
Treatment of Polycythemia Vera With Hydroxyurea and
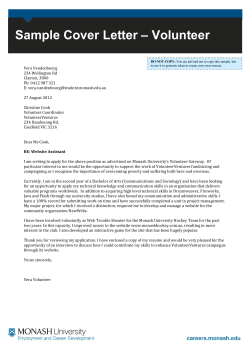
VOLUME 29 䡠 NUMBER 29 䡠 OCTOBER 10 2011 JOURNAL OF CLINICAL ONCOLOGY O R I G I N A L R E P O R T Treatment of Polycythemia Vera With Hydroxyurea and Pipobroman: Final Results of a Randomized Trial Initiated in 1980 Jean-Jacques Kiladjian, Sylvie Chevret, Christine Dosquet, Christine Chomienne, and Jean-Didier Rain Jean-Jacques Kiladjian, Sylvie Chevret, Christine Dosquet, Christine Chomienne, and Jean-Didier Rain, Hoˆpital Saint-Louis; and Jean-Jacques Kiladjian, Universite´ Paris 7, Paris, France. Submitted March 22, 2011; accepted July 14, 2011; published online ahead of print at www.jco.org on September 12, 2011. The content of this article, the data interpretation, and the decision to submit it for publication in Journal of Clinical Oncology was made by the authors independently. Authors’ disclosures of potential conflicts of interest and author contributions are found at the end of this article. Corresponding author: Jean-Jacques Kiladjian, MD, PhD, Centre d’Investigations Cliniques, Hoˆpital Saint-Louis, AP-HP, 1 avenue Claude Vellefaux, Paris, France 75010; e-mail: jean-jacques.kiladjian@ sls.aphp.fr. © 2011 by American Society of Clinical Oncology 0732-183X/11/2929-3907/$20.00 A B S T R A C T Purpose The overall impact of hydroxyurea (HU) or pipobroman treatments on the long-term outcome of patients with polycythemia vera (PV) has not been assessed in randomized studies. We report final analyses from the French Polycythemia Study Group (FPSG) study, which randomly assigned HU versus pipobroman as first-line therapy in 285 patients younger than age 65 years. Patients and Methods The full methodology has been described previously. FPSG results were updated with a median follow-up of 16.3 years. Statistical analysis was performed by using competing risks on the intention-to-treat population and according to main treatment received. Results Median survival was 17 years for the whole cohort, 20.3 years for the HU arm, and 15.4 years for the pipobroman arm (P ⫽ .008) and differed significantly from that in the general population. At 10, 15, and 20 years, cumulative incidence of acute myeloid leukemia/myelodysplastic syndrome (AML/MDS) was 6.6%, 16.5%, and 24% in the HU arm and 13%, 34%, and 52% in the pipobroman arm (P ⫽ .004). Cumulative myelofibrosis incidence at 10, 15, and 20 years according to main treatment received was 15%, 24%, and 32% with HU versus 5%, 10%, and 21% with pipobroman (P ⫽ .02). Conclusion Data from this unique randomized trial comparing HU with another cytoreductive drug in PV showed that (1) survival of patients with PV treated with conventional agents differed from survival in the general population, (2) evolution to AML/MDS is the first cause of death, (3) pipobroman is leukemogenic and is unsuitable for first-line therapy, and (4) incidence of evolution to AML/MDS with HU is higher than previously reported, although consideration should be given to the natural evolution of PV. DOI: 10.1200/JCO.2011.36.0792 J Clin Oncol 29:3907-3913. © 2011 by American Society of Clinical Oncology INTRODUCTION Polycythemia vera (PV) is a chronic myeloproliferative neoplasm that typically presents at a median age of 60 years and is characterized by the occurrence of vascular complications.1-4 Over time, PV may undergo hematologic evolution to myelofibrosis (MF), acute myeloid leukemia (AML), and myelodysplastic syndrome (MDS). Although the mechanisms behind these evolutions remain unclear, there is some evidence suggesting that PV therapy, such as radioactive phosphorus or alkylating agents, may increase the frequency of progression.5 The incidence of such evolution in untreated patients or patients treated only with phlebotomy appears to be low at less than 2%.1,6-8 The aim of treatment for PV is to reduce the risk of vascular events in the short term while mini- mizing the risk of transformation to AML and MF in the long-term.2 According to the recently published European LeukemiaNet (ELN) guidelines, hydroxyurea (HU) and interferon alfa (IFN-␣) are recommended as first-line treatment in high-risk patients with PV.9 HU displays a good efficacy and tolerability profile and is associated with significant reductions in thrombotic complications.10-12 It has been suggested that long-term HU therapy may increase the risk of leukemic evolution, with AML incidence rates ranging from approximately 5% to 15%.10,11 However, the largest randomized trial in PV to date, the European Collaboration on LowDose Aspirin in Polycythemia Vera (ECLAP) study, suggested that HU therapy is not associated with an increased risk of evolution to AML.13 It should be noted that the prospective follow-up at time of publication was short (2.8 years), and the study design © 2011 by American Society of Clinical Oncology Downloaded from jco.ascopubs.org on September 9, 2014. For personal use only. No other uses without permission. Copyright © 2011 American Society of Clinical Oncology. All rights reserved. 3907 Kiladjian et al prevented real assessment of the total exposure time to HU. Thus, the potential leukemic risk associated with long-term therapy with HU is still not clearly defined. This prompted the expert panel of the ELN to underscore that it is wise to proceed with caution when considering the use of HU in young patients or patients with cytogenetic abnormalities.9 Patients with PV may also be treated with pipobroman, a bromide derivative of piperazine. This compound has similarities to alkylating agents and mediates its effects using one of two mechanisms: by inhibiting DNA and RNA polymerase or by reducing pyrimidine nucleotide incorporation into DNA. Early research in the United States showed pipobroman to be an effective agent in the treatment of PV,14 and it is extensively used in Europe, particularly in France and Italy.15,16 Survival rates in PV have increased dramatically since the introduction of cytoreductive treatments1; however, the underlying association with disease progression means that long-term comparison of compounds is essential for making informed clinical treatment decisions. The French Polycythemia Study Group (FPSG), recently reconstituted as the French Intergroup of Myeloproliferative Neoplasms (FIM), conducted a randomized clinical study comparing HU and pipobroman in 292 patients with PV younger than age 65 years. They reported no difference between HU and pipobroman in terms of survival, risk of thrombosis, or evolution to AML, MDS, or MF at the time of first analysis, and median follow-up was 7 years.17 This article provides updated long-term data from the FPSG/ FIM study after a median follow-up of 16.3 years in patients with PV treated with either HU or pipobroman. PATIENTS AND METHODS The full methodology for the FPSG study, including details of ethics committee approval and the informed consent process, was published previously.17 Patients younger than age 65 years received either HU 25 mg/kg/d followed by low-dose HU maintenance of 10 to 15 mg/kg/d or pipobroman 1.25 mg/kg/d followed by low-dose pipobroman maintenance of 0.4 to 0.7 mg/kg/d. Here we report the updated results of the FPSG trial at the reference date of April 15, 2008, with a median follow-up of 16.3 years. To allow treatment crossovers to be taken into account, statistical analyses were performed both in the intention-to-treat (ITT) patient population and according to the main treatment received. Estimated survival curves generated via the Kaplan-Meier method were compared by using the log-rank test. Cumulative incidences of AML/MDS were estimated in a competing risks setting in which death precluded the occurrence of the specific event of interest and were then compared by using the Gray test. The expected annual mortality rates for each patient were based on French life tables according to the patient’s sex and age during that calendar year. The expected number of deaths for patients were calculated as the sum of the expected rates during their survival times. The standardized mortality rate (SMR; the ratio of the observed number of deaths to the expected number) was computed for each group of interest. Confidence intervals for the SMRs were computed. All statistical tests were two-sided, with P values of ⱕ .05 denoting statistical significance. SAS v9.2 (SAS Institute, Cary, NC) and R v2.10.1 software packages (R Foundation for Statistical Computing, Vienna, Austria) were used for statistical analysis. 3908 © 2011 by American Society of Clinical Oncology Patients with polycythemia vera (n = 285) Random assignment Pipobroman (n = 149) Hydroxyurea (n = 136) Follow-up Hydroxyurea only (n = 94) Switch to pipobroman (n = 42) Pipobroman only (n = 130) Switch to hydroxyurea (n = 19) Fig 1. CONSORT diagram. RESULTS Patient Characteristics The ITT population consisted of 285 patients randomly assigned to 136 (48%) in the HU treatment arm and 149 (52%) in the pipobroman treatment arm. At follow-up, 94 patients (33%) had received only HU and 130 (46%) only pipobroman. Sixty-one patients (21%) had received both drugs, including 42 patients who had switched from HU to pipobroman and 19 patients who had switched from pipobroman to HU during the complete follow-up period. Seven patients were excluded from the final analysis because of incomplete follow-up data (Fig 1). The median age at study enrollment was 55 years (range, 19 to 80 years) and 125 patients (54%) were male. Of note, 27 patients older than age 65 years were enrolled onto the trial (protocol deviations) and were randomly allocated to either HU (n ⫽ 16) or pipobroman (n ⫽ 11). Because of the ITT principle, these patients were analyzed in the arm they were randomly assigned to. Importantly, this older subgroup of patients did not affect the overall outcome, and no evidence of treatment by age interaction was found (Gail and Simon heterogeneity test P ⫽ .17). Complete baseline characteristics of patients were previously reported in the interim analysis of this study17 (original data available in Appendix Table A1, online only). There was no significant difference between patients randomly assigned to the HU and pipobroman treatment arms in terms of clinical and hematologic characteristics or cardiovascular risk factors. Primary End Point Median overall survival (OS) in the total patient cohort was 17 years (95% CI, 15.4 to 19.4 years; Table 1; Fig 2A). Compared with the age- and sex-matched general French population, the mortality rates were increased significantly with an SMR of 1.84 (95% CI, 1.50 to 2.23). Moreover, median OS significantly differed according to the arm of treatment received. In the ITT population, patients in the HU treatment arm had a median OS of 20.3 years (95% CI, 16.4 to 25.0 years) compared with 15.4 years (95% CI, 13.4 to 17.0 years) in the pipobroman treatment arm (P ⫽ .008; Fig 2B). A similar difference in JOURNAL OF CLINICAL ONCOLOGY Downloaded from jco.ascopubs.org on September 9, 2014. For personal use only. No other uses without permission. Copyright © 2011 American Society of Clinical Oncology. All rights reserved. Long-Term Follow-Up From the FPSG Trial Table 1. Summary of Outcome Hematologic Events in ITT and Main Treatment Received Analyses Outcome Median overall survival, years Cumulative incidence of AML/MDS Analysis ITT ITT Main treatment Cumulative incidence of MF Follow-Up (years) ITT Main treatment 10 15 20 10 15 20 10 15 20 10 15 20 Hydroxyurea Arm Pipobroman Arm Total Cohort % 95% CI % 95% CI P % 95% CI 20.3 16.4 to 25.0 15.4 13.4 to 17.0 .008 17 15.4 to 19.4 .004 9.8 23.6 33.9 — 6.6 16.5 24.2 7.5 14.3 21.9 12.6 19.4 26.9 15.4 24.3 31.6 13.1 34.1 52.1 12.2 37.5 55.9 7.8 15.7 26.9 5.1 9.8 21.3 .008 .07 .02 10.2 17.7 26.1 — Abbreviations: AML, acute myeloid leukemia; ITT, intention to treat; MDS, myelodysplastic syndrome; MF, myelofibrosis. median OS was found between the two arms when follow-up data were analyzed according to the main treatment received (P ⫽ .026; Fig 2C). Since 21% of patients received both drugs during follow-up, we also analyzed the influence of switching with a time-dependent covariate introduced into a Cox model. In patients randomly allocated to HU treatment, switching to pipobroman during follow-up significantly increased the risk of death (hazard ratio, 2.06; 95% CI, 1.09 to 3.87; P ⫽ .026) following the switch compared with patients who remained on HU. In patients randomly assigned to pipobroman therapy, switching to HU during follow-up did not modify the risk of death (hazard ratio, 1.37; 95% CI, 0.61 to 3.08; P ⫽ .45). At the time of evaluation, 95 patients (33%) had died, with the three main causes of death attributed to evolution to AML/MDS in 51 patients (54%), vascular events in 14 patients (15%), and solid tumor development in 11 patients (12%). Of the 51 patients who developed AML/MDS, 10 patients developed MDS, including three that displayed MF at transformation. Forty-one patients developed AML, including five patients for whom AML was preceded by an MDS phase. Evolution to AML/MDS and MF The cumulative incidence of AML/MDS for the total cohort of patients was 9.8%, 23.6%, and 33.9% at 10, 15, and 20 years, respectively (Table 1). Within the ITT population, the cumulative incidence of AML/MDS in the HU treatment arm was 6.6%, 16.5%, and 24.2% at 10, 15, and 20 years, respectively. The corresponding values in the pipobroman treatment arm were 13.1%, 34.1%, and 52.1%, respectively (P ⫽ .004; Fig 3A). Patients receiving HU treatment had a significantly longer median duration of treatment (12 years) than those receiving pipobroman treatment (9.5 years; P ⬍ .001; Fig 4). This may be attributed to a shortage in pipobroman delivery in France between 1983 and 1984. Therefore, analyses were also performed according to the main treatment actually received by patients. These analyses demonstrated a cumulative incidence of AML/MDS transformation of 7.5%, 14.3%, and 21.9% with HU and 12.2%, 37.5%, and 55.9% with pipobroman www.jco.org at 10, 15, and 20 years, respectively (P ⫽ .008; Fig 3B). These findings confirmed the results obtained in the ITT analyses. Results from patients who received only one treatment during the entire follow-up period (HU alone in 94 patients or pipobroman alone in 130 patients) showed a cumulative incidence of AML/MDS transformation at 10, 15, and 20 years of 7.3%, 10.7%, and 16.6%, respectively in the HU treatment arm compared with 14.6%, 34%, and 49.4%, respectively, in the pipobroman treatment arm (P ⫽ .002; Fig 3C). In the ITT population analysis, the cumulative incidence of MF at 10, 15, and 20 years for patients in the HU treatment arm was 12.6%, 19.4%, and 26.9%, respectively. This was comparable to the pipobroman arm at 7.8%, 15.7%, and 27%, respectively (P ⫽ .07; Fig 5A). However, analysis according to main treatment received showed a significantly higher incidence of MF in patients who had received HU. The incidence rate for patients treated with HU at 10, 15, and 20 years was 15.4%, 24.3%, and 31.6% compared with 5.1%, 9.8%, and 21.3%, respectively, in patients whose main treatment was pipobroman (P ⫽ .02; Fig 5B). Vascular Events A total of 85 patients experienced vascular complications, including thrombosis (n ⫽ 80) and hemorrhage (n ⫽ 5) or both (n ⫽ 5). Cumulative incidence of such events according to treatment arms, in both the ITT population and according to main treatment received, are displayed in Figure 6. Across all conducted comparisons, no difference in vascular events was seen between the two treatment arms (P ⫽ .61 and P ⫽ .32 in ITT and according to main treatment received analysis, respectively), showing that both drugs were equally active with respect to vascular event reduction. DISCUSSION The aim of this FPSG/FIM study was to compare HU with pipobroman as first-line treatment for patients with PV and, to the best of our knowledge, this is the only randomized trial to compare HU with another cytoreductive drug in this setting after more than 16 years of © 2011 by American Society of Clinical Oncology Downloaded from jco.ascopubs.org on September 9, 2014. For personal use only. No other uses without permission. Copyright © 2011 American Society of Clinical Oncology. All rights reserved. 3909 Kiladjian et al 1.0 A Observed Expected Cumulative Incidence of AML/MDS (probability) Overall Survival (probability) A 0.8 0.6 0.4 0.2 0 5 10 15 20 25 30 35 1.0 Hydroxyurea Pipobroman 0.8 P = .004 0.6 0.4 0.2 0 5 10 15 Time (years) 1.0 B Hydroxyurea Pipobroman 0.8 Cumulative Incidence of AML/MDS (probability) Overall Survival (probability) B P = .008 0.6 0.4 0.2 0 5 10 15 20 25 30 35 P = .026 0.6 0.4 0.2 0 5 10 15 20 25 30 35 Time (years) Fig 2. Median overall survival (A) in the total patient cohort and compared with a general French population, (B) in the intention-to-treat population receiving hydroxyurea or pipobroman, and (C) according to main treatment received, hydroxyurea or pipobroman. follow-up. Previous data concerning the impact of HU therapy on PV outcome consist of a small number of prospective trials, including the nonrandomized Polycythemia Vera Study Group PVSG-08 study18 and the large ECLAP study, the primary objective of the latter being to assess the role of aspirin in reducing thrombotic complications.19 Furthermore, the FPSG/FIM trial is the first to provide data over a median follow-up of more than 12 years, thus allowing effective assessment of life expectancy and outcomes for the long term in newly diagnosed patients with PV. When analyzed and published in 1997, the study17showed that after a median follow-up of less than 10 years, no difference in OS, vascular events, or transformation to AML/MDS was observed between the two treatment arms. In the final analysis, longer follow-up demonstrated important differences in results re3910 © 2011 by American Society of Clinical Oncology 35 P = .008 0.6 0.4 0.2 5 10 15 20 25 30 35 Time (years) C Hydroxyurea Pipobroman 0.8 30 Hydroxyurea Pipobroman 0.8 0 Cumulative incidence of AML/MDS (probability) Overall Survival (probability) 1.0 25 1.0 Time (years) C 20 Time (years) 1.0 Hydroxyurea alone Pipobroman alone 0.8 P = .002 0.6 0.4 0.2 0 5 10 15 20 25 30 Time (years) Fig 3. Transformation to acute myeloid leukemia/myelodysplastic syndrome (AML/MDS). Cumulative incidence of AML/MDS according to (A) the intentionto-treat population receiving hydroxyurea or pipobroman, (B) the main treatment received (hydroxyurea or pipobroman), and (C) patients who received only one treatment. garding the long-term outcome of patients with PV as well as the impact of HU and pipobroman therapies (summarized in Table 1). The median OS of the entire cohort was 17 years. Overall, we found that life expectancy of patients with PV was significantly altered compared with that of the age- and sex-matched general population, with an SMR of 1.84. Similar results have been previously reported in retrospective studies.20 Furthermore, in the ITT population analysis, the median OS was significantly longer in patients treated with HU (20.3 years) compared with those who received pipobroman (15.4 years). Of note, the main cause of death in patients with PV who were younger than 65 years of age at diagnosis was evolution to AML/MDS (54%), with vascular events responsible for cause of death in 15% of JOURNAL OF CLINICAL ONCOLOGY Downloaded from jco.ascopubs.org on September 9, 2014. For personal use only. No other uses without permission. Copyright © 2011 American Society of Clinical Oncology. All rights reserved. Long-Term Follow-Up From the FPSG Trial 0.8 A Hydroxyurea stopped Pipobroman stopped Death prior to hydroxyurea discontinuation Death prior to pipobroman discontinuation P = .002 0.6 0.4 0.2 0 5 10 15 20 25 30 Cumulative Incidence of VE/Hemorrhages (probability) Cumulative Incidence (probability) 1.0 1.0 Hydroxyurea arm Pipobroman arm 0.8 0.6 0.4 0.2 0 5 10 Time (years) patients. These results are similar to those reported in a phase II study of pipobroman involving 164 patients with PV21 in whom evolution to AML/MDS was responsible for 29% of deaths in the entire patient cohort and 51% of deaths in patients younger than age 60 years at time of inclusion. The combined results of these two long-term, prospective trials indicate that in younger patients with accurately managed PV and minimized vascular risk, evolution to AML/MDS is the most important long-term concern. Importantly, compared with the first analysis,17 the number of transformations to AML/MDS increased from 13 to 51, establishing a cumulative incidence of AML/MDS of 23.6% at 15 years. This is Cumulative Incidence (probability) 1.0 0.8 Myelofibrosis, hydroxyurea treatment Myelofibrosis, pipobroman treatment Death prior to myelofibrosis, hydroxyurea treatment Death prior to myelofibrosis, pipobroman treatment P = .07 0.6 0.4 0.2 0 5 10 15 20 25 30 35 Time (years) Cumulative Incidence (probability) B 1.0 0.8 Myelofibrosis, hydroxyurea treatment Myelofibrosis, pipobroman treatment Death prior to myelofibrosis, hydroxyurea treatment Death prior to myelofibrosis, pipobroman treatment P = .02 0.6 0.4 0.2 0 5 10 15 20 25 30 35 Time (years) Fig 5. Cumulative incidence of myelofibrosis (A) according to treatment randomization and (B) according to main treatment received (hydroxyurea or pipobroman). www.jco.org Cumulative Incidence of VE/Hemorrhages (probability) B Fig 4. Treatment duration after random assignment. A 15 20 25 30 35 Time (years) 1.0 Hydroxyurea arm Pipobroman arm 0.8 0.6 0.4 0.2 0 5 10 15 20 25 30 35 Time (years) Fig 6. Cumulative incidence of vascular events (VEs) according to treatment arm: (A) intention-to-treat population; (B) per protocol analysis. clearly higher than previously reported incidence rates, which have been reported to range from approximately 5% to 16%.10,11 In addition, a significant difference in favor of HU arose. The higher incidence of leukemic evolution in patients treated with pipobroman, along with the shorter median OS, clearly indicates that this drug should no longer be used as first-line therapy but may be reserved for use as second-line treatment in patients with a short life expectancy. Of note, this increased risk observed with pipobroman was not dependent on treatment duration (Grambsch and Therneau proportional hazard test P ⫽ .75), suggesting that its indication should not be based solely on the age of the patient. These findings are particularly important in countries such as France and Italy where pipobroman is still used as first-line treatment for PV. The data presented here provide further evidence for the debate on the leukemogenicity of HU. Evolution to AML is part of the natural history of PV, but data on the impact of HU on this evolution are not established. Early comparisons of HU and phlebotomy showed no significant difference between incidences of leukemic transformation.18 Indeed, such evolution has been reported in untreated patients and in those treated with phlebotomies only.1,7 On the basis of the available evidence, the main short-term risk associated with PV is assumed to be the occurrence of vascular events. Therefore, management has been based on cytoreduction aimed at increasing the patient’s life expectancy by lowering the risk of fatal thrombosis. In this study, we confirm that HU and pipobroman are both equally active in efficiently reducing the risk of thrombosis in PV. However, PV is a chronic disorder requiring ongoing treatment, and little is known from prospective studies about the risk of AML in © 2011 by American Society of Clinical Oncology Downloaded from jco.ascopubs.org on September 9, 2014. For personal use only. No other uses without permission. Copyright © 2011 American Society of Clinical Oncology. All rights reserved. 3911 Kiladjian et al patients receiving HU over the long term. To date, evidence suggests that HU may have an impact on cytogenetic abnormalities and biologic features of PV and may slightly enhance the risk of transformation to leukemia.6 Follow-up data from PVSG-08 have allowed the long-term leukemogenic potential of HU in PV to be assessed.7 As previously mentioned, early data (378 weeks of treatment) from the same study18 suggested that HU was not associated with an increased risk of leukemic conversion. However, at a median follow-up of 8.6 years (maximum, 795 weeks), 5.9% of patients receiving HU developed AML compared with 1.5% receiving phlebotomies.7 The increased cumulative incidence of AML/MDS seen with HU in this study may be due to patients living longer as a result of more effective therapeutic options. A longer survival period potentially provides a greater time frame for leukemic evolution because patients spend longer with PV and also receive cytotoxic treatment for a longer period. Thus, it is currently unclear whether the observed incidence of AML/MDS should be attributed to the natural long-term evolution of PV, which is unaffected by palliative HU therapy, or cumulative HU therapy per se. More information on prospective long-term follow-up is still required to help establish any clear patterns between HU treatment and AML incidence. Studies started more than 10 years ago are expected to show interesting data, but follow-up across a time frame similar to the one in this study has not yet been reported. It has been shown that treatment with more than one agent in succession adversely affects the outcome of patients.13 In this study, we found that a switch from HU to pipobroman was clearly associated with an increased risk of death. However, this result should be interpreted cautiously, because the need for changing therapy may simply reflect a more aggressive disease. Hematologic evolution to MF was found to be higher in patients treated predominantly with HU (32% at 20 years) compared with those treated with pipobroman. This is in line with results seen in the previous analysis.17 Silverstein et al22 previously reported that patients with PV who developed MF appeared to have a higher rate of leukemia transformation compared with those who did not. A similar trend has been seen in essential thrombocythemia; results from a study in 231 patients suggested that prior MF was a risk factor for subsequent leukemia transformation (P ⫽ .008).23 The number of patients in this study who developed AML/MDS after MF was small, and there are insufficient data to determine whether MF may be an intermediate stage in the progression to AML in patients with PV. In conclusion, the data from this study show that the most important long-term concern in patients with PV younger than age 65 REFERENCES 1. Berk PD, Goldberg JD, Donovan PB, et al: Therapeutic recommendations in polycythemia vera based on Polycythemia Vera Study Group protocols. Semin Hematol 23:132-143, 1986 2. McMullin MF, Bareford D, Campbell P, et al: Guidelines for the diagnosis, investigation and management of polycythaemia/erythrocytosis. Br J Haematol 130:174-195, 2005 3. Michiels JJ, Berneman ZN, Schroyens W, et al: Pathophysiology and treatment of platelet-mediated microvascular disturbances, major thrombosis and bleeding complications in essential thrombocythaemia and polycythaemia vera. Platelets 15:67-84, 2004 3912 © 2011 by American Society of Clinical Oncology years should be the evolution to AML/MDS, which was the primary cause of death in these patients. Although pipobroman clearly appears leukemogenic even when used as a single agent, long-term follow-up of this prospective, randomized study also found a risk of evolution to AML with HU higher than that previously reported. However, there is no conclusive evidence for a leukemogenic risk associated with HU, particularly given that the development of AML is part of the natural history of PV. Nevertheless, our analysis highlights the importance of evaluating the long-term leukemogenic risk of conventional treatments such as HU versus supposed nonleukemogenic agents such as IFN-␣.24,25 A large randomized trial is currently being performed jointly in the United States and Europe to compare HU and IFN-␣ in the first-line treatment of high-risk patients with PV (Myeloproliferative Disorders Research Consortium Clinical Trial 112). This trial may provide data for resolving the question of associated leukemogenic risk of each treatment. In addition, current development of new drugs targeting Janus kinase may provide new agents without anticipated leukemogenic potential to treat patients with PV.26 AUTHORS’ DISCLOSURES OF POTENTIAL CONFLICTS OF INTEREST Although all authors completed the disclosure declaration, the following author(s) indicated a financial or other interest that is relevant to the subject matter under consideration in this article. Certain relationships marked with a “U” are those for which no compensation was received; those relationships marked with a “C” were compensated. For a detailed description of the disclosure categories, or for more information about ASCO’s conflict of interest policy, please refer to the Author Disclosure Declaration and the Disclosures of Potential Conflicts of Interest section in Information for Contributors. Employment or Leadership Position: None Consultant or Advisory Role: None Stock Ownership: None Honoraria: Jean-Jacques Kiladjian, Novartis, Celgene, YM BioSciences, Shire, AOP Orphan Pharmaceuticals Research Funding: None Expert Testimony: None Other Remuneration: None AUTHOR CONTRIBUTIONS Conception and design: Jean-Didier Rain Collection and assembly of data: Jean-Jacques Kiladjian, Sylvie Chevret, Christine Chomienne, Jean-Didier Rain Data analysis and interpretation: All authors Manuscript writing: All authors Final approval of manuscript: All authors 4. Spivak JL: Polycythemia vera: Myths, mechanisms, and management. Blood 100:4272-4290, 2002 5. Berk PD, Goldberg JD, Silverstein MN, et al: Increased incidence of acute leukemia in polycythemia vera associated with chlorambucil therapy. N Engl J Med 304:441-447, 1981 6. Barbui T: The leukemia controversy in myeloproliferative disorders: Is it a natural progression of disease, a secondary sequela of therapy, or a combination of both? Semin Hematol 41:15-17, 2004 7. Fruchtman SM, Mack K, Kaplan ME, et al: From efficacy to safety: A Polycythemia Vera Study group report on hydroxyurea in patients with polycythemia vera. Semin Hematol 34:17-23, 1997 8. Passamonti F, Malabarba L, Orlandi E, et al: Polycythemia vera in young patients: A study on the long-term risk of thrombosis, myelofibrosis and leukemia. Haematologica 88:13-18, 2003 9. Barbui T, Barosi G, Birgegard G, et al: Philadelphia-negative classical myeloproliferative neoplasms: Critical concepts and management recommendations from European LeukemiaNet. J Clin Oncol 29:761-770, 2011 10. Tatarsky I, Sharon R: Management of polycythemia vera with hydroxyurea. Semin Hematol 34: 24-28, 1997 11. Weinfeld A, Swolin B, Westin J: Acute leukaemia after hydroxyurea therapy in polycythaemia vera and allied disorders: Prospective study of efficacy and leukaemogenicity with therapeutic implications. Eur J Haematol 52:134-139, 1994 JOURNAL OF CLINICAL ONCOLOGY Downloaded from jco.ascopubs.org on September 9, 2014. For personal use only. No other uses without permission. Copyright © 2011 American Society of Clinical Oncology. All rights reserved. Long-Term Follow-Up From the FPSG Trial 12. West WO: Hydroxyurea in the treatment of polycythemia vera: A prospective study of 100 patients over a 20-year period. South Med J 80:323327, 1987 13. Finazzi G, Caruso V, Marchioli R, et al: Acute leukemia in polycythemia vera: An analysis of 1638 patients enrolled in a prospective observational study. Blood 105:2664-2670, 2005 14. Monto RW, Tenpas A, Battle JD Jr, et al: A-8103 in polycythemia. JAMA 190:833-836, 1964 15. Brusamolino E, Salvaneschi L, Canevari A, et al: Efficacy trial of pipobroman in polycythemia vera and incidence of acute leukemia. J Clin Oncol 2:558561, 1984 16. Passamonti F, Brusamolino E, Lazzarino M, et al: Efficacy of pipobroman in the treatment of polycythemia vera: Long-term results in 163 patients. Haematologica 85:1011-1018, 2000 17. Najean Y, Rain JD: Treatment of polycythemia vera: The use of hydroxyurea and pipobroman in 292 patients under the age of 65 years. Blood 90:33703377, 1997 18. Kaplan ME, Mack K, Goldberg JD, et al: Longterm management of polycythemia vera with hydroxyurea: A progress report. Semin Hematol 23: 167-171, 1986 19. Landolfi R, Marchioli R, Kutti J, et al: Efficacy and safety of low-dose aspirin in polycythemia vera. N Engl J Med 350:114-124, 2004 20. Passamonti F, Rumi E, Pungolino E, et al: Life expectancy and prognostic factors for survival in patients with polycythemia vera and essential thrombocythemia. Am J Med 117:755-761, 2004 21. Kiladjian JJ, Gardin C, Renoux M, et al: Longterm outcomes of polycythemia vera patients treated with pipobroman as initial therapy. Hematol J 4:198-207, 2003 22. Silverstein MN, Brown AL Jr, Linman JW: Idiopathic myeloid metaplasia: Its evolution into acute leukemia. Arch Intern Med 132:709-712, 1973 23. Chim CS, Kwong YL, Lie AK, et al: Long-term outcome of 231 patients with essential thrombocythemia: Prognostic factors for thrombosis, bleeding, myelofibrosis, and leukemia. Arch Intern Med 165: 2651-2658, 2005 24. Kiladjian JJ, Cassinat B, Chevret S, et al: Pegylated interferon-alfa-2a induces complete hematologic and molecular responses with low toxicity in polycythemia vera. Blood 112:3065-3072, 2008 25. Quinta´s-Cardama A, Kantarjian H, Manshouri T, et al: Pegylated interferon alfa-2a yields high rates of hematologic and molecular response in patients with advanced essential thrombocythemia and polycythemia vera. J Clin Oncol 27:54185424, 2009 26. Verstovsek S, Kantarjian H, Mesa RA, et al: Safety and efficacy of INCB018424, a JAK1 and JAK2 inhibitor, in myelofibrosis. N Engl J Med 363:1117-1127, 2010 ■ ■ ■ Shape Your Future and Ours: Apply for ASCO’s Leadership Development Program If you completed your final subspecialty training between 2002 and 2007 and are interested in becoming a future leader in both ASCO and the pracce of oncology, ASCO’s Leadership Development Program is for you. If selected, you will: • • • • Network with and receive mentorship from ASCO leadership Gain exposure to ASCO commiees and government research agencies Enhance leadership skills through interacve sessions Receive first-hand advocacy experience on Capitol Hill To apply or learn about the eligibility requirements for the Leadership Development Program, please visit www.asco.org/leadership www.jco.org © 2011 by American Society of Clinical Oncology Downloaded from jco.ascopubs.org on September 9, 2014. For personal use only. No other uses without permission. Copyright © 2011 American Society of Clinical Oncology. All rights reserved. 3913











© Copyright 2026