
The Effect of a Polyvalent Antivenom on the Serum Venom Antigen
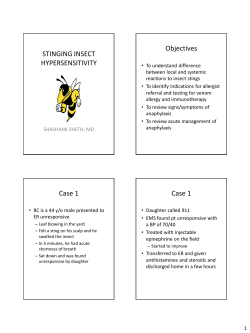
Basic & Clinical Pharmacology & Toxicology Doi: 10.1111/bcpt.12398 The Effect of a Polyvalent Antivenom on the Serum Venom Antigen Levels of Naja sputatrix (Javan Spitting Cobra) Venom in Experimentally Envenomed Rabbits Michelle Khai Khun Yap1, Nget Hong Tan1, Si Mui Sim2, Shin Yee Fung1 and Choo Hock Tan2 CENAR and Department of Molecular Medicine, University of Malaya, Kuala Lumpur, Malaysia and 2Department of Pharmacology, Faculty of Medicine, University of Malaya, Kuala Lumpur, Malaysia 1 (Received 18 November 2014; Accepted 20 March 2015) Abstract: The treatment protocol of antivenom in snake envenomation remains largely empirical, partly due to the insufficient knowledge of the pharmacokinetics of snake venoms and the effects of antivenoms on the blood venom levels in victims. In this study, we investigated the effect of a polyvalent antivenom on the serum venom antigen levels of Naja sputatrix (Javan spitting cobra) venom in experimentally envenomed rabbits. Intravenous infusion of 4 ml of Neuro Polyvalent Snake Antivenom [NPAV, F(ab0 )2] at 1 hr after envenomation caused a sharp decline of the serum venom antigen levels, followed by transient resurgence an hour later. The venom antigen resurgence was unlikely to be due to the mismatch of pharmacokinetics between the F(ab0 )2 and venom antigens, as the terminal half-life and volume of distribution of the F(ab0 )2 in serum were comparable to that of venom antigens (p > 0.05). Infusion of an additional 2 ml of NPAV was able to prevent resurgence of the serum venom antigen level, resulting in a substantial decrease (67.1%) of the total amount of circulating venom antigens over time course of envenomation. Our results showed that the neutralization potency of NPAV determined by neutralization assay in mice may not be an adequate indicator of its capability to modulate venom kinetics in relation to its in vivo efficacy to neutralize venom toxicity. The findings also support the recommendation of giving high initial dose of NPAV in cobra envenomation, with repeated doses as clinically indicated in the presence of rebound antigenemia and symptom recurrence. Venomous snakebite is an important yet neglected public health threat, especially in tropical and subtropical countries where the majority of snakebite victims comprises agricultural workers [1]. It can lead to local and systemic manifestation of venom toxicity, a condition called envenomation. Snakebite cases are known to be under-reported worldwide. Nevertheless, it has been estimated that envenomation incidence may soar as high as 1,800,000 with 94,000 deaths yearly [2]. The management for snakebite envenomation faces various challenges, one of which is pertaining to the availability of effective antivenom and the optimization of its use. Antivenom remains to date the only definitive treatment for envenomation [3,4]. The sustainability of antivenom supply has been great challenge worldwide with financial constrain being cited as the major reasons especially in developing countries [5]. Therefore, the existing therapeutic protocols for antivenoms should be further optimized on the basis of pharmacokinetics of venoms/toxins, and how antivenom could alter the clinicopharmacokinetic profile of venoms/toxins, which is essential for better tailoring of antivenom dosages. In this context, changes of venom pharmacokinetics induced by antivenoms should be part of pre-clinical assessment to study the in vivo time-based neutralization profile of antivenoms in animal models. However, there are only few studies Author for correspondence: Dr. Michelle Khai Khun Yap, Department of Molecular Medicine, Faculty of Medicine, University of Malaya, 50603 Kuala Lumpur, Malaysia (fax +603 79674957, e-mail [email protected]). that addressed the effects of antivenom on the pharmacokinetics of venoms in experimentally envenomed animals, limited to only certain types of venom and antivenom. In the case of Vipera aspis venom, Riviere et al. [6] reported that the F(ab0 )2 antivenom given at the right dose and via the appropriate route of administration induced a complete and durable depletion of plasma venom level in envenomed rabbits, while Pepin-Covatta et al. [7] showed that an enhanced F(ab0 )2 antivenom redistributed the tissue-deposited venom into blood and caused a decline in the venom’s terminal half-life in rabbits. Rocha et al. [8] demonstrated in mice a similar redistribution phenomenon for Bothrops erythromelas venom. Besides, comparison of different forms of antivenom [IgG, F(ab0 )2, Fab] on their kinetic behaviours optimal for in vivo neutralization has also been performed using pharmacokinetic model; for instance, F(ab0 )2 has been indicated to be the most suitable for treating envenomation by V. aspis [6] and Walterinnesia aegyptia [9] because of their unique pharmacokinetic characteristics. In Asia, pharmacokinetics of several venoms or toxins have been reported [10–15], but the modifying effect induced by antivenom on the venom/toxin pharmacokinetics in vivo has not been well characterized. One of the medically important venomous snakes in the South-East Asia is the Javan spitting cobra (Naja sputatrix). Its pharmacokinetic profile in rabbits has been characterized in our earlier study, including the findings of intramuscular bioavailability (41.7%) that indicated extent of absorption of the intramuscularly inoculated venom © 2015 Nordic Association for the Publication of BCPT (former Nordic Pharmacological Society) MICHELLE KHAI KHUN YAP ET AL. 2 into the systemic circulation to cause lethality [13]. The venom, as with several other Asiatic cobra venoms, has been recently shown to be effectively neutralized by a regional polyvalent antivenom, Neuro Polyvalent Antivenom (NPAV) in mouse lethality assay [16]. Neuro Polyvalent Antivenom is a newly developed polyvalent F(ab0 )2 antivenom (Queen Saovabha Memorial Institute, Bangkok) derived from horses by immunization against four common Thai elapid venoms: Naja kaouthia (Thai monocled cobra), Ophiophagus hannah (king cobra), Bungarus candidus (Malayan krait) and Bungarus fasciatus (banded krait). In this study, we examined the modifying effect of NPAV on the serum venom levels of N. sputatrix venom in experimentally envenomed rabbits for potential therapeutic optimization. Materials and Methods Ethics statement. All animals were handled according to CIOMS (Council for International Organisations of Medical Sciences) guidelines on animal experimentation [17]. The experimental protocol on the animal study was approved by the Animal Care and Use Committee, Faculty of Medicine, University of Malaya (Ethics clearance number: 2013-06-07/MOL/R/FSY). Venom, polyvalent antivenom, reagents and separation media. Lyophilized N. sputatrix venom was purchased from Latoxan (Valence, France). NPAV was a gift from Queen Saovabha Memorial Institute, Thai Red Cross Society, Thailand. The NPAV (lyophilized; Batch no: 0030208) is a purified F(ab0 )2 obtained from sera of horses hyperimmunized against a mixture of the venoms of Naja kaouthia (Thai monocled cobra), Ophiophagus hannah (king cobra), Bungarus candidus (Malayan krait) and Bungarus fasciatus (branded krait). Sephadexâ G-25 gel and Protein A affinity column were purchased from GE Healthcare (Princeton, New Jersey, USA). Goat anti-rabbit IgG-horseradish peroxidase (HRP) was obtained from Abcam (Cambridge, UK). Ion-exchange media and all other reagents used in this study were of analytical grade and purchased from Sigma-Aldrich (St. Louis, CA, USA). Animals. The animals used in this study (New Zealand white rabbits, 2 kg; and ICR mice, 18–20 g) were supplied by Chenur Supplier (Selangor, Malaysia). The animals were housed in Laboratory Animal Centre, Faculty of Medicine, University of Malaya, and received water and food ad libitum throughout the experiment. Preparation of antibodies IgG and IgG-HRP against N. sputatrix venom. The immunoglobulin G (IgG) against N. sputatrix venom was produced in rabbits as described earlier [13]. Anti-N. sputatrix IgG was purified by Sephadexâ G-25 gel filtration chromatography followed by Protein A affinity chromatography [18]. The IgGhorseradish peroxidase conjugate (IgG-HRP) conjugate was prepared as described by Wisdom [19]. Determination of serum venom antigen levels using double-sandwich ELISA. Double-sandwich ELISA was conducted as described previously [20]. It was used to monitor the serum venom antigen levels after experimental envenomation in individual rabbits. ELISA microplates were coated with 100 ll of the anti-N. sputatrix IgG (4 lg/ml) at 4°C overnight. Plates were then incubated with 100 ll of diluted serum samples (1:20) collected at different time intervals from the pharmacokinetic study. This was followed by incubation of 100 ll of anti-N. sputatrix IgG-HRP conjugate (1:400) for 2 hr, and 100 ll of the substrate o-phenyldiamine dihydrochloride (0.4 mg/ml) was then added. The reaction was terminated 1 hr later by adding 50 ll of 12.5% (v/v) sulphuric acid, and the absorbance at 492 nm was determined using Bio-Rad Model 690 microplate reader. A standard curve was constructed using pre-envenomed sera spiked with varying dilutions of the venom. The effect of NPAV on the pharmacokinetics of N. sputatrix venom in experimentally envenomed rabbits. Pharmacokinetics of intramuscularly injected N. sputatrix venom. A sublethal dose of 1 mg of N. sputatrix venom (0.5 mg/kg) dissolved in 500 ll normal saline was injected intramuscularly into the hind leg of rabbits (n = 3). This served as the control group (envenomation without antivenom treatment). Blood samples were collected from the central ear artery before and at 5, 30 min., 1, 1.5, 2.5, 4.5, 6.5, 12 and 24 hr after venom injection. The collected blood samples were centrifuged at 3500 9g for 20 min. to obtain the serum which was kept at 20°C until further analysis. Serum venom antigen levels were monitored using the double-sandwich ELISA as described above. Pharmacokinetics of N. sputatrix venom in the presence of a single dose NPAV. A sublethal dose of 1 mg N. sputatrix venom (0.5 mg/ kg) was dissolved in 500 ll normal saline and injected intramuscularly into the hind leg of rabbits (n = 3). One hour after venom injection, 4 ml of NPAV was infused into the marginal ear vein of rabbits over 20 min. Blood samples were collected from the central ear artery before and at 5, 30 min., 1, 1.5, 2.5, 4.5, 6.5, 12 and 24 hr after experimental envenomation. The collected blood samples were centrifuged at 3500 9g for 20 min. to obtain the serum which was kept at 20°C for double-sandwich ELISA. Pharmacokinetics of N. sputatrix venom after repeated dosing of NPAV. In the second series of experiment, an additional 2 ml of NPAV was infused intravenously into experimentally envenomed rabbits 1 hr after the initial 4-ml infusion. Blood samples were collected before and at 5, 30 min., 1, 1.33, 1.83, 2.33, 2.5, 4.5, 6.5, 12 and 24 hr after experimental envenomation. The collected blood samples were processed as described above. Pharmacokinetic analysis. The pharmacokinetic parameters were determined using the method of feathering [21]. The area under the curve (AUC) was calculated from 1 hr (post-experimental envenomation) to the last experimental time-point by trapezoidal rule. The initial phase rate constant (a) and terminal phase rate constant (b) were determined by the method of feathering using the best fit line obtained for the initial phase and terminal phase, respectively. The initial phase half-life (T1/2a) and terminal phase half-life (T1/2b) were determined by the formula T1/2a or T1/2b = 0.693/a or b, respectively. The distribution rate constants for the transfer between central compartment (designated as 1) and peripheral compartment (designated as 2) were calculated from the equations: k21 ¼ ðAb þ BaÞ=ðA þ BÞ and k12 ¼ a þ b k21 ðab=k21 Þ: The other important pharmacokinetic parameters were determined as follows: Volume of distribution by area, Vd, area = CL/b. Clearance, CL = dose (Fi.v. or Fi.m.)/AUC0–∞, where Fi.v. is the intravenous bioavailability which is 1, while Fi.m. is the intramuscular bioavailability, hence: © 2015 Nordic Association for the Publication of BCPT (former Nordic Pharmacological Society) ANTIVENOM’S EFFECT ON SERUM VENOM LEVELS Fi:m: ¼ AUCi:m: Dosei:v: AUCi:v: Dosei:m: Determination of the median lethal dose (LD50) of N. sputatrix venom. The intravenous median lethal dose (LD50 i.v.) of the venom was determined by injecting appropriate dilutions of the venom into the caudal vein of mice (n = 4, 18–20 g). The intramuscular median lethal dose (LD50 i.m.) of the venom was determined by injecting various amounts of the venom into the thigh muscle of mice (n = 4, 18–20 g). The survival ratio was determined after 24 hr. The LD50(95% confidence interval) was then calculated by the probit analysis [22]. Neutralization of N. sputatrix venom by NPAV. Neutralization of N. sputatrix venom by antivenom was carried out with slight modification from the method described by Ramos-Cerrillo et al. [23], where the venom was pre-incubated with the antivenom prior to injection: N. sputatrix venom (2.5 LD50 i.v.) was pre-incubated with varying dilutions of NPAV (50–200 ll) for 30 min. at 37°C and the total injected volume was adjusted to 300 ll. The mixture (300 ll) was then injected slowly into the caudal vein of mice (n = 4). The control group consists of mice injected with a mixture (300 ll) of N. sputatrix venom (2.5 LD50 i.v.) dissolved in normal saline. The number of mice surviving after 24 hr was recorded. Neutralization capacity of the antivenom was expressed in terms of median effective dose, ED50 (ll antivenom/2.5 LD50 i.v.), which is defined as the amount of antivenom required to neutralize the venom at 50% survival. ED50 was calculated by the probit method [22]. Another series of neutralization experiment for N. sputatrix venom was carried out by intramuscular injection of N. sputatrix venom (2.5 LD50 i.m.) into mice (n = 4) at caudal thigh muscle, followed by intravenous injection of varying dilutions of NPAV (50–200 ll) 10 min. later (experiments without pre-incubation of venom and antivenom). The number of mice surviving after 24 hr was recorded. The control group consists of mice (n = 4) injected with the same 2.5 LD50 dose of N. sputatrix venom, followed by intravenous injection of normal saline 10 min. later. Median effective dose, ED50 (ll antivenom/2.5 LD50 i.m.), was calculated by the probit method [22]. Neutralization potency of the antivenom, expressed as mg/ml, or the amount of venom that is completely neutralized by one unit volume of the reconstituted antivenom, was calculated according to Morais et al. [24]. 3 0.82 mg of the venom, neutralized by 1 ml of NPAV, respectively. The effect of NPAV on the serum venom antigen levels of N. sputatrix venom. Fig. 1 shows the serum venom antigen–time profile of the intramuscularly injected N. sputatrix venom (solid line). Part of the pharmacokinetic parameters were published in an earlier report [13] with AUC0-∞ of 6193.59 676.79 ng/ml.hr, T1/2b of 18.86 5.61 hr, Vd, area of 1.88 0.72 l and CL of 67.89 7.05 ml/hr. Serum venom antigen peaked at approximately 1 hr after injection. Fig. 1 also shows the serum venom antigen–time profile of the injected N. sputatrix venom when 4 ml of NPAV was infused intravenously into the rabbit, over 20 min., 1 hr after the i.m. injection of the venom. There was a sharp decline in the venom antigen levels immediately after the infusion of the antivenom, from a peak 300 ng/ml to 80 ng/ml 1 hr after the antivenom infusion (fig. 1). This was, however, followed by transient resurgence of the serum venom antigen level to about 90 ng/ml 3 hr later (i.e. at 4th post-injection of the venom), and decreased gradually thereafter. As a result, the 4 ml of NPAV only reduced the AUC1–24 h value of the venom antigens by 41.6% (table 1). In the second series of experiment, an additional 2 ml of NPAV was infused intravenously 1 hr after the initial infusion of 4 ml of NPAV. This managed to reduce the serum venom antigen levels to <50 ng/ml by 5 hr (fig. 1). This was followed by a steady decline with the mean antigen levels at subsequent time-points being significantly lower than controls and rabbits treated with 4 ml NPAV (p < 0.05). The mean AUC1–24 h value was significantly reduced by 67.1% compared to controls, and by an extra 25.5% compared to the group treated with 4 ml NPAV (p < 0.05) (table 1). Discussion Statistical analysis. Median lethal dose, LD50, of the venoms and ED50 of antivenom are expressed as mean with 95% confidence intervals (CI) and were calculated using the probit method [22]. All data are reported as the mean S.D. or mean (95% CI). The mean difference between two independent groups was determined by Student’s t-test, and one-way ANOVA was used to compare mean differences between two or more independent groups. The level of significance was set at p = 0.05. The statistical analysis was conducted using SPSS 20.0 (SPSS Inc., Chicago, IL, USA). Results Neutralization of N. sputatrix venom by NPAV. The intravenous LD50 and intramuscular LD50 of the N. sputatrix venom in mice were determined to be 0.9 lg/g (0.59– 1.36 lg/g, 95% CI) and 1.12 lg/g (0.62–1.64 lg/g, 95% CI), respectively. The median effective doses (ED50) of NPAV were found to be 136.72 ll/2.5 LD50 in experiments with preincubation of venom and antivenom, and 136.68 ll/2.5 LD50 in experiments when venom and antivenom were injected independently. These values are equivalent to 0.65 mg and In this study, the level of venom antigen in the serum was measured as a whole, using the anti- N. sputatrix IgG. Our earlier study using ELISA and immunoblotting methods has established that the anti- N. sputatrix IgG reacted mainly with low molecular weight toxins of the venom, which represent the bulk of venom proteins (>80%) and also the most important toxins, that is the neurotoxins, cardiotoxins and phospholipase A2 [13]. Thus, the present approach represents a good approximation of the true picture of the serum kinetics of N. sputatrix venom. Neuro Polyvalent Antivenom is a polyvalent antivenom raised against four Thai elapid venoms, one of which is the venom of Thai monocellate cobra, N. kaouthia. Our neutralization assays using both inoculation with venom–antivenom pre-mixture and independent injections of the venom and antivenom into mice confirmed that NPAV could effectively cross-neutralize N. sputatrix venom, with effective dose and potency results comparable to those reported by Leong et al. [16]. Interestingly, although the pre-mixture inoculation © 2015 Nordic Association for the Publication of BCPT (former Nordic Pharmacological Society) MICHELLE KHAI KHUN YAP ET AL. 4 Fig. 1. The effects of Neuro Polyvalent Antivenom (NPAV) on the serum concentration–time profile of Naja sputatrix venom. The serum concentration–time profiles of N. sputatrix venom (in semi-logarithmic plot) of three series of experiments are illustrated. The first series is the control group (solid line) where only the venom (0.5 mg/kg) was injected intramuscularly into rabbits (control data extracted from Yap et al. [13]). In the second series of experiment (dash line), 4 ml of NPAV was infused into the marginal ear veins of the rabbits 1 hr after venom injection. In the third series of experiment (dash dot line), 4 ml of NPAV was infused into the marginal ear veins of the rabbits 1 hr after venom injection, followed by infusion of another 2 ml of NPAV 1 hr later. Insert: Serum concentration–time profile of N. sputatrix venom (in arithmetic scale) during the first 2.5 hr, with and without NPAV administration. All data shown are mean S.D. (n = 3). Table 1. Area under curve (AUC1–24 h) values with and without Neuro Polyvalent Antivenom (NPAV) antivenom immunotherapy. Antivenom immunotherapy Without NPAV immunotherapy Infusion of 4 ml of NPAV Infusion of 4 + 2 ml of NPAV AUC1–24 h (ng/ml.h) Reduction in AUC1–24 h value (%) 3409.1 1234.7 – 1991.4 140.5 41.6 1118.9 86.7 67.1 Data are expressed as mean S.D. (n = 3, 2 kg each) for each group. Reduction in AUC1–24 h value is expressed in percentage (%) of the AUC1–24 h in the absence of NPAV. method is generally considered not representative of a post-envenomation treatment, our study has shown nearly identical efficacy and potency of NPAV used in neutralizing the lethal effects of N. sputatrix venom tested on both assays. The pharmacokinetic study further elucidated how NPAV affects the serum venom antigen levels in animals. While venom lethality test (and the corresponding lethality protection test) was conducted in mice reasonably as permitted by the institutional animal use ethics, rabbits were used in pharmacokinetic modelling as they are larger animals ensuring sufficient blood collection from the same animal over a several-day schedule possible. Considering the fact that serum venom antigens peaked 1 hr after venom injection [13], NPAV was administered at that point of time to observe any noticeable venom level depleting in the animals. The antivenom NPAV was delivered via intravenous route [4] in contrast to intramuscular for two main reasons: (i) intramuscular injection is associated with incomplete and slow antivenom absorption that hampers the desired antivenom effect for rapid immunoneutralization; and (ii) intramuscular injection causes intense local tissue reaction and can be disastrous in envenomation associated with coagulopathy. In this study, the initial NPAV infusion rapidly reduced the serum venom antigen levels remarkably ~70% within 1 hr, indicating the capability of NPAV in rapidly forming immunocomplex with the venom antigens in vivo. The subsequent gradual and transient resurgence of serum venom antigen levels, however, implied that the antivenom at the given dose and time induced only partial neutralization of the circulating venom antigens. In fact, the AUC was only reduced by 41.6%, even though the amount of antivenom injected (4 ml, with a neutralization potency 0.82 mg/ml, that is able to neutralize 3.28 mg of venom) should be more than sufficient to neutralize the amount of venom injected (1 mg). This phenomenon of resurgence of snake venom antigen levels in blood, that is rebound venom antigenemia after antivenom administration, has been observed in both animal [6,8] and clinical studies of snakebite treatment [25–29]. The redistribution of tissue-bound antigens into the vascular compartment following a shift in the intercompartmental equilibrium is induced by the removal of the intravascular venom antigens [6,30], while the rebound antigenemia exceeds the limit for antivenom to bind. This phenomenon is in fact not uncommon © 2015 Nordic Association for the Publication of BCPT (former Nordic Pharmacological Society) ANTIVENOM’S EFFECT ON SERUM VENOM LEVELS in immunotherapy as the similar rebound antigenemia has been reported in the treatment for digoxin and colchicine poisoning using Fab [31,32]. Clinically, this can result in recurrent toxicities, for example relapsed neuromuscular paralysis and haemorrhages in envenomation [25,33,34], worse still if the seemingly recovering patients are weaned of treatment. As the monitoring of venom antigenemia is not routinely performed clinically, it is hence of upmost importance to optimize antivenom posology and protocol according to different venoms and antivenom products, in addition to meticulous syndrome monitoring. The rebound N. sputatrix antigenemia was perhaps partially contributed by a small amount of venom continuously absorbed from injection site within first several hours. Therefore, it directly resulted in the exhaustion of free F(ab0 )2 in the blood for immunocomplexation that causes venom resurgence. The terminal half-lives of other reported F (ab0 )2 antivenom in rabbit, 55 9 hr [6], 49.52 3.07 hr [35] and 61.4 7 hr [36], indicated that F(ab0 )2 antivenom is not eliminated earlier than the venom, hence excluding the half-life mismatch as the cause for the resurgence for venom antigen level. Theoretically, an ideal antivenom possesses the ability to redistribute tissue-bound antigens into the vascular compartment for the circulating antivenom to bind for elimination [37]. The rebound N. sputatrix venom antigenemia in the current study was successfully diminished when a ‘4 + 2 ml’ antivenom infusion regimen was applied. Compared with the 4 ml single dosing, the additional 2 ml of antivenom 1 hr later was sufficient to neutralize the resurged venom antigens and to reduce further the subsequent antigenemia to significantly lower levels, resulting in a significant decrease in the total antigenemia (67.1%, indicated by AUC1–24 h) compared with the untreated group. The result suggests that NPAV at the given regimen is able to reduce or reverse the toxic effects of N. sputatrix venom as serum venom antigen level is known to correlate with the severity of envenomation [38,39]. Overall, our results support the use of a high initial dose of NPAV, as recommended by the manufacturer (10 vials, equivalent to 100 ml) to rapidly induce a sharp decline in venom antigen levels. The finding of rebound antigenemia also implies that the use of the antivenom product for N. sputatrix envenomation can potentially induce venom redistribution, and supports the recommendation of giving repeated antivenom doses to alleviate recurrent symptoms and to enhance the elimination of toxins from the body [25,40,41]. As the bioavailability of i.m. injected N. sputatrix venom was reported to be approximately 41.7% [13], it is thus estimated that when 1 mg of the venom was injected into the rabbit (0.5 mg/kg rabbit), about 0.42 mg of the venom was absorbed into systemic circulation. However, our results indicated that 4 ml and ‘4 + 2 ml’ dosing regimen over the time course only managed to reduce the total amount of venom in the circulation by 41.6% (0.17 mg) and 67.1% (0.28 mg) of venom, respectively, although according to in vivo neutralization assay (venom and antivenom were injected independently into mice), the ‘4 + 2 ml’ dosing was capable to neutralize 4.92 mg of venom (as indicated by potency = 0.82 mg/ml). 5 This apparent ‘discrepancy’ in the efficacy of antivenom treatment reflects an important point for antivenom assessment and its result interpretation: the pharmacokinetic study provides in vivo evidence of antivenom physically neutralizes the venom antigens (via immunocomplexation), in contrast to the neutralization test which instead provides measurement of the capability of antivenom to prevent the impending death caused by venom. In fact, the animals survived from neutralization test within the observation period might still have persistent, low but sublethal venom levels in the circulation which could still be harmful and with possibility of symptom recurrence. Thus, the neutralization potency of antivenoms determined in mice can be useful for efficacious comparison between different antivenoms or against different venoms [16,42]. However, it is not an absolute indicator of its therapeutic capability to deplete venom antigenemia vis- a-vis complete neutralization of venom toxicity in animals or human beings. Therefore, for an optimal treatment outcome using NPAV in this study, our pharmacokinetic results suggest the necessity to administer a far larger amount of antivenom in the case of human envenomation by N. sputatrix venom than was determined by conventional neutralization assay. Furthermore, in anticipation of recurrent antigenemia, the patients should be monitored meticulously after antivenom administration. A repeated and booster dose of antivenom should be given where indicated clinically as the patients show worsening systemic signs. Acknowledgements The authors thank Queen Saovabha Memorial Institute, Thai Red Cross Society, for supplying the antivenoms. This work was funded by RM 282-14APR and RG348-15AFR from University of Malaya, Kuala Lumpur, Malaysia. Conflict of Interest The authors disclose that there are no conflict of interests. References 1 Gutierrez JM, Theakston RDG, Warrell DA. Confronting the neglected problem of snake bite envenoming: the need for a global partnership. PLoS Med 2006;3:727–31. 2 Kasturiratne A, Wickremasinghe AR, de Silva N, Gunawardena NK, Pathmeswaran A, Premaratna R et al. The global burden of snakebite: a literature analysis and modelling based on regional estimates of envenoming and deaths. PLoS Med 2008;5:e218. 3 Warrell DA. Snake bite. Lancet 2010;375:77–88. 4 World Health Organisation. WHO Guidelines for the Production Control and Regulation of Snake Antivenom Immunoglobulins. WHO Press, World Health Organisation, Geneva, 2010. 5 Brown NI. Consequences of Neglect: analysis of the Sub – Saharan African snake antivenom market and global context. PLoS Negl Trop Dis 2012;6:e1670. 6 Riviere G, Choumet V, Audebert F, Sabouraud A, Debray M, Scherrmann JM et al. Effect of antivenom on venom pharmacokinetics in experimentally envenomed rabbits: toward an optimisation of antivenom therapy. J Pharmacol Exp Ther 1997;281:1–8. 7 Pepin-Covatta S, Lutsch C, Lang J, Scherrmann JM. Preclinical assessment of immunoreactivity of a new purified equine F(ab’)2 against European viper venom. J Pharm Sci 1998;87:221–5. © 2015 Nordic Association for the Publication of BCPT (former Nordic Pharmacological Society) 6 MICHELLE KHAI KHUN YAP ET AL. 8 Rocha ML, Valencßa RC, Maia MB, Guarnieri MC, Araujo IC, Araujo DA. Pharmacokinetics of the venom of Bothrops erythromelas labelled with 131I in mice. Toxicon 2008;53:526–9. 9 Ismail M, Abd-Elsalam MA, Al-Ahaidib MS. Pharmacokinetics of 125 I-labelled Walterinnesia aegyptia venom and its specific antivenins: flash absorption and distribution of the venom and its toxin versus slow absorption and distribution of IgG, F(ab’)2 and F(ab) of the antivenin. Toxicon 1998;36:83–114. 10 Maung M-T, Khin M-M, Mi M-K, Thein T. Kinetics of envenomation with Russell’s viper (Vipera russelli) venom and of antivenom use in mice. Toxicon 1988;6:373–8. 11 Sim SM, Saremi K, Tan NH, Fung SY. Pharmacokinetics of Cryptelytrops purpureomaculatus (mangrove pit viper) venom following intravenous and intramuscular injections in rabbits. Int Immunopharmacol 2013;17:997–1001. 12 Tan CH, Sim SM, Gnanathasan CA, Fung SY, Tan NH. Pharmacokinetics of the Sri Lankan hump-nosed pit viper (Hypnale hypnale) venom following intravenous and intramuscular injections of the venom into rabbits. Toxicon 2014;79:37–44. 13 Yap MKK, Tan NH, Sim SM, Fung SY. Toxicokinetics of Naja sputatrix (Javan spitting cobra) venom following intramuscular and intravenous administrations of the venom into rabbits. Toxicon 2013;68:18–23. 14 Yap MKK, Tan NH, Sim SM, Fung SY, Tan CH. Pharmacokinetics of Naja sumatrana (Equatorial spitting cobra) venom and its major toxins in experimentally envenomed rabbits. PLoS Negl Trop Dis 2014;8:e2890. 15 Zhao H, Zheng J, Jiang Z. Pharmacokinetics of thrombin-like enzyme from venom of Agkistrodon halys ussuriensis Emelianov determined by ELISA in the rat. Toxicon 2001;39:1821–6. 16 Leong PK, Sim SM, Fung SY, Sumana K, Sitprija V, Tan NH. Cross neutralization of Afro-Asian Cobra and Asian Krait venoms by a Thai Polyvalent Snake Antivenom (Neuro Polyvalent Snake Antivenom). PLoS Negl Trop Dis 2012;6:e1672. 17 Howard-Jones NA. A CIOMS ethical code for animal experimentation. WHO Chron 1995;39:51–6. 18 Hudson L, Hay FC. Practical Immunology. Blackwell Scientific Publications, Palo Alto, 1980. 19 Wisdom GB. Horseradish peroxidase labelling of IgG antibody. In: Walker JM, (ed.). The Protein Protocols Handbook. Humana Press, Totowa, New Jersey, 1996;273–4. 20 Tan NH, Lim KK, Jaafar MI. An investigation into the antigenic cross-reactivity of Ophiophagus Hannah (king cobra) venom neurotoxin, phospholipase A2, haemorrhagin and L-amino acid oxidase using enzyme linked immunosorbent assay. Toxicon 1993;31:865– 72. 21 Shargel L, Wu-Pong S, Yu ABC. Applied Biopharmaceutics and Pharmacokinetics, 6th edn. McGraw Hills, New York, 2012. 22 Finney DJ. Probit Analysis. Cambridge University Press, Cambridge, UK, 1952. 23 Ramos-Cerrillo B, de Roodt AR, Chippaux JP, Olguın L, Casasola A, Guzman G et al. Characterisation of a new polyvalent antivenom (Antivipmynâ Africa) against African vipers and elapids. Toxicon 2008;52:881–8. 24 Morais V, Ifran S, Berasain P, Massaldi H. Antivenoms: potency or median effective dose, which to use? J Venom Anim Toxins Incl Trop Dis 2010;16:191–3. 25 Ariaratnam CA, Sj€ostr€om L, Raziek Z, Kularatne SA, Arachchi RW, Sheriff MH et al. An open, randomised comparative trial of two antivenoms for the treatment of envenoming by Sri Lankan Russell’s viper (Daboia russelii russelii). Trans R Soc Trop Med Hyg 2001;95:74–80. 26 Warrell DA, Looareesuwan S, Theakston RD, Phillips RE, Chanthavanich P, Viravan C et al. Randomised comparative trial of three monospecific antivenoms for bites by the Malayan pit viper (Calloselasma rhodostoma) in southern Thailand: clinical and laboratory correlations. Am J Trop Med Hyg 1986;35:1235–47. 27 Khin OL, Aye AM, Tun P, Theingie N, Min N. Russell’s viper venom levels in serum of snake bite victims in Burma. Trans R Soc Trop Med Hyg 1984;78:165–8. 28 Seifert SA, Boyer LV, Dart RC, Porter RS, Sjostrom L. Relationship of venom effects to venom antigen and antivenom serum concentrations in a patient with Crotalus atrox envenomation treated with a Fab antivenom. Ann Emerg Med 1997;30:49–53. 29 Dart RC, Seifert SA, Boyer LV, Clark RF, Hall E, Mckinney P et al. A randomised multicentre trial of crotalinae polyvalent immune Fab (ovine) antivenom for the treatment of Crotaline snakebite in the United States. Arch Intern Med 2001;161:2030–6. 30 Chippaux JP. Snake Venoms and Envenomations (FW Huchzermeyer, Trans.). Krieger Publishing Company, Malabar, FL, 2006. 31 Smith TW, Haber E, Yeatman L, Butler VP Jr. Reversal of advanced digoxin intoxication with Fab fragments of digoxin specific antibodies. N Engl J Med 1976;294:797–800. 32 Sabourad AE, Urtizberea M, Cano NJ, Grandgeorge M, Rouzioux JM, Scherrmann JM. Colchicine-specific Fab fragments alter colchicine disposition in rabbits. J Pharmacol Exp Ther 1992;260:1214–9. 33 Wetzel WW, Christy NP. A king cobra bite in New York City. Toxicon 1989;27:393–5. 34 Ho M, Silamut K, White NJ, Karbwang J, Looareesuwan S, Phillips RE et al. Pharmacokinetics of three commercial antivenoms in patients envenomed by the Malayan pit viper, Calloselasma rhodostoma, in Thailand. Am J Trop Med Hyg 1990;42:260–6. 35 Pepin-Covatta S, Lutsch C, Grandgeorge M, Lang J, Scherrmann JM. Immunoreactivity and pharmacokinetics of horse anti-scorpion venom F(ab’)2-scorpion venom interactions. Toxicol Appl Pharmacol 1996;141:272–7. 36 Bazin-Redureau M, Pepin S, Hong G, Debray M, Scherrmann JM. Interspecies scaling of clearance and volume of distribution for horse antivenom F(ab’)2. Toxicol Appl Pharmacol 1998;150:295–300. 37 Gutierrez JM, Leon G, Lomonte B. Pharmacokinetic-pharmacodynamic relationships of immunoglobulin therapy for envenomation. Clin Pharmacokinet 2003;42:721–41. 38 Barraviera B, Sartori A, Pereira da Silva MF, Kaneno R, Peracßoli MTS. Use of an ELISA assay to evaluate venom, antivenom, IgG and IgM human antibody levels in serum and cerebrospinal fluid from patients bitten by Crotalus durissus terrificus in Brazil. J Venom Anim Toxins Incl Trop Dis 1996;2:14–27. 39 Otero R, Gutierrez JM, Nunez V, Robles A, Estrada R, Segura E et al. A randomised double blind clinical trial of two antivenoms in patients bitten by Bothrops atrox in Columbia. Trans R Soc Trop Med Hyg 1996;90:696–700. 40 Seifert SA. Pharmacokinetic analysis of a crotalid Fab antivenom and theoretical considerations for the prevention of coagulopathic recurrence. J Toxicol Clin Toxicol 1998;36:526–7. 41 Warrell DA. Guidelines for the Management of Snake-Bites. World Health Organisation, Regional Office for South-east Asia, India, 2010. 42 Leong PK, Tan CH, Sim SM, Fung SY, Sumana K, Sitprija V et al. Cross neutralization of common Southeast Asian viperid venoms by a Thai polyvalent antivenom (Hemato Polyvalent Snake Antivenom). Acta Trop 2014;132:7–14. © 2015 Nordic Association for the Publication of BCPT (former Nordic Pharmacological Society)









© Copyright 2026