
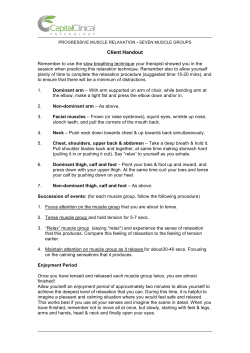
PRINTER EMULATOR FOR TESTING - The California State University
THE EFFECTS OF HAND POSITION ON MAXIMAL PERFORMANCE DURING ARM ERGOMETRY ____________ A Thesis Presented to the Faculty of California State University, Chico ____________ In Partial Fulfillment of the Requirements for the Degree Master of Arts in Kinesiology ____________ by Patrick William Cottini Spring 2012 DEDICATION I would like to dedicate my thesis to my parents, William & Constance Cottini. Without their support and perseverance to accomplish this goal in life, I cannot repay them enough. Throughout the many years that it has taken me to finish, and not without having many trials and tribulations, they stuck by my side no matter how I was feeling at anytime, they were always there! I would also like to dedicate this to my late service dog Olly. She also helped me in a large and small way by making sure I made it to the college on time by pulling me as fast as she could go. Sometimes this was not always a good thing, knowing when I needed her help without even asking her for it. I owe her my gratitude for not only performing an amazing service to me, but also being my best friend. You are missed Olly! iii ACKNOWLEDGEMENTS I would like to first acknowledge my thesis chair Dr. John Azevedo. Without his guidance, knowledge, time, effort, and dedication that he spends with graduate students and their thesis projects, I would have not been able to achieve this goal by finishing my thesis. I would also like to acknowledge my thesis committee Dr. Tom Fahey for always keeping a smile on my face no matter what the circumstance. Every time we would end a conversation he would say “Ok My Boy.” I will always remember that. To Dr. David Swanson, for always keeping me feeling that everything always had a way of working itself out. He would always make me feel important when I would stop by his office, he would acknowledge me by saying “Dr. Cottini.” I still do not know the reason, but I never questioned him because of the way it made me feel. I want to also give my thanks to a few of my fellow grad students Martin, for reminding me “it’s your thesis,” Carmen for helping me at stressful times, and Alesha for her guidance using the statistical computer software. Last but definitely not least, I would like to thank Josie Cline for her dedication to the Bewell program. Without it I would have not been strong and healthy mentally nor physically to get through my masters program! iv TABLE OF CONTENTS PAGE Dedication .................................................................................................................. iii Acknowledgements.................................................................................................... iv List of Tables ............................................................................................................. vii List of Figures ............................................................................................................ viii Abstract ...................................................................................................................... ix CHAPTER I. II. III. IV. Introduction................................................................................................. 1 Statement of the Problem................................................................... Operational Definitions...................................................................... Limitations ......................................................................................... Delimitations...................................................................................... Assumptions....................................................................................... 2 3 3 4 4 A Review of Literature ............................................................................... 5 Introduction........................................................................................ Summary ............................................................................................ 5 16 Methodology ............................................................................................... 17 Subjects .............................................................................................. Anthropometric Measurements.......................................................... Aerobic Capacity ............................................................................... Statistical Methods............................................................................. 19 20 20 21 Results and Discussion ............................................................................... 22 Discussion .......................................................................................... 30 v CHAPTER V. PAGE Summary, Conclusions, and Recommendations ....................................... 38 Summary ............................................................................................ Conclusions........................................................................................ Recommendations for Future Research ............................................. 38 38 38 References.................................................................................................................. 39 Appendices A. B. C. D. Informed Consent Letter ............................................................................. Medical and Exercise History..................................................................... Human Subjects Clearance Letter............................................................... Post Data Collection Questionnaire ............................................................ vi 48 52 55 56 LIST OF TABLES TABLE PAGE 1. Subjects Characteristics................................................................................... 19 2. Mean Data of Female and Male Subjects........................................................ 20 vii LIST OF FIGURES FIGURE PAGE 1. Maximal Power Output (Watts) for All 10 Subjects Across All Four Trials ................................................................................................. 23 2. Power Output Mean Results, Makes and Female Subjects in All Four Trials ................................................................................................. 23 3. Mean Ventilatory Response of All Subjects ................................................... 24 4. Maximum Ventilation Rate (L/Min) in Make and Female Subjects in All Four Trials....................................................................................... 24 5. Heart Rate Response in Males and Females ................................................... 25 6. Maximal Heart Rate for All Ten Subjects for All Four Trials ........................ 26 7. Response of Oxygen Consumption with Power Output.................................. 27 8. Absolute maximal oxygen consumption VO2max, (L/min) for all ten subjects in all four trails ................................................................. 28 9. Absolute Consumption (VO2max, L/min) in Male and Female Subjects for All Four Trails....................................................................... 28 10. Scaled Maximal Oxygen Consumption Per Kilogram Body Mass (VO2max, ml/kg min) of Male and Female Subjects Across All Four Trials ................................................................................................. 29 11. Scaled Maximal Oxygen Consumption Per Kilogram Lean Body Mass (VO2max, ml/kg min) of Male and Female Subjects Across All Four Trials............................................................................... 30 12. Mean of All Ten Subjects in All Four Trials of Maximal Oxygen Consumption Plotted As a Function of Maximal Power........................... 31 viii ABSTRACT THE EFFECTS OF HAND POSITION ON MAXIMAL PERFORMANCE DURING ARM ERGOMETRY by Patrick William Cottini Master of Arts in Kinesiology California State University, Chico Spring 2012 The purpose of this study was to find if hand position (pronated v. semivertical) and/or crank configuration (synchronized v. asynchronized) had any effect on maximal performance. The four trials investigated were synchronous prone (SP), synchronous vertical (SV), asynchronous prone (AP), asynchronous vertical (AV). To that end, maximal performance of 10 subjects was assessed in each of the four trials (in random order). Performance variables were maximal power output (POmax), ventilatory response (VEmax), oxygen consumption (VO2max), heart rate (HRmax), and respiratory exchange ratio (RERmax). No differences were observed across the four trials for all 10 subjects or when comparing the four trials for males only or females only. Males had significantly higher POmax, VEmax and VO2max than females. However, HRmax and RERmax were not ix different between males and females. Lastly, VO2max was highly dependent upon POmax. It may be concluded that hand position and crank configuration have no effect on maximal arm crank performance. x CHAPTER I INTRODUCTION Arm ergometry was first used during World War II for testing and training wounded soldiers (Vanlandewijck & Thompson, 2011). Today, arm ergometry and upper extremity training is popular for building cardiorespiratory fitness in individuals with disabilities who rely on their upper extremities for mobility. Upper body training for aerobic with arm ergometry, typically uses asynchronous, (ie, reciprocal) arm cranking (Mossberg, Willman, Crook, & Patak, 1999). The asynchronous crank movement in arm ergometry studies evolved from leg cycle ergometers placed on table tops. Synchronous arm cranking was first used in patients with ischemic heart disease (Shaw et al., 1974). Since the 1970’s, research has validated arm cranking exercise as a tool for fitness evaluation and cardiovascular conditioning (Casaburi, Barstow, Robinson, & Wasserman, 1992), particularly among individuals with disabilities with impaired lower mobility. Arm crank cycles evolved from the arm ergometers developed in the mid 1970’s. They are alternatives to wheelchair propulsion that can be enjoyed by recreationally active individuals and elite athletes. Currently, hand cycling is the world’s fastest growing wheelchair sport and recreational activity for people with lower limb disabilities (Goosey-Tolfrey, 2010). 1 2 A disparity exists between contemporary hand cycling designs and arm laboratory arm ergometers. The hand positions on hand cycles are more vertical than on arm ergometers which supinates the forearms. This recruits the brachioradialis muscle during elbow flexion, which increases force production. (Bressel, E., Bressel, M., Marquez, Heise, 2001). Laboratory arm ergometer design does not reflect changes in hand cycles. The typical laboratory arm-crank ergometer has an asynchronous crank arrangement. The hand holds are perpendicular to the crank, which puts the hands in complete pronation. This position does not allow the recruitment of the brachioradalis muscle, and thus reduces force production during elbow flexion (Bressel et al., 2001). To date, no studies have examined the effects of hand position on heart rate, oxygen consumption, and ventilation during synchronous and asynchronous arm ergometry. This study measured the effects of hand position during synchronous and asynchronous arm exercise on maximal oxygen consumption, maximal ventilation, maximal heart rate, and maximal respiratory exchange ratio. Statement of the Problem The purpose of this study was to assess the effects of hand and arm crank position during arm ergometry on maximal power output and cardiorespiratory responses. The investigation attempted to determine if hand position (pronated v. semi-vertical) and crank arm position (synchronous v. asynchronous) affected maximal performance as measured by maximal oxygen consumption (VO2max), maximal ventilation (VEmax), maximal respiratory exchange ratio (RERmax), maximal power output (POmax), and maximal heart rate (HRmax). 3 Operational Definitions The following operational definitions were used in this study: 1. AP – Asynchronized prone (crank style like on a bicycle, hands palm down on grips) 2. SP – Synchronized (both crank arms pedal together, hands palm down on grips) 3. AV – Asynchronized vertical (crank style like on a bicycle, hand position like shaking hands on grips) 4. SV– Asynchronized vertical (both crank arms pedal together, hand position like shaking hands on grips) 5. VE – ventilations measured in liters per minute 6. Power – work/time, measured in watts 7. VO2max – the highest level of oxygen consumption achieved graded arm exercise testing. 8. HR(bpm) – heart rate (beats per minute) 9. RER – respiratory gas exchange ratio; VCO2/VO2 10. Trials – each subject participated in 4 main trials (AP, SP, AV, SV) 11. BOD POD® - a device that measures body density Limitations Subjects used in this study were healthy able-bodied under-graduate college students. Subject size n=10 (female n=5, male n=5). Each subject participated in five trials. The first trial familiarized the subjects with the various arm ergometry techniques and allowed them exercise at various power outputs. The crank arms on the arm 4 ergometer had three positions to place the hand grips to vary crank arm length. In this study, the most distal position was utilized for all subjects. Subjects were volunteers with unknown levels of upper-body physical fitness or cardiovascular capacity. The study was limited by a small sample size. Delimitations The study was delimited to able-bodied undergraduate college students with no experience with hand cycling or arm ergometry. Able-bodied subjects were recruited to reduce bias from past experience with arm exercise and hand positions during hand cycling. All subjects were undergraduate Kinesiology majors. Assumptions The following assumptions were made during this study: 1. Subjects were able-bodied. 2. Self-reported levels of physical activity were accurate. (medical history form) 3. All subjects abstained from eating and drinking at least 9 hours prior to exercise trial. 4. All subjects abstained from vigorous exercising 24 hours prior to exercise trial. 5. All subjects worked to exhaustion during each trial. 6. All subjects were motivated to try their best during each trial. 7. All subjects had no prior experience using an arm ergometer. CHAPTER II A REVIEW OF THE LITERATURE Introduction Oxygen is a necessary requirement for life. It is critical for performance during aerobic exercise. Oxygen consumption is proportional to energy transformations during exercise, which determines maximal aerobic performance. Ventilation increases during exercise, which maintains an optimal diffusion gradient in the lungs for the movement of oxygen and carbon dioxide into and out of the blood. The exchange of gases takes place in the alveoli, small sacs where the diffusion of oxygen from air is transferred into pulmonary blood. Oxygen is mainly transported by red blood cells that contain hemoglobin, which carries the oxygen in the blood. The oxygenated blood is carried from the lungs to the heart, which pumps the blood from the left ventricle. The major arteries exiting the heart branch off into smaller arteries and arterioles and deliver blood to capillaries. The capillaries serve as conduits between the blood stream and cells that permit exchange of gases, substrates, and hormones. Oxygen enters the cells from the capillaries where it diffuses into mitochondria, participating in energy transformations reactions that produce adenosine triphosphate (ATP). Blood passes through the capillaries to the venules and veins, which transports the blood back to the heart and lungs. 5 6 Maximum oxygen uptake or aerobic capacity has been a focus of research since the 1920’s. English Nobel Laureate and physiologist Archibald V. Hill first presented the concept (Boone & Warpeha, 2003). He determined that oxygen consumption reached a ceiling at maximum exercise intensities. Defined Aerobic exercise consists of prolonged activity that, in general, uses large muscle groups such as cross-country skiing, cycling, running, aerobic exercise and swimming (Robergs & Roberts, 1997). Maximum oxygen uptake (VO2max) is defined as the highest rate that oxygen can be consumed during intense exercise (Bassett & Howley, 1997). Aerobic performance or oxygen consumption is defined as the product of cardiac output (Q) in liters per minute and arteriovenous oxygen difference ((a-v)O2). Arteriovenous oxygen difference is dependent upon muscle mitochondrial content (Bassett & Howley, 2000). Taken together, the above parameters make up the Fick relationship (VO2 = Q x (a-v)O2). Thus, the relationship between central (Q) and peripheral ((a-v)O2) factors contribute to oxygen consumption. Limitations of Maximal Oxygen Consumption Maximal oxygen consumption may be limited by any process involved in delivering oxygen from the atmosphere to mitochondria in cells. Limiting factors include pulmonary ventilation, pulmonary diffusion, ventilation-perfusion ratio, cardiac output, heart rate, stroke volume, blood volume, mitochondrial density, and cell capillary density. Oxygen consumption for able-bodied athletes increases with incremental aerobic exercise until maximum. According to classic studies by Hill (1923) oxygen consumption levels 7 off even in the face of increasing exercise intensities (Hill, 1923). During aerobic exercise when local fatigue occurs before central cardio respiratory fatigue, maximal oxygen uptake level is reached (VO2max), which representing maximum effort (Brooks, Fahey, & Baldwin, 2005). Past studies devoted to examining factors that limit maximum oxygen uptake usually focused on single factors to determine the upper limits of oxygen delivery and uptake. There are normally two categories, both have greatly increased our understanding of mammal respiratory systems: Oxygen flows through structures with O2 uptake by the mitochondria, and O2 delivery by circulation or O2 uptake by the lungs, which are relative resistance factors that can be estimated with the overall limit approximated. Central Limitations: Ventilation and Cardiac Output The central limitations to oxygen delivery are pulmonary diffusion, cardiac output and blood volume (Bassett & Howley, 1997). Cardiac output, the volume of blood pumped by each ventricle of the heart per minute, determines the volume of oxygen delivered to the cells their mitochondria. Ultimately, cardiac output determines the capacity to produce ATP. There is no pulmonary limitation to aerobic performance at sea level in people with normal lung function. Ventilation can be increased further after achieving maximal oxygen consumption. Also, oxygen partial pressure in the pulmonary vein is the same at rest and during maximal exercise. This shows a remarkable ability to deliver oxygenated blood to the blood from the lungs. 8 With reference to the present investigation, ventilation could be affected by crank configuration. It was demonstrated that synchronous cranking tended to produce higher ventilations during submaximal exercise. However this effect was observed only in able-bodied subjects (Mossberg et al., 1999). Thus it is predicted that enhanced ventilation may lead to higher oxygen consumptions in the synchronous crank configuration. Cardiac output is the product of heart rate and stroke volume. It is commonly identified as the principle limiting factors of oxygen delivery and VO2max (Bassett & Howley, 2000). Some researchers have suggested that cardiac output accounts for 7085% of the limitations in VO2max (Cerretelli & DiPrampero, 1987). This was elegantly shown by Ekblom, Goldbarg, and Gullbring (1972) who artificially increased cardiac output by increasing the oxygen carrying capacity of blood. They withdrew and stored two units (800 mL) of blood and then reinfused it one month later. This was equivalent to increasing maximal cardiac output by nearly 20 percent. Subjects experienced substantial increases in maximal oxygen consumption and endurance. “Blood doping,” as it came to be called, is a banned procedure by the International Olympic Committee because of its effects on performance. Peripheral Limitations (Tissue Extraction of Oxygen Exercising muscles have an increased ability to extract and use oxygen that is transported to it by the cardio respiratory system. Exercise scientists call this the peripheral component of VO2max (Robergs & Roberts, 1997). Potential sites for VO2max limitation in the peripheral component include muscle diffusion capacity, mitochondrial 9 enzyme levels (molecules that facilitate ATP production in mitochondria), capillary density, cardiac output, hemoglobin concentration, and transport of oxygen between blood, the muscle microcirculation, and mitochondria. Oxygen Transport Across Cell Membranes An oxygen pressure gradient (difference) exists between the blood and muscle cells which also allow the transportation of oxygen from the red blood cells into the mitochondria via diffusion (Kravitz, & Dalleck, 2002). Factors such as capillary density and diffusion distance could limit oxygen transport. Muscle Mitochondrial Content Mitochondrial respiration relies on an adequate supply of oxygen. Aerobic training increases mitochondrial enzymes levels, allowing working muscles to use more oxygen. This results in a higher VO2max. It appears that peripheral factors present a potent peripheral limitation to VO2max (Honig, Connett, & Gayeski, 1992). A 20% increase in capillary density has been reported with aerobic training, indicating improved distribution and extraction of blood within the muscle (Robergs & Roberts, 1997). An early study of muscle properties including VO2max indicated that mitochondrial volume density, was proportional to VO2max from sedentary individuals to athletes (Hoppeler, Lothi, Claassen, Weibel, & Howald, 1973). Later studies appear to contradict this proportionality showing a 40% increase in quadriceps with exercise training but only a 15% increase in whole body VO2max (Hoppeler et al., 1985). Davies and colleagues showed that mitochondrial mass was highly related to endurance capacity—much more so than maximal oxygen consumption (Davies, Packer, & Brooks, 1981). 10 Heart Rate Response to Arm Exercise It has been demonstrated that arm exercise elicits a greater heart rate response than leg exercise (Mukherjee & Samanta, 2000; Powers & Howley, 2009). This is likely due to a greater catecholamine response, both sympathetic as well as adrenal response during arm exercise. The heart rate and oxygen consumption response to exercise varies with the activity and active muscle mass. For example Kimura, Yeater, & Martin (1990) reported that during five experimental exercises (tethered swimming, simulated swimming, arm cranking, treadmill running, and cycling) the mean maximal heart rate (HRmax) at VO2max ranged from 182 beats per min (arm cranking) to 202 beats per min (running and cycling). Results showed no apparent differences in HR max attained in any of the tests. There was a significant difference for the mean absolute (l/min) and scaled (ml/kg min) for VO2max for all tests. VO2max (ml/kg min) was lower during arm exercise and swimming than running or cycling (Kimura et al., 1990). Critical Muscle Mass (leg vs. leg + arm cycling) Several studies have compared arm exercise to leg and arm + leg exercise. Making the comparisons between arm exercise, leg exercise and arm + leg exercise provides unique opportunities to examine limitations of maximal oxygen consumption as a function of muscle mass and the volume of blood flow to support exercising limbs of different masses. Gross mechanical efficiency to arm and leg as well as arm + leg ergometry was evaluated by Eston & Brodie (1986). Efficiency was significantly lower during arm work compared to leg work or combined. Further, ventilatory response was 11 higher during arm exercise compared to leg exercise (Eston & Brodie, 1986). Eston and Brodie (1996) hypothesized that delivery of oxygenated blood to smaller upper body muscle masses is adequate to perform arm exercise. However, lower limbs have larger muscle mass that need to be supplied with oxygenated blood, thus in larger muscle masses, distribution of blood supply, and therefore oxygen supply, appears to limit oxygen consumption (Eston & Brodie, 1986). Secher, Niels, Ruberg-Larsen, Binkhorst, Bonde-Petersen (1974) assessed VO2max during arm exercise, leg exercise and arm + leg exercise. They found that the addition of arm exercise to leg exercise increased whole body VO2max suggesting that the addition of arm exercise to leg exercise added critical muscle mass to total exercising muscle resulting in a redistribution of blood flow as well as increasing active tissue beds. Taken together, the results cited above underscore the reliance on whole-body oxygen consumption on a variety of factors, namely blood flow, active muscle mass and muscle mitochondrial content. Power Output In an attempt to determine how additional exercising muscle mass may contribute to increasing VO2max, Secher et al. (1974) also assessed power outputs in the various exercise modalities as outlined above. Adding arm exercise to leg exercise yielded increased power outputs compared to leg exercise alone. Interestingly, the authors determined that arms accounted for 27% of total power during arm + leg exercise; however when the arms were exercising alone they generated 42% of the total power that legs were able to generate. The fact that arms alone could generate almost half the power of legs, but contribute only approximately one fourth (1/4th) of the power 12 during arm + leg exercise indicate a high level of cardiorespiratory and metabolic control over total exercising muscle mass. In other words, the body has to decide how to distribute its resources. Oxygen Consumption During Arm, Leg and Arm + Leg Exercise Previous studies have suggested that arm position could have an effect on cardiovascular and metabolic adjustment to arm cycling. For example, Cummins and Gladden (1983) examined heart rate during submaximal and maximal arm cycling with arm positions at three different levels in relationship to the heart. Results indicated no difference between arm exercise with arms positioned below, at or above the level of the heart suggesting that the body is able to direct blood flow as needed regardless of the position of the exercising limbs relative to the heart. Contrary to the results cited above, it has been demonstrated that crank (arm) position relative to the heart has an effect on the VO2 response to the onset of exercise (Cerretelli, Pendergast, Paganelli, and Rennie, 1979). Cerretelli et al. found that when crank above the heart there was an increased rate of rise of VO2 at the onset of exercise compared to an upright position (crank at heart level) (Cerretelli et al., 1979). These differences may have been caused by the increased vertical distance between the exercising muscles and heart in the supine position. As a result, there were similar differences between the heart and exercising muscles when the arms were placed in various positions. 13 Muscle Recruitment as a Function of Hand Position While Arm Cranking Several upper body muscle groups are used during arm ergometry. In addition, there are several smaller muscles in the shoulder and forearm that are crucial to maximize arm crank performance. For example, Bressel et al. (2001) investigated the effects of handgrip position during arm cranking exercise. They examined five different muscles (biceps brachii (BB), lateral head of triceps brachii (TB), middle deltoid (DT), infraspinatus (IS), and brachioradialis (BR) in the arm and measured the recruitment using an EMG. They measured three different handgrip positions pronate, neutral, and supinate. Brachioradialis muscle recruitment was 64% and 73% greater during the neutral hand position than the supinated or pronated handgrip positions. There were no differences between hand position in the four other muscle groups. Other exercise modalities utilize upper body (arm) exercise. For example, rowing engages muscles in the torso, back, arms and legs, thus crew athletes (rowing exercise) can provide insight as to how the human body distributes resources (e.g., blood flow distribution) during exercise to maximize power output. With an increase in interest in rowing exercise, there have been developments in ergometers to mimic rowing. It has been shown that differences during maximum exercise between rowing ergometry and on water rowing are minimal (Vogler, Rice, & Gore, 2010). However, the data must be carefully interpreted as maximal data were not normalized for power output during the on-water exercise trial as it is technically difficult to quantify power output while rowing in a rowing scull. Further, individuals tested found it difficult to reach their true maximum during OW testing because of the technical aspects of on-water sculling 14 compared to ergometer rowing (Vogler, Rice, & Gore, 2010). The data cited above demonstrates an additional example of arm-based exercise, but also allows investigators to explore limitations of performance providing limbs could be isolated (e.g. arm only exercise v. leg only exercise v. arm + leg exercise) again with the emphasis on how the human body regulates the distribution of resources. Three Wheel Crank Chair The specific purpose of the present study was to assess physiological responses as a function of different hand positions and crank configurations in handcycling type exercise. The first hand cycle was simply a wheelchair converted to use a bicycle crank mechanism on a third wheel for propulsion. It was called the armpropelled three-wheeled chair (APTWC). Not surprisingly, heart rate response was similar to what is observed in able-bodied individuals (i.e., heart rate increases as speed of locomotion increases). Further, Mukherjee and Samanta (2000) found that arm cranking was more efficient than standard wheelchair propulsion. That is, subjects could go faster using arm cranking compared to standard wheelchair propulsion at the same metabolic cost. Conversely, at any given speed of propulsion, the metabolic cost of propulsion (locomotion) is lower while utilizing arm cranking as opposed to standard wheelchair propulsion. Based on the above data, Mukherjee and Samanta (2000) developed the physiological cost index (PCI). These authors utilized PCI as a means to quantify physiological strain as a function of mode of propulsion. Lastly, Mukherjee & Samanta (2000) found that PCI was lowest at a moderate speed of propulsion. In other words, at slow propulsion speeds, the PCI is greater than at moderate propulsion speeds. Further, as expected, PCI increase with increasing 15 propulsion speeds. The PCI curve forms a “U”-shaped curve similar to the energetic cost of locomotion observed while walking at different speeds when energetic cost of locomotion is scaled according to distance traveled (Willis, Ganley & Herman, 2005). Taken together, the data above indicate that the body self-selects to minimize the cost of locomotion (or maximize economy) regardless of mode of locomotion. Comparison of Synchronous v. Asynchronous Arm Cranking Several studies compared the differences between synchronous and asynchronous cranking. Mossberg et al. (1999) found that there were significant differences between the two crank configurations, with synchronous crank configuration resulting in a higher oxygen output. Contrary to the above findings, it has also been shown that oxygen consumption was greater during asynchronous arm cranking than synchronous arm cranking (Dallmeijer, Ottjes, De Waardt & van der Woude, 2004). When assessing maximal power output, it was found that synchronous crank configuration yielded significantly higher maximum power compared to the asynchronous crank configuration (Abel, Rojas-Vega, Bleicher, & Platen, 2003). We can infer from these data that crank configuration affects oxygen consumption as well as power output. Hand Position (Prone v. Vertical) Hand grip position has been shown to influence muscle recruitment during arm crank exercise. Bressel et al. (2001) reported that the brachioradialis muscle was recruited to a greater extent when the hands of subjects were in a neutral or vertical position as opposed to the horizontal or prone position while arm cranking. These 16 findings suggest that arm cranking using the neutral, or vertical, hand position may result in greater maximal power output and oxygen consumption by virtue of the availability of the brachioradialis muscle to be recruited during arm cranking exercise. Summary Oxygen is a requirement for all life and directly relates to aerobic exercise when using a arm crank ergometer. The oxygen delivery system and the process used to measure VO2max through rigorous exercise are key factors in determining an individual’s maximum effort. Though there are numerous limiting factors, the primary one is matching the rate muscles consume oxygen with the rate oxygenated blood can be delivered. When comparing arm and leg exercises results were parallel, indicating exercise intensity were similar. Hand grip position in the neutral position displayed greater muscle activity versus pronation hand grip. The use and development of the arm ergometer has helped evolve into the arm propelled three wheeled chairs that was a key factor in what is known today as the handcycle. CHAPTER III METHODOLOGY The Human Subject Review board at California State University, Chico approved this study. All subjects signed an informed consent and a medical history form before participating in the study. The subject’s rights and confidentiality procedure were explained before and during the trials. Each trial was in accordance to the approved protocol. The purpose of this study was to assess the effects of hand and arm crank position on maximal performance. The crank arms of hand cycles are synchronous as opposed to asynchronous cranks used on bicycles. Further, the hand position on hand cycles is "semi-vertical" (~75 degree angle). However the laboratory/rehabilitation equipment designed to test metabolic and cardiovascular responses to arm exercise use asynchronous crank arms with the hands in a horizontal or pronated position. This investigation sought to determine the effects of hand position (pronated v. semi-vertical) and crank arm position (synchronous v. asynchronous) on maximal oxygen consumption (VO2max), maximal ventilation (Vemax), maximal respiratory exchange ratio (RERmax), maximal power output (POmax), and maximal heart rate (HRmax). Subjects visited the laboratory on five occasions. The first visit was to familiarize the subjects to arm ergometry and upper body exercise. All subjects completed the orientation session in order to familiarize themselves with the test procedures and instrumentation. The remaining four visits were to assess the effects of crank configuration and hand position. 17 18 During each session there was constant supervision to observe exercise tolerance and to terminate the tests when subjects could not sustain a cadence of 70 rpm. After informed consent is obtained, subjects reported to the human performance lab (HPL) between 0700 and 1000 after an overnight fast. Able-body rather than disabled people were used as subjects to avoid bias impose by previous hand cycling experience. An arm crank ergometer (Monark, 881E) which allows for adjustment of the crank arms to the synchronous or asynchronous positions as well as separate hand holds to allow for the prone and vertical hand positions mounted to an adjustable table and a upright chair that is also adjustable to accommodate different arm lengths. Subjects were seated in front of the ergometer (with the center of arm crank level with top of armpit (Van Drongelen, Maas, Scheel-Sailer, & van der Woude, 2009). They wore a wide elastic belt around the abdominal region for upper body stabilization and to prevent excess recruitment of other muscle groups such as abdominal muscles and hip flexors. The feet were suspended in straps so that their knees were extended and their hips flexed (sitting with legs straight out). This was done so that subjects were not able to use their legs to assist in exercise performance. Subjects were requested to maintain the arm crank cadence at 70 RPM throughout the test (a metronome helped pace the cadence). Resistance of the arm ergometer was increased 10 watts every two minutes until subject could no longer maintain the cadence. VO2, VE, and RER were measured continuously by a metabolic cart (Parvomedics, TrueMax 2400) approximately every 10-second heart rate was obtained from a Polar heart rate monitor and recorded during each two-minute exercise stage. 19 Subjects Ten ambulatory subjects volunteered to participate in this study. All subjects met the recommended ACSM guidelines for physical exercise, exercising at least one to two hours a day, three days per week. Subjects were within a normal, healthy weight range. None of the subjects had any adverse health conditions that would prevent them from completing the four trials. Characteristics of all 10 subjects are shown in Table 1. It was noted that there were clear differences between male and female subjects upon examination of several of the physiological parameters. Thus, mean subject characteristic data for males and females are shown in Table 2. Table 1 Subject Characteristics Subject Sex Age (yrs) 1 F 21 67 56.2 23.7 42.9 2 F 20 69 50.1 24.4 37.8 3 M 21 69 70.9 14.2 60.8 4 M 30 73 89.1 29.0 63.3 5 F 20 67 64.5 26.0 47.7 6 M 23 70 69.4 9.8 62.6 7 M 21 71 69.2 11.1 61.5 8 F 19 61 53.1 24.5 40.1 9 F 24 74 87.5 27.0 63.9 10 M 23 68 68.3 20.4 54.4 MEAN 22.2 ± 3.0 Height (in) 68.9 ± 3.4 Weight (kg) 67.8 ± 12.4 Body fat % 21.0 ± 6.5 LBM (kg) 53.5 ± 9.9 20 Table 2 Mean Data of Female and Male Subjects Age (yrs) Height (in) Weight (kg) Body Fat (%) LBM (kg) Females 20.8±1.7 67.6±4.2 62.3±13.5 25.1±1.2 46.5±9.3 Males 23.6±3.3 70.2±1.7 73.4±7.9 16.9±7.1 60.5±3.2 Undergraduate college students were recruited. Informed consent was obtained from all subjects in accordance with the established human subjects’ protocol at California State University, Chico (Appendix A). Anthropometric Measurements Body composition was obtained using a BOD POD®. Weight was measured to the nearest kilogram using a load cell on-line with the BOD POD®. Height was selfreported. Aerobic Capacity Maximum oxygen uptake (VO2max), maximal ventilation (VEmax), maximal power output (POmax), maximal respiratory exchange ratio (RERmax), and maximal heart rate (HRmax) were all assessed during graded exercise tests to volitional fatigue using an arm crank ergometer (Monark 881E, Sweden) in four separate trials. The four trials, carried out in random order, were asynchronous vertical (AV), asynchronous prone (AP), synchronous vertical (SV) and synchronous prone (SP). The arm ergometer was adjusted specifically to each subject. The crank axis was set to the height of the top of the 21 subjects’ arm pits with arm extended straight out with a 15 to 30 degree bend in elbows. Subjects were seated with legs extended and suspended using a strap with loops at both ends and one around their waist and back of chair to minimize lower body support as well as trunk movement. While subjects were seated, an abdominal strap a heart monitor sensor was located on their chest just below the zyphoid process. Subjects were seated three minutes to obtain resting values for VO2 and HR (VO2rest and HRrest). After the initial three minutes, the subjects cranked at one of four trials at a cadence of 70 rpm and the power output started at 10 watts and increased 10 watts every two minutes. Statistical Methods Two factor ANOVA with repeated measures to determine differences between treatments with the second factor to determine differences between males and females. Statistical analysis was not performed on any of the “response” or time-course data (i.e. VE, HR and VO2 response curves) as the focus of the study was to evaluate maximal data only. Significance was set at p < 0.05. CHAPTER IV RESULTS AND DISCUSSION The maximal PO(watts), VO2(L/min), VE (L/min), RER(VCO2/VO2), and HR(bpm) were achieved during the progressive arm crank ergometer test ranging between 50 and 150 watts. Overall no differences were observed across the four trials for all 10 subjects or when comparing the four trials for males only or females only. Maximal power outputs were 89, 88, 95 and 97 watts for SP, SV, AP and AV trials respectively (Figure 1). There were no differences across trials in maximal power output. However, males produced almost twice the maximal power output than females (Figure 2). When maximal power outputs were subdivided by sex there was clear dichotomy between males and females (p < 0.001). Maximal power output in males was 118, 112, 124 and 128 watts in SP, SV, AP and AV, respectively while in females it was 60, 64, 66 and 60 watts in SP, SV, AP and AV, respectively (Figure 2). Ventilatory response to incremental exercise was curvilinear across all four trials for all subjects (Figure 3). Maximal ventilation in females was not statistically different across the four trials (Figure 4). However maximal ventilation rate was nearly twice as great in men than in women (p < 0.001), though as in female subjects, there was no difference in maximal ventilation rate observed in males (Figure 4). 22 23 Figure 1. Maximal power output (watts) for all 10 subjects across all four trials. Values are means ± SE. No statistical difference existed between trials. * * * Figure 2. Power output mean results, males and female subjects in all four trials. Values are means ± SE. * p < 0.001 between males and females. * 24 Figure 3. Mean ventilatory response of all subjects. Data are means of four trials for males and means of four trials for females. * * * * Figure 4. Maximum ventilation rate (L/min) in male and female subjects in all four trials. Values are means ± SE. * p < 0.001 between males and females. 25 Heart rate increased more rapidly in females than males (Figure 5). That is, at any given power output heart rates in females are higher than in males. This is consistent with the concept that females tend to have smaller hearts. Thus to maintain cardiac output and oxygen delivery, heart rates must be higher to compensate for the smaller stroke volumes (cardiac output = heart rate x stroke volume, Q = HR x SV). Maximal heart rates (HRmax) were approximately 174 bpm across all four trials. No significant differences were observed across the four trials, further there were no differences in maximal heart rates between males and females for any of the trials thus there was no need to divide the data by sex as with ventilation (Figure 6). Figure 5. Heart rate response in males and females. Data are means of four trials for males and means of four trials for females. Oxygen consumption increased linearly with power output in all four trials (Figure 7). Because there were no differences in oxygen consumption 26 Figure 6. Maximal heart rate for all ten subjects for all four trials. Values are means ± SE. There were no statistical differences between males and females, therefore grouped data are presented. either between trials or between males and females, VO2 response is plotted as the mean of four trials for all 10 subjects. Oxygen consumption was about 0.25 L/min at rest for all four trials and increased to about 2.5 L/min. It must be noted that the data up to about 60 to 80 watts represent all ten subjects while above 80 watts only males are represented as the female subjects could not maintain power outputs above 80 watts. The data from 120 watts up to 150 watts represents fewer and fewer subjects as each subject could attain his respective maximal capacity. Absolute maximal oxygen consumption was not statistically different across the four trials. It was 1.6, 1.6, 1.7 and 1.6 L/min in SP, SV, AP and AV trials, respectively (Figure 8). The same pattern observed between males and females with POmax was also observed with VO2max (p < 0.001, Figure 9). Maximal oxygen consumption in males was 2.1, 2.1, 2.2 and 2.2 L/min in SP, 27 Figure 7. Response of oxygen consumption with power output. Data are means of all ten subjects for all four trials. No difference existed in oxygen consumption between subjects up to each subject’s maximal oxygen consumption thus data are grouped. SV, AP and AV trials, respectively (Figure 7) while VO2max in females was 1.1, 1.1, 1.2 and 1.1 L/min in SP, SV, AP and AV trials, respectively (Figure 9). Scaling VO2max to body weight reduced the difference between males and females, however scaled VO2max in males was still significantly greater than in females (p < 0.01). However no differences existed across trials in either males or females (Figure 10). Scaled VO2max values were 27.3, 29.0, 30.9 and 31.5 ml/kg min in SP, SV, AP and AV trials, respectively in males while scaled VO2max values were 18.0, 18.0, 19.7 and 17.6 ml/kg min in SP, SV, AP and AV trials, respectively in females (Figure 10). 28 Figure 8. Absolute maximal oxygen consumption VO2max (L/min) for all ten subjects in all four trails. Values are means ± SE. Figure 9. Absolute maximal oxygen consumption (VO2max, L/min) in male and female subjects for all four trials. Values are means ± SE. * p < 0.001 between males and females. 29 Figure 10. Scaled maximal oxygen consumption per kilogram body mass (VO2max, ml/kg min) of male and female subjects across all four trials. Values are means ± SE. * p < 0.01 between males and females. Scaling VO2max per kilogram lean body mass (LBM) further closed the gap between males and females (p < 0.01, Figure 11). Scaled VO2max per kg LBM was 34.4, 34.8, 36.6 and 36.5 ml/kg LBM min in SP, SV, AP and AV trials, respectively in males while in females it was 24.1, 24.0, 26.3 and 23.4 ml/kg LBM min in SP, SV, AP and AV trials, respectively (Figure 11). Respiratory exchange ratio increased more rapidly in females than in males, similar to the VO2 response (data not shown). However, maximal respiratory exchange ratios (RER) were not different between trials or due to sex. Maximal RER values were 1.05, 1.04, 1.02 and 1.05 in SP, SV AP and AV trials, respectively. The lack of difference in maximal RER values indicates that gross fuel utilization was not different between sexes or due to hand position or crank configuration. 30 Figure 11. Scaled maximal oxygen consumption per kilogram lean body mass (VO2max, ml/kg min) of male and female subjects across all four trials. Values are means ± SE. * p < 0.01. Because of the disparity between males and females with observed POmax and VO2max the data from all four trials for each subject were averaged then plotted to evaluate the relationship between maximal oxygen consumption and maximal power output. There was a very strong (r2 = 0.96) relationship between maximal power output and VO2max (Figure 12). This relationship addresses the importance of power output on oxygen consumption. Discussion This study examined the effect of crank configuration and hand position during arm ergometry on maximal power output and maximal oxygen consumption. Previous studies comparing asynchronous and synchronous, crank configuration found conflicting results and few studies addressed the effects of hand position. However, through an extensive literature review, there were no 31 Figure 12. Mean of all ten subjects in all four trials of maximal oxygen consumption plotted as a function of maximal power. Each point was generated as a mean of maximal power output for all four trials for both VO2max and POmax for each subject. studies comparing physiological response to the interaction of hand position and crank configuration. The study compared synchronous and asynchronous cranking and prone and vertical hand positions. Measurements included maximal oxygen consumption (VO2max), power output, and heart rate. The study did not measure pulmonary diffusion, ventilation perfusion ratio, cardiac output, heart rate, stroke volume, mitochondrial density, and cell capillary density. The cardiorespiratory system provides the necessary oxygen to the upper body muscles to perform arm exercise, which is noted as the peripheral component of VO2max (Robergs & Roberts, 1997). Oxygen is then transported by red blood cells to the mitochondria via diffusion (Kravitz & Dalleck, 1984). A greater mitochondrial 32 content allows working muscles to use more oxygen which results in higher VO2max levels. Muscle groups that are recruited during arm ergometry/hand cycling, consist of the major upper body muscles such as shoulder, upper and lower arm, latissimus dorsi, rhomboids, trapezius, all of the neck muscles. The chest and abdominal muscle groups are also recruited, provided they are fully innervated. In light of previous work evaluating muscle recruitment patterns using various hand positions while performing arm-crank ergometry, it might have been anticipated that the neutral, or vertical, hand position, regardless of crank configuration may have elucidated higher VO2max values. If functional, this would be due to the finding by Bressel et al. (2001) that the vertical hand position allows for the recruitment of the brachioradialis muscles during from approximately 120 degrees of crank angle to approximately 260 degrees of crank angle, i.e. when the elbows are going through the flexion phase of the cranking cycle. However the present study did not find any differences in maximal oxygen consumption or maximal power output as a function of hand position. This might be attributed to the fact that the brachioradialis is relatively small thus does not represent a significant addition to working muscle mass during arm crank ergometry. This may have several effects on the observed, or lack thereof, physiological responses in the present study. Firstly the additional working muscle of the brachioradialis would not likely place a burden on the cardiovascular system. Though not measured, the increased blood flow required by the recruitment of the brachioradialis muscle would not tax the cardiovascular 33 system as is observed when comparing leg exercise with arm plus leg exercise. The vascular system is able to distribute blood flow to very large muscle masses when arms and legs are exercising simultaneously. A more likely explanation for the lack of any observed change in maximal, or peak, oxygen consumption is more likely due to the fact that the bulk of elbow flexion is more likely attributed to the biceps brachii muscles. However, more importantly, the majority of force generation during arm crank ergometry is during the extension portion of the cranking cycle of each arm. Thus to summarize, it is not that the brachioradialis muscle is not recruited during arm cranking while the hands are in the vertical position, it most certainly is, but it simply does not add a significant mass of muscle to the overall working muscle of the arms during arm cranking. Additionally most force generation during arm cranking is during the extension portion of arm cranking (Bressel et al., 2001). In addition to any difference as a function of hand position in either the synchronous as well as asynchronous crank configuration, no differences were observed as a function of crank configuration. This is consistent with previous findings in which not only is there no difference in oxygen consumption as a function of synchronous and asynchronous crank configuration, there is also no difference between paraplegic and able-bodied subjects (Mossberg et al., 1999). The lack of difference between synchronous and asynchronous crank configurations might have been unexpected in both the previous research as well as the present study. It might have been predicted that the asynchronous crank 34 configuration would yield higher oxygen consumptions because of the reciprocal motion and therefore muscle recruitment patterns that are necessary for the asynchronous crank configuration (Bafghi, Abbasi, De Haan, Horstman, & van der Woude, 2007). While one half of the torso and the associated arms are contributing to extension movements, the opposite side of the torso and its associated arm is contributing to flexion motions. The most basic motions in life are reciprocal, walking, swimming, climbing stairs. Thus in arm cranking it might have been predicted that by virtue of motor control, subjects might reach higher power outputs and therefore higher maximal oxygen consumption. Additionally simultaneous extension and flexion motions may lead to the use of the trunk to aid in the force generation. Indeed this was observed in some subjects, however similar to the lack of muscle mass of the brachioradialis muscle adding to overall power output as well as oxygen consumption. Perhaps total trunk muscle mass recruited during synchronous arm cranking is comparable to total muscle mass recruited during asynchronous arm cranking. It must be noted that muscle recruitment patterns were not measured in the present study, thus any conclusions about recruitment patterns and magnitude between synchronous and asynchronous arm cranking are purely speculative. Further, the present study attempted to restrict trunk movement by utilizing a wide elastic belt that was strapped around each subject for each trial. The belt restricted, but did not completely eliminate, the ability of subjects to perform trunk flexion. Given this restriction of trunk flexion, this might have contributed to greater maximal power output as well as maximal oxygen 35 consumption values during the asynchronous trials as the belt was not able to restrict rotational motion of the trunk while exercising. This became especially apparent during the higher power outputs. Each subject utilized an exaggerated amount trunk rotation to generate force during the higher power outputs regardless of hand position. Additionally, while the abdominal strap did assist to restrict trunk motion, it did not completely eliminate it. Indeed subjects were observed incorporating a substantial amount of trunk flexion while performing the synchronous trials, again, regardless of hand position. Also significant to the present study are the findings of Mossberg et al. (1999), that there are no differences in the metabolic response between paraplegic and able-bodied subjects. Paraplegia, by definition is, paralysis characterized by motor or sensory loss in the lower limbs and trunk after a thoracic spinal cord injuries. The recruitment of arm as well as trunk muscles are not affected in paraplegic subjects compared to able-bodied subjects. Thus in the present study, the utilization of able-bodied subjects would have direct application to the paraplegic population. Additionally, because most able-bodied subjects do not engage in arm-based exercise (with the exception of swimmers) they would not have a pre-determined bias of synchronous as opposed to asynchronous arm cranking whereas experienced hand-cyclists may have a bias toward synchronous arm cranking as most hand cycles are set up in a synchronous manner. The present study found that maximal oxygen consumption is highly related to maximal power output (Figure 12). These data illustrate important 36 issues in maximal performance. Classically, aerobic performance was thought to be the major predictor of athletic performance (Fitchett, 1985) as the focus of exercise physiology focused on endurance type exercise. However recently, it has been shown that even in a classically categorized activity, the five thousand meter run that increasing power was able to increase performance in the form of decreasing run times (Pollock, Mengelkoch, Graves, Lowenthal, Limacher, Foster, & Wilmore, 1997). This occurred in the face of decreasing VO2max values. Thus an event that lasts 12 to 14 minutes can be positively affected with power training. Further, that aerobic capacity is not the limiting factor in athletic performance in the five thousand meter run, again a classically identified aerobic activity (Pollock et al., 1997). The present study showed a very strong relationship between maximal power output and maximal oxygen consumption (Figure12). Further, there is a clear dichotomy between subjects. The lower cluster of data points in Figure 12 are females while the upper cluster of data points are the males. Further, two of the males were swimmers, one being a “pure” swimmer while the other being a water polo player. Both exhibited superior upper body power as well as maximal oxygen consumption. The swimmer reached the highest power output as well as maximal oxygen consumption while the water polo player reached the second highest power and maximal oxygen consumption of all subjects. The findings of the present study are in agreement with the findings of (Reybrouck, Heigenhauser, & Faulkner, 1975) who studied arm v. leg v. arm + leg exercise with regard to recruitment of greater muscle mass leads greater 37 maximal oxygen uptake values. Firstly, in general, and in the present study, males tend to have more muscle mass than females, hence the sex differences observed in maximal power output as well as maximal oxygen consumption. Thus the ability to attain a higher power output by virtue of greater upper body strength easily explains the findings in the present study of males reaching higher maximal oxygen consumption values. Further, within the males, the two swimmers reached the highest power output as well as maximal oxygen consumption values. Given the regularity of upper-body exercise performed by these two subjects, it may be assumed that the muscles in their torsos and arms have undergone the adaptations that are typically observed in muscles (e.g., elevated mitochondrial content and increased capillary content as well as increased strength likely due to increased muscle mass) it is not surprising that they reached the highest maximal power output as well as the highest maximal oxygen consumption values. Thus in the present study the fact that maximal oxygen consumption is highly dependent on how much external power may be attributed to increased muscle mass in males, enhanced strength and oxidative capacity (though not measured) in the two swimmers indicates that performance, per se, is not dependent on aerobic capacity, but quite the contrary, in the present study aerobic capacity is dependent upon maximal strength and power. CHAPTER V SUMMARY, CONCLUSIONS, AND RECOMMENDATIONS Summary No differences were found between crank configuration and hand position in POmax, HRmax, VEmax, VO2max and RERmax. This study found no differences in the physiological responses to crank configuration or hand position. However, significant differences were found between males and females in maximal power output, ventilation and oxygen consumption. Lastly, aerobic performance was highly dependent on power output. Conclusions Hand position and crank configuration had no effect on POmax, HRmax, VEmax, VO2max and RERmax. Maximal oxygen consumption was limited by maximal power output (Figure 12). Recommendations for Future Research Future endeavors might include the use experienced hand cyclists. The biomechanical and metabolic effects of a wide (shoulder-width) hand position as well as crank arm length may have an impact on performance. Future research might examine the effects of seat position relative to crank arms on performance. 38 REFERENCES REFERENCES Abel, T., Rojas-Vega, S., Bleicher, I., & Platen, P. (2003). Handbiking: Physiological responses to synchronous and asynchronous crank montage. European Journal of Sport Science, 3(4), 1-9. Bafghi, H. Abbasi, De Haan, A., Horstman, A., & van der Woude, L. (2007). Biophysical aspects of submaximal hand cycling. International Journal of Sports Medicine, 29(8), 630-638. doi: 10.1055/s-2007-989416 Bassett, D. R., & Howley, E. T. (1997). Maximal oxygen uptake: “Classical” versus “contemporary” viewpoints. Medicine & Science in Sports and Exercise, 29(5), 591-603. Bassett, D. R., Jr., & Howley, E. T. (2000), Limiting factors for maximum oxygen uptake and determinants of endurance performance. Medicine and Science in Sport and Exercise, 32(1), 70-84. Boone, T. [Editor-in-Chief], & Warpeha, J. (2003, September). Limitation of maximal oxygen consumption: The holy grail of exercise physiology or fool’s gold? Professionalization of Exercise Physiology, 6(9). Retrieved from http://faculty.css.edu/tboone2/asep/limitationsmaximumoxygenconsumption.h tml 40 41 Bressel, E., Bressel, M., Marquez, M., & Heise, G. D. (2001). The effect of handgrip position on upper extremity neuromuscular responses to arm cranking exercise. Journal of Electromyography and Kinesiology, 11(4), 291-298. Brooks, G. A., Fahey, T. D., Baldwin, K. M. (2005). Exercise physiology: Human bioenergetics and its applications. (Fourth Edition), New York: The McGrawHill Companies, Inc. Carlson, K. F., Wilt, T. J., Taylor, B. C., Goldish, G. D., Niewoehner, C. B., Shamliyan, T. A., & Kane, R. L. (2009). Effect of exercise on disorders of carbohydrate and lipid metabolism in adults with traumatic spinal cord injury: Systematic review of the evidence. The Journal of Spinal Cord Medicine, 32(4), 361-378. Casaburi, R., Barstow, T. J., Robinson, T., & Wasserman, K. (1992). Dynamic and steady-state ventilatory and gas exchange responses to arm exercise. Medicine and Science in Sports and Exercise, 24(12), 1365-1374. Cerretelli, P., Pendergast, D., Paganelli, W. C., & Rennie, D. W. (1979). Effects of specific muscle training on VO2 on response and early blood lactate. Journal of Applied Physiology, 47(4), 761-769. Cerretelli, P., & DiPrampero, P. E. (1987). Gas exchange in exercise. In Handbook of Physiology. A. P. Fishman, L. E. Farhi, S. M. Tenney, & S. R. Geiger (Eds.), Bethesda, Maryland: American Physiological Society, 297-339. Cummins, T. D., & Gladden, L. B. (1983). Responses to submaximal and maximal arm cycling above, at and below heart level. Medicine and Science in Sports and Exercise, 15(4), 295-298. 42 Dallmeijer, A. J., Ottjes, L., De Waardt, E., & van der Woude, L. H. V. (2004). A physiological comparison of synchronous and asynchronous hand cycling. International Journal of Sports Medicine, 25(8), 622-626. doi: 10.1055/s-2004-817879 Davies, K. J. A., Packer, L., Brooks, G. A. (1981). Biochemical adaptation of mitochondria, muscle and whole-animal respiration to endurance training. Archives of Biochemistry and Biophysics, 209(2), 539-554. DiCarlo, S., & Leonardo, J. (1983). Hemodynamic and energy cost responses to changes in arm exercise technique. Journal of American Physical Therapy Association, 63(10), 1585-1590. Ekblom, B., Goldbarg A. N., & Gullbring, B. (1972). Response to exercise after blood loss and reinfusion. Journal Applied Physiology, 33(2), 175-180. Eston, R. G., & Brodie, D. A. (1986). Responses to arm and leg ergometry. British Journal of Sports Medicine, 20(1), 4-6. Fitchett, A. M., (1985). Predictability of VO2 max from submaximal cycle ergometer and bench stepping tests. British Journal of Sports Medicine, 19(2), 85-88. Franklin, B. A. (1985). Exercise testing, training and arm ergometry. Sports Medicine, 2(2), 100-119. Goosey-Tolfrey, V., Alfano, H., & Fowler, N. (2008). The influence of crank length and cadence on mechanical efficiency in hand cycling. European Journal of Applied Physiology, .102(2), 189-194. Goosey-Tolfrey, V. [Editor] (2010). Wheelchair sport: A complete guide for athletes, coaches, and teachers. USA: Sheridan Books. 43 Hagerman, F. C. (1984). Applied physiology of rowing. Sports Medicine, 1(4), 303-326. Harries, M. (1994, July 9). Endurance exercise. British Medical Journal 309 doi: 10.1136/bmj. 309.6947.113 Hayes, A. M., Myers, J. N., Ho, M., Lee, M. Y., Perkash, I., & Kiratli, B. J. (2005). Heart rate as a predictor of energy expenditure in people with spinal cord injury. Journal of Rehabilitation Research & Development, 42(5), 617-624. Hill, A. V., & Lupton, H., (1923). Muscular exercise, lactic acid, and the supply and utilization of oxygen. Quarterly Journal of Medicine (Oxford), 16: 135-171. doi: 10.1093/qjmed/os-16.62.135 Hintzy, F., Tordi, N., & Perrey, S. (2002). Muscular efficiency during arm cranking and wheelchair exercise: A comparison. International Journal of Sports Medicine, 23(6), 408-414. Hjeltnes, N., Galuska, D., Bjornholm, M., Aksnes, A.-K., Lannem, A., Zierath, J. R., & Wallberg-henriksson, H. (1998). Exercise-induced overexpression of key regulatory proteins involved in glucose uptake and metabolism in tetraplegic persons: Molecular mechanism for improved glucose homeostasis. The FASEB Journal, 12(15), 1701-1712. Honig, C. R., Connett, R. J., & Bayeski, T. E. J. (1992). O2 transport and its interaction with metabolism: A systems view of aerobic capacity. Medicine and Science in Sport and Exercise, 24(1), 47-53. 44 Hoppeler, H., Lothi, P., Claassen, H., Weibel, E. R. and Howald, H. (1973).The ultrastructure of the normal human skeletal muscle. A morphometric analysis on untrained men, women, and well-trained orienteers. Pflugers ArchivEuropean Journal of Physiology, 344(3), 217-232. Hoppeler, H., Howald, H., Conley, K. E., Lindstedt, S. L., Claassen, H., Vock, P. & Weibel, E. R. (1985, August). Endurance training in humans: Aerobic capacity and structure of skeletal muscle. Journal of Applied Physiology, 59(2), 320-327. Hubner-Wozniak, E., Lutoslawska, G., Kosmol, A., & Zuziak, S. (2006). The effect of training experience on arm muscle anaerobic performance in wrestlers. Human Movement, 7(2), 147-152. Jensen, E. B., Zheng, D., Russell, R. A., Bassel-Duby, R., Williams, R. S., Olson, A. L., & Dohm, G. L. (2009). American Journal of Physiolog –Regulatory, Integrative and Comparative Physiology, 296(6), R1820-R1828. doi: 10.1152/ajpregu.90651.2008 Kimura, Y., Yeater, R. A., & Martin, R. B. (1990). Simulated swimming: a useful tool for evaluation of vo2max of swimmers in the laboratory. British Journal of Sports Medicine; 24(3), 201-206. Kravitz, L. & Dalleck, & Lance, C. (2002). Physiological factors limiting endurance exercise capacity. University of New Mexico: Idea Health and Fitness Inc. 45 Kwarciak, A. M., Sisto, S. A., Yarossi, M., Price, R., Komaroff, E., & Boninger, M. L. (2009). Redefining the manual wheelchair stroke cycle: Identification and impact of nonpropulsive pushrim contact. American Journal of Physical Medicine & Rehabilitation Services, 90(1), 20-26. Linstedt, S. L., & Conley, K. E. (2001, September). Human aerobic performance: Too much ado about limits to VO2. The Journal of Experimental Biology, 204(Pt 18), 3195-3199. Low, A. & Hatch, C. (1998). The limitation to VO2 max is central! School of Physiotherapy, Curtin University, Bentley, WA. Retrieved from http://physiotherapy.curtin.edu.au/resources/educationalresources/exphys/98/central.cfm Marincek, C. R. T., & Valencic, V. (1977). Arm cycloergometry and kinetics of oxygen consumption in paraplegics. Paraplegia, 15(2), 178-185. McArdle, W. D., Katch, F. I., & Katch, V. L. (1996). Exercise physiology: Energy, nutrition, and human performance. Baltimore, Maryland: Williams & Wilkins. Mossberg, K., Willman, C., Topor, M. A., Crook, H., & Patak, S. (1999). Comparison of asynchronous versus synchronous arm crank ergometry. Spinal Cord, 37(8): 569-574. Mukherjee, G., & Samanta, A. (2000). Evaluation of ambulatory performance of the arm propelled three-wheeled chair using heart rate as a control index. Disability and Rehabilitation, 22(10), 464-470. 46 Mukherjee, G., Bhowmik, P., & Samanta, A. (2001). Physical fitness training for wheelchair ambulation by the arm crank propulsion technique. Clinical Rehabilitation, 15(2), 125-132. Noakes, T. D. (1996). Challenging beliefs: Ex Africa simper aliquid novi. Medicine and Science in Sports and Exercise, 29(5), 571-590. Pollock, M. L., Mengelkoch, L. J., Graves, J. E., Lowenthal, D. T., Limacher, M. C., Foster, C., & Wilmore, J. H. (1997). Twenty-year follow-up of aerobic power and body composition of older track athletes. Journal of Applied Physiology: 82(5), 1508-1516. Powers, K. S., & Howley, T. E., (2009). Exercise physiology: Theory and application to fitness and performance. 7th edition. New York, NY: McGraw Hill Companies, Incorporated. Reybrouck, T., Heigenhauser, G. F., & Faulkner, J. A. (1975). Limitations to maximum oxygen uptake in arms, leg, and combined arm-leg ergometry. Journal of Applied Physiology: 38(5), 1508-1516. Robergs, R. A., & Roberts, S. (1997). Exercise physiology: Exercise, performance, and clinical applications. St Louis, Missouri: Mosby. Seals, Douglas R., & Mullin, John P. (1982). VO2Max in variable type exercise among well-trained upper body athletes. Research Quarterly for Exercise and Sport, 53(1), 58-63. Secher, Niels H., Ruberg-Larsen, N., Binkhorst, R. A., & Bonde-Petersen, F. (1974). Maximal oxygen uptake during arm cranking and combined arm plus leg exercise. Journal of Applied Physiology, 36(5), 515-518. 47 Shaw, D. J Crawford, M. H., Karliner, J. S., DiDonna, G., Carleton, R. M., Ross Jr., J., & O’Rourke, R. A. (1974). Arm-crank ergometry: A new method for the evaluation of coronary artery disease. The American Journal of Cardiology, 33(6), 801-805. doi: org/10.1016/0002-9149(74)90225-2 Stallard, J., G. K., Rose. (1980). Clinical decision making with the aid of ambulatory monitoring of heart rate. Prosthetics and Orthotics International. 4(2), 91-96. Van Drongelen, S., Maas, J. C., Scheel-Sailer, A., & van der Woude, L. H. V. (2009). Submaximal arm crank ergometry: Effects of crank axis positioning on mechanical efficiency, physiological strain and perceived discomfort. Journal of Medical Engineering & Technology, 33(2), 151-157. Vanlandewijck, Y. C., & Thompson, W. R. (2011). The paralympic athlete: Handbook of sports medicine and science. UK: Wiley-Blackwell. Verellen, J., Theisen, D., & Vanlandewijck, Y. (2004). Influence of crank rate in hand cycling. Medicine & Science in Sports & Exercise, 36(10), 1826-1831. Vogler-Andrew, A. J., Rice, A. J., & Gore, J. C. (2010). Physiological responses to ergometer and on-water incremental rowing tests. International Journal of Sports Physiology and Performance, 5(3), 342-358. Wagner, P. O. (1992). Gas exchange and peripheral diffusion limitation. Medical Science Sports and Exercise, 24(1), 54-58. Willis, W. T., Ganley, K. J., & Herman, R. M. (2005). Fuel oxidation during human walking. Metabolism Clinical and Experimental, 54(6), 793-799. APPENDIX A California State University, Chico Kinesiology Department Informed Consent My name is Patrick W. Cottini. I am a graduate student in the Kinesiology and Exercise Science department at California State University, Chico and the primary investigator for this study. I am conducting this study for my thesis for the Master’s degree requirement at CSU, Chico. PURPOSE The purpose of the present investigation is to assess maximal performance (i.e. maximal power output (POmax), maximal oxygen consumption (VO2max), maximal heart rate (HRmax), maximal ventilation (VEmax), and maximal respiratory exchange ratio (RER). The effects of hand position during maximal arm crank ergometry. While placing the cranks in a synchronized vs. asynchronized position, and whether hand position effects maximal performance. PROCEDURES The following procedures have been demonstrated and explained to me and I agree to voluntarily participate in the following with the supervision of the primary or co-investigator: 1. I understand that I will be wearing headgear with a mouthpiece in my mouth for each trial as well as a nose clip on my nose to assure that all airflow goes into the mouth piece. I understand that this may cause some discomfort while using the arm crank ergometer (e.g. excessive production of saliva, mouth may become dry). I understand that the entire experimental protocol will take approximately 8 to 15 min. 2. I understand that my participation is strictly voluntary and I may choose to withdraw or not participate at any time and that there is no penalty for non-participation or withdrawing from the study. 3. I understand that the data will be published but all names, consent forms, and other identifiable information will be kept confidential under lock and key. After the publication of the study, all information will be destroyed. 4. I understand that, if I choose, I will receive a copy of the results. 5. I understand that the study will be performed at the California State University, Chico Exercise lab on five separate days. I understand the risks and discomforts involved with the study. 6. I will pedal on an arm crank ergometer four different times. Each time (and it will vary between hand position and crank position). I will be allowed to warm up on the arm crank for three to five minutes prior to the start of the trials. I will crank on the arm ergometer at the following power output (Watts) and time for two (2) minutes per stage. Power output watts will increase in10 Watt increments until volitional fatigue (e.g. 10, 20, 30, 40, 50, etc. until 2, 4, 6, 8, 10, etc. minutes. 49 50 RISKS I understand that the exercise may be uncomfortable and there are risks related with any exercise. Although rare, the risk of muscle or ligament strain, sprain or heart attack can occur due to maximal exercise. There will be slight discomfort due to finger stick for the blood draw prior to and at the end of each exercise bout. BENEFITS There will be no direct benefit to you as a participant in this study. However, the results and conclusions from this study will be available to you upon request. CONFIDENTIALITY As a subject, you will be assigned a code number and the key to that code will be kept by the principal investigator. Records of this study will be stored in a locked file cabinet in room 134 Yolo Hall and destroyed two years after publication or five years after the study (i.e. after the investigators have exhausted all publication options). You will not be personally identified in any reports or publications that may result from this study. RIGHT TO REFUSE OR WITHDRAW Participation is voluntary. There is no penalty for non-participation. You may choose to participate or withdraw from the study at anytime without penalty or reprisal. QUESTIONS If you have any questions, please feel free to contact me (530-570-3947). You may also report any comments regarding the manner in which this study is being conducted to the Human Subjects Research Committee at CSUC (898-4766). MY SIGNATURE BELOW INDICATES THAT I HAVE CHOSEN TO VOLUNTEER AS A RESEARCH PARTICIPANT AND THAT I HAVE READ, UNDERSTOOD, AND HAVE RECEIVED A COPY OF THIS CONSENT FORM. Participant name (print name)______________________________Date_____________ Participant name (signature)__________________________________ Investigator (print name)___________________________________Date____________ Investigator (signature)______________________________________ Primary Investigator: Patrick W. Cottini Co-Investigator: John L. Azevedo, Jr. APPENDIX B CALIFORNIA STATE UNIVERSITY, CHICO MEDICAL AND EXERCISE HISTORY NAME__________________________ DATE_____________________ BIRTHDATE______________ AGE_____ HEIGHT_______ WEIGHT______ 1. How many days do you exercise in a week? (circle one) 1-2 3-4 5+ 2. On average, what is the duration of a typical exercise session for you? (circle one) 10-20 30-60 60+ min/session 3. Describe the intensity of your exercise (circle one) 1 = none 2 = light (e.g. casual walking, golf) 3 = moderate (e.g. brisk walking, jogging, cycling, swimming) 4 = heavy (e.g. running, high intensity sport activity) 4. What types of exercise do you engage in and how much do you do each session? (circle all that apply) 1 = none 2 = walking 3 = jogging/running 4 = swimming 5 = cycling 6 = team sports (basketball, softball, soccer, etc.) 7 = racquet sports 8 = weight training 9 = other ________________________________________________________________ 5. Do you measure your heart rate during exercise? 1 = yes 2 = no 6. How long have you had a regular exercise program?_________Months - Years 7. What condition or shape do you consider yourself to be in now (in terms of physical fitness)? 1 = poor 2 = fair 3 = good 4 = excellent 8. Do you smoke? 1 = yes 2 = no 52 53 9. 10. Has a close blood relative had or died from heart disease or related disorders (Heart Attack, Stroke, High Blood Pressure, Diabetes etc.)? 1=Mother 2=Father 3=Brother - Sister 4=Aunt - Uncle 5=Grandmother - Grandfather 6=None If yes- Give ages at which they died or had the problems. _______________________________________________________________________________ Indicate which of the following apply to you (circle all that apply). 1 = high blood pressure 2 = high blood fats or cholesterol 3 = cigarette smoking 4 = known heart disease or abnormalities 5 = family history of heart disease (parents or siblings before age 50) 6 = sedentary lifestyle 7 = stressful lifestyle at home or at work 8 = diabetes mellitus 9 = gout (high uric acid) 10 = obesity 11. Any medical complaints now (illness, injury, limitations, neurological symptoms)? 1 = yes If yes, describe completely__________________________________________ 2 = no ________________________________________________________________ _________________________________________________________________ 12. Any major illness in the past? 1 = yes If yes, describe completely__________________________________________ 2 = no _______________________________________________________________ _________________________________________________________________ _________________________________________________________________ 13. Any surgery or hospitalization in the past? 1 = yes If yes, describe completely_________________________________________ 2 = no ______________________________________________________________ ________________________________________________________________ ________________________________________________________________ 14. Are you currently taking any medications (prescription or over-the-counter: including birth control)? 1 = yes If yes, list drugs and dosages _________________________________________ 2 = no _______________________________________________________________ _________________________________________________________________ 15. Have you ever had any neurological problems? 1 = yes If yes, describe completely__________________________________________ 2 = no _______________________________________________________________ _________________________________________________________________ 16. Do you now have, or have you ever had, any of the following? (circle all that apply) 1 = heart murmurs 2 = any chest pain at rest 54 3 = any chest pain upon exertion 4 = pain in left arm, jaw, neck 5 = any palpitations 6 = fainting or dizziness 7 = daily coughing 8 = difficulty breathing at rest or during exercise 9 = any known respiratory diseases 10 = any bleeding disorders or problems with bleeding Please describe fully any items you circled:______________________________________ ________________________________________________________________________ 17. Do you now have, or have you ever had, any of the following? (circle all that apply) 1 = any bone or joint injuries 2 = any muscular injuries 3 = muscle or joint pain following exercise 4 = limited flexibility 5 = any musculoskeletal problems which might limit your ability to exercise Please describe fully any items you circled:___________________________________________ APPENDIX C 56 APPENDIX D 58








© Copyright 2026