ABC
docz
Explore
Log in
Create new account
Download
Report
No category
here - Planetree
JOB FAIR - Careerlink Lehigh Valley
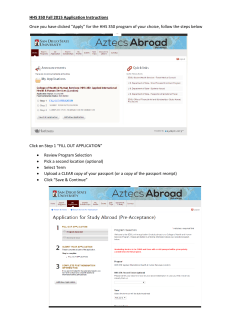
HHS 350 Fall 2015 Application Instructions Once you have clicked
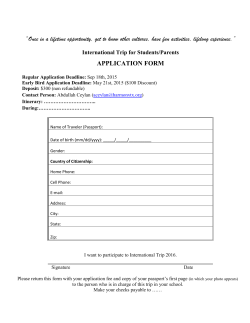
âOnce in a lifetime opportunity, get to know other cultures, have fun
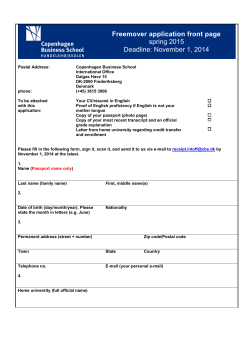
Freemover application front page spring 2015 Deadline: November 1, 2014
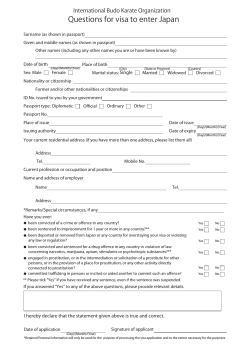
Questions for visa to enter Japan
Cabin crew Ad
How to use the State Department Passport Application Go to the
International Affiliation - jutsu kan karate do federation
Wednesday May 27, 2015 at 7:45 am Contract
Level of Care Utilization Review Process Changing July 1
© Copyright 2026
About abcdocz
DMCA / GDPR
Report