
Prescriptions of Chinese Herbal Medicine for Constipation Under the National Health
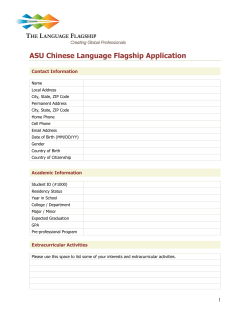
ORIGINAL ARTICLE Prescriptions of Chinese Herbal Medicine for Constipation Under the National Health Insurance in Taiwan Maw-Shiou Jong1,5, Shinn-Jang Hwang2,4, Yu-Chun Chen2,4, Tzeng-Ji Chen2,4, Fun-Jou Chen3, Fang-Pey Chen1,5* 1 Center for Traditional Medicine, 2Department of Family Medicine, Taipei Veterans General Hospital, Taipei; 3 Graduate Institute of Integrated Chinese and Western Medicine, Chinese Medical University, Taichung; 4 Division of Family Medicine, Department of Medicine, and 5Institute of Traditional Medicine, National Yang-Ming University School of Medicine, Taipei, Taiwan, R.O.C. Background: Constipation is a common gastrointestinal problem worldwide. The aim of this study was to determine the frequency of use and prescriptive patterns of Chinese herbal medicine (CHM) in treating constipation by analyzing the claims data of traditional Chinese medicine (TCM) from the National Health Insurance (NHI) in Taiwan. Methods: The computerized claims dataset of the TCM office visits and the corresponding prescription files in 2004 compiled by the NHI Research Institute in Taiwan were linked and processed. Visit files with the single diagnostic coding of constipation (ICD-9-CM code 564.0) were extracted to analyze the frequency and pattern of corresponding CHM prescriptions. The association rule was applied to analyze the co-prescription of CHM in treating constipation. Results: There were 152,564 subjects who visited TCM clinics only for constipation in Taiwan during 2004 and received a total of 387,268 CHM prescriptions. Subjects between 20 and 29 years of age comprised the largest number of those treated (25.5%). Female subjects used CHM for constipation more frequently than male subjects (female:male = 3.31:1). There was an average of 4.6 items of single Chinese herbs or formula in a single prescription for constipation. Ma-zi-renwan was the most commonly prescribed herbal formula, while Da-huang (Rheum palmatum) was the most commonly used single Chinese herb. According to the association rule, the most common prescribed pattern of 2-drug combination of CHM for treating constipation was Ban-xia-xie-xin-tang plus Ma-zi-ren-wan, while the 3-drug combination of CHM was Fang-feng-tong-sheng-san, Rheum palmatum and Ma-zi-ren-wan. Conclusion: This study showed the pattern of single Chinese herbs or herbal formulae used in treating constipation in Taiwan. Further clinical trials are needed to evaluate the efficacy and safety of these CHMs in treating constipation. [J Chin Med Assoc 2010;73(7):375–383] Key Words: Chinese herbal medicine, constipation, pharmacoepidemiology, traditional Chinese medicine Introduction Constipation is a condition in which bowel movements are infrequent, irregular, or difficult.1 It is a disorder resulting from different causes such as insufficient intake of dietary fiber, emotional influence, dysfunction of the nervous system, structural abnormality, systemic disease, or drug effects.1 Constipation is a common gastrointestinal problem worldwide, and it affects at least 8.5% of individuals in Taiwan, based on Rome II diagnostic criteria.2 It often occurs in females, with advanced age, low socioeconomic class and low educational position.2,3 The aim of treating constipation is to treat the underlying causes, improve symptoms, and resume the normal physiological function of the bowel. Treating constipation can be a comprehensive therapy tailored to the individual.4 Drugs commonly used include bulk laxatives, osmotic laxatives, non-absorbable sugar, stimulant laxatives, cholinergic agents and other prokinetic *Correspondence to: Dr Fang-Pey Chen, Center for Traditional Medicine, Taipei Veterans General Hospital, 201, Section 2, Shih-Pai Road, Taipei 112, Taiwan, R.O.C. E-mail: [email protected] Received: December 9, 2009 Accepted: June 22, 2010 ● J Chin Med Assoc • July 2010 • Vol 73 • No 7 © 2010 Elsevier Taiwan LLC and the Chinese Medical Association. All rights reserved. ● 375 M.S. Jong, et al agents. Selective chloride channel activators, which can increase intestinal water secretion, thereby increasing intestinal motility and facilitating the bowel movement, are also used.4,5 After excluding secondary constipation caused by other problems, primary (idiopathic) constipation can be classified into 3 categories: normal transit or irritable bowel syndrome, pelvic floor dysfunction, and slow transit constipation. These 3 types of constipation overlap frequently. Normal and slow transit constipation are usually treated by the drugs mentioned above.5 In Eastern countries, traditional Chinese medicine (TCM) is another option in addition to Western medicine for treating constipation.6 The principles of diagnosis and treatment of constipation in TCM are primarily based on the manifestations of the syndrome Therefore, the principal signs and symptoms of patients from which a corresponding prescription of Chinese herbal medicine (CHM) is provided, is largely dependent on the experience of the Chinese herbal doctors or from the records of ancient Chinese books. The optimal choice of CHM prescription for constipation is unknown. Furthermore, whether these Chinese herbs or formulae have modern pharmacological effects in the treatment of constipation remains to be elucidated. In Taiwan, the National Health Insurance (NHI) has reimbursed medical expenses for Western medicine for nearly all inhabitants since 1995 (22,134,270 beneficiaries at the end of 2004, covering nearly 98% of the total population in Taiwan).7,8 The use of TCM has been reimbursed by the NHI since 1996. People in Taiwan are free to choose Western medicine or TCM, and are allowed to visit primary care clinics or hospitals without referral. Because all claims data are available to researchers in electronic form, a large-scale survey of pharmacoepidemiological issues can be easily conducted. The aim of the current study was to explore the frequency and pattern of CHM use for subjects with constipation by analyzing the NHI database in 2004 in Taiwan. (CM_CD2004.DAT and CM_OO2004.DAT), for 2004 from the NHIRD in Taiwan. The visit files recorded the dates of encounters, the medical care facilities and specialties, patients’ sex, birth date, and up to 3 diagnoses according to the International Classification of Diseases, 9th Revision, Clinical Modification (ICD-9CM). For privacy protection, the identification data of patients and institutions was scrambled cryptographically to ensure anonymity. The prescription files contained the prescription records of CHM corresponding to the office visits. A CHM prescription contains 1 to several single Chinese herbs or herbal formulae. The Chinese herbal formulae or single herbs are made in powder or fine granules in Taiwan, and can be easily mixed and dispensed into small packages so that 1 prescription can be taken at a time. All TCMs are provided only in ambulatory clinics under the coverage of NHI in Taiwan and there is no inpatient care. In addition, only licensed TCM physicians are qualified for reimbursement. The insurance benefits of TCM in Taiwan include CHM, acupuncture and traumatology manipulative therapy, especially for joint dislocation. Study design Methods Although the concept of disease entities in TCM is quite different from that in Western medicine, the TCM physicians in Taiwan are requested to make the diagnosis based on ICD-9-CM coding for visiting claims. In this study, we utilized the data of subjects with the single diagnostic code for constipation (i.e. ICD-9 code 564.0) among TCM visits. According to the theory of TCM, a single prescription from a TCM physician may contain a single Chinese herb or multiple herbs of various dosages, namely a compound (Fu-Fang) or a classical formula (regimen, remedy or Fang-Ji). These are a combination of compatible Chinese herbs in fixed dosages ascribed to classical or well-known Chinese textbooks of medicine, or a classical formula plus some Chinese herbs called ChiaChien-Fang. In addition, several formulae can be put together with or without 1 or several Chinese herbs for different symptoms and signs manifested by a patient. Data sources Data analysis The NHI program in Taiwan was initiated in 1995, and the Bureau of the NHI began to release all claims data in electronic form to the public under the National Health Insurance Research Database (NHIRD) project since 1999. The structure of the claims files is described in detail on the NHIRD website and in our previous report.6 Briefly, we obtained the database of TCM claims, including the visit files and prescription files The database software, IBM DB2 version 8.1 (IBM, Armonk, NY, USA), was used for data linkage and processing. Regular statistics (mean and percentage) were displayed for the frequency of use and pattern of CHM prescriptions for constipation. Association rule mining, originally developed in the 1990s to identify which groups or sets of items were likely to be purchased together in the market, was applied to calculate the 376 J Chin Med Assoc • July 2010 • Vol 73 • No 7 Chinese herb use for constipation in Taiwan prescription of the Chinese herbs for constipation.9,10 An association rule was applied to prescriptions as follows: when a physician prescribes drug A (or drugs {A1,A2}, drugs {A1,A2,A3}, etc.), he/she will also prescribe drug B in X% of cases, and this co-prescribing is present in Y% of all prescriptions. The support factor is the ratio of co-prescriptions of all prescriptions (i.e. Y% in the above example). The confidence factor is the ratio of co-prescriptions to prescriptions for drug A (i.e. X% in the above example). For executing the program to identify association rules in our dataset, we chose 0.5% as the minimum support factor and 30% as the minimum confidence level.11 Mu-xiang-bin-lang-wan (4.8%), San-huang-xie-xin-tang (4.7%), Tao-ren-cheng-qi-tang (4.6%), and Gan-luyin (4.5%; Table 2). Single Chinese herbs The most common single Chinese herb prescribed for constipation was Rheum palmatum (Da-huang) (18.4%), followed by Magnolia officinalis (Hou-pu) (6.6%), Scrophularia ningpoensis (Xuan-shen) (6.3%), Citrus aurantium (fruit; Zhi-shi) (6.1%), Rehmannia glutinosa (Sheng-di-huang) (6.0%), Ophiopogon japonicus (Mai-dong) (6.0%), Crataegus pinnatifida (Shanzha) (5.7%), Cannabis sativa (Huo-ma-zen) (5.1%), Glycyrrhiza uralensis (Gan-cao) (5.0%), and Citrus aurantium (peel; Zhi-ke) (4.5%; Table 3). Results Combination of CHM Epidemiology Among the 22,134,270 valid beneficiaries of the NHI at the end of 2004 in Taiwan, 6,224,436 (28.1%) subjects had used TCM during that year, and 152,564 (2.5%) subjects visited the TCM clinics and used CHM only for constipation. Among these constipation subjects, there were a total of 387,268 CHM prescriptions. The peak age of subjects with constipation treated by TCM was between 20 and 29 years of age (25.5%), followed by 30–39 years of age (19.4%), and 40–49 years of age (15.7%; Table 1). Female subjects used CHM for constipation more frequently than male subjects (female:male = 3.31:1). Chinese herbal formulae Ma-zi-ren-wan (34.4%) was the most commonly prescribed Chinese herbal formula for subjects with constipation, followed by Fang-feng-tong-sheng-san (17.6%), Run-chang-wan (12.4%), Run-chang-tang (7.7%), Da-chai-hu-tang (6.6%), Ping-wei-san (4.9%), There was an average of 4.6 Chinese herbal items in a single prescription for subjects with constipation. The most common number of items in the prescription of Chinese herbal formulae or single Chinese herbs for subjects with constipation in Taiwan is 5 (16.6%), followed by 4 (16.5%), and 3 (15.3%; Figure 1). According to the association rule, the most commonly prescribed pattern of a 2-drug combination of CHM for treating constipation was Ban-xia-xie-xin-tang plus Ma-zi-ren-wan (Table 4), while the 3-drug combination of CHM was Fang-feng-tong-sheng-san, Rheum palmatum and Ma-zi-ren-wan (Table 5). The most common 4-drug combination of CHM for constipation was Ophiopogon japonicus, Rehmannia glutinosa, Scrophularia ningpoensis and Run-chang-wan, which accounted for 0.3% of all prescriptions. The most common 5-drug combination of CHM was An-zhong-san, Mu-xiang-bin-lang-wan, Run-chang-tang, Fang-fengtong-sheng-san and Ma-zi-ren-wan, which accounted for 0.2% of all prescriptions. Table 1. Age-specific frequency of the use of TCM in patients with constipation in Taiwan during 2004* Subjects with constipation using TCM Age (yr) 0–9 10–19 20–29 30–39 40–49 50–59 60–69 70–79 ≥ 80 Total Total patients Males† Females† 11,013 (7.2) 16,713 (11.0) 38,961 (25.5) 29,969 (19.6) 23,938 (15.7) 11,607 (7.6) 7,621 (5.0) 8,968 (5.9) 3,774 (2.5) 152,564 (100) 4,997 (3.3) 3,716 (2.4) 4,203 (2.8) 4,279 (2.8) 4,480 (2.9) 3,311 (2.2) 3,275 (2.1) 5,131 (3.4) 1,978 (1.3) 35,370 (34.05) 6,016 (3.9) 12,997 (8.6) 34,758 (22.7) 25,690 (16.8) 19,458 (12.8) 8,296 (5.4) 4,346 (2.9) 3,837 (2.5) 1,796 (1.2) 117,194 (65.95) *Data presented as n (%); †male:female ratio is 1:3.31. TCM = traditional Chinese medicine. J Chin Med Assoc • July 2010 • Vol 73 • No 7 377 M.S. Jong, et al Table 2. Top 10 Chinese herbal formulae prescribed for constipation in Taiwan during 2004* Chinese herbal formulae (Chinese name) Ma-zi-ren-wan Fang-feng-tong-sheng-san Run-chang-wan Run-chang-tang Da-chai-hu-tang Ping-wei-san Mu-xiang-bin-lang-wan San-huang-xie-xin-tang Tao-ren-cheng-qi-tang Gan-lu-yin Ingredients Prescriptions, n (%) Cannabis sativa, Paeonia lactiflora, Citrus aurantium, Rheum palmatum, Magnolia officinalis, Prunus armeniaca Saposhnikovia divaricata, Forsythia suspenae, Gardenia jasminoides, Schizonepeta tenuifolia, Ephedra sinica, Ligusticum chuanxiong, Angelica sinensis, Paeonia lactiflora, Atractylodes macrocephala, Rheum palmatum, Mirabilite, Scutellaria baicalensis, Talcum, Gypsum Fibrosum, Mentha haplocalyx, Platycodon grandiflorum, Glycyrrhiza uralensis, Zingiber officinale Angelica sinensis, Notopterygium incisum, Rheum palmatum, Prunus persica, Cannabis sativa Rheum palmatum, Angelica sinensis, Rehmannia glutinosa, Cannabis sativa, Prunus persica, Prunus armeniaca, Citrus aurantium, Scutellaria baicalensis, Magnolia officinalis, Glycyrrhiza uralensis Bupleurum chinense, Scutellaria baicalensis, Paeonia lactiflora, Pinellia ternate, Citrus aurantium, Rheum palmatum, Ziziphus jujuba, Zingiber officinale Atractylodes lancea, Magnolia officinalis, Citrus reticulate, Glycyrrhiza uralensis, Zingiber officinale, Ziziphus jujuba Saussurea lappa, Areca cathechu, Rheum palmatum, Coptis chinensis, Phellodendron amurense, Cyperus rotundus, Ipomoea nil, Citrus reticulate, Citrus reticulate (unripe), Curcuma phaeocaulis, Citrus aurantium, Sparganium stoloniferum, Mirabilite Rheum palmatum, Coptis chinensis, Scutellaria baicalensis Prunus persica, Rheum palmatum, Cinnamomum cassia, Glycyrrhiza uralensis, Mirabilite Rehmannia gultinosa, Asparagus cochinchinensis, Ophiopogon japonicus, Dendrobium nobile, Artemisia scoparia, Eriobotrya japonica, Scutellaria baicalensis, Citrus aurantium, Glycyrrhiza uralensis 133,288 (34.4) 68,264 (17.6) 47,870 (12.4) 29,927 (7.7) 25,504 (6.6) 18,885 (4.9) 18,689 (4.8) 18,081 (4.7) 17,935 (4.6) 17,482 (4.5) *Total number of prescriptions = 387,268. Table 3. Top 10 single Chinese herbs prescribed for constipation in Taiwan during 2004* Single Chinese herb (Chinese name) Generic name Da-huang Hou-pu Xuan-shen Zhi-shi (fruit) Sheng-di-huang Mai-dong Shan-zha Huo-ma-zen Gan-cao Zhi-ke (peel) Rheum palmatum Magnolia officinalis Scrophularia ningpoensis Citrus aurantium Rehmannia glutinosa Ophiopogon japonicus Crataegus pinnatifida Cannabis sativa Glycyrrhiza uralensis Citrus aurantium Prescriptions, n (%) 71,133 (18.4) 25,379 (6.6) 24,528 (6.3) 23,443 (6.1) 23,212 (6.0) 23.052 (6.0) 22,055 (5.7) 19,708 (5.1) 19,273 (5.0) 17,501 (4.5) *Total number of prescriptions = 387,268. Discussion The current study, the first large-scale survey of the use of CHM in the treatment of constipation in a Chinese population, analyzed the claims dataset of TCM office visits covered by the NHI in Taiwan. Our results showed that females were dominant among TCM users, which is in agreement with the results of 378 a systematic review by Peppas et al,3 who reported that for those aged between 20 and 29 years, the femaleto-male ratio was 8.1. Chiarelli et al12 proposed that hormonal factors may contribute to constipation in women. Progesterone secreted during the luteal phase of the menstrual cycle or during gestation is thought to decrease the intestinal transit time, leading to constipation.12 In addition, we also found that most people J Chin Med Assoc • July 2010 • Vol 73 • No 7 Chinese herb use for constipation in Taiwan 80,000 70,000 63,853 64,227 59,172 60,000 Number of prescriptions 54,187 49,405 50,000 40,000 33,968 30,000 26,663 18,926 20,000 8,553 10,000 4,105 0 1 2 3 4 5 6 7 8 9 ≥10 Number of Chinese herbal formulae or single herbs in a single prescription Figure 1. The number of combinations of Chinese herbal medicine related to the number of prescriptions. The most common combination of Chinese herbal medicine used for treating constipation was 5, followed by 4 and then 3 items of Chinese herbal formulae or single herbs. There was a mean of 4.6 Chinese herbal items in a single prescription for subjects with constipation. Table 4. Most common prescription patterns of a 2-drug combination of Chinese herbs in a single prescription for constipation in Taiwan during 2004* Chinese herbal formulae or single herbs Ban-xia-xie-xin-tang plus Ma-zi-ren-wan Shao-yao-gan-cao-tang plus Ma-zi-ren-wan Yi-zi-tang plus Ma-zi-ren-wan Platycladus orientalis plus Ma-zi-ren-wan San-huang-xie-xin-tang plus Ma-zi-ren-wan Xie-fu-zhu-yu-tang plus Ma-zi-ren-wan Liu-wei-di-huang-wan plus Ma-zi-ren-wan Gan-lu-yin plus Run-chang-wan Da-huang-mu-dan-pi-tang plus Ma-zi-ren-wan Cyperus rotundus plus Ma-zi-ren-wan Support (%) Prescription number 0.7 0.7 0.6 0.6 0.6 0.6 0.6 0.6 0.5 0.5 2,855 2,781 2,441 2,301 2,297 2,209 2,203 2,150 2,097 2,087 *Total number of prescriptions = 387,268. using TCM for constipation were between 20 and 29 years of age (25.5%), followed by those between 30 and 39 years of age (19.6%), with the majority being females. This result is different from the findings reported by Higgins and Johanson,13 who showed an increase in the prevalence of constipation with age. Further studies are needed to clarify this issue and reveal other causes. J Chin Med Assoc • July 2010 • Vol 73 • No 7 Rheum palmatum, the most common single Chinese herb for constipation, is also a component of 8 of the 10 most commonly used herbal formulae for constipation. Rheum palmatum was first recorded in the classical Chinese medical tome “Shennongbencaojing”, the earliest Materia Medica in China, before 25–225 AD. At that time, Rheum palmatum was used as a type of purgative agent. The major bioactive constituents of Rheum 379 M.S. Jong, et al Table 5. Most common prescription patterns of a 3-drug combination of Chinese herbs in a single prescription for constipation in Taiwan during 2004* Chinese herbal formulae or single herbs Fang-feng-tong-sheng-sa, Rheum palmatum and Ma-zi-ren-wan Angelica sinensis, Cistanche tubulosa and Ma-zi-ren-wan Citrus aurantium, Magnolia officinalis and Ma-zi-ren-wan Rehmannia glutinosa, Fang-feng-tong-sheng-san and Rheum palmatum Areca catechu, Saussurea lappa and Ma-zi-ren-wan Da-chai-hu-tang, Fang-feng-tong-sheng-san and Rheum palmatum Crataegus pinnatifida, Fang-feng-tong-sheng-san and Ma-zi-ren-wan Run-chang-tang, Rheum palmatum and Ma-zi-ren-wan Citrus aurantium, Rheum palmatum and Ma-zi-ren-wan Run-chang-wan, Rheum palmatum and Ma-zi-ren-wan Support (%) Prescription number 0.6 0.5 0.4 0.3 0.3 0.3 0.3 0.3 0.3 0.3 2,462 1,817 1,405 1,280 1,223 1,177 1,164 1,083 1,074 1,060 *Total number of prescriptions = 387,268. palmatum are phenolic compounds, among which sennosides and anthraquinone glycosides are considered to be the main purgative components.14 This stimulant laxative or its metabolites in the human body can stimulate the intestinal wall, enhance intestinal peristalsis, or change the transport of liquid and electrolytes, thereby enhancing gastrointestinal secretion and leading to purgation.15 Besides Rheum palmatum, other Chinese herbs also have the ability to modulate gastrointestinal function. Mirabilite (sodium sulfate decahydrate) has been reported to have osmotic laxative activity through poor absorption of sulfate, which increases osmotic pressure and results in water and electrolytes being retained in the intestinal cavity.16 Ipomoea nil extracts may affect the ion transport of rat intestinal epithelia, leading to water movement.17 The aqueous crude extract of Prunus persica possesses spasmogenic activity in isolated guinea pig ileum, which may be partially through the cholinergic pathway.18 In animal experiments, the constituent arecoline in Areca catechu can stimulate colonic motility through muscarinic acetylcholine receptors.19 Angelica sinensis may possess the ability to react with serotonin receptors and then promote serotonergic activity, thereby stimulating intestinal motility.20,21 The active ingredient in Rehmannia glutinosa, catalpol, is an iridoid glycoside,22,23 and Gardenia jasminoides, which contains iridoid, may also possess purgative activity.24 In ritonavir-treated rats with slower gastric emptying capability, gastrointestinal dysfunction is improved after administration of a Scutellaria baicalensis extract.25 Zingiber officinale can speed up gastrointestinal transit in mice fed with a charcoal meal.26 The water-soluble components of Zizyphus jujuba can reduce gastrointestinal transit time, thus enhancing water retention in feces.27 The components of commonly used herbal formulae for treating constipation mostly have a purgation 380 effect, as described above by modern pharmacology. However, there are some Chinese herbs that have an opposite pharmacological function. For example, cannabidiol is a Cannabis sativa-derived compound that can selectively inhibit croton oil-induced intestinal hypermotility in mice,28 and decrease gastrointestinal movement.29 Cyperus rotundus possesses antidiarrheal activity.30 These Chinese herbs, which decrease gastrointestinal movement, have been used for the treatment of constipation. Different pharmacological functions may be due to the difference between a pure compound and a crude extract of the herb, or the combined effects of multi-component formulations, or through different pathological mechanisms. How 1 Chinese herb can exert effects that are diametrically opposed is still not fully understood and deserves further investigation. Glycycoumarin is 1 active component in Glycyrrhiza uralensis. It has an antispasmodic effect on the contraction of mouse jejunum through inhibition of the phosphodiesterase 3 mechanism.31 Other Chinese medicines such as Magnolia officinalis,32 Mentha sp.,33 and Paeonia lactiflora34 have a spasmolytic effect, which could possibly be beneficial for spasmodic constipation.35 In isolated animal tissue, the aqueous-methanol crude extract of Saussurea lappa possesses a spasmogenic effect through the cholinergic pathway. However, under conditions such as a higher drug concentration or intestinal hypermotility, the spasmolytic effect appears through a calcium channel blocker mechanism.36 Therefore, even for the same Chinese herb, there may be different pharmacological functions with different dosages or physical conditions. Among the top 10 single Chinese herbs prescribed for constipation, Scrophularia ningpoensis contains a bioactive compound, iridoid, which possibly possesses a purgative effect,23 and Crataegus pinnatifida was once reported to have an antispasmodic effect.37 In the J Chin Med Assoc • July 2010 • Vol 73 • No 7 Chinese herb use for constipation in Taiwan classification of Chinese medicine, Ophiopogon japonicus is categorized as a Yin-tonifying medicinal, capable of nourishing Yin fluid and therefore moistening the intestine. In the top 10 Chinese herbal formulae prescribed for constipation, Fang-feng-tong-sheng-san (Bofutsusho-san in Japanese) is usually used to combat obesity.38 Da-chai-hu-tang extracts and San-huangxie-xin-tang extracts relax smooth muscle tone in the gastrointestinal tract through phosphodiesterase inhibition, and are therefore capable of treating spasmodic constipation.39 Ping-wei-san is usually applied for the treatment of heartburn and gastritis.40 It is worth noting that Fang-feng-tong-sheng-san and Da-chai-hu-tang have been reported to cause interstitial pneumonia or hepatitis during clinical practice.41,42 It is often difficult to completely understand the underlying mechanisms. Therefore, it is necessary to conduct randomized, double-blinded, placebo-controlled trials to assess the efficacy and safety of these Chinese medicines in patients with constipation. Additionally, Cistanche tubulosa contains iridoid glycosides, and thus possibly has purgative effects.43 Ban-xia-xie-xin-tang is reported to have antidiarrheal activity,44 and Shao-yao-gan-cao-tang has an antispasmodic effect.45 In our study, an average of 4.6 items, either Chinese herbal formulae or single herbs, were contained in each prescription for constipation. According to our results, the most commonly prescribed CHM drug combination for treating constipation was mainly an herbal formula and single herb. This study was a retrospective analysis of the use of CHM to treat constipation. Unlike clinical trials, which can provide direct evidence of efficacy, many herbs in the herbal formulae or single herbs frequently prescribed have been found to contain ingredients that assist defecation via varied mechanisms as discussed above. In fact, the principle of TCM treatment is different from that of Western medicine, as TCM involves the patient’s constitutional needs, e.g. Bianzheng Lunzhi (ᙃᢞᓵए, syndrome differentiation and treatment),46 and therefore, it is difficult to create a constitutionallymatched control group. With regard to the treatment of constipation, although Chinese and Western medicine view the causes of the disease differently, both are in agreement that constipation is a symptom rather than a diagnosis. TCM treatment for constipation is based on the syndrome of its subclassification; for example, if the symptoms include a dry mouth, yellow urine, a red tongue and surging pulse, it is subclassified as excess syndrome (ኔᢞ) for which a formula such as Ma-zi-renwan can be prescribed, as it can discharge excessive heat.47 On the other hand, if the symptoms include J Chin Med Assoc • July 2010 • Vol 73 • No 7 fatigue, a pale complexion, pale tongue and a thready, weak pulse, it is subclassified as deficient syndrome (ဠᢞ). Therefore, a formula or single herb that can nourish Qi and Yin will be administered; in this case, Runchang-tang or Ophiopogon japonicus is a good choice. In young people, constipation is mostly subclassified as excess syndrome, which may explain why this study found Ma-zi-ren-wan to be the formula most commonly prescribed for the treatment of constipation. In conclusion, based on the availability of electronic health care claims data in Taiwan, a population-based survey of Chinese herbal pharmacoepidemiology on constipation determined the frequency of use and patterns of prescriptions in a Chinese population. Nevertheless, the therapeutic effects and safety of those herbal formulae or single herbs used requires further elucidation through efficiency-based clinical studies or well-designed randomized, double-blinded, placebocontrolled trials. Acknowledgments This study was based on a portion of data from the NHI Research Database provided by the Bureau of NHI, Department of Health, and was managed by the NHI Research Institutes in Taiwan. The interpretation and conclusions contained herein do not represent those of the Bureau of NHI, Department of Health, or National Health Research Institutes. References 1. Longstreth GF, Thompson WG, Chey WD, Houghton LA, Mearin F, Spiller RC. Functional bowel disorders. Gastroenterology 2006;130:1480–91. 2. Lu CL, Chang FY, Chen CY, Luo JC, Lee SD. Significance of Rome II-defined functional constipation in Taiwan and comparison with constipation-predominant irritable bowel syndrome. Aliment Pharmacol Ther 2006;24:429–38. 3. Peppas G, Alexiou VG, Mourtzoukou E, Falagas ME. Epidemiology of constipation in Europe and Oceania: a systematic review. BMC Gastroenterol 2008;8:5. 4. Johanson JF. Review of the treatment options for chronic constipation. Medgenmed [Computer file]. MedGenMed 2007;9:25. 5. Bharucha AE. Constipation. Best Pract Res Clin Gastroenterol 2007;21:709–31. 6. Chen FP, Chen TJ, Kung YY, Chen YC, Chou LF, Chen FJ, Hwang SJ. Use frequency of traditional Chinese medicine in Taiwan. BMC Health Serv Res 2007;7:26. 7. Cheng SH, Chiang TL. The effect of universal health insurance on health care utilization in Taiwan: results from a natural experiment. JAMA 1997;278:89–93. 8. Bureau of National Health Insurance, Department of Health, Executive Yuan, R.O.C. Available at: http://www.nhi.gov.tw/ webdata/webdata.asp?menu=1&menu_id=4&webdata_id= 1399&WD_ID= [Date accessed: August 10, 2005] 381 M.S. Jong, et al 9. Berry MJ, Linoff G. Data Mining Techniques: For Marketing Sales, and Customer Support. New York: Welly Press, 1997. 10. Han J, Kamber M. Data Mining: Concepts and Techniques. San Francisco: Morgan Kaufmann Press, 2001. 11. Chen TJ, Chou LF, Hwang SJ. Application of a data-mining technique to analyze coprescription patterns for antacids in Taiwan. Clin Ther 2003;25:2453–63. 12. Chiarelli P, Brown W, McElduff P. Constipation in Australian women: prevalence and associated factors. Int Urogynecol J 2000; 11:71–8. 13. Higgins PD, Johanson JF. Epidemiology of constipation in North America: a systematic review. Am J Gastroenterol 2004; 99:750–9. 14. Xiao P, He L, Wang L. Ethnopharmacologic study of Chinese rhubarb. J Ethnopharmacol 1984;10:275–93. 15. Ewe K. The physiological basis of laxative action. Pharmacology 1980;20(Suppl):2–20. 16. Heizer WD, Sandler RS, Seal E Jr, Murray SC, Busby MG, Schliebe BG, Pusek SN. Intestinal effects of sulfate in drinking water on normal human subjects. Dig Dis Sci 1997;42: 1055–61. 17. Tsai JC, Tsai S, Chang WC. Comparison of two Chinese medical herbs, Huangbai and Qianniuzi, on influence of short circuit current across the rat intestinal epithelia. J Ethnopharmacol 2004; 93:21–5. 18. Gilani AH, Aziz N, Ali SM, Saeed M. Pharmacological basis for the use of peach leaves in constipation. J Ethnopharmacol 2000;73:87–93. 19. Xie DP, Chen LB, Liu CY, Zhang CL, Liu KJ, Wang PS. Arecoline excites the colonic smooth muscle motility via M3 receptor in rabbits. Chin J Physiol 2004;47:89–94. 20. Deng S, Chen SN, Yao P, Nikolic D, van Breemen RB, Bolton JL, Fong HH, et al. Serotonergic activity-guided phytochemical investigation of the roots of Angelica sinensis. J Nat Prod 2006;69:536–41. 21. Galligan JJ, Vanner S. Basic and clinical pharmacology of new motility promoting agents. Neurogastroenterol Motil 2005;17: 643–53. 22. Tian YY, An LJ, Jiang L, Duan YL, Chen J, Jiang B. Catalpol protects dopaminergic neurons from LPS-induced neurotoxicity in mesencephalic neuron-glia cultures. Life Sci 2006;80:193–9. 23. Tundis R, Loizzo MR, Menichini F, Statti GA, Menichini F. Biological and pharmacological activities of iridoids: recent developments. Mini Rev Med Chem 2008;8:399–420. 24. Yamauchi K, Fujimoto N, Kuwano S, Inouye H, Inoue K. The mechanism of purgative action of geniposide, an iridoid glucoside of the fruit of Gardenia, in mice. Planta Med 1976;30: 39–47. 25. Mehendale S, Aung H, Wang CZ, Tong R, Foo A, Xie JT, Yuan CS. Scutellaria baicalensis and a constituent flavonoid, baicalein, attenuate ritonavir-induced gastrointestinal side-effects. J Pharm Pharmacol 2007;59:1567–72. 26. Yamahara J, Huang QR, Li YH, Xu L, Fujimura H. Gastrointestinal motility enhancing effect of ginger and its active constituents. Chem Pharm Bull 1990;38:430–1. 27. Huang YL, Yen GC, Sheu F, Chau CF. Effects of water-soluble carbohydrate concentrate from Chinese jujube on different intestinal and fecal indices. J Agric Food Chem 2008;56:1734–9. 28. Capasso R, Borrelli F, Aviello G, Romano B, Scalisi C, Capasso F, Izzo AA. Cannabidiol, extracted from Cannabis sativa, selectively inhibits inflammatory hypermotility in mice. Br J Pharmacol 2008;154:1001–8. 29. De Filippis D, Iuvone T, D’Amico A, Esposito G, Steardo L, Herman AG, Pelckmans PA, et al. Effect of cannabidiol on 382 30. 31. 32. 33. 34. 35. 36. 37. 38. 39. 40. 41. 42. 43. 44. 45. 46. 47. sepsis-induced motility disturbances in mice: involvement of CB(1) receptors and fatty acid amide hydrolase. Neurogastroenterol Motil 2008;20:919–27. Uddin SJ, Mondal K, Shilpi JA, Rahman MT. Antidiarrhoeal activity of Cyperus rotundus. Fitoterapia 2006;77:134–6. Sato Y, Akao T, He JX, Nojima H, Kuraishi Y, Morota T, Asano T, et al. Glycycoumarin from Glycyrrhizae Radix acts as a potent antispasmodic through inhibition of phosphodiesterase 3. J Ethnopharmacol 2006;105:409–14. Chan SS, Zhao M, Lao L, Fong HH, Che CT. Magnolol and honokiol account for the anti-spasmodic effect of Magnolia officinalis in isolated guinea pig ileum. Planta Med 2008;74:381–4. Grigoleit HG, Grigoleit P. Gastrointestinal clinical pharmacology of peppermint oil. Phytomedicine 2005;12:607–11. Yang HO, Ko WK, Kim JY, Ro HS. Paeoniflorin: an antihyperlipidemic agent from Paeonia lactiflora. Fitoterapia 2004;75:45–9. Quartero AO, Meineche-Schmidt V, Muris J, Rubin G, de Wit N. Bulking agents, antispasmodic and antidepressant medication for the treatment of irritable bowel syndrome. Cochrane Database Syst Rev 2005;2:CD003460. Gilani AH, Shah AJ, Yaeesh S. Presence of cholinergic and calcium antagonist constituents in Saussurea lappa explains its use in constipation and spasm. Phytother Res 2007;21:541–4. Chang Q, Zuo Z, Harrison F, Chow MS. Hawthorn. J Clin Pharmacol 2002;42:605–12. Akagiri S, Naito Y, Ichikawa H, Mizushima K, Takagi T, Handa O, Kokura S, et al. Bofutsushosan, an oriental herbal medicine, attenuates the weight gain of white adipose tissue and the increased size of adipocytes associated with the increase in their expression of uncoupling protein 1 in high-fat diet-fed male KK/Ta mice. J Clin Biochem Nutr 2008;42:158–66. Saegusa Y, Sugiyama A, Takahara A, Nagasawa Y, Hashimoto K. Relationship between phosphodiesterase inhibition induced by several Kampo medicines and smooth muscle relaxation of gastrointestinal tract tissues of rats. J Pharmacol Sci 2003;93:62–8. Riedlinger JE, Tan PW, Lu W. Ping wei san, a Chinese medicine for gastrointestinal disorders. Ann Pharmacother 2001; 35:228–35. Hatanaka N, Yamagishi T, Kamemura H, Nakazawa I, Hirano Y, Hosaka K, Sanno K, et al. A case of hepatitis and pneumonitis caused by Bofutsusyo-san herbal medicine. Nihon Kokyuki Gakkai Zasshi 2006;44:335–9. [In Japanese] Ikegami F, Sumino M, Fujii Y, Akiba T, Satoh T. Pharmacology and toxicology of Bupleurum root-containing Kampo medicines in clinical use. Hum Exp Toxicol 2006;25:481–94. Xie H, Morikawa T, Matsuda H, Nakamura S, Muraoka O, Yoshikawa M. Monoterpene constituents from Cistanche tubulosa: chemical structures of kankanosides A-E and kankanol. Chem Pharm Bull 2006;54:669–75. Kase Y, Hayakawa T, Ishige A, Aburada M, Komatsu Y. The effects of Hange-shashin-to on the content of prostaglandin E2 and water absorption in the large intestine of rats. Biol Pharm Bull 1997;20:954–7. Ai M, Yamaguchi T, Odaka T, Mitsuhashi K, Shishido T, Yan J, Seza A, et al. Objective assessment of the antispasmodic effect of shakuyaku-kanzo-to (TJ-68), a Chinese herbal medicine, on the colonic wall by direct spraying during colonoscopy. World J Gastroenterol 2006;12:760–4. Chen FP, Chen FJ, Jong MS, Tsai HL, Wang JR, Hwang SJ. Modern use of Chinese herbal formulae from Shang-Han Lun. Chin Med J 2009;122:1889–94. Cheng CW, Bian ZX, Wu TX. Systematic review of Chinese herbal medicine for functional constipation. World J Gastroenterol 2009;15:4886–95. J Chin Med Assoc • July 2010 • Vol 73 • No 7 Chinese herb use for constipation in Taiwan Appendix I. Summary of the scientific and Chinese equivalents of herbs and names appearing in this article Angelica sinensis Areca catechu Artemisia scoparia Asparagus cochinchinensis Atractylodes lancea Atractylodes macrocephala Bupleurum chinense Cannabis sativa Cinnamomum cassia Citrus aurantium Citrus reticulate Cistanche tubulosa Coptis chinensis Crataegus pinnatifida Curcuma phaeocaulis Cyperus rotundus Dendrobium nobile Ephedra sinica Eriobotrya japonica Forsythia suspense Gardenia jasminoides Glycyrrhiza uralensis Gypsum Fibrosum Ipomoea nil ᅝូ ឳᄏ ౼ຫ ֚॰מ ፧ؠ ؠػ ־ո ெࣤ ᷾ኔʻླྀʼ ॹʻຫʼؼ ۚⳠፚ ႓ຑ ՞⛹ ⌇ؠ ଉॵ فක ႓ ࣣᆺ ຑ ՞ඹ ز౻ فፏ ׄ Ligusticum chuanxiong Magnolia officinalis Mentha haplocalyx Mirabilite (sodium sulfate decahydrate) Notopterygium incisum Ophiopogon japonicus Paeonia lactiflora Phellodendron amurense Pinellia ternate Platycladus orientalis Platycodon grandiflorum Prunus armeniaca Prunus persica Rehmannia glutinosa Rheum palmatum Saposhnikovia divaricata Saussurea lappa Schizonepeta tenuifolia Scrophularia ningpoensis Scutellaria baicalensis Sparganium stoloniferum Talcum Zingiber officinale Ziziphus jujuba ՟ᮺ দڸ ᜳ๛ᆺ ߝ࿎ ु ຽ॰מ ߟᢐ ႓ਹ ת ਹո ே ޖո ո چ႓ Օ႓ ଅ ֵଉ ౸ग़ خ ႓ᴗ Կᆆ ᄶف س᜶ Օའ Appendix II. Summary of the English (Hanyu Pinyin) and Chinese equivalents of formulae and names appearing in this article An-zhong-san Ban-xia-xie-xin-tang Da-chai-hu-tang Da-huang-mu-dan-pi-tang Fang-feng-tong-sheng-san Gan-lu-yin Liu-wei-di-huang-wan Ma-zi-ren-wan Mu-xiang-bin-lang-wan ڜխཋ תើ֨ྏ Օྏ Օ႓߃կྏؼ ଅຏᆣཋ زႏ ք࠺چ႓Մ ոՄ Ping-wei-san Run-chang-tang Run-chang-wan San-huang-xie-xin-tang Shao-yao-gan-cao-tang Tao-ren-cheng-qi-tang Xie-fu-zhu-yu-tang Yi-zi-tang ؓષཋ ᑮᆩྏ ᑮᆩՄ Կ႓ើ֨ྏ ߟᢐز౻ྏ ոʻுʼࢭྏ ۨࢌດᅟྏ Ԭྏڗ ֵଉឳᄏՄ J Chin Med Assoc • July 2010 • Vol 73 • No 7 383








© Copyright 2026