
Allergic Contact Dermatitis to Plant Extracts in Cosmetics
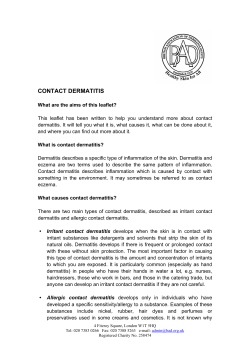
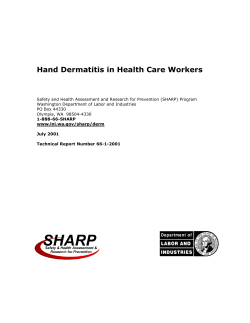
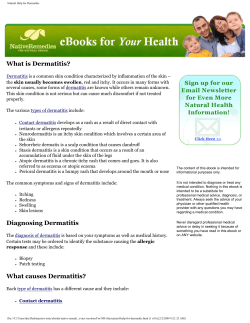
Allergic Contact Dermatitis to Plant Extracts in Cosmetics Alexander R. Jack, MD, Patricia L. Norris, MD, and Frances J. Storrs, MD Topically applied cosmetics and medicaments containing botanical extracts are commonly used. Despite popular beliefs of their benignancy, some botanicals have been implicated in causing allergic contact dermatitis in susceptible patients. The offending allergen may be the botanical extract itself or another ingredient such as a fragrance, preservative, dye, or sunscreen found in the product. Specific botanicals implicated in causing cosmetic contact dermatitis include Compositae family plants, tea tree oil, peppermint, lavender, lichens, henna, and others. Semin Cutan Med Surg 32:140-146 © 2013 Frontline Medical Communications KEYWORDS allergic contact dermatitis, cosmetics, botanicals, plants D uring the past several decades, there has been increasing use of topical cosmetics and medicaments containing botanical extracts.1,2 In a recent survey of 400 dermatology and allergy patients, 60.25% of respondents reported the use of ‘natural’ topical products.3 The popular appeal of botanicals may be attributed to the conventional wisdom that plant products have beneficial effects, such as treating common illnesses, while having little risk of adverse effects.4 Despite popular beliefs of their benignancy, cosmetic products containing botanicals have been implicated in causing adverse cutaneous reactions. In the aforementioned study of 400 patients, 6.22% of users reported unpleasant skin reactions to one or more of their botanical products.3 Previous reviews have shown that many popular botanical extracts have been reported to cause allergic contact dermatitis.4,5 The majority of adverse reactions to cosmetic products are irritant, which can manifest with unpleasant sensations (eg, burning, stinging) and/or nonimmunologically mediated skin inflammation in areas where the product is applied.6,7 Allergic contact dermatitis to cosmetics typically presents as a low-grade chronic eczematous dermatitis rather than an acute vesicular eruption as most cosmetic allergens are lowgrade.8 Affected areas are typically located on the face and localized to areas where the cosmetic is applied; however, connubial dermatitis (transfer of allergen from skin contact Department of Dermatology, Oregon Health & Science University, Portland, Oregon. Disclosures: The authors have completed and submitted the ICMJE Form for Disclosure of Potential Conflicts of Interest and none were reported. Correspondence: Alexander R. Jack, MD, Oregon Health & Science University, 3303 SW Bond Ave., CH16D, Portland, OR 97239. E-mail: [email protected] 140 with another person) and dermatitis from transfer of allergens from fomites (eg, pillowcases, towels) has been reported.7 It is important to note that allergic contact dermatitis to cosmetics is relatively infrequent given their widespread use, but still occurs in a significant number of patients. Incorporating data from a number of studies, Biebl et al reported pooled prevalence of allergic contact dermatitis to cosmetics at 9.8% in patients undergoing patch testing and 0.4% in the general population.7 Cosmetic dermatitis patients may have contact allergy to a botanical extract found in their product.9 However, one must consider a reaction to other components of the cosmetic such as fragrances, preservatives, and sunscreens.9 Some studies have estimated the prevalence of botanical extract allergy in patients with contact dermatitis to cosmetics. In a prospective study of 29 patients with cosmetic dermatitis, 79% of patients demonstrated positive patch-test reactions to Fragrance Mix I and 34% to Balsam of Peru.10 Patients in this study were tested with an extended series of plant extract allergens; the most prevalent reactions were 39% to one or more Compositae plants and 24% to tea tree oil.10 Simpson et al showed that in 21 patients at ‘high risk’ for botanical allergy (those using botanical products whose contact allergen was not explained by patch testing to standard allergens), 48% had a relevant reaction to a botanical extract.11 Of these relevant reactions, the most prevalent were Compositae plants, tea tree oil, lichens, and geranium.11 Of all patients with positive patch test reactions, the most common allergens were fragrance mix (33%), Balsam of Peru (30%), Compositae mix (20%), and sesquiterpene lactone mix (6.7%).11 These results suggest that fragrance mix and Bal- 1085-5629/13/$-see front matter © 2013 Frontline Medical Communications DOI: 10.12788/j.sder.0019 Allergic contact dermatitis in cosmetics sam of Peru may be useful screening allergens for botanical extract allergy. In the upcoming sections, specific plant allergens implicated in cosmetic contact dermatitis will be reviewed. Compositae Family The Compositae family of plants is one of the largest in the world and includes common weeds (eg, ragweed), ornamental plants (eg, chrysanthemum), vegetables (eg, artichoke), and herbs (eg, chamomile). They are mostly herbaceous plants with characteristic flowers generally consisting of 1-2 layers of numerous small flowers (florets) radially clustered to form a flower head (capitulum) subtended by an involucre (whorl of bracts) (Figure 1).12 The major sensitizers are sesquiterpene lactones (SQLs), which are found in stems, leaves, and flowers.12 They are a diverse group of compounds containing a sesquiterpene (C15H24) and a lactone ring (cyclic ester).12 Many of the most widely used medicinal plants contained in cosmetics and topical medicaments are from the Compositae family. Those reported to have caused allergic contact dermatitis are listed in Table 1.5,13 Compositae dermatitis typically presents in an airborne distribution and affects those with exposure to plants including outdoor workers, farmers, loggers, gardeners, and florists.12,13 Of all cases of Compositae dermatitis, topical agents may be a relatively uncommon culprit. In a review of 118 141 Table 1 Compositae Plants Implicated in Causing Allergic Contact Dermatitis Common Name Scientific Name Arinca Marigold German chamomile Roman chamomile Feverfew Dandelion Yarrow Purple coneflower Elecampane Sticky elecampane Mugwort Great burdock Dog fennel Costus French marigold Arnica montana Calendula officinalis Chamomilla recutita Chamaemelum nobile Tanacetum parthenium Taraxacum officinale Achillae millefolium Echinacea purpurea Inula helenium Inula viscose Artemisia vulgaris Arctium lappa Anthemis cotula Saussurea lappa Tagetes patula patients with positive patch-test reactions to Compositae mix, Hausen reported only 10 patients (8.5%) whose dermatitis was explained by contact with a topical medicament or cosmetic.14 Note that this study was published in 1996 and dermatitis to botanical extracts in cosmetics may be more common at the present time as usage of these products has increased. More recent studies have demonstrated that a large proportion of patients with Compositae allergy may be sensitized through the use of topical agents. Paulsen et al reported that 8 of 12 patients sensitive to chamomile and 5 of 6 patients sensitive to arnica had positive patch-test reactions to cosmetics and herbal remedies containing these plant extracts.15 In another study involving 443 patch-test patients, 5 (1.13%) reacted to arnica and 9 (2.03%) reacted to Calendula (marigold).16 Of these, 3 of 5 arnica-sensitive patients and 6 of 9 marigold-sensitive patients recalled using a topical product containing the respective botanical extracts.16 Taken together, these findings suggest that patients sensitized to a Compositae plant through any means (either through outdoor exposure or through usage of a topical product) should avoid products containing Compositae extracts.14-16 The North American Contact Dermatitis Group (NACDG) screening panel contains 2 standard allergens relevant to Compositae dermatitis: sesquiterpene lactone mix (SL mix) and Compositae mix (CM). SL mix is composed of 3 purified sesquiterpene lactones: costunolide, dehydrocostuslactone, and alantolactone.17 CM is comprised of extracts from 5 Compositae plants:14 Figure 1 Yarrow, a member of the Compositae family. Note the herbaceous foliage and numerous flowers consisting of small, radially clustered florets. Arnica montana, Matriacaria recutica, Tancetum parthenium, Tancetum vulgare, and Achiellea millefolium. The utility of SL mix relative to CM has been questioned as some reports11,18-20 have demonstrated a low prevalence of positive patch-test reactions to SL mix in Compositae-sensitive patients; however, another study showed that SL mix and A.R. Jack, P.L. Norris, and F.J. Storrs 142 Table 2 Plant Allergens Included in the Supplemental Plant Series (Chemotechnique Diagnostics, Vellinge, Sweden) Allergen Relevance Anthemis nobilis extract Diallyl disulfide Arnica montana extract Taraxacum officinale Achillea millefolium extract Propolis Chrysanthemum cinerariaefolium Sesquiterpene lactone mix ␣-Methylene-␥-butyrolactone Tanacetum vulgare extract Alantolactone Lichen acid mix Parthenolide Chamomilla recutita extract Roman chamomile (Compositae family) Irritant found in Allium plants (e.g. garlic) Arnica (Compositae family) Dandelion (Compositae family) Yarrow (Compositae family) Resinous mixture from honeybee Pyrethrum (Compositae family), used in production of insecticide Screen for Compositae allergy Screen for Compositae allergy Tansy (Compositae family) Screen for Compositae allergy Screen for lichen allergy Feverfew (Compositae family) German chamomile (Compositae family) CM produce similar results.21 Limitations of CM include lack of both a standardized manufacturing protocol and detailed specification of constituent plants, which may result in variable concentrations of sesquiterpene lactones in different batches.22 Given the potential for both SL mix and CM to miss Compositae allergy, it is reasonable to patch-test patients with suspected allergic contact dermatitis to Compositae-containing cosmetics to their own products in addition to these standardized mixes. Additionally, a supplemental plant series that contains a number of specific Compositae plant extracts is available (Chemotechnique Diagnostics, Vellinge, Sweden) (Table 2). Tea Tree Oil Tea tree oil (TTO) is an essential oil extracted via steam distillation from the leaves of the tree Melaleuca alternifolia, which is a member of the Myrtaceae family and indigenous to northeastern Australia. Well-known for its purported antimicrobial effects, TTO is found in many products including shampoos, massage oils, aromatherapy candles, compresses, inhalers, mouthwashes, laundry detergents, fabric softeners, and moisturizers.23 TTO contains many distinct chemical compounds. Both its antimicrobial and sensitizing properties are likely attributable to the terpene and hydrocarbon components, notably terpinen-4-ol.23 Degradation products created by photo-oxidation of TTO are more potent sensitizers than fresh TTO, thus using an old product may result in a higher potential for sensitization.24 A retrospective study of 2,520 patients undergoing patch testing in Australia demonstrated a 1.8% prevalence of positive patch tests to TTO; 41% of positive reactions were deemed relevant.25 This prevalence rate was higher than that reported by other groups in Europe and North America.24,26 The North American Contact Dermatitis Group has reported a 1.4% prevalence of positive patch-test reactions in 20052006, a significant increase from the 0.9% prevalence seen in 1994-2004.27 Allergic contact dermatitis due to TTO has been reported when it has been used as treatment for dog scratches, tinea pedis, insect bites, hand dermatitis, folliculitis, acne, bronchitis, warts, vulvovaginitis, and skin abrasions (Figure 2).28 Additionally, an erythema multiform-like id reaction secondary to allergic contact dermatitis to TTO has been reported.29 Figure 2 (A) Eczematous plaques on the extensor knee of a patient using a topical preparation containing tea tree oil for joint pain. (B) Note the positive patch test reaction to tea tree oil 5% in pet. Allergic contact dermatitis in cosmetics The NACDG screening panel contains TTO 5% in petrolatum. When the index of suspicion is high, patch testing with both TTO 5% in petrolatum and with the patient’s own products is recommended.30 Patch-test results should be interpreted carefully as TTO, particularly in high concentrations, is a known irritant.23 Peppermint Oil Peppermint oil (PO) is extracted via steam distillation from the above-ground portion of Mentha piperita, a perennial herb native to the Mediterranean region but is now widely cultivated. Mentha piperita is a member of the Labiatae family, which includes other fragrant herbs such as lavender. PO is well-known for its fresh odor, pungent taste, and cooling effects when topically applied. It has been used as a fragrance, flavoring agent, antipruritic, and analgesic.31 Products containing PO include lip balms, mouthwashes, breath fresheners, toothpastes, chewing gums, dental floss, teas, confections, and dissolving oral strips.31,32 The primary constituents of PO are menthol and menthone; notable minor constituents include limonene, carvone, and pulegone, the last of which is a known hepatotoxin.33,34 Tran et al published a recent case series of 4 patients with allergic contact cheilitis that were deemed most likely secondary to peppermint oil in lip balm and other lip products.32 Allergic contact dermatitis to PO has been reported with topical use on skin.35,36 Additionally, PO has been implicated in provoking disorders of the oral cavity including stomatitis, burning mouth syndrome, recurrent oral ulcers, and oral lichenoid reactions.37 There is a case report of systemic contact dermatitis presenting as vulvar dermatitis thought to be secondary to oral ingestion of peppermint tea.38 Mentha piperita oil 2% in petrolatum was a new addition to the NACDG screening panel in the 2009-2010 reporting period.39 During this period, the NACDG has reported a 0.6% prevalence of positive patch-test reactions to PO with 72% being of definite, probable, or possible relevance.39 It should be noted that PO in higher concentrations (over 5%) may be an irritant.31,33 Lavender Oil Lavender oil (LO) is an essential oil that is most commonly derived from 1 of 4 species of lavender, Lavandula augustifolia. LO has been used for its purported sedative, antidepressive, and antimicrobial and fragrant properties.40 Products containing LO include soaps, cleansers, moisturizers, massage oils, and aromatherapy oils.41 The main components of LO include linalool, linalyl acetate, and camphor.40 Allergic contact dermatitis to LO has been reported in armoatherapists; massage therapists; reflexologists; and physiotherapists through occupational exposure to massage oil and aromatherapy oil.42,43 The prevalence of allergic contact dermatitis to LO may be particularly high in Japan where it has gained widespread household use. Sugiura et al reported that 3.8% of 1,483 patients with suspected cosmetic 143 contact dermatitis had positive patch-test reactions to LO.44 The percentage of positive patch-test reactions increased from 1.1% in 1990 to 13.8% in 1998, which correlated with increased household use of LO during the study period.44 A potential limitation of this study is that the authors used a concentration of 20% LO in petrolatum to patch test, which may have resulted in a high proportion of irritant reactions. Like PO, LO is a recent addition to the NACDG screening panel and is patch tested with Lavandula augustifolia oil 2% in petrolatum.39 During the 2009-2010 reporting period, the NACDG reported a 0.2% prevalence of positive patch-test reactions with 80% of reactions being of definite, probable, or possible relevance.39 Lichens Lichens are an extremely diverse group of plant-like, composite organisms that consist of a fungus living in symbiosis with an alga or cyanobacterium. They have become popular additions to cosmetics, particularly deodorants, moisturizers, and ‘healing’ creams, due to their purported antimicrobial properties.45 The principle allergens in lichens include usnic acid, atranorin, and everinic acid, which are produced by the fungal component.46 Sheu et al reported a case series of 4 patients with allergic contact dermatitis to lichen extract in deodorants (Figure 3).46 Three of 4 patients presented with axillary dermatitis; however, 1 patient presented with an ear dermatitis due to connubial allergen transfer from the deodorant in her husband’s axilla.46 The NACDG screening panel does not contain a specific allergen screen for lichen allergy. Lichen acid mix— consisting of 0.1% d-usinc acid, 0.1% atranorin, and 0.1% everinic acid pet—is available (Chemotechnique Diagnostics, Vellinge, Sweden). It should be noted that Fragrance Mix I contains oak moss absolute, which is derived from the extract of the lichen Evernia prunastri. However, there is no known cross reactivity between lichen mix and oak moss absolute. Henna Henna is derived from the flowering plant Lawsonia inermis, which grows in tropical and subtropical regions of Africa, southern Asia, and northern Australia. Henna is a member of the Lythraceae family. Reconstituted powder from dried henna leaves have been used since medieval times as a dye for coloring and tattooing the skin, hair, and nails. Para-phenylenediamine (PPD), a widely reported sensitizer, is often added to henna dye to enhance coloring. The PPD additive significantly increases the risk of allergic contact dermatitis to products containing henna.47 Henna tattoos have been suggested as an important means of sensitization to PPD, which may increase one’s risk for developing contact dermatitis to conventional hair-dyeing products.48 Although the sensitizer in cosmetics containing henna is often PPD or other additives, allergic contact dermatitis may be secondary to lawsone (2-hydroxy-1, 4-naphthoquinone) in henna itself.49 A 3-year-old girl was reported to have severe bullous A.R. Jack, P.L. Norris, and F.J. Storrs 144 Figure 3 (A) Eczematous plaques in the axillary vault of a patient using a ‘natural’ deodorant containing lichen extract. (B) Note the positive patch test reactions to lichen acid mix 0.3% in pet, D-usnic acid 1% in pet, and the deodorant. allergic contact dermatitis from pure henna without PPD.49 Another case of contact dermatitis to pure henna was reported in a man using a henna solution topically for rheumatic pain.50 A 9-year-old boy was found to be sensitized to both PPD and henna in an allergic contact reaction to a henna tattoo.51 The NACDG standard tray contains PPD and therefore will suffice for screening of most cases of contact dermatitis to henna-containing products. In patients with suspected dermatitis to henna products that are PPD patch test negative, it would be reasonable to patch test with 10% henna in petrolatum.49 Other Plant Allergens There are many plant extracts that have been reported to cause allergic contact dermatitis through cosmetic use in one or a limited number of reports. These include Aloe vera,52 Azadirachta indica oil (neem oil),53,54 Centella asiatica (centella),55,56 Curcuma longa (tumeric),57-59 Glycyrrhiza glabra (licorice),60 Hamamelis virginiana (witch hazel),61 Olea europaea oil (olive oil),62 Ricinus communis oil (castor oil plant),63-65 Rosa centifolia (cabbage rose),66 Rosmarinus officinalis (rosemary),67-69 Salvia officinalis (sage),70 Simmondsia chinensis (jojoba),71,72 and Thymus vulgaris (thyme).67 Conclusions Already commonly used, cosmetics and medicaments containing botanical extracts are likely to increase in popularity. Allergic contact dermatitis to topically applied botanical products is relatively infrequent given their widespread use. However, the allergic reaction certainly does occur in a small percentage of individuals. When there is a high suspicion for botanical contact dermatitis, a careful history should be obtained including a review of ingredients in all of the patient’s cosmetics and topical medicaments. Note potential offending allergens include fragrances, preservatives, dyes, sunscreens, and botanical extracts. Plant allergens commonly implicated in causing cosmetic contact dermatitis are summarized in Table 3. When patch testing for suspected cosmetic dermatitis, one should note that the fragrance mixes and Balsam of Peru are useful screening allergens.11 Relevant allergens on the NACDG standard tray specific to botanicals include Compositae mix, sesquiterpene lactone mix, tea tree oil, Mentha piperita oil, and Lavandula augustifolia oil. Patch tests for botanical extracts should be interpreted with caution as in the case of fragrance mixes, which are known to have a high prevalence of positive reactions but low relevance due to irritancy.73 In addition to standard allergens, supplemental plant allergen trays may be considered. Patch testing a “leave on” cosmetic product may be done, but a high frequency of irritant reactions should be anticipated. Finally, performing a repeated open-application test (ROAT) by rubbing the suspected product into the antecubital skin twice daily for 1 week may aid in judging relevance.74 Table 3 Plant Extracts in Cosmetics Commonly Implicated in Causing Allergic Contact Dermatitis Plant Family Sensitizing Component Relevant Plant Species Compositae Myrtaceae Labiatae Sesquiterpene lactones Terpenes, hydrocarbons Menthol, menthone, limonene, carvone, linalool, linayl acetate, camphor Usnic acid, atranorin, everinic acid Lawsone See Table 1 Tea tree (Melaleuca) Peppermint (Mentha) Lavender (Lavandula) Many species (not a true plant) Henna (Lawsonia) Lichens Lythracae Allergic contact dermatitis in cosmetics References 1. Bedi MK, Shenefelt PD. Herbal therapy in dermatology. Arch Dermatol. 2002;138(2):232-242. 2. Eisenburg DM, Kessler RC, Foster C, Norlock FE, Calkins DR, Delbanco TL. Unconventional medicine in the United States: Prevalence, costs and pattern use. N Engl J Med. 1993;328(4):246-252. 3. Corazza M, Borghi A, Lauriola MM, Virgili A. Use of topical herbal remedies and cosmetics: a questionnaire-based investigation in dermatology out-patients. J Eur Acad Dermatol Venereol. 2009;23(11):12981303. 4. Kiken DA, Cohen DE. Contact dermatitis to botanical extracts⬘. Am J Contact Dermatitis. 2002;13(3):148-152. 5. Aberer W. Contact allergy and medicinal herbs. J Dtsch Dermatol Ges. 2008;6(1):15-24. 6. Orton DI, Wilkinson JD. Cosmetic allergy: incidence, diagnosis, and management. Am J Clin Dermatol. 2004;5(5):327-337. 7. Biebl KA, Warshaw EM. Allergic contact dermatitis to cosmetics. Dermatol Clin. 2006;24(2):215-232, vii. 8. De Groot AC, Weiland JW, Nater JP. Unwanted Effects Of Cosmetics And Drugs Used In Dermatology. 3rd ed. Amsterdam, The Netherlands: Elsevier Science; 1994. 9. Travassos AR, Claes L, Boey L, Drieghe J, Goossens A. Non-fragrance allergens in specific cosmetic products. Contact Dermatitis. 2011;65(5): 276-285. 10. Thomson KF, Wilkinson SM. Allergic contact dermatitis to plant extracts in patients with cosmetic dermatitis. Br J Dermatol. 2000;142(1): 84-88. 11. Simpson EL, Law SV, Storrs FJ. Prevalence of botanical extract allergy in patients with contact dermatitis. Dermatitis. 2004;15(2):67-72. 12. Mcgovern TW, Barkley TM. Botanical dermatology. Int J Dermatol. 1998;37(5):321-334. 13. Paulsen E. Contact sensitization from Compositae-containing herbal remedies and cosmetics. Contact Dermatitis. 2002;47(4):189-198. 14. Hausen BM. A 6-year experience with compositae mix. Am J Contact Dermatitis. 1996;7(2):94-99. 15. Paulsen E, Chistensen LP, Andersen KE. Cosmetics and herbal remedies with Compositae plant extracts - are they tolerated by Compositaeallergic patients? Contact Dermatitis. 2008;58(1):15-23. 16. Reider N, Komericki P, Hausen BM, Fritsch P, Aberer W. The seamy side of natural medicines: contact sensitization to arnica (Arnica montana L.) and marigold (Calendula officinalis L.). Contact Dermatitis. 2001;45(5):269-272. 17. Ducombs G, Benezra C, Talaga P, et al. Patch testing with the ”sesquiterpene lactone mix”: a marker for contact allergy to Compositae and other sesquiterpene-lactone-containing plants. A multicentre study of the EECDRG. Contact Dermatitis. 1990;22(5):249-252. 18. Green C, Ferguson J. Sesquiterpene lactone mix is not an adequate screen for Compositae allergy. Contact Dermatitis. 1994;31(3):151-153. 19. Goulden V, Wilkinson SM. Patch testing for Compositae allergy. Br J Dermatol. 1998;138(6):1018-1021. 20. von der Werth JM, Ratcliffe J, English JS. Compositae mix is a more sensitive test for Compositae dermatitis than the sesquiterpene lactone mix. Contact Dermatitis. 1999;40(5):273-276. 21. Isaksson M, Hansson C, Inerot A, et al; Swedish Contact Dermatitis Research Group. Multicentre patch testing with compositae mix by the Swedish Contact Dermatitis Research Group. Acta Derm Venereol. 2011; 91(3):295-298. 22. Jacob M, Brinkmann J, Schmidt TJ. Sesquiterpene lactone mix as a diagnostic tool for Asteraceae allergic contact dermatitis: chemical explanation for its poor performance and Sesquiterpene lactone mix II as a proposed improvement. Contact Dermatitis. 2012;66(5):233-240. 23. Crawford GH, Sciacca JR, James WD. Tea tree oil: cutaneous effects of the extracted oil of Melaleuca alternifolia. Dermatitis. 2004;15(2):5966. 24. Hausen BM, Reichling J, Harkenthal M. Degradation products of monoterpenes are the sensitizing agents in tea tree oil. Am J Contact Dermatitis. 1999;10(2):68-77. 25. Rutherford T, Nixon R, Tam M, Tate B. Allergy to tea tree oil: retrospective review of 41 cases with positive patch tests over 4.5 years. Australas 145 J Dermatol. 2007;48(2):83-87. 26. Lisi P, Meligeni L, Pigatto P, Ayala F, Suppa F, Foti C, Angelini G. Prevalenza della sensibilizzazione all’olio essenziale di Melaleuca. Ann Ital Dermatol Allergol It. Ann Clin Exp Allergol Dermat. 2000;54:141-144. 27. Zug KA, Warshaw EM, Fowler JF, et al. Patch-test results of the North American Contact Dermatitis Group 2005-2006. Dermatitis. 2009; 20(3):149-160. 28. Hartford O, Zug KA. Tea tree oil. Cutis. 2005;76(3):178-180. 29. Khanna M, Qasem K, Sasseville D. Allergic contact dermatitis to tea tree oil with erythema multiforme-like id reaction. Am J Contact Dermatitis. 2000;11(4):238-242. 30. Larson D, Jacob SE. Tea tree oil. Dermatitis. 2012;23(1):48-49. 31. Herro E, Jacob SE. Mentha piperita (peppermint). Dermatitis. 2010; 21(6):327-329. 32. Tran A, Pratt M, Dekoven J. Acute allergic contact dermatitis of the lips from peppermint oil in a lip balm. Dermatitis. 2010;21(2):111-115. 33. Nair B. Final report on the safety assessment of Mentha Piperita (Peppermint) Oil, Mentha Piperita (Peppermint) Leaf Extract, Mentha Piperita (Peppermint) Leaf, and Mentha Piperita (Peppermint) Leaf Water. Int J Toxicol. 2001;20(Suppl 3):61-73. 34. Mckay DL, Blumberg JB. A review of the bioactivity and potential health benefits of peppermint tea (Mentha piperita L.). Phytother Res. 2006; 20(8):619-633. 35. Wilkinson SM, Beck MH. Allergic contact dermatitis from menthol in peppermint. Contact Dermatitis. 1994;30(1):42-43. 36. Foti C, Conserva A, Antelmi A, Lospalluti L, Angelini G. Contact dermatitis from peppermint and menthol in a local action transcutaneous patch. Contact Dermatitis. 2003;49(6):312-313. 37. Morton CA, Garioch J, Todd P, Lamey PJ, Forsyth A. Contact sensitivity to menthol and peppermint in patients with intra-oral symptoms. Contact Dermatitis. 1995;32(5):281-284. 38. Vermaat H, van Meurs T, Rustemeyer T, Bruynzeel DP, Kirtschig G. Vulval allergic contact dermatitis due to peppermint oil in herbal tea. Contact Dermatitis. 2008;58(6):364-365. 39. Warshaw EM, Belsito DV, Taylor JS, et al. North American Contact Dermatitis Group patch test results: 2009 to 2010. Dermatitis. 2013; 24(2):50-59. 40. Wu PA, James WD. Lavender. Dermatitis. 2011;22(6):344-347. 41. Household Products Database: Lavender oil. US Department of Health and Human Services. Available at: http://householdproducts.nlm.nih. gov/. Accessed March 25, 2013. 42. Bleasel N, Tate B, Rademaker M. Allergic contact dermatitis following exposure to essential oils. Australas J Dermatol. 2002;43(3):211-213. 43. Trattner A, David M, Lazarov A. Occupational contact dermatitis due to essential oils. Contact Dermatitis. 2008;58(5):282-284. 44. Sugiura M, Hayakawa R, Kato Y, Sugiura K, Hashimoto R. Results of patch testing with lavender oil in Japan. Contact Dermatitis. 2000;43(3): 157-160. 45. Schalock PC. Lichen extracts. Dermatitis. 2009;20(1):53-54. 46. Sheu M, Simpson EL, Law SV, Storrs FJ. Allergic contact dermatitis from a natural deodorant: a report of 4 cases associated with lichen acid mix allergy. J Am Acad Dermatol. 2006;55(2):332-337. 47. Kang IJ, Lee MH. Quantification of para-phenylenediamine and heavy metals in henna dye. Contact Dermatitis. 2006;55(1):26-29. 48. Kind F, Scherer K, Bircher AJ. Contact dermatitis to para-phenylenediamine in hair dye following sensitization to black henna tattoos - an ongoing problem. J Dtsch Dermatol Ges. 2012;10(8):572-578. 49. Belhadjali H, Akkari H, Youssef M, Mohamed M, Zili J. Bullous allergic contact dermatitis to pure henna in a 3-year-old girl. Pediatr Dermatol. 2011;28(5):580-581. 50. Polat M, Dikilitas¸ M, Oztas¸ P, Alli N. Allergic contact dermatitis to pure henna. Dermatol Online J. 2009;15(1):15. 51. Jung P, Sesztak-greinecker G, Wantke F, Götz M, Jarisch R, Hemmer W. The extent of black henna tattoo’s complications are not restricted to PPD-sensitization. Contact Dermatitis. 2006;55(1):57. 52. Ferreira M, Teixeira M, Silva E, Selores M. Allergic contact dermatitis to Aloe vera. Contact Dermatitis. 2007;57(4):278-279. 53. Greenblatt DT, Banerjee P, White JM. Allergic contact dermatitis caused by neem oil. Contact Derm. 2012;67(4):242-243. 146 54. Reutemann P, Ehrlich A. Neem oil: an herbal therapy for alopecia causes dermatitis. Dermatitis. 2008;19(3):E12-E15. 55. Danese P, Carnevali C, Bertazzoni MG. Allergic contact dermatitis due to Centella asiatica extract. Contact Dermatitis. 1994;31(3):201. 56. Izu R, Aguirre A, Gil N, Díaz-pérez JL. Allergic contact dermatitis from a cream containing Centella asiatica extract. Contact Dermatitis. 1992; 26(3):192-193. 57. Nath AK, Thappa DM. Kumkum-induced dermatitis: an analysis of 46 cases. Clin Exp Dermatol. 2007;32(4):385-387. 58. Thompson DA, Tan BB. Tetrahydracurcumin-related allergic contact dermatitis. Contact Dermatitis. 2006;55(4):254-255. 59. Lamb SR, Wilkinson SM. Contact allergy to tetrahydrocurcumin. Contact Dermatitis. 2003;48(4):227. 60. O’connell RL, White IR, White JM, Mcfadden JP. Liquorice extract in a cosmetic product causing contact allergy. Contact Dermatitis. 2008; 59(1):52. 61. Granlund H. Contact allergy to witch hazel. Contact Dermatitis. 1994; 31(3):195. 62. Beukers SM, Rustemeyer T, Bruynzeel DP. Cheilitis due to olive oil. Contact Dermatitis. 2008;59(4):253-255. 63. Sasseville D, Desjardins M, Almutawa F. Allergic contact dermatitis caused by glycyrrhetinic acid and castor oil. Contact Dermatitis. 2011; 64(3):168-169. 64. Sánchez-guerrero IM, Huertas AJ, López MP, Carreño A, Ramírez M, Pajarón M. Angioedema-like allergic contact dermatitis to castor oil. Contact Dermatitis. 2010;62(5):318-319. A.R. Jack, P.L. Norris, and F.J. Storrs 65. Taghipour K, Tatnall F, Orton D. Allergic axillary dermatitis due to hydrogenated castor oil in a deodorant. Contact Derm. 2008;58(3):168169. 66. Nardelli A, Thijs L, Janssen K, Goossens A. Rosa centifolia in a ‘nonscented’ moisturizing body lotion as a cause of allergic contact dermatitis. Contact Dermatitis. 2009;61(5):306-309. 67. Martínez-gonzález MC, Goday buján JJ, Martínez gómez W, Fonseca Capdevila E. Concomitant allergic contact dermatitis due to Rosmarinus officinalis (rosemary) and Thymus vulgaris (thyme). Contact Dermatits. 2007;56(1):49-50. 68. Inui S, Katayama I. Allergic contact dermatitis induced by rosemary leaf extract in a cleansing gel. J Dermatol. 2005;32(8):667-669. 69. Fernandez L, Duque S, Sanchez I, Quiñones D, Rodriguez F, Garciaabujeta JL. Allergic contact dermatitis from rosemary (Rosmarinus officinalis L.). Contact Dermatitis. 1997;37(5):248-249. 70. Mayer E, Gescheidt-shoshany H, Weltfriend S. Allergic contact dermatitis caused by Salvia officinalis extract. Contact Dermatitis. 2011;64(4): 237-238. 71. Di berardino L, Di berardino F, Castelli A, Della torre F. A case of contact dermatitis from jojoba. Contact Derm. 2006;55(1):57-58. 72. Wantke F, Hemmer W, Götz M, Jarisch R. Contact dermatitis from jojoba oil and myristyl lactate/maleated soybean oil. Contact Dermatitis. 1996;34(1):71-72. 73. Storrs FJ. Fragrance. Dermatitis. 2007;18(1):3-7. 74. Rietschel RL, Fowler JF, Fisher AA. Recommendations for cosmetic testing. In Rietschel RL, Fowler JF, Fisher AA, eds. Contact Dermatitis. Lewiston, NY: BC Decker; 2008:296







© Copyright 2026