
Allergic skin diseases in dogs and cats: an introduction R.E.W. Halliwell
DERMATOLOGY Allergic skin diseases in dogs and cats: an introduction R.E.W. Halliwell(1) for the development of the Coombs’ test, and who died in 2005. He and his colleague proposed four types based upon the then current understanding of the underlying immunological mechanisms. • Type 1, with an onset from minutes to hours after allergen exposure, and involving IgE antibody and mast cells. • Type 2, involving antibody-dependant cytotoxicity. • Type 3, involving antigen/antibody immune complexes. • Type 4, or delayed hypersensitivity in which the onset occurs 24-48 hours after application of the antigen, and which is mediated by lymphocytes rather than antibody. This paper was commissioned by FECAVA for publication in EJCAP. Allergy in man – a brief history The study of allergy, and of the allergic diseases has fascinated scientists in the medical and veterinary field for many years. The immune responses are supposed to be protective. How and why does the damaging immune response – which we term allergy, develop? Allergy in the dog and cat The earliest documented report of the existence of a condition resembling atopic dermatitis (AD) in man concerned the Emperor Octavian Augustus who was born in 63BC. In the 1920s, Coca and Cooke had introduced the term “atopy”, literally meaning “strange disease” to include the conditions of allergic asthma and hay fever, both of which had familial tendencies [1]. Immunotherapy was used extensively at that time, with the first report of its successful use appearing in 1911 [2]. The classical work of Prausnitz and Küstner showed in a series of elegant experiments that the antibody associated with these conditions (termed “reagin”) was an unusual one, in that it (i) was heat labile, and (ii) could be transferred to the skin of normal individuals as shown by a resultant wheal and flare reaction upon subsequent injection of allergen [3]. The study of AD really commenced in the 1930s, when it was termed Prurigo Besnier. It was included under the heading of “atopy” in that it shared the same familial tendencies, and children who suffered from AD often went on to develop asthma or hay fever Also, similarly to the former two conditions, affected patients usually had positive skin tests to environmental allergens. The importance of allergy in skin diseases of dogs and cats became apparent to veterinarians in the USA in the 1930s. Schnelle, working at the Angel Memorial Hospital in Boston documented that 15% of all cases seen were accorded a diagnosis of “eczema”, and further that 56.9% of all dogs with skin disease, and 26.6% of all cats similarly affected were deemed to be suffering from this condition [6]. Similar figures were reported from the clinics at Cornell University in Ithaca, New York [7]. Although it was generally believed that “eczema” was a manifestation of allergy, the exact nature of the inciting cause was controversial, with most emphasis being placed upon foods. The seasonal nature of many cases puzzled the early workers, and it was Kisileff who in 1938 proposed that an allergic reaction to the bites of fleas was the cause of ”summer eczema” [8]. In 1941, Whittich, who was a human allergist, reported on a dog with perennial pruritus due to a food allergy that suffered seasonal exacerbations from a concomitant pollen allergy [9]. This was, in fact, the first well-documented case of canine AD. The dog was treated with an appropriate hypoallergenic diet and effectively hyposensitized with injections of allergenic extracts of the pollens to which sensitivity was shown. Little progress was made in further unravelling the pathogenesis until the 1960s. At that time it was believed that the reagin was IgA. But the painstaking work of the Ishizakas showed that it was a previously undescribed immunoglobulin class that they termed IgE [4]. In the 1960s and 1970s, the condition was known as canine “atopy” or “atopic disease”, and was studied extensively by Schwartzman and colleagues at the University of Pennsylvania [e.g. 10]. These terms were at that time preferred to that of atopic dermatitis in that it was unclear whether the canine disease represented the true analogue of the well-characterised At that time, the nomenclature used to describe the allergic diseases was in some disarray, and it was Gell and Coombs who proposed the modern day classification [5]. Robin Coombs was a Cambridge veterinary graduate, who of course is best known 1) Richard E.W. Halliwell Royal (Dick) School of Veterinary Studies, Easter Bush Veterinary Centre, Roslin Midlothian EH25 9RG, UK 209 EJCAP - Vol. 19 - Issue 3 December 2009 pruritic dogs [23]. Reliable information on the incidence of atopic dermatitis and of AFRs in the cat, and on the relative incidence of the two is not available. atopic dermatitis of children. It was also termed “allergic inhalant dermatitis” from the mistaken belief that the route of access of allergen was primarily, if not exclusively via the respiratory tract. Indeed it was not until 2006 that the major route was shown to be percutaneous [11], with research over the past two decades highlighting the similarities between the canine disease and human AD [e.g. 12, 13]. Fewer studies have been conducted on allergic contact dermatitis in animals, but it is clear that the incidence in dogs is far less than that of either AD or AFRs. True allergic contact dermatitis is exceedingly rare in the cat, although the susceptibility of this species to contact sensitisation has been demonstrated [24]. In the 1970s, canine IgE was identified, purified and characterized. It was shown to share common antigenic determinants with its human counterpart, and to be associated with mast cells in canine skin [14]. Indeed the dog was the first species in which this was directly demonstrated. At that time also techniques for the serological quantitation of allergen-specific IgE were developed for both man and dogs. Genetic susceptibility to allergic skin diseases Atopic dermatitis Under the original definition of an atopic disease, a genetic trait is a prerequisite, and familial tendencies in both man and in the dog have long been known. Hence breed predispositions are inevitable, and are well-known. These will vary from one part of the world to another. In a study conducted at the University of California, where the incidence was compared to the base clinic population, the Labrador retriever, golden retriever, West Highland white terrier, Chinese shar-pei, bull terrier, bichon frisé, Tibetan terrier and English springer spaniel were all significantly over-represented, whereas mixed breeds were protected [25]. The populations of teaching hospitals can be biased, however, and more reliable data is obtained when comparisons are made with the national population. The requirement in Switzerland for a national canine register has enabled such a study, in which the West Highland white terrier, boxer, French bulldog, bull terrier, Dalmatian, Vizsla and Basset hound were significantly over represented [26]. In a study conducted in the United Kingdom, the heritability of AD amongst Labrador and golden retrievers was found to be high, at 0.47, implying a strong genetic trait [27]. Few studies have been conducted in cats, apart from a report of three littermates all of whom were affected with AD [28]. Research on the mechanisms of the allergic diseases in cats lagged behind the canine studies by several decades. Although the existence of feline IgE could have been readily anticipated, and evidence of cross-reactivity between canine and putative feline IgE was provided in 1993 [15], it was not until 1998 that the production of antisera specific for that isotype was reported [16]. Incidence of allergic skin diseases It is widely held that skin disease is very common, and in a recent survey in the UK such cases comprised 24% of all nonroutine presentations to veterinarians for treatment [17] and this was the single most common system affected. In temperate climates there is no doubt that flea infestation and/or allergy has contributed the highest proportion of such cases, but the availability of the newer ectoparasiticides, some as over-thecounter products, has helped to reduce these numbers. The reported incidence of canine AD has ranged from a high of 15% of the general population [18] to 8% of referrals to a teaching hospital – which obviously is a selected and biased population [19]. In a recent survey of >30,000 cases presented to 52 private practices in the USA, a diagnosis of atopic/allergic dermatitis, allergy or atopy was made in 8.7%, which accounted for 21.6% of dogs and cats presented with skin or ear disease [20]. Given the clear heritability of AD, an attempt was made to develop a beagle model by selective inbreeding for IgE levels [29]. This high IgE-producing beagle strain also has the abnormal barrier function that is a feature of AD in both man and dogs [30], and develops a disease indistinguishable from AD upon epicutaneous exposure with house dust mite antigen. The incidence of adverse food reactions (AFRs) in dogs will depend upon the rigor with which the diagnosis is made. Commonly, one hypoallergenic diet trial, using either a commercial or home-prepared diet, is cited in publications as justification for excluding a diagnosis in a perennially pruritic dog. Lamb and rice was a popular choice, in that lamb is uncommonly fed. But the demonstration that cross-reacting antigens between beef and lamb are frequently recognized [21] implies that AFRs have probably been underdiagnosed in the past. It is generally agreed that AFRs, as a cause of perennial pruritus in dogs, are much less frequent than is AD. In a recent study of 181 perennially pruritic dogs, the diagnosis was made (often with concomitant AD) in 29% and 32% of cases respectively using a home prepared or commercial hydrolysate diet [22], with AD presumably being responsible for the greater proportion. However the incidence relative to AD was apparently higher in another study of 113 dogs in which AFRs were implicated in 41% of perennially Human AD is not caused by a single gene defect, but is a polygenic disorder with complex inheritance. Recently, results of a canine study using microarray and quantitative PCR analysis of candidate genes, demonstrated striking similarities with the gene abnormalities reported in man [31]. Other allergic skin disease It has been shown that atopic dogs are predisposed to the development of flea allergy dermatitis [32,33,34], but no further studies on the heritability have been undertaken. No predisposition to allergic contact dermatitis has been noted in man, and a heritable trait would not be expected in animals. But interesting recent information has emerged regarding AFRs. In the Swiss study referred to above, a breed predisposition has been shown for West Highland white terriers, German 210 Allergic skin diseases in dogs and cats: an introduction - R.E.W. Halliwell shepherds, pugs, boxers and the Rhodesian ridgeback [26]. Also clearly indicating a genetic trait was the chance discovery of an inbred colony of beagle Maltese crosses showing spontaneous IgE-mediated food allergy with both gastrointestinal and dermatological signs [35]. conditions in small animals in general practice. Vet Rec. 2006; 158:533-539. [18] Chamberlain KW. Atopic (allergic) dermatitis. Vet Clin N Am. 1974; 4: 29-39. [19] Scott DW, Paradis M. A survey of canine and feline skin disorders seen in a university practice: small animal clinic, University of Montreal, Saint-Hyacinthe, Quebec, (1987-1988). Can Vet J. 1990; 31: 830-835. [20] Lund EM, Armstrong PJ, Kirk CA, Kolar LM, Klausner JS. Health status and population characteristics of dogs and cats examined at private veterinary practices in the United States. J Am Vet Med Assoc. 1999; 214: 1336-1441. [21] Martin A, Sierra M-P, Gonzales JL, Arevalo M-A. Identification of allergens responsible for cutaneous adverse food reactions to lamb, beef and cow’s milk. Vet Dermatol. 2004; 15: 349-356. [22]. Loeffler A, Soares-Magalhaes R, Bond R, Lloyd DH. A retrospective analysis of case series using home-prepared and chicken hydrolysate diets in the diagnosis of adverse food reactions in 181 pruritic dogs. Vet Dermatol. 2006; 17: 273-279. [23] Jackson HA, Murphy KM, Tater KC, Olivry T, Hummel JB, Itensen J et al. The pattern of allergen hypersensitivity (dietary or environmental) of dogs with non-seasonal atopic dermatitis cannot be differentiated of the basis of historical or clinical information: a prospective evaluation 2003-2004. Vet Dermatol. 2005; 16: 200. [24] Schultz KT, Maguire HC. Chemically induced delayed hypersensitivity in the cat. Vet Immunol Immunopathol. 1982; 3: 585-590. [25] Zur G, Ihrke PJ, White SD, Kass PH. Canine atopic dermatitis: A retrospective study of 266 cases examined at the University of California, Davis, 1992-1998. Part 1. Clinical features and allergy testing results. Vet Dermatol. 2002; 13: 89-102. [26] Picco F, Zini E, Nett C, Naegeli B, Bigler B, Rufenacht S et al. A prospective study on canine atopic dermatitis and food-induced allergic dermatitis in Switzerland. Vet Dermatol. 2008; 19: 150155. [27] Shaw SC, Wood JLN, Freeman J, Littlewood JD, Hannant D. Estimation of the heritability of atopic dermatitis in Labrador and Golden Retrievers. Am J Vet Res. 2004; 65: 1014-1020. [28] Moriello, K. Feline atopy in three littermates. Vet Dermatol. 2001; 12: 177-181. [29] Olivry T, Deangelo KB, Dunston SM, Clarke KB, McCall CA. Patch testing of experimentally sensitized beagle dogs: development of a model for skin lesions of atopic dermatitis. Vet Dermatol. 2006; 17: 95-102. [30] Marsella R, Girolomoni G. Canine models of atopic dermatitis: A useful tool with untapped potential. J Invest Dermatol 2009; 19: 2351-2357. [31] Wood SH, Clements DN, Ollier WE, Nuttall T, McEwan NA, Carter SD. Gene expression in canine atopic dermatitis and correlation with clinical severity scores. J Dermatol Sci. 2009; 55: 27-33. [32] Halliwell REW, Preston JF, Nesbitt J. Aspects of the immunopathogenesis of flea allergy in dogs. Vet Immunol Immunopathol. 1987; 17: 483-494. [33] Schick RO, Fadok VA. Responses of dogs to regional allergens: 268 cases 1981-1984. J Am Vet Med Assoc. 1986; 189: 14931496. [34] Carlotti DN, Costargent F. Analysis of positive skin tests in 449 dogs with allergic dermatitis. Eur J Comp Anim Pract. 1994; 4: 42-59. [35] Jackson HA, Hammerberg B. Evaluation of a spontaneous canine model of immunoglobulin E-mediated food hypersensitivity: dynamic changes in serum and fecal allergen-specific immunoglobulin E values relative to dietary change. Comp Med. 2002; 52: 316-321. Conclusions Allergic skin diseases continue to pose challenges for clinicians and researchers alike. Close interaction between these two, and between those investigating the human disease counterparts with veterinary colleagues will surely enable speedier progress. Nonetheless, the past three decades has seen remarkable advances both in our understanding of the disease processes, and the delivery of better therapeutic approaches, many of which are detailed in this issue. References [1] [2] [3] [4] [5] [6] [7] [8] [9] [10] [11] [12] [13] [14] [15] [16] [17] Noon L. Prophylactic inoculation against hay-fever. Lancet 1911; 1: 1572-1573. Prausnitz C, Küstner H. Studien über die Uberimfindlichkeit. Zentralb Bact. 1921; 86: 160-169. Coca AF, Cooke RA. On the classification of the phenomenon of hypersensitiveness. J Immunol. 8: 163-166, 1923. Ishizaka K, Ishizaka T. Identification of γ-E antibodies as carriers of reaginic antibody. J Immunol. 1967; 99: 1187-1198. Coombs RRA, Gell PGH. Classification of allergic reactions responsible for clinical hypersensitivity and disease. In: Gell PGH, Coombs RRA (Eds). Clinical Aspects of Immunology. Blackwell Scientific, Oxford, 1975; 761-770. Schnelle GB. Eczema in dogs – an allergy. North Am Vet. 1933; 14: 37-40. Milks HJ. The role of allergy in skin diseases of dogs. Cornell Vet. 1938; 28: 142-147. Kissilef A. The dog flea as a causative agent in summer eczema. J Am Vet Med Assoc. 1938; 93: 21-25. Wittich FW. Spontaneous allergy (atopy) in the lower animal. J Allergy. 1941; 12: 247-251. Halliwell REW, Schwartzman RM. Atopic disease in the dog. Vet Rec. 1971; 89: 209-214. Marsella R, Nicklin C, Lopez J. Studies on the routes of allergen exposure in high IgE-producing beagle dogs sensitized to house dust mites. Vet Dermatol. 2006; 17: 306-312. Olivry T, Moore PF, Affolter VK, Nayadan DK. Langerhans cell hyperplasia and IgE expression in canine atopic dermatitis. Arch Dermatol Res. 1996; 288: 579-585. Olivry T, Naydan DK, Moore PF. Characterization of the cutaneous inflammatory infiltrate in canine atopic dermatitis. Am J Dermatopathol. 1997; 19: 477-486. Halliwell REW. The localization of IgE in canine skin – an immunofluorescent study. J Immunol. 1973; 110: 422-430. De Boer DJ, Saban R, Schultz KT, Bjorling DE. Feline immunoglobulin E: preliminary evidence of its existence and cross-reactivity with canine IgE. Ihrke PJ, Mason IS, White SD (eds). Advances in Veterinary Dermatology 11. Pergamon, Oxford, 1993; 51-62. Gilbert S, Halliwell REW. Production and characterisation of polyclonal antisera against feline IgE. Vet Immunol Immunopathol 1998; 63: 223-233. Hill PB, Eden CA, Huntley S, Morey V, Ramsey S, Richardson C et al. Survey of the prevalence and treatment of dermatological 211 EJCAP - Vol. 19 - Issue 3 December 2009 UB Cam 2.0TM Videoscope A useful tool for various applications in veterinary clinics • • • • • Small and handy Excellent image quality Live recordings as well as still images Easy way to show images (before/after) to client Easy way to file image documentation UB Cam enables the vet to record high resolution images, eg as image documentation in terms of patient journalisation. The videoscope is also an excellent tool for visual client information from narrow spaces such as the ear ducts and the oral cavity. These options make the videoscope highly useful for eg otoscopy, dermatoscopy and as an oral camera during dental procedures. Includes: 5 different speculae (funnels): 3 mm, 4 mm, 5 mm short, 5 mm long and 7 mm 1 speculum, 7 mm, with working channel 1 ear speculum, 9 mm 1 speculum for dermatoscopy and ophthalmoscopy, 35 mm 5 m extension cable Used here as a dermatoscope to depict skin changes Cat. No 270175 EXPERIENCE · QUALITY · SERVICE For more information please contact JØRGEN KRUUSE AS · tel +45 72 14 15 16 · e-mail: [email protected] 212 DERMATOLOGY The immunopathogenesis of allergic skin diseases in dogs and cats R.E.W. Halliwell(1) SUMMARY Hypersensitivity in veterinary medicine has been recently redefined as “Objectively reproducible clinical signs initiated by exposure to a defined stimulus at a dose tolerated by normal dogs” [1]. A number of different types exist, broadly mediated by antibody or immunocompetent lymphoid cells. However this represents an oversimplification, and, as exemplified especially by atopic dermatitis (AD), a complex interplay between various arms of the innate and acquired immune systems is involved. that accompany AD, are attributable to defects in the innate immune system, which has been extensively studied in man, and which has several components. There have been few studies in veterinary medicine, but the similarities in the disease between man and dog are such that similar abnormalities are likely. The description that follows draws heavily on studies undertaken in man [2], with veterinary studies specifically referred to when available. This paper was commissioned by FECAVA for publication in EJCAP. Atopic dermatitis The currently accepted definition of canine atopic dermatitis (AD) is: “A genetically predisposed inflammatory and pruritic skin disease with characteristic clinical features associated with IgE antibodies most commonly directed against environmental allergens” [1]. There exists also a subset of canine AD in which IgE antibodies are not detectable. This is termed “atopic-like” dermatitis, and appears to be the equivalent of intrinsic AD in man. (a). Pattern recognition receptors: These receptors recognize pathogens in the context of broad molecular patterns termed “pathogen-associated molecular patterns” (or PAMPS). Best characterised are the Toll-like receptors (TLRs). They are expressed by antigen-presenting cells, mast cells, neutrophils and keratinocytes. One of these, TLR2, has been shown to be deficient in some patients with AD thus rendering the skin more susceptible to infection. The definition of classical canine AD implies a pivotal role for IgE in the pathogenesis which may well be the case. However in fact the pathogenesis of AD is exceedingly complex, and can be categorised under three headings, viz (i) defects in innate immunity, (ii) defects in barrier function, and (iii) defects in acquired immunity. (b). Neutrophils: Histopathology of both human and canine AD patients – even in the face of significant infection – are notable for the paucity of neutrophils. A number of studies in man have shown that upregulation of the leucocyte adhesion molecule CD11b is markedly decreased in human patients with AD as compared to normal individuals. (i) Defects in innate immunity The innate immune system is phylogenetically the oldest, and provides the first line of defence against invading microorganisms. In man, 80-100% of nonlesional skin of AD patients is colonised with Staph aureus as compared with 5-30% of normals. This, and many of the other abnormalities (c). Antimicrobial peptides (AMPs): These come from a number of sources, including keratinocytes, neutrophils, sebocytes and the cells of sweat gland ducts. They are generally present at low or undetectable levels, and at markedly increased levels in the 1) Richard E.W. Halliwell Royal (Dick) School of Veterinary Studies, Easter Bush Veterinary Centre, Roslin Midlothian EH25 9RG, UK 213 EJCAP - Vol. 19 - Issue 3 December 2009 face of injury. They have broad antimicrobial activity. A number have been shown to be deficient in human patients with AD, including LL-37. Vitamin D enhances LL-37 activity, and thus vitamin D, and particularly D3, may offer potential in treating infections. Canine studies on AMPs, however, have so far shown equivocal results [3]. high IgE-producing beagle model, have suggested that a Th2 response is associated with the acute phase of AD, whereas a Th1 response is associated with the chronic phase, were secondary infection is superimposed [15, 16, 17, 18, 19, 20]. The cytokines derived respectively from a Th2 and Th1 response promote that response via a positive feedback mechanism. Conversely, they are mutually inhibitory – i.e. γIFN inhibits the Th2 response, which has led to the use of γ-INF as a treatment for CAD [21]. Similarly, successful immunotherapy in CAD is accompanied by a shift from Th2 to Th1 [22]. Defects in barrier function That barrier function is abnormal in both human and canine AD is well known. Barrier function is at two levels: (i) at the level of the Stratum corneum, composed of terminally differentiated corneocytes surrounded by a matrix of specialised lipids, and (ii) the tight junctions of the Stratum granulosa. In man, a mutation of filaggrin has been shown to be highly associated with AD, but is not present in all cases, and so other abnormalities must contribute [4]. In the dog, studies regarding filaggrin are ongoing, but it has been shown that the skin of dogs with AD contain lipids in globules, rather than dispersed to fill in all the intercellular spaces [5,6]. In man, abnormalities of the tight junctions have also been shown and are associated with reduction of claudin-1 in patients with AD [7]. Mediators involved The preformed, mast cell derived mediators are clearly of importance in canine and feline AD. They include histamine, proteases and serotonin, although there is little evidence that the latter is contributory. The limited efficacy of antihistamines as a sole treatment implies that other mediators are likely to have more pronounced pruritogenic and inflammatory effects. The membrane-derived mediators, especially the leukotrienes, and particularly LTB4 are implicated in a range of inflammatory dermatoses including AD and are promising targets for pharmacologic intervention [23]. In addition, the inflammatory cell milieu that characterizes AD offers the potential for the involvement of many other inflammatory mediators that are derived from keratinocytes and other epidermal and dermal sources. The spectrum of inflammatory mediators is thus multiple, which explains why drugs that target single mediators are generally only marginally effective. Abnormalities in acquired immunity Histopathology of the lesions A study of the histopathology and immunohistochemistry of infiltrating cells gives valuable insights into disease pathogenesis. This has been studied in clinical cases, and also in atopy patch tests, were an antigen (usually house dust mite) is applied to the skin under occlusion. Biopsies of cases of canine AD, show evidence of epidermal Langerhans’ cell hyperplasia, and these often appear in clusters [8]. Armed with IgE antibody, these play a pivotal role in allergen capture and processing. Also noted are increased numbers of dermal dendritic cells that have similar functions [8,9]. Mast cell hyperplasia is frequently noted on histopathology reports, but careful studies have failed to demonstrate significant differences in the mast cell density in the dermis of atopic and normal dogs, [10]. Lymphocytes are frequent in the cellular infiltrate, with the vast majority being T cells, with only few B cells [9]. Both CD4+ and CD8+ cells are found in increased numbers, with a major increase in CD8+ cells in the epidermis. Finally, neutrophils and eosinophils are certainly seen in biopsies of affected skin, but in neither case are they a dominant feature. Secondary features in the pathogenesis Both bacterial overgrowth and overt pyoderma are common features of canine AD, although much less so in feline AD. A major reason for this is the enhanced ability of canine staphylococcal species to adhere to corneocytes of atopic dogs. This has been demonstrated by both in vitro and in vivo studies [24, 25]. The fact that IgE antibodies to antigens of the organism can develop makes this an important factor in the disease process [26]. Similarly, malassezia overgrowth is well documented [27], although precise quantitative studies comparing colonisation densities in atopic and normal dogs are lacking. As is the case with staphylococcal infection, an IgE response can compound the disease process [28]. Malassezia overgrowth has also been documented in allergic cats [29]. Histopathological features of feline AD are highly variable from case to case, although to an extent this may be reflective of a lack of defined criteria for the diagnosis [11]. There is generally an increase in the numbers of mast cells and eosinophils, with the latter being more prominent than in the dog [12]. Increases in CD4+ and CD8+ cells are noted as is an increase in dermal dendritic cells [13, 14]. The likely sequence of events The complexity of the immunopathogenesis of AD is such that any schematic representation of the chain of events involved must of necessity be speculative. Nonetheless, it is helpful to document the current views of the process – albeit in simplified form (see Fig 1). 1. Impaired barrier function facilitates the percutaneous absorption of allergen. 2. Allergen is captured by Langerhans’ cells armed with IgE antibody. 3. In the resultant immune response to the allergen, the genetic features of the atopic trait favour the development of an IgE response (Th2) – which is largely elaborated in the local lymph node. Th1 vs Th2 It is well established that T cell responses in man and animals fall into one of two patterns – a Th1 response associated with IL-2, IL-12, γ-IFN and IL-18, which is expressed as cell-mediated immunity, and a Th2 response associated with IL-4, IL-5, IL-6 and IL-13 and facilitating antibody production, including IgE. Multiple studies undertaken in dogs and cats, including the 214 The immunopathogenesis of allergic skin diseases in dogs and cats - R.E.W. Halliwell Fig. 1 A simplified scheme depicting the acquisition of sensitivity and the development of inflammation in canine atopic dermatitis. 4. Exposure of mast cells armed with IgE antibody initiates release of preformed and newly generated mediators, which aids the influx of inflammatory cells. 5. In turn, these release other pro-inflammatory mediators. 6. Particularly in the chronic phase, a concomitant Th1 response occurs with γIFN prominent. 7. Secondary infection compounds the problem, leading to further Th1 responses. 8. A failure of immune regulation allows the continuation of the immune responses and resultant inflammation. organ that is affected (e.g. skin vs gastrointestinal tract). That IgE-mediated food hypersensitivity exists in the dog is clear from (i) studies on experimental induction [30], (ii) on thorough immunological investigations of spontaneous cases [31], and (iii) on the characterization of an in-bred colony of beagle/Maltese crosses [32]. However it should be emphasized that although in the latter case IgE to incriminated allergens is readily demonstrable, dynamic changes in allergen-specific levels do not reliably follow withdrawal of the incriminated food and challenge – for which there are a number of possible explanations. The pathogenesis of food hypersensitivity However IgE-mediated food hypersensitivity is likely to be involved only in cases that relapse within 24-48 hrs of challenge – which accounts for only a small proportion of the confirmed cases [33]. Conventionally, adverse reactions to foods are divided into food hypersensitivity, where immune mechanisms are involved, and food intolerance where pharmacological factors are responsible (e.g. histamine and histamine-releasing factors). There is no data on the relative incidence of the two types. This discussion will dwell solely on the former. If one extrapolates from the situation in man, the majority of cases are likely to result from a combination of IgEmediated reactions, with cell-mediated hypersensitivity and/ or IgG antibody. In people with atopic dermatitis where food hypersensitivity is involved, the best diagnostic results are achieved when IgE is measured and patch testing with food antigens is also undertaken, and this is probably reflective of the dual nature of the immunopathogenesis [34]. Compared to the situation in man, there is a paucity of data on the pathogenesis of food hypersensitivity, and the veterinary literature contains a plethora of dogma based upon unreliable information. The first point to emphasize is that food hypersensitivity is not one disease – rather it is a spectrum of diseases that vary in their immunological mechanisms and in the 215 EJCAP - Vol. 19 - Issue 3 December 2009 A B C D Fig. 2 Histopathology depicting the immunopathogenesis of canine flea allergy dermatitis. (a) Acute oedema 15 minutes after a flea bite. (b) Histpathology of the immediate (15 minute) reaction showing egress of eosinophils from a blood vessel into the dermis. (c) Predominantly mononuclear infiltrate at 48 hrs after a flea bite depicting the delayed (cell-mediated) hypersensitivity component. (d) Biopsy 12 hrs after a flea bite showing influx of basophils (arrows) as compared to mast cells (pink arrow). The pathogenesis of flea allergy dermatitis The relevance of IgG antibody measurements, and hence of the involvement of this isotype in the pathogenesis is controversial. In a study which measured food-specific IgE and IgG in 22 cases of confirmed adverse food reactions, the difference in antibody levels between normal dogs and those with confirmed adverse food reactions was actually greater in the case of IgG than it was for IgE [35]. However, association is not causation. Similarly, in a recent study of irritable bowel syndrome in man, a placebo-controlled diet trial was undertaken based upon the measurement of food antigen-specific IgG. Those patients who were fed a diet that excluded antigens to which an IgG response was shown exhibited significantly superior outcomes than did those fed a diet including such antigens [36]. Again, this does not, of course, necessarily indicate that the IgG was implicated in the disease process – it could well be an epiphenomenon. The immunopathogenesis of flea allergy dermatitis (FAD) has been the subject of much study over the past 3 decades. Initially, it was assumed that the work done on guinea pigs in the 1960s was directly applicable to the dog and cat, but it was established that this was not the case. The flea allergen It is generally held that salivary allergens injected when the flea sucks blood are responsible for the immune response. Early work suggested that the allergen was a hapten which became a complete allergen on union with dermal collagen [37], but more recent studies have shown that there are a number of protein allergens involved [38], and the major allergen which is recognised by some 90% of flea allergic dogs has been cloned and produced in recombinant form [39]. In summary, there is good data on the role of IgE in a small proportion of cases. Whether cell-mediated hypersensitivity or IgG antibody is responsible for the majority of cases, perhaps in conjunction with IgE, must await results of further studies. 216 The immunopathogenesis of allergic skin diseases in dogs and cats - R.E.W. Halliwell dogs often maintain this state indefinitely, although with time the incidence of hypersensitivity tends to decline [38, 43]. It does not appear, however, that the same features are applicable to feline FAD [45]. The pathogenesis of allergic contact dermatitis It is generally believed that uncommon condition results from a delayed, cell-mediated hypersensitivity [46, 47]. However the characteristic epidermal spongiosis that is seen in man is infrequently observed in clinical cases and in biopsies of positive patch test sites, and whilst the dermal infiltrate does contain mononuclear cells, a significant neutrophilic influx suggests that the immunopathogenesis, and hence the cytokine milieu may differ from that in man (Fig 3) [48]. The infrequency with which this condition is observed in veterinary medicine makes in depth investigations difficult. Conclusions The current state of knowledge of the pathogenesis of allergic skin diseases in the dog and cat has been reviewed. Although much progress has been made over the past three decades, much remains to be done. The realization that canine AD in particular is a good model for the study of human AD, will likely facilitate further studies in this area. Fig. 3 Biopsy of a positive patch test in a case of allergic contact dermatitis. Epidermal spongiosis with a mixed cell inflammatory infiltrate is seen. References Immunological mechanisms involved Observation of the sites of flea feeding in allergic dogs show that in the majority of dogs, an immediate reaction occurs which is papular or urticarial. This may wane to be replaced by a papular eruption which is maintained for up to 4-5 days. Histopathology of these reaction sites at varying times has revealed features of both immediate (IgE-mediated) hypersensitivity evidenced by oedema between the collagen bundles, and an egress of eosinophils from dermal blood vessels and of delayed (cellmediated) hypersensitivity with a perivascular predominantly mononuclear cell infiltrate (Fig 2 a, b, c) [40]. In some 10-20% of patients, delayed reactions only are noted, and assays for flea allergen-specific IgE will be negative. If biopsies are taken between 4 and 18hrs after a flea bite, special processing and staining will reveal an influx of basophils which may account for up to 20% of the cellular infiltrate (Fig 2 d) [41]. The pathogenesis is thus quite complex, and it is also possible that IgG antibodies may be involved, as they are readily detectable in the sera of patients with FAD [42]. Interestingly, animals who are continually exposed and who suffer no obvious clinical signs are totally or partially immunologically tolerant, and their sera have an absence of IgE antibodies, and low or undetectable levels of IgG [42, 43]. [1] Halliwell R. Revised nomenclature for veterinary allergy. Vet Immunol Immunopathol. 2006; 114: 207-208. [2] De Benedetto A, Agnihothri R, McGirt LY, Bankova LG, Beck LA. Atopic dermatitis: a disease caused by innate immune defects? J Invest Dermatol. 2009; 129: 14-30. [3] Van Damme CMM, Willemse T, van Dijk A, Haagsman HP, Veldhuizen EJA. Altered cutaneous expression of β-defensins in dogs with atopic dermatitis. Molecular Immunol. 2009; 46: 22492455. [4] Barker JN, Palmer CN, Zhao Y, Liao H, Hull PR, Lee SP et al. Null mutations in the filaggrin gene (FLG) determine major susceptibility to early-onset atopic dermatitis that persists into adulthood. J Invest Dermatol. 2007; 127: 564-567. [5] Inman AO, Olivry T, Dunston SM, Montiero-Rivierre NA, Gatto H. Electron microscopic observations of stratum corneum intercellular lipids in normal and atopic dogs. Vet Pathol. 2001; 38: 720-723. [6] Marsella R, Girolomoni G. Canine models of atopic dermatitis: A useful tool with untapped potential. J Invest Dermatol 2009; 19: 2351-2357. [7] De Benedetto A, Latchney L, McGirt L, Vidyasagar S, Cheadle C, Barnes KC et al. The tight junction protein claudin-1 is dysregulated in atopic dermatitis. J Allergy Clin Immunol. 2008; 119: s280 (abstr). [8] Olivry T, Moore PF, Affolter VK, Nayadan DK. Langerhans cell hyperplasia and IgE expression in canine atopic dermatitis. Arch Dermatol Res. 1996; 288: 579-585. [9] Olivry T, Naydan DK, Moore PF. Characterization of the cutaneous inflammatory infiltrate in canine atopic dermatitis. Am J Dermatopathol. 1997; 19: 477-486. [10] Welle MM, Olivry T, Grimm S, Suter M. Mast cell density and subtypes in the skin of dogs with atopic dermatitis. J Comp Pathol. 1999; 120: 187-197. The development of hypersensitivity Studies on the experimental induction of FAD have shown that all dogs can become sensitized, although atopic dogs are predisposed [44]. Early antigenic exposure and continual exposure tend to be protective, whereas intermittent exposure favours the development of hypersensitivity. Once hypersensitive, 217 EJCAP - Vol. 19 - Issue 3 December 2009 dog: A model for food allergy. Lab Anim Sci. 1997; 47: 40-49. [31] Martin A, Sierra M-P, Gonzales JL, Arevalo M-A. Identifications of allergens responsible for cutaneous adverse food reactions to lamb, beef and cow’s milk. Vet Dermatol. 2004; 15: 349-356. [32] Jackson HA, Hammerberg B. Evaluation of a spontaneous model of IgE-mediated food hypersensitivity; dynamic changes in serum and fecal allergen-specific immunoglobulin E values relative to dietary change. Comp Med. 2002; 52: 316-321. [33] Rosser EJ. Diagnosis of food allergy in dogs. J Am Vet Med Assoc. 1993; 203: 259-262. [34] Roehr CC, Reibel S, Zeigert M, Sommerfield C, Wahn U, Niggemann B. Atopy patch test, together with determination of specific IgE levels, reduces the need for oral food challenges in children with atopic dermatitis. J Allergy Clin Immunol. 2001; 107: 548-553. [35] Halliwell REW, Gordon CM, Horvath C, Wagner R. IgE and IgG antibodies to food antigens in sera from normal dogs, dogs with atopic dermatitis and dogs with adverse food reactions. In: Hillier A, Foster AP, Kwochka KW (eds). Advances in Veterinary Dermatology Vol 5, Blackwell, Oxford, 2005, 28-35. [36] Atkinson W, Sheldon TA, Shaath N, Whorwell PJ. Food elimination tests based upon IgG antibodies in irritable bowel syndrome: a randomised controlled trial. Gut. 2004; 53: 1459-1464. [37] Michaeli D, Benjamini E, Deburen FP, Larivee DH, Feingold BF. The role of collagen in the induction of flea bite hypersensitivity. J Immunol. 1965; 95: 162-170. [38] Halliwell REW, Preston JF, Nesbitt J. Aspects of the immunopathogenesis of flea allergy in dogs. Vet Immunol Immunopathol. 1987; 17: 483-494. [39] McDermott MJ, Weber E, Hunter S, Stedman KE, Best E, Frank GR et al. Idenification, cloning and characterization of a major cat salivary flea allergy (Cte f 1). Molecular Immunol. 2000;37:361375. [40] Gross TL, Halliwell REW. The histopathology of experimental flea allergy dermatitis in dogs. Vet Pathol. 1985; 22: 78-81. [41] Halliwell REW, Schemmer KR. The role of basophils in the immunopathogenesis of hypersensitivity to fleas (Ctenocephalides felis) in dogs. Vet Immunol Immunopathol. 1987; 15: 283-289. [42] Halliwell REW, Longino, SL. IgE and IgG antibodies to flea allergen in differring dog populations. Vet Immunol Immunopathol. 1985; 8: 215-223. [43] Halliwell REW. Clinical and immunological aspects of allergic skin diseases in domestic animals. In: von Tscharner C, Halliwell REW (eds). Advances in Veterinary Dermatology Vol 1, Balliere Tindall, London, 1990, 91-116. [44] Carlotti DN, Costargent F. Analysis of positive skin tests in 449 dogs with allergic dermatitis. Eur J Comp Anim Pract. 1994; 4: 42-59. [45] Kunkle GA, McCall CA, Stedman KE, Pilny C, Nicklin C, Logas DB. Pilot study to assess the effects of early flea exposure on the development of flea hypersensitivity in cats. J Fel Med Surg. 2003; 5: 287-294. [46] Kunkle GA. Contact dermatitis. Vet Clin N Am Small Anim Pract. 1988; 18: 1061-1068. [47] Kunkle GA, Gross TL. Allergic contact dermatitis to Tradescantia fluminensis (wandering Jew) in a dog. Comp Cont Ed Pract Vet. 1984; 5: 925-929. [48] Thomsen MK, Thomsen HK. Histopathological changes in canine allergic contact dermatitis patch test reactions. A study on spontaneously hypersensitive dogs. Acta Vet Scand. 1989; 30: 379-384. [11] Taglinger K, Day MJ, Foster AP. Characterization of inflammatory cell infiltration in feline allergic skin disease. J Comp Pathol. 2007; 137: 211-223. [12] Roosje PJ, Koeman JP, Thepen T, Willemse T. Mast cells and eosinophils in feline allergic dermatitis: A qualitative and quantitative analysis. J Comp Pathol. 2004; 131: 61-69. [13] Roosje PJ, van Kooten PJS, Thepen T, Bihari IC, Rutten VPMG, Koeman JP et al. Increased numbers of CD4+ and CD8+ T cells in lesional skin of cats with allergic dermatitis. Vet Pathol. 1998; 35: 268-273. [14] Roosje PJ, Thepen T, Rutten VPMG, van den Brom WE, BruijnzeelKoomen CAFM, Willemse T. Immunophenotyping of the cutaneous cellular infiltrate after atopy patch testing in cats with atopic dermatitis. Vet Immunol Immunopathol. 2004; 101: 143151. [15] Olivry T, Dean GA, Tomkins MB, Dow JL, Moore PF. Toward a canine model of atopic dermatitis: Amplification of cytokine-gene transcripts in the skin of atopic dogs. Exp Dermatol. 1999;8:204211. [16] Nuttall TJ, Knight PA, McAleese SM, Lamb JR, Hill PB. T-helper 1, T-helper 2 and immunosuppressive cytokines in canine atopic dermatitis. Vet Immunol Immunopathol. 2002; 87: 379-384. [17] Nuttall TJ, Knight PA, McAleese SM, Lamb JR, Hill PB. Expression of Th1, Th2 and immunosuppressive cytokine gene transcripts in canine atopic dermatitis. Clin Exp Allergy. 2002; 32: 789-795. [18] Marsella R, Olivry T, Maeda S. Cellular and cytokine kinetics after epicutaneous allergen challenge (atopy patch testing) with house dust mites in high-IgE beagles. Vet Dermatol. 2006; 17: 111-120. [19] Roosje PJ, Dean GA, Willemse T, Rutten VPMG, Thepen T. Interleukin 4-producing CD4+ T cells in the skin of cats with allergic dermatitis. Vet Pathol. 2002; 39: 228-233. [20] Taglinger K, Van Nguyen N, Helps CR, Day MJ, Foster AP. Quantitative real-time RT-PCR measurement of cytokine mRNA expression in the skin of normal cats and cats with allergic skin disease. Vet Immunol Immunopathol. 2008; 122: 216-230. [21] Iwasaki T, Hasegawa A. A randomized comparative clinical trial of recombinant canine interferon-gamma (KT-100) in atopic dogs using antihistamine as control. Vet Dermatol. 2006; 17: 195-200. [22] Shida M, Kadoya M, Park S-J, Nishifuji, K, Momoi Y, Iwasaki T. Allergen-specific immunotherapy induces Th1 shift in dogs with atopic dermatitis. Vet Immunol Immunopathol. 2004;102:19-31. [23] Kietzmann M. Eicosanoid levels in canine inflammatory skin disease. In: Von Tscharner C, Halliwell REW (Eds). Advances in Veterinary Dermatology, Vol 1, Balliere Tindall, London, 211-220. [24] McEwan NA, Kalna G, Mellor D. A comparison of adherence by four strains of Staphylococcus intermedius and Staphyloccus hominus to canine corneocytes collected from normal dogs and dogs suffering from atopic dermatitis. Res Vet Sci. 2005; 78: 193198. [25] Simou C, Thoday KL, Forsythe PJ, Hill PB. Adherence of Staphylococcus intermedius to corneocytes of healthy and atopic dogs: Effect of pyoderma, pruritus score, treatment and gender. Vet Dermatol. 2005; 16: 385-391. [26] Morales CA, Schultz KT, DeBoer DJ. Antistaphylococcal antibodies in dogs with recurrent staphylococcal pyoderma. Vet Immunol Immunopathol. 1994;42:137-147. [27] Nardoni S, Dini M, Taccini F, Mancianti F. Occurrence, distrtibution and population size of Malassezia pachydermatis on skin and mucosae of atopic dogs. Vet Microbiol. 2007; 122: 172-177. [28] Nuttall TJ, Halliwell RE. Serum antibodies to Malassezia yeasts in canine atopic dermatitis. Vet Dermatol 2001; 12: 327-332. [29] Ordeix L, Galeotti F, Scarampella F, Dedola C, Bardagi M, Romano E et al. Malassezia spp overgrowth in allergic cats. Vet Dermatol. 2007; 18: 316-323. [30] Ermel RW, Kock M, Griffey SM, Reinhart GA, Frick OL. The atopic 218 DERMATOLOGY Clinical signs and diagnosis of canine atopic dermatitis C. Favrot1) SUMMARY Canine Atopic Dermatitis (CAD) is the most frequent canine dermatosis. It has been defined by the International Task Force on Canine Atopic Dermatitis ( ITFCAD) as a “genetically predisposed inflammatory and pruritic allergic skin disease with characteristic clinical features associated with IgE antibodies most commonly directed against environmental allergens”[1]. A ITFCAD-revised nomenclature for veterinary allergy also takes into account dogs with clinical signs of atopic dermatitis but no demonstrable allergen-specific IgE (Intradermal tests and/or serology): the term atopic-like dermatitis (ALD) was coined to described this group of dogs[1]. breeds while some others have been based on a comparison between atopic dogs and the hospital or insurance population [5-13]. The former do not present any statistical analysis and the latter may be biased by the absence or the underrepresentation of healthy dogs. One single study is based on a large population of insured dogs but contains another potential bias: the authors did not make the diagnosis of CAD themselves but referred to the diagnosis of general practitioners, who may have This paper was commissioned by FECAVA for publication in EJCAP. Introduction In veterinary dermatology, cutaneous adverse food reaction (CAFR) and CAD have been historically considered as two different conditions[2]. In fact, CAFR includes both immunemediated and non immune-mediated food intolerances and may be associated with a wide range of clinical signs such as gastro-intestinal disturbances, urticaria, angioedema, and signs mimicking those of atopic dermatitis. This latter point has led the ITFCAD International Task Force on Canine Atopic Dermatitis to suggest that some cases of CAFR may trigger flares of atopic dermatitis[3]. The clinical signs of CAD may thus be associated with sensitization to environmental (CAD sensu stricto), food allergens (CAFR with clinical signs of CAD: Food-Induced Atopic Dermatitis: FIAD) or with ALD. The present article will consequently describe the clinical features and diagnostic methods of dogs affected by CAD from whatever cause. The clinical signs and diagnostic methods of food allergy are however beyond the scope of this article. used variable inclusion criteria [6]. To further complicate the analysis, predisposed breeds may vary by geographical areas [14, 15]. One single study is based on the comparison of a population of atopic dog and a validated population of healthy dogs [16]. This study was however limited to Switzerland. Some breeds such as West Highland white terriers, boxers, Bulldogs are, however, mentioned in virtually all these studies. Some others such as German shepherd dogs, golden retrievers or Labrador retrievers seem to be predisposed for CAD only in some geographical regions. Signalement of CAD dogs Reports of sex predisposition in CAD dogs are inconsistent. Some studies reported predisposition for male, female or for neither sex [14]. We have recently studied a large population of 843 CAD dogs and no sex predilection was detected when the whole population was taken into account [17]. However, some sex predispositions were detected in some breed such as golden or Labrador retrievers (more female) or Boxer (more male). The definition of CAD suggests strong breed and/or familial predispositions. Reliable evaluation of breed predispositions for veterinary diseases is complicated by the fact that the population at risk is often unknown. Several studies have, however, addressed the question of breed predisposition for CAD [4]. Some studies only mentioned the most frequently represented The typical age at onset of CAD is reported to be between 6 months and 3 years [14]. We have however recently shown that about 78% of CAD present with clinical signs before three years of age [17]. It does mean that every fifth CAD dog develops the first clinical signs later in life. 1) Claude Favrot, Clinic for Small Animal Internal Medicine, Vetsuisse Faculty, University of. Zurich 219 Clinical signs and diagnosis of canine atopic dermatitis - History of CAD dogs Information regarding the history of the affected dog should be recorded carefully. Some important questions have already been mentioned (age at onset, breed, familial predisposition) but some others such as seasonality, presence of “pruritus sine material” (pruritus with no skin changes) at onset, efficacy of previous treatment, should be asked before any clinical examination. Clinical signs of CAD may be seasonal or not but seasonality is often present at onset (42-75%) [14]. Approximately 80% of dogs with seasonal signs are symptomatic in spring or summer while the others exhibit signs in winter or autumn [18]. It should be mentioned that some dogs with non seasonal disease do exhibit worsening of clinical signs during one specific season. Fig. 2 Secondary infections develop in the vast majority of atopic dogs ( in this case, malassezia dermatitis) Pruritus must be present and its absence rules out the diagnosis CAD. In fact, some CAD dogs do exhibit initially pruritus sine material. This feature was recorded in 61% of affected dogs in our recent study [17]. As well, 43% of CAD dogs presented first with an episode of otitis externa. In comparison, associated conjunctivitis /blepharitis are much rarer. CAD dogs are often treated with glucocorticoids and responses to such therapy should be evaluated carefully. In the same study, we have shown that 78% of CAD dogs responded adequately to such treatment. In the first stages of the disease, the pruritus responds well and readily to the administration of reduced amount of glucocorticoid (i.e. 0.3-0.5mg/kg Prednisolone daily). In chronic cases however, the development of secondary bacterial or yeast infections usually corresponds with a poorer response to such treatment. to the lack of pathognomonic signs and the protean clinical picture. Erythema and pruritus are however virtually always present and often represent the first clinical signs (Fig. 1). However, mild pruritus may remain unrecognized by the owner and the veterinarian may sometimes rely on indirect proofs of pruritus such as the presence of excoriations or saliva-coloured hairs. Most of the signs are actually due to self-trauma and/or secondary infections. In fact, small erythematous papules, which are considered the primary lesion of CAD, are rarely observed in CAD dogs [14]. The practitioner will usually observe the consequences of the inflammation and pruritus, namely excoriations and self-induced alopecia and/or the signs of the secondary bacterial infection (papules, pustules, crusts, erosions) and/or the symptoms of secondary yeast dermatitis (epidermal hyperplasia, hyperpigmentation, lichenification). Recurrent or chronic skin or ear infections are very frequently observed in CAD (Fig. 2): In our study, bacterial infections were observed in 66% of the patients while malassezia dermatitis and otitis externa were present in 33% and 50% of all affected dogs, respectively. Last but not least, we have also showed that 82% of atopic dogs spend most of their time indoor. This suggests that prolonged exposure to house dust mites may trigger or worsen CAD clinical signs. Clinical signs of CAD Although very frequent, CAD may be difficult to diagnose owing Fig. 1 Pruritus and erytham are virtually always present in atopic dogs. Fig. 3 Feet are very often affected in atopic dogs. 220 EJCAP - Vol. 19 - Issue 3 December 2009 Tab. 1 Criteria for the diagnosis of canine atopic dermatitis and associated sensitivity and specificity. 1. Age at onset < 3years 2. Mostly indoor 3. Corticosteroid-responsive pruritus 4. Chronic or recurrent yeast infections 5. Affected front feet 6. Affected ear pinnae 7. Non –affected ear margins 8. Non-affected dorso-lumbar area Sensitivity when 5 criteria are fulfilled: 85% Specificity when 5 criteria are fulfilled: 79% Sensitivity when 6 criteria are fulfilled: 58% Specificity when 6 criteria are fulfilled: 88% Fig. 4 Axillae are affected in about 62% of atopic dogs. Most of these signs are however not specific at all and the distribution of these lesions is consequently more helpful. The most often affected areas are the pinnae (58%), the axillae (62%), the abdomen (66%), the front (79%) and hind feet (75%), the lips (42%) and the perineal area (43%) (Figures 3 and 4). Unfortunately, all these areas are rarely simultaneously affected in the same individual, except in chronic cases. ruled out. Depending on the clinical presentation and the age of the affected dog, some other differentials, i.e.demodicosis, dermatophytosis, cheyletiellosis, cutaneous lymphoma should be properly ruled out. It should also be mentioned that the histological aspect of allergic skin is usually not specific and that this test is consequently not adequate to make the diagnosis. It may be indicated, however, to perform skin biopsies in some instances, to rule out some differentials such as cutaneous lymphoma, for example. As well, allergy testing (serological evaluation of allergen-specific IgE and intradermal skin testing) are not regarded as criteria for the diagnosis of CAD. This is because numerous healthy dogs are sensitized to environmental allergens and are consequently positive (poor specificity of this criterion) and ALD and some FIAD dogs are deemed negative. These tests should consequently be only carried out to identify the offending allergens (i.e. to choose the allergens for allergenspecific immune therapy: desensitization). In the same way, inorder to identify FIAD dogs, a 6-to 8-week elimination diet and a subsequent challenge with the previous food should be carried out in all dogs with clinical signs of CAD. Dermatological (pyotraumatic dermatitis, interdigital fistulae) and non dermatological signs are sometimes associated with CAD and their presence should reinforce the suspicion. Spring/summer conjunctivitis, for example, is presented in approximatively 20% of CAD dogs while gastro-intestinal signs (soft stools, diarrhea, vomiting) are recognized in 26% of FIAD dogs. Clinical signs of FIAD dogs differ very slightly from those of classical, environment-induced AD. In fact, in our study, statistically significant differences were only uncovered for gastro-intestinal signs, seasonality, cortico-sensible pruritus and pruritus sine material (less frequent in FIAD dogs). As well, more FIAD dogs show the first clinical signs early in life (less than one year) or, on the contrary, rather late (more than 6 years of age). Several sets of criteria have been proposed for the diagnosis of CAD. These criteria are however mainly used for clinical trial to increase homogeneity of the recruited dogs [12, 14, 19, 20]. We have recently performed a study, in which 1800 pruritic dogs were included by experienced dermatologists throughout the world [17]. One of the goals of the study was to identify criteria for the diagnosis of CAD. The best identified set of criteria (see table) has been associated with a sensitivity and specificity of about 80%, when 5 out of 8 criteria are fulfilled (Tab. 1). It does mean that using these sole criteria would lead the practionner to make a wrong diagnosis in every fifth dog. These data confirm that ruling out resembling diseases should always be a compulsory prerequisite for the diagnosis of CAD. Diagnosis of CAD The diagnosis of CAD is based on the history (age at onset, seasonality, pruritus sine material at onset, familial or breed predisposition, previous response to glucocorticoids), the development of the disease (seasonality, “wax and wane” character, development of secondary skin infections) and the lesional pattern. A diagnosis of CAD should however never been made, as long as resembling diseases such as fleas, ectoparasites (sarcoptic mange) and primary skin infections have not been 221 Clinical signs and diagnosis of canine atopic dermatitis - References [1] Halliwell R. Revised nomenclature for veterinary allergy. Vet Immunol Immunopathol. 2006; 114(3-4): p. 207-8. [2] Hillier A, Griffin CE. The ACVD task force on canine atopic dermatitis (X): is there a relationship between canine atopic dermatitis and cutaneous adverse food reactions? Vet Immunol Immunopathol. 2001; 81: p. 219-226. [3] Olivry T, et al. Food for thought: pondering the relationship between canine atopic dermatitis and cutaneous adverse food reactions. Vet Dermatol. 2007; 18(6): p. 390-1. [4] Sousa CA, Marsella R. The ACVD task force on canine atopic dermatitis (II): genetic factors. Vet Immunol Immunopathol. 2001; 81: p. 153-158. [5] Koch HJ, Peters S. 207 intrakutantests bei hunden mit verdacht auf atopische dermatitis. Kleintierprax. 1994; 39: p. 25-36. [6] Nodtvedt A. et al. Canine atopic dermatitis: validation of recorded diagnosis against practice records in 335 insured Swedish dogs. Acta Vet Scand. 2006; 48(1): p. 8. [7] Nodtvedt A. et al. Incidence of and risk factors for atopic dermatitis in a Swedish population of insured dogs. Vet Rec. 2006; 159(8): p. 241-6. [8] Saridomichelakis MN. et al. Canine atopic dermatitis in Greece: clinical observations and the prevalence of positive intradermal test reactions in 91 spontaneous cases. Vet Immunol Immunopathol. 1999; 69(1): p. 61-73. [9] Sture GH. et al. Canine atopic disease: the prevalence of positive intradermal skin tests at two sites in the north and south of Great Britain. Vet Immunol Immunopathol. 1995; 44(3-4): p. 293-308. [10] Tarpataki N. et al. Prevalence and features of canine atopic dermatitis in Hungary. Acta Vet Hung. 2006; 54(3): p. 353-66. [11] Willemse A, Brom WE vand den. Investigations of the symptomatology and the significance of immediate skin test reactivity in canine atopic dermatitis. Research in Veterinary Sciences. 1983; 34: p. 261-265. [12] Willemse TA. Atopic dermatitis: a review and reconsideration of diagnostic criteria. Journal of Small Animal Practice. 1986; 27: p. 771-778. [13] Carlotti D, Costargent F. Analysis of positive skin tests in 449 dogs with allergic dermatitis. European Journal of Companion Animal Practice. 1994; 4: p. 42-59. [14] Griffin CE, De boer DJ. The ACVD task force on canine atopic dermatitis (XIV): clinical manifestations of canine atopic dermatitis. Vet Immunol Immunopathol. 2001; 81: p. 255-269. [15] Nodtvedt A. et al. The spatial distribution of atopic dermatitis cases in a population of insured Swedish dogs. Prev Vet Med. 2007; 78(3-4): p. 210-22. [16] Picco F. et al. A prospective study on canine atopic dermatitis and food-induced allergic dermatitis in Switzerland. Vet Dermatol. 2008; 19(3): p. 150-5. [17] Favrot C. et al. A prospective study on the clinical features of chronic canine atopic dermatitis and its diagnosis. Veterinary Dermatology. 2009; 20: p. In Press. [18] Scott DW. Obersvations on canine atopic dermatitis. Journal of the American Animal Hospital Association. 1981; 17: p. 89-102. [19] Prélaud P. et al. [Reevaluation of diagnostic criteria of canine atopic dermatitis]. Rev Med Vet. 1998; 149: p. 1057-1064. [20] Williams HC. Diagnostic criteria for atopic dermatitis. Lancet. 1996; 348(9038): p. 1391-2. The big relief! For cats and dogs! The effective approach to allergy in dogs and cats starts with the Artuvetrin® Serum Test; the reliable allergy test that makes the allergen-specific IgE in the serum visible via the Fc region. Based on the outcome of this test, we can provide you with an allergen-specific vaccine: a big relief for allergy patients! The authority on animal allergies T E L . : + 3 1( 0 ) 3 2 0 - 2 6 7 9 0 0 - W W W. A R T U V E T R I N . C O M DERMATOLOGY Feline atopic dermatitis: Clinical signs and diagnosis C. Prost (1) SUMMARY Although feline atopy was first decribed more than 25 years ago, the immunopathogenesis of this disease is still not entirely understood. It is thought to be similar to that of canine atopy .Cats can develop a variety of pruritic skin conditions including self-induced alopecia, cervico-facial pruritus and eosinophilic dermatosis (miliary dermatitis, eosinophilic plaques, eosinophilic granuloma and indolent ulcer). Feline atopy can also present as a respiratory disease similar to human atopic asthma. Establishing a diagnosis of atopy is difficult and requires exclusion of other cutaneous diseases such as flea bite allergy, food hypersensitivity, parasitic diseases and dermatophytosis. Evaluating the allergic status in cats with intradermal allergy testing or in vitro methods remains a challenge. Here is a diagnostic approach for identifying cats with atopic dermatitis. Atopy is a genetic predisposition to develop IgE-mediated allergy to environmental allergens. In cats, atopy usually results in pruritic skin diseases, but there may also be a relationship between atopy and asthma. Feline atopy remains poorly understood, but its immunopathogenesis is thought to be similar to that of canine atopy. Characterization of inflammatory cell infiltration in feline allergic skin diseases showing one or more features (alopecia, eosinophilic plaques or granulomas, papulocrusting lesions) confirm infiltration of activated antigenpresenting cells and T lymphocytes in addition to increased numbers of dermal mast cells. This pattern mimics the dermal inflammation that occurs in the chronic phase of both canine and human atopic dermatitis [1]. In cats with recurrent “miliary” papulo-crusting dermatitis a significant total increase in dermal T-cells numbers was reported. Significantly more IL-4 positive cells were found in lesional and non lesional skin from allergic cats than from healthy controls [2]. Nevertheless, atopic cats do not have significantly higher concentrations of allergen-specific IgE than normal cats [3]. Clinical signs Estimates of the incidence of Feline Atopic Dermatitis (FAD) vary widely. Genetic predilection has not been proved. The strongest evidence to date in support of heritability is the presence of a disease closely resembling atopic dermatitis in three littermates [4]. FAD is associated with several cutaneous reaction patterns. Lesions include self-induced alopecia, cervico-facial dermatoses, miliary dermatitis and feline eosinophilic skin diseases such as feline eosinophilic plaques, feline eosinophilic granuloma and feline indolent ulcer. The age of onset is usually under 3 years of age. A unifying description of expected clinical features is not available for cats. The most consistent clinical feature is chronic recurrent pruritus manifested by scratching, biting and licking. Some cats hide to lick and tend to be secret groomers. Owners are often unable to distinguish pruritus from normal grooming behavior and may deny that the cat traumatizes itself. Pruritus may then need to be deduced clinically via indirect evidence such as trichograms revealing barbered hairs, tufts of hair in the cat’s hiding places, vomiting of hair balls and excess hair in the feces. Self-traumatized areas may be localized or generalized. The face, neck, pinnae, forelegs and ventrum may, as in dogs, be more severely affected. Nevertheless chronic skin changes such as lichenification and hyperpigmentation and secondary skin and ear infections due to bacteria or Malassezia yeasts are less common in atopic cats than in atopic dogs. 1) Christine Post, DVM, DECVD, TUFTS VETS 525 South Street Walpole, MA 02081, USA Email: [email protected] 223 EJCAP - Vol. 19 - Issue 3 December 2009 Eosinophilic plaques in atopic cat with intradermal positive reactions to pollens. Eosinophilic plaques, eosinophilic granuloma, and eosinophilic ulcers are often grouped into what is called the ‘eosinophilic granuloma complex”. This term is not completely accurate, since the only condition histologically consistent with a granulomatous lesion is the eosinophilic granuloma and the etiology of these conditions is not always the same. Eosinophilic dermatoses occur when there is an underlying pruritic condition irrespective of whether the cause is parasitic, allergic (atopy included), or fungal in nature. However, the ulcer and eosinophilic granuloma can be asymptomatic. Miliary dermatitis of the cat is the eosinophilic dermatosis most specific to cats. It is characterized by small crusty papules, more or less erosive or ulcerated. They can be localized (along the back, face and neck) or generalized. Histologically, intercellular edema of the keratinocytes (spongiosis) is observed, with or without epidermal vesiculation ,and eosinophilic exocytosis. Dermal inflammation consists mostly of eosinophils and mast cells. In the most severe cases, marked spongiosis and secondary focal erosions or ulcerations make it difficult to distinguish the lesions of miliary dermatitis from those of eosinophilic plaques [6]. In fact, miliary dermatitis lesions are thought to be precursors of eosinophilic plaques, and both types of lesion can be found concurrently on the same animal. Miliary dermatitis is caused most frequently by allergic reactions, most notably associated Eosinophilic granuloma presenting as nodules and plaques on the head. Severely inflammed eosinophilic plaques in a cat allergic to house dust mites. with flea bite hypersensitivity but also allergy to environmental allergens. Eosinophilic plaques accompanied by severe pruritus are typically localized on the ventral abdomen, medial aspect of thighs, and peri-anal region. They are firm, raised, often ulcerated, and markedly inflamed. Chronic trauma due to constant licking contributes to the development of these plaques. Histologically, severe epidermal and follicular acanthosis, eosinophilic exocytosis , spongiosis , and epidermal and follicular mucinosis are frequently noted. The dermis is densely infiltrated with eosinophils associated with mast cells and a small degree of lympho- plasmacytic inflammation. An allergic reaction (e,g. to 224 Feline atopic dermatitis: Clinical signs and diagnosis- C. Prost Eosinophilic granuloma presenting as painful edema of the paws. Severe facial pruritus with secondary crusts and ulcerations. ectoparasites, food allergens or airborne allergens) is mostly to blame for this type of lesion. • As pododermatitis with ulcerations of the toe pads, interdigital erythema, or edema of the toe pads. • Edema of the lower lip or chin • \Very firm nodules affecting the tongue and/or palate, sometimes ulcerated. Buccal lesions are sometimes accompanied by other signs including malodorous breath, anorexia, dysphagia, or hypersalivation. The eosinophilic granuloma is a clinical entity that occurs very frequently in the cat. The histological appearance of this lesion is pathognomonic for the condition. In the cat, lesions tend to have a cutaneous, muco-cutaneous, or oral location. They typically present in one of the following ways: • As plaques or very firm papules, erythematous and occasionally yellowish, well circumscribed and with a linear distribution. They are located on the caudal thighs, or more rarely on the neck, thorax, or front legs. • As plaques or nodules on the ears These lesions do not initially seem pruritic. Eosinophilic degranulation may lead to the development of small, pinpoint, white or pink spots which cause pruritus and secondary erosion or ulceration due to chronic licking. Face and neck pruritus in an atopic cat. Linear eosinophilic granuloma. 225 EJCAP - Vol. 19 - Issue 3 December 2009 Seasonal bilateral indolent ulcer in a atopic cat. The diverse clinical appearances of the eosinophilic granuloma make it difficult to diagnose, and cutaneous biopsies are often necessary to distinguish the nodular form of eosinophilic granuloma from neoplasia, mycosis, or abscess. Histological H&E staining reveals irregular and granular collagen fibers that suggest a degenerative process. However, studies using special stains such as Gallego’trichrome and Masson’trichrome and electron microscopy have shown that the collagen fibers in eosinophilic granulomas are not degenerate, but covered by granules and products released during eosinophil degranulation that agglutinate around them (= flame figures). It is the poorly soluble proteins released by the eosinophilic granules that cause granulomatous reactions visible in their chronic form as zones surrounded by macrophages and giant cells, often is palisading array. [9]. Seasonal keratitis concomitant with the lip ulcer. of the upper lip apposing the lower canine tooth, just lateral to the philtrum. Lesions are usually solitary and unilateral, sometimes bilateral. They can create a somewhat monstrous appearance to the face. The lesion is bothersome to the affected cat especially as it makes eating difficult, but is not painful. An accompanying lymphadenopathy is sometimes described. The co-existence of an indolent ulcer with plaques or an eosinophilic granuloma suggests that an underlying allergy plays a role in its pathogenesis especially as the lesion often resolves with anti-parasitic therapy, an elimination diet, or immunotherapy. In one study, flea allergy dermatitis was induced in 10 cats both with intermittent and continual flea exposure. Five of the ten cats developed lip ulcers during this study period and all were exposed to fleas at the time of onset [10]. The POWER study identified hereditary transmission of the syndrome in a family of cats that developed lesions spontaneously without associated pathology. A genetic predisposition is therefore likely [11]. The main causes of eosinophilic granulomas are allergic or parasitic, sometimes complicated by secondary bacterial infection. The indolent ulcer is a very common condition, although its pathogenesis is unknown. Lesions are well defined ulcers, with raised firm edges, varying from 2mm-5cm in size. The most common site is the junction of the skin and mucous membrane Extensive alopecia in an atopic cat. 226 Feline atopic dermatitis: Clinical signs and diagnosis- C. Prost Differential diagnosis should include ulcers of infectious origin (bacterial, fungal, or secondary to FeLV), traumatic ulcers, and neoplasia (e.g.carcinoma, mast cell tumors and lymphoma). The chronic indolent ulcer is characterized by a cellular infiltrate consisting of mononuclear cells and neutrophils, dermal fibrosis, and focal necrosis in the deepest areas of the dermis. If the lesion is biopsied in its acute phase, the cellular infiltrate consists mostly of eosinophils and mast cells, macrophages, and neutrophils. However, granulomatous changes are occasionally noted. In some cases, the interstitial and perivascular infiltrate consists of neutrophils and the ulcer is colonized by bacteriae. This is a dermatosis for which therapeutic failures are common and remission is often short lived. All four forms of eosinophilic dermatoses may occur simultaneously or at different times in the same cat. Intradermal skin testing in a cat. the cat is sedated, hair is clipped and skin is marked to visualize the injections dots. believed to involve a type I hypersensitivity to inhaled allergens. In a recent study, 20 cats presented with respiratory signs (recurrent bouts of coughing, wheezing, dyspnea) , radiographic images and bronchial cytology compatible with asthma showed positive reactions on intradermal allergy testing. Avoidance of dried food in 3 cats positive for storage mites or cockroach led a good and lasting remission of clinical signs. Specific immunotherapy was effective in controlling signs in12 cats [13]. ) It is likely than airborne allergens act as starting factors in feline asthma. Feline asthma is another clinical presentation of atopy in cats. Feline self-induced alopecia (= feline symmetrical alopecia) presents as hair loss due to constant excessive licking with no inflammatory lesions. The ventral abdomen is commonly affected but medial and lateral limbs, flanks and lumbosacral region may also be involved. Notable histopathological findings are superficial eosinophilic and mild lymphohistiocytic infiltrate. Differential diagnosis includes psychogenic alopecia. A recent study suggests that psychogenic alopecia is overdiagnosed in cats and that a medical cause (e.g. adverse food reaction or atopy) of pruritus is present in 76 % of feline patients with a presumptive diagnosis of behavior problem [12]. Diagnosis Considering so many diseases with similar signs, it is often difficult to make an accurate clinical diagnosis of atopic dermatitis in cats. The same cutaneous reaction patterns may accompany flea hypersensitivity, adverse food reaction and feline atopy. It is essential to perform a thorough physical examination and obtain a detailed history before proceeding to diagnostic tests and therapeutic trials to rule out differentials and confirm feline atopic dermatitis. The following diagnostic approach is proposed: Cervicofacial pruritus leads to severe inflammatory selfinduced lesions including erosions, ulcers and crusts. The location of the head may be due to the snooping behavior of cats and their tendency for hunting that expose the head to transmissible organisms or offending allergens, the sparseness of hair on the preauricular , dorsal muzzle and pinnae areas or anatomical particularities such as voluminous sebaceous glands on the chin . The lesions appear sometimes very impressive to owners. Atopy may be a cause of face and neck pruritus. Secondary bacterial infections occur more commonly than they are reported ( probably underdiagnosed). 1. First and foremost it is critical to identify the type of lesion present. A biopsy may be necessary for atypical eosinophilic granuloma presentations and for nodular lesions. Cytological evaluation can also be very useful, and may reveal the presence of many eosinophils (confirming the diagnosis of eosinophilic dermatoses) or the presence of bacteria and granulocytes (suggesting pyoderma or even Malassezia dermatitis). Feline asthma is very similar to human asthma. Feline asthma is Miliary dermatitis in an allergic Positive skin tests in an atopic cat. cat, distinct papules. 2. Basic diagnostic tests and therapeutic trials must always be carried out before specific allergy testing for environmental allergens. a. skin scrapings, direct examination of the cerumen and ear cytology are indicated particularly with facial lesions, b. use of Wood’s lamp, direct examination of hair and scale, fungal cultures are systematically performed c. a flea control trial with topical flea products for 1-2 months in affected cats and in other pets living in the same environment should be conducted first. The best choice is an adulticide with effects on egg production and/or larva emergence or an adulticide associated with 227 EJCAP - Vol. 19 - Issue 3 December 2009 Positive skin tests with erythematous papules. Positive skin tests in a white atopic cat, see the erythematous wheals. Stress induces a rise in serum cortisol, corticotropin, and α MSH (melanocyte stimulating hormone), which interferes with the reactivity of the test. As a result, cats should be anesthetized for intra-dermal skin testing in order to limit the stress response. The author recommends that the animal should not be hospitalized beforehand, and that the test should be performed as soon as the cat arrives at the clinic. Cats can be sedated with medetomidine, tiletamine/zolazepam, xylazine hydrochloride or ketamine hydrochloride. an insect growth regulator. The goal is to minimize the number of fleas or at least maintain it below the threshold which triggers an allergic reaction, and to provide long term control of parasitic infestation. Regular application of all products is critical to prevent recurrence. Bimonthly treatment is recommended for diagnostic purposes, and should be continued during the season in which fleas are most abundant. For the remainder of the year even in winter, monthly treatment can be administered. Products containing fipronil, imidacloprid, or selamectin can be used. In the cat, anti-parasitic therapy alone often leads to resolution of signs. However, lesions with a significant inflammatory component such as eosinophilic plaques may require a short course of corticosteroids. In these cases, absence of recurrence following cessation of corticosteroid therapy confirms the importance of anti parasitic therapy. d. elimination diet of 8 weeks duration then. It can be a hydrolyzed protein diet or a home-cooked diet with a novel protein meat source (e.g. horse, lamb, rabbit, pork).A vegetable source is not required in the cat, although many cats seem to enjoy pumpkin. Beef, dairy, fish, eggs, and chicken have been implicated as the most commonly offending food allergens. Preservatives and other additives are also occasionally involved. e. Search for hypersensitivity to environmental allergens Cat skin is finer and tougher than dog skin. Interpretation of intra-dermal testing requires some experience; there is currently a lack of consensus as how to interpret these tests in the cat. Interpretation should take place 15 minutes following injection, with the following signs to be evaluated: presence of erythema, swelling of the injection site, firmness of the swelling, diameter of the swelling, and to some degree the presence of pseudopods. Interpretation occurs ‘with the eye and with the hands’. Subjective comparisons are inevitably made with positive and negative controls. Examination of the reaction sites is made in dim light with an oblique light source to examine the margins of the reaction sites, their size and volume. Erythema in cats with light colored skin is best visualized under normal lighting. When in doubt, reactions should be considered negative. One study suggested the use of liquid fluorescein in 10% saline injected intravenously (5-10 mg/kg) after the last intra-dermal injection to facilitate interpretation of the cutaneous reactions. A Wood’s lamp would then be used after 15-30 minutes to compare the diameter of each reaction to positive and negative controls, with a positive result being a diameter equal to or larger than the average of the positive and negative controls. The intensity of the fluorescence is not a necessary criterion for interpretation of the test. [14]. Allergy testing is reserved for those patients where environmental allergies are strongly suspected. The goal is to identify offending allergens for inclusion in specific immunotherapy. Intra-dermal allergy testing was for a long time the only test available for cats. Skin testing is still considered the “gold standard” in feline allergy medicine. Selection of seasonal allergens to be included in the test is based on geographical location of the cat’s home. Testing with allergen mixtures is not recommended unless strong cross-reactions have been proved (grasses). Intra-dermal skin testing is considered difficult to perform and to interpret in the cat. Diagnostic blood testing in the cat with hypersensitivity has not proved to be very useful. This is because of poor correlation with the results of skin testing, and because feline anti-IgE has questionable specificity in cats. All studies even the most recent ones have failed to demonstrate significant differences in allergen-specific IgE levels in sera from supposed atopic cats and that of normal cats. These studies have concluded that IgE Steroids should be stopped 2 months before skin testing is performed; anti-histamines should be stopped 2 weeks before. 228 Feline atopic dermatitis: Clinical signs and diagnosis- C. Prost References serology should not be used to diagnose feline atopy [15,16]. Direct cat basophil activation test or passive sensitization of human basophils by cat sera can be applied to allergy diagnosis in cats. Tests are based on the measurement of basophil activation or on the release of mediators such as histamine and LTC4 by flow cytometry. In a preliminary study, good clinico-biological correlation was obtained using a basophil activation model in a population of 40 allergic cats [17]. A more recent study adapted this method as a tool for the diagnosis of feline flea bite hypersensitivity on cats experimentally sensitized to fleas [18]. [1] [2] [3] House dust mites are the most commonly incriminated allergens. In a study of 90 cats, Dermatophagoides farinae was positive in 80 % of cases and Dermatophagoides pteronyssinus in 46% of cases. 40 % of cats had one or more positive reactions to pollens [19]. In another study, house dust mites were reported to be common causes of positive intradermal test reactions [8]. [4] [5] [6] In a study on 20 atopic cats with feline asthma, intradermal allergic tests were performed in 18 cats [13]. Three of these were negative even after when tested for a second time. 15 cats had positive reactions to Dermatophagoides farinae (8/15), Acarus siro (6/15), Glyciphagus domesticus (4/15), Dermatophagoides pteronyssinus (4/15), Tyrophagus putrescentiae (4/15), Cockroach (2/15), Ox-eye daisy, ragweed, false acacia (2/15), Hazel-tree, plane-tree (1/15), flea (3/15) Specific immunotherapy was prescribed in 12 cats. [7] [8] [9] [10] [11] In conclusion, it is difficult to make an accurate clinical diagnosis of atopic dermatitis in cats as we lack the major and minor clinical criteria that we have in dogs. The diagnosis of feline atopic dermatitis is based on dermatological clinical signs specific to cats, exclusion of other skin diseases such as flea bite allergy, food hypersensitivity, ectoparasitic infestation and dermatophytosis, and skin test results. Evaluating the allergic status in cats with intradermal allergy testing or in vitro methods remains a challenge. Offending environmental allergens should be identified in order to initiate specific immunotherapy. Working on experimental models of allergic feline asthma might help to improve our understanding of the immunopathogenesis of feline atopy. [12] [13] [14] [15] [16] [17] [18] [19] 229 Taglinger K, Day MJ, Foster AP. Characterization of Inflammatory Cell Infiltration in Feline Allergic Skin Disease. J.Comp. Path. 2007; vol.137: 211-223 Roosje PJ, Thepen T, Rutten VPMG, Van den Brom WE, BruijnzeelKoomen CAFM, Willemse T. Immunophenotyping of the cutaneous cellular infiltrate after atopy patch testing in cats with atopic dermatitis. Vet Immunol Immunopathol 101. 2004; 143-151 Taglinger K, Helps CR, Day MJ, Foster AP. Measurement of serum immunoglobulin E (IgE) specific for house dust mite antigens in normal cats and cats with allergic skin disease. Vet Immunol Immunopathol 105. 2005; 85-93 Moriello KA. Feline Atopy in three littermates. Vet Dermatol. 2001; 12 (3): 177-181 Prost C. Atlas d’allergologie cutanee chez les carnivores domestiques. Editions Med’Com, Paris 2000 Gross TL, Ihrke PJ, Walder EJ, Affolter VK. Feline Eosinophilic Plaque in Skin Diseases of the dog and cat, Clinical and Histopathologic Diagnosis, II Edition, Blackwell. 2005; 109-111 Foster A. Clinical approach to feline eosinophilic granuloma complex. In Practice Jan. 2003; p. 2-9 Foster A. Diagnosing and treating feline atopy. Vet Med March. 2002; pp 226-240 Fondati A, Fondevila D, Ferrer L. Histopathological study of feline eosinophilic dermatoses. Vet Dermatol. 2001; 12: 333-338 Colombine S, et al. Induction of feline flea allergy dermatitis and the incidence and histopathological characteristics of concurrent indolent lip ulcers. Vet Dermatol. 2001; 12: 155-161 Power HT, Irhke PJ. .Selected eosinophilic skin diseases. Vet Clinics of North America. 1995; 25: 833-850 Waisglass SE, Landsberg GM, Yager JA, Hall JA. Underlying medical conditions in cats with presumptive psychogenic alopecia. JAVMA, Vol 228, No.11, June 1, 2006 Prost C. L’asthme felin : apport des tests allergiques et de l’immunotherapie specifique. A propos de 20 cas. Revue Francaise d’Allergologie et d’Immunologie Clinique 48. 2008; 409-413 Schleifer SG, Willemse T. Evaluation of skin test reactivity to environmental allergens in healthy cats and cats with atopic dermatitis. American journal of veterinary Research, 2003; vol 64: 773-778 Bexley J, et al. Levels of house dust mite-specific serum immunoglobulin E (IgE) in different cat populations using a monoclonal based anti-IgE enzyme-linked immunosorbent assay (ELISA). Vet Dermatol, vol 19 supp 1, november 2008; p20 Diesel A., DeBoer D.J – Allergen specific IgE in atopic and healthy cats – comparison of rapid screening immunoassay and completepanel analysis. Proceedings of the 24th North American Veterinary Dermatology Forum, Savannah, April 15-18, 2009; p 208 Prost C. Allergy diagnosis in companion animals: clinical experience with the basophil activation model. Vet Dermatol. 1998; 9: 213215 Stuke K, Monitoring of basophil sensitization to antigens of the cat flea (Ctenocephalides felis felis): a new tool for the diagnosis of feline flea bite hypersensitivity? Parasitol Res. 2008; 103: 807-820 Prost C. Diagnosis of feline allergic disease, a study of 90 cats.in Advances in Veterinary Dermatology, vol 3, C. von Tscharner et al eds, Butterworth Heinemann, Oxford. 1998; 516-517 DERMATOLOGY Food allergy in dogs- clinical signs and diagnosis H. A. Jackson(1) SUMMARY Clinicians have long recognized a dermatitis which appears to be triggered by dietary components. The first descriptions of food induced canine dermatitis date back to 1933 [1,2]. However, although we make a clinical diagnosis of canine “food allergy” it is not clear at this time whether these cases are truly immunologically mediated or due to a “food intolerance” (Tab. 1). Furthermore, although there is evidence of a role for IgE in the pathogenesis of food allergy in colony dogs with spontaneous food allergy [3] it is not clear whether this is representative of the disease in the general population. Thus for the purpose of this discussion, although the term food allergy is used throughout, it should be recognized that this term is a presumptive clinical diagnosis and adverse food reaction is a more accurate term for these canine cases. This paper was commissioned by FECAVA for Other presentations of food allergy are recognized such as a recurrent superficial pyoderma [7,8] and pruritic papular eruptions over the trunk and head (Fig. 4). Recurrent otitis externa is a common complaint and may be present in 56% to 80% of cases [7-11]. Dogs may present with only otitis externa and occasionally this affects a single ear. There is debate over the frequency of concurrent gastrointestinal signs in patients with dermatologic signs of food allergy [5-7,10,11]. In this author’s experience, intermittent vomiting, diarrhoea, colitis, or borborygmus may be present. It has been reported that canine food allergy may respond poorly to antipruritic doses of glucocorticoids, but most clinicians now agree this distinction is not a useful diagnostic feature. Two studies report that the majority of dogs with food allergy present before three years of age (Fig. 5) [5,6]. However, this disorder can occur at any age and should be considered in the older dog with no previous history of pruritus (Figures 6 and 7). Labrador retrievers, West Highland White terriers, boxers, Rhodesian ridgebacks and pugs are reportedly at increased risk for developing food allergy [5,6,10]. publication in EJCAP. Clinical presentation Food allergy in dogs often assumes the clinical presentation that we traditionally associate with canine atopic dermatitis (CAD) triggered by environmental allergens [5,6]. Thus, they present with pruritus and the ventral abdomen, axillae, groin, muzzle, periocular, perianal, and palmar or plantar and dorsal interdigital skin are usually involved (Figures 1-3). Not all body regions are necessarily affected in individual dogs. A primary papular eruption may also be present. Secondary infections with Staphylococci or Malassezia often occur. A history of non-seasonal pruritus is present in the older dog, but a pattern cannot be determined in puppies and young adults with only a few weeks to months of discomfort. Food allergy often coexists with environmental allergies in the same individual, the reported incidence varying from 33-49% of allergic dogs [5-7]. Atopy a genetic predisposition to develop allergic disease Atopic disease any manifestation of atopy i.e. dermatitis, conjunctivitis etc. Atopic dermatitis a genetically predisposed inflammatory and pruritic allergic skin disease with characteristic clinical features. Adverse food reaction any clinically abnormal response attributable to the ingestion of food or food additive Food intolerance abnormal physiological response to food with no immunological basis Food allergy Immunologically mediated adverse food reaction. Tab. 1. 1) Hilary A Jackson BVM&S DVD DipACVD MRCVS, Dermatology Referral Service, 528 Paisley Road West, Glasgow G51 1RN, Scotland 230 EJCAP - Vol. 19 - Issue 3 December 2009 Fig. 1 Chronic facial dermatitis and otitis in a dog with food allergy. Fig. 3 Ventral interdigital erythema and pruritic pododermatitis. Fig. 4 Multifocal alopecia and papules on the trunk of a young dog with food allergy. Fig. 2 Lichenification and erythema of the axilla, limb and sternum of the same dog (Fig. 1). of questions which might be asked to determine what the dog is currently being fed. The optimal duration of a diet trial has not been determined but most veterinary dermatologists recommend a period of six to eight weeks which allows for evaluation of sustained improvement. Additionally, it is often the case that other treatments are instituted along with the initiation of the diet trial such as antibiotic or antifungal therapy for concurrent microbial infections. The diet needs to be continued once this treatment has finished in order to determine whether clinical improvement is sustained or merely attributable to the antimicrobal treatment itself. It is usually easiest to perform the challenge with a small amount of previously fed dog food. Clinical signs generally manifest within 2 weeks of challenge although, in my experience often within 2-48 hours. If the dog does not relapse with “dog food” then other previously fed treats should be introduced one by one. Serological or intradermal testing for Prior to embarking on a diagnostic work up for food allergy the possibility of the presence of other pruritic skin diseases should be entertained. Ectoparasitic infestations in particular should be ruled out. If skin scrapings and coat brushings are negative then a therapeutic trial with a parasiticide is warranted. Diagnosis of food allergy A diagnosis is achieved by documenting a clinical improvement during the course of feeding a novel diet (see below) with recrudescence of clinical signs when previously fed foods are re-introduced. This diet should be fed exclusively and any additional food elements avoided. Table 2 provides an example 231 Food allergy in dogs- clinical signs and diagnosis - H. A. Jackson 1. What is your dog’s current and past dog food? 2. What dog treats does your dog receive? 3. Do you feed your dog table scraps? 4. Does your dog get raw hide chews, pigs ears or anything similar? 5. If you need to give your dog pills do you hide them in food? 6. What does your dog drink? 7. Does your dog have access to the cat food? 8. If there is another dog in the house what does it eat and do the dogs share bowls? 9. Will your dog eat food it finds on the street or in the park? 10.Does anyone else feed your dog ie the neighbour or dog walker? Tab. 2 Diet history. food allergy is not diagnostically reliable at this time and is not to be recommended. Fig. 5 A six month old Labrador with facial pruritus due to food allergy. Pruritus was so intense the dog had been put in an Elizabethan collar. Performing an effective food trial is challenging. It takes time to determine the dog’s current food intake and educate the client about performing a diet trial correctly. It is often the case that the interview is conducted with one family member who embraces the concept and plan but the diet fails because other family members continue to feed treats. It is a good idea to make contact with the owners one or two weeks after initiating the trial to ensure the diet is going to plan and offer moral support. Clients generally find the first week the hardest, particularly of the dog is habituated to a lot of extra treats and table scraps. Fig. 6 A ten year old dog with a 6 month history of ventral pruritus. Food allergy was diagnosed. Before and during the diet trial the dog’s weight should be monitored carefully. Diets designed for the diagnosis and management of food allergy are nutritionally complete but occasionally a rapid gain or loss of weight can be seen. Diet selection Fig. 7 A close up view of the same dog (Fig. 6). Malassezia was demonstrated on cytology from the ventral abdomen. Limited antigen diets in common use fall into three categories: commercially available novel protein diets, hydrolysed protein diets and novel protein home cooked diets. Commercially available diets are generally designed for the management of true food allergy, although as discussed, the true incidence of immunologically mediated disease in the dog is currently unknown. Food allergens have been characterized at the molecular level in man and are generally glycoproteins with a molecular weight greater than 10 000 kD and they are stable to digestive processes [12]. The nature of food allergens in the dog is largely unknown. Home cooked diets are often advocated when performing a diet trial, thus avoiding pet food additives which might have the potential to cause adverse reactions. However, although additives are often incriminated as causing adverse reactions in pets there are no well documented reports to support this 232 EJCAP - Vol. 19 - Issue 3 December 2009 References idea. Furthermore, the use of home cooked diets often lead to poor client compliance due to the added effort required for diet preparation. Home cooked diets are contra-indicated in growing animals and should be nutritionally balanced if used for long term feeding. [1] Burns PW. Allergic reactions in dogs. Journal of the American Veterinary Medical Association. 1933; 83: 627-34. [2] Schnelle GB. Eczema in dogs-an allergy. North American Vet. 1933; 14: 37-44. [3] Jackson HA, Hammerberg B. Evaluation of a spontaneous canine model of immunoglobulin E-mediated food hypersensitivity: dynamic changes in serum and fecal allergen specific IgE values relative to diet change. Comparative medicine. 2002; 52: 316-21. [4] Loeffler A, Lloyd DH, Bond R, Kim JY, Pfeiffer DU. Dietary trials with a commercial chicken hydrolysate diet in sixty three pruritic dogs. Veterinary Record. 2004; 154: 519-22. [5] Jackson HA, Murphy KM, Tater KC, et al. The pattern of allergen hypersensitivity (dietary or environmental) of dogs with nonseasonal atopic dermatitis cannot be differentiated on the basis of historical or clinical information: A prospective evaluation 20032004 (abstract). Vet Dermatol. 2004; 16: 200. [6] Picco F, Zini E, Nett C, Naegeli C, Bigler B, Rufenacht S et al. A prospective study on canine atopic dermatitis and food-induced allergic dermatitis in Switzerland. Vet Dermatol. 2008; 19: 150-155 [7] Chesney CJ. Food sensitivity in the dog: A quantitative study. Journal of Small Animal Practice. 2002; 43: 203-207. [8] Harvey R. Food allergy and dietary intolerance in dogs: a report of 25 cases. J Small Anim Pract. 1993; 34:175-179. [9] Olson M, Hardin JA, Buret A, et al. Hypersensitivity reactions to dietary antigens in atopic dogs. In: Rheinhart GA, Carey DP, eds. Recent advances in canine and feline nutrition, Vol. 3. Wilmington, Ohio: Orange Frazer Press, 2000;69-77. [10] Rosser EJ Jr. Diagnosis of food allergy in dogs. J Am Vet Med Assoc. 1993; 203: 259-262. [11] Carlotti D, Remy I, Prost C. Food allergy in dogs and cats. A review and report of 43 cases. Vet Dermatol. 1990; 1: 55-62. [12] Taylor SL, Lehrer SB. Principles and characteristics of food allergens. Critical Reviews in Food Science and Nutrition. 1996; 36(S): S91-S118. [13] Biourge VC, Fontaine J, Vroom MW. Diagnosis of adverse reactions to food in dogs: efficacy of a soy-isolate hydrolysate based diet. Journal of Nutrition. 2004; 134: 2062S-64S. [14] Rosser ER. Evaluation of a novel carbohydrate and hydrolyzed protein containing diet in previously confirmed food allergic dogs (abstract). Vet Dermatol. 2001; 12: 230. [15] Olivry T, Kurata K, Paps JS et al. A blinded randomized controlled trial evaluation the usefulness of a novel diet (Aminoprotect Care) in dogs with spontaneous food allergy. Journal of Veterinary Medical Science. 2007a; 69: 1025-31. [16] Jackson HA, Jackson MW, Coblentz L et al. Evaluation of the clinical and allergen specific serum immunoglobulin E responses to oral challenge with cornstarch, corn, soy and a soy hydrolysate diet in dogs with spontaneous food allergy. Vet Dermatol. 2003; 14: 181-7. [17] Ricci R., Jackson H.A., Paps J.S., Hammerberg B. The magnitude of the clinical response to oral proteins in dogs with spontaneous chicken allergy is significantly reduced when the protein is hydrolyzed (abstract). Vet Dermatol. 2006; 17: 210. [18] Beale KM and Laflamme DP. Comparison of a hydrolyzed soy protein diet containing corn starch with a positive and negative control diet in corn- or soy-sensitive dogs (abstract). Veterinary Dermatology. 2001; 12: 237. [19] Glos K, Linek M, Loewenstein C, Mayer U, Mueller RS. The efficacy of commercially available veterinary diets recommended for dogs with atopic dermatitis. Vet Dermatol. 2008; 20: 280-7 [20] Bensignor E, Morgan DM, Nuttall T Efficacy of an essential fatty acid-enriched diet in managing canine atopic dermatitis: a randomized, single-blinded, cross-over study. Vet Dermatol. 2008; 19; 156-62 Commercial novel protein diets contain whole proteins which are not commonly found in dog foods. Although a truly “novel” protein is becoming more difficult to find as the diets available for general consumption increasingly contain more varied and exotic ingredients. The diet should be selected on the basis of the protein content which should be one which has not routinely been fed to the pet in the past, and ideally not at all. Hydrolysed diets theoretically negate the need to find a “novel” protein. The Parent protein in these diets is usually from a readily available source such as chicken or soy in which the peptide bonds of the parent protein have been broken to create small peptide fragments. These peptides are too small to bridge adjacent allergen specific IgE molecules on the surface of mast cells thus degranulation does not occur. The rationale behind the use of these diets assumes that canine food allergy is mediated by IgE, which as previously discussed has not been determined. Various studies have examined the performance of hydrolysed diets in a clinical setting and found them to be well tolerated [5,13-15]. There is less critical evaluation however on the performance of these diets in dogs known to be hypersensitive to the parent protein. A small number of studies suggest that 20-50% of individuals will react adversely to the hydrolysed diet if they are sensitive to the parent protein [16-18]. Furthermore these diets tend to be more costly and less palatable. For optimal compliance the selected diet should be of similar consistency to the diet currently being fed. Thus, if the dog is on a mixture of dry and moist food this should be adhered to if at all possible. Long term management of the food allergic dog For long term management the dog with food allergy may be maintained on the limited antigen diet which was used in the diet trial. Alternatively, and if the offending allergens have been identified, an alternative diet which is “allergen” free for that dog can be utilized. In the author’s experience some dogs with food allergy can develop a hypersensitivity to the new diet after months to years on this diet and under such circumstances a new diet needs to be found. Young dogs may also progress to develop concurrent hypersensitivities to environmental allergens. Dietary responsive disease Various studies have demonstrated an apparent beneficial effect of feeding limited antigen diets to dogs with AD in the absence of demonstrable food allergy [19,20]. This precise reason is undetermined but may be attributable to the enhanced essential fatty acid content of these diets. 233 DERMATOLOGY Food hypersensitivity in the cat E. Guaguère1, P. Prélaud2 SUMMARY The term food hypersensitivity refers to all the clinical manifestations of allergy to ingested allergens (immunological mechanisms), and intolerance (non-immunological mechanisms). Few studies of the immunopathogenesis of feline food allergy have been conducted so most immunological data are extrapolated from the human field. The list of incriminated foods varies according to local feeding habits in countries where the animals live. In cats, the most common food allergens are beef, lamb, milk, fish, tinned food and dried food. Food hypersensitivity often manifests in cats as a pruritic dermatosis of the face and neck, miliary dermatitis, self-induced alopecia and generalised scaling or symmetrical alopecia. In addition to the other clinical presentations, all the entities of the eosinophilic granuloma complex should be considered. The incidence of gastrointestinal involvement is underestimated. Most cases of recurrent lymphoplasmacytic colitis seem to be related to food hypersensitivity. In practice, establishing a definitive diagnosis can be difficult and requires a rigorous approach. An elimination diet of one or more foodstuffs, never previously eaten by the cat, should be fedover six to ten weeks, period considered optimal by most dermatologists. Introduction was not routinely undertaken. Food hypersensitivity represents the third most important cause of feline hypersensitivity [5, 11, 12, 26, 35]. The term food hypersensitivity refers to all the clinical manifestations of allergy to ingested allergens (immunological mechanisms), and intolerance (non-immunological mechanisms). However, in the vast majority of cases, neither identification of the actual allergen responsible nor elucidation of the exact immunological mechanisms involved is possible so it may be wiser to use the term food intolerance [11, 12, 14, 27, 31, 35, 39]. Moreover, certain kinds of clinical problem may be associated with the ingestion of foodstuffs but without any evidence of any causal immunological reaction : food can contain pharmacologically active substances (e.g. histamine which induces vasodilatation) [19]; metabolic reactions due to some kind of enzyme deficiency (e.g. lactase) are common ; and both fungal toxins (in dried, poorly prepared or inadequately preserved food) and plant toxins (e.g. tannins and alkaloids) can elicit non-immunological reactions [11]. Aetiopathogenesis Few studies of the immunopathogenesis of feline food allergy have been conducted so most immunological data are extrapolated from the human field. Food allergens Any foodstuff is potentially allergenic but, in practice, a finite number of ingredients are involved [2, 5, 10, 17, 27, 36, 38, 39]. The actual list varies according to local feeding habits in countries where the animals live. In cats, the most common food allergens are beef, lamb, milk, fish, tinned food and dried food. Less commonly, chicken, gluten and additives can also induce reactions. The incidence of food intolerance in cats is difficult to establish with any precision because it depends on both the definition of food intolerance and to what extent the possibility of food intolerance is considered in the diagnosis. The reported prevalence of food hypersensitivity varies from 1% to 11% of all feline dermatoses [31,36]. In a recent study [5], 6% of all dermatoses in cats were attributed to food intolerance but this figure cannot be taken as definitive because challenge testing The foodstuffs most likely to be allergenic are those which contain the most protein and those which are most commonly fed. The cat will often have been eating the foodstuff in question for a long time [2, 5, 10, 17, 27, 36, 38, 39] and the more a particular protein has been consumed, the more likely it is to induce hypersensitivity [12, 35]. The exact nature of allergenic proteins in cats has never been studied. (1) Eric Guaguère, Doct Vét, Dip ECVD, DESV D, Clinique Vétérinaire Saint Bernard, 598 avenue de Dunkerque, F 59160 Lomme, France (2) Pascal Prélaud, Doct Vét, Dip ECVD, DESV D, Clinique Vétérinaire Advetia, 5 rue Dubrunfaut. F 75012 Paris, France 234 EJCAP - Vol. 19 - Issue 3 December 2009 Fig. 1 Facial pruritus and erythema on the lateral pinnae of a cat with food allergy. Fig. 2 Same cat as in Figure 1, erythema on the lateral pinnae. It is likely that many foodstuffs are also responsible for nonimmunologically based intolerance. Certain fish contain high levels of histamine, e.g. tuna and any dried or inadequately preserved fish. Shellfish – common allergens in humans – have not often been identified as allergens in cats even though they are a common ingredient in “cat treats”. Nevertheless, prawns may induce non-specific histamine release [11, 19]. allergy is probably a Type I immediate hypersensitivity although Type III (Arthus) reactions and Type IV (delayed) hypersensitivity may also occur [5, 12, 14, 27, 31, 35, 36]. Immediate responses appear within minutes or hours of ingestion of the allergen whereas delayed responses take several hours or days. Defence mechanisms to prevent development of food allergy include the protective gastrointestinal mucosa and immune tolerance maintained by cellular immunity associated with the digestive tract [6, 17, 30]. The mucosal barrier excludes most ingested allergens although it is permeable to peptides and small proteins, especially if there is any kind of inflammation, e.g. due to viral or parasitic infection [8]. Although no exact mechanisms have been demonstrated in cats, it is assumed that local and systemic IgA eliminates potential allergens and that any defect in this defence would predispose an animal to potentially damaging hypersensitivity reactions. Food allergy can develop along with other kinds of allergy, e.g. flea allergy dermatitis, atopic dermatitis, etc. [8,19,20]. Most of the commonly suspected additives are haptens (small molecules which are allergenic only when conjugated with a carrier protein), and hypersensitivity to this type of antigen has never been demonstrated in cats. Many of the additives used in the human food industry, like benzoates and tartrazine, are never used in cat food. However, the use of others is widespread, including sodium bisulphite, monosodium glutamate, azodyes, sodium nitrite, spices, sodium alginate, vegetable gums, propylene glycol and ethoxyquin [28]. Storage (forage) mites in commercial, dried cat food could be a major source of oral sensitisation for carnivorous animals [13]. In dogs, allergy to storage mites is common although in cats it has never been possible to demonstrate that the sensitivity is specific to forage mites and not due to cross-reaction with house dust mites or mites present in food. Clinical features Food allergy is a non-seasonal dermatosis with no age, breed or sex predilection. Age of onset varies between 3 months and 11 years with most studies showing a mean age of 4 to 5 years [2, 10, 26, 33, 38]. There is no breed predilection although two different studies have shown a higher incidence in Siamese and Immune response The most common immunological response involved in food Fig. 4 Facial pruritus, erythema, scaling and crusting in a Persian cat with food allergy. Fig. 3 Same cat as in Figures 1-2, lesions of miliary dermatitis. 235 Food hypersensitivity in the cat - E. Guaguère Fig. 5 Erosions around the skin behind the ears in a cat with food allergy. Fig. 6 Same cat as in Figure 5, blepharoconjunctivitis. Burmese cats [12, 32, 35]. It is usually believed that food allergy is more common in cats than in dogs although it is impossible to carry out meaningful epidemiological studies because allergic dermatitis is poorly defined and the means of investigating feline allergies are limited [12]. As it is easier to carry out an elimination diet and control flea allergy dermatitis in the cat than it is to perform intradermal allergy testing, food allergy is usually considered the most likely differential in this species (unlike in the dog) after flea allergy dermatitis [12]. otitis, pododermatitis and perianal inflammation are sometimes observed (Figs 10, 11). Food hypersensitivity can also present as miliary dermatitis (Fig. 12), self-induced alopecia and generalised scaling or symmetrical alopecia (Figs 13,14), each of which carries a detailed differential diagnosis. In addition to the other clinical presentations, all the entities of the eosinophilic granuloma complex should be considered, e.g. indolent lip ulcers (Fig. 15) and eosinophilic plaques, wherever they occur [24]. Urticaria and secondary bacterial or fungal infections (e.g. Malassezia dermatitis) seem to be relatively rare in cats [10, 31, 32]. Dermatological signs Clinical signs are not specific although varying degrees of nonseasonal pruritus (either generalised or localised) have been reported in over 90% of cases [2,10,16,18, 26,38]. Response to glucocorticosteroid therapy was good in almost 50% of cases [10]. In some studies, glucocorticosteroids have been found to be less effective although these were either retrospective studies of chronic cases or studies that involved doses similar to those used in dogs [2, 26, 32, 33, 38, 39]. Gastrointestinal signs The incidence of gastrointestinal involvement, which may or may not be associated with dermatological signs, is underestimated. In a series of 17 cases [10], gastrointestinal involvement (e.g. vomiting and intermittent diarrhoea) was observed in 30% of the animals. Most cases of recurrent lymphoplasmacytic colitis, common in cats, seem to be related to food hypersensitivity in this species [6, 17, 22]. In one case, food hypersensitivity mimicked alimentary lymphoma [37]. Food hypersensitivity is characterised by a clinical polymorphism [2, 4, 5, 10-12, 14, 18, 26, 27, 31-33, 35, 38, 39]. It often manifests in cats as a pruritic dermatosis of the face (cheilitis and bilateral blepharitis) and neck with erythema, papules, erosions and crusts (Figs 1-9). Bilateral erythemato-ceruminous Diagnosis In practice, establishing a definitive diagnosis can be difficult and requires a rigorous approach. The animal’s history must Fig. 7 Severe facial pruritus and very crusty lesions in a Persian cat with food allergy (sardines). Fig. 8 Same cat as in Figure 7 seen after clipping, showing severe erosive and ulcerative lesions on the face. 236 EJCAP - Vol. 19 - Issue 3 December 2009 Fig. 9 Erosions, excoriations and facial pruritus in a domestic short-haired cat with food allergy (beef). Fig. 10 Same cat as in Figure 9, erythematous pododermatitis. be thoroughly reviewed, including the cat’s living and eating habits, and the diet itself, especially with respect to protein and carbohydrate sources. The physical examination should be methodical. Food hypersensitivity should always be considered in an animal with a non-parasitic pruritic dermatosis [12, 31, 32]. Certain preliminary guidelines are important: the food must be offered on a plate (avoid plastic or metal), toys should be taken away and, in theory, no treats, vitamins, mineral supplements or drugs should be given during the time of the diet [10,12, 25, 27, 31-33, 35, 39]. Prescribing glucocorticosteroids, antihistamines or cyclosporine A cannot always be avoided. In cases, the special diet can be started immediately but, for proper assessment of its effect, it should be prolonged for at least two weeks following the end of the drug course [12, 31, 32]. If pills must be given with food, all protein sources, including butter, cheese, ice cream, meat and animal treats must be avoided. Honey is preferable [25]. Differential diagnosis The differential diagnosis is that of all pruritic dermatoses, including initially the ectoparasitic infestations (e.g. cheyletiellosis, notoedric mange, trombiculiasis and pediculosis), other causes of allergic dermatitis and dermatophytosis [5,12, 27, 31, 32, 33, 35, 39]. Facial involvement requires a more detailed diagnostic approach to rule out auto-immune dermatoses, mural lymphocytic folliculitis and certain viral infections [5,12, 27, 31, 32, 33, 35, 39]. Selecting an elimination diet Protein ln an elimination diet, protein must be restricted to sources never previously eaten by the animal. Duck, horse, lamb and white fish are often appropriate [12, 14, 27, 29-33, 35, 38, 39]. Hydrolysed proteins are low in molecular weight and allergenicity, highly digestible and can be used whatever their origin. Most hydrolysed diets are poultry- or soya-based [3]. None of the industrial foods on the market has a sufficient amount of hydrolysed proteins to guarantee a complete absence of allergens (on average, molecular weight of 12 kd). In fact, in order to guarantee the absence of allergens, it would be necessary for hydrolysed proteins to contain peptides at a maximum level of 1 to 3 kd. This would lead to the cost of hydrolysis and ultrafiltration becoming excessive. It is reasonable to choose an industrial diet that does not contain any protein sources to which the cat may be sensitive. In general, diets containing hydrolysed proteins are effective and well-tolerated [3, 25]. Diagnostic tests Haematological profiles (differential count, etc.) are worthless; at best they might reveal non-diagnostic eosinophilia. Histopathological examination of skin biopsies does not provide any specific information, but usually reveals perivascular inflammation with varying numbers of eosinophils and mast cells, indicating allergic dermatitis in general [9, 10, 12, 31, 32]. In rare cases, histopathological features include a mural lymphocytic folliculitis [4, 9]. Dietary history Elimination diets The next stage is to instigate an elimination diet of one or more foodstuffs which the cat has never previously eaten. Although this sounds simple, in practice it can be fraught with problems. This is partly because commercial cat foods nowadays contain a wide variety of different proteins and partly because owners often find it difficult to make their cat follow a strict diet; prior to settling on a diet, it is crucial to assess the owner’s motivation [12]. Home-prepared diets Home-prepared diets should include just one source of protein and one source of carbohydrate. The choice of foodstuffs should take into account the cat’s normal eating habits. The choice of diet needs to be a joint decision, taken with the owner, and the cat’s eating habits should not be changed too rapidly [12]. The new diet should therefore be introduced gradually, over the course of 4 to 5 days. It should also be given at the same times and correspond to about the same total amount of food Before the effects of an elimination diet can be properly evaluated, all secondary and concomitant skin conditions must be controlled, e.g. flea allergy dermatitis and secondary infections (although these are rare in cats). 237 Food hypersensitivity in the cat - E. Guaguère Fig. 11 Same cat as in Figures 9-10, perianal erythema. Fig. 12 Severe miliary dermatitis in a domestic short-haired cat with food allergy (beef). as given previously. It must include a relatively lean protein source (lamb, chicken, turkey, horse, duck, rabbit or game), offered either cooked or raw, together with boiled vegetables (potatoes, tomatoes, lentils, banana, pumpkin, etc.). The advantage of these diets lies with the owner having control over all basic ingredients. For cats used to home-prepared diets, they are often more palatable than commercial dry diets (Tab. 1) [12, 25, 31-32, 39]. The advantage of commercial diets is their ease of use (Tab. 2). However, this should not lead the owner to underestimate the difficulties of sticking to such a diet. A commercial diet should be fed as strictly as a home-prepared diet in relation to amount and timing of feeding, preventing other foods being eaten, checking for gastrointestinal side-effects and monitoring the animal’s weight [25]. Tab. 1 Examples of protein and carbohydrate sources in a home-prepared diet [25]. Tab. 2 Advantages and disadvantages of home-prepared and commercial diets [25]. Protein Carbohydrate - Advantages: Rice White fish Maize Advantages: Duck Tapioca (cassava) Owner becomes involved Practical Chicken Potato No additives Turkey Lentils Well-balanced, highly digestible Game Sweet potato Control over protein sources Low allergenicity / hydrolysed Lamb Banana Diversity of protein sources Palatability Rabbit Pumpkin Efficacy Palatability Commercial diets There are a multitude of commercial diets marketed as hypoallergenic or for skin allergies [14, 16, 28-33, 35, 39]. These diets fit into three categories: - Commercial Horse Ostrich - Home-prepared protein coming mostly from specific sources. These diets cannot be considered suitable as elimination diets as the protein source is too varied. protein coming entirely from specific sources (e.g. ostrich, kangaroo, catfish, rabbit and duck). These diets are suitable but may contain hidden traces of food allergens. hydrolysed protein. These diets are theoretically less likely to be allergenic than non-hydrolysed diets. Hydrolysis reduces protein into small, low molecular weight peptides. Hydrolysed diets are therefore the most practical commercial preparations [3, 25, 35]. Hydrolysis effectively reduces the molecular weight and intrinsic antigenicity of the food and also makes it more digestible. These two factors combine to provide low stimulation to the gastrointestinal immune system [3, 25, 35]. Disadvantages: Disadvantages: Preparation time consuming No control over protein sources Often too rich in protein Additives Need to balance the diet for growing cats Large range of foods Side-effects Cost Palatability Palatability Monitoring The patient must be monitored to ensure good compliance. Potential side-effects such as weight loss / gain and gastrointestinal problems, or practical difficulties such as refusing to eat or behavioural changes can also be spotted. To reduce the likelihood of gastrointestinal problems, the elimination diet should be introduced gradually, over at least 4 days, alongside the familiar diet. If the cat loses weight, the diet must be adjusted (for example, protein intake increased) [12]. 238 EJCAP - Vol. 19 - Issue 3 December 2009 Fig. 14 Self-induced alopecia on the abdomen of a domestic shorthaired cat with food allergy. Fig. 13 Generalised scaling dermatitis (mural lymphocytic folliculitis) associated with eosinophilic plaques in a domestic short-haired cat with food allergy (beef). Challenge tests The principle of the challenge test is to reintroduce, at regular intervals, each of the foodstuffs for a period of one week and monitor for reappearance of signs. This is a demanding process which is often rejected by the owner, does not absolutely prove that any particular foodstuff is responsible, and gives no information on mechanisms. However, this approach can be useful because few allergens tend to be involved; just one or two account for over 90% of cases [2, 10, 27, 38, 39]. The vast majority of cats do not relapse when an incriminated foodstuff is reintroduced. This may be due to a change in the immune response with time or, more likely, because eating very digestible food for a while gives the intestine time to re-establish normal permeability. Length of diet Six to eight weeks is considered optimal by most dermatologists. A response can be observed by the end of the third week (Figs 16, 17) but it may take up to 10 weeks for the diet to have any effect [2, 10, 12, 26, 27, 35, 38, 39]. If no response is observed with a hypoallergenic commercial diet, it does not necessarily mean that the cat does not have any kind of food allergy. In this case, a traditional elimination diet should be instigated [30]. If only a partial response is observed, there may be other, concomitant skin problems (and it should be checked with the owner that the diet was rigorously followed). If no response is seen within 10 weeks, the diagnosis should be reviewed. Feeding a cat commercial food ensures a balanced diet – a recent study on hypoallergenic diets prescribed by American vets revealed that 90% failed to provide the officially recommended daily intakes for adult animals [28]. Allergy tests Allergenic extracts derived from food allergens Commercially available extracts of animal-derived food allergens (e.g. beef, milk, fish and eggs) are of very variable allergenicity but give satisfactory results in humans. In contrast, studies in humans have shown that extracts of plant-derived food allergens need to be native and prepared immediately before use; laboratory preparations are inactive [30]. However, it has never been possible to extrapolate these findings to cats. There are no published data on what concentrations of these extracts should be used in cats. One study investigated the use of two different brands of hypoallergenic product with non-hydrolysed proteins, sold in cans (chicken/rice) and in containers (lamb/rice) for cats with food allergy [16]. Of 20 cats included in the study, 8 experienced relapses with the lamb/rice diet (40%) and 13 cats had relapses with the chicken/ rice diet (65%). On the other hand, only 3 of the cats experienced relapses while exposed to the two diets at the same time (15%). Home-prepared diets seem superior to commercial wet food diets, deemed hypoallergenic through diagnostic tests [16]. Fig. 16 Same cat as in Figure 15, erosions and ulcerations on upper and lower lips. Fig. 15 Indolent ulcer on the upper lip of a domestic short-haired cat with food allergy (milk). 239 Food hypersensitivity in the cat - E. Guaguère mg/kg dexamethasone BID) are effective especially in the early stages [12, 31, 32]. Antihistamines are ineffective. Some reports have recommended chlorpheniramine (4-8 mg/animal BID, orally) [12, 32]. Cyclosporine A (5 mg/kg SID) can be also used for controlling pruritus and cutaneous lesions associated with food allergy [23, 34]. Treating secondary infections Secondary skin infections are rare but, in cats with gastrointestinal signs, it is important to control bacteria in the small intestine by prescribing a suitable antibiotic (e.g. metronidazole). The aim of this is to break the vicious cycle of sensitisation followed by the aggravation of gastrointestinal lesions leading to exacerbated dermatological signs [11]. Fig. 17 Same cat as in Figures 15-16, 3 weeks after starting an elimination diet. References Diagnostic value of intradermal testing and in vitro IgE testing Intradermal skin testing [1, 15], in vitro IgE testing [21] and cellular testing have no value in the diagnosis of food allergy in cats. A particular foodstuff cannot be excluded on the basis of a negative result and asymptomatic sensitisation is common [11]. These tests are theoretically useful in human medicine because they are helpful in establishing a more acceptable elimination diet, i.e. a more varied diet can be prescribed once certain important potential food allergens have been eliminated. Even so, opinions are divided on this approach which could get it seriously wrong [7]. It has been stated that “an elimination diet should always be well-constructed and never put together on the basis of a few misleading positive in vitro test results”. [1] [2] [3] [4] [5] [6] [7] In veterinary medicine, such an approach is definitely worthless because we can impose as strict a diet as necessary for a period of weeks without any serious problem. Nevertheless, this has not stopped certain companies from promoting food allergenspecific IgE assays to diagnose food allergy. This commerciallyappealing approach often goes down well with owners. Whatever the outcome, the change in diet is often associated with clinical improvement, if only because the new diet is more balanced or more digestible than the former one. In this way, food intolerance can be misdiagnosed as food allergy [12]. [8] [9] [10] Treatment [11] Hypoallergenic diets The only acceptable, effective way of treating food intolerance is by eliminating the foodstuff(s) responsible. However, this must not adversely affect the nutritional balance of the diet. [12] [13] Hypoallergenic diets cannot be prolonged for more than 3 weeks without risking skeletal damage [29], unless vitamin and mineral supplements are included. Therefore, owners can either feed their animals a balanced home-prepared diet based on the hypoallergenic diet used in the diagnosis, or give very digestible commercial products [16,25]. [14] [15] [16] Symptomatic therapy Corticosteroids (1-2 mg/kg prednisolone SID, orally, 0.2 to 0. 5 [17] 240 AUGUST JR. The reactions of canine skin to the intra-dermal injection of allergic extracts. J Am Anim Hosp Ass. 1982; 18: 157163. CARLOTTI DN, REMY I, PROST C. Food allergy in dogs and cats: a review and report of 43 cases. Vet Dermatol. 1990; 1: 55-62. CAVE NJ. Hydrolyzed protein diets for dogs and cats. Vet Clin Small Anim Pract. 2006; 36: 1251-1268. DECLERCQ J. A case of diet-related lymphocytic mural folliculitis in a cat. Vet Dermatol. 2000; 11: 75–80. DENIS S, PARADIS M. L’allergie alimentaire chez le chien et le chat. II : étude rétrospective. Le Médecin Vétérinaire du Québec. 1994; 24: 15-20. DENNIS JS. Lymphocytic/plasmacytic colitis in cats; 14 cases (1985-1990). J Am Vet Med Ass. 1993; 202: 313-318. DUTAU G, FRANCE F, JUCHET A, FEJJI S, NOUIIHAN P, BREMONT F. De l’eczéma atopique à l’asthme et à l’allergie. Rev Fr Allergol. 1985; 35: 429-439. GILBERT S, HALLIWELL REW. The effects of endoparasitism and of the administration of viral vaccines on the immune reponse to orally administered antigen in cats: possible implications for the pathogenesis of food hypersensitivity. Proc. AAVD-ACVD, San Antonio. 1998: 105-106. GROSS TL, IHRKE PJ, WALDER EJ, AFFOLTER VK. Skin Diseases of the dog and cat: clinical and histopathologic diagnosis. second edition, Editions Blackwell Publishing Company. 2005; pp 932. GUAGUERE E. Intolérance alimentaire à manifestations cutanées: à propos de 17 cas chez le chat. Prat Méd Chir Anim Comp. 1993; 28: 451-460. GUAGUERE E, PRELAUD P. Les intolérances alimentaires. Prat Méd Chir Anim Comp. 1998; 33: 389-407. GUAGUERE E, PRELAUD P Food Intolerance In Practical Guide of Feline Dermatology (Eds Guaguère E, Prélaud P) Editions Merial. 1999; 11.1-11.17. KAMPHUES J. Mites infestation of feedstuffs for small companion animals. J Nutr. 1991; 121: S165. KENNIS RA. Food Allergies: Update of pathogenesis, diagnoses, and management. Vet Clin Small Anim Pract. 2006; 36: 175184. KUNKLE GA, HORNER S. Validity of testing for diagnosis of food allergy in dogs. J Am Vet Med Ass. 1992; 200: 677-680. LEISTRA M, WILLEMSE T. Double-blind evaluation of two commercial hypoallergenic diets in cats with adverse food reactions. J Feline Med Surg. 2002; 4: 185-188. MARKWELL PJ, GUILFORD WG, JONES BR, HARTE JG, WILLS EJCAP - Vol. 19 - Issue 3 December 2009 [18] [19] [20] [21] [22] [23] [24] [25] [26] [27] [28] [29] ROUDEBUSH P, MCKEEVER P. Evaluation of a commercial canned lamb and rice diet for the management of cutaneous adverse reactions to foods in cats. Vet Dermatol. 1993; 4: 1-4. [30] ROUDEBUSH P, GROSS KL, LOWRY SR. Protein characteristics of commercial canine and feline hypoallergenic diets. Vet Dermatol. 1994; 5: 69-74. [31] SCOTT DW. Feline dermatology (1983-1985): the secret sits. J Am Anim Hosp Ass. 1987; 23: 255-274. [32] SCOTT DW, MILLER WH, GRIFFIN CE. Muller & Kirk’s Small Animal Dermatology, 6th edition, Saunders, W.B., Philadelphia. 2000; pp 1528. [33] STOGDALE L, BOMZOM L, VAN DEN BERG P. Food allergy in cats. J Am Anim Hosp Ass. 1982; 18: 188-194. [34] VERCELLI A, RAVIRI B, CORNEGLIANI L. The use of oral cyclosporin to treat feline dermatoses: a retrospective analysis of 23 cases. Vet Dermatol. 2006; 17: 201-206. [35] VERLINDEN A, HESTA M, MILLET S. Food allergy in dogs and cats: A review. Critical Reviews in Food Science and Nutrition. 2006; 46: 259-273. [36] WALTON GS. Skin responses in the dog and cat to ingested allergens. Vet Rec. 1967; 81: 709-713. [37] WASMER ML. Food intolerance mimicking alimentary lymphosarcoma. J Am Anim Hosp Ass. 1995; 31: 463-466. [38] WHITE SD, SEQUOIA D. Food hypersensitivity in cats: 14 cases (1982-1987). J Am Vet Med Ass. 1989; 194: 692-695. [39] WILLIS JM. Diagnosis and managing food sensitivity in cats. Vet Med. 1992; 87: 884-892. J. Prevalence of food sensitivity in cats with chronic pruritus, vomiting, or diarrhea in Advances in Veterinary Dermatology vol. 3 (eds Kwochka, K.W., Willemse, - T. & von Tscharner, C.), Butterworth & Heinemann Oxford. 1998; 493. MEDLEAU L, LATIMER KS, DUNCAN JR. Food hypersensitivity in a cat. J Am Vet Med Ass. 1986; 189: 692-693. MONERET-VAUTRIN DA. Allergies alimentaires et fausses allergies alimentaires in Allergologie. vol. 3 (eds Charpin, J. & Vervloet, D.), Flammarion Médecine Sciences, Paris. 1992; 349-365. MONERET-VAUTRIN DA, KANNY G, RANCE F, DUTAU G. Dermatite atopique et allergie alimentaire. Rev Fr Allergol. 1996; 36: 239-244. MUELLER RS, TSOHALIS J. Evaluation of serum allergen specific IgE for the diagnosis of food adverse reaction in the dog. Vet Dermatol. 1998; 9: 167-171. NELSON RW, DIMPERIO ME, LONG GG. Lymphocytic-plasmacytic colitis in the cat. J Am Vet Med Ass. 1984; 184: 1133-1135. NOLI C, SCARAMPELLA F. Prospective open pilot study on the use of ciclosporin for feline allergic skin disease. J Small Anim Pract. 2006; 47: 434-438. POWER HT, IHRKE PJ. Selected feline eosinophilic skin diseases (eosinophilic granuloma complex). Vet Clin Small Anim Pract. 1995; 25: 833-850. PRELAUD P, POWER HT. Atopic dermatitis syndrome. In Practical Guide of Canine Dermatology (Eds Guaguère E, Prélaud P ; Craig M), Editions Merial. 2008; 229-252. ROSSER EJ. Food allergy in the cat: A prospective study of 13 cats. in Advances in Veterinary Dermatology. vol. 2 (eds Ihrke, P.J., Mason, I. & White, S.D.), Pergamon, Oxford. 1993; 33-39. ROSSER EJ. Food allergy In dogs and cats: A review. Vet Allergy Clin Immunol. 1998; 6: 21-24. ROUDEBUSH P, COWELL CS. Results of a hypoallergenic diet survey of veterinarians in North America with a nutritional evaluation of homemade diet prescriptions. Vet Dermatol. 1992; 3: 23-28. 241 DERMATOLOGY Flea allergy in dogs: Clinical signs and diagnosis C. Laffort-Dassot(1) SUMMARY Flea allergy is a very common pruritic dermatological condition in the dog. This dermatitis occurs in young adult dogs of any sex. Certain breeds may be predisposed. Clinical signs are usually more severe during the warm season. They are characterised by a pruritic erythematous papular eruption affecting the caudal aspect of the dog. Dorsolumbar pruritus and lesions are characteristic diagnostic criteria. With time, lichenification, hyperpigmentation, scaling and crusts appear gradually. Recurrent pyotraumatic dermatitis in the dorsolumbar area, and fibropruritic nodules and crusted papules in the umbilical area may be particularly suggestive of flea allergy dermatitis. Secondary infections are common. Demonstration of fleas or their feces can be difficult because flea allergic dogs remove them from their hair coat during excessive grooming. A flea comb can greatly improve this examination but a negative search should not rule out this hypothesis. Whatever the test used (live flea challenge, intradermal skin testing with flea extracts, in vitro serological or cellular test) allergy testing is controversial in the diagnosis of flea allergy dermatitis because of its poor reliability. Although not perfect, a clinical approach combining thorough history and physical examination, elimination of other differentials and response to strict anti-flea treatment is adopted by most authors. sensitisation introduced many veterinary practitioners and dermatologists to dermato-allergology [2] and for decades, a positive reaction with this test was required to make a definitive diagnosis of flea allergy dermatitis [3]. This paper was commissioned by FECAVA for publication in EJCAP. Introduction Historical findings Flea allergy dermatitis (FAD) is one of the most common small animal dermatological conditions and probably the most common pruritic dermatosis in these species. This is particularly true in areas of the world where fleas are endemic, i.e. where fleas find the optimal environment in which to proliferate: lowaltitude geographical location, a temperature of approximately 23°C and a relative humidity of 78% [1]. Frequently, clinical signs associated with flea infestation are mild with low to moderate pruritus, the intensity of which is directly correlated to flea burden. Simple infestation is not associated with hypersensitivity reactions. On the other hand, in flea allergy dermatitis, clinical signs and pruritus are not related to the parasitic load and may be extremely severe. Suggestive historical and clinical data sustain the diagnosis of flea allergy dermatitis. In the 1980’s, intradermal skin testing with flea extracts documenting Suggestive historical data include the presence and/or recurrence of a pruritic dorsolumbar dermatitis in young adult dogs. FAD can occur in animals of any age although clinical signs rarely develop in animals under 6 months of age [4]. The most common age of onset is 3 to 5 years [3]. There is no sex or breed predilection although one study showed a breed predisposition in ChowChows, Labrit, Pyrenean Shepherd dogs, Setters, Fox-terriers, Pekinese and Spaniels [5]. Pruritus may or may not be seasonal, depending on the geographical location and climate. Even when pruritus is yearround, clinical signs are usually more severe during the warm season. Owners may report onset or increase in pruritus following the introduction of a new pet, or visit to a boarding or grooming facility [6]. 1) Catherine Laffort-Dassot, Clinique Vétérinaire Alliance – 8 Boulevard Godard – F-33000 Bordeaux. Tel: +33(0)556391548, fax: +33(0)556699089 Email: [email protected] 242 EJCAP - Vol. 19 - Issue 3 December 2009 Initially, corticosteroids produce a marked but temporary remission [7]. The presence of fleas reported by the owner reflects only infestation. In-contact animals, particularly cats, can also be infested and are sometimes the source of infestation. Clinical signs Canine flea allergy dermatitis is characterised in its early stages by a pruritic, erythematous and papular dermatitis affecting the caudal aspect of the dog. Lesions are confined to the dorsolumbar area, inner and posterior thighs, ventral abdomen and flanks (Fig. 1) [3]. FAD is the only known canine pruritic dermatitis that consistently affects this region [8, 9] even though one study showed dorsolumbar involvement in only Fig. 3 Brownish stain of the hairs in the 76% of flea-allergic dogs. Furthermore, Fig. 1 Alopecia and scaling in the dorsolombar area of a flea allergic West the dorsolumbar region was involved dorsolombar area in a flea allergic dog. Highland White terrier. in 39% of atopic dogs. In this study, 34% of dogs with FAD exhibited facial pruritus and lesions but the feet were involved in only 1.2% Pruritus is associated with self-induced alopecia, excoriations, [10]. Whether these signs were related to an adverse food pyotraumatic dermatitis, and a dull and coarse hair coat [6]. reaction and/or atopic dermatitis or to FAD could have been Flea allergy dermatitis could be the underlying cause of a evaluated for example, by using appropriate flea control. It must majority of recurrent pyotraumatic dermatitis cases arising in the be emphasised that atopic status may predispose to flea allergy dorsolumbar region in dogs with a dense hair coat (Fig. 2) [3, dermatitis [1, 4]. Another study evaluated the diagnostic value 9]. In dogs with a light coat colour, hair is stained brown from of some clinical clues in the diagnosis of flea allergy dermatitis: it licking and saliva (Fig. 3) [9]. was found that dorsolumbar involvement (lesions and pruritus) was a discriminating diagnostic criterion. Its sole presence in With time, lichenification and hyperpigmentation, crusts and a pruritic dermatitis has a sensitivity of 92% and a specificity scaling appear gradually. Fibropruritic nodules may also occur of 84% when compared to response to strict flea control [9]. in some chronic cases, usually in the dorsolumbar area. They Sometimes, particularly in severely hypersensitive dogs, lesions represent a highly characteristic clinical marker of flea allergy become generalised and may mimic scabies [3]. dermatitis in susceptible dogs [8, 9]. Possibly more frequent in old (over 8 years old) German Shepherd dogs with chronic flea Lesions consist of erythema and papules that may become allergy dermatitis, they consist of multiple, firm, alopecic and crusted. Crusted papules in the umbilical area may be particularly sometimes pedunculated nodules (diameter from 0,5 to 2 cm) suggestive of flea bite allergy, especially in male dogs [3, 8]. (Fig. 4) [9]. Fig. 2 Pyotraumatic dermatitis in a flea allergic dog: alopecia, erosions, erythema and oozing in the flank region Fig. 4 Pruritic and fibrotic nodule in a flea allergic boxer. 243 Flea allergy in dogs: Clinical signs and diagnosis - C. Laffort-Dassot Fig. 5 Bacterial folliculitis in a flea allergic dog: erythema, papules, pustules, crusts and eipdermal collarettes. Fig. 6 Flea feces dissolving to form brown stain on a wet piece of blotting paper. Secondary infections such as superficial bacterial folliculitis or Malassezia dermatitis are common [3]. They increase inflammation and pruritus. Malassezia dermatitis seems to be less frequent in dogs with flea allergy dermatitis than in dogs with atopic dermatitis but secondary superficial bacterial folliculitis is commonly noted (Fig. 5) [9].If corticosteroids are used for long-term pruritus management, superficial bacterial infection can lead to deep pyoderma with furunculosis in the dorsolumbar area [3, 9]. study, fleas were observed in only 65% of flea-allergic dogs. In 15% of these cases, neither fleas nor flea faeces were found [12]. Differential diagnosis The differential diagnosis includes all pruritic dermatoses. The most common differentials are bacterial folliculitis, Malassezia dermatitis, scabies, trombiculosis, cheyletiellosis, pediculosis, demodicosis, adverse food reaction and atopic dermatitis. Sometimes diagnosis is made difficult by the association of flea allergy dermatitis with one of these other dermatoses, especially bacterial folliculitis and/or Malassezia dermatitis [3]. Histopathological examination of skin biopsies reveals superficial perivascular inflammation with variable eosinophilia. This pattern can be seen in other hypersensitivity reactions [13] and is nonspecific. In severely infested dogs, clinical anaemia may be present [3]. Due to the fastidious grooming induced by pruritus, some dogs can ingest adult fleas carrying the tapeworm Dipylidium caninum and may have segments of it in their faeces or around the anus [3]. Demonstration of fleas Close examination of the skin and hair coat may reveal the presence of adult fleas or flea faeces. This can be difficult, sometimes impossible because flea-allergic dogs scratch and lick themselves more than other dogs, removing fleas from their skin and hair coat. The reliability of this examination can be considerably improved by using a flea comb. Combing for a few minutes, especially in lesional areas, after applying an insecticidal spray can help reveal adult fleas. Even if adult fleas are not found, it is sometimes possible to demonstrate flea faeces. These small, reddish-brown comma-shaped fragments, [11] made from haemoglobin crystals, will readily dissolve to form reddish-brown stains if placed on a wet piece of blotting paper (Fig. 6). They can also be examined under the microscope to reveal their characteristic colour and shape. Blood eosinophilia and anaemia are sometimes reported [3]. Allergy testing Provocative tests are considered to be the gold standard in allergy testing, particularly for food or contact hypersensitivity. They have also been used in flea allergy dermatitis diagnosis (live flea challenge tests), especially to compare the diagnostic value of different assays [14]. A few, newly-emerged, unfed fleas are placed in a universal container the open end of which is covered by a gauze lid, through which the fleas can feed. This container is held for 15 to 20 minutes against the clipped skin of the dog to be tested, usually the skin of the lateral thorax. The container is then removed. The fleas are killed and then crushed to ensure that they contain ingested blood, confirming feeding and exposure of the dog to flea saliva allergens. The challenge site is inspected at 15/20 minutes for evidence of immediate reactivity, then at 24h and/or 48h. Possible lesions include erythema, papules, skin thickening, oedema, wheals, crusts or a combination thereof [14, 15]. Human infestation with young adults, recently emerged from their cocoons, may be an indirect sign of a severely infested environment. In many instances, neither fleas nor flea faeces will be demonstrated but this should not be used to rule out a diagnosis of flea allergy dermatitis if clinical suspicion is high. In a French 244 EJCAP - Vol. 19 - Issue 3 December 2009 Fig. 7 Intradermal skin testing with flea extracts (lecture at 20 min): from top left to bottom right, negative control, positive control, biophady extract, Greer extract, pure flea saliva, Cte f1(2 dilutions). Fig. 8 Intradermal skin testing with flea extract (lecture at 48h): erythematous papule. Intradermal skin testing Intradermal skin testing with flea extracts is used to demonstrate in vivo immediate (at 20 minutes) and/or delayed (at 48h) hypersensitivity reactions. Non-standardised whole-body extracts of Ctenocephalides felis felis at a concentration of 1:1000 (W/v) are currently the only flea allergens commercially available for intradermal skin testing. These provocative exposure tests are practical on a research basis, but not for most veterinary practitioners and dermatologists. Moreover, their reliability is not excellent: in a study where they took into account only immediate reactions after provocative exposure, Stolper et al. showed that sensitivity of this reference test was only around 50% although specificity was excellent (94%). [15] The intradermal skin testing protocol for flea extracts is the same as that for aeroallergens. It requires experience and practice to avoid the most frequent causes of false positive and false negative reactions. For example, all drugs that could interfere with testing must be withdrawn for a suitable length of time prior to the intradermal test (3 weeks for oral and topical glucocorticoids, 8 weeks for injectable glucocorticoids, 10 days for antihistamines, and 10 days for products and diets containing w3/w6 fatty acids)[3]. It seems that even a short administration of glucocorticoids could strongly decrease delayed reactions at 48h [1]. Secondary infections should be cleared and stressed dogs can be anaesthetised. Allergenic extracts of Ctenocephalides felis felis Whole-body flea extracts Allergenic extracts used for immunotherapy and in vivo and in vitro diagnosis are whole-body flea extracts. They are produced after crushing of the flea bodies, protein extractions and purification. They are not biologically standardised; their composition and allergenicity may vary, altering diagnostic reproducibility and therapeutic efficacy. Furthermore, crossreactivity to other insect antigens has been demonstrated [16]. A few studies have tried to identify the allergens included in these extracts: several proteins with molecular weights between 14 and 150kδ have been isolated [14, 16]. Purified fractions of these could be less active [15]. Dogs are placed in lateral recumbency and clipped carefully over the thorax. After the area has been cleaned with ether, injection sites are marked with a felt-tip pen. Each solution (0.05 mL) is injected strictly intradermally in a standard order, equidistant to the others. Two controls are used: a positive control (histamine phosphate 0.01%) and a negative control (phenolated physiological diluent). Flea Salivary extracts An artificial flea feeding system on membranes has allowed the in vitro collection and purification of flea saliva. Several antigenic fractions have been isolated but results from different studies are controversial. Lee et al. isolated 2 proteins with molecular masses of 8-12 kδ and 40 kδ [18]. Franck et al. isolated 15 fractions, some of which could elicit a positive immediate intradermal test reaction in sensitised dogs [19]. One of these proteins with a molecular mass of 18 kδ was then cloned and expressed to produce a recombinant allergen; rCte f1 could be a major allergen of flea saliva as IgE directed against this protein has been detected in 95% of experimentally-induced flea-allergic dogs. In naturally occurring flea-allergic dogs, IgE directed against Cte f 1 were detected in only 80% of dogs [20]. Reactions are first read after 15/20 minutes in the dark with the aid of an oblique light source. A raised erythematous wheal is considered a positive reaction. If erythema is absent, the result is considered negative, even if a small wheal is visible. The greatest diameter of each reaction is measured precisely using a ruler provided by the allergen suppliers. To be considered positive, the diameter of the wheal at the suspected allergen injection site has to be greater than or equal to the mean of the wheal diameters at the histamine and diluent control sites (Fig. 7). 245 Flea allergy in dogs: Clinical signs and diagnosis - C. Laffort-Dassot When the reaction read at 15/20 minutes is negative, a second measurement is made at 48h. This interval is considered optimal because the immediate reaction can sometimes persist for up to 24h. Moreover, in a delayed reaction, maximal development of a cutaneous lesion provoked by intradermal injection of an antigen in a sensitive dog occurs between 12 and 72 h [11]. The delayed reaction to flea extract appears as a skin thickening (detected by palpation of a skin fold) or as a papule, both of which can be encrusted (Fig. 8) [4]. allergy dermatitis based on history, clinical signs and response to strict flea control [7]. This result is in accordance with another study which showed that flea allergens involved in flea allergy dermatitis are mostly found in flea saliva [24]. The fact that flea saliva only represents 0.5% of the proteins in whole-body flea extracts might somehow explain why intradermal skin testing with whole-body flea extracts has been associated with variable results [24]. In the same study, rCte f1 was also used as a reagent for intradermal skin testing and the results were not as accurate as for pure flea saliva: sensitivity was 40% and specificity 90% [7]. Pure flea saliva and rCte f1 are not commercially available for skin testing. The majority of dogs show an immediate reaction followed by a delayed reaction. Halliwell and Gorman demonstrated that 60% of dogs show an immediate and a delayed reaction, 25% only an immediate reaction and 14% only a delayed reaction [4]. For others, the percentage of delayed reactions can be as high as 33% [2]. In vitro tests Serological tests The use of serological tests for the diagnosis of flea allergy dermatitis has also been a great source of debate. Sensitivity, specificity and reproducibility vary greatly, as does the quality of flea allergens used. Whatever the technique used, delayed reactions are missed. Whatever the immediate and/or delayed reaction, a positive reaction only means that the dog is sensitised to flea extracts and does not prove that the dermatological problem the clinician is dealing with is flea allergy dermatitis. Results of intradermal skin testing have always to be interpreted in the light of history and clinical signs [3]. These tests are based on the detection by enzyme-linked immunosorbent assays (ELISA) of specific immunoglobulin IgE or IgG. IgE or IgG specific to Ctenocephalides felis felis in the serum of a dog suspected of FAD is detected by addition of an antiglobulin linked to an enzyme; the complex immunoglobulin/ antiglobulin/enzyme is then detected and measured by addition of the enzyme substrate [26]. In the case of IgE, this system has to be very sensitive because of the small concentration of IgE in serum [20]. Results of different studies using these serological tests vary considerably: some authors have found high levels of IgE or IgG in flea-allergic dogs when compared with normal dogs [27] whereas others have found the opposite [24, 28]. Reports of reliability of intradermal skin testing using wholebody flea allergens for the diagnosis of canine flea allergy dermatitis vary greatly. Although some authors report that they give reliable results [2, 3], most of them report poor reliability with sensitivity varying between 70 and 80% and specificity around 60% [21]. This controversy is in part linked to the fact that results vary considerably between studies, one reason for this being whether or not delayed reactions were taken into account. One of the most recent assays uses the high affinity Fc epsilon receptor (FcεRIα) to detect anti-flea saliva IgE in canine sera. This test has an excellent specificity whereas sensitivity is improved by the use of highly purified flea salivary antigens and rCte f1. In one study, when results of this test were compared to those of intradermal skin testing with pure flea saliva in clinical cases of flea allergy artificially sensitised dogs, and dogs never exposed to fleas, the test was found to be reliable for FAD diagnosis (sensitivity 78%; specificity 91% and accuracy 88%) [29]. In another independent study, results of this in vitro test were compared to a clinical approach to FAD diagnosis based on history, clinical signs and response to strict flea control. Sensitivity of the test was 87%, specificity 53% and accuracy 64% [7]. It must be emphasised that positive reactions may be observed in clinically normal dogs. In Florida, a flea-rich environment, immediate positive reactions have been detected in 24% of clinically normal dogs [22]. Furthermore, this was not predictive of the future development of flea allergy dermatitis as two years later, only 2.5% of these dogs had developed clinical signs of flea allergy dermatitis. However, in Norway, a flea-scarce environment, only 2% of clinically diagnosed “atopic dermatitis” dogs and no clinically normal dogs or dogs with dermatoses other than atopic dermatitis had positive reactions to flea [23]. Positive reactions against flea allergens in atopic and clinically normal dogs in a flea-rich environment might represent truly false positive reactions, subclinical hypersensitivity [22] or crossreactivity to other insect antigens [16]. This poor specificity has led some authors to abandon intradermal skin testing with flea extracts as a diagnostic tool for flea allergy dermatitis. Cellular tests Only direct activation of canine basophils has been used with flea extracts. In this test, basophil degranulation is provoked by contact with the offending allergen, in this case coming from a flea extract. When results of this assay are compared with those of intradermal skin testing with flea extracts, sensitivity and specificity were 80%. However, the diagnostic value of these tests for the diagnosis of FAD has not yet been established [21]. Furthermore it seems that not all commercially available flea extracts have the same diagnostic value. One study showed that sensitivity varied between 27 and 67% and specificity varied between 83 and 90% when whole-body flea extracts were used as reagents for intradermal skin testing. When pure flea saliva was used, sensitivity raised to 93% and specificity 90%. The results of intradermal tests comprising immediate and delayed reactions were compared to clinical diagnosis of flea 246 EJCAP - Vol. 19 - Issue 3 December 2009 Response to flea control Referenses In the face of poor reliability of allergy testing with commercially available flea assays, response to strict flea control can be used to confirm flea allergy dermatitis. Trial flea control should involve the flea-allergic dog, all in-contact animals and their environment. The aim is to kill adult fleas on affected animals, to eliminate fleas acquired from infested premises and to prevent re-infestation. Effective residual insecticides are nowadays available to kill adult fleas, and insect growth regulators should be used to disrupt the flea life cycle. A permethrin-pyriproxyfen spray has been found to be a useful product for performing a therapeutic trial to confirm a diagnosis of flea allergy dermatitis in dogs [30]. [1] [2] [3] [4] [5] Mechanical control procedures (vacuuming, cleaning, possibly removing all furniture or materials the pets are in contact with) and preventing other animals that can carry fleas from entering resting areas of pets are also important. Cats that wander in and out are a frequent cause of treatment failure [8]. [6] [7] Trial flea control is not always reliable in FAD diagnosis because it must take into account the level of flea challenge and the level of “allergenic threshold” for that individual dog. It is essential for the clinician to be aware of efficacy, frequency of administration, dosage and mode of action of flea control products. In the study with the permethrin-pyriproxyfen spray, flea control was applied weekly on the flea allergic dogs only (no flea control on the in-contact animals or in the environment was performed) for 3 times. This extra-label use led to a reduction in lesional and pruritus scores of more than 75% in all of these dogs. No sideeffects were observed [30]. Strict owner compliance is necessary both at the outset of flea control measures and also throughout their duration. [14]. Even with adequate flea control, clinical improvement can take a long time (4 to 8 weeks) [31, 32]. [8] [9] [10] [11] [12] [13] No anti-pruritic drug should be used during the trial. This can be a problem in dogs that show slow clinical improvement. When secondary infections are present, they must be cleared but treatment required in these cases makes interpretation of the trial difficult. [14] [15] Conclusion [16] Diagnosis of canine flea allergy dermatitis relies on a thorough history and physical examination, eliminating other differential dermatoses, providing appropriate flea control for the fleaallergic dog, all in-contact animals and their environment. Clinical signs and lesion distribution are strongly suggestive of the diagnosis. Dorsolumbar lesions and pruritus have been found, in many cases, to be discriminating criteria . However, this is not sufficient for a definitive diagnosis. Demonstration of fleas is not always possible in flea allergic dogs and appropriate flea control is often difficult both to initiate and maintain. Some in-vivo and in-vitro allergy tests can be used to document sensitisation to flea allergens in flea-allergic dogs but their use is controversial. A definitive diagnosis of flea allergy in the dog is made by pooling evidence from different sources. [17] [18] [19] [20] 247 Reedy LH, Miller WH, Willemse T. Arthropod hypersensivity disorders. In: Allergic skin disease of dogs and cats, 2nd edn. Philadelphia. W.B.Saunders. 1999: 202-33. Carlotti DN. Diagnostic de la dermatite par allergie aux piqûres de puces (DAPP) chez le chien. Intérêt des intradermoreactions. Pratique Médicale et Chirurgicale de l’Animal de Compagnie. 1985; 20: 41-7. Scott DW, Miller WH, Griffin CE. Muller and Kirk’s Small Animal Dermatology 6th edn. Philadelphia: WB Saunders. 2001: 543666. Halliwell REW, Gorman NT. In: Veterinary Clinical Immunology. Philadelphia: W.B.Saunders. 1989: 261-7. Carlotti DN, Costargent F. Analysis of positive skin tests in 449 dogs with allergic dermatitis. The European Journal of Companion Animal Practice. 1994; 4: 42-59. Yu A, Lam A. Overview of Flea Allergy Dermatitis. Compendium: continuing Education for Veterinarians. 2009, 220-5. Laffort-Dassot C, Carlotti DN, Pin D, Jasmin P. Diagnosis of flea allergy dermatitis: comparison of intradermal testing with flea antigens and a fceRIa-based assay in response to flea control. Veterinary Dermatology. 2004, 15: 321-30. Ihrke PJ. Flea Allergy Dermatitis (how I treat). Proceedings of the 31st annual meeting of the WSAVA, Prague. 2006, p 32-5. Prélaud P. Diagnostic clinique des dermatites allergiques. Revue de Médecine vétérinaire. 2004, 155 : 12-19. Bourdeau P. Relationship between the distribution of lesions and positive intradermal reactions in 307 dogs suspected of atopy and/ or flea bite hypersensitivity. Proceedings of the Annual Member Meeting of the ESVD/ECVD, Maastricht, 1998, p 157-8. Vroom M. Flea allergy dermatitis. In: Guaguère E., Prélaud P. eds, A practical guide to feline dermatology, Lyon: Mérial, 1999: 916. Carlotti DN, Héripret D. La dermatite par allergie aux piqûres de puces chez le chien Pratique Médicale et Chirurgicale de l’Animal de Compagnie. 1986; 21 (suppl): 1-64. Gross TL, Ihrke PJ, Walder, EJ, coll. Skin diseases of the dog and cat. Clinical and histopathological diagnosis 2nd Ed. London: Blackwell Publishing, 2005: 932p. Bond R, Hutchinson MJ, Loeffler A. Serological, intradermal and live flea challenge tests in the assessment of hypersensitivity to flea antigens in cats (Felis domesticus). Parasitology Research. 2006, 4: 392-7. Stolper R, Opdebeeck JP. Flea allergy dermatitis in dogs diagnosed by intradermal skin tests. Research Veterinary Science. 1994; 57: 21-7. Pucheu-Haston CM, Grier TJ, Esch RE. et al. Allergenic crossreactivities in flea-reactive canine serum samples. American Journal of Veterinary Research. 1996; 57: 1000-5. Greene WK, Carnegie RL, Shaw SE. et al. Characterization of allergens of the cat flea, Ctenocephalides felis: detection and frequency of IgE antibodies in canine sera. Parasite Immunology. 1993 ; 15 : 69-74. Lee SE, Johnstone IP, Lee RP. et al. Putative salivary allergens of the cat flea, Ctenocephalides felis felis. Veterinary Immunology and Immunopathology. 1999; 69: 229-37. Frank GR, Hunter SW, Stiegler GL. et al. Salivary allergens of Ctenocephalides felis: collection, purification and evaluation by intradermal skin testing in dogs. In: Kwochka K.W. et al, eds. Advances in veterinary Dermatology III. Boston: Butterworth Heinemann, 1998: 201-12. McDermott MJ, Weber E, Hunter S. et al. Identification, cloning and characterization of a major cat flea salivary allergen (Cte f 1). Molecular Immunology. 2000; 37: 361-75. Flea allergy in dogs: Clinical signs and diagnosis - C. Laffort-Dassot [21] Prélaud P. Allergies aux parasites et aux insectes piqueurs. In: Masson, ed. Allergologie canine, Paris. 1999: 85-106. [22] Kunkle GA, Jones L, Petty P. Immediate intradermal flea antigen reactivity in clinically normal adult dogs from South Florida, USA. Veterinary Dermatology. 2000; 11: 9-11. [23] Saevik BK, Ulstein TL. Immediate intradermal flea antigen reactivity in dogs in a flea scarce environnement. Proceedings of the Annual Member Meeting of the AAVD/ACVD, New Orleans, 2002, 18. [24] Lee SE, Jackson LA, Opdebeeck JP. Salivary antigens of the cat flea, Ctenocephalides felis felis. Parasite Immunology. 1997; 19: 13-9. [25] Cook CA, Stedman KE, Frank GR et al. the in vitro diagnosis of flea bite hypersensitivity : flea saliva vs whole flea extracts. In: Kwochka K.W. et al, ed. Advances in veterinary Dermatology III. Boston: Butterworth Heinemann, 1998: 494-5. [26] Tizard IR. Veterinary Immunology: an introduction. 6th ed. Philadelphia: WB Saunders Co, 2000: 191-209. [27] Halliwell REW, Longino SJ. IgE and IgG antibodies to flea antigen in differing dog populations. Veterinary Immunology and Immunopathology. 1985; 8 : 215-23. [28] McKeon SE, Opdebeeck JP. IgE and IgG antibodies against antigens of the cat flea, Ctenocephalides felis felis, in sera of allergic and non allergic dogs. International Journal of Parasitology. 1994; 24: 259-63. [29] McCall CA, Stedman KE, Penner SJ. et al. FceRIa- based measurement of antiflea Saliva IgE in Dogs. Compendium on Continuing Education: Small Animal Practice. 1997; 19 (suppl): 24-8. [30] Jasmin P, Briggs M, Schroeder H, Sanquer A. Comparison of a permethrin-pyriproxyfen spray and fipronil spot-on used alone in a therapeutic trail for diagnosis of canine flea allergy dermatitis. Veterinary Dermatology. 2004, 15 (suppl 1): 47. [31] Prélaud P. Diagnostic de la dermatite par allergie aux piqûres de puces. Proceedings of the Annual Meeting of the CNVSPA AFVAC 2001, Lille, 144. [32] Medleau L, Clekis T, McArthur TR, Alva R, Barrick RA, Jeannin P, Irwin J. Evaluation of fipronil spot-on in the treatment of flea allergy dermatitis in dogs. Journal of Small Animal Practice. 2003, 44: 71-5. 248 DERMATOLOGY Flea allergy in cats – clinical signs and diagnosis C. Noli(1) SUMMARY Fleas are the most common ectoparasites and flea bite allergy is often seen in cats. The clinical signs are represented by pruritus, excoriations, self-inflicted alopecia, manifestations of the eosinophilic granuloma complex and miliary dermatitis, which often, but not exclusively, involve the posterior dorsal and ventral part of the body. The diagnosis is obtained with the clinical presentation and response to flea control, and is supported by finding fleas, their feces or taenia infestation, and by a positive intradermal and/or in vitro allergy test. immediate wheal, when injected intradermally with a commercial flea allergen [21]. Also allergen-specific IgE can be found in the serum of flea allergic dogs by means of ELISA or RAST [4, 16, 23]. In some dogs a type-4 (delayed) cell-mediated reaction may also be present, as an indurated wheal may appear 2448 hours after the intradermal injection of the allergen [10,23]. Other types of immunologic response, in addition to the classic type-1 and type-4 reaction have been suggested in dogs [11], i.e. a late phase IgE-mediated cellular response, which occurs 3 to 6 hours after the antigen exposure and a cutaneous basophil hypersensitivity, with infiltration of basophils in the dermis. This paper was commissioned by FECAVA for publication in EJCAP. Introduction More than 2000 species of fleas have been identified, which infest mammals and birds. The species identified in cats is Ctenocephalides felis felis, by far the most prevalent flea in cats, dogs and ferrets. Many diseases have been associated with fleas, such as anemia, tape worm infestations, Lyme disease, the pest, viruses, hemoparasites, cat scratch disease and flea allergy [22]. Flea allergy is the most frequent dermatological disease associated with fleas [21], and its prevalence depends on the geographical region. Less is known about the pathogenesis of flea allergy in cats. Most flea allergic cats have immediate positive intradermal skin test reactions to flea allergens, and delayed type-4 reactions have been also described [14]. As in dogs, allergen-specific IgE can be found in the serum of flea allergic cats by means of ELISA [17]. Late phase IgE-mediated cellular response and cutaneous basophil hypersensitivity have not yet been identified in cats. Pathogenesis of flea allergy Fleas of both sexes bite the host several times a day [6]. It is thought that non-allergic animals suffer little or no discomfort while being bitten, and that only flea-allergic subjects develop pruritus and skin disease. Dogs continuously exposed to fleas become tolerant and fail to become allergic. On the contrary, dogs intermittently exposed to fleas develop immediate positive and/or delayed skin reactions within 12 weeks, and have allergen-specific IgG and IgE antibodies in their serum [11]. In a study specifically designed to clarify the role of intermittent exposure to flea bites in the development of flea bite allergy in cats it was concluded that it had neither a protective nor a predisposing effect on the development of clinical signs [3]. Several studies have dealt with the pathogenesis of flea bite allergy in dogs. These investigations have suggested that the allergic reaction in this species is most probably a type-1 (immediate) IgE-mediated response, with development of an 1) Chiara Noli, DVM, Dip ECVD, Ospedale Veterinario Cuneese, Via Vocaturo 13, 12016 Peveragno (CN), Italy 249 EJCAP - Vol. 19 - Issue 3 December 2009 Fig. 1 Small, round crusts typical of miliary dermatitis on the back of a cat with flea bite allergy. Fig. 2 Large areas of self inflicted alopecia on the abdomen. It has been reported that dogs exposed to fleas early in their life are less likely to develop flea allergy than dogs exposed at a later age [10]. Results of a study of early sensitization of 12 weeks-old kittens, which developed only mild clinical signs in 10/18 subject, suggest that this may be true in the cat also [13]. The authors suggested that early ingestion of fleas could induce tolerance, as cats experimentally exposed to fleas orally tended to have limited symptoms and lower in vivo and in vitro test scores, although this was not statistically different from the controls [13]. dorsolumbar region, has been associated with flea allergy, less frequently it can be due to other causes including bacterial infection, dermatophytosis, drug reactions, pemphigus foliaceus, and ectoparasites. Self-inflicted alopecia Self-induced alopecia in the cat is caused by licking either as a result of pruritus due to flea or other allergies, parasitism or a psychological disturbance. The sites of the licking in case of flea bite allergy most commonly are the ventral abdomen, dorsum, medial and lateral thighs (Fig. 2). Less commonly the lick induced alopecia extends to the entire trunk. The affected areas may be completely bald or have clumps of hair which the cat’s tongue has not damaged as much. With a magnifying lens or by stroking the skin against the line of the fur, broken hairs can be detected emerging from the follicular openings. The faeces or vomit of the cat may contain excessive quantities of hair. The incidence of positive skin tests to flea antigen in atopic dogs is significantly greater than in the general population. This indicates that the atopic state may predispose the animals to the development and maintenance of flea allergy [2]. It is not know if the same is true for the cat. Clinical appearance The eosinophilic plaque The eosinophilic plaque is a very pruritic, well circumscribed, round to oval, erythematous, oozing, ulcerated plaque, mostly located on the abdomen and medial thighs (Fig. 3). Less frequently it may develop on other skin sites. It is found in cats of all ages and breeds, and is often seen associated with flea There is no breed or sex predilection, and animals may develop flea bite hypersensitivity at any age [21]. In most cases flea control of these animals is absent or incomplete or wrong. Flea bite hypersensitivity may be observed the whole year round in warm climates, although signs are usually worse in the warmer months, particularly at the end of the summer, when the flea population is at its highest point. Fig. 3 Lesions of eosinophilic plaque on the medial aspect of a thigh. Clinical signs of flea allergy in cats are miliary dermatitis, self-inflicted alopecia, eosinophilic plaque and eosinophilic granuloma, indolent ulcus and pruritus [15, 21]. All of these signs could be reproduced in experimental sensitization studies [3]. Miliary dermatitis The macroscopic lesions of miliary dermatitis are represented by discrete light-brown crusts, diffusely distributed on the trunk (Fig. 1). The animals are often only mildly pruritic. Histologically the lesions appear similar to eosinophilic plaque (see herunder), but less severe. These lesions have been considered the initial stage of the eosinophilic plaque, because they share a common histologic picture and because they may be seen on the same animal. Miliary dermatitis, particularly if observed on the 250 Flea allergy in cats – clinical signs and diagnosis - C. Noli allergy, as well as with atopic dermatitis and food allergy. The eosinophilic plaque probably develops due to chronic trauma caused by the cat’s tongue, when licking pruritic areas. A secondary bacterial infection is frequent. Histologically this lesion appears as a hyperplastic superficial to deep perivascular to diffuse eosinophilic dermatitis with high amounts of mastcells and an ulcerated epidermis [7] (Fig. 4). This pattern is similar to that of miliary dermatitis, suggesting a common pathogenesis. The eosinophilic granuloma The eosinophilic granuloma is a well circumscribed, raised, firm, yellow-pink, linear lesion usually located on the caudal thigh (Fig. 5). It may also be located on the chin, paws or oral cavity. It is generally asymptomatic but can occasionally ulcerate and show pinpoint white foci of collagen degeneration and become pruritic. The eosinophilic granuloma has been associated to fleabite allergy, as well as to food hypersensitivity, atopic dermatitis, mosquito bites, insect hypersensitivity, genetic predisposition, bacterial and viral infections (calicivirus) [20]. Histologically it appears as a nodular to diffuse granulomatous dermatitis with multifocal areas of “eosinophilic mush” (formerly called “collagen degeneration”, now it appears that collagen is not degenerated at all) [7] (Fig. 6). The eosinophilic material seen is probably formed by granules of degranulated eosinophils and these, along with multinucleated giant cell, form a palisading granuloma around the foci of eosinophilic mush. The epidermis is initially unaffected, and may ulcerate as the eosinophilic material is expelled as a foreign body through the skin surface and the hair follicles. Fig. 5 Linear lesions of eosinophilic granuloma on the caudal aspect of a thigh. Fig. 4 Histological appearance of eosinphilic plaque: a thick eosinophilic crust overlies an area of epidermal ulceration, interstitial eosinophilic infiltrate in the underlying dermis (Hematoxilin-Eosin 100x). The indolent ulcer The indolent ulcer is a well circumscribed, necrotic ulcer with raised borders located mono- or bilaterally on the upper lip (Fig. 7). It is usually not painful. The indolent ulcer has also been associated with flea allergy in experimental flea sensitization studies [3]. The histological picture is usually non diagnostic: a hyperplastic, ulcerated superficial perivascular dermatitis with variable amounts of neutrophils, mononuclear cells and fibrous tissue. A eosinophilic infiltrate or eosinophilic mush may be observed. Differential diagnoses The main differential diagnoses of flea allergy in all its clinical manifestations are other allergies, such as adverse reactions to food and atopic dermatitis. In case of pruritus one should also consider otodectic and notoedric mange and dermatophytosis. Differentials of allergic self-inflicted alopecia are psychogenic alopecia and Cheyletiella infestation. Common differential diagnosis for eosinophilic granuloma is xanthomatosis, and, if the lesion is a solitary nodule, mast cell tumour. Extended erosions/ ulcerations on the abdomen similar to eosinophilic plaque may be seen in autoimmune diseases (pemphigus foliaceus, other autoimmune disases), metastases of mammary tumours, or bacterial/deep fungal ulcerative diseases. Indolent ulcer can appear similar to labial squamous cell carcinoma. Miliary dermatitis has as differentials cheyletiellosis, dermatophytosis, mild pemphigus foliaceus and incipient paraneoplastic desquamative diseases. 251 EJCAP - Vol. 19 - Issue 3 December 2009 Fig. 6 Histological appearance of eosinphilic granulma: large aggregates of eosinophilic “mush” are visible in the dermis (Hematoxilin-Eosin 40x). Fig. 7 Monolateral lesions of indolent lip ulcer in a cat. Diagnostic approach hours), but it can be a good alternative in animals with a very sensitive skin, which do not stand any topical application. There are several problems in the approach to flea allergy in cats. The first is that it is difficult per se to make an inequivocal diagnosis of allergy in this species, the reason being, that allergies have not yet been well defined in cats. A more practical flea control measure involves a spot-on adulticide (imidacloprid, fipronil, selamectin, metaflumizone) given every three to four weeks, associated with an insect growth regulator (IGR). The latter can be sprayed in the environment or be contained in the spot-on product (methoprene, piryproxiphene) or administered systemically to the cat as an injectable or oral formulation (lufenuron). Some adulticides, such as imidacloprid [12] or selamectin [18], also provide an IGR effect, as treated hairs shed in the environment are able to inhibit eggs’ hatching. The use of an IGR is fundamental to reduce the environmental flea population, thus the flea burden on the cat and the consequent clinical symptomatology. A product with a rapid knock down effect would allow flea death before these parasites bite and inject their antigens into the cat’s body, and would particularly indicated in allergic animals. Unfortunately molecules with the best knock down effect (pyrethroids) are toxic in cats and cannot be used. Clinical manifestations of allergy in cats are not as site-specific as in dogs, e.g. a cat scratching on the neck may have a flea allergy as well as food allergy, or a cat licking on its belly may have a flea allergy, food allergy or atopic dermatitis. To make things even more complicated, in cats there are some clinical manifestations of flea allergy which may be due to other causes. For example a “bold belly” may be due to allergy, as well as to psychogenic causes, and a linear granuloma may be associated to flea hypersensitivity or may be hereditary or idiopathic. Finding fleas or flea dirt is not always possible, because even one or a few fleas can elicit severe pruritus. Allergic cats in particular are excellent groomers and can eliminate all of the fleas put on them in less than 48 hours. Furthermore recent bathing may also have removed all fleas and feces. Infestation with Dipylidium caninum is a useful sign of flea presence. The diagnosis of flea allergy may be confirmed by performing an intradermal skin test. The flea allergen is injected (0.05 ml) intradermally together with a negative (saline) and a positive (histamine) control, and reactions are read at 15 minutes, 24 and 48 hours. Current or recent administration of steroids or antihistamines may cause false-negative results. False-positive reactions in normal cats have been described : in one study 36% of clinically normal cats that had been exposed to fleas had a positive immediate skin test reaction to flea antigens (19). The best way to identify a flea allergy is to first treat all secondary infections (rare in cats and mainly bacterial, seen on eosinophilic plaques and/or excoriations) and all other possible parasitic diseases (with spot on selamectin or moxidectin), then perform a correct flea control for at least two months and then recheck the animal. A flea infestation can be best and quickly eliminated with oral nitempyran. Its effect is seen as soon as 15-30 minutes after administration [5]. Nitenpyran is thus an excellent means of diagnosing the presence of fleas, if given as soon as the cat enters the clinic, as fleas can be seen falling on the table during the consultation. However, being it’s duration of effect so short (>90% eliminated in 48h in cats), it is not very practical as a flea prevention means (the drug should be administered every 48-72 A positive predictive value of 85-100% has been reported in earlier studies (3, 8), while a more recent study performed with three different extracts obtained a sensitivity of 0.33 and a specificity of 0.78 to 1 [1]. In a study on laboratory induction of flea hypersensitivity the presence of a positive immediate intradermal test reactions did not correlate with the development of symptoms [13]. 252 Flea allergy in cats – clinical signs and diagnosis - C. Noli Allergens used initially for this test were whole body flea extracts (1:1000 w/v), now flea saliva or purified salivary antigens have been developed for a more sensitive in vivo test [9]. However, in experimentally induced feline flea bite allergy, results of intradermal tests with purified allergens were not superior than crude extracts in the correlation with clinical signs [3, 13]. [7] [8] [9] In vitro serologic tests (ELISA) with whole flea extracts or flea saliva are available for determination of allergen-specific IgE in the feline serum. It is questioned if these tests only identify animals with IgE mediated disease and fail to diagnose those individuals who only show a delayed reaction. Furthermore, there are normal cats who may have allergen-specific IgE in the absence of clinical disease [1, 3, 13]. Sensitivity and specificity of serological tests were reported to be 0.88 and 0.77 respectively in one study [1] and 0.77 and 0.72 in another study [8], with a low positive predictive value of 0.58 in the latter one. [10] [11] [12] [13] Flea saliva represents only 0.5% of whole flea extracts, and in vitro tests performed with flea salivary antigens gave much better results in dogs than those performed with whole flea extracts [4]. Furthermore, a new ELISA technology based on FcεR1α has been developed for the in vitro diagnosis of feline flea bite hypersensitivity [17]. In vitro test with salivary antigens and the use of high-affinity receptors gave an overall accuracy of 82% and may represent a more reliable tool for the diagnosis of flea allergy in cats [17]. [14] [15] [16] Conclusion [17] Flea bite hypersensitivity is one of the most important allergic skin conditions in cats, which can manifest with different clinical signs, and which has many possible differential diagnoses. Intradermal and in vitro allergy tests are not always reliable diagnostic tools, and a rigorous flea control, by means of adulticides and insect growth regulators, represents the best means of diagnosing and treating this condition. [18] References [19] [1] [20] [2] [3] [4] [5] [6] Bond R, Hutchinson MJ, Loeffler A. Serological, intradermal and live flea challenge tests in the assessment of hypersensitivity to flea antigens in cats (Felis domesticus). Parasitol Res. 2006; 99(4): 392-7. Carlotti DN, Costargent F. Analysis of positive skin tests in 449 dogs with allergic dermatitis. Eur J Comp Anim Pract. 1994; 4: 42-59. Colombini S, Hodgin EC, Foil CS, Hosgood G, Foil LD. Induction of feline flea allergy dermatitis and the incidence and histopahological characteristics of concurrent indolent lip ulcers. Vet Dermatol. 2001; 12(3): 155-61. Cook CA, Stedman KE, Frank GR, Wassom DL. The in vitro diagnosis of flea bite hypersensitivity: Flea saliva vs. whole flea extracts. Proceedings of the 3rd Veterinary Dermatology World Congress, 1996 Spet 11-14; Edinburgh, Scotland; 1996. p. 170. Dobson P, Tinembart O, Fisch RD, Junquera P. Efficacy of nitenpyram as a systemic flea adulticide in dogs and cats. Vet Rec. 2000 Dec 16; 147(25): 709-13. Dryden MW, Rust MK. The cat flea: biology, ecology and control. Vet Parasitol. 1994; 52: 1-19. [21] [22] [23] 253 Fondati A, Fondevila D, Ferrer L. Histopathological study of feline eosinophilic dermatoses. Vet Dermatol. 2001; 12(6): 333-8. Foster AP, O’Dair H. Allergy skin testing for skin disease in the cat in vivo vs in vitro tests. Vet Dermatol. 1993; 4(3): 111-115. Frank GR, Hunter SW, Wallenfels Lj, Kwochka KW. Salivary allergens of Ctenocephalides felis: Collection, purification and evaluation by intradermal skin testing in dogs. Proceedings of the 3rd Veterinary Dermatology World Congress; 1996 Spet 11-14; Edinburgh, Scotland; 1996. p. 26 . Halliwell REW, Preston JF, Nesbitt JG Aspects of the immunopathogenesis of flea bite dermatitis in dogs. Vet Immunol Immunopathol. 1987; 17: 483-94. Halliwell REW, Gormann T : Nonatopic allergic skin diseases. In: Halliwell REW, Goman NT, editors. Veterinary Clinical Immunology. Philadelphia: WB Saunders; 1989. p. 262-7. Jacobs DE, Hutchinson MJ, Stanneck D, Mencke N. Accumulation and persistence of flea larvicidal activity in the immediate environment of cats treated with imidacloprid. Med Vet Entomol. 2001; 15(3): 342-5. Kunkle GA, McCall CA, Stedman KE, Pilny A, Nicklin C, Logas DB. Pilot study to assess the effects of early flea exposure on the development of flea hypersensitivity in cats. J Fel Med Surg. 2003; 5: 287-294. Lewis DT, Ginn PE, Kunkle GA. Clinical and histological evaluation of immediate and delayed flea antigen intradermal skin test and flea bite sites in normal and flea allergic cats. Vet Dermatol 1999; 10, 29-38. MacDonald JM. Flea allergy dermatitis and flea control. In: Griffin, CE, Kwochka K, MacDonald JM editors. Current Veterinary Dermatology. St. Louis: Mosby; 1993. p. 57-71. McCall CA, Stedmann KE, Penne SJ et al. Fcε RIα-based measurment of anti-flea saliva IgE in dogs. Comp Cont Educ Pract Vet. 1997; 19(Suppl. 1): 24-8. McCall CA, Stedman KE, Bevier DE, Kunkle GA, Foil CS, Foil LD. Correlation of feline IgE, determined by Fcε RIα-based ELISA technology, and IDST to Ctenocephalides felis salivary antigens in a feline model of flea bite allergic dermatitis. Comp Cont Educ Pract Vet. 1997; 19(Suppl. 1): 29-32 McTier TL, Shanks DJ, Jernigan AD, Rowan TG, Jones RL, Murphy MG, et al. Evaluation of the effects of selamectin against adult and immature stages of fleas (Ctenocephalides felis felis) on dogs and cats.Vet Parasitol. 2000 (Aug 23); 91(3-4): 201-12. MorielloKA, McMurdy MA. The prevalence of positive intradermal skin test reactions to lea extracts in clinically normal cats. Comp Anim Pract. 1989; 19: 28-30. Rosenktantz WS. Feline Eosinophilic Granuloma Complex. In Griffin CE, Kwochka KW, MacDonald JM (editors). Current Veterinary Dermatology. St. Louis: Mosby Year Book; 1993. p. 319-24. Scott DW, Miller WH, Griffin CE. Skin immune system and allergic skin disease. In Scott DW, Miller WH, Griffin CE (editors) Small Animal Dermatology, Philadelphia: WB Saunders; 2001. p. 6325. Shaw SE, Birtles RJ, Day MJ. Arthropod-transmitted infectious diseases of cats. J Feline Med Surg. 2001; 3(4):193-209. Wilkerson MJ, Bagladi-Swanson M, Wheeler DW, Floyd-Hawkins K, Craig C, Lee KW, Dryden M. The immunopathogenesis of flea allergy dermatitis in dogs, an experimental study, Vet Immunol Immunopathol. 2004, 99: 179-192. DERMATOLOGY Microbial diseases secondary to allergic skin disease – clinical significance and control D. H. Lloyd(1) SUMMARY Allergic skin diseases predispose dogs and cats to cutaneous infections including microbial overgrowth and surface, superficial and deep pyoderma, most commonly involving pathogenic staphylococci and Malassezia pachydermatis. These can be treated successfully with systemic and topical antimicrobial agents but tend to recur unless the allergy is well controlled. In the face of emerging multiresistance in Europe, particularly in Staphylococcus aureus and S. pseudintermedius, antibacterial treatment should be based on culture and sensitivity tests, and adoption of treatment regimens ensuring good compliance and antimicrobial administration for appropriate periods. Recurrence of infection can be controlled with topical antimicrobials and especially shampoos containing chlorhexidine and benzoyl peroxide but long term low dose or pulse therapy should be avoided. Staphylococcal vaccines can be effective in some cases of superficial pyoderma. amongst the commonest diagnoses. Systemic antibiotics were prescribed in 25% of cases [3]. Thus dealing effectively with infection secondary to allergy has a high priority in small animal practice. This paper was commissioned by FECAVA for publication in EJCAP. Introduction Allergy and microbial infection The skin is a very effective defensive organ. Despite exposure to dirt, trauma and changing environments, under normal conditions it remains healthy or recovers quickly with minimal attention. This is because intact skin has an efficient epidermal barrier with its own self-cleaning process, represented by continual desquamation of the stratum corneum and a variety of immune mechanisms which resist proliferation and invasion by pathogens [1,2]. Cutaneous infection occurs only when these processes fail. One important factor which impairs these processes is allergic skin disease. Both animals and humans with allergic skin disease are predisposed to secondary microbial infection of the skin. Allergy induces changes in skin, which lead to colonisation and infection with pathogenic staphylococci in both dogs and in humans. Colonisation and infection with other organisms and particularly species of the genus Malassezia are also promoted. These changes have been best studied in staphylococcal disease associated with atopy. In man more than 90% of patients with atopic dermatitis have massive skin colonisation with S. aureus and in lesional skin up to 107 colony-forming units per cm2 of skin may be present [4]. Up to 68% of dogs with canine atopy have been reported to have pyoderma and populations of S. intermedius that are significantly elevated in both lesional and non-lesional skin and, also in the mucosae [5]. Cutaneous hypersensitivity reactions have also been shown to be associated with increased skin permeability to substances including bacterial virulence factors such as staphylococcal protein A [6,7]. Allergy and recurrent bacterial infection are amongst the commonest reasons for consultation and treatment of dogs and cats in small animal practice. In a survey of the prevalence, diagnosis and treatment of dermatological conditions in general practice in the UK, involving 3707 small animal consultations, pruritus was the most common presenting sign (30-40% of dermatological consultations) and bacterial infections were 1) David H. Lloyd, Department of Veterinary Clinical Sciences, Royal Veterinary College Hawkshead Campus, North Mymms, Hertfordshire AL10 0EJ, United Kingdom. Tel: +44 1707 666234, Fax: +44 1707 666298. E-mail: [email protected] 254 EJCAP - Vol. 19 - Issue 3 December 2009 Dry skin commonly occurs in humans with atopy and evidence has been produced indicating that they have ceramide and sphingosine deficiencies in the lipid barrier of the epidermis. However, such deficiency does not appear to be a feature of atopy itself as comparison of uninvolved skin of atopic dermatitis patients with healthy skin has shown no difference in ceramide profiles [8]. Furthermore, in dogs, studies of water absorption-desorption in normal and atopic dogs have not shown differences suggesting that the water barrier is not affected [9]. However, electron microscopy has demonstrated abnormal intercellular lipid lamellae and reduced thickness and continuity of lipid lamellae in the stratum corneum of canine atopic skin, supporting the concept of defective barrier lipid function [10]. If sphingosine deficiency is a feature of atopic skin, this may favour colonisation by pathogenic staphylococci since sphingosine has potent antimicrobial activity against S. aureus [11]. Staphylococcal activity could also cause or enhance damage to the epidermal barrier in various ways. For instance, ceramidase from S. aureus can cause hydrolysis of ceramides in atopic skin whilst IL-4 from T helper type 2 (TH2) cells in atopic skin has been shown to suppress ceramide production in human epidermal sheets and induce synthesis of fibronectin, an adherence target of staphylococci [12]. Once established at the skin surface a staphylococcal biofilm may become established, as in bacterial overgrowth, promoting adherence and toxin production. Thus bacterial action may be able to further reduce barrier function and promote changes in the epidermis favouring colonisation and infection in atopic skin. Thus confirmation of the presence and type of infection is an important part of the diagnostic process. The great majority of bacterial skin infections involve grampositive organisms and particularly the coagulase positive staphylococci. The commonest of these is Staphylococcus pseudintermedius which represents over 90% of infections. This new species was first described in 2005 and was formed by the division of isolates previously known as S. intermedius into 2 species [13]. The name S. intermedius is now applied to isolates that are principally found in pigeons. Infections with S. aureus are relatively uncommon (around 5% or less). S. schleiferi coagulans and S. schleiferi schleiferi (coagulase negative) are less often recognised as causes of infection, but are found particularly in otitis and in certain regions [14]. S. hyicus is occasionally implicated. Other coagulase-negative staphylococci are rarely involved and normally only if immunity is greatly reduced or when implants are used. Gram-negative bacteria are sometimes found in pyoderma, particularly when lesions are moist. Organisms such as Proteus and coliforms may be secondary invaders that fail to persist when more significant pathogens are removed. Pseudomonas aeruginosa is more serious and requires specific therapy [15]. Deep infections are much less common but are more serious and can involve a wide variety of organisms including staphylococci, Nocardia and Actinobacillus and mycobacteria. Anaerobic infections are particularly associated with faecal contamination and may involve Actinomyces spp., Clostridium spp., Peptostreptococcus spp., Bacteroides spp., Fusobacterium spp., and Prevotella spp. [16]. A further cause of damage to the skin leading to microbial infections in allergic dogs and cats is self-inflicted trauma caused by pruritus. Pruritus is one of the primary signs in allergy and is also a consequence of surface and superficial microbial infections. Thus a vicious circle can readily occur in allergic animals causing an itch-scratch cycle and exacerbating the disease. The Diagnostic Approach Cytology of exudate or aspirates of lesions will commonly confirm the presence of bacteria and a neutrophilic exudate. Cocci will normally be staphylococci but occasionally streptococci. Rods are normally gram-negative. Evidence of phagocytosis is good evidence of infection but is not always present. Cytology may be supported by culture to confirm bacterial identity and provide sensitivity data. Cultures are essential in severe, recurrent or nonresponsive cases, and where there is a recognised problem with highly resistant organisms in the area where the affected animal resides. In deep pyoderma, samples of exudate or tissue obtained from deep lesions by biopsy or aspiration may be required. Other diagnostic procedures are necessary to investigate concurrent underlying problems which could reduce immunity and promote infection, in addition to allergic skin disease Allergic skin diseases are common but may be difficult to diagnose. Even when an accurate diagnosis has been established they may be difficult to control and require continual therapy. The consequences of inadequate control in many dogs and cats are recurrent microbial overgrowth, pyoderma and otitis. These diseases require repeated or long-term therapy with topical and systemic antimicrobial agents, incurring cost and the risk of acquiring resistant organisms. This review focuses on the diagnosis and management of pyoderma and microbial overgrowth with an emphasis on monitoring and prompt therapy that will minimise infection and reduce the use of antimicrobials. Pyoderma in Dogs Canine pyoderma can be conveniently considered according to the depth of infection within the skin (Tab. 1). Not all forms of pyoderma are predisposed by allergic skin disease. Pyoderma Pyoderma in its various manifestations is one of the commonest problems in small animal practice. Particularly in dogs, cases are often chronic or recurrent and cause considerable suffering. Although “pyoderma” literally means “pus in skin” the term is generally used to denote bacterial infections where pus may not always be visible macroscopically. However, many conditions in addition to bacterial infection can result in accumulation of pus, including some fungal infections and autoimmune disease. Surface pyoderma This involves damage and bacterial proliferation only in the outermost layers of the skin and can normally be resolved with minimal antibacterial therapy provided that underlying problems are identified and resolved. Skin immunity is not compromised. 255 Microbial diseases secondary to allergic skin disease – clinical significance and control - D. H. Lloyd Skin fold pyoderma is associated with irritation and lack of ventilation between skin folds. Bacteria other than the pathogenic staphylococci may also be involved and Malassezia populations may be raised as in microbial overgrowth which is described below; demodicosis is an important differential diagnosis. The occluded skin is moist, erythematous and may be malodorous, especially in the lip folds. Exudate may sometimes be seen flowing from affected folds (Fig. 2). The clinical appearance is diagnostic in almost every case and can be confirmed by tape strip cytology. If in doubt, histopathology should be carried out. Surface pyoderma • Acute moist dermatitis (pyotraumatic dermatitis, “hot spots”) • Skin fold pyoderma (intertrigo) Superficial pyoderma • • • • • Impetigo (“puppy pyoderma”)* Superficial spreading pyoderma Superficial folliculitis Mucocutaneous pyoderma* Dermatophilosis* Treatment of surface pyoderma is based on normalising the surface microbial populations. In acute moist dermatitis, prevention of further trauma is essential and will sometimes allow healing without further therapy. It is important to ensure that there is no underlying folliculitis or furunculosis. Recovery is normally rapid. However, lesions are often painful and topical therapy, requiring direct contact with skin, can be hazardous. Topical antibiotic and steroid gels or creams are effective but spraying with a soothing, antimicrobial, astringent preparation [17] has been shown to be as effective and is likely to be less dangerous. Lesions should be substantially healed in 7-10 days. Where there is marked pruritus, glucocorticoids may be required and can be given conveniently systemically, or topically using hydrocortisone aceponate spray. Treatment of fold pyoderma can be carried out as described below for microbial overgrowth. Surgery to remove the folds is effective where this is feasible. Deep pyoderma • Muzzle folliculitis and furunculosis “canine acne”)* • Pyotraumatic folliculitis and furunculosis • Localised deep pyoderma (nasal, pedal, pressure point and acral lick pyoderma,)* • Generalised deep pyoderma* • Bacterial granuloma* Tab. 1 Classification of Canine Pyoderma *Not normally associated with allergic skin disease. Acute moist dermatitis commonly occurs when self-inflicted damage disrupts the epidermis and allows proliferation of grampositive and gram-negative bacteria. It commonly occurs in flea allergy. Moist, painful, focal area(s) of erythema and hair loss, often on the gluteal region, arise within hours (Fig. 1). Diagnosis is based on the characteristic history and clinical signs. Some cases may also involve deeper infection (pyotraumatic folliculitis and furunculosis). After cleansing, look for satellite papules and pustules which are indicative of this syndrome. If in doubt or the lesion does not resolve quickly, histopathology should be carried out. Superficial Pyoderma This involves infection of the epidermis, often affecting the hair follicle epithelium. Superficial folliculitis is very common. It is characterised by focal erythema, papules and pustules centred on hair follicles and is usually very pruritic. Pustules give rise to thin scabs Fig. 2 Exudate can be seen flowing from the facial folds of this bulldog with fold pyoderma and atopy. Fig. 1 Acute moist dermatitis affecting the thigh of a dog with fleabite hypersensitivity. 256 EJCAP - Vol. 19 - Issue 3 December 2009 can be reduced to once or twice a week; in winter weekly to monthly shampooing may be sufficient to maintain remission. Glucocorticoids should be avoided as they can mask clinical signs which enable the clinician to judge when to stop antimicrobial therapy; they may also impair the immune response. Where there is recurrent infection and underlying causes cannot be controlled, long-term treatment options need to be considered. Regular use of antibacterial shampoo may give control. Otherwise, the main options are pulse therapy with antibiotics and staphylococcal vaccination. Vaccination is a better choice. Well-prepared autogenous vaccines (bacterins) are effective in up to 50% of cases; responding dogs may not need other therapy [18]. An American bacterial lysate prepared from S. aureus, has also been shown to reduce the frequency of folliculitis and decrease the need for repeated antibiotic therapy [19]. Pulse or continual low dose therapy [20] should be a last resort as it may promote development of antimicrobial resistance and acquisition of more resistant bacteria. Fig. 3 Papules and pustules affecting the ventral abdomen of a dog with recurrent superficial pyoderma. and may spread centrifugally. Loss of the scab may leave a circular epidermal collarette. Lesions often occur on the ventral areas, axillae, medial surfaces of the thighs and groin (Fig. 3). Lesions of the trunk are associated with focal areas of hair loss and in shorthaired dogs these are apparent as focal areas of alopecia, so-called ‘shorthaired dog pyoderma’. Clinical signs are characteristic but other causes of pustular disease (e.g. demodicosis, dermatophytosis, impetigo, pemphigus foliaceous, sterile eosinophilic pustulosis, subcorneal pustular dermatosis) need to be considered. Cytology demonstrating a neutrophilic exudate and bacteria and or biopsy may be used to confirm the diagnosis. The increasing recognition of meticillin-resistant strains of S. aureus (MRSA) and recently of meticillin-resistant S. pseudintermedius (MRSP) in dogs and cats is a problem that requires vigilance when treating pyoderma [21, 22]. These organisms can be resistant to a wide range of antimicrobials and may be acquired from infected or carrier individuals when animals are being treated with agents to which they are resistant. Owners and veterinary staff may become carriers. S. schleiferi schleiferi and S. schleiferi coagulans that are meticillin-resistant are also sometimes isolated in canine pyoderma, particularly in certain countries, but are generally less resistant than MRSA or MRSP [23]. Thus antimicrobial sensitivity tests should be carried out whenever the identity and sensitivity of infecting organisms cannot be predicted or when treatment does not yield the expected response. Superficial spreading pyoderma is a syndrome seen in association with superficial folliculitis and with similar underlying causes. The pathogenesis is not understood but may relate to production of exfoliative toxin by S. pseudintermedius. Erythematous macules give rise to expanding erythematous rings with borders formed by thin, peeling crusts. Lesions generally occur in relatively hairless, intertriginous zones. Diagnosis and treatment is as for superficial folliculitis. Deep Pyoderma This is rarer and generally involves much more threatening infections. Occurrence of such diseases often indicates presence of more severe localised or generalised predisposing causes compared with superficial pyoderma. Only those conditions likely to be associated with allergic skin disease are described here. Treatment of superficial folliculitis. Normally systemic antimicrobial therapy is used and the registered doses based on accurate weights of the affected animals will be effective in uncomplicated cases. Bacteriostatic antibiotics can be used but bactericides are likely to be more effective. Treatment for at least one week beyond clinical cure is advisable and drug regimens facilitating compliance, e.g. with palatable tablets, should be chosen if possible. In cases of adverse food reaction/dietary hypersensitivity care should be taken to avoid flavourings or capsules that contain substances to which the affected animal may be sensitive. Deep folliculitis and furunculosis involves infection of both hair follicles and the dermis with rupture of hair follicles and consequent exposure of hair fragments to dermal inflammatory mechanisms leading to foreign body reactions (foreign body granuloma). Furunculosis is indicated by the presence of large papules or nodules and thicker crusts, dark lesions suggesting haemorrhage and or necrosis, and by presence of pus, which may be haemorrhagic, draining from fistulae (Fig. 4). In longhaired dogs, extent and severity of lesions may be disguised by the coat. Recovery may be promoted by use of antibacterial shampoos containing chlorhexidine or benzoyl peroxide, which aid removal of crusts and reduce surface bacterial populations. Mild superficial pyoderma can be treated with such shampoos without systemic antibiotic but this is labour-intensive; shampooing every 2-3 days is required. Once lesion resolution occurs, shampooing Bacteria other than the pathogenic staphylococci are more often present, particularly gram-negatives including coliforms, Pseudomonas and Proteus spp. A variety of underlying factors may be involved and must be thoroughly investigated; 257 Microbial diseases secondary to allergic skin disease – clinical significance and control - D. H. Lloyd Fig. 4 Nodular lesions with haemorrhagic crusts on the limb of a dog with deep pyoderma. Fig. 5 Microbial overgrowth affecting the foot of a boxer; all four feet were affected. The dog alo suffered from recurrent superficial pyoderma. hypothyroidism and demodicosis are common but in some instances no cause may be found. Cytology, culture and sensitivity, blood screens and biopsy will be required in most cases. Deep fungal infection may be involved and thus both fungal and bacteriological cultures should be requested. Pyoderma in Cats Cats occasionally develop superficial and deep pyoderma in dogs but seem much more resistant to these diseases. Essentially the same processes of diagnosis are used. Skin infections in cats are most commonly abscesses, which occur following bite wounds. Pyotraumatic folliculitis and furunculosis presents as acute moist dermatitis but concealing deeper infection. Lesions commonly occur on the cheeks and neck and in young dogs, particularly in retrievers, St. Bernards and Newfoundlands. Histopathology is advisable to confirm the nature of infection; underlying causes including allergy should be investigated. Microbial overgrowth Bacterial overgrowth is a newly described skin condition of dogs characterised by the presence of substantially increased populations of bacteria, particularly Staphylococcus pseudintermedius [24]. Commonly, the yeast Malassezia pachydermatis is also present and in such cases the term “microbial overgrowth” is appropriate. When only M. pachydermatis is present the condition is equivalent to Malassezia dermatitis [25]. However, bacterial overgrowth and microbial overgrowth occur much more commonly and in a wider range of clinical situations than has been classically described for Malassezia dermatitis. These conditions are often an unrecognised cause of pruritus, particularly in occluded areas such as the pedal webs. They commonly occur in atopy or other allergic dermatoses and successful treatment will often greatly reduce the measures needed to bring pruritus under control. Failure to recognise the microbial cause may lead to inappropriate and excessive prescription of anti-inflammatory drugs. Treatment of deep pyoderma. It is essential to correctly identify the causative bacteria and use appropriate systemic antimicrobial therapy, selecting bactericidal drugs if possible and ensuring compliance. Registered doses are effective but commonly higher doses are used in more severe cases. Systemic antimicrobial treatment is given for a period at least two weeks beyond clinical resolution of the lesions. Recovery may be promoted by the use of topical antimicrobial shampoos containing chlorhexidine or benzoyl peroxide every two to three days. This is aided by clipping the coat which allows easier access to the affected skin and can promote compliance as the owners are able to see the extent and severity of the disease. Continuing use of antibacterial shampoos may help to prevent recurrence and vaccines may be helpful in recurrent cases but seem less effective than in superficial pyoderma. Aetiology and pathogenesis Bacteria. Bacteria generally maintain low populations on healthy skin as a consequence of the unfavourable surface microenvironment and defensive measures maintained by the skin [2]. When the skin is damaged or its defences are impaired bacterial adherence to the keratinocytes is promoted and the bacteria are able to proliferate. The pathogenic staphylococci and, in dogs, particularly S. pseudintermedius (formerly S. intermedius) seem especially able to take advantage of such changes. When high local cell densities (biofilm formation) of staphylococci are established, quorum sensing can take place. If the pyoderma fails to respond to antimicrobial therapy despite evidence of compliance with an appropriate treatment regimen, cytology and cultures should be repeated and biopsy specimens submitted for histopathology, ensuring that infected tissue deep within the lesions is sampled. In all cases of deep pyoderma it is very important to identify and resolve underlying causes. Treatment with glucocorticoids is contraindicated. 258 EJCAP - Vol. 19 - Issue 3 December 2009 This is a mechanism in which cell density signals are exchanged amongst the staphylococci when population sizes reach a certain threshold allowing them to initiate the production of toxins that can irritate and damage the skin [26]. Once toxin production has been initiated, more cutaneous damage is induced and immunity may be further impaired leading to a vicious circle of damage and bacterial proliferation. treatment of microbial overgrowth will often permit other underlying pruritic or inflammatory diseases to be identified. Unless such underlying problems are identified and controlled, overgrowth is likely to recur. Treatment and Control The condition normally responds to topical therapy with antimicrobial shampoos containing chlorhexidine, or chlorhexidine and miconazole that are active against staphylococci and Malassezia. Benzoyl peroxide shampoo can also be used. Shampooing every 2-3 days for 2 weeks will normally bring the condition under control. Then treatment once or twice a week is usually sufficient. An astringent, soothing antimicrobial spray has also been shown to be a convenient and effective treatment for microbial overgrowth [24], especially in areas that are localised or difficult to reach. It can also be used for prophylaxis in recurrent cases. In severe or extensive cases of microbial overgrowth or when washing/spraying of the affected areas is not practicable, systemic therapy with cefalexin at 15 mg/kg twice daily [29] and or imidazoles (if Malassezia is present) can be very helpful, depending on the nature of the microbes involved. Ketoconazole (5-10 mg/kg twice daily with food) or itraconazole (5 mg/kg twice daily or 10 mg/kg once daily) are effective when used for 2-4 weeks. Malassezia. M. pachydermatis is present as a commensal of the skin and mucosae of most dogs. In healthy animals it exists at higher population densities at the lips and interdigital skin than at the ears [27]. The anus seems to be the most frequently colonised mucosal site. M. pachydermatis acts as an opportunistic pathogen and factors promoting its pathogenicity may include increased temperature and humidity, excessive lipid secretion, intercurrent diseases, and therapy with antibiotics and glucocorticoids; however, this remains controversial [28]. Breed-related factors are important in Malassezia dermatitis; basset hounds and West Highland white terriers are particularly predisposed. Since S. pseudintermedius and M. pachydermatis are inhabitants of the mucosae, including the oral cavity, they will continually be transferred to the skin, particularly in areas which require cleaning or grooming, and which are pruritic. Thus there is potential for the establishment of microbial overgrowth whenever the skin is damaged or there is underlying disease impairing cutaneous function. Whatever treatment is used, it is important to monitor response and adjust the nature and frequency of treatment as necessary. This can be quickly and easily be achieved using tape strip specimens stained with DiffQuik. Clinical Features Microbial overgrowth is characterised by the presence of erythema, greasiness or exudation, pruritus and saliva staining in the absence of papules and pustules. Pruritus may be quite marked. Owners may be unaware of the lesions and careful clinical examination with good illumination is necessary. In chronic or severe lesions there may be excoriation and lichenification. There is commonly malodour, especially when Malassezia is involved. Overgrowth is normally seen in areas of skin that are moist or occluded such as the lips, between the pads and digits, in the groin, perivulvar and perianal areas, on the ventral abdomen, in the axillae, on the pinnae of the ears, and in skin folds. It is frequently present in dogs with allergic skin disease. It can be very localised or may affect several sites on a dog. Microbial Overgrowth in Cats Overgrowth of bacteria and Malassezia in cats is relatively rare but increasingly recognised [30]. It is suggested that Malassezia spp. overgrowth may represent a secondary cutaneous problem in allergic cats with greasy adherent brownish scales. Favourable response to treatment with imidazole antifungal treatments alone suggests that, as in dogs, Malassezia spp. may be partly responsible for both pruritus and cutaneous lesions in such cats [31]. Devon rex cats appear to be particularly prone to Malassezia dermatitis. Conclusions Diagnosis Microbial overgrowth should be suspected when pruritus occurs and compatible lesions are present, even if they are mild. Diagnosis is confirmed by cytology using tape strip samples, glass slide impressions or swab smears stained with DiffQuik showing elevated populations of bacteria or Malassezia. Tape strips are preferred because they organisms are sometimes not located at the surface of the lesions and repeated application of the tape to the same site will reveal deeper populations. The technique is quick and easy to perform and, with experience, tapes can be examined in the microscope and diagnosis made within 2-3 minutes. The presence of numbers of bacteria above 5 or Malassezia above 2 per high power x1000 oil immersion field is suggestive of microbial overgrowth. Commonly populations are very much higher but the organisms may be found in clusters so at least 20 high power fields should be examined. Successful The microbial infections associated with allergic skin disease can be effectively treated with antimicrobial drugs and, if the allergy is brought under good control, may cease to be a problem. Where only partial control is achieved, vaccines, and topical antimicrobial therapy with shampoos and sprays, may enable recurrence to be minimised. Emerging problems with multi-resistant bacteria emphasise the need to reduce the duration of use antimicrobials. This can be done by selecting the most effective appropriate antimicrobial with the aid of culture and sensitivity tests and ensuring good compliance in the treatment regimen, so that exposure of the animal to systemic antimicrobial agents ceases as soon as the lesions have resolved and the one or two-week extra treatment periods specified for superficial and deep pyoderma have been observed. 259 Microbial diseases secondary to allergic skin disease – clinical significance and control - D. H. Lloyd In cases of recurrent pyoderma, pulse therapy or continual low dose therapy should be avoided if at all possible and further efforts made to identify and correct underlying problems. the American Veterinary Medical Association. 2003; 222: 451-4. [15] Hillier A, Alcorn JR, Cole LK, Kowalski JJ. Pyoderma caused by Pseudomonas aeruginosa infection in dogs: 20 cases. Veterinary Dermatology. 2006; 17: 432-9. [16] Scott DW, Miller WH, Griffin CE. (2001) Bacterial skin disease. In: Muller and Kirk’s Small Animal Dermatology 6th ed. Philadelphia, WB Saunders Company. 2001, pp. 274-335. [17] Ascher, Madin, Guaguere et al. Intérêt d’une solution topique non antibiocorticoide dans le traitement de la dermatite pyotraumatique du chien. Pratique Médicale et Chirurgicale de l’Animal de Compagnie. 1995; 30: 345-54. [18. Curtis CF, Lamport AI, Lloyd DH. Masked, controlled study to investigate the efficacy of a Staphylococcus intermedius autogenous bacterin for the control of canine idiopathic recurrent superficial pyoderma. Veterinary Dermatology. 2006; 17: 163-8. [19] DeBoer DJ, Moriello KA, Thomas CB, Schultz KT (1990) Evaluation of a commercial staphylococcal bacterin for management of idiopathic recurrent pyoderma in dogs. American Journal of Veterinary Research. 1990; 51: 636-9. [20] Carlotti D-N, Jasmin P, Gardey L, Sanquer A. Evaluation of cephalexin intermittent therapy (weekend therapy) in the control of recurrent idiopathic pyoderma in dogs: a randomized, doubleblinded, placebo-controlled study. Veterinary Dermatology. 2004; 15 (s1): 8-9. [21] Loeffler A, Linek M, Moodley A, Guardabassi L, Sung JML, Winkler, M, Weiss R, Lloyd DH. First report of multi-resistant, mecA-positive Staphylococcus intermedius in Europe: 12 cases from a veterinary dermatology referral clinic in Germany. Veterinary Dermatology. 2007: 18; 412-21. [22] Leonard FC, Markey BK. Meticillin-resistant Staphylococcus aureus in animals: a review. Veterinary Journal. 2008; 175: 27-36. [23] Jones RD, Kania SA, Rohrbach BW, Frank LA, Bemis DA. Prevalence of oxacillin- and multidrug-resistant staphylococci in clinical samples from dogs: 1,772 samples (2001-2005). Journal of the American Veterinary Medical Association. 2007; 230: 221-7. [24] Pin D, Carlotti D-N, Jasmin P, DeBoer DJ, Prelaud P. Prospective study of bacterial overgrowth syndrome in eight dogs. Veterinary Record. 2006; 158: 436-41. [25] Bond R, Ferguson EA, Curtis CF, Craig JM, Lloyd DH. Factors associated with elevated cutaneous Malassezia pachydermatis populations in dogs with pruritic skin disease. Journal of Small Animal Practice. 1996; 37: 103-7. [26] Sung JML, Chantler PD, Lloyd DH. The accessory gene regulator locus of Staphylococcus intermedius. Infection and Immunity. 2006; 74: 2947-56. [27] Bond R, Saijonmaa-Koulumies L, Lloyd DH. Population sizes and frequency of Malassezia pachydermatis at skin and mucosal sites in healthy dogs. Journal of Small Animal Practice. 1995; 36: 14750. [28] Guillot J, Bond R. Malassezia pachydermatis: a review. Medical Mycology. 1999; 37: 295-306. [29] Jasmin P, Pin D, Carlotti DN. Efficacy and interest of a systemic antibiotic treatment with cephalexin in dogs affected with bacterial overgrowth (BOG). Proceedings of the 7th FECAVA and 47th Annual Congress of the FK-DVG, Berlin, October 2001, p. 51. [30] Ordeix L, Galeotti F, Scarampella F, Dedola C, Bardagí M, Romano E, Fondati A. Malassezia spp. overgrowth in allergic cats. Veterinary Dermatology. 2007; 18: 316-23. [31] Ahman S, Perrins N, Bond R. Treatment of Malassezia pachydermatis-associated seborrhoeic dermatitis in Devon Rex cats with itraconazole - a pilot study. Veterinary Dermatology. 2007; 18: 171-4. Acknowledgements The author is most grateful to colleagues of the Royal Veterinary College, London, Dermatology Unit for providing illustrations used in this review. References [1] [2] [3] [4] [5] [6] [7] [8] [9] [10] [11] [12] [13] [14] Elias PM. The skin barrier as an innate immune element. Seminars in Immunopathology. 2007; 29: 3-14. Lloyd DH. The canine skin microbiota: habitats, acquisition, interactions and exchange. European Journal of Companion Animal Practice. 2008; 18: 61-8. Hill PB, Lo A, Eden CA, Huntley S, Morey V, Ramsey S, Richardson C, Smith DJ, Sutton C, Taylor MD, Thorpe E, Tidmarsh R, Williams V. Survey of the prevalence, diagnosis and treatment of dermatological conditions in small animals in general practice. Veterinary Record. 2006; 158: 533-9. Matsui K, Nishikawa A, Suto H, Tsuboi R, Ogawa H. Comparative study of Staphylococcus aureus isolated from lesional and nonlesional skin of atopic dermatitis patients. Microbiology and Immunology. 2000; 44: 945-7. Saijonmaa-Koulumies, L.E., Lloyd, D. H. Colonisation of the canine skin with bacteria. Veterinary Dermatology. 1996; 7: 153-63. Mason IS, Lloyd, DH. The role of allergy in the development of canine pyoderma. Journal of Small Animal Practice. 1989; 30: 216-8. Mason IS, Mason KV, Lloyd DH. A review of the biology of canine skin with respect to the commensals Staphylococcus intermedius, Demodex canis and Malassezia pachydermatis. Veterinary Dermatology. 1996; 7: 119-32. Farwanah H, Raith K, Neubert RH, Wohlrab J. Ceramide profiles of the uninvolved skin in atopic dermatitis and psoriasis are comparable to those of healthy skin. Archives for Dermatological Research. 2005; 296: 514-21. Chesney CJ. The microclimate of the canine coat: The effect of heating on coat and skin temperature and relative humidity. Veterinary Dermatology. 1997; 8: 183. Inman AO, Olivry T, Dunston SM, Monteiro-Riviere NA, Gatto H. Electron microscopic observations of stratum corneum intercellular lipids in normal and atopic dogs. Veterinary Pathology. 2001; 38: 720-723. Arikawa J, Ishibashi M, Kawashima M, Takagi Y, Ichikawa Y, Imokawa G. Decreased levels of sphingosine, a natural antimicrobial agent, may be associated with vulnerability of the stratum corneum from patients with atopic dermatitis to colonization by Staphylococcus aureus. Journal of Investigative Dermatology. 2002; 119: 433-9. Hatano Y, Terashi H, Arakawa S, Katagiri K. Interleukin-4 suppresses the enhancement of ceramide synthesis and cutaneous permeability barrier functions induced by tumor necrosis factoralpha and interferon-gamma in human epidermis. Journal of Investigative Dermatology. 2005; 124: 786-92. Devriese LA, Vancanneyt M, Baele M, Vaneechoutte M, De Graef E, Snauwaert C, Cleenwerck I, Dawyndt P, Swings J, Decostere A, Haesebrouck F. Staphylococcus pseudintermedius sp. nov., a coagulase-positive species from animals. International Journal of Systematic and Evolutionary Microbiology. 2005; 55: 1569-73. Frank LA, Kania SA, Hnilica KA, Wilkes RP, Bemis DA. Isolation of Staphylococcus schleiferi from dogs with pyoderma. Journal of 260 DERMATOLOGY Flea control in flea allergic dogs and cats Marie-Christine Cadiergues(1) SUMMARY Flea allergy dermatitis (FAD) remains the most common allergic skin disease of dogs and cats, although its frequency varies according to geographical location. Despite the availability of safe, effective products, treating FAD remains a challenge. This challenge should be more readily overcome once both practitioner and owner(s) are entirely convinced of the diagnosis. The main difficulties and pitfalls facing the practitioner are described. Treatment requires appropriate knowledge of the flea life cycle and flea-related biology, and understanding of the mode of action of the relevant flea control products. An integrated approach to treatment should be adopted, involving all the players in the flea life cycle - the FAD patient, all in-contact pets, and the environment. Each case must be customised, with effective flea control products used in combination with cleaning measures such as steaming, vacuuming and regular grooming. The vet should ensure that the client understands these relevant basic principles of flea biology. This paper was commissioned by FECAVA for publication in EJCAP. Host phase The adult stage of both Ctenocephalides felis felis and Ctenocephalides canis (also called cat flea and dog flea respectively), lives permanently in the hair coat of its host. Exchanges between animals are possible but limited, and should not be considered the main source of infestation. Fleas have a tendency to leave their host when the host’s temperature decreases (e.g. death, anaesthesia), when the species is not well adapted to the host (e.g. C. canis in cats) or when the on host population is extremely high [2]. Introduction Flea allergy dermatitis (FAD) remains the most common allergic skin disease of dogs and cats, although its frequency varies according to geographical location. The past twenty years have brought important advances in flea biology as well as better insecticides [1]. Nevertheless, flea control in general, and more specifically in dogs and cats with FAD, remains a real challenge for vets. Early onset of blood feeding Once the adult (imago) has colonised a new host, it will take its first blood meal very rapidly. About 25% of cat fleas start to feed within 5 minutes of being free in the coat and about 97% have taken a blood meal within 1 hour [3]. Although C. canis takes its meal more slowly, 72.5% of fleas begin blood feeding within one hour [4]. The mean duration of the first blood meal, evaluated on individual fleas confined on animals, has been found to be 25± 18 minutes in females C. felis and 11± 8 minutes in males C. Felis [3]. It was significantly shorter (5 and 6 minutes, respectively for C. canis) [4]. These data demonstrate the difficulty if not the impossibility of preventing newly emerged fleas from taking a blood meal and hence injecting their saliva. This paper will be divided into four sections. The first will focus on flea biology on which flea control programmes are based. In the second, the main difficulties and pitfalls facing practitioners will be described. The third section will outline the various active ingredients and formulations currently available.The last chapter will consider specific flea control recommendations. Flea biology and flea control Various aspects of flea biology may be useful in improving flea control and/or understanding failure or inadequacy of flea control programmes. 1) Marie-Christine Cadiergues, DrMedVet, DipECVD, PhD, MRCVS, Groupe de Recherches Animaux de Compagnie- Ecole Nationale, Vétérinaire de Toulouse, 23 chemin des Capelles 31076 Toulouse cedex France. E-mail: [email protected] 261 EJCAP - Vol. 19 - Issue 3 December 2009 Blood feeding and lifespan Although it is clearly established that blood-feeding is necessary for mating and laying viable eggs [2], the number of blood meals and their frequency remain unknown. It is thought that fleas will continue to bite and have blood meals until they die. The lifespan of C. felis felis is usually considered to be between 2 and 3 weeks. Under experimental conditions, mean survival of C. canis in the canine coat was 8.6 days [5]. Clearly, flea lifespan depends highly on the level of grooming (by the animal itself or the owner). Survival of 250 unfed fleas of both species was evaluated in the environment at 19°C and 27°C (RH 70%). Mean survival of 50% of C. canis was 15.9 days (19°C) and 9.0 days (27°C). Under similar conditions, mean survival of C. felis was 11.7 days (19°C) and 9.6 days (27°C). After 48 hours on a dog, mean survival of females was 7.9 days (19°C) and 4.8 days (27°C) for C. canis and 4.9 days (19°C) and 3 days (27°C) for C. felis. Survival of males was shorter [5]. formed out of various bits of environmental debris stuck together. Pupae are often found in well-protected areas such as the back of carpets, skirting boards and cushion seams. Inside, the future imagos remain dormant for several months (the so-called “pupal window”) until stimulated to hatch by triggers such as vibrations, increased carbon dioxide levels and/or temperature changes. Pupae are resistant to freezing, desiccation, insecticides and IDIs. First eggs Female fleas lay their first eggs between 24 and 36 hours after colonising a host. Eggs are laid in the coat and subsequently fall to the ground. They are then susceptible to insect development inhibitors (IDIs) applied on the coat or on the ground, as well as insecticidal products. Egg production reaches a peak (around 15-20 eggs per day) during the second and third weeks and then decreases, but a female will lay eggs until it dies. Cat flea egg production usually peaks during the night, coinciding with normal sleep periods for indoor pet dogs and cats [6], hence a higher density of immature stages in animal resting places, including bedrooms. Around areas such as sofas and beds, where pets jump and play, eggs and flea faeces will be more easily dislodged from the haircoat [6]. Preventing a new life cycle would require killing all the adults in the first 24-36 hours of infestation and/or applying an IDI either to the adult or to the immature stages before pupa formation. Vacuuming is not very effective due to the mobility and positive geotaxis of the larvae. Although immature stages concentrate in rooms or areas where animals spend most of their time, it is crucial to take into account places visited infrequently or visited by other animals including wildlife. Imago Once stimulated, the imago tears open the cocoon, probably as a consequence of its agitated movements, and jumps onto the first mobile, warm “object”, usually an animal. The young, unfed adult is susceptible to adulticides and IDIs. As stated earlier, the unfed flea survives longer in the environment than fed fleas. The entire life cycle can be completed in 13 to 14 days under optimal conditions but can take up to 7-9 months. Main difficulties and pitfalls Convincing the owner and customising flea control measures Surprisingly, one major difficulty in FAD control is convincing the owner (and sometimes the referring practitioner) that FAD is the correct diagnosis. It is rather common to be faced with owner disbelief or scepticism. Because fleas are not seen by the owner, and their presence is difficult to prove on animals with FAD, the owner is sometimes absolutely convinced that fleas cannot be the cause of his/her pet’s dermatitis. Some people associate fleas with a lack of hygiene and cannot accept that their pet(s) might have fleas. Other people, who recognise fleas in dogs to be common, doubt that their pet would present with a flea-related skin disease when other pets with fleas do not have a skin problem? Furthermore, why should pruritus be so severe if only a few fleas are present? Owners may be sceptical because they think, or have been told, that they are doing everything they can to kill fleas and/or that they have used the wonder product. Environmental phase and factors affecting egg production Once on the ground, eggs require favourable environmental conditions (humidity and temperature) to develop further. Ideal conditions for the life cycle of the cat flea (relative humidity of 70% and a temperature of between 20 and 30°C) are provided by a modern home environment. The environmental phase has major implications in control because larval and pupal stages develop there and because pupae remain dormant in the environment for an extended period of time. Larval instars The first-instar larvae hatch from eggs in the pet’s immediate environment. They then tend to move to the base of the carpet, not travelling far from where they hatched. They search for suitable food, particularly dried blood faeces [6] but also other debris including non-viable flea eggs [7]. The second-instar larvae tend to search more widely for food and darker areas where they are less likely to be disturbed. They tend to move away from carpets, making vacuuming, which only removes 15-27% of the larvae, a rather ineffective procedure. However, regular vacuuming of pet resting places can remove 90% or more of flea eggs as well as flea faeces [6]. Clinical features, at least in dogs, may help to convince a sceptical owner. These include a typical dorso-lumbar distribution pattern extending to the tail base, perineum and medial/caudal thighs, and crusted papules in the umbilical fold (especially in male dogs). The presence of fipropruritic nodules is also highly suggestive. The client might accept the diagnosis more readily if given clear and simple explanations about both allergy in general and flea allergy in particular. Emphasising the difference between flea infestation and flea allergy, and outlining the role of flea saliva and therefore that of flea bites is important. Describing the life cycle in relation to the pet’s individual circumstances may help the owner to understand why fleas are still present. Additional Pupal stage The third-instar larva becomes a pupa encased within a cocoon 262 Flea control in flea allergic dogs and cats - Marie-Christine Cadiergues testing and strict trial flea control for 6 weeks might finally convince the owner. Swimming, bathing and excessive grooming Dogs that swim or bathe regularly should receive systemic treatment (e.g. nitenpyram once daily or every other day, selamectin once monthly) as swimming or bathing degrades the efficacy of topical products. Spinosad, a new oral, beef-flavoured tablet for dogs, not yet available in Europe, would also be a product of choice as it kills fleas rapidly and remains effective for one month after application. Cutaneous inflammation, hyperhydrosis, cornification disorders (primary and secondary) and excessive grooming should be considered when applying a topical flea product. Not only may the product irritate the skin but its diffusion may also be impaired by the skin changes. Excessive grooming might reduce the amount of insecticide present on the skin thereby reducing or delaying its efficacy. Once convinced, the owner needs guidance and motivation. Again, a clear explanation of the flea life cycle combined with information on the way products work is usually helpful. Demonstrating how to apply the product(s) correctly is recommended; a small area on the skin of the back of the neck could be shaved to ensure that a spot-on formulation is applied onto the skin and not in the fur. The therapeutic regimen should always be customised, necessitating a thorough patient history and details of the owner’s circumstances. In-contact animals and premises All the in-contact animals should be treated, albeit less strictly perhaps that the patient with FAD. Cats, especially, are easily forgotten either because they live outdoors or because they may not be around when it is time to treat the dog(s). Cats can also be difficult to medicate and are sometimes not considered by owners to be part of the problem. All areas regularly visited by the pet with FAD (including cars and sheds) should be treated with a suitable product at an appropriate frequency. Visiting pets inadequately treated for fleas, represent a risk as they can re-introduce fleas (mainly immature stages which can develop and lead to delayed re-infestations but possibly also adults) in a well-controlled household. Similarly, visiting infested places can trigger a flare. When such possibilities cannot be avoided, strict preventive treatment, similar to a trial therapy regimen, should be recommended. Over-the-counter products Extensive and long-term flea control measures require considerable effort and expense. This can produce a progressive reduction in compliance, and may also explain why over-thecounter (OTC) products are sometimes preferred by owners. Most OTC products do not have the efficacy, residual activity or safety profile of the veterinary products. With time, substitution of OTC products could lead to poor control of FAD, owner’ frustration or even suspicion of resistance. Active ingredients and formulations Neonicotinoids This class of insecticides was developed for crop protection and subsequently found to be highly effective for flea control in dogs and cats, with an excellent tolerance. Imidacloprid (Advantage®, Advantix®, Advocate® - Bayer Health Care), nitenpyram (Capstar® - Novartis SAS) and dinotefuran (Vectra 3D - Summit VetPharm, unavailable to date in Europe) are the active ingredients available for pets. Maintaining consistency of flea control After a while, particularly when there is clinical improvement, attention given to flea control tends to flag. However, this must not be allowed to happen. The practitioner and/or well-trained nurses from the practice must regularly emphasise the importance of consistent flea control. Reminders can be sent, using modern communication forms (text messages, Multimedia Messaging Services on mobile phones, emails). These are sometimes offered free of charge by pharmaceutical companies. Imidacloprid has a high affinity for the nicotinergic acetylcholine receptors in the post-synaptic region of the central nervous system (CNS) in insects. The ensuing inhibition of cholinergic transmission in insects results in paralysis and death of the parasite. It is only available as a spot-on with surface action. It is effective against adult fleas, requiring 8 hours of contact [9-11]. It also has, in common with most insecticidal products, a larvicidal effect [12, 13]. Combination with permethrin is likely to enhance its speed of action [14, 15]. Efficacy of ectoparasiticides [8] Controlled studies are advocated to assess the efficacy of flea control products. Classically, efficacy is determined by comparing parasite numbers on groups of treated and control animals after experimental infestations. Fleas are deposited 48 to 72 hours before the application of a product to be assessed. Immediate therapeutic efficacy is evaluated 24 or 48 hours post-treatment by combing off and counting the surviving fleas. Parasite counts 24 or 48 hours following subsequent infestation(s) at 7-day intervals are used for residual efficacy calculations. Residual efficacy is evaluated by re-infesting the animals in each study. A threshold of 90 or 95% efficacy is required. Most products with a European licence have a 95% efficacy threshold 48 hours after infestation. TEven if a product is applied according to the manufacturer’s recommendations, 100% efficacy should not, therefore, be expected. Furthermore, efficacy tends to decrease with time. Nitenpyram is a fast-acting, orally administrated flea treatment. Like imidacloprid, it acts on the nicotinic acetylcholine receptor channel. It is readily absorbed, with peak plasma levels reached within 30 minutes and a half-life of about 8 hours [16, 17]. First signs of efficacy are seen 15 minutes or more after infestation. Fleas are dislodged after 30 minutes, and within 6 hours, over 95% are killed. The effect is prolonged for 24-48 hours [17, 18]. Dinotefuran is a third generation neonicotinoid; dinotefuran was synthesised with acetylcholine as the lead compound whereas imidacloprid was based on nicotine. It is also a fast-killing insecticide, effective for 30 days following application [19]. It is 263 EJCAP - Vol. 19 - Issue 3 December 2009 available in the US as a spot-on. For dogs, it is combined with pyriproxyfen and permethrin, and for cats with pyriproxyfen only. Pyrethrins and Pyrethroids These products cause spontaneous depolarisation, augmented neurotransmitter secretion, and neuromuscular blockade by sodium and potassium ion transport disruptions in nerve membranes. Action is extremely rapid, but paralysed insects can also recover rapidly. Natural pyrethrum is extracted from chrysanthemum flowers and notable for its rapid but brief action and relatively good tolerance in dogs and cats. Synthetic pyrethroids are pyrethrum-like compounds with greater potency and residual effects. They are, however, toxic in cats. This is especially true for permethrin, a second-generation pyrethroid. Permethrin is available in several formulations and is particularly prominent in over-the-counter products, for which efficacy data are difficult to find. Among the formulations which have been extensively evaluated, spot-on formulations include a 65%-permethrin spot-on [35-37] (Defend Exspot® treatment for dogs – Schering-Plough Animal Health), combination products e.g. imidacloprid10%/permethrin 50% [14, 15] (K9 Advantix® – Bayer) and pyriproxyfen 0.3%/permethrin 40% (Duowin® Contact – Virbac). Sprays containing 2% permethrin (Defendog® – Virbac) or combination products such as pyriproxyfen 0.02%/permethrin 1.9% (Duowin® – Virbac) are also available. Efficacy against fleas was assessed in several trials. After one application, under controlled conditions, adulticidal efficacy of the imidacloprid 10%/permethrin 50% product was 99.4% (day 1), 95.7% (day 29) and 90.4% (day 36) [15]. The same formulation was assessed in a field trial at 23 centres in Germany, France and Italy on 229 dogs treated once. 134 other dogs were treated once with a topical 10% fipronil formulation. The immediate (day 2) efficacy against fleas of the imidacloprid permethrin combination vs. the control product was 98.3% vs. 97.0%. Residual efficacy (day 28) of the two products was 92.5% vs. 93.5% [14]. Phenylpyrazoles Introduced in Europe in 1994, fipronil has been a market leader ever since. First available as a spray (Frontline® spray – Merial), fipronil later became available in a spot-on formulation (Frontline® spot-on, Frontline® Top spot – Merial) eventually being combined with methoprene, still as a spot-on (Frontline® Combo, Frontline® Plus – Merial). More recently, pyriprole from the same chemical group has become available as a spot-on (Practic® - Novartis). Now that fipronil’s patent has expired, generic products have appeared on the market (e.g. Effipro® - Virbac). Phenypyrazoles block the gamma-aminobutyric acid (GABA)-gated chloride channels of neurons in the central nervous system, sharing a common binding site with cyclodienes. Fipronil also binds to two different glutamate-gated chloride channels [20, 21]. Efficacy of fipronil was evaluated in dogs [22] and cats [23] with FAD. The 10%-fipronil solution, applied monthly three times, reduced flea counts on day 90 by 98%. Pruritus was reduced or eliminated in 84% of dogs [22]. The same formulation, applied monthly to cats with FAD, reduced flea counts by 94% on day 90 with pruritus reduced or absent in 78% of cats [23]. In a study comparing efficacy of selamectin, imidacloprid and fipronil in dogs experimentally infested with both Ctenocephalides felis and C. canis, the efficacy of fipronil, 48 hours after each infestation, was 100%. This persisted for 35 days after one application [24]. In studies investigating the efficacy of a single application of a 12.5% pyriprole spot-on formulation, persistence of the active ingredient was assessed after repeated washing and shampooing. Neither shampooing 24 hours post-treatment nor weekly washes altered the efficacy which was 99.8-100% and 100%, respectively, for 30 days [25]. Metaflumizone Metaflumizone (Promeris®, Promeris®Duo – Fort Dodge) is derived from pyrazoline and acts by binding the voltagedependent sodium channels in insects. Studies in controlled environment (experimental infestations, comb-counts 48h after treatment and re-infestations) showed over 90%-efficacy for 6 weeks in dogs [38] and 7 weeks in cats [39]. Speed of kill was evaluated in adult cats and compared with a product containing a combination of fipronil-(S) and methoprene. It was found to be slower [40]. A European multicentric study was performed on 170 dogs with flea infestation, randomly allocated to one of two treatments, metaflumizone plus amitraz (minimum dosage of 20 plus 20mg/kg) or fipronil (at the recommended label rate). Both treatments resulted in consistent (>89%) reductions in flea numbers relative to baseline counts, throughout the study (8 weeks), although fipronil resulted in numerically higher reductions on each count day [41]. Avermectins Selamectin (Stronghold®, Revolution® – Pfizer) is believed to bind to glutamate-gated chloride channels in the parasite’s nervous system, increasing permeability and allowing the rapid and continued influx of chloride ions into the nerve cell. This inhibits nerve activity thereby causing paralysis [26]. Selamectin is applied topically, is rapidly absorbed through the skin, and is distributed via the blood [27]. It has activity against both internal and external parasites. Several studies have been published supporting its efficacy against fleas [10, 12, 24, 28-32]. Topical application was over 98% effective after 36 hours in dogs and 24 hours in cats [31, 32]. In dogs, mean efficacy, 3 and 8 hours after treatment, was 39.7 and 74.4%, respectively [11]. A study performed in dogs and cats with FAD housed in flea-infested, simulated home environments [33] and a multicentre field trial performed in dogs [34] both showed a significant reduction in clinical signs of FAD in dogs and cats after two applications, one month apart. The multicentre study did not show any difference between the group treated with fipronil and the group treated with selamectin. Improvement was observed after two weeks and clinical signs had almost resolved after two months [34]. Spinosad Spinosad is an aerobic fermentation product of the soil bacterium, Saccharopolyspora spinosa. Spinosad kills insects through activation of the acetylcholine nervous system through nicotinic receptors. The mode of action is unique and incompletely understood. It is available in the United States as an chewable tablet (Comfortis® – Lilly). Its efficacy against fleas 264 Flea control in flea allergic dogs and cats - Marie-Christine Cadiergues appears excellent (98-100%) [42, 43]. A recent controlled study showed that when administered to infested dogs, efficacy was 81%, four hours post-treatment. When treated animals were re-infested, efficacy was over 96% for 14 days, four hours after infestation [44]. A female flea starts laying eggs within 24-36 hours and then continues to do so for the rest of its life. Consequently, to prevent additional environmental contamination, a product which becomes effective in under 24 hours should be recommended. Adulticidal products on the animal with FAD Given what has already been said about the testing and evaluation of antiparasitic substances, and also the effects of over-grooming, excessive bathing, and skin inflammation on reducing product efficacy, it might be wise either to apply a product more frequently (for example, every 2-3 weeks) than recommended by the manufacturer or, better still, alternate every fortnight, between two different products each with a different mode of action. Juvenile hormone analogues (JHAs) The pharmacological properties of juvenile hormone analogues are characterised by mimicking the juvenile hormones of insects resulting in interference with metamorphosis and reproduction. Prevention of larval development breaks the flea life cycle. Due to specificity of juvenile hormone for insects, pyriproxyfen has virtually no effects on mammals. Two products, methoprene and pyriproxyfen, are used for flea control, either administered to the animal or applied in the environment. They are usually combined with an adulticide: fipronil (Frontline® Combo/Frontline® Plus – Merial) [45] or permethrin (Duowin®, Duowin®Contact – Virbac). A spot-on containing 1% pyriproxyfen only (Fleegard® - Bayer) [46] and a commercial diet (Virbac Vet Complex® dermatology – Virbac) containing 50 mg/kg are also available in several countries. The efficacy of insecticidal products is dose-dependent. The dose itself is time-dependent, varying according to whether the product is applied all over the body surface or to a more restricted area. Systemic products have the advantage of not being altered by any skin change/action. Similarly, applying a product all over the body (e.g. spraying in dogs), should, assuming the correct dose is given, ensure rapid and homogenous covering of the body surface with adequate amount of product. Insect developmental inhibitors (IDIs) Lufenuron (Program® - Novartis) is a systemic IDI which interferes with chitin synthesis, polymerisation and deposition [47]. Lufenuron has no effect on adult fleas. Excreted in flea faeces, it prevents normal pupation of larvae feeding on those flea faeces. Numerous studies have shown its efficacy either administered orally to dogs or cats or injected to cats [18, 28, 48-50] Treatment of in-contact-animals All must be treated, including cats. Their treatment regimen does not have to be as strict as that of the pet with FAD. A single adulticidal product (instead of possibly two on the animal with FAD), applied according to the manufacturer’s recommendations (instead of every fortnight) should be suggested. Should the animal with FAD be treated with a systemic (or possibly topical) IGR such as lufenuron (or methoprene/pyriproxyfen), all incontact animals should also be treated. Recommendations As yet, the ideal product does not exist Flea avoidance is certainly the goal for a dog or cat with FAD. This is difficult and takes time. Symptomatic, antipruritic therapy (beyond the scope of this article) is often necessary. Furthermore, there are so many opportunities for a dog to pick up fleas (e.g. environment, neighbourhood and occasional visiting animal) that even if flea control is considered optimal, it may still fail. Allergen-specific immunotherapy has, to date, not been helpful. Targeting the different steps of the life cycle: integrated control An insect growth regulator (IGR) - JHA or an IDI - should be combined with an adulticide(s), either on the animal or in the environment. Prior to application of flea control products in the environment, hygienic measures should be recommended, bearing in mind the relative lack of efficacy of vacuuming against larvae. Prior steam cleaning should be suggested. The ideal product to protect an animal with FAD against fleas would be one with repellent action, i.e. a product which ideally, would prevent fleas (mainly newly-emerged adults but also fleas coming from infested animals) from jumping on, or at least disturbing any fleas that did arrive in the coat so that they would leave immediately without biting (flushing effect). Unfortunately, although such products are effective against some insects (e.g. mosquitoes), they are not very helpful in flea control. When premises are too large, or when young children are at high risk of coming in contact with the products (particularly pyrethroids) whilst playing on carpets, the IGR should be administered directly to the animal, preferably systemically. Customising flea control Factors which may influence failure in a flea control programme may be product-related or animal/owner-related. Client compliance, short-term and long-term, is essential in FAD cases. Therefore, any control plan has to be practical for the owner and must be adapted to individual circumstances. Compliance, ability, health, financial resources, presence of young children, degree of pet and owner contact must all be taken into consideration. One should remember that a newly-emerged flea will start feeding within a few minutes of its arrival on the host. The first blood meal lasts from 10 minutes (males) to 25 minutes (females) [3]. It is therefore, not surprising that none of the aforementioned products is able to kill fleas before the fleas start to bite. However, some of them (particularly pyrethroids, but also nitempyram and spinosad) can certainly shorten the blood meal duration thereby reducing the amount of saliva injected. 265 EJCAP - Vol. 19 - Issue 3 December 2009 13. Fourie LJ, Kok DJ, Peter RJ. Control of immature stages of the flea Ctenocephalides felis (Bouche) in carpets exposed to cats treated with imidacloprid. J S Afr Vet Assoc. 2000; 71(4): 219-21. 14. Hellmann K, Knoppe T, Krieger K, Stanneck D. European multicenter field trial on the efficacy and safety of a topical formulation of imidacloprid and permethrin (Advantix) in dogs naturally infested with ticks and/or fleas. Parasitol Res. 2003; 90 Suppl 3: S125-6. 15. Epe C, Coati N, Stanneck D. Efficacy of the compound preparation imidacloprid 10%/permethrin 50% spot-on against ticks (I. ricinus, R. sanguineus) and fleas (Ct. felis) on dogs. Parasitol Res. 2003; 90 Suppl 3: S122-4. 16. Dobson P, Tinembart O, Fisch RD, Junquera P. Efficacy of nitenpyram as a systemic flea adulticide in dogs and cats. Vet Rec. 2000; 147(25): 709-13. 17. Rust MK, Waggoner MM, Hinkle NC, Stansfield D, Barnett S. Efficacy and longevity of nitenpyram against adult cat fleas (Siphonaptera: Pulicidae). J Med Entomol. 2003; 40(5): 678-81. 18. Cadiergues MC, Steffan J, Tinembart O, Franc M. Efficacy of an adulticide used alone or in combination with an insect growth regulator for flea infestations of dogs housed in simulated home environments. Am J Vet Res. 1999; 60(9): 1122-5. 19. Correia TR, Cruz VP, Ribeiro Fde A, Melo RM, Fernandes JI, Verocai GG, et al. [Residual activity in vitro of treated dog’s hair coat with dinotefuran on larvae and adults of Ctenocephalides felis felis (Bouche, 1835) (Siphonaptera: Pulicidae)]. Rev Bras Parasitol Vet. 2008; 17(4): 195-9. 20. Zhao X, Yeh JZ, Salgado VL, Narahashi T. Fipronil is a potent open channel blocker of glutamate-activated chloride channels in cockroach neurons. J Pharmacol Exp Ther. 2004; 310(1): 192201. 21. Zhao X, Salgado VL, Yeh JZ, Narahashi T. Differential actions of fipronil and dieldrin insecticides on GABA-gated chloride channels in cockroach neurons. J Pharmacol Exp Ther. 2003; 306(3): 91424. 22. Medleau L, Clekis T, McArthur TR, Alva R, Barrick RA, Jeannin P, et al. Evaluation of fipronil spot-on in the treatment of flea allergic dermatitis in dogs. J Small Anim Pract. 2003; 44(2): 71-5. 23. Medleau L, Hnilica KA, Lower K, Alva R, Clekis T, Case J, et al. Effect of topical application of fipronil in cats with flea allergic dermatitis. J Am Vet Med Assoc. 2002; 221(2): 254-7. 24. Cadiergues MC, Caubet C, Franc M. Comparison of the activity of selamectin, imidacloprid and fipronil for the treatment of dogs infested experimentally with Ctenocephalides canis and Ctenocephalides felis felis. Vet Rec. 2001; 149(23): 704-6. 25. Schuele G, Barnett S, Bapst B, Cavaliero T, Luempert L, Strehlau G, et al. The effect of water and shampooing on the efficacy of a pyriprole 12.5% topical solution against brown dog tick (Rhipicephalus sanguineus) and cat flea (Ctenocephalides felis) infestations on dogs. Vet Parasitol. 2008; 151(2-4): 300-11. 26. Zakson-Aiken M, Gregory LM, Meinke PT, Shoop WL. Systemic activity of the avermectins against the cat flea (Siphonaptera: Pulicidae). J Med Entomol. 2001; 38(4): 576-80. 27. Dupuy J, Derlon AL, Sutra JF, Cadiergues MC, Franc M, Alvinerie M. Pharmacokinetics of selamectin in dogs after topical application. Vet Res Commun. 2004; 28(5): 407-13. 28. Ritzhaupt LK, Rowan TG, Jones RL, Cracknell VC, Murphy MG, Shanks DJ. Evaluation of the comparative efficacy of selamectin against flea (Ctenocephalides felis felis) infestations on dogs and cats in simulated home environments. Vet Parasitol. 2002; 106(2): 165-75. 29. Shanks DJ, Rowan TG, Jones RL, Watson P, Murphy MG, Smith DG, et al. Efficacy of selamectin in the treatment and prevention of flea (Ctenocephalides felis felis) infestations on dogs and cats housed in simulated home environments. Vet Parasitol. 2000; 91(3-4): 213-22. Conclusion Despite the availability of safe, effective products, treating FAD remains a challenge. This challenge should be more readily overcome once both practitioner and owner(s) are entirely convinced of the diagnosis. Appropriate knowledge of the flea life cycle and flea-related biology, an understanding of the mode of action of flea control products, and motivation are all required. An integrated approach to treatment should be adopted, involving all the players in the flea life cycle - the FAD patient, all in-contact pets, and the environment. Each case must be customised, with effective flea control products used in combination with cleaning measures such as steaming, vacuuming and regular grooming. References 1. Rust MK. Advances in the control of Ctenocephalides felis (cat flea) on cats and dogs. Trends Parasitol. 2005; 21(5): 232-6. 2. Hsu MH, Wu WJ. Off-host observations of mating and postmating behaviors in the cat flea (Siphonaptera: Pulicidae). J Med Entomol. 2001; 38(3): 352-60. 3. Cadiergues MC, Hourcq P, Cantaloube B, Franc M. First bloodmeal of Ctenocephalides felis felis (Siphonaptera: Pulicidae) on cats: time to initiation and duration of feeding. J Med Entomol. 2000; 37(4): 634-6. 4. Cadiergues MC, Santamarta D, Mallet X, Franc M. First blood meal of Ctenocephalides canis (Siphonaptera: Pulicidae) on dogs: time to initiation of feeding and duration. J Parasitol. 2001; 87(1): 214-5. 5. Cadiergues MC, Roques M, Franc M. Survival performances of the dog flea, Ctenocephalides canis and the cat flea, Ctenocephalides felis felis : a comparative study. In: ESVD-ECVD-GEDAC, editor. 18th ESVD-ECVD Annual Congress; 2002 September 26-28, 2002; Nice (France); 2002. p. 216. 6. Robinson WH. Distribution of cat flea larvae in the carpeted household environment. Vet dermatol. 1995; 6(3): 145-150. 7. Hsu MH, Hsu YC, Wu WJ. Consumption of flea faeces and eggs by larvae of the cat flea, Ctenocephalides felis. Med Vet Entomol. 2002; 16(4): 445-7. 8. Marchiondo AA, Holdsworth PA, Green P, Blagburn BL, Jacobs DE. World Association for the Advancement of Veterinary Parasitology (W.A.A.V.P.) guidelines for evaluating the efficacy of parasiticides for the treatment, prevention and control of flea and tick infestation on dogs and cats. Vet Parasitol. 2007; 145(3-4): 332-44. 9. Dryden MW, Denenberg TM, Bunch S. Control of fleas on naturally infested dogs and cats and in private residences with topical spot applications of fipronil or imidacloprid. Vet Parasitol. 2000; 93(1): 69-75. 10. Ritzhaupt LK, Rowan TG, Jones RL. Evaluation of efficacy of selamectin, fipronil, and imidacloprid against Ctenocephalides felis in dogs. J Am Vet Med Assoc. 2000; 217(11): 1669-71. 11. Schenker R, Tinembart O, Humbert-Droz E, Cavaliero T, Yerly B. Comparative speed of kill between nitenpyram, fipronil, imidacloprid, selamectin and cythioate against adult Ctenocephalides felis (Bouche) on cats and dogs. Vet Parasitol. 2003; 112(3): 249-54. 12. Mehlhorn H, Hansen O, Mencke N. Comparative study on the effects of three insecticides (fipronil, imidacloprid, selamectin) on developmental stages of the cat flea (Ctenocephalides felis Bouche 1835): a light and electron microscopic analysis of in vivo and in vitro experiments. Parasitol Res. 2001; 87(3): 198-207. 266 Flea control in flea allergic dogs and cats - Marie-Christine Cadiergues 30. Benchaoui HA, Clemence RG, Clements PJ, Jones RL, Watson P, Shanks DJ, et al. Efficacy and safety of selamectin against fleas on dogs and cats presented as veterinary patients in Europe. Vet Parasitol. 2000; 91(3-4): 223-32. 31. McTier TL, Jones RL, Holbert MS, Murphy MG, Watson P, Sun F, et al. Efficacy of selamectin against adult flea infestations (Ctenocephalides felis felis and Ctenocephalides canis) on dogs and cats. Vet Parasitol. 2000; 91(3-4): 187-99. 32. McTier TL, Shanks DJ, Jernigan AD, Rowan TG, Jones RL, Murphy MG, et al. Evaluation of the effects of selamectin against adult and immature stages of fleas (Ctenocephalides felis felis) on dogs and cats. Vet Parasitol. 2000; 91(3-4): 201-12. 33. Dickin SK, McTier TL, Murphy MG, Bond R, Mason IS, PayneJohnson M, et al. Efficacy of selamectin in the treatment and control of clinical signs of flea allergy dermatitis in dogs and cats experimentally infested with fleas. J Am Vet Med Assoc. 2003; 223(5): 639-44. 34. Prelaud P, Calmon J, Delmas H, Deveze M, Guillaume P, MLaumonier M. Double blind comparative study of the efficacy of selamectin and fipronil in the treatment of canine flea allergy dermatitis: a multiple field trial. Rev. Med. Vet. 2003; 154(11): 689-694. 35. Endris RG, Hair JA, Katz TL, Zobre E, Pennington RG, Meyer JA. Efficacy of three dose volumes of topically applied 65% permethrin against Ctenocephalides felis and Rhipicephalus sanguineus on dogs weighing 30 kg or more. Vet Ther. 2002; 3(4): 435-40. 36. Endris RG, Hair JA, Anderson G, Rose WB, Disch D, Meyer JA. Efficacy of two 65% permethrin spot-on formulations against induced infestations of Ctenocephalides felis (Insecta: Siphonaptera) and Amblyomma americanum (Acari: Ixodidae) on beagles. Vet Ther. 2003; 4(1): 47-55. 37. Endris RG, Everett R, Cunningham J, Katz TL, Thompson K. Efficacy of two 65 % permethrin spot-on formulations against canine infestations of Ctenocephalides felis and Rhipicephalus sanguineus. Vet Ther. 2002; 3(3): 326-33. 38. Rugg D, Hair JA, Everett RE, Cunningham JR, Carter L. Confirmation of the efficacy of a novel formulation of metaflumizone plus amitraz for the treatment and control of fleas and ticks on dogs. Vet Parasitol. 2007; 150(3): 209-18. 39. Holzmer S, Hair JA, Dryden MW, Young DR, Carter L. Efficacy of a novel formulation of metaflumizone for the control of fleas (Ctenocephalides felis) on cats. Vet Parasitol. 2007; 150(3): 21924. 40. Franc M, Beugnet F. A comparative evaluation of the speed of kill and duration of efficacy against weekly infestations with fleas on cats treated with fipronil-(S)-methoprene or metaflumizone. Vet Ther. 2008; 9(2): 102-10. 41. Hellmann K, Adler K, Parker L, Pfister K, Delay RL, Rugg D. Evaluation of the efficacy and safety of a novel formulation of metaflumizone plus amitraz in dogs naturally infested with fleas and ticks in Europe. Vet Parasitol. 2007; 150(3): 239-45. 42. Robertson-Plouch C, Baker KA, Hozak RR, Zimmermann AG, Parks SC, Herr C, et al. Clinical field study of the safety and efficacy of spinosad chewable tablets for controlling fleas on dogs. Vet Ther. 2008; 9(1): 26-36. 43. Snyder DE, Cruthers LR, Slone RL. Preliminary study on the acaricidal efficacy of spinosad administered orally to dogs infested with the brown dog tick, Rhipicephalus sanguineus (Latreille, 1806) (Acari: Ixodidae). Vet Parasitol. 2009. 44. Franc M, Bouhsira E. Evaluation of speed and duration of efficacy of spinosad tablets for treatment and control of Ctenocephalides canis (Siphonaptera: Pulicidae) infestations in dogs. Parasite. 2009; 16(2): 125-8. 45. Young DR, Jeannin PC, Boeckh A. Efficacy of fipronil/(S)methoprene combination spot-on for dogs against shed eggs, emerging and existing adult cat fleas (Ctenocephalides felis, Bouche). Vet Parasitol. 2004; 125(3-4): 397-407. 46. Stanneck D, Larsen KS, Mencke N. Pyriproxyfen concentration in the coat of cats and dogs after topical treatment with a 1.0% w/v spot-on formulation. J Vet Pharmacol Ther. 2003; 26(3): 233-5. 47. Dean SR, Meola RW, Meola SM, Sittertz-Bhatkar H, Schenker R. Mode of action of lufenuron in adult Ctenocephalides felis (Siphonaptera: Pulicidae). J Med Entomol. 1999; 36(4): 486-92. 48. Dryden MW, Perez HR, Ulitchny DM. Control of fleas on pets and in homes by use of imidacloprid or lufenuron and a pyrethrin spray. J Am Vet Med Assoc. 1999; 215(1): 36-9. 49. Jacobs DE, Hutchinson MJ, Fox MT, Krieger KJ. Comparison of flea control strategies using imidacloprid or lufenuron on cats in a controlled simulated home environment. Am J Vet Res. 1997; 58(11): 1260-2. 50. Franc M, Cadiergues MC. Use of injectable lufenuron for treatment of infestations of Ctenocephalides felis in cats. Am J Vet Res. 1997; 58(2): 140-2. 267 DERMATOLOGY How to treat atopic dermatitis in dogs D. N. Carlotti(1) SUMMARY This paper summarizes all the aspects of the therapy of canine atopic dermatitis, particularly on a long-term basis. The principles of threshold phenomenon and summation of effects are underlined. Treatment of the disease includes first the treatment of dermatoses which are related or secondary to atopic dermatitis: microbial infection (bacteria and Malassezia), flea allergy dermatitis, food reactions, keratoseborrhoeic skin disease, otitis externa and pyotraumatic dermatitis. Specific therapy is then envisaged: it includes allergen eviction and allergen-specific immunotherapy which is a major approach for the long-term management of the disease. Finally, symptomatic therapy with various drugs, including glucocorticoids, various topicals and ciclosporin, is detailed. A “combination therapy” is needed and should be tailored for each case. infestation or a mild pyoderma may produce marked discomfort while either condition on its own might be asymptomatic (PJ Ihrke – dermatology course – School of veterinary medicine, UC Davis, 1982). This paper was commissioned by FECAVA for publication in EJCAP. Introduction Treatment of dermatoses which are related or secondary to atopic dermatitis Canine Atopic Dermatitis is a very common disease. Management of this disease, both on a long term basis and during acute flares has led to multiple studies published in the veterinary literature. This review encompasses all the therapeutic aspects of the management of CAD. 1 - Treatment of microbial infections: An adequate antibacterial treatment regimen of secondary pyoderma, based upon systemic antibiotics and appropriate antibacterial topicals, may return the animal to a quasi-normal state. Such a case of CAD will only be treated specifically in case of regular reoccurrence of pyoderma and/or if the clinical signs of CAD itself become a concern. Also, some atopic dogs will respond to a well carried out antibiotic treatment, even without visible signs of secondary pyoderma [1]. A true bacterial overgrowth (BOG) syndrome is plausible in such cases and the author treats with antibiotics patients showing an abundant coccoid surface flora after cytological tests, as an empiric therapeutic test [2]. Threshold phenomenon and summation of effects Two important principles must be remembered in the frame of CAD therapy. 1 - Threshold phenomenon: A certain allergic load may be tolerated by an individual without any disease manifestations, but a small increase in that load may push the individual over the threshold and initiate clinical signs (PJ Ihrke – dermatology course – School of veterinary medicine, UC Davis, 1982). The same reasoning is undoubtedly applicable as well to cases of Malassezia dermatitis. Systemic (ketoconazole) and topical therapy are required with a careful follow-up (Figures 1 and 2) [3]. 2 – Summation of effects: Concomitant diseases fostering pruritus may raise an animal above its pruritic threshold. Therefore, all factors contributing to pruritus must be investigated: i.e., a subclinical allergy in combination with a flea 2 - Treatment of Flea Allergy dermatitis (FAD): A well conducted flea control regimen can eliminate the FAD and therefore, in certain cases can enable the animal to fall under 1) Didier Noel Carlotti, Dip ECVD, Ospedale Veterinario Cuneese, Via Vocaturo 13, 12016 Peveragno (CN), Italy 268 EJCAP - Vol. 19 - Issue 3 December 2009 Fig. 1 Malassezia dermatitis on the face of an atopic Labrador retriever. Fig. 2 Same dog as illustrated in figure 1, twenty days after initiation of antifungal therapy. its pruritic threshold (Figures 3 and 4) [4]. In such a case, atopic dermatitis treatment is not necessary if the clinical signs are not obvious. If this not the case, the atopic dermatitis should be treated while maintaining absolute antiparasitic treatment. 5 - Treatment of otitis externa: Otitis externa is a major feature of canine atopic dermatitis which causes inflammation of the external ear canal and ear pinnae. Secondary infections occur (bacterial and fungal) and perpetuating factors such as hyperplasia of epidermis and both sebaceous and apocrine glands lead to chronicity. It is typically erythemato-ceruminous at the beginning of the disease and it becomes eventually suppurative. The associated lesions of the ear pinnae (lichenification, alopecia, crusting) require therapy. Ear cleansing must be repeated regularly (eg twice or three times a week). Numerous commercial otic preparations are available which are usually easy to use and effective. They contain active substances such as antibiotic, antifungal and corticosteroid agents. Selection must be made after performing a smear and bacterial culture and sensitivity testing if the smear shows rods and/or if the otitis is suppurative. Corticosteroids included in otic preparations reduce pruritus, pain and proliferative reactions. They also decrease cerumen secretion. Systemic antibiotic therapy can be useful in otitis externa due to CAD, particularly if it is suppurative, because of associated otitis media which has to be diagnosed by imaging. Surgical therapy can be avoided in many circumstances with appropriate medical therapy. Surgical failure is often due to failure to recognise and control CAD [8]. 3 - Management of food reactions: Food intolerance may resemble CAD or may trigger flares of atopic dermatitis [5], which leads to the concept of food-induced atopic dermatitis, in comparison to CAD sensu stricto. An elimination diet should be performed in all cases of CAD and followed by sequential reintroductions in case of good response. If an offending food is identified, this should be definitely withdrawn from the patient’s diet, which is easy to perform. A concomitant CAD sensu stricto should be treated specifically only if clinical signs can be attributed to it [6]. 4 - Treatment of keratoseborrhoeic skin disease: A keratoseborrhoeic disorder can occur in CAD particularly in ancient cases. Treatment is mainly topical although systemic Essential Fatty Acids, used in the treatment of CAD may have an effect on seborrhoea. Shampoos and moisturizing agents are valuable supporting therapy in keratoseborrhoeic skin disorders [7]. Fig. 3 Flea allergy dermatitis in an atopic German shepherd. Fig. 4 Same dog as illustrated in figure 3, three months after initiation of flea-control. 269 How to treat atopic dermatitis in dogs - D. N. Carlotti 6 – Treatment of pyotraumatic dermatitis: Lesions of pyotraumatic dermatitis are common in CAD. They are poorly understood. They should be differentiated from pyotraumatic folliculitis. Although there may be a spontaneous healing in a few days, treatment is beneficial. Clipping and cleansing with antiseptic shampoos can be followed by the application of creams containing antibiotics and corticosteroids. If pruritus or above all pain are important, a short systemic glucocorticoid treatment is useful [9]. and grasses) or not (particularly house dust mites and above all Dermatophagoides farinae, but also storage mites, moulds and danders). Test results are to be interpreted in an anamnesis and clinical light in each of the cases. A (good) test means ONLY that the animal has developped specific IgE towards allergens. It does not mean that the clinical signs are linked to this sensitization. Indeed the clinical signs must be compatible with Flea Allergy Dermatitis and/or Atopic Dermatitis to take in account positive tests. In addition, in case of positive reactions, allergens should be included in an immunotherapy protocol only if they are present in the environment (however cat dander can in fact be transported through the air or by people [17]). Specific treatment 1 – Allergenic eviction: Allergenic eviction is “theoretically” the ideal treatment for all cases of allergic dermatitis in enabling the animal to fall beneath its pruritic/allergic threshold. Pollens cannot be avoided but it is possible to eliminate environmental feathers and fabrics, and moulds can be destroyed by antiseptic or antifungal sprays or even anti-mould paint. However, the role of these allergens in dogs’ atopic dermatitis is minimal in Europe [10] and moreover feathers and fabrics are mostly sources of house dust mite allergen [11]. No standardisation exists for the ASIT methods used. Only aqueous extracts are used in North America, whereas in Europe, mainly alum precipitated extracts are available [13]. It seems that the combination of moulds and pollen extracts alters their quality (due to the presence of protease in the mould extracts) and that different types of vials are necessary [18]. Various methods exist to destroy house dust mites and these may be tried around atopic dogs such as the use of acaricide sprays and foggers (some of which contain an Insect Growth Regulator [IGR] and a denaturing agent such as tannic acid which is very efficient for both mites’ faeces and fungal spores). The elimination of house dust mites has been shown to be effective in human atopic dermatitis but only one study has been published in canine dermatology, showing good efficacy [12]. Fig. 5 Erythema, excoriations and crusts in an atopic Fox Terrier. 2 – Allergen Specific Immunotherapy (ASIT): ASIT (hyposensitisation, desensitisation) has been used in humans for a century, to treat asthma, allergic rhinitis and hypersensitivity to hymenoptera bites but not treat allergic skin disease. It started in dogs in the 1940s, and become commonly used in North America in the 1960s and in Europe in the 1980s. The first explanation for desensitisation efficacy in man was in the production of blocking antibodies (lgG), which combine with allergens before they combine with the IgE. Today, many mechanisms are proposed [13,14]. In particular, acting on Th2Th1 substitution will lead to a reduction in the IL4 production and an increase in the INF-gamma production [15]. The IL4 offers potential for the IgE synthesis, increases the number of weak affinity IgE receptors or their CD23 soluble form. The INFgamma inhibits IgE synthesis. Late phase reaction inhibition in desensitized subjects is accompanied by the apparition of T-lymphocytes with a Th1 profile. Finally, desensitization may be accompanied by a cellular and tissue hyposensitisation. These mechanisms can sequentially intervene and differ between the induction and maintenance phases. Recently, the role of blocking antibodies has been emphasized again in the dog [16]. Fig. 6 Close-up of the face of the dog illustrated in figure 5. The choice of allergens mainly depends on the in vivo (skin-tests) or in vitro (ELISA = Enzyme-Linked Immuno-Sorbent Assay) test results. Allergy testing, including selection of allergens for testing, is discussed in many dermatology manuals. The allergens that are used are seasonal (pollens of trees, weeds 270 EJCAP - Vol. 19 - Issue 3 December 2009 The results of ASIT are more or less difficult to evaluate in dogs. In fact, they depend on the animals (age and especially diagnostic criteria), evaluation criteria (telephone follow-up, clinical score), follow-up duration, and recognition or not of “loss of follow-up” as setbacks. Presently, it is considered that 50 to 100 % of animals respond to immunotherapy in open studies (Figures 5,6,7,8,9,10) [13,14]. T. Willemse demonstrated in 1984 the method’s efficacy through a double blind placebo controlled study [19]. The 9-month evaluation seems important: it is usual that improvement at this stage is followed by success. The result variation factors include (apart from the diagnostic method and the clinical criteria of each one), allergens nature (controversial), number of allergens (controversial), breed and sex (controversial), age (probably no influence) and appropriate patients’ follow-up (indispensable) [13,14]. Also, specifity of ASIT has been confirmed, including recently [20]. As far as the allergen identification method is concerned, it is of course impossible to confirm for all in vitro tests the same success rates in immunotherapy as the one obtained after skin-tests (i.e. 60 to 100 % of improvement) but it is likely that the best in vitro tests will give a high percentage of good results, comparable to skin testing. In addition, it is also felt that some dogs with negative skin tests or poor results to immunotherapy based on skin tests may respond well to immunotherapy based on in vitro testing. It is also possible that the combination of in vivo and in vitro tests increase success rates. Fig. 7 Close-up of an ear pinna of the dog illustrated in figure 5. The use of highly purified allergens (Der f 15 and Der f 18?) could improve results. No study has yet proven that the use of corticosteroids or ciclosporin during desensitisation would have a very harmful effect on its efficacy. Fig. 8 Same dog as illustrated in figure 5, six months after initiation of allergen-specific immunotherapy. Rare cases of secondary effects have been mentioned in an anecdotal manner (urticaria, angioedema, anaphylaxis). An exacerbation of clinical signs’ is often noticed in the hours following injections. Limited local reactions which are spontaneously reversible often appear with alum precipitated extracts. A majority of veterinary dermatologists believe that the efficacy and absence of secondary effects justifies ad vitam eternam hyposensitization. They empirically remarked that the clinical signs reappear in a period of months to years after the treatment has been stopped. Fig. 9 Close-up of the face of the dog illustrated in figure 6, six months after initiation of allergen-specific immunotherapy. Fig. 10 Close-up of the ear pinna of the dog illustrated in figure 7, six months after initiation of allergen-specific immunotherapy. 271 How to treat atopic dermatitis in dogs - D. N. Carlotti Rush immunotherapy could be effective but secondary effects occur in a fourth of the cases [21]. The use of immunostimulatory liposome-nucleic acid complexes could be interesting [22]. Recently a monodose ASIT technique has been proposed in a preliminary study, in association with a long-term therapy with cetirizine [23]. hepatomegaly, inhibition of the hypothalamo-hypophysoadrenal axis, dryness of the skin and the haircoat and even iatrogenic Cushing’s syndrome with alopecia. Secondary infections (pyoderma, demodicosis, dermatophytosis) can occur. The following rules must be respected regarding their long term side effects: glucocorticoids should be used as little as possible, at the lowest possible dose, preferably every other day and only if alternative anti-pruritic medications are not effective enough. Symptomatic treatment This is useful at the beginning of immunotherapy (within the first year in successful cases) or on a long-term basis in failed cases (total or partial), or even in cases where immunotherapy is not required (aged animal, owner’s hesitation or even, clinically slightly worrying cases apart from a few signs). Symptomatic therapy is also indicated for canine atopic-like dermatitis. Major reviews on evidence-based pharmacotherapy of CAD, including a recent “Cochrane” systematic review of randomized controlled trials, have been made and include most of the following data [24,25]. 2 - Non steroidal topicals Various non steroidal topicals can be used. Non steroidal antipruritic sprays or rinses, e.g. containing colloidal oatmeal or aloe vera can be useful. A spray containing Hamamelis extract and menthol has become popular to treat localized lesions and has been shown to kill Malassezia [27]. Two microemulsion lotions/sprays have been developed to complement shampoos specifically designed for canine atopic dermatitis (see below). One contains mono and oligosaccharides (free and in Spherulites®), vitamin E and linoleic acid, the other (available also in concentrate) contains phytosphingosine (see below), hinokitiol (= β-thujaplicin, antimicrobial and anti-inflammatory) and essential fatty acids from raspberry seed oil. Tacrolimus, a calcineurin inhibitor with immunomodulatory properties has been shown to be effective in the treatment of localized lesions of canine atopic dermatitis. 1 - Glucocorticoids Glucocorticoids are the most effective medications to treat allergic dermatitis. They have anti-inflammatory and antipruritic properties as well as antiproliferative and immunosuppressive effects. They act at almost all inflammation and immunologic response stages. Their activity, however, varies tremendously. There is no consistency in the individual response not only in relation to the glucorticoid used but also for the same glucocorticoid. The effect is reduced over time, and the doses required are increased. They are used topically or systemically. Topical glucocorticoid ointments, creams and gels are useful for localised lesions (e. g. cheilitis, blepharitis, pododermatitis, nasal lesions, excoriations and pyotraumatic dermatitis). Many molecules are available in human dermatology, classified from class I (the least potent) to class IV (the most potent). Some potent human formulations can be used in the dog (e.g. clobetasol propionate). Most of the traditional veterinary formulations are in fact combined with antimicrobials and contain less potent agents. However, their overuse can lead to tachyphylaxis, atrophy and microbial infections. All shampoos are likely to remove allergens from the skin, and this is probably helpful in CAD. They also help to rehydrate dry skin (xerosis) particularly when associated to humectant sprays. Shampoos containing fatty acids can help in allergic skin disorders. Shampoos with an antipruritic effect (colloidal oatmeal) can be good adjunctive treatments. A micro-emulsion shampoo specifically designed for canine atopic dermatitis contains linoleic acid and gamma linolenic acid, mono and oligosaccharides, vitamin E, and piroctone olamine and has been shown to be effective on pruritus [28]. In fact, exogenous monosaccharides downregulate the inflammatory response to allergen challenge. This is why they are used in topical products for atopic/reactive skin patients in humans and are beneficial in animal with allergic skin disease. Another shampoo containing phytosphingosine, hinokitiol and raspberry seed oil in an hydrating formulation has also been shown to be beneficial in atopic dermatitis, in association with the corresponding spray (see above), in a comparative study with the previous one [29]. Glucocorticoids are also available in lotions, rinses, sprays and even shampoos in the USA. Small spray containers are used to treat localized lesions, as creams and ointments. Several glucocorticoids are available, usually not the most potent. A new class of glucocorticoids, the diesters, is used in human dermatology. Diesters are lipophilic compounds that quickly penetrate the stratum corneum and are stored and metabolised within the skin after topical application (with reduced systemic secondary effects). They have consequently a high therapeutic index. One of them, hydrocortisone aceponate, is now available as a medium-sized spray as a veterinary product for dogs and has been shown to be effective in the management of CAD [26]. 3 - Antihistamines AntiH1 antihistamines, which block H1 receptors, may be useful (whereas antiH2 are inefficient). They are not effective in human atopic dermatitis. Many studies have been performed in dogs but there is insufficient evidence to conclude for or against the efficacy of antihistamines for treatment of CAD (15 to 25 % good results, close to a placebo effect) [30]. In an evidence-based review [31], the following agents were considered as having: – no or low efficacy: chlorpheniramine, pheniramine, diphenhydramine, hydroxyzine, promethazine, trimeprazine (first generation), astemizole and loratadine (second generation) Systemic glucocorticoid therapy should be limited to the administration of prednisolone or methyl-prednisolone by oral route (0.5 to 1 mg/kg/day during 5 to 7 days followed by 1 mg/kg every other day, as shortly as possible). They have significant side effects including polyuria-polydipsia, polyphagia, 272 EJCAP - Vol. 19 - Issue 3 December 2009 – conflicting evidence of efficacy: terfenadine (second generation) – medium efficacy: clemastine, chlorpheniramine-hydroxyzine combination (first generation), oxatomide (second generation). and there is no supplement or diet that is appropriate to all. Several tests can be made as for antihistamines. A dietary approach, based on a high quantity of omega-3 and the ratio omega-3/omega-6 may also be helpful. A sub-population of non-responsive atopic dogs is likely. Perhaps the dosage of clemastine should be increased in the dog. More recently, cetirizine has been shown to be ineffective and topical diphenhydramine has been shown to be relatively effective. Moreover, some frequently used products such as ketotifene or rupatidine have not been evaluated at all. There are still doubts, so, on the real efficacy of EFA in CAD especially since several elements have not yet been made clear: the dosage (varying from 2 to 10 times the recommended doses), minimal duration of the therapeutic test to predict efficacy (1 to 12 weeks), optimal ratio between omega-3 and omega-6 (between 5 and 10), the function of co-factors, criteria to select responder dogs, responder breeds, synergy with other anti-inflammatory agents. They are to be principally used with other anti-pruritic treatments. They have few side effects. The relatively low success rates of these antiH1 justify successive tests during at least one week at a time, until a satisfactory result is obtained. Trimeprazine, which alone is inefficient, has proven to be able to clearly reduce the need for prednisone. There is a synergic effect between the essential fatty acids and antihistamines. 5 - Ciclosporin Ciclosporin, an orally administered calcineurin inhibitor, is an effective drug for the treatment of CAD, as shown in four controlled studies including two placebo controlled doubleblind studies and two showing a similar effect as prednisolone and methylprednisolone [32]. 4 - Essential Fatty Acids Many clinical studies have been done in dogs on the use of Essential fatty acids (EFA) for the treatment of CAD, although there are not used in human atopic dermatitis. They are polyunsaturated, administered by oral route, particularly omega-3 series eicosapentanoic acid (EPA) and omega-6 series gamma linolenic acid (GLA). These fatty acids compete with the arachidonic acid in the cascade of eicosanoids synthesis where leukotrienes and prostaglandins are formed having an anti-inflammatory activity or at least a pro-inflammatory activity which is much less significant than that observed with the metabolites emitted from arachidonic acid. Oral fatty acids could also reinforce the defective cutaneous barrier of atopic dogs. In another study relapses were more common during 2 months in dogs treated with methylprednisolone than in dogs treated with ciclosporin and lesions were less severe in the latter (pruritus was identical). After 4 weeks of daily administration it is possible to administer the drug only every other day in 39 % of the cases and after 12 weeks every other day or twice a week in 22 % and 36 % of the cases respectively. In a recent study therapy was discontinued in 6 to 24 months in 45 % of the cases because of failures (22 %) or success (24 %) without relapses over a period of 3 to 22 months. So a long-term treatment (several months) is justified and then the treatment is stopped. The omega-6/omega-3 ratio could be important according to an in vitro study and should be 5 to 10. Recent in vitro studies show that addition of omega-3 and GLA decrease the production of mediators of inflammation by mast cells. This molecule has become, despite its high cost, a very effective symptomatic treatment of CAD, particularly in severe forms (Figures 11 and 12). Its efficacy is dose-dependent but the assay of its blood level has no value since it cannot predict the clinical response. Secondary effects are limited and are mainly gastrointestinal, with more rarely gingival hyperplasia, verrucous lesions or hypertrichosis. The long-term secondary effects known in man (renal insufficiency, hypertension) have not been reported in dogs. Last but not least ciclosporin does not enhance the risk of secondary infections. Doses are variable and empirical in the clinical studies. Amongst them there are only eight double blind placebo controlled studies, including three in cross-over. Perhaps high doses could be necessary to get a result but studies using high doses of omega-6 or omega-3 give variable results, with duration of treatment from 6 to 16 weeks. Supplementation in EFA does not take in account the intake from the diet in these studies, that can be important and only the three cross-over studies overcome this drawback of variability of dietary EFA intake but their results are variable. 6 - Other non steroidal systemic anti-inflammatory/ antipruritic agents – Anti-depressor and psychotropic drugs: Fluoxetine, an antidepressive agent which inhibits serotonin uptake, doxepin and amitriptyline, tricyclic anti-depressive agents with a antiH1 activity, appear to be moderately efficient giving good results comparable to the “best” antihistamines (20 to 30 %). Dextromethorphan has no effect. – Leukotriene inhibitors have been tried in a few clinical trials. Zileuton and Zafirlukast were not very effective in placebo controlled studies but tepolaxin showed a certain efficacy in milder cases of CAD. – Misoprostol, a prostaglandin E analog, has shown a moderate More recently, clinical studies have been performed with specific diets or with supplements added to standard diets that show the beneficial effect of omega-3 with or without GLA. A glucocorticoid sparing effect has also been shown. The mechanism of action remains obscure since there is no correlation between the EFA concentrations in the skin and plasma and the clinical improvement. In summary, the reaction of atopic dogs to fatty acids varies 273 How to treat atopic dermatitis in dogs - D. N. Carlotti Fig. 11 Alopecia, lichenification and hyperpigmentation in a severely affected atopic German shepherd. Fig. 12 Same dog as illustrated in figure 11, six months after initiation of control of microbial overgrowths, antiseborrhoeic topical therapy and ciclosporin therapy. effect, including in a randomized controlled study. – Phosphodiesterase inhibitors have shown a moderate efficacy in comparative (arophylline) or double blind placebo controlled cross-over (pentoxyfilline) studies. Arophylline is poorly tolerated. Papaverin is ineffective. – Interferons: recombinant canine gamma interferon injections showed a good-to-excellent efficacy to control skin lesions or pruritus in about 80% of dogs with CAD and in a recent study, we showed a good efficacy of a recombinant omega interferon (rfeIFN-ω), comparable to ciclosporin [33]. – Various agents: an injectable formulation of fatty acid copolymers, a phytotherapy preparation of Chinese herbs, MS-antigen (a peptide extracted from urine of allergic humans), aminopterine (an antifolate), have given interesting results. References [1] Mueller RS, Bettenay SV (1996) Long-term Immunotherapy of 146 Dogs with Atopic Dermatitis - a Retrospective Study. Aust. Vet. Practit., 26, 128-132. [2] Pin D, Carlotti DN, Jasmin P, DeBoer DJ, Prélaud P (2006) Prospective study of bacterial overgrowth syndrome in eight dogs. Vet. Record., 158, 437-441. [3] Guillot J, Bond R (1999) Malassezia pachydermatis: a review. Med. Mycol., 37, 295-306. [4] Carlotti DN, Jacobs DE (2000) Therapy, control and prevention of flea allergy dermatitis in dogs and cats. Vet. Dermatol., 11, 8398. [5] Olivry T et al (2007) Food for thought: pondering the relationship between canine atopic dermatitis and cutaneous adverse reaction. Vet. Dermatol., 18, 390-391. [6] Chesney CJ (2001) Systematic review of evidence for the prevalence of food sensitivity in dogs. Vet. Rec., 148, 445-448. [7] Carlotti D.N., Bensignor E. Management of keratoseborrhoeic disorders. Eur Journal Comp Anim Pract, 2002; 12: 123-133. [8] Harvey RG, Harari J, Delauche AJ (2001) Ear diseases of the dog and cat, London, Manson Publishing Ltd. [9] Holm BR, Rest JR, Seewald W (2004) A prospective study of the clinical findings, treatment and histopathology of 44 cases of pyotraumatic dermatitis. Vet. Dermatol., 15, 369-376. [10] Carlotti DN, Costargent F (1994) Analysis of positive skin-tests in 449 dogs with allergic dermatitis. Eur Journal Comp Anim Pract, 4, 52-59. [11] Prelaud P, olivry T (1998) Etiopathogénie de la dermatite atopique canine. Prat. Méd. Chir. Anim. Comp., 33 (numéro spécial), 315329. [12] Swinnen C, Vroom M (2004) The clinical effect of environmental control of house dust mites in 60 fouse dust mite-sensitive dogs. Vet. Dermatol., 15, 31-36. [13] Griffin CE, Hillier A (2001) The ACVD task force on canine atopic dermatitis (XXIV): allergen-specific immunotherapy. Vet. Immunol. Immunopathol., 81, 363-383. [14] Loewenstein C, Mueller RS (2009) A review of allergen-specific immunotherapy in human and veterinary medicine. Vet. Dermatol., 20, 84-98. Other treatments were considered as ineffective: erythromycin, doxycycline, tetracycline-niacinamide, cyproheptadine, ascorbic acid, tranilast, an homeopathic preparation, azathioprine and proanthozone. Conclusion: Combination therapy case management Long-term management of CAD is difficult. Therapy of dermatoses which are related or secondary is essential. The hygienic and clinical value of topicals designed for canine dermatology should be underlined, as in human dermatology. The treatment, as for all allergic dermatoses, shall act on the pruritic threshold, by specific immunotherapy and symptomatic treatments and can also include allergen eviction. It should be remembered that placebo effect exists in canine medicine and is around 9 % in pruritus due to CAD (less for lesions). This effect must be taken in account in clinical studies. Each case is different and deserves a “combination therapy”, which associates treatment of complications, eventual allergen eviction measures, allergen-specific immunotherapy and symptomatic therapy. It is the key to success. 274 EJCAP - Vol. 19 - Issue 3 December 2009 [31] Olivry T, Mueller RS and the international task force on canine atopic dermatitis (2003) Evidence-based veterinary dermatology: a systematic review of the pharmacotherapy of canine atopic dermatitis. Vet. Dermatol., 14, 121-146. [32] Steffan J, Favrot C, Mueller R (2006) A systematic review and meta-analysis of the efficacy and safety of cyclosporine for the treatment of atopic dermatitis in dogs. Vet. Dermatol., 17, 3-16. [33] Carlotti DN, Boulet M, Ducret J, Machicote G, Jasmin P, Reme C, Albouy M (2009) The use of recombinant omega interferon therapy in canine atopic dermatitis. A double-blind controlled study. Vet. Dermatol. 20,405-411. [15] Shida M, Kadoya M, Park SJ, Nishifuji K, Momoi Y, Iwasaki T (2004) Allergen-specific immunotherapy induces Th1 shift in dogs with atopic dermatitis. Vet. Immunol. Immunopathol. 102, 19-31. [16] Hou C, Griffin C, Hill PB (2008) Dermatophagoides farinae-specific IgG responses in atopic dogs undergoing allergen-specific immunotherapy with aqueous vaccines. Vet. Dermatol., 19, 215220. [17] Bollinger ME et al (1996) Cat antigen in homes with and without cats may induce allergic symptoms. J. Allergy Clin. Immunol., 97, 907-914. [18] Rosenbaum MR et al (1996) Effects of Mold Proteases on the Biological Activity of Allergenic Pollen Extracts. Amer. J. Vet. Res., 57, 1447-1452. [19] Willemse T, van den Brom WE, Rijnberg A (1984) Effect of hyposensitization on atopic dermatitis in dogs. J. Am. Vet. Med. Assn., 184, 1277-1280. [20] Willemse T, Bardagi M, Carlotti DN, Ferrer L, Fondati A, Fontaine J, Leistra M, Noli C, Ordeix L, Scarampella F, Schleifer S, Sinke J, Roosje P (2009) Dermatophagoides farinae–specific immunotherapy in atopic dogs with hypersensitivity to multiple allergens: a randomized, double blind, placebo-controlled study. Vet. J., 180, 337-342. [21] Mueller RS, Bettenay SV (2001) Evaluation of the safety of an abbreviated course of injections of allergen extracts (rush immunotherapy) for the treatment of dogs with atopic dermatitis. Am. J. Vet. Res., 62, 307-310. [22] Mueller RS, Veir J, Fieseler KV, DOW SW (2005) Use of immunostimulatory liposome-nucleic acid complexes in allergenspecific immunotherapy of dogs with refractory atopic dermatitis - a pilot study. Vet. Dermatol., 16, 61-68. [23] Cochet-Faivre N, Prelaud P (2007) Monodose allergen-specific immunotherapy for treatment of canine atopic dermatitis: preliminary safety study. Vet. Dermatol., 18, 385-386 (abstract). [24] Olivry T, Mueller RS and the international task force on canine atopic dermatitis (2003) Evidence-based veterinary dermatology: a systematic review of the pharmacotherapy of canine atopic dermatitis. Vet. Dermatol., 14, 121-146. [25] Olivry T, Foster AP, Mueller RS (2009) Interventions for Atopic Dermatitis in Dogs: A Systematic Review of Randomized Controlled Trials. Vet. Dermatol., in press. [26] Nuttal T, Mueller R, Bensignor E, Verde M, Noli C, Schmidt V, Reme C (2009) Efficacy of a 0.0584% hydrocortisone aceponate spray in the lmanagement of canine atopic dermatitis: a randomised, double blind, placebo-controlled trial. Vet. Dermatol., 20, 191198. [27] Carlotti DN, Reme CA (2004) Efficacy of a soothing astringent topical spray for the management of Malassezia pododermatitis in dogs: a preliminary open-label clinical trial. Proc. BSAVA 47th Annual Congress, Birmingham, 103. [28] Löflath A, Von Voigts-Rhetz A, Jaeger K, Schmid M, Kuechenhoff H, Mueller RS (2007) The efficacy of a commercial shampoo and whirpooling in the treatment of canine pruritus – a double-blind, randomized, placebo-controlled study. Vet. Dermatol., 18, 427431. [29] Bourdeau P, Bruet V, Gremillet C (2007) Evaluation of phytosphingosine-containing shampoo and microemulsion spray in the clinical control of allergic dermatoses in dogs: preliminary results of a multicentre study. Vet. Dermatol., 18, 177-178 (abstract). [30] Deboer DJ, Griffin CE (2001) The ACVD task force on canine atopic dermatitis (XXI): antihistamine pharmacotherapy. Vet. Immunol. Immunopathol, 81, 323-329. THE LEADING COMPANY IN ALLERGY TESTING Artuvetrin Serum Test ® Reliable allergy test Comprehensive panels including Malassezia Easy to interpret results Full technical support and advice Hyposensitisation vaccine available within 8 working days P.O.Box 612 . 8200 AP Lelystad . The Netherlands Tel. 0031-320 267 900 . Fax: 0031-320 256 060 E-mail: [email protected] W W W . A R T U V E T R I N . C O M 275 DERMATOLOGY How to treat atopy in cats? E. Vidémont (1), D. Pin(1) SUMMARY Therapy of atopic dermatitis (AD) can be a challenge to the clinician’s therapeutic skills and selecting the best treatment plan for individual situations is an art. Cats diagnosed with AD are treated in a variety of ways depending upon the severity of clinical signs, duration or owner preference. Treatment options include allergen avoidance, treatment of aggravating factors, allergen specific immunotherapy (ASIT) and symptomatic therapy of pruritus. This article presents an update of these different options. and insect growth hormone regulators, and steam cleaning of sleeping areas [24]. This paper was commissioned by FECAVA for publication in EJCAP. Treatment of aggravating factors and disease Introduction Microbial proliferation Although bacterial [24] and Malassezia [22] overgrowth are less common in cats than in dogs, they can be observed in allergic cats and cause additional pruritus. These complications should be searched for by taking tape strip impressions and, treated, if present, with appropriate antimicrobial or antifungal therapy. Antiseptic shampoos, particularly those containing chlorhexidine, could help prevent relapse. In cats, shampoos are rarely used because cats have a reputation (often unjustified) for not liking being washed. However, shampoos, when it is possible to apply them easily, form an effective adjunctive therapy. Antiseptic solutions can now be applied in a spray formulation. Canine shampoos containing quaternary ammonium compounds and phenols can be toxic in cats and must be avoided. AD in cats is not well known and its pathophysiology is unclear. Some authors consider feline atopy to be similar to the human and canine form while others have obtained contradictory findings. There may be particular differences relating to cats but investigation of these has not been performed. There have been very few controlled studies in cats. Such studies that have been carried out must be examined critically partly because they often involve only small numbers of cats and partly because of differences in approach to diagnosis. For example, in some studies, there is confusion between flea bite hypersensitivity and AD. As in the dog, it is important to consider the hypersensitivity threshold concept. Each animal has its own pruritic threshold, the level of stimuli resulting in pruritus. Once this threshold is reached, additional stimuli will increase pruritus and other clinical signs. It is therefore important to reduce or eliminate additional stimuli. Infections must be searched for and treated. Strict flea control must be maintained. Dry skin Dry skin is associated with atopic dermatitis. The functional integrity of the epidermis relies particularly on intercorneocyte sheets of lipids. Disorders of epidermal lipid metabolism account for the defect in barrier function in atopic dog [23]. If we assume that a similar phenomenon occurs in the cat, several approaches can be used to restore epidermal barrier function. Allergen avoidance In practice, only food allergens can really be avoided. Avoidance of aeroallergens is only practical if the allergens concerned are in a limited area from which the allergic cat can be excluded. The most important allergens for cats in Europe are house dust mites and although various measures aimed at reducing their number can be recommended, these are only likely to be effective if combined with other procedures: very regular ventilation of the cats’ surroundings, frequent aeration of duvets, mattresses and blankets, use of a vacuum cleaner fitted with special filters, treatment of resting areas with a combination of insecticides • Essential fatty acids (EFA) The used of EFAs is proposed for several reasons: - They seem to contribute to the restoration of skin barrier function [23], - They have been shown to exert anti-inflammatory effects in various in vitro and in vivo models, and - They seem to have positive effects on the quality and luster of the hair coat. 1) Emilie Vidémont and Didier Pin, Unité Dermatologie, Ecole Nationale Vétérinaire de Lyon, France E-mail: [email protected] 276 EJCAP - Vol. 19 - Issue 3 December 2009 EFA products generally contain a mixture of gamma linolenic acid and eicosapentaenoic acid. EFAs can be administered in food as a capsule, oil or spray. For several years, EFAs have also been supplied in some dry pet foods. There are few reports on the effectiveness of fatty acid supplements to control pruritus in the cat [Table 1]. In several open trials [10, 11, 12, 19], cats with pruritus, eosinophilic granuloma complex (EGC) and miliary dermatitis secondary to flea bite hypersensitivity or atopy were treated with various combinations of evening primrose oil and fish oil. These studies suggest that cats respond favorably to EFA with variable efficacy. A double-blinded study by Logas et al. showed no significant difference between two groups of cats receiving either evening primrose oil liquid or olive oil [15]. Side-effects of EFA are very uncommon (occasional vomiting) but palatability is, often, considered to be poor. To summarise, EFA supplementation may improve coat condition but its true clinical efficacy remains uncertain. been performed in feline atopic patients and most information is anecdotal. The mechanism of action in both the canine and feline atopic patient has not been fully elucidated. For an effective response to ASIT, the relevant allergens must be selected, typically by identification of high levels of allergenspecific IgE in the sera and/or by positive skin test results to the allergen. One of the major problems in the cat is the low level of accuracy associated with these tests. [see previous article in this issue] The injection schedule is borrowed from canine medicine and depends on the company that prepares treatment. No standardisation exists in cats. The schedule involves injecting a gradually increasing amount of allergen over a period of several weeks (induction phase). This is then followed by a gradual reduction in the frequency of injections but leaving the amount of allergen constant (maintenance phase). Current recommendations [33] are to encourage owners to continue ASIT for at least 1 year before discontinuing therapy. Improvement may be monitored by the dose and frequency required of additional medications and the pruritus scores that owners have assigned to their pet during the course of the therapy. In cats that exhibit only minimal to moderate improvement during the first year of ASIT, the clinician and owner have to decide whether or not continuing ASIT provides therapeutic benefit to the patient. In patients that exhibit good to excellent response to ASIT after 6 months to 1 year, the recommendation would be to reduce gradually the frequency of the injections over the subsequent year. If, after one year, the cat’s allergies are controlled with no clinical signs attributable to allergy or need for other medications, the recommendation would be to discontinue the injections and monitor the patient for recurrence of clinical signs. Although immunotherapy is usually continued lifelong, it may, in a few cases, be discontinued after some years without recurrence of clinical signs. • Moisturisers and emollients They are useful in the treatment of dry skin. Products with propylene glycol, glycerine and urea can be used in cats. Psychogenetic factors A link has been established in man between anxiety and atopy, with stress aggravating the clinical signs. It is possible that a similar link exists in the cat. Severe, prolonged pruritus can induce a state of anxiety and behavioural problems. When cats have extensive lesions, especially on the face, marking is decreased. Moreover, owners are sometimes reluctant to stroke their pets. If anxiety or behavioural problems are suspected, behavioural therapy or treatment with pheromones or psychotropic drugs may be given. Several sedating antihistamines also have anxiolytic properties. It may be speculated that this is the reason for some of the beneficial effects of this group of drugs in atopy. Allergen-specific immunotherapy Allergen-specific immunotherapy is defined as the practice of administering gradually increasing quantities of an allergen extract in order to reduce or eliminate the signs associated with subsequent exposures to the causative allergen. Few studies have Reported success rates [Table 2] range from 50 to 100 % in feline atopic patients [3, 4, 9, 16, 25, 26]. However, a placebocontrolled trial demonstrating unequivocally that cats respond to immunotherapy would be useful. In the majority of studies, Tab. 1 Trials reporting treatment with EFA in management of feline AD. Study Product Patients Results Harvey 1991 [10] Evening Primrose oil + fish oil (Efa-Vet 2 capsules) 8 cats with military dermatitis 6 cats good response with absence of papules, decrease of pruritus and improvement in coat condition Harvey 1993 [12] Evening primrose oil (6 cats) or sunflower oil (5 cats) 11 cats with military dermatitis Improvement of all cats, better efficacy of evening primrose oil Harvey 1993 [11] Various combinations of 14 cats with military dermatitis evening primrose oil and fish oil Improvement with evening primrose oil. No effect of fish oil alone Miller 1993 [19] DVM Derm Caps LiquidTM 1 mL/9.1 kg once daily 14 days 28 cats with various pruritic dermatosis, military dermatitis and EGC Complete resolution in 13 cats At least 50 % improvement in 3 cats Logas 1993 [15] Double-blinded study. Evening Primrose oil versus olive oil 15 cats No significant differences between the two groups 277 How to treat atopy in cats? - E. Vidémont, D. Pin Studies and their result on ASIT in the cat Number of cats Response rate (%) Reedy 1982 [26] 20 55 % response McDougal 1986 [16] 13 69 % : good response 23 % : moderate response 8 % : bad response Carlotti 1988 [4] 6 66 % excellent response Prost 1992 [25] 28 78 % response Bettenay 1996 [3] 29 Overall success rate of 50 %. Success rate decreases after 3 years of follow-up Halliwell 1997 [9] 42 Improvement ranges from 53.3 % (hair loss) to 100 % (linear granuloma) according to the dermatologic signs Tab. 2 Trials reporting results of ASIT in the management of feline AD. period evaluation is short, generally under a year and it is interesting that success rate decreases when the follow-up period is longer. In a study by Bettenay [3], success rate after one year is similar to than in other studies but it decreases significantly after 3 years of treatment. It is unusual to rely on topical therapy alone because cats are adept at grooming away topical products. Hydrocortisone aceponate, now commercially available, could be used. Its rapid penetration of the stratum corneum and metabolism in the skin are interesting. Side-effects are rare and include worsening of clinical signs for a few hours to days, local reactions at injection site and anaphylaxis. Increased pruritus or local reactions can usually be managed by reducing the injection dose. The dose can later be increased gradually after a period of stabilisation. Even though life-threatening anaphylaxis is extremely rare, it is important to educate owners about this possibility. Anaphylaxis occurs within the first 30 to 60 minutes after the injection. Animals should be monitored during this time. If vomiting, diarrhoea, dyspnoea or collapse occur, the owner must seek immediate veterinary emergency care. The risk of inducing fibrosarcoma has never been investigated. Injectable preparations are popular, especially with cats that resent being given pills. Methylprednisolone acetate is often successful at a dose of 20 mg (or 4 mg/kg) every two to three weeks for a total of three injections [6]. Maintenance doses may be given every six to 12 weeks. Unfortunately, an initial beneficial response to injectable therapy can be followed by a reduced response and, consequently, a reduction in the interval between injections. Therefore, injectable methylprednisolone acetate should not be a standard therapy. Prednisolone or methylprednisolone are used orally at a dose of 1 to 2 mg/kg per day. After seven days, the dose should be reduced by 50 per cent for a further seven days followed by alternate day therapy and a search for the minimal effective dose. Some cats can be maintained on doses of 0.5-1 mg/kg on alternate day to alleviate pruritus. Cats have unpredictable absorption or metabolism (to the active form) of prednisone, which should not therefore be used in this species. Other oral steroids that may be useful in cases that fail to respond, or become resistant to the effects of the previously mentioned steroids, include oral triamcinolone (0.1-0.2 mg/kg/day) and dexamethasone (0.1-0.2 mg/kg/day). Their long duration of action requires an administration only every 3 days if they are used long-term [6]. Rush allergen specific immunotherapy (RIT) is a technique of advancing an allergic patient to a maintenance dose of an extract over a shorter period of time than that required for the traditional induction period. RIT would minimise the owner’s burden and may result in improved compliance. Typically, RIT is given over 8 hours as opposed to 25 days usually needed for induction. At present, RIT has been evaluated in 4 feline atopic patients [32] and in an experimental model of feline asthma [27]. Further studies are required. Symptomatic therapy of pruritus Intralesional injections of corticosteroid have been described for severe refractory indolent ulcer (IU) and eosinophilic granuloma (EG) but benefit remains unproven. Therapeutic options include the use of glucocorticoids, antihistamines, EFA and cyclosporin. Although glucocorticoids are effective and safer in cats than dogs, they are not without side-effects and often become less effective with time. Adverse effects include polydipsia, polyphagia, weight gain, diabetes mellitus, iatrogenic hyperadrenocorticism with fragile skin syndrome and urinary tract infections, dermatophytosis, demodicosis, and gastric ulceration. Glucocorticoids Until recently, corticosteroids were the mainstay of therapy for allergic cats. Glucocorticoids can be administered by injection, orally or topically. 278 EJCAP - Vol. 19 - Issue 3 December 2009 Drug Clemastine fumarate Hydroxyzine hydrochloride Mechanism of action H1-blocker antihistamine. Centrally mediated, synergistic with EFA Stabilizes mast cell membranes, centrally mediated Diphenhydramine Dosage 0.34-0.68 mg/cat PO BID Comments Study Diarrhea, lethargy, fixed Miller 1994 [20]: 10 drug eruption cats 0.68 mg/CT, response in 5/10 cats 1-10 mg/kg PO BID or TID Behavioral changes (hyperexcitability or depression), teratogenic Liquid form : alcohol base that cats strongly dislike Miller 1990 [18] Transient drowsiness, unpalatable (extremely 26 cats 2 mg/cat every bitter tasting) 12 hours. Excellent response in 73 % Polyphagia, behavioral Scott 1998 [31] changes, vocalization, 20 cats, 2 mg, q12h, sedation, vomiting, for 2 weeks. Good or affectionate behavior excellent response in 9 cats (side effects in 8 cats, severe in 3) 1-2 mg/kg BID to TID Chlorpheniramine maleate Centrally mediated 2-4 mg/cat PO SID to TID Cyproheptadine hydrochloride H1-blocker antihistamine and serotonin antagonist 2 mg/cat PO BID (1 mg/cat, q 24h, to 8 mg/cat, q8h) Tab. 3 Trials reporting treatment with antihistamines in the management of feline AD. Glucocorticoids can be considered a reasonable choice in animals with mild seasonal pruritus of only a few months duration but their long-term use should be undertaken with care. CsA is not licensed for use in cats. It is available as a solution or capsule. Dermatologists tend to use the microemulsion concentrate which is presumed to provide better absorption. It is not known if food affects the absorption of CsA in cats but a majority of authors recommend giving CsA at least 2 hours before or after meals. One study found no difference between the two formulations, although cats given capsules received a lower dose [34]. The liquid form allows more flexible dosing but is bitter tasting. Initial doses vary between 3.6 to 13.3 mg/ kg but in the majority of cases are about 5 mg/kg or 25 mg/cat once daily. CsA must be administrated once daily until complete remission of clinical signs, then in an alternate day regimen for least two months and eventually a twice weekly administration for an unlimited duration. If it is stopped immediately after remission of clinical signs, relapse will probably occur [8]. Therefore, it is important to prolong maintenance therapy by increasing the interval between administrations and searching for the minimal effective dose. Antihistamines Several antihistamines have been used in cats [Table 3]. There are no placebo-controlled studies of antihistamines in cats, so the dosages recommended are empirical and based on open trials. Efficacy is often low and very variable with different authors reporting a success rate of 20 to 73 % [6, 18, 20, 31]. Administer the antihistamine for at least three weeks before evaluating a patient’s response. If effective, antihistamines must usually be given once a day indefinitely. The success rate may be increased by trying several different antihistamines sequentially as patients may be responsive to one antihistamine but not to another. The advantage of antihistamines is the rare occurrence of side-effects. The main side-effects are increased appetite and sedation, although paradoxically, there can be hyperexcitability. Gastrointestinal signs are uncommon. The frequent administration (two to three times daily) limits their long-term use in many feline patients. In cats, successful use of CsA has been described principally in small, open and uncontrolled trials [Table 4]. Efficacy is generally very good. It is difficult however to compare the results of studies because formulation, clinical signs and evaluation period are different. Sometimes, the study period is too short [21], generally one month. This could lead to a lower success rate because remission of clinical signs may take longer than one month. In one study, pruritus and EG were the clinical signs which responded best, with a significant improvement seen after 10 days of treatment and complete remission after 30 days. However, it took 60 days to obtain complete remission of eosinophilic plaque (EP) lesions [8]. It is sometimes necessary to administer the drug once daily for two or three months before obtaining remission. Only one study compares the effects of prednisolone and CsA on skin lesions and pruritus in a doubleblind pattern [36]. The effect of CsA is approximatively 70 % and Antihistamines may be synergistic with glucocorticoids or EFAs. Essential fatty acids (EFAs) See part 3. Cyclosporin A (CsA) CsA is a potent inhibitor of cell-mediated immunity, and a less potent inhibitor of humoral immunity. CsA also has a variety of anti-inflammatory effects on leucocytes other than lymphocytes, and on other types of cell, including keratinocytes and endothelial cells [28]. 279 How to treat atopy in cats? - E. Vidémont, D. Pin Study Guaguère 2000 [8] Noli 2006 [21] Vercelli 2006 [34] Wisselink 2009 [36] Protocol Outcome 12 cats with ECG. 25 mg CsA/cat once By day 60, cats with EP and daily (4.9-12.5 mg/kg/day) for 2 months EG were completely cured. In 2 cases, relapse by day 90. In 3 cases of indolent ulcer, only partial regression 10 cats. 25 mg/cat once daily (3.6-8.3 Good to excellent mg/kg/day), preferably on an empty improvements was observed stomach, for one month in 40 % of cats for pruritus, 57 % of cats for alopecia, 60 % of cats for erythema and 50 % of cats for the total lesions. 15 cats with EGC 5.8 – 13.3 mg/kg Cure in all cats Solution once daily or caps twice a day, 2 h before or after meals, for one month.Then CsA continued every other day for 1 or 2 months until remission. Maintenance regimen: twice a week administration for an unlimited duration Study period: 6 months 29 cats Oral therapy for 4 weeks with No significant difference either one capsule of CsA 5 mg/kg SID between the two groups. (18 cats) or one capsule of prednisolone The effect of CsA is approximatively 70 % 1 mg/kg SID (11 cats) 2h before meals Side effects Mild diarrhea in one cat, which disappeared promptly with symptomatic therapy without the cessation of the ciclosporin therapy In one cat, capsules caused diarrhea, disappeared with liquid formulation 11 cats treated with CsA involving intermittent vomiting, diarrhea or loose stools, hyperactivity, increased appetite, polydipsia Tab. 4 Trials reporting treatment with cyclosporin A in the management of feline AD. no significant difference was found between the two groups. prior to initiation of immunomodulatory therapy, as well as during immunosuppressive therapy, might be helpful to detect seroconversion. When seroconversion occurs, or significant rises in toxoplasma antibody titres are observed in association with developing clinical illness in cats which were seropositive prior to initiation of immunosuppressive treatment, antitoxoplasma chemotherapy should be started immediately to prevent acute systemic toxoplasmosis. The main disadvantage of CsA is its high cost. In cats, few adverse reactions to CsA have been reported [29]. Gastrointestinal signs (vomiting, diarrhoea and anorexia) are most frequently reported. Other adverse events include salivation, headshaking, intermittent soft faeces, gingival hyperplasia [14], hyperactivity, increased appetite and polydipsia [36]. Vomiting can often be overcome by giving the drug with a very small amount of food. To minimise vomiting, the dose can be gradually increased or metoclopramide can initially be given concomitantly. These measures are difficult to apply in practice. It may be helpful to evaluate serological antibody status of cats for both A recent concern associated with CsA therapy is the increased risk of developing systemic toxoplasmosis and viral diseases. No publication exists at present concerning the association of viral diseases such as feline immunodeficiency virus (FIV) and feline leukemia virus (FeLV) with CsA treatment. In a study by Vercelli, no clinical expression of viral disease was apparent during the 6-month study period in the two cats found to be FIV-positive before CsA therapy [34]. Therapeutic doses of CsA have induced fatal toxoplasmosis in three cats following renal transplant surgery [2], two cats with atopy [1, 13] and one cat with immune-mediated haemolytic anaemia. Cats can develop systemic toxoplasmosis either by reactivation of latent infection or by primary infection. Precautions to consider during immunomodulatory therapy would include feeding only commercial cat food or other cooked foods, avoiding raw meat, poultry, viscera or bones and preventing hunting and scavenging. Monitoring of serological antibody status, for both IgG and IgM class antibodies to Toxoplasma gondii, both Tab. 5 General recommendations concerning the use of CsA in management of feline CsA. - Before treatment: Check for FIV/FeLV and toxoplasmosis serological status - In first intention: Microemulsion concentrate, capsules giving at least 2 hours before or after meal - Induction phase: One capsule of 25 mg/cat once daily until complete remission of clinical signs (sometimes two to three months) - Maintenance regimen: Increasing intervals between administrations and searching for the minimal effective dose. - Whole blood level of 250 to 500 ng/mL is recommended. Whole blood levels higher than 1000 ng/mL can cause side effects. Measuring blood CsA concentrations in cats 2 h after oral administration [17]. 280 EJCAP - Vol. 19 - Issue 3 December 2009 Treatment Dose Mode of action Side effects Chlorambucil 0.1 to 0.2 mg/kg daily or every other day, in combination with steroids DNA synthesis and inhibition of rapidly proliferating cells at all stages of the cell cycle Vomiting, diarrhea, anorexia and, more importantly, bone marrow suppression Gold salt therapy Chrysotherapy Sodium aurothiomalate 1 mg/kg intramuscularly every week, then every month variety of influences on immune function including neutrophil migration, lymphocyte function and immunoglobulin production glomerulonephritis, bone marrow suppression, thrombocytopenia and cutaneous eruption Megestrol acetate anti-inflammatory properties polyuria, polydispsia, mammary gland hyperplasia, behavioral problems, potentially irreversible diabetes mellitus, iatrogenic hyperadrenocorticism and, possibly, mammary neoplasia Tab. 6 Some of old treatments recommended in the literature in the management of ECG and pruritus in cats. [3] FIV/FeLV and toxoplasmosis before starting CsA. However, the risk seems to be low. Others treatments Several others treatments have been recommended in the literature, especially for the management of EGC lesions. All reports of these treatments are anecdotal with no proof of efficacy. [4] [5] [6] Old treatments include chlorambucil, aurothioglucose and progestagens [7]. These options are expensive, usually unlicensed, require careful monitoring and are not always effective [Table 6]. More recently, amoxicillin-clavulanate [35], an analogue of palmitolethanolamide called PLR-120 [30] and interferon α have been proposed [5] but further studies are necessary to evaluate these drugs. [7] [8] [9] Conclusion [10] Feline atopy is a disease recognised more frequently in recent years and there have been many studies concerning its management. In the majority of cases, a combination of treatments is needed. Topical treatments are often useful. The results of ASIT are very inconstant in cats. Antihistamines and essential fatty acids may be synergistic with others drugs but their efficacy is often low. Steroids, when used as long-term maintenance therapy, are associated with several side-effects. Cyclosporin may be a useful alternative therapy because it is safe and effective in most cases. However, the existence of a new antipruritic drug is no excuse for avoiding the difficult task of establishing a definitive diagnosis in the itchy cat! [11] [12] [13] [14] References [15] [1] [16] [2] Barrs VR, Martin P, Beatty JA. Antemortem diagnosis and treatment of toxoplasmosis in two cats on cyclosporin therapy. Aust Vet J. 2006; 84: 30-35. Bernsteen L, Gregory CR, Aronson LR, Lirtzman RA, Brummer DG. Acute toxoplasmosis following renal transplantation in three cats and a dog. J Am Vet Med Assoc. 1999; 215: 1123-1126. [17] 281 Bettenay SV. Response of hyposensitization in 29 atopic cats. In Advances in Veterinary Dermatology. Vol. 3. Eds : Kwochka KW, Willemse T, Von Tscharner C. Butterworth and Heinemann, Oxford, 1998. P 517-518. Carlotti DN, Prost C. L’atopie feline. Point Vét. 1988; 20: 777784. Fondati A. Feline eosinophilic skin diseases. In: Proceeding of the 18th annual congress of the ESVD-ECVD. Nice, France; 2002; p. 135-139. Foster A. Diagnosing and treating feline atopy. Vet Med. 2002: 226-240. Foster A. Clinical approach to feline eosinophilic granuloma complex. In Pract. 2003: 2-9. Guaguère E, Prélaud P. Efficacy of cyclosporine in the treatment of 12 cases of eosinophilic granuloma complex. Vet Dermatol. 2000; 11 (Suppl 1), S31. Halliwell REW. Efficacity of hyposensitization in feline allergic diseases based upon results of in vitro testing for allergen-specific immunoglobulin E. J Am Anim Hosp Assoc. 1997; 33: 282-288. Harvey RG. Management of feline military dermatitis by supplementing the diet with essential fatty acids. Vet Rec. 1991; 128: 326-329. Harvey RG. Effect of varying proportions of evening primrose oil and fish oil on cats with crusting dermatosis (“military dermatitis”). Vet Rec. 1993; 133: 208-211. Harvey RG. A comparison of evening primrose oil and sunflower oil for the management of papulocrustous dermatitis in cats. Vet Rec. 1993; 133: 571-573. Last RD, Suzuki Y, Manning T, Lindsay D, Galipeau L, Whitbread TJ. A case of fatal systemic toxoplasmosis in a cat being treated with cyclosporin A for feline atopy. Vet Dermatol. 2004; 15: 194198. Latimer KS, Rakich PM, Purswell BJ, Kircher IM. Effects of cyclosporine A administration in cats. Vet Immunol Immunopathol. 1986; 11: 161-173. Logas DB, Kunkle GA. Double-blinded study examining the effects of evening primrose oil on feline pruritis dermatitis. Vet Dermatol. 1993; 4: 181-184. McDougal BJ. Allergy testing and hyposensitization for 3 common feline dermatoses. Mod Vet Pract. 1986: 629-633. Mehl ML, Kyles AE, Craigmill AL, Epstein S, Gregory CR. Disposition of cyclosporine after intravenous and multi-dose oral administration in cats. J Vet Pharmacol Therap. 2003; 26: 349354. How to treat atopy in cats? - E. Vidémont, D. Pin [18] Miller WH, Scott DW. Efficacy of chlorpheniramine maleate for management of pruritus in cats. J Am Vet Med Assoc. 1990; 197: 67-70. [19] Miller WH, Scott DW, Wellington JR. Efficacity of DVM Derm Caps LiquidTM in the management of allergic and inflammatory dermatoses of the cat. J Am Anim Hosp Assoc. 1993; 29: 37-40. [20] Miller WH, Scott DW. Clemastine fumarate as an antipruritic agent in pruritic cats: results of an open clinical trial. Can Vet J .1994; 35: 502-504. [21] Noli C, Scarampella F. Prospective open pilot study on the use of ciclosporin for feline allergic skin disease. J Small Anim Pract. 2006; 47: 434-438. [22] Ordeix L, Galeotti F, Scarampella F, Dedola C, Bardagi M, Romano E, Fondati A. Malassezia spp. overgrowth in allergic cats. Vet Dermatol. 2007; 18: 316-323. [23] Piekutowska A, Pin D, Rème CA, Gatto H, Haftek M. Effects of a topically applied preparation of epidermal lipids on the stratum corneum barrier of atopic dogs. J Comp Pathol. 2008; 138: 197203. [24] Prélaud P, Gilbert S. Atopic dermatitis. In: A practical guide to feline dermatology. Eds Guaguère E, Prélaud P. Blackwell Science, Oxford. 2000: 101-108. [25] Prost C. Atopy in the cat: 28 cases. In: Proceeding of the Second World Congress of Veterinay Dermatology. Montreal, Quebec, Canada, 1992: 87. [26] Reedy LM. Results of allergy testing and hyposensitization in selected feline skin diseases. J Am Anim Hosp Assoc. 1982; 18: 618-623. [27] Reinero CR, Byerly JR, Berghaus RD, Berghaus LJ, Schelegle ES, Hyde DM, Gershwin LJ. Rush immunotherapy in an experimental [28] [29] [30] [31] [32] [33] [34] [35] [36] model of feline allergic asthma. Vet Immunol Immunopathol 2006; 110: 141-153. Robson D. Review of the properties and mechanisms of action of cyclosporine with an emphasis on dermatological therapy in dogs, cats and people. Vet Rec. 2003; 152: 768-772. Robson D. review of the pharmacokinetics, interactions and adverse reactions of cyclosporine in people, dogs and cats. Vet Rec. 2003; 152: 739-748. Scarampella F, Abramo F, Noli C. Clinical and histological evaluation of an analogue of palmitoythanolamide, PLR 120 (comicronized Palmidrol INN) in cats with eosinophilic granuloma and eosinophilic plaque: a pilot study. Vet Dermatol. 2001; 12: 29-39. Scott DW, Rothstein E, Beningo KE, Miller WH. Observations on the use of cyproheptadine hydrochloride as an antipruritic agent in allergic cats. Can Vet J. 1998; 39: 634-637. Trimmer AM, Griffin CE, Boord MJ, Rosenkrantz WS. Rush allergen specific immunotherapy protocol in feline atopic dermatitis: a pilot study of four cats. Vet Dermatol. 2005; 16: 324-329. Trimmer AM, Griffin CE, Rosenkrantz WS. Feline immunotherapy. Clin Tech Small Anim Pract. 2006; 21: 157-161. Vercelli A, Raviri G, Cornegliani L. The use of oral cyclosporin to treat feline dermatoses : a retrospective analysis of 23 cases. Vet Dermatol. 2006; 17: 201-206. Wildermuth BE, Griffin CE, Rosenkrantz WS. Response of feline eosinophilic cutaneous plaques and eosinophilic lip ulcers to amoxicillin-clavulanate therapy. Vet Dermatol. 2009; Abstract. 223. Wisselink MA, Willemse T. The efficacity of cyclosporine A in cats with presumed atopic dermatitis: a double blind randomized prednisolone-controlled study. Vet J. 2009; 180: 55-59 The big relief! For cats and dogs! The effective approach to allergy in dogs and cats starts with the Artuvetrin® Serum Test; the reliable allergy test that makes the allergen-specific IgE in the serum visible via the Fc region. Based on the outcome of this test, we can provide you with an allergen-specific vaccine: a big relief for allergy patients! The authority on animal allergies T E L . : + 3 1( 0 ) 3 2 0 - 2 6 7 9 0 0 - W W W. A R T U V E T R I N . C O M
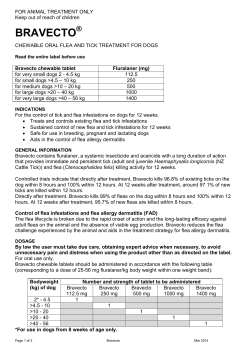








© Copyright 2026