
1 AANA Journal Course Anesthesia Case Management for Endovascular Aortic Aneurysm Repair
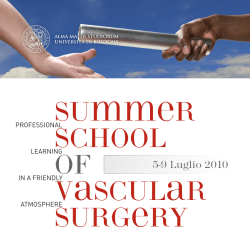
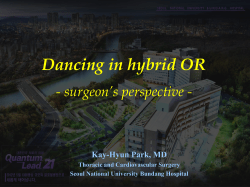
AANA Journal Course 1 Update for Nurse Anesthetists Anesthesia Case Management for Endovascular Aortic Aneurysm Repair Sass Elisha, CRNA, EdD John Nagelhout, CRNA, PhD, FAAN Jeremy Heiner, CRNA, EdD Mark Gabot, CRNA, MSN The incidence of angiopathology involving the aorta and microvasculature is expected to become more prevalent because of increased life expectancy and incidence of obesity. With the advent of endovascular aortic repair (EVAR), patients who were not considered surgical candidates for abdominal aortic aneurysmectomy because of their tenuous physical status can undergo corrective treatment and return to their activities of daily living. Because of the limited invasiveness of the procedure, it is unnecessary to cross-clamp the aorta, which minimizes hemodynamic variability and release of inflammatory mediators. As a result, the rate of myocardial ischemia, acute kidney injury, Objectives mesenteric ischemia, and blood loss is decreased. However, there are serious complications that can occur with EVAR, which include cerebral and myocardial ischemia, rapid massive hemorrhage, damage to access vessels, and endoleak. Presently, the most common anesthetic technique provided to patients undergoing EVAR is local anesthesia and monitored anesthetic care. A thorough understanding of the surgical procedure, perioperative process, and anesthetic considerations is vital to provide comprehensive care. Keywords: Endoleak, endovascular aortic repair, endovascular stent graft, EVAR. At the completion of this course, the reader should be able to: 1.Discuss strategies that can be employed to decrease perioperative mortality for patients having endovascular aortic repair (EVAR). 2.Create a comprehensive anesthetic plan for patients undergoing EVAR. 3. Describe the surgical advantages and disadvantages comparing EVAR with the traditional open approach for abdominal aortic aneurysmectomy. 4. Identify specific complications that can occur during intraoperative anesthetic management for patients having EVAR. 5. Discuss the postoperative anesthetic and surgical concerns after EVAR. allow surgeons to perform minimally invasive surgery, endovascular aortic repair (EVAR) has emerged as the preferred method for repair of abdominal aortic aneurysm (AAA). Endovascular aortic repair has evolved as the treatment of choice for AAA repairs. The surgical technique was initially developed in the late 1990s for patients who had significant comorbidities, which excluded them as a candidate for open surgical repair. The perioperative surgical and anesthetic management for patients with an AAA is multifaceted and must be individualized to the patient’s vascular anatomy and type and severity of coexisting disease. The occurrence of major perioperative complications such as myocardial infarction, acute kidney injury, mesenteric ischemia, postoperative pneumonia and inflammatory mediator release is less with EVAR than with the traditional open approach.1 Introduction Surgical Procedure As surgical and technologic advancements continue to Endovascular aortic aneurysm repair involves deploy- AANA Journal Course No. 34 (Part 1): AANA Journal course will consist of 6 successive articles, each with objectives for the reader and sources for additional reading. At the conclusion of the 6-part series, a final examination will be published on the AANA website and in the AANA Journal. This educational activity is being presented with the understanding that any conflict of interest on behalf of the planners and presenters has been reported by the author(s). Also, there is no mention of off-label use for drugs or products. www.aana.com/aanajournalonline AANA Journal April 2014 Vol. 82, No. 2 145 •Electrocardiogram •Echocardiogram (if history of congestive heart failure or other major risk factors) • Cardiac stress testing (if history of myocardial ischemia) • Angioplasty (according to risk factors) •Aneurysm scanning and ultrasound imaging for surgical planning (per surgeon) • Pulmonary function tests • Chest X-ray • Complete blood count • Blood chemistry • Estimated glomerular filtration rate • Blood urea nitrogen Figure 1. Comparison of Traditional Open Approach (A) and Endovascular Aortic Repair (B) ment of an endovascular stent graft within the aortic lumen. The graft reinforces the portion of the aorta where the aneurysm exists. A comparison of the traditional open procedure and EVAR is included in Figure 1. This procedure can be performed for patients who have descending thoracic aortic aneurysms or AAAs. The femoral arteries will be cannulated via a percutaneous approach or by dissection, depending on the size of the patient. Systemic anticoagulation with heparin, 50 to 100 units/kg, is accomplished before catheter insertion and manipulation into the femoral arteries. A sheath that contains the endovascular stent graft (EVSG) is inserted over a guidewire and positioned at the aneurysm location using radiographic imaging. The proximal end of the sheath must extend beyond the aneurysm. Once the EVSG is deployed, radial force or fixation mechanisms such as hooks or barbs become embedded into the aortic wall to prevent migration. The distal ends of the graft are then deployed and extend into both iliac arteries. After the EVSG is correctly positioned, the guidewire and sheath are removed followed by closure of both femoral artery insertion points. The procedure can take place in an interventional radiology suite or in the operating room (OR). Compared with the conventional surgical method, advantages of the endovascular approach include no aortic cross-clamping; improved hemodynamic stability; and decreased incidence of embolic events, blood loss, stress response, incidence of renal dysfunction, and postoperative discomfort.2 Endovascular graft design and durability continue to improve. Graft devices are either unibody (1 piece) or modular (multiple pieces). The endograft fabric is either woven polyester (Dacron) or polytetrafluoroethylene. The graft skeleton is constructed of stainless steel, nitinol, or elgiloy. Nitinol stents are popular because they exhibit minimal shortening after deployment. Future developments may include the use of drug-eluting endovascular stents. Drugs being tested are immunomodulators, anti- 146 AANA Journal April 2014 Vol. 82, No. 2 • Serum creatinine • Coagulation profile • Arterial blood gases analysis • Urine analysis • Hemoglobin A1c (if the patient is diabetic) • Blood glucose • Liver function tests Table 1. Suggested Preoperative Testing inflammatory, and antiproliferative agents. Initial clinical trial findings note that the rate of restenosis is improved with third- and fourth-generation endovascular stents.3 Improvements in surgical techniques, imaging, and graft devices will allow a greater number of patients to experience the technical and physiologic advantages of EVAR. Preoperative Evaluation and Preparation Patients undergoing EVAR are often elderly and have significant comorbidities. Preexisting cardiac, respiratory, and renal disease may significantly influence surgical outcomes.4 A thorough preoperative evaluation is required to determine if any essential testing is necessary to identify interventions to improve outcomes. Suggested preoperative testing is summarized in Table 1. Extensive radiographic imaging is performed by the surgical team to determine whether the patient is a candidate for EVAR as well as the best operative approach and the optimum EVSG for the aneurysm repair. The guiding principle for preoperative evaluation is to identify information that will alter management to improve postoperative outcomes or provide baseline information that can be used to guide perioperative care. Preoperative testing most often involves identifying and characterizing cardiac, respiratory, renal, endocrine (such as diabetes), atherosclerotic, and peripheral arterial occlusive disease. Cardiac complications, especially related to coronary artery disease, remain the most frequent cause of mortality following either open aortic repair or EVAR.5 Guidelines have been developed for cardiac evaluation of patients scheduled for noncardiac vascular surgery.6 Patients are www.aana.com/aanajournalonline Evaluation Activity level 1. Is there an active cardiac condition? Clinical risk factors Recommendation Unstable coronary syndrome Unstable or severe angina Recent MI (< 1 mo) Decompensated CHF Significant arrhythmias Severe valvular disease Presence cancels or delays aortic aneurysm repair until condition is treated. Implement medical management and consider coronary angiography. 2. Does the patient have good functional capacity without symptoms? MET ≥ 4 Mild angina pectoris Prior MI Compensated or prior CHF Diabetes mellitus Renal insufficiency May proceed with aneurysm repair. In patient with unknown cardiovascular disease or at least one clinical risk factor, β-blockade is appropriate. 3. Is functional capacity poor or unknown? MET < 4 Mild angina pectoris Prior MI Compensated or prior CHF Diabetes mellitus Renal insufficiency In patients with ≥ 3 clinical risk factors, preoperative noninvasive testing is appropriate if it will change management. Table 2. Preoperative Cardiac Evaluation for Patients Undergoing Aneurysm Repair Abbreviations: CHF, congestive heart failure; MET, metabolic equivalent unit; MI, myocardial infarction. (Adapted from Chaikof et al6 and Fleisher LA, Beckman JA, Brown KA, et al. ACC/AHA 2007 Guidelines on perioperative cardiovascular evaluation and care for noncardiac surgery: executive summary. Circulation. 2007;116(17): e418-e500. Used with permission.) ranked according to the number of risk factors present and their overall functional capacity. Risk factors include the following: symptomatic heart disease and the presence of angina, prior history of myocardial infarction, compensated congestive heart failure (CHF), renal disease, diabetes, and cerebrovascular accident. The extent of testing will depend on the individual patients’ symptoms and the number of risk factors. Stress testing and myocardial reperfusion scans are helpful in predicting possible adverse events in higher risk patients.7 Coronary angiography may be considered for patients with active myocardial ischemia or disease of the left coronary artery. An electrocardiogram is required in all patients, and an echocardiogram is included for those with a history of CHF or other major cardiac risk factors or symptoms. Table 2 summarizes cardiac evaluation guidelines.6,8 Antihypertensive agents, statins, β-blockers, aspirin, and other antiplatelet drugs are widely used in these patients and should be assessed for proper dosing and efficacy. Statin therapy results in significant risk reduction in vascular surgery and should be started in all patients 1 month before surgery and continued indefinitely. Oral β-blockers should be given to all patients with intermediate to high cardiac risk. They should be started as early as possible before surgery, preferably 1 month, and titrated to a target heart rate of 60 to 70 beats/min. Administration of intravenous (IV) high-dose β-blockers immediately before surgery may be detrimental and should be avoided.8 Antiplatelet drugs are not a contraindication for EVAR, and aspirin is frequently continued throughout the perioperative period. Warfarin therapy is discontinued 5 to 7 days before surgery, and the patient is bridged to treatment with low-molecularweight heparin or unfractionated heparin if kidney injury www.aana.com/aanajournalonline is present.4,8 If regional anesthesia is planned, a detailed protocol should be in place and followed for managing perioperative anticoagulation for neuraxial blockade, catheter insertion, and catheter removal. As smoking is a major risk factor for the development of AAA, many of these patients have chronic respiratory disease. A respiratory assessment, including chest radiograph, pulmonary function testing, and blood gas analysis, will help guide anesthesia providers to create a comprehensive plan for perioperative ventilation. Patients with a history of respiratory disease, especially chronic obstructive pulmonary disease, should have their therapy optimized. Smoking cessation 2 weeks before surgery, along with chest physical therapy, incentive spirometry, and early ambulation, may all be beneficial in avoiding postoperative respiratory complications.6 Recent steroid use should be ascertained and appropriate coverage instituted to avoid the potential for acute adrenal crises. Preexisting renal disease is the most significant risk factor for postoperative kidney injury after aortic aneurysm repair. In addition, coexisting renal artery occlusion may be present in up to 38% of patients with an AAA.5 Renal compromise may result from inadvertent procedural vascular occlusion and possible radiographic contrast nephropathy. Renal assessment and protection strategies may improve postoperative outcomes. Determination of serum creatinine and estimated glomerular filtration rate (eGFR) will help guide potential renal protection strategies. An analysis of the effect of renal status on postoperative outcomes in 8,701 patients in the National Surgical Quality Improvement Program database was recently reported.9 Patients were assigned to a chronic kidney disease (CKD) class based on eGFR AANA Journal April 2014 Vol. 82, No. 2 147 values according to the National Kidney Foundation clinical guidelines.10 With the CKD classification system, the eGFR and CKD severity were categorized as normal to mild (CKD stage 1 or 2), moderate (CKD stage 3), and severe (CKD stage 4 or 5). This information is presented in Table 3. The presence of moderate or severe CKD is associated with significantly increased mortality and therefore should figure prominently in clinical decision making. The high mortality in AAA repair in patients with severe CKD may be a contraindication to an elective repair except in extenuating clinical circumstances.9 In a retrospective analysis of 208 patients who underwent EVAR, acute kidney injury occurred in 15% to 19% of patients.10 Major risk factors for renal injury are preexisting renal disease (eGFR < 60), advanced age, operative time, contrast volume, and preoperative use of angiotensinconverting enzyme inhibitors. Intravenous hydration to maintain an adequate urine output is effective in reducing renal complications. This requires careful management in patients with renal disease. They may benefit from strategies to minimize the inherent renal risks of EVAR, including the use of alternate diagnostic methods that allow for the administration of reduced volumes or different contrast mediums. Other strategies that may reduce renal injury include the administration of N-acetylcysteine, preoperative bicarbonate, and ascorbic acid.4,6 Diabetic patients should be managed according to standard hospital protocols. Intraoperative Considerations Intraoperative objectives for patients undergoing EVAR should focus on maintaining hemodynamic stability, providing analgesia and anxiolysis, and planning to rapidly convert to general anesthesia (GA) if an open procedure is necessary. Anesthetic techniques employed during EVAR can include GA, neuraxial (spinal and epidural) anesthesia, or local infiltration with sedation. Traditionally, GA or neuraxial anesthesia (NA) was the preferred anesthetic techniques for EVAR. Currently, there is evidence to suggest that patients who receive local anesthesia (LA) with sedation or NA, compared with GA, have decreased cardiac, respiratory, and renal complications; fewer postoperative admissions to the intensive care unit (ICU); and a decreased length of hospitalization.11-15 Researchers evaluated more than 5,500 patients from the EUROSTAR database in an attempt to determine if anesthesia influenced patient outcomes: mortality, morbidity, hospital stay, and ICU admission. There were no significant differences in mortality, but a reduction in cardiac complications, decreased overall ICU stay, and length of hospitalization was achieved for those patients who received LA as the primary anesthetic.16 Results from studies also indicated that plasma catecholamine concentrations and mediators of the systemic immune response were decreased in patients who underwent 148 AANA Journal April 2014 Vol. 82, No. 2 StageDescription GFR 1 Kidney damage with normal or increased GFR > 90 (with CKD risk factors) 2 Kidney damage with mild or decreased GFR 60-89 3 Moderately decreased GFR 30-59 4 Severely decreased GFR 15-29 5 Kidney failure < 15 (or dialysis) Table 3. National Kidney Foundation Classification: Stages of Chronic Kidney Disease Abbreviations: GFR, glomerular filtration rate; CKD, chronic kidney disease. (Adapted from Pisimisis et al.10 Used with permission.) EVAR compared with conventional open repair.17 Plasma cortisol release was lower in patients having EVAR than in traditional open AAA repair. The EVAR group also experienced a decreased incidence of sepsis and systemic immune response syndrome.18 Endograft complications that can arise from EVAR include thrombosis, EVSG migration or rupture, and infection. Procedural complications include iliac artery rupture and lower extremity ischemia.19 Fatal cerebral embolism resulting in sudden respiratory arrest has also occurred during EVAR.20 A consensus regarding the preferred anesthetic technique for EVAR has yet to be determined. Indications for GA, NA, and LA for EVAR are listed in Table 4. Research is ongoing to determine an ideal anesthetic technique that results in a decreased mortality within 30 days postoperatively. • General Anesthesia. General anesthesia is most often reserved for complex vascular anatomy or if the patient is unable to tolerate NA or LA. The use of GA has been associated with increased blood loss, volume of ionized contrast medium administered, and exposure to radiation compared with LA and NA.11 A review of more than 6,000 EVAR procedures from the American College of Surgeons National Surgical Quality Improvement Program database indicated that increased pulmonary complications and longer hospitalization are associated with GA.21 In healthy patients, cerebral and coronary artery autoregulation is maintained at a mean arterial pressure between 60 mm Hg and 140 mm Hg.22 When mean arterial pressures are below this general range, blood flow becomes largely pressure dependent. For patients with vascular disease, it must be assumed that there is some degree of angiopathology in the cerebral and coronary vasculature. Higher mean arterial pressures may be necessary to adequately perfuse the heart and brain because of autoregulatory changes. One of the most important intraoperative goals during GA for EVAR includes achieving hemodynamic stability and maintaining adequate blood flow to vital organs. • Neuraxial Anesthesia. Spinal anesthesia can be successfully performed using 0.75% bupivacaine as a single www.aana.com/aanajournalonline General anesthesia Neuraxial anesthesia Local anesthesia • Retroperitoneal approach •History of difficult airway management • History of difficult airway management • Local anesthetic allergy •Cardiac, respiratory, and renal disease •Inability to obtain patient cooperation • Sleep apnea •Severe cardiac, respiratory, and renal disease • Severe gastroesophageal reflux • Obstructive sleep apnea •Inability to lie still for long periods of time • Need for an awake patient • Severe gastroesophageal reflux • Previous groin surgery •Currently prescribed antiplatelet or anticoagulant medications • Surgeon’s preference • Need for an awake patient • Severe anxiety •Challenging aneurysm morphology • Obesity (BMI > 35 kg/m²) •Need for associated abdominal procedures requiring general anesthesia •Need to convert to open aortic repair Table 4. Indications for the Use of General, Neuraxial, and Local Anesthesia for Endovascular Aortic Repair Abbreviation: BMI, body mass index. injection. Epidural anesthesia using 0.5% bupivacaine divided into 5-mL bolus doses to achieve a T6-T8 level provides adequate anesthesia. Additional bolus doses may be given throughout the intraoperative period. The use of NA eliminates pain associated with initial cannulation, dilation, and manipulation of the femoral arteries, and it prevents movement of the lower extremities. Systemic anticoagulation is established before sheath insertion and EVSG deployment. Because of systemic anticoagulation, the potential risk of hemorrhage from neuraxial techniques is increased. If an epidural catheter has been placed, the return of normal coagulation parameters should be verified before removal. • Local Anesthesia. The pain associated with EVAR originates from cannulation of the femoral artery. Adequate anesthesia can be accomplished by providing both bilateral ilioinguinal and iliohypogastric nerve blocks and local infiltration at the femoral insertion sites using local anesthetics combined with epinephrine. Sedation is titrated for patient comfort while maintaining adequate spontaneous ventilation. Dexmedetomidine and remifentanil may be especially useful because of their short duration of action. Dexmedetomidine can work synergistically with opioids decreasing the transient ischemic pain associated with femoral artery occlusion during stent deployment.23 Furthermore, dexmedetomidine has the potential to cause diuresis by inhibiting vasopressin secretion, inducing sympatholysis and enhancing glomerular filtration resulting in an increase in urine output, which may help to clear radiographic contrast dye. When receiving LA compared with NA and GA, the patient retains the ability to sense severe discomfort during insertion of the femoral sheaths. Ischemic pain www.aana.com/aanajournalonline resulting from femoral artery occlusion by the sheath can be a sign of impending femoral artery rupture.23 In addition, the use of LA may promote improved hemodynamic stability because fewer cardiac and respiratorydepressant medications are required. The preferred monitoring for EVAR is outlined in Table 5. Arterial blood pressure monitoring should be considered before the beginning of the procedure, especially since this patient population has vascular and cardiac comorbidities and accurate blood pressure measurements are necessary to guide therapeutic interventions. Venous access should consist of 1 to 2 large-bore peripheral IV access and is strongly recommended. Central venous access can be considered in patients with severe cardiac disease, although many researchers believe it is not required because prolonged infusions of vasoactive medications and ICU admissions are rare.24 Lead shielding is required for the patient and OR personnel because of extensive use of radiologic imaging during EVAR. Bradycardia can occur during deployment of the EVSG because of increased pressure transmitted to the aortic baroreceptors. If bradycardia occurs, it is most often of short duration and can be treated by anticholinergic medications. A major complication during the EVAR procedure is severe hemorrhage. Hemorrhage may occur from damage to the femoral arteries or aortic rupture. A type and screen should be ordered and resuscitation equipment should be readily available, as shown in Table 5.25 The anesthetist should be prepared to secure the patient’s airway with an endotracheal tube in the event that surgeons need to convert to an open procedure. If there is substantial blood loss, rapid transfusion of blood and blood products should be initiated. AANA Journal April 2014 Vol. 82, No. 2 149 MonitoringEquipment • Five-lead electrocardiography • Intravenous access supplies • Pulse oximetry • Forced-air convective warming device • End-tidal CO2 • Fluid warmers • Automatic intermittent blood pressure cuff • Crystalloid and colloid fluids • Temperature monitor • Invasive monitoring access supplies and transducers • Foley catheter • Medication infusion pumps • Intra-arterial pressure monitoring • Level 1 rapid infuser • Central venous pressure monitoring (as indicated) • Blood analysis equipment • Type and screen • Lead aprons for OR personnel •Electrolytes • Complete blood cell count • Coagulation assays • Blood glucose Table 5. Anesthetic Preparation for Endovascular Aortic Repair Abbreviations: CO2, carbon dioxide; OR, operating room. Thoracic Endovascular Aortic Repair •Endoleak Thoracic aortic aneurysms comprise 25% of aortic aneurysms and affect approximately 15,000 people in the United States per year.26 In 2010, the American College of Cardiology Foundation and other organizations proposed evidence-based guidelines for the diagnosis and treatment of patients with thoracic aortic disease.27 These experts recommend that thoracic endovascular aortic repair (TEVAR) be strongly considered for patients with degenerative or traumatic aneurysms of the descending thoracic aorta exceeding 5.5 cm, saccular aneurysms, or postoperative pseudoaneurysms.27 Thoracic endovascular aortic repair has been used for treatment of aneurysms of the descending aorta and more proximal aneurysms using 2-staged or hybrid procedures such as combined endovascular and surgical extra-anatomic bypass grafting.26 Intraoperative transesophageal echocardiography has gained increasing acceptance because of its ability to assess ventricular function and provide diagnostic information.28 Somatosensory and motor evoked potentials and electroencephalographic monitoring have also been used to assess spinal cord and cerebral ischemia, respectively.26,28 Cerebrospinal fluid (CSF) drainage is recommended as a spinal cord protective strategy to promote spinal cord perfusion in TEVAR and open procedures for patients at high risk of spinal cord ischemic injury. Spinal cord ischemia and stroke remain the most devastating complications associated with TEVAR. The incidence has been reported to be as high as 8%.26 However, the incidence of paraplegia has been reported to be as high as 20% when aortic cross-clamping is used in an open approach.29 Compromised blood flow as a result of hypotension, graft occlusion, inadequate collateral perfusion, or atheroembolism to the anterior spinal artery or vertebral arteries has been suggested as possible causes. Intraoperative neuromonitoring, blood pressure support • Arterial damage 150 AANA Journal April 2014 Vol. 82, No. 2 o Iatrogenic aneurysm rupture oIliac artery damage during arterial access, placement of sheath, or delivery device o Iliac or aortic dissection •Embolization (distal embolization of atheromatous material causing ischemia to the bowel, lower extremities, spinal cord, kidneys, or other organs; proximal embolization to the aortic arch causing cerebral ischemia and neurologic deficit) • Hemorrhage, either overt or covert (eg, retroperitoneal) • Endograft-related complications o Failed or delayed displacement of graft o Migration or malpositioning of graft o Occlusion of renal, mesenteric, or other major aortic ostia •Contrast related complications (eg, allergic reaction to contrast media, contrast nephropathy) •Postimplantation syndrome (eg, fever, back pain, leukocytosis, elevated C-reactive protein) •Infection Table 6. Surgical-Related Complications Associated With Endovascular Aortic Repair (Adapted from Smaka et al24 and Walker et al.30 Used with permission.) with volume expansion and vasopressor therapy, and lumbar CSF drainage have been cited as strategies to decrease the risk of spinal cord ischemia.26,28 Postoperative Considerations Postoperative considerations related to EVAR can be divided into patient and surgical-related complications. These may be attributed to coexisting medical conditions such as cardiac, renal, respiratory, and other vascular disease. Subsequent exacerbation of an underlying pathologic process, for example, myocardial ischemia, acute www.aana.com/aanajournalonline Classification Defining characteristics Type 1Failure to achieve complete seal between endograft and aortic or iliac artery wall; persistent flow into aneurysm sac through proximal or distal endograft attachment site Type 2Retrograde flow into aneurysm sac, usually from lumbar artery or inferior mesenteric artery Type 3Flow into aneurysm sac due to inadequate overlap at junction of modular graft components or to defect in graft fabric Type 4Blood flow through pores in fabric of stent graft into aneurysm sac Table 7. Classification of Endoleak (Types 1-4) (Adapted from Smaka et al24 and Walker et al.30 Used with permission.) Figure 2. Schematic Representations of Endoleak (Types 1-4)a a Type 1 endoleak = inadequate proximal graft seal resulting in kidney injury, or respiratory failure, occurs because of the physiologic stress of surgery and anesthesia. Surgicalrelated complications are found in Table 6.24,30 Endoleak, or continued blood flow outside the EVSG into the residual aneurysm sac, is the most common surgical complication following EVAR.30 Endoleak diagnosed with the use of postoperative computed tomography (CT) has been reported to occur in 15% to 52% of patients.31 Endoleak may cause aortic rupture by exposing the weakened aneurysm wall to continued pressure from blood flow. Endoleaks are classified according to the source of continued perfusion of the aneurysm sac. Characteristics and an illustration of endoleak can be found in Table 7 and Figure 2.24,30 Type 2 endoleaks caused by collateral retrograde flow are the most common type of endoleak. Seventy percent of type 2 endoleaks are self-limiting and resolve spontaneously in the first month after implantation.31 Type 1 and type 3 endoleaks may require secondary reintervention to minimize blood flow to the aneurysm sac. Treatment of an endoleak varies according to patient symptoms and radiographic findings, and may involve medical management or surgical intervention. Possible surgical reintervention may include coil embolization, endograft removal, implantation of a graft sleeve, or open repair.3,30 If secondary endovascular reinterventions fail, then an open abdominal aortic aneurysmectomy is required. Because of the lack of quantitatively established longterm outcomes, postoperative follow-up care for patients who have undergone EVAR is critical. Physical examination and contrast medium–enhanced CT are recommended at 1, 6, 12, and 18 months postoperatively and then annually. Abdominal radiographs should be obtained on a regular basis. Lifelong radiographic evaluation and surveillance is necessary to monitor aneurysm size, graft migration, and endoleak. Intensive follow-up care, the need for reinterventions, and the cost of the endograft make EVAR more expensive than open repair.32 www.aana.com/aanajournalonline perigraft blood flow; type 2 endoleak = retrograde blood flow from collateral vessels pressurize aneurysm sac; type 3 endoleak = graft failure and modular disconnection of graft sections; and type 4 endoleak = blood flow through graft skin over time. Three prospective randomized trials comparing early and late morbidity and mortality following open repair and EVAR have been reported. The results indicate the following: (1) the 30-day morbidity rates are significantly lower after EVAR than open repair; (2) 2-, 4-, and 6-year morbidity rates are similar in both groups; and (3) reintervention rates after EVAR are higher than after open repair.33 A multicenter, randomized trial by Lederle et al34 determined that no significant difference existed in long-term (9-year) all-cause mortality between EVAR and open repair. This may be due to the fact that the life expectancy for patients with severe systemic angiopathology is decreased. Endovascular aortic repair was also associated with improved long-term outcome for patients less than 70 years of age, but for older patients EVAR reduced survivability.34 A comprehensive knowledge of all aspects of the surgical procedure and the patient’s physical status is necessary for competent anesthesia care. Despite the minimal surgical invasiveness of EVAR compared with the traditional open procedure, serious and life-threatening complications such as massive hemorrhage, myocardial or cerebral infarction, embolism, acute kidney injury, and vascular damage are possible. By being informed and prepared, all members of the surgical team can safely contribute to high-quality patient care in patients undergoing EVAR. REFERENCES 1. Marjanović I, Jevtić M, Misović S, et al. Early inflammatory response following elective abdominal aortic aneurysm repair: a comparison between endovascular procedure and conventional, open surgery [Serbian]. Vojnosanit Pregl. 2011;68(11):948-955. 2. Schermerhorn ML, O’Malley AJ, Jhaveri A, Cotterill P, Pomposelli F, Landon BE. Endovascular vs. open repair of abdominal aortic aneu- AANA Journal April 2014 Vol. 82, No. 2 151 rysms in the Medicare population. N Engl J Med. 2008;358(5):464474. doi:10.1056/NEJMoa0707348. 3. Ren S, Fan X, Ye Z, Liu P. Long-term outcomes of endovascular repair versus open repair of abdominal aortic aneurysm. Ann Thorac Cardiovasc Surg. 2012;18(3):222-227. 4. Moll FL, Powell JT, Fraedrich G, et al. Management of abdominal aortic aneurysms clinical practice guidelines of the European Society for Vascular Surgery. Eur J Vasc Endovasc Surg. 2011;41(suppl)1:S1S58. doi:10.1016/j.ejvs.2010.09.011. 5. Tracci MC, Cherry KJ Jr. Aorta. In: Townsend CM Jr, Beauchamp RD, Evers BM, Mattox KL, eds. Sabiston Textbook of Surgery: The Biological Basis of Modern Surgical Practice. 19th ed. Philadelphia, PA: Elsevier Saunders; 2012:1697-1724. 6. Chaikof EL, Brewster DC Dalman RL, et al. The care of patients with an abdominal aortic aneurysm: the Society for Vascular Surgery practice guidelines. J Vasc Surg. 2009;50(4 suppl):S2-S49. doi:10.1016/j. jvs.2009.07.002. 7. Hartley RA, Pichel AC, Grant SW, et al. Preoperative cardiopulmonary exercise testing and risk of early mortality following abdominal aortic aneurysm repair. Br J Surg. 2012;99(11):1539-1546. doi:10. 1002/bjs.8896. 8. Schouten O, Sillesen H, Poldermans D; European Society of Cardiology. New guidelines from the European Society of Cardiology for perioperative cardiac care: a summary of implications for elective vascular surgery patients. Eur J Vasc Endovasc Surg. 2010;39(1):1-4. doi:10.1016/j.ejvs.2009.10.005. 9. Patel VI, Lancaster RT, Mukhopadhyay S, et al. Impact of chronic kidney disease on outcomes after abdominal aortic aneurysm repair. J Vasc Surg. 2012;56(5):1206-1213. doi:10.1016/j.jvs.2012.04.037. 10. Pisimisis GT, Bechara CF, Barshes NR, Lin PH, Lai WS, Kougias P. Risk factors and impact of proximal fixation on acute and chronic renal dysfunction after endovascular aortic aneurysm repair using glomerular filtration rate criteria. Ann Vasc Surg. 2013;27(1):16-22. doi:10.1016/j.avsg.2012.05.006. 11. Verhoeven EL, Cinà CS, Tielliu IF, et al. Local anesthesia for endovascular abdominal aortic aneurysm repair. J Vasc Surg. 2005;42(3):402-409. 12. Franz R, Hartman J, Wright M. Comparison of anesthesia technique on outcomes of endovascular repair of abdominal aortic aneurysms: a five-year review of monitored anesthesia care with local anesthesia vs. general or regional anesthesia. J Cardiovasc Surg Torino. 2011;52(4):567-577. 13 Geisbüsch P, Katzen BT, Machado R, Benenati JF, Pena C, Tsoukas AI. Local anaesthesia for endovascular repair of infrarenal aortic aneurysms. Eur J Vasc Endovasc Surg. 2011;42(4):467-473. doi:10.1016/ j.3jfw.2011.05.018. 14. Bakker EJ, van de Luijtgaarden KM, van Lier F, et al. General anaesthesia is associated with adverse cardiac outcome after endovascular aneurysm repair. Eur J Vasc Endovasc Surg. 2012;44(2):121-125. doi:10.1016/j/.ejvs.2012.04.028. 15. Edwards MS, Andrews JS, Edwards AF, et al. Results of endovascular aortic aneurysm repair with general, regional, and local/monitored anesthesia care in the American College of Surgeons National Surgical Quality Improvement Program database. J Vasc Surg. 2011;54(5):1273-1282. doi:10.1016/j.jvs2011.04.054. 16. Ruppert V, Leurs LJ, Steckmeier B, Buth J, Umscheid T. Influence of anesthesia type on outcome after endovascular aortic aneurysm repair: an analysis based on EUROSTAR data. J Vasc Surg. 2006;44(1):16-21; discussion 21. 17. Elisha S. Anesthesia for vascular surgery. In: Nagelhout JJ, Plaus K, eds. Nurse Anesthesia. 5th ed. St Louis, MO: Saunders Elsevier; 2014:561-589. 18. Pearson S, Hassen T, Spark JI, Carbot J, Cowled P, Fritridge R. Endovascular repair of abdominal aortic aneurysm reduces intraoperative cortisol and perioperative morbidity. J Vasc Surg. 2005;41(6):919-925. 19. Dattilo JB, Brewster DC, Fan CM, et al. Clinical features of endovascular abdominal aortic aneurysm repair: incidence, causes and management. J Vasc Surg. 2002;35(6):1137-1144. 20. Zaugg M, Lachat ML, Pfammatter T, Cathomas G, Schmid ER. Sudden respiratory arrest resulting from brain stem embolism in a patient undergoing endovascular abdominal aortic aneurysm repair. Anesth Analg. 2001;92(2):335-337. 152 AANA Journal April 2014 Vol. 82, No. 2 21. Wylie SJ, Wong GT, Chan YC, Irwin MG. Endovascular aneurysm repair: a perioperative perspective. Acta Anaesthesiol Scand. 2012;56: (8)941-949. doi:10.1111/j/1399-6576.2012.02681.x. 22. Elisha S. Cardiovascular anatomy, physiology, pathophysiology and anesthesia management. In: Nagelhout JJ, Plaus K, eds. Nurse Anesthesia. 5th ed. St Louis, MO: Saunders Elsevier; 2014:561-589. 23.Karthikesalingam A, Thrumurthy SG, Young EL, Hinchliffe RJ, Holdt PJ, Thompson MM. Locoregional anesthesia for endovascular aneurysm repair. J Vasc Surg. 2012;56(2):510-519. doi:10.1016/j/jvs. 2012.02.047. 24. Smaka TJ, Cobas M, Velazquez OC, Lubarsky DA. Perioperative management of endovascular abdominal aortic aneurysm repair: update 2010. J Cardiothorac Vasc Anesth. 2011;25(1):166-176. doi:10.1053/j. fvac.2010.08.010. 25. Pichel AC, Serracino-Inglott F. Anaesthetic considerations for endovascular abdominal aortic aneurysm repair (EVAR). Curr Anaesth Crit Care. 2008;19:150-162. 26. Gutsche JT, Szeto W, Cheung AT. Endovascular stenting of thoracic aortic aneurysm. Anesthesiology Clin. 2008;26(3):481-499. doi:10. 1016/j.1ndlin.2008.03.006. 27. Hiratzka LF, Bakris GL, Beckman JA, et al. 2010 ACCF/AHA/AATS/ ACR/ASA/SCA/SCAI/SIR/STS/SVM guidelines for the diagnosis and management of patients with thoracic aortic disease: a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines, American Association for Thoracic Surgery, American College of Radiology, American Stroke Association, Society of Cardiovascular Anesthesiologists, Society for Cardiovascular Angiography and Interventions, Society of Interventional Radiology, Society of Thoracic Surgeons, and Society for Vascular Medicine. Circulation. 2010;121(13):3266-3269. doi:10.1161/ CIR.0b013e3181d4739e. 28. Andritsos M, Desai ND, Grewal A, Augoustides JG. Innovations in aortic disease management: the descending aorta. J Cardiothorac Vasc Anesth. 2010;24(3):523-529. doi:10.1053/j.jvca.2010.02.004. 29.Demetriades D, Velmahos G, Scalae T, et al. Operative repair of endovascular stent graft in blunt traumatic thoracic aortic injuries: results of an American Association for the Surgery of Trauma multicenter study. J Trauma. 2008;64(3):561-570; discussion 570-571. doi:10.1097/TA.Ob013e3181641bb3. 30. Walker TG, Kalva SP, Yeddula K. Wicky S, Kundau S, Drescher P, et al. Clinical practice guidelines for endovascular abdominal aortic aneurysm repair: Written by the Standards of Practice Committee for the Society of Interventional Radiology and Endorsed by the Cardiovascular and Interventional Radiological Society of Europe and the Canadian Interventional Radiology Association. J Vasc Interv Radiol. 2010;21(11):1632-1655. doi:10.1016/j.jvir.2010.07.008. 31. Buth J, Laheij RJ. Early complications and endoleaks after endovascular abdominal aortic aneurysm repair: report of a multicenter study. J Vasc Surg. 2000;311(pt 1):134-146. 32.Rutherford RB. Open versus endovascular stent graft repair for abdominal aortic aneurysms: an historical view. Semin Vasc Surg. 2012;25(1):39-48. doi:10.1053/j.semvascsurg.2012.03.005. 33. Schanzer A, Messina L. Two decades of endovascular abdominal aortic aneurysm repair: enormous progress with serious lessons learned. J Am Heart Assoc. 2012;1(3):e000075. doi:10.1161/JAHA.111.000075. 34.Lederle FA, Freischlag JA, Kyriakidas TC, et al; OVER Veterans Affairs Cooperative Study Group. Long-term comparison of endovascular and open repair of abdominal aortic aneurysm. N Engl J Med. 2012;367(21):1988-1997. doi:10.1056/NEJMOA1207481. AUTHORS Sass Elisha, CRNA, EdD, is the assistant director of the Kaiser Permanente School of Anesthesia in Pasadena, California. Email: [email protected]. John Nagelhout, CRNA, PhD, FAAN, is the program director of the Kaiser Permanente School of Anesthesia in Pasadena, California. Jeremy Heiner, CRNA, EdD, is an educator at the Kaiser Permanente School of Anesthesia in Pasadena, California. Mark Gabot, CRNA, MSN, is an educator at the Kaiser Permanente School of Anesthesia in Pasadena, California. www.aana.com/aanajournalonline










© Copyright 2026