
View/Open - University of the Western Cape
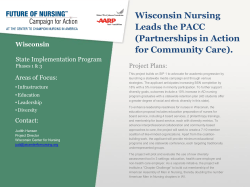
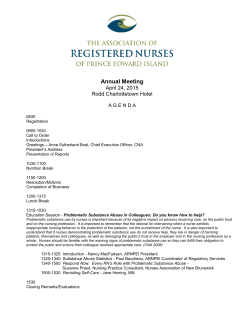
International Journal of Africa Nursing Sciences 2 (2015) 26–33 Contents lists available at ScienceDirect International Journal of Africa Nursing Sciences journal homepage: www.elsevier.com/locate/ijans Developing a context appropriate clinical guideline for post-operative pain management in Ghana: A participatory approach Lydia Aziato a,⇑, Oluyinka Adejumo b a b School of Nursing, University of Ghana, P.O. Box LG43, Legon, Ghana School of Nursing, University of the Western Cape, Private Bag X17, Bellville 7535, South Africa a r t i c l e i n f o Article history: Received 6 May 2014 Received in revised form 21 November 2014 Accepted 10 March 2015 Available online 17 March 2015 Keywords: Collaboration Post-operative pain Consensus Stakeholder Expert review a b s t r a c t Clinical guidelines involve statements that guide clinicians to provide effective care to patients. However, there are no context appropriate clinical guidelines for post-operative pain (POP) management in Ghana. This study sought to develop such a clinical guideline. The study adopted a participatory approach drawing from the existing literature to develop the guideline with the involvement of 27 experts and stakeholders including nurses, doctors, anaesthetists, pharmacists, patients, and patients’ relatives. Also, the guideline statements were discussed and finalised at a multidisciplinary consensus forum made up of 29 members. Consensus was achieved by employing procedures similar to a modified nominal group technique. Purposive sampling was employed. The guideline was made up of four dimensions described in a conceptual Radial Venn which emphasised inter-relationships among patient and family education, team work, monitoring and input by hospital leadership, and application of appropriate scientific recommendations for POP management. The effective collaboration with stakeholders resulted in the adoption of the clinical guideline by the Ghana Health Service for use within the Ghanaian health system. Ó 2015 The Authors. Published by Elsevier Ltd. This is an open access article under the CC BY-NC-ND license (http://creativecommons.org/licenses/by-nc-nd/4.0/). 1. Background Clinical guidelines are defined as statements that are developed systematically to help health care providers and patients make appropriate decisions about specific clinical issues (Hewitt-Taylor, 2004). The statements of a clinical guideline are based on the best available evidence relating to the specific aspect of care or procedure. The process of guideline development involves establishing the scope or parameters of the guideline. This forms the foundation of the clinical guideline, whereby specific limits of the guideline are clearly stated, such as the objective of the guideline, the target patient group and the specific procedure or patient care activity involved (Hewitt-Taylor, 2004; National Institute for Health and Clinical Excellence (NICE), 2014; Scottish Intercollegiate Guideline Network (SIGN), 2013; The Appraisal of Guidelines Research and Evaluation in Europe (AGREE) Collaboration, 2013). The development of a clinical guideline also involves identification of a multidisciplinary team or stakeholders to ensure that all relevant areas are incorporated. It is recommended that the team should have a balance of disciplines and that the membership should be kept at a manageable size to ensure effectiveness ⇑ Corresponding author. Tel.: +233 244719686. (Hewitt-Taylor, 2004; Keeley, 2003). Another hallmark of clinical guideline development is a systematic review of the evidence for which the clinical guideline is developed (National Institute for Health and Clinical Excellence (NICE), 2014). Thus, a systematic review was conducted as part of the doctoral study from which this paper was derived (Aziato, 2012) to ensure that guideline statements included evidence-based recommendations for POP management. Clinical practice guidelines may be procedure-based, unitbased, institution-based or for national use. (Haljamäe & Stomberg, 2003; Lindenfeld & Kelly, 2010; Rolley, Salamonson, Wensley, Dennison, & Davidson, 2011). Therefore, it is necessary for the limits of a particular clinical guideline to be well demarcated to avoid ambiguity and confusion regarding its use, as this could have negative repercussions Thus, the development of clinical guidelines follows standard processes stipulated by recognised bodies such as the National Institute for Clinical Excellence in the UK, the Scottish Intercollegiate Guidelines Network, and The Appraisal of Guidelines Research and Evaluation in Europe Collaboration. This study drew from these standard processes to develop a contextual clinical guideline for post-operative pain (POP) management in Ghana. Guideline development institutes most often develop guidelines for specific conditions and procedures at the national E-mail address: [email protected] (L. Aziato). http://dx.doi.org/10.1016/j.ijans.2015.03.001 2214-1391/Ó 2015 The Authors. Published by Elsevier Ltd. This is an open access article under the CC BY-NC-ND license (http://creativecommons.org/licenses/by-nc-nd/4.0/). L. Aziato, O. Adejumo / International Journal of Africa Nursing Sciences 2 (2015) 26–33 level, and therefore such guidelines have a wider spectrum (Hewitt-Taylor, 2004). However, this paper describes the development of a clinical guideline for a specific clinical issue (post-operative pain management on a surgical ward). On a surgical ward, there may be different guidelines for various procedures that guide the health professional to provide the best possible care. For example, there are guidelines for the administration of drugs such as opioids, for the nursing care of a patient receiving patient-controlled analgesia or epidural analgesia, and intravenous fluids (Rolley et al., 2011). Generally, such guidelines reflect current evidence-based standards and are reviewed periodically. However, within resource constrained countries, the authors were not aware of any clinical guideline for POP management at the time of the study. Many patients continue to experience moderate to severe postoperative pain globally and researchers over the years have devoted attention to many aspects of pain (Abdalrahim, Majali, & Bergbom, 2010; Qu, Sherwood, McNeill, & Zheng, 2008). Although pain is a personal phenomenon, patients respond to POP differently (Aziato & Adejumo, 2014c). Also, the socio-cultural background of the patient influences pain response (Lovering, 2006). In view of this, individual and contextual factors are to be incorporated in the planning and delivery of care. Therefore, the guideline developed for a resource-limited clinical context is necessary as it is suitable to address the uniqueness of such context. Lack of understanding of context factors could lead to inappropriate guideline statements. The inappropriate statements will result in difficulties in the use of the clinical guidelines (Ploeg, Davies, Edwards, Gifford, & Miller, 2007; Taba et al., 2012). In this study, a resource-limited clinical context is defined as a situation/scenario where there is limited staff education, equipment and non-use of methods such as patient controlled analgesia [PCA]). Thus, the scope and limits of the clinical guideline were derived from in-depth understanding of contextual factors that influenced post-operative pain management and a systematic review of the literature. For example, patients and nurses in Ghana do not have adequate knowledge on POP management due to inadequate education and training (Aziato & Adejumo 2014a; Aziato & Adejumo 2014b; Aziato & Adejumo 2014c; there are no advanced techniques for pain management such as PCA. Nurses fear patients will be addicted to opioids such as pethidine and hence do not administer adequate opioids (Aziato & Adejumo 2014a). There was also inadequate knowledge on pain management, team work, and supervision. Post-operative pain management is seen as inadequate in Ghana (Aziato & Adejumo, 2014a; Clegg-Lamptey & Hodasi, 2005). Incorporating systematic reviews in clinical guideline development is recommended by accredited guideline development agencies such as The Cochrane Collaboration, Scottish Intercollegiate Guideline Network (SIGN), National Institute for Health and Clinical Excellence (NICE), and The Appraisal of Guidelines Research and Evaluation in Europe (AGREE) Collaboration (Hewitt-Taylor, 2004). It is necessary to appraise included studies based on an established hierarchy of the evidence. The hierarchical order of the scientific evidence is systematic reviews and meta-analysis, randomized controlled trials (RCT), cohort studies, case-controlled studies, cross sectional surveys, case reports, expert opinion, and anecdotal evidence (Keeley, 2003). The method used for appraisal of the evidence is determined by the type of studies involved in a particular systematic review. This article provides a detailed account of a participatory process undertaken to develop a clinical guideline for POP management in Ghana. The participatory process employed ensured that relevant stakeholders were actively involved and their views incorporated in the clinical guideline developed. Participatory processes have been adopted by community-based projects and this 27 approach has been demonstrated to be effective (Kraemer Diaz, Spears Johnson, & Arcury, 2013; Ritchie et al., 2013). The approach has been employed successfully for promoting environmental health (Liu et al., 2011). The report is derived from a multi-stage doctoral study by the first author. 2. Methods The study was approved by the Ethics Committee at the University of the Western Cape (South Africa) and the Ghana Health Service Ethics Committee. Steps were taken to ensure anonymity and confidentiality of participants, through the use of identification codes. Participation was voluntary and individual informed consent was obtained by signing the informed consent form. The study was conducted in two hospitals in Accra, Ghana. A systematic review was attempted in January to April, 2012. The aim of the review was to answer the question: ‘What measures ensure effective POP management among adult general surgical patients in a resource limited environment?’ The review adopted an exploratory approach targeting both quantitative and qualitative literature with a comparable group or control group. Data sources searched included several online databases, books, and non-electronic journals. The selection of articles was done with focus on the study (intervention for POP management) and not the author, particular journal or the author affiliation. Both authors independently selected the relevant article to avoid selection bias. A critical independent review of the abstracts resulted in exclusion of eight (8) of the selected studies because findings were not applicable to the Ghanaian clinical setting (Arya, Abdollahi, Golalipour, Kazemnezhad, & Mohammadi, 2007; Bardiau, Taviaux, Albert, Boogaerts, & Stadler, 2003; Closs, Briggs, & Everitt, 1999; Good et al., 1999; Good et al., 2001; Roykulcharoen & Good, 2004; Seers, Crichton, Carroll, Richards, & Saunders, 2004; Wong, Chan, & Chair, 2010); and only one study included (Mac Lellan, 2004) based on a nurse-led intervention rather than the use of advanced pain management technique (Table 1). Subsequently, a focused review was undertaken as a remedial review to identify studies applicable to a resource-limited context. Identified studies emphasised effective leadership and team work, pre-emptive analgesia, regular around-the-clock analgesia, multimodal analgesia, and patient education (Table 2). The focused review was necessary because of paucity of evaluative research for pain management in resource-limited clinical environment. The studies identified were appraised for quality and applicability to resourcelimited clinical context and not the level of scientific evidence. The identification of studies during the focused review was based on an in-depth understanding of context factors (Aziato, 2012). Subsequently, two participatory approaches were adopted and included participant/expert review and the conduct of a consensus forum oriented towards a modified nominal group technique to achieve consensus (Jackson, Hettinga, Mead, & Mercer, 2009). A full understanding of the contextual factors influencing POP management in Ghana (Aziato & Adejumo, 2014a,b,c), a systematic review (Aziato, 2012), and a review of existing clinical guidelines on acute pain management in other countries such as the USA, Australia, New Zealand, Canada, UK and South Africa (American Society of Anaesthesiologists (ASA), 2012; Australian and New Zealand College of Anaesthetists (ANZCA), 2010; European Association of Urology, 2010; The British Pain Society, 2007; The South African Society of Anaesthesiologists (SASA), 2009), indicated that the existing guidelines could not be applied in a resource-limited clinical context as occurs in Ghana. The reason for this assertion is that the existing guidelines included statements for PCA and epidural techniques which were not available in resource-limited clinical context at the time of study. Thus, the authors developed initial 28 L. Aziato, O. Adejumo / International Journal of Africa Nursing Sciences 2 (2015) 26–33 Table 1 Included study. Author and year Objective (s) of study Design and sampling Participants (no./age) Setting Interventions Findings Conclusions Mac Lellan (2004) To introduce a nurse-led intervention to improve pain management after surgery and evaluate its effectiveness by measuring patients’ pain scores Experimental (pretest-post-test); conducted in three (3) phases. Sampling: Convenient sampling 800 male and female patients – 200 pre-intervention and 200 post-intervention in each hospital. Patients had different surgeries such as urological, gynaecologic, orthopaedic, and general surgery Two (2) teaching hospitals in Ireland; the 2 hospitals were studied prospectively Education for nurses in the form of short pain courses. Introduction of regular pain assessment. Profiling of pain at hospital level Pain score reduction in the order of 0.73 cm (7.3%) on a visual analog scale (VAS) 0 to 10 cm, was statistically significant for day of surgery and 2 days postop (q = 0.05) in the intervention hospital. A reduction was not seen in the control hospital Introduction of nurse-led intervention reduced patients’ pain scores guideline statements following an insight into the contextual factors and the systematic review of the literature. These statements were subjected to participant and expert review. Experts in this study were individuals with expert knowledge or experience (personal or clinical) in post-operative pain. Expert knowledge was recognised through publications on pain and clinical expertise involved at least 5 years post qualification clinical experience. 2.1. Participant/expert review According to Rycroft-Malone (2001), the processes for incorporating input from experts and participants should be clearly described by guideline developers. Thus, the authors sought a review of the initial draft guideline statements from external experts and experts in the two hospitals, as well as patients and patients’ relatives. Purposive sampling was used to recruit reviewers to ensure that all relevant reviewers were involved. The expert reviewers included nurses, doctors, anaesthetists, hospital leaders, patients’ relatives, patients, nurse educators and an international reviewer. The draft statements and summary of the contextual findings and literature review were disseminated through electronic mail (e-mail) and personal delivery. The heads of surgery (nursing and medical) at each hospital helped to identify ‘experts’ to review the statements. The summary of the contextual findings and literature review was to help reviewers relate the guideline statements to the ‘local’ context. A form was designed for feedback. The reviews were done in private and it focused on the structure, Table 2 Studies identified from ‘focused review’. Author (s)/year Aim Findings/conclusion Contemporary measure recommended Joshi, Rawal, Kehlet, and The PROSPECT collaboration (2011) Systematic review (SR) to evaluate the available literature on the management of pain after open hernia surgery Field block with or without wound infiltration, either as a sole anaesthetic/analgesic technique or as adjunct to general anaesthesia is recommended to reduce post-operative pain (POP) Pre-emptive analgesia reduces POP Fredericks et al. (2010) SR to examine who would most benefit from postop education, type or approach, and dose of education Delivery of postop patient education through the individualisation of content, use of combined media for delivery, provision of education on a one-on-one basis, and in multiple sessions is associated with improvement in educational or health outcomes Patient education improves health/ education outcomes such as better POP management Cummings et al. (2010) SR to examine the relationships between various styles of leadership outcomes for the nursing workforce and their work environment Leadership styles that focused on people and relationships (transformational, resonant, supportive, and consideration) were associated with nurse job satisfaction and leadership styles focused on task (dissonant, instrumental, and management by exception) were associated with lower nurse job satisfaction Emphasises effective leadership improves workforce Jirarattanaphochai and Jung (2008) SR to assess the efficacy and safety of nonsteroidal anti-inflammatory drugs (NSAIDS) in addition to analgesics on POP management in lumber surgery Meta-analysis provides evidence that the addition of NSAIDS to opioid analgesic in lumber surgery provided better pain control than opioid analgesics alone Combination or multimodal analgesic is better than single analgesic therapy Paice et al. (2005) Quality improvement study to determine the efficacy and safety of scheduled dosing of opioid analgesics among patients on the medical unit Scheduled doing was associated with decreased pain intensity ratings; there is no difference in adverse events between the scheduled and the PRN groups. Thus, scheduled dosing of opioids provides improved analgesia with no increased risk of adverse events among inpatient medical patients Scheduled dosing of opioids provides more stable plasma levels of the opioid administered rather than a PRN administration Meterko et al. (2004) Quantitative study to investigate the relationship between team work culture of hospitals and patients’ satisfaction with care received Team work culture for hospitals is positively associated with patients’ satisfaction. Thus, health care organisations should develop a culture that emphasises team work and limit aspects of bureaucracy that do not assure efficiency and quality care Highlights the relevance of team work in health care L. Aziato, O. Adejumo / International Journal of Africa Nursing Sciences 2 (2015) 26–33 content, format, and applicability of the guideline statements. Feedback was obtained within two weeks after administration by e-mail, telephone, and face-to-face interaction. The feedback was synthesised and incorporated in a revised version (Draft 2). The process drew from previous authors regarding clinical guideline development (National Institute for Health and Clinical Excellence (NICE), 2014; Rolls & Elliott, 2008; Scottish Intercollegiate Guideline Network (SIGN), 2013; The Appraisal of Guidelines Research and Evaluation in Europe (AGREE) Collaboration, 2013). The synthesis of the feedback resulted in the re-structuring of statements, modification of sentences, re-ordering of statements, and modification of headings. The reviewed clinical guideline (Draft 2) was then subjected to a multidisciplinary stakeholders’ consensus forum. 2.2. Consensus forum Formal consensus method involves a process of group decisionmaking that ensures that decisions made are representative of the group’s ideas or concerns. The process ensures that each member is given an opportunity to make a comment (Rolls & Elliott, 2008). The emphasis on group decisions in a consensus process is to enhance ‘ownership’ of research outcome. The context-appropriate consensus process adapted for this study was drawn from the work of previous researchers leaning towards a modified group technique (Fig. 1) (Berry, Davidson, Nicholson, Pasqualotto, & Rolls, 2011; Jackson et al., 2009; Nair, Aggarwal, & Khanna, 2011; Rolley et al., 2011; Rolls & Elliott, 2008). The authors liaised with the Director of the Institutional Care Division (ICD) of the Ghana Health Service (GHS) to identify all of the relevant stakeholders for the consensus forum. These included one representative each from the GHS, the West African College of Nursing, Ghana Anaesthetists’ Society, Ghana College of Physicians and Surgeons, Pharmacy Council, the Commission on Human Rights and Administrative Justice, and the WHO. Others were tutors from the Peri-Operative Nursing School, the Diploma General Nursing School, the Graduate Nursing Programme; Nurses, Surgeons, Pharmacists, Anaesthetists, Hospital leaders, and patients. The authors discussed the list of stakeholders to ensure that all relevant members were invited. On the day of the forum, only two stakeholders could not attend. Dra 1 Expert Review Final consensus statement Group modificaon Dra 2 Group Discussion Independent Decisions Modify/Maintain (Group level) - integrate, split, re-word, collapse, add a statement Maintain/Modify All Panel Discussion Fig. 1. Consensus forum process for development clinical guideline. 29 Letters of invitation signed by the Director General of the GHS at the time of study was sent to stakeholders and it was emphasised that appropriate individuals who could make meaningful contributions on the guideline should be nominated. The authors believed that the collaboration with the GHS was necessary to ensure adequate participation. Also, the nomination of individual stakeholder by individual organisations helped to minimise selection bias on the part of the authors. The attachments to the invitation letter were the reviewed guideline (Draft 2), a summary of the contextual findings, a summary literature review and a feedback form. These were dispatched to stakeholders at least two weeks before the day of the forum. The date, time and venue of the forum were decided in consultation with the hospital authorities, the Director (ICD), and heads of surgical departments of the two hospitals. A conference room was identified at the tertiary health facility to ensure proximity for most of the participants and enhance attendance. The authors identified a facilitator and two research assistants for the forum. The facilitator was an experienced researcher and was not directly affiliated with any of the stakeholders. The first author met with the facilitator and the two research assistants prior to the day of the forum to discuss and explain the formal consensus process and the roles of the facilitator and the research assistants, as well as a draft programme. One research assistant served as a recorder and a time-keeper and the other research assistant was at the registration desk and ensured that participants were comfortable. On the day of the forum, there was a brief opening ceremony after which the first author presented an overview of the study and highlighted the contextual findings and the findings from a systematic review that informed the draft clinical guideline. Also, a summary report of the participant/expert review on the initial draft was given. Thereafter, the research team assigned participants purposively to four groups guided by the four dimensions of the guideline as follows: (1) Patient and family require adequate information and education on POP management. (2) Effective team work is required between nurses, doctors and other health team members regarding POP management. (3) Input and monitoring from hospital management and departmental leadership is required to achieve effective pain management. (4) Evidence-based contemporary recommendations for POP management should be employed (Aziato, 2014). Assignment to groups was also according to the background of each participant and the ability to offer meaningful contributions. Each group discussed and reviewed statements as necessary. Inspite of the fact that participants had access to the guideline document two weeks in advance, the group discussion afforded them (especially those who could not read the guideline before the forum) an opportunity to review the statements. The facilitator ensured that groups were well-coordinated. After the group discussion, group leaders made presentations on statements. Some statements were rearranged and separated (adding 2 statements). Further comments on statements were invited from the larger group for discussion, review and adoption. Subsequently, when there were no further comments on the statements, the facilitator explained the decision process with an emphasis on independent individual decisions. Independent anonymous decisions (individual private decisions without names on decision forms) were taken on individual statements as follows: A = Agree (maintain statement); B = Modify statement; C = Abstain (will go by decision of others); D = Delete/remove statement. End- 30 L. Aziato, O. Adejumo / International Journal of Africa Nursing Sciences 2 (2015) 26–33 points of decisions such as ‘Abstain’ were included to allow flexibility in decisions, so that non-technical participants such as patients would not be forced to make a decision on a technical area. The independent or private decisions were adopted for the study based on the heterogeneous nature of the participants. The end-point decisions adopted were denoted A, B, C, and D to ensure ease of decision making. Decisions A (Agree) and C (Abstain) meant final end-points; and decisions B (modify statement) and D (delete) attracted further discussions and another round of decisions on those specific statements. Thus, after the first round of decisions, five statements were modified and second round decisions were taken. The independent and anonymous individual decisions ensured that participants made decisions without coercion or intimidation. No participant wrote a D; so no statement was deleted. The facilitator read the consensus statements of the guideline maintained. At the end of the consensus forum, two statements were added (Table 3 indicates the number of statements at each phase). 2.3. Findings – Outcome of the participatory process The participatory process culminated in a context appropriate clinical guideline for POP management for Ghana which has been adopted by the GHS. The clinical guideline developed had specific consensus statements that supported the four dimensions of the guideline (Table 4). The statements did not indicate the levels of evidence as pertains to other clinical guidelines because statements focused largely on the contextual evidence rather than the wider literature. Thus, for consistency and ease of use, the four statements derived from literature did not indicate levels of evidence. The four dimensions of the guideline were described with a framework that demonstrated the linkages and inter-relationships between the statements. It was realised that effective management of POP in a resource-limited clinical context depends on the use of all the statements within the four dimensions depicted in Fig. 1. The conceptual Radial Venn relates to the interconnectedness of the four dimensions of the guideline emphasising that none of the components should be ignored by pain management personnel. The diagram for the framework was adapted from designs of Microsoft Office 2010 called Radial Venn. The central concept of the Radial Venn is congruent with the concept of inter-relationship of the four dimensions of the clinical guideline developed. The Radial Venn is used for both overlapping relationships and their relationship to a central idea in a cycle. Hence, the diagram was appropriate for the framework of a POP management guideline. (See Fig. 2) Table 3 Number of guideline statements for the four guideline components. Number of statements Components Draft 1 Draft 2 Final Patient and family require adequate information and education on POP management Effective team work is required between nurses, doctors and other health team members regarding POP management Input and monitoring from hospital management and departmental leadership is required to achieve effective pain management Evidence-based contemporary recommendations for POP management should be employed 10 12 10 15 15 15 8 7 9 3 3 4 3. Discussion The statements supporting the four dimensions are simple and address specific context findings. For example patients lack knowledge on POP and are reluctant to ask health professionals questions on POP management (Aziato & Adejumo, 2014c). Therefore, statements on the patient domain give specific instructions and education on POP. Patient education has been confirmed to enhance POP management outcomes (Fredericks, Guruge, Sidani, & Wan, 2010). Also, ineffective team work has been reported from the context of the study (Aziato & Adejumo, 2014a) and statements on team work address all specific areas that could enhance effective team work. Team work that creates a positive environment could lead to improved pain management and improve patient satisfaction (Meterko, Mohr, & Young, 2004). Nurses report ineffective leadership and lack of monitoring which results in lapses in clinical practice such as inadequate analgesic administration (Aziato & Adejumo, 2014a). Adherence to specifications of statements of leadership could enhance work output and indirectly lead to effective pain management as supported by previous authors (Cummings et al., 2010). Nurses in Ghana do not administer regular analgesics post-operatively and analgesics are not administered pre-emptively (Aziato & Adejumo, 2014a). Clear specific statements on contemporary recommendations for POP such as regular administration of analgesic, using more than one form of analgesic for POP, and giving the drug before patient experiences pain have been found to improve POP management (Jirarattanaphochai & Jung, 2008; Joshi, Rawal, Kehlet, & The PROSPECT collaboration, 2011; Paice, Noskin, Vanagunas, & Shott, 2005). The authors reflect on the approach used for this study. It pre-supposes that researchers should develop appropriate ways of involving stakeholders as appropriate (Mason et al., 2013). The participatory process should be non-threatening to participants and respect the culture within which the study is undertaken. Other authors have demonstrated that groups where members feel threatened or do not respect each other’s opinions result in ineffective discussions and findings from such groups are biased or skewed (Wibowo & Deng, 2013). In this regard, researchers are admonished to understand the context and culture of the research setting so that groups will be constituted according to the cultural ethos of the setting (Liu et al., 2011). Participant commitment and understanding of the research process also enhances effective responses and participation. Timely and effective comments were received and this could mean that the participants had full understanding of the processes in this study. The effective cooperation or involvement of research participants in a given study has been noted to enhance the outcome of the study (Liu et al., 2011). The high response for the consensus forum could be because the GHS hosted the forum. Although the first author was actively involved in the planning of the forum, the GHS was recognised as the official host. However, the consensus forum was coordinated by the research team. Further, the specific consensus guideline statements were developed systematically following standard processes of guideline development (National Institute for Health and Clinical Excellence (NICE), 2014; Scottish Intercollegiate Guideline Network (SIGN), 2013; The Appraisal of Guidelines Research and Evaluation in Europe (AGREE) Collaboration, 2013; The Cochrane Collaboration, 2011). Thus, there was incorporation of an international pain consultant and all relevant stakeholders. Independent private decision ensured that guideline statements were not skewed in favour of a dominant group or individuals. A guideline for resource-limited clinical environment is of relevance to other similar context. It is realised that most African countries are deficient in terms of contemporary gadgets for post- 31 L. Aziato, O. Adejumo / International Journal of Africa Nursing Sciences 2 (2015) 26–33 Table 4 Guideline statements supporting four broad areas. Patient and family information and education 1. Pain is a personal and individual experience, and it is important to tell the nurses or doctors about the severity and duration of your pain to ensure the best treatment is given 2. Your nurses and doctors are committed to providing you with the safest and most effective post-operative pain management available. Do not think that reporting your pain is a bother to the nurses and doctors 3. Talk about your pain management with the nurses or doctors so that whatever concerns or questions you have about pain will be answered. Always report before your pain is severe, because severe pain can delay recovery and affect other aspects of your health 4. Ask the nurses or doctors what kind of pain medicine you will be given and how often you can take each of them so that you can help keep your pain under control by asking for the pain medicine on time. Also ask about the possible side-effects of your pain medicines 5. Remember that it is important to ask everything you can about your pain medicine because taking the right pain medicine in the right amount and in regular doses will help you feel more comfortable so that you can heal and recover faster 6. You may not be able to eat or drink right after surgery, so you may be given pain medicine in the form of an injection (needle) or inserted in the anus; but as your condition improves, your pain medicines may be given by mouth (swallowed) 7. It is important to take your pain medicine so that you can be comfortable enough to deep breathe, turn, and walk. Tell the nurses or doctors if you have a problem with pain medicine that is provided so that an alternative may be given 8. Ensure that if prescriptions for pain-medicines are given to you, the drugs are made available so that the nurses can give you at the right time. Pain after an operation is best treated with pain medicines 9. Family members who notice relations are in pain should report to the nurses or doctors and to do so before pain becomes severe 10. Do not allow anyone other than the nurses and doctors to give you any medicines while you are in the hospitalIf you require more information about post-operative pain management contact your nurses and doctors Team work 1. Unrelieved pain produces many adverse effects and can negatively impact patient outcomes. It is important that nurses and doctors work together to ensure that patients’ pain management needs are met so that patients can deep breathe, cough, turn, and walk safely after surgery 2. Pain is a subjective and individual experience, and the patient is the best judge of his or her own pain. Nurses and doctors should encourage patients to promptly report pain so that appropriate or individualised actions can be taken to relieve it 3. The doctor and other health personnel (as allowed by the institution) are responsible for prescribing appropriate analgesics in the patients’ folder, on the treatment chart, prescription form, or the National Health Insurance (NHI) medication form as necessary 4. Doctors and nurses share the responsibility for providing the patient and family with adequate information about how post-operative pain will be managed and to involve them in pain management decisions to enhance their co-operation 5. Doctors, clinical pharmacists and ward in-charges should follow-up on prescribed analgesics and ensure that the patient receives the prescribed dosage of analgesics. Deficits (missed-dose or under-dose) should be promptly investigated and corrected 6. Anaesthetist and clinical pharmacist should be actively involved in the management of patients’ pain 7. Although the patient’s report of pain is the gold standard of pain assessment, there may be non-verbal cues of pain (e.g., grimacing, bracing, moaning, and change in activity) that nurses and doctors may observe. These non-verbal pain cues should be looked out for and investigated and addressed 8. Opioid analgesics should never be withheld because of fear of addiction. The risk of addiction when opioids are taken for post-operative pain relief is extremely rare. If pain persists beyond expected duration and severity depending on the type of surgery, then it should be investigated 9. It is important to keep pain at the level that will allow patients to participate in recovery activities with relative ease. Waiting for patients to report severe pain is strongly discouraged; severe pain can be avoided by ensuring that all post-operative patients are given the right analgesic at the right time 10. Pain is often worse at night. A doctor should be available or easily accessible during the night to enhance effective pain management during this time. Nurses should ensure at all times that patients are given all their prescribed analgesics and patients are monitored for pain and the safety of the prescribed analgesics 11. Nurses should effectively document and inform the other team members about their patients’ pain reports and other pain management concerns raised by patients and their families to afford continuity of care 12. Nurses and other team members should regularly up-date their knowledge on pain management (e.g., pain assessment and analgesics) so that they will be more confident in their pain management activities. The team should also regularly evaluate their patient care objectives or goals 13. Uncontrolled pain requires immediate attention. Pain management protocol should be established to enhance patients’ pain management 14. If a patient refuses an analgesic by a particular route, an alternative route of administration should be prescribed and given so that the patient will not suffer unduly. Pain management education should be reinforced in such cases 15. Non-pharmacologic measures may be helpful and encouraged to supplement but not replace analgesic administration in the management of post-operative pain Leadership 1. Leadership should recognise that effective and safe post-operative pain management will improve patient outcomes. There should be pain management policies in all healthcare institutions. The necessary equipment should also be provided to enhance the management of post-operative pain 2. Leadership should be responsible for providing pain management education for the team (i.e. Doctors, nurses, pharmacists, physiotherapists, etc.) This is accomplished through organisation of initial and regular up-dates 3. Leadership should ensure that all policies are strictly adhered to and all violations sanctioned appropriately 4. Leadership should ensure regular audit/evaluation of pain management and dissemination of results to all concerned 5. Leadership should ensure regular departmental clinical meetings on pain management 6. Leadership should institute award schemes to deserving health teams/individuals in pain management 7. Leadership should ensure the proper storage and documentation of use of narcotic drugs in all units/departments 8. There should be hospital-based research committees to facilitate research at the hospitals. Findings from research should be implemented into practice, e.g., the use of a validated and reliable self-report pain assessment tool 9. Leadership should establish a complaints system and information/education unit in all Units/departments to encourage feedback from clients on pain management (continued on next page) 32 L. Aziato, O. Adejumo / International Journal of Africa Nursing Sciences 2 (2015) 26–33 Evidence-based recommendations 1. Pre-emptive analgesia (analgesic given before a painful stimulus) – the anaesthetist should ensure patient receives appropriate analgesic whiles in the operating theatre by the best recommended route such as rectal, intrathecal, or intravenous and should suggest the surgeon infiltrate the surgical site with appropriate analgesic or local anaesthetic 2. Multi-modal analgesia (using two or more forms of analgesic concurrently, e.g., non-opioid + opioid + local anaesthetic) is the recommended approach to the management of post-operative pain. Surgeons should ensure that different forms of analgesics are prescribed to enhance their synergistic effect. Pharmacists should supply the correctly prescribed medication and nurses should administer all of the analgesics as prescribed 3. Time-scheduled analgesic administration (giving the analgesics according to the time prescribed regularly) is recommended. Surgeons should prescribe the regular administration of analgesics, clinical pharmacists should ensure the availability of prescribed analgesics, and nurses should administer analgesic at regular intervals around-the-clock as prescribed 4. Non pharmacological methods of relieving pain such as early mobilisation, passive mobilisation, positioning, and other appropriate measures should be used as adjuncts to analgesic administration for post-operative pain management guidelines for different clinical setting such as emergency wards regarding pain management. Paent and family informaon and educaon Input and monitoring by Hospital and Departmental leadership Effecve POP Management 4. Conclusion Effecve teamwork among health professionals Evidence-based contemporary recommendaons of POP management The study employed a participatory approach for the development of a context appropriate clinical guideline for the management of POP. The authors realised that the effective collaboration of relevant stakeholders contributes to effective guideline development as stipulated by recognised guideline development bodies. Researchers should be conversant with their context and adapt appropriate measures to effectively involve relevant stakeholders. The conceptual framework for the clinical guideline emphasises the inter-relationship of the four dimensions as appropriate for POP management in a resource-limited clinical environment. Hence, it is highlighted that patient and family education, effective team work, monitoring by leadership, and the use of evidencebased recommendations for POP management are necessary to enhance POP management. Fig. 2. Framework for clinical guideline for post-operative pain management. Funding operative pain management such as PCA. An extensive literature review to explore the use of such gadgets in Africa identified the use of PCA in South Africa (Shipton, Beeton, & Minkowitz, 1993; Upton, Beeton, Minkowitz, & Shipton, 1992). It could pre-suppose that some pilot modern gadgets are being used in other countries but studies have not reported their use for POP management. Indeed, a systematic review conducted as part of the doctoral from which this paper was drawn confirmed paucity of evaluative research in post-operative pain management in resource limited environment (Aziato, 2012). Thus, most of the studies were explorative and reported the persistence of moderate to severe POP among post-operative patients (Clegg-Lamptey & Hodasi, 2005; Finnström & Söderhamn, 2006; Klopper, Andersson, Minkkinen, Ohlsson, & Sjöström, 2006; Ohene-Yeboah, 2006). The persistence of pain is a wake-up call for further research on POP within resource-limited clinical context. The study was supported by Centre of Teaching and Learning Scholarship (CENTALS) at the University of the Western Cape. Conflict of interest The authors report no conflict of interest in this study. Acknowledgements The authors are grateful to the GHS for hosting the consensus forum, Chris Pasero, Prof. Clegg-Lamptey, Prof. Slyvester Achio, for review of the guideline, and all the experts who contributed in the development of the clinical guideline for POP management in Ghana. References 3.1. Limitations of the study Although this study did not develop a clinical guideline with a wide spectrum of applicability, it is possible to apply the clinical guideline developed and conceptualised with a framework of a Radial Venn in resource-limited clinical contexts. The active involvement of the GHS could have covertly influenced some participants during the consensus forum. However, it is reiterated that the GHS did not coordinate the forum. The guideline in this study was developed for patients who can self-report post-operative pain. Future studies could develop guidelines for other types of pain and for patients with limitations regarding self-report of pain. Also, future studies could develop Abdalrahim, M. S., Majali, S. A., & Bergbom, I. (2010). Jordanian surgical nurses’ experiences in caring for patients with postoperative pain. Applied Nursing Research, 23(3), 164–170. American Society of Anaesthesiologists (ASA) (2012). Practice guidelines for acute pain management in the perioperative setting: An updated report by the American Society of Anaesthesiologists Task Force on Acute Pain Management. Anaesthesiology, 116 (2 P 248–73). Arya, B., Abdollahi, A.-A., Golalipour, M.-J., Kazemnezhad, K., & Mohammadi, M. R. (2007). Evaluation of post-operative analgesic efficacy of intramuscular pethidine, compared to indometacin and diclofenac Na suppositories in unilateral inguinal hernioplasty patients. Journal of Medical Sciences, 7(2), 311–314. Australian and New Zealand College of Anaesthetists (ANZCA) (2010). Acute Pain Management: Scientific Evidence. Retrieved from <http://sydney.edu.au/ medicine/pmri/pdf/Acute-pain-management-scientific-evidence-third-edition. pdf>. L. Aziato, O. Adejumo / International Journal of Africa Nursing Sciences 2 (2015) 26–33 Aziato, L. (2012). Development of clinical guidelines for the management of post-operative pain within the medico-socio-cultural context of Ghana (Ph.D. thesis). South Africa: University of the Western Cape. Aziato, L., & Adejumo, O. (2014a). The Ghanaian surgical nurse and postoperative pain management: A clinical ethnographic insight. Pain Management Nursing, 15(1), 265–272. Aziato, L., & Adejumo, O. (2014b). Determinants of nurses’ knowledge gap on pain management in Ghana. Nurse Education in Practice, 14(2), 195–199. Aziato, L., & Adejumo, O. (2014c). An ethnographic exploration of postoperative pain experiences among Ghanaian surgical patients. Journal of Transcultural Nursing. http://dx.doi.org/10.1177/1043659614526246. Aziato, L. (2014). The concept of pain and trends in post-operative pain management: Implications for nursing practice in Ghana. In L. Aziato, A. Kwashie, K. A. Korsah, & F. Naab (Eds.), Footprints of the nursing profession: Current trends and emerging issues in Ghana (pp. 56–74). Accra: Sub-Saharan Publishers. Bardiau, F. M., Taviaux, N. F., Albert, A., Boogaerts, J. G., & Stadler, M. (2003). An intervention study to enhance postoperative pain management. Anaesthesia and Analgesia, 96, 179–185. Berry, A. M., Davidson, P. M., Nicholson, L., Pasqualotto, C., & Rolls, K. (2011). Consensus based clinical guideline for oral hygiene in the critically ill. Intensive and Critical Care Nursing, 27(4), 180–185. Clegg-Lamptey, J. N. A., & Hodasi, W. M. (2005). An audit of aspects of informed consent and pain relief in general surgical units of Korle-Bu Teaching Hospital. Ghana Medical Journal, 39(2), 63–67. Closs, S. J., Briggs, M., & Everitt, V. E. (1999). Implementation of research findings to reduce postoperative pain at night. International Journal of Nursing Studies, 36(1), 21–31. Cummings, G. G., MacGregor, T., Davey, M., Lee, H., Wong, C. A., Lo, E., et al. (2010). Leadership styles and outcome patterns for the nursing workforce and work environment: A systematic review. International Journal of Nursing Studies, 47(3), 363–385. European Association of Urology (2010). Guidelines on Pain Management. Retrieved from <http://www.uroweb.org/gls/pdf/Pain%20Management%202010.pdf>. Finnström, B., & Söderhamn, O. (2006). Conceptions of pain among Somali women. Journal of Advanced Nursing, 54(4), 418–425. Fredericks, S., Guruge, S., Sidani, S., & Wan, T. (2010). Postoperative patient education: A systematic review. Clinical Nursing Research, 19(2), 144–164. Good, M., Stanton-Hicks, M., Grass, J. A., Anderson, G. C., Lai, H.-L., Roykulcharoen, V., et al. (2001). Relaxation and music to reduce postsurgical pain. Journal of Advanced Nursing, 33(2), 208–215. Good, M., Stanton-Hicks, M., Grass, J. A., Cranston Anderson, G., Choi, C., Schoolmeesters, L. J., et al. (1999). Relief of postoperative pain with jaw relaxation, music and their combination. Pain, 81(1–2), 163–172. Haljamäe, H., & Stomberg, M. W. (2003). Postoperative pain management – Practice guidelines. Current Anaesthesia & Critical Care, 14, 203–206. Hewitt-Taylor, J. (2004). Clinical guidelines and care protocols. Intensive and Critical Care Nursing, 20(1), 45–52. Jackson, A., Hettinga, D. M., Mead, J., & Mercer, C. (2009). Using consensus methods in developing clinical guidelines for exercise in managing persistent low back pain. Physiotherapy, 95(4), 302–311. Jirarattanaphochai, K., & Jung, S. (2008). Nonsteroidal anti-inflammatory drugs for postoperative pain management after lumbar spine surgery: A metaanalysis of randomized controlled trials. Journal of Neurosurgery: Spine, 9, 22–31. Joshi, G. P., Rawal, N., Kehlet, H., & The PROSPECT collaboration (2011). Evidencebased management of postoperative pain in adults undergoing open inguinal hernia surgery. British Journal of Surgery, 99(2), 168–185. Keeley, P. W. (2003). Clinical guidelines. Palliative Medicine, 17, 368–374. Klopper, H., Andersson, H., Minkkinen, M., Ohlsson, C., & Sjöström, B. (2006). Strategies in assessing post-operative pain – A South African Study. Intensive and Critical Care Nursing, 22, 12–21. Kraemer Diaz, A. E., Spears Johnson, C. R., & Arcury, T. A. (2013). Variation in the interpretation of scientific integrity in community-based participatory health research. Social Science & Medicine, 97, 134–142. Lindenfeld, J., & Kelly, P. A. (2010). Developing a cardiology–oncology clinical practice guideline. Progress in Cardiovascular Diseases, 53(2), 173–179. Liu, J., McCauley, L., Leung, P., Wang, B., Needleman, H., & Pinto-Martin, J. (2011). Community-based participatory research (CBPR) approach to study children’s health in China: Experiences and reflections. International Journal of Nursing Studies, 48(7), 904–913. Lovering, S. (2006). Cultural attitudes and beliefs about pain. Journal of Transcultural Nursing, 17(4), 389–395. 33 Mac Lellan, K. (2004). Postoperative pain: Strategy for improving patient experiences. Journal of Advanced Nursing, 46(2), 179–185. Mason, M. J., Tanner, J. F., Piacentini, M., Freeman, D., Anastasia, T., Batat, W., et al. (2013). Advancing a participatory approach for youth risk behavior: Foundations, distinctions, and research directions. Journal of Business Research, 66(8), 1235–1241. Meterko, M., Mohr, D. C., & Young, G. J. (2004). Teamwork culture and patient satisfaction in hospitals. Medical Care, 42(5), 492–498. Nair, R., Aggarwal, R., & Khanna, D. (2011). Methods of formal consensus in classification/diagnostic criteria and guideline development. Seminars in Arthritis and Rheumatism, 41(2), 95–105. National Institute for Health and Clinical Excellence (NICE) (2014). Developing NICE clinical guidelines. Journal. Retrieved from <http://www.nice.org.uk/>. Ohene-Yeboah, M. (2006). Acute surgical admissions for abdominal pain in adults in Kumasi, Ghana. ANZ Journal of Surgery, 76(10). Paice, J. A., Noskin, G. A., Vanagunas, A., & Shott, S. (2005). Efficacy and safety of scheduled dosing of opioid analgesics: A quality improvement study. The Journal of Pain, 6(10), 639–643. Ploeg, J., Davies, B., Edwards, N., Gifford, W., & Miller, P. E. (2007). Factors influencing best-practice guideline implementation: Lessons learned from administrators, nursing staff, and project leaders. Worldviews on Evidence Based Nursing, 4(4), 210–219. Qu, S., Sherwood, G. D., McNeill, J. A., & Zheng, L. (2008). Postoperative pain management outcome in Chinese inpatients. Western Journal of Nursing Research, 30(8), 975–990. Ritchie, S. D., Jo Wabano, M., Beardy, J., Curran, J., Orkin, A., VanderBurgh, D., et al. (2013). Community-based participatory research with Indigenous communities: The proximity paradox. Health & Place, 24, 183–189. Rolley, J. X., Salamonson, Y., Wensley, C., Dennison, C. R., & Davidson, P. M. (2011). Nursing clinical practice guidelines to improve care for people undergoing percutaneous coronary interventions. Australian Critical Care, 24(1), 18–38. Rolls, K. D., & Elliott, D. (2008). Using consensus methods to develop clinical practice guidelines for intensive care: The Intensive Care Collaborative project. Australian Critical Care, 21(4), 200–215. Roykulcharoen, V., & Good, M. (2004). Systematic relaxation to relieve postoperative pain. Journal of Advanced Nursing, 48(2), 140–148. Rycroft-Malone, J. (2001). Formal consensus: The development of a national clinical guideline. Quality in Health Care, 10, 238–244. Scottish Intercollegiate Guideline Network (SIGN) (2013). SIGN 50: A Guideline for Developer’s Handbook. Retrieved from http://sign.ac.uk/guidelines/fulltext/50/ index.html. Seers, K., Crichton, N., Carroll, D., Richards, S., & Saunders, T. (2004). Evidence-based postoperative pain management in nursing: Is a randomized-controlled trial the most appropriate design? Journal of Nursing Management, 12(3), 183–193. Shipton, E. A., Beeton, A. G., & Minkowitz, H. S. (1993). Introducing a patientcontrolled analgesia-based acute pain relief service into southern Africa–the first 10 months. South African Medical Journal = Suid-Afrikaanse Tydskrif Vir Geneeskunde, 83(7), 501–505. Taba, P., Rosenthal, M., Habicht, J., Tarien, H., Mathiesen, M., Hill, S., et al. (2012). Barriers and facilitators to the implementation of clinical practice guidelines: A cross-sectional survey among physicians in Estonia. BMC Health Services Research, 12(455), 1–7. The Appraisal of Guidelines Research and Evaluation in Europe (AGREE) Collaboration (2013). Electronic Library for Guideline Developers. Journal. Retrieved from <http://www.agreecollaboration.org>. The British Pain Society (2007). Recommended guidelines for Pain Management Programmes for adults: A consensus statement prepared on behalf of the British Pain Society. Retrieved from <http://www.anaesthesiauk.com/documents/pmp_ 0306_v9.pdf>. The Cochrane Collaboration (2011). Cochrane Handbook for Systematic Reviews of Interventions. Retrieved from The Cochrane Collaboration <http:// www.cochrane-handbook.org/>. The South African Society of Anaesthesiologists (SASA) (2009). South African acute pain guidelines. Retrieved from <http://www.sasaweb.com/content/images/ SASA_Pain_Guidelines.pdf>. Upton, P. M., Beeton, A. G., Minkowitz, H. S., & Shipton, E. A. (1992). Patientcontrolled analgesia. Its South African debut in a provincial hospital. South African Medical Journal = Suid-Afrikaanse Tydskrif Vir Geneeskunde, 81(2), 74–76. Wibowo, S., & Deng, H. (2013). Consensus-based decision support for multicriteria group decision making. Computers & Industrial Engineering, 66(4), 625–633. Wong, E. M.-L., Chan, S. W.-C., & Chair, S.-Y. (2010). The effect of educational intervention on pain beliefs and postoperative pain relief among Chinese patients with fractured limbs. Journal of Clinical Nursing, 19(17/18), 2652–2655.






© Copyright 2026