
Camp Make New Friends Spy Camp 2014
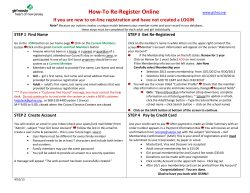
This summer hang with the girls at Camp Make New Friends Spy Camp 2014 July 21-24, 2014 (Monday-Thursday) Camp Make New Friends is a community outreach camp designed as an introductory program for girls who are not currently Girl Scouts. WHO: Girls in Grades K through 5th grade* *2013-2014 school year WHERE: A.S. Rhodes Elementary HOURS: 9:00 a.m.– 3:00 p.m. FEE: $20 for week • (Financial Assistance available) Make checks payable to GSCNC Message Decoding Finding clues • • • Laser Field Much More! Includes: Membership * Songs * Crafts * Games *Snack *T-shirt *Special Guests Mail Registration and Fee to: Camp Make New Friends Girl Scout Council of the Nation’s Capital 153 McMillan Court Martinsburg, WV 25404 FREE BUS TRANSPORTATION AVAILABLE FROM SHENANDOAH COUNTY Or you can register online at: http://www.gscnc.org/Camp_Make_New_Friends.html CAMP WILL FILL-UP QUICKLY, REGISTER NOW ! Application on the back FOR INFORMATION CONTACT: Beverly Soule 540-313-4191 [email protected] 2014 Registration for Make New Friends—July 21-25, 2014; $20 for the week (payable to GSCNC) Please only 1 girl per form, form may be duplicated Child’s Name: __________________________________________________ Age: School: __ State: Is the girl currently registered as a Girl Scout? No Yes, Troop # Date of Birth: Grade: Address: Apartment # _______________ City: _______ State: (13/14 school year) ZIP Code: Mother/Guardian: _______ E-mail: Phone: Day Evening: ______ Cell: Father/Guardian: ______ _E-mail: Phone: Day Evening: ______ Cell: If divorced or legally separated, please indicate the custodial parent(s): Must have information for emergency contact if parent(s) cannot be reached (please print clearly): Name/ Relationship: Phone: Name/ Relationship: Phone: Please select a bus stop: ___Stonewall Jackson High School ___Strasburg High School ___Central High School ___Parents will drop off and pick up T-shirt Size (please indicate youth S,M,L,XL or Adult S,M,L,XL) ________________________________________________ We encourage you to voluntarily provide the following information on racial background and ethnicity. This information will be used by Girl Scouts of the USA to help improve outreach efforts and advance the Girl Scout movement. The registrant’s racial background is: (Please circle as many as apply) American Indian or Alaskan Native Asian Black or African American Hawaiian Pacific Islander White Other The registrant’s ethnic background is: (please circle one) Hispanic or Latina Not Hispanic or Latina HEALTH HISTORY: To be completed for ALL participants. Please use additional sheet to describe symptoms of allergies and details of illnesses or health restrictions. Allergies: Insect Bites/Stings Hay Fever Poison Ivy/Oak Other Please specify any accommodations that are needed: Health Concerns: Ear Infections Asthma Diabetes Convulsions Skin Conditions Other Please specify any accommodations needed: Disabilities: ADD/ADHD Emotional Disability Learning Disability Physical Disability Visual Disability Deaf/Hard of Hearing Behavioral Problems Other Please specify any accommodations needed: Operations or serious injuries: Dates: Immunization History: Are all immunizations up-to-date? Yes No DTP or DT (Tetanus) Date: __________________ If immunizations are not up to date, including the DTP, please submit a state certificate from physician or parent stating medical or religious reason. General Information – Please fill out all information Family Physician: Health Insurance Company: Address: City: Phone: Policy #: State: Zip: PARENT/ GUARDIAN PERMISSION STATEMENT: The information and health history is correct so far as I know, and the person herein described has my permission to participate in all prescribed activities as noted. If she/he appears to be ill, I will not send her/him to the program. I understand my daughter will become a registered member of Girl Scouts of the USA through participation in this program. The council may use photographs in which my child appears to promote Girl Scouting: ___Yes ___No EMERGENCY AUTHORIZATION: I hereby give permission to the medical personnel selected by the camp director or her/ his designee to order x-rays, routine tests and treatment for my child. In the event I cannot be reached in an emergency, I hereby give permission to the physician selected by the camp director or her/his designee to hospitalize, secure proper treatment for, and/or order injection and/or anesthesia and/or surgery for my child as named above. Signature: *Registration is invalid without a parent/guardian signature FINANCIAL ASSISTANCE: Date: Our family can pay $__________, we request $__________ in financial assistance











© Copyright 2026