
Thyroid Eye Disease: Current and Emerging Therapies Clinical Update
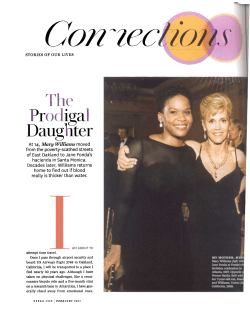
Clinical Update OCU LOPL A STICS Thyroid Eye Disease: Current and Emerging Therapies by denny smith, contributing writer interviewing kimberly p. cockerham, md, and raymond s. douglas, md, phd E r ay m o n d s . d o u g l a s , m d , p h d xcept perhaps for diabetic retinopathy, thyroid eye disease, or TED, may be the most multifaceted medical challenge that ophthalmologists face. The characteristic exophthalmos, eyelid retraction, strabismus and diplopia familiar to ophthalmologists are just a few of the many symptoms of hyperthyroidism, a systemic autoimmune disorder also known as Graves disease. The systemic symptoms of hyperthyroidism include arrhythmias, myopathy, hyperhidrosis, menstrual irregularities, insomnia, anxiety, weight loss, mood disorders, fatigue and shortness of breath. But the ocular manifestations may have a greater psychosocial impact and may call for a more customized approach than the systemic problems. “Without intervention, the disfigurement and dysfunction of TED can lead to job loss, quality-of-life issues and divorce,” said Kimberly P. Cockerham, MD, who has cared for many TED patients in her oculoplastic and neuro-ophthalmology practice in Los Altos, Calif. Control of Systemic Disease Is No Cure for TED Medical management of systemic thyroid disease is well established with radioactive iodine or antithyroid medications. If these treatments fail, thyroidectomy is a possible next step. Fortunately, in at least nine out of 10 patients, the disease resolves with treatment. Moreover, “the active phase O r bi t al D e c o mp r e s si o n Patient who had exposure keratopathy as a result of exophthalmos is shown before (left) and two months after (right) orbital decompression surgery. of disease lasts for 18 to 36 months in most patients and will evolve into an inactive state even without any intervention,” said Dr. Cockerham. However, systemic therapy does not address the exophthalmos caused by TED, for which corticosteroids have long been the main treatment. But because the side effects of corticosteroids have made clinicians hesitant to use them for extended periods, steroidsparing immunosuppressive agents such as azathioprine, cyclosporine and methotrexate, along with biologics like adalimumab and rituximab, have been tried for TED. A stepwise approach to TED. Nevertheless, Dr. Cockerham has found that her patients generally respond to a course of steroids that is limited enough in dose and duration to avoid serious side effects. “My average TED patient is not going to be treated with immunosuppressants. If the patient has moderate to severe TED, IV steroids, such as 250 mg of methylprednisolone given weekly for six weeks, can be effective and will avoid the side effects of oral steroids,” she said. She also wants her patients to be comfortable during this period. “In mild active disease, Nasonex [mometasone nasal inhalation], which is lipophilic, can enter the orbit through the thin medial wall. This, used along with preservative-free artificial tears, can improve patient comfort.” For her patients who don’t respond to that six-week steroid course, Dr. Cockerham offers surgical decompression of the orbit; and, if that fails, her next step is x-ray therapy. Only when the results of XRT are inadequate does she try immunosuppressive therapy. “Immunosuppressants are usually reserved for patients whose condition defies steroids, radiation and surgical decompression.” Customization is key. Raymond S. Douglas, MD, PhD, associate professor of ophthalmology and director of the TED center at the University of Michigan in Ann Arbor, uses the same therapies but varies their order and emphasis. Dr. Douglas said that corticosteroids are indeed the first-line therapy for most Canadian and European ophthalmologists. “But in the e y e n e t 31 Oculoplastics United States, we try to use them sparingly, often as a bridge between therapies. The effects of steroids are transient, and studies have demonstrated minimal long-term improvement with their use. I probably take more patients off steroids than I put on. My treatment rationale is customized based upon the severity of the disease and the likelihood of double vision or optic neuropathy threatening the patient’s vision. So my preferred initial therapy is patience, possibly with short-term steroids, followed by decompression surgery. XRT is way down on my list, since controlled studies have uniformly shown it to be ineffectual.” Rituximab to the rescue. However, Dr. Douglas is optimistic about one agent now being tried for TED treatment: the biologic agent rituximab. “Thus far, studies of rituximab are limited; but, in our anecdotal experience, we have had fantastic results with it. The effect of rituximab in patients with severe disease that has failed to respond to steroids has been dramatic, and I will consider its use in patients who are not candidates for surgery. At 500 mg, administered intravenously by slow infusion twice, two weeks apart, rituximab stops the progression of TED virtually immediately. Within two to four weeks, the disease became quiescent in more than 20 patients we have followed.” Collaborate with endocrinologists. Dr. Douglas also customizes TED treatment by collaborating closely with endocrinologists who are managing his patients’ systemic thyroid disorder. “We like to have the thyroid controlled medically, surgically or with radioactive iodine prior to orbital management if possible.” C o ul d Ri t u x imab B e a G am e Chang e r? Every once in a while, a drug appears to have so many uses that it generates the claims—and the concerns—of a “miracle” product. Rituximab, one of the newest agents being studied in the treatment of TED, could be one of those drugs. This monoclonal antibody, which targets the CD20 antigen on B cells, is currently marketed as Rituxan in the United States and MabThera elsewhere. Administered by slow IV infusion, it costs $5,000 to $10,000 per dose. Originally approved in the 1990s to treat relapsed or refractory B-cell non-Hodgkin lymphoma, its approved indications have since expanded to encompass chronic lymphocytic leukemia as well as rheumatoid arthritis, Wegener granulomatosis and microscopic polyangiitis. It is also being used off label in the treatment of uveitis, diabetes, systemic lupus erythematosus, hemolytic anemia, idiopathic thrombocytopenic purpura and Sjögren syndrome. It is even being studied in organ transplant rejection and chronic fatigue syndrome. Dr. Douglas was one of the principal investigators in a trial that looked at rituximab in treating TED. In this case series, all six patients with corticosteroid-refractory disease experienced rapid and sustained resolution of orbital inflammation and optic neuropathy following treatment with rituximab.1 Another recent study of 12 patients also achieved promising results,2 and a randomized, double-blind trial is currently under way at the Mayo Clinic. However, Dr. Douglas said that drugs that modulate the immune cascade pose a threat of opportunistic infection, and some patients taking rituximab run the risk of a devastating reactivation of previously quiescent infections, including progressive multifocal leukoencephalopathy (PML), the subject of a black box warning. “Although I am very optimistic about rituximab, we currently cannot treat with it because it is not covered by insurance; and the manufacturer, Genentech, is not interested in additional clinical trials in nonmalignant disease due to the risk of PML.” 1 Khanna, D. et al. Ophthalmology 2010;117(1):133–139.e2. 2 Silkiss, R. Z. et al. Ophthal Plast Reconstr Surg 2010;26(5):310–314. generally remains quiescent after it has been controlled. “Once hyperthyroidism is inactive, it is unusual to see it reactivate,” Dr. Cockerham said. “I have had only two patients reactivate over 23 years.” Good News on TED Prognosis Dr. Douglas noted that, despite the sometimes severe cosmetic problems associated with exophthalmos, less than 5 percent of patients suffer visual loss, most commonly from optic neuropathy secondary to optic nerve compression. In addition, unlike other autoimmune disorders, hyperthyroidism Future Therapies Even though treatment success rates are high, Dr. Cockerham would like a more reliable and safer protocol for her TED patients. “Ideally, there would be a minimally invasive treatment that would prevent the complications of TED.” Drug-eluting devices. Dr. Cockerham is pursuing the possibility of using ocular implant technology for treating exophthalmos in TED. “The best bet would be an orbital implant that elutes immunomodulators. Eluting technology has evolved, but because orbital disease is a relatively 32 2 0 1 1 n o v e m b e r / d e c e m b e r infrequent diagnosis, financial backing is tough to get. I am currently funded by the U.S. Department of Defense to optimize an episcleral implant, and I hope to translate that into orbital applications.” IGF-I blockers. Dr. Douglas noted another novel therapeutic approach in TED: “The insulinlike growth factor I receptor has been implicated in TED, and a drug blocking the interaction of the IGF-I receptor with the immune system may be highly beneficial. So while specific, potent immunomodulators such as rituximab remain interesting for the treatment of TED, I am even more excited about the prospect of a new class of treatment that will block recognition and activation of autoantigens in this disease.” Drs. Cockerham and Douglas report no financial disclosures.











© Copyright 2026