
BK Virus: A Clinical Review Mark D. Reploeg, Gregory A. Storch,
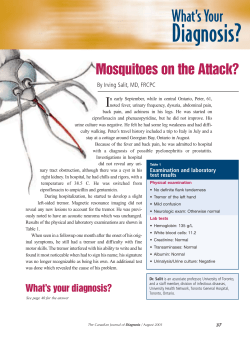
REVIEW ARTICLE BK Virus: A Clinical Review Mark D. Reploeg,1 Gregory A. Storch,2 and David B. Clifford1 1 Department of Neurology and 2Departments of Pediatrics, Medicine, and Molecular Microbiology, Washington University School of Medicine, St. Louis BK virus, a relative of JC virus, which is the etiologic agent of progressive multifocal leukoencephalopathy (PML), was first isolated in 1971 from a urine sample obtained from a renal transplant recipient [1]. The name of the virus refers to the first patient’s initials, which is also true of JC virus [2]. This member of the polyoma subgroup of papovaviruses, which includes BK virus, JC virus, and simian virus 40 (SV-40) [3], is a ubiquitous virus with peak seroprevalence in early childhood that ranges from 60% to 100% [4–9]. Epidemiological studies were performed in a variety of countries, including England (peak seroprevalence in early childhood, 83%) [7], Finland (60%) [8], Germany (71%) [10], Italy (83%) [6], and the United States (69%, 100%) [4, 5]. Differences in percentages can be explained by the age of the tested subjects and the antibody titer threshold that is considered to be positive. Primary infection with this double-stranded DNA Received 26 July 2000; revised 7 December 2000; electronically published 20 June 2001. Reprints or correspondence: Dr. Mark D. Reploeg, c/o Dr. David B. Clifford, Washington University School of Medicine, Neurology, Box 8111, 660 S. Euclid, Saint Louis, MO 63110 ([email protected]). Clinical Infectious Diseases 2001; 33:191–202 2001 by the Infectious Diseases Society of America. All rights reserved. 1058-4838/2001/3302-0009$03.00 virus is generally asymptomatic and occurs in childhood. The most common symptoms, when symptoms are noted, are fever and nonspecific upper respiratory infection [3, 5, 8, 11]. After primary infection has occurred, the virus can remain latent in many sites [12–27], most notably the kidney [24] (there is controversy regarding latent infection of other sites [26, 28–32]). Transmission may occur by means of exposure to bodily fluids, such as oral secretions, or via transplacental passage [10, 17, 18, 33–35]. In states of relative or absolute cellular immunodeficiency, the virus can become reactivated and cause disease. Figure 1 illustrates the course of BK viral infection. The kidney, lung, eye, liver, and brain are sites of BK virus–associated disease, both primary and reactivated. BK virus infection in the kidney manifests as hemorrhagic and nonhemorrhagic cystitis [36–46], ureteric stenosis [1, 47, 48], and nephritis [19, 49–60]. Pulmonary diseases that involve BK virus include pneumonitis [19, 59, 61] and acute nonspecific upper respiratory tract infection [8, 11, 62]. To date, reports regarding ophthalmologic manifestations are limited to one description of a patient with bilateral atypical retinitis [63]. Liver involvement has also been reported only rarely [64]. BK virus has also been detected in the tissue samples of a variety of neoplasms, which have predominantly been brain tumors of glial and neural BK Virus • CID 2001:33 (15 July) • 191 Downloaded from http://cid.oxfordjournals.org/ by guest on September 9, 2014 We present a review of the clinically oriented literature about BK virus, a relative of JC virus, which is the etiologic agent of progressive multifocal leukoencephalopathy (PML). The kidney, lung, eye, liver, and brain have been proposed as sites of BK virus–associated disease, both primary and reactivated. BK virus has also been detected in tissue specimens from a variety of neoplasms. We believe that BK virus is most often permissively present in sites of disease in immunosuppressed patients, rather than being an etiologic agent that causes symptoms or pathologic findings. There is, however, strong evidence for BK virus–associated hemorrhagic cystitis and nephritis, especially in recipients of solid organ or bone marrow transplants. Now that BK virus can be identified by use of specific and sensitive techniques, careful evaluation of the clinical and pathologic presentations of patients with BK virus will allow us to form a clearer picture of viral-associated pathophysiology in many organ systems. We selected articles for review on the basis of a complete search of the Medline database that was conducted in September 2000 and that used the key words “BK virus” and the subject “Polyomavirus hominis 1.” We selected 577 English-language articles from the 611 citations. Articles were then screened for their general applicability to clinical practice. Further citations were identified from the reference sections of selected individual articles. By use of this method, a total of 158 papers were analyzed in detail for review. BK VIRUS TRANSMISSION origin [16, 65–70], although there is controversy regrading associations between these neoplasms and BK virus [71–77]. A few investigators have proposed various mechanisms whereby BK virus can induce neoplasia [20, 65, 68, 70, 78–87]. Table 1 summarizes the proposed mechanisms of BK virus–induced neoplasia. There may even be an association between BK virus and autoimmune disease [90]. Although rarely recognized, BK virus might cause both primary CNS disease and reactivation CNS disease as well [19, 49, 91, 92]. Table 2 summarizes the diseases that have been reported to be associated with BK virus. Our study is intended as a review of the literature regarding all reported types of BK virus–associated disease, with some emphasis on neurologic manifestations of BK virus. The development of diagnostic testing has made clinical correlations with BK infection possible. In this article, we review clinical observations associated with this virus and we summarize the observations that have been made to date in this evolving clinical diagnostic era. Both primary and reactivated disease in various organs, along with pertinent pathologic findings, diagnosis, and treatment, where appropriate, will be discussed. It is important to understand the spectrum of disease that may be attributed to BK virus, because BK virus may cause disease in multiple organ systems, especially in immunosuppressed patients. 192 • CID 2001:33 (15 July) • Reploeg et al. Downloaded from http://cid.oxfordjournals.org/ by guest on September 9, 2014 Figure 1. Proposed life cycle of BK virus as applicable to human disease. URI, upper respiratory infection; ?, organ systems or disease processes whose association with BK virus has uncertain support in the literature. Many different routes for the transmission of BK virus have been hypothesized. According to many authors, respiratory transmission is the most likely route [17, 33]. The supportive studies are epidemiological in nature, and no laboratory, to our knowledge, has isolated BK virus on cultures of samples of respiratory secretions. Sexual transmission has been proposed as another mechanism [18, 94]. Monini et al. [18] detected BK virus in 57% of specimens of genital tissues and 95% of sperm samples. Because primary infection generally occurs before the age of sexual activity, this hypothesis would assume a sexually transmitted trigger for reactivation of BK disease [5]. A final proposed mechanism of transmission is transplacental passage of BK virus. This mechanism was postulated soon after the discovery of BK virus [10, 34], although further studies were unable to demonstrate isolation of BK virus from specimens of either maternal or fetal tissues [95]. It was not until more sensitive techniques were developed, such as PCR, that Pietropaolo et al. [35] demonstrated the presence of BK viral DNA in a high proportion of aborted fetuses and in the products of normal pregnancies. Other modes can be considered for BK viral transmission, including via urine and blood. As is discussed in the BK Latency section, BK virus can remain latent in the kidney in immunocompetent and immunodeficient patients with viruria with a range of 0%–60% of patients [96], depending on the assay that was used in the study [3, 97–99]. In one study, an increase in prevalence of viruria correlated with a decrease in CD4 cell count [99]. Although it is unknown whether transmission via urine may be another means by which BK virus is spread, it should be noted that BK virus has been isolated in cultures of urine samples cultured with human embryonic kidney [47] and lung [1, 100] cell lines. A similar argument can be made regarding the spread of BK virus via exposure to blood, because BK virus has been demonstrated to be present in peripheral blood leukocytes by use of in situ DNA hybridization (ISH) [21]. However, demonstration of the presence of BK virus by means of cultures of peripheral blood leukocytes, to our knowledge, has not been successfully attempted. Table 1. Proposed mechanisms by which BK virus may induce neoplasia. BK virus substrate Interaction Host cell substrate Mechanism of neoplasia Reference BK T Ag Binding p53 Blockade of apoptosis [82] BK T Ag Unknown pRb, p107, p130 Blockade of apoptosis [82–84] BK T Ag Unknown E2F Increased cell growth or division [82, 84] BK T Ag Unknown Host cell DNA Chromosomal aberrations [82, 85, 86] BK T Ag Unknown Estrogen receptors Estrogen-mediated cell growth or division [88, 89] BK DNA Binding HIV Tat1 protein Induce expression of BK virus genes [81] BK DNA promoter Rearrangement BK DNA promoter Increased BK viral replication [65, 68, 87] BK VIRUS LATENCY BK VIRUS AND RENAL DISEASE Primary BK virus infection is proposed as the cause of a variety of renal diseases, including hemorrhagic and nonhemorrhagic cystitis in immunocompetent and immunocompromised patients [38–40]. There are also 2 case reports of tubulointerstitial nephritis; one patient had underlying hyperimmunoglobulin M immunodeficiency [51], and the other patient had cartilage hair hypoplasia and Hodgkin’s disease [52]. To date, the kidney is the most reported site of BK virus reactivation. Disease associations range from asymptomatic hematuria to hemorrhagic cystitis in recipients of bone marrow transplants and renal allograft transplants [36, 37, 41–44, 46]. It should be noted that acute, late-onset, long-duration hemorrhagic cystitis is the type of cystitis that is most often associated with BK virus [45, 46, 100], rather than early-onset transient cystitis, which often is secondary to treatment with cyclophosphamide [46]. In recipients of renal allograft transplants, BK virus–induced ureteric stenosis [1, 47, 48] and tubulointerstitial nephritis [50, 53–55, 58, 60] may be observed, as demonstrated by means of ISH [47] and IHC [50, 53–55, 58, 60] techniques, respectively. Hypotheses regarding the association of BK virus with hemorrhagic and nonhemorrhagic cystitis are supported by seroepidemiologic evidence—that is, increases in immunoglobulins that are specific for BK viral proteins and the circumstantial presence of BK viruria at the time of presentation [36, 37, 41–44, 46]. BK virus–induced allograft nephropathy may be more common in patients who are treated with certain immunosuppressive regimens. Some supportive evidence exists for an association with tacrolimus [53, 56, 109] and mycophenolate mofetil [57], although prospective data are needed to confirm these findings. Other renal BK Virus • CID 2001:33 (15 July) • 193 Downloaded from http://cid.oxfordjournals.org/ by guest on September 9, 2014 Many authors have reported that BK virus can exist in a latent phase in various organs [12–27]. Much of the data are based on PCR experiments; exceptions are mentioned below. Similar in concept to the latent state of the herpesvirus [101], these authors propose that BK virus can remain within a cell in a nonreplicating or minimally replicating form. Within the cell, the latent viral genome may either remain episomal or it may be integrated in the host cell genome. In either state, few if any viral genes are transcribed, thereby keeping the virus out of reach of the immune system. Implicit in the definition of latency is the concept of virus reactivation in certain settings [101]. Virus reactivation and the variety of primary infections that are associated with BK virus, according to organ system, are discussed below. The kidney is the most common reported site of latent infection [24–26]. This has been demonstrated by means of both immunohistochemistry (IHC) [102] and ISH [24, 26]. The second most common reported site of latent infection is the brain [12, 14–16, 27], although some laboratories have failed to reproduce these findings [26, 30–32]. Peripheral blood leukocytes are also proposed as a site of latency [16, 21–23]; one laboratory demonstrated this by means of ISH [21], although others laboratories have failed to replicate their results [28, 29]. A more recent study has even suggested that BK virus is only present in the blood during the period of reactivation and not during latency [103]. There are limited data that suggest the involvement of other sites and tissues, including the pituitary gland [13], tonsils and nasopharynx [17], genital tissues and sperm [18], lung [19], liver [20], and bone [16]. In the sites of latent BK virus infection, the particular cell types that are involved include blood leukocytes [21], connective tissue cells, uroepithelial cells, endothelial cells, ependymal cells in the brain, and astrocytes [33, 102]. Reactivation disease is observed in patients with relative or absolute immunodeficiency (generally cellular immunodeficiency rather than humoral immunodeficiency), which is made evident by the increased frequency of reactivation disease in HIV-infected patients and patients who have received organ transplants [3]. States of mild immune impairment can lead to increased virus replication and the presence of the virus in urine. This phenomenon occurs, for example, in pregnant women [92, 104, 105], patients with diabetes [106], and elderly patients [107]. States of more severe immune compromise, such as AIDS, lymphoproliferative disease, or immunosuppressive therapy, occasionally result in rampant virus replication and damage to the involved organs [33, 108]. Table 2. Diseases to date that have been associated with BK virus. a Site, type of disease Disease Reference CNS Primary Reactivation Encephalitis [91] Guillain-Barre´ syndrome [92] Meningoencephalitis [19, 49] Hemorrhagic or nonhemorrhagic cystitis [38–40] Kidney Primary Reactivation Tubulointerstitial nephritis [51, 52] Hemorrhagic cystitis or hematuria [36, 37, 41–44, 46] Tubulointerstitial nephritis [19, 49, 50, 53–60] Ureteric stenosis [1, 47, 48] Pulmonary system URI nonspecific [8, 11, 17, 62] Interstitial desquamative pneumonitis [19, 59, 61] Atypical retinitis [63] Eyes Reactivation Liver Hepatitis (transient) [64] Autoimmune system Systemic lupus erythematosus [90] CNS neoplasms Astrocytoma [16, 68] Choroid plexus papilloma [16] Ependymoma [16, 65, 67, 68] Glioblastoma [16, 66, 68] Glioma [65, 66] Meningioma [65, 66, 68] Neuroblastoma [16, 65] Oligodendroglioma [16, 66, 68] Spongioblastoma [16, 68] Pancreas Islet cell tumors [68, 93] Renal neoplasms Kidney and urinary tract [20, 87] Sarcoma neoplasms Ewing’s tumor [65] Osteogenic [65] Bone neoplasms Reticulum cell [69] Giant cell [16] a Causality has not been proven for most of these diseases. manifestations that have been reported include 5 cases of nephritis in patients with AIDS [19, 49, 50, 58, 59]. Of note, 2 of these 5 patients were also found to have BK virus–associated neurologic disease [19, 49]. Pathologic lesions in the kidney after BK virus infection have a characteristic appearance. Macroscopically, investigators report streaky fibrosis of the medulla and circumscribed cortical scars [19, 49]. Microscopically, one sees sclerosed glomeruli, atrophic and necrotic tubules, and interstitial fibrosis associated with a mononuclear cell infiltration [19, 49, 51, 58, 59]. Fibrocytes and tubule cells are often enlarged with intranuclear inclusions that test positive for BK viral DNA by use of ISH [19, 52, 102]. Because of this strong histopathologic evidence, 194 • CID 2001:33 (15 July) • Reploeg et al. BK virus can be considered an important cause of disease in the kidney, especially tubulointerstitial nephritis in patients who have received transplants [53–55]. Diagnosis of BK virus–induced kidney disease has relied heavily on biopsy-based evidence because of the nonspecificity of BK viruria [3, 56, 96–99]. Recently, PCR testing of plasma samples obtained from recipients of renal allograft transplants, which used seminested primers, has proven to be a sensitive (100%) and specific (88%) means to determine BK virus– associated nephropathy [110], although we recommend performing a renal biopsy to confirm a positive PCR result. This significant finding may pave the way to a greater understanding of all BK virus–associated diseases. Downloaded from http://cid.oxfordjournals.org/ by guest on September 9, 2014 Primary Reactivation BK VIRUS AND PULMONARY DISEASE Some children with acute, nonspecific, upper respiratory tract infections have primary BK virus infections, as demonstrated by the finding of serologic studies of an increase in the levels of IgM specific for BK viral proteins [8, 11, 62]. One article described an 8-month-old child who had fatal BK virus– associated interstitial pneumonia after the child underwent bone marrow transplantation [61]. Goudsmit et al. [11] also found BK viral DNA in the tonsils of children with recurrent attacks of upper respiratory tract infection, although the researchers could not recover any infectious virus particles. Another report demonstrated the presence of BK viral DNA in 2 of 201 nasopharyngeal aspirates specimens obtained from children with acute, nonspecific, upper respiratory tract infections; however, once again, no infectious particles were isolated, and the results of IHC that was specific for BK viral antigens were negative [17]. The inability to isolate the virus from these samples and the infrequency of aspirates that test positive for BK virus brings into question issues regarding primary respiratory infection. Reactivation pulmonary disease in association with BK virus has been reported twice in the literature. One case report described a patient with AIDS for whom the findings of a pathologic examination, which included results of IHC that were positive for BK viral antigens, confirmed interstitial desquamative pneumonitis [19]. Of note, this patient also had neurologic symptoms. Another patient with AIDS who had interstitial pneumonitis was recently described; the interstitial pneumonitis progressed to acute respiratory distress syndrome and the patient died [59]. Fibrosis, although nonspecific, is the most common finding in tissues samples obtained from patients who have experienced BK viral infection and replication. The pathologic findings of the lung of the patient reported by Vallbracht et al. [19] were consistent with those of BK viral infection in that the primary finding was fibrosis. There were intra-alveolar aggregates of pneumocytes, focal hemorrhages, and areas of focal interstitial fibrosis associated with a mononuclear cell infiltrate. Pneumocytes, fibrocytes, and occasional endothelial cells were found to contain BK viral DNA, by means of ISH, and viral antigens, by means of IHC [19]. The second patient with AIDS had similar pathologic findings—diffuse alveolar damage and mild interstitial inflammation [59]. The ISH evidence makes the association strong, but again, there is no proof of causality. BK VIRUS AND OPHTHALMOLOGIC DISEASE Ophthalmologic manifestations are described in only 1 recent report of a case of reactivation disease that presented as bilateral atypical retinitis in a patient with AIDS [63]. The patient presented with subacute visual deterioration and other neurologic symptoms [49]. The lesions that were found during the clinical examination were consistent with those of multifocal retinitis and were unlike the lesions that are frequently associated with cytomegalovirus (CMV) or toxoplasmosis [63]. Pathologic investigation of the eye disclosed several areas of retinal necrosis of full thickness in the outer portion of the retina. BK viral DNA was found by use of PCR; CMV DNA was also revealed in some samples. Further investigation determined CMV to be a contaminant from peripheral blood cells [63], because BK virus was present, as determined by use of ISH and IHC, whereas CMV was not. Further studies are required before BK virus can be considered an important cause of ophthalmologic disease. BK VIRUS AND HEPATIC DISEASE There is a single report in the literature regarding an association between BK virus and hepatic dysfunction. Transient elevations of liver enzymes were found in a majority of patients who were concurrently found to be excreting virus in the urine [64]. There are no reports of pathologic findings in the liver associated with BK viral infection, although one study did demonstrate the presence of BK viral DNA in normal liver tissue [20]. To our knowledge, these observations have not been replicated, and we include them here only for the sake of completeness. BK VIRUS AND AUTOIMMUNE DISEASE There is literature that described an association between BK virus infection and a number of autoimmune disorders— namely, systemic lupus erythematosus. Many researchers have BK Virus • CID 2001:33 (15 July) • 195 Downloaded from http://cid.oxfordjournals.org/ by guest on September 9, 2014 There is a small amount of literature concerning the treatment of patients with BK virus disease in the kidney. For example, surgical intervention to relieve obstruction has been used to treat patients with ureteric stenosis [60]. Vogeli et al. [46] reviewed the means of treating bone marrow transplant recipients with hemorrhagic cystitis associated with BK virus. When hemorrhagic cystitis is mild, it has been treated with intravenous hyperhydration with some success. In more severe cases, such treatments as laser vaporization of papulous tumors (if present at the site of bleeding) and insertion of suprapubic catheters, followed by continuous bladder irrigation, have met with more modest success, although they are only reserved for life-threatening situations [46]. One recent study of patients who had interstitial nephritis after they underwent kidney allograft transplantation found that a reduction in the doses of the drugs used in immunosuppressive therapy is currently the best therapeutic approach [55]. This therapy is difficult to administer to patients who have undergone transplantation because of the risk of graft rejection. noted the induction of anti–double-stranded DNA and histone antibodies caused by primary BK virus infection and reactivation disease [89, 111–115]. This finding in humans has been replicated experimentally in mouse models [116]. Another group of researchers reported an increased prevalence and persistence of BK viruria in patients with systemic lupus erythematosus. In their study, the prevalence of BK viruria was 16% in patients with systemic lupus erythematosus and 0% in controls. Of the 20 patients who were tested, persistent or recurrent viruria was found in 60% of patients with systemic lupus erythematosus [90]. This same relationship is seen between BK virus and other autoimmune diseases, including rheumatoid arthritis and polymyositis [117]. Although whether there is causality has not been determined, the possibility of an association deserves further consideration and research. Neoplastic tissue types. The transforming activity of BK virus has long been known from many authors’ work with human, transgenic, and other mammalian cell lines [66, 79, 92, 118–121]. Subsequent work has focused on the search for BK virus DNA in many human neoplasms. In particular, brain tumors, such as ependymomas, meningiomas, glioblastomas, gliomas, neuroblastomas, oligodendrogliomas, spongioblastomas, choroid plexus papillomas, and neurinomas, have been shown to contain BK viral DNA [15, 16, 65–68]. There is some controversy, however, concerning the presence of BK viral DNA in glioblastoma multiforme tumors [71, 72]. In the literature, other tumors, including pituitary adenomas [13], pancreatic islet cell tumors [68, 93], reticulum cell sarcomas [69], Ewing’s sarcomas, osteogenic sarcomas [65], carcinomas of the kidney and urinary tract [20, 87], and giant cell tumors of bone [16], have been reported to be associated with BK virus. In some studies, BK viral DNA was found integrated into the host genome; in other studies, it was found to be merely episomal. It should be noted, however, that BK viral DNA can be present episomally in BK virus–transformed human cell lines [119, 122]. Because of the ubiquity of BK viral infection and the variable location of the DNA within the cells, a few investigators have questioned the association of these tumors with BK virus [71, 73–77]. Because of the amount of negative evidence, it is difficult to consider BK virus to be the causative agent of any human cancer. In fact, one tumor type that was previously associated with BK virus, Kaposi’s sarcoma [18], is now thought to be caused by human herpesvirus type 8 [123, 124]. Although it is not proof of causality, the strongest data, including demonstration of viral DNA integration into tumor cell genomes, and even the findings of some in situ studies, support a correlation between BK virus and many brain and urinary tract tumors [66, 70, 87]. 196 • CID 2001:33 (15 July) • Reploeg et al. Downloaded from http://cid.oxfordjournals.org/ by guest on September 9, 2014 BK VIRUS AND NEOPLASIA General mechanisms for neoplasia. There are many proposed mechanisms for BK virus–induced neoplasia, as was recently described in a review by Imperiale [125] (table 1). Some researchers have found that BK virus T antigen can bind to and functionally inhibit p53 and the p53-mediated response to DNA damage in vivo and in vitro [82]. Also, there are data that show T antigen can bind and inhibit pRb tumor– suppressor gene products in vitro, either by directly [83] or indirectly [84] binding pRb. Other in vivo studies demonstrate that T antigen can induce serum independent cell growth and the expression of free E2F, which is a protranscriptional protein [82, 84]. These findings have found additional support in studies of human neuroblastoma tumors, which once again have demonstrated the binding of the BK virus T antigen and p53 in situ [70]. Other researchers that have observed the same phenomenon from a different perspective have examined the association of BK viral infection with an increased number of chromosomal aberrations. The induction of chromosomal aberrations via BK virus T antigen is observed in vitro in human fibroblast cell lines [85]. Also, one study reported that a group of patients with polyomavirus infection who were exposed to radiation experienced a greater number of chromosomal aberrations than did a similar group of persons without infection [86]. Sequence variability. A topic that is often discussed in the literature about BK virus–related neoplasia is the variability noted among strains of the virus [17, 126–132]. These unique strains have been characterized ever since BK viral DNA was first fully sequenced [133]. A great deal of recent work centers on the various strains of BK and the differences in the transcriptional control region, as was recently reviewed by Moens et al. [132]. Knepper and diMayorca [20] examined BK viral DNA that was isolated from a healthy liver and a kidney carcinoma. They found that the BK viral DNA isolated from the kidney carcinoma had overrepresented promoter and origin regions, which suggests that transformation may follow DNA rearrangement [20], as is seen with other human DNA viruses, namely hepatitis B and CMV [134, 135]. Although there is disagreement [136], a number of other studies elegantly support the view that certain strains of BK virus are capable of contributing to the formation of unique neoplasms [65, 68, 87]. Rearrangements that lead to increased and differential pathogenicity are not limited to neoplasia [50, 137, 138]. Jin et al. [137], building on earlier studies, have developed PCR techniques to identify 4 major strains of BK virus. Their laboratory also noted differences in the isolated strains of BK virus among groups of infected patients [138]. Although the associations were not strong enough to lead to any definitive conclusions, they suggest that certain strains of virus may require certain host susceptibilities for infection. Another study found a mutation in BK viral DNA associated with tubulointerstitial ne- BK VIRUS AND NEUROLOGIC DISEASE Before a discussion of BK virus and neurologic disease can happen, some background information must be provided regarding the related papovavirus, JC virus, because the literature about both viruses is intimately linked. JC virus is the etiologic factor in PML [2, 141, 142]. Its presence in the CSF of patients who are suspected of having PML, as detected by PCR, is rather specific (range of specificity, 83%–100%) [12, 143–150], depending on the technique that was used in the study. JC viral DNA has also been detected in specimens of brain tissue obtained from patients without PML, which suggests that the virus has a latent phase [12, 27, 30, 31, 146, 151–154]. The reported prevalence of latency is as high as 68% [30]. The authors of other studies disagree with the concept of JC viral latency in the brain and propose that JC virus is only found in the samples of brain tissues obtained from patients with PML [14, 25, 32, 155, 156]. The literature about BK virus has a similar history: some studies support [12, 15, 16, 27] and other studies refute [26, 30–32] theories regarding the possibility of BK viral latency in brain tissue. The studies that were able to detect BK viral DNA consistently in specimens of brain tissue used PCR assays as the sole technique. The percentage of specimens of brain tissue obtained from patients without HIV and PML that tested positive by use of PCR ranged from 20% [27] to 100% [16]. Vago et al. [12] detected BK virus DNA by use of PCR in specimens of brain tissue of 2 of 13 HIV-infected patients who had PML and 1 of 16 HIV-infected patients who did not have PML. It is likely that the differences between the laboratory findings can be explained by the differential sensitivity of the assays that were used in each of the laboratories. It is known that BK viral DNA is present in very low copy numbers, from 1 to 20 genome equivalents per 200 cells [27]. These low numbers may lead to false negative results, depending on the size and the quality of the sample that was tested, especially for ISH studies. Therefore, it is predictable that we were unable to find a study in the literature that had ISH data to support the concept of BK viral latency in the brain. There are a number of arguments against the concept of latency that explain the presence of BK virus in the brains of healthy people. One argument is that the presence of BK viral DNA, as demonstrated by use of PCR, may have been the result of contamination by peripheral blood leukocytes, which BK virus is known to inhabit [16, 21–23]. It is unclear how much this observation affects the interpretation of the literature regarding BK virus. In light of the difficulties in obtaining ISH evidence and the potential for contamination, we believe that there is not yet enough data to conclude that BK virus can remain latent in the brains of both healthy persons and immunosuppressed persons. Further investigation is required to either support or refute the concept of viral latency in the brain for BK virus and other viruses, including JC virus. BK viral DNA has only rarely been reported in samples of CSF; this is not true of JC virus, which is common in the CSF samples obtained from patients with PML. To our knowledge, there are 4 cases reported in the literature that do not have CSF data, and there are 3 recent reports that demonstrate evidence of BK viral DNA in the CSF [19, 49, 89, 150]. There are 2 reports from 1977 that mention BK virus in association with neurologic symptoms, but CSF analysis is not included in the reports. One article reviewed 3 cases of BK virus seroconversion (as determined by a rise in IgM BK virus–specific antibodies in the serum), associated with neurologic symptoms. One patient was a 3-year-old child with the symptoms of an upper respiratory tract infection and convulsions [92]. The other 2 patients experienced serologically determined BK viral primary infection at the ages of 33 and 45 years. Both of these patients had the symptoms of a respiratory infection, and it is interesting to note that both patients developed an acute inflammatory polyradiculopathy [92]. The second study from 1977 described a recipient of a bone marrow transplant who developed BK viruria and neurologic symptoms [157]. The report is somewhat confounded by the concurrent presence of CMV infection and the lack of description of the BK Virus • CID 2001:33 (15 July) • 197 Downloaded from http://cid.oxfordjournals.org/ by guest on September 9, 2014 phritis that leads to end stage renal failure. The authors suggest that this mutation may have led to the increased virulence of BK virus [50]. Viral trans activation. Another mechanism to increase virulence is via trans activation, either by native cell proteins or proteins produced by other viruses. Much of the early work on this topic centered on the SV-40 virus, the simian counterpart to JC and BK viruses. However, one group of researchers looked specifically at BK virus: Moens et al. [88, 89] demonstrated indirect interaction between the large T antigen of BK virus and native cell estrogen receptors that, via trans activation, enhances the promoter of BK virus. The researchers postulated that there was a hormone-mediated association with BK virus reactivation and even neoplasia, although the relationships have yet to be fully elucidated. Trans activation also may play a role in interactions between HIV and BK that lead to an increased expression of HIV DNA [139]. The relationship of concomitant HIV infection with BK virus and neoplasia has also been explored. There is in vitro evidence to suggest that an interaction between intracellular HIV-1 Tat protein and BK viral DNA may lead to hyperplastic, dysplastic, and metastatic lesions in mice [78–81]. Tada et al. [140] hypothesize that HIV plays a role in the trans activation of many DNA viruses, and vice versa, which may explain the prevalence of unique virus-mediated complications of HIV infection in addition to the degree of immunosupression caused by HIV itself. BK VIRUS AND TREATMENT To date, there is little in the literature concerning the treatment of patients with BK viral infection. One of the few, more-recent reports discussed treatment in a retrospective study of children with hemorrhagic cystitis after they underwent bone marrow transplantation [46]. The treatments are based not on the cause but rather the effect of the viral infection. A study of interstitial nephritis in patients who had undergone kidney allograft trans- 198 • CID 2001:33 (15 July) • Reploeg et al. plantation found that reducing the dose of immunosuppressive therapy is currently the best therapeutic approach [55]. Theoretically, decreasing the amount of immune suppression, if it present from any cause, would lead to better host clearance of the virus. This therapy has obvious deleterious implications regarding one of the largest groups of patients affected by BK virus—renal and bone marrow transplant recipients—and, therefore, this therapy is limited in its application. However, in patients with HIV, improved control of HIV infection by use of highly active antiretroviral therapy should lead to decreased BK virus–associated symptoms. To date, this has yet to be shown in any studies. CONCLUSION Nearly 3 decades of research have led to only a minimal understanding of BK virus and its pathophysiology. This fact attests to the elusive nature of viruses and the challenge they pose to their investigators. From the information we have, it appears that humans are nearly universally exposed to BK virus in childhood with minimal symptoms. Although the data are largely epidemiological and circumstantial, BK virus is likely transmitted via the respiratory route. After a patient has primary infection, BK virus can remain latent in many tissues, including the kidney and possibly the brain. States of relative or absolute cellular immunodeficiency may lead to viruria or reactivation disease. Also, as is apparent from the neoplasia literature, viral coinfection and trans activation may play a role in reactivation disease and even in tumor induction. We believe that BK virus is most often permissively present in sites of disease in immunosuppressed patients, rather than being an etiologic agent that causes symptoms or pathologic findings. The strongest evidence for a BK virus–associated disease exists for hemorrhagic cystitis and BK virus–associated nephritis, especially in recipients of solid organ or bone marrow transplants. BK virus can now be identified by use of specific and sensitive techniques. A careful evaluation of the clinical and pathologic presentations of patients with BK virus will allow us to form a clearer picture of virus-associated pathophysiology in other organ systems, including the liver, lungs, eyes, and CNS, and in other disease processes, including neoplasia. Acknowledgments We thank Dr. Sandra C. Paek, Dr. Paula K. Raybuck, and Nancy Green for their assistance in the preparation of this article. Downloaded from http://cid.oxfordjournals.org/ by guest on September 9, 2014 neurologic symptoms. Although the connection between BK virus and neurologic symptoms is loose, these are some of the few appearances in the literature of this association. The first more-recent case of neurologic symptoms associated with BK virus was from 1993, when BK virus was identified as the causative agent of subacute meningoencephalitis in a 27year-old man with hemophilia type A and AIDS [19]. The patient was also noted to have a tubulointerstitial nephropathy, interstitial desquamative pneumonitis, and evidence of internal hydrocephalus 14 weeks before he died. Histologic examination that involved ISH and IHC proved that BK virus was present in the brain, kidneys, and lungs of the patient. Then, in 1996, BK virus primary infection was seen in a 34-year-old immunocompetent man with encephalitis whose serologic status, as determined by IgM titers, was consistent with primary infection [91]. It should be noted that a biopsy was not performed, so there is no tissue-related evidence to support this case. This same pattern of more-severe, adult-acquired primary infection can be seen with other viruses, such as varicella [158]. Finally, in 1999, BK virus was implicated in another case of meningoencephalitis, this time involving a 26-year-old homosexual man with AIDS [49, 150]. In the 10 months preceding his death, the patient developed bilateral atypical retinitis and nephritis. Microscopic examination of the brain showed thickened, fibrotic leptomeninges, a finding that is characteristic of BK virus–induced pathologic findings, whereas the underlying cortex showed mild astrocytosis. The periventricular regions showed small patches of destroyed ependyma, and the choroid plexus was noted to be fibrotic. The presence of BK virus was determined by use of PCR, ISH, and IHC in the brain, kidneys, and retinal tissues. Of note, there were no signs of HIV-related encephalopathy. In all the aforementioned recent cases, the results of PCR for other viruses (CMV, herpes simplex virus, JC virus, and Epstein-Barr virus) and the results of assays for related CNS infections were all negative, with the exception of a presumed peripheral blood mononuclear cell contamination of CMV in the retinal tissues of the patient described by Bratt et al. [49]. These cases provide evidence of a strong association, but not proof of a causal relationship, between these disease processes and BK virus, especially in the absence of other agents known to infect the CNS. References 23. 24. 25. 26. 27. 28. 29. 30. 31. 32. 33. 34. 35. 36. 37. 38. 39. 40. 41. 42. 43. 44. 45. BK Virus • CID 2001:33 (15 July) • 199 Downloaded from http://cid.oxfordjournals.org/ by guest on September 9, 2014 1. Gardner SD, Field AM, Coleman DV, et al. New human papovavirus (B.K.) isolated from urine after renal transplantation. Lancet 1971; 1(7712):1253–7. 2. Padgett BL, ZuRhein GM, Walker DL, et al. Cultivation of papovalike virus from human brain with progressive multifocal leukoencephalopathy. Lancet 1971; 1(7712):1257–60. 3. Shah KV. Polyomaviruses. In: Fields BN, Knipe DM, et al. Virology. 2d ed. New York: Raven Press, 1990:1609–1623 4. Padgett BL, Walker DL. Prevalence of antibodies in human sera against JC virus, an isolate from a case of progressive multifocal leukoencephalopathy. J Infect Dis 1973; 127:467–70. 5. Shah KV, Daniel RW, Warszawski RM. High prevalence of antibodies to BK virus, and SV-40 related papovavirus, in residents in Maryland. J Infect Dis 1973; 128:784–7. 6. Portolani M, Marzocchi A, Barbanti-Brodano G, et al. Prevalence in Italy of antibodies to a new human papovavirus (BK Virus). J Med Microbiol 1974; 7:543–6. 7. Gardner SD. Prevalence in England of antibody to human polyomavirus (B.K.). Br Med J 1973; 1:77–8. 8. Mantyjarvi RA, Meurman OH, Vihma L, et al. A human papovavirus (B.K.), biological properties and seroepidemiology. Ann Clin Res 1973; 5:283–7. 9. Flaegstad T, Permin H, Husebekk A, et al. BK virus infection in patients with AIDS. Scand J Infect Dis 1988; 20:145–50. 10. Rziha H, Bornkamm GW, zur Hausen H. BK virus: I. Seroepidemiologic studies and serologic response to viral infection. Med Microbiol Immunol (Berl) 1978; 165:73–81. 11. Goudsmit J, Dillen PW, van Strien A, et al. The role of BK virus in acute respiratory tract disease and the presence of BKV DNA in tonsils. J Med Virol 1982; 10:91–9. 12. Vago L, Cinque P, Sala E, et al. JCV-DNA and BKV-DNA in the CNS tissue and CSF of AIDS patients and normal subjects: study of 41 cases and review of the literature. J Acquir Immune Defic Syndr Hum Retrovirol 1996; 12:139–46. 13. Woloschak M, Yu A, Post KD. Detection of polyomaviral DNA sequences in normal and adenomatous human pituitary tissues using the polymerase chain reaction. Cancer 1995; 76:490–6. 14. Moret H, Guichard M, Matheron S, et al. Virologic diagnosis of progressive multifocal leukoencephalopathy: detection of JC Virus DNA in cerebrospinal fluid and brain tissue of AIDS patients. J Clin Microbiol 1993; 31:3310–3. 15. De Mattei M, Martini F, Tognon M, et al. Polyomavirus latency and human tumors. J Infect Dis 1994; 169:1175–6. 16. De Mattei M, Martini F, Corallini A, et al. High incidence of BK virus large-T-antigen–coding sequences in normal human tissues and tumors of different histotypes. Int J Cancer 1995; 61:756–60. 17. Sundsfjord A, Spein A, Lucht E, et al. Detection of BK virus DNA in nasopharyngeal aspirates from children with respiratory infections but not in saliva from immunodeficient and immunocompetent adult patients. J Clin Microbiol 1994; 32:1390–4. 18. Monini P, Rotola A, De Lellis L, et al. Latent BK virus infection and Kaposi’s sarcoma pathogenesis. Int J Cancer 1996; 66:717–22. 19. Vallbracht A, Lohler J, Gossmann J, et al. Disseminated BK type polyomavirus infection in an AIDS patient associated with central nervous system disease. Am J Pathol 1993; 143:29–39. 20. Knepper JE, diMayorca G. Cloning and characterization of BK virus–related DNA sequences from normal and neoplastic human tissues. J Med Virol 1987; 21:289–99. 21. Dorries K, Vogel E, Gunther S, et al. Infection of human polyomaviruses JC and BK in peripheral blood leukocytes from immunocompetent individuals. Virology 1994; 198:59–70. 22. Sundsfjord A, Flaegstad T, Flo R, et al. BK and JC viruses in human immunodeficiency virus type 1–infected persons: prevalence, excre- tion, viremia, and viral regulatory regions. J Infect Dis 1994; 169: 485–90. De Santis R, Azzi A. Duplex polymerase chain reaction for the simultaneous detection of the human polyomavirus BK and JC DNA. Mol Cell Probes 1996; 10:325–30. Heritage J, Chesters PM, McCance DJ. The persistence of papovavirus BK DNA sequences in normal human renal tissue. J Med Virol 1981;8: 143–50. Grinnell BW, Padgett BL, Walker DL. Distribution of nonintegrated DNA from JC papovavirus in organs of patients with progressive multifocal leukoencephalopathy. J Infect Dis 1983; 147:669–75. Chesters PM, Heritage J, McCance DJ. Persistence of DNA sequences of BK virus and JC virus in normal human tissues and in diseased tissues. J Infect Dis 1983; 147:676–84. Elsner C, Dorries K. Evidence of human polyomavirus BK and JC infection in normal brain tissue. Virology 1992; 191:72–80. Bogdanovic G, Ljungman P, Wang F, et al. Presence of human polyomavirus DNA in the peripheral circulation of bone marrow transplant patients with and without hemorrhagic cystitis. Bone Marrow Transplant 1996; 17:573–6. Schneider EM, Dorries K. High frequency of polyomavirus infection in lymphoid cell preparations after allogeneic bone marrow transplantation. Transplant Proc 1993; 25:1271–3. White FA III, Ishaq M, Stoner GL, et al. JC virus DNA is present in many human brain samples from patients without progressive multifocal leukoencephalopathy. J Virol 1992; 66:5726–34. Ferrante P, Caldarelli-Stefano R, Omodeo-Zorini E, et al. PCR detection of JC virus DNA in brain tissue from patients with and without progressive multifocal leukoencephalopathy. J Med Virol 1995; 47: 219–25. Perrons CJ, Fox JD, Lucas SB, et al. Detection of polyomaviral DNA in clinical samples from immunocompromised patients: correlation with clinical disease. J Infect 1996; 32:205–9. Dorries K. Molecular biology and pathogenesis of human polyomavirus infections. Dev Biol Stand 1998; 94:71–9. Taguchi F, Nagaki D, Saito M, et al. Transplacental transmission of BK virus in human. Jpn J Microbiol 1975; 19:395–8. Pietropaolo V, Di Taranto C, Degener AM, et al. Transplacental transmission of human polyomavirus BK. J Med Virol 1998; 56:372–6. Chan PKS, Ip KWY, Shiu SYW, et al. Association between polyomaviruria and microscopic hematuria in bone marrow transplant recipients. J Infect 1994; 29:139–46. Arthur RR, Shah KV, Baust SJ, et al. Association of BK viruria with hemorrhagic cystitis in recipients of bone marrow transplants. N Engl J Med 1986; 315:230–4. Hashida Y, Gaffney PC, Yunis EJ. Acute hemorrhagic cystitis of childhood and papovavirus-like particles. J Pediatr 1976; 89:85–7. Saitoh K, Sugae N, Koike N, et al. Diagnosis of childhood BK virus cystitis by electron microscopy and PCR. J Clin Pathol 1993; 46:773–5. Padgett BL, Walker DL, Desquitado MM, et al. BK virus and nonhemorrhagic cystitis in a child. Lancet 1983; 1(8327):770. Andrews CA, Shah KV, Daniel RW, et al. A serological investigation of BK virus in JC virus infections in recipients of renal allografts. J Infect Dis 1988; 158:176–81. Coleman DV, Gardner SD, Field AM. Human polyomavirus infection in renal allograft recipients. Br Med J 1973; 3:371–5. Bedi A, Miller CB, Hanson JL, et al. Association of BK virus with failure of prophylaxis against hemorrhagic cystitis following bone marrow transplantation. J Clin Oncol 1995; 13:1103–9. Bogdanovic G, Priftakis P, Taemmeraes B, et al. Primary BK virus (BKV) infection due to possible BKV transmission during bone marrow transplantation is not the major cause of hemorrhagic cystitis in transplanted children. Pediatr Transplant 1998; 2:288–93. Goddard AG, Saha V. Late-onset hemorrhagic cystitis following bone marrow transplantation: a case report. Pediatr Hematol Oncol 1997; 14:273–5. 200 • CID 2001:33 (15 July) • Reploeg et al. 69. Takemoto KK, Rabson AS, Mullarkey MF, et al. Isolation of papovavirus from brain tumor and urine of a patient with Wiskott-Aldrich Syndrome. J Natl Cancer Inst 1974; 53:1205–7. 70. Flaegstad T, Andersen PA, Johnsen JI, et al. A possible contributory role of BK virus infection in neuroblastoma development. Cancer Res 1999; 59:1160–3. 71. Arthur RR, Grossman SA, Ronnett BM, et al. Lack of association of human polyomaviruses with human brain tumors. J Neurooncol 1994; 20:55–8. 72. Shah K. BK virus in brain tumors. Dev Biol Stand 1998; 94:153. 73. Wold WSM, Mackey JK, Brackman KH, et al. Analysis of human tumors and human malignant cell lines for BK virus–specific DNA sequences. Proc Natl Acad Sci U S A 1978; 75:454–8. 74. Di Mayorca G, Fiori M. Occurrence of BK virus DNA in DNA obtained from certain human tumors. Proc Natl Acad Sci U S A 1976;73: 4662–6. 75. Israel MA, Martin MA, Takemoto KK, et al. Evaluation of normal and neoplastic human tissue for BK virus. Virology 1978; 90:187–96. 76. Volter C, zur Hausen H, Alber D, et al. Screening human tumor samples with a broad-spectrum polymerase chain reaction method for the detection of polyomaviruses. Virology 1997; 237:389–96. 77. Grossi MP, Meneguzzi G, Chenciner N, et al. Lack of association between BK virus and ependymomas, malignant tumors of pancreatic islets, osteosarcomas and other human tumors. Intervirology 1981; 15:10–8. 78. Altavilla G, Trabanelli C, Merlin M, et al. Morphological, histochemical, immunohistochemical, and ultrastructural characterization of tumors and dysplastic and non-neoplastic lesions arising in BK virus/ tat transgenic mice. Am J Pathol 1999; 154:1231–44. 79. Rusnati M, Coltrini D, Campioni D, et al. Upregulation of urokinasetype plasminogen activator by endogenous and exogenous HIV-1 tat protein in tumour cell lines derived from BK Virus/tat-transgenic mice. AIDS 1997; 11:727–36. 80. Corallini A, Campioni D, Rossi C, et al. Promotion of tumour metastasis and induction of angiogenesis by native HIV-1 Tat protein from BK virus/tat transgenic mice. AIDS 1996; 10:701–10. 81. Campioni D, Corallini A, Zauli G, et al. HIV type 1 extracellular Tat protein stimulates growth and protects cells of BK virus/tat transgenic mice from apoptosis. AIDS Res Hum Retroviruses 1995; 11:1039–48. 82. Harris KF, Chang E, Christensen JB, et al. BK virus as a potential cofactor in human cancer. Dev Biol Stand 1998; 94:81–91. 83. Dyson N, Bernards R, Friend SH, et al. Large T antigens of many polyomaviruses are able to form complexes with the retinoblastoma protein. J Virol 1990; 64:1353–6. 84. Harris KF, Christensen JB, Radany EH, et al. Novel mechanisms if E2F induction by BK virus large-T antigen: requirement of both the pRb-binding and the J domains. Mol Cell Biol 1998; 18:1746–56. 85. Trabanelli C, Corallini A, Gruppioni R, et al. Chromosomal aberrations induced by BK virus T antigen in human fibroblasts. Virology 1998; 243:492–6. 86. Lazutka JR, Neel JV, Major EO, et al. High titers of antibodies to two human polyomaviruses, JCV and BKV, correlate with increased frequency of chromosomal damage in human lymphocytes. Cancer Lett 1996; 109:177–83. 87. Monini P, Rotola A, Di Luca D, et al. DNA rearrangements impairing BK virus productive infection in urinary tract tumors. Virology 1995; 214:273–9. 88. Moens U, Subramaniam N, Johansen B, et al. A steroid hormone response unit in the late leader of the noncoding control region of the human polyomavirus BK confers enhanced host cell permissivity. J Virol 1994; 68:2398–408. 89. Moens U, Van Ghelue M, Johansen B, et al. Concerted expression of BK virus large T- and small T-antigens strongly enhances oestrogen receptor-mediated transcription. J Gen Virol 1999; 80:585–94. 90. Sundsfjord A, Osei A, Rosenqvist H, et al. BK and JC viruses in patients with systemic lupus erythematosus: prevalent and persistent Downloaded from http://cid.oxfordjournals.org/ by guest on September 9, 2014 46. Vogeli TA, Peinemann F, Burdach S, et al. Urological treatment and clinical course of BK polyomavirus-associated hemorrhagic cystitis in children after bone marrow transplantation. Eur Urol 1999; 36:252–7. 47. Coleman DV, Mackenzie EFD, Gardner SD, et al. Human polyomavirus (BK) infection and ureteric stenosis in renal allograft recipients. J Clin Pathol 1978; 31:338–47. 48. Gardner SD, Mackenzie EFD, Smith C, et al. A prospective study of the human polyomaviruses BK and JC and cytomegalovirus in renal transplant recipients. J Clin Pathol 1984; 37:578–86. 49. Bratt G, Hammarin AL, Grandien M, et al. BK virus as the cause of meningoencephalitis, retinitis, and nephritis in a patient with AIDS. AIDS 1999; 13:1071–5. 50. Smith RD, Galla JH, Skahan K, et al. Tubulointerstitial nephritis due to a mutant polyomavirus BK virus strain, BKV(Cin), causing endstage renal disease. J Clin Microbiol 1998; 36:1660–5. 51. Rosen S, Harmon W, Krensky AM, et al. Tubulo-interstitial nephritis associated with polyomavirus (BK type) infection. N Engl J Med 1983; 308:1192–6. 52. De Silva LM, Bale P, de Courcy J, et al. Renal failure due to BK virus infection in an immunodeficient child. J Med Virol 1995; 45:192–6. 53. Mathur VS, Olson JL, Darragh TM, et al. Polyomavirus-induced interstitial nephritis in two renal transplant recipients: case reports and review of the literature. Am J Kidney Dis 1997; 29:754–8. 54. Purighalla R, Shapiro R, McCauley J, et al. BK virus infection in a kidney allograft diagnosed by needle biopsy. Am J Kidney Dis 1995;26: 671–3. 55. Randhawa PS, Finkelstein S, Scantlebury V, et al. Human polyoma virus–associated interstitial nephritis in the allograft kidney. Transplantation 1999; 67:103–9. 56. Nickeleit V, Hirsch HH, Binet IF, et al. Polyomavirus infection of renal allograft recipients: from latent infection to manifest disease. J Am Soc Nephrol 1999; 10:1080–9. 57. Howell DN, Smith SR, Butterly DW, et al. Diagnosis and management of BK polyomavirus interstitial nephritis in renal transplant recipients. Transplantation 1999; 68:1279–88. 58. Nebuloni M, Tosoni A, Boldorini R, et al. BK virus renal infection in a patients with the acquired immunodeficiency syndrome. Arch Pathol Lab Med 1999; 123:807–11. 59. Cubukcu-Dimopulo O, Greco A, Kumar A, et al. BK virus infection in AIDS. Am J Surg Pathol 2000; 24:145–9. 60. Pappo O, Demetris AJ, Raikow RB, et al. Human polyoma virus infection of renal allografts: histopathologic diagnosis, clinical significance, and literature review. Mod Pathol 1996; 9:105–9. 61. Sandler ES, Aquino VM, Goss-Shohet E, et al. BK papova virus pneumonia following hematopoietic stem cell transplantation. Bone Marrow Transplant 1997; 20:163–5. 62. Goudsmit J, Baak ML, Slaterus KW, et al. Human papovavirus isolated from urine of a child with acute tonsilitis. Br Med J (Clin Red Ed) 1981; 283:1363–4. 63. Hedquist BG, Bratt G, Hammarin AL, et al. Identification of BK virus in a patient with acquired immune deficiency syndrome and bilateral atypical retinitis. Ophthalmology 1999; 106:129–32. 64. O’Reilly RJ, Lee FK, Grossbard E, et al. Papovavirus excretion following marrow transplantation: incidence and association with hepatic dysfunction. Transplant Proc 1981; 13:262–6. 65. Negrini M, Rimessi P, Mantovani C, et al. Characterization of BK virus variants rescued from human tumours and tumour cell lines. J Gen Virol 1990; 71:2731–6. 66. Dorries K, Loeber G, Meixenberger J. Association of polyomavirus JC, SV40, and BK with human brain tumors. Virology 1987; 160: 268–70. 67. Corallini A, Barbanti-Brodano G, Bortoloni W, et al. High incidence of ependymomas induced by BK virus, a human papovavirus: brief communication. J Natl Cancer Inst 1977; 59:1561–4. 68. Corallini A, Pagnani M, Viadana P, et al. Association of BK virus with human brain tumors and tumors of pancreatic islets. Int J Cancer 1987; 39:60–7. 91. 92. 93. 94. 95. 96. 97. 98. 100. 101. 102. 103. 104. 105. 106. 107. 108. 109. 110. 111. 112. 113. 114. Moens U, Seternes OM, Hey AW, et al. In vivo expression of a single viral DNA-binding protein generates systemic lupus erythematosus– related autoimmunity to double-stranded DNA and histones. Proc Natl Acad Sci U S A 1995; 92:12393–7. 115. Flaegstad T, Fredriksen K, Dahl B, et al. Inoculation with BK virus may break immunological tolerance to histone and DNA antigens. Proc Natl Acad Sci U S A 1988; 85:8171–5. 116. Rekvig OP, Moens U, Sundsfjord A, et al. Experimental expression in mice and spontaneous expression on human SLE of polyomavirus T-antigen. J Clin Invest 1997; 99:2045–54. 117. Chang D, Tsai R, Wang M, et al. Different genotypes of human polyomaviruses found in patients with autoimmune diseases in Taiwan. J Med Virol 1996; 48:204–9. 118. Theile M, Grabowski G. Mutagenic activity of BKV and JCV in human and other mammalian cells. Arch Virol 1990; 113:221–33. 119. Grossi MP, Caputo A, Meneguzzi G, et al. Transformation of human embryonic fibroblasts by BK virus, BK virus DNA and a subgenomic BK virus DNA fragment. J Gen Virol 1982; 63:393–403. 120. Sekiguchi M, Miyazaki S, Fujikawa K, et al. BK virus–induced osteosarcoma (Os515) as a model of human osteosarcoma. Anticancer Res 1996; 16:1835–42. 121. Corallini A, Pagnani M, Viadana P. Induction of malignant subcutaneous sarcomas in hamsters by a recombinant DNA containing BK virus early region and the activated human c-Harvey-ras oncogene. Cancer Res 1987; 47:6671–7. 122. Takemoto KK, Linke H, Miyamura T, et al. Persistent BK papovavirus infection of transformed human fetal brain cells. J Virol 1979; 29: 1177–85. 123. Gallo RC. The enigmas of Kaposi’s sarcoma. Science 1998; 282:1837–9. 124. Neipel F. The role of HHV-8 in Kaposi’s sarcoma. Semin Cancer Biol 1999; 9:151–64. 125. Imperiale M. The Human Polyomaviruses, BKV and JCV: molecular pathogenesis of acute disease and potential role in cancer. Virology 2000; 267:1–7. 126. Watanabe S, Yoshiike K. Evolutionary changes of transcriptional control region in a minute-plaque viable deletion mutant of BK virus. J Virol 1986; 59:260–6. 127. Sundsfjord A, Johansen T, Flaegstad T, et al. At least two types of control regions can be found among naturally occurring BK virus strains. J Virol 1990; 64:3864–71. 128. Rubinstein R, Pare N, Harley EH. Structure and function of the transcriptional control region of nonpassaged BK virus. J Virol 1987; 61:1747–50. 129. Negrini M, Sabbioni S, Arthur RR, et al. Prevalence of the archetypal regulatory region and sequence polymorphisms in nonpassaged BK virus variants. J Virol 1991; 65:5092–5. 130. Tavis JE, Frisque RJ, Walker DL, et al. Antigenic and transforming properties of the DB strain of the human polyomavirus BK virus. Virology 1990; 178:568–72. 131. Pagnani M, Negrini M, Reschiglian P, et al. Molecular and biological properties of BK virus–IR, a BK virus variant isolated from a human tumor. J Virol 1986; 59:500–5. 132. Moens U, Johansen T, Johnsen JI, et al. Noncoding control region of naturally occurring BK virus variants: sequence comparison and functional analysis. Virus Genes 1995; 10:261–75. 133. Seif I, Khoury G, Dhar R. The genome of human papovavirus BKV. Cell 1979; 18:963–77. 134. Koch S, von Loringhoven AF, Hofschneider PH, et al. Amplification and rearrangement in hepatoma cell DNA associated with integrated hepatitis B virus DNA. EMBO J 1984; 3:2185–9. 135. Nelson JA, Fleckenstein B, Jahn G, et al. Structure of the transforming region of human cytomegalovirus AD 169. J Virol 1984; 49:109–15. 136. Sugimoto C, Hara K, Taguchi F, et al. Growth efficiency of naturally occurring BK virus variants in vivo and in vitro. J Virol 1989; 63: 3195–9. 137. Jin L, Gibson PE, Booth JC, et al. Genomic typing of BK virus in BK Virus • CID 2001:33 (15 July) • 201 Downloaded from http://cid.oxfordjournals.org/ by guest on September 9, 2014 99. BK viruria, sequence stability of the viral regulatory regions, and nondetectable viremia. J Infect Dis 1999; 180:1–9. Voltz R, Jager G, Seelos K, et al. BK virus encephalitis in an immunocompetent patient. Arch Neurol 1996; 53:101–3. Van Der Noorda J, Wertheim-Van Dillen P. Rise in antibodies to human papova virus BK and clinical disease. Br Med J 1977; 3:1471. Caputo A, Corallini A, Grossi MP, et al. Episomal DNA of a BK virus variant in a human insulinoma. J Med Virol 1983; 12:37–49. Peterman TA, Jaffe HW, Beral V. Epidemiologic clues to the etiology of Kaposi’s sarcoma. AIDS 1993; 7:605–11. Coleman DV, Wolfendale MR, Daniel RA, et al. A prospective study of human polyomavirus infection in pregnancy. J Infect Dis 1980; 142:1–8. Rziha H, Belohradsky BH, Schneider U, et al. BK virus: II. Serologic studies in children with congenital disease and patients with malignant tumors and immunodeficiencies. Med Microbiol Immunol (Berl) 1978; 165:83–92. Lecatsas G, Prozesky OW, Van Wyk J, et al. Papova virus in urine after renal transplantation. Nature 1973; 241:343–4. Markowitz R, Thompson HC, Mueller JF, et al. Incidence of BK virus and JC virus viruria in human immunodeficiency virus–infected and –uninfected subjects. J Infect Dis 1993; 167:13–20. Degener AM, Pietropaola V, Di Taranto C, et al. Detection of JC and BK viral genome in specimens of HIV-1 infected subjects. Microbiologica 1997; 20:115–22. Apperley JF, Rice SJ, Bishop JA, et al. Late-onset hemorrhagic cystitis associated with urinary excretion of polyomaviruses after bone marrow transplantation. Transplantation 1987; 43:108–12. Samuelson J, Von Lichtenberg F. Robbins pathologic basis of disease. 5th ed. Philadelphia: WB Saunders, 1994. Shinohara T, Matsuda M, Cheng SH, et al. BK virus infection of the human urinary tract. J Med Virol 1993; 41:301–5. Dolei A, Pietropaolo V, Gomes E, et al. Polyomavirus persistence in lymphocytes: prevalence in lymphocytes from blood donors and healthy personnel of a blood transfusion centre. J Gen Virol 2000; 81:1967–73. Chang D, Wang M, Ou W, et al. Genotypes of human polyomaviruses in urine samples of pregnant women in Taiwan. J Med Virol 1996; 48:95–101. Borgatti M, Costanzo F, Portolani M, et al. Evidence for reactivation of persistent infection during pregnancy and lack of congenital transmission of BK virus, a human papovavirus. Microbiologica 1979; 2:173–8. Kahan AV, Coleman DV, Koss LG. Activation of human polyomavirus infection-detection by cytologic techics. Am J Clin Pathol 1980; 74: 326–32. Kitamura T, Aso Y, Kuniyoshi N, et al. High incidence of urinary JC virus excretion in nonimmunosuppressed older patients. J Infect Dis 1990; 161:1128–33. Hogan TF, Broden EC, McBain JA, et al. Human polyomavirus infections with JC virus and BK virus in renal transplant patients. Ann Intern Med 1980; 92:373–8. Binet IF, Nickeleit V, Hirsch HH, et al. Polyomavirus disease under new immunosuppressive drugs: a cause of renal graft dysfunction and graft loss. Transplantation 1999; 67:918–22. Nickeleit V, Klimkait T, Binet IF, et al. Testing for polyomavirus type BK DNA in plasma to identify renal-allograft recipients with viral nephropathy. N Engl J Med 2000; 342:1309–15. Fredriksen K, Skogholm A, Flaegstad T, et al. Antibodies to dsDNA are produced during primary BK virus infection in man, indicating that anti-dsDNA antibodies may be related to virus replication in vivo. Scand J Immunol 1993; 38:401–6. Rekvig OP. Polyoma induced autoimmunity to DNA; experimental systems and clinical observations in human SLE. Clin Exp Rheumatol 1998; 16:325–6. Rekvig OP, Moens U, Fredriksen K, et al. Human polyomavirus BK and immunogenicity of mammalian DNA: a conceptual framework. Methods 1997; 11:44–54. 138. 139. 140. 141. 142. 143. 145. 146. 147. 148. 202 • CID 2001:33 (15 July) • Reploeg et al. 149. 150. 151. 152. 153. 154. 155. 156. 157. 158. koencephalopathy: diagnosis by in situ hybridization with a biotinylated JC virus DNA probe using an automated histomatic codeon slide stainer. Am J Surg Pathol 1991; 15:791–7. Bogdanovic G, Priftakis P, Hammarin AL, et al. Detection of JC virus in cerebrospinal fluid (CSF) samples from patients with progressive multifocal leukoencephalopathy but not CSF samples from patients with herpes simplex encephalitis, enteroviral meningitis, or multiple sclerosis. J Clin Microbiol 1998; 36:1137–8. Hammarin AL, Bogdanovic G, Svedhem V, et al. Analysis of PCR as a tool for detection of JC virus DNA in cerebrospinal fluid for diagnosis of progressive multifocal leukoencephalopathy. J Clin Microbiol 1996; 34:2929–32. Shimada H, Noda K, Mori M, et al. Papovavirus detection by electron microscopy in the brain of an elderly patient without overt progressive multifocal leukoencephalopathy. Virchows Arch 1994; 424:569–72. Boldorini R, Caldarelli-Stefano R, Monga G, et al. PCR detection of JC virus DNA in the brain tissue of a 9-year-old child with pleomorphic xanthoastrocytoma. J Neurovirol 1998; 4:242–5. Mori M, Kurata H, Tajima M, et al. JC virus detection by in situ hybridization in brain tissue from elderly patients. Ann Neurol 1991; 29:428–32. Vago L, Cinque P, Sala E, et al. JCV-DNA in CNS of AIDS patients with and without PML [abstract 334B]. Int Conf AIDS 1994; 10:10. Jochum W, Weber T, Frye S, et al. Detection of JC virus by anti-VP1 immunohistochemistry in brains with progressive multifocal leukoencephalopathy. Acta Neuropathol (Berl) 1997; 94:226–31. Heinonen O, Syrjanen S, Mantyjarvi RA, et al. JC virus infection and Alzheimer’s disease: reappraisal of an in situ hybridization approach. Ann Neurol 1992; 31:439–41. Henry K, Bird R, Watson G, et al. Aplastic anaemia, bone-marrow transplantation, and polyoma and other virus infections. Lancet 1977; 1(8013):695–6. Wilkins EGL, Leen CLS, McKendrick MW, et al. Management of chickenpox in the adult: a review prepared for the UK Advisory Group on chickenpox on behalf of the British Society for the study of infection. J Infect 1998; 36:49–58. Downloaded from http://cid.oxfordjournals.org/ by guest on September 9, 2014 144. clinical specimens by direct sequencing of polymerase chain reaction products. J Med Virol 1993; 41:11–7. Jin L, Pietropaola V, Booth JC, et al. Prevalence and distribution of BK virus subtypes in healthy people and immunocompromised patients detected by PCR-restriction enzyme analysis. Clin Diagn Virol 1995; 3:285–95. Gendelman HE, Phelps W, Feigenbaum L, et al. Trans-activation of the human immunodeficiency virus long terminal repeat sequence by DNA viruses. Proc Natl Acad Sci U S A 1986; 83:9759–63. Tada H, Rappaport J, Lashgari M, et al. Trans-activation of the JC virus late promoter by the tat protein of type 1 human immunodeficiency virus in glial cells. Proc Natl Acad Sci U S A 1990; 87:3479–83. Major EO, Amemiya K, Tornatore CS, et al. Pathogenesis and molecular biology of progressive multifocal leukoencephalopathy, the JC virus–induced demyelinating disease of the human brain. Clin Microbiol Rev 1992; 5:49–73. Brooks BR, Walker DL. Progressive multifocal leukoencephalopathy. Neurol Clin 1984; 2:299–313. Garcia de Viedma D, Alonso R, Miralles P, et al. Dual qualitativequantitative nested PCR for detection of JC virus in cerebrospinal fluid: high potential for evaluation and monitoring of progressive multifocal leukoencephalopathy in AIDS patients receiving highly active antiretroviral therapy. J Clin Microbiol 1999; 37:724–8. Koralnik IJ, Boden D, Mai VX, et al. JC virus DNA load in patients with and without progressive multifocal leukoencephalopathy. Neurology 1999; 52:253–60. Weber T, Klapper PE, Cleator GM, et al. Polymerase chain reaction for detection of JC virus DNA in cerebrospinal fluid: a quality control study. J Virol Methods 1997; 69:231–7. Telenti A, Aksamit AJ, Proper J, et al. Detection of JC virus DNA by polymerase chain reaction in patients with progressive multifocal leukoencephalopathy. J Infect Dis 1990; 162:858–61. Henson J, Rosenblum M, Armstrong D, et al. Amplification of JC virus DNA from brain and cerebrospinal fluid of patients with progressive multifocal leukoencephalopathy. Neurology 1991; 41:1967–71. Hulette CM, Downey BT, Burger PC. Progressive multifocal leu-









© Copyright 2026