
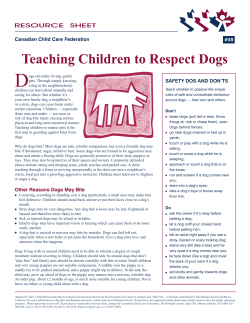
Infectious Diseases of the Dog and Cat, 3rd Edition ACTINOMYCOSIS
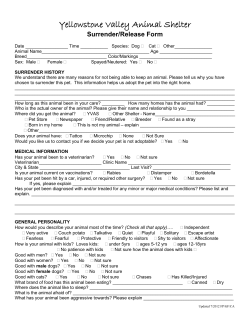
Infectious Diseases of the Dog and Cat, 3rd Edition 49 CHAPTER 49 Actinomycosis and Nocardiosis David F. Edwards 49.1 ACTINOMYCOSIS 49.1.1 Etiology and Epidemiology Actinomycosis is a chronic, pyogranulomatous disease characterized by pleural and peritoneal exudates, dense fibrous masses, frank abscesses, and fistulous tracts with draining sinuses. The disease is caused by anaerobic actinomycetes that are endogenous saprophytes of mucous membranes and members of the family Actinomycetaceae. Actinomyces bowdenii, Actinomyces canis, Actinomyces catuli, Actinomyces 67a hordeovulneris, Actinomyces odontolyticus, Actinomyces turicensis, Actinomyces viscosus, and Arcanobacterium pyogenes (formerly Actinomyces pyogenes) have been recovered from infected dogs.* A. bowdenii, A. viscosus, Actinomyces meyeri, and A. pyogenes have been recovered from infected 12,13,90,91,108 Anaerobic actinomycetes are part of the normal bacterial flora of the mucous membranes. In cats. addition to streptococci, actinomycetes colonize the peridontal mucosal surfaces and adhere to the tooth surface 145 to form plaque. A. viscosus, A. odontolyticus, Actinomyces israelii, Actinomyces bovis, and Actinomyces naeslundii have been cultured from the dental plaque of dogs, and Actinomyces colecocanis has been cultured 64 from the canine vagina. A. viscosus, A. hordeovulneris, and Actinomyces denticolens have been cultured from 452 92 normal feline gingiva. These endogenous saprophytes are not normally pathogenic, but if Actinomyces species are inoculated into tissues with associated bacteria, an insidious pyogranulomatous disease can develop. (Use of the term “Actinomyces species” refers to [1] species currently classified in the genus Actinomyces and [2] related Actinomyces-like bacteria classified in other genera but that cause the clinical disease recognized as actinomycosis.) Actinomycosis occurs most commonly in young adult to middle-age large-breed male dogs that are used or kept 58,74 in an outdoor environment. Hunting dogs have the highest prevalence of disease, and males and females seem to be affected equally. Actinomycosis in outdoor dogs is related in large part to their chronic exposure to 19,46,47,67,106 Inhaled or ingested florets or awns contaminated in the oropharynx migrate to various grasses. sites and act as the nidus of infection. Although infrequently reported in cats, actinomycosis is often attributed 90 to bite wounds. Because of the difficulty in culturing Actinomyces species and their susceptibility to many antibiotics, the true prevalence of actinomycosis in dogs and cats is greater than that suggested by the literature. * 49.1.2 References 13, 24, 37, 43, 49, 63, 65, 67a, 108, 123. Pathogenesis Actinomyces species are opportunistic pathogens that depend on mechanical disruption of normal mucosal barriers. Because of the organism's normal habitat, infections must somehow be linked to the mucous membranes, usually the oropharyngeal area. The disease characteristically spreads by direct extension and is 67a unimpeded by normal tissue planes; however, rare instances of hematogenous dissemination occur. The most common clinical forms of actinomycosis in cats and dogs involve the cervicofacial region, thorax, abdomen, retroperitoneal space, and subcutaneous tissue.* Infection of the cervicofacial region can develop from bite wounds, perforation of the oropharynx by a foreign body, or chronic gingivitis-periodontitis. Pulmonary CHAPTER 49 Actinomycosis and Nocardiosis Page 1 of 21 Infectious Diseases of the Dog and Cat, 3rd Edition infections can develop by aspiration of oropharyngeal material, which may include inhalation of a contaminated 42 grass awn. Preexisting lung disease (e.g., neoplasia) can act as a nidus for infection. Alternative routes of thoracic infection include involvement of the mediastinum from esophageal perforation and direct extension of cervicofacial or abdominal disease. Intraabdominal actinomycosis develops from swallowed organisms or plant material penetrating the gastrointestinal (GI) mucosa. In people, GI disease, abdominal trauma, or surgery often precedes infection. Penetration of the GI tract by a bullet or other foreign bodies, including plant material, also increase the risk of infection for animals. Like thoracic infections, abdominal involvement can occur by direct extension. Infection of the retroperitoneal space in dogs is often associated with grass foreign bodies. Theoretically, contaminated grass florets or awns migrate to the space by migrating through the lung and up the crus of the diaphragm to its dorsal attachment, or by perforating the intestinal wall and migrating via the mesentery to its dorsal attachment. Actinomycosis of the limbs is caused by bite wounds, foreign bodies, and lacerations contaminated by licking. Infection of the subcutaneous tissue in dogs usually represents an extension of cervicofacial, thoracic, or retroperitoneal disease, whereas in cats it is caused by bite wounds. Central nervous system (CNS) infections develop from hematogenous or lymphatic dissemination from a primary site or direct extension from a contiguous infection. Actinomycosis is characteristically a polymicrobial infection, and the pathogenicity of Actinomyces species is dramatically increased in mixed infections. The associated bacteria are commensal organisms from the oral cavity or intestinal tract that produce and maintain an anaerobic tissue environment. Inoculation of pure cultures of Actinomyces species or the associated bacteria alone often do not produce infection. Actinomyces species with fimbriae bind to specific cell surface receptors on other bacteria. This coaggregation markedly inhibits 107 neutrophil phagocytosis of and bactericidal activity on the bacterial complex. If not bound to other bacteria, actinomycetes bind to specific receptors on neutrophils, initiating phagocytosis and degranulation. Additionally, Actinomyces species induce neutrophil chemotaxis, activate macrophages, and stimulate B-lymphocyte hyperplasia. These bacterial-cellular interactions produce the characteristic actinomycosis lesion—a dense mat of Actinomyces species and associated organisms surrounded by neutrophils, macrophages, and plasma cells. Proteolytic enzymes from the associated bacteria, macrophages, and degranulated neutrophils destroy 145 connective tissue, facilitating extension of the disease through normal tissue planes. * 49.1.3 49.1.3.1 References 12, 37, 47, 58, 67, 74, 90, 91, 106. Clinical Findings Dog Cervicofacial actinomycosis produces acute to chronic subcutaneous soft tissue swelling in the head or neck 37,42,106,128 The lesion can be fluctuant or firm, may be indurated, and can be ulcerated or have region. draining sinuses. The mandible, submandibular region, and ventral or lateral cervical area are most frequently affected, but infections involving the face, retrobulbar space, and temporal area have been reported. Radiographically, adjacent bone can have periosteal new bone formation, and a chronic infection may be characterized by osteomyelitis. Ultrasonography and magnetic resonance imaging can be used to 46a,124a Material aspirated from fluctuant masses or discharged from identify linear grass awn foreign bodies. sinuses appears serosanguineous to purulent and may contain macroscopic, yellow-tan granules (i.e., sulfur granules), which are small, soft macroscopic colonies of actinomycetes that are often present in exudates or infected tissue. The term sulfur granule was derived from the frequently seen yellow pigmentation of the granule; however, granule color can vary from white to tan to gray (Fig. 49-1). Aspiration of firm lesions may yield only a few drops of blood. CHAPTER 49 Actinomycosis and Nocardiosis Page 2 of 21 Infectious Diseases of the Dog and Cat, 3rd Edition Actinomycosis involving the thoracic or abdominal cavity is characteristically chronic and progressive; weight loss, often severe, and fever are the most common clinical signs. Thoracic actinomycosis may be limited to the lung parenchyma but can involve multiple structures within the thorax, including the mediastinum, pleura, heart, and chest wall.* Other clinical features include cough, tachypnea, dyspnea, decreased lung sounds (from empyema or a mass lesion), and subcutaneous soft tissue masses on the lateral thorax. Thoracic wall masses often develop a draining sinus. Radiographically, lung disease appears as alveolar and interstitial infiltrates with consolidation. Variable findings include pleural thickening, pleural effusion (often loculated to one side), pericardial effusion, widening of the mediastinum, mass lesions, and periosteal new bone formation or osteomyelitis involving adjacent ribs, vertebral bodies, or sternebrae. Clinical features of abdominal actinomycosis include palpable masses and abdominal distention 452 453 29,43,49,58 Subcutaneous masses, which may have draining sinuses, are rarely present unless the (effusion). abdominal disease develops from an extension of thoracic or retroperitoneal infections. Radiographic manifestations include variable amounts of peritoneal effusion and mass lesions that incorporate or displace adjacent structures. Pleural, pericardial, and peritoneal effusions resemble the exudate from cervicofacial abscesses. Fig 49-1 Thoracic exudate in Petri dish containing numerous macroscopic sulfur granules. (Courtesy David F. Edwards, University of Tennessee, Knoxville, Tenn.) 37,47,67,77 Retroperitoneal actinomycosis is characterized by back pain and rear leg paresis or paralysis. A subcutaneous mass with a draining sinus involving the caudal thorax or flank area is often present. Radiographic findings include periosteal new bone formation involving the ventral aspects of two or three adjacent vertebral bodies (usually T-13 through L-3); involvement of disk spaces is uncommon (Fig. 49-2). Chronic disease may cause the vertebral bodies to develop osteomyelitis and compression fractures. This CHAPTER 49 Actinomycosis and Nocardiosis Page 3 of 21 Infectious Diseases of the Dog and Cat, 3rd Edition finding contrasts with diskospondylitis caused by embolic spread of bloodborne bacteria or fungi to the disk space (see Chapters 40, 64, and 86). Cutaneous-subcutaneous actinomycosis is characterized by a soft to firm mass, which may have a draining 37,47,74,106,128 sinus. These infections are typically located in the head and neck area, lateral thoracic wall, and flank region and are usually extensions of cervicofacial, thoracic, or retroperitoneal actinomycosis. Rare cases of actinomycosis involving the extremities and CNS have been reported. Lameness, mass lesions 20,58 with draining sinuses, and periosteal new bone formation are characteristic of limb involvement. 128,5,34 Actinomycosis of the brain is rare, whereas involvement of the spinal cord is a common sequela to 43,67,77 Clinical findings associated with brain infections are nonlocalizing and subvertebral infections. include altered behavior, decreased consciousness, neck pain, ataxia, abnormal reflexes, and seizures. With spinal cord involvement, pain, paresis, paralysis, and abnormal reflexes are noted, and radiographic evidence of a bony change in adjacent vertebral bodies is present. Cystitis in dogs has been associated with Arcanobacterium pyogenes and a Nocardia-like organism, which most likely represents A. turicensis, a 13,66,68,117 common isolate from wogenital tract infections. Fig 49-2 Spinal radiograph of an 8-year-old pointer with retroperitoneal actinomycosis. Periosteal new bone growth (arrows) is present on ventral aspect of vertebral bodies of L-2 and L-3. (Courtesy David F. Edwards, University of Tennessee, Knoxville, Tenn.) * 49.1.3.2 References 18, 28, 37, 43, 46, 47, 58, 89, 115, 124, 128. Cat Pyothorax and subcutaneous bite wound abscesses are the most common disorders in cats from which 90,91 The abscesses have a malodorous, yellow to sanguineous exudate Actinomyces species are isolated. without a granulomatous mass, and the Actinomyces species is always mixed with two to five other pathogens. Actinomycosis as described in the dog has been reported infrequently in cats. The feline cases CHAPTER 49 Actinomycosis and Nocardiosis Page 4 of 21 Infectious Diseases of the Dog and Cat, 3rd Edition have involved the cervicofacial region, 12,127 the spinal canal. 49.1.4 49.1.4.1 30,84,147 60 thoracic cavity, and subcutaneous tissue with extension to 13 Otitis external secondary to A. pyogenes has been reported in a cat. Diagnosis Clinical Laboratory Findings Hematologic test results in animals with actinomycosis vary according to the location and duration of disease. Animals with focal lesions (e.g., cervicofacial and limb infections) may have few abnormal results, whereas animals with more extensive, chronic disease have mild to moderate nonregenerative anemia, leukocytosis with a left shift and monocytosis, hypoalbuminemia, and hyperglobulinemia (sometimes marked). Dogs with body cavity effusions may be hypoglycemic. Aspirates of abscesses or effusions, tracheal lavages, and sinus discharges are suppurative to pyogranulomatous, whereas aspirates of firm masses may reveal only blood. In some specimens, especially those from effusions, sulfur granules are visible macroscopically (see Fig. 49-1). Microscopically, mixed bacterial populations containing rods and cocci are common. The actinomycetes appear individually or in dense aggregates (sulfur granules) as gram-positive, non–acid-fast filamentous organisms that are occasionally branched (Fig. 49-3). Nocardia species and Filifactor villosus– gram-positive filamentous rods can be confused with Actinomyces species. 91,135 Fig 49-3 Smear of thoracic fluid. Dense mat of infrequently branched, filamentous rods (i.e., sulfur granule). Note presence of other bacterial species (×198). (Courtesy David F. Edwards, University of Tennessee, Knoxville, Tenn.) 453 CHAPTER 49 Actinomycosis and Nocardiosis Page 5 of 21 Infectious Diseases of the Dog and Cat, 3rd Edition 49.1.4.2 453 454 Bacterial Isolation and Identification The disease is confirmed by culture of the organism, but frequently culture results are negative or contain only associated bacteria. Actinomyces species either are facultative (A. canis, A. catuli, A. coleocanis, A. bowdenii, A. denticolens, A. hordeovulneris, A. naeslundii, A. odontolyticus, A. viscosus, A. pyogenes) or 16,63-65,108 Specimens should be collected and processed obligate (A. bovis, A. israelii, A. meyeri) anaerobes. anaerobically and cultured on blood agar or enriched thioglycolate media in the presence of 5% to 10% carbon dioxide. Species that are facultatively anaerobic are variably aerotolerant and can grow aerobically. A. viscosus actually grows best in aerobic conditions. All species cultured aerobically require carbon dioxide, except A. bowdenii, A. naeslundii, and A. odontolyticus. 61 Growth of Actinomyces species can be observed within 48 hours but usually requires 5 to 7 days. It may be necessary to hold plates 2 to 4 weeks. Colonies on blood agar are flat to convex, circular with entire or irregular margins, and translucent to opaque and white; surfaces are smooth and moist or rough (bread crumb or molar tooth surface). Some strains of A. israelii produce aerial filaments, resulting in a powdery, or cotton ball, appearance. Microscopically Actinomyces species are gram-positive, non–acid-fast short rods and filaments. The filaments are less than 1 μm wide, vary considerably in length, may branch, and can stain 18,29,43,58,74 irregularly, producing a beaded appearance. Actinomyces species are heterogeneous, and species 120 identification using traditional biochemical tests is difficult. Results of 16S rRNA gene sequence analysis of previously identified species indicates that several genera in addition to Arcanobacterium and 31,56,112 Variants of A. Actinobaculum will emerge from the species now classified in the genus Actinomyces. hordeovulneris that are cell wall deficient have been produced in culture, suggesting that L forms of Actinomyces species may be associated with clinical disease; however, because of special culture 23 requirements, these variants would be isolated infrequently. Actinomycosis is characteristically a mixed bacterial infection.* Three to five associated bacteria are typically recovered from properly handled specimens. The most commonly isolated organisms are resident flora of the oral cavity or intestinal tract and include Bacteroides species, Corynebacterium species, Escherichia coli, Eubacterium species, Fusobacterium species, Pasteurella multocida, Peptostreptococcus species, Staphylococcus aureus, and Streptococcus species. Most of the associated bacteria are facultative or obligate anaerobes, therefore isolation requires appropriate specimen handling. Unfortunately, the growth of a mixed microflora can impair the isolation of Actinomyces. 61 Because Actinomyces species are sensitive to many antibiotics, the treatment of animals before obtaining specimens for culture can prevent recovery of the organisms. This fact, compounded by improperly handled specimens and polymicrobial growth, accounts for the frequent failure of Actinomyces isolation from infected animals. The diagnosis is often based on the cytologic or histologic identification of the organism in specimens from animals with appropriate clinical signs. Because Actinomyces is a commensal oral bacteria, it is commonly swallowed, inhaled, and transferred by licking, therefore culture of the organism from the airways, GI tract, or skin does not necessarily constitute infection. * References 19, 47, 58, 74, 90, 91, 134. CHAPTER 49 Actinomycosis and Nocardiosis Page 6 of 21 Infectious Diseases of the Dog and Cat, 3rd Edition 49.1.5 Pathologic Findings † Actinomycosis is characterized by a poorly defined, often indurated mass that incorporates adjacent structures. The mass may contain one or more pockets of a reddish-brown exudate. Fistulas and sulfur granules may be found. Thoracic and abdominal infections produce a diffuse, red, velvety to granular thickening of the parietal pleura and peritoneum and omentum. The visceral pleura and peritoneum may be less affected. A variable amount of a reddish-brown exudate that may contain sulfur granules is present. Lung involvement is usually localized and may appear as a consolidation or mass; infrequently, multiple pulmonary nodules are present. Masses can affect multiple internal structures (e.g., heart, mediastinum, lung, diaphragm, and chest wall) and produce an external subcutaneous swelling that may have a draining sinus. With abdominal disease, only one 29,43,49 organ may be affected (e.g., liver), but typically a mass or masses involve multiple adjacent structures. Subcutaneous masses may be ulcerated and in dogs are usually an extension of cervicofacial, thoracic, or 37,47,67 retroperitoneal disease. The histologic reaction to Actinomyces species infection is characterized by a core of neutrophils encapsulated by fibrosing granulation tissue. The granulation tissue contains macrophages, plasma cells, and lymphocytes in a dense, fibrous tissue matrix. The centrally located actinomycotic (sulfur) granule or grain can be very difficult to find, so multiple tissue sections may be needed to confirm the diagnosis. When associated with appropriate clinical signs, identification of true actinomycotic granules is diagnostic of actinomycosis. In tissue sections stained with hematoxylin and eosin (H and E), the granules appear as round, oval, or scalloped amphophilic solid masses with an outer basophilic band (Fig. 49-4, A). The granules vary in size (from 30 to 3000 μm in diameter) and often are rimmed by partially confluent radiate, eosinophilic serrate, or club-shaped structures (i.e., the Splendore-Hoeppli phenomenon). Neutrophils frequently contact or appear enmeshed in this material. Individual actinomycete filaments are not delineated by H and E stain or Gridley's fungal or periodic acid-Schiff reactions, whereas Gram staining of tissues (i.e., the Brown-Brenn procedure) reveals clumps of tangled, intermittently branched, thin (less than 1 μm in diameter) filaments that are gram-positive and slightly beaded (Fig. 49-4, B). Gram-positive or gram-negative nonfilamentous bacteria can be mixed with the Actinomyces species. Actinomyces species are non–acid-fast when stained by the Fite-Faraco modification of the Ziehl-Neelsen technique, which uses a weaker decolorizing agent of 1% sulfuric or 1% hydrochloric acid. With the rare exception of some Nocardia species, other fungi and bacteria that produce tissue granules can be reliably distinguished from Actinomyces by tinctorial and morphologic properties. distinguish it from actinomycosis are listed in Table 49-1. † 49.1.6 27 Features of nocardiosis that References 28, 29, 43, 60, 89, 128, 134. Therapy Successful treatment of actinomycosis involves prolonged administration of antibiotics; the role of surgery varies with the form of the disease. Large doses of penicillin given for prolonged periods (weeks to months) is 81 the treatment of choice (Table 49-2). No strains of Actinomyces species have shown in vitro resistance to easily attainable serum concentrations of penicillin, and acquired resistance in vivo has not been confirmed. Poor drug penetration of the dense granulomatous tissue reaction necessitates the prolonged, high-dose therapy. A minimal dose of penicillin G (benzyl penicillin) or penicillin V (phenoxymethyl penicillin) of 40 mg/kg 43 every 8 hours is recommended. Units of penicillin equivalency per milligram depend on the formulation (see Appendix 8). The therapeutic advantage of initial parenteral administration is questionable, therefore if the 43,105 animal is stable clinically, oral therapy can be started from the outset. Because food reduces the CHAPTER 49 Actinomycosis and Nocardiosis Page 7 of 21 Infectious Diseases of the Dog and Cat, 3rd Edition absorption of most penicillins, medication should be given 1 hour before or 2 hours after feeding. Therapy must be extended significantly (weeks to months) beyond resolution of measurable disease to prevent relapse; in 43,58 454 456 Drugs other than penicillin that are effective against most some cases, treatment can exceed 1 year. Actinomyces species include erythromycin, clindamycin, ampicillin, tetracycline, minocycline, doxycycline, chloramphenicol, imipenem, and first-generation cephalosporins and ceftriaxone. 81,123,146 Anecdotal success 94 with ciprofloxacin was reported in a human patient with recalcitrant actinomycosis of 20 years’ duration; however, recently described Arcanobacterium bernardiae and Actinomyces neuii are resistant to ciprofloxacin, and in vitro resistance to fluorinated quinolones was reported for an Actinomyces species isolate from a dog 16,41 Oxacillin, dicloxacillin, cephalexin, metronidazole, and aminoglycosides have poor with thoracic disease. in vitro activity against most Actinomyces species; however, A. pyogenes is sensitive to aminoglycosides (other 55 than streptomycin) but resistant to tetracycline, minocycline, and doxycycline. Poor response to appropriate 81 doses of penicillin may be attributable to poor surgical drainage and failure to eliminate associated bacteria. Infections by these organisms usually resolve with penicillin, but on occasion they require broader spectrum antibiotics during the initial treatment period followed by long-term administration of penicillin. Cats with pyothorax or subcutaneous abscess that have not developed a granulomatous tissue reaction often can be cured with drainage and a shorter duration of antibiotic treatment. Fig 49-4 A, H and E stained section of abdominal mass from 5-year-old neutered female boxer dog. Actinomycotic tissue granule is surrounded by neutrophils. Encapsulating fibrous tissue has mononuclear cell infiltrate. (The long dimension of the granule measures 695 μm; ×13.2). B, Tissue section (Gram stain, Brown-Brenn procedure) of intrathoracic mass from 4-year-old German shorthaired pointer. Actinomycotic tissue granule showing infrequently branched, filamentous rods characteristic of Actinomyces organisms (×132). (A, Courtesy David F. Edwards, University of Tennessee, Knoxville, Tenn.) CHAPTER 49 Actinomycosis and Nocardiosis Page 8 of 21 Infectious Diseases of the Dog and Cat, 3rd Edition Table 49-1 Comparison of Actinomycosis Versus Nocardiosis ACTINOMYCES SPECIES Culture 1. Facultative or obligate anaerobe 2. Fastidious growth requirements; often not cultured 3. Two to five associated microbes usually recovered NOCARDIA SPECIES 1. Aerobe 2. Usually cultured 3. Sole isolate unless from contaminated sample (e.g., tracheal wash, ulcerated skin) Staining Characteristics 1. Irregular staining that can produce slight beading 2. Gram-positive and non–acid-fast using Fite-Faraco modification of Ziehl-Neelsen technique Cytopathologic Characteristics 1. Suppurative to pyogranulomatous inflammation with a mixed bacterial population; macroscopic and microscopic dense mats of long filamentous bacteria often present (see Fig. 49-3) Histopathologic Characteristics 1. Pyogranulomatous inflammation with marked encapsulating fibrosis (see Fig. 49-4) 2. Variable presence of tissue granules (30–3000 mm diameter) Clinical Disease 1. In adult outdoor dogs (especially hunting breeds); with bite wounds and pyothorax in cats 2. Direct spread to adjacent structures 3. Sensitive to high doses of penicillin 4. Low mortality 1. Irregular staining that can produce marked beading 2. Gram-positive and partially acid-fast using Fite-Faraco modification of Ziehl-Neelsen technique 1. Suppurative to pyogranulomatous inflammation; long filamentous bacteria typically present singly or in loose aggregates (see Fig. 49-6); infrequently macroscopic and microscopic dense mats of long filamentous bacteria present 1. Pyogranulomatous inflammation; significant fibrosis present only in chronic skin infections (see Fig. 49-7) 2. Granules present only in skin infections (15–200 mm diameter) 1. In dogs younger than 2 years old; from fight wounds in cats 2. Hematogenous spread; can see lesions at noncontiguous sites 3. Variable sensitivity to sulfonamides 4. Moderate to high mortality Table 49-2 Drugs Used to Treat Actinomycosis in Dogs and Cats SPECIES a DRUG Penicillin G Penicillin G Penicillin V B B c B Clindamycin Erythromycin Chloramphenicol Rifampin Minocycline c B B D C D B B b DOSE 100,000 U/kg ROUTE INTERVAL (HOURS) d IV, IM, SC PO d PO 8 SC PO PO, IV, IM, SC PO, IV, IM, SC PO IV, PO IM, SC, PO 12 8 8 12 12 12 6 40 mg/kg 40 mg/kg 5 mg/kg 10 mg/kg 50 mg/kg 50 mg/kg 10 mg/kg 5–25 mg/kg 20–40 mg/kg Ampicillin (amoxicillin) B, Dog and cat; D, dog; C, cat; IV, intravenous; IM, intramuscular; SC, subcutaneous; PO, by mouth. a See Appendix 8 for more information on these drugs. b Dose per administration at specified interval. For duration, see text. c Give at least 1 hr before or 2 hr after feeding to facilitate GI absorption. d Minimum recommended dose (see text); 1 mg = 1600 U (see Appendix 8). CHAPTER 49 Actinomycosis and Nocardiosis 6–8 8 Page 9 of 21 Infectious Diseases of the Dog and Cat, 3rd Edition Surgery has a controversial role in the treatment of acti-nomycosis. Draining of abscesses and effusions 58,60,115 (thoracic, abdominal, and pericardial) should always be used as an adjunct to antibiotic treatments. 46,134 Continuous suction and intermittent drainage techniques have been used for thoracic effusions in dogs. Drain tubes are removed when the purulent exudate changes to a serosanguineous transudate, usually within 4 to 10 days. Daily lavage with fluids containing crystalline penicillin G may be beneficial. Using sodium penicillin rather than potassium penicillin in the lavage fluid prevents the development of cardiotoxicity from 6 hyperkalemia. (Crystalline potassium penicillin G contains 1.7 mEq potassium per 10 U.) Complications of drainage include pneumothorax and subcutaneous abscess formation at the drain tube insertion site. Animals 46,115,134 In animals not responding to drainage and appropriate antibiotic therapy warrant exploratory surgery. with pulmonary abscesses, diseased lung lobes often require removal. The characteristic invasive fibrotic lesions obliterate tissue planes, preventing conservative dissection, and the tissue is well vascularized, therefore moderate to severe bleeding is common. With diffuse disease involving body cavities, tissue resection should be restricted to decrease the chance of death. In dogs with solitary masses involving the thoracic and abdominal 46 walls, radical surgical excision has a high cure rate, although repeat surgeries may be needed. The masses often can be reduced and better defined by an initial period of antibiotic therapy. Frequently, grass florets or 46,46a,67,124a awns are found in these lesions and during surgical exploration of diseased retroperitoneal regions. Surgery should never be performed in lieu of and should always be followed by appropriate antibiotic therapy. Appropriate treatment of dogs with actinomycosis, which can involve extremely prolonged use of antibiotics 43,46,58 and surgery, results in a cure rate of greater than 90%. Because of the infrequent documentation of actinomycosis in cats, a meaningful cure rate is not available, but it is likely similar to the cure rate in dogs. 49.1.7 Public Health Considerations No reports exist of actinomycosis being transmitted from clinically infected animals to humans or to other 113 animals; however, humans bitten by dogs, cats, or other people can develop actinomycosis. Nevertheless, animal care workers handling infected tissues or discharge should wear protective gloves to avoid inadvertent contact by inoculation or through damaged skin. 49.2 NOCARDIOSIS 49.2.1 Etiology and Epidemiology Nocardiosis is a suppurative to granulomatous, localized or disseminated bacterial infection caused by aerobic 10,11 Nocardia asteroides is the most commonly actinomycetes that are members of the family Nocardiaceae. isolated species in dogs and cats, but infections by Nocardia brasiliensis (in the dog and cat), Nocardia otitidiscaviarum (in the dog and cat), Nocardia nova (in the cat), and N. africana (in the cat) have been reported.* As historically defined, N. asteroides, 126,116 N. brasiliensis, 136 N. nova, 33 456 457 108a N. otitidiscaviarum 142 and Nocardia transvalensis consist of several subtypes and species. Recent publications cite approximately 34 valid species of Nocardia; to date, at least 20 species have been implicated in human infections. It is certain previous reports of nocardiosis in dogs and cats understate the number of species producing disease. These aerobic actinomycetes are ubiquitous soil saprophytes that degrade organic matter and are found in soil, in 10,99 Infections are considered opportunistic, occurring by either inhalation of organisms or water, and on plants. inoculation through puncture wounds. CHAPTER 49 Actinomycosis and Nocardiosis Page 10 of 21 Infectious Diseases of the Dog and Cat, 3rd Edition In a survey of 53 dogs with nocardiosis, males were infected three times more frequently than females; 65.4% of the dogs were younger than 1 year, 82.7% were younger than 2 years, and only 7.8% were older than 6 years; 11 26.9% had an underlying condition, most often canine distemper. Apparently in dogs, like in people, predisposing factors (i.e., diseases) increase susceptibility to nocardiosis. Approximately 40% of people with nocardiosis have primary disorders that involve immunosuppressive drug therapy, obstructive pulmonary disease, metabolic disorders (e.g., hyperadrenocorticism, diabetes mellitus), neoplasia (lymphosarcoma, leukemia), immunologic disease (systemic lupus erythematosus, dysgammaglobulinemia), or infectious 10,99 diseases (e.g., acquired immunodeficiency syndrome). In 20 reported cases of feline nocardiosis, 15 † involved males and 4 involved females. Ages ranged from 2 to 15 years (with a median age of 7 years). Fourteen of the cats had draining wounds or abscesses that were associated with scratches or bite wounds. 49.2.2 * References 2, 11, 59, 62, 93. † References 2, 3, 6, 9, 26, 38, 59, 62, 78, 93, 95, 102, 109, 131, 141. Pathogenesis Similar to the systemic mycoses, pulmonary nocardiosis probably results from inhalation of soil organisms. Nocardial lesions develop in alveolar spaces and frequently erode into blood vessels, resulting in systemic spread of the disease. Secondary lesions from systemic spread can develop in any tissue. Involvement of contiguous structures within the thorax (e.g., pleura, mediastinum, pericardium) is also common. Localized cutaneous, subcutaneous, and regional lymph node infections result from inoculation through a puncture wound (e.g., bite, scratch, foreign body). Other solitary extrapulmonary sites of infection are likely caused by 10,99 localization from a transient bacteremia. The primary source may be an inapparent pulmonary infection. Pathogenicity of Nocardia species is influenced by the strain and growth phase of the organism and host susceptibility. Normal host response to infection is characterized by an initial neutrophil mobilization that may inhibit growth but not kill the organism. Subsequent cell-mediated immunity consisting of activated macrophages and T lymphocytes is normally bactericidal. Diminished host resistance is a primary factor in nocardiosis, but not all diseased animals have identifiable predisposing conditions. Virulent strains of Nocardia are facultative intracellular pathogens that inhibit phagosome-lysosome fusion, neutralize phagosomal acidification, resist oxidative burst, and alter lysosomal enzymes within neutrophils and macrophages. These effects are partly related to the content and structure of mycolic acids within the bacterial cell wall, which vary among strains and during the growth phase. Some strains exhibit organ-specific trophism (e.g., brain), and the filamentous, logarithmically growing organisms are 10 times more virulent than the coccoid stationary-phase cells. 49.2.3 49.2.3.1 10,99 Clinical Findings Dog Pulmonary nocardiosis can have a peracute onset characterized by inspiratory dyspnea, hemoptysis, 85 hypothermia, collapse, and death ; however, subacute to chronic clinical symptoms are more 1,26,36,76,96 The signs are often similar to those of distemper and include mucopurulent characteristic. oculonasal discharge, anorexia, weight loss (often emaciation), cough, dyspnea, diarrhea, and hyperthermia. Lung sounds may be increased (from bronchopneumonia) or decreased (from a mass lesion or empyema). CHAPTER 49 Actinomycosis and Nocardiosis Page 11 of 21 Infectious Diseases of the Dog and Cat, 3rd Edition 11 Coinfection by the canine distemper virus is commonly reported. The radiographic appearance of lesions varies and includes multiple, diffuse pulmonary nodules, intrapulmonary or extrapulmonary solitary masses, focal or diffuse bronchointerstitial to alveolar infiltrates, lobar consolidations, pleural effusions, and often, dramatic hilar lymphadenopathy (Fig. 49-5). Systemic, or disseminated, nocardiosis, defined by lesions at two or more noncontagious sites within the body, is typically associated with pulmonary disease and rarely develops without obvious associated pulmonary disease.* The most frequently involved extrathoracic organs are skin and subcutaneous tissue, the kidney, the liver, the spleen, lymph nodes, the CNS, bone, and joints. The cutaneous-subcutaneous lesions are characterized by firm to fluctuant swellings that may ulcerate or develop fistulous tracts through which a reddish-brown exudate is discharged. Involvement of the liver, the spleen, and lymph nodes is detected because of organomegaly. CNS lesions may cause seizures. Bone or joint infection results in swelling and lameness; radiographic findings include soft tissue swelling, bone lysis, and periosteal new bone growth. Solitary extrapulmonary nocardiosis develops infrequently and usually occurs as a cutaneous-subcutaneous 8 20,119 40 abscess or an actinomycotic mycetoma. A case of humeral osteomyelitis has been reported. Mycetoma is a localized, subcutaneous granulomatous tumor that contains organized aggregates (grains or granules) of free-living or exogenous, geophilic actinomycetes (actinomycotic mycetoma) or fungi (eumycotic mycetoma). Mycetomas usually develop on extremities, may involve underlying bone, and typically form abscesses that result in fistulas to the skin. Because Actinomyces is endogenous, tumorous infections of subcutaneous tissues are not classified as mycetomas. Nocardia infections have been reported 66 in 10 dogs with thoracolumbar vertebral osteomyelitis and in one dog with cystitis ; however, many of these dogs were probably infected with Actinomyces species (see Actinomycosis, Clinical Findings, in this chapter). * 49.2.3.2 17,103,122,125 References 1, 8, 72, 73, 76, 96, 114, 121, 129. Cat The clinical forms of feline nocardiosis (pulmonary, systemic, and solitary extrapulmonary) are similar to those described in the dog; however, in cats, cutaneous-subcutaneous disease (abscesses and actinomycotic mycetomas) is the most common clinical form. Of 20 reported cases of nocardiosis, 14 cats had † 5,59,62,102 cutaneous-subcutaneous lesions involving the extremities, inguinal area, 3,6,78,95,109 had pulmonary disease (nodules or empyema), 131 one had peritonitis, 2,3,59,95,141 and neck. 23,62 Five cats and five had systemic All those with systemic disease had a primary cutaneous-subcutaneous lesion. nocardiosis. Macroscopic sulfur granules were noted in the exudate of five cats (representing all three forms of clinical disease). 26,38,62,131 CHAPTER 49 Actinomycosis and Nocardiosis 457 458 Page 12 of 21 Infectious Diseases of the Dog and Cat, 3rd Edition Fig 49-5 Right lateral thoracic radiograph of 8-month-old male Labrador retriever with pulmonary nocardiosis. Radiographic abnormalities include bronchointerstitial pattern and marked hilar lymphadenopathy. (Courtesy Royce Roberts, University of Georgia Veterinary Teaching Hospital, Athens, Ga.) † 49.2.4 49.2.4.1 References 72, 38, 62, 93, 95, 141. Diagnosis Clinical Laboratory Findings Animals with nocardiosis have nonregenerative anemia, neutrophilic leukocytosis with a left shift, monocytosis, and hyperproteinemia. Hypercalcemia associated with granulomatous disease has been 102 reported. Pleural effusions, bronchial lavages, and aspirates of abscesses are suppurative to pyogranulomatous. Gram-positive, partially or weakly acid-fast, beaded, branching filamentous organisms are often observed individually or in loose aggregates (Fig. 49-6). Macroaggregates (i.e., sulfur granules) have been noted infrequently in effusions. Unlike actinomycosis, mixed bacterial populations from deep tissue sites are rare and probably caused by contamination of the sample (e.g., bronchial lavage, ulcerated skin abscess). 1,8,76,96 CHAPTER 49 Actinomycosis and Nocardiosis Page 13 of 21 Infectious Diseases of the Dog and Cat, 3rd Edition 49.2.4.2 Bacterial Isolation and Identification The presence in clinical specimens of a gram-positive, partially acid-fast, beaded, branched filamentous organism 0.5 to 1 μm in diameter warrants specific therapy for nocardiosis, but the diagnosis is confirmed by culture of the organism. Nocardia species grow aerobically at a wide temperature range on simple media (e.g., Sabouraud's glucose agar, blood agar). Growth is enhanced by 10% carbon dioxide, modified Thayer-Martin medium and buffered charcoal-yeast extract agar but is retarded by inhibitory medium used for fungal isolation. Organisms are usually recovered in pure cultures, and colonies are often visible after 2 days. However, 2 to 4 weeks of incubation may be necessary, especially if samples contain multiple bacterial species (e.g., bronchial lavage) or are from animals receiving antibiotics. Colonies can be smooth and moist or rugose with a powdery surface from aerial filaments. Because most Nocardia species produce 10,82,99 Microscopically, carotenoid-like pigments, colony color varies (cream, yellow, orange, pink, or red). Nocardia species grown on solid media appear as branched filaments that fragment into pleomorphic, rod-shape, or coccoid elements. Nocardia species are gram-positive and variably acid-fast. In clinical specimens or primary isolates, Nocardia species are often partially acid-fast, but a Fite-Faraco modification of the Ziehl-Neelsen technique decolorized with 1% sulfuric or 1% hydrochloric acid must be used. Not all pathogenic strains of Nocardia species are acid-fast—a characteristic that may disappear after subculture. 10,82,99 Fig 49-6 Impression smear of chronic (15 months duration), ulcerated cutaneous lesion on lateral thorax of 3-year-old female domestic shorthaired cat. Loose aggregate of infrequently branched, filamentous rods with beading from irregular staining is typical of Nocardia organisms (×330). (Courtesy David F. Edwards, University of Tennessee, Knoxville, Tenn.) CHAPTER 49 Actinomycosis and Nocardiosis Page 14 of 21 Infectious Diseases of the Dog and Cat, 3rd Edition Identification of the species of Nocardia isolates is important for prediction of antimicrobial susceptibility. Traditionally, species have been distinguished by phenotypic features, including growth characteristics and antibiotic susceptibility patterns; however, modern molecular methods have provided a more reliable and 32,75,138 Restriction fragment length polymorphism (RFLP) analysis of polymerase rapid means of speciation. chain reaction (PCR) products from the 16S rRNA gene identifies most pathogenic Nocardia organisms at a level of therapeutic relevance, but ultimate differentiation of closely related Nocardia species may require RFLP analysis of hsp gene products, 16S rRNA and hsp gene sequencing, or DNA-DNA hybridization. 33,116,142 L-form 22 disease in people and a dog. Nocardia spp., cell wall–deficient variants, have been associated with clinical 458 459 These bacteria require special media for isolation and culture (see Chapter 33). Pathogenic Nocardia species are not common laboratory contaminants, therefore the isolation of a single colony from a closed lesion is significant. Because Nocardia organisms are ubiquitous in soil and in certain circumstances may act as respiratory saprophytes, the isolation of small numbers of organisms from 10,82,99 ulcerated skin lesions or the respiratory tract must be interpreted in conjunction with clinical signs. 49.2.5 Pathologic Findings Nocardiosis is characterized by suppurative necrosis and abscess formation and infrequently produces granulomas. The gross lesions on internal organs typically are numerous small (1 mm) to large (1 cm), discrete 72,114,121,129 The nodules are usually subserosal and when cut to coalescing, raised white or gray-white nodules. appear caseous to purulent. Affected lung tissue may appear congested. Lymph nodes are enlarged, often 36,76,114 massively, and are firm to fluctuant with a caseous to purulent core. 1,8,128 present in the pleural or peritoneal space or within abscesses. noted. A reddish-brown exudate may be Yellow granules in the exudate have been 76,131 The histologic reaction to nocardial infection is characterized by a central region of necrosis and suppuration 114,121,129 Clusters of epithelioid macrophages and surrounded by macrophages, lymphocytes, and plasma cells. multinucleated giant cells may be observed. Except with some skin infections, fibrous tissue is usually poorly structured, producing thin or incomplete encapsulation of the lesion. In chronic cutaneous-subcutaneous 20,36 infections, pyogranulomatous foci may be interspersed within a dense fibrous tissue matrix. Nocardial organisms are usually present and often abundant in the necrotic and suppurative tissue reactions. Gram staining of tissue (e.g., the Brown-Brenn procedure) is best for seeing the filaments, but tissues can also be stained by methenamine silver preparations, especially with prolonged silver nitrate exposure (i.e., 80 to 100 minutes). Nocardia filaments are not visible in tissue sections stained with H and E or with Gridley's fungal or periodic acid-Schiff reactions. The organisms are characteristically but not invariably partially acid-fast when a weak decolorizing solution is used (i.e., 1% sulfuric or 1% hydrochloric acid). Nocardia species appear as beaded, branching filaments that are 10 to 30 μm or more long and 0.5 to 1.0 μm wide. The filaments usually appear individually or in tangled, loose aggregates. In chronic skin infections, tissue granules characterized by colonies arranged in large, rosette-like arrays have been reported (Fig. 49-7). In human nocardiosis, tissue granules are uncommon; when present, the granules are small (15 to 200 μm), usually not associated with the Splendore-Hoeppli phenomenon, and usually produced in chronic skin infections by N. brasiliensis. CHAPTER 49 Actinomycosis and Nocardiosis Page 15 of 21 Infectious Diseases of the Dog and Cat, 3rd Edition 49.2.6 Therapy Sulfonamides, including trimethoprim-sulfonamide combinations, are the primary drugs for treating nocardiosis (Table 49-3). Most Nocardia species, with the possible exception of N. otitidiscaviarum, are susceptible to sulfonamide therapy, but treatment must be continued for a prolonged period. From 1 to 3 months is recommended in people with cutaneous infections, up to 6 months for uncomplicated pulmonary infections, and 12 months or longer for systemic infections or infections in those who are immunocompromised. Clinical improvement should be observed within 7 to 10 days of starting treatment. Abscesses or empyema usually must 82,99 be surgically drained to cure the patient. Antibiotics in addition to or other than sulfonamides may be needed because not all Nocardia isolates are sensitive to sulfonamides, in vitro susceptibility may not be associated with clinical response, and resistance can develop during treatment. administration. 133 82,99,111 459 460 Adverse drug reactions may prevent prolonged sulfonamide High doses of trimethoprim-sulfadiazine given for long periods to dogs and cats produces 35,88 Drug susceptibility testing of Nocardia isolates is reversible myelosuppression (anemia and leukopenia). technically difficult and should be done at experienced laboratories. The National Committee for Clinical 143 Laboratory Standards has approved a standard for susceptibility testing by broth microdilution, and a 4 comparative study of several conventional susceptibility testing methods has been published. PCR identification and drug susceptibility testing of Nocardia species can be done at the University of Texas Health Center at Tyler.* CHAPTER 49 Actinomycosis and Nocardiosis Page 16 of 21 Infectious Diseases of the Dog and Cat, 3rd Edition Fig 49-7 A, H and E–stained section of chronic, ulcerated cutaneous lesion on flank of 3-year-old male domestic longhaired cat. Nocardia tissue granules are surrounded by pyogranulomatous inflammatory reaction. (Long dimension of largest granule is 110 μm; ×66.) B, Acid-fast stain (Fite-Faraco modification of Ziehl-Neelsen technique) of same tissue section (×132). (Courtesy David F. Edwards, University of Tennessee, Knoxville, Tenn.) CHAPTER 49 Actinomycosis and Nocardiosis Page 17 of 21 Infectious Diseases of the Dog and Cat, 3rd Edition Table 49-3 Drugs Used to Treat Nocardiosis in Dogs and Cats a DRUG Triple sulfa no. 4 Sulfadiazine d DOSE ROUTE b c 60 mg/kg 80 mg/kg 50 mg/kg a INTERVAL (HOURS) IV 12 PO PO 8 8 Sulfasoxazole Amikacin 8–12 mg/kg IV, IM, SC Imipenem-cilastatin 2–5 mg/kg IV Cefotaxime 20–80 mg/kg IV, IM Minocycline 5–25 mg/kg IV, PO Erythromycin 10 mg/kg PO Ampicillin 20–40 mg/kg IV, IM, SC, PO Linezolid 8–20 mg/kg PO IV, Intravenous; PO, by mouth; IM, intramuscular; SC, subcutaneous. 8 8 6 12 8 6 24 a See Appendix 8 for more information on these drugs. b Dose per administration at specified interval. For duration, see text; usually a minimum of 6 weeks is required with all the drugs. c 120 mg/kg IV initially. d Also sulfamethizole. CHAPTER 49 Actinomycosis and Nocardiosis Page 18 of 21 Infectious Diseases of the Dog and Cat, 3rd Edition Table 49-4 Percentage of Pathogenic Nocardia Species Isolates with Sensitivity or Intermediate Sensitivity to Various Drugs In Vitro a a DRUG ISOLATE N. asteroides complex AMK A-C AMP CTX CTA CIPRO ERY S S S S — R I S — — — S S S S S S S S S — S/I — — S — 100 6 84 96 96 0 100 100 — 100 98 88 — N. africana N. veterana (5) — — 100 — — — 100 — 0 — — — 0 S I/S S I/R R/I R S S S/R S I S — Type V: N. 99 79 7 6 17 80 9 83 3 100 96 76 95 S R/S — I/S I/S R — I/R — 100 I S S S — — — S — — S — — S 100 100 <10 100 29 10 pseudobrasiliensis N. otitidiscaviarum 100 15 10 9 COMPLEX N. transvalensis — — 10 COMPLEX N. transvalensis 0 0 12 33 3 87 140 Type I: N. abscessus (1) IMP GENTLNZMINOT-SSULFA b Type II: N. brevicatena c,44,140 N. paucivorans (3) Type III: N. nova type 21,101,137,140 strain 144 33,52,110,14 21,101,132,139,140 farcinia Type IV: N. asteroides sensu stricto (3) 21,104 132 N. cyriacigeorgici (1) N. brasiliensis COMPLEX 21,54,137 N. brasiliensis N. 21,14 e,14,21,45,51,140 e,21,100 142 — — <17 0 <10 100 100 98 97 83 95 — <10 — 100 26 94 — 29 78 55 f 57 86 100 100f 31 31 50 50 60 50 90 — 100 54 82 90 — — — — — — 20 — — — — 87 — — — — — — 12 — — — — 100 R S S S — — 0 — S — S — — — — 100 — 4 — — — — d 94/<50 92/<50 78 9 d sensu stricto 142 New taxon 1 87,142 New taxon 2 (1) Type IV: N. asteroides 126,142 COMPLEX AMK, Amikacin; A–C, amoxicillin-clavulanate;; AMP, ampicillin; CTX, cefotaxime; CTA, ceftriaxone; CIPRO, ciprofloxacin; ERY, erythromycin; IMP, imipenem; GENT, gentamicin; LNZ, linezolid; MINO, minocycline; T-S, trimethoprim-sulfamethoxazole; SULFA, sulfonamides; S, sensitive; I, intermediate sensitivity; R, resistant. a If data from only a small number of clinical isolates were available, the number of isolates is indicated in parentheses following the species name and susceptibility patterns are designated by S (sensitive), I (intermediate sensitivity) and R (resistant). When 2 letters (e.g., S/I) are present the first letter represents the susceptibility pattern of the majority of isolates. b To date, no clinical isolates have been tested. c N. paucivorans has tentatively been categorized as a type II N. asteroides complex based on a 99.7% 16S rRNA gene sequence similarity to N. brevicatena. (Yassin AF, et al. 2000. Int J Sys Evol Microbiol 50:803–809.) CHAPTER 49 Actinomycosis and Nocardiosis Page 19 of 21 Infectious Diseases of the Dog and Cat, 3rd Edition d Cited references report significantly different susceptibility patterns to third-generation cephalosporins. e Susceptibility data for N. otitidiscaviarum and N. transvalensis complex isolates are confounded by lack of separation of more recently identified species. f Approximately 50% of isolates were of only intermediate sensitivity. 460 Susceptibility studies have identified relatively characteristic species-associated resistance patterns (Table 49-4) and led to the use of various antibiotics other than or in conjunction with sulfonamides to treat nocardiosis in people. In vitro, combinations of imipenem with cefotaxime or trimethoprim-sulfamethoxazole and amikacin with trimethoprim-sulfamethoxazole were synergistic, increasing minimum inhibitory concentrations four times or more for the majority of 26 isolates of N. asteroides complex. Combinations of amikacin with imipenem or 53 cefotaxime were predominantly additive. Nocardia species tested. 21,33,54 461 Linezolid, an oxazolidinone, had in vitro activity against all Based on in vitro data, topical imidazoles and ketaconazole may be effective 41 against some Nocardia species. Treatment success has been reported with amikacin, ampicillin, broad-spectrum cephalosporin, clarithromycin, doxycycline, erythromycin, imipenem, minocycline, ofloxacin, 82,99,83,104,130 Nocardiosis in animals that are severely ill, have systemic and linezolid alone or in combination. diseases, or have predisposing conditions may warrant initial combination drug therapy. If CNS disease is present, use of drugs with excellent CNS penetration, which include third-generation cephalosporins, imipenem, and linezolid, may be more effective than sulfonamides alone. Longer term use of linezolid in 50 humans produces a reversible myelosuppression (anemia and thrombocytopenia) and rarely has been 79,80 Ideally, drug selection should be based on susceptibility associated with optic and peripheral neuropathies. studies of the isolate but if the information is not available, logical choices can be made using the in vitro data in Table 49-4. Substitution of antibiotics within a class of drugs may not provide effective treatment; for example, although sensitive to amikacin, Nocardia farcinia isolates are resistant to gentamicin (see Table 49-4), 54 and although sensitive to minocycline, N. brasiliensis isolates are mostly resistant to doxycycline. Drug susceptibility patterns of Nocardia species more recently isolated from human patients (Nocardia abscessus, Nocardia asiatica, Nocardia cyriacigeorgici, Nocardia inohanensis, Nocardia yamanashiensis, Nocardia 48,68-71 niigatensis, and Nocardia beijingensis) have not yet been fully characterized. 11 In a review of 53 dogs with nocardiosis, 50% of the dogs died and 38.5% were euthanized. Nine of 19 cats with nocardiosis either were euthanized or died.* The high mortality rate is partly attributable to predisposing conditions (distemper in dogs), delayed diagnosis, and inappropriate therapy. With earlier diagnosis and multidrug therapy, mortality of nocardiosis in animals may decrease to the rate reported in people. Only 19.8% of people with primary infections died, whereas 42.4% of patients with predisposing conditions and more than 10 50% of patients with either systemic or CNS nocardiosis died. 49.2.7 * Mycobacteria/Nocardia Research Laboratory, Department of Microbiology, University of Texas Health Center at Tyler, 11937 US Highway 271, Tyler, TX 75708. Phone: 903-877-7685; Fax: 903-877-7652. * References 2, 3, 6, 9, 26, 38, 59, 62, 78, 93, 95, 102, 109, 131, 141. Public Health Considerations No cases of human nocardiosis acquired from direct contact with an infected dog or cat have been reported; however, several cases of cutaneous nocardiosis transmitted to people by a scratch or bite from clinically healthy cats and dogs have been documented. 7,15,45,86,118 Nocardia species, which are ubiquitous in the soil, CHAPTER 49 Actinomycosis and Nocardiosis Page 20 of 21 Infectious Diseases of the Dog and Cat, 3rd Edition can contaminate the claws and teeth of dogs and cats, although the risk of a person contracting nocardiosis by an animal bite or scratch wound is no greater than the risk associated with getting a puncture wound while gardening. Special precautions are warranted when a person with suppressed immunity (e.g., who is receiving immunosuppressive drug therapy, who has human immunodeficiency virus infection) is caring for a dog or cat with nocardiosis. 49.3 Acknowledgment The author would like to thank Barbara Brown-Elliott, Mycobacteria/Nocardia Research Laboratory, Department of Microbiology, University of Texas Health Center at Tyler, for her comments regarding the methods used for speciation of Nocardia isolates. 49.4 * Suggested Readings * See the CD-ROM for a complete list of references. 31. Clarridge, JE III , Zhang, Q: Genotypic diversity of clinical Actinomyces species: phenotype, source, and disease correlation among genospecies. J Clin Microbiol. 40, 2002, 3442–3448. 108. Pascual, C, Foster, G, Falsen, E, et al.: Actinomyces bowdenii sp. nov., isolated from canine and feline clinical specimens. Int J Syst Bacteriol. 49, 1999, 1873–1877. 116. Roth, A, Andrees, S, Kroppenstedt, RM, et al.: Phylogeny of the genus Nocardia based on reassessed 16S rRNA gene sequences reveals underspeciation and division of strains classified as Nocardia asteroides into three established species and two unnamed taxons. J Clin Microbiol. 41, 2003, 851–856. 124. Sivacolundhu, RK, O'Hara, AJ, Read, RA: Thoracic actinomycosis (arcanobacteriosis) or nocardiosis causing thoracic pyogranuloma formation in three dogs. Aust Vet J. 79, 2001, 398–402. 135. Walker, AL, Jang, SS, Hirsch, DC: Bacteria associated with pyothorax of dogs and cats: 98 cases,1989-1998. J Am Vet Med Assoc. 216, 2000, 359–363. CHAPTER 49 Actinomycosis and Nocardiosis Page 21 of 21










© Copyright 2026