
Document 141603
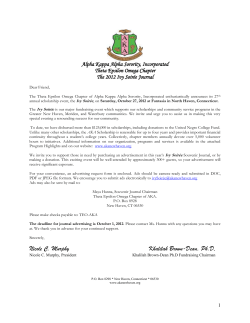
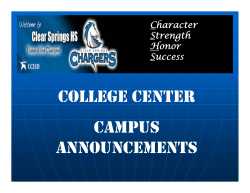
American Journal of Gastroenterology C 2008 by Am. Coll. of Gastroenterology Published by Blackwell Publishing ISSN 0002-9270 doi: 10.1111/j.1572-0241.2008.01955.x CME Liver Disease in Alpha 1-Antitrypsin Deficiency: A Review Kyrsten D. Fairbanks, M.D. and Anthony S. Tavill, M.D., F.A.C.P., F.R.C.P., F.A.C.G. Department of Gastroenterology and Hepatology, Cleveland Clinic Foundation, Cleveland, Ohio Alpha 1-antitrypsin deficiency is an inherited metabolic disorder that predisposes the affected individual to chronic pulmonary disease, in addition to chronic liver disease, cirrhosis, and hepatocellular carcinoma. Just over one-third of genetically susceptible adult patients with the most severe phenotype, PiZZ, develop clinically significant liver injury. The clinical presentation of liver disease is variable, and the genetic and environmental factors that predispose some individuals to liver disease while sparing others are unknown. The mechanisms of liver and lung disease are distinct and unique. This article reviews the liver disease associated with alpha 1-antitrypsin deficiency, emphasizing the genetic defect, molecular pathogenesis, natural history, and promising therapies. (Am J Gastroenterol 2008;103:2136–2141) INTRODUCTION Alpha 1-antitrypsin deficiency is an inherited metabolic disorder in which mutations in the coding sequence of the serine protease inhibitor, alpha 1-antitrypsin, prevent its export from the hepatocyte. As a result, there is a deficiency in the concentration of circulating alpha 1-antitrypsin, predisposing to early-onset panlobular emphysema, even in nonsmokers (1). In addition, the abnormal accumulation of the glycoprotein in hepatocytes results in programmed cell death, hepatic inflammation, fibrosis, and cirrhosis. Histopathologic examination of liver specimens from patients with alpha 1-antitrypsin deficiency demonstrates the classic intracellular globules that stain positive with periodic acid-Schiff (PAS) after treatment with diastase (Fig. 1). These globules represent polymerized mutant protein retained in the rough endoplasmic reticulum. The aim of this article is to review the liver disease associated with alpha 1-antitrypsin deficiency, with emphasis on the genetic defect, molecular pathogenesis, natural history, and promising therapies. For a recent review of lung disease associated with alpha 1-antitrypsin deficiency, refer to Stoller and Aboussouan (2). GENETICS AND EPIDEMIOLOGY The gene for alpha 1-antitrypsin is located on the long arm of chromosome 14, and has been mapped to 14q31–32 (3). Alpha 1-antitrypsin deficiency is inherited as an autosomal recessive disorder with codominant expression, as each allele contributes 50% of the total circulating enzyme inhibitor. To date, more than 100 alleles have been identified (4), only some of which are associated with liver disease. Phenotypes are classified based on migration of the protein product in gel electrophoresis, and these define the allelic genotypes. Disease states are associated with mutations in the normal To access a continuing medical education exam for this article, please visit www.acg.gi.org/journalcme. gene product, designated PiM, giving rise to the most common deficiency variants PiS (expressing 50–60% of alpha 1-antitrypsin, as defined by immunoassay or nephelometry) and PiZ (expressing 10–20% of alpha 1-antitrypsin). Among whites, the most common allele, M, accounts for 95% of alleles, while S and Z account for 2–3% and 1% of alleles, respectively. The most prevalent carrier phenotypes are PiMS and PiMZ, and deficiency phenotypes are PiSS, PiSZ, and PiZZ. Rare deficiency alleles, accounting for <5% of Pi variants in patients with alpha 1-antitrypsin deficiency, include Mmalton, Mduarte, and null, among others. In general, these alleles contribute 0–15% of normal concentration of alpha 1-antitrypsin. Both Mmalton and Mduarte are associated with liver inclusions and clinically apparent liver disease (5). The null phenotype occurs as a result of various mutations, such as stop codons in coding exons of the alpha 1-antitrypsin gene, or complete deletion of alpha 1-antitrypsin coding exons, and leads to the absence of any alpha 1-antitrypsin production (6). The latter is therefore not associated with liver cell inclusions or liver disease, but can lead to pulmonary manifestations. Severe alpha 1-antitrypsin deficiency (PiZZ) is found in approximately 1:3500 live births, and has been described in all races (7–9). It is, however, most commonly a disease of whites, as the most prevalent deficiency alleles, Z and S, are overwhelmingly derived from Northern European ancestry (Z and S alleles), and some Southern European ancestry (S allele). Although it has been described in all races, the frequency of PiZ varies greatly, being extremely rare in Asian and Mexican Americans, uncommon in Black Americans (2.6 per 1,000), and more common in Hispanic (9.1 per 1,000) and White Americans (14.0 per 1,000) (10). DIAGNOSIS The diagnosis of alpha 1-antitrypsin deficiency is confirmed solely on laboratory assays. There are several laboratory methods available for testing alpha 1-antitrypsin deficiency, 2136 Liver Disease in Alpha 1-Antitrypsin Deficiency 2137 alone cannot distinguish a homozygous deficiency state from a heterozygous allele paired with a null allele. Diagnosis at a molecular level, by genotyping, provides definitive diagnosis of specific known phenotypic variations. It also may identify suspected new mutations. Commercial kits are available to detect the most common S and Z alleles. The task force of the American Thoracic Society and the European Respiratory Society determined that phenotyping by isoelectric focusing is the accepted “gold standard” for the diagnosis of alpha 1-antitrypsin deficiency (12). MOLECULAR PATHOGENESIS Figure 1. Liver biopsy photomicrographs from a 31-yr-old male with PiZZ alpha 1-antitrypsin deficiency showing periodic acidSchiff-positive diastase resistant globules (A) confirmed by immunoperoxidase staining, magnification ×128 (B) in hepatocyte cytoplasm, consistent with retained alpha 1-antitrypsin-Z molecules, magnification ×128. including quantification of the enzyme inhibitor, phenotyping, and genotyping. Serum alpha 1-antitrypsin concentration is usually measured by nephelometry, which is replacing the older immunoassays. Alpha 1-antitrypsin is an acute phase protein; that is, its synthesis and release from the hepatocyte is augmented by systemic inflammation. Levels may be thereby transiently elevated and falsely reassuring in some heterozygous individuals. However, levels of alpha 1-antitrypsin in the PiZZ homozygous individual would rarely, if ever, reach a value that would obscure a deficiency state. Low serum concentrations of alpha 1-antitrypsin have some correlation with the risk of pulmonary emphysema, whereby the risk rises below a threshold level of 11 micromolar (570–800 µg/mL, 57–80 mg/dL) (11). Although concentration assays are readily commercially available, protease inhibitor levels alone should not be used to exclude alpha 1-antitrypsin deficiency, as they lack both sensitivity and specificity. Phenotype is defined by isoelectric focusing migration patterns, whereby each alpha 1-antitrypsin isoform migrates to an electroneutral position in polyacrylamide gel. While phenotyping can identify both common and rare alleles, the assay is time-consuming and not readily commercially available. In addition, results may be challenging to interpret. Phenotyping Alpha 1-antitrypsin is a glycoprotein produced predominantly in the hepatocyte, and to a lesser extent by other tissues, including macrophages, renal tubular, and small intestinal epithelial cells (13). It functions as a serine protease inhibitor, and is the predominant inhibitor of neutrophil elastase. Alpha 1-antitrypsin, as is true for other proteins in the serpin family of protease inhibitors, undergoes marked conformational change when it encounters its protease. Inhibition of elastase is a multistep process beginning with its docking in the reactive center of alpha 1-antitrypsin. Elastase then cleaves the reactive center of alpha 1-antitrypsin. This allows marked tertiary structural change in alpha 1-antitrypsin, which irreversibly inhibits elastase by destroying its structural integrity and thereby promotes its degradation. A single amino acid substitution of lysine for glutamate at position 342 in the coding sequence produces the most common alpha 1-antitrypsin mutant molecule, PiZ (14). Mutation in the coding sequence promotes spontaneous polymerization in the hepatocyte through insertion of the reactive center of one protein into the β-sheet of another, known as “loop-sheet” insertion (15). Polymers of alpha 1-antitrypsin protein in the endoplasmic reticulum of the hepatocyte are unable to complete the remainder of the secretory pathway necessary for secretion from the cell. The S allele, either in the homozygous state or when coinherited with the M allele, is not associated with liver disease, as the kinetics of protein production, degradation, and cellular export promote intracellular protein retention but a lesser degree of glycoprotein polymerization. However, if the S and Z alleles are coinherited, the protein product will form polymers that are retained intracellularly, and result in the clinical predisposition to liver disease. The rate of polymerization of the S protein is much slower than that of the Z protein, which favors less hepatocyte retention and milder serum deficiency when the mutant alleles are combined (16–18). Protein accumulation in the hepatocyte reflects the relative contributions of synthesis, intracellular degradation, and cellular export. There are at least two pathways responsible for degradation of mutant alpha 1-antitrypsin in the endoplasmic reticulum. One pathway involves binding of alpha 1-antitrypsin to the transmembrane endoplasmic reticulum chaperone calnexin, and subsequent binding of ubiquitin to 2138 Fairbanks and Tavill the complex, followed by degradation (19). The other pathway involves ubiquitin-independent proteosomal and nonproteosomal mechanisms, such as autophagy (20). Approximately 37% of adult PiZZ patients have cirrhosis at the time of death (21, 22). This suggests that other environmental and/or genetic traits predispose some patients to liver injury while sparing others. A delay in intracellular degradation of the mutant protein, rather than its accumulation in the endoplasmic reticulum, appears to be one physiologic trait that separates the unaffected from the susceptible host. It has been hypothesized that this lag in degradation may be as a result of abnormalities in calnexin, a protein that interacts with the mutant alpha 1-antitrypsin protein in the endoplasmic reticulum, and may be necessary for initiating or maintaining the pathway of endoplasmic reticulum degradation (23). The mechanisms of lung and liver injury are distinct and unique. Lung injury occurs as a result of deficiency in the concentration of circulating alpha 1-antitrypsin, allowing uninhibited proteolytic damage to the connective tissue of the lung. While lung injury may be thought of as a result of “loss of function,” liver disease occurs because of “gain of function.” While this may be a misnomer in so far that amplification of intracellular serine protease binding has not been implicated, the retained alpha 1-antitrypsin glycoprotein in the endoplasmic reticulum contributes directly to liver injury. CLINICAL PRESENTATION Alpha 1-antitrypsin deficiency is the most common genetic cause of liver disease in neonates and children (10). Adults with alpha 1-antitrypsin deficiency may present with asymptomatic abnormal liver enzymes indistinguishable from other common causes of abnormal enzymes, clinical manifestations of advanced cirrhosis, or hepatocellular carcinoma. The clinical presentation of liver disease in PiZZ alpha 1-antitrypsin-deficient persons is variable. There is a distinct bimodal distribution consisting of neonatal hepatitis and cholestatic jaundice in infants, and chronic liver disease in adults with mean age of diagnosis in the fifth decade. Only 10% of alpha 1-antitrypsin-deficient neonates develop neonatal hepatitis, the majority of whom clinically recover. Only 2–3% of PiZZ children progress to advanced fibrosis or cirrhosis requiring transplantation during childhood (24). By early adulthood, most patients have normal liver enzymes and minimal or no symptoms of liver disease (10, 25). Autopsy studies, however, have demonstrated that just over onethird of adult PiZZ patients (predominantly males) may develop cirrhosis (21, 22). Interestingly, these were significantly older than the noncirrhotics, leading the authors to speculate that the latter may have succumbed at an earlier age because of more advanced lung disease. Survival following diagnosis of cirrhosis was very limited with 30% having primary liver cancer at autopsy (22). The genetic and environmental factors that predispose some patients to liver disease while Figure 2. Percentage of PiZ individuals with abnormal liver enzymes over time; figure derived from data in reference 25. sparing others are unknown. One retrospective cohort study reported that both male gender and elevated mean body mass index were associated with more advanced liver disease (26). Whether gender predilection reflects differences in hormonal milieu or prevalence of confounding hepatotoxins such as alcohol, is unclear. A population-based cohort study from Sweden reported a strong correlation between alpha 1-antitrypsin deficiency and both cirrhosis and primary liver cancer, significant only for men (21). Studies using the PiZ mouse model of alpha 1-antitryspin deficiency have demonstrated increased hepatocellular proliferation restricted to male mice or to female mice administered exogenous testosterone (18). The only prospective study of the natural history of the liver disease of alpha 1-antitrypsin deficiency comes from a Swedish registry of 200,000 infants born between 1972 and 1974 who were screened for alpha 1-antitrypsin deficiency. One hundred twenty-two infants were deficient (120 PiZZ and 2 PiZnull). During the first 6 months of life, cholestasis occurred in 14/122 (11%) of PiZ infants, and 8/122 (6%) had clinical manifestations of liver disease, such as hepatosplenomegaly, late umbilical stump bleeding, or failure to gain weight (8). Approximately 50% of clinically well PiZ infants had abnormal liver enzymes in the neonatal period. In early childhood, two died of cirrhosis, and two died of unrelated causes with liver fibrosis noted at autopsy. Children were followed for clinical or biochemical signs of liver disease, and were last reported at the age of 18 yr (25). No surviving patient manifested any clinical sign of liver disease, and fewer than 10% had abnormal liver enzymes, supporting an excellent prognosis of alpha 1-antitrypsin PiZ during childhood and adolescence (Fig. 2). Cirrhosis resulting from alpha 1-antitrypsin deficiency is an established risk factor for hepatocellular carcinoma. Studies using the PiZ mouse model have demonstrated that the fraction of proliferating hepatocytes is limited almost entirely to cells devoid of PAS-positive globules (27), suggesting a proliferative advantage to cells without significant retained alpha 1-antitrypsin. This has led to the hypothesis that older cells, which have accumulated mutant alpha 1-antitrypsin glycoprotein, stimulate younger cells with a proliferative advantage to divide (28). Hepatocellular adenomas and carcinomas arise as a result of accumulated genetic mutations in stimulated and dividing cells residing in a background Liver Disease in Alpha 1-Antitrypsin Deficiency of chronic inflammation. This paradigm is consistent with the clinical observation that hepatocellular carcinomas in patients with alpha 1-antitryspin deficiency arise specifically in regions of the liver lacking cytoplasmic globules. The association between heterozygosity of alpha 1antitrypsin deficiency alleles and risk of developing chronic liver disease is controversial. A single-center study of all adult patients undergoing orthotopic liver transplantation found an increased prevalence of the PiMZ phenotype among all etiologic subgroups of chronic liver disease except cholestatic diseases. Patients with cryptogenic cirrhosis had an almost 10-fold increase in PiMZ phenotype, while patients with viral, alcoholic, or autoimmune disease had between two- and fourfold higher prevalence than estimates for the general population (29). Other investigators have found a significant increased prevalence of heterozygous alpha 1-antitrypsin in patients with cirrhosis (30, 31). However, this association is not universally accepted (32). While the PiMZ phenotype may confer some increased risk for the development of chronic liver disease, neither the PiMS nor PiSS phenotypes have any direct correlation with liver disease (18, 29). Primary liver cancer in liver disease typically develops in patients with well-established cirrhosis. However, this paradigm does not always hold true for patients with underlying alpha 1-antitrypsin deficiency states. Cholangiocarcinoma and combined hepatocholangiocarcinoma have an increased incidence in patients with alpha 1-antitrypsin deficiency type PiZ. Moreover, these cancers are often found in patients who have no fibrosis or varying stages of fibrosis, which fall short of cirrhosis, and in patients with heterozygous mutations without alternative concurrent liver diseases (33, 34). The development of pulmonary function impairment in PiZ patients is extremely variable, although cigarette smoking has been clearly shown to adversely affect lung function. Many PiZ patients have no clinically significant pulmonary disease even into late middle age (35). In addition to pulmonary and liver disease, alpha 1-antitrypsin deficiency has been associated with systemic vasculitis (36), interstitial fibrosis in patients with rheumatoid arthritis (37), relapsing panniculitis (38), multiple sclerosis (39), peripheral neuropathy (40), and intracranial aneurysms (41). TREATMENT There is currently no approved treatment for the liver disease associated with alpha 1-antitrypsin deficiency short of liver transplantation. Patients with emphysema resulting from alpha 1-antitrypsin deficiency may be treated with intravenous purified pooled human plasma alpha 1-antitrypsin, otherwise known as augmentation therapy (42). Augmentation therapy has been shown to have biochemical efficacy (i.e., raising serum levels of alpha 1-antitrypsin above a protective threshold), although evidence for clinical efficacy (i.e., decreasing rate of decline of FEV1 [forced expiratory volume in 1 2139 second]) is less robust (2). Reduced serum concentration of alpha 1-antitrypsin does not contribute to liver injury, and augmentation therapy is not considered a potential treatment option for liver disease. Promising experimental work using adenovirus-associated, recombinant gene therapy has demonstrated successful gene transfer to peripheral skeletal muscle with sustained therapeutic secretion of alpha 1-antitrypsin into serum (43). Gene augmentation strategies such as this would be expected to ameliorate lung disease while having little, if any, impact on liver disease. Treatment strategies for liver disease may be divided into therapies that prevent protein polymerization, decrease liver injury, enhance secretion of the mutant protein, or increase its intracellular, hepatic degradation. The molecular requirements for a peptide that could selectively block polymerization of mutant alpha 1-antitrypsin proteins have been defined (44), but this has not yet translated into clinical practice. Cyclosporin A has been shown to reduce hepatic mitochondrial injury, even in the presence of accumulated mutant alpha 1-antitrypsin protein (45). The chemical chaperone phenylbutyric acid enhances secretion of functionally active alpha 1-antitrypsin in cell culture and mouse models without affecting synthesis or degradation (46). However, a single study in humans showed no increase in serum levels of alpha 1-antitrypsin with 14 days of phenylbutyric acid treatment, and significant side effects (47). While the glucosidase inhibitor castanospermine and the mannosidase inhibitors kifunensine and deoxymannojirimycin all mediate increased secretion of functionally active alpha 1-antitrypsin in cell culture, the latter two are less promising, as they are associated with markedly decreased degradation of alpha 1antitrypsin (48). Theoretically, at least, these mannosidase inhibitors may ameliorate lung injury while permitting liver damage to continue unchecked. Recent gene therapy studies using small-interfering RNAs have demonstrated the ability to downregulate endogenous Z-alpha 1-antitrypsin through delivery of anti-alpha 1-antitrypsin ribozymes, resulting in decreased secretion of mutant alpha 1-antitrypsin and decrease in intracellular accumulation. To date, these studies have been limited to cell culture and transgenic mice models (49). For patients who develop decompensated cirrhosis or early-stage hepatocellular carcinoma, liver transplantation both replaces the diseased liver and corrects the underlying metabolic disorder. In pediatric transplant centers, liver transplantation for metabolic liver disease is second only to biliary atresia as the most common indication for transplant. Alpha 1-antitrypsin deficiency is the primary metabolic liver disease leading to a transplant in the pediatric age group (50). Overall outcomes after liver transplantation are excellent in children, with 3-yr survival rates approaching 85% (51). Prognostic variables associated with poor outcome without a liver transplant in childhood include jaundice persisting for more than 6 wk, higher aminotransferases at presentation, and severe bile duct proliferation and stage of fibrosis on liver histology (52). While children with alpha 1-antitrypsin deficiency 2140 Fairbanks and Tavill often present with jaundice as a predominant feature, adults typically come to medical attention because of complications of portal hypertension or early onset obstructive lung disease. Alpha 1-antitrypsin deficiency is a rare indication for liver transplantation among adults. Transplant recipients acquire the donor phenotype and have normalization of alpha 1-antitrypsin levels (53). Despite this, it is not known if liver transplantation can delay the onset or progression of lung disease. Both graft and patient survival for adults transplanted for metabolic liver disease is similar to that of other indications for liver transplant (54). CONCLUSION Alpha 1-antitrypsin deficiency is a chronic underrecognized metabolic disease that causes significant liver and lung injury. Since the initial description more than 40 yr ago of the absence of the alpha-1 band on serum protein electrophoresis (55), and subsequent recognition of the association between the alpha 1-antitrypsin deficiency state and liver disease (56), remarkable progress has been made in understanding its clinical course and molecular basis for disease. ACKNOWLEDGMENT We gratefully acknowledge Dr. Mary Petrelli for the original photomicrographs of the liver biopsy. Reprint requests and correspondence: Kyrsten D. Fairbanks, M.D., Department of Gastroenterology and Hepatology, Cleveland Clinic Foundation, Cleveland, OH 44195. Received November 1, 2007; accepted March 11, 2008. REFERENCES 1. Black LF, Kueppers F. Alpha 1-antitrypsin deficiency in nonsmokers. Am Rev Respir Dis 1978;117:421–8. 2. Stoller JK, Aboussouan LS. Alpha 1-antitrypsin deficiency. Lancet 2005;365:2225–36. 3. Darlington GJ, Astrin KH, Muirhead SP, et al. Assignment of human alpha 1-antitrypsin to chromosome 14 by somatic cell hybrid analysis. Proc Natl Acad Sci USA 1982;79:870– 3. 4. DeMeo DL, Silverman EK. Alpha 1-antitrypsin deficiency, 2: Genetic aspects of alpha 1-antitrypsin deficiency: Phenotypes and genetic modifiers of emphysema risk. Thorax 2004;59:259–64. 5. Cox DW, Billingsley GD. Rare deficiency types of alpha 1antitrypsin: Electrophoretic variation and DNA haplotypes. Am J Hum Genet 1989;44:844–54. 6. Brantly M, Nukiwa T, Crystal RG. Molecular basis of alpha 1-antitrypsin deficiency. Am J Med 1988;84(Suppl 6A):13– 31. 7. de Serres FJ. Worldwide racial and ethnic distribution of alpha1-antitrypsin deficiency: Summary of an analysis of published genetic epidemiologic surveys. Chest 2002;122:1818–29. 8. Sveger T. Liver disease in alpha1-antitrypsin deficiency detected by screening of 200000 infants. N Engl J Med 1976;294:1316–21. 9. Silverman EK, Miletich JP, Pierce JA, et al. Alpha 1antitrypsin deficiency: High prevalence in the St. Louis area determined by direct population screening. Am Rev Respir Dis 1989;140:961–6. 10. de Serres FJ, Blanco I, Fernandez-Bustillo E. Genetic epidemiology of alpha-1 antitrypsin deficiency in North America and Australia/New Zealand: Australia, Canada, New Zealand and the United States of America. Clin Genet 2003;64:382–97. 11. Crystal RG. The alpha 1-antitrypsin gene and its deficiency states. Trends Genet 1989;5:411–7. 12. American Thoracic Society/European Respiratory Society Statement. Standards for the diagnosis and management of individuals with alpha 1-antitrypsin deficiency. Am J Respir Crit Care Med 2003;168:818–900. 13. Carlson JA, Rogers BB, Sifers RN, et al. Multiple tissues express alpha 1-antitrypsin in transgenic mice and man. J Clin Invest 1988;82:26–36. 14. Jeppsson JO. Amino acid substitution Glu-Lys in alpha 1antitrypsin PiZ. FEBS Lett 1976;76:195–7. 15. Carrell RW, Lomas DA. Alpha 1-antitrypsin deficiencya model for conformational diseases. N Engl J Med 2002;346:45–53. 16. Mahadeva R, Chang W-SW, Dafforn TR, et al. Heteropolymerization of S, I, and Z alpha 1-antitrypsin and liver cirrhosis. J Clin Invest 1999;103:999–1006. 17. Lomas DA, Mahadeva R. Alpha 1-antitrypsin polymerization and the serpinopathies: Pathobiology and prospects for therapy. J Clin Invest 2002;110:1585–90. 18. Teckman JH, Qu D, Perlmutter DH. Molecular pathogenesis of liver disease in alpha 1-antitrypsin deficiency. Hepatology 1996;24:1504–16. 19. Qu D, Teckman JH, Omura S, et al. Degradation of a mutant secretory protein, alpha 1-antitrypsin Z, in the endoplasmic reticulum requires proteasome activity. J Biol Chem 1996;271:22791–5. 20. Teckman JH, Gilmore R, Perlmutter DH. Role of ubiquitin in proteasomal degradation of mutant alpha 1-antitrypsin Z in the endoplasmic reticulum. Am J Physiol Gastrointest Liver Physiol 2000;278:G39–48. 21. Eriksson S, Carlson J, Velez R. Risk of cirrhosis and primary liver cancer in alpha 1-antitrypsin deficiency. N Engl J Med 1986;314:736–9. 22. Eriksson S. Alpha 1-antitrypsin deficiency and liver cirrhosis in adults: An analysis of 35 Swedish autopsied cases. Acta Med Scand 1987;221:461–7. 23. Wu Y, Whitman I, Molmenti E, et al. A lag in intracellular degradation of mutant alpha 1-antitrypsin correlates with the liver disease phenotype in homozygous PiZZ alpha 1-antitrypsin deficiency. Proc Natl Acad Sci USA 1994;91:9014–18. 24. Sveger T. The natural history of liver disease in alpha 1-antitrypsin deficiency children. Acta Paediatr Scand 1988;77:847–51. 25. Sveger T, Eriksson S. The liver in adolescents with alpha 1-antitrypsin deficiency. Hepatology 1995;22:514–7. 26. Bowlus CL, Willner I, Zern MA, et al. Factors associated with advanced liver disease in adults with alpha 1-antitrypsin deficiency. Clin Gastroenterol Hepatol 2005;3:390–6. 27. Rudnick DA, Liao Y, An JK, et al. Analyses of hepatocellular proliferation in a mouse model of alpha 1-antitrypsin deficiency. Hepatology 2004;39:1048–55. 28. Rudnick DA, Perlmutter DH. Alpha 1-antitrypsin deficiency: A new paradigm for hepatocellular carcinoma in genetic liver disease. Hepatology 2005;42:514–21. 29. Graziadei IW, Joseph JJ, Wiesner RH, et al. Increased risk of chronic liver failure in adults with heterozygous Liver Disease in Alpha 1-Antitrypsin Deficiency 30. 31. 32. 33. 34. 35. 36. 37. 38. 39. 40. 41. 42. 43. 44. alpha 1-antitrypsin deficiency. Hepatology 1998;28:1058– 63. Hodges JR, Millward-Sadler GH, Barbatis C, et al. Heterozygous MZ alpha 1-antrtrypsin deficiency in adults with chronic active hepatitis and cryptogenic cirrhosis. N Engl J Med 1981;304:557–60. Carlson J, Eriksson S. Chronic “cryptogenic” liver disease and malignant hepatoma in intermediate alpha 1-antitrypsin deficiency identified by a Pi Z-specific monoclonal antibody. Scand J Gastroenterol 1985;20:835–42. Bell H, Schrumpf E, Fagerhol MK. Heterozygous MZ alpha 1-antitrypsin deficiency in adults with chronic liver disease. Scand J Gastroenterol 1990;25:788–92. Zhou H, Ortiz-Pallardo ME, Ko Y, et al. Is heterozygous alpha 1-antitrypsin deficiency type PiZ a risk factor for primary liver carcinoma? Cancer 2000;88:2668–76. Zhou H, Fischer HP. Liver carcinoma in PiZ alpha 1antitrypsin deficiency. Am J Surg Pathol 1998;22:742–8. Silverman EK, Pierce JA, Province MA, et al. Variability of pulmonary function in alpha 1-antitrypsin deficiency: Clinical correlates. Annals Intern Med 1989;11:982– 991. Patterson CC. Alpha 1-antitrypsin deficiency and HenochSch¨onlein purpura associated with anti-neutrophil cytoplasmic and anti-endothelial cell antibodies of immunoglobulinA isotype. J Cutan Pathol 2005;32:300–6. Michalski JP, McCombs CC, Scopelitis E, et al. Alpha 1antitrypsin phenotypes, including M subtypes, in pulmonary disease associated with rheumatoid arthritis and systemic sclerosis. Arthritis Rheum 1986;29:586–91. McBean J, Sable A, Maude J, et al. Alpha 1-antitrypsin deficiency panniculitis. Cutis 2003;71:205–9. Lolin YI, Ward AM. Alpha 1-antitrypsin phenotypes and associated disease patterns in neurological patients. Acta Neurol Scand 1995;91:394–8. Frederick WG, Enriquez R, Bookbinder MJ. Peripheral neuropathy associated with alpha 1-antitrypsin deficiency. Arch Neurol 1990;47:233–5. Schievink WI, Puumala MR, Meyer FB, et al. Giant intracranial aneurysm and fibromuscular dysplasia in an adolescent with alpha 1-antitrypsin deficiency. J Neurosurg 1996;85:503–6. Wewers MD, Casolaro MA, Sellers SE, et al. Replacement therapy for alpha 1-antitrypsin deficiency associated with emphysema. NEJM 1987;316:1055–62. Song S, Morgan M, Ellis T, et al. Sustained secretion of human alpha 1-antitrypsin from murine muscle transduced with adeno-associated virus vectors. Proc Natl Acad Sci 1998;95:14384–8. Zhou A, Stein PE, Huntington JA, et al. How small peptides block and reverse serpin polymerization. J Mol Biol 2004;342:931–41. 2141 45. Perlmutter DH. Liver injury in alpha 1-antitrypsin deficiency: An aggregated protein induces mitochondrial injury. J Clin Invest 2002;110:1579–83. 46. Burrows JA, Willis LK, Perlmutter DH. Chemical chaperones mediate increased secretion of mutant alpha 1antitrypsin (alpha 1-AT) Z: A potential pharmacological strategy for prevention of liver injury and emphysema in alpha 1-AT deficiency. Proc Natl Acad Sci 2000;97:1796– 1801. 47. Teckman JH. Lack of effect of oral 4-phenylbutyrate on serum alpha 1-antitrypsin in patients with alpha 1antitrypsin deficiency: A preliminary study. J Pediatr Gastroenterol Nutr 2004;39:34–7. 48. Marcus NY, Perlmutter DH. Glucosidase and mannosidase inhibitors mediate increased secretion of mutant alpha 1antitrypsin Z. J Biol Chem 2000;275:1987–92. 49. Cruz PE, Mueller C, Cossette TL, et al. In vivo posttranscriptional gene silencing of alpha 1-antitrypsin by adeno-associated virus vectors expressing siRNA. Lab Invest 2007;87:893–902. 50. Esquivel CO, Iwatsuki S, Gordon RD, et al. Indications for pediatric liver transplantation. J Pediatr 1987;111:1039–45. 51. Prachalias AA, Kalife M, Francavilla R, et al. Liver transplantation for alpha 1-antitrypsin deficiency in children. Transpl Int 2000;13:207–10. 52. Francavilla R, Castellaneta SP, Hadzic N, et al. Prognosis of alpha 1-antitrypsin deficiency-related liver disease in the era of paediatric liver transplantation. J Hepatol 2000;32:986– 92. 53. Hood JM, Koep LJ, Peters RL, et al. Liver transplantation for advanced liver disease with alpha 1-antitrypsin deficiency. New Engl J Med 1980;302:272–5. 54. Zhang KY, Tung BY, Kowdley KV. Liver transplantation for metabolic liver disease. Clin Liver Dis 2007;11:265–81. 55. Laurell CB, Eriksson S. The electrophoretic alpha 1 globulin pattern of serum in alpha 1-antitrypsin deficiency. Scand J Clin Lab Invest 1963;15:132–40. 56. Sharp HL, Bridges RA, Krivit W, et al. Cirrhosis associated with alpha 1-antitrypsin deficiency: A previously unrecognized inherited disorder. J Lab Clin Med 1969;73:934–9. CONFLICT OF INTEREST Guarantor of the article: Kyrsten Fairbanks, M.D. Specific author contributions: Kyrsten Fairbanks wrote and edited the article. Anthony Tavill provided guidance in the writing and editing of the article. Financial support: None. Potential competing interests: None.









© Copyright 2026