
How to Prepare for Your Health Screening Medical
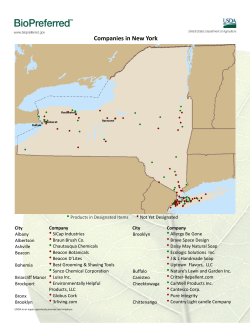
How to Prepare for Your Health Screening Medical Thank you again for booking an Executive Medical. Your visit will last about three hours and we would ask that you please aim to arrive 15 minutes prior to your appointment time to complete your registration. We have enclosed a questionnaire which you will need to complete and bring with you on the day of your medical. If you previously visited us for a medical, we would ask that you just include any updated medical details since your previous visit. Please also take the time to look through the directions to The Well which we have enclosed. If you have any problems finding us on the day, please do not hesitate to call us on (01) 294 5444 for further assistance. In addition please note the following preparation required: Fasting You will need to fast for 12-14 hours before your medical. The reason for this is that certain test values may change after you eat such as blood sugar. It is important to drink water while fasting but no juice, tea or coffee and avoid smoking, chewing gum or exercising all of which may alter the test results. If you have conditions such as diabetes or other conditions which may be affected by fasting, please call us on 01-2945444 in advance for further information Medication If you are on medication, please continue taking it but be sure to bring the name of it with you as sometimes it can affect the blood results FOB Kit (Faecal Occult Blood test) If you are over 50, an FOB kit will be sent to you in the post prior to your medical. The FOB test is used to check for blood in the stool which could potentially be a sign of colorectal abnormalities. Detailed instructions will be included as to how to use. If your booking is confirmed less than 5 days before your medical, we will provide you with am FOB kit on the day of the medical which will need to be returned at a later date. Glasses or corrective lenses If you wear either, please remember to bring glasses or spare contacts as you will be required to take out your contacts for a specific test. Body lotion Please refrain from applying body lotion on the morning of your appointment as it may prevent the ECG pads from sticking Questionnaire Please complete your medical questionnaire in advance of your medical. It is very important to do this as it will start preparing you for the medical and it will also ensure that your medical starts on time. What to wear Please wear whatever you are comfortable wearing. If you have any questions about the above, please do not hesitate to contact us on 01-2945444 or by email [email protected] Your Day With Us The day of your appointment On arrival in ‘The Well’ at the appointed time, you will be welcomed by our receptionist who will confirm your details and complete the registration process. You will be then be brought to your room, where you will be based for the duration of your appointment. Meeting with the nurse The medical starts with a meeting with one of our specialist nurses who you will be with for about 75 minutes. o o o o o o o o The consultation will start with your nurse taking a sample of blood which will be sent to the lab immediately She will then go through your completed questionnaire and take a full personal and medical history. The next stage involves the nurse taking your blood pressure, heart rate, weight, height, and body mass index measurement You will be asked to provide a urine sample for urinalysis to check liver and kidney function and for infection A heart assessment (Resting ECG) will then be performed You will be asked to perform our Spirometry test to check lung function An eye test is also completed to check visual acuity (Keystone), near and far vision, and a separate test to screen for glaucoma risks (Tonometry) Towards the end of the nurses consultation, you will complete a hearing test that will be carried out in our Audiometry booth Age based tests: o o A DEXA bone scan to screen for Osteoporosis will be performed on women over the age of 40 An FOB test to detect blood in the stools will have been provided for those over the age of 50 Once the consultation with the nurse is completed, you will be provided with a healthy breakfast or a light lunch depending on the time of the day. Doctor Consultation The final part of the medical is a meeting with one of our doctors who will be with you for an hour. o o o The doctor will complete a head to toe physical examination including a breast or prostate / colorectal examination as appropriate He / she will go through and explain the results of all the tests and the assessments carried out including the blood results. The doctor will also chat to you about any particular medical concerns that you may have – it is important to note these concerns on your questionnaire in advance of your medical as you may be too busy to remember on the day. Appropriate Diagnostic tests Based on the results of the medical and following the consultation with your doctor, additional appropriate diagnostic tests may be completed. Where possible, these will be arranged for the same day or as quickly as possible afterwards. You should note that all additional tests incur an additional cost so please discuss this with our doctor or receptionist in advance of completing the test. The most common additional diagnostic tests are as follows: Exam / Test Catalyst Cost CT Scan- Angiography Based on cardiac risk profile 650 Based on clinical examination and / or & risk profile 360 Based on risk profile as determined by sleep questionaire 300 CT Scan of Brain/Chest/Thorax/Abdomen/Pelvis (+IV Contrast) Sleep Apnoea Course Urine C & S (R) 24 Hour Blood Pressure Monitor Based on urinalysis containing blood / leucocytes / protein / glucose Based on BP x 3 over 140/90. Generally instructed to repeat with GP beforehand 55 150 Testicular Ultrasound Based on clinical examination 175 Breast Ultrasound Based on clinical examination and / or age & risk profile 180 Ultrasound - Thyroid Based on clinical examination 175 Pelvis/Abdominal Ultrasound Based on clinical examination 175 Xray (single) Based on clinical examination 120 Mammogram - Beacon Based on clinical examination and / or age & risk profile 190 MRI Scan Based on clinical examination 480 Full STI Screening Optional Extra 40 ‘Many of the above tests are not reimbursable by your health insurer at the above locations but you should mention to The Well Doctor and receptionist what plan you have and they will investigate your options in advance of having the test performed. You can also visit the following websites to see your entitlements in advance’ www.vhi.ie - www.quinn-healthcare.com - www.aviva.ie/online/health Med 1 form – Claiming back against personal taxes If you are paying taxes under the PAYE system, it is possible to claim the cost of certain medical expenses, including health screening, back against your personal taxes at the end of the year. As from Jan 1st 2009, the relief is granted at 20% on cumulative medical expenses over €125. Other costs that are covered under this benefit include GP consultations, prescribed drugs and medications so it is easy enough to reach this threshold of €125. Follow-up report A full and detailed report is sent out within 10 days following the medical including a personalised lifestyle plan and materials to promote a healthy lifestyle. The report is developed by the nurse and doctor and includes a summary of the results of the tests, recommendations from the doctor and nurse and a detailed and scientifically valid exercise and nutrition prescription designed with the input from our lifestyle consultants. With the consent of the visitor, a copy of the report is also sent to their own GP, their primary health care provider to ensure continuity of care. Male Executive Medical Questionnaire EXECUTIVE MEDICAL QUESTIONNAIRE Please complete this confidential questionnaire as fully as possible and bring it with you to your appointment. Doctor’s notes First name: Surname: Date of birth: Home address: Home telephone no.: Work telephone no.: Mobile no.: Are you: E-mail: Single Married Divorced Separated Widowed Living with a partner What is your main reason for attending ‘The Well’? Review of Health Specific Medical Problem Company related If company related, what is the name of your company? If you have any particular health concerns, please note them below: If you would like your doctor to receive a copy of your report, please give their name, phone number and address: Name: Phone: Address: If you have private health insurance, which company are you with? Vhi Quinn Healthcare Hibernian Aviva Health Other None Where did you hear about us? Would you like to receive a copy of our e newsletter & details of our special offers Yes No OCCUPATIONAL HISTORY Are you currently employed outside of the home? Yes Do you work: Full-time Part-time Are you: Self-employed Retired No If you are not already retired, please complete the following: What is your current occupation? Please give details of what your position entails: Do you currently find your work fulfilling? Yes No 1 LIFESTYLE BACKGROUND SMOKING Are you: A current smoker Do you/did you smoke: Cigarettes Ex-smoker Never Smoked Doctor’s notes Cigars Pipe Other If yes, on average how many do/did you smoke daily? If you have given up smoking, how many years ago did you stop? years For how many years have you been a smoker? years ALCOHOL Please give details of your typical weekly alcohol consumption: (1 standard drink is roughly 1/2 pint of beer, 1 (100ml) glass of wine or 1 (30ml) measure of a spirit) Beer Wine Spirits None Total no. of Standard drinks Are you concerned about the effect of alcohol on your: Physical health Yes No Psychological health (incl. memory, concentration, moods) Yes No Social well-being Yes No Family life Yes No Work life Yes No How often in a normal week would you drink alcohol? How many drinks do you have on a typical day when you are drinking? How often do you have six drinks or more on any one occasion? DRUGS Do you take any of the following? Sleeping tablets Pain Killers Cannabis Cocaine Other: EXERCISE AND HOBBIES Please detail your hobbies, interests and passions: Please describe your average weekly exercise pattern: 2 FAMILY MEDICAL HISTORY Are you aware of your family medical history? If yes, it is very helpful for us to know the following: Current age Or age at death Yes No State of health/cause of death Doctor’s notes Father Mother Partner/Spouse Brothers Sisters Daughters Sons Do you have any other particular concerns about your family medical history such as incidence of bowel, prostate or skin cancer, thyroid disease, mental health or sudden death under the age of 60? MEDICAL HISTORY Please list any history of past significant illnesses or medical conditions (eg. High blood pressure, raised cholesterol), injuries or accidents - Please list the most recent first: Please list any hospital admissions and the reason for admission - Please list the most recent first: Please detail any investigations/procedures that you may have undergone (endoscopy, colonoscopy or any other day case procedure): Please list any medications you are taking and how long you have been taking them: Please list any allergies (in particular to medications) you may have: 3 WELL-BEING Would you describe yourself as generally being a happy person? Yes No Persistent worrying Yes No Difficulty in making decisions Yes No Difficulty in relaxing Yes No Difficulty concentrating Yes No Disrupted sleep pattern Yes No Feeling unhappy and depressed Yes No Do you snore loudly? Yes No Do you snore every night? Yes No Have you ever been told that you hold your breath while sleeping? Yes No Have you recently experienced any of the following? Doctor’s notes Please give details of any particular concerns you may have: SLEEP PATTERN If yes to any of the above, please describe: Dozing Situation Chance of Dozing 0= would never doze 1= slight chance of dozing 2= moderate chance of dozing 3= high chance of dozing Sitting and reading Watching TV Sitting inactive in a public place (i.e. theatre or meeting) As a passenger in a car for an hour without a break Lying down to rest in the afternoon when circumstances permit Sitting talking to someone Sitting quietly after lunch without alcohol In a car, while stopped for a few minutes in traffic TOTAL SCORE DERMATOLOGY Do you have any previous/present skin problems such as eczema, psoriasis, acne etc? Yes No Is there any history of melanoma in your family? Yes No Do you have any moles on your skin that you are concerned about? Yes No Have you ever been severely sunburned? Yes No Do you have any moles that are unusual or changing? Yes No Does anyone in your family have osteoporosis? Yes No Have you had a fracture at low impact? Yes No If yes, please describe: MUSCULOSKELETAL 4 HEALTH QUESTIONS FOR MEN Do you regularly examine your testes? Yes No Have you noticed any lumps or swelling in your testes? Yes No Do you get up in the night to pass urine on a regular basis? Yes No Have you noticed any change in the flow rate or stream of your urine? Yes No Doctor’s notes If so, how many times? If yes, please describe: Have you ever had a PSA (Prostate Specific Antigen) blood test? Yes No Yes No If yes, when was the last time and what was the result? Have you ever had a digital rectal examination of the prostate? If yes, when was the last time and what was the result? I __________________________________ consent to having the below procedure(s) performed as discussed by the Doctor: DRE PSA – usually for those over 40 Testicular exam Signed: _____________________________________________ The above is to be signed in the presence of a clinician. Do you have any problems with sexual function? Yes No Do you have any problems with erectile function? If yes, please give details: Yes No Do you have any concerns regarding sexually transmitted diseases? Yes If yes, please describe: No 5 CLINICAL FINDINGS – (For office use only) LIFESTYLE NOTES Weight: Height: Target Weight: Waist Measure: Body Fat %: Target Fat %: BMI: Hip Measure: Ratio: Water %: Diet: Exercise: Weight Management: Fitness Score: Flexibility Score: Core Stability Score: BP: HR: CLINICAL NOTES Bloods: Yes No PSA: Yes No TSH: Yes No Any Additional Tests: Coronary CT Angio booked: Yes No CT CA booked : Yes Keystone: Yes No If not why? Tonometry: Yes No If not why? Spirometry: Yes No If not why? Audiometry: Yes No If not why? Urinalysis: Yes No If not why? FOB kit given: Yes No If not why? No Result: +: -: Note: Stress Level: Additional notes: Any areas of concern: 6 CNS/PNS REVIEW Headaches/Migraines Visual disturbance, hearing RESPIRATORY REVIEW Shortness of breath Wheezing CARDIOVASCULAR REVIEW Chest pain (symptoms) Palpitations GASTROINTESTINAL REVIEW Acid reflux/Heartburn/indigestion Altered bowel habit Blood in the bowel motion GENITO-URINARY REVIEW Frequency of urine Prostatism MUSCULOSKELETAL REVIEW Any Joint problems SKIN REVIEW Any skin problems Moles PHYSICAL RESULTS Head and Neck ENT Respiratory Heart Carotids Peripheral Pulses Abdomen DRE Genitals Neurological Low Med High Yes No Yes CVS Risk CT Angio Mole Mapping Osteoporosis Risk Dexa Other Investigations OSA Risk Sleep Study No 7 Notes 8 Beacon Consultants Clinic Sandyford Dublin 18 Ireland Phone: +353 1 294 5444 Fax: +353 1 294 5466 [email protected] www.thewell.ie Vhi SwiftCare Clinic The Plaza, City Gate Mahon Cork Phone: 1800 928820 Fax: +353 21 240 9400 [email protected] www.thewell.ie Patient Name: Date of Birth: Date of Visit: The Well Lifestyle Questionnaire Yes No Yes No Yes No Dietary Habits Are you currently trying to lose weight? Are you on a specific diet/weight loss regime? Give detail of what diets if any you have tried in the past Are you happy with your weight? If yes, explain Do have any specific dietary requirements like Coeliac Disease, Diabetes or any food intolerances? Have you ever had raised Cholesterol? If yes are you on medication for same? Which do you think best describes your current eating pattern? Tick appropriate Grazing and nibbling throughout the day Often skipping meals Three meals a day Three meals a days plus snacks Eating out more than twice a week Never have breakfast Food intake breakdown How many times a week (out of 21 meals) would you eat the following? Red Meat Fish Chicken Ready Prepared meals Eating out in Restaurants Takeaways Give an example of an average day’s food intake for you Breakfast No. of times per week Lunch Dinner Dairy products (ring appropriate full or low fat) No. of times per week How many times a week do you consume the following? Full fat Low Fat Milk Full/Low fat Butter Full/Low fat Cheese Full/Low fat Yogurt Full/Low fat Do you take cream? If yes, how many times a week? Fruit and Vegetables (portion=1 piece of fruit/1 large serving spoon of Vegetables) No. per day How many portions of fruit would you have a day? How many portions of vegetables would you have a day? Snacks No. per day How often do you snack each day? Give examples of what you snack on Junk Food How often would you eat the following each week? No. of times per week Crisps Chocolate Chips Sweets Liquid intake How many glasses/cups of the following do you have each day: No. per day Water Juice Tea Coffee Herbal/Fruit Tea Fizzy drinks Alcohol On a weekly basis, how many glasses/pints do you drink each week? Glasses of wine Pints of beer Spirits No. of glasses/pints per week Smoking Have you ever smoked? Yes No Ex Yes No Type Do you presently smoke? Cigarettes/Cigars How many do you smoke a day? Would you like to give up smoking? Have you ever attempted to give up smoking? Years How long have you given up? What methods have you tried Exercise. Do you feel you……? Tick appropriate Take enough exercise Need to take more exercise Do not have time to take exercise Do not need to exercise How to Rate Your Activity Level Tick appropriate • Very low activity. You spend most of your day sitting. You rarely exercise. • Low activity. You work in an office, but your day includes some walking, bicycling, or stairclimbing. Or you exercise at least 20 to 45 minutes at least once a week. • Moderate activity. Your daily routine involves walking or standing most of the day or includes some brisk or uphill walking or some lifting. Or you exercise at least 20 to 45 minutes about three times a week. • Very good level of activity. Your daily routine keeps you moving most of the time or includes some running, heavy lifting, or swimming. Or you exercise at least 20 to 45 minutes every day. • Exceptional activity. You're unstoppable. You're training daily for an athletic event, or you're a professional dancer or athlete with a strenuous schedule. What would be your regular exercise regime - give details: Nurse use only: Weight kg: Target Weight: Body Fat%: Target Fat%: Water: Target Water%: Waist: Hip: BP Pulse FOB MSU Additional Notes: Height cm: WH Ratio: Smear BMI: Directions to ‘The Well’ at the Beacon Consultants Clinic Directions from the M50 South Bound • Take the Sandyford/Dundrum exit from the M50 - North Bound • Take the Sandyford exit to the M50 Exit 13 • Take the third turn off the roundabout towards • Cross the bridge over the M50 Sandyford • Turn left at the next set of traffic lights (at the roundabout) and get into the right hand side lane • At the next set of traffic lights turn right, ("Beacon Hotel" on your right). • Take the first right on to Blackthorn Road (after about 100metres). • About 20m down on the right hand side is an entrance to the underground car park (Beacon Hotel/Court/Clinic/Hospital car park) • You will be directed to the visitors parking area. Take the stairs up to ground level and follow the signs for the Beacon Clinic, which is in the adjacent building • 'The Well' is on the ground floor of the Beacon Clinic Coming from the N11 (Southbound towards Bray – from the City centre) • Follow the N11 southbound through Donnybrook and Stillorgan • After passing the Stillorgan Park Hotel (on the left) and the Stillorgan village junction, turn right at the next lights (St John of God hospital on the left hand side) onto Brewery Road • At the end of Brewery Road, take the fourth exit off the roundabout, heading into the Sandyford Industrial Estate • At the T -junction at the end of this road, (grey Avid building in front of you) turn left onto Blackthorn Road • Just before the end of the road on the left hand side is an entrance to an underground car park (Beacon Hotel/Court/Clinic/Hospital car park). Follow the signs to the Beacon Clinic and ‘The Well’ is located in the ground floor Coming from the N11 (Northbound towards Dublin) • Follow the N11 toward Dublin. • After passing Foxrock Church (on the right), at the next traffic lights turn left - onto Leopardstown Road • At the end of Leopardstown Road (Racecourse on your left) take 3rd exit off the roundabout, heading into the Sandyford Industrial Estate • At the T -junction at the end of this road, (grey Avid building in front of you) turn left onto Blackthorn Road • Just before the end of the road on the left hand side is an entrance to an underground car park (Beacon Hotel/Court/Clinic/Hospital car park) Coming from Dundrum village via Kilmacud Road Upper • At the Dundrum village crossroads, take the Upper Kilmacud Road towards the Sandyford Estate • At the fourth set of traffic lights, turn right onto the new road • At the next lights (Beacon Hotel across the junction, on your left), turn left • Take the next right onto Blackthorn Road (opposite the Alo Kavanagh Mercedes Garage) • About 20m down on the right hand side is an entrance to an underground car park (Beacon Hotel/Court/Clinic/Hospital car park) By LUAS – on foot only Going towards Sandyford Going towards Town • Disembark at the "Kilmacud" LUAS stop • Walk up the stairs and follow the path to the road • Turn left and continue up the road to the 2 traffic lights • Disembark at the "Kilmacud" LUAS stop nd set of • Walk up the stairs and follow the path to the road • Turn right and continue up the road to the traffic lights • Turn left and walk until the next set of traffic lights • At the traffic lights, turn left passing the Beacon Hotel on your right and turn right onto Blackthorn road. • Take the first turn to the right onto Bracken Road and continue up the road for about 300m • There is an entrance to Beacon Court on the right hand side (sand coloured walls with water coming down the walls and flags at the entrance) • Go through the security barrier and continue down the avenue • The Beacon Clinic is the last building on your left hand side • 'The Well' is located on the ground floor of the Beacon Clinic If you have any problems finding us, please call us on 01-2945444 and we will direct you further Mount Anville Rd Taney Rd Dundrum Town Centre GOAT PUB Lower Kilmacud Rd Balally S.C BEACON HOTEL KILMACUD LUAS STOP MERCEDES BENZ B L AC K T The Well BEACON CLINIC HORN D LONDIS RIVE LUAS PARKING ENTRANCE TO CAR PARK Bracken Rd MICROSOFT STILLORGAN LUAS STOP LUAS PARKING AVID BLACKTHORN AVENUE Heather Rd BLACKTHORN ROAD Furze Rd Kilmacud Rd LUAS line BLACKTHORN ROAD AIB SANDYFORD LUAS STOP Arena Rd and y fo rd WOODIES DIY EXIT 13 M50 BURTON HALL ROAD to S AD Y RO WER BRE Central Park Bewleys Hotel RACECOURSE Business Park The Well, Beacon Clinic, Sandyford Industrial Estate, Dublin 18 Ph: 01-2945444 Fax: 01-2945466 Email: [email protected] www.thewell.ie N11 M50 DRUMMARTIN LINK ROAD VHI SWIFTCARE BALALLY LUAS STOP Kilmacud Rd Upper BEACON HOSPITAL AND CLINICS VISITOR MAP Beacon Consultants Clinic Suites 1-32 The Avenue - Advanced Radiology - Beacon Dental Clinic - Beacon Eye Clinic - Cancer Support Centre - The Well Beacon Consultants Concourse Suites 1-12 Second Floor The Concourse Building Beacon Hall Suite 36 - Beacon Dermatology - Beacon Medical Group - Motivation Weight Management Clinic - Sandra Cummings (Audiologist) - Wellington Eye Clinic THE AVENUE Advanced Radiology Reception Suite 8 SOUTH MALL Pharmacy Monday - Friday 8.30am to 6pm NORTH MALL THE CONCOURSE Beacon Hotel Beacon Renal Suite 35 Lift Pharmacy Beacon Hospital First Floor Revolving Door Information Desk Hospital Entrance Beacon Hospital Reception Lobby Information Graphic by LoinesFurnival © 2007 www.l-f.co.uk Main Entrance Photo Guided Tour Photo Walk Through Directions from the Lift From Blackthorn Road, turn into the Beacon car park. Turn right and go through the barrier. Keep the security room on your left hand side Park and walk to the “Beacon Court Entrance” Take the lift to the Concourse Level by Pressing “0” On exiting the lift, turn left into the Concourse (common seating area) Walk to the far right hand side of the open area to the revolving door. Walk through the revolving door Walk until you get to the miniature model of the Beacon Complex Turn right at the model and go through the door The Beacon Consultant Clinic is straight ahead. The Well is located on the ground floor of the Clinic










© Copyright 2026