ABC
docz
Explore
Log in
Create new account
Download
Report
health and fitness
disorders
mental disorder
a.d.d.
here. - Movincog Initiative â Centre for Brain Research
Dyslexia 101 Final draft - The State Education Resource Center
Dr. Karen Smith. UofM Presentation.April 18 2015
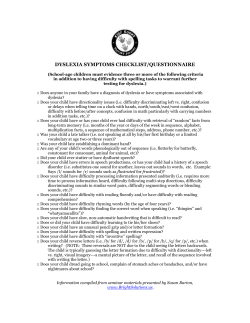
DYSLEXIA SYMPTOMS CHECKLIST/QUESTIONNAIRE
WHY TA AKE FLIG
The HIDDEN IMPAIRMENTS PROJECT (HIP) What is it? Hidden Impairments (HI)
Maydayreturns Brochure
Devon Outreach and Devon Outreach QE SpLD Support and
Ben Glenn has been a full-time speaker since 1995, sharing with
Dyslexia FREE Information for teachers and other professionals
CAMPUS NEWS HUDSPETH REGIONAL CENTER Important Dates
Indsæt navn, adresse mv - Center for Neuroplasticity and Pain
© Copyright 2026
About abcdocz
DMCA / GDPR
Report