
Robust MR assessment of cerebral blood volume
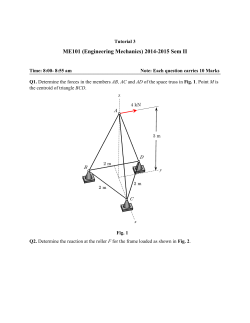
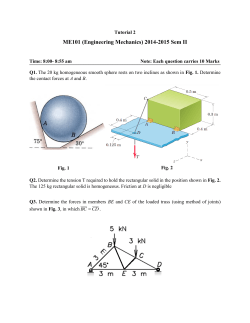
NeuroImage 112 (2015) 382–389 Contents lists available at ScienceDirect NeuroImage journal homepage: www.elsevier.com/locate/ynimg Technical Note Robust MR assessment of cerebral blood volume and mean vessel size using SPION-enhanced ultrashort echo acquisition S.H. Han a, J.H. Cho a, H.S. Jung a, J.Y. Suh b, J.K. Kim c, Y.R. Kim d, G. Cho b,⁎, H. Cho a,⁎ a Ulsan National Institute of Science and Technology, Ulsan, South Korea Korea Basic Science Institute, Ochang, South Korea Asan Medical Center, Seoul, South Korea d Martinos Center for Biomedical Imaging, Charlestown, MA, USA b c a r t i c l e i n f o Article history: Received 8 December 2014 Accepted 16 March 2015 Available online 24 March 2015 Keywords: Cerebral blood volume Mean Vessel Size Index SPION UTE a b s t r a c t Intravascular superparamagnetic iron oxide nanoparticles (SPION)-enhanced MR transverse relaxation rates (ΔR2⁎ and ΔR2) are widely used to investigate in vivo vascular parameters, such as the cerebral blood volume (CBV), microvascular volume (MVV), and mean vessel size index (mVSI, ΔR2⁎/ΔR2). Although highly efficient, regional comparison of vascular parameters acquired using gradient-echo based ΔR2⁎ is hampered by its high sensitivity to magnetic field perturbations arising from air–tissue interfaces and large vessels. To minimize such demerits, we took advantage of the dual contrast property of SPION and both theoretically and experimentally verified the direct benefit of replacing gradient-echo based ΔR2⁎ measurement with ultra-short echo time (UTE)-based ΔR1 contrast to generate the robust CBV and mVSI maps. The UTE acquisition minimized the local measurement errors from susceptibility perturbations and enabled dose-independent CBV measurement using the vessel/tissue ΔR1 ratio, while independent spin-echo acquisition enabled simultaneous ΔR2 measurement and mVSI calculation of the cortex, cerebellum, and olfactory bulb, which are animal brain regions typified by significant susceptibility-associated measurement errors. © 2015 Elsevier Inc. All rights reserved. Introduction Alternations in microvascular parameters, such as cerebral blood volume (CBV) and microvascular size, are often caused by cerebrovascular disease (Gibbs et al., 1984; Hamberg et al., 1993; Kucharczyk et al., 1993; Warach et al., 1992), vascular malfunction (Spetzler et al., 1977), and neovascularization within tumors (Aronen et al., 1994; Aronen et al., 1995). Detection of these microvascular variations plays an important role in assessing brain diseases and monitoring the therapeutic response in both preclinical and clinical settings (Dennie et al., 1998). Many non-invasive estimation methods of microvascular anatomy have been investigated, such as iodinated contrast radiography (Grubb et al., 1973; Risberg et al., 1969), positron emission tomography studies using oxygen-15-labeled carbon monoxide (Eichling et al., 1975; Leggett and Williams, 1991; Phelps et al., 1979; Powers and Raichle, 1985), and single photon emission computed tomography studies using 99 mTc-pertechnetate labeled red blood cells (Toyama et al., 1990). However, exposure to ionizing radiation and the lack of spatial resolution in radioactive tracer approaches pose critical limitations for the accurate quantification of CBV and vessel information. Recently, ⁎ Corresponding author at: Unist-gil 50 (100 Banyeon-ri), Eonyang-eup, Uljugun, Ulsan Metropolitan City, 689-798, Republic of Korea. Fax: +82 52 217 2509. E-mail address: [email protected] (H. Cho). http://dx.doi.org/10.1016/j.neuroimage.2015.03.042 1053-8119/© 2015 Elsevier Inc. All rights reserved. several methods to obtain microvascular information using steadystate MRI and various contrast agents have been proposed to overcome the limitations of radioactive tracer approaches (Kuppusamy et al., 1996; Moseley et al., 1992; Schwarzbauer et al., 1993). One of these methods is the use of superparamagnetic iron oxide nanoparticles (SPION), which have a long blood half-life (Wu et al., 2004a). SPION induces sustained intravascular susceptibility perturbations in the surrounding tissue, as reflected by an increase in the transverse magnetic resonance (MR) relaxation rates, i.e., ΔR2⁎ and ΔR2 from gradient and spin echoes, respectively (Loubeyre et al., 1999; Weissleder et al., 1990). The ΔR2⁎ and ΔR2 values are often used to calculate the CBV and microvascular volume (MVV) and have been widely used for microvascular characterizations (Yablonskiy and Haacke, 1994). However, these MR transverse relaxation measurements alone may not provide a representative regional comparison of vascular parameters. For example, the capillary direction with respect to main B0 magnetic field changes the magnitude of susceptibility-induced field inhomogeneities around the vessel and confounds the quantification of CBV from ΔR2⁎ and ΔR2 measurements (Boxerman et al., 1995; Tropres et al., 2001). Moreover, the CBV of the local tissue from gradient-echo based ΔR2⁎ measurements can be further biased in tissue neighboring large vessels or air–tissue interfaces (Kim et al., 2013). These geometrical and environmental variations often complicate the interpretation of MR transverse relaxation rates based on CBV measurements in regions such as the cortex, where S.H. Han et al. / NeuroImage 112 (2015) 382–389 vessels are fairly well aligned, and in the olfactory bulb and cerebellum, which are close to air–tissue interfaces. In addition, an accurate knowledge of the in vivo SPION concentration is required to compensate the dose dependency of transverse relaxation rates. Accordingly, when regional and dose-independent CBV measurement is necessary, the ratio between tissue and vessel signal enhancements (i.e., fractional blood volume) from the ΔR1-contrast is preferable. A positive ΔR1 ratio between the tissue and vessel is not influenced by local susceptibility field variations from the capillary structure, and reflects the doseindependent concentration-ratio of the intravascular contrast agent. Furthermore, when obtaining size information on the microvasculature, the ΔR2⁎/ΔR2 ratio is often used to estimate the mean vessel size index (mVSI), by taking advantage of the sustained strong transverse relaxation rates of SPION and molecular diffusion modeling in the presence of a susceptibility-induced field (Dennie et al., 1998; Tropres et al., 2001; Prinster et al., 1997). However, when biased susceptibilityinduced field inhomogeneities from variable capillary orientation or air–tissue interface impair local gradient-based ΔR2⁎ measurements, the mVSI estimations may also become unreliable. Previously, for robust simultaneous measurements of the regional CBV from ΔR1 contrast and the mVSI from ΔR2⁎/ΔR2 contrast, in vivo administration of Gd-based intravascular T1 and SPION-based T2/T2* contrast agents was commonly employed in order to extract both microvascular parameters (Beaumont et al., 2009; Huang et al., 2013; Kim et al., 2008). The recently introduced ultra-short echo time (UTE) pulse sequence minimizes susceptibility perturbations (Glover et al., 1992; Holmes and Bydder, 2005; Pauly et al., 1989; Robson et al., 2003), and provides an unique opportunity for dual-contrast microvascular acquisitions using a single intravascular agent, namely SPION, when combined with conventional spin-echo acquisition (Jung et al., 2014). However, despite the potential importance, direct and systematic comparisons between UTE-based and ΔR2⁎-based CBV measurements via UTE acquisitions have not been reported as of yet. In this study, Monte-Carlo spin dynamics simulations were performed to show the dependence of transverse relaxation rates on vessel orientation and the unwanted bias in ΔR2⁎ of tissues near air-tissue interfaces. Additionally, the feasibility of alternative mVSI measurements using UTE-based regional CBV values instead of ΔR2⁎ measurements was proposed and validated. Experimentally, direct comparisons were performed between in vivo UTE-based and ΔR2⁎-based CBV maps in the cortex, cerebellum, and olfactory bulb regions in nude mice, which clearly showed inconsistent ΔR2⁎ measurements at the vicinity of the air-tissue interface and large vessels. Correspondingly, for the validation of mVSI mapping with UTE acquisition, in vivo ΔR2⁎/ΔR2 versus UTE-based CBV/ ΔR2 maps were compared in the same brain regions. Next, the regional relationships between the UTE-based and the ΔR2⁎-based CBV were investigated in the olfactory bulb, cortex, caudate putamen, thalamus, superior colliculus, and cerebellum in a large cohort. The regional relationships between the ΔR2⁎/ΔR2 versus UTE-based CBV/ΔR2 were investigated as well. The UTE-based CBV was compared with previously reported regional CBVs in multiple studies. The dose dependency of the UTE-based and the ΔR2⁎-based regional CBV were compared. Method Monte Carlo (MC) simulations General methodology All MC simulations in this study were performed using an in-house Matlab script, which is similar to the method described by Pathak et al. (2008). First, 3 dimensional-binary matrices were generated to emulate the vascular structure using randomly oriented cylinders. The number of cylindrical vessels was set to match the blood volume fraction (Vb), e.g., approximately 100 cylinders were used for a 2% Vb, and the number of cylinders was increased proportionally for 5% and 10% Vb. The vessel length was set to be 40 times greater than the vessel 383 radius (Rv). The binary matrix for the vascular structure was generated three times to obtain the mean and standard deviation for each data point in the relaxation simulations. The, finite perturber method (FPM) was then used to calculate the magnetic field shift caused by the intravascular contrast agent filling the cylinder using the Fourier convolution theorem (Pathak et al., 2008). In FPM, the magnetic field shift by an arbitrary structure is calculated as the sum of the magnetic field shifts (ΔB) by uniformly packed small perturbers within the structure. The FPM inputs were the binary matrix of the vascular structure, the magnetic susceptibility difference between the intravascular contrast agent and surrounding tissue (Δχ), and the main magnetic field (B0). Finally, the Monte Carlo simulation was performed to calculate the MR transverse relaxation rates (ΔR2 and ΔR2⁎) caused by proton diffusion in the presence of a susceptibility induced inhomogeneous magnetic field. Initially, 200,000 protons were positioned randomly within the diffusion space that was filled by the cylinders. Each proton moved to an adjacent position with each increment of the simulation time (Δt) in a random trajectory and at a standard deviation of displacepffiffiffiffiffiffiffiffiffiffiffiffi ment following the diffusion length ( 2DΔt , D is the diffusion coefficient). Subsequently each spin experienced different magnetic field shifts at corresponding positions. This process induced the phase accumulation of each spins at each diffusion step. The total accumulated phase of the nth proton during time t is given by the following equation: Xt=Δt γΔBðP n ðiΔt ÞÞΔt ð1Þ ϕn ðt Þ ¼ i¼1 where Δt is the diffusion time step, γ is the proton gyromagnetic ratio (2.675 × 108 rad/T/s), Pn (t) is the position of the nth proton at time t, and ΔB (P) is the magnetic field shift at position P. The MR signal was then calculated from the mean accumulated phase of N total diffusing protons: SðtÞ ¼ 1 XN iΦn ðt Þ e : n¼1 N ð2Þ The change in the associated relaxation rates were calculated as follows: ΔR2 ; ΔR2 ¼ − ln ½SðTEÞ : TE ð3Þ Several parameters were kept consistent in all the simulations. Each diffusion process used 1000 randomly placed protons, and was repeated 200 times to obtain the mean MR signal. Hence, the number of total spins (Nt) was 2 × 105. The diffusion coefficient (D) was set to 10−5 cm2/s, the diffusion time step (Δt) to 0.2 ms, and the vessels were assumed impermeable to molecular diffusion. The Vb, Rv, B0, Δχ, TE (SE), and TE (GE) parameters were set as variables for the particular simulation. Validation of the MC simulations The simulation of the ΔR2 and ΔR2⁎ was performed as a function of vessel radius (Supplementary Fig. 1A) (Boxerman et al., 1995; Pathak et al., 2008). The parameters were identical to the previously reported values (Boxerman et al., 1995; Pathak et al., 2008): Vb was set to 2%, B0 to 1.5 T, Δχ to 10−7, TE (SE) to 100 ms, and TE (GE) to 60 ms. The Rv of each vascular structure varied from 1 μm to 23 μm at a fixed Vb. To determine representative experimental conditions, the dependency of ΔR2 and ΔR2⁎ as a function of TE was investigated at two different magnetic susceptibilities of the intravascular contrast agent (Δχ), 2 × 10−7 and 4 × 10−7 (Supplementary Fig. 1B). The main magnetic field (B0), blood volume (Vb), and vessel diameter (VD) were set to 3 T, 2%, and 2 μm, respectively. Vulnerability of transverse relaxation rates The dependency of ΔR2 and ΔR2⁎ values on the vessel orientation and air–tissue interface is shown in Fig. 1. In both simulations, the Vb was set 384 S.H. Han et al. / NeuroImage 112 (2015) 382–389 (A) Effect of vessel orientation (A-1) (A-2) 20 40 along x along y along z B0, z-axis 14 35 ΔR2* [1/s ] 16 12 10 140 along x along y along z 120 ΔR2* , ΔR 2 [1/s] 18 ΔR2 [1/s ] (B) Effect of air-tissue interface 30 25 20 15 8 6 −20 0 20 40 60 80 Relative portion of randomly oriented vessels [%] 100 120 100 80 60 40 20 10 −20 0 20 40 60 80 100 0 −0.05 120 0 0.05 0.1 0.15 0.2 0.25 0.2 Bubble size [Radius/Space size] Relative portion of randomly oriented vessels [%] Fig. 1. ΔR2 and ΔR⁎2 curves due to vessel orientations as a function of randomness (Figs. 1A-1 and A-2) and air–tissue interface within the tissue as a function of bubble size (Fig. 1B). The total blood volume and vessel radius (Rv) were set to 2% and 2 μm, respectively. Magnetic susceptibility differences between pre- and post-SPION injection (ΔχSPION), and between the captured air-bubble and tissue (Δχair-bubble) were set to 4 × 10−7 and 7 × 10−7 ,respectively. The blue, red, and black lines indicate the vessel alignment along the x, y, and zdirections, respectively. SPION, superparamagnetic iron oxide nanoparticles. to 2%, Rv to 2 μm, B0 to 3 T along the z-direction, magnetic susceptibility difference of the intravascular contrast agent to 4 × 10−7, the TE (SE) to 100 ms, and the TE (GE) to 15 ms. In the simulation of vessel orientation effect for ΔR2 (Fig. 1A-1) and ΔR2⁎ (Fig. 1A-2), all the vessels were initially set to be aligned along a certain direction, e.g. x-axis, as shown in the vessel structure of Fig. 1A-1. Then, the relative portion of randomly oriented vessels was increased from 0% (all aligned) to 100% (all randomly oriented), while keeping the total Vb. This simulation was performed for three cases with the vessels aligned in the x, y, and z-directions. Next, in the simulation investigating the effect of the air–tissue interface on the transverse relaxation (Fig. 1B), the air-bubble was set as a sphere and was located in the center of the vascular space, with all the vessels (the total Vb of 2%) set to random orientation. The bubble radius was then increased as shown in vascular structure of Fig. 1B. More specifically, the ratio of the bubble radius to the one directional length of total vascular matrix was varied from 0 to 1/5. The magnetic susceptibility difference between the captured air-bubble and tissue (Δχair-bubble) was set to 7 × 10−7, which was estimated based on a tissue magnetic susceptibility of ~ 7 × 10−7 (Schenck, 1996), and an air (80% Nitrogen and 20% Oxygen gas) magnetic susceptibility of ~ 5.6 × 10− 9 (Glick, 1961). Additionally, each proton was not allowed to exist inside the air-bubble initially and the air-bubble was assumed impermeable. Mean vessel size simulations The vessel size dependency was examined in four MR vascular parameters, ΔR2, ΔR2⁎, ΔR2⁎/ΔR2, and the UTE-based CBV/ΔR2. The strength of the magnetic field (B0) was 3 T and the magnetic susceptibility difference between pre- and post-SPION injection (ΔχSPION) was set to 2 × 10−7 and 4 × 10−7 for the simulation. These ΔχSPION values were estimated based on the administered SPION dose in the animal experiment (Kim et al., 2013). The fractional blood volume (Vb) was set to 2%, 5%, and 10%, and these values were used for the corresponding UTEbased CBV in the simulations. As shown in Fig. 2, the vessel radius (Rv) varied from 1 μm to 23 μm for each given Vb (2%, 5%, and 10%). For the calculation of ΔR2 and ΔR2⁎, the TE (SE) and TE (GE) were set to 100 ms and 15 ms, respectively. In vivo experiments All studies were performed on a 3T MRI scanner (Philips Achieva, Best, Netherlands). The Institutional Animal Care and Use Committee of the Korea Basic Science Institute approved the in vivo animal experiments conducted in this study. Animal and contrast agent protocols A total 29 male nude mouse (20g ~ 28 g) were used in these studies. The contrast agent used in this study was SPION, whose particle size, half-life and MR relaxivity values were characterized in a previous study (Jung et al., 2014). In most of the studies, UTE, MEGE and MSME MR images were acquired before and after SPION was intravenously administered at 70 μmol/kg (n = 21). For the dose dependency characterization, higher SPION doses were administered at 120 μmol/kg (n = 4) and 140 μmol/kg (n = 4). Regional CBV measurements An MRI anatomical brain atlas template was registered to the T2⁎ images from the MEGE sequence in order to obtain regional CBV information. The MRI anatomical brain template was accessed at http:// scalablebrainatlas.incf.org/main/coronal3d.php?template=WHS10. Slice averaging of the template was performed due to the differing slice thickness between the template and T2⁎ images. Representative six brain regional masks were shown in Supplementary Fig. 2. CBV measurements from UTE acquisitions The UTE images were acquired under the following parameters in order to maximize the intravascular T1 vessel/tissue contrast while minimizing the T2⁎ effect of SPION: FA = 90°, TR = 50 ms, TE = 90 μs, FOV = 5 × 5 × 8 cm3, and resolution = 195 × 195 × 1000 μm3. The signal intensity from UTE is presented by before (Stissue _ pre = (1 − Vb)Sextra + VbSintra) and after (Stissue _ post = (1 − Vb)Sextra + VbSintra′) SPION administration based on a two-compartment tissue model with intravascular and extravascular spaces. The Vb is the blood volume fraction. The Sextra and Sintra are the signal intensities of the extravascular and intravascular compartments before SPION administration, respectively. After administering the intravascular contrast agent, the signal in the intravascular compartment is only altered due to the T1-shortening effect of the intravascular contrast agent. (FA = 90° was used to minimize the extravascular signal alteration from trans-vascular water exchange in the presence of T1-shortening intravascular contrast agent.) The Sintra′ represents the intravascular space signal after injection. Since Sblood_pre and Sblood_post can be replaced by Sintra and Sintra′ respectively, and they are measurable on images, Vb was quantified from the following equation: Vb ¼ Stissue Sblood post −Stissue pre post −Sblood pre : ð4Þ S.H. Han et al. / NeuroImage 112 (2015) 382–389 -7 = 2 x 10 , B0 = 3T (A-2) 20 15 50 40 30 10 20 5 10 0 0 0 100 10 10 0 10 0.1 −0.1 10 −0.3 10 −0.5 10 100 0 Radius [ µm] 10 100 Radius [ µm] = 4 x 10 , B0 = 3T (B-1) (B-3) (B-2) 50 40 30 20 −0.1 10 140 120 R2*/ R2 BV 2% BV 5% BV 10% 60 R2* [1/s] 160 100 80 60 40 10 20 0 0 0 10 -7 (B) R2 [1/s] 0 100 Radius [ µm] Radius [µm] 70 10 UTE-based CBV/ R2 R2 [1/s] 25 (A-4) (A-3) 80 70 60 UTE-based CBV/ R2 BV 2% BV 5% BV 10% 30 R2* [1/s] (A-1) 35 R2*/ R2 (A) 0 385 10 Radius [µm] 100 0 10 100 0 Radius [ µm] 10 100 (B-4) 10 −0.3 10 −0.5 10 −0.7 10 −0.9 10 0 Radius [ µm] 10 100 Radius [ µm] Fig. 2. Vessel size dependence of four MR parameters, ΔR2 (Figs. 2A-1 and B-1), ΔR⁎2 (Figs. 2A-2 and B-2), ΔR⁎2 /ΔR2 (Figs. 2A-3 and B-3), and UTE-based CBV/ΔR2 (Figs. 2A-4 and B-4). Figs. 2A and B show the effect under two different magnetic susceptibility values, 2 × 10−7 and 4 × 10−7, respectively. The red, blue, and black lines correspond to simulation performed at a blood volume of 2%, 5%, and 10%, respectively. MR, magnetic resonance. CBV measurements from MEGE acquisitions The MEGE images were acquired using the following parameters to determine ΔR2⁎: TR = 3000 ms, FOV = 5 × 5 × 2.4 cm3, resolution = 195 × 195 × 1000 μm3, and TE = 7, 13, 19, 25, 31, and 37 ms. To extract ΔR2⁎ values in accordance with simulation, data points whose signal amplitudes were 5 times above the noise level were linearly fitted on a semi-log plot and the signals before and after SPION administration were obtained at TE = 15 ms. Then, the signal differences before and after SPION administration were converted to ΔR2⁎ values at TE = 15 ms, using the single exponential model (ΔR2⁎ = ln(Spre/Spost)/TE) (Tropres et al., 2001). Assuming that the static dephasing was dominant, the fractional CBV (%) was estimated from the linear relationship relative to the ΔR2⁎ as follows (Tropres et al., 2001): ΔR2 ¼ 4 π ð1−Hct Þ V b Δχ γB0 3 ð5Þ where Vb is the blood volume fraction, γ is the gyromagnetic ratio (2.675 × 108 rad/T/s), Hct is the hematocrit set at 0.4, and Δχ is the susceptibility difference of the contrast agent (0.36 ppm) at 3 T and 15 mg Fe/kg (Kim et al., 2013). ΔR2⁎-based and UTE-based mVSI measurements The MSME images were acquired using the following parameters to determine the ΔR2 : TR = 3800 ms, FOV = 5 × 5 × 2.4 cm3, resolution = 195 × 195 × 2000 μm3, and TE = 60 and 100 ms. The signal differences before and after SPION administration at TE = 60 ms were converted to ΔR2 values, using the single exponential model (ΔR2 = ln(Spre/Spost)/TE) (Dennie et al., 1998; Tropres et al., 2001; Prinster et al., 1997). The signals at TE = 100 ms were not used due to lowered signal to noise ratio. The ΔR2⁎-based mVSI was calculated from the ratio of ΔR2⁎ and ΔR2, obtained with MEGE and MSME acquisitions, respectively (Dennie et al., 1998; Tropres et al., 2001; Prinster et al., 1997). The UTE-based mVSI was calculated from the ratio of the UTE-based CBV and ΔR2, obtained with UTE and MSME acquisitions, respectively. As MSME measurements were performed with slice thickness of 2 mm, slice averaging of the UTE and MEGE images was performed for the following mVSI analyses. Results Validation of the MC simulations The dependency of ΔR2 and ΔR2⁎ on vessel size was evaluated to validate the computational accuracy of our simulation, compared to previous results (Boxerman et al., 1995; Pathak et al., 2008). As shown in Supplementary Fig. 1A, the ΔR2 and ΔR2⁎ in the current simulation agree with the previous values obtained under the same conditions (B0 = 1.5 T and Δχ = 1 × 10−7). The dependency of ΔR2 and ΔR2⁎ on TE was also evaluated to optimize experimental TE values for the MSME and MEGE acquisitions at 3 T. As shown in Supplementary Fig. 1B, both ΔR2 and ΔR2⁎ drastically increased as the TE increased, and rate of increase decreased at TE values of ~ 30 ms for ΔR2 and ~ 5 ms for ΔR2⁎. Vulnerability of transverse relaxation rates The effects of vessel orientation (Fig. 1A) and air–tissue interface (Fig. 1B) on ΔR2 and ΔR2⁎ were examined. Fig. 1A showed the behavior of ΔR2 and ΔR2⁎ as the relative portion of randomly oriented vessels increased, while maintaining the total Vb at 2%. The blue, red, and black lines indicate the initial vessel alignment along the x-, y-, and zdirections, respectively. Similar trends were observed between ΔR2 and ΔR2⁎ as the relative portion of randomly oriented vessels increased in all 386 S.H. Han et al. / NeuroImage 112 (2015) 382–389 directions (Fig. 1A). The ΔR2 and ΔR2⁎ decreased as the relative portion of randomly oriented vessels increased that were initially aligned along the x- and y-directions, but the opposite relationship was observed shown in vessels that were initially aligned along the main magnetic field direction (z-direction). Fig. 1B shows the effect of the air–tissue interface on the ΔR2 and ΔR2⁎. Generally, both ΔR2 and ΔR2⁎ (blue and red lines, respectively) increased as the radius of the air-bubble increased from zero to onefifth of the total space size. However, the increasing rate of ΔR2⁎ was much higher than that of ΔR2, which shows that the gradient-echo based ΔR2⁎ value is more sensitive to influence by the air–tissue interface than the spin-echo based ΔR2 value is. Mean vessel size index (mVSI) simulations The vessel size dependency of the four MR parameters, ΔR2, ΔR2⁎, ΔR2⁎/ΔR2, and UTE-based CBV/ΔR2 at 3T was shown in Fig. 2. Figs. 2A and B showed the corresponding results at both magnetic susceptibility values of 2 × 10−7 and 4 × 10−7, respectively. The red, blue, and black lines correspond to the cases performed at a total Vb of 2%, 5%, and 10%, respectively. At Δχ = 2 × 10−7, the ΔR2 peaked at an approximately 2 μm-radius and decreased as the radius increased (Fig. 2A-1). The ΔR2⁎ increased and plateaued at an approximately 3 μm-radius (Fig. 2A-2). This pattern was observed at all three Vb conditions (2%, 5%, and 10%). At the increased value of Δχ = 4 × 10−7, the ΔR2 steadily decreased as the radius increased (Fig. 2B-1). The ΔR2⁎ quickly plateaued to a constant value over the entire radius range for all Vb (Fig. 2B-2). Next, the ΔR2⁎/ΔR2 and UTE-based CBV/ΔR2 were plotted as a function of vessel size for all Vb. At both Δχ values (2 × 10− 7 and 4 × 10−7), neither the ΔR2⁎/ΔR2 nor the UTE-based CBV/ΔR2 showed any significant dependency on the blood volume (Figs. 2A-3, A-4, B-3, and B-4). For Δχ = 2 × 10−7, the UTE-based CBV/ΔR2 pattern was in a good agreement with the ΔR2⁎/ΔR2 pattern, except at a radius of 1 μm; the UTE-based CBV/ΔR2 decreased from 1 μm to 2 μm and became proportional to the increase in radius (Fig. 2A-3). The ΔR2⁎/ΔR2 steadily increased as the radius increased (Fig. 2A-4). At Δχ = 4 × 10− 7, the UTE-based CBV/ΔR2 showed a steady increase, which was consistent with the ΔR2⁎/ΔR2 pattern (Figs. 2B-3 and B-4). This steady increase as a function of vessel size and its independency from blood volume make the UTE-based CBV/ΔR2 suitable for robust mVSI estimation at our experimental conditions. (A-1) (B-1) (C-1) UTE-based CBV(%) Direct comparison of CBV and mVSI maps from UTE, MEGE, and MSME Representative voxel-wise maps of the regional CBV and mVSI calculated from the UTE, MEGE and MSME sequences were shown in Fig. 3. The T2⁎-weighted images of the cortex, cerebellum, and olfactory bulb regions were shown in Fig. 3A. The UTE-based CBV maps from Eq. (4) are shown in Fig. 3B. The MEGE- and MSME-derived ΔR2⁎ and ΔR2 values were shown in Figs. 3C and D, respectively. Conventional mVSI maps using ΔR2⁎/ΔR2 were shown in Fig. 3E. The alternative mVSI maps constructed using UTE-based CBV/ΔR2 were shown in Fig. 3F. There were several notable differences between the ΔR2⁎-based and UTE-based CBV maps in Figs. 3B and C. As indicated in Figs. 3B-1 and C-1 with black arrows, the UTE-based CBV showed positive values as the blood volume increased, but the ΔR2⁎ showed negative values in the corresponding region. For the region indicated by black arrows in Fig. 3B-2, no signal enhancement was observed in either map of the air–tissue interface region near both ears; this area was also negatively enhanced on the gradient-echo acquisition shown in Fig. 3C-2. The UTE-based CBV was able to clearly distinguish the high blood volume region from the air–tissue interface, while the gradient-echo-based ΔR2⁎ failed to identify the corresponding regions. In addition, a spatial shift was observed in the image on the ΔR2⁎ maps due to the field inhomogeneity compared with the UTE-based CBV and ΔR2 maps, which would require an additional registration process for the direct voxel comparison and analysis. Consequently, the resulting conventional mVSI (ΔR2⁎/ΔR2) showed an unstable voxel map. As indicated in Fig. 3E-1 with a white arrow, the mVSI was decreased in cortical regions containing large vessels. However, the corresponding mVSI showed a higher mVSI value than in other regions (Fig. 3F-1, white arrow). The conventional mVSI map in the cerebellum was severely inconsistent between the hemispheres due to ΔR2⁎ artifacts near the air-tissue interface (Fig. 3E-2, white arrow) compared to the UTEbased mVSI (Fig. 3F-2, white arrow). The olfactory bulb region showed similar artifacts due to the large vessel penetrating perpendicular to the main field (Fig. 3E-3, white arrow) compared to the UTE-based mVSI (Fig. 3F-3, white arrow). Comparison of regional CBV and mVSI values Direct comparisons of the ΔR2⁎-based CBV (%) and UTE-based CBV (%) values for the olfactory bulb, cortex, caudate putamen, thalamus, superior (D-1) 10 0 −10 (E-1) R2 [1/s] R2* [1/s ] 50 0 −50 R2*/ R2 [1/s] 5 0 −5 (F-1) UTE-based CBV(%)/ R 2 20 0 −20 5 0 −5 Cortex (A-2) (B-2) (C-2) 10 0 −10 (D-2) 50 0 −50 (E-2) 5 0 −5 (F-2) 20 0 −20 5 0 −5 Cerebellum (A-3) (B-3) (C-3) 10 0 −10 (D-3) 50 0 −50 (E-3) 5 0 −5 (F-3) 20 0 −20 5 0 −5 Olfactory bulb Fig. 3. MR imaging of nude mice before and after SPION administration in the cortex, cerebellum, and olfactory bulb. (A) T⁎2 MR image before SPION administration. (B) UTE-based CBV map. (C) ΔR⁎2 -based CBV map. (D) ΔR2 map. (E) ΔR⁎2 -based mVSI (ΔR⁎2 /ΔR2). (F) UTE-CBV based mVSI (UTE-CBV/ΔR2). MR, magnetic resonance; SPION, superparamagnetic iron oxide nanoparticles; CBV, cerebral blood volume; mVSI, mean vessel size index. S.H. Han et al. / NeuroImage 112 (2015) 382–389 colliculus, and cerebellum were shown in Fig. 4A. The standard deviation of the measured CBV values was marked on the plot. The gradient-echobased ΔR2⁎-based CBV (%) showed a significantly larger standard deviation than that of the UTE-based CBV (%). By contrast, ΔR2⁎-based and the UTE-based CBVs across the different brain regions were linearly correlated when a large sample size was included. To further validate its feasibility, the UTE-based CBV in various brain regions were compared with previously reported values shown in Table 1. Each CBV ratio was calculated by dividing the regional CBV by the cortical CBV in order to identify the correlation between regional CBV values in the different studies. The cortex, thalamus, caudate putamen, and cerebellum generally showed CBV values consistent with earlier reports; our CBV was close to or lied between the minimum and maximum values in prior studies. For instance, the measured CBV in the cortex was 2.03, which ranged from 1 to 4 in earlier reports, indicating agreement between our cortical CBV the earlier values. The same trend was observed in the CBV of the thalamus, caudate putamen, and cerebellum. However, in the olfactory bulb and superior colliculus, our CBV was greater than the earlier values. The CBV ratio was consistent with previous results in every brain region except the superior colliculus. Accordingly, regional ΔR2⁎/ΔR2 and UTEbased CBV/ΔR2 values were compared as shown in Fig. 4B. Numerical values of respective experimental mVSI estimations consistently fell within the range of simulational calculations as shown in Figs. 2A-3 and A-4. Considering apparent good coefficient of determination (r2 = 0.90) between UTE-based CBV and ΔR2⁎-based CBV across the different brain regions from Fig. 4A, UTE-based mVSI showed reduced linearity (r2 = 0.04, r2 w/o olfactory = 0.49, and r2 w/o olfactory & thalamus = 0.85) with respect to ΔR2⁎-based mVSI. The reduced linearity between both mVSI values is likely from the relative spatial shift of MEGE images with respect to MSME and UTE images, which is conspicuous in olfactory bulb region as shown in Fig. 3C-3 due to susceptibility mismatch. Significantly larger standard deviations of ΔR2⁎-based mVSI were also observed for olfactory bulb and thalamus regions, where air–tissue interfaces and macro-vessels exist. 387 Table 1 Regional CBV compared between previous and the current study for the cortex, thalamus, caudate putamen, olfactory bulb, superior colliculus, and cerebellum. The CBV ratio was calculated by dividing the regional CBV with the cortex CBV in order to identify the correlation of the regional CBV to those of the previous investigations. CBV, cerebral blood volume. Cortex Thalamus Caudate putamen Olfactory bulb Superior colliculus Cerebellum CBV (ml∙100g−1) CBV ratio Method animal 4.07 1.63 1.13 1.03 0.934 3.26 2 1 1 1 1 1 1 1 Rat Rat Rat Mouse Rat Rat Rat 2.44 2.03 3.03 1.11 1.1 0.785 3.56 2.87 1 1 1.86 0.98 1.07 0.84 1.75 0.71 MRI (Tropres et al., 2001) MRI (Schwarzbauer et al., 1997) Autoradiography (Lear et al., 1990) MRI (Wu et al., 2004b) CT (Cremer and Seville, 1983) MRI (Chugh et al., 2009) Autoradiography (Julien‐Dolbec et al., 2002) CT (Everett et al., 1956) MRI (our study) MRI (Schwarzbauer et al., 1997) Autoradiography (Lear et al., 1990) MRI (Wu et al., 2004b) CT (Cremer and Seville, 1983) MRI (our study) MRI (Tropres et al., 2001) 0.88 0.629 2 1.3 1.07 0.78 0.673 0.82 0.64 1.04 Autoradiography (Lear et al., 1990) CT (Cremer and Seville, 1983) CT (Everett et al., 1956) MRI (our study) MRI (Wu et al., 2004b) Rat Rat Rat Mouse Mouse 2.3 1.31 1.13 1.27 MRI (our study) MRI (Wu et al., 2004b) Mouse Mouse 1.03 4.82 1.17 1.09 4.28 3.78 1.10 2.37 1.14 1.17 1.31 1.86 CT (Cremer and Seville, 1983) MRI (our study) MRI (Wu et al., 2004b) CT (Cremer and Seville, 1983) MRI (Chugh et al., 2009) MRI (our study) Rat Mouse Mouse Rat Rat Mouse Rat Mouse Rat Rat Mouse Rat Mouse Rat Comparison of dose dependency in CBV from UTE and MEGE The dose dependent behaviors of the ΔR2⁎-(1/s) and UTE-based CBV (%) values in the different regions of interest (ROI) of the mouse brain are shown in Figs. 4C and D, respectively. An increased contrast dose elevated the Δχ (Kim et al., 2013), thus increasing the ΔR2⁎-(1/s), as shown in Fig. 4C. Dose correction was required to calculate the (B) rte x pu tam en tha su lam pe rio us rc oll icu lus ce reb ell um co ca ud ate ac tor yb ulb 0 MEGE−CBV(1/s) 30 20 8 6 4 2 10 0 rte x pu tam en tha su lam pe rio us rc oll icu lus ce reb ell um 2 5 10 80 100 120 concentration (µmol/kg) 140 0 80 100 120 140 concentration (µmol/kg) ud ate 4 ulb 6 10 40 co 8 15 olfactory bulb cortex caudate putamen thalamus superior colliculus cerebellum 12 2 ca 10 mean Vessel Size Index (mVSI) 12 3 x UTE-CBV/ΔR2(TE = 60ms) ΔR2*(TE = 15ms)/ΔR2(TE = 60ms) r (all) = 0.04, r (w/o olfactory) = 0.49 2 r (w/o olfactory & thalamus) = 0.85 tor yb r2 (all) = 0.90 14 (D) 50 2 ac 16 olf Blood volume fraction (%) UTE-CBV MEGE-CBV(TE = 15ms) 18 olf (C) 20 20 UTE−CBV(%) (A) ΔR2⁎-based CBV (%) shown in Fig. 4A, which was generally larger than the value calculated from the UTE-based CBV (%). By contrast, the UTE-based CBV showed constant behavior at different doses. This dose independency proves the stability of measuring the CBV using the UTE sequence. Fig. 4. (A) UTE-based CBV and MEGE (ΔR2⁎)-based CBV in the olfactory bulb, cortex, caudate putamen, thalamus, superior colliculus, and cerebellum regions (slice thickness = 1 mm). The coefficient of determination (r2) was 0.90. (B) Corresponding (3 × UTE-based CBV)/ΔR2 and ΔR2⁎/ΔR2 derived mVSI values in the olfactory bulb, cortex, caudate putamen, thalamus, superior colliculus, and cerebellum regions (slice thickness = 2 mm). The coefficient of determination (r2) were 0.04, 0.49, and 0.85 for all regions, regions without olfactory, and regions without olfactory & thalamus, respectively. (C) The MEGE (ΔR2⁎)-based and (D) UTE-based CBV at SPION doses of 70 μmol/kg (n = 21), 120 μmol/kg (n = 4), and 140 μmol/kg (n = 4) in the different regions. CBV, cerebral blood volume; mVSI, mean vessel size index; SPION, superparamagnetic iron oxide nanoparticles. 388 S.H. Han et al. / NeuroImage 112 (2015) 382–389 Discussion Microvascular parameters such as the CBV and mVSI are typically measured using transverse relaxation changes, i.e., the ΔR2⁎ and ΔR2 in the presence of intravascular SPION, usually known as a T2 contrast agent. However, transverse relaxation measurements on a gradient echo sequence are easily biased by geometrical and environmental conditions, and may cause several potential artifacts when estimating microvascular parameters. In this study, by taking advantage of the dual contrast ability of SPION, we theoretically and experimentally verified the direct benefit of replacing the gradient-echo-based ΔR2⁎ measurement with an ultrashort echo time (UTE)-based ΔR1 contrast to generate robust CBV and mVSI maps. As suggested by the Monte Carlo simulations, the experimental ΔR2⁎based CBV showed larger standard deviations within the cohort than those from the UTE-CBV. Different geometrical alignments relative to the main magnetic field, vascular environments, and shimming value for each subject may account for the ΔR2⁎ variations. This larger variation in the ΔR2⁎-based CBV should be considered when longitudinal studies of small cohorts are performed. A ΔR1-based CBV should be less influenced by these external parameters in a large cohort, because R1 measurement does not include spin signal dephasing due to molecular diffusion in the presence of field inhomogeneity. This was verified by the stable CBV measurements in the animal experiment (n = 29) with UTE acquisition. Furthermore, the conventional mVSI (ΔR2⁎/ΔR2) map showed significant artifacts near the air–tissue interfaces and large vessels due to unaccounted variations in the ΔR2⁎ measurements. In comparison, the newly proposed mVSI method (UTE-based CBV/ΔR2) showed consistent values in both hemispheres and distinguished the high blood pool area from the air–tissue interface region, truly reflecting the in vivo concentration variation in the SPION. Another possible advantage of dual contrast, SPION-assisted MR lies in the unambiguous CBV fraction (UTE-based CBV) that is obtained independent of the size of underlying vessels. When traditional vessel size index (ΔR2⁎/ΔR2) information is necessary for the specific purpose, the UTE-based CBV and ΔR2⁎/ΔR2 can be separately measured using a single agent without the confounding effect resulting from multiple contrast agents. In this way, accurate ΔR1 and sensitive ΔR2⁎ contrasts may be synergistically combined to enhance in vivo SPION contrast for tailored applications (Jung et al.,2014 ; Girard et al., 2011). It should be cautioned that the UTE-based CBV mapping with SPION, which is independent of the hematocrit value and susceptibility effect still provides fractional CBV, while dynamic susceptibility contrast (DSC)-MRI is known to provide absolute CBV with suitable pharmacokinetic modeling with arterial input function information (Calamante et al., 1999; Cha et al., 2002). Direct comparisons of these values will shed light on the potential opportunities and limitations of UTE-based CBV. Additionally, even though minimized from UTE acquisition with 90° flip angle excitation, the underlying assumption of R1-insensitivity of extravascular signal from intravascular SPION or perfusion effect is not fully experimentally proven for the determination of UTE-based CBV, and future investigations may be focused on either compensating or utilizing these potential errors of apparent CBV for the quantification of trans-vascular water exchange using UTE acquisition. Technically, variations of achievable shortest UTE echo time and worsening of temporal resolution is still challenging for the wide-spread use of UTE acquisition and future technical advances in UTE-related hardware and acquisitions/reconstructions may further facilitate UTE applications to microvascular characterizations. A potential translational limitation of our study is that the SPION we used is not yet clinically approved. However, a chemically equivalent iron oxide nanoparticle (Feraheme, AMAG Pharmaceuticals, Lexington, MA, USA) has been clinically approved for the treatment of irondeficiency anemia and is under consideration for use in MRI (Christen et al., 2013; D'Arceuil et al., 2013; Li et al., 2005). Additional characterization of the MR contrast properties of this nanoparticle may validate the clinical applications of dual-contrast microvascular quantification described in this study. In summary, by taking advantage of the dual contrast property of SPION, UTE acquisition minimizes susceptibility perturbations and enables regional CBV measurements from the vessel/tissue ΔR1 ratio, while consecutive spin-echo acquisition provides robust vessel size information through simultaneous ΔR2 measurements in the cortex, cerebellum, and olfactory bulb areas of the animal brain, which is subject to significant susceptibility perturbation. Application of this method in longitudinal follow-up investigations of microvasculature brain disease may enable clear quantification of microvascular parameters. Supplementary data to this article can be found online at http://dx. doi.org/10.1016/j.neuroimage.2015.03.042. Acknowledgments This work was supported by the National Research Foundation of Korea Grants funded by the Korean Government (no. 2010-0028684 and no. 2014 R1A1A1 008255). References Aronen, H.J., Gazit, I.E., Louis, D.N., Buchbinder, B.R., Pardo, F.S., Weisskoff, R.M., Harsh, G.R., Cosgrove, G., Halpern, E.F., Hochberg, F.H., 1994. Cerebral blood volume maps of gliomas: comparison with tumor grade and histologic findings. Radiology 191, 41–51. Aronen, H.J., Glass, J., Pardo, F., Belliveau, J., Gruber, M., Buchbinder, B., Gazit, I., Linggood, R., Fischman, A., Rosen, B., 1995. Echo-planar MR cerebral blood volume mapping of gliomas: clinical utility. Acta Radiol. 36, 520–528. Beaumont, M., Lemasson, B., Farion, R., Segebarth, C., Rémy, C., Barbier, E.L., 2009. Characterization of tumor angiogenesis in rat brain using iron-based vessel size index MRI in combination with gadolinium-based dynamic contrast-enhanced MRI. J. Cereb. Blood Flow Metab. 29, 1714–1726. Boxerman, J.L., Hamberg, L.M., Rosen, B.R., Weisskoff, R.M., 1995. MR contrast due to intravascular magnetic susceptibility perturbations. Magn. Reson. Med. 34, 555–566. Calamante, F., Thomas, D.L., Pell, G.S., Wiersma, J., Turner, R., 1999. Measuring cerebral blood flow using magnetic resonance imaging techniques. J. Cereb. Blood Flow Metab. 19 (7), 701–735. Cha, S., Knopp, E.A., Johnson, G., Wetzel, S.G., Litt, A.W., Zagzag, D., 2002. Intracranial mass lesions: dynamic contrast-enhanced susceptibility-weighted echo-planar perfusion MR imaging. Radiology 223, 11–29. Christen, T., Ni, W., Qiu, D., Schmiedeskamp, H., Bammer, R., Moseley, M., Zaharchuk, G., 2013. High‐resolution cerebral blood volume imaging in humans using the blood pool contrast agent ferumoxytol. Magn. Reson. Med. 70, 705–710. Chugh, B.P., Lerch, J.P., Yu, L.X., Pienkowski, M., Harrison, R.V., Henkelman, R.M., Sled, J.G., 2009. Measurement of cerebral blood volume in mouse brain regions using microcomputed tomography. Neuroimage 47, 1312–1318. Cremer, J.E., Seville, M.P., 1983. Regional brain blood flow, blood volume, and haematocrit values in the adult rat. J. Cereb. Blood Flow Metab. 3, 254–256. D'Arceuil, H., Coimbra, A., Triano, P., Dougherty, M., Mello, J., Moseley, M., Glover, G., Lansberg, M., Blankenberg, F., 2013. Ferumoxytol enhanced resting state fMRI and relative cerebral blood volume mapping in normal human brain. Neuroimage 83, 200–209. Dennie, J., Mandeville, J.B., Boxerman, J.L., Packard, S.D., Rosen, B.R., Weisskoff, R.M., 1998. NMR imaging of changes in vascular morphology due to tumor angiogenesis. Magn. Reson. Med. 40, 793–799. Eichling, J.O., Raichle, M.E., Grubb, R., Larson, K.B., Ter-Pogossian, M., 1975. In vivo determination of cerebral blood volume with radioactive oxygen-15 in the monkey. Circ. Res. 37, 707–714. Everett, N.B., Simmons, B., Lasher, E.P., 1956. Distribution of blood (Fe59) and plasma (I131) volumes of rats determined by liquid nitrogen freezing. Circ. Res. 4, 419–424. Gibbs, J., Leenders, K., Wise, R., Jones, T., 1984. Evaluation of cerebral perfusion reserve in patients with carotid-artery occlusion. Lancet 323, 310–314. Girard, O.M., Du, J., Agemy, L., Sugahara, K.N., Kotamraju, V.R., Ruoslahti, E., Bydder, G.M., Mattrey, R.F., 2011. Optimization of iron oxide nanoparticle detection using ultraschort echo time pulse sequences: comparisons of T1, T2*, and synergistic T1T2* contrast mechanisms. Magn. Reson. Med. 65, 1649–1660. Glick, R., 1961. On the diamagnetic suceptibility of gases. J. Phys. Chem. 65, 1552–1555. Glover, G.H., Pauly, J.M., Bradshaw, K.M., 1992. Boron‐11 imaging with a three‐dimensional reconstruction method. J. Magn. Reson. Imaging 2, 47–52. Grubb Jr., R.L., Phelps, M.E., Ter-Pogossian, M.M., 1973. Regional cerebral blood volume in humans: X-ray fluorescence studies. Arch. Neurol. 28, 38. Hamberg, L., Macfarlane, R., Tasdemiroglu, E., Boccalini, P., Hunter, G., Belliveau, J., Moskowitz, M., Rosen, B., 1993. Measurement of cerebrovascular changes in cats after transient ischemia using dynamic magnetic resonance imaging. Stroke 24, 444–450. Holmes, J.E., Bydder, G.M., 2005. MR imaging with ultrashort TE (UTE) pulse sequences: basic principles. Radiography 11, 163–174. S.H. Han et al. / NeuroImage 112 (2015) 382–389 Huang, S., Kim, J.K., Atochin, D.N., Farrar, C.T., Huang, P.L., Suh, J.Y., Kwon, S.J., Shim, W.H., Cho, H., Cho, G., 2013. Cerebral blood volume affects blood–brain barrier integrity in an acute transient stroke model. J. Cereb. Blood Flow Metab. 33, 898–905. Julien‐Dolbec, C., Tropres, I., Montigon, O., Reutenauer, H., Ziegler, A., Decorps, M., Payen, J.F., 2002. Regional response of cerebral blood volume to graded hypoxic hypoxia in rat brain. Br. J. Anaesth. 89, 287–293. Jung, H., Park, B., Lee, C., Cho, J., Suh, J., Park, J., Kim, Y., Kim, J., Cho, G., Cho, H., 2014. Dual MRI T1 and T2(⁎) contrast with size-controlled iron oxide nanoparticles. Nanomedicine: nanotechnology, Biology and Medicine 10, 1679–1689. Kim, Y., Tejima, E., Huang, S., Atochin, D., Dai, G., Lo, E., Huang, P., Bogdanov, A., Rosen, B., 2008. In vivo quantification of transvascular water exchange during the acute phase of permanent stroke. Magn. Reson. Med. 60, 813–821. Kim, S.G., Harel, N., Jin, T., Kim, T., Lee, P., Zhao, F., 2013. Cerebral blood volume MRI with intravascular superparamagnetic iron oxide nanoparticles. NMR Biomed. 26, 949–962. Kucharczyk, J., Roberts, T., Moseley, M.E., Watson, A., 1993. Contrast‐enhanced perfusion‐ sensitive MR imaging in the diagnosis of cerebrovascular disorders. J. Magn. Reson. Imaging 3, 241–245. Kuppusamy, K., Lin, W., Cizek, G.R., Haacke, E.M., 1996. In vivo regional cerebral blood volume: quantitative assessment with 3D T1-weighted pre-and postcontrast MR imaging. Radiology 201, 106–112. Lear, J.L., Kasliwal, R., Feyerabend, A., 1990. Mapping regional cerebral vascular transit time by simultaneous determination of local cerebral blood flow and local cerebral blood volume. Metab. Brain Dis. 5, 155–165. Leggett, R., Williams, L., 1991. Suggested reference values for regional blood volumes in humans. Health Phys. 60, 139–154. Li, W., Tutton, S., Vu, A.T., Pierchala, L., Li, B.S., Lewis, J.M., Prasad, P.V., Edelman, R.R., 2005. First‐pass contrast‐enhanced magnetic resonance angiography in humans using ferumoxytol, a novel ultrasmall superparamagnetic iron oxide (USPIO)‐based blood pool agent. J. Magn. Reson. Imaging 21, 46–52. Loubeyre, P., De Jaegere, T., Bosmans, H., Miao, Y., Ni, Y., Landuyt, W., Marchal, G., 1999. Comparison of iron oxide particles (AMI 227) with a gadolinium complex (Gd‐ DOTA) in dynamic susceptibility contrast MR imagings (FLASH and EPI) for both phantom and rat brain at 1.5 tesla. J. Magn. Reson. Imaging 9, 447–453. Moseley, M.E., Chew, W.M., White, D.L., Kucharczyk, J., Litt, L., Derugin, N., Dupon, J., Brasch, R.C., Norman, D., 1992. Hypercarbia‐induced changes in cerebral blood volume in the cat: a 1H MRI and intravascular contrast agent study. Magn. Reson. Med. 23, 21–30. Pathak, A.P., Ward, B.D., Schmainda, K.M., 2008. A novel technique for modeling susceptibility-based contrast mechanisms for arbitrary microvascular geometries: the finite perturber method. Neuroimage 40, 1130–1143. Pauly, J., Conolly, S., Nishimura, D., Macovski, A., 1989. Slice-Selective Excitation for Very Short T2 Species. Proceedings of SMRM, p. 28. 389 Phelps, M., Huang, S., Hoffman, E., Kuhl, D., 1979. Validation of tomographic measurement of cerebral blood volume with C-11-labeled carboxyhemoglobin. J. Nucl. Med. (U. S. A.) 20. Powers, W.J., Raichle, M.E., 1985. Positron emission tomography and its application to the study of cerebrovascular disease in man. Stroke 16, 361–376. Prinster, A., Pierpaoli, C., Turner, R., Jezzard, P., 1997. Simultaneous measurement of ΔR2 and ΔR2* in cat brain during hypoxia and hypercapnia. Neuroimage 6, 191–200. Risberg, J., Lundberg, N., Ingvar, D.H., 1969. Regional cerebral blood volume during acute transient rises of the intracranial pressure (plateau waves)*. J. Neurosurg. 31, 303–310. Robson, M.D., Gatehouse, P.D., Bydder, M., Bydder, G.M., 2003. Magnetic resonance: an introduction to ultrashort TE (UTE) imaging. J. Comput. Assist. Tomogr. 27, 825–846. Schenck, J.F., 1996. The role of magnetic susceptibility in magnetic resonance imaging: MRI magnetic compatibility of the first and second kinds. Med. Phys. 23, 815–850. Schwarzbauer, C., Syha, J., Haase, A., 1993. Quantification of regional blood volumes by rapid T1 mapping. Magn. Reson. Med. 29, 709–712. Schwarzbauer, C., Morrissey, S.P., Deichmann, R., Hillenbrand, C., Syha, J., Adolf, H., Nöth, U., Haase, A., 1997. Quantitative magnetic resonance imaging of capillary water permeability and regional blood volume with an intravascular MR contrast agent. Magn. Reson. Med. 37, 769–777. Spetzler, R., Wilson, C., Weinstein, P., Mehdorn, M., Townsend, J., Telles, D., 1977. Normal perfusion pressure breakthrough theory. Clin. Neurosurg. 25, 651–672. Toyama, H., Takeshita, G., Takeuchi, A., Anno, H., Ejiri, K., Maeda, H., Katada, K., Koga, S., Ishiyama, N., Kanno, T., 1990. Cerebral hemodynamics in patients with chronic obstructive carotid disease by rCBF, rCBV, and rCBV/rCBF ratio using SPECT. J. Nucl. Med. (U. S. A.) 31. Tropres, I., Grimault, S., Vaeth, A., Grillon, E., Julien, C., Payen, J.F., Lamalle, L., Decorps, M., 2001. Vessel size imaging. Magn. Reson. Med. 45, 397–408. Warach, S., Li, W., Ronthal, M., Edelman, R., 1992. Acute cerebral ischemia: evaluation with dynamic contrast-enhanced MR imaging and MR angiography. Radiology 182, 41–47. Weissleder, R., Elizondo, G., Wittenberg, J., Rabito, C., Bengele, H., Josephson, L., 1990. Ultrasmall superparamagnetic iron oxide: characterization of a new class of contrast agents for MR imaging. Radiology 175, 489–493. Wu, E.X., Tang, H., Jensen, J.H., 2004a. Applications of ultrasmall superparamagnetic iron oxide contrast agents in the MR study of animal models. NMR Biomed. 17, 478–483. Wu, E.X., Tang, H., Asai, T., Yan, S.D., 2004b. Regional cerebral blood volume reduction in transgenic mutant APP (V717F, K670N/M671L) mice. Neurosci. Lett. 365, 223–227. Yablonskiy, D.A., Haacke, E.M., 1994. Theory of NMR signal behavior in magnetically inhomogeneous tissues: the static dephasing regime. Magn. Reson. Med. 32, 749–763.








© Copyright 2026