
Document 16174
U\II'I-D
ST.\TI]S DEPART\Itr\T
OF LABOR
FR.'\\CES PERKINS. Srcnrrrnr-
CH ILDREN'S
BUREAU
Katharine F. Lenroot. Chief
Comparabilityof Maternal Mortality Rates
in the United Statesand Certain Foreign
Countries
A Sruoy oF THE Errrcrs or Varrarrows rN
Assrcwunxt Pr.oceruRns, DerrNr::roNs or
LrvB BrnrHS, AND ColrplrrrNrss
or Brnrn
Rncrstne.rrow
BY
ELIZABETH C. TANDy, D. Sc-
Bureau Publication
TINITED
GOVERNMENT
7t{o. 229
STATES
PRINTING
OFFICE
\1ASHI\GTON : 1935
MCH
Collection
Vashington,D. C,
Pricc 5 ceotr
Document Number 212
Provided by the Maternal and Child Health Litrrary, Georgetown University
CO\IPAR.\BILITY
OF
\f..\TER\AL
\IORTALITY
RATE
S
CONTENTS
l , e t t e r o f t r a n s m i t t a l __ - _
- \ r e t n o oo 1 s t u d ) - _ _ - -__ _
Proportion of deaths assignedto puerperal and nonpuerperal
causes by the difierent
countries___-__
Differences in methods of assignment to puerperal and
nonpuerperar causes in the
difrerent countries____
__
\{aternal mortality rates that would have obtained
in the united states under
m e t h o d so f a s s i g n m e n o
t f v a r i o u s f o r e i g nc o u n t r i e s _ - _ _ _ _ _ _ _ _ _ _ _ _
comparison of the united states rate for deaths assigned
to the puerperal state
with those for all deaths associatedwith pregnancy
and childbirth in ,i* r"."ig"
countries---___
Trend of maternal mortality in the United states and
certain foreign countries---Efect of differencesin definitions of live births and in compreteness
of registration_
Summary and conclusions
R e c o m m e n d a t i o n s-- - - - - - - - - - - _ List of references
Pog"
I
5
8
l3
14
t6
19
11
22
(nr)
Provided by the Maternal and Child Health Litrrary, Georgetown University
IORT.{LITY
R.{TE S
LETTER OF TRANSMITTAL
UNnnp SrarBs DcpenrrreNr or
Lanon,
Cnrr,onarv's Bunrau.
December3, 1934.
Maoau: There is transmitted trrrr*i(ot'ington'
of\,{aternal
lro.t"iityRates
in ,r,"u,iii'le,i,'.t?ft*HT:?:1,:l
countries' The st'rdy was initiated
by the subcommittee on cn--o.
abilitv of Maternal Mortarity R"t".
oi the committee on ,r",.;ji'u"::
Nlaternal care of the whitl House
conference on ch'd Hearth and
Protection' Dr. Elizabeth c. Tandy,
Director of the statistical Division
of the children's Bureau, who was'.hui.-rn
of the ,ub.o-r'itt"e, r,vas
in chargeof the study and has written
the report.
The study incruded.anarl.sis
of foreign laws and registration practices
and.the speciaranarysisof a representa-tive
group of United states death
certi{rcateson which pregnancy or
chirdbirth ."vas*"ntio.rJ'by
the
certifying physician. These certificates
had U""n
by
the
Bureau of the cens'rs. At the request
"rr._UtJ
of the subcommitte"-ih.,
*...
transmitted by the Bureau of the census
to officials in charge of vital
statistics in 24 foreign countries,with
the request that they indicate
in
eachinstancewhether under their practice
the ieath *.ur; ;; urirn"o ,o
a puerperal or a nonpuerperal cause.
Replies were received from
16
countries.
The report has the approval of Dr.
F. L. Adair, chairman of the
committee on prenatar and Maternal care,
and that cf the membersof
the subcommittee: Or. y.
J. V. Deacon, Director of the Bureau of
Records and Statistics, Staie Department
of Health, Michigan; Dr.
Haven Emerson, professorof pubiic Health
Administration, co'ege of
Physicians
and
surgeons,
columbiauniversity;r"rrr o. spl;ir,x.;rt"nt
Director,Divisionof Vital Statistics,
st"t. D.pur,.rr.n,oi-uliirr, x"*
York; Dr. T. F. Murphy,ChiefSt"Urtl.i"r,f.,
Vii"f-S,"iiril*,.Uri,.a
states Bureau of the census,.and Dr. Tandy.
valuable suggestionswere
also received from the f.l!.Tilr, who
the report: b?." alUo.r,
"pprorr"d
formerly chief of the cliildrer,', Bu*"u;
Dr. Robert B.-crr"aao.r.,
Professorof Sociology and Statistics,Columbia
University; Dr.
James
R. \{cCord, Professorof Obsterricsand
Gynecology,Emory lniu.rri,y
School
of \fedicine;
Dr. Lowell;. neea,proL*o. oi il;*i",i.ri..,
11f
Schoot
publicHealthjJohns
of Hygieneand
ilopkinsi;;;rt,r.
Respectfully
submitted.
Hon. Fnescrs pnnrrNs
Secretaryof Labor.
ATHARINEF' LnNnoor, chief'
(v)
Provided by the Maternal and Child Health Library, Georgetown University
C1lqurlbility of Maternal Mort ality Ratesin
the
United Statesand CertainForeignCountri..;'
Method of Study
This report deals with the similarities
and differencesin methods of
assigningcauseto deaths certified to
be associatedwith pregnancy and
childbirth in the united.States and 16
foreign countriesand discussesthe
effect of the differenc,
ciarmaternar-.,,"riiili.1::''iffi;Jii,""'ti,!iTffi
*,l,j'JiiI;.f;
of variations in the definition of live
births and in the completenessof
birth registration.
The term "deaths associatedwith pregnancy
or childbirth,, is used to
-pr.grr"n.y
include all deathsin which a-condition
of
or childbirth is stated
on the death certificateby the physician
*ho."gi.tered the death. Such
deaths are of two main tyDes:
(1) Deaths due direcily to the puerperar
state. These incrude alr
deaths in which the condition of p."gn"ncy
or ch'dbirth is the onrv
causementioned on the death certificate,
and deaths ir, *lrl.t a ;;;r;";:
peral diseaseis mentioned jointly with
ihe puerperal, the nonpuerperar
diseasebeing one which probably would
not have proved fatar .*..p, to.
the pregnancyor childbirth.
(2) Deaths due to nonpuerperalcauses
in which the puerperal condition existedconcurrently but in which the nonpuerperal
condition wourd
probably have proved fatal even if the
condition oi pr.gnr".y
.rr'abirth had not been present.
",
It is obvious that the great majority of
deaths associatedwith preg_
nancy and childbirth would everywherebe
classifiedin the n.ri-group.
certain types of deaths, ho*.r..r, such as
abortions induced forI ttullnontherapeuticreasonswhich would be classified
as puerperali; ,;;; ..rrI This report covers
one sectron of an investigation initiated
through a subcommittee oi
the committee on prenatal and Maternal
carJ of the white House conference
on child
Health and Protection, of which Dr. Fred L.
Adair was chairman. This subcommittee
on
comparability and trend of maternal mortality
rates was charged *itr, in*.tig;,i*
,f tlr"
factors underlying the similarities and diferences
in the officlal figures of .h? l^po.."n,
countries of the world and exposition of the general
characteristicsof the rates. The com_
p.lereinvestigation is expected ultimately
to
th" definitions of live births and stillbirths
"lrre.
:hat obtain in the various countries, description
of the procedure of.egistratiof -",rroa,
or
assigning cause of death to deaths certified
as associated *ith p*g,i"o.f
.rrriaui*r,,
description of the trend of the rates, and
interpretation of the findings. "ri
The study was
bcgun during the early months of the white House
conf"..n.", but it was impossibreto com_
:lere an' part oI it in time for incrusion in the
report of the committee on prenatal
an,l
\[aternal Care.
(l)
Provided by the Maternal and Child Health Library, Georgetown University
CO}IPARABILITY
OF
X'IATERNAL
\IORT^\LITY
R.\TES
on account o{ differencesin
tries, would be called nonpuerPeralin others
in procedurervith regard
l.gui p.o."d,-,r". There wtuld also be difierences
causeswere certified
puerperal
and
to deaths in which nonpuerperal
to the causatir-e
regard
with
opinion
jointly, due to variation i" *"dit"l
u'itfr the
concurrent
was
that
condition
i-pora"n." of the nonpuerperal
years have called attenp-..*urr.y or childbirth' Many reports in recent
in procedure,
difierences
from
arising
tion to the lack of comparability
butnonesofarhasattemptedtoevaluatetheefiectofthesedifferences
upon the maternal mortality rates'
upon the effect of diiIn order to obtain dut, ih^t would throw light
of maternal morcomparability
the
on
ferencesin assignmentprocedure
t"lityr*terit*"rpi^rr.redtosendtothebureausofvitalstatisticsinthe
the pertinent information from 1,073 United
principal
'sa"a", foreign countries
2
or childbirth rn"as
death certificates f.ot 1927 on which Plegnancy
as puerperal
death
each
mark
office
each
mentioned, with a request that
of cause'
assignm-ent
of
method
own
to its
o, .otpn"rp"r"l
"..ordi,'g
TheBureauoftheCensushadcodedalldeathslor]-92Tinaccordance
of Causesof Death and
rvith the 1920 revision of the International List
latter being used for
the
Death'
of
the 1925 Manual of Joint Causes
Of the
simultaneousiy'
reported
are
causeswhen two or more
assigning
"g.orrp
as
physician
attending
the
by
of 1'073 deaths certified
."*"pt.
ruies'
States
United
the
under
pu"ip"ru1, the Bureau of the Census,
3
76 (7'l percent)
9g7 (92.g percent) to the puerperal state and
"r.igt"d
to nonpuerperal conditions'
to each cause rubric
The number and percentageof deaths assigned
table 1 lor the 997
in
shown
are
included under the puerperal state
puerperal deaths in
all
for
and
in the sample
fn..p..ut deaths included
' The differences
t927
dttitg
area
the United States birth-registration
the sample and in
in
causes
various
the
in ait" p.r."ntage of deaths from
that they are
demonstrates
test
the toial are unimportant. Statistical
-'fft"r..*incateshadbeenselectedatrandombythelateDr'W'H'Davis'thenChief
for
United States Bureau of the Census, from transcripts
Statistician for Vital S,*i*i.r,
purpose of studying comparability of United
the
for
bureau,
that
at
onlile
l9z7
year
the
a.d Wule.. Through cooperatio' with Dr' T' F'
States methods *i,fr ,f,"." .in.gland
United States Bureau of the Census,certifilirrpfry, Chie{ Statistici", i., ViLf Statistics,
c a t e s r e p r e s e n t i n g e v e r y , r ' t i n t f u a t a i n t h e t o t a l w e r e c h o s e n f r o m t h i s o r i g i n a l g rfore
o u pign
and
The lists were transmitted to the
the pertinent information'."t .p i, list Jorm. .
bureausofvitalstatistics,and.theoriginaltabulationsofthereturnsweremadeinthe
of the Census.
Bureau
childbirth
iirri, percentaSe (g2.g) of the 1,073 deaths^associatedwith pregnancy and
difierent from the.percentage(90'7)
sign-ificantly
i,
arr"lu..p.."l.i"t"
assigned,o
were
that
the l"t"rt ,vear{or which the Bureau o{
so assignedfor the birth-iJg-J.urlo. "rg" l.rigzs,
both primary and contributory cause'
by
the Census has tabulated ieaths for the area
o{ the usual situation in the
representative
not
perhaps
is
however,
percentage'
The 1925
UnitedStates.Forthereisalsoasig'ifi.antdillerencebetweenTg25andT9TTandbetween
1925and|925_29inthedistributionbyca.s"groupsofthedeathswitlrinthepuerperal
(2)
Provided by the Maternal and Child Health Library, Georgetown University
CO]IP.\R.\BILITY
OF
XI\TERNAL
X,IORTAI, ITY
RATES
rvithin the limits of expectationon the basisof chance in the processof
dran'ing the sample from the total group.a Therefore the distribution
by- ."ui" of tne 997 deaths assignedto pregnancy and childbirth which
aie included in this sampleis typical of that o{ all deaths assignedto the
puerperalstate in the united states birth-registration area dvng 1927.
oJ puerperal c/uset amon-gthe deaths included in the sample and
l.-Dlrtribution
Tasla
'""-among oll purrpiroi i"liths in the (Inited siater bith-registration area; 1927
United States birthregistration area 2
Cause of death I
1 , 2 5 9I
1 , 4 5 6|
1
, 5 4 2|
q tqi I
6 1 sI
3 ,5 5 6|
491
------l
9.r
10.5
111
.
38.7
+.+
23.7
0.3
0 .1
1 Accordirg ro the Irtcrnational List o[ Cau'e. of Death. 1920,
2 U. S, Birreru o{ the Census.
Among the 1,073 certificatesincluded in the sample were many that
were identical or very similar. For transmittal to foreign countries'
there{ore, 477 certificateswere carefully selectedso as to include at least
1 death of every type in the sample. For some of these477 deathsoniy
1 causehad been certified,as puerperalsePsisor eclampsiaor self-induced
abortion, but for by far the greater proportion 2 or even 3 causesr'vere
mentionedby the physicianwho made out the certificate'
The in{ormation from the 477 certificates, set up in list form u,'ith each
line representingone death (see sample, p. 4), consisted of the case
,rumb"i, age of mother' primaqr and contributory cause of death, and
performanceor nonperformanceof an operation and of an autopsy' At
the right two blank columns v/ere provided. It was asked that the first
of these columns be checkedif the death would be classedas puerperal
and the secondif it would be classedas nonpuerperalby the statistical
bureau in charge of coding causeof death in each country. No in{ormation was given with regard to the causeassignedin the United States.
These lists urere sent to 24 f.oreigncountries during January 1931, and
were checkedand returned by 16 countriesby the middle of April of the
same year.
r The similarity of the distributions has been determined by the chi-square test deF o r f o r m u l a a n d m e t h o d s e e :T a b l e s f o r S t a t i s v e l o p e db y P e a r s o n :x 2 - 1 0 . 5 1 , P : 0 . 1 1 .
ticians and Biometricians, edited by Karl Pearson, pp. xxxi-xxxiii (Cambridge Universitt'
P r e s s ,L o n d o n , 1 9 1 4 ) .
(3)
10t39Lo_35-Z
Provided by the Maternal and Child Health Library, Georgetown University
RATES
lIORTALITY
\IATERNAL
OF
CO]IP.\R.{BILITY
6 A @ 6
oaao
>">
rttl
tltl
rlrl
rlrl
r;rr
ii
i;
il b: o! ; e
r.{
;tr
t
a
o
>G
q
< 6 r \ N
I
\s
o
9.PGY
o
o
O
o
6
coat
'o
N
M
: !
b
E
Btr
rl@A
t
d
c
6
@
=->s
:isd9
'o
:iid
i;.FF
E b Fg
,Ep:ds
a
=
o
ho
p
(.)
a
IE
s
CA
ru.
|
o
P.E
I
|
I
|
J
O
::
-l
?
'
i'
:9 €
F g
1' e
9 i
';e' t r
3
il
,o
*5E0
Ii
;
i
I sU
i '?,9
a
,o
;
; .e i E*
E ;
'o
li
JU
ot'-,8
o!,=,2
=
ri
l v !
i L
qtt==
o
;N
i
,
.l
d L - d ' Y .
>
+E!.zaE+
:.=<
-ri
.
9
H
a
/
=
^^
:
c
d
c
li
;
;i
x
?
!l;
e d^ >
sa as
:
3 i
.Eho^-2ii=*
o
tr
"^'i
o
;i
-Y
;
2
!
X
t C . ='F
-=
a
!!
E
I
E
1
!
i
u
tr -E
:E]Id<
h
.- s
?
s\OmqO\
N
$
N
ct|h\ONAO\O
Zl-HN
d
&c-o'O
.+t
L...
50
".:
i
'A:
o
=
t
O.
u
d tr
=5
H9
.=
H
y
=
!9 '9 h
xc.
I
h
O
r)
E
d
ia ;
d
'tr
'7>
ad
E@
o.=
o
o
m
a
'Fe
&P
E>\
c,odd\O<>
.+dt+dN$
NS*4h\o
dNNdNN
Provided by the Maternal and Child Health Library, Georgetown University
COIIPARABILITY
OF
MATERNAL
MORTALITY
RATES
Upon the return of the lists the 596 deaths in the original group not
sent abroad but identical with those sent were classedas puerperal or
nonpuerperalin accordancewith the assignmentsmade by the foreign
countries for those that had been transmitted. The groups of deaths
were then thrown together, and a tabulation of the 1,073certificateswas
prepared showing the assignmentof the United States Bureau of the
Census and the classificationas puerperal or nonpuerperal by each
foreign bureau that complied with the request.
Proportion of Deaths Assigned to Puerperal and
Nonpuerperal Causesby the Diferent
Countries
Tabie 2 showsthe number of deathsclassifieCas puerperal and as nonpuerperal by the United States and by each country that furnished
information. No decision was reached by some countries with regard
to the classificationof a few of the deaths,as under their proceduremore
information would have been required before the classification could
be determined.
As has been noted, the United States had assignedto the puerperal
state 997 (92.9 percent) of the 1,073 deaths associated with pregnancy
and childbirth. Denmark, the only country that would have so assigned
more deaths than the United States, ciassified1,054 (99.4 percent) as
puerperal. Norway would have assignedthe fewest,825 (76.9 percent),
and England and Wales came next to Norway with 844 (78.7 percent).
The proportion of deaths assignedto nonpuerperalcausesvaried from
23.1 percent for Norway to six-tenthsof 1 percent for Denmark.
The proportions (in the United States) assignedto puerperal causes
(92.9 percent) and to nonpuerperalcauses(7.1 percent) are not significantly different from those for Australia, the Netherlands, New Zealand,
and Scotland.5 These countries must be considered to have made
assignmentsin approximately the same ratio to puerperal and nonpuerperal causesas the United States. Italy, Canada, Chile, Czechoslovakia,
Northern Ireland, France, Irish Free State, Sweden,Estonia, England
6 The probable errors of the respective percentageshave been computed by the formula
P*'*t)
p.s.: g.67a5
{P=+sI!rcm:
'
l\umoer rn sampre
The probable error of the difference of two percentages,by the formula:
r
P. E. of ain.:-/
A difrerence between percentagesis considered significant whenever it exceeds 3 times
its probable error.
(s)
Provided by the Maternal and Child Health Library, Georgetown University
CO\TP.\RA.BILITY OF I{ATERNAL
ITORTALITY
RATES
and \\-ales, and Norwayr on the other hand, assignedsignificantly more
to nonpuerperaland significantlylessto puerperalcausesthan the United
States.
Of the 4 countries which assignedthe deaths to puerperal and nonpuerperalcausesin approximately the same ratio as the United States,3
(Australia, New Zealand, and the Netherlands) have officially adopted
the United States Manual of Joint Causesof Death, and the fourth,
Scotland, uses this manual, although it has never adopted it officially.
Canadausesthe United StatesManual of Joint Causesto supplementthe
trnglish rules wheneverthe latter do not seemto apply.6 The percentage
of deaths assignedto puerperal causesby the Canadian o{fice (89.6) is
more similar to that of the United States (92.9) thao to that of England
and Wales (78.7).
Testn2.-Assignmen! to puerp.rul and nonpuerperalcausesby tp t!{11( Slatesand rertain
foreisn countriesl o{ 1.073 dcathsassociatidwith pregnancvand childbirth that ortwred in
lhe UnrteditaleJ durtnf lY4/
Puerperal causcs
Total
Count.y
United States----
1,073
997
92.9
A u s t r a l i a 3- -- - - - C a n a d a - - - - - - - - - - -- - - - - - - - - - - - - - l
Chile-------------- - ----- -------i
t,073
1,073
1,073
1,073
1,073
1,073
1,073
r,073
1,073
1,073
1,073
1,073
1,073
t,073
r,073
1,073
995
953
950
899
l, 054
844
857
884
869
971
986
996
899
825
989
8#
92.7
89.6
88.6
8 5 .3
99.+
78.7
79.9
82.7
81.0
90.5
9t.9
92.8
83.9
76.9
92.3
80.5
Czechoslovakia --- -- --::--:
Denmark-----------,,
England and Wales------------------1
D-.^-: - -------l
lrance----------I r i s h F r e e S t a t e -- - - - - - - - - - - - - - -
---- -----:----l
ii"rt ------------3j
- -- --- - --- - - - - - - -- - -- Netherlands
NewZealand3---Northern Ireland--------------------l
-- -- ---------]
Norway--------S c o t l a n d3 - - - - - - - Sweden-----------------------------I
I
I Countries to which lists were scnt but from which no rcturns were received were Belgium' Finland, Hungary'
-J a p a n , L i t h u a n i a , S a l c a d o r , S w i t z e r l a n d , a n d U r u g u a y .
r Based on total dealhs classified.
3 Percentages assigned not significantly
difierent from those of the Unitcd States'
With regard to the assignmentby the Danish ofice of 99.4 percent to
the puerperal group and 0.6 percent to the nonpuerperal,it should be
noted that the deaths were assignedin 1931 and that several changes
have been made in the last few years in the Danish classificationof cause
of death. The statistical reports for Denmark published annually by
the National Health Service (D/dsaarsagernei Kongeriget Danmark)
show that in 1928 and earlier the Danish nomenclature included only
ttFebris puerperalis" and "In aut brevi
two types of puerperal causes:
6Macphail, E. s.: Rules for choice of causes of Death in the Dominion Bureau o{
Statistics. Canadian Public Health Journal, vol. 24, oo. 9 (Sept' 1933)' pp' 413419'
Provided by the Maternal and Child Health Library, Georgetown University
CO},IPA RABILITY
OF
MATERNAL
MORTALITY
RATE
S
postpartllm mort. (Fb. puerp. excl.)." In 1929, however, the inclusion
was broadenedand the number of titles was increased;and the nomenclature used in 1930 and 1931 shows even more detail for the puerperal
state than the latest revision of the international list (1929).
This developmentof the nomenclatureof Denmark is no doubt due,
at least in part, to the interest in comparability that has becomewidespread in recent years. The stimulus was probably brought to a focus
by the Committee on Maternal Mortality and Morbidity of the British
Ministry o{ Health, which has made a specialinvestigation of the comparability of the statistical aspects of Danish and English maternal
mortality.T
Tesrn 3.-Assi.gnment to puerperal.and no.np.uuperal causcs; deaths associatedwith pr€Knancy
and childbirth that occuned in thc United Statet and in six Joreign countricst Znd-dtatis
included in the United States samplcz classif.cd according to the mcthods of thesecountries
Percentage of dcaths associated with pregnancy and
childbirth-
Country
Occurring in thc rcspectivc
countries I assigned to-
Puerperal
causes
Includcd in the United
Statcs samplc assigncd top,,--^--^l
. causea
I
Nonpuerperal
cauSes
92.9
7.1
89.6
78.7
81.0
92.8
839
.
92.3
10.4
21.3
1 90
.
7.2
16.I
7.7
r Figures Jor the United States are for 1925, the latcst ycar for which the Burcau of the Ccnsus has tabulated
deaths.byborh primary ar-d.contribut-ory causc: those for foreign countries arc for the following periods: Cenada,
E-n-gland and Wales and New Zealand, L925-3O; Irish Free Statc and Nonhern-Iieland,
fQlJ-Jf;
1925-J2;
Scodand,1931-32.
z 1,073 dcaths that occurred in the United Statcs during 1927.
In connectionwith the classificationof the 1,073deaths in the sample,
it is of interest to examinethe percentagesof their own deathsassociated
with pregnancy and childbirth which the countries assign to puerperal
causes. Table 3 presentsthis information for the six foreign countries
that publish the basic material and for the United States, and also the
percentagesof the United States sample assignedto puerperaicausesby
these countries. The Irish Free State assignedto puerperal causesa
Iarger proportion of its own maternal deathsthan of the sample; Canada
and Scotland assigneda smaller proportion; and New Zealand, England
and Wales, and Northern Ireland assigned approximately the same
proportions of their own deaths and of the sample. This suggeststhat
the various types of nonpuerperal causesmay be certified in approxi7 Final report of Departmental Committee on Maternal N{ortality and Morbidity.
Britain Ministry of Health. London, 1932.
Great
(7)
Provided by the Maternal and Child Health Library, Georgetown University
CO\IPARA,BILITY
OF }TATERNAL
MORTALITY
RATES
mately the sameproportion as that of the united states, in the countries
n'hich assignto the puerperal state apProximately the same percentage
of their own deathsand of the sampleand that thesetypes may be certified
in
in a somewhat difierent proportion from that of the united States
of
countries which assign to the puerperal state difierent percentages
percentage
their own deaths and of the sample. The differencesin the
of the sample and of their own deaths assignedin the various countries
to nonpuerperalcausesindicate either difierences.infrequency of occurcomrence of the causative diseasesand conditions or differencesin the
pleteness with which physicians certifying cause of death describe the
morbid conditions.
Diferences in Methodsof Asignment to.Puerperal
and Nonbuerqeral Causesin the
Diferint Countries
Thenumberofdeathcertificates(+77)inthegroupsentabroadwas
procedtoo small to warrant final conclusionsregarding the assignment
Horvever'
received.
were
ures of the countries from which returns
that
study of these certificates in connection with the correspondence
of
available
examination
with
and
accompanied them upon their return
mater.n"nuui. for assigningcauseof death, and study of tables showing
published
are
that
cause
nal deaths by blth primary and contributory
real differby a few countries in their annual reports, demonstrate that
mortaiity,
high
in
resulting
diseases
.rr.., io procedureexist. Infectious
given
precedence
invariably
such as pn"rr*oni" and influenza,are almost
given precedence
by ..rt"in countries,whereasin other countriesthey are
was no evithere
when
or
only *h"., the onset followed normal delivery
would
pregnancy
that
or
dence that an abortion would have occurred
haveterminatedotherthannormally,exceptfortheintercurrentdisease.
by some countries
Heart conditions are given frecedence more frequently
to the pregnancy
prior
existing
than by others. Pulmonary tuberculosis
favor the
countries
but
some
*1. g*.."tty considered a primary cause,
countries
most
by
considered
prrerf,"ral condition. Acute nephritis is
but by
convulsions
and
*"r.ly another name for puerperal albuminuria
of
tissue
functional
the
of
some as a distinct diseasein which destruction
in
country'
One
death'
the
for
the kidney is primarily responsible
puerto
be
specif,ed
when
even
contrast to all others, assignsembolism,
AII countries include the majority of
peral, to the nonpuerp"r"i.l"tt'
by " self or party unifr. i""th. from aborlion, but abortions induced
small country, which
one
and
known,, are excludedby severalcountries;
of death'
adopted the international classification of causes
,...ntly
class'
places abortions due to accidentsin the nonpuerperal
previously stated
The United States Manual of Joint Causesof Death'
Scotland' and
Zealand'
New
to be used by the lJnited States,Australia,
(8)
Provided by the Maternal and Child Health Library, Georgetown University
COI,IPARABILITY
OF
MATERNAL
MORTALITY
R.ATES
the Netherlands,and also by canada wheneverthe Engrish rules
do not
seemto apply, (p. 6), designatesin great detail the causeto which
the
death should be assignedwhen two or more causesare certified jointry.
In England and wales 8 and in Italy e much effort is directedtoward
facilitating an expressionof opinion by the certifying practitioner as to
which
of two or more causesis the primary causeof death. Generar
rures for
precedence
are in usein the statisticalofices, but it is considereddesirable
that the selectionof the primary causeshould be determinedin the
main
by the opinion of the certifier rather than by rigid rules. In sweden,
at
the other extreme from the united states, the doctor,s certification
as
to the main causeis usually taken as correct.ro
The differencesin methodsof assignmentjust discussedusually resulted
in charging to the nonpuerperalclasscertificatesclassifiedin the
United
states as puerperal. certain combinations of joint causesassigned
in
this country to the nonpuerperalgroup, however,werefrequently
assigned
by other countriesto the puerperalstate.
Maternal Mortality Rates That wourd Haae obtained in the
United Statesunder Methods of Assignment
of Various Foreign CountriesTable 4 shows the total number of deaths in the sampre that were
assignedto the puerperal state and the number assignedto sepsis
and
other puerperalcausesin the united states, the number th"t *ould
h"rr.
been so assignedby each foreign country under its assignmentprocedure,
and the percentagechangethat would have obtained in the united
States
under the assignmentprocedureof each of the foreign countries.
In this
connectionit should be called to mind that the foreign ofices were
not
askedto specifythe type of puerperalcauseto which the death rvould
be
assigned. Sepsis,however, generally has preferenceover other types
of
puerperalcauses,and the deathsthat were consideredpuerperalgenerally
would have been assignedto the sepsisrubric ,"hen"v"r that causeu,as
mentionedand to other puerperalcauseswhen there was no mention
of a
septiccondition.
since the puerperal-causedistribution of the deaths included in the
samplewas typical of that of all deaths of the year 1927 assignedby
the
E Manual of the International List
of causes of Death, as adapted for use in ungland
and wales, scotland, and Northern Ireland, pp. vi-viii. Registrar General, London,
r931.
e Nomenclature Nosologiche per la
Statistica delle Cause di NIorte e Dizionario delle
Malattie, p. 58. Istituto cenrrale di statistica del Regno d'Italia. Rome, 1933.
l0Hultquist, Gustaf : Nigra Anmirkningar
till vir Nya Dcidsorsaksstatistik. Allminna
_
s v e n s k a L l k a r t i d n i n g e n , l l t h y e a r , n o . 5 l ( D e c . 1 8 ,l g l a ) , p . l l z 9 . s e e a l s o F i n a l
Reportof
Departmental committee on Maternal Mortarity and Morbidity, p. 95 (Great
Britain
Ministry of Health, London, 1932).
(e)
Provided by the Maternal and Child Health Library, Georgetown University
CO\IP.\R.,\BILITY
OF
}TATERNAL
XIORTALIl'Y
RATtrS
Bureau of the Censusto the puerperalstate,the proportionsof the sample
classedas "puerperal" under the methods of assignmentof the different
countries indicate the variations that wouid have occurred had all the
deathsof that year associatedwith pregnancyand chitrdbirthbeen transmitted for assignment. On the basisof the percentagechangesshown in
table 4 therefore it is legitimate to estimate the total deaths in the
United Statesin 1927 that would have been assignedto puerperalcauses
by eachforeign country and to compute the maternal mortality rates that
would have obtained in this country under the assignmentprocedureof
the various foreign offices.
Te,3Ln 4.-Perccntage change that would hau obtained in the mortality. d.ueto putrperal causcs
in the tlnitci Stales-tnder the assignment procedure oJ the diferent countries
t _l h.e
I
t'-
DuerDeral
stalc
l-r-
I Number ofl Percentof Number of
deaths
deaths I charge
I
--
U n i t e dS t a t e s - - - -
]
997
392
995
953
950
899
l,054
844
857
88,1
869
971
986
996
899
825
98
86.1
388
L
Australia---------- -----------------l
---------l
Canada-----------------Chile-------------- - -----L
Czechoslovakia-------Denmark-----
Ii,igi".Jl.i-rv"r"r----------,-----'
l'lstonia-----------,
- --
--
----:--]
L.- - ^-
i , i l i ' i ' i .3. i " , " - - - - - - - - - - - - - - - - - -
Itall'---- - - - - - ------ - -. - -- -- - --- --- -l
Netherlands- - -,New Zealand----Northera lreland---------------
__---:-N;;"t- ____
__-____-__-____
Scotland--------. LI
Sweden-----------
382
370
393
338
311
367
328
386
389
387
374
364
390
3&
Percent of
^L"---
"
;- ;5;. 0
-o_
I
-12.6
+9.3
-16.
4
-9. I
-1+.5
-10.6
-3.3
-t.3
+-0.7
-13.2
-23.8
-1.0
-17.+
Because of the variation that occurs in the different countrles in
certification of cause as weli as the possible differencesin the relative
frequency of the occurrenceof the various diseasesin eonnectionwith
deathsassignedto pregnancyand childbirth, the effectsof the similarities
and difierencesin assignmentprocedureare measurableonly in terms of
what the United Statesrate would have beenhad its deathsbeen classified
in the foreign bureausof vital statistics. The rates thus obtained for the
United Statesmay, of course,be comparedrvith the ratesof the countries
themselves.
Table 5 showsthe actuai ratesof the United Statesfrom deathsassigned
to the puerperal state and from puerperal sepsisand other puerperal
causes,and estimatedrates for the United Statesbasedon the assignment
methodsof eachof the foreignofilces. In juxtaposition to theseestimated
rates for the United States the actual rates of the foreign countries are
sholvr,. For each country except France the official rate is computed
cn the basis of total live births. The French rate is basedon the total
(10)
Provided by the Maternal and Child Health Library, Georgetown University
CO\IP.\RABILITY
OF
IIATERNAL
I,fORTALITY
RAT
I - ]S
births of infants reported as living at the time of registration,but is not
significantly different from the rate that would result from using total
live births.1l The differencesbetweenthe estimatedrates for the United
Statesbased on the foreign methods of assignmentand the rates of the
foreign countriesthemselvesmust be consideredas representativeof real
differencesin mortality arising from variation in such factors as social
and economic conditions, racial and physiologicaltypes, general public
health, community provision for maternal welfare,and obstetric practice.
'ltsre
S.-Maternal mortality rates that would haae obtained in thc Unitcd States under thc
methorls of asstgnment of certain foreign counbict and thc oficial rates oJ these countries;
1927
Dcaths
assigoed to the pucrpcral
Puerperal
Cruntry
I
I
i
i
I
I
Kate ot
I
United Statesi
lunder methodi Olficial
lof assignmenti rate of
j of.spccificd country
Iorergtr.
I
r l
I couotry
state per 10.000 livc births
scpticcmia
All other puerperal
causes
Ratc of
States
,method
I asslgnmcnt
of spccificd
forcign
country I
64.7
39.7
59.2
55.5
57.7
35.8
r40.5
4 1 .I
4 1 .I
528.7
45.1
26.4
29.0
49.1
48. 0
24.5
64.3
27.8
37.7
36.4
38.1
1 6 .0
127.9
1 Estimate based on sample of 1,073 deaths that occurred in the Unitcd
! Figures fron olicial sources.
3 Not significantly difierent from the United Statcs omcial rate,
I Rate for 1931.
6 Based on total births rcported as livc,
2 5+
.
32.5
| 17.3
32.3
1 7+
.
20.0
2+.O
30.0
t+.3
+5.3
15.1
States in 1927.
The lowest maternal mortality rate for the United States would have
occurred if the practice in assignmentof causeof death of Norway had
1 1U n d e r t h e l a w o f F r a n c e a l l b i r t h s m u s t b e r e g i s t e r e dw i t h i n 3 d a y s ,
and'it must be
specifiedwhether the child was alive at date of registration (pr6:entl vitant) or dead at that
time (mort-ni). It is not obligatory to specify whether the mort-n6s were born alive or
born dead, but spacefor this information is provided on the certificate, and the information
is generally given for statistical use. Every year there are from 3,000 to 4,000 mort-n6s
for which there is no report as to condition of life at birth. In the rates shown in tables 5
and 7 these births are not included. I{ all of them were considered born alive-thev
unquestionably include many still-born fetuses-the total live births would be increased
from 0.4 to 0.5 percent annually, and the maternal mortality rates would be decreasedat
most 0.2 per 10,000.
(I I )
ts-Provided by the Maternal and Child Health Library, Georgetown University
CO\TPARABILITY
OF }TATERNAL
I,TORTALITY RATES
beenused (53.5per 10,000livebirths). If England and Wales had made
the assignments,the rate would have been 54'8. These minimums are to
be contrastedwith the maximum rate (68.4) which would have obtained
under the procedureof Denmark, and with the oficial rate of the United
Statesitself (6+.7). The rates that would have obtained for the United
States from assignment by countries in which the percentage of deaths
associatedwith pregnancyand childbirth that were assignedto the puerperal state was approximately the same12as that of the United States
were: Austr alia, 64.6;New Zealand, 64.6; Scotlar^d,64.2; and the Netherlands, 64.0.
The rates {or the United States if the assignmentsof cause had been
made in accordance with the ofRcial practice in the respective foreign
ofices were, with but one exception (Scotland), in excessof the oficial
flgures of the respective countries. Under the procedure of Scotland the
United States rate would have beer. 64.2 and the Scottish rate was 64.3.
After adjustment of assignment procEduresthe United States rates exceeded the ofrcial rates of five countries (Norway, Sweden, France,
Italy, and the Netherlands) by at least 100 percent.
In discussionsof official maternal mortality rates the United States is
often referred to as heading the list; that is, having the highest rate. The
United States rate under the assignmentproceduresof Australia, New
Zealand, and Denmark would maintain this position with respect to the
official rates of those countries. The best position that the United States
could have achieved would be fifth from the highest, when its rate is
determined under the system of Norway and of England and Wales.
(Countries with .higher rates would be Scotland, Australia, Chile, and
Canada.) Under every system of assignmentthe United States has a
very high maternal mortality rate in comparisonwith other countries.
The oficial United States rate from puerperal sepsiswas 25'0 per 10,000
live births, a figure in excessof that of every country except New Zealand
(25.1). The United states rates from sepsisestimated on the basis of
the foreign procedures varied from a minimum of 19.8 per 10,000 live
births, which would have obtained if the assignmentshad been made by
Estonia, and 20.9under the procedureof the Irish Free State, to a maximum of 25.1 under the Danish procedure. The offlcial rates o{ these
countriesfor deathsfrom sepsiswere 8.6 (Estonia), 12.8 (Irish Free State),
and 12.6' (Denmark). The rates are for the same year as the sample,
1927, exceptthat of Denmark, which is for 1931, a year when classification
was more nearly similar to that of the United States (seep. 7). The
estimates for the United States when the foreign method of classification
was used were, in every instance excePt New Zealand, higher than the
oficial rates of the countries themselves. The adjusted United States.
r?As tesied by tl;e method described for significanceof differences. Seep' 5, footnote 5
(r2)
Provided by the Maternal and Child Health Library, Georgetown University
COMPARABILITY
OF
IVIATERNAL
}IORT,\LITY
R.{TES
rates were more than double the rates of Estonia, France, Italy, the
Netherlands, and Norway. Under the proceduresof Estonia and the
Irish Free state the United states would have stood third from the highest
in its maternal mortality rate from sepsis,New Zealand and Australia
being higher. Under the assignmentprocedureof every other countr\the United Stateswould have had the highestor next to the highestsepsis
rate with respectto the oficial rates of the countriesthemselves.
The estimated rates for the United States from all other oueroeral
causesvaried from 30.3 basedon the procedureof Norway to 43.4 basecl
on the procedureof Denmark, the oftcial rate for the United Statesbeing
39.7. In contrast to theserates, the oficial rates of the foreign countries
varied from 14.3 for Norway to 38.1 for Chile and 45.3 for Scotland,the
last two being the only countrieswhoseown figuresexceedthe comparable
rates estimated for the United States. Five foreign countries had rates
lessthan 20, nine had rateslessthan 30 per 10,0@live births. The official
United Statesrate is next to the highest. If the deathshad been assigned
by the procedureof Norway, which affords the minimum estimate, the
United States rvould have been seventh in the list as comDaredwith the
oftcial rates of the foreisn countries.
Comparison of the United StatesRate for Deaths ,4ssigned
to the Puerperal Statewith Thosefor All Deaths
Associatedutith Pregnancy and Childbirth
in Six Foreign Countries
Further evidencethat the height of the maternal mortality rates in the
United States is not due solely to the method of assignmentof cause
appears in table 6, which gives for the years l92S-32 the mortality
rates from all deaths associatedwith pregnancy and childbirth in six
foreign countriesthat publish the basic facts, and the United Statesrates
for deaths assignedto puerperal causes. The United States figures of
course exciude deaths in which pregnancy or childbirth was mentioned
on the death certificate together with a nonpuerperalcause considered
primary under the rules,whereasthe ratesfor the foreign countriesinclude
ail deaths in which pregnancyor childbirth was mentioned on the death
certificate. In each year the United States rate for deaths assignedto
the puerperal state either exceededor was approximately the same as
those of the other countriesfor all deaths in connectionwith which the
puerperalstate was mentioned,exceptCanadain 1925 an.d1926and Scotland in I93l and 1932.
(l 3 )
Provided by the Maternal and Child Health Library, Georgetown University
CO}IPARABILITY
OF
MATERNAL
RATES
MORTALITY
Taglg6.-jllorralityratest'rorndeathsassigned.tothepuerpefalstateintheUniudStaxsand
fromallt]tathsassociated'with?r,gnoncyandchitdbirthinsixforeigncountrics,l92S_32
I Deaths associated with
pregnaocv and childbirth
Coutrtry
!927
65.6
64.7
67.5
51.4
53.8
45.0
(4. +
54.3
48.5
5 1 6.
OL. L
Lgro I tnrt
1928
1e3z
ltl
69.5
I
66. 0
56.2
6 8 .9 I
5 8 . 2|
48. 6 I
50.7
6 5 .1
62.6 I
5J.
I
1
lliff;::1::t:t'*l;'tl:',';
no!puerpe!alcauses.
per 10'@0 live births t
r.r
l
6 6 . 1 16 3 . 3
6
6.3
( (
5 7 . 9l - - - - - - - -
! d .i
4 i : 6 - i - - - - 48c
Q
5 3 . 7\ - _ - - - - - - l - - - - - - - 63.7
6 0 . 7I 6 5 . s I
1
72.t177.7
that were aesignedto
erclude deaths associatedwith pregnancv and childbirth
Trend'ofMaternalMortalityinthe(JnitedStatesand
Certain F oreign Countries
and t9 puerperal
The trend of mortality assignedto the puerperalstate
figures' is
official
by
sepsisand all other prl..p"t"1 causesas indicated
area,
birth-registration
,ho*., in table 7 for the united states expanding
years
the
for
country
foreign
for the years 1925 to 1933 and for each
rn'ithint.hisperiodforwhichtheinformationisavailable.Itisevident
from this tJle that the rates for the yeat 1927 are' for most countries'
fairlytypicaloftheperiod.IntheUnitedStatesexpandingbirth.regisfrom deaths assigned
tration area and in most foreign countriesthe rates
by fluctuation'
mainly
to the puerperai state have been characterized
significantly
been
have
there
In Chiie, Czechoslovakia,and Denmark,
The
consideration'
under
t'rirtt". rates in the later years of the period
morthe
where
is
Canada
oniy country showing a significant decrease
previous years'
tulity hu, been markedly lower since 1931 than in
Inmostofthe{oreigncountriesbirthsanddeathswbreregisteredeach
ur"u, comprisedwithin the political boundaries'
y"r. ir-, practicaily
"lf
TheUnitedStatesbirth.registrationarea,insharpcontrast'includeda
from 33 Statesin 1925
constantly increasingnumber of States,expanding
the
United Stateswould
of
area
to 48 in 1933' The rates for a constant
bemuchmorecomparablewiththefiguresforforeigncountriesthan
Table 8 shows the
those for the expanding areaof the United States'
sepsisand
puerperal
from
and
mortality rates from tlie puerperal state
the
during
area
all other puerperal causesin the 1925 birth-registration
of
the
area
this
countries'
Unlike most foreign
y"^r, wiS;9T.
lower
considerably
were
that
United states had rates from these causes
in|g32thaninlg25.Duringtheperiodunderreviewfluctuationisof
(14)
Provided by the Maternal and Child Health Library, Georgetown University
CONIPARABILITY
'[a,etE
7.-Trcnd
OF
MATERNAL
RATES
MORTALITY
of maternal mortality in thc United States and certain foreign countrit::
1925-33
Deaths assigncd to pregnancy and childbirth
births !
per 10,000 live
Country
:l:
925
TEE
United
PUERPEM'-
STATE
& . 7 o). o
56.4 5 3 .0
Stateg 2----
5 6 .4
6 1 .1
33.3
23.6
40. 8
38.2
23.8
46.9
28. I
26.3
46.5
44.4
26.8
6t.6
26.3
PVE&PERAL
United
Statce
56.6
5 8 .3
34. 0
26.6
41.2
40.5
24.4
48.9
2 5 .5
28.7
+2. 5
56. 1
31.8
64. 0
29.+
s9.2 59.
50.8
JJ. )
56. 5 7 . 0
5 8 . 7 7. 8
JJ. d
39. + 2 . 8
31.7
30.6 27.
4 3 .+
4 1 .I
50. 46.0
4 1 .I
29.3
2 8 . 7 29.
45. 1 49.3 i 4 1 . 0
2 8 .8
26.+ 28.
.
29.0 3 3 . 3 35
48.2
+9.
49. I
49.2
4 8 .0 5 2 .
36.2
2+.5 30.
68.7
6 4 . 3 69.
. i 37.9
2 7 . 8 3 30
l
SEPTICEMIA
r----
t7.+
Denmark -- - England and Wales-,----------
Italy-----------Netherlands-----New Zealand----Northern Ireland
NT^-.-,-,,
. 0 26.4
2 + . 3, 2 4 . 2 2 5 . 0
16.8
15.0
14.3
9. 1
15.6
3.9
9.3
t6.9
t0.2
8.6
1+.9
9.8
7.8
16.4
t2.2
t6.4
18.6
15.7
i3. I
10.9
16.0
4.0
9.7
18.8
8.4
9.3
13.7
17.4
10.0
16.9
16.0
21.5
1 9 .1
19.6
t9.7
10.5
t5.7
8.6
11.4
12.8
9. I
8.9
2 5 .I
180
.
10.2
1 90
.
12.7
20.5 l
1 8 .5
20.
2+.
u.
17.
10.
II.
17.
9.
9.
20.
15.
16.
24.
17.
1 7 .I
19.6
33.6
23.6
10.0
180
.
7.3
11.6
13.7
9.2
13.3
1 8 .3
14.6
1 90
.
23.8
20.6
1933
61.9
53.0
57.7
67.7
40.7
38.3
44.0
49.3
26.7
47.6
27.2
33.3
50.8
52.9
30.3
69.5
34.8
55.7
50.2
7 t . 0 -t4s.
42.8
3 5 . 0 36.
+ 2 . 1 3 43.
+2.5 33.9
54.8
50.5
7 5 .0
41.+
40.5
41.1
24.9
i;-;'
43.1 +i. )
2 7 . 8 29.I
3 2 . 0 30.2
2 4 . 61 2 3 . 0|
I
I
1 8 . 8 2 r . rI 2r.91
20.6 r 8 . 0 1 7 . 3|
i 32' '8 . 5 |
2 8 .1 - ) 1 . 0
2 s . 2|
22.6
1 1 . 8 t 2 . 6 1 0 . 7|
t 9 . 2 1 6 . 6I 1 6 . 1 I
2 3 .I 1 3 . 3| 1 0 . 1 I
9 . 8 8 . 71 -, , , _ t
1 3 . 9 r 1 . 6l 1 3 . 9|
8 . 8 10.6 1 1 1 |
1 1 . 4 10.2 q t I
2 1 . 3 1 7 . 7| T J , I
1 5 . 1 1 6 . 7| 1 5 . 5
1 4 . 0 1 1 1. | 1 0 - 1 l
2 3+
. 2 2 . 6l 2 6 . 7
186
. 1 8 . 231 0 .1
I
I
ALL OTEER PUERPERAL CAUSES
Unired Statcst---
44.4
41.+
Au6tralia--------Canada----------
39.0
39.6
46. I
19.0
1 4 .5
25.2
3+.Z
14.5
30.0
17.8
1 7 .8
3t.6
34.7
1 9 .I
45.2
14. I
36.6
380
.
42.6
21.0
15.7
25.2
r
I
I
.
I
II
39.7 +4.2 4 3 . 2 4 3 . 3 4 1 . s1 4 0 _ 3|
37.7
36.+
3 8 .1
16.0
20.1
2 5 .+
JO. )
32.5
t+.7 t7.3
30.I
1 7 .I
1 9 .4
28. 8
38.7
21.8
47.1
13.4
i41.6
40.6 44.4
53.4
26.4 'si.1
63.3
26.6
5 1 .4
27.0
59. 1
36. 8
17.4
20.0
24.O
30.0
t+.3
+5.3
1 5 .I
39.3
37.7
380
.
15.4
15.3
26.3
39.9
18.0
3t.9
18.6
2+.I
28.7
37.4
14.0
44.2
19.2
2t.7
25.3
38.7
17.7
2 7. 3
t9.6
20.3
29.9
3+.6
t7.2
44.9
15.1 t7.3
34.1
3 7 .I
39.6
18.2
26.5
2+.8
26.2
16.9
33.8
18.4
22.0
29.5
37.9
16.3
+6.I
16.2
l
33.8 33.8
3 2 . 5i 3 2 . 9
4 2 .5
20.4 ?1 7. 6
27.9
2 4 . 5' l 26. t-)
2 9 . 2 2 1 .8
1 6 . 7 ;;-;3 15
. )t. /
t 7. 3 1 80.
218
. 21.1
30.1 2 + . 9
.
3 + . 7' 3 7 S
1 5 . 9 1 6 .i
3 6 .5 : { , 6
l E . 6 31 6 .5
Fieures from oficial sources.
Th"e Uoited States birth-registration area expandcd from 33 States iq 1925 to 48 Staces in l9iJ.
Provieional.
Bascd on total births rcported o livq
(1s)
Provided by the Maternal and Child Health Library, Georgetown University
CO]TP..\R^\BILITY
OF
IUORTALITY
\{ATERNAL
RATES
courseapparent but on the whole an averagedecreaseof about I percent
per annum 13is shown in the rates from all deaths assignedto pregnancy
and childbirth, in the rates from puerperal sepsis,and in the rates from
all other puerperalcauses.
TaeLn8.-Trcnd
oJ maternal mortality in tfu Unitcd Statcs birth-rcgistration arca oJ 1925;
1925-33
Cause o{ death
or(
r93l 1932| 1933
6 2 . 2 5 9 . 4 5 8 .5
,n
+3 2+.I t t t I t z z 2 + . 6 2 2 . 3 2 3 . 8 ,n
4 0 . 4i + 1 . 3 3 8 . 4I 4 0 . 4 3 9 . 6 3 9 . 7 3 8 . 4 3 7 . 31 3 6 . 3
64.7
I
t Compiledfrom figuressuppliedby thc U' S. Bureau of the Ccnsus.
Efect of Diferences in Def.nitions of Liae Births and
oJ Registration
in Completeness
In addition to differencesin assignmentprocedure,two other matters
are frequently discussedin connection with the comparability of the
United States and foreign figures: (1) Differencesin definitions of live
births and (2) variations in completenessof registration. These are factors of considerableimportance,sincethe total live births registeredconstitute the divisor in the computation of maternal mortality rates.
The registration of live births is legally compulsory in every country
i n c l u d e d i n t h e p r e s e n tr e p o r t e x c e p t F r a n c e ( s e ep . 1 1 , f o o t n o t e 1 1 ) ,
where it is only obligatory to report the condition of life at time of registration; but the distinctionbetweenlive-born and still-bornfetusesusually
is made on the basis of rules and regulationsof the statistical bureau.
Two types of definition of stillbirths, and conversely of live births, exist.
The Health Committee of the League of Nations has recommendedthe
international adoption of "breathing" as the evidenceof life to be used
in distinguishing between live births and stillbirths, and this is the
definition most frequently used. 1a Most of the statistical offices of the
13The average annual rate of change in the rates has been computed by the ordinary
{ormula for geometric progression
log Y: a1 6*
in which y is the death rate and x is the time.
la See Report o{ the Committee Studying the Definition of Dead-Birth, in Minutes oI
Foulth Session,League oI Nations Health Committee, pp. 7G80 (Geneva,1925),
(16)
Provided by the Maternal and Child Health Library, Georgetown University
CO\TPARABILITY
oF
MATERNAL
MoRTALITY
RA-fES
united states and canada, however,in accordwith the rule of the American Public Health Associationadopted in 1908 and further developedin
1913, differentiateon the basis of "any evidenceof life after complete
separation of the child from the body of the mother, evidence of 1ife
including action of heart, breathing, movement of voluntary muscle."15
The differentiation in England and wales under the Births and Deaths
RegistrationAct of 1926 is similar to that of the United States. Information as to the determining factor is not available for all the foreign
countries, but in at least chile, czechoslovakia, Denmark, Estonia,
Norway, Sweden,and some of the States of Australia, the definition of
stillbirth is in the generalterms ',born without signsof life.', 16
It is of legal and administrative importance to have a clear line of
demarcation, and highly desirablefrom the statistical point of view to
have uniformity, not only from State to state but from country to
country. The League of Nations commission of Expert statisticians
has acknowledged,however,that the practiceof the ljnited states and of
England, although not identical with the commission'srecommendation,
gives comparableresults.17 The committeeon the definition of stillbirth
of the American Public Health Associationshowedby a specialstudy of
l,74lrive births in the Boston Lying-in Hospital inigza th"t the use of
action of the heart, breathing, movement of voluntary muscle, as com_
pared with breathing alone, as a test of life would increasethe number
of live births only about four-tenths of 1 percent. 18 Many of the infants
who fail to breathe but have heart action or movement of voluntary
muscle are already registeredas live born in this country, so that the
increasein live births would not amount to four-tenths oi 1 percent for
the United states as a whole. Acceptance by all the states of the
American Public Health Association rule and the establishment of
uniformity in practice would not lower the maternal mortality rate of
15Replies from State officials
to a letter asking information regarding the distinction
between live births and stillbirths show general accord with the American public
Hea6h
A s s o c i a t i o nr u l e i n 3 6 S t a t e sa n d t h e D i s t r i c t o f c o l u m b i a . I n 2 o f t h e s e S t a t e s
the defini_
tion is incorporared in the law, in at least 11 it is printed on the birth certificate,
and in 9
others incorporated in the rules of the department or included in the instructions
to
phvsicians. Breathing was reported to be the test of life in only 5
states. Replies from 5
of the remaining 7 States for which no information was obtained as to the evijence
of life
i n u s e s t a t e d t h a t n o i n s t r u c t i o n sh a d b e e n i s s u e d .
16Period of uterogestation enters
into the registration of stillbirths but not that of live
births. All births of any period are required to be registered if the prescribed signs
of life
are evidenced by the fetus.
17See Report of the Second
Sessionof the Commission of Expert Statisticians, in \,{inutes
of Fourteenth session, League of Nations Health committee, pp. 97-103 (Geneva,
l9z9).
18Definition of Stillbirth (report
of the American Public Health Association committee
t o c o n s i d e rt h e p r o p e r d e f i n i t i o n o f s t i l l b i r t h ) . A m e r i c a n
Journal of public Healrh, vol. lE,
no. 1 (January 1928), pp. 25*32.
(Lt1
Provided by the Maternal and Child Health Library, Georgetown University
C O . . . 1P , \ R A B I L I T Y
OF
ITATERNAL
\IORTALITY
R''\TES
this country. The question is evidently not \,vorthseriousconsideiation
in connectionwith comparability.
rn
completenessof registration is of greater statistical importance
lir-e.orrrr".tio., with comparability than the iine of demarcation between
has been
born and stillborn infants. Sincethe registrationof live births
and in all,
compulsoryin most Europeancountriesfor severalgenerations,
regime,
,r.l,rii.rg Estonia, wher. it was establishedunder the Russian
be expected
well before the beginning of the twentieth century' it is to
countries
these
in
registered
be
would
the
births
of
proportion
that a larger
estabnot
was
area
birth-registration
the
where
States,
than in the Cnited
the
of
lished until 1915. The standard of the united States Bureau
perleast 90
census for inclusion in the birth-registration area is that at
in Nelv
particuiarly
States,
some
In
registered.
be
cent of the births
just as in Europe' but in
England, practically all births are registered,
oficial figures
*olt St"t", registration is at least partly defective' No
in this country, but it is certainly
have beenissuedregardingcompleteness
90 and the ideal
in excessof the minimu- .trnd..d-5emsiMh61e between
100 percent.le
Theefiectofincompletenessofbirthregistrationuponthecomparabil.
that
ity of maternal mortality rates may be gaged by postulating first
a
estimating
and
in
1927
complete
percent
95
only
birth registrationwas
and
second,
to
100,
raised
were
completeness
if
rate that would obtain
similar
by postulating 90 percent completenessin L927 and making a
births.
per
live
10,000
64.7
was
1927
for
rate
estimate. The oftcial
rate
the
lowers
completeness
percent
of
95
Adjustment on the hypothesis
it
lorvers
completeness
percent
of
90
basis
the
ao 61.5, and adjustment on
on
the
adjustment
and
figure
the
official
to 58.3. The difierencebetween
the basisof 90 percent completeness(6.4 points) rePresentsthe maximum
of birth
oossibleexcessin the oficial rate arising from incompleteness
show
estimates
Both
less.
probably
is
excess
registration. The actual
a
few
than
more
to
explain
inadequate
is
that defectivebirth registration
United
the
postulate
either
Under
rate.
ooints of the maternal mortality
The
ba"a"* would retain a position near the top of the list of countries.
is
country
this
in
existing
registration
degreeof incompletenessof birth
the
comwith
in
connection
importance
evidently not a matter of great
parability o{ maternal mortality rates'
tr *"
in the 1927 area was probably about 94 percent complete in 1930'
*-tration
of Birth Registration in
This is estimated on the basis of figures given in The completeness
Statistical AssociaAmerican
the
of
the
in
Whelpton,
P.
K'
b1'
Journal
the United States,
tion, vol. 29, no. 186 (June 1934),pp' 125-136'
(18)
Provided by the Maternal and Child Health Library, Georgetown University
C O\IPARABILITY
OF
tr'IATERNAL
MORTALITY
RATES
SUMMARY AND CONCLUSIONS
This study of the comparability of maternal mortality rates of th6
united states and foreigrrcountriesis based on 1,073 deaths associated
with pregnancy and childbirth that occurred during the year 1927,
including 997 deaths assignedto the puerperal state and 76 deaths
assignedto nonpuerperal causesby the united States Bureau of the
to
C"rrsrrr. The distribution by cause of the 997 deaths was similar
is,
sampie
The
state.
puerperal
the
to
assigned
in1927
that of all deaths
there{ore,representativeof the deaths so classifiedin the United States
during th" y"ur. Information in regard to 177 deaths that included
one of every type and one of every combination of circumstances representedin the samplel,073 was sent abroad,and the deathswere classified
as puerperalor nonpuerperalby the statistical officesin charge of classificatiorrof causeof death of 16 foreign countries'in accordancewith the
rules in force in these ofices. The countries making the assignments
were: Australia, Canada, Chile, Czechoslovakia,Denmark, EnglanJ
and wales, Estonia, France, Irish Free State, Itai,v, Netherlands, Ne1r'
Zealatd, Northern Ireland, Norway, Scotland' and Sr"'eden'
In addition to this material, the study is basedon information obtained
from the manuals for assigningcauseof death and the official reports of
the statistical bureausof the various countries,the reports of the Health
Committee of the Leagueof Nations and of the Committee on Definition
of stillbirth of the American Public Health Association,and specialstudies
of maternal mortality made by the British Ministry of Health and b1'
individual investigators.
The findings are particularly applicable to 1927, since the deaths
included occurred during that year; but since the assignmentswere
made in the spring of 1931,and a great deal of interpretative information
has been brought together from other sources'the findings are believed
to be indicative of the general situation with regard to comparability,
not oniy f.or 1927 but also for the years preceding and immediately
following the adoption of the 1929revisionof the international classification of causeof death. Unless radical changeshave been made verv
recently with regard to which no information is available they arc
indicative of the situation at the presenttime'
The study shows: First: That the methods of assignmentin use in
Australia, Netheriands,New Zealand,and Scotland are similar to that of
the United States, and the ofiicial maternal mortality rates are directly
(1e)
FE._
Provided by the Maternal and Child Health Library, Georgetown University
CO\IPARABILITY
OF
MATERNAL
MORTALITY
RATES
comparablewithin a small margin of error; that under the method of
Denmark a larger number of deaths would be assignedto the puerperal
state and the rate for the united states would be significantly higher
than it is now; that under the methodsof the other countriesincluded in
the study-Canada, Chile, Czechoslovakia,England and Wales, Estonia,
France,Irish Free State, Italy, Northern Ireland, Norway, and Swedena smaller number of deaths would be assignedto the puerperal state and
the rates for the united States would consequentrybe somewhat lower.
second: That differencesin methods of assignment are insuftcient to
explain the high maternal mortality rate of the united states as compared with foreign countries. The oftcial figure of the united states,
which in the last few years has exceededthat of every country except
Scotland, remains high no matter what method of assignmentis used.
Even if the method of the country assigningthe smallest proportion of
deathsto the puerperalstate were in use in the United Stat"r, the United
states figure would still exceedthat of all the countriesexcept Australia,
canada, chile, and scotland. Rates for the united states estimated i.
accordancewith the assignmentprocedure of the respective countries
are in every instanceexcept Scotlandin excessof and are in five instances
more than double the oftcial rates of the countries themselves. No
matter what method of procedure is used the united states retains an
exceedinglyhigh rate as comparedwith other countries.
Difference in definition of live births is shown to have a negligible effect
upon maternal mortality rates. Incompletenessof birth registration has
more weight, but it, too, is insufficient to account for more than a few
points of the excessof the united Statesrate over those of most foreign
countries. Neither factor is of great importance in connection with
comparability.
(20)
Provided by the Maternal and Child Health Library, Georgetown University
CO\IPARABILITY
OF
NfATERNAL
N{ORTALITY
R.A,TE S
RECOMMENDATIONS
Bureau of the Censusto
1. It would be desirablefor the United States
with pregnancy and
associated
p.rltiJ annually a table showing deaths
a table showing
also
and
cause
childbirth by primary and contributory
by color' in
States'
by
deaths associatedwith pregnancy and childbirth
urban and in rural districts in the States'
procedure and the
2. An investigation of the difierencesin assignment
formulationofrulesuniformlyacceptabletoimportantcountries.should
Institute at an early date.
be undertaken by the Internaiional statistical
is the first goal'
procedure
International uniformity in assignment
Thisuniformityisanessentialbasisforreliablestatisticaljudgmentas
tothecomparativeefiectuponmaternalmortalityofsuchfactorsas
socio-economic
g.ogr"pfti."i conditions, physiological. characteristics'
provision'
health
i".trr, obstetric practice, and community
(2t)
l**-.
Provided by the Maternal and Child Health Library, Georgetown University
CO}IPARABILITY
OF
\'IATERNAL
}IORTALITY
RATES
LIST OF REFERENCES
GeneralReferences
Definition of Stillbirth:
Report of the Committee to Consider the Proper Definition
of Stillbirth, American Public Health Association. American Journal of Public
Health, vol. 28, no. I (January t92B), pp.25-32'
Dudfield, Reginald:
Stillbirths in Relation to Infantile Mortality.
Royal Statistical Society, vol. 76, part I (December 1912), pp. 1-16.
Ministry
of Health:
Great Britain.
on l,laternal Mortality and Nlorbidity.
\,Iorbidity.
Journal of the
Interim Report of Departmental Committee
London, 1930. 151 pp.
: Final Report of Departmental Committee on Nlaternal Mortality
London, 1932. 156 pp.
and
Hultquist,
Gustaf : Nigra Anmirkningar till Vir Nya Dcidsorsaksstatistik. Allmlnna
S v e n s k aL a k a r t i d n i n g e n , e l e v e n t h y e a r , n o . 5 1 ( D e c . 1 8 , 1 9 1 4 ) , p ' 1 1 7 9 .
Kerr, J. l{. Munro:
\{aternal \,Iortality and Morbidity;
E . & S . L i v i n g s t o n e ,E d i n b u r g h , 1 9 3 3 . 3 8 2 p p .
League of Nations.
Health
Committee:
a study of their problems.
Minutes, 192+-1931.
Macphail, E. S.: Rules for Choice of Causes of Death in the Dominion Bureau of Statistics. Canadian Public Health Journal , voL 24, no. 9 (September 1933), pp. 413419,
Pearson, Karl, ed.: Tables for Statisticians and Biometricians. Cambridge University
Press, London, 1914. 143 pp.
de I'Etat Civil
Actuelle des Statistiques
sur I'Organisation
Rensei!,nements
dans Divers Pays. Ofice Permanent de l'Institut International de Statistique, The
Hague, L929, 73 pp.
Children's Bureau: Maternal Mortality; theriskof
U. S. Department of Labor.
death in childbirth and {rom all diseasescaused by pregnancy and confinement, by
Robert lvlorse Woodbury. Publication No. 158. Washington, 1926. 163 pp.
P. K.: The Completenessof Birth Registration in the United States. JourWhelpton,
nal of the American Statistical Association, vol. 29, no. 186 (June 1934), pp. 125-136,
Manuals of Cauvs of Death
Australia. Commonwealth Bureau of Censusand Statistics: The Nomenclature of Diseasesand Causes of Death as Revised and Adopted in 1900 by the International Commission, together with a Guide for Tabulation in CasesWhere N{ore than One
Cause of Death Is Assigned. Nlelbourne, 1907. 93 pp.
Nomenclatures Internationales des
MinistBre
des Affaires ftrangbres:
France.
\Iaiadies et des Causes de D6cds devant servir i l'6tablissement des Statistiques Nosologiques arr€tEespar la Commission internationale charg6e de la revision decennaledans
s a t r o i s i d m es e s s i o n1 9 2 0 . P a r i s , 1 9 2 1 . 7 7 p p .
Registrar General: \'Ianual of the International List of Causes of
Great Britain.
Death as Adapted {or Use in England and Wales, Scotland, and Northern Ireland.
Based on the Irourth Decennial Revision by the International Commission. London,
1931. 146 pp.
(22)
Provided by the Maternal and Child Health Library, Georgetown University
COMPARABILITY
OF
I\{ATERNAL
\tORT.TLITT
i'--::
--:e&:**
x****del Regno d'Italia: \
centrale di statistica
Istituto
\l:l:::L.
F-*rge*
del]e
p". la Statistica delle Cause di Morte e Dizionario
*'|n+rulle disposizioni relative alle denuncie delle causedi mo:re 3 ft--q
I"n'i.om-"ri
infettive. Fourth edition, Rome, 1933' 274 pp'
Italy.
--,i.t'"
Bureau of the Census: \la::e:' :f
of Commerce'
United States. Department
T
h
i
r
d revision, 1920. Washington, 191{.
D
e
a
t
h
.
o
f
the International List of Causes
302 pp.
Manual of the International List of Causesof Death' Fourth
r e v i s i o n ,1 9 2 9 ' W a s h i n g t o n , 1 9 3 1 ' 3 4 2 p p '
\fanual of Joint Causeso{ Death Showing Assignment to the pre. -i
ferredTitleofthelnternationalListofCausesofDeathWhenTwoCausesAreSimulta.
pp'
neously Reported. Second edition' Washington, 1925' 209
Assignment to the
Showing
of
Death
Causes
of
Manuai
Joint
when Two Causes are SimulPreferred Title of the International List of Causesof Death
255 pp'
taneously Reported. Third edition' Washington, 1933'
Ofi.cial Statistical
RePorts
Australia. Commonwealth Bureau of Census and Statistics: Australian
Demography. Bulletins43 to 51,1925to 1933' Canberra'
Ottawa.
Canada. Dominion Bureau of Statistics: Vital Statistics,L925to 1933.
de la Repiblica
Estadistico
Anuario
Estadistica:
de
General
Direcci6n
Chile.
EstadisticaAnualdela Repriblicade chile, Demografia,
dechile, Demografia,1925,1926;
1928;
de chile, Demografiay Beneficencia,
Repirblica
de
la
Anual
Estadistica
1g27;
1932;
Estadistica
1930,
1929,
Social,
y
Asistencia
EstadisticaAnual, Demografia
Chilena,monthly bulletins,1931' Santiagode Chile'
NlitteilungendesStatistischen
Czechoslovak Republic. St6tnl Uiad Statisticki:
Repub1ik,1926to 1932. Prague.
der iechoslovakischen
Staatsamtes
AnnuaireStatistiquedelaR6publiqueTch6coslovaque,1934.Prague.
i KongerigetDanmark, 1925to
hedsstyrelsen: Dgdsaarsagerne
Sund
Denmark.
1933. Copenhagen.
StaRegistrar-General's
England and Wales. Registrar General [GreatBritain]:
London'
L932'
to
parrI,1925
tistical Reviewof Englandand Wales,
Kuukiri (RecueilMensuel
Estonia. Riigi Statistika Keskbtiroo: Eesti Statistika
1932;Jatuary
du Bureau central Statistiquede i'Estonie),December1930;February
1933;FebruarY1934. Tallinn.
G6n6ralede la France,
France. Bureau de la Statistique G6n6rale: Statistique
to 1931;Annuaire
S6rie,1925
Nouvelle
la
Population,
de
du
Nlouvement
Statistique
Statig:ique,1927to 1932. Paris.
Annual Report of the RegistrarIrish Free State. General Reglster Ofhce:
General,SaorstatEireann,1931,193?' Dublin'
delle
Italy. Istituto Centrale di Statlstica del Re$no d'Italia: Statistica
Causedi Mo:te, 1976. Rome.
Annuario Statistico Italiano. Terza Serie,|928, |933; Quarta Serie,
193+. Rorne.
Netherlands. Centraal Bureau voof de Statistiek: Jaarcijfersvoor Nederland
(AnnuaireStatistiquedesPays-Bas),1929to 1933' The Hague'
Dood, 1925tol932. The Hague.
(23)
6aE-
Provided by the Maternal and Child Health Library, Georgetown University
CO\IPARABILITY
OF
MATERNAL
MORTALITY
RATES
New Zealand. Census and Statistics Office: Reporton the Vital Statisticsof the
Dominionof New Zealand,7925to 1933. Wellington.
Ministry of Finance. Registrar-General's Division:
Northern lreland.
Annual Report for 1932. Bel{ast.
Registrar-General's
Statistisk Arbok for Kongeriket Norge
Norway. Statistlske Centralbyri:
(AnnuaireStatistiquede 1aNorvdge)1934: Sundhctstilstanden
og Medisinalforholdene,
NorgesOffisielleStatistikk,1925to 1931. Oslo.
Scotland. General Register House: Annual Report of the Registrar-Generalfor
Scotland,
1933. Edinburgh.
Sweden. Statistiska Centralbyrdrn: Statistisk Arsbok for Sverige (Annuaire
SverigesOftciella Statistik, 1925to L931.
Statistiquede ia Suide ) 1933;Dodsorsaker,
Stockholm.
United States. Department of Commerce. Bureau of the Census: Mortality
Statistics. Annuai Reports1925to 1930. Unpublishedfigures1931to 1933. Washington.
Birth, Stillbirth,and Infant Mortality Statistics. AnoualReporta
L925ro 1930. Unpublishedfiguresl93l to 1933. Washington.
(2+)
o
Provided by the Maternal and Child Health Library, Georgetown University



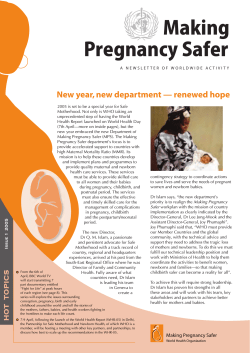

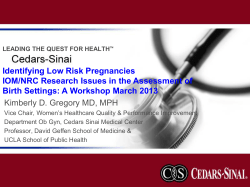




© Copyright 2026