
polaschek-2014
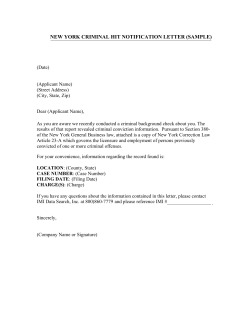
535211 research-article2014 CDPXXX10.1177/0963721414535211PolaschekCriminals With Psychopathy Adult Criminals With Psychopathy: Common Beliefs About Treatability and Change Have Little Empirical Support Current Directions in Psychological Science 2014, Vol. 23(4) 296–301 © The Author(s) 2014 Reprints and permissions: sagepub.com/journalsPermissions.nav DOI: 10.1177/0963721414535211 cdps.sagepub.com Devon L. L. Polaschek Victoria University of Wellington Abstract Criminals with psychopathy have historically been thought to be resistant to change and unresponsive to psychological treatment. But despite vast amounts of empirical research on psychopathy, very little of it has investigated treatment or change. In this article, I review a small and recent scientific research literature suggesting that (a) psychopathic characteristics, especially those most related to criminal offending, can change over the life course; (b) although adult criminals with psychopathy are among the hardest to work with in treatment, treatment causes them—like other offenders—to reoffend less; and (c) there is no good evidence that criminals with psychopathy take advantage of treatment services to wreak havoc on therapists or the community. Taken together, these findings suggest that like other high-risk criminals, those with psychopathy can benefit from psychological treatment. Keywords criminal psychopathy, psychological treatment, treatability, PCL-R Imagine this: You are a member of a parole board. In front of you stands a man who has been imprisoned for 12 years for attempted murder. His psychologist’s report says he is a psychopath. But the man himself declares that he has changed—he has been rehabilitated. It is your job to decide whether he is safe to be released. You have heard that psychopaths are consummate manipulators and cannot change who they are. Or can they? Answering this question is the purpose of this article. Psychopaths—or, more correctly, people with psychopathy—have a personality disorder. They can be grandiose, fearless, superficially charming, callous, irresponsible, manipulative, impulsive, emotionally shallow, hot headed, cold hearted, and stress resilient. Intuitively, they must be challenging to treat and resistant to change: At best, they sound unpleasant and difficult to work with; at worst, as if they could easily get the better of a hapless therapist. Although people with psychopathy can be found throughout society, the ones who strike fear among ordinary people are not the Fortune 500 CEOs but the sometimes violent, mostly male, habitual criminals. In this article, I focus on these men, addressing three common misconceptions: (a) that criminal psychopaths cannot change who and what they are, (b) that treatment does not reduce their potential for crime, and (c), worse still, that they misuse treatment for antisocial ends. Before tackling these misconceptions, it is important to establish how psychopathy is diagnosed. Because accurate diagnosis is a prerequisite for any research on mental disorders, we might consider turning to the fifth edition of the Diagnostic and Statistical Manual of Mental Disorders (DSM-5; American Psychiatric Association, 2013) for assistance. But psychopathy was omitted from the DSM-III (American Psychiatric Association, 1980), and this trend has continued to the present day.1 Consequently, an alternative diagnostic tradition has developed based on a widely accepted and psychometrically validated tool, the Psychopathy Checklist–Revised (PCL-R; Hare, 2003). The PCL-R was originally designed with two correlated factors—interpersonal-affective and antisocial— that were later divided again into two facets each. As Figure 1 shows, the four resulting components describe Corresponding Author: Devon L. L. Polaschek, School of Psychology, Victoria University of Wellington, P.O. Box 600, Wellington 6140, New Zealand E-mail: [email protected] Downloaded from cdp.sagepub.com by guest on March 19, 2015 Criminals With Psychopathy 297 Psychopathy Checklist–Revised (PCL-R) 100 Factor 1: Interpersonal-Affective Scale 80 Recidivism (%) Facet 1: Interpersonal Facet 2: Affective Factor 2: Antisocial Scale Facet 3: Lifestyle Facet 4: Antisocial Psychopathic Personality Inventory–Revised (PPI-R) PPI-I: Fearless Dominance 60 56.7 48 40 34.5 23.1 20 0 Low PPI-II: Self-Centered Impulsivity ModerateLow ModerateHigh High Change Fig. 1 Factor structure of two psychopathy measures: the Psychopathy Checklist–Revised (Hare, 2003) and the Psychopathic Personality Inventory–Revised (Lilienfeld & Widows, 2005). interpersonal, affective, lifestyle, and antisocial aspects of psychopathy (Hare, 2003). Although PCL-psychopathy is a dimensional construct, cutoff scores (e.g., 30 or more out of 40; Hare, 2003) are often used to make a dichotomous diagnosis. Conveniently for this article, the PCL-R was developed specifically for use with adult criminals. Scores on the PCL-R rely heavily on past criminal behavior, and as it turns out, those scores—especially on the combined antisocial scale—moderately predict future criminal and violent behavior. But there are alternatives. For example, a more recent instrument that does not require a history of criminal behavior for completion is a self-report questionnaire known as the Psychopathic Personality Inventory–Revised (PPI-R; Lilienfeld & Widows, 2005). It also has two major factors, known as PPI-I (fearless dominance) and PPI-II (impulsive antisociality; see Fig. 1). A second important preliminary issue is to establish whether “ordinary” adult criminals—those with little or no psychopathy—are leopards who can change their spots. After all, if these “ordinary” criminals cannot change, how could their psychopathic counterparts be expected to improve? Many people seem unaware that psychological treatments can help rehabilitate a wide variety of criminals, including the most persistently antisocial. In fact, a substantial body of research over the last 20 years has shown that when criminals take part in certain treatment programs, they are less likely to be reconvicted—the proxy for reoffending—than similar criminals who do not take part. The most effective programs have four important characteristics. They (a) provide services only where they can have the most impact: to those most likely to reoffend; (b) base the goals of treatment on the Fig. 2. Violent-crime recidivism rates in a 3-year fixed follow-up among criminals in a treatment program as a function of level of therapeutic change. Adapted from “The Violence Risk Scale: Predictive Validity and Linking Changes in Risk With Violent Recidivism in a Sample of HighRisk Offenders With Psychopathic Traits,” by K. Lewis, M. E. Olver, and S. C. P. Wong, 2013, Assessment, 20, p. 157. Copyright 2013 by Sage. Adapted with permission. changeable correlates of reoffending, such as a criminal’s relationships with criminal peers, “pro-crime” attitudes and beliefs, and misuse of alcohol and drugs; (c) use methods with good empirical support to help criminals change (e.g., modeling of desired behavior, positive reinforcement for change); and (d) monitor therapists and programs carefully to minimize drift away from these core principles (Andrews & Bonta, 2010). Most of these treatments are based on cognitive behavioral therapy approaches and take place in groups: in prisons, hospitals, or juvenile secure institutions, and in the community (e.g., Polaschek & Kilgour, 2013). How do we know if these treatments work? At a time interval after men who complete programs have been released into the community, they are compared with a like sample of untreated released men. One can determine if there is a treatment effect by examining whether the proportion with new convictions is significantly lower for treated criminals than for untreated criminals. In a meta-analysis of 374 studies, the (weighted) mean of this difference was about 0.12 (Andrews & Bonta, 2010), a small but important effect2—especially compared to the effect of imprisonment on reconviction, which at best is approximately 0.00 (Cullen, Jonson, & Nagin, 2011). Of course, examining what happens to criminals months or years later is an indirect method for judging the effectiveness of an intervention. A more direct method is to measure how men change (or do not Downloaded from cdp.sagepub.com by guest on March 19, 2015 Polaschek 298 change) on the factors above between the start and the end of a treatment program. As we would hope, research adopting this approach has shown that significantly fewer of those who change the most are reconvicted (e.g., Lewis, Olver, & Wong, 2013; see Fig. 2). In short, there is little evidence that criminals really are the leopards of the clinical kingdom. Instead, these “ordinary” criminals can benefit from certain psychological- treatment programs, and in fact, these types of programs are among the few interventions that do anything to counteract the ineffectiveness of punitive criminal-justice sanctions (Andrews & Bonta, 2010). We are now on solid footing to evaluate the extent to which psychopaths are capable of change and whether psychological treatments can help criminal psychopaths to become less criminal, and perhaps even less psychopathic. Is Psychopathy Mutable? The only constant in life is change, according to the preSocratic Greek philosopher Heraclitus. Even our personalities—which we may think of as particularly resistant to environmental influences—change modestly during the course of normal development and aging (e.g., Ferguson, 2010). Many people believe that psychopaths cannot change, though there is almost no research addressing this issue. One widely cited study of psychopathic criminals suggested that some aspects change while others do not (Harpur & Hare, 1994). In this study, although the interpersonal and affective aspects of psychopathy were unrelated to age, the lifestyle and antisocial aspects were less prominent in older than in younger criminals. But this study was not longitudinal—that is, the same men were not examined at different ages—so these results may have simply reflected generational differences rather than change over the life span. Nonetheless, a recent longitudinal study of men measured at age 17 and then again at age 24 with a different measure of psychopathy (the PPI-R; see Fig. 1) showed a similar overall pattern, although change was also seen in affective and interpersonal qualities in some (Blonigen, Hicks, Krueger, Patrick, & Iacono, 2006). Taken together, these studies suggest that psychopathy does attenuate, although the most distinctive personality characteristics—the affective and interpersonal qualities—may be more resistant to spontaneous change than the lifestylerelated aspects. Of course, clinical scientists aim to do better than simply waiting around for psychopaths to “grow out of it.” I have already described how psychological treatments can help rehabilitate more ordinary criminals, but can psychological treatments help rehabilitate psychopathic criminals? Can Treatment Make Criminal Psychopaths Less Criminal? Prominent experts on psychopathy are among those who have taken the view that no effective treatments are available for psychopaths (Cleckley, 1988; Hare, 2003; Harris & Rice, 2007). But at least three studies with criminal samples have examined whether psychopathy is related to outcomes in programs designed to reduce recidivism, with incarcerated youths (Caldwell, Skeem, Salekin, & van Rybroek, 2006), with community psychiatric patients (Skeem, Monahan, & Mulvey, 2002) and with prisoners (Olver, Lewis, & Wong, 2013). The first two studies showed that treated people were significantly less likely to be reconvicted than similar untreated criminals, regardless of the severity of their psychopathy. A caveat: Both of these studies used quasi-experimental designs. That is, rather than randomly assigning cases to treatment or not, researchers statistically matched treated and untreated people retrospectively on key criteria that are themselves predictors of reconviction (e.g., age). But although prospective experimental designs offer more rigor than quasi-experimental designs, they are difficult to conduct in these settings, and other research on criminals has found surprisingly little difference between the two designs in patterns of effects (see Hollin, 2008). A third study showed significant treatment change with adult psychopathic male prisoners, demonstrating that those who made more change were less likely to be reconvicted for violence (Olver et al., 2013). However, the authors rated treatment change and psychopathy retrospectively from file notes, no specific data were reported on rater reliability, and there was no comparison group. Considered together, and with these caveats, these three studies lead to the conclusion that psychopathy per se may have no bearing on the success of treatment designed to reduce a criminal’s risk of committing new crimes. Treated psychopaths avoid reconviction about as often as other similar criminals and more often than their untreated counterparts; they do indeed change, and the amount of change they make inversely predicts whether they will be reconvicted. Although at first glance these findings seem like good news, they raise another concern. Perhaps in treatment, while other criminals avoid reconviction by learning helpful prosocial skills, psychopaths achieve their success by more nefarious means, instead teaching themselves how to mislead people more skillfully, lie to parole boards, get released under false pretenses, and then evade apprehension. Although no research has targeted this question directly, we can partially address the concern by turning to what we know about how criminals— including those with psychopathy—use treatment to reduce their risk of new convictions. At the heart of this Downloaded from cdp.sagepub.com by guest on March 19, 2015 Criminals With Psychopathy 299 research is the Violence Risk Scale (VRS; Wong & Gordon, 2000); in using it, a therapist identifies a criminal’s pretreatment risk factors: impulsivity, contact with criminal peers, lack of community support, and so on. The criminal’s goal in treatment is to improve on those factors. At the end of the program, therapists again complete the VRS to measure the criminal’s progress. If all goes well, the result is an empirically measured amount of positive change unique to each criminal. The difference between post-treatment and pre-treatment scores represents (hopefully) the amount of reduction in risk associated with undertaking treatment. Research with the VRS suggests that the more psychopaths change on these important treatment goals, the less likely they are to be convicted for new violent and sexual crimes—exactly the same effect we would expect for nonpsychopaths in treatment (Olver et al., 2013; Wong, Gordon, Gu, Lewis, & Olver, 2012). On the face of it, then, we might conclude that psychopaths tend to respond to the treatments the way other highly risky criminals do and make the same kinds of changes on the same factors. But these findings are only part of the story. To complete the picture, we might also consider whether psychopaths are harder to work with than other criminals and less likely to make it through to the end of treatment. Indisputably, men with high PCL-R scores have difficult personal characteristics that can make treatment challenging. They are evasive, argumentative, hostile, resistant to change, less committed and compliant, and less likely to finish treatment—whether because they leave prematurely or because therapists terminate their treatment early (Polaschek & Daly, 2013). Naturally, therapists notice their difficult behavior, rating such clients as less motivated and less malleable (e.g., Hobson, Shine, & Roberts, 2000). But studies of other highrisk offenders—identified using tools unrelated to —have revealed that many of them also psychopathy behave badly. So, rather than concluding that psychopathy leads to difficult behavior in therapy, it may simply be that high-risk criminals in general behave that way. These high-risk criminals are in turn the highest priority for treatment, so dealing with poor behavior may just be part of the fabric of working therapeutically with these criminals, psychopathic or not. Is There a Risk That Psychopaths Will Use Treatment for Antisocial Ends? Perhaps the evidence thus far has been intriguing, raising the possibility that good psychological treatment programs can help both ordinary criminals and psychopathic criminals. But are psychopaths not consummate liars who charm and manipulate others? If so, then surely they can manipulate therapists, using treatment as a means of learning new ways to wreak havoc with ordinary people. Therapists and others have shared these concerns (Harris & Rice, 2007). Indeed, anxiety about psychopathic nefariousness blossomed from the results of the infamous Canadian “Oak Ridge study” (Harris, Rice, & Cormier, 1994), whose investigators used the PCL-R retrospectively to examine the outcomes of a radically innovative 1960s hospital program. By modern standards, this treatment program— involuntarily attended by mentally disordered Canadians, including people with psychopathy—would be considered unethical and probably harmful. Much of the time, patients mingled freely, with little staff oversight. They were sometimes forced to spend days together naked in “encounter bubbles” with wall-mounted feeding tubes. Patients received various psychoactive substances— including alcohol, methedrine, and LSD—to help break through psychic defenses. The researchers examined the criminal records of those people who had been released from the program, comparing the proportion who had new convictions with that of a group of untreated prisoners whose PCL-R scores were equivalent. A much greater percentage of psychopathic patients were convicted of new violent crimes compared with psychopathic prisoners: 78% versus 55%. This pattern was seen only in convictions for violent crimes, and only for psychopaths; convictions for nonviolent crime did not differ between the two groups, and among those who had been convicted, patients and prisoners with low PCL-R scores did not differ from each other on either type of new crime (Rice, Harris, & Cormier, 1992). Does the pattern of apparently increased post-treatment violence fit with the idea that psychopaths had learned in treatment how to better manipulate and exploit people? Rice et al. (1992) proposed this explanation. But although no published evidence supports or refutes it, the explanation seems unlikely for two reasons. First, if these psychopaths had developed excellent skills in manipulating others, they should have been less prone to adopt a crude method of manipulation such as violence in favor of something more sophisticated. They should also have been more capable of avoiding both capture and conviction. After all, fewer than 10% of violent offences ever result in conviction, so there is plenty of scope for avoiding detection (Farrington, 2007). But that is not what the Oak Ridge researchers found. Instead, they found that psychopaths were more likely to have been convicted for violence. Second, there is a more plausible alternative possibility: The Oak Ridge program’s regime of punishment increased psychopaths’ propensity for violence. In fact, other Oak Ridge data fit with this possibility: Regardless of whether patients were psychopathic, time Downloaded from cdp.sagepub.com by guest on March 19, 2015 Polaschek 300 spent being punished for “noncompliant behavior” in treatment was correlated with later convictions for violent crimes. Unsurprisingly, psychopaths were more difficult patients; they were punished more, spent more time locked in bare cells on their own, and received more potentially harmful drugs (Rice et al., 1992). Remember, patients could not leave this program of their own accord; their experiences may simply have made them more angry and hostile—potential risk factors for new violence. Thankfully, the Oak Ridge treatment program is a far cry from programs of today. Its results have sometimes been used to deny psychopaths treatment on the grounds that trying to treat them risks more harm than good. But although people fear that psychopaths’ personal characteristics may enable them to use what they learn in treatment to better exploit others, there is no compelling evidence for this concern. Conclusions Psychopaths have sometimes been excluded from criminal-justice interventions because of beliefs about psychopathy’s immutability and their untreatability. A small and recent research literature suggests that populist ideas about psychopaths and their treatability largely lack substance—findings that should open the way for a revitalization of research on psychopathy, treatment, and change. This revitalization is sorely needed. The research reported in this article primarily limited the notion of psychopathy to “what the PCL-R measures,” reflecting the dominance of the PCL-R as both a measurement tool and a model of psychopathy in criminal populations. A much more interesting future for treatment research lies in breaking away from this tradition, which hides the surprising degree of disagreement and confusion within the scientific community about what psychopathy is, and is not. Just as important, it is not yet clear whether treatments that reduce the risk of criminal behavior in those with and without psychopathy have any effect on psychopathic characteristics themselves: Does treatment improve behavior but leave core interpersonal and affective features largely intact? Finally, research on children and adolescents has been excluded from this article, but the indications from that field are that (a) the diagnosis of psychopathy is even more controversial in children (Salekin & Lynam, 2010) and (b) early findings hold promise that the key personality traits—particularly callous-unemotional traits—may respond to treatment (Hawes & Dadds, 2007). An integration of research across the life span is needed to inform diagnosis, treatment design, and interventions if we are to further unravel the intriguing complexity of psychopathy. Recommended Reading Andrews, D. A., & Bonta, J. (2010). (See References). An empirically grounded approach to the assessment and effective treatment of criminals, in use in most Western nations. D’Silva, K., Duggan, C., & McCarthy, L. (2004). Does treatment really make psychopaths worse? A review of the evidence. Journal of Personality Disorders, 18, 163–177. A review of the treatment-response literature for psychopaths. Harris, G. T., & Rice, M. E. (2007). (See References). An overview of the historically important Oak Ridge program that argues for therapeutic pessimism regarding the treatment of psychopaths. Olver, M. E., Lewis, K., & Wong, S. C. P. (2013). (See References). A recent empirical article linking therapeutic changes by psychopathic violent offenders to reductions in violent reconvictions. Patrick, C. J. (Ed.). (2006). Handbook of psychopathy. New York: Guilford. A comprehensive reference source on psychopathy, mainly pertaining to adults. Polaschek, D. L. L., & Daly, T. (2013). (See References). A more detailed review of the issues traversed in this article. Salekin, R. T., & Lynam, D. R. (Eds.). (2010). (See References). A comprehensive source for theory and research on psychopathy prior to adulthood Salekin, R. T., Worley, C., & Grimes, R. D. (2010). Treatment of psychopathy: A review and brief introduction to the mental model approach for psychopathy. Behavioral Sciences and the Law, 28, 235–266. A review of historical context and recent studies of treatment in both youths and adults. Skeem, J. L., Polaschek, D. L. L., Patrick, C. J., & Lilienfeld, S. O. (2011). Psychopathic personality: Bridging the gap between scientific evidence and public policy. Psychological Science in the Public Interest, 12, 95–162. A lengthy and comprehensive review of the state of scientific theory and research on psychopathy, and the implications for policy and practice. Acknowledgments My thanks to Maryanne Garry, Scott Lilienfeld, and two anonymous reviewers for their helpful comments on earlier drafts of this manuscript. Declaration of Conflicting Interests The author declared no conflicts of interest with respect to the authorship or the publication of this article. Notes 1. Psychopathy is included as one of the specifiers for antisocial personality disorder in the alternative model for personality disorders at the end of the DSM-5. It is omitted from the main section, “Diagnostic Criteria and Codes.” In contrast to the Downloaded from cdp.sagepub.com by guest on March 19, 2015 Criminals With Psychopathy 301 DSM-III, the DSM-I and the DSM-II also omitted psychopathy as a diagnosis but included antisocial-personality diagnoses that somewhat resembled psychopathy. 2. An effect size of .12 here indicates a 12% difference between the two groups in the proportion of people reconvicted. So, for example, if half of the untreated comparison group were reconvicted, the corresponding proportion for the treatment group would be .38—a relative reduction of 24%. References American Psychiatric Association. (1980). Diagnostic and statistical manual of mental disorders (3rd ed.). Washington, DC: Author. American Psychiatric Association. (2013). Diagnostic and statistical manual of mental disorders (5th ed.). Arlington, VA: Author. Andrews, D. A., & Bonta, J. (2010). The psychology of criminal conduct (5th ed.). Newark, NJ: Matthew Bender. Blonigen, D. M., Hicks, B. M., Krueger, R. F., Patrick, C. J., & Iacono, W. G. (2006). Continuity and change in psychopathic traits as measured via normal-range personality: A longitudinal-biometric study. Journal of Abnormal Psychology, 115, 85–95. Caldwell, M. F., Skeem, J., Salekin, R., & van Rybroek, G. (2006). Treatment response of adolescent offenders with psychopathy features. Criminal Justice and Behavior, 33, 571–596. Cleckley, H. M. (1988). The mask of sanity: An attempt to reinterpret the so-called psychopathic personality (5th ed.). Oxford, England: Mosby. Cullen, F. T., Jonson, C. L., & Nagin, D. S. (2011). Prisons do not reduce recidivism: The high cost of ignoring science. The Prison Journal, 91, 48S–65S. Farrington, D. P. (2007). Origins of violent behavior over the life span. In D. J. Flannery, A. T. Vazsonyi, & I. D. Waldman (Eds.), The Cambridge handbook of violent behavior and aggression (pp. 19–48). Cambridge, England: Cambridge University Press. Ferguson, C. J. (2010). A meta-analysis of normal and disordered personality across the life span. Journal of Personality and Social Psychology, 98, 659–667. Hare, R. D. (2003). The Hare Psychopathy Checklist–Revised technical manual (2nd ed.). Toronto, Ontario, Canada: Multi-Health Systems. Harpur, T. J., & Hare, R. D. (1994). The assessment of psychopathy as a function of age. Journal of Abnormal Psychology, 103, 604–609. Harris, G. T., & Rice, M. E. (2007). Psychopathy research at Oak Ridge: Skepticism overcome. In H. Hervé & J. C. Yuille (Eds.), The psychopath: Theory, research, and practice (pp. 57–75). Mahwah, NJ: Erlbaum. Harris, G. T., Rice, M. E., & Cormier, C. (1994). Psychopaths: Is a therapeutic community therapeutic? Therapeutic Communities, 15, 283–299. Hawes, D. J., & Dadds, M. R. (2007). Stability and malleability of callous-unemotional traits during treatment for childhood conduct problems. Journal of Clinical Child & Adolescent Psychology, 36, 347–355. Hobson, J., Shine, J., & Roberts, R. (2000). How do psychopaths behave in a prison therapeutic community? Psychology, Crime & Law, 6, 139–154. Hollin, C. R. (2008). Evaluating offending behaviour programmes: Does only randomization glister? Criminology & Criminal Justice, 8, 89–106. Lewis, K., Olver, M. E., & Wong, S. C. P. (2013). The Violence Risk Scale: Predictive validity and linking changes in risk with violent recidivism in a sample of high-risk offenders with psychopathic traits. Assessment, 20, 150–164. Lilienfeld, S. O., & Widows, M. (2005). Psychopathic Personality Inventory–Revised professional manual. Odessa, FL: PAR. Olver, M. E., Lewis, K., & Wong, S. C. P. (2013). Risk reduction treatment of high-risk psychopathic offenders: The relationship of psychopathy and treatment change to violent recidivism. Personality Disorders: Theory, Research, and Treatment, 4, 160–167. Polaschek, D. L. L., & Daly, T. (2013). Treatment and psychopathy in forensic settings. Aggression and Violent Behavior, 18, 592–603. Polaschek, D. L. L., & Kilgour, T. G. (2013). New Zealand’s special treatment units: The development and implementation of intensive treatment for high-risk male prisoners. Psychology, Crime & Law, 19, 511–526. doi:10.1080/10683 16X.2013.759004 Rice, M. E., Harris, G. T., & Cormier, C. A. (1992). An evaluation of a maximum security therapeutic community for psychopaths and other mentally disordered offenders. Law and Human Behavior, 16, 399–412. Salekin, R. T., & Lynam, D. R. (Eds.). (2010). Handbook of child and adolescent psychopathy. New York, NY: Guilford. Skeem, J. L., Monahan, J., & Mulvey, E. (2002). Psychopathy, treatment involvement, and subsequent violence among civil psychiatric patients. Law and Human Behavior, 26, 577–603. Wong, S., & Gordon, A. (2000). Violence Risk Scale. Saskatoon, Canada: University of Saskatchewan. Wong, S. C. P., Gordon, A., Gu, D., Lewis, K., & Olver, M. E. (2012). The effectiveness of violence reduction treatment for psychopathic offenders: Empirical evidence and a treatment model. International Journal of Forensic Mental Health, 11, 336–349. doi:10.1080/14999013.2012.746760 Downloaded from cdp.sagepub.com by guest on March 19, 2015









© Copyright 2026