
Initial presentation of stasis dermatitis mimicking solitary lesions: A previously unrecognized
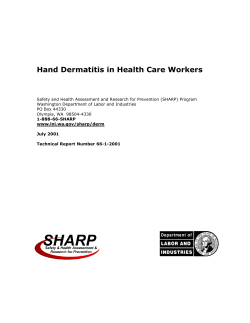
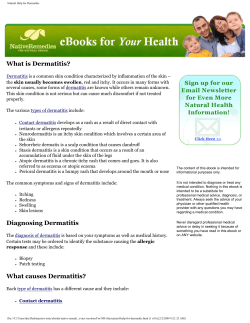
Initial presentation of stasis dermatitis mimicking solitary lesions: A previously unrecognized clinical scenario Joshua Weaver, MD,a and Steven D. Billings, MDa,b Cleveland, Ohio Background: Stasis dermatitis is a common skin condition secondary to chronic venous insufficiency. Characteristic dermatologic changes in well-developed disease include bilateral erythematous, scaly, and slightly discolored papules and plaques on the lower legs. Earlier signs, such as prominent superficial veins and pitting ankle edema, are well known. Early recognition of signs and appropriate diagnosis can lead to timely treatment that can prevent painful complications, such as leg ulcers which are at risk for development of squamous cell carcinoma. Objective: Herein we describe a yet unrecognized early sign of venous dermatitis—a solitary lesion, some mimicking neoplastic processes. Methods: Thirty-seven cases of stasis dermatitis submitted with the clinical diagnosis of a solitary lesion were identified. Thirty-three had no clinical history of venous insufficiency. All cases of stasis dermatitis presenting for the first time as a solitary lesion were reviewed retrospectively both clinically and pathologically. Results: Squamous cell carcinoma was most commonly suspected (33%), followed by basal cell carcinoma (24%), and a variety of other solitary lesions. The histopathology was characteristic of stasis dermatitis in all cases with absent or mild spongiosis (82%), variable acanthosis and dermal fibrosis, and proliferation of papillary dermal thick-walled vessels were prominent (2-3+) in nearly all cases ( $ 90%) along with hemosiderin-laden macrophages and extravasated red blood cells ( $ 95%). Limitations: The study is limited by its retrospective nature and absence of clinical images on all cases. Conclusion: Stasis dermatitis may present as a solitary lesion mimicking a neoplasm. Early recognition of stasis dermatitis can lead to appropriate treatment and possibly prevent further morbidity. ( J Am Acad Dermatol 2009;61:1028-32.) INTRODUCTION S tasis dermatitis is a cutaneous manifestation and marker of increased venous pressure of the lower extremities. It is a common condition affecting predominantly middle-aged to elderly From the Departments of Anatomic Pathologya and Dermatology,b Cleveland Clinic. Funding sources: None. Conflicts of interest: None declared. A portion of this work was presented at the 45th Annual Meeting of the American Society of Dermatopathology in San Francisco, CA. Reprint requests: Steven D. Billings, MD, Department of Anatomic Pathology/L25, The Cleveland Clinic. 9500 Euclid Ave, Cleveland, OH 44195. E-mail: [email protected]. 0190-9622/$36.00 ª 2009 by the American Academy of Dermatology, Inc. doi:10.1016/j.jaad.2009.04.025 1028 Abbreviations used: H&E: hematoxylin-eosin (stain) PAS: periodic acideSchiff individuals that usually presents as erythematous, slightly yellow to brown pigmented patches over the bilateral lower legs with or without conspicuous varicose veins. Most cases are caused by insufficient deep venous system valves preventing proper return of blood to the central circulation through the muscular pumping action of the lower legs. Venous valvular insufficiency can be caused by prior thrombophlebitis or congenital fragility. Pregnancy, obesity, and other causes of increased abdominal pressure can also lead to chronic venous insufficiency. Weaver and Billings 1029 J AM ACAD DERMATOL VOLUME 61, NUMBER 6 Stasis dermatitis can be associated with signifisolitary lesion and in some cases mimicking a neocant complications. Long-standing stasis dermatitis plastic process. accounts for approximately half of chronic leg ulcers.1 Chronic venous leg ulcers lead to significant METHODS decreases in the quality of these patients’ lives A computerized search through the pathology through physical pain, negative emotions, and archives at the Cleveland Clinic was performed monetary loss.2 Development of squamous cell using the keywords ‘‘stasis dermatitis’’ in the diagcarcinoma in long-standing nosis field between Jan 1, chronic venous ulcers is 1992 (time when clinical CAPSULE SUMMARY another risk that patients data from the pathology reqwith stasis dermatitis face. uisition form were added to Stasis dermatitis can commonly (7%) Therefore diagnosis of stasis the database) and March 25, manifest early as a solitary lesion before dermatitis early in the pro2008. All electronic and more typical clinical diagnostic changes cess is important as it may physical clinical charts were develop. allow for earlier intervention available for review docuThese solitary lesions most commonly to potentially prevent these menting at the initial visit: clinically mimic neoplasms, including complications. presence or absence of a SCC (33%) and BCC (24%). Although most cases are history of stasis dermatitis, diagnosed clinically through presence or absence of a The histopathology of stasis dermatitis history and physical findhistory of another concurconsists predominantly of dermal ings, a biopsy is often emrent or metachronous eczechanges including lobular proliferation ployed if there is no clear matous process, evidence of of thick-walled papillary dermal blood history and physical findings pedal edema on physical vessels with evidence of dermal are atypical. Histologically, examination, symptoms of hemorrhage. Epidermal changes are stasis dermatitis demondependent ankle swelling usually mild. strates a lobular proliferation during prolonged standing, Early recognition of this clinical scenario of thick-walled blood vesclinical presentation and deof stasis dermatitis initially presenting as sels in the papillary dermis scription of the lesion, age, a solitary lesion can lead to appropriate with a variable proportion of sex, and the clinical differtreatment and prevent further morbidity. other features including exential diagnosis. Available travasated red blood cells, follow-up information hemosiderin-laden macrophages, and dermal fibrothrough the electronic and physical clinical charts sis.3 The variation of dermal changes is thought to was reviewed to document the development of be related to the age of the lesion with prominent classic broader patches of stasis dermatitis. For fibrosis and siderophages in long-standing disease. inclusion in the study, the cases had to clinically The distribution of siderophages can help distinpresent as a solitary lesion, and the patient could guish stasis dermatitis from pigmented purpuric not have an already established diagnosis of stasis dermatosis, with the macrophages present throughdermatitis or chronic vascular insufficiency. out the dermis in the former, but only in the upper Cases meeting the selection criteria were reviewed one third of the dermis in the latter.3 Variable for histological changes including the degree of changes of the epidermis occur as well, such as acanthosis, spongiosis, parakeratosis, proliferation spongiosis, parakeratosis, and development of a of vessels, dermal fibrosis, presence of hemosiderincrust. The variation of these changes depend on laden macrophages, thickness of vessels, and hemorwhether there is an overlying eczematous dermarhage based on a scale from +1 to +3 (mild, moderate, titis thought to be caused by the oversensitive or severe). Additionally, the presence or absence of nature of the skin in stasis dermatitis—so-called spongiotic vesicle and crust formation was noted. Any ‘‘autoeczematization’’. available additional special stains (eg, Gomori methThe initial stage of venous insufficiency is cusenamine silver) and recuts were also reviewed. In tomarily edema of the lower legs. However, we have addition, two deeper hematoxylin-eosinestained noted many cases of stasis dermatitis on skin biopsy (H&E) sections were performed to rule out possible specimens submitted with differential diagnoses previously unrecognized preneoplastic/neoplastic consistent with a solitary disease process. Herein processes left in the paraffin block that could otherwe report a series of cases describing a previously wise explain the presence of a solitary lesion. undocumented phenomenon of stasis dermatitis Furthermore, all cases with H&E findings of intraeppresenting in an initial evaluation clinically as a idermal neutrophils, intraepidermal lymphocytes, or d d d d 1030 Weaver and Billings J AM ACAD DERMATOL DECEMBER 2009 Table I. Demographics, clinical features, and diagnosis Patient No. Sex Age (y) Clinical morphologic description (if available) 1 2 3 4 5 6 F F F F M F 59 42 49 67 61 59 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27 28 29 30 31 32 33 M M M F F F F F F M F M F F F M F M F F F F M F M M M 64 79 76 52 64 82 89 77 60 57 53 87 75 57 66 64 78 74 84 68 79 66 46 76 56 61 65 15-mm scaly plaque w/ central erosion on R lower leg 12-mm scaly nummular patch on L pretibial area 7-mm scaly erythematous papule on L pretibial area 9-mm erythematous atrophic plaque w/ smooth surface on R medial malleolus Erythematous red firm papule on L lower leg 2-cm erythematous atrophic plaque w/ minimal circumferential scale w/ adjacent hypopigmented scar on R pretibial leg 7-mm erythematous scaly patch on L medial lower leg Small flesh-colored flat plaque on R leg Thick keratotic area on lower leg 8-mm erythematous scaly papule on R mid anterior pretibial leg 6-cm ulcer with surrounding mild erythema on R lower anterior leg Not available L posterior leg ulcer Erythematous papule on R lower leg 8-mm erythematous scaly irregular plaque on R lateral calf 1-cm lesion w/ central erosion on L leg 2-cm, somewhat eczematous, erythematous irregular patch on L pretibial area Erythematous plaque w/ ulceration on R lower leg 13-mm erythematous shallow plaque on L pretibial leg Not available 3-cm shiny atrophic plaque, slightly hypopigmented on L pretibial leg Not available Erythematous scaly plaque on L lateral calf Not available 2.3-cm violaceous crusted plaque on L medial ankle Not available Not available 2-cm erythematous plaque w/ scale on R lower leg Erythematous plaque with central ulceration and crust on R lower leg Not available Not available 5-mm papule on L ankle 18-mm firm erythematous scaly nodule on L lower leg Clinical diagnosis ISK SCC BCC ISK GA Scar ISK BCC SCC BCC PG GA SCC SCC SCC Nevus BCC SCC GA BCC Scar Kaposi sarcoma BCC AK SCC BCC SCC BCC PG SCC Scar SCC SCC AK, Actinic keratosis; BCC, basal cell carcinoma; F, female; GA, granuloma annulare; ISK, irritated seborrheic keratosis; L, left; M, male; PG, pyoderma gangrenosum; R, right; SCC, squamous cell carcinoma. impetiginized serum crust were evaluated with a periodic acideSchiff stain, if fungal stains were not performed during initial evaluation, in order to rule out the possibility of superficial dermatophytosis. The study was approved by the institutional review board of the Cleveland Clinic. RESULTS The initial query identified 483 cases with the primary diagnosis of stasis dermatitis. Of the initial 483 cases, 37 patients presented with a clinical diagnosis of a solitary lesion. Four patients with a history of chronic venous insufficiency were excluded from the study, leaving 33 cases for the study, representing 7% of all cases of stasis dermatitis (Table I). None of the remaining 33 patients had history of a previously diagnosed nummular eczema or irritant dermatitis prior to the biopsy of the lower leg solitary lesion. Demographically, this under-recognized event occurred in the usual setting for stasis dermatitis: the lower extremities of older adults (average age, 66 years-old), with a female predominance (female:male, 1.8). Eleven cases (33%) had evidence of pedal edema on initial physical examination; however, only 3 patients (9%) were elicited to describe symptoms of ankle swelling after prolonged standing. Detailed clinical descriptions were available on a subset of cases (n = 29). The most common presentation was a single erythematous plaque on the lower portion of the leg, affecting either lower extremity with equal frequency (right:left, 0.8) (Fig 1). The exact location of the lesions on the lower legs could not be ascertained in the majority of cases due to the J AM ACAD DERMATOL Weaver and Billings 1031 VOLUME 61, NUMBER 6 Fig 1. The most common clinical presentation of stasis dermatitis mimicking a solitary lesion was a single erythematous plaque on the lower portion of either leg. lack of additional detail provided in the clinical notes during the retrospective chart reviews. Only 3 cases were specifically mentioned to have occurred on the medial malleolus, which is the classic location of the initial onset of stasis dermatitis; however, this number is likely an underestimation because of the limitations of this retrospective study. The average size of the lesion was 1.6 cm. Out of a total of 21 cases described as a papule, plaque, nodule, or patch; the most common presentation was a plaque (57%), followed by papule (24%), patch (14%), and nodule (5%). Fifty-six percent of cases presented with some erythema, 40% described scaling, while only 24% were eroded. The most common clinical diagnosis was squamous cell carcinoma (33%) followed by basal cell carcinoma (24%). Another 3 (9%) cases were thought clinically to be consistent with a granuloma annulare and another 3, irritated seborrheic keratosis. Other clinical differential diagnoses included scars, pyoderma gangrenosum, actinic keratosis, Kaposi’s sarcoma, nevus, and a neoplasm, not otherwise specified. The histopathology of all the cases demonstrated the classical morphologic picture of stasis dermatitis with variable acanthosis and mild spongiosis of the epidermis and underlying proliferation of thickwalled blood vessels in the papillary dermis with deposition of hemosiderin and extravasation of red blood cells (Fig 2). Spongiotic change in the epidermis was absent or mild (0 or 1+) in 27 cases (82%), and spongiotic vesicles were never demonstrated. Parakeratosis was present in roughly half of the cases (58%), which correlated with the clinical impression of a scale also approximately half of the time. A serum crust was only identified in 5 cases (15%). The characteristic lobular proliferation of thick-walled Fig 2. A, Skin biopsies of all cases demonstrated classical morphologic picture of stasis dermatitis with mild acanthosis and spongiosis of the epidermis and underlying proliferation of thick-walled blood vessels in papillary dermis. B, Evidence of hemorrhage including extravasated erythrocytes, hemosiderin deposition, and siderophages were essentially always present. (A and B, Hematoxylineosin stain; original magnifications: A, 3100; B, 3400.) blood vessels in the papillary dermis was always present; in the vast majority of the cases ([90%), this finding was moderate to marked (2-3+). Evidence of hemorrhage including extravasated erythrocytes, hemosiderin deposition, and siderophages were essentially always present ([95%). Some dermal fibrosis was present in all cases, but in variable proportions. All recuts or levels performed at the time of original diagnosis (n = 6; 18%) and all subsequent deeper levels performed (n = 33; 100%) showed similar histologic findings as the original H&E slides with no evidence of an additional process that could explain a localized lesion. Special stains (Gomori methenamine silver, PAS, Steiner, Gram, and Twort’s) for microorganisms were performed during the initial evaluation on 9 of the cases (27%). All were negative for fungal or bacterial organisms. Six cases required additional PAS stain for the histopathologic findings of intraepidermal neutrophils, intraepidermal lymphocytes, or impetiginized serum crust to rule out dermatophyte infection. None of the cases showed evidence of fungal forms on PAS stain. Only 1032 Weaver and Billings J AM ACAD DERMATOL DECEMBER 2009 one case had an iron stain performed, which was positive for hemosiderin within macrophages. Follow-up clinical data were available for 31 of 33 patients (94%) and demonstrated that 64% (14/22) of patients undergoing biopsy during 2004 and earlier developed classic broader patches of stasis dermatitis, whereas only 11% (1/9) of patients undergoing biopsy during 2005 and since have currently developed classic findings of stasis dermatitis. DISCUSSION Stasis dermatitis caused by chronic venous insufficiency is a common condition that affects older individuals. The diagnosis is typically straightforward and made on routine history and physical examination by identifying the usual dermatologic manifestations—pruritic bilateral scaly erythematous papules and plaques located on the lower third of the legs. Hyperpigmentation and hair loss may also be associated with the above findings. The hyperpigmentation is usually a yellow-brown discoloration thought to be secondary to the hemosiderin deposition from extravasated red blood cells which is then engulfed by dermal macrophages. In a minority of cases melanin in the form of dermal melanophages and melanocytes have been implicated in contributing to the hyperpigmentation of stasis dermatitis.4 The pigment incontinence may be explained by resolution of a concurrent eczematous process; so-called autoeczematization which has been described in this population. Initial signs before the characteristic lower leg skin changes include congestion and dilation of the saphenous vein with fibrosis and pitting edema of the medial aspect of the ankle and lower shins.5 Early diagnosis and appropriate treatment with compression therapy in combination with patient education can help prevent the development of painful and difficult-to-treat venous stasis ulcers and therefore decreases the risk of development of an ulcer-associated malignancy.6-9 Herein we have demonstrated the rare occurrence of stasis dermatitis presenting as a solitary lesion as an initial manifestation before more typical clinically diagnostic changes. This early manifestation of stasis dermatitis accounts for 7% of all cases of stasis dermatitis in our clinical material. Importantly, the patients had no history of chronic venous insufficiency; therefore the solitary lesion frequently mimicking a neoplasm was the initial presenting sign of disease. Interestingly, 64% of patients (14/22) with follow-up longer than 4 years had already progressed to a more definitive clinical picture with the development of classic broad patches of stasis dermatitis, whereas only 11% of patients (1/9) with less extensive follow-up had undergone the same process. These findings suggest that a relatively long (4 years) period of time is required for the solitary patch of stasis dermatitis to progress to a more definitive clinical picture. The remaining 8 patients without significant progression of their stasis dermatitis are most likely still at risk of developing a classic clinical picture of stasis dermatitis down the line. Therefore the evidence supports the findings that stasis dermatitis can initially present as a solitary lesion with or without other classic signs or symptoms of chronic venous insufficiency; furthermore a significant subset of these patients go on to develop more classic broad patches of typical stasis changes on their legs. As it is well-known that patients with a longstanding history of stasis dermatitis with associated ulcers are at risk of developing squamous cell carcinoma and rarely basal cell carcinoma,7-9 dermatologists and dermatopathologists should also be aware that stasis dermatitis may clinically mimic neoplasms. Furthermore, the histopathology of stasis dermatitis has not been extensively described in the literature. This series emphasizes that the dermal changes including the lobular proliferation of thick-walled papillary dermal blood vessels and evidence of dermal hemorrhage are the essential findings in stasis dermatitis. Epidermal changes are usually mild in the lesions clinically mimicking neoplasms. REFERENCES 1. James WD, Berger TG, Elston DM. Andrews’ Diseases of the skin clinical dermatology. 10th ed. Philadelphia: Saunders Elsevier; 2006. p. 845-7. 2. Phillips T, Stanton B, Provan A, Lew R. A study of the impact of leg ulcers on quality of life: financial, social, and psychologic implications. J Am Acad Dermatol 1994;31:49-53. 3. Weeden D. Skin pathology. 2nd ed. Edinburgh: Churchill Livingstone; 2002. p. 112. 4. Kim D, Kang WH. Role of dermal melanocytes in cutaneous pigmentation of stasis dermatitis: a histopathological study of 20 cases. J Korean Med Sci 2002;17:648-54. 5. Worley CA. ‘It hurts when I walk:’ venous stasis disease—differential diagnosis and treatment. Dermatol Nurs 2006;18:582-3. 6. Erickson CA, Lanza DJ, Karp DL, Edwards JW, Seabrook GR, Cambria RA, et al. Healing of venous ulcers in an ambulatory care program: the roles of chronic venous insufficiency and patient compliance. J Vasc Surg 1995;22:629-36. 7. Baldursson B, Sigurgeirsson B, Lindelof B. Leg ulcers and squamous cell carcinoma. An epidemiological study and a review of the literature. Acta Derm Venereol 1993;73:171-4. 8. Baldursson BT, Hedblad MA, Beitner H, Lindelof B. Squamous cell carcinoma complicating chronic venous leg ulceration: a study of the histopathology, course and survival in 25 patients. Br J Dermatol 1999;140:1148-52. 9. Combemale P, Bousquet M, Kanitakis J, Bernard P. Malignant transformation of leg ulcers: a retrospective study of 85 cases. J Eur Acad Dermatol Venereol 2007;21:935-41.








© Copyright 2026