
`Canberra Ra o` â A simplified ADC ra o that is reliable and
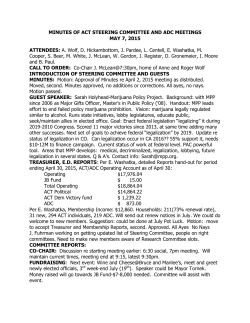
‘Canberra Ra?o’ – A simplified ADC ra?o that is reliable and reproducible in demonstra?ng diffusion restric?on in clinically significant prostate cancer foci Rajeev JYOTI1, Heath Liddell2, Hodo Z HAXHIMOLLA2,3 1Universal Medical Imaging, Calvary Hospital, Bruce, ACT 2Department of Urology, The Canberra Hospital, Garran, ACT 3The Australian Na:onal University, Garran, ACT INTRODUCTION RESULTS Diffusion weighted imaging (DWI) is an important component of the mul:parameteric prostate MRI (mpMRI), especially for detec:ng prostate cancer foci in peripheral zone. There are a number of publica:ons valida:ng that clinically significant prostate cancer foci demonstrate a reduc:on in apparent diffusion coefficient (ADC value) compared with ADC values within normal prosta:c :ssue. A wide range of low ADC values as a cut-‐off for presence of cancer has been proposed. A reduc:on in ADC value within each lesion can vary with MRI equipment, scanning protocols and viewing plaJorms used. We have developed a simplified ADC ra:o that is an easily reproducible and reliable tool for evalua:ng and repor:ng ADC changes within prostate lesions and assists in predic:ng their risk of prostate cancer. 40 lesions with abnormal in-‐gantry MR guided results, including Gleason 3+3=6 or greater, and prosta::s were retrospec:vely review using the ‘Canberra ra:o.’ Demographic, biopsy data and MRI data is presented below. Demographic data Characteris?cs of lesions Number of pa:ents 33 Number of lesions 40 Age (Mean) 67.3 yrs Median prostate vol AIM To determine whether a simplified ADC ra:o, which would be comparable across various plaJorms, would act as a reliable tool in detec:ng prostate cancer on mpMRI. 57.7 cc Total of lesions 40 Malignant 31 Gleason 6 11 Gleason 7 15 Gleason 8-‐10 5 Benign 9 Prosta::s 9 ADC ra?o data ADC ra:o < 0.4 ADC ra:o > 0.4 Mean ADC ra:o Malignant 31 0 0.32 Benign 0 9 0.59 PIRADS 3 2 6 0.46 PIRADS 4 22 3 0.42 PIRADS 5 18 0 0.31 Malignant lesions and those lesions graded with adverse PIRADS scores demonstrated lower ADC ra:o values METHODS 40 lesions with abnormal in-‐gantry MR guided biopsy results, including Gleason 3+3 = 6 or more and prosta::s were retrospec:vely evaluated using the ‘Canberra Ra:o’. ‘Canberra ra:o’ was calculated for each lesion by dividing lowest ADC value within each lesion by highest ADC value focus anywhere within the prostate, which shows normal signal characteris:cs on T1 and T2. One experienced radiologist and one senior urology registrar with only liYle experience in mpMRI of prostate performed the evalua:on of all the lesions using the ‘Canberra Ra:o’. Results were compared with in-‐gantry MR guided biopsy results and also with previous radiology reports prepared based upon absolute ADC values. Lesion loca?on data No of lesions Mean ADC ra:o Peripheral zone 29 Benign 7 0.57 Malignant 22 0.31 Transi:on zone 11 Benign 2 0.65 Malignant 9 0.34 Malignant lesions demonstrated ADC ra:o values below 0.4. This finding is irrespec:ve of the loca:on of the lesion within the prostate CONCLUSIONS REFERENCES The ‘Canberra Ra:o’ has poten:al to be a reliable and reproducible tool in demonstra:ng diffusion restric:on within clinically significant prostate cancer foci using a value of 0.40 or less as a cut-‐off. A greater number of lesions will need to be analyzed to validate this tool before it can be u:lised in clinical decision making. Kim CK, Park BK, Lee HM, Kwon GY, Value of diffusion-‐weighted imaging for the predic:on of prostate cancer loca:on at 3T using a phased-‐array coil: Preliminary results. Invest Radiol 2007; 42(12): 842 – 847 Park SY, Kim CK, Park BK, Kwon GY, Comparison of ADC calcula:on between two point and mul:point b-‐value, analysis in Prostate Ca and benign prostate :ssue at 3.0T: preliminary experience. AJR 2014; 203:W287–W294 Hambrock T, Somford D, Huisman H , van Oort I, Witjes J , Hulsbergen-‐van de Kaa C , Scheenen T, Barentsz J. Rela:onship between ADC at 3.0-‐T MR Imaging and Gleason Grade in Peripheral Zone Prostate Cancer. Radiology 2011 May 259(2): 453-‐461 ACKNOWLEDGEMENTS Universal Medical Imaging, Canberra, ACT 2604 Wang X, Qian Y, Liu B, Cao L, Fan Y, Zhang J, Yu Y. High-‐b-‐value diffusion-‐weighted MRI for the detec:on of prostate cancer at 3T, Clinical Radiology 2014 e1ee6 Vargas H, Akin O, Franiel T, Mazaheri Y, Zheng J, Udo C, Eastham J, Hricak H , Diffusion-‐weighted Endorectal MR Imaging at 3 T for Prostate Cancer: Tumor Detec:on and Assessment of Aggressiveness. Radiology 2011 Jun 259(3): 775-‐84








© Copyright 2026