
What the Tumor Does to Nutrition and What Poor Nutrition Does to
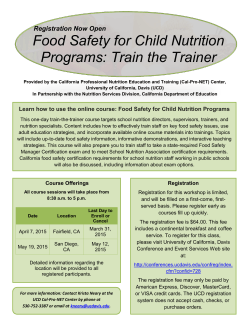
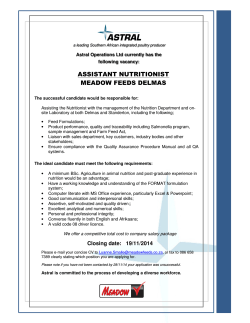
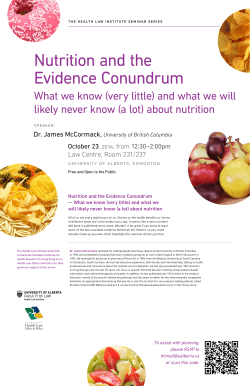
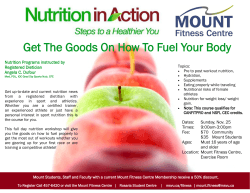
What the Tumor Does to Nutrition and What Poor Nutrition Does to the Patient and Treatment Outcomes Columbus Chapter Oncology Nursing Society 26th Annual Spring Conference Kaleidoscope of Oncology Care March 26, 2015 Anne Coble Voss, PhD, RDN, LD Associate Research Fellow, Abbott Nutrition R&D Cancer Nutrition Therapy GDS_80000_Title_v1 1 Disclosure The speaker is an Associate Research Fellow in Adult Nutrition Science at Abbott Nutrition but will not be discussing Abbott products. Cancer Nutrition Therapy 2 GDS_80000_Title_v1 2 Presentation Objectives 1. Identify the impact the tumor and anti-cancer treatments have on nutrition status in the adult oncology patient 2. Determine the effect of lean body mass loss on treatment outcomes in the adult oncology patient 3. Characterize the effect of cancer and its treatment on outcomes 4. Recognize national/international guidelines and recommendations 5. Develop early nutrition screening and intervention plan . Cancer Nutrition Therapy 3 GDS_80000_Title_v1 3 1 MALNUTRITION Cancer Nutrition Therapy 4 GDS_80000_Title_v1 4 Historic definitions of malnutrition marasmus • kwashiorkor • protein-energy undernutrition Cancer Nutrition Therapy Jensen GL, et al. JPEN J Parenter Enteral Nutr. 2009;33:710-716. 5 GDS_80000_Title_v1 5 What is malnutrition? A state of nutrition in which a deficiency, excess, or imbalance of energy, protein, and other nutrients causes measurable adverse effects on body function and clinical outcome.1 Up to 1 in 2 adults admitted to hospital or care homes is or at risk of malnutrition. – Somanchi M, et al. JPEN. Mar 2011;35(2):209-216 Estimated up to 80% of advanced patients with cancer have malnutrition. – Poole K, Froggatt K. Palliative medicine. 2002;16(6):499-506 1. Elia M, ed. Guidelines for Detection and Management of Malnutrition: A Report of the Malnutrition Advisory Group. 6 Maidenhead, UK: British Association for Parenteral and Enteral Nutrition (BAPEN); 2000. GDS_80000_Title_v1 Cancer Nutrition Therapy 6 2 Malnutrition and weight loss are common in cancer patients • At cancer diagnosis, approximately 50% of patients present with some nutritional issues1 • In certain cancers, up to 85% of patients will develop malnutrition/weight loss2,3 during treatment • Involuntary weight loss of just 5% results in decreased survival5 Most common secondary diagnosis for cancer patients is malnutrition4 1. Halpern-Silveira D, et al. Support Care Cancer. 2010;18(5):617-625; 2. Laviano A, Mequid MM. Nutrition. 1996;12(5):358-371; 3. Bozzetti F. Nutrition support in patietns with cancer. In: Payne-James J, Grimble G, Silk D, eds. Artificial Nutrition Support in Clinical Practice. 2nd ed. London: GMM; 639-680; 4. National Cancer Institute. Nutrition in Cancer Care. www.cancer.gov/cancertopics/pdq/supportivecare/nutrition/HealthProfessional/page1. 5. Dewys WD, et al. Am J Med 1980;69(4):491-7 Cancer Nutrition Therapy 7 GDS_80000_Title_v1 7 Malnutrition in the Adult Oncology Patient • Weight loss and malnutrition are common in the oncology patient • In a classic paper by Dewys 1980 malnutrition ranged from 31% to 87%1 • Recent paper by Hebuterne 2014 40% of hospitalized oncology patients were malnourished2 This concept is similar to hospital malnutrition and “The Skeleton in the Hospital Closet” 3 1. Dewys Am J Med 1980; 2. Hebuterne JPEN 2014; Butterworth Today’s Dietitian 1974 Cancer Nutrition Therapy 8 GDS_80000_Title_v1 8 Malnutrition & Weight Loss • Oncology nutrition risk studies show: • 32% outpatients mixed tumor types were malnourished1 • 34% malnourished, 42% at nutrition risk advanced colorectal cancer2 • 88% pancreatic cancer3 • 58% GI tumors4 • 45% of GI cancer patients were malnourished by Patient Generated –Subjective Global Assessment (PG-SGA)5 • 49% med oncology patients by PGSGA6 1. Bozzetti Supp Care Cancer 2012; 2. Thoresen Clin Nutr 2013; 3. La Torre J Surg Onc 2013; 4. Poziomyck Nutr Cancer 2012; 5. Dias do Prado 2013 6. Isenring Nutr Cancer 2010. Cancer Nutrition Therapy 9 GDS_80000_Title_v1 9 3 Malnutrition & Weight Loss • Oncology nutrition risk studies show: • 66% advanced H&N by >10% weight loss in 6 months; 26% had BMI <20 at 6 month1 • 32% of patients with GI cancer had mild to moderate and 16% had severe malnutrition by SGA2 1. Silander Laryngosope 2013; 2. Garth J Hum Nutr Diet 2010 Cancer Nutrition Therapy 10 GDS_80000_Title_v1 10 Malnutrition in the Adult Oncology Patient • Oncology nutrition risk studies show: • Pancreatic surgery patients • 88% medium-severe nutrition risk by Nutrition Risk Index (NRI) • 83% medium to high risk by Malnutrition Universal Screening Tool (MUST)1 • 35% of patients with lung cancer were malnourished by BMI < 18.5, weight loss > 10% or BMI <20 and weight loss > 5%2 • 25% of patients with gynecological cancer were malnourished by PG-SGA3 1. La Torre J Surg Onc 2013; 2. Percival Resp Med 2013; 3. Laky BMC Cancer 2010 Cancer Nutrition Therapy 11 GDS_80000_Title_v1 11 Causes of Malnutrition in Cancer Patients • Decreased dietary intake • Increased nutrient requirements • Impaired nutrient digestion / absorption • Increased losses of nutrients Cancer Nutrition Therapy 12 GDS_80000_Title_v1 12 4 Common Treatment-related Side Effects Negatively Impact Nutritional Status Symptom Chemo Radiation Surgery Weight loss Fatigue Nausea/Vomiting Taste alterations Oral mucositis Constipation * * Diarrhea Dry mouth Loss of appetite *Occurs as a result of pain medication. Cancer Nutrition Therapy 13 GDS_80000_Title_v1 13 Cancer Patients Often suffer from Multiple Side Effects that Impact Nutritional Status Medical Oncology Patients (N=191) Percentage of patients who are malnourished Number of Symptoms PG-SGA=Patient Generated-Subjective Global Assessment (Ottery 2000). 14 Isenring E, et al. Nutr Cancer. 2010;62(2):220-228. GDS_80000_Title_v1 Cancer Nutrition Therapy 14 Cancer Induced Weight Loss and the Tumor • Cancer induced weight loss has no direct relationship with the weight of the tumor, presence of metastases and its anatomic localization • Cancer induced weight loss can be present when the tumor weighs < than 0.01% of the host’s body weight • Bigger tumors might not cause cancer induced weight loss Tisdale MJ. Physiology 2005; 20:340-8. Cancer Nutrition Therapy 15 GDS_80000_Title_v1 15 5 Identification of Oncology Patients at Risk of Developing Malnutrition • Nutrition Screening tools identify patients at risk of developing cancer associated malnutrition and/or unintentional weight loss • Nutrition Screening Tools found to be valid and reliable for oncology patients – Outpatient: • Malnutrition Screening Tool • Patient Generated Subjective Global Assessment – In Patient: • f Add references Cancer Nutrition Therapy 16 GDS_80000_Title_v1 16 Quiz #1 Cancer Nutrition Therapy 17 GDS_80000_Title_v1 17 Quiz: which statement is not correct? • Consider weight loss and malnutrition in oncology patients: – Patients with cancer have greater rates of malnutrition than patients without cancer – Oncology patients rarely have weight loss prior to diagnosis – Malnutrition is the second most common diagnosis in patients with cancer – Patients with breast and prostate are less likely to experience weight loss Cancer Nutrition Therapy 18 GDS_80000_Title_v1 18 6 Quiz: which statement is not correct? • Consider weight loss and malnutrition in oncology patients: – Patients with cancer have greater rates of malnutrition than patients without cancer – Oncology patients rarely have weight loss prior to diagnosis – Malnutrition is the second most common diagnosis in patients with cancer – Patients with breast and prostate are less likely to experience weight loss Cancer Nutrition Therapy 19 GDS_80000_Title_v1 19 LEAN BODY MASS Cancer Nutrition Therapy 20 GDS_80000_Title_v1 20 Bed Rest, Age, and Disease Increase Loss of Muscle Loss of Lean Leg Mass (lbs) all measurements represent single leg loss Healthy Young (26-46 years of age) 28 Days’ Inactivity1 Elderly Inpatients (≥65 years of age) 3 Days’ Hospitalization3 0 –0.5 –1.0 Approx –1.5 1.0 lb –2.0 –2.5 1. 2. Healthy Older Adults (67 years of age) 10 Days’ Inactivity2 Approx 2.2 lbs Paddon-Jones D, et al. J Clin Endocrinol Metab. 2004 Kortebein P, et al. JAMA. 2007 3. Paddon-Jones D. Presented at: 110th Abbott Nutrition Research Conference; June 23-25, 2009; Columbus, OH. Cancer Nutrition Therapy 21 GDS_80000_Title_v1 Approx 2.2 lbs 21 7 Type of Weight Loss is Critical to Outcomes and Survival in Cancer Patients Malnutrition Weight Loss Muscle Mass Loss Muscle mass functions include: • Skin integrity • Immune function • Healing/Repair • GI integrity/Digestion 22 Wardlaw GM, Kessel M. Perspectives in Nutrition. 5th ed. New York, NY: McGraw-Hill; 2002. GDS_80000_Title_v1 Cancer Nutrition Therapy 22 Progressive Muscle Loss Can Be Associated with Severe Complications 23 Loss of Total Muscle Mass (%) Complications Associated Mortality (%) 10 Decreased immunity, increased infections 10 20 Decreased healing, weakness, infections 30 30 Too weak to sit, pressure ulcers, pneumonia, no healing 50 40 Death, usually from pneumonia 100 Demling RH. Eplasty. 2009;9:65-94. GDS_80000_Title_v1 Cancer Nutrition Therapy 23 Effects of Loss of LBM in Patients with Cancer • Low muscle mass is common and independent predictor of immobility and mortality 1 • Low muscle mass is an independent adverse prognostic indicator in obese patients 2 • Patients with sarcopenia seem prone to toxic effects during chemotherapy3,4,5 requiring dose reductions and treatment delays5 1. Prado, et al. Lancet Oncol. 2008;9:629-635. 2. Tan, et al. Clin Cancer Res 2009;15:6973-79. 3. Prado, et al. Curr Opino Support Palliat Care 2009;3:269-275. 4. Prado, et al. Clin Cancer Res 2007;13:3264-3268. 5. Prado, et al. Clin Cancer Res 2009;15:2920-2926. Cancer Nutrition Therapy 24 GDS_80000_Title_v1 24 8 Loss of Lean Body Mass • Patients with muscle mass loss have greater toxicity and shorter survival1 • Shortest survival times are among obese patients with sarcopenia2 • Median survival of patients with low muscle density was compared to high muscle density: – 14 vs. 20 months (p=0.001)2 1. Tan, et al. Clin Ca Res 2009;15:6973-6379. 2. Antoun, et al. Cancer 2013;19:3377-3384. Cancer Nutrition Therapy 25 GDS_80000_Title_v1 25 BMI is a False Indicator of Loss of Muscle Mass BMI LBM Cachectic 17 Equal Normal 25 Equal Obese 38 Equal One study found that 79% of patients identified as malnourished were normal weight, overweight, or obese.1 Image: Fearon et al., Nature 2013, 1. Davidson W, et al. Oncol Nurs Forum. 2012;39:E340-E345. 26 GDS_80000_Title_v1 26 Cancer Nutrition Therapy 26 Impact of Lean Body Mass • LBM determinant of epirubicin toxicity in pts with breast cancer1 – Same BSA but wide variation in LBM – Low LBM predicts toxicity p=0.002 – LBM positively correlated with neutropenia nadir r=0.05, p=0.023 Capecitabine Tx of metastatic breast cancer2 – Low LBM is determinant of CT toxicity and time to progression 1. Prado, et al. Cancer Chemother Pharmacol 2011;67:93-101 2. Prado, et al. Clin Cancer Res 2009;15:2920-26 Cancer Nutrition Therapy 27 GDS_80000_Title_v1 27 9 Impact of Lean Body Mass • Sorafenib’s common toxic effects limit patient’s ability to receive full-dose treatment and account for: – dose reductions in 13% of patients – treatment termination in 21% of patients • BMI < 25 kg/m2 with decreased muscle mass is a significant predictor of toxicity in metastatic RCC patients treated with sorafenib. Antoun S, et al. Annals of Oncology 2010 doi:10/1093/annoc/md605 Cancer Nutrition Therapy 28 GDS_80000_Title_v1 28 Impact of Lean Body Mass • Mayo Clinic regimen 5-FU/leucovorin CRC – 35% had toxicity resulting in dose reduction, Tx discontinuation, hosp, death – Dose based on Body Surface Area (BSA) – 20mg 5-FU/kg LBM cut point for developing toxicities p=0.005 – 56% had dose reductions or Tx delays – Toxicities febrile neutropenia, fatigue, diarrhea, N&V 5FU/BSA or 5FU/kg B Wt not predictive Prado, et al. Clin Cancer Research 2007;13:3264-68 Cancer Nutrition Therapy 29 GDS_80000_Title_v1 29 Chemotherapy, Toxicity and Malnutrition • Greater toxicity in patients with lower LBM but also in malnourished patients • N=100 patients • Malnutrition and hypoalbuminemia were associated with chemotherapy toxicity Cancer Nutrition Therapy 30 GDS_80000_Title_v1 30 10 Quiz # 2 Cancer Nutrition Therapy 31 GDS_80000_Title_v1 31 Quiz: which answer is not correct • Loss of lean body mass in oncology patients is associated with: – – – – Greater toxicities of chemotherapy Loss of strength, performance and activity Increased leg strength Poorer outcomes in obese patients Cancer Nutrition Therapy 32 GDS_80000_Title_v1 32 Quiz: which answer is not correct • Loss of lean body mass in oncology patients is associated withn: – – – – Greater toxicities of chemotherapy Loss of strength, performance and activity Increased leg strength Poorer outcomes in obese patients Cancer Nutrition Therapy 33 GDS_80000_Title_v1 33 11 Patient-centered outcomes Cancer Nutrition Therapy 34 GDS_80000_Title_v1 34 Nutrition awareness • Among medical practitioners, nutritional awareness is low – Not considered important by many medical practitioners – Little or no nutrition education in medical school – “I’ll cure the cancer and the nutrition problem will go away.” • Patients and families do worry • Use of herbs, supplements, potions, pills, devices, treatments is high Cancer Nutrition Therapy 35 GDS_80000_Title_v1 35 Awareness of Patient Reported Outcomes • In a recent prospective study in patients with NSCLC, survival was correlated with Patient Reported Outcomes.1 • How applicable are Patient Reported Outcomes for predicting quality of life in your practice? • 51% not or only slightly applicable2 1. Gralla, et al. J Clin Oncol 2013 2. NCCN Trends™ Highlights: Cancer Anorexia-Cachexia 6/19/2014 Cancer Nutrition Therapy 36 GDS_80000_Title_v1 36 12 Nutrition Intervention Improves Outcomes in CIWL • Nutritional status and intake are independent determinants of QoL as much as stage of disease, location of the cancer and treatment regimen in some types of cancer1 • Intensive nutrition therapy including ONS shown to improve2 – – – – – Body weight and LBM Hand grip strength Physical activity3 Performance status Dietary intake 6% 1% 10% 30% 3% Stage Location Intake Weight loss Duration Chemotherapy Surgery 30% 1. Ravasco P, et al. Supp Care Cancer 2004;12:246-2521 2. Von Meyenfeldt M, et al. Am Soc Clin Onc 2002 3. Moses A, et al. Br J Cancer 2004;90:996-1002 20% Cancer Nutrition Therapy 37 GDS_80000_Title_v1 37 Nutrition Intervention Can Help Improve Quality of Life 38 Baldwin C, et al. J Natl Cancer Inst. 2012;104(5):371-378. GDS_80000_Title_v1 Cancer Nutrition Therapy 38 SURVIVAL AND NUTRITION Cancer Nutrition Therapy 39 GDS_80000_Title_v1 39 13 Weight loss has a significant impact on survival Patients with pancreatic, gastric cancer and lung had the highest frequency of weight loss (83-87%) and tumor types less likely to produce weight loss breast, prostate, sarcoma. DeWys WD et al. Amer J Med 1980; 69: 491-497 Cancer Nutrition Therapy 40 GDS_80000_Title_v1 40 Weight Loss is Associated with Worse Outcomes 41 Cancer Nutrition Therapy Andreyev HJN, et al. Eur J Cancer. 1998;34(4):503-509. GDS_80000_Title_v1 41 Weight Loss Impacts Survival in Colorectal Cancer Results 100 Percentage 80 60 No Weight Loss (n=472) 40 Weight Loss (n=246) 20 P<.00001 0 0 1 2 3 4 5 Time Since Treatment (Years) Andreyev HJN, et al. Eur J Cancer. 1998;34(4):503-509. 42 GDS_80000_Title_v1 Cancer Nutrition Therapy 42 14 Nutrition Intervention in Weight Losing Patients Unresectable Pancreatic Cancer • Dietary counseling and Oral Nutrition Supplements over 8 weeks n=107 • Weight stabilization – Longer survival – Improved QoL (EORTC) • Improved dietary intake Davidson W, et al. Clin Nutr 2004;23:239-247 Cancer Nutrition Therapy 43 GDS_80000_Title_v1 43 Early Supportive Care in Patients with NSCLC Improves Survival • Early Supportive Care vs. Standard Care n=151 – Improved Quality of Life (p=0.04) – Longer survival 1.6 vs. 8.9 mos (p=0.02) Improved QoL (EORTC) Temel J, et al. N Eng J Med 2010;363:733-742 Cancer Nutrition Therapy 44 GDS_80000_Title_v1 44 Early Intervention for Cancer Cachexia • Early palliative care correlates with longer survival in patients with NSCLC.1 How early should an intervention start for cancer anorexia-cachexia? • (69%) With any weight loss or patients most likely at risk for developing weight loss.2 1. Temel, et al. N Engl J Med 2010;363:733-742. 2. NCCN Trends™ Highlights: Cancer Anorexia-Cachexia 6/19/2014 Cancer Nutrition Therapy 45 GDS_80000_Title_v1 45 15 NUTRITION INTERVENTIONS Cancer Nutrition Therapy 46 GDS_80000_Title_v1 46 Appropriate nutrition can support cancer treatment goals Goals of cancer treatment • Be effective • Be well tolerated • Minimize complications • Maximize quality of life • Allow for healing and recovery Levin RM. Oncology Issues. Nutrition: The 7th Vital Sign. November/December 2010:32-35. 47 accc-cancer.org/oncology_issues/articles/NovDec2010/ND10-Levin.pdf. Accessed March 26, 2012. GDS_80000_Title_v1 Cancer Nutrition Therapy 47 Early nutrition intervention has been shown to improve outcomes in cancer patients Nutrition intervention started as early as possible can result in: Nutritional status Performance status Quality of life (QOL) Response and tolerance to treatment Rate of complications Morbidity 48 Marín Caro MM, et al. Clin Nutr. 2007;26(3):289-301. GDS_80000_Title_v1 Cancer Nutrition Therapy 48 16 Patients Treated with a Nutrition Pathway Experienced Improved Outcomes and Treatment Tolerance1 Results Control Group Treatment Group (Nutrition Pathway) 33% 54% 0.05 Weight change during treatment (%) -8.9 ± 5.9% -4.2 ± 6.4% 0.003 Patients who had a chemotherapy dose reduction (%) 42% (n=10) 29% (n=7) 0.34 Patients who completed radiation (%) 50% (n=12) 92% (n=22) 0.001 33% 27% 0.71 Patients receiving enteral nutrition Patients who experienced radiation therapy breaks (for those who completed treatment) Patients who had an unplanned hospital admission (%) Total length of stay for all unplanned hospital admissions (days) 49 75% (n=18) 46% (n=11) 0.04 13.5 ± 14.1 days 3.2 ± 5.4 days 0.002 1. Odelli C et al. Clinical Oncology 2005; 17: 639-625. GDS_80000_Title_v1 P Value Cancer Nutrition Therapy 49 EXPERT GUIDELINES Cancer Nutrition Therapy 50 GDS_80000_Title_v1 50 Experts Have Recognized the Importance of Ongoing Nutrition Intervention in Oncology Patients The American College of Surgeons Commission on Cancer 2012 Cancer Survivorship Standards1 • Evaluation process starting in 2015 • “The cancer committee develops and implements a process to provide a comprehensive treatment summary and follow-up plan to patients who are completing treatment; the process is monitored, evaluated, and reported to the cancer committee each year.” • Continued care that considers the big picture: Cancer recurrence and… other chronic disease 51 1. American College of Surgeons Commission on Cancer. Cancer Program Standards 2012: Ensuring Patient Centered Care. Chicago, IL: American College of Surgeons. 2011. Cancer GDS_80000_Title_v1 Nutrition Therapy 51 17 Society Guidelines Support Proactive Nutrition Intervention Across the Cancer Continuum 1. American College of Surgeons Commission on Cancer. Cancer Program Standards 2012: Ensuring Patient Centered Care. Chicago, IL: American College of Surgeons; 2011. 2. McCallum PD. In: Elliott L, Molseed LL, Davis P, Grant B, (eds). The Clinical Guide to Oncology Nutrition. 2nd ed. Washington, DC: Oncology Nutrition Dietetic Practice Group, American Dietetic Association; 2006:44-53. 3. The Association of Community Cancer Centers Cancer Nutrition Services: A Practical Guide for Cancer Programs, 2012. Cancer Nutrition Therapy 52 GDS_80000_Title_v1 52 A Simple and Effective Plan to Ensure Consistency of Care “Nutritional care is a fundamental aspect of nursing practice and nurses are ideally placed to play an essential role in the early detection and screening of malnutrition in patients with cancer.”1 53 1. Davies M. Eur J Oncol Nurs. 2005;9(suppl 2):S64-S73. GDS_80000_Title_v1 Cancer Nutrition Therapy 53 Make Nutrition Part of Your Oncology Patient Care Plan • Early nutrition screening and intervention requires a multidisciplinary approach – Integrate into existing pathways or protocols, especially for highrisk cancers – DO NOT WAIT for serious nutrition concerns Cancer Nutrition Therapy 54 GDS_80000_Title_v1 54 18 What did she say? 1. Cancer induced weight loss results in: • • • 2. Type of weight loss is important • • 3. Decreased quality of life Increased complications Poorer response to therapy LBM is predominant type of tissue lost Over weight patients have greater LBM loss and poorer survival Nutritional impact of treatment-related side effects • • LBM loss contributes to greater treatment associated toxicities Dose reductions and treatment delays . Cancer Nutrition Therapy 55 GDS_80000_Title_v1 55 THANK YOU! QUESTIONS? Cancer Nutrition Therapy 56 GDS_80000_Title_v1 56 19






© Copyright 2026