ABC
docz
Explore
Log in
Create new account
Download
Report
health and fitness
addiction
alcoholism
Individual Differences in Drug Response - Home
Dear Parent, You are requested to furnish a Declaration cum
TRAINING AND DEVELOPMENT 1
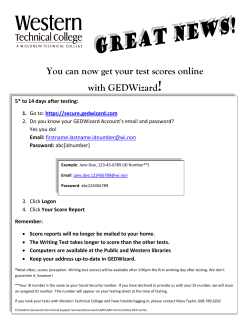
! You can now get your test scores online with GEDWizard
The test - Wayzata Public Schools
Contents - Alcohol and Alcoholism
Choosing a block of land
Non-Cultural Methods for Aspergillosis
Seventh assignment Math 217 Probability and Statistics
Pediatric CMA Patient Brochure-112014-FINAL-Low-Res
ISQ Personal Development Profile Chart
© Copyright 2026
About abcdocz
DMCA / GDPR
Report