
Ensuring Success p. 11 Remarkable Drive p. 23
Ensuring Success p. 11 UVA’s new approach to teaching medicine required an innovative method of gauging – and assuring – achievement. Remarkable Drive p. 23 How a pioneer in driving simulation is expanding the understanding of diabetes, ADHD and the teenage mind. Volume 3, 2013 Contents Volume 3, 2013 4 Letter From the Dean 5 Interprofessional Education A collaborative education initiative enables students from the School of Medicine and the School of Nursing to learn together – and from each other. 9 Cardiac Hypertrophy A massive new computational model of cardiac hypertrophy is facilitating the development of drugs and therapies for heart failure. 5 11 Developmental Assessment UVA’s developmental assessment program offers an innovative way of gauging, and ensuring, student success. 15 DNA Discovery Anindya Dutta’s discovery of “microDNA” outside chromosomes has been named one of 2012’s biggest research advances. 17 4 Breakthroughs The Department of Molecular Physiology and Biological Physics is producing groundbreaking discoveries at a remarkable pace. 21 OpenAnesthesia Edward C. Nemergut’s “OpenAnesthesia” site has become the field’s go-to graduate medical education resource. 11 15 23 27 23 Driving Simulation Could driving simulators offer an effective alternative to in-car tests? Virginia has enlisted a UVA researcher to find out. on the cover Simulations are just one way the School of Medicine’s innovative curriculum fosters critical thinking skills. Students from different disciplines work side by side. 27 Understanding Anthrax Research at the School of Medicine has upended science’s understanding of how cattle can be infected with deadly anthrax. 31 News and Notes Contents Volume 3, 2013 4 Letter From the Dean 5 Interprofessional Education A collaborative education initiative enables students from the School of Medicine and the School of Nursing to learn together – and from each other. 9 Cardiac Hypertrophy A massive new computational model of cardiac hypertrophy is facilitating the development of drugs and therapies for heart failure. 5 11 Developmental Assessment UVA’s developmental assessment program offers an innovative way of gauging, and ensuring, student success. 15 DNA Discovery Anindya Dutta’s discovery of “microDNA” outside chromosomes has been named one of 2012’s biggest research advances. 17 4 Breakthroughs The Department of Molecular Physiology and Biological Physics is producing groundbreaking discoveries at a remarkable pace. 21 OpenAnesthesia Edward C. Nemergut’s “OpenAnesthesia” site has become the field’s go-to graduate medical education resource. 11 15 23 27 23 Driving Simulation Could driving simulators offer an effective alternative to in-car tests? Virginia has enlisted a UVA researcher to find out. on the cover Simulations are just one way the School of Medicine’s innovative curriculum fosters critical thinking skills. Students from different disciplines work side by side. 27 Understanding Anthrax Research at the School of Medicine has upended science’s understanding of how cattle can be infected with deadly anthrax. 31 News and Notes letter from the dean In creating our new, next-generation curriculum at the University of Virginia School of Medicine, we wanted to free our students from lecture-hall seats and plunge them into an immersive, Steven T. DeKosky, MD, FAAN, FACP Vice President / Dean of the School of Medicine interactive learning experience. We wanted to break down the silos between disciplines and have our students learn not just from our faculty but from each other. In this issue, we highlight one way we’re doing just that. Our new interprofessional education program is bringing together students from the School of Medicine and the School of Nursing for common learning experiences that help them better appreciate each others’ roles and prepare them for some of the most complex challenges they will face, including difficult conversations about end-of-life care. It’s an exciting new approach, and our students are becoming better clinicians because of it. Our new curriculum also required us to devise new ways to evaluate and ensure student success. You’ll read about our innovative solution in this issue, along with stories on several major breakthroughs in the past few months. I am delighted to be able to share these stories with you, because they reflect the dynamic, collaborative culture we have established at the UVA School of Medicine. I hope you enjoy the issue! Interprofessional Education Bridging the gap between medical school and real-life practice. letter from the dean In creating our new, next-generation curriculum at the University of Virginia School of Medicine, we wanted to free our students from lecture-hall seats and plunge them into an immersive, Steven T. DeKosky, MD, FAAN, FACP Vice President / Dean of the School of Medicine interactive learning experience. We wanted to break down the silos between disciplines and have our students learn not just from our faculty but from each other. In this issue, we highlight one way we’re doing just that. Our new interprofessional education program is bringing together students from the School of Medicine and the School of Nursing for common learning experiences that help them better appreciate each others’ roles and prepare them for some of the most complex challenges they will face, including difficult conversations about end-of-life care. It’s an exciting new approach, and our students are becoming better clinicians because of it. Our new curriculum also required us to devise new ways to evaluate and ensure student success. You’ll read about our innovative solution in this issue, along with stories on several major breakthroughs in the past few months. I am delighted to be able to share these stories with you, because they reflect the dynamic, collaborative culture we have established at the UVA School of Medicine. I hope you enjoy the issue! Interprofessional Education Bridging the gap between medical school and real-life practice. W Measuring the abstract hen it comes to applying one’s education But putting a comprehensive workshop together is one thing; in the real world, healthcare professionals measuring its success is another. What makes an IPE program are uniquely familiar with the importance of effective? A recent $746,000 grant from the New York-based Unlike written test results that measure how much experiencing life “in the field.”The unpredictability of patients Josiah Macy Jr. Foundation has served as a valuable catalyst for information a student can retain on a given subject, and reactions from family members; the complexities of UVA to dig even deeper into this subject and pinpoint the measuring success in IPE is much more abstract. Success disease and the human body as an ever-changing organism; behaviors that must “stick” for IPE to be applied successfully is not determined by a student’s ability to memorize a and the overlapping responsibilities shared among doctors in a real-life clinical setting. script or perform the same simulation exercises over and over again. Success in IPE comes down to students’ and nurses are just a few variables at play in the clinical setting. “We constantly ask ourselves, ‘What is collaboration, behaviors and their ability to apply what they’ve learned in Because medical and nursing schools have vastly different and how do we measure it?’” said Leslie J. Blackhall, MD, unpredictable situations. curricula and schedules, it’s not unusual for recent graduates associate professor and expert clinician on interprofessional to enter the clinical environment without having “practiced” palliative end-of-life care. “Collaboration isn’t just two By developing “behavior checklists” that include the what situations would be like with a physician or nurse colleagues being nice to each other. It’s easy when everyone profession-specific and teamwork skills needed to care counterpart at their side. Interprofessional education (IPE) agrees. What happens when colleagues get along but they for patients in each of the four scenarios, the UVA IPE team experts at the UVA School of Medicine have changed that, disagree on something? What happens when someone has is able to see where students are excelling and where they and they’ve blazed a new trail along the way. to have a really difficult conversation with a patient or a family may need further coaching. John A. Owen, EdD, MSc, member? Our goal is to teach collaborative skills in a way coordinates data analysis for the study. Owen is an that students can readily apply their education to a range education evaluation expert on the Macy grant team. A new educational paradigm of real-life scenarios.” For the better part of a decade, UVA’s School of Medicine “There is a set of national guidelines for how these illnesses and School of Nursing have been working together to expand should be managed,” said Valentina L. Brashers, MD, IPE opportunities for students and create best practices for professor of nursing, founder and co-chair of UVA’s collaborative patient care. IPE initiative. “Guidelines cover the whole lifespan of a patient and run the gamut of care setting, from outpatient to inpatient to the ICU. The guidelines also tell you care should UVA’s IPE workshops are structured around one of four cases: 1Critical illness: adults in ICU with sepsis 2 3 4 Difficult conversations at end-of-life: adults with cancer Transitions from hospital to home: elderly patients with Alzheimer’s disease Chronic progressive illness: children with muscular dystrophy be provided in a team, but they don’t tell you how. i n novat i o n 7 W Measuring the abstract hen it comes to applying one’s education But putting a comprehensive workshop together is one thing; in the real world, healthcare professionals measuring its success is another. What makes an IPE program are uniquely familiar with the importance of effective? A recent $746,000 grant from the New York-based Unlike written test results that measure how much experiencing life “in the field.”The unpredictability of patients Josiah Macy Jr. Foundation has served as a valuable catalyst for information a student can retain on a given subject, and reactions from family members; the complexities of UVA to dig even deeper into this subject and pinpoint the measuring success in IPE is much more abstract. Success disease and the human body as an ever-changing organism; behaviors that must “stick” for IPE to be applied successfully is not determined by a student’s ability to memorize a and the overlapping responsibilities shared among doctors in a real-life clinical setting. script or perform the same simulation exercises over and over again. Success in IPE comes down to students’ and nurses are just a few variables at play in the clinical setting. “We constantly ask ourselves, ‘What is collaboration, behaviors and their ability to apply what they’ve learned in Because medical and nursing schools have vastly different and how do we measure it?’” said Leslie J. Blackhall, MD, unpredictable situations. curricula and schedules, it’s not unusual for recent graduates associate professor and expert clinician on interprofessional to enter the clinical environment without having “practiced” palliative end-of-life care. “Collaboration isn’t just two By developing “behavior checklists” that include the what situations would be like with a physician or nurse colleagues being nice to each other. It’s easy when everyone profession-specific and teamwork skills needed to care counterpart at their side. Interprofessional education (IPE) agrees. What happens when colleagues get along but they for patients in each of the four scenarios, the UVA IPE team experts at the UVA School of Medicine have changed that, disagree on something? What happens when someone has is able to see where students are excelling and where they and they’ve blazed a new trail along the way. to have a really difficult conversation with a patient or a family may need further coaching. John A. Owen, EdD, MSc, member? Our goal is to teach collaborative skills in a way coordinates data analysis for the study. Owen is an that students can readily apply their education to a range education evaluation expert on the Macy grant team. A new educational paradigm of real-life scenarios.” For the better part of a decade, UVA’s School of Medicine “There is a set of national guidelines for how these illnesses and School of Nursing have been working together to expand should be managed,” said Valentina L. Brashers, MD, IPE opportunities for students and create best practices for professor of nursing, founder and co-chair of UVA’s collaborative patient care. IPE initiative. “Guidelines cover the whole lifespan of a patient and run the gamut of care setting, from outpatient to inpatient to the ICU. The guidelines also tell you care should UVA’s IPE workshops are structured around one of four cases: 1Critical illness: adults in ICU with sepsis 2 3 4 Difficult conversations at end-of-life: adults with cancer Transitions from hospital to home: elderly patients with Alzheimer’s disease Chronic progressive illness: children with muscular dystrophy be provided in a team, but they don’t tell you how. i n novat i o n 7 We realized we needed to develop specific information about how this care should be provided by teams, and then work it into the curriculum organically.” The future of collaboration “Our team plans to extend this work throughout UVA Health System to involve practicing nurses and physicians in IPE projects,“ said Jeanne M. Erickson, PhD, RN, assistant professor of nursing and oncology nurse on the IPE team. “It’s important to align the education of our students with healthcare practitioners across disciplines. Interprofessional collaboration is essential for optimal quality and safety outcomes as well as cost savings in our healthcare systems.” UVA is already using the Collaborative Care Best Practice Model approach to create new IPE experiences. Plans are underway to partner with other Macy grantees, including the University of Washington and the National Center for Interprofessional Practice and Education, to expand the best practice model into graduate education and faculty development. “What happens when someone has to have a really difficult conversation with a patient or a family member? Our goal is to teach collaborative skills in a way that students can readily apply ... to a range of reallife scenarios.” - Leslie J. Blackhall, MD The interprofessional approach emphasizes not just the science of medicine but the skills and empathy necessary for dealing with the most difficult discussions. 8 i n novat i o n Cardiac Hypertrophy How UVA pioneered the most complete computational model ever created of the hypertrophy signaling network. We realized we needed to develop specific information about how this care should be provided by teams, and then work it into the curriculum organically.” The future of collaboration “Our team plans to extend this work throughout UVA Health System to involve practicing nurses and physicians in IPE projects,“ said Jeanne M. Erickson, PhD, RN, assistant professor of nursing and oncology nurse on the IPE team. “It’s important to align the education of our students with healthcare practitioners across disciplines. Interprofessional collaboration is essential for optimal quality and safety outcomes as well as cost savings in our healthcare systems.” UVA is already using the Collaborative Care Best Practice Model approach to create new IPE experiences. Plans are underway to partner with other Macy grantees, including the University of Washington and the National Center for Interprofessional Practice and Education, to expand the best practice model into graduate education and faculty development. “What happens when someone has to have a really difficult conversation with a patient or a family member? Our goal is to teach collaborative skills in a way that students can readily apply ... to a range of reallife scenarios.” - Leslie J. Blackhall, MD The interprofessional approach emphasizes not just the science of medicine but the skills and empathy necessary for dealing with the most difficult discussions. 8 i n novat i o n Cardiac Hypertrophy How UVA pioneered the most complete computational model ever created of the hypertrophy signaling network. Jeffrey J. Saucerman, PhD | In creating the most complete computational model of the hypertrophy signaling network yet, Saucerman and Ryall have facilitated the development of new drugs and therapies. enthusiasm, they report. “I think people are excited we’re starting to put all the parts together, rather than just having focused experiments on an individual pathway,” Ryall said. “There hasn’t been a lot done with cardiac hypertrophy in terms of putting it all together in this larger network.” Already the model has shed new light on cardiac hypertrophy. “I expected that certain downstream transcription factors or gene regulators would be most important,” Saucerman said. “But that’s really not what happens at all. Instead, the hypertrophy network has a bow-tie structure, with the protein Ras acting as a central controller of network activity.” I In addition to providing a better understanding of n creating their new model of cardiac hypertrophy, the causes of the condition, the model will have UVA’s Jeffrey J. Saucerman, PhD, and graduate long-term benefits for patients by facilitating the student Karen Ryall wanted to get at the big picture. development of drugs and new therapies for heart failure. “The models never completely eliminate The result is the most complete computational model of experiments,” Saucerman said, “but they make them the hypertrophy signaling network ever created — bigger much more efficient.” than the largest previous model by a factor of 15. Developmental “We know about individual players that have been shown Assessment: to affect hypertrophy, but there’s little known about how all these pieces are connected together as a working system to control how the heart grows,” explained Saucerman, an assistant professor of biomedical The School of Medicine curriculum gets a modern makeover – and innovative tools to gauge student success. engineering. “Our computational model integrates the different pathways and interactions that are known or thought to be involved in this process so we can run simulations to test which targets might be better for drugs or gene therapies.” Saucerman and Ryall have made the model freely available, both publishing the code and offering a user-friendly download. It’s been greeted with great 10 i n novat i o n “I think people are excited that we’re starting to put all the parts together,” said graduate student Karen Ryall. Jeffrey J. Saucerman, PhD | In creating the most complete computational model of the hypertrophy signaling network yet, Saucerman and Ryall have facilitated the development of new drugs and therapies. enthusiasm, they report. “I think people are excited we’re starting to put all the parts together, rather than just having focused experiments on an individual pathway,” Ryall said. “There hasn’t been a lot done with cardiac hypertrophy in terms of putting it all together in this larger network.” Already the model has shed new light on cardiac hypertrophy. “I expected that certain downstream transcription factors or gene regulators would be most important,” Saucerman said. “But that’s really not what happens at all. Instead, the hypertrophy network has a bow-tie structure, with the protein Ras acting as a central controller of network activity.” I In addition to providing a better understanding of n creating their new model of cardiac hypertrophy, the causes of the condition, the model will have UVA’s Jeffrey J. Saucerman, PhD, and graduate long-term benefits for patients by facilitating the student Karen Ryall wanted to get at the big picture. development of drugs and new therapies for heart failure. “The models never completely eliminate The result is the most complete computational model of experiments,” Saucerman said, “but they make them the hypertrophy signaling network ever created — bigger much more efficient.” than the largest previous model by a factor of 15. Developmental “We know about individual players that have been shown Assessment: to affect hypertrophy, but there’s little known about how all these pieces are connected together as a working system to control how the heart grows,” explained Saucerman, an assistant professor of biomedical The School of Medicine curriculum gets a modern makeover – and innovative tools to gauge student success. engineering. “Our computational model integrates the different pathways and interactions that are known or thought to be involved in this process so we can run simulations to test which targets might be better for drugs or gene therapies.” Saucerman and Ryall have made the model freely available, both publishing the code and offering a user-friendly download. It’s been greeted with great 10 i n novat i o n “I think people are excited that we’re starting to put all the parts together,” said graduate student Karen Ryall. The remodeled curriculum features built-in assessment tools and progress checkpoints that keep students on top of course material in a more readily applicable way. Instead of traditional hour-long lectures, students start many classes Located in the School of Medicine’s $40.7 million Claude Moore Medical Education Building, the Medical Simulation Center lets healthcare trainees practice skills and case scenarios in clinical settings that mimic actual situations. “These are all skills that physicians continually develop throughout their careers; our goal is to give UVA medical students a head start.” Randolph J. Canterbury, MD Senior Associate Dean for Education Charting a new course T with self-assessment tests to gauge their understanding of the material before continuing on to a test case or application exercise. These exercises then reinforce critical thinking skills, and SOM faculty members are able to get a clearer picture he days of rote learning and regurgitating facts have been replaced by a more hands-on of students’ progress before they move on to more approach encouraging students to be lifelong learners, thanks to a new developmental advanced stages in the program. assessment program headed by Randolph J. Canterbury, MD, senior associate dean for education at the UVA School of Medicine. While memorization is an important component of medical education, it’s only one part of a Professors link to students’ laptops using interactive technology, while podcasts give students the freedom to listen to and review lecture as often as needed to absorb the material. larger quation. Knowing the body inside and out and understanding the pathology of disease are part of a solid foundation. By teaching students earlier how to apply this knowledge in real Simulation is a key element in the modern curriculum, time – with real and simulated patients and in unpredictable situations – UVA is fostering a creating a safe environment for students to make mistakes new generation of medical students who will be able to handle clinical roles more intuitively. and think through what went wrong. Students participate in A curriculum for modern times “Our new curriculum was born out of the realization the cookie-cutter model of lectures, written tests and ‘putting in your time’ was very outdated and impractical,” Canterbury said. “The standard four-year curriculum has been around for more than a century, yet about half of all medical knowledge becomes obsolete every five years. Healthcare is changing at such an accelerated pace it only makes sense to reevaluate how we’re educating our future practitioners.” simulation exercises as early as their first year, putting their knowledge of emergency life support into practice and getting comfortable in group learning sessions. Problem-solving group sessions serve as a glimpse into the reality of healthcare today; instead of one standardized patient and one doctor, it’s a patient, a doctor and an interprofessional team, reinforcing what students learn in class and encouraging them to think collaboratively. Empathy. Confidence. Patience. Compassion. Surveys show that these are some of the most sought-after qualities patients look for in a physician. The new curriculum gives students a chance to develop these skills long before they graduate and head off to residency. i n novat i o n 13 The remodeled curriculum features built-in assessment tools and progress checkpoints that keep students on top of course material in a more readily applicable way. Instead of traditional hour-long lectures, students start many classes Located in the School of Medicine’s $40.7 million Claude Moore Medical Education Building, the Medical Simulation Center lets healthcare trainees practice skills and case scenarios in clinical settings that mimic actual situations. “These are all skills that physicians continually develop throughout their careers; our goal is to give UVA medical students a head start.” Randolph J. Canterbury, MD Senior Associate Dean for Education Charting a new course T with self-assessment tests to gauge their understanding of the material before continuing on to a test case or application exercise. These exercises then reinforce critical thinking skills, and SOM faculty members are able to get a clearer picture he days of rote learning and regurgitating facts have been replaced by a more hands-on of students’ progress before they move on to more approach encouraging students to be lifelong learners, thanks to a new developmental advanced stages in the program. assessment program headed by Randolph J. Canterbury, MD, senior associate dean for education at the UVA School of Medicine. While memorization is an important component of medical education, it’s only one part of a Professors link to students’ laptops using interactive technology, while podcasts give students the freedom to listen to and review lecture as often as needed to absorb the material. larger quation. Knowing the body inside and out and understanding the pathology of disease are part of a solid foundation. By teaching students earlier how to apply this knowledge in real Simulation is a key element in the modern curriculum, time – with real and simulated patients and in unpredictable situations – UVA is fostering a creating a safe environment for students to make mistakes new generation of medical students who will be able to handle clinical roles more intuitively. and think through what went wrong. Students participate in A curriculum for modern times “Our new curriculum was born out of the realization the cookie-cutter model of lectures, written tests and ‘putting in your time’ was very outdated and impractical,” Canterbury said. “The standard four-year curriculum has been around for more than a century, yet about half of all medical knowledge becomes obsolete every five years. Healthcare is changing at such an accelerated pace it only makes sense to reevaluate how we’re educating our future practitioners.” simulation exercises as early as their first year, putting their knowledge of emergency life support into practice and getting comfortable in group learning sessions. Problem-solving group sessions serve as a glimpse into the reality of healthcare today; instead of one standardized patient and one doctor, it’s a patient, a doctor and an interprofessional team, reinforcing what students learn in class and encouraging them to think collaboratively. Empathy. Confidence. Patience. Compassion. Surveys show that these are some of the most sought-after qualities patients look for in a physician. The new curriculum gives students a chance to develop these skills long before they graduate and head off to residency. i n novat i o n 13 DNA Discovery ‘Who knew that microDNA segments could be transmitted independently of chromosomes?’ Designed with the patient in mind “The old curriculum was backwards,” Canterbury said. “Students were taught a bunch of facts about anatomy, physiology, biochemistry and so forth, and then they were thrown into clinical situations without really knowing how to apply that knowledge to individual patient cases. Problem-solving group sessions serve as a glimpse into the reality of healthcare today. “Our new model teaches students early on how to communicate with patients, how to ask questions and obtain a comprehensive medical history, how to have difficult conversations with patients and family members, how to use their clinical reasoning skills to determine the best course of action for the patient, and how to work collaboratively with their healthcare colleagues. These are all skills that physicians continually develop throughout their careers; our goal is to give UVA medical students a head start.” 14 i n novat i o n The Next-Generation Curriculum is designed around five key areas: 1 Basic scientific knowledge acquired through lectures, reading and written tests 2 Communication skills - such as how to talk with patients and ask the right questions the right way 3 Physical examination skills practiced on real and standardized patients 4 Clinical reasoning skills 5 Technical skills - such as inserting central lines, often practiced in the Medical Simulation Center DNA Discovery ‘Who knew that microDNA segments could be transmitted independently of chromosomes?’ Designed with the patient in mind “The old curriculum was backwards,” Canterbury said. “Students were taught a bunch of facts about anatomy, physiology, biochemistry and so forth, and then they were thrown into clinical situations without really knowing how to apply that knowledge to individual patient cases. Problem-solving group sessions serve as a glimpse into the reality of healthcare today. “Our new model teaches students early on how to communicate with patients, how to ask questions and obtain a comprehensive medical history, how to have difficult conversations with patients and family members, how to use their clinical reasoning skills to determine the best course of action for the patient, and how to work collaboratively with their healthcare colleagues. These are all skills that physicians continually develop throughout their careers; our goal is to give UVA medical students a head start.” 14 i n novat i o n The Next-Generation Curriculum is designed around five key areas: 1 Basic scientific knowledge acquired through lectures, reading and written tests 2 Communication skills - such as how to talk with patients and ask the right questions the right way 3 Physical examination skills practiced on real and standardized patients 4 Clinical reasoning skills 5 Technical skills - such as inserting central lines, often practiced in the Medical Simulation Center Anindya Dutta, MD, PhD| A team led by Dutta discovered free-floating circles of DNA outside chromosomes in normal tissues. The “microdeletions” that produce the little loops appear to be creating a mosaic of genetically varied cells within the same tissue. Yoshiyuki Shibata, PhD | Shibata and the other members of Dutta’s team are continuing to explore the implications of the discovery. I t was one of 2012’s biggest research advances, behind “microdeletions” in the chromosomal DNA, proclaimed the director of the National Institute of producing a mosaic of genetically varied cells within the Mental Health. “Who knew,” Thomas R. Insel, MD, same tissue – possibly leading to functional differences wrote, “that microDNA segments could be transmitted between the cells. independently of chromosomes?” “In most cases, the microdeletions are silent,” Dutta said. He was describing the discovery of short circles of a cell’s “But occasionally, just from sheer chance, they could own DNA floating outside chromosomes in normal affect a gene important for function of that particular cell tissues, as reported by a team led by UVA’s Anindya in that particular tissue. There are all these diseases Dutta, MD, PhD. Those little loops have upended we look at – schizophrenia, autism, manic-depressive longstanding beliefs about DNA and could impact psychosis – for which we think there is a genetic diseases ranging from autism to schizophrenia. connection but we can never find the mutations in specific genes. Perhaps this is why: some of the genetic “We have always been taught that in each cell division that differences creep in as the cells in the brain are born. occurs during the development of normal tissues the We’ll never find those genetic lesions by looking at the machinery that copies our genetic material, the DNA in genetic material in the blood cells of the patient, as is our chromosomes, makes perfect copies to be passed commonly done when we evaluate the genes on to the daughter cells,” said Dutta, chair of the School of of a patient.” Medicine’s Department of Biochemistry and Molecular Genetics. “The free-floating circles of DNA are suggesting Dutta and his team are continuing to explore implications this is not always true.” of the finding, published to much interest in Science. “I’ve never had this kind of a reaction to a discovery,” Dutta Dutta and his team concluded that the excision of these said. “It makes you appreciate that we’re in unknown circles from chromosomal DNA occasionally leaves territory, looking at something we haven’t seen before.” 4 Breakthroughs High-profile papers speak to the work of the Department of Molecular Physiology and Biological Physics. Anindya Dutta, MD, PhD| A team led by Dutta discovered free-floating circles of DNA outside chromosomes in normal tissues. The “microdeletions” that produce the little loops appear to be creating a mosaic of genetically varied cells within the same tissue. Yoshiyuki Shibata, PhD | Shibata and the other members of Dutta’s team are continuing to explore the implications of the discovery. I t was one of 2012’s biggest research advances, behind “microdeletions” in the chromosomal DNA, proclaimed the director of the National Institute of producing a mosaic of genetically varied cells within the Mental Health. “Who knew,” Thomas R. Insel, MD, same tissue – possibly leading to functional differences wrote, “that microDNA segments could be transmitted between the cells. independently of chromosomes?” “In most cases, the microdeletions are silent,” Dutta said. He was describing the discovery of short circles of a cell’s “But occasionally, just from sheer chance, they could own DNA floating outside chromosomes in normal affect a gene important for function of that particular cell tissues, as reported by a team led by UVA’s Anindya in that particular tissue. There are all these diseases Dutta, MD, PhD. Those little loops have upended we look at – schizophrenia, autism, manic-depressive longstanding beliefs about DNA and could impact psychosis – for which we think there is a genetic diseases ranging from autism to schizophrenia. connection but we can never find the mutations in specific genes. Perhaps this is why: some of the genetic “We have always been taught that in each cell division that differences creep in as the cells in the brain are born. occurs during the development of normal tissues the We’ll never find those genetic lesions by looking at the machinery that copies our genetic material, the DNA in genetic material in the blood cells of the patient, as is our chromosomes, makes perfect copies to be passed commonly done when we evaluate the genes on to the daughter cells,” said Dutta, chair of the School of of a patient.” Medicine’s Department of Biochemistry and Molecular Genetics. “The free-floating circles of DNA are suggesting Dutta and his team are continuing to explore implications this is not always true.” of the finding, published to much interest in Science. “I’ve never had this kind of a reaction to a discovery,” Dutta Dutta and his team concluded that the excision of these said. “It makes you appreciate that we’re in unknown circles from chromosomal DNA occasionally leaves territory, looking at something we haven’t seen before.” 4 Breakthroughs High-profile papers speak to the work of the Department of Molecular Physiology and Biological Physics. T he manuscripts Department chair since 2007, Mark J. Yeager, MD, PhD, has fostered were published in an atmosphere of communication, collaboration and mentorship. top journals Science, He’s worked to attract and retain top-tier faculty, and equip them with Nature and Nature Methods, by scientists in the Department of Molecular Physiology and Biological Physics, which provides a research-intensive T he discovery of a mechanism by which hemoglobin controls delivery of nitric oxide may point to a new the tools, technology and facilities needed to produce cutting-edge research. “Historically, it’s been a strong department, and I wanted therapeutic target for treating high blood to fortify that,” Yeager says of his arrival at UVA. “It was important to pressure and have far-reaching implications leverage that critical mass of excellence to recruit the next generation for organ systems and illnesses. of excellence.” environment for training undergraduate, graduate Analyzing the successes of his department, Yeager credits the backing and medical students and of UVA leadership and the enterprise and ingenuity of his faculty. postdoctoral fellows. The “Elements allowing this to happen were a shared vision across the papers were notable for breakthrough discoveries and their appearance within university combined with existing excellence in the department. We’re fortunate to have strong backing from the Board of Visitors, the provost, UVA research, led by Brant E. Isakson, PhD, Jochen Zimmer, DPhil I n a discovery that could have major ramifications for biofuel production and the battle against bacterial infections, UVA’s Jochen Zimmer, DPhil, and colleagues shows a complete system within the myoendothelial junction – the “bridge” between smooth muscle and endothelial cells lining blood vessel walls – allowing hemoglobin the vice president of research and the dean of the School of Medicine, have deciphered the secrets of cellulose production, the to regulate nitric oxide delivery, essentially timing was coincidental, it as well as philanthropic support,” Yeager said. “We have assembled a most common natural polymer on Earth. controlling the size of the blood vessel. speaks to the caliber, ambition group of exceptional scientists faced with common problems but each and breadth of research here. performing unique science.” weeks of each other. Although In their Nature paper, Zimmer, Jacob L.W. Morgan and Joanna Strumillo first determined the components necessary to produce and secrete cellulose and then mapped out the three-dimensional architecture of the enzyme complex responsible for cellulose production. The enzyme is unique in both producing cellulose polymers and pushing them outside the cell simultaneously; usually the division of labor is different, with production and movement handled separately or by different enzymes. The findings are of particular interest to the federal Department of Energy, which is seeking ways to facilitate the production of biofuels. Understanding the production and deposition of cellulose, the primary component of plant cell The mechanism may play a role in other parts walls, may lead to new ways to tear it down or create plants of the body, as well as in many illnesses. with weaker walls. “There are scattered reports of hemoglobin Similarly, the UVA findings may offer new targets for battling and [nitric oxide signaling] expressed in the bacteria and preventing infections. Cellulose is one of the lungs, for example, and in neurons. Maybe components that bacteria produce to form biofilms that allow it’s very similar to what we show here: They them to clump together and cling to surfaces. “If we can prevent biofilm formation, we would expect to make it easier Mark J. Yeager, MD, PhD | Yeager (center) is chair of the Department of Molecular Physiology and Biological Physics. His department is producing groundbreaking research on a wide array of topics. Brant E. Isakson, PhD form this macromolecular complex and can to get rid of the bacteria,” Zimmer says. “You could also very tightly regulate how much nitric oxide is prevent them from adhering to surgical devices and other delivered,” Isakson says. tools used in hospitals.” i n novat i o n 19 T he manuscripts Department chair since 2007, Mark J. Yeager, MD, PhD, has fostered were published in an atmosphere of communication, collaboration and mentorship. top journals Science, He’s worked to attract and retain top-tier faculty, and equip them with Nature and Nature Methods, by scientists in the Department of Molecular Physiology and Biological Physics, which provides a research-intensive T he discovery of a mechanism by which hemoglobin controls delivery of nitric oxide may point to a new the tools, technology and facilities needed to produce cutting-edge research. “Historically, it’s been a strong department, and I wanted therapeutic target for treating high blood to fortify that,” Yeager says of his arrival at UVA. “It was important to pressure and have far-reaching implications leverage that critical mass of excellence to recruit the next generation for organ systems and illnesses. of excellence.” environment for training undergraduate, graduate Analyzing the successes of his department, Yeager credits the backing and medical students and of UVA leadership and the enterprise and ingenuity of his faculty. postdoctoral fellows. The “Elements allowing this to happen were a shared vision across the papers were notable for breakthrough discoveries and their appearance within university combined with existing excellence in the department. We’re fortunate to have strong backing from the Board of Visitors, the provost, UVA research, led by Brant E. Isakson, PhD, Jochen Zimmer, DPhil I n a discovery that could have major ramifications for biofuel production and the battle against bacterial infections, UVA’s Jochen Zimmer, DPhil, and colleagues shows a complete system within the myoendothelial junction – the “bridge” between smooth muscle and endothelial cells lining blood vessel walls – allowing hemoglobin the vice president of research and the dean of the School of Medicine, have deciphered the secrets of cellulose production, the to regulate nitric oxide delivery, essentially timing was coincidental, it as well as philanthropic support,” Yeager said. “We have assembled a most common natural polymer on Earth. controlling the size of the blood vessel. speaks to the caliber, ambition group of exceptional scientists faced with common problems but each and breadth of research here. performing unique science.” weeks of each other. Although In their Nature paper, Zimmer, Jacob L.W. Morgan and Joanna Strumillo first determined the components necessary to produce and secrete cellulose and then mapped out the three-dimensional architecture of the enzyme complex responsible for cellulose production. The enzyme is unique in both producing cellulose polymers and pushing them outside the cell simultaneously; usually the division of labor is different, with production and movement handled separately or by different enzymes. The findings are of particular interest to the federal Department of Energy, which is seeking ways to facilitate the production of biofuels. Understanding the production and deposition of cellulose, the primary component of plant cell The mechanism may play a role in other parts walls, may lead to new ways to tear it down or create plants of the body, as well as in many illnesses. with weaker walls. “There are scattered reports of hemoglobin Similarly, the UVA findings may offer new targets for battling and [nitric oxide signaling] expressed in the bacteria and preventing infections. Cellulose is one of the lungs, for example, and in neurons. Maybe components that bacteria produce to form biofilms that allow it’s very similar to what we show here: They them to clump together and cling to surfaces. “If we can prevent biofilm formation, we would expect to make it easier Mark J. Yeager, MD, PhD | Yeager (center) is chair of the Department of Molecular Physiology and Biological Physics. His department is producing groundbreaking research on a wide array of topics. Brant E. Isakson, PhD form this macromolecular complex and can to get rid of the bacteria,” Zimmer says. “You could also very tightly regulate how much nitric oxide is prevent them from adhering to surgical devices and other delivered,” Isakson says. tools used in hospitals.” i n novat i o n 19 A groundbreaking new technique developed by Gary K. Owens, PhD, and colleagues is allowing scientists to examine histone modifications of genetic loci – a process that regulates gene expression – in single cells. The technique enables researchers, for the first time, to analyze the process within individual cell types that make up complex tissues, overcoming a major limitation of traditional analysis and offering unprecedented opportunities for understanding mechanisms contributing to development of human diseases. The UVA researchers believe their technique may have broad applications for most biomedical areas, including elucidating mechanisms that contribute to development of complex tissues. A valuable feature of this new method is it can be used to study Michael C. Wiener, PhD B y cracking the molecular structure of the enzyme Ste24p, Michael C. Wiener, PhD, and colleagues have shed new light on early aging diseases in children. The finding may lead to new treatments and provide better understanding of the aging process in humans, as well as facilitate redevelopment of HIV medications to avoid side effects, such as diabetes. mechanisms of gene regulation in single cells in fixed histological sections, including large archives Wiener and fellow UVA Center for Membrane Biology of human autopsy specimens. Although developed researchers Peter S. Horanyi, PhD, and Edward E. to look at histone modifications at single gene loci in Pryor Jr., PhD, collaborated with groups from individual cells, it may be adapted to looking at any protein-DNA interactions. Hauptman-Woodward Medical Research Institute and University of Rochester School of Medicine and Dentistry to determine the molecular structure of the enzyme, publishing their findings in Science. The team focused on Ste24p because defects in the protein in humans are responsible for a number of progerias. (In humans, improper processing and assembly of lamins lead to laminopathies, which include muscular dystrophy, cardiomyopathies and progerias.) In addition, some frequently used HIV and AIDS medications used in Highly Active Antiretroviral Therapy (HAART) also interact with Ste24p, altering how patients taking the drugs metabolize fat and leading to side effects, including insulin resistance and diabetes. Gary K. Owens, PhD Knowing how the protein is structured could aid 20 The method was described in an article in Nature researchers in developing drugs to treat progerias Methods authored by Delphine Gomez, Laura S. and assist in the redesign of HAART medications to avoid Shankman, Anh T. Nguyen and Owens. side effects, Wiener says. i n novat i o n OpenAnesthesia How a UVA researcher created the online destination for graduate education in anesthesia. A groundbreaking new technique developed by Gary K. Owens, PhD, and colleagues is allowing scientists to examine histone modifications of genetic loci – a process that regulates gene expression – in single cells. The technique enables researchers, for the first time, to analyze the process within individual cell types that make up complex tissues, overcoming a major limitation of traditional analysis and offering unprecedented opportunities for understanding mechanisms contributing to development of human diseases. The UVA researchers believe their technique may have broad applications for most biomedical areas, including elucidating mechanisms that contribute to development of complex tissues. A valuable feature of this new method is it can be used to study Michael C. Wiener, PhD B y cracking the molecular structure of the enzyme Ste24p, Michael C. Wiener, PhD, and colleagues have shed new light on early aging diseases in children. The finding may lead to new treatments and provide better understanding of the aging process in humans, as well as facilitate redevelopment of HIV medications to avoid side effects, such as diabetes. mechanisms of gene regulation in single cells in fixed histological sections, including large archives Wiener and fellow UVA Center for Membrane Biology of human autopsy specimens. Although developed researchers Peter S. Horanyi, PhD, and Edward E. to look at histone modifications at single gene loci in Pryor Jr., PhD, collaborated with groups from individual cells, it may be adapted to looking at any protein-DNA interactions. Hauptman-Woodward Medical Research Institute and University of Rochester School of Medicine and Dentistry to determine the molecular structure of the enzyme, publishing their findings in Science. The team focused on Ste24p because defects in the protein in humans are responsible for a number of progerias. (In humans, improper processing and assembly of lamins lead to laminopathies, which include muscular dystrophy, cardiomyopathies and progerias.) In addition, some frequently used HIV and AIDS medications used in Highly Active Antiretroviral Therapy (HAART) also interact with Ste24p, altering how patients taking the drugs metabolize fat and leading to side effects, including insulin resistance and diabetes. Gary K. Owens, PhD Knowing how the protein is structured could aid 20 The method was described in an article in Nature researchers in developing drugs to treat progerias Methods authored by Delphine Gomez, Laura S. and assist in the redesign of HAART medications to avoid Shankman, Anh T. Nguyen and Owens. side effects, Wiener says. i n novat i o n OpenAnesthesia How a UVA researcher created the online destination for graduate education in anesthesia. Edward C. Nemergut, MD (right) , edits OpenAnesthesia with the aid of Julie Huffmyer, MD, and Robert Thiele, MD. O penAnesthesia is at a turning point. It’s It’s a group effort, an international collaboration. Nemergut not the number of page views the site has still does much heavy lifting, but he’s assisted by an able team received – now measured in millions – or of editors at UVA and other top institutions, from Duke to the number of visitors – more than 50,000 and growing Johns Hopkins. fast – but the scope of knowledge it contains. Despite the rapid growth, one thing has remained constant, The site, www.openanesthesia.org, has become the Nemergut said: “I think we’re still true to our underlying go-to destination for graduate education in anesthesia. goal of users sharing what they know with other users and It’s a collaborative community of people eager to learn improving the understanding of the community.” and share, a place where the field’s latest discoveries can travel instantly around the globe, an enormous library of anesthesia information, tools, quizzes and podcasts. It’s a vast resource, and it’s getting bigger by the day. “It may be reaching the point where it contains a It’s a vast resource and it’s getting bigger every day. breadth of information that really doesn’t exist in a single source that I know of,” said UVA’s Edward C. The site is getting sleek new graphics, so that its appearance Nemergut, MD, an associate professor of anesthesia matches the quality of its content. Nemergut likens at the School of Medicine. the upgrade to a new coat of paint, and he has other improvements in mind. But he’s also eager to see what his The site is Nemergut’s brainchild, and he looks after it collaborators have in store, to see what new tool or resource daily, creating content, guiding its direction, providing gets added, what idea gets shared. summaries of the latest journal issue from the site’s sponsor, the International Anesthesia Research Society. Like many in his field, he’s excited to see where But OpenAnesthesia long ago became something more. OpenAnesthesia goes next. 22 i n novat i o n Driving Simulation Groundbreaking discoveries emerge from behind the wheel. Edward C. Nemergut, MD (right) , edits OpenAnesthesia with the aid of Julie Huffmyer, MD, and Robert Thiele, MD. O penAnesthesia is at a turning point. It’s It’s a group effort, an international collaboration. Nemergut not the number of page views the site has still does much heavy lifting, but he’s assisted by an able team received – now measured in millions – or of editors at UVA and other top institutions, from Duke to the number of visitors – more than 50,000 and growing Johns Hopkins. fast – but the scope of knowledge it contains. Despite the rapid growth, one thing has remained constant, The site, www.openanesthesia.org, has become the Nemergut said: “I think we’re still true to our underlying go-to destination for graduate education in anesthesia. goal of users sharing what they know with other users and It’s a collaborative community of people eager to learn improving the understanding of the community.” and share, a place where the field’s latest discoveries can travel instantly around the globe, an enormous library of anesthesia information, tools, quizzes and podcasts. It’s a vast resource, and it’s getting bigger by the day. “It may be reaching the point where it contains a It’s a vast resource and it’s getting bigger every day. breadth of information that really doesn’t exist in a single source that I know of,” said UVA’s Edward C. The site is getting sleek new graphics, so that its appearance Nemergut, MD, an associate professor of anesthesia matches the quality of its content. Nemergut likens at the School of Medicine. the upgrade to a new coat of paint, and he has other improvements in mind. But he’s also eager to see what his The site is Nemergut’s brainchild, and he looks after it collaborators have in store, to see what new tool or resource daily, creating content, guiding its direction, providing gets added, what idea gets shared. summaries of the latest journal issue from the site’s sponsor, the International Anesthesia Research Society. Like many in his field, he’s excited to see where But OpenAnesthesia long ago became something more. OpenAnesthesia goes next. 22 i n novat i o n Driving Simulation Groundbreaking discoveries emerge from behind the wheel. and symptoms their blood sugar is affecting their driving and give them the skills to deal with the problem. “It’s really cool because you can do this intervention in the privacy of your own home,” Cox said. “You don’t have to admit to anybody that you have hypoglycemia and driving problems. You don’t have to be close to a major medical center or the University of Virginia. You could be in Wyoming or California or Hawaii.” Cox now enjoys a strong relationship with many The simulation work has shed light on topics ranging from Attention Deficit/Hyperactivity Disorder to diabetes to the development of teenagers’ brains. diabetes advocates and groups, but he had to overcome some initial hostility. “We’ve done a whole series of studies on driving and diabetes,” Cox said. don’t raise blood sugar very quickly,” Cox said. “The “Originally the diabetes community was really angry only thing that really affects blood sugar quickly is with us, because we were documenting a problem. dextrose tablets.” I kept explaining to people, we have to understand the phenomenon before we can help you.” Cox’s latest projects represent the culmination of years of work in driving simulation, dating UVA’s driving simulator plunges users into an immersive driving experience, one allowing scenarios too dangerous on the roads. W His research has produced some surprising findings, back to the 1990s. After being impressed with findings that sometimes run contrary to conventional the immersiveness of a driving arcade game, he wisdom about diabetes. “It turns out to be extremely contacted an Atari ® engineer who agreed to help specific what they should eat [to combat hypoglycemia]. develop a driving simulator. This led to a 20 year hen the Commonwealth of Virginia wanted to allowing drivers to face treacherous conditions and It’s not orange juice, it’s not Coca-Cola®® ® , not their relationship and the current simulator consider whether high-tech simulators could unexpected hazards that would be simply too dangerous favorite candy or ice cream. A lot of these things (GeneralSimulation.com). “We were trying to one day offer an alternative to in-car road tests, in the real world (http://uvahealth.com/blog/index. evaluate the effects of low blood sugar, or php/2013/03/29/simulating-the-driving-experience/). hypoglycemia, that people with type 1 diabetes To determine drivers’ reactions to the technology, Cox and frequently have, on a functional skill,” Cox recalled. Lawmakers had already relied on his research in deciding to the state have installed simulators at two Department of “We’d done all the studies bringing patients into the lower the legal blood alcohol concentration for driving from Motor Vehicles locations. Drivers come in to renew their hospital, infusing IV insulin in them, to produce 1.0 percent to .08 percent. And Cox had spent years license or conduct other business and, while they’re there, hypoglycemia and having them do the regular conducting pioneering driving simulation research, using have a chance to try the technology of tomorrow and offer simulation to evaluate the effects of conditions ranging from feedback. Cox is collecting data and opinions from the diabetes to Attention Deficit/Hyperactivity Disorder on experiment so he can compile a report for state lawmakers. state officials turned to UVA’s Daniel J. Cox, PhD. driving skills. His research has shed light on executive function, cognitive development, the effects of aging and much Cox sees many potential advantages to using the simulator for more, while producing useful tools for people with diabetes road tests, including ensuring fairness. “Wherever you were and other drivers to reduce their risk behind the wheel. evaluated, you would be held to the same standards,” he said. Now his work could shape the future of driver evaluation in Even with that major project under way, he’s also developing Virginia – and possibly beyond. Cox, a professor of psychiatry an Internet program to help people with diabetes manage and neurobehavioral sciences at the School of Medicine, is their condition while behind the wheel (diabetesdriving.com). testing whether simulators could offer a safer and more The online intervention, now the subject of a clinical trial, aims discriminating alternative to in-car driving evaluations, to teach people with diabetes to become aware of the signs i n novat i o n 25 and symptoms their blood sugar is affecting their driving and give them the skills to deal with the problem. “It’s really cool because you can do this intervention in the privacy of your own home,” Cox said. “You don’t have to admit to anybody that you have hypoglycemia and driving problems. You don’t have to be close to a major medical center or the University of Virginia. You could be in Wyoming or California or Hawaii.” Cox now enjoys a strong relationship with many The simulation work has shed light on topics ranging from Attention Deficit/Hyperactivity Disorder to diabetes to the development of teenagers’ brains. diabetes advocates and groups, but he had to overcome some initial hostility. “We’ve done a whole series of studies on driving and diabetes,” Cox said. don’t raise blood sugar very quickly,” Cox said. “The “Originally the diabetes community was really angry only thing that really affects blood sugar quickly is with us, because we were documenting a problem. dextrose tablets.” I kept explaining to people, we have to understand the phenomenon before we can help you.” Cox’s latest projects represent the culmination of years of work in driving simulation, dating UVA’s driving simulator plunges users into an immersive driving experience, one allowing scenarios too dangerous on the roads. W His research has produced some surprising findings, back to the 1990s. After being impressed with findings that sometimes run contrary to conventional the immersiveness of a driving arcade game, he wisdom about diabetes. “It turns out to be extremely contacted an Atari ® engineer who agreed to help specific what they should eat [to combat hypoglycemia]. develop a driving simulator. This led to a 20 year hen the Commonwealth of Virginia wanted to allowing drivers to face treacherous conditions and It’s not orange juice, it’s not Coca-Cola®® ® , not their relationship and the current simulator consider whether high-tech simulators could unexpected hazards that would be simply too dangerous favorite candy or ice cream. A lot of these things (GeneralSimulation.com). “We were trying to one day offer an alternative to in-car road tests, in the real world (http://uvahealth.com/blog/index. evaluate the effects of low blood sugar, or php/2013/03/29/simulating-the-driving-experience/). hypoglycemia, that people with type 1 diabetes To determine drivers’ reactions to the technology, Cox and frequently have, on a functional skill,” Cox recalled. Lawmakers had already relied on his research in deciding to the state have installed simulators at two Department of “We’d done all the studies bringing patients into the lower the legal blood alcohol concentration for driving from Motor Vehicles locations. Drivers come in to renew their hospital, infusing IV insulin in them, to produce 1.0 percent to .08 percent. And Cox had spent years license or conduct other business and, while they’re there, hypoglycemia and having them do the regular conducting pioneering driving simulation research, using have a chance to try the technology of tomorrow and offer simulation to evaluate the effects of conditions ranging from feedback. Cox is collecting data and opinions from the diabetes to Attention Deficit/Hyperactivity Disorder on experiment so he can compile a report for state lawmakers. state officials turned to UVA’s Daniel J. Cox, PhD. driving skills. His research has shed light on executive function, cognitive development, the effects of aging and much Cox sees many potential advantages to using the simulator for more, while producing useful tools for people with diabetes road tests, including ensuring fairness. “Wherever you were and other drivers to reduce their risk behind the wheel. evaluated, you would be held to the same standards,” he said. Now his work could shape the future of driver evaluation in Even with that major project under way, he’s also developing Virginia – and possibly beyond. Cox, a professor of psychiatry an Internet program to help people with diabetes manage and neurobehavioral sciences at the School of Medicine, is their condition while behind the wheel (diabetesdriving.com). testing whether simulators could offer a safer and more The online intervention, now the subject of a clinical trial, aims discriminating alternative to in-car driving evaluations, to teach people with diabetes to become aware of the signs i n novat i o n 25 “We know that driving is the leading cause of death among adolescents, and that’s attributed frequently to inexperience and poor judgment.” U nderstanding Anthrax - Daniel J. Cox, PhD Daniel J. Cox, PhD | Cox’s groundbreaking research using driving simulation has made him a valued resource for Virginia lawmakers. cognitive tests, the neuropsychological tests. We’d “We know that driving is the leading cause of death find deficits, but what do deficits of 2 milliseconds among adolescents, and that’s attributed frequently mean in the real world, in terms of reaction times?” to inexperience and poor judgment. Turns out that about half the novice drivers don’t have accidents, Driving simulation gave him the answer. “Trying to but they all have inexperience,” Cox said. “The logic think of a universal functional skill is hard. You try is that poor judgment is possibly more important to think of something that almost everybody does. than the inexperience, and poor judgment could Well, now it could be use of a cell phone, but back be reflected by what we call executive function. It’s then, cell phones weren’t ubiquitous,” Cox said. “One a complex cognitive ability that doesn’t completely thing almost everybody does is drive. Not only is it a mature until about age 25.” universal activity, but it’s a universal activity with real-world impacts, both positive and negative.“ There’s still more work to be done on that study, just one of many projects he has underway – such as his Driving can be particularly dangerous for novice new efforts with traumatic brain injury and driving, drivers, especially teenagers first setting out behind and autism and driving. the wheel. Cox is looking into why some teens make for safer drivers than others. It’s not just a question of personality, Cox suspects, but of developmental physiology. 26 i n novat i o n For Cox, one of the nation’s foremost driving simulation experts, there is always a new discovery down the road. How UVA researchers upended conventional wisdom about the spread of B. anthracis. “We know that driving is the leading cause of death among adolescents, and that’s attributed frequently to inexperience and poor judgment.” U nderstanding Anthrax - Daniel J. Cox, PhD Daniel J. Cox, PhD | Cox’s groundbreaking research using driving simulation has made him a valued resource for Virginia lawmakers. cognitive tests, the neuropsychological tests. We’d “We know that driving is the leading cause of death find deficits, but what do deficits of 2 milliseconds among adolescents, and that’s attributed frequently mean in the real world, in terms of reaction times?” to inexperience and poor judgment. Turns out that about half the novice drivers don’t have accidents, Driving simulation gave him the answer. “Trying to but they all have inexperience,” Cox said. “The logic think of a universal functional skill is hard. You try is that poor judgment is possibly more important to think of something that almost everybody does. than the inexperience, and poor judgment could Well, now it could be use of a cell phone, but back be reflected by what we call executive function. It’s then, cell phones weren’t ubiquitous,” Cox said. “One a complex cognitive ability that doesn’t completely thing almost everybody does is drive. Not only is it a mature until about age 25.” universal activity, but it’s a universal activity with real-world impacts, both positive and negative.“ There’s still more work to be done on that study, just one of many projects he has underway – such as his Driving can be particularly dangerous for novice new efforts with traumatic brain injury and driving, drivers, especially teenagers first setting out behind and autism and driving. the wheel. Cox is looking into why some teens make for safer drivers than others. It’s not just a question of personality, Cox suspects, but of developmental physiology. 26 i n novat i o n For Cox, one of the nation’s foremost driving simulation experts, there is always a new discovery down the road. How UVA researchers upended conventional wisdom about the spread of B. anthracis. B. anthracis can attack Acanthamoeba Ian J. Glomski, PhD | Glomski and his colleagues discovered an unexpected way anthrax can spread. castellanii and other amoebas (and potentially other protozoa as well) because the bacterium contains two plasmids needed for growth, the UVA researchers believe. This was borne out in the lab, where tests using an anthrax strain without plasmids generated no additional spores. That information could help scientists begin to determine which genes allow B. anthracis to reproduce in amoeba. “We may find other species of amoeba that are even better at this than what we were using in the lab,” said UVA researcher Paul S. Hoffman, PhD, a professor of infectious diseases. “We may be at the tip of the iceberg.” The UVA researchers began pursuing their A unconventional line of thought after a discussion with nthrax typically strikes livestock after “Amoebas, in their cyst state, sit in their seed form rainy weather in warm summer months. waiting for the right conditions, much like the anthrax Usually those animals have been grazing spores,” explained UVA researcher Ian J. Glomski, an in depressions where the grass is greenest. So it’s assistant professor of microbiology. “So they’re in long been assumed that rainwater runoff depressions in the soil as well. When it rains, the concentrates spores of the bacteria that cause amoeba come out of their dormancy and potentially anthrax in low-lying areas, allowing them to sit, eat things like spores – including Bacillus anthracis.” dormant, until consumed by an unwitting animal. While amoebas typically eat bacteria and kill them, germinate and do their deadly work. B. anthracis is able to manipulate the amoeba so it But it turns out the anthrax bacterium Bacillus can grow inside, essentially turning the amoeba into an anthrax incubator allowing B. anthracis to overcome its primary challenge to reproducing in the science suspected. To find out, the UVA team set out to recreate the warm, wet conditions in the lab. When the researchers placed germination. But when they combined spores and Acanthamoeba castellanii, the result came quickly: There was a nearly fiftyfold increase in spores within 72 hours. Under optimal conditions of approximately 37 degrees Celsius, the spores increased nearly a hundredfold. In enabling B. anthracis to reproduce, the amoeba is at the UVA School of Medicine have determined “The bacteria that are naturally in the soil are much B. anthracis has an effective way to reproduce and better competitors,” Glomski explained. “Basically all grow while in the soil. It can do so, UVA researchers the other bacteria eat up what it would like to eat, so discovered, by attacking a common soil and water it doesn’t do very well.” But once devoured by the amoeba, Acanthamoeba castellanii. It’s a process that amoeba, B. anthracis has what it needs. become a more effective pathogen. there was more happening in the warm, moist earth than soil: competition. anthracis isn’t content just to lurk and wait. Researchers both allows the bacterium to grow its numbers and to knowledgeable about amoebas. Perhaps, Dey suggested, spores in sterile creek water, nothing happened. No Then, once inside their host, the bacteria can There are whole fields where cattle can’t graze without dying. Rafik Dey, an enterprising postdoctoral fellow breeding a more effective pathogen, making it a greater threat to mammals and people, Glomski said. “The interactions with the amoeba, essentially, are making certain that the anthrax has the tools to kill the amoebas, and those same tools are potentially being used to infect animals and humans,” he said. Paul S. Hoffman, PhD | In terms of implications of the discovery, “we may be at the tip of the iceberg,” B. anthracis can attack Acanthamoeba Ian J. Glomski, PhD | Glomski and his colleagues discovered an unexpected way anthrax can spread. castellanii and other amoebas (and potentially other protozoa as well) because the bacterium contains two plasmids needed for growth, the UVA researchers believe. This was borne out in the lab, where tests using an anthrax strain without plasmids generated no additional spores. That information could help scientists begin to determine which genes allow B. anthracis to reproduce in amoeba. “We may find other species of amoeba that are even better at this than what we were using in the lab,” said UVA researcher Paul S. Hoffman, PhD, a professor of infectious diseases. “We may be at the tip of the iceberg.” The UVA researchers began pursuing their A unconventional line of thought after a discussion with nthrax typically strikes livestock after “Amoebas, in their cyst state, sit in their seed form rainy weather in warm summer months. waiting for the right conditions, much like the anthrax Usually those animals have been grazing spores,” explained UVA researcher Ian J. Glomski, an in depressions where the grass is greenest. So it’s assistant professor of microbiology. “So they’re in long been assumed that rainwater runoff depressions in the soil as well. When it rains, the concentrates spores of the bacteria that cause amoeba come out of their dormancy and potentially anthrax in low-lying areas, allowing them to sit, eat things like spores – including Bacillus anthracis.” dormant, until consumed by an unwitting animal. While amoebas typically eat bacteria and kill them, germinate and do their deadly work. B. anthracis is able to manipulate the amoeba so it But it turns out the anthrax bacterium Bacillus can grow inside, essentially turning the amoeba into an anthrax incubator allowing B. anthracis to overcome its primary challenge to reproducing in the science suspected. To find out, the UVA team set out to recreate the warm, wet conditions in the lab. When the researchers placed germination. But when they combined spores and Acanthamoeba castellanii, the result came quickly: There was a nearly fiftyfold increase in spores within 72 hours. Under optimal conditions of approximately 37 degrees Celsius, the spores increased nearly a hundredfold. In enabling B. anthracis to reproduce, the amoeba is at the UVA School of Medicine have determined “The bacteria that are naturally in the soil are much B. anthracis has an effective way to reproduce and better competitors,” Glomski explained. “Basically all grow while in the soil. It can do so, UVA researchers the other bacteria eat up what it would like to eat, so discovered, by attacking a common soil and water it doesn’t do very well.” But once devoured by the amoeba, Acanthamoeba castellanii. It’s a process that amoeba, B. anthracis has what it needs. become a more effective pathogen. there was more happening in the warm, moist earth than soil: competition. anthracis isn’t content just to lurk and wait. Researchers both allows the bacterium to grow its numbers and to knowledgeable about amoebas. Perhaps, Dey suggested, spores in sterile creek water, nothing happened. No Then, once inside their host, the bacteria can There are whole fields where cattle can’t graze without dying. Rafik Dey, an enterprising postdoctoral fellow breeding a more effective pathogen, making it a greater threat to mammals and people, Glomski said. “The interactions with the amoeba, essentially, are making certain that the anthrax has the tools to kill the amoebas, and those same tools are potentially being used to infect animals and humans,” he said. Paul S. Hoffman, PhD | In terms of implications of the discovery, “we may be at the tip of the iceberg,” While the availability of a T veterinary vaccine helps he UVA findings, published by the journal Applied and Environmental Microbiology, could prove instrumental in preventing anthrax outbreaks in many areas of the world. While the prevent outbreaks in the News & Notes U.S., other countries lack access to the vaccine. availability of a veterinary vaccine helps prevent outbreaks in the U.S., other countries lack access to The finding also offers new targets for researchers the vaccine, meaning that there are whole fields where seeking to prevent the spread of anthrax, Glomski cattle can’t graze without dying, Hoffman said. said. “If we can figure out any way to disrupt the cycle, that would effectively eliminate the problem. “Just the knowledge [of what is happening in the soil] It could be doing something to the bacterium, doing gives you a general sense of where not to put your something to the amoeba, doing something to animals if you do have problems,” Hoffman said. “In prevent their interaction.” he said. “If we really developing countries that don’t have a lot of resources, understand those interactions, we’ll have more and you can strategize how to avoid certain areas because more points of intervention to think about.” you know that will be problematic at a particular period of the year.” Dunlap to succeed DeKosky as dean of School of Medicine Nancy E. Dunlap, MD, PhD, MBA, will become the new dean of the UVA School of Medicine upon the retirement of Dean Steven T. DeKosky, MD, FAAN, FACP. DeKosky is stepping down this summer to return to teaching and focus on his groundbreaking research into Alzheimer’s disease and traumatic brain injury. Dunlap, a pulmonologist, comes to UVA from the National Governors Association Center for UVA’s executive vice president and provost. Dunlap is expected to be with UVA for at least 18 months as UVA hires a new executive vice president for health affairs. Before joining the National Governors Association, Dunlap served with distinction at the University of Alabama at Birmingham, concluding her time there as professor of medicine and business. She also served as vice chairwoman for clinical affairs, vice president of the UAB Health System for Ambulatory Services and chief of staff and chief operating officer for the Kirklin Clinic, a sizable multi-specialty academic clinic. Best Practices in Washington, D.C. “Dr. Dunlap’s strong record of accomplishments as a faculty member, researcher and administrator, coupled with her familiarity with the complex and changing health care environment, makes her the best person to lead the School of Medicine during this important time of transition,” said John D. Simon, PhD, 30 i n novat i o n i n novat i o n 31 While the availability of a T veterinary vaccine helps he UVA findings, published by the journal Applied and Environmental Microbiology, could prove instrumental in preventing anthrax outbreaks in many areas of the world. While the prevent outbreaks in the News & Notes U.S., other countries lack access to the vaccine. availability of a veterinary vaccine helps prevent outbreaks in the U.S., other countries lack access to The finding also offers new targets for researchers the vaccine, meaning that there are whole fields where seeking to prevent the spread of anthrax, Glomski cattle can’t graze without dying, Hoffman said. said. “If we can figure out any way to disrupt the cycle, that would effectively eliminate the problem. “Just the knowledge [of what is happening in the soil] It could be doing something to the bacterium, doing gives you a general sense of where not to put your something to the amoeba, doing something to animals if you do have problems,” Hoffman said. “In prevent their interaction.” he said. “If we really developing countries that don’t have a lot of resources, understand those interactions, we’ll have more and you can strategize how to avoid certain areas because more points of intervention to think about.” you know that will be problematic at a particular period of the year.” Dunlap to succeed DeKosky as dean of School of Medicine Nancy E. Dunlap, MD, PhD, MBA, will become the new dean of the UVA School of Medicine upon the retirement of Dean Steven T. DeKosky, MD, FAAN, FACP. DeKosky is stepping down this summer to return to teaching and focus on his groundbreaking research into Alzheimer’s disease and traumatic brain injury. Dunlap, a pulmonologist, comes to UVA from the National Governors Association Center for UVA’s executive vice president and provost. Dunlap is expected to be with UVA for at least 18 months as UVA hires a new executive vice president for health affairs. Before joining the National Governors Association, Dunlap served with distinction at the University of Alabama at Birmingham, concluding her time there as professor of medicine and business. She also served as vice chairwoman for clinical affairs, vice president of the UAB Health System for Ambulatory Services and chief of staff and chief operating officer for the Kirklin Clinic, a sizable multi-specialty academic clinic. Best Practices in Washington, D.C. “Dr. Dunlap’s strong record of accomplishments as a faculty member, researcher and administrator, coupled with her familiarity with the complex and changing health care environment, makes her the best person to lead the School of Medicine during this important time of transition,” said John D. Simon, PhD, 30 i n novat i o n i n novat i o n 31 182 Best Doctors Best Doctors in America® ® recognizes outstanding physicians at UVA The School of Medicine, nationally recognized for its outstanding primary care program, saw more than 40 percent of its Class of 2013 enter the field of primary care. U.S.News & World Report ranks the School of Medicine 18th in the nation for primary care. It’s fitting, then, that 58 of 145 members of the Class of 2013 chose to enter the field. UVA Health System saw 182 of its physicians named to the 2013 Best Doctors in America®® List by Best Doctors Inc. Only about 5 percent of U.S. doctors earn a spot on the prestigious roll, according to Best Doctors. Selections to the list are based on physician surveys. According to Best Doctors, physicians are asked questions including, “If you or a loved one needed a doctor in your specialty, to whom would you refer them?” After compiling an initial list of candidates through the survey, Best Doctors extensively evaluates the nominated physicians, reviewing their credentials and clinical activity, to determine the honorees. “I am pleased to see so many of our physicians highlighted by their fellow doctors for providing high-quality patient care,” Dean DeKosky said. “Awards such as Best Doctors reflect not only the dedication of our physicians but the entire team of healthcare providers here at UVA Health System.” Primary care, a UVA strength, a hot field for Class of 2013 The top five most popular residencies for the class: 1 2 Internal medicine: 23 3 Anesthesiology: 14 4 Family practice: 9 5 Orthopaedics: 8 Pediatrics: 19 Graduates will continue their training in 32 states and Washington, D.C., with class members heading to prestigious institutions such as Yale, Johns Hopkins, Vanderbilt, Duke and Harvard. Twenty-five graduates will be doing all or part of their residencies at UVA. UVA’s Erik L. Hewlett, MD, a professor of medicine, infectious diseases and international health, has received Virginia’s highest honor for college faculty. The State Council of Higher Education for Virginia presented Hewlett with a 2013 Outstanding Faculty Award, recognizing his many accomplishments in teaching, research and public service. “I love all the aspects of my work at the university – teaching, research, clinical medicine and development of translational research – and appreciate very much the opportunities I have had in the course of these activities,” Hewlett said. Professor earns state’s highest honor for college faculty In a letter of support for Hewlett’s nomination, Dean DeKosky described Hewlett’s service to the university as “legendary.” “What is most impressive to me is the impact he has made as a teacher,” DeKosky wrote. “There is no better teacher than one who is actively expanding the body of knowledge in that discipline.” 182 Best Doctors Best Doctors in America® ® recognizes outstanding physicians at UVA The School of Medicine, nationally recognized for its outstanding primary care program, saw more than 40 percent of its Class of 2013 enter the field of primary care. U.S.News & World Report ranks the School of Medicine 18th in the nation for primary care. It’s fitting, then, that 58 of 145 members of the Class of 2013 chose to enter the field. UVA Health System saw 182 of its physicians named to the 2013 Best Doctors in America®® List by Best Doctors Inc. Only about 5 percent of U.S. doctors earn a spot on the prestigious roll, according to Best Doctors. Selections to the list are based on physician surveys. According to Best Doctors, physicians are asked questions including, “If you or a loved one needed a doctor in your specialty, to whom would you refer them?” After compiling an initial list of candidates through the survey, Best Doctors extensively evaluates the nominated physicians, reviewing their credentials and clinical activity, to determine the honorees. “I am pleased to see so many of our physicians highlighted by their fellow doctors for providing high-quality patient care,” Dean DeKosky said. “Awards such as Best Doctors reflect not only the dedication of our physicians but the entire team of healthcare providers here at UVA Health System.” Primary care, a UVA strength, a hot field for Class of 2013 The top five most popular residencies for the class: 1 2 Internal medicine: 23 3 Anesthesiology: 14 4 Family practice: 9 5 Orthopaedics: 8 Pediatrics: 19 Graduates will continue their training in 32 states and Washington, D.C., with class members heading to prestigious institutions such as Yale, Johns Hopkins, Vanderbilt, Duke and Harvard. Twenty-five graduates will be doing all or part of their residencies at UVA. UVA’s Erik L. Hewlett, MD, a professor of medicine, infectious diseases and international health, has received Virginia’s highest honor for college faculty. The State Council of Higher Education for Virginia presented Hewlett with a 2013 Outstanding Faculty Award, recognizing his many accomplishments in teaching, research and public service. “I love all the aspects of my work at the university – teaching, research, clinical medicine and development of translational research – and appreciate very much the opportunities I have had in the course of these activities,” Hewlett said. Professor earns state’s highest honor for college faculty In a letter of support for Hewlett’s nomination, Dean DeKosky described Hewlett’s service to the university as “legendary.” “What is most impressive to me is the impact he has made as a teacher,” DeKosky wrote. “There is no better teacher than one who is actively expanding the body of knowledge in that discipline.” University of Virginia School of Medicine | PO Box 800793 | Charlottesville, VA 22908 | medicine.virginia.edu









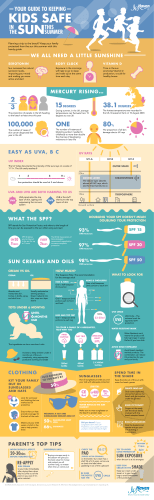
© Copyright 2026