ABC
docz
Explore
Log in
Create new account
Download
Report
No category
Foley Catheter Management Protocol
Document 110822
The BVI International Arbitration Centre (BVI IAC) has an
BVI 6100
IE 201 – Sample Midterm Questions
AIM Statement Next Steps Run Chart Reduce CAUTIs from 2011 baseline
What is TransParenting? **
5.24.15 bulletin - new life church of foley
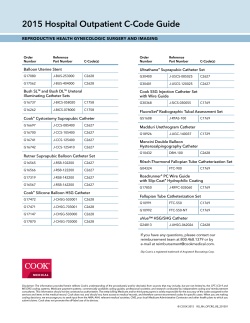
Reproductive Health Hospital Outpatient C-Code
Scott Foresman Science
Assistant Program Director, John H. Stroger, Jr. Hospital; Assistant Professor
© Copyright 2026
About abcdocz
DMCA / GDPR
Report