performed preoperatively and postoperatively in 121 consecutive patients who underwent PEETS in the period between 2011 and 2012. The series consisted of 37 somatotroph adenomas, 4 prolactinomas, and 8 corticotroph and 72 nonfunctioning adenomas. 110 were macroadenomas and 11 were microadenomas. Remission was defined as hormonal excess normalization on the third postoperative day in functioning adenomas and as normal MRI findings approximately four months postoperatively in nonfunctioning adenomas. Hypocortisolism was assessed through necessity for replacement therapy within 3 months postoperatively. Methods: Embalmed heads underwent thin cut CT scans for the purpose of neuronavigation. The heads were registered with our neuronavigation system. An endonasal endoscopic transsphenoidal exposure was performed. Various measurements were taken some of which include: the inter carotid distance at the level of the distal dural rings (DDR), the distance between the ICA at the distal dural ring and the optic chiasm and the distance between the ICA and the pituitary stalk. The ratio of inter carotid distance to distance between the OCRs was also calculated. Results: A total of 10 cadaver heads were studied. Neuronavigation was used achieving excellent accuracy in all cases. The average distance between the carotids at the distal dural rings was 10.4mm. The average distance between the ICA at the distal dural ring and the optic chiasm is 9.5mm. The average ratio of inter carotid distance at the DDR to inter OCR distance is 0.354. We also observed significant variability in the course of the distal C4, C5 and proximal C6 ICA. Results: Remission was achieved in 84% of patients: in 100% of microadenoma and 70% of macroadenoma patients (P ‹0.001, odds ratio [OR], 28.16, 95% confidence interval [CI], 1.61 491.36), respectively. Endocrinological complications occurred in 17.1% of patients: in 9% of microadenoma and 24% of macroadenoma patients (P = 0.049, OR, 3.06; 95% CI, 1.03 9.08). Duration of hydrocortisone replacement therapy was significantly shorter in microadenoma patients (P ‹0.001). Seventy five percent of preoperatively present hormonal deficiencies improved after the surgery. Between tumor types there were no significant differences in remission, complications, and normal pituitary function recovery. Conclusions: Expansion of endonasal endoscopic techniques for treatment of various intracranial pathology necessitates improved understanding of the clinoidal and proximal intradural ICA anatomy and its relationship to surrounding structures. This will enable surgeons to more reliably predict the location of the ICA and its relationship to surrounding structures, decreasing the potential for vascular injury. Conclusions: Patients with microadenomas had higher remission and lower complication rates following PEETS, emphasizing the necessity for early detection and treatment of pituitary adenomas. PEETS is a discussion worthy method for microprolactinoma treatment. 119. Endoscopic Surgical Management Of Grade IV Juvenile Nasopharyngeal Angiofibromas Amjad Anaizi, MD; John York, MD; Lee Zimmer, MD, PhD; Philip Theodosopoulos, MD (Cincinnati, OH) Introduction: Juvenile nasopharyngeal angiofibromas (JNA) are histologically benign vascular tumors found in prepubertal and adolescent males. These can be locally aggressive with potential intracranial extension. Traditionally these lesions have been treated using open surgical techniques, however recently endoscopic approaches have been implemented in hopes of minimizing morbidity. We present a series of stage IV JNAs treated endoscopically at our institution. Methods: We retrospectively reviewed the charts of patients with Stage IV JNAs treated endoscopically at our institution. We recorded the number of operations, estimated blood loss, extent of resection, any complications and length of hospital stay. 38 Results: 4 patients were surgically treated for stage IV JNAs. All are male with an average age of 16 years. Average follow up is 29.7 months. All patients underwent pre operative tumor embolization. All underwent an endonasal endoscopic approach with/without a Caldwell Luc approach. One patient underwent an initial open transfacial approach and required a subsequent endoscopic approach. Patients underwent an average of 2.25 resection operations. Mean EBL was 1829cc. A subtotal resection was achieved in all cases. Two patients underwent radiation therapy during the course of their treatment. There were no mortalities. Conclusions: Stage IV JNAs are difficult lesions to treat. Open surgical resection can achieve good tumor control, but can be exceedingly morbid. Given the tendency for these lesions to regrow, multiple surgeries are often required. We believe an endoscopic approach for subtotal resection in combination with pre operative embolization and post operative adjuvant treatment in select patients can achieve good tumor control while minimizing morbidity. 120. Epidemiological Datas Support Early Surgery Of Incidentally Discovered Diffuse Low Grade Glioma Emmanuel Mandonnet; Philip de Witt Hamer, MD, PhD; Johan Pallud, MD; Hugues Duffau (Paris, France) Introduction: Early surgery for incidentally discovered diffuse low grade glioma (DLGG) has been subject of debate, because of potential overtreatment in these clinically silent patients. We thus propose to compare the number of patients with silent DLGG Dying from Another Cause over a period of N years DAC(N) with the number of patients Dying from their Silent Glioma that became symptomatic during the same period DSG(N). Methods: We used DAC(N)=pxmxN, where p and m respectively denote the prevalence of silent DLGG and the overall mortality rate in the population. DSG(N) is given by DSG2+DSG3+DSG4, where DSGn(N)=inxdn(1)+inxdn(2)+…+inxdn(N), in being the incidence of symptomatic glioma of grade n arising from a silent DLGG and dn(x) the proportion of symptomatic glioma patients dying from their glioma of grade n after x years. To compute i3 and i4, we assumed that among high grade glioma, only those IDH1/2 mutated arised from a silent DLGG. Numerical values were estimates from the french register of CNS tumors, the national institute of statistics, and published series of glioma survivals. 121. Epilepsy Associated With Protoplasmic Astrocytoma: Case Report And Review Of The Literature William C. Gump, MD; Karen Skjei, MD; Shefali Karkare, MD (Louisville, KY) Introduction: Protoplasmic astrocytoma is a rarely described WHO grade II infiltrative tumor. We report a new case in a pediatric patient. Methods: A 4 year old girl presented with generalized seizures. MRI of the brain revealed an extensive diffuse nonenhancing area of abnormal signal involving the right frontal and temporal lobes. She was taken to surgery for biopsy, and returned to surgery eight months later for electrocorticography guided seizure focus resection. Seizure frequency decreased to zero over the following three months. Results: Protoplasmic astrocytomas account for roughly 5% of low grade astrocytomas. Compared with gemistocytic, protoplasmic astrocytomas have less potential to behave aggressively. In two case series encompassing 18 patients, average age at presentation was 25 years. Most lesions were in the frontal or temporal lobes. For 7 patients with unresectable lesions, biopsy was performed; all others underwent attempted gross total resection. Five patients subsequently received radiation therapy and one also had chemotherapy. The youngest patient (age 2 years at diagnosis) died 36 months after subtotal resection without further adjuvant therapy; all others were alive with or without residual tumor 2 to 108 months postoperatively. One additional case report describes a 3 year old with diffuse leptomeningeal disease who died from tumor progression despite chemotherapy. Although all patients presented with seizures, seizure outcomes have not been well documented. Our patient achieved seizure freedom. Conclusions: Protoplasmic astrocytoma is a rare low grade glioma which can be associated with medically resistant epilepsy. Tailored surgery for unresectable lesions can be beneficial for seizure control. Results: We found DAC(N)=Nx0,3/100 000. The curve DSG(N) was shown to grow exponentially with N, being below DAC(N) up to 4 years, crossing the curve DAC(N) at 4 years, and DSG(N) being twice DAC(N) at 8 years. Conclusions: Patients with silent DLGG are more likely to die from transformation of the silent DLGG to symptomatic glioma than dying from another cause with the silent DLGG, unless patient survival is expected to be less than 4 years. This epidemiological argumentation supports early surgery for incidentally discovered glioma. 39 122. Establishing Standard Performance Measures For Adult Brain Tumor Patients: A Nationwide Inpatient Sample Database Study Maryam Rahman, MD; Dan Neal, MS; Kyle Fargen, MD; Brian Hoh, MD (Philadelphia, PA) Introduction: The Agency for Healthcare Research and Quality (AHRQ) patient safety indicators (PSIs) and the Centers for Medicare and Medicaid Services (CMS) hospital acquired conditions (HACs) are used to evaluate the safety and quality of healthcare. We determined the incidence rates of PSIs and HACs among brain tumor patients in the Nationwide Inpatient Sample (NIS) database. Methods: We queried the NIS, part of the AHRQ Healthcare Cost and Utilization Project (Rockville, MD), for all hospitalizations between 2002 and 2010 involving a brain tumor using ICD 9 codes. To identify patients who had undergone surgery, we used brain tumor surgery ICD 9 codes. We used the SAS statistical software package (Version 9.3) to calculate means, standard deviations and frequencies for all patient and hospital characteristics and to estimate all PSI and HAC incidence rates. Results: Among the 501,908 hospitalizations involving a brain tumor in the NIS database, there were 102,046 occurrences of an AHRQ PSI, with 16% of patients experiencing one or more AHRQ PSI. For brain tumor patients treated without surgery 17.2% of patients experienced one or more PSI. For brain tumor patients treated with surgery 9.8% patients experienced one or more PSI. The most common PSIs included postoperative respiratory failure, deep vein thrombosis, and sepsis. The total number of HACs associated with brain tumor patients was 13,778, with 2.63% patients experiencing one or more HAC. For brain tumor patients treated without surgery 3.0% experienced one or more HAC. For brain tumor patients treated with surgery 7.4% experienced one or more HAC. The most common HACs included falls and trauma and pressure ulcers. Increasing comorbidity score was associated with increased likelihood of almost all PSIs and HACs. Conclusions: Patient safety and delivery of quality care is an important part of our national healthcare agenda. Our results demonstrate baseline national rates of PSIs and HACs in brain tumor patients. These data may be used to determine individual institutional improvements or success by comparison. 123. Expression Of JCV T Antigen In Glioblastomas Causes Nuclear Translocation of IRS 1 And Alterations In Faithful DNA Repair Mechanisms Anna Magdalena Wilk; Amanda Parker Struckhoff, PhD; Krzysztof Reiss, PhD; Frank Culicchia, MD; Luis Del Valle, MD (New Orleans, LA) Introduction: Despite significant advances in surgical techniques and new chemotherapeutic agents, Glioblastomas are always associated with poor prognosis. One of the molecular hallmarks of Glioblastomas is genomic instability, which leads to the development catastrophic mutations. Thus, basic DNA repair mechanisms responsible for the preservation of genomic integrity could be impaired in Glioblastomas. We have previously reported the detection of DNA sequences of the human neurotropic JC Virus and expression of its oncoprotein, T Antigen, in brain tumors of glial and neuroectoermal origin. Here we study the association of T Antigen with proteins that impair faithful DNA repair in Glioblastomas. Methods: We performed immunohistochemistry for gH2AX (a marker of DNA damage), IRS 1 and T Antigen and Rad 51 (the main component of homologous recombination DNA repair) in archival samples and primary cell lines derived from Glioblastomas. Results: We demonstrate the accumulation of IRS 1 in the cytoplasm of T Antigen negative tumors, while in T Antigen positive samples IRS 1 in translocated to the nucleus. Double labeling studies corroborate the co localization between IRS 1 and T Antigen. Immunohistochemistry for histone gH2AX, showed a much stronger immunolabeling in the nuclei of JCV T Antigen positive Glioblastoma cells, as well as co localization between gH2AX and nuclear IRS 1, and between nuclear IRS 1 and the major enzymatic component of HRR, Rad51. Conclusions: Our findings suggest the involvement of JCV T Antigen / IRS 1 signaling in the impairment of homologous recombination in Glioblastomas, a critical mechanism for the fidelity of DNA repair, which could provide a novel target for the treatment of these highly aggressive tumors. 124. Extracranial Metastatic Meningioma: Imaging Appearance With Bevacizumab Christine Lauro; Douglas Ney, MD; Robert Bert, MD, PhD; Allen Waziri, MD; Bette DeMasters, MD; Denise Damek, MD; Laurie Gaspar, MD (Aurora, CO) Introduction: Metastatic meningioma is a rare entity, occurring in less than 1% of all meningiomas. Bevacizumab has recently demonstrated encouraging anti tumor effect in the treatment of recurrent and progressive meningiomas. The imaging characteristics of meningiomas undergoing bevacizumab treatment have not been extensively described. Methods: While undergoing systemic therapy on bevacizumab with a sustained intracranial response, a 55 year old man with a locally recurrent WHO grade III meningioma developed a biopsy proven left sided neck metastasis and radiographic findings consistent 40 Conclusions: Fluorescence guided resection for complex meningiomas have shown to be an effective intraoperative tool to achieve maximal citoreduction. In meningioma lesions we assume that the breakage of the blood brain barrier increasing vascular permeability and by this mechanism the 5 ALA reaches the peritumoral area. with pulmonary metastases. The magnetic resonance imaging (MRI) appearance of this patient’s extracranial neck disease and pulmonary metastases differed from his intracranial disease. Results: The primary intracranial meningioma was a homogeneously, avidly enhancing extra axial mass on magnetic resonance imaging (MRI). The recurrent intracranial lesion was isointense to surrounding brain on T1 imaging and hyperintense on T2 weighted images. The radiographic characteristics of the patient’s neck metastasis differed from the primary lesion. The neck metastasis was weakly, inhomogeneously enhancing on both computed tomography (CT) and MRI. The mass was centered in the obliquus capitis inferior muscle and was associated with erosive bony changes. The neck lesion was isointense to muscle on noncontrast T1 imaging, and nearly isointense to gray matter on T2 weighted images. There were four subcentimeter, nonenhancing parenchymal lung nodules appreciated on chest CT, consistent with pulmonary metastatic disease. 126. Hyperostosis In Intracranial Pediatric Meningioma Jeffrey Murray; John Honeycutt, MD; Hayden Head, MD; Linda Margraf, MD (Fort Worth, TX) Introduction: Meningioma is the most common intracranial neoplasm in adults, though rare in children and adolescents. Cranial hyperostosis in association with adult meningioma occurs frequently. The osteopathophysiology of this phenomenon is poorly understood and controversial, with actual bone invasion by tumor or reactive changes due to adjacent tumor having been posited as explanations. Metalloproteins have also been suggested as playing a role. Hyperostosing meningioma is rarely reported in children. Conclusions: This case illustrates the imaging appearance of intracranial anaplastic meningioma and extracranial metastases while on bevacizumab. Further study of imaging characteristics of recurrent and progressive meningiomas while undergoing treatment with anti angiogenic therapies is warranted. Methods: Following IRB approval, the medical record of a child with intracranial hyperostosing meningioma was abstracted for diagnostic, treatment and outcome details. The medical literature on meningioma and hyperostosis conditions was surveyed. 125. Fluorescence Guided Resection Of Complex Meningiomas Results: A 15 year old boy presented with progressive nausea, vomiting and headaches. Gastroenterologic evaluations were negative and therapy for reflux disease was ineffective. Imaging revealed a lobulated solid cystic mass in the right frontal region, with overlying irregular cranial bone thickening. Skull palpation revealed painless fullness without scalp changes. Via a large craniotomy flap, the tumor was found to be arising from the dura and adherent to the skull, without gross invasion. The flap was hyperostotic and the inner table and cancellous bone were drilled out using a high speed air drill. The tumor was microsurgically completely resected and the bone flap was replaced. The lesion showed classic syncytial features, yet with hypercellularity and an elevated MIB 1 index, consistent with atypical meningioma, W.H.O. grade 2. Tumor was identified in the bone curettings. Due to the higher grade histology and tumor in the bone, adjuvant radiation therapy was administered. He remains in remission three years later. Salvador Manrique, MD; Lucino Castillo, MD; Jaime Torres Corzo, MD; Ricardo Berrone, MD (Mexico City, Mexico) Introduction: Recently, 5 aminolevulinic acid (5 ALA) has demonstrated optimizing surgical resection for high grade tumors incorporating selective accumulations of photosensitive protoporphyrin IX (PpIX). The extent of resection in intracranial brain tumors determine survival rate. For extra axial tumors, such as, meningiomas the usefulness of fluorescence guided surgery will help to achieve maximal resection in complex cases where occult tumor cells spreads beyond the arachnoid layer or in to bone structures. Methods: We present an illustrative case of a 37 year old female with past medical history relevant for overweight and penicillin allergy. Her symptoms were characterized by headache, nausea, amaurosis fugax, left eye ptosis with facial asymmetry. An MRI was done and a left frontal extra axial lesion was found. After written informed consent, she was brought in to operative room and standard microsurgical (Carls Zeiss Opmi Pentero 900®) and neuro navigations (AxiEM Medtronic, Inc.®) techniques were performed. 5 ALA was orally administered (20 mg/kg [Medac GmbH®)4 to 6 h prior to skin incision. There were no surgical complications. She was discharged 4 days after the tumor resection. Conclusions: Only a paucity of pediatric cases of hyperostosing meningioma have ever been reported. There is no reported correlation between hyperostosis and histologic tumor grade and bone invasion by tumor. Our report confirms that this phenomenon occurs in children. The pathophysiologic mechanisms may be the same as in adults. We recommend ongoing reporting of this rare condition in youth, so as to inform of preferred management strategies. Results: The patient did not experience any additional neurological deficits after surgery. There was no evidence of increased liver function test. The pathology report was consistent with a WHO Grade I meningioma. Currently the patient is seen in the outpatient clinic. Most of the general symptoms have remarkable improved. Facial asymmetry has also been substantially reduced. 41 127. Histopathologic Transformation Of Anaplastic Glioma And Not Radiographic Progression Is Associated With Reduced Survival Allen L Ho; Andrew Chi, MD, PhD; Fred Barker II, MD; Tracy Batchelor, MD, MPH; Shota Tanaka, MD; April Eichler, MD; Daphne Wang; Daniel Yang; Daniel Cahill, MD, PhD; William Curry, MD (Irvine, CA) Introduction: Histologic transformation to glioblastoma (grade IV) is often presumed when anaplastic (grade III) gliomas progress radiographically. We aimed to determine the clinical impact of histologically proven transformation. Methods: We retrospectively identified patients with anaplastic gliomas who had surgery at our center upon first radiographic progression. We examined the impact of clinical and molecular factors on transformation and outcome. Results: Between 1993 and 2012, 85 patients met study criteria; 24 with oligodendrogliomas, 22 with oligoastrocytomas, and 39 with astrocytomas. 33 (38.8%) patients transformed to glioblastoma. Transformation was associated with shorter overall survival (OS) from initial diagnosis (median OS 6.3 vs 17.4 years, p=0.001) and from second surgery (1.5 vs 10.8 years,). Conclusions: Fewer than half of radiographically progressive anaplastic gliomas transformed to glioblastoma histologically. Transformation is associated with reduced OS from the time of diagnosis and from the second surgery. Tissue diagnosis may be warranted for prognostic counseling at the time of radiographic progression. 128. Imaging Genomic Necrosis Mapping Reveals Gender Specific Survival And Molecular Determinants in GBM Pascal Zinn, MD, PhD; Pascal Zinn, MD, PhD; Rivka Colen, MD (Houston, TX) Introduction: Despite recent discoveries of new molecular targets and pathways, the search for an effective therapy for Glioblastoma (GBM) continues. A newly emerged field, imaging genomics, links gene expression profiles with MRI phenotypes. Cell death in GBM may arise from tumor suppressor and/or oncogene activation, amongst other mechanisms. Thus, an imaging genomic necrosis screen has the potential to uncover novel molecular determinants of cell death in GBM. Here, we present the first comprehensive radiogenomic analysis using quantitative necrosis MRI volumetrics and large scale gene and microRNA expression profiling in GBM. Methods: Based on The Cancer Genome Atlas (TCGA) and The Cancer Imaging Archive (TCIA) gene, microRNA, and quantitative MR imaging as well as histopathology data sets were created in 78 patients. Gender specific analysis was performed and the top concordant genes and microRNAs correlated with high volumes of necrosis were further characterized using Ingenuity Pathway Analysis, whole genome transcriptional factor analysis, and cognate microRNA gene networks were created. Results: Female patients demonstrated significantly lower volumes of necrosis than male patients. Thus, a gender specific analysis was chosen and revealed in both MRI and histopathology data that female patients with high necrosis had a significantly shorter survival compared to both females with lower necrosis or males with high necrosis. Survival in males was not statistically different in patients with high versus low tumor necrosis. The survival data was concordant with the genomic analysis suggesting that predominantly MYC driven oncogenic pathways were associated with necrosis in female patients, while male patients showed a strong positive association of the MRI necrosis phenotype with the P53 tumor suppressor pathway. Gender independent necrosis pathway analysis showed equal distribution of both tumor suppressors and oncogenes. Conclusions: Here, we propose a novel diagnostic method to screen for molecular correlates of necrosis in GBM. Our findings suggest distinct oncogenic pathways promoting MRI and histopathology necrosis phenotypes in male versus female GBM patients. 129. Impact Of Antidepressant Therapy On Overall Survival In High Grade Glioma Heather M. Kistka; Elliot Min, BA; Rebecca Kasl, BS; Soo Yang, BA; Lola Chambless, MD (Nashville, TN) Introduction: The prevalence of depression in patients with high grade glioma(HGG) is significantly higher than that of the general population. In prior studies, depression has been associated with decreased quality of life and shorter overall survival. Antidepressant therapy is a widespread and generally well tolerated treatment of depression which can increase quality of life. We investigated whether pharmacologic treatment of depression has an impact on overall survival. Methods: We conducted a retrospective cohort study of 206 patients with a diagnosis of HGG(WHO III/IV) between 2000 and 2011 treated at our institution. Univariate analysis isolated possible predictors of survival. Variables with p<0.1 were then included in a multivariate Cox model. Results: Median survival was 15.8 months. 37% of patients had a diagnosis of depression and 33% of patients were treated with an antidepressant. Univariate analysis of antidepressant treatment revealed significantly prolonged survival in the treatment group(p=0.02, median survival 18.0 vs. 14.3 mos). Analysis based on class of antidepressant was not significant. Multivariate analysis controlled for age, tumor grade, extent of resection, Karnofsky Performance Score, reoperation, antidepressant therapy, diabetes, radiation and temazolamide therapy. Antidepressant therapy was not an independent predictor of prolonged survival in this analysis(p=0.90). 42 Conclusions: Patients with HGG on antidepressant therapy have significantly prolonged overall survival in univariate analysis. Although this effect did not reach significance in multivariate analysis, the trend warrants further investigation. Prospective studies closely monitoring antidepressant treatment and its effects are necessary to evaluate the potential benefit of both improving quality of life and prolonging survival with a single therapy. 130. Withdrawn 131. Induction Of Antitumor Effect Of 5 Aminolevulinic Acid In Malignant Glioma By Low Frequency Ultrasound Fumio Yamaguchi, MD, PhD; Takayuki Asakura; Tadashi Higuchi, MD; Hiroshi Takahashi, MD, MSC; Takayuki Kitamura, MD, MSC; Akira Teramoto, MD, MSC (Tokyo, Japan) Introduction: High frequency sonodynamic therapy has been reported to be effective; however the effectiveness of low frequency sonication with sonodynamic agents was not studied. We investigated the feasibility of sonodynamic therapy for malignant glioma by low frequency ultrasound with 5 aminolevulinic acid (5 ALA), a precursor of protoporphyrin IX (PpIX) in heme synthetic process. Methods: In vivo tumor model was made by inoculating human glioma cell line U87 MG subcutaneously in nude mice. The tumor was sonicated by 25 kHz ultrasound 4 hours following administration of 5 ALA. Results: The tumor size decreased in 5 ALA administered (ALA(+)US(+)) mice, while increased in non 5 ALA administrated (ALA( )US(+)) mice and non sonicated mice (ALA(+)US( ). The immunohistochemical analysis revealed an apoptotic change in tumor tissue of 5 ALA (+) mice. The results showed the therapeutic effect of 25 kHz ultrasound for the glioma in 5 ALA administered tumor bearing mice by inducing apoptotic change of tumor cells. Conclusions: This is a first report to elucidate the feasibility of therapeutic use of 25 kHz ultrasound in sonodynamic therapy using 5 ALA as a sonosensitizer precursor. This may be a realistic intraoperative malignant gioma therapy in addition of tumorectomy, since 25kHz is a frequency of ultrasonic aspirator. 132. Integration Of Genome Wide Approaches Identifies lncRNAs Of Adult Neural Stem Cells And Their Progeny In Vivo Alexander Ramos; Aaron Diaz, PhD; Abhinav Nellore, PhD; Ryan Delgado, BS; Ki Youb Park, PhD; Gabriel Gonzales Roybal, PhD; Joanna Phillips, MD, PhD; Michael Oldham, PhD; Jun Song, PhD; Daniel Lim, MD, PhD (San Francisco, CA) Introduction: An emerging class of functional long noncoding RNAs (lncRNAs) have recently been characterized in developmental processes and disease states, including cancer. The subventricular zone (SVZ) of the adult mouse brain represents an ideal system for the study of lncRNAs in vivo. Throughout life, SVZ neural stem cells (SVZ NSCs) generate large numbers of neuroblasts that migrate to the olfactory bulb (OB) where they differentiate into interneurons. We leveraged this unique developmental system to interrogate lncRNA expression and function. Methods: We utilized complementary genome wide techniques including RNA seq, RNA CaptureSeq, and ChIP seq to associate specific lncRNAs with neural cell types, developmental processes, and human disease state, and performed shRNA mediated knockdown experiments in cultured SVZ NSCs to assess the function of these lncRNAs. Results: We were able to identify thousands of lncRNAs loci, including loci uniquely expressed in the SVZ. By integrating data from chromatin state maps, custom microarrays, and FACS purified cells, we stringently identify lncRNAs with potential roles in adult neurogenesis, and accurately predict their expression patterns in the SVZ and OB. shRNA mediated lncRNA knockdown demonstrated a role of lncRNAs in SVZ neurogenesis. Finally, we used our custom lncRNA microarrays to discover lncRNAs that are dysregulated in mouse models of glioma. Conclusions: Our data indicate that lncRNAs can play a role in neurogenic lineage specification of SVZ NSCs. More broadly, our data and workflow provide a uniquely coherent in vivo lncRNA analysis that will be relevant for future studies of lncRNAs in development and tumorigenesis. 43 133. Intermittent Obstructive Hydrocephalus Secondary To Third Ventricular Cysts J. Bryan Iorgulescu; Konstantinos Margetis, MD; A. Tsiouris, MD; Joshua Marcus, MD; Mark Souweidane, MD (New York, NY) Introduction: Mass lesions within the third ventricle have long been postulated to present a risk for intermittent cerebrospinal fluid obstruction. This phenomenon, however, has seldom been documented with an imaging correlate and quantitative evaluation. Methods: The clinical and radiographic features, quantitative assessments, treatments, and outcomes were reviewed for two patients with lesions in the third ventricle, in which remitting clinical symptoms of raised intracranial pressure were either characteristic of or associated with intermittent ventriculomegaly on imaging. Additionally, the few documented cases of intermittent obstructive hydrocephalus with concomitant intraventricular cysts are examined. Results: Two patients, a 3 month and a 9 year old male, presented with paroxysmal symptoms of raised intracranial pressure and imaging confirmation of varying ventriculomegaly with a third ventricular pineal and choroid plexus cyst, respectively. Both were treated by a primary endoscopic cyst fenestration and remain without symptoms, complications, or placement of an indwelling shunt at 20 and 3 months of follow up, respectively. Conclusions: Our cases add to a growing body of evidence that a normal sized ventricular system cannot rule out the diagnosis of intermittent hydrocephalus in a patient who presents both with symptoms suggestive of increased intracranial pressure and a lesion that can potentially obstruct CSF flow. Additionally, an absence of intraventricular cysts on traditional CT or MR imaging should not automatically rule out the possibility of an intermittently obstructive cyst. Our findings suggest that patients experiencing symptoms of raised intracranial pressure concomitantly with third ventricular cystic masses and normal sized ventricles should be offered cyst decompression. 134. Intradiploic Meningioma Of The Orbit Mimicking Osteoma: A Rare Case Report And Literature Review Maria Blagia; Giuseppe Orunesu, MD; Salvatore Serra, MD; Salvatore Cossu, MD (Nuoro, Italy) Introduction: Intradiploic meningiomas, are a subset of extradural meningiomas that arise in bone. These types of meningiomas are relatively rare cranial lesions and constitute fever than 2% of meningiomas overall, but they represent two thirds of all extradural meningiomas. On radiographic findings, these lesions may present as an osteolytic or osteoblastic skull lesions. Methods: We report a case of a 53 year old female who presented with a gradual onset exopthalmos of the right eye. The plain radiographs of the skull showed hyperostosis af the right orbital roof and the lateral orbital wall. The computerized tomography (CT) scan revealed an extra axial, intradiploic orbital roof tumor involving the frontal and temporal bone. Results: The tumor, including the surrounding normal bone, was totally excised by an extradural route using a basal fronto temporal craniotomy. The histopathological study confirmed a meningotheliomatous meningioma. A split calvarial frontal bone graft was used to reconstruct the orbit. The patient was discharged after 6 days. There is no evidence of recurrence after a follow up of 3 months. Conclusions: Intradiploic meningiomas are often asymptomatic, but can cause proptosis and neurological symptoms depending on their size and location. Radiographic and clinical presentations generate diagnostic suspicion that may assist with preoperative planning. The majority of these tumors cause hyperostosis that may mimic meningioma en plaque, osteoma, osteosarcoma, Paget disease, and fibrous displasia. The treatment of choise is resection, which is potentially curative. Tumors that cannot be compleely resected may be require adjuvant therapy, which may include radiation therapy, chemotherapy, or bisphosphonate therapy. 135. Intraoperative MRI Obtained T2 And FLAIR Signal Volumes Compared To Pre And Post Operatively Measured Comparison Volumes. Randy Lynn Jensen, MD, PhD, FAANS; Karen Salzman, MD (Salt Lake City, UT) Introduction: Intraoperative MRI is a useful tool in the operative management of human gliomas. In non contrast enhancing gliomas, and to a lesser extent enhancing tumors, the T2 and FLAIR signals are important targets to determine target volumes for resection margins. We hypothesized that intraoperatively obtained MRI T2 and FLAIR signal volumes might not reflect corresponding post operative volumes due to tumor edema after resection and brain manipulation. Methods: We examined 12 low grade gliomas (LGG, 9 low grade astrocytomas and 3 oligodendrogliomas) and compared them to 13 high grade tumors (HGG, 4 anaplastic astrocytomas, 3 anaplastic oligodendrogliomas, and 5 glioblastomas). Volumetric assessment of T2 and FLAIR signals were performed using the OSRIX image analysis program and ratios calculated for preoperative, intraoperative, and post operative MRI images for each patient. Results: Not surprisingly, for both LGG and HGG intraoperative and postoperative FLAIR and T2 signal volumes were significantly lower than post operative volumes. Interestingly, for LLG the ratio of intraoperative FLAIR volume was on average 249% higher than postoperative FLAIR volume (range of 11 982%) and intraoperative T2 volume was 56% (range 0 149%). of postoperative T2 signal volume. For HGG, the ratio of intraoperative FLAIR volume was on average 255% higher than postoperative FLAIR volume (range of 19 1432%). Intraoperative T2 volume was 79% (range 27 168%) of postoperative T2signal volume. When all tumor grades are analyzed together similar trends are found. Conclusions: Postoperative FLAIR signal volumes are significantly lower and T2 signal volumes significantly higher than 44 Methods: We analyzed the relation between the sphenozygomatic suture and the marginal tubercle of the frontal process of the zygoma 60 dried skulls. Minipterional craniotomy was performed in 10 cadaveric specimens. The approach was utilized to 18 sphenoid wing meningiomas. intraoperatively obtained corresponding volumes for LGG. HGGs demonstrated a similar trend for FLAIR signal volumes while T2 signal volume was similar for both intraop and post op images. 136. Withdrawn Results: The marginal tubercle was hiding the sphenozygomatic suture when it is ‹8mm, it required drilling to enhance the exposure. Anterior to posterior sub periosteal dissection and retraction of the temporalis muscle, and avoiding cuts along the origin of the muscle allows excellent cosmetic outcome. All 18 meningiomas (3 to 5 cm in size) were successfully resected without morbidity or mortality through a 3.5 to 4 cm bone flap 137. Withdrawn 138. Withdrawn 139. Meningiomas A Population Based Perspective Conclusions: Minipterional approach is an excellent option to approach sphenoid wing meningiomas. The minimally invasive access allows minimal soft tissue trauma, smaller bony opening, less pain, and excellent cosmetic outcome Quinn T. Ostrom; Carol Krutcho, BS; Jill Barnholtz Sloan, PhD (Cleveland, OH) Introduction: The Central Brain Tumor Registry of the United States (CBTRUS) database contains the largest aggregation of population; based data on the incidence of all primary brain and CNS tumors in the United States. We used this data to describe the current epidemiology of meningiomas in the United States between the years of 2005 and 2009. 142. Minimally Invasive Eyelid Approach For Anterior Skull Base Meningiomas Khaled M. A. Aziz, MD, PhD, FAANS; Mohab Darwish, MD; Mohamed Ragaee, MD; Alexander Yu, MD; Erik Happ, MD; Sebastian Froelich, MD (Pittsburgh, PA) Methods: Using incidence data from 49 population based cancer registries (44 NPCR and 5 SEER), we calculated age adjusted incidence rates per 100,000 person years and 95% confidence intervals for meningiomas by gender, race, and Hispanic ethnicity using SPSS and SEER*Stat. We also calculated survival rates for all malignant menginiomas. Introduction: Fronto orbital minicraniotomy is the most commonly used minimally invasive approaches for anterior cranial fossa lesions. Methods: We describe our novel technique with the transpalpebral eyelid incision to obtain access to the anterior cranial fossa. We describe the approach and technique of the transpalpebral eyelid incision in a step by step fashion and discuss the results of retrospectively analyzed eighteen cases. Results: Meningiomas are the most common type of brain tumor in the United States, compromising 35.5% of all brain tumors. There was an overall incidence rate of 7.22. They are more common in women than men (incidence rates of 9.75 and 4.28, respectively). They are more common in blacks than whites (incidence rates of 8.55 and 7.00, respectively) 1.7% of all meningiomas diagnosed in this time period were malignant. For malignant menginiomas, there were 1, 5 and 10 year survival rates of 82.0%, 64.2% and 55.3%, respectively. Results: Incisions in the eyelid region should therefore be as horizontal as possible. A relative safety zone; free of facial nerve branches was identified that exists up to 2.5 cm lateral to the lateral canthus. We apply knowledge of upper eyelid anatomy, which allow us to utilize an avascaular plane of dissection that maintains functionality of the eyelid and avoids disfiguring cosmetic results. We describe the bony cuts necessary to complete our one piece fronto orbital approach. We perform an eyelid craniotomy Eighteen Tumors: 9 Supra/para sellar meningioma, 6 Olfactory groove meningioma, 1 Large frontal cavernoma, 2 Medial sphenoid wing osteoma We describe the closure process necessary for a good cosmetic result, including dural closure, bone flap re approximation, temporalis reattachment and skin closure. Complications in one patient who developed deep wound infection required re operation. Conclusions: Though most menginiomas are not malignant, their frequency and potential resulting morbidity makes them of significant clinical and scientific relevance. Awareness of the populations most at risk for these tumors assists physicians and scientists in focusing on developing new ways to serve these patient populations. 140. Withdrawn 141. Mini Pterional Craniotomy: An Alternative Approach For Sphenoid Wing Meningiomas Conclusions: The transpalpebral approach provides dissection in natural anatomical planes, affords preservation of the frontalis muscle, avoids injury to nerve VII branches, and results in an excellent cosmetic outcome. Khaled M. A. Aziz, MD, PhD, FAANS; Mohab Darwish, MD; Mohamed Ragaee, MD; Alexander Yu, MD; Mohamed Hammad, MD, PhD; Sebastian Froelich, MD (Pittsburgh, PA) Introduction: Mini pterional craniotomy is a modification of the standard pterional (fronto temporal) Craniotomy. It provides the same microsurgical exposure as the standard frontotemporal approach. 45 143. Modern Treatment Of Planum/Olfactory Meningiomas Results: Incidence of cortical injury while making dural incision, adequacy of operative exposure and ease of the actual excision of the tumor, difficulties encountered during dural closure and post operative CSF leaks were minimized while using the modified dural incisions. Corinna C. Zygourakis, MD; Michael Sughrue, MD; Andrew Parsa, MD, PhD; Mitchel Berger, MD; Michael McDermott, MD (San Francisco, CA) Introduction: Given their location and slow growth, olfactory groove and planum sphenoidale meningiomas often grow to large sizes before they present with clinical symptoms and pose significant surgical challenges. The goal of our study is to identify which preoperative symptoms and MRI findings are correlated with specific postoperative outcomes in order to better counsel patients pre operatively. Conclusions: The modified dural incisions are safe, easier to perform and close with lesser complications. 145. Molecular Genomic Alterations In Meningiomas Methods: We retrospectively identified 44 patients with planum/ olfactory meningiomas treated at our institution between 1996 and 2006. We then used univariate and multivariate regression models to analyze the effect of several MRI characteristics (including tumor volume, distance to optic chiasm, anterior cerebral artery encasement, paranasal sinus invasion, and sellar invasion) on preoperative symptoms and postoperative outcomes, including complication rate and tumor recurrence. Results: Only brain tumor volume (‹42 cm3), but not distance to the optic chiasm, is independently associated with an increased likelihood of preoperative visual symptoms. Tumors with nasal sinus invasion are significantly more likely to cause postoperative surgical complications, and tumors with ACA encasement are associated with a higher likelihood of both postoperative complications and tumor recurrence. Conclusions: We conclude that large tumor bulk is the most likely factor to cause a planum/olfactory meningioma to become symptomatic. In terms of predicting surgical complications, nasal sinus invasion and ACA encasement are associated with higher risk profiles when surgery becomes necessary. Thus, it is prudent to take these specific variables into consideration when advising patients about the risks of observation and surgery for olfactory/ planum meningiomas. 144. Modified Dural Incisions Mohammad Arif Malik, MBBS, FCPS; Muhammad Usman Malik, MBBS (Rawalpindi, Pakistan) Introduction: Dural incisions in cranial and spinal surgeries are standardized and being practised without much modifications. While making these dural incisions we encountered certain difficulties whole opening the dura, while performing the procedure and during closure of dural incisions. To overcome these difficulties we modified some of these incisions. The potential benefits and possible complications along with outline of various dural incisions for cranial and spinal tumors will be presented supplemented by personal experience. Methods: Prospective descriptive study documenting the benefits and pitfalls of various dural incisions for sellar/supra sellar lesions, pterional trans sylvian approach, midline cerebral lesions and intra dural extra medullary spinal tumors. Jing Wu; Riane Hoffman, BA; Carolyn Quinsey, MD; D. Hayes, MD, MPH; Matthew Ewend, MD (Chapel Hill, NC) Introduction: Meningioma, when inoperable or recurrent, can have significant neurological consequences and few options for effective treatment. Potentially actionable molecular alterations that might be driving the growth of these neoplasms have been reported. To better understand these molecular alterations and their correlation with clinical outcomes in cancer patients, we developed a clinical sequencing program, UNCSeqTM, capable of reporting a broad spectrum of clinically actionable mutations. Methods: All adult patients with brain tumors including meningioma undergoing surgery are offered enrollment; the collected tumors undergo next generation sequencing of tumor DNAs. Confirmed, actionable molecular targets are identified and are made available for clinical use. Other potential targets and genetic alterations are also evaluated but not reported to the treating physicians. Results: 17 patients have been enrolled and will be discussed. As of the submission date, 7 patients have been sequenced and 5 confirmed. 60% have actionable somatic mutations including c.134delA mutation in NF2 gene, and two AKT1 gene abnormalities: SMO c.1234C<T mutation and c.49G<A mutation. Mutations in the AKT1 and SMO genes were found in grade I meningiomas; the NF2 mutation was found in an atypical meningioma. Conclusions: Newly characterized genetic alterations in meningioma have been found through UNCSeqTM. 60% of the first cohort in this ongoing analysis had genetic targets identified amenable to treatment with available targeted agents. Next generation sequencing can identify targets, providing a personalized approach to meningioma therapy. 146. Neuro Oncologic Disease Patterns In A Prospective Study Of 2502 Consecutive Patients Of Haiti Ernest Barthelemy; Ernest Benjamin, MD; Geneviève Poitevien, MD; Irene Osborn, MD; Marlon Bitar, MD; Jerry Bitar, MD; Isabelle Germano, MD (New York, NY) Introduction: No study has yet explored CNS tumor prevalence in Haiti. Characterization of Haitian neuro oncologic disease patterns will enable productive allocation of neurosurgical resources and training efforts. This study sought to describe disease presentation of patients with CNS masses admitted to a Haitian emergency room (ER). 46 Methods: A prospective study of consecutive ER admissions was conducted at a metropolitan Haitian hospital with a CT scanner from August 1st to October 31st 2012. Ethical approval was obtained at both US and Haitian institutions. De identified data on patients with CNS masses was collected using Microsoft Excel and analyzed using standard statistical analysis for disease presentation and prevalence. Conclusions: Though this is an ongoing study and more sample size is needed for conclusion, our preliminary data indicates that in most of our GBM cases, notch signalling contributes significantly to the process of tumorigenesis, strongly supporting this pathway as a promising therapeutic target for this malignancy. Results: During the study period, there were 2502 ER admissions. Of these, 86 required neurosurgical consultation including five (6%) diagnosed with cerebral masses. Presenting symptoms were seizures (80%), neurological deficits (60%) and fever (40%). A single patient had head CT without and with contrast; two had non contrast CT. In all 3 cases, images were consistent with brain tumor. No images were obtained in 2 patients; one of which had an exploratory craniotomy revealing a subdural empyema. 148. O6 Benzylguanine (BG) And Temozolomide (TMZ) Therapy Of Glioblastoma Multiforme (GBM) With Infusion Of Autologous Lentiviral Transduced P140KMGMT+ Hematopoietic Progenitors To Protect Hematopoiesis: Preliminary Results Of A Phase I Study Andrew E. Sloan, MD, FAANS; Jane Reese, PhD; Lisa Rogers, DO; Hillard Lazarus, MD; Dona Kane, RN; Boro Dropulic, PhD; Stanton Gerson, MD (Cleveland, OH) Introduction: Radiation therapy (RT) and concomitant temozolomide (TMZ) for the treatment of newly diagnosed glioblastoma (GBM) is associated with modestly prolonged survival and this benefit is restricted to patients whose tumor exhibits MGMT Promotor methylation. Conclusions: In our sample, the diagnosis of cerebral mass accounted for 6% of admissions requiring neurosurgical consultation. Seizures were the most common presenting symptom. While Haitian CNS tumor prevalence cannot be determined by this survey, the data indicates the need to further study this disease pattern. Limitations on availability of diagnostic tools and neurosurgical resources are significant barriers to the identification and management of patients in Haiti with CNS tumors. Methods: We used ex vivo gene transfer of autologous hematopoetic progenitor cells (HPCs) transduced with lentiviral P140K MGMT, an MGMT mutant highly resistant to inactivation by the irreversible MGMT inhibitor O6 benzylguanine (BG), to combine to reduce or prevent the myelosuppressive effects of combined TMZ+ BG. The primary objective is to assess the safety and feasibility in newly diagnosed GBM. This Phase I study includes three cohorts of at least three evaluable patients per cohort. Cohort 1 receives standard RT and concomitant TMZ prior to infusion of autologous lentiviral P140K MGMT transduced HPCs, followed by adjuvant TMZ+ BG. Cohort 2 will receive induction TMZ+BG followed by infusion of autologous LV P140K MGMT HSCs prior to concomitant RT +TMZ and adjuvant TMZ+ BG. Cohort 3 will include GB and intra patient dose escalation of TMZ in patients who exhibit detectable levels of P140K MGMT marked cells in vivo, using the design (i.e. cohort 1 or 2) proven to be safest and most effective. 147. Notch Pathway In Glioblastoma Multiforme: Therapeutic Stratification On The Basis Of HES 1 Gene Expression Puneet Gulati, MD; Tapojyoti Das, MD; Sumit Deb, MD; S.N Ghosh, MD; Uttara Chatterjee, MD; Sarang Rote, MD; Surajit Dhara, PhD (Calcutta, India) Introduction: Glioblastoma Multiforme (GBM) is the most common Central Nervous System (CNS) malignancy characterised by high proliferation and local invasiveness. In spite of optimal treatment, median survival is less than 15 months. Aberrant activation of notch signalling is reported in many human malignancies including GBM and targeted therapy in this disease with pharmacological inhibitors of this pathway is under clinical trial. Stratification of GBM patients on the basis of notch pathway activity is crucial for targeted therapy with the appropriate inhibitors. For this reason, we sought to classify a series of GBM cases in eastern India based on their expression patterns of HES 1, a key notch target gene. Results: The first two patients have undergone debulking surgery, RT, HPC mobilization and infusion of transgene therapy followed by three cycles of adjuvant BG + TMZ. Post infusion enrichment has resulted in P140k MGMT gene marking in 0.3 5.5 % of both blood and bone marrow. Toxicity has been minimal and well tolerated. Methods: We estimated the mRNA expression levels of HES 1, the key notch target gene and the bona fide molecular marker for notch pathway activity, and also of GFAP (Glial Fibrillary acidic protein), an astrocytic marker, relative to the levels of β actin (ACTB) expression by quantitative reverse transcriptase polymerase chain reaction (qRT PCR) method in a cohort of 24 CNS tumors. Conclusions: Transgene therapy for GBM patients is feasible and may enable tolerance of higher dose adjuvant TMZ. Results: We found Hes 1 expression in almost all tumors of astrocytic/non astrocytic origin. We sub classified only the GBM cases into three subgroups based on their HES 1 gene expression levels (High, moderate and low Notch pathway activity) 47 149. Phase I Trial Of Superselective Intraarterial Cerebral Infusion Of Temozolomide Kartik Kesavabhotla; Sirish Kishore, MD; Ashley Ray; Athos Patsalides, MD; Howard Riina, MD; John Boockvar, MD (Plainsboro, NJ) Introduction: High grade malignant brain tumors are the most common and most aggressive adult brain tumors with median overall survival durations of only 9 12 months for glioblastoma multiforme (GBM), and 3 4 years for anaplastic astrocytoma (AA). All patients experience a recurrence after first line therapy, so improvements in both first line and salvage therapy are critical to enhancing quality of life and prolonging survival. Temozolomide is an oral alkylating agent often used along with radiation therapy after initial GBM resection. A phase I clinical research trial was designed to test the hypothesis that temozolomide can be safely used by direct intracranial superselective intraarterial cerebral infusion (SIACI) to increase delivery to the brain and ultimately enhance survival of patients with primary GBM. By achieving the aims of this study we will determine the toxicity profile and maximum tolerated dose (MTD) of SIACI temozolomide. Methods: Subjects with primary high grade glioma were treated with mannitol followed by a single SIACI of temozolomide. Dose was started at 75/m2 with intent to undergo dose escalation to 250 mg/m2 to determine maximal tolerated dose. Results: Fourteen patients were treated at dose of 75 mg/m2, 100 mg/m2, or 150 mg/m2. The maximal tolerated dose has not been reached. Two patients reported mild headaches and nausea within the first month post infusion. One seizure was reported at 1 week post infusion. One patient who received a 100 mg/m2 suffered a brainstem toxic encephalopathy from streaming effect during the catheterization. Conclusions: Temozolomide can be safely tolerated through intra arterial delivery at least up to a dose of 150 mg/m2. However, particular caution must be used around small end artery infusion to prevent streaming effect which can lead to high level of toxic doses of temozolomide. 150. Withdrawn 151. Prenatal Diagnosis Of Craniopharyngiomas; A Novel Treatment Paradigm Aimed At Reducing Operative Morbidity Verrad Kwasi Nyame, MD; Chung Ho Chang, MD; Sandeep Sood, MD (Detroit, MI) Introduction: Craniopharyngiomas are histologically benign lesions that result from disordered embryogenesis. They are most commonly encountered in the pediatric population. Due to their proximity to vital neural and vascular structures they pose a significant operative challenge to the neurosurgeon and a malignant clinical course to the patient. The neurosurgical community has questioned the feasibility of total resection with acceptable morbidity. The authors present a novel paradigm and case illustration in the treatment of prenatally diagnosed craniopharyngiomas aimed at reducing operative morbidity. We also review the relevant literature supporting errors in neurulation as the cause of these clinically malignant but histologically benign tumors of childhood. Methods: We report the case of a prenatally diagnosed craniopharyngioma that has been completely resected without any operative morbidity to illustrate a novel paradigm in management. Results: An ultrasound at 30 weeks gestation demonstrated a large suprasellar lesion. The patient was born at 35 weeks of gestation via spontaneous vaginal delivery with poor feeding and decreased activity. He underwent delayed total surgical resection at four months of age without associated morbidity. Conclusions: To our knowledge this is the seventh case of a prenatally diagnosed craniopharyngioma reported in the literature that underwent attempted resection. The literature has questioned the feasibility of total resection with acceptable morbidity. The trend however based on current literature has advocated attempted total resection. We present this case to support the feasibility of total resection with limited to no surgical morbidity and postulate that the standard of care should be gross total resection. 152. Proteostasis Modulators Prolong Missense VHL Protein Activity And Halt Tumor Progression Chunzhang Yang; Russell Lonser, MD; Zhengping Zhuang, MD, PhD (Bethesda, MD) Introduction: von Hippel Lindau disease (VHL) is a heritable multisystem cancer syndrome attributable to a germline mutation of VHL. The most frequent mutations are missense but the mechanism of tumorigenesis is not known. Methods: We investigated the protein stability and intrinsic E3 ligase function of mutant pVHL that carries pathogenic mutations. Results: We found a quantitative reduction of missense mutant VHL protein (pVHL) in VHL associated tumors associated with physiologic mRNA expression. Mutant pVHL is unstable and degraded contemporarily with translation. However, mutant pVHL retains its E3 ligase function, including hypoxia inducible factor degradation. We found that premature pVHL degradation is due to misfolding and imbalance of chaperonin binding. Histone deacetylase inhibitors (HDACis) modulate this pathway by inhibiting the HDAC6 Hsp90 chaperone axis, stabilizing pVHL and restoring activity comparable to wild type protein in vitro and in vivo. HDACi mediated stabilization of missense pVHL significantly attenuates the growth of 786 O xenografts. Conclusions: These findings provide direct insight into the pathobiology of VHL associated tumors, as well as elucidate a new treatment paradigm for VHL. 48 153. Quantitative Resection Map Comparison Of Glioma Surgery Using Brain Stimulation Mapping With 2 And 15 Years Of Experience 155. Recurrence Rates Of Pituitary Adenomas After Purely Endoscopic Resection With Modern Endocrine And Imaging Criteria Philip C. de Witt Hamer, MD; Eef Hendriks, MD; Emmanuel Mandonnet, MD; Aeilko Zwinderman, PhD; Hugues Duffau, MD (Bennebroek, Netherlands) Christopher Ian Sanders Taylor, MD; Amjad Anaizi, MD; Jennifer Kosty, MD; Lee Zimmer, MD; Phillip Theodosopoulos, MD (Cincinnati, OH) Introduction: Intraoperative brain stimulation mapping reduces permanent deficits and extends tumor removal in resective surgery for glioma. Successful application of this technique is considered to depend on the level of experience of the surgical team. In this study the extent of glioma resection (EOR) is quantitated and compared between a surgical team with 15 and 2 years of experience with stimulation mapping. Introduction: The purpose of this study was to define recurrence rates and timing of recurrence following endoscopic pituitary adenoma resection to aid in management of imaging surveillance. Methods: Adult patients with glioma were consecutively included who had resective surgery targeted at the MRI FLAIR hyperintense volume and limited by functional boundaries. The senior surgical team contributed 56, and the junior team 60 consecutive patients. The surgical technique was very similar including the stimulation mapping. Because the localization of tumor within the brain is essential in comparing EOR, a novel approach was applied using resection maps that quantitate and compare the likelihood of resection throughout the brain at 1mm resolution. Considerations for spatial dependence of voxels and multiple comparisons were taken into account. Results: The patient cohorts were comparable in age, preoperative tumor volume, lateralization, and lobe localization. The resection maps detected 0 of 705.164 voxels in left sided tumors and 58 of 638.033 voxels in right sided tumors that were differentially resected. Conclusions: The EOR for patient cohorts can be quantitated using resection maps. These resection maps are similar for surgical teams with 2 and 15 years of experience in stimulation mapping. This indicates that stimulation mapping is a robust and reproducible technique and supports more universal implementation. Methods: A retrospective review was conducted from November 2005 to present for patients undergoing purely endoscopic resection for pituitary adenoma by a single surgeon team. 200 patients were identified with postoperative imaging and operative reports defining gross total versus subtotal resections. Patients were followed with serial imaging occurring yearly with one intermediate scan in the first year. Progression was defined as enlargement on serial imaging or biochemical failure. Data was analyzed using Fisher exact test to determine significance. Results: Overall recurrence/progression rates were 16% with non secreting tumors recurring/progressing at 10.4 % versus secreting tumors at 30.4% (p = 0.001). Recurrence/progression rates for non secreting tumors was 4.0% for gross total resection versus 17.4% for subtotal resection (p = 0.012), whereas recurrence/progression rates for secreting tumors was 29.0% versus 33.3% for gross total and subtotal resection, respectively (p = 0.763). Average time to recurrence/progression was 21.4 months (SEM = 1.3), ranging from 15.8 months to 25.3 months in subgroups with a wide range of standard deviation (10.9 to 24.3 months). Six tumor recurrences occured on or after 5 years. Conclusions: As expected secretory tumors recurred/progressed at a significantly higher rate than non secreting tumors. Although gross total resection proved to offer benefit in non secreting tumors, there was no significant difference in recurrence relating to resection in secreting tumors. Given the chronological variability of recurrence/progression, continued long term radiographic surveillance may be necessary. 154. Withdrawn 156. Withdrawn 49 157. Revisiting The Architecture Of The Cerebral Hemispheric White Matter: A New Parcellation Strategy Reveals That Invasion Of The Deep White Matter Is An Independent Predictor Of Mortality For Glioma Patients Jackson D. Hamilton, Jr.; Vinodh Kumar, MD; Dawid Schellingerhout, MD; Komal Shah, MD; Linda Chi, MD; Jill Hunter, MD; Tom Naidich, MD; Lakshmi Chavali, BS; Norman Leeds, MD; Sujit Prabhu, MD; Ashok Kumar, MD; L Hayman, MD (Houston, TX) Introduction: Underlying tumor stromal interactions may guide diffuse glioma spread beyond gyral and sulcal anatomy. The shape and position of cortex white matter architectural volume units can be used to define if the tumor is growing in a single area or spreading to other areas. Methods: Seventy four patients with diffuse gliomas (Grade II IV) with serial MR imaging and at least 2 years of follow up were retrospectively reviewed by a consensus of 3 9 neuroradiologists, blinded to survival data. Tumors were determined to be growth pattern (GP; confined only to limbic system or within in a neocortical volume defined by Brodmann numbered cortex and underlying superficial/intermediate white matter) or were spread pattern (SP; extension to the crossing, deep white matter fibers). This was compared to other predictors of survival. Results: Gliomas with GP (limited) spread had approximately 50% longer survival than SP (diffuse) spread (47+/ 36 months versus 20 +/ 24; p =0.0002), independent of tumor grade or size. Patients with GP glioblastomas had similar survivals to SP, grade II III tumors. This single determination had similar performance to previously verified multiparameter criterion (VAK) and improved all modelling predictions by at least 5%. Conclusions: Gliomas' shape and location is an independent survival predictor much like the staging of other cancer sites. This strategy is best demonstrated in common locations, such as near the central sulcus and sylvian fissures, where well defined white matter "stalks" course perpendicular to deep fibers. This parcellation strategy could group outcomes for research, improve communication and facilitate treatment planning. 158. Risk Factors For Postoperative CSF Leak And Meningitis After Endoscopic Endonasal Surgery Michael Edward Ivan, MD; Andrew Parsa, MD, PhD; Michael McDermott, MD; Ivan El Sayed, MD; Steven Pletcher, MD; Manish Aghi, MD, PhD (San Francisco, CA) Introduction: Postoperative CSF leak is a serious complication of transphenoidal surgery, which can lead to meningitis and often require reparative surgery. We sought to identify preoperative risk factors for CSF leaks and meningitis. Methods: The results of 98 consecutive endoscopic endonasal surgeries performed from 2008 20012 were retrospectively analyzed for preoperative comorbidities, intraoperative techniques, and postoperative care. Univariate and multivariate analysises were performed. Results: Pathologies addressed included pituitary adenoma, meningioma, esthesioneuroblastoma, adenocarcinoma, chondrosarcoma, chordoma, lymphoma, squamous cell carcinoma and angiofibroma. There were 11 CSF leaks (11%) and11 CNS infections (11%). Planum, tuberculum, sellar, and clival locations were not found as a risk factor for CSF leak (p=0.84) however planum lesions were found to have a higher risk for infections (p=0.05). Multivariate analysis showed patients with non ideal BMI were associated with higher rate of postoperative CSF leak and meningtis (p<0.01 and p<0.01 respectively). Also, patients with increasing age were associated with increased CSF leak (p<0.03) in a univariate analysis. Endoscopic transphenoidal surgeries combined with open cranial cases had a higher postoperative CSF leak and CNS infection rate thantransphenoidal surgeries alone or surgeries staged with open cases (p<0.01). 4 deaths were noted in this study which were found to be associated with CNS infection (p‹0.01). Conclusions: In this series of endoscopic transphenoidal surgeries preoperative BMI and age are two predictive values for CSF leak and infection. Risks associated with complex surgical resections when combining open and endoscopic approaches could be minimized by staging these procedures. 159. Withdrawn 160. Role Of Microenvironment In Glioma Anwar Hossain; Joy Gumin, BS; Feng Gao, MD; Tatsuya Takezaki, MD, PhD; Javier Figueroa, MS; Frederick Lang, MD (Houston, TX) Introduction: Mesenchymal stem cells (MSC) have been implicated as components of the microenvironment of several cancers, but their contribution to human brain tumors, particularly gliomas, remains obscure. Methods: We isolated MSC like cells, called Glioma Associated human Mesenchymal Stem Cells (GA hMSC), from 20 of 31 human glioma surgical specimens using established culture, surface markers and mesenchymal differentiation criteria. We used standard in vitro and in vivo techniques to delineate the role of GA hMSCs in glioma. 50 Results: We have found that in contrast to Glioma Stem Cells (GSCs), which are the tumor initiating cells in gliomas, GA hMSCs were non tumorigenic and did not harbor common genetic anomalies seen in GSCs. Importantly, in in vitro co culture experiments, GA hMSCs significantly increased the proliferation and self renewal of GSCs compared with controls. When grown in vivo in the flanks of nude mice, GSCs mixed with GA hMSCs formed larger tumors than GSC controls. After implantation into the brain of nude mice, GSCs formed intracranial tumors more frequently after co culture with GA hMSCs than after co culture with controls. Likewise, the survival of mice implanted intracranially with GSCs that were co culture with GA hMSCs, was significantly shorter compared with mice implanted with GSCs co cultured with controls. Increased proliferation and self renewal of GSCs were dependent on GA hMSC secreted Interleukin 6, which activated STAT3 in recipient GSCs. GA hMSC co cultured GSCs also increased expression of mesenchymal genes in vitro. patients and were worsened in 5.9%. Conclusions: Our results have shown that surgery for cerebral metastases in the central area can be done safely and improve or stabilize the neurological function of most patients. Surgery also promptly addresses symptoms related to cerebral edema, mass effect, and midline shift. Microsurgical resection of central area metastases should be a treatment option for patients with single or multiple lesions who present a focal neurological deficit. 163. Study Of 5 ALA PD In Our 100 Cases Of Brain Tumor Tadashi Higuchi; Fumio Yamaguchi, MD, PhD; Hirotomo Ten, MD; Tomoko Oomura, MD, PhD; Koji Adachi; Akira Teramoto (Kita ku, Japan) Introduction: It has been established that 5 aminolevulinic acid (5 ALA) induces the accumulation of fluorescent protoporphyrin, a phenomenon potentially exploitable to guide tumor resection. In this study, we examined the useful of photodiagnosis (PD) by 5 ALA for the 100 cases during brain tumor surgery. Conclusions: Together these results represent the first evidence that hMSCs are a stromal component of human gliomas and that they enhance the proliferation and self renewal of GSCs by cross talk via IL 6 activation of STAT3. Methods: In our institute, 100 patients was performed tumor resection using 5 ALA from 2005 to 2012. The patients received oral doses of 5 ALA 2 hours before induction of anesthesia. Retrospectively, we compared for positive/negative of photodynamic diagnosis for each tumor. 161. Withdrawn Results: 79 cases showed positive responses, and 21 cases showed negative responses. Malignant brain tumors (i.e. anaplastic astrocytoma, glioblastoma multiforme etc.) and meningiomas tended to show strong positive fluorescence. On the other hand, pilocytic astrocytomas, diffuse astrocytomas, and recurrent high grade gliomas, etc. showed negative or weak responses. 162. Selective Excision Of Cerebral Metastases From The Central Area Robert Givens Kellogg, MD; Lorenzo Munoz, MD (Chicago, IL) Introduction: The surgical management of central area cerebral metastases remains under discussion. Central area lesions are often treated with whole brain radiation therapy (WBRT) or stereotactic radiosurgery (SRS) because of the concern for causing post operative neurological deficits. Surgery has an important role in acutely alleviating symptoms from cerebral edema and mass effect that radiation cannot address. Additionally, there is evidence in the literature that radiation therapy carries significant risk of complications. We present a series of patients who were symptomatic from a central area metastasis and underwent surgical excision. Conclusions: 5 ALA PD contributes to increasing the tumor resection volume. However, the sensitivity of PD varies among tumors, therefore it is important to use this technique in combination with the other intraoperative support tools. Methods: During a 2 year period from 2010 to 2012, 17 consecutive patients harboring a cerebral metastasis within the central area underwent microsurgical resection. Cases were selected by reviewing all cases of cerebral metastasis by the senior author and identifying those patients with a central area lesion that was surgically removed. The prerequisite for neurosurgical treatment was stable systemic disease and life expectancy greater than 6 months as determined by the patient oncologist. Patients also were required to harbor a symptomatic lesion within the central area, defined as the pre or post central gyri. Results: We present the 3 month neurological outcome for this group of patients. Surgery was uneventful and without any severe peri operative complications in all 17 patients. Gadolinium enhanced T1 weighted MRI scans obtained on post operative day #1 revealed a gross total resection in all patients. At 3 month follow up, symptoms had improved or been stabilized in 94.1% of 51 164. Surface Down Modulation Of MICA On Malignant Glioma Cells By Herpes Simplex Virus 167. Survival Advantage In Patients With De Novo Versus De Differentiated Anaplastic Meningioma Carl Irwin Odom; James Markert, MD, MPH; Kevin Cassady, MD (Birmingham, AL) Jennifer Moliterno Gunel, MD; William Cope, BS; Emma Vartanian, BS; Anne Reiner, MS; Roselyn Kellen, BS; Shahiba Olgilvie, MS; Jason Huse, MD, PhD; Murat Gunel, MD; Philip Gutin, MD (Branford, CT) Introduction: Oncolytic Herpes Simplex Virus (oHSV) vectors are experimental adjuctive therapies for malignant gliomas. Deletions of the diploid γ134.5 gene render oHSV aneurovirulent and targets viral replication to malignant cells. Portions of tumor clearance may occur by lysis. However, natural killer (NK) cells may target infected glioma cells and restrict lytic replication. NK cell cytotoxicity is regulated by activating and inhibitory ligands on cell surfaces. An extensively studied ligand/receptor pair is MHC class 1 polypeptide related chain A (MICA) and Natural Killer Group 2 member D (NKG2D). Members of the herpes family, including HSV 1, modify MICA presentation. We hypothesized that HSV 1 is capable of MICA down modulation in glioma cells by a post translational mechanism. Introduction: While most meningiomas are benign, 1–3% display anaplastic features with little being understood regarding the molecular mechanisms underlying their formation. In a large, single center cohort, we tested the hypothesis that 2 distinct subtypes of anaplastic meningiomas, those that arise de novo and those that progress from lower grade tumors, exist and exhibit different clinical behavior. Methods: Pathology reports and clinical data of 37 patients treated between 1999 to 2012 for anaplastic meningioma at MSKCC, were retrospectively reviewed. Patients were divided into those whose tumors arose de novo and those whose tumors progressed from previously documented benign or atypical meningiomas. Methods: Flow cytometery was used to quantify surface and total MICA and transferrin receptor during infection. Immunofluorescence was used to visualize MICA and validate anti MICA antibodies. RT qPCR was used to quantify MICA mRNA. Results: Overall, the median age at diagnosis was 59 years and 57% of patients were female. Most patients underwent two craniotomies (38%, range: 1–5 surgeries), aimed at gross total resection (59%), which afforded longer median survival when compared with sub total resection (3.3 vs. 2.6 years, respectively P=0.047). Results: Flow cytometery demonstrated that HSV 1 down modulates surface MICA; permeabilization showed no increase in total MICA. Immunofluorescence did not show intracellular sequestration. MICA mRNA decreased during infection, and were lower with VHS containing virus. VHS decreases MICA mRNA but is not required for surface protein down modulation. Transferrin receptor increased for each condition, demonstrating that MICA down modulation is protein specific. 23 patients (62%) presented with apparently de novo anaplastic meningiomas. Compared with progressed tumors, de novo patients were more likely to be female (70% vs. 36%, P=0.04), experienced longer median survival (3.0 vs. 2.4 years, P=0.04), and harbored cerebral hemispheric, as opposed to skull base tumors (91% vs. 43%, P=0.02) Conclusions: Further work is needed to determine the role NK cells play in tumor lysis following oHSV therapy, as well as the mechanism by which oHSV down modulates activating ligands. If the recruitment of innate immune cells for tumor clearance enhances oHSV efficacy, vectors may be modified to circumvent immune ligand modulation. Conclusions: Like malignant glial tumors, anaplastic meningiomas can arise de novo or dedifferentiate from lower grade tumors, and these groups appear to have distinct clinical behavior. Similarly, de novo tumors may well be molecularly distinct and this is being investigated. Aggressive GTR affords a survival advantage in both groups. 165. Withdrawn 168. Susceptibility Changes In Meningiomas Increase The Mean Apparent Diffusion Coefficient In Diffusion Weighted MRI 166. Withdrawn Lucia Schwyzer, MD; Jatta Berberat, PhD; Larissa Boxheimer, MD; Luca Remonda, MD; Ulrich Roelcke, MD (Zurich, Switzerland) Introduction: Diffusion weighted magnetic resonance imaging (DWI) provides information of water diffusivity which is expressed by the apparent diffusion coefficient (ADC). In gliomas it has been shown that ADC values correlate with tumor cell density and allow early treatment response assessment. At the present time it is not known which biological aspects of meningiomas are reflected by their behavior in ADC images. Further it is not known whether intra tumoral susceptibility changes alter ADC values. In susceptibility weighted MRI (SWI) the hypointense changes (SWIpos) in meningiomas can be associated with intra tumoral calcification. Here we analyzed whether intra tumoral SWIpos influences ADC values in untreated meningiomas. 52 Methods: We retrospectively analyzed pre operative SWI and DWI of patients (n=35, ±17yrs; mean+SD) with newly diagnosed meningiomas. We grouped our patients into meningiomas with substantial intra tumoral SWIpos (n=11) and SWI negative meningiomas (n=24). SWIpos was defined as dot like or fine linear hypointense signal changes not to be attributed to flow signal from vessels. ADC values were calculated based on region of interest (ROI) analysis. ADC values of SWIpos and negative meningiomaswere compared. Conclusions: Targeted radiofrequency ablation represents a safe and effective new technique in the treatment of malignant spinal metastasis. This technique allows for treatment of lesions not controlled by conventional therapy or in patients who may not tolerate systemic therapy. 170. Targeting Glioma Stem Cells In GBM: A Randomized Phase 0/II Study Of Hedgehog Pathway Inhibitor GDC 0449 Andrew E. Sloan, MD, FAANS; Charles Nock, MD (Cleveland, OH) Results: The mean age of patients with SWIpos meningiomas was higher (63+12yrs) when compared to patients with SWI negative meningiomas (56+15yrs). The mean ADC values in SWIpos meningiomas were higher (1.14+0.28x10 3mm2/s) compared to SWI negative meningiomas (0.82±0.08 x10 3 mm2/s; ppos could be attributed to possible calcification based on the phase shift ROI analysis. Introduction: New therapeutic approaches are urgently needed for recurrent GBM (rGBM). Recent studies suggest that GBM recurrence is regulated by glioma stem cells (GSC). Our hypothesis was that interrupting the sonic hedgehog signaling pathway (SHh), an integral mediator of stem cell proliferation, would slow tumor progression and improve progression free survival (PFS) in correlation with decreased GSC proliferation; self renewal. Conclusions: SWIpos in meningiomas influences DWI results by increasing ADC values on average by 38%. The frequency of SWIpos in elderly patients is in line with the known age associated calcification in meningiomas. The shift of ADC values due to susceptibility changes needs to be considered when drawing conclusions on tumor behavior from DWI. Methods: Two armed, randomized phase 0/II study of GDC 0449, an inhibitor of SHh, in 40 patients undergoing resection for rGBM. Arm I was randomized to receive GDC 0449 pre operatively; all patients were treated post operatively. Our primary objective was to estimate PFS6, with secondary endpoints of mOS, response and toxicity. Correlative studies included determination of PK, PD, inhibition of SHh signaling and inhibition of GSC proliferation and self renewal. 169. Targeted Radiofrequency Ablation Of Spinal Metastases: Initial Multicenter Experience Joseph Graham, DO; Jack Jennings, MD, PhD; Bassem Georgy, MD; Frank D. Vrionis, MD, PhD; Shelby McCraw, BSN; Nam D. Tran, MD, PhD (Tampa, Florida) Results: Median PFS and OS was 1.8m and 8.3m respectively; toxicity was minimal. PK/PD data and tumor specimens obtained from 39/40 patients demonstrated plasma and tissue levels within therapeutic range. SHh signaling intermediates (Gli 1, Gli 2, PTCH 1b) determined by RT PCR were significantly lower in Arm I (treated pre operatively) vs. Arm II (untreated pre op) (p<0.0002) as were the proportion of tumor derived CD133+ neurospheres undergoing proliferation (p ‹0.0053) and self renewal (p<0.003) in Arms I vs. II. Introduction: Approximately 85% of patients with metastatic disease will develop bony metastasis. Nearly three fourth of these will involve the axial skeleton, thus increasing the risk of bone pain, pathologic fractures, and compression of neural elements. Therapeutic goals are pain control, spinal stabilization, reducing risk of spinal cord compression, and tumor control. Targeted radiofrequency ablation (t RFA) of malignant spinal lesions represents a novel minimally invasive approach to achieving these goals in the oncology population. Conclusions: GDC 0449 was well tolerated but poorly efficacious as a single agent in rGBM. However, phase O/II studies suggest the therapeutic PK, PD and biological activity of this agent on proliferation and self renewal of GBM derived CD133+ neurospheres. Novel combinations pairing GDC 0449 with other agents should be pursued despite lack of single agent efficacy. Methods: Retrospective chart review was performed on patients treated with t RFA at three centers, between 2011 and 2013 (n=85). Demographic data, type of tumor, tumor location, number of levels treated, history of previous or concurrent therapy, pain score (VAS), functional score (ODI, Karnofsky), opiod requirement, total ablation time, use of cement augmentation, complications, and tumor progression at treated level were collected. Results: Spinal metastases involved a wide spectrum of tumor etiology extending from T2 S2. Cement augmentation was utilized in nearly all t RFA treated malignant spinal lesions. No complications of thermal injury occurred. Cement augmentation following t RFA resulted in predictable cement filling. All patients reported improvements in pain, with significant improvements in VAS. Functional performance increase was demonstrated in all participants. 53 171. Temozolomide Conjugated To Perillyl Alcohol Demonstrates Potent Anti tumor Effects In Vitro On Meningioma Cell Lines to treat tumor volumes of 1 to 16 cc. Risk of PTE development was 8x higher in falx/parasagittal locations compared to other sites (31% vs 4%). 75 % of patients with post GKRS PTE had evidence of PTE pretreatment. All patients in parasagittal/falx locations had pretreatment PTE. Time to first radiological signs of PTE was 3 6 month. PTE peaked around 6 8 months and began to resolve around 12 15 months. Clinical symptoms onset temporally correlated with peak edema. Two patients whose symptoms were resistant to aspirin and/or steroids were treated successfully with bevacizumab with eventual resolution of symptoms. Prior radiation therapy, tumor volume and treatment dose conformality and gradient indexes did not significantly correlate with PTE. Gabriel Zada, MD; Rocky Pramanik; Thomas Chen; Florence Hofman (Los Angeles, CA) Introduction: Limited chemotherapeutic options exist for invasive, atypical, and anaplastic meningiomas. Perillyl alcohol (POH), a naturally occurring limonene compound, has known anti tumor properties. We tested the anti tumor potential of a newly conjugated compound, temozolomide perillyl alcohol (TMZ POH) using an in vitro meningioma cell model. Methods: Human meningioma cells (IOMM Lee, CH157, and primary tumor cells) were cultured in increasing concentrations of temozolomide (TMZ) alone, equimolar TMZ and POH, or conjugated TMZ POH for 48 hours. Cell survival was determined via MTT assay as well as long term (<14 days) colony formation assay (CFA). Flow cytomtery (FACS) was performed for DNA cell cycle analysis. Conclusions: PTE remains a significant complication following GKRS for falcine and parasagittal meningiomas. Symptomatology can appear as early as 3 months after GKRS and can be medically controlled in the majority of the cases. Symptomatology from PTE can last beyond 15 months and bevacizumab may be helpful in resistant cases. Results: More potent attenuation of cell survival occurred with TMZ POH in all meningioma cell lines tested, compared to TMZ alone or TMZ in combination with POH. The IC50 of IOMM Lee cells assessed via MTT was 15.5 uM in the TMZ POH group versus 33 uM in the TMZ group (p50 of IOMM Lee cells was 8.4 uM for TMZ POH vs. 20.1 uM for TMZ (p50 of CH157 cells was 44 uM in the TMZ POH group and 132.5 uM in the TMZ group (MTT). The IC50 of CH157 cells assessed via CFA was 20 uM in the TMZ POH group vs. 50 uM with TMZ. In primary surgically resected meningioma cells, the IC50 for TMZ POH was 140 uM, but cells treated with TMZ alone did not reach IC50 at the highest concentration (250 uM) (MTT). TMZ POH and TMZ both induced apoptosis and cell cycle arrest in the G2/M phase, but TMZ POH was at least. 173. The Influence Of Mesenchymal Stem Cell Exosomes In The Tumor Microenvironment On Glioma Stem Cell Growth Javier Figueroa; Tal Shahar, MD; Frederick Lang, MD (Houston, TX) Introduction: Cells within the tumor niche use an intricate network of communication not only to establish the tumor microenvironment, but also promote the growth and evolution of the malignancy. In this range of communication systems, the contribution of exosome transfer between tumor forming glioma stem cells (GSCs) and glioma associated mesenchymal stem cells (GA MSCs) is not well established. Methods: Therefore, we hypothesize that exosomes released by GA MSCs represent a novel intra tumoral communication mechanism that promotes aggressive behavior in GBM. Using ultracentrifugation methods we harvested exosomes from four GA MSC lines, extracted from patient tumors, and characterized the content of these nano vesicles to include membrane bound proteins and various RNA. Exosome transfer and uptake was subsequently demonstrated when GA MSC exosomes labeled with fluorescent membrane dye, were spontaneously absorbed and sorted by four GSC lines (isolated from patient tumors), two of which had matching GA MSC lines. twice as potent. Conclusions: Compared to temozolomide alone, TMZ POH consistently demonstrated more potent anti tumor effects in the in vitro meningioma cell model, although the mechanism of action with regard to DNA damage was similar. TMZ POH may be an effective therapeutic option for meningiomas, especially given its potential for inhaled/intranasal delivery. 172. Temporal Evolution Of Peritumoral Edema After Gamma Knife Radiosurgery Of Meningiomas Results: In vitro experiments then revealed that the tumor enhancing effects of GA MSCs on co cultured GSCs, could not be solely attributed to excreted growth factors and other proteins, but must also include exosome exchange. We found that the delivery of a single concentrated dose of GA MSC exosomes increased the proliferation of GSCs between 30% and 145%, when compared to untreated controls. Furthermore, GSC clonogenicity increased between 25% and 50% with the addition of GA MSC exosomes. Sacit Bulent Omay, MD; Ben Taylor, MD, PhD; Frank Barbiero; James Yu, MD; Veronica Chiang, MD (New Haven, CT) Introduction: Analysis of the temporal evolution of peritumoral edema (PTE) in meningiomas after GKRS (Gamma Knife Radio Surgery). Methods: Retrospective analysis of 83 patients who underwent GKRS for treatment of intracranial meningiomas. Patients who showed radiological signs of new and/or increased PTE were analyzed for demographics, tumor locations, radiosurgery dosing conformality and clinical outcomes. Conclusions: Although exosome delivery and GSC altering mechanisms have yet to be established, GA MSC exosomal miRNA are likely candidates due to their ability to alter recipient GSC gene expression, thus adding another significant pathway by which the microenvironment can impact tumor progression. Results: Of the 83 patients analyzed eight had MRI findings of new and/or increased PTE (10%). 15 18Gy marginal doses were used 54 174. The Maxillary Strut: An Anatomic Evaluation And Its Clinical Application cells. The proportion wasassessed on the basis of the percentage of immunopositivecells as follows: 0, 0 %; +1, less than 10 %; +2, 10 to 50 %; and +3, greater than 50 %. Sanjeet Singh Grewal; Almaz Kurbanov, MD; Amjad Anaizi, MD; Jeffrey Keller, PhD; Philip Theodosopoulos, MD; Lee Zimmer, The staining intensity was evaluated as weak (+1), moderate (+2) and strong (+3). The MIB 1 labeling index was calculated in a representative maximal activity and evaluated by counting the percentage of positive nuclei in a high powered field. MD (Cincinnati, OH) Introduction: The maxillary strut is bone that divides the foramen rotundum and the superior orbital fissure. Tumors involving the lateral wall of the sphenoid sinus, posterior ethmoid, or posterior maxillary sinus may invade this region. We detail the anatomy of the strut, and present a case series to emphasize the import and utility of an endonasal endoscopic approach to lesions in this region. Results: The expression level of COX 2 in meningioma cells was significantly correlated with WHO grade (P = 0.0153). In addition, COX 2 expression was significantly correlated with MIB 1 labeling index for all 76 cases of meningioma (P = 0.0075), suggesting tumor promotion by COX 2 in meningioma progression. Methods: Endonasal endoscopic dissections were performed on four formalin fixed cadaver heads. We also conducted morphometric studies of one hundred skulls using CT scans and Brain Lab software. Conclusions: Our results may indicate the therapeutic value of non steroidal anti inflammatory drugs against meningioma, especially for patients with elevated proliferation, to regulate the tumorigenic activity of COX 2 in meningioma cells. We performed a retrospective review of two patients charts who underwent procedures requiring exposure of the maxillary strut. 176. The Role Of 11C Methionine Positron Emission Tomography In Prediction Of Meningioma Recurrence And Progression Results: The strut is trapezoidal shaped with an average cross sectional area of the strut 17.09mm2 + 0.76 and an average thickness of 4.39mm + 0.15. The maxillary strut was present bilaterally in all studied skulls. The average AP length of the strut was 4.23mm + 0.15 on the right and 4.02 mm + 0.14 on the left. Patient A is 53 year old male who underwent resection of recurrent T3 squamous cell carcinoma involving the infratemporal fossa and extending up to the foramen rotundum. The maxillary strut was removed and superior extent of the tumor visualized and resected. A gross total resection was achieved without complications. Patient B is a 31 year old female with an expansile lesion involving the left pterygopalatine fossa and petrous apex. V2 was visualized and followed back to the foramen rotundum. The maxillary strut was drilled, revealing abnormal bone consistent with a benign bone cyst. Yuzo Terakawa; Hidetoshi Ikeda, MD; Naohiro Tsuyuguchi, MD; Noritsugu Kunihiro, MD; Kenichi Ishibashi, MD; Takeo Goto, MD; Kenji Ohata, MD (Osaka, Japan) Introduction: Meningioma is mostly a benign tumor, but the recurrence rate of tumor after treatment and the progression rate during observation are not negligible. Currently, a definitive method to predict recurrence or progression of this disease has not yet been established. In this study, we used 11C methionine (MET) positron emission tomography (PET) in patients with meningioma to determine whether MET PET can be used to predict tumor recurrence or progression. Methods: A total of 37 patients newly diagnosed as intracranial meningioma were examined using MET PET before treatment. The lesion to normal tissue (L/N) ratios were generated by dividing the mean MET uptake of the lesion by that of the contralateral frontal lobe gray matter. Patient characteristics, location and histopathology of tumor, extent of resection, Ki 67labeling indices, and L/N ratios were analyzed especially with respect to tumor recurrence and progression. Conclusions: An endoscopic endonasal approach can be used to expose the maxillary strut. The improved understanding of this anatomy can extend the utility of the approach to the biopsy or resection of lesions in the lateral sellar compartment, the pterygopalatine fossa, and aspects of the middle cranial fossa. 175. The Clinicopathological Evaluation Of Cyclooxygenase 2 Cxpression In Meningioma Results: Among 37 patients enrolled in this study, 33 patients were surgically treated and four patients were followed without surgery. Recurrence occurred in six of 33 surgically treated patients and progression was seen in two of four observed patients during a mean follow up period of 80 months. Multivariate analysis found high L/N ratios, small extent of resection, and high WHO grade to be significant risk factors for recurrence and progression. Receiver operating characteristic curve analysis indicated that an L/N ratio of greater than 3.18 provided the best sensitivity and specificity for recurrence and progression, 63% and 79%, respectively. Yasutaka Kato; Hiroshi Nishihara, MD, PhD; Hiroyuki Kobayashi, MD, PhD; Shunsuke Terasaka, MD, PhD; Kiyohiro Houkin, MD, PhD; Shinya Tanaka (Hokkaido, Sapporo, Japan) Introduction: Tumorigenic activity of cyclooxygenase 2 (COX 2), a rate limiting enzyme in the production of prostaglandins (PGs), has been proved for some types of cancer, including brain tumors. We evaluated expression of COX 2 in meningioma, one of the most common intracranial tumors in adults. Methods: We performed immunostaining for COX 2 and MIB 1 in 76 cases of meningioma consisting of 44 cases of low grade (WHO Grade I) and 32 cases of high grade (29 cases of Grade II and 3 cases of Grade III) meningioma. Immunostaining ofCOX 2was evaluated in terms of the proportion andstaining intensity of tumor Conclusions: MET PET may provide quantitative values in prediction of meningioma recurrence or progression, although they are not absolute indicators. 55 177. Withdrawn II, 16 grade III, and 4 grade IV) taken to surgery from 2010 2012. Volumetric analysis of 3D T2 weighted imaging was completed for 43 non enhancing and 13 minimally enhancing lesions using IPlan software (BrainLAB). Pre operative, intra operative, and post operative tumor volumes were used to calculate EOR. 178. Use Of Gliadel Wafers For Treatment Of Recurrent Malignant Meningiomas: Case Series Elena Fomchenko; Linda Liau, MD, PhD; Marvin Bergsneider, MD (Los Angeles, CA) Results: Median pre operative tumor volume was 22.38cc. Complete resection was considered feasible in 27 patients based on pre operative imaging alone. 24 of the other 29 patients underwent intra operative electrocorticography, and 5 had tumors involving deep functional structures. 26 of 56 patients did not undergo further resection following IoMRI: 14 showed complete resection at IoMRI and 12 evidenced critical structure involvement. Median intra operative EOR for all patients was 88% (intra operative median residual tumor volume (mRTV): 2.61cc), and 46% of patients had EOR greater than 90%. In 30 patients undergoing further resection, median intra operative EOR was 84% (intra operative mRTV: 3.93cc). Following further resection, post operative EOR in these patients was 98.2% (post operative mRTV: 0.41cc), and 90% had EOR greater than 90%. Introduction: The prognosis for recurrent grade II/III meningiomas failing radiotherapy is poor, associated with 60% progression at 8 months and 17% PFS at one year. Few alternatives exist, as prior trials with chemotherapy, hormonal agents, and small molecule inhibitors have largely been ineffective. Here, we investigate the use of Gliadel BCNU wafers implanted during image complete resection of grade II/III meningiomas. Methods: Three patients ages 27 65 at first resection, diagnosed with grade II/III meningiomas with15 30% Ki 67+ cells and 4 18 mitoses/10X field, having failed 1 4 cycles of stereotactic radiosurgery and chemotherapy, KPS‹80%, were treated with Gliadel wafer implantation during resection at 1st, 4th, and 8th meningioma recurrences. One patient was concurrently treated with Temodar+Avastin. Patients were followed with serial imaging and neurologic examinations, and assessed for toxicity, complications, PFS and OS. Conclusions: Use of high field IoMRI improves the extent of resection in non enhancing gliomas that do not involve functional structures. Results: PFS after the last recurrence prior to Gliadel implantation for all three patients ranged from 2 to 8 months. After Gliadel implantation for recurrent atypical meningioma, PFS was 21, 23 and 48 months in our three patients (30.6 months average), indicating significant improvement in local tumor control compared to prior stereotactic radiosurgery and chemotherapy. Patient who had surgery + Gliadel at 8th recurrence remains progression free for <23 months, the longest period of tumor control during last 5 recurrences. There were no additional toxicities/complications attributable directly to the use of Gliadel in these patients that were unrelated to their underlying co morbidities. 180. Valproic Acid Has Anti Tumor Action In A Primary In Vitro Model Of Glioblastoma Multiforme Abdel Nasser Hosein; Yi Chieh Lim, PhD; Bryan Day, PhD; Brett Stringer, MD, PhD; Stephen Rose, PhD; Richard Head, PhD; Andrew Boyd, MD; Leah Cosgrove, PhD; Michael Fay, MD; Jennifer Martin, MD, PhD (Mississauga, Canada) Introduction: Glioblastoma multiforme (GBM) has nearly a 100% mortality rate and a median survival of less than two years. While there has not been any novel anti GBM therapeutics for many years, there has been the gradual accumulation of clinical data suggesting that the anti convulsant agent, valproic acid (VPA), may significantly prolong survival in GBM patients. Aim: To determine if VPA treatment decreases the viability of GBM cell lines in a primary in vitro model, both as monotherapy and in combination with chemotherapy and irradiation. Conclusions: Gliadel wafers may be safe and effective in controlling local recurrence in selected patients with grade II/III recurrent meningiomas that have failed radiation therapy. Further randomized, controlled studies of Gliadel wafers for refractory meningiomas may be warranted. Methods: Our group has established numerous GBM primary cell lines from patients at the Royal Brisbane and Women Hospital. Primary GBM cell lines were plated and exposed to increasing concentrations of VPA (1 15mM) in order to establish a monotherapy dose response curve. VPA was then used as a pre treatment modality in combination with temozolamide (TMZ) or gamma irradiation. Cells were incubated for 72 hours and cell numbers were quantified with the MTS colormetric assay. 179. Use Of High Field Intra Operative MRI Improves Extent Of Resection In Non Enhancing Gliomas T. Barrett Sullivan; Alireza Mohammadi, MD; Jason Schroeder, MD; Gene Barnett, MD; Violette Recinos, MD; Lilyana Angelov, MD; Michael Vogelbaum, MD, PhD (Cleveland, OH) Introduction: Intra operative MRI (IoMRI) is used to improve the extent of resection (EOR) of brain tumors. Prior studies of IoMRI have focused on enhancing tumors, where the goal is resection of all contrast enhancing tumor. Defining the surgical target is different for non enhancing tumors and requires use of non T1 weighted MRI sequences. Results: VPA as a monotherapy was effective, with nearly all tested lines demonstrating at least 50% kill at a concentration of 15mM. Conversely, response to combination therapy varied across the panel of primary GBM samples, although most did show a synergistic effect with VPA in combination with either irradiation or TMZ. Interestingly, a markedly additive effect was observed when the three treatment modalities were combined. Methods: An IRB approved retrospective review was performed on 56 patients with predominantly non enhancing gliomas (36 grade 56 Conclusions: VPA significantly decreased the viability of primary GBM cell lines in vitro. These findings provide a significant rationale for the investigation of VPA in GBM patients in the clinical setting. 182. Withdrawn 183. miR 142 3p Modulates The M2 Macrophage Phenotype And Exerts Therapeutic Efficacy Against Murine Glioma Amy B. Heimberger, MD, FAANS; Shuo Xu, PhD; Jun Wei, PhD; Ling Yuan King, PhD; Tiffany Doucette, PhD; Ganesh Rao, MD; Greg Fuller, MD; George Calin, PhD (Houston, TX) 181. Velocity Of Tumor Spontaneous Expansion Predicts Long Term Outcomes For Diffuse Low Grade Gliomas. A Multicentre Analysis From 407 Cases Introduction: The immune therapeutic potential of microRNAs (miRNAs) in the context of tumor mediated immune suppression has not been previously described for glioma associated macrophages (derived from the peripheral blood monocyte), which are the largest infiltrating immune cell population in glioblastomas, are predominately M2 and facilitate gliomagenesis. Johan Pallud, MD; Marie Blonski; Emmanuel Mandonnet; Etienne Audureau; Denys Fontaine; Nader Sanai; Luc Bauchet; Philippe Peruzzi; Jacques Guyotat; Luc Taillandier; Laurent Capelle; Hugues Duffau (Paris, France) Introduction: Supratentorial diffuse low grade gliomas present a slow macroscopic tumor growth that can be quantified through the measurement of their velocity of diametric expansion. We assessed whether spontaneous velocity of diametric expansion can predict long term outcomes. Methods: On the basis of miRNA gene expression microarrays of glioblastoma infiltrating macrophages and matched peripheral monocytes, miR 142 3p was identified as the most significantly down regulated miRNA candidate in the glioblastoma macrophage population. Methods: 407 adult patients with newly diagnosed supratentorial diffuse low grade gliomas in adults were studied. Results: Ex vivo human macrophage induction assays confirmed the preferential down regulation of miR 142 3p during macrophage differentiation in M CSF-derived immune suppressive M2 macrophages relative to the GM CSF-derived pro inflammatory M1. Forced over expression of miR 142 3p in M2 macrophages resulted in the down regulation of the M2 marker CD163, induction of apoptosis, and diminished phagocytosis; indicating miR 142 3p may induce a preferential elimination of M2 macrophages and/or a M2 to M1 like phenotypic shift. This is attributed to disruption of TGFBR1 autocrine signaling in the M2 population. In vivo local and systemic miR 142 3p administration resulted in glioma growth inhibition and extended median survival in immune competent GL261 glioma bearing mice and in genetically engineered murine models of glioma with correlative enhanced anti tumor immune responses. Results: The mean spontaneous velocity of diametric expansion before first line treatment was 5.8 ±6.3 mm/year. During the follow up, 209 patients presented a malignant transformation and 87 died. The malignant progression free survival and the overall survival were significantly longer in cases of slow velocity of diametric expansion (median, 103 and 249 months, respectively) than in cases of fast velocity of diametric expansion (median, 35 and 91 months, respectively) (p‹0.001). In multivariate analyzes, spontaneous velocity of diametric expansion as a categorical variable (‹4, ≥4 and ‹8, ≥8 and ‹12, ≥12 mm/year), was an independent prognostic factors for malignant progression free survival (p‹0.001; hazard ratio, 3.87; 95%CI, 2.67 5.52) and for overall survival (p‹0.001; hazard ratio, 4.62; 95%CI, 2.58 7.97). Velocity of diametric expansion was also an independent prognostic factor for overall survival as a continuous predictor, showing a linear relationship between overall survival and spontaneous velocity of diametric expansion (HR: 1.09 per one unit increase; 95%CI, 1.06 1.12; p<0.001). Conclusions: These data indicate a unique role of miR 142 3p in glioma immunity by modulating glioma infiltrating macrophage function, as well as a novel immunotherapeutic approach with transitional potential in glioma treatment. Conclusions: Independently to the molecular status, the spontaneous velocity of diametric expansion allows the identification of rapidly growing diffuse low grade gliomas (at higher risk of worsened evolution) during the pre-therapeutic period and without delaying treatment. 57 184. Catenin Signaling Initiates Astrocyte Activation And Contributes To The Pathogenesis of Astrocytomas 185. Long Term Follow-up After Stereotactic Radiosurgery for the Treatment of Meningiomas Shervin Rahimpour; Chunzhang Yang, PhD; Russell Lonser, MD; Zhengping Zhuang, MD, PhD (Bethesda, MD) John M. McGregor, MD; John Grecula; Mario Ammirati; Christopher Pelloski; Nina Mayr; Lanchun Lu; Nilendu Gupta; Susan Bell Introduction: Astrocyte injury results in disruption of intra/ extracellular contacts, loss of contact inhibition and subsequent migration and proliferation. Dysregulation of pathways involved in this response may be involved in the proliferative nature of neoplasias. Introduction: Complete surgical resection of intracranial meningiomas including the dura of origin and infiltrated bone remains the treatment of choice. Factors such as residual disease, advanced tumor grade, location within the cranial vault, or patient comorbidities may limit the success of surgery alone. Stereotactic radiosurgery (SRS) expands the options for treatment. We review the outcomes in patients with meningiomas treated with SRS at our institution from 1999 – 2012. Methods: Primary human and mouse astrocytes were cultured and an in vitro scratch assay was used for injury. Immunofluorescence staining, PCR array, and western blot analysis were performed to identify the spatial and temporal expression of molecular markers associated with astrocyte activation. β catenin siRNA knockdown studies were also performed in normal astrocytes and tumor sphere forming glioma cultures. Finally, both frozen and paraffin embedded tumor samples were stained for relevant markers. Methods: A retrospective review was performed of 78 patients with 82 presumed or confirmed meningiomas treated with SRS over the 13 year period. The median age was 56 (range 17-84). There were 19 males and 59 females. The median marginal dose was 15.95 Gy (range 10 -31 Gy) to an averaged 51% isodose line (range 47 – 70%). 39 patients had undergone surgery previous to treatment (50%). 10 patients had undergone previous radiation therapy prior to SRS (13%). The patients were followed clinically and radiographically at 1, 3, 5 and ≥10 years after SRS. Results: Following injury, GFAP and Nestin expression increased at the margins of the wound. PCR array revealed increased β catenin expression and an associated decrease in cadherin expression. Western blot analysis further showed that membrane bound β catenin decreased, while phosphorylated and cytoplasmic levels increased. siRNA knockdown of β catenin resulted in decreased expression of GFAP and nearly abolished expression of Nestin and SOX2 while in glioma cells, siRNA knockdown decreased tumor sphere size and S phase population. Results: The majority (n = 53) of tumors (65%) were located in the falx/parasagital or cerebral convexities while the others (n = 28) involved the skull base (34%). Tumor histology when available included 21 WHO grade I, 15 WHO grade II and 1 WHO grade III meningiomas. 45 patients had no definitive pathologic analysis. In reviewing all 82 tumors, 7 lesions required further treatment during the follow up period (9%), either further radiation or surgery. Three of these progressive lesions were tumors at the skull base, and 4 were convexity/parasagital in location. Four of these tumors were known WHO grade ll. Two were WHO grade l, and one did not have confirmatory pathology. Conclusions: We discovered that the loss of contact inhibition plays a critical role in the initiation and regulation of reactive astrocytes in the healing of wounds. In particular, injury of the astrocytes interrupts and destabilizes the - cadherin catenincomplexes at the cell membrane leading to nuclear translocation of β catenin and characteristic changes associated with the activation of astrocytes. Similar signaling pathways are not only found to be active, but also dysregulated, in astrocytomas. Conclusions: Radiosurgery is a reasonable adjunct to management of patients with primary, residual or recurrent meningiomas and presumed meningiomas. The control rates are ›90%. Longer follow up evaluations are still needed. 58 we are expanding geaux to booth 103 for the news Gliadel® is manufactured by Eisai Inc. for Arbor Pharmaceuticals, LLC. Gliadel® is a registered trademark of Eisai Inc. ©2013 Arbor Pharmaceuticals, LLC. All rights reserved. March 2013 GL020.001


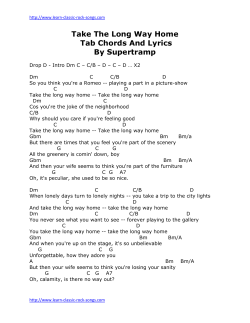









© Copyright 2026